Auriculotherapy for Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials Gary N. Asher, MD, MPH, 1,2 Daniel E. Jonas, MD, MPH, 3 Remy R. Coeytaux, MD, PhD, 4 Aimee C. Reilly, LAc, 1 Yen L. Loh, MD, 1 Alison A. Motsinger-Reif, PhD, 5 and Stacey J. Winham, MS 5 Abstract Objectives: Side-effects of standard pain medications can limit their use. Therefore, nonpharmacologic pain relief techniques such as auriculotherapy may play an important role in pain management. Our aim was to conduct a systematic review and meta-analysis of studies evaluating auriculotherapy for pain management. Design: MEDLINE, Ò ISI Web of Science, CINAHL, AMED, and Cochrane Library were searched through December 2008. Randomized trials comparing auriculotherapy to sham, placebo, or standard-of-care control were included that measured outcomes of pain or medication use and were published in English. Two (2) reviewers independently assessed trial eligibility, quality, and abstracted data to a standardized form. Standardized mean differences (SMD) were calculated for studies using a pain score or analgesic requirement as a primary outcome. Results: Seventeen (17) studies met inclusion criteria (8 perioperative, 4 acute, and 5 chronic pain). Aur- iculotherapy was superior to controls for studies evaluating pain intensity (SMD, 1.56 [95% confidence interval (CI): 0.85, 2.26]; 8 studies). For perioperative pain, auriculotherapy reduced analgesic use (SMD, 0.54 [95% CI: 0.30, 0.77]; 5 studies). For acute pain and chronic pain, auriculotherapy reduced pain intensity (SMD for acute pain, 1.35 [95% CI: 0.08, 2.64], 2 studies; SMD for chronic pain, 1.84 [95% CI: 0.60, 3.07], 5 studies). Removal of poor quality studies did not alter the conclusions. Significant heterogeneity existed among studies of acute and chronic pain, but not perioperative pain. Conclusions: Auriculotherapy may be effective for the treatment of a variety of types of pain, especially post- operative pain. However, a more accurate estimate of the effect will require further large, well-designed trials. Introduction P ain affects more Americans than diabetes, heart dis- ease, and cancer combined, 1 and accounts for more than 20% of medical visits and 10% of prescription drug sales. 2 One of the most common approaches to managing pain relief, the World Health Organization analgesic ladder, 3 details the use of both opioid and nonopioid medications in a stepwise fashion. However, up to 80% of patients receiving opioid medications experience at least one adverse event, most commonly constipation (41%), nausea (32%), or somnolence (29%); the number needed to harm for these common events is between three and five. 4 Additionally, gastrointestinal toxic- ity related to the use of nonsteroidal anti-inflammatory drugs (NSAID) is estimated to cause more than 100,000 hospitali- zations and over 16,000 deaths annually in the United States. 5 Cardiovascular risk is also elevated with use of most NSAIDs. 6 For these reasons, methods of nonpharmacologic pain relief, such as acupuncture, mind–body interventions, and manipulative therapies, have been advocated as adjuncts to pharmacologic therapy. 7–9 Acupuncture has been shown to be effective for pain relief due to a variety of causes including low back pain, 10,11 oste- oarthritis, 12 and headache. 13 Auriculotherapy is an adjunct to 1 Department of Family Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC. 2 Program on Integrative Medicine, Department of Physical Medicine and Rehabilitation, University of North Carolina at Chapel Hill, Chapel Hill, NC. 3 Department of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC. 4 Department of Community and Family Medicine, Duke University, Durham, NC. 5 Department of Statistics, North Carolina State University, Raleigh, NC. THE JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINE Volume 16, Number 10, 2010, pp. 1097–1108 ª Mary Ann Liebert, Inc. DOI: 10.1089/acm.2009.0451 1097

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Auriculotherapy for Pain Management:A Systematic Review and Meta-Analysis
of Randomized Controlled Trials
Gary N. Asher, MD, MPH,1,2 Daniel E. Jonas, MD, MPH,3 Remy R. Coeytaux, MD, PhD,4
Aimee C. Reilly, LAc,1 Yen L. Loh, MD,1 Alison A. Motsinger-Reif, PhD,5 and Stacey J. Winham, MS5
Abstract
Objectives: Side-effects of standard pain medications can limit their use. Therefore, nonpharmacologic pain relieftechniques such as auriculotherapy may play an important role in pain management. Our aim was to conduct asystematic review and meta-analysis of studies evaluating auriculotherapy for pain management.Design: MEDLINE,� ISI Web of Science, CINAHL, AMED, and Cochrane Library were searched throughDecember 2008. Randomized trials comparing auriculotherapy to sham, placebo, or standard-of-care control wereincluded that measured outcomes of pain or medication use and were published in English. Two (2) reviewersindependently assessed trial eligibility, quality, and abstracted data to a standardized form. Standardized meandifferences (SMD) were calculated for studies using a pain score or analgesic requirement as a primary outcome.Results: Seventeen (17) studies met inclusion criteria (8 perioperative, 4 acute, and 5 chronic pain). Aur-iculotherapy was superior to controls for studies evaluating pain intensity (SMD, 1.56 [95% confidence interval(CI): 0.85, 2.26]; 8 studies). For perioperative pain, auriculotherapy reduced analgesic use (SMD, 0.54 [95% CI:0.30, 0.77]; 5 studies). For acute pain and chronic pain, auriculotherapy reduced pain intensity (SMD for acutepain, 1.35 [95% CI: 0.08, 2.64], 2 studies; SMD for chronic pain, 1.84 [95% CI: 0.60, 3.07], 5 studies). Removal ofpoor quality studies did not alter the conclusions. Significant heterogeneity existed among studies of acute andchronic pain, but not perioperative pain.Conclusions: Auriculotherapy may be effective for the treatment of a variety of types of pain, especially post-operative pain. However, a more accurate estimate of the effect will require further large, well-designed trials.
Introduction
Pain affects more Americans than diabetes, heart dis-ease, and cancer combined,1 and accounts for more than
20% of medical visits and 10% of prescription drug sales.2 Oneof the most common approaches to managing pain relief,the World Health Organization analgesic ladder,3 details theuse of both opioid and nonopioid medications in a stepwisefashion. However, up to 80% of patients receiving opioidmedications experience at least one adverse event, mostcommonly constipation (41%), nausea (32%), or somnolence(29%); the number needed to harm for these common events is
between three and five.4 Additionally, gastrointestinal toxic-ity related to the use of nonsteroidal anti-inflammatory drugs(NSAID) is estimated to cause more than 100,000 hospitali-zations and over 16,000 deaths annually in the United States.5
Cardiovascular risk is also elevated with use of mostNSAIDs.6 For these reasons, methods of nonpharmacologicpain relief, such as acupuncture, mind–body interventions,and manipulative therapies, have been advocated as adjunctsto pharmacologic therapy.7–9
Acupuncture has been shown to be effective for pain reliefdue to a variety of causes including low back pain,10,11 oste-oarthritis,12 and headache.13 Auriculotherapy is an adjunct to
1Department of Family Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC.2Program on Integrative Medicine, Department of Physical Medicine and Rehabilitation, University of North Carolina at Chapel Hill,
Chapel Hill, NC.3Department of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC.4Department of Community and Family Medicine, Duke University, Durham, NC.5Department of Statistics, North Carolina State University, Raleigh, NC.
THE JOURNAL OF ALTERNATIVE AND COMPLEMENTARY MEDICINEVolume 16, Number 10, 2010, pp. 1097–1108ª Mary Ann Liebert, Inc.DOI: 10.1089/acm.2009.0451
1097

traditional acupuncture and over the last 60 years has devel-oped into a distinct treatment system of its own. It is based ona set of anatomical maps superimposed onto the ear. Stimu-lating a point on the map is proposed to affect the grossanatomical organ associated with that point. For the ear, au-ricular points may be stimulated with needles (auricularacupuncture); Vaccaria seeds, probes, or fingers (acupressure);electrical units attached to auricular needles (percutaneouselectrical nerve stimulation) or directly to the skin (TENS—transdermal electrical nerve stimulation or auricular electro-acupuncture); or laser; all of which may be considered formsof auriculotherapy.
Early studies of auriculotherapy have demonstrated bene-ficial effects on both pain and anxiety including pain associ-ated with cancer,14 knee arthroscopy,15 and hip fracture andhip arthroplasty.16 Several recent small studies have sug-gested that auricular acupuncture alone can relieve pain andanxiety in the prehospital transport phase of hip fracture16,17
and reduce acute pain due to a variety of causes in theemergency department setting.18 Recently, a systematic re-view of auriculotherapy for perioperative pain concluded thatthe evidence for efficacy was ‘‘promising but not compel-ling.’’19 However, because auriculotherapy is currently usedin a wide range of acute and chronic pain conditions beyondthe perioperative period, it is important to assess its clinicalutility in general. Therefore, in this review our primary ob-jective was to conduct a systematic review and meta-analysisof the efficacy of auriculotherapy for all types of pain. Wepresent these data as a whole and also by category of pain(perioperative, acute, and chronic).
Materials and Methods
Data sources and searches
We searched MEDLINE,� Cochrane Database of Systema-tic Reviews, Cochrane Central Register of Controlled Trials,AMED, ISI Web of Science, and CINAHL from inceptionthrough December 2008, using the following terms: ‘‘auricularacupuncture,’’ ‘‘ear acupuncture,’’ and ‘‘auriculotherapy.’’ Welimited the electronic searches to human subjects and, due toresource constraints, English language. We attempted toidentify additional studies through hand searches of referencelists, as well as our own files. All citations were imported intoan electronic database (Endnote v. X1).
Study selection
Trials were included if they (1) were randomized; (2)compared auriculotherapy to sham auriculotherapy control,standard medical care, or waiting-list control; (3) measuredthe effect on pain or medication use; (4) and were published inEnglish in a peer-reviewed journal. We chose to excludestudies that compared auriculotherapy to a nonauricul-otherapy active control treatment that did not have clearevidence of efficacy. Two (2) reviewers independently as-sessed titles and abstracts, which were excluded only if bothreviewers agreed that the trial did not meet eligibility criteria.Full-text articles of remaining citations were retrieved andassessed for inclusion by 2 reviewers. Disagreements wereresolved by consensus. Results published only in abstractform were not included unless adequate details were avail-able for quality assessment.
Data abstraction and quality (internal validity)assessment
We designed and used a structured data abstraction form.Trained reviewers abstracted data from each study and as-signed an initial quality rating. A second reviewer read eachabstracted article, evaluated the completeness of the dataabstraction, and confirmed the quality rating. Differences inquality ratings were resolved by discussion or by involving athird senior reviewer. The following data were extracted:study design, setting, population characteristics (includingage, sex, and race), inclusion and exclusion criteria, inter-ventions, comparisons, additional medications or interven-tions allowed, outcome assessments, attrition, withdrawalsattributed to adverse events, results, and adverse events re-ported. We recorded intention-to-treat results if available.
For the auriculotherapy interventions, we abstracted de-tails based on the STRICTA (Standards for Reporting Inter-ventions in Controlled Trials of Acupuncture) criteria for thereporting of acupuncture trials,20 including point selectionmethod, point locations, number of points per ear, needletype, use of electrical or laser stimulation, number of treat-ments, treatment frequency, and duration of each treatment.We also abstracted data on the practitioner type, years ofexperience, and acupuncture style. For the control interven-tion, we abstracted similar details. The country of the studywas also recorded.
We assessed the quality of trials based on the criteria of theU.S. Preventive Services Task Force and the National HealthService Centre for Reviews and Dissemination (U.K.).21,22
Quality assessment elements included randomization meth-od, allocation concealment, and blinding; similarity of com-pared groups at baseline; maintenance of comparablegroups; reporting of dropouts, crossover, adherence, andcontamination; overall and differential loss to follow-up; andintention-to-treat analysis. Attrition was defined as thenumber of randomized subjects who did not reach the studyendpoint.23
Trials that met all criteria were rated ‘‘good quality,’’ whilethose that failed to meet combinations of items were rated‘‘poor quality.’’ The remainder received a quality rating of‘‘fair.’’ This includes studies that presumably fulfilled allquality criteria but did not report their methodologies to anextent that answered all of our questions. As the fair-qualitycategory is broad, studies with this rating vary in theirstrengths and weaknesses. A poor-quality trial is not likely tobe valid—the results are at least as likely to reflect flaws in thestudy design as the true difference between the interventionand control.
Data synthesis and analysis
We summarized the overall strength of evidence for theefficacy of auriculotherapy for each set of pain indications intoevidence profiles. The overall strength of evidence for a par-ticular key question reflects the design, quality, consistency,and magnitude of effect of the set of studies relevant to thequestion. We rated the overall strength of evidence as low,moderate, high, or insufficient using an approach establishedby the Agency for Healthcare Research and Quality Evidence-Based Practice Centers.24 High strength of evidence indicateshigh confidence in the estimate of effect and that the evidencereflects the true effect; further research is unlikely to change
1098 ASHER ET AL.

our confidence. Moderate strength of evidence indicatesmoderate confidence, and further research may change ourconfidence in the estimate as well as the estimate itself. Lowstrength of evidence indicates low confidence in the estimateand further research is likely to change our confidence inthe estimate and is likely to change the estimate. Insufficientindicates that evidence is unavailable or does not permit es-timation of an effect.
Standardized mean differences (SMD) and 95% confidenceintervals (CI) were calculated for all comparisons. A stan-dardized mean difference refers to the raw difference in thesample treatment mean and the sample control mean dividedby the pooled standard deviation of both the treatment andcontrol groups. Because the times to study endpoints greatlyvaried among the studies, weighted mean differences werenot calculated. The use of the pooled standard deviation in theSMD accounts for the inconsistent study endpoints by placingthe treatment differences on the same comparable scale. SMDstherefore are not interpreted on the original scale, but areinterpreted in terms of number of standard deviations. Forexample, an SMD of 3.0 would mean that the treatment meanis approximately 3.0 standard deviations higher than thecontrol mean. Mean differences around 0.2 are often consid-ered small while those �0.8 are considered large.25 For ex-ample, a mean difference of 0.5 indicates that the mean of thetreated group is at the 69th percentile of the comparisongroup—a moderate effect—while a difference of 1.5 indicatesthat the mean of the treated group is at the 93% of the com-parison group—a large effect.
Study comparisons based on pain scales compared thestandardized difference in mean decrease in pain from base-line (to end of study) between the treatment and controlgroup. The numerical rating scale (NRS) was converted to a100-point scale for comparisons with the 100-point visualanalogue scale (VAS). Study comparisons based on painmedication use compared the percentage decrease in painmedication use between treatment and control groups. Wetested whether these decreases, in either pain scale or painmedication use, were significantly different from zero acrossstudies. For the overall meta-analysis comparing acupunctureto a control, only the studies that utilized a pain scale measurewere included because of concerns of comparability betweenthe pain scale and analgesic use outcomes. For all compari-sons, an SMD of zero indicates no difference between groups.
Study results were combined using the two-tailed p-valuesreported from each individual study. If a p-value was notreported, it was calculated from the reported standard error.Because study sample sizes and variances were not constant,reported differences were converted to standardized meandifferences; studies were weighted by the inverse of the studyvariance so that studies with lower variance received moreweight. A formal hypothesis test for heterogeneity was per-formed using Cochran’s Q statistic.26 As an alternative to Q,the inconsistency index I2 is reported,27 as well as t2,28 thebetween-study variance. Results for both random and fixed-effects models were calculated, but because significant het-erogeneity among studies was often found, we report theresults from random effects models only.29 To further inves-tigate heterogeneity, studies that employed multiple controlgroups14,30,31 were compared using the control group with theleast active intervention, and studies that used an activecontrol known to be efficacious for pain were excluded.32,33
Analysis was performed using the software package Com-prehensive Meta Analysis (www.meta-analysis.com).
Subgroup analyses were performed for perioperativestudies reporting pain medication use, studies of acute pain,and studies of chronic pain. Although other subgroups maybe important to consider, too few studies were available forsuch analyses.
Forest plots and funnel plots were created for the overallresults and for each subgroup analysis. Sensitivity analysiswas performed by removing each study and recalculatingthe overall results of the analysis. Cumulative analysis wasperformed to assess the possible treatment effect over time.Comparisons were performed with and without poor qualitystudies to assess the effect of study quality. This study wasapproved by the University of North Carolina institutionalreview board.
Results
Our search revealed 554 citations, of which 133 full-textarticles were reviewed. A total of 17 studies (1009 subjects) metour inclusion criteria (Fig. 1) and were included in the review.Attempts were made to contact the authors of an additionalthree publications that may have been eligible for inclusion butwere not because no replies were elicited.34–36 For 5 of the17 included studies, additional data were obtained from theauthors to enable inclusion in the meta-analysis.30–33,37 Four(4) studies included in the review were excluded from themeta-analysis due to incomplete data.17,38–40
The 17 included studies encompassed a wide variety ofauriculotherapy interventions (Table 1) including auricularneedles that were placed and removed after a single session(two studies); indwelling auricular needles that could remainin place for up to 30 days (six studies); electrical stimulation ofeither indwelling auricular needles (five studies) or transcu-taneously without needles (two studies); laser stimulation(one study); and acupressure (one study). Most studies usedeither a VAS (10/17) or measures of the amount of painmedication use (5/17) as a primary outcome measure. Theremaining studies used other measures, including a NRS andreports of ‘‘pain relief’’ or ‘‘pain decrease.’’
Thirty-five percent (6/17) of trials were rated as goodquality, 24% (4/17) were fair quality, and 41% (7/17) werepoor quality (see Appendix). Selection of auricular acupointswere varied among the studies based on the type and loca-tion of pain being treated; however, shenmen was the mostcommonly included point (10 studies) followed by thalamus(4). Visual inspection of the funnel plots for each comparisondid not indicate substantial publication bias. Table 1 liststype of intervention and control treatments, primary out-come measures, and acupoints for each study.
All pain types
Overall, 12 studies reported primary outcome effects infavor of auriculotherapy, 3 studies found mixed results (dif-ferent direction of outcomes for multiple outcome scales ormultiple times of outcome measurement), and 2 studies re-ported no difference between auriculotherapy and controlinterventions (Table 1). Of the 17 studies included in our re-view, 8 reported sufficient data for change in pain intensity tobe included in an overall meta-analysis; 3 studies that didreport on pain intensity did not provide enough data to be
AURICULOTHERAPY FOR PAIN 1099

included in the meta-analysis.17,39,40 Auriculotherapy inter-ventions for studies incorporated into the meta-analysis in-cluded auricular acupuncture with and without electricalstimulation, TENS, and laser auriculotherapy; control grouptreatments included sham auriculotherapy, placebo pill, andstandard medical care. Auriculotherapy was significantlymore effective than control procedures at decreasing painintensity as measured by VAS or NRS (SMD 1.56; 95% CI:0.85, 2.26; eight studies) (Fig. 2A). Though significant het-erogeneity existed among the studies (Q-value¼ 58.6,p< 0.001, I2¼ 88), sensitivity analyses indicated no differencein conclusions with any single study removed, and cumula-tive analysis showed that results become more positive overtime. When poor quality studies were removed, results re-mained statistically significant (SMD 2.17; 95% CI: 1.20, 3.13;five studies) and heterogeneity remained (Q-value¼ 43.4,p< 0.001, I2¼ 91). Two (2) studies were clear outliers.32,33
These studies included 21 and 61 participants, respectively(10% of our sample) and utilized a summed weekly pain scorein addition to including only subjects with high baseline painscores. When removed from the analysis, heterogeneity wasreduced nominally (Q-value¼ 19.18, p< 0.002, I2¼ 74) and
the SMD dropped to 1.01 (95% CI: 0.51, 1.51). The overallstrength of evidence for efficacy of auriculotherapy for painwas rated as moderate (Table 2).
Perioperative pain
Eight (8) studies assessed perioperative auriculotherapy.Two (2) studies assessed intraoperative use for anestheticrequirement,31,41 and six studies reported on the effects ofpostoperative auriculotherapy on pain relief or pain medi-cation use.15,16,30,37,39,40 Three (3) of these studies were ratedas high quality, three were rated fair, and two were ratedpoor (Table 1).
Three (3) studies in this subgroup were excluded from themeta-analysis due to missing data or an outcome measureother than analgesic use.31,39,40 Analgesic consumption wassignificantly lower in the auriculotherapy group comparedto controls (SMD 0.54; 95% CI: 0.30, 0.77; five studies) (Fig.2B). Statistical heterogeneity did not exist for this subgroupof studies (Q-value¼ 4.48, p¼ 0.35, I2¼ 10.62, t2¼ 0.007).Sensitivity analyses indicated no differences in the conclu-sions with any single study removed. All studies included
FIG. 1. Flow chart of screened,excluded, and analyzed studies. RCT,randomized controlled trial; AT,auriculotherapy.
1100 ASHER ET AL.

Ta
bl
e1.
St
ud
ie
so
fA
ur
ic
ul
ot
he
ra
py
fo
rP
ain
Ma
na
ge
me
nt
Au
thor
,a
yea
rco
un
try
Ind
icat
ion
,sa
mp
lesi
zeQ
ual
ity
rati
ng
bR
esu
ltIn
terv
enti
ontr
eatm
ent
Con
trol
trea
tmen
tc
Pri
mar
you
tcom
em
easu
reA
cup
oin
ts
Per
iop
erat
ive
pai
nL
i39
Po
sto
per
ativ
ep
ain
(liv
erre
sect
ion
)P
oo
rM
ixed
AA
,h
erb
s,ep
idu
ral
mo
rph
ine
Pla
ceb
op
ill
VA
S,p
eth
idin
eu
seH
eart
,lu
ng
,an
dsh
enm
en19
94C
hin
a16
d
Mic
hal
ek-S
aub
erer
30
To
oth
extr
acti
on
Fai
r�
Ind
wel
lin
gE
AIn
dw
elli
ng
AAþ
mo
ckE
Aan
dn
o-n
eed
lem
ock
EA
Ty
len
ol�
use
To
oth
,m
ou
th,
shen
men
2007
e14
9A
ust
ria
Sat
or-
Kat
zen
shla
ger
31
Intr
aop
erat
ive
pai
n(o
ocy
teas
pir
atio
n)
Go
od
þIn
dw
elli
ng
EA
Ind
wel
lin
gA
Aþ
mo
ckE
A&
no
-nee
dle
mo
ckE
AV
AS
Ute
rus,
shen
men
,cu
shio
n20
06f
Au
stri
a94
Usi
chen
ko
16
2005
eP
ost
op
erat
ive
pai
n(T
HA
)F
air
þIn
dw
elli
ng
AA
Ind
wel
lin
gA
Aat
no
nac
up
un
ctu
rep
oin
tsP
irit
ram
ide
use
Sh
enm
en,
thal
amu
s,lu
ng
,h
ipG
erm
any
61
Usi
chen
ko
37
Po
sto
per
ativ
ep
ain
(kn
eear
thro
sco
py
)18
Fai
rþ
Ind
wel
lin
gA
AIn
dw
elli
ng
AA
atn
on
acu
pu
nct
ure
po
ints
Ibu
pro
fen
use
Sh
enm
en,
lun
g,
kn
ee20
05e
Ger
man
y
Usi
chen
ko
41
Intr
aop
erat
ive
pai
n(T
HA
)G
oo
dþ
Ind
wel
lin
gA
AIn
dw
elli
ng
AA
atn
on
acu
pu
nct
ure
po
ints
Fen
tan
yl
req
uir
emen
tS
hen
men
,lu
ng
,h
ip,
fore
hea
d20
06e
Ger
man
y64
Usi
chen
ko
15
Po
sto
per
ativ
ep
ain
(kn
eear
thro
sco
py
)12
0
Go
od
þIn
dw
elli
ng
AA
Ind
wel
lin
gA
Aat
no
nac
up
un
ctu
rep
oin
tsIb
up
rofe
nu
seS
hen
men
,lu
ng
,k
nee
2007
e
Ger
man
yW
igra
m4
0P
ost
op
erat
ive
pai
n(a
bd
.su
rger
y)
34
Po
or
�In
dw
elli
ng
EA
Sta
nd
ard
med
ical
care
VA
SN
R19
86U
.K.
Acu
tep
ain
Bar
ker
17
Hip
frac
ture
(pre
ho
spit
altr
ansp
ort
)38
Go
od
þA
PS
ham
AP
(no
nin
dic
ated
po
ints
)V
AS
Sh
enm
en,
hip
,v
aliu
m20
06A
ust
ria
Go
ertz
18
Acu
tep
ain
syn
dro
mes
Fai
rM
ixed
Ind
wel
lin
gA
AS
tan
dar
dm
edic
alca
reN
RS
Cin
gu
late
gy
rus,
thal
amu
s20
06e,f
100
US
A
Gu
38
Acu
teb
ilia
ryco
lic
Po
or
þA
AIM
atro
pin
ean
dp
hen
erg
anP
ain
reli
efo
rd
ecre
ase
Po
int
zero
1993
48C
hin
a
(con
tin
ued
)
1101

Ta
bl
e1.
(C
on
tin
ue
d)
Au
thor
,a
yea
rco
un
try
Ind
icat
ion
,sa
mp
lesi
zeQ
ual
ity
rati
ng
bR
esu
ltIn
terv
enti
ontr
eatm
ent
Con
trol
trea
tmen
tc
Pri
mar
you
tcom
em
easu
reA
cup
oin
ts
Lew
is4
2A
cute
bu
rnP
oo
rþ
TE
NS
Pla
ceb
op
ill
VA
SS
hen
men
,lu
ng
,an
dth
alam
us
1990
e,f
11g
US
A
Ch
ron
icp
ain
Ali
mi1
4N
euro
pat
hic
pai
nG
oo
dþ
Ind
wel
lin
gA
AIn
dw
elli
ng
AA
&A
Pat
no
nco
nd
uct
ance
pts
VA
SIn
div
idu
aliz
edb
ased
on
der
mal
con
du
ctan
ce20
03c,
f90
Fra
nce
Lo
ng
ob
ard
i44
Dis
tal
extr
emit
yp
ain
Po
or
Mix
edT
EN
SP
lace
bo
pil
lV
AS
,P
RI
Sh
enm
en,
lun
g,
thal
amu
s,þ
2:to
e,an
kle
,k
nee
;o
rfi
ng
er,
wri
st,
elb
ow
1989
e,f
15U
SA
Maz
zett
o4
3T
MJ
pai
nP
oo
rþ
LA
TM
ock
LA
TV
AS
Ex
tern
alau
dit
ory
can
alju
stp
ost
e-ri
or
toth
etr
agu
s
2007
e,f
48B
razi
l
Sat
or-
Kat
zen
shla
ger
33
Ch
ron
icn
eck
pai
nG
oo
dþ
Ind
wel
lin
gE
AIn
wel
lin
gA
Aþ
mo
ckE
AV
AS
Cer
vic
alsp
ine,
shen
men
,cu
shio
n20
03e,f
21A
ust
ria
Sat
or-
Kat
zen
shla
ger
32
Ch
ron
iclo
w-b
ack
pai
nF
air
þIn
dw
elli
ng
EA
Ind
wel
lin
gA
AV
AS
Cu
shio
n,
shen
men
,lu
mb
arsp
ine
2004
e,f
87A
ust
ria
AA
,au
ricu
lar
acu
pu
nct
ure
;V
AS
,v
isu
alan
alo
gsc
ale;
Ind
wel
lin
g,
AA
usi
ng
AS
Pn
eed
les,
pre
ssta
cks,
or
typ
ical
nee
dle
s;E
A,
elec
tro
acu
pu
nct
ure
;T
HA
,to
tal
hip
arth
rop
last
y;
NR
,n
ot
rep
ort
ed;
NR
S,
nu
mer
ical
rati
ng
scal
e;IM
,in
tram
usc
ula
r;T
EN
S,t
ran
sder
mal
elec
tric
aln
erv
est
imu
lati
on
;A
P,
acu
pre
ssu
re;
PR
I,p
ain
rati
ng
ind
ex;
TM
J,te
mp
oro
man
dib
ula
rjo
int;
LA
T,
lase
rau
ricu
loth
erap
y;þ
,b
enefi
tfr
om
auri
culo
ther
apy
;–,
no
ben
efit
fro
mau
ricu
loth
erap
y.
aA
llst
ud
ies
wer
era
nd
om
ized
con
tro
lled
tria
ls.
bQ
ual
ity
rati
ng
sw
ere
bas
edo
nA
gen
cyfo
rH
ealt
hca
reR
esea
rch
and
Qu
alit
y(A
HR
Q)
gu
idel
ines
.c A
cup
oin
tsfo
rco
ntr
ol
and
trea
tmen
tg
rou
ps
wer
eth
esa
me
un
less
oth
erw
ise
ind
icat
ed.
d3�
2fa
cto
rial
des
ign
.eS
tud
ies
use
dfo
rsu
bg
rou
pan
aly
ses.
f Stu
die
su
sed
ino
ver
all
met
a-an
aly
sis.
gC
ross
ov
erd
esig
n.
1102
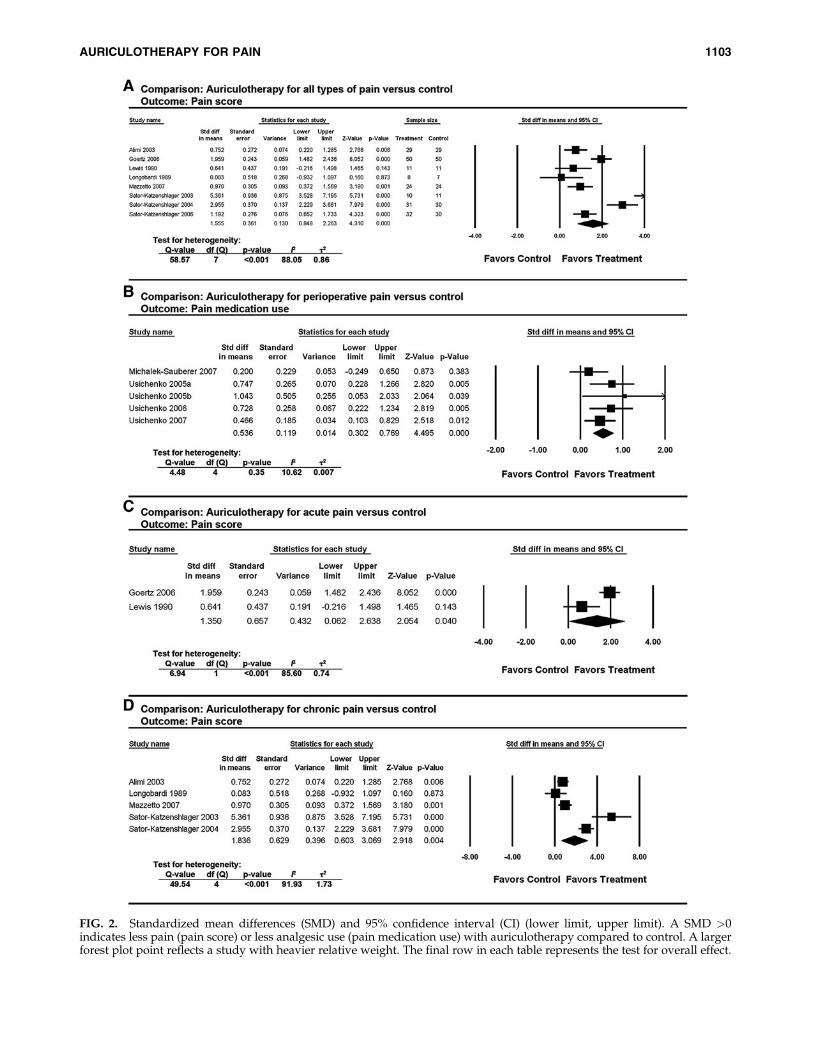
FIG. 2. Standardized mean differences (SMD) and 95% confidence interval (CI) (lower limit, upper limit). A SMD >0indicates less pain (pain score) or less analgesic use (pain medication use) with auriculotherapy compared to control. A largerforest plot point reflects a study with heavier relative weight. The final row in each table represents the test for overall effect.
AURICULOTHERAPY FOR PAIN 1103

for this analysis were rated either good or fair quality. Of thethree studies not included, two were rated poor and reportedeither mixed or negative results, and one study was ratedgood that reported favorable results. The strength of evi-dence for efficacy for this subgroup was rated as moderate(Table 2).
Four of the five studies included in the perioperativesubgroup15,16,37,41 examined the effect of auricular acupunc-ture at true acupoints compared to sham points, allowing fora comparison of the effect of point specificity. Meta-analysisfor these studies show a significant reduction in analgesic usefor the true acupuncture group (SMD 0.63; 95% CI: 0.88, 4.97;four studies). Significant heterogeneity was not detectedamong this subgroup of studies (Q-value¼ 1.79, p¼ 0.62,I2< 0.001, t2< 0.001), and sensitivity analysis indicated nodifferences in conclusions with any single study removed.This was the only group of studies that compared the effectsof penetrating true and sham acupuncture.
Acute pain
We identified four eligible studies of auriculotherapy foracute pain. One (1) study, however, did not provide enoughdata to be included in the meta-analysis.17 The pain etiologiesstudied were the following: hip fracture17; biliary colic38;wound debridement in burn patients42; and acute pain from avariety of different pain etiologies among patients in anemergency care center.18 We rated only one study as goodquality. Of the remaining three studies, one was rated fair,and two were rated poor (Table 1).
Because of the different scales used for primary outcomemeasures within this group, only two studies reported suffi-cient data for meta-analysis (Fig. 2C).18,42 The results com-
paring SMD for decrease in pain from baseline to end ofstudy between treatment and control group favor aur-iculotherapy (SMD 1.35; 95% CI: 0.08, 2.64; two studies).There was significant heterogeneity between these two stud-ies (Q-value¼ 6.94, p< 0.001). The two studies not included inthis subgroup analysis both reported positive effects for aur-iculotherapy. The strength of evidence for efficacy of thissubgroup was rated as low (Table 2).
Chronic pain
Five (5) studies using auriculotherapy to treat chronicmusculoskeletal pain met our inclusion criteria. The range ofconditions studied included chronic neck,33 low back,32 can-cer,14 temporomandibular joint,43 and distal extremity pain.44
Of the five studies, two were rated good, one was rated fair,and two were rated poor (Table 1).
The overall change in pain score shows significant im-provement for acupuncture treatment versus control (SMD1.84; 95% CI: 0.60, 3.07; five studies). Significant heterogeneitywas detected among the studies (Q-value¼ 49.54, p< 0.001)(Fig. 2D). However, sensitivity analysis indicated no differ-ences in the conclusions with any single study removed, andcumulative analysis showed that effect estimates becamelarger with later publication dates. When poor quality studieswere removed, results still favored auriculotherapy (SMD2.86; 95% CI 0.70, 5.02; three studies). The strength of evidencefor efficacy of this subgroup was rated as low (Table 2).
Adverse events
Of the 17 studies included in this review, 7 (41%) did notreport on adverse events, 5 (29%) reported no adverse events,
Table 2. Comparative Efficacy of Auriculotherapy for Treatment of Pain
Number of studies(no. of subjects) Design Quality Consistency
Magnitude of effect(95% CI; no. of studies
in meta-analysis)Other modifying
factorsaOverall strength
of evidence
All pain types combinedOutcomes: analgesic use or change in pain score17 (1009) RCT Good (6); Fair
(5); Poor (6)High For change in pain score:
SMD 1.56 (0.85, 2.26;eight)
None Moderate
Perioperative painOutcomes: analgesic use or change in pain score8 (551) RCT Good (3); Fair
(3); Poor (2)High For analgesic use: SMD
0.54 (0.30, 0.77; five)Most studies were
done by sameresearch team.Analgesic use isa proxy for painintensity.
Moderate
Acute painOutcome: change in pain score4 (197) RCT Good (1); Fair
(1); Poor (2)High SMD 1.35 (0.08, 2.64; two) none Low
Chronic painOutcome: change in pain score5 (261) RCT Good (2); Fair
(1); Poor (2)High SMD 1.84 (0.60, 3.07; five) none Low
aImprecise or sparse data, a strong or very strong association, high risk of reporting bias, evidence of a dose response gradient, effect ofplausible residual confounding.
CI, confidence interval; RCT, randomized controlled trial; SMD, standardized mean differences.
1104 ASHER ET AL.

and 5 (29%) reported some acupuncture-related adverseevent. All 10 studies that reported on adverse events (4445needle punctures) used indwelling auricular needles for boththe intervention and control procedures, except for onestudy39 that used auricular needles for the intervention pro-cedure and placebo pill for the control. The most commonlyreported events were ear pain (n¼ 16) and tiredness (n¼ 16).Other events reported include local minor bleeding (n¼ 2),dizziness and nausea (n¼ 1), and headache (n¼ 1). No in-fections or other serious adverse events associated with aur-iculotherapy were reported.
Discussion
We found a large difference between auriculotherapy andcontrol for reduction in pain scores for a wide variety oftypes of pain. The overall SMD was 1.56 (95% CI: 0.85, 2.26),indicating that on average, the mean decrease in pain scorefor the auriculotherapy group was 1.56 standard deviationsgreater than the mean decrease for the control group (i.e., themean of the auriculotherapy group was at the 94th percen-tile of the control group). Removing two outliers reduced theeffect size somewhat (SMD 1.01), but for either estimate, theeffect size is considerably large. For comparison, a recentmeta-analysis of traditional acupuncture for all types of painfound effect sizes (SMD) of 0.17 for body acupuncture versusplacebo acupuncture, and 0.42 for placebo acupunctureversus no acupuncture.45 It is unclear what accounts for thelarge effect sizes found for these studies. Adequate blindingprocedures are often challenging for studies of acupunc-ture, with acupuncturists often unblinded and questionableblinding of participants. However, the studies with the bestblinding procedures tended to have the highest effect esti-mates.16,31–33,37,43 Additionally, when poor quality studieswere removed, which are more likely to contain unmeasuredbias, the effect estimates remained relatively unchanged.
Subgroup analyses for postoperative, acute, and chronicpain also revealed significant reductions in either pain scoresor analgesic consumption. In addition, the estimates did notchange significantly when poor quality studies were re-moved. These results are further supported by the results ofthe random effects overall test for effect, sensitivity analyses,and cumulative analyses (Fig. 2).
Postoperative pain was the largest subgroup we analyzedand contained the only results that were not statistically het-erogeneous. We conducted two analyses of this group: studiesmeasuring analgesic use, and studies comparing penetratingauricular acupuncture at true acupoints verses nonacupunc-ture points. Similar to a recent review of auriculotherapy forpostoperative pain,19 results for analgesic use suggest thatauriculotherapy, specifically indwelling auricular acupunc-ture, is effective at reducing postoperative pain.
Perhaps more interesting are the comparisons for pene-trating auricular acupuncture at true acupoints versus non-acupuncture points, since this comparison controls for theeffects of needle puncture, demonstrating the effect of trueacupuncture points. Our results suggest that for auricularacupuncture, pain relief may be dependent on the use of trueacupuncture points. In contrast, the results of several recentstudies of full body acupuncture suggest that the effects ofacupuncture may be related simply to skin penetration andnot to the use of true acupuncture points.13,46–48 Two (2)
considerations may help explain these discordant findings:(1) the effects of auriculotherapy may indeed be point spe-cific and work through different mechanisms than full bodyacupuncture, or (2) auriculotherapy is not point specific butmay have regional specificity.
The regional innervations of the ear remain an unexploredarea of investigation for auriculotherapy. The auricle receivesnerve fibers from three distinct but overlapping groups:fibers from the superior cervical plexus largely innervate thehelix and lobe; the pinna is innervated by the trigeminalnerve; and the conchae are predominantly innervated bythe vagus nerve with some facial and glossopharyngealnerve innervations.49 It is possible that the effects noted inthe subgroup analysis comparing auricular acupuncture attrue acupoints versus nonacupuncture points are due to theregional grouping of the needles. In all four of these studies,the intervention treatment points were located in the con-chae, while the control points were located along the helix. Ithas been demonstrated that needle stimulation of the con-chae can induce significant parasympathetic stimulation.50 Itis possible that regional specificity, and not point specificity,is responsible for the results of these studies.
The results from studies of acute pain, though in favor ofauriculotherapy, are difficult to generalize because only twostudies were included in that meta-analysis. Likewise, be-cause of the clinical heterogeneity among the studies ofchronic pain, interpretation and generalizability of these re-sults are limited. While it is possible that auriculotherapyanalgesia works via central mechanisms that are independentof the type of pain experienced, there are a paucity of data onthe mechanisms that might be responsible for auriculotherapyanalgesia and there are not yet enough high quality studiesacross the wide spectrum of chronic pain syndromes to beconfident that our results are generalizable to all chronic painconditions. However, the positive results from analyses ofthese two subgroups do add a little information, in favor ofauriculotherapy, to our overall conclusion that auriculo-therapy appears to be beneficial for pain reduction across awide spectrum of pain conditions. Further studies to elucidatethe mechanisms responsible for acupuncture analgesia, andhigh quality studies of clinical pain syndromes will help tofurther clarify the benefits of auriculotherapy.
Overall, we rated the strength of evidence for efficacy ofauriculotherapy compared to control for the treatment ofpain as moderate (Table 2). This was based on the magnitudeof the mean differences we found overall and for each sub-group, the high consistency in direction and magnitude ofeffects noted throughout the studies, the lack of evidence ofpublication bias, the preponderance of good and fair qual-ity studies, and the stability of our estimates with poorquality studies removed. Although we acknowledge thegenerally low strength of evidence of efficacy for acute andchronic pain subcategories, overall we note that the directionof effect appears to favor efficacy of auriculotherapy.
Limitations
Our search identified two studies that may have beenappropriate to include in our review but were unavailable inEnglish.51,52 Additionally, since our search strategy includedonly U.S. and European databases, we may have overlookedstudies contained in the Asian literature.53 However, it has
AURICULOTHERAPY FOR PAIN 1105

been noted that studies of acupuncture that are indexed inMEDLINE and published in English score significantlyhigher on standardized quality scales than those that do notmeet these criteria,54 and some countries have been shown topublish exclusively positive results for studies of acupunc-ture.55 For these reasons, we believe our results likely reflectthe results of higher quality studies and reduced publicationbias. For the meta-analyses, significant heterogeneity existedfor all groups analyzed except for the perioperative sub-group. Though heterogeneity among pooled results maylimit the strength of our findings, we note that most trialsshowed positive effects for auriculotherapy, sensitivity ana-lyses revealed that results were not influenced by any singlestudy, and cumulative analyses most often showed thatstudies became more significant over time. Additionally,because random-effects models were used for the conclu-sions of the current study, homogeneity was not assumed forthese analyses.29 However, we recognize that the magnitudeof the effect estimates found may reflect biases that are dif-ficult to overcome in studies of acupuncture.
Conclusions
The evidence from this review suggests that aur-iculotherapy may be effective for the treatment of a variety oftypes of pain, especially postoperative pain, and may be areasonable adjunct for patients having difficulties withpharmacologic pain therapies.
Acknowledgments
We would like to thank Denise Esserman, PhD for herhelp in reviewing some of the trials, and participants of theUniversity of North Carolina NRSA Primary Care Researchfellowship for reviews of the manuscript. Financial supportwas provided by National Institutes of Health/NationalCenter for Complementary and Alternative Medicine grantT32AT003378 (GNA), and NIH/NIGMS grant T32GM081057(SJW).
Disclosure Statement
No competing financial interests exist.
References
1. Health, United States, National Center for Health StatisticsReport. National Center for Health Statistics Report. Onlinedocument at: www.cdc.gov/nchs/data/hus/hus07.pdf Ac-cessed July 17, 2008.
2. Max MB. How to move pain and symptom research fromthe margin to the mainstream. J Pain 2003;4:355–360.
3. National Cancer Control Programmes: Policies and Man-agerial Guidelines. Genera, Switzerland: World Health Or-ganization, 2002.
4. Kalso E, Edwards JE, Moore RA, McQuay HJ. Opioids inchronic non-cancer pain: Systematic review of efficacy andsafety. Pain 2004;112:372–380.
5. Wolfe MM, Lichtenstein DR, Singh G. Gastrointestinal tox-icity of nonsteroidal antiinflammatory drugs. NEJM 1999;340:1888–1899.
6. Schlansky B, Hwang JH. Prevention of nonsteroidal anti-inflammatory drug-induced gastropathy. J Gastroenterol2009;44(suppl 19):44–52.
7. Li JM. Pain management in the hospitalized patient. MedClin North Am 2008;92:371–385, ix.
8. McCarberg BH. Rheumatic diseases in the elderly: Dealingwith rheumatic pain in extended care facilities. Rheum DisClin North Am 2007;33:87–108.
9. Tyring SK. Management of herpes zoster and postherpeticneuralgia. J Am Acad Dermatol 2007;57(6 suppl):S136–S142.
10. Brinkhaus B, Witt CM, Jena S, et al. Acupuncture in patientswith chronic low back pain: A randomized controlled trial.Arch Intern Med 2006;166:450–457.
11. Haake M, Muller HH, Schade-Brittinger C, et al. GermanAcupuncture Trials (GERAC) for chronic low back pain:Randomized, multicenter, blinded, parallel-group trial with3 groups. Arch Intern Med 2007;167:1892–1898.
12. Manheimer E, Linde K, Lao L, et al. Meta-analysis: Acu-puncture for osteoarthritis of the knee. Ann Intern Med2007;146:868–877.
13. Linde K, Streng A, Jurgens S, et al. Acupuncture for patientswith migraine: A randomized controlled trial. JAMA 2005;293:2118–2125.
14. Alimi D, Rubino C, Pichard-Leandri E, et al. Analgesic effectof auricular acupuncture for cancer pain: A randomized,blinded, controlled trial. J Clin Oncol 2003;21:4120–4126.
15. Usichenko TI, Kuchling S, Witstruck T, et al. Auricularacupuncture for pain relief after ambulatory knee surgery: Arandomized trial. CMAJ 2007;176:179–183.
16. Usichenko TI, Dinse M, Hermsen M, et al. Auricular acu-puncture for pain relief after total hip arthroplasty: A ran-domized controlled study. Pain 2005;114:320–327.
17. Barker R, Kober A, Hoerauf K, et al. Out-of-hospital auricularacupressure in elder patients with hip fracture: A randomizeddouble-blinded trial. Acad Emerg Med 2006;13:19–23.
18. Goertz CM, Niemtzow R, Burns SM, et al. Auricular acu-puncture in the treatment of acute pain syndromes: A pilotstudy. Mil Med 2006;171:1010–1014.
19. Usichenko TI, Lehmann C, Ernst E. Auricular acupuncturefor postoperative pain control: A systematic review of ran-domised clinical trials. Anaesthesia 2008;63:1343–1348.
20. MacPherson H, White A, Cummings M, et al. Standards forReporting Interventions in Controlled Trials of Acupuncture:The STRICTA recommendations. J Altern Complement Med2002;8:85–89.
21. Harris RP, Helfand M, Woolf SH, et al. Current methods ofthe US Preventive Services Task Force: A review of theprocess. Am J Prev Med 2001;20(3 suppl):21–35.
22. Khan KS, ter Riet G, Glanville J, et al., eds. UndertakingSystematic Reviews of Research on Effectiveness: CRD’sGuidance for Those Carrying Out or Commissioning Re-views. York, UK: Centre for Reviews and Dissemination,University of York, 2001.
23. Egger M, Smith G, Altman D. Systematic Reviews in HealthCare, 2nd ed. London: BMJ Books, 2001.
24. U.S. Preventive Services Task Force Grade Definitions,Agency for Healthcare Research and Quality, Rockville, MD.May 2008. Online document at: www.ahrq.gov/clinic/uspstf/grades.htm Accessed December 17, 2008.
25. Cohen J. Statistical Power Analysis for the Behavioral Sci-ences. 2nd ed. Mahwah, NJ: Lawrence Erlbaum, 1988.
26. Glasziou P, Irwig L, Bain C, Colditz. Systemic Reviews inHealth Care: A Practical Guide. Cambridge: CambridgeUniversity Press, 2001.
27. Higgins JP, Thompson SG. Quantifying heterogeneity in ameta-analysis. Stat Med 2002;21:1539–1558.
1106 ASHER ET AL.

28. DerSimonian R, Laird N. Meta-analysis in clinical trials.Control Clin Trials 1986;7:177–188.
29. Fleiss JL. The statistical basis of meta-analysis. Stat MethodsMed Res 1993;2:121–145.
30. Michalek-Sauberer A, Heinzl H, Sator-Katzenschlager SM, etal. Perioperative auricular electroacupuncture has no effecton pain and analgesic consumption after third molar toothextraction. Anesth Analg 2007;104:542–547.
31. Sator-Katzenschlager SM, Wolfler MM, Kozek-LangeneckerSA, et al. Auricular electro-acupuncture as an additionalperioperative analgesic method during oocyte aspiration inIVF treatment. Hum Reprod 2006;21:2114–2120.
32. Sator-Katzenschlager SM, Scharbert G, Kozek-LangeneckerSA, et al. The short- and long-term benefit in chronic lowback pain through adjuvant electrical versus manual auric-ular acupuncture. Anesth Analg 2004;98:1359–1364.
33. Sator-Katzenschlager SM, Szeles JC, Scharbert G, et al. Elec-trical stimulation of auricular acupuncture points is moreeffective than conventional manual auricular acupuncture inchronic cervical pain: A pilot study. Anesth Analg 2003;97:1469–1473.
34. Alimi D, Rubino C, Leandri EP, Brule SF. Analgesic effectsof auricular acupuncture for cancer pain. J Pain SymptomManage 2000;19:81–82.
35. Kou WT. The effects of low-energy laser in the auriculo-therapy in individuals with chronic low back pain. Dis-sertation Abstracts Int 1991;4:1946.
36. Gori L, Firenzuoli F. Ear acupuncture in the treatment of lowback pain in cancer patients. J Soc Integr Oncol 2005;3:130.
37. Usichenko TI, Hermsen M, Witstruck T, et al. Auricularacupuncture for pain relief after ambulatory knee arthros-copy: A pilot study. Evid Based Complement Alternat Med2005;2:185–189.
38. Gu XD. Clinical-study on analgesia for biliary colic with earacupuncture at point erzhong. Am J Acupuncture 1993;21:237–239.
39. Li QS, Cao SH, Xie GM, et al. Combined traditional Chinesemedicine and Western medicine: Relieving effects of Chineseherbs, ear-acupuncture and epidural morphine on postoper-ative pain in liver cancer. Chin Med J (Engl) 1994;107:289–294.
40. Wigram JR, Lewith GT, Machin D, Church JJ. Electroacu-puncture for postoperative pain. Physiother-Pract 1986;2:83–88.
41. Usichenko TI, Dinse M, Lysenyuk VP, et al. Auricular acu-puncture reduces intraoperative fentanyl requirement dur-ing hip arthroplasty: A randomized double-blinded study.Acupunct Electrother Res 2006;31:213–221.
42. Lewis SM, Clelland JA, Knowles CJ, et al. Effects of auricularacupuncture-like transcutaneous electric nerve stimulationon pain levels following wound care in patients with burns:A pilot study. J Burn Care Rehabil 1990;11:322–329.
43. Mazzetto MO, Carrasco TG, Bidinelo EF, et al. Low intensitylaser application in temporomandibular disorders: A phase I
double-blind study. Cranio J Craniomandib Pract 2007;25:186–192.
44. Longobardi AG, Clelland JA, Knowles CJ, Jackson JR. Effectsof auricular transcutaneous electrical nerve stimulation ondistal extremity pain: A pilot study. Phys Ther 1989;69:10–17.
45. Madsen MV, Gotzsche PC, Hrobjartsson A. Acupuncturetreatment for pain: systematic review of randomised clinicaltrials with acupuncture, placebo acupuncture, and no acu-puncture groups. BMJ 2009;338:a3115.
46. Witt C, Brinkhaus B, Jena S, et al. Acupuncture in patientswith osteoarthritis of the knee: A randomised trial. Lancet2005;366:136–143.
47. Melchart D, Streng A, Hoppe A, et al. Acupuncture inpatients with tension-type headache: Randomised controlledtrial. BMJ 2005;331:376–382.
48. Scharf HP, Mansmann U, Streitberger K, et al. Acupunctureand knee osteoarthritis: A three-armed randomized trial.Ann Intern Med 2006;145:12–20.
49. Peuker ET, Filler TJ. The nerve supply of the human auricle.Clin Anat 2002;15:35–37.
50. Haker E, Egekvist H, Bjerring P. Effect of sensory stimula-tion (acupuncture) on sympathetic and parasympatheticactivities in healthy subjects. J Auton Nerv Syst 2000;79:52–59.
51. Ceccherelli F, Ambrosio F, Adami MG, et al. Failure of highfrequency auricular electrical stimulation to relieve postop-erative pain after cholecystectomy: Results not improved byadministration of aprotinin (double blind trial). Dtsch ZAkupunktur 1985;4:87–92.
52. Strom H. Controlled triple-blind investigation of the effect ofelectro-ear- acupuncture on movement and pain in the kneeafter meniscectomy. Ugeskr-Laeg 1977;39:2326–2329.
53. Kim YS, Jun H, Chae Y, et al. The practice of Korean med-icine: An overview of clinical trials in acupuncture. EvidBased Complement Alternat Med 2005;2:325–352.
54. Linde K, Jonas WB, Melchart D, Willich S. The methodo-logical quality of randomized controlled trials of homeopa-thy, herbal medicines and acupuncture. Int J Epidemiol2001;30:526–531.
55. Vickers A, Goyal N, Harland R, Rees R. Do certain countriesproduce only positive results? A systematic review of con-trolled trials. Control Clin Trials 1998;19:159–166.
Address correspondence to:Gary N. Asher, MD, MPH
Department of Family MedicineUniversity of North Carolina at Chapel Hill
590 Manning Drive, CB#7595Chapel Hill, NC 27599
E-mail: [email protected]
(Appendix follows?)
AURICULOTHERAPY FOR PAIN 1107
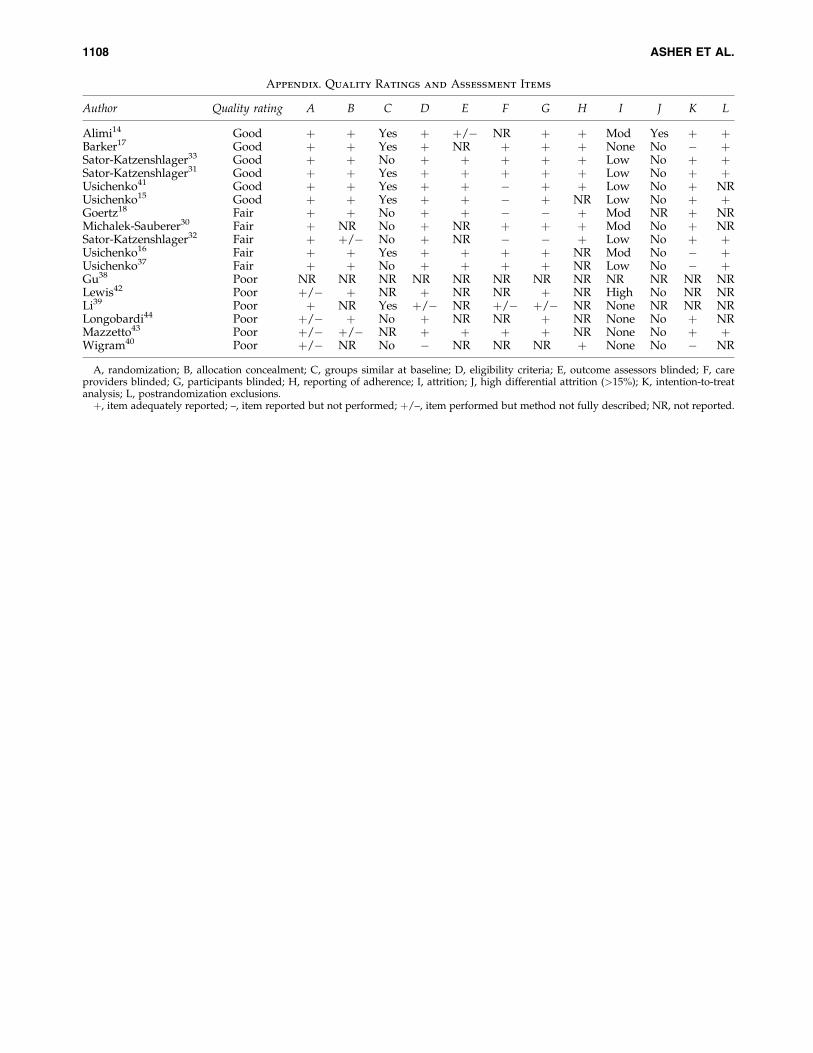
Appendix. Quality Ratings and Assessment Items
Author Quality rating A B C D E F G H I J K L
Alimi14 Good þ þ Yes þ þ/� NR þ þ Mod Yes þ þBarker17 Good þ þ Yes þ NR þ þ þ None No � þSator-Katzenshlager33 Good þ þ No þ þ þ þ þ Low No þ þSator-Katzenshlager31 Good þ þ Yes þ þ þ þ þ Low No þ þUsichenko41 Good þ þ Yes þ þ � þ þ Low No þ NRUsichenko15 Good þ þ Yes þ þ � þ NR Low No þ þGoertz18 Fair þ þ No þ þ � � þ Mod NR þ NRMichalek-Sauberer30 Fair þ NR No þ NR þ þ þ Mod No þ NRSator-Katzenshlager32 Fair þ þ/� No þ NR � � þ Low No þ þUsichenko16 Fair þ þ Yes þ þ þ þ NR Mod No � þUsichenko37 Fair þ þ No þ þ þ þ NR Low No � þGu38 Poor NR NR NR NR NR NR NR NR NR NR NR NRLewis42 Poor þ/� þ NR þ NR NR þ NR High No NR NRLi39 Poor þ NR Yes þ/� NR þ/� þ/� NR None NR NR NRLongobardi44 Poor þ/� þ No þ NR NR þ NR None No þ NRMazzetto43 Poor þ/� þ/� NR þ þ þ þ NR None No þ þWigram40 Poor þ/� NR No � NR NR NR þ None No � NR
A, randomization; B, allocation concealment; C, groups similar at baseline; D, eligibility criteria; E, outcome assessors blinded; F, careproviders blinded; G, participants blinded; H, reporting of adherence; I, attrition; J, high differential attrition (>15%); K, intention-to-treatanalysis; L, postrandomization exclusions.þ, item adequately reported; –, item reported but not performed; þ/–, item performed but method not fully described; NR, not reported.
1108 ASHER ET AL.
Related Documents











