Clinical audit tool: Ectopic pregnancy and miscarriage (2012) Page 1 of 12 NICE clinical guideline [XX] Ectopic pregnancy and miscarriage: ultrasound for determining viable intrauterine pregnancy Clinical audit tool Implementing NICE guidance 2012 NICE clinical guideline 154

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical audit tool: Ectopic pregnancy and miscarriage (2012)Page 1 of 12
Audit supportIssue date: [Year]Short title of guidelineNICE clinical guideline [XX]
Ectopic pregnancy and miscarriage: ultrasound for determining viable
intrauterine pregnancy
Clinical audit toolImplementing NICE guidance
2012
NICE clinical guideline 154
This clinical audit tool accompanies the clinical guideline: Ectopic pregnancy and
miscarriage: diagnosis and initial management in early pregnancy of ectopic pregnancy
and miscarriage.
Issue date: 2012
This document is a support tool for clinical audit based on the NICE guidance. It is not
NICE guidance.
Acknowledgements
NICE would like to thank the following people who have contributed to the development
of this clinical audit tool and have agreed to be acknowledged:
Dr TR Wiggins, General Practitioner, Queensview Medical Centre.
Miss Natasha Pradhan, Independent Emergency Nursing Consultant.
NICE has adapted the action plan template produced by the Healthcare Quality
Improvement Partnership (HQIP) in their template clinical audit report.
National Institute for Health and Clinical Excellence
Level 1A, City Tower, Piccadilly Plaza, Manchester M1 4BT; www.nice.org.uk
© National Institute for Health and Clinical Excellence, 2012. All rights reserved. This material
may be freely reproduced for educational and not-for-profit purposes. No reproduction by or for
commercial organisations, or for commercial purposes, is allowed without the express written
permission of NICE.
Clinical audit tool: Ectopic pregnancy and miscarriage (2012)Page 2 of 12

Ectopic pregnancy and miscarriage: ultrasound for determining
viable intrauterine pregnancy clinical audit tool
This document can be used as a starting point for a local clinical audit project that aims
to improve the use of ultrasound to determine viable intrauterine pregnancy. It contains:
• clinical audit standards
• a data collection form
• an action plan template.
There is also an electronic audit tool available, which can be used with this document
or on its own to collect and analyse the data.
The audit standards and data collection form can be adapted to focus on a smaller part
of the tool or expanded to include other local priorities.
The audit could be carried out in the following services: dedicated early pregnancy
assessment services or other facilities that offer specialist clinical assessment and
ultrasound scanning when an early pregnancy assessment service is not available
(such as gynaecology wards or accident and emergency [A&E] services with access to
specialist gynaecology support).
The audit should involve clinical and non-clinical stakeholders, which may include all
staff within the early pregnancy assessment service (or other facility), clinical audit staff
and patients. The audit contains a standard about women being assessed by a
healthcare professional before referral to an early pregnancy assessment service and
relevant stakeholders may also include these healthcare professionals.
The audit sample should include women attending the early pregnancy assessment
service with pain and/or bleeding or atypical symptoms suggestive of early pregnancy
problems. Early pregnancy is defined as the first trimester. Advice on how to decide on
sample size is available on HQIP’s website.
The audit standards are based on the NICE clinical guideline for ectopic pregnancy
and miscarriage. An audit tool is also available for expectant management of
miscarriage. In developing these tools consideration has been given to the clinical
issues covered by the guideline, the key priorities for implementation and the potential
Clinical audit tool: Ectopic pregnancy and miscarriage (2012)Page 3 of 12

challenges of data collection. The appendix highlights the parts of the care pathway
covered in this audit tool. There may be other recommendations within the guideline
suitable for the development of audit standards or an audit project.
The guidance includes recommendations about support and information giving for
women with early pregnancy complications (including recommendations 1.4.4, 1.4.13,
1.4.14, 1.4.15 and 1.4.16). It can be difficult to include standards relating to these
recommendations in a retrospective audit of patient records. Organisations could
consider other methods of measuring and improving practice in this area.
A baseline assessment tool is available. This can help to compare practice with the
guideline’s recommendations and prioritise implementation activity, including clinical
audit.
The audit standards in this document include a reference to the guideline
recommendation numbers, and any associated NICE quality standard statements
and exceptions. Exceptions not explicitly referred to in the guideline can be added
locally – for example, patients declining treatment.
NICE recommends compliance of 100%. If this is not achievable an interim local target
could be set, although 100% should remain the ultimate aim.
A data collection form should be completed for each episode. There is a section for
demographic information that can be completed if this information is essential to the
project. Patient identifiable information should never be recorded.
Following the audit the action plan template can be used to develop and implement
an action plan to take forward any recommendations made.
Re-audit is a key part of the clinical audit cycle, required to demonstrate that
improvement has been achieved and sustained. Once a re-audit has been completed,
the shared learning database can be used to share the experience of putting NICE
guidance into practice.
For further information about clinical audit refer to a local clinical audit professional in
your own organisation or the HQIP website. To ask a question about this clinical audit
tool, or to provide feedback to help inform the development of future tools, please
email [email protected]
Clinical audit tool: Ectopic pregnancy and miscarriage (2012)Page 4 of 12
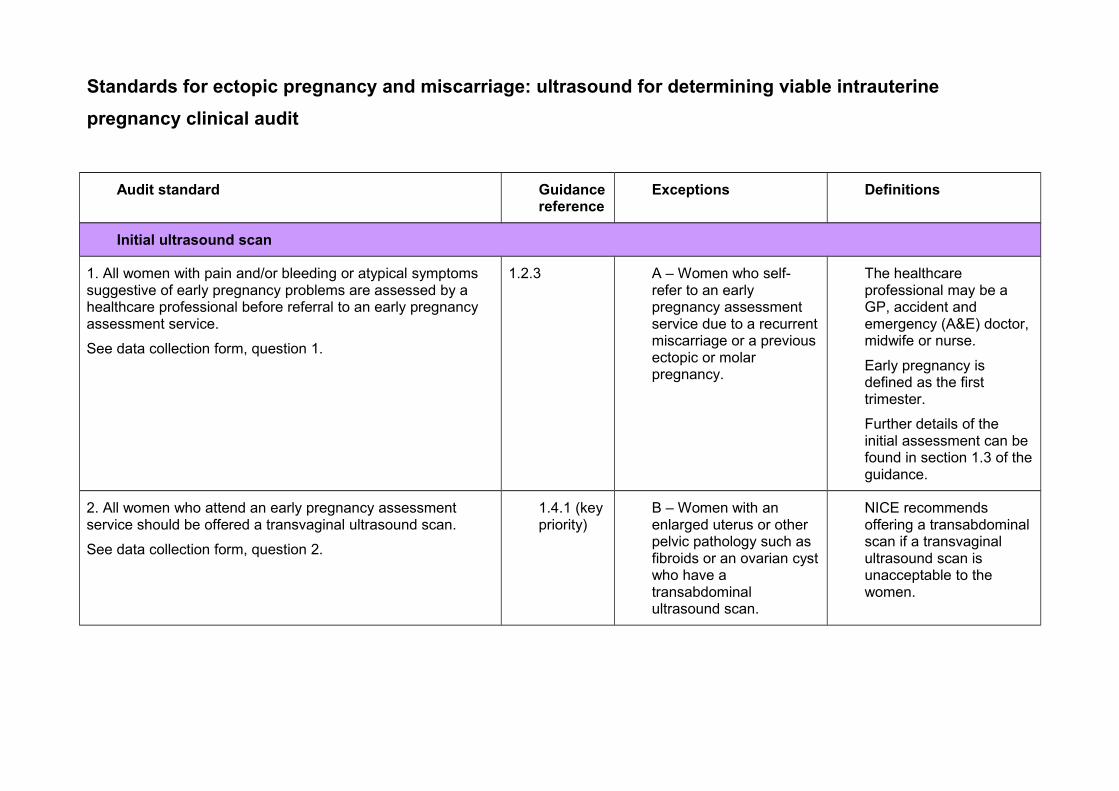
Standards for ectopic pregnancy and miscarriage: ultrasound for determining viable intrauterine
pregnancy clinical audit
Audit standard Guidance reference
Exceptions Definitions
Initial ultrasound scan
1. All women with pain and/or bleeding or atypical symptoms suggestive of early pregnancy problems are assessed by a healthcare professional before referral to an early pregnancy assessment service.
See data collection form, question 1.
1.2.3 A – Women who self-refer to an early pregnancy assessment service due to a recurrent miscarriage or a previous ectopic or molar pregnancy.
The healthcare professional may be a GP, accident and emergency (A&E) doctor, midwife or nurse.
Early pregnancy is defined as the first trimester.
Further details of the initial assessment can be found in section 1.3 of the guidance.
2. All women who attend an early pregnancy assessment service should be offered a transvaginal ultrasound scan.
See data collection form, question 2.
1.4.1 (key priority)
B – Women with an enlarged uterus or other pelvic pathology such as fibroids or an ovarian cyst who have a transabdominal ultrasound scan.
NICE recommends offering a transabdominal scan if a transvaginal ultrasound scan is unacceptable to the women.
Audit standard Guidance reference
Exceptions Definitions
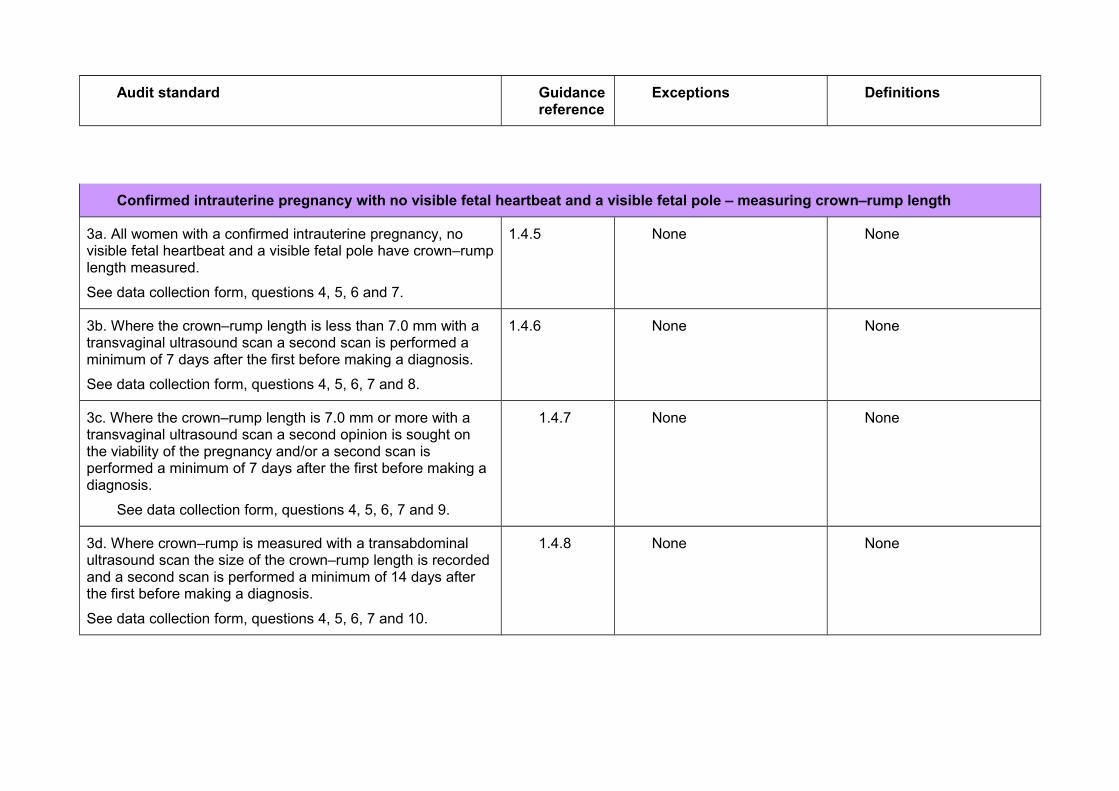
Confirmed intrauterine pregnancy with no visible fetal heartbeat and a visible fetal pole – measuring crown–rump length
3a. All women with a confirmed intrauterine pregnancy, no visible fetal heartbeat and a visible fetal pole have crown–rump length measured.
See data collection form, questions 4, 5, 6 and 7.
1.4.5 None None
3b. Where the crown–rump length is less than 7.0 mm with a transvaginal ultrasound scan a second scan is performed a minimum of 7 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 7 and 8.
1.4.6 None None
3c. Where the crown–rump length is 7.0 mm or more with a transvaginal ultrasound scan a second opinion is sought on the viability of the pregnancy and/or a second scan is performed a minimum of 7 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 7 and 9.
1.4.7 None None
3d. Where crown–rump is measured with a transabdominal ultrasound scan the size of the crown–rump length is recorded and a second scan is performed a minimum of 14 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 7 and 10.
1.4.8 None None

Audit standard Guidance reference
Exceptions Definitions
Confirmed intrauterine pregnancy with no visible fetal heartbeat and no visible fetal pole – measuring mean gestational sac diameter
4a. All women with a confirmed intrauterine pregnancy with no visible fetal heartbeat and no visible fetal pole have mean gestational sac diameter measured.
See data collection form, questions 4, 5, 6 and 11.
1.4.5 None None
4b. If the mean gestational sac diameter is less than 25.0 mm using a transvaginal ultrasound scan, a second scan is performed a minimum of 7 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 11 and 12.
1.4.9 None None
4c. If the mean gestational sac diameter is 25.0 mm or more using transvaginal ultrasound scan, a second opinion is sought on the viability of the pregnancy and/or a second scan is performed a minimum of 7 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 11 and 13.
1.4.10 None None
4d. If the mean gestational sac diameter is measured using a transabdominal ultrasound scan, the size of the mean gestational sac diameter is recorded and a second scan is performed a minimum of 14 days after the first before making a diagnosis.
See data collection form, questions 4, 5, 6, 11 and 14.
1.4.11 None None
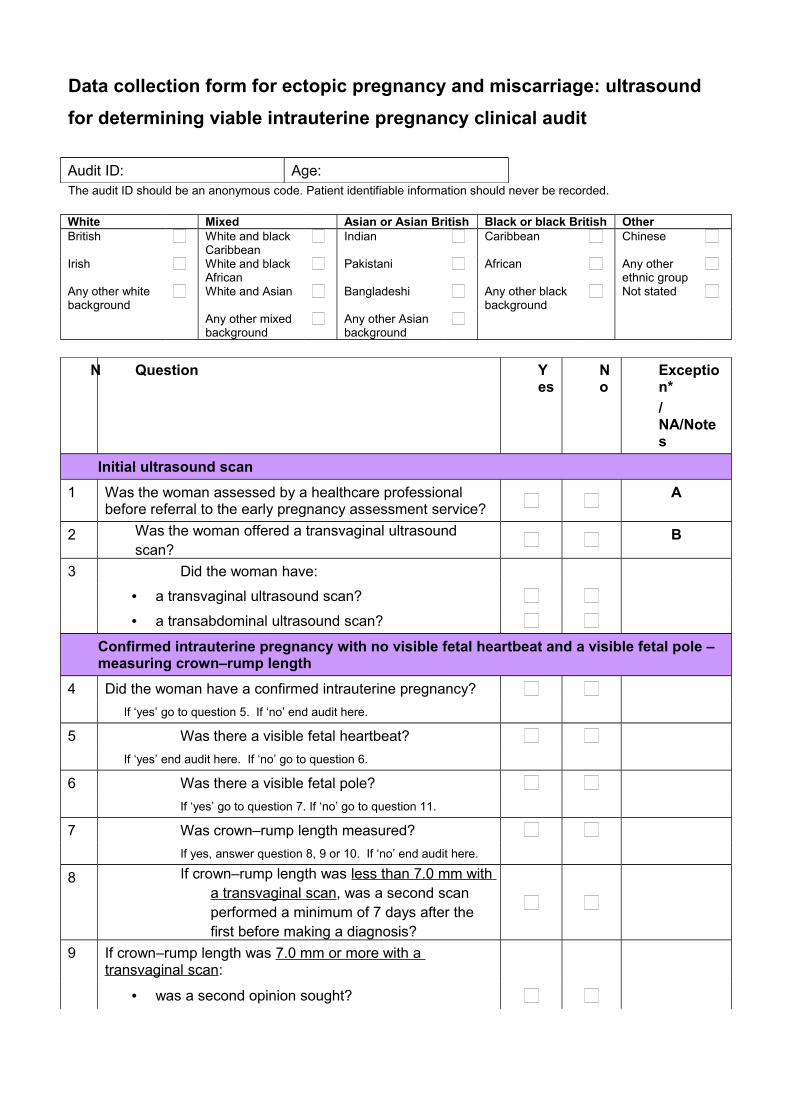
Data collection form for ectopic pregnancy and miscarriage: ultrasound
for determining viable intrauterine pregnancy clinical audit
Audit ID: Age:The audit ID should be an anonymous code. Patient identifiable information should never be recorded.
White Mixed Asian or Asian British Black or black British OtherBritish White and black
CaribbeanIndian Caribbean Chinese
Irish White and black African
Pakistani African Any other ethnic group
Any other white background
White and Asian Bangladeshi Any other black background
Not stated
Any other mixed background
Any other Asian background
N Question Yes
No
Exception*
/NA/Notes
Initial ultrasound scan
1 Was the woman assessed by a healthcare professional before referral to the early pregnancy assessment service?
A
2 Was the woman offered a transvaginal ultrasound scan?
B
3 Did the woman have:
• a transvaginal ultrasound scan?
• a transabdominal ultrasound scan?
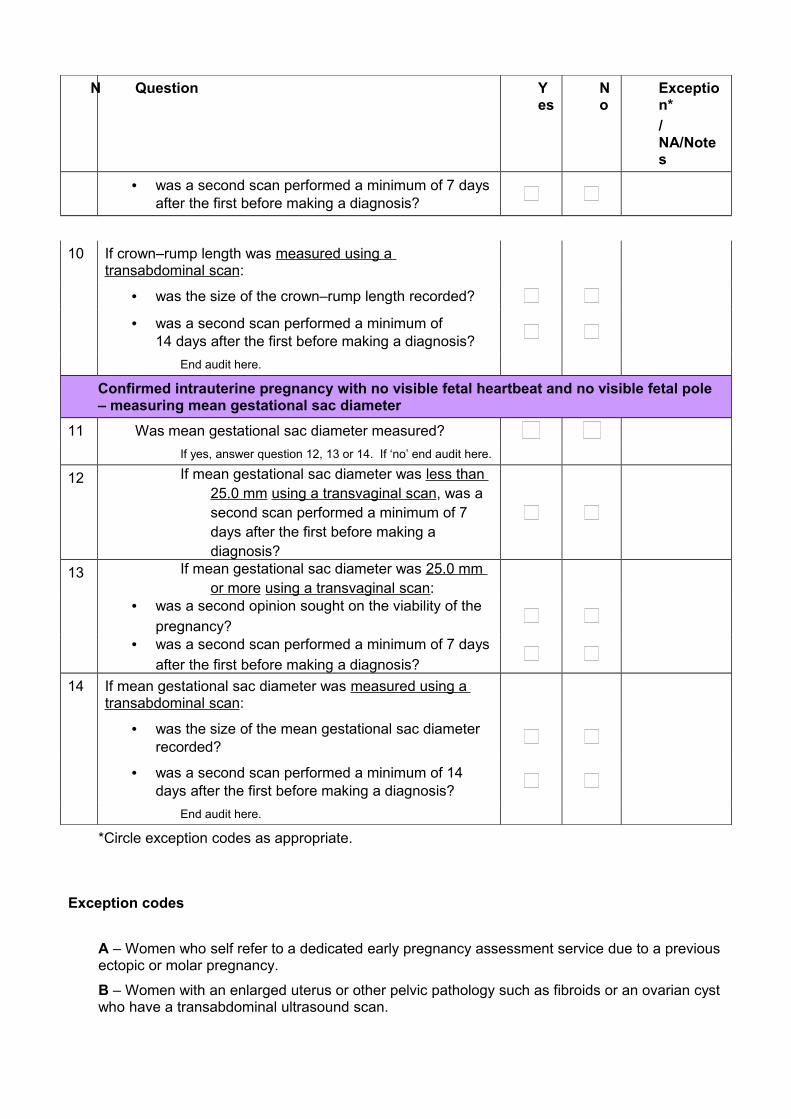
Confirmed intrauterine pregnancy with no visible fetal heartbeat and a visible fetal pole – measuring crown–rump length
4 Did the woman have a confirmed intrauterine pregnancy?
If ‘yes’ go to question 5. If ‘no’ end audit here.
5 Was there a visible fetal heartbeat?
If ‘yes’ end audit here. If ‘no’ go to question 6.
6 Was there a visible fetal pole?
If ‘yes’ go to question 7. If ‘no’ go to question 11.
7 Was crown–rump length measured?
If yes, answer question 8, 9 or 10. If ‘no’ end audit here.
8 If crown–rump length was less than 7.0 mm with a transvaginal scan, was a second scan performed a minimum of 7 days after the first before making a diagnosis?
9 If crown–rump length was 7.0 mm or more with a transvaginal scan:
• was a second opinion sought?
N Question Yes
No
Exception*
/NA/Notes
• was a second scan performed a minimum of 7 days after the first before making a diagnosis?
10 If crown–rump length was measured using a transabdominal scan:
• was the size of the crown–rump length recorded?
• was a second scan performed a minimum of 14 days after the first before making a diagnosis?
End audit here.
Confirmed intrauterine pregnancy with no visible fetal heartbeat and no visible fetal pole – measuring mean gestational sac diameter
11 Was mean gestational sac diameter measured?
If yes, answer question 12, 13 or 14. If ‘no’ end audit here.
12 If mean gestational sac diameter was less than 25.0 mm using a transvaginal scan, was a second scan performed a minimum of 7 days after the first before making a diagnosis?
13 If mean gestational sac diameter was 25.0 mm or more using a transvaginal scan:
• was a second opinion sought on the viability of the
pregnancy?• was a second scan performed a minimum of 7 days
after the first before making a diagnosis?
14 If mean gestational sac diameter was measured using a transabdominal scan:
• was the size of the mean gestational sac diameter recorded?
• was a second scan performed a minimum of 14 days after the first before making a diagnosis?
End audit here.
*Circle exception codes as appropriate.
Exception codes
A – Women who self refer to a dedicated early pregnancy assessment service due to a previous ectopic or molar pregnancy.
B – Women with an enlarged uterus or other pelvic pathology such as fibroids or an ovarian cyst who have a transabdominal ultrasound scan.

Action plan for ectopic pregnancy and miscarriage: ultrasound for determining a viable intrauterine
pregnancy clinical audit
Action plan lead
Name: Title: Contact:
The ‘Actions required’ should specifically state what needs to be done to achieve the recommendation. All updates to the action plan should be included in the ‘Comments’ section.
Recommendation Actions required (specify ‘None’, if none required)
Action by date
Person responsible
Comments/action status(Provide examples of action in progress, changes in practices, problems encountered in facilitating change, reasons why recommendation has not been actioned etc)
Change stage
(see Key)
When making improvements to practice, organisations may like to use the tools developed by NICE to help implement the clinical guideline on ectopic pregnancy and miscarriage.
KEY (Change status)1 Recommendation agreed but not yet actioned2 Action in progress3 Recommendation fully implemented4 Recommendation never actioned (please state reasons)5 Other (please provide supporting information)

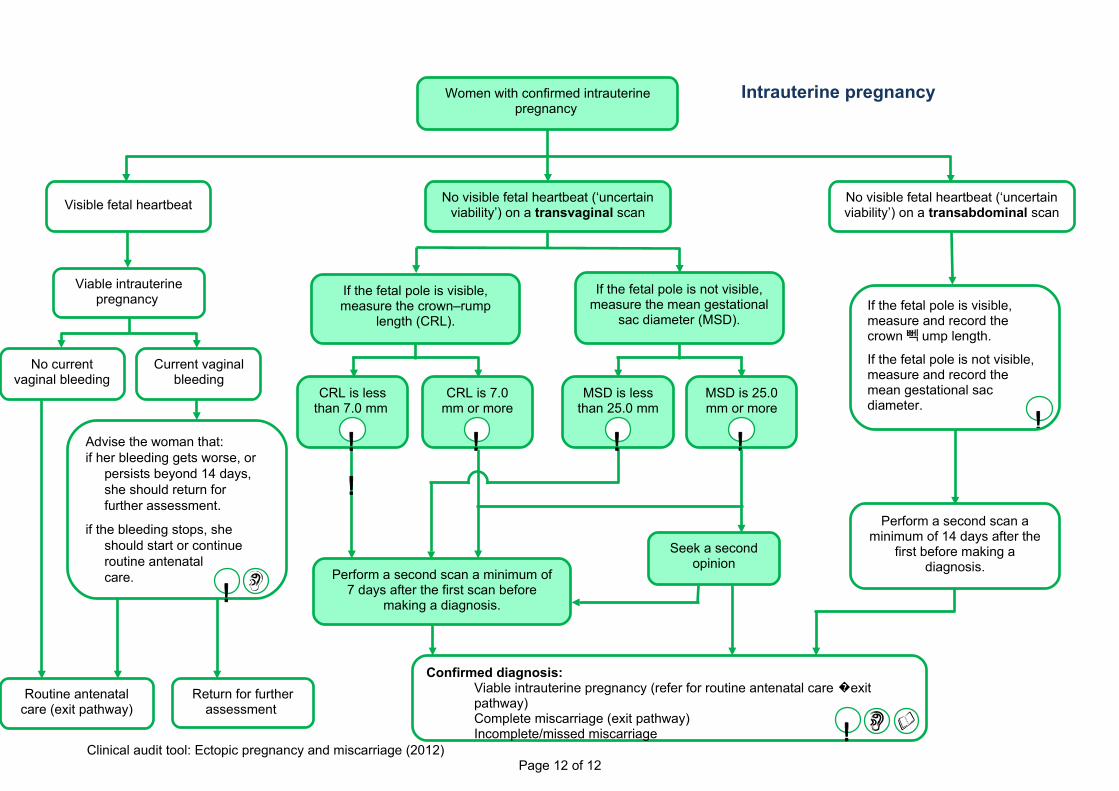
Appendix
These extracts from the care pathway has been taken from the full guideline. The shaded boxes show the parts of the care pathway that are included in the audit tool.
Initial ultrasound scan
Throughout the care pathway, where these symbols appear, provide women with information about:
Where to seek help in an emergency
Where to access support and counselling services
The recovery period!
Ectopic pregnancy Pregnancy of unknown location
Transvaginal ultrasound scan(unless transabdominal scan is indicated or is
the woman’s preference)
Suspected molar pregnancy (outside
scope of guideline – exit pathway)
Intrauterine pregnancy (see below)
Women referred to an early pregnancy assessment service (or out-of-hours gynaecology service if the early pregnancy assessment service is not open)
Women who have self-referred to an early pregnancy assessment service because they have had recurrent miscarriage or a previous ectopic or molar pregnancy
!!
!
If the fetal pole is visible, measure and record the crown뻭 ump length.
If the fetal pole is not visible, measure and record the mean gestational sac diameter.
Perform a second scan a minimum of 14 days after the
first before making a diagnosis.
Confirmed diagnosis:Viable intrauterine pregnancy (refer for routine antenatal care exit �pathway)Complete miscarriage (exit pathway) Incomplete/missed miscarriage !
Seek a second opinion
Perform a second scan a minimum of 7 days after the first scan before
making a diagnosis.
If the fetal pole is visible, measure the crown–rump
length (CRL).
If the fetal pole is not visible, measure the mean gestational
sac diameter (MSD).
MSD is less than 25.0 mm
!
CRL is 7.0 mm or more
!
MSD is 25.0 mm or more
!
CRL is less than 7.0 mm
!
!
Viable intrauterine pregnancy
No current vaginal bleeding
Current vaginal bleeding
Women with confirmed intrauterine pregnancy
Visible fetal heartbeatNo visible fetal heartbeat (‘uncertain
viability’) on a transvaginal scanNo visible fetal heartbeat (‘uncertain viability’) on a transabdominal scan
Advise the woman that:if her bleeding gets worse, or
persists beyond 14 days, she should return for further assessment.
if the bleeding stops, she should start or continue routine antenatal care.
Routine antenatal care (exit pathway)
Return for further assessment
!
Clinical audit tool: Ectopic pregnancy and miscarriage (2012)Page 12 of 12
Intrauterine pregnancy
Related Documents





