Arnold J. Greenspon M.D. Professor of Medicine Jefferson Medical College Philadelphia, PA ATRIAL FIBRILLATION 2014: AN UPDATE Disclosure of Financial Relationships Disclosure of Financial Relationships Arnold J. Greenspon M.D. Has no relationships with any entity producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Arnold J. Greenspon M.D.
Professor of Medicine
Jefferson Medical College
Philadelphia, PA
ATRIAL FIBRILLATION 2014:
AN UPDATE
Disclosure of Financial RelationshipsDisclosure of Financial Relationships
Arnold J. Greenspon M.D.
Has no relationships with any entity producing, marketing, re-selling, or
distributing health care goods or services consumed by, or used on, patients.

EpidemiologyScope of the Problem
EpidemiologyScope of the Problem
� More than 2 million patients in the US with AF
� Major impact on the elderly
� Prevalence increase as population ages
� Substantial morbidity due to symptoms
� Associated with stroke, heart, failure, and death
� Most common arrhythmia requiring hospitalization
Atrial Fibrillation Demographics by Age
Adapted from Feinberg WM. Arch Intern Med. 1995;155:469-473.
U.S. population
Population with
atrial fibrillation
Age, yr
<5 5-
9
10-
14
15-
19
20-
24
25-
29
30-
34
35-
39
40-
44
45-
49
50-
54
55-
59
60-
64
65-
69
70-
74
75-
79
80-
84
85-
89
90-
94
>95
U.S. population x 1000 Population with AF x 1000
30,000
20,000
10,000
0
500
400
300
200
100
0
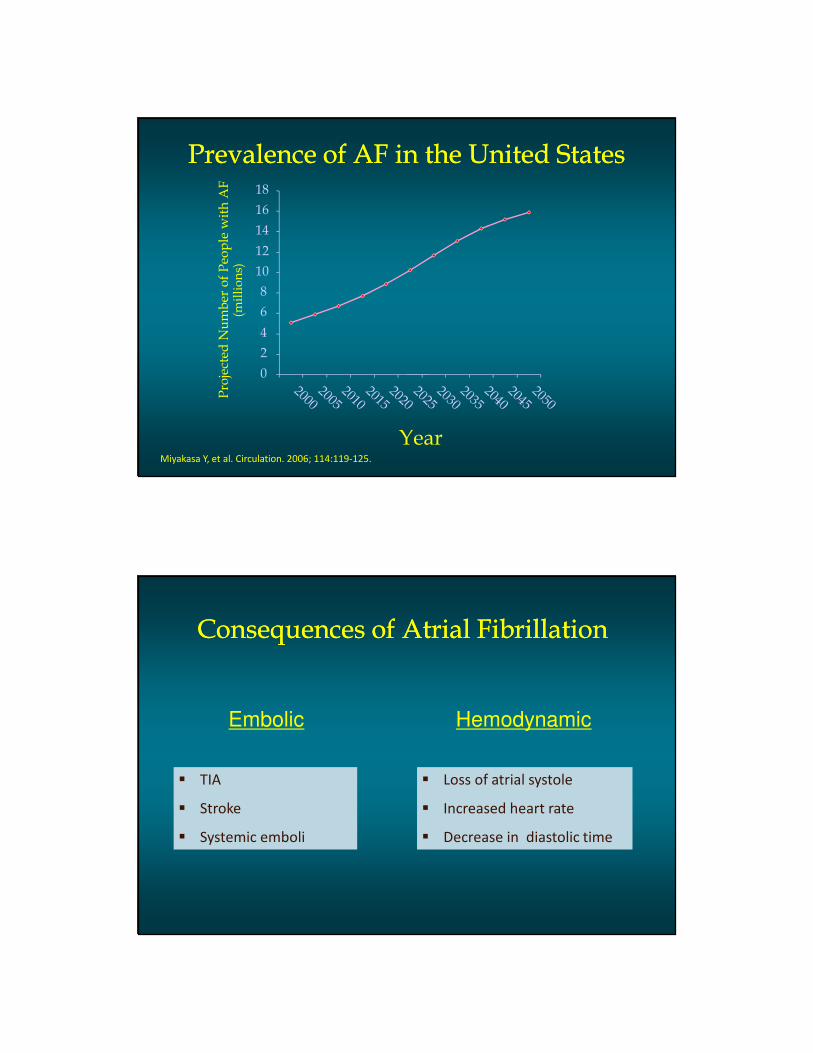
Prevalence of AF in the United StatesPrevalence of AF in the United States
0
2
4
6
8
10
12
14
16
18
Year
Pro
ject
ed N
um
ber
of
Peo
ple
wit
h A
F
(mil
lio
ns)
Miyakasa Y, et al. Circulation. 2006; 114:119-125.
Consequences of Atrial FibrillationConsequences of Atrial Fibrillation
Embolic Hemodynamic
� TIA
� Stroke
� Systemic emboli
� Loss of atrial systole
� Increased heart rate
� Decrease in diastolic time

Management of Atrial FibrillationManagement of Atrial Fibrillation
Control of symptoms
� Rate vs Rhythm
� Role of cardioversion
Stroke Prevention
� Risk assessment
� Role of anticoagulation
Types of Atrial FibrillationTypes of Atrial Fibrillation
Episode of AF
Paroxysmal Persistent Permanent

Atrial Fibrillation: DefinitionsAtrial Fibrillation: Definitions
� Paroxysmal
� AF that terminates spontaneously within 7 days
� Persistent
� AF that requires cardioversion for termination
� Permanent
� Sinus rhythm cannot be restored
Atrial Fibrillation is Associated with StrokeAtrial Fibrillation is Associated with Stroke
Hart et al. Ann Intern Med. 1999;131:492-501.
Str
oke (
%)
AFASAK SPAF BAATAF CAFA SPINAF
Stroke Rates in Placebo-Treated Patients With AF
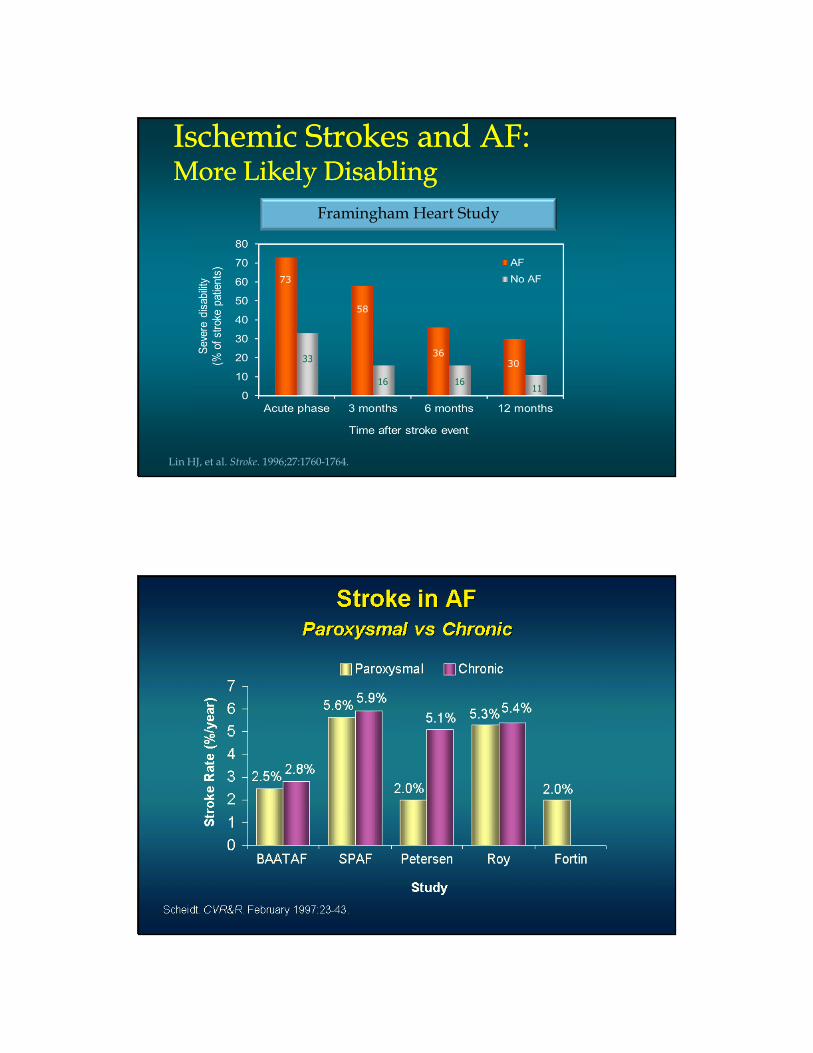
Ischemic Strokes and AF:More Likely DisablingIschemic Strokes and AF:More Likely Disabling
73
33
58
16
36
16
30
11
Framingham Heart Study
Lin HJ, et al. Stroke. 1996;27:1760-1764.
Prevalence of Stroke vs AgeFramingham Data
Prevalence of Stroke vs AgeFramingham Data
Age Groups
Str
ok
e R
ate
/10
00
Wolf et al. Arch Intern Med. 1987;147:1561-1564.
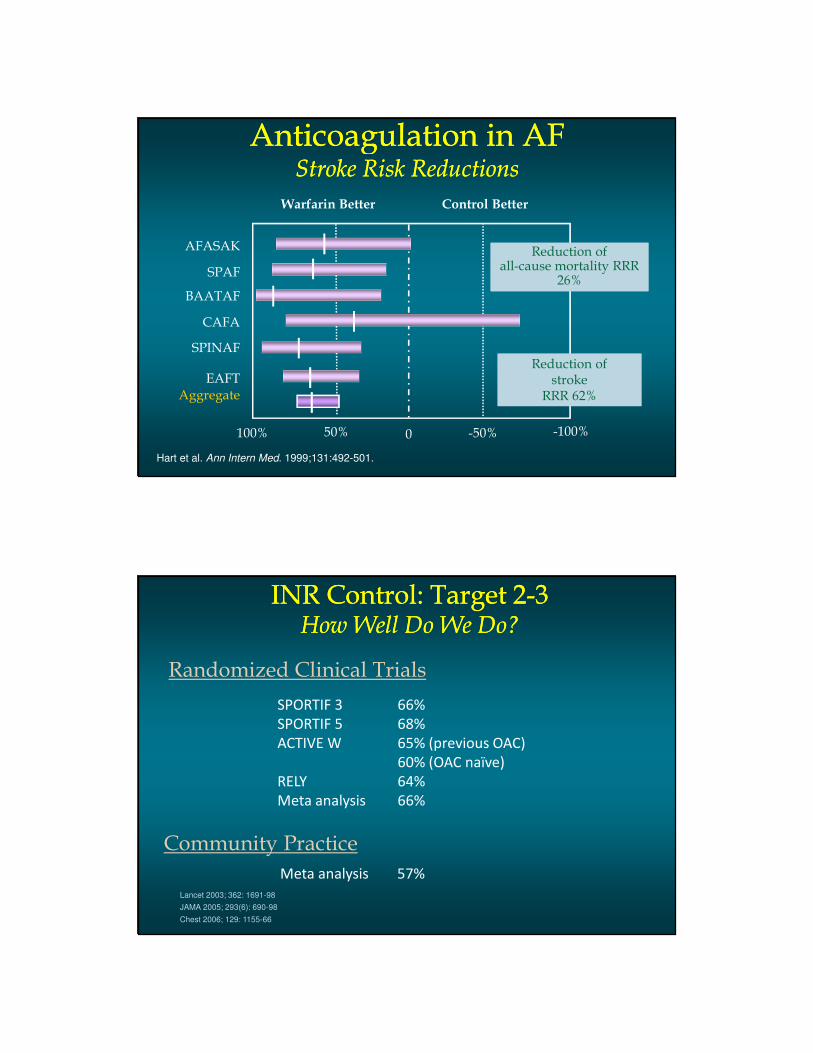
Anticoagulation in AFStroke Risk Reductions
Anticoagulation in AFStroke Risk Reductions
Hart et al. Ann Intern Med. 1999;131:492-501.
Aggregate
Warfarin Better Control Better
AFASAK
SPAF
BAATAF
CAFA
SPINAF
EAFT
100% 50% 0 -50% -100%
Reduction of stroke
RRR 62%
Reduction of stroke
RRR 62%
Reduction ofall-cause mortality RRR
26%
Reduction ofall-cause mortality RRR
26%
INR Control: Target 2-3How Well Do We Do?
INR Control: Target 2-3How Well Do We Do?
Lancet 2003; 362: 1691-98
JAMA 2005; 293(6): 690-98
Chest 2006; 129: 1155-66
SPORTIF 3 66%
SPORTIF 5 68%
ACTIVE W 65% (previous OAC)
60% (OAC naïve)
RELY 64%
Meta analysis 66%
Randomized Clinical Trials
Community Practice
Meta analysis 57%

Ischemic Stroke andIntracranial BleedingIschemic Stroke andIntracranial Bleeding
Fuster et al. J Am Coll Cardiol. 2001;38:1231-1265; Hylek et al. Ann Intern Med. 1994;120:897-902.
INR
Od
ds R
ati
o
20
15
10
5
1
1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0
Ischemic stroke
Intracranial bleeding
Issues and Challenges for Stroke Prevention in AF Patients
Issues and Challenges for Stroke Prevention in AF Patients
� Warfarin is effective but difficult to use
� Not all patients take or tolerate warfarin
� Time in therapeutic range often low
� Risk of bleeding
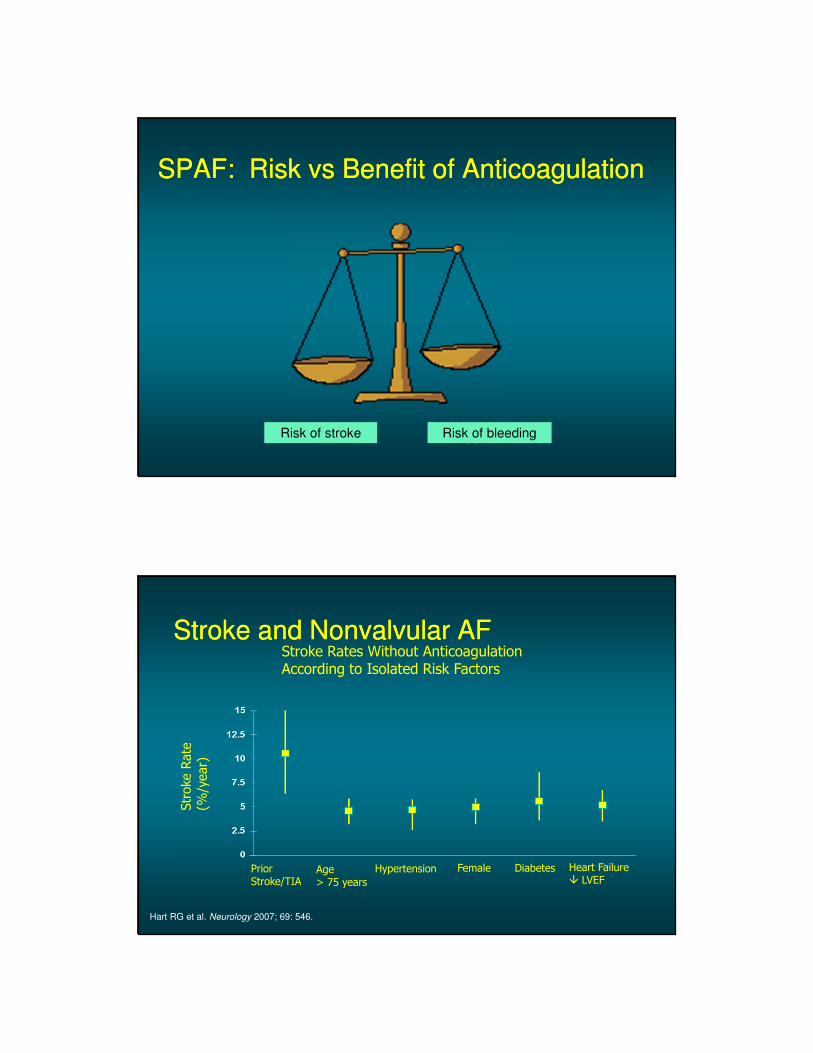
SPAF: Risk vs Benefit of AnticoagulationSPAF: Risk vs Benefit of Anticoagulation
Risk of stroke Risk of bleeding
Stroke and Nonvalvular AFStroke and Nonvalvular AF
PriorStroke/TIA
Age> 75 years
Hypertension Female Diabetes Heart Failure� LVEF
Hart RG et al. Neurology 2007; 69: 546.
Stroke Rates Without AnticoagulationAccording to Isolated Risk Factors

The CHADS2 ScoreStroke Risk Score for Atrial Fibrillation
The CHADS2 ScoreStroke Risk Score for Atrial Fibrillation
Congestive Heart failure 1 32
Hypertension 1 65
Age > 75 years 1 28
Diabetes mellitus 1 18
Stroke or TIA 2 10
Moderate-High risk >2Low risk 0-1
VanWalraven C, et al. Arch Intern Med 2003; 163:936.
Prevalence (%)Score (points)
CHADS2 Score: Targeted TherapyCHADS2 Score: Targeted TherapyCHADS2
Score
Adjusted Stroke Rate†
(95% CI)
CHADS2
Risk Level
0 1.9 (1.2-3.0) Low
1 2.8 (2.0-3.8) Low
2 4.0 (3.1-5.1) Moderate
3 5.9 (4.6-7.3) Moderate
4 8.5 (6.3-11.1) High
5 12.5 (8.2-17.5) High
6 18.2 (10.5-27.4) High
†Expected rate of stroke per 100 patient-years.
Snow et al. Ann Intern Med. 2003;139:1009-1017.
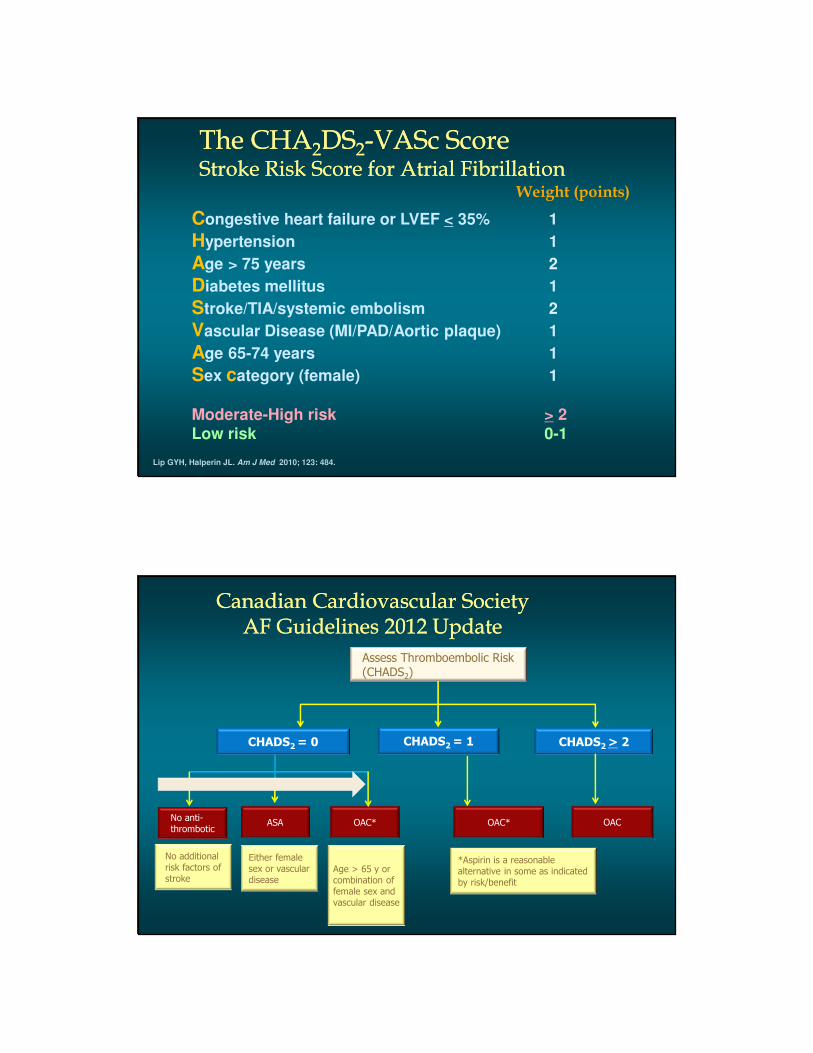
The CHA2DS2-VASc ScoreStroke Risk Score for Atrial Fibrillation
The CHA2DS2-VASc ScoreStroke Risk Score for Atrial Fibrillation
Lip GYH, Halperin JL. Am J Med 2010; 123: 484.
Congestive heart failure or LVEF < 35% 1
Hypertension 1
Age > 75 years 2
Diabetes mellitus 1
Stroke/TIA/systemic embolism 2
Vascular Disease (MI/PAD/Aortic plaque) 1
Age 65-74 years 1
Sex category (female) 1
Moderate-High risk > 2Low risk 0-1
Weight (points)
Canadian Cardiovascular SocietyAF Guidelines 2012 Update
Canadian Cardiovascular SocietyAF Guidelines 2012 Update
Increasing stroke risk
CHADS2 = 0 CHADS2 = 1 CHADS2 > 2
No anti-thrombotic
ASA OAC* OAC* OAC
No additionalrisk factors of stroke
Either female sex or vascular disease
Age > 65 y or combination of female sex and vascular disease
*Aspirin is a reasonable alternative in some as indicated by risk/benefit
Assess Thromboembolic Risk (CHADS2)

Risk of Bleeding: HAS-BLED ScoreRisk of Bleeding: HAS-BLED Score
Hypertension (> 160 mm Hg systolic) 1
Abnormal renal or hepatic function 1-2
Stroke 1
Bleeding history or anemia 1
Labile INR (TTR < 60%) 1
Elderly (age > 75 years) 1
Drugs (antiplatelet, NSAID) or alcohol 1-2
High risk (> 4%/year) > 4Moderate risk (2-4%/year) 2-3Low risk (< 2%.year) 0-1
Pisters R, et al. Chest 2010; 138: 1093.
Lip GYH, et al. J Am Coll Cardiol 2010; 57: 173.
Risk Score for Predicting Bleeding inAnticoagulated Patients with Atrial Fibrillation
CHADS2 vs CHADS2-VAScCHADS2 vs CHADS2-VASc
2012 focused update of the ESC Guidelines for the management of atrial fibrillation: Europace. 2012 Aug 24
� Guideline recommends a shift towards focus on low risk
� No recommendation on composite bleeding stroke risk score

Subclinical AF and Risk of StrokeSubclinical AF and Risk of Stroke
Healey JS, et al. NEJM 2012; 366:120-129
Str
oke o
r S
yste
mic
Em
bolis
m
Years
Atrial tachyarrhythmia > 6 min ≤ 3 months after pacemaker or defibrillator implantation
Progression of Atrial FibrillationProgression of Atrial Fibrillation
Paroxysmal
Self-Terminating
Persistent
Lasts > 7 Days
Permanent
Cardioversion Failed or Not Attempted
Normal Sinus Rhythm
Atrial Fibrillation
Paroxysmal AF is as likely to cause stroke aspersistent or permanent AF
SPAF: The Challenge of Assessing Stroke Risk
SPAF: The Challenge of Assessing Stroke Risk
• Paroxysmal AF is difficult to detect.
• 24h Holter is often insufficient. Prolonged monitoring may
be necessary.
• Many strokes are misclassified as “cryptogenic”.
• The misclassified strokes are really thromboembolic and
warrant anticoagulation.
• Patients with PAF and risk factors need OAC.
SPAF: Challenges for the FutureSPAF: Challenges for the Future
� Better risk-stratification
� Balancing stroke vs bleeding
� Methods to better predict events and guide therapy
� Successful rhythm control over time (?)
� Safer treatments for the highest risk patients
� Role of new anticoagulants
VIIIntrinsic
Pathway
Extrinsic
Pathway
IX
II (prothrombin)
XI
XIIXIIa
XX
VIIaIXa
XIa
II (thrombin)
XXa
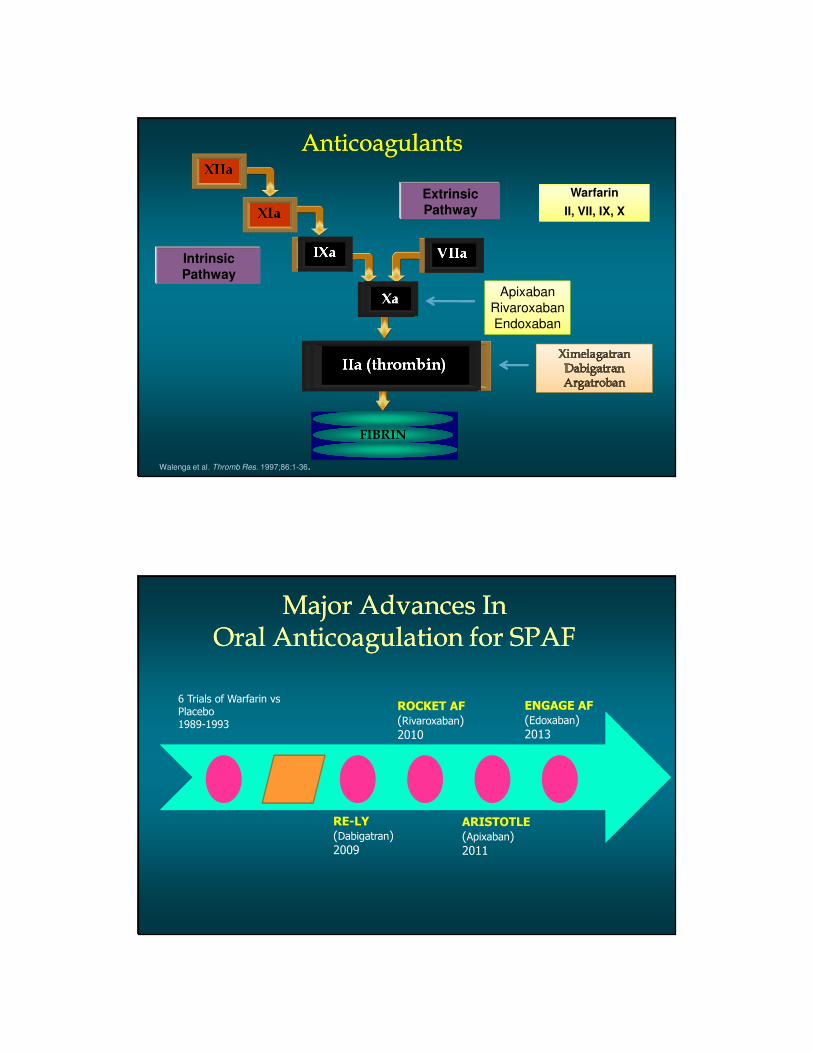
AnticoagulantsAnticoagulants
XXa
IIa (thrombin)
Warfarin
II, VII, IX, X
VIIaIXa
XXa
IIa (thrombin)
FIBRINOGENFIBRINOGENFIBRINFIBRIN
Walenga et al. Thromb Res. 1997;86:1-36.
Apixaban
Rivaroxaban
Endoxaban
Major Advances In Oral Anticoagulation for SPAF
Major Advances In Oral Anticoagulation for SPAF
6 Trials of Warfarin vs Placebo1989-1993
RE-LY
(Dabigatran)2009
ROCKET AF
(Rivaroxaban)2010
ARISTOTLE
(Apixaban)2011
ENGAGE AF
(Edoxaban)2013
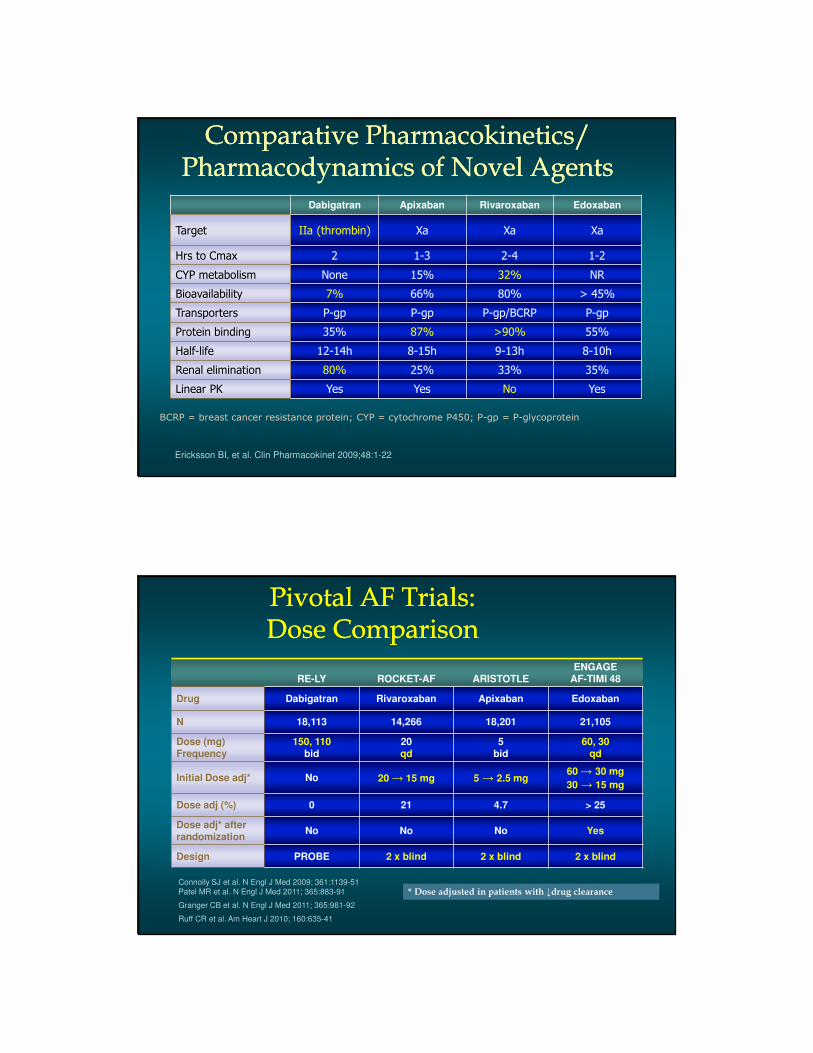
Comparative Pharmacokinetics/ Pharmacodynamics of Novel Agents
Comparative Pharmacokinetics/ Pharmacodynamics of Novel Agents
Dabigatran Apixaban Rivaroxaban Edoxaban
Target IIa (thrombin) Xa Xa Xa
Hrs to Cmax 2 1-3 2-4 1-2
CYP metabolism None 15% 32% NR
Bioavailability 7% 66% 80% > 45%
Transporters P-gp P-gp P-gp/BCRP P-gp
Protein binding 35% 87% >90% 55%
Half-life 12-14h 8-15h 9-13h 8-10h
Renal elimination 80% 25% 33% 35%
Linear PK Yes Yes No Yes
Ericksson BI, et al. Clin Pharmacokinet 2009;48:1-22
BCRP = breast cancer resistance protein; CYP = cytochrome P450; P-gp = P-glycoprotein
Pivotal AF Trials:Dose ComparisonPivotal AF Trials:Dose Comparison
RE-LY ROCKET-AF ARISTOTLEENGAGE
AF-TIMI 48
Drug Dabigatran Rivaroxaban Apixaban Edoxaban
N 18,113 14,266 18,201 21,105
Dose (mg)Frequency
150, 110bid
20 qd
5bid
60, 30qd
Initial Dose adj* No 20 → 15 mg 5 → 2.5 mg60 → 30 mg
30 → 15 mg
Dose adj (%) 0 21 4.7 > 25
Dose adj* after randomization
No No No Yes
Design PROBE 2 x blind 2 x blind 2 x blind
Connolly SJ et al. N Engl J Med 2009; 361:1139-51
Patel MR et al. N Engl J Med 2011; 365:883-91
Granger CB et al. N Engl J Med 2011; 365:981-92
Ruff CR et al. Am Heart J 2010; 160:635-41
* Dose adjusted in patients with ↓drug clearance
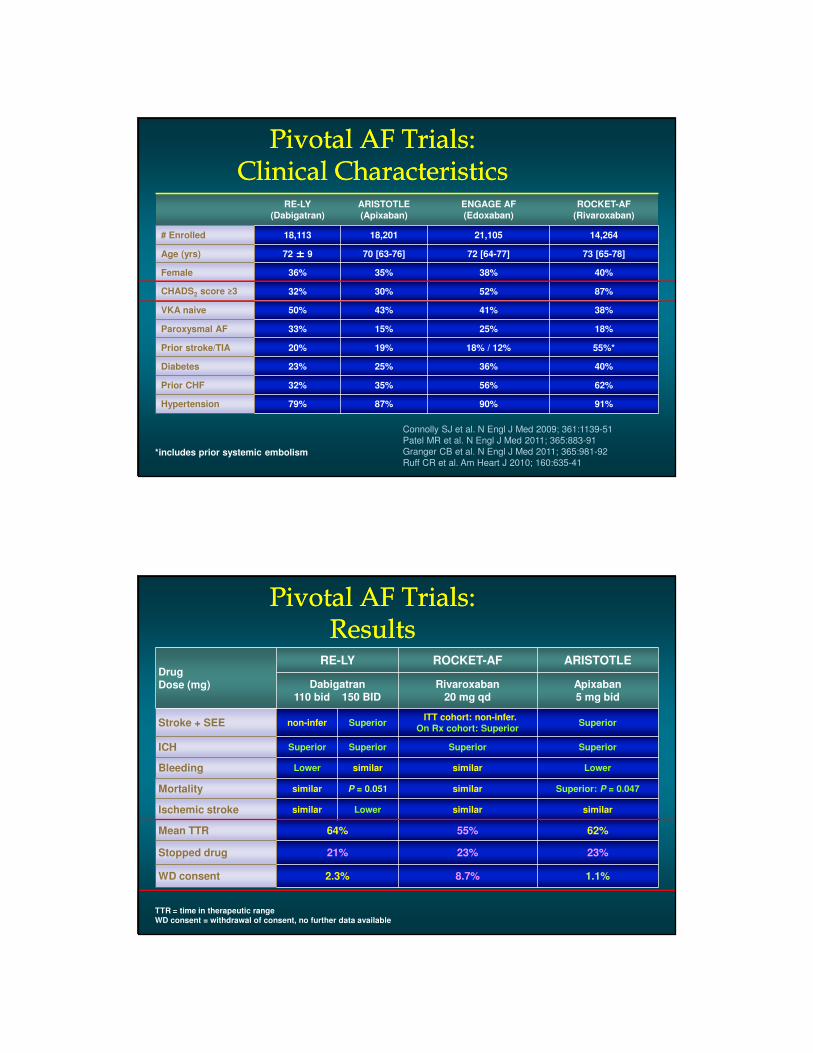
Pivotal AF Trials:Clinical Characteristics
Pivotal AF Trials:Clinical Characteristics
RE-LY
(Dabigatran)
ARISTOTLE
(Apixaban)
ENGAGE AF
(Edoxaban)
ROCKET-AF
(Rivaroxaban)
# Enrolled 18,113 18,201 21,105 14,264
Age (yrs) 72 ±±±± 9 70 [63-76] 72 [64-77] 73 [65-78]
Female 36% 35% 38% 40%
CHADS2 score ≥3 32% 30% 52% 87%
VKA naive 50% 43% 41% 38%
Paroxysmal AF 33% 15% 25% 18%
Prior stroke/TIA 20% 19% 18% / 12% 55%*
Diabetes 23% 25% 36% 40%
Prior CHF 32% 35% 56% 62%
Hypertension 79% 87% 90% 91%
*includes prior systemic embolism
Connolly SJ et al. N Engl J Med 2009; 361:1139-51
Patel MR et al. N Engl J Med 2011; 365:883-91
Granger CB et al. N Engl J Med 2011; 365:981-92
Ruff CR et al. Am Heart J 2010; 160:635-41
Pivotal AF Trials:Results
Pivotal AF Trials:Results
DrugDose (mg)
RE-LY ROCKET-AF ARISTOTLE
Dabigatran110 bid 150 BID
Rivaroxaban20 mg qd
Apixaban5 mg bid
Stroke + SEE non-infer Superior ITT cohort: non-infer.
On Rx cohort: SuperiorSuperior
ICH Superior Superior Superior Superior
Bleeding Lower similar similar Lower
Mortality similar P = 0.051 similar Superior: P = 0.047
Ischemic stroke similar Lower similar similar
Mean TTR 64% 55% 62%
Stopped drug 21% 23% 23%
WD consent 2.3% 8.7% 1.1%
TTR = time in therapeutic rangeWD consent = withdrawal of consent, no further data available
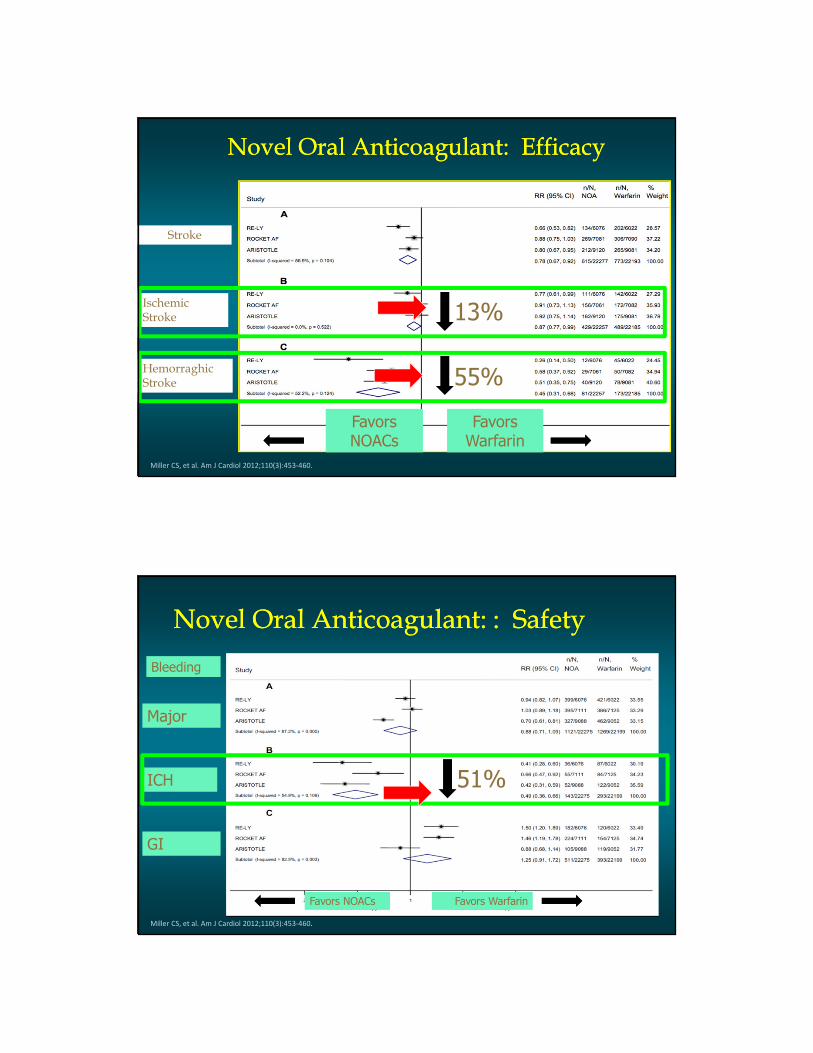
Novel Oral Anticoagulant: EfficacyNovel Oral Anticoagulant: Efficacy
Stroke
Ischemic Stroke
HemorraghicStroke
Miller CS, et al. Am J Cardiol 2012;110(3):453-460.
Favors NOACs
Favors Warfarin
13%
55%
Novel Oral Anticoagulant: : Safety Novel Oral Anticoagulant: : Safety
Major
ICH
GI
Bleeding
Favors NOACs Favors Warfarin
Miller CS, et al. Am J Cardiol 2012;110(3):453-460.
51%
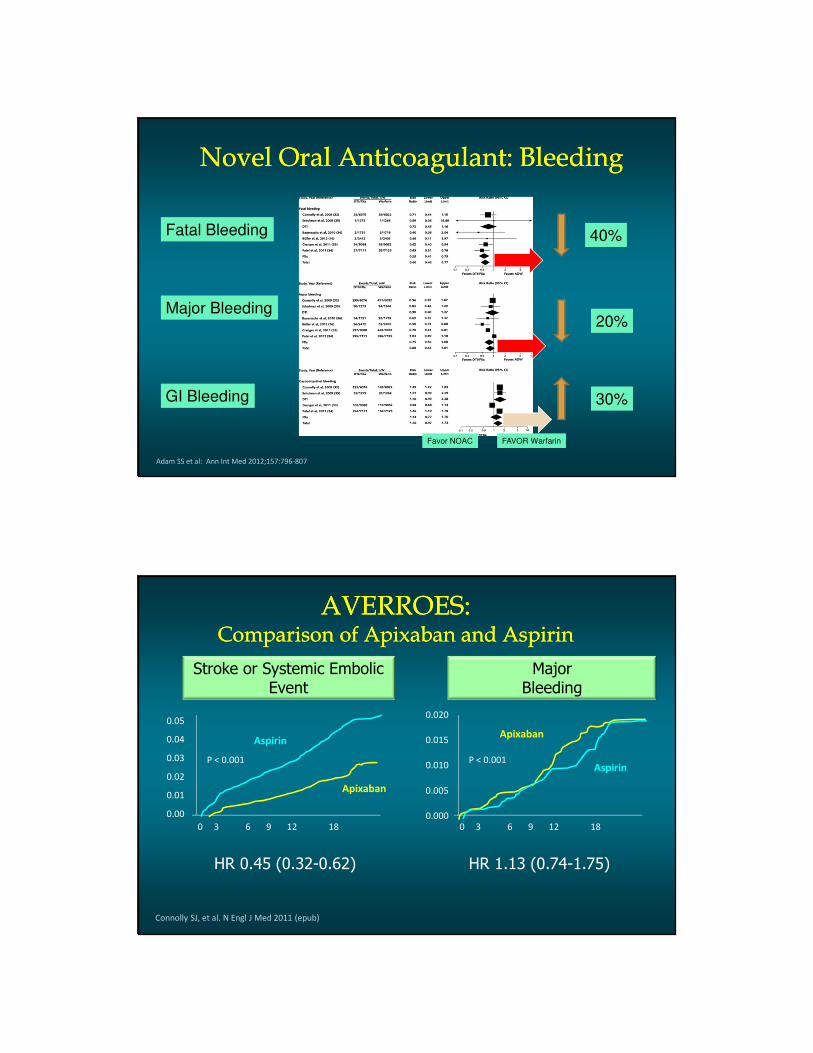
Novel Oral Anticoagulant: BleedingNovel Oral Anticoagulant: Bleeding
Fatal Bleeding
Major Bleeding
GI Bleeding
40%
20%
30%
Favor NOAC FAVOR Warfarin
Adam SS et al: Ann Int Med 2012;157:796-807
AVERROES: Comparison of Apixaban and Aspirin
AVERROES: Comparison of Apixaban and Aspirin
Stroke or Systemic Embolic Event
Major Bleeding
HR 0.45 (0.32-0.62) HR 1.13 (0.74-1.75)
Connolly SJ, et al. N Engl J Med 2011 (epub)
Aspirin
Apixaban
P < 0.001
0 3 6 9 12 18
0.05
0.04
0.03
0.02
0.01
0.00
Aspirin
Apixaban
P < 0.001
0 3 6 9 12 18
0.020
0.015
0.010
0.005
0.000
Summary of SPAF GuidelinesSummary of SPAF Guidelines
� The CHADS2-VASc is probably best for identifying low-
risk patients
� The HAS-BLED score assesses bleeding risk.
� Correct the correctable
� HAS-BLED>3- caution and regular review advised
� NOACs offer better efficacy, and convenience
compared to VKAs
� No data to recommend one over the other
� Efficacy of ASA is weak
� Risk of bleeding same as OAC
Atrial Fibrillation: ManagementAtrial Fibrillation: Management
Rate control Rhythm control
Why Are There No New Drugs for Rhythm Control??
Why Are There No New Drugs for Rhythm Control??
Antiarrhythmic Drugs=
Poisons with beneficial side effects
Definition:
Drugs for Rhythm ControlDrugs for Rhythm Control
� Class I Drugs- Na+ Blockers (slow conduction)
� IA Quinidine or Disopyramide
� IC (avoid in pts with CAD, CM)
� Flecainide 100-225mg bid
� Propafenone 150-225 mg tid or bid
� Class III Drugs- K+ Blockers (prolong repolarization)
� Sotalol 80-160 mg bid (may not be tolerated in CHF)
� Dofetilide 0.125-0.500 mg bid (may be used in CHF, but must watch QTc, K+, creatinine)
� Dronedarone 400 mg BID (avoid CHF or permanent AF)
� Amiodarone 100-200 mg daily (drug of choice in pts with CHF)

Canadian Trial of Atrial Fibrillation (CTAF):
Rhythm Control
Canadian Trial of Atrial Fibrillation (CTAF):
Rhythm Control
Rate of recurrence lowest with amiodarone
Roy D, Talajic M, Dorain P et al: N Eng J Med 2000;342:913
AFFIRM: Rate control versus Rhythm controlAFFIRM: Rate control versus Rhythm control
Wyse DG, Waldo AL, DiMarco JP, et al: N Eng J Med 2002;3347:1825
p=0.058

Mortality
Rhythm or Rate Control in AF
Rate
Control
Rhythm
Control P-value
PIAF 1 (0.8%) 2 (1.6%) ns
STAF 8 (8%) 4 (4%) ns
AFFIRM 306 (26%) 356 (27%) .058
RACE 18 (7.0%) 18 (6.7%) ns
0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8 2.0
Rhythm Control Worse
Rhythm Control Better
AFFIRM(n=4060)
1.28 (0.95 – 1.72)
RACE(n=522)
2.25 (1.88 – 5.75)
STAF(n=200)
3.01 (0.35 – 25.30)
PIAF(n=252)
4.92 (0.58 – 41.50)
TOTAL(n=5034)
1.36 (1.03 – 1.78)
2.2P=.04
2.4
Cerebrovascular Events
Rhythm or Rate Control in AF

Relationship between NSR, Treatment, and Survival in AFFIRM: AFFIRM substudyRelationship between NSR, Treatment, and Survival in AFFIRM: AFFIRM substudy
Covariate p-value H.R. 99% CI
Sinus rhythm <0.0001 0.53 0.39-0.72
Warfarin use <0.0001 0.50 0.37-0.69
Digoxin use 0.0007 1.42 1.09-1.86
AAD use 0.0005 1.49 1.11-2.01
Time-Dependent Co-variates Associated with Survival
AFFIRM Investigators: Circulation 2004;109:1509-1513
Toxicity of antiarrhythmic drugs counterbalances the benefits of SR
AF Clinical Trials: Rhythm vs Rate Control
� Mortality is similar, regardless of treatment strategy
� Lenient control (mean rate<110 bpm) as good as
strict control (mean rate <80 bpm)
� RACE II: NEJM 2010;362:1363
� Anticoagulation in patients at high risk for stroke is
important, regardless of rate or rhythm treatment
strategy

What AFFIRM did not answer:
� Is NSR associated with an
improved outcome in high-risk,
symptomatic patients?
� Is NSR preferable in young
patients?
� Is rhythm control superior if
patients receive OAC?
The management cascade for patients with AFCardioversion, TEE and anticoagulation
AF = atrial fibrillation; DCC = direct current cardioversion; LA = left atrium; LAA = left atrial appendage; OAC = oral anticoagulant;SR= sinus rhythm; TEE= transesophageal echocardiography.AF = atrial fibrillation; DCC = direct current cardioversion; LA = left atrium; LAA = left atrial appendage; OAC = oral anticoagulant;SR= sinus rhythm; TEE= transesophageal echocardiography.
Eur Heart J 2013;31:2369-2429
TEE
Recent onsetConventional strategyTEE strategy
Standard OAC or TEE

Choose antiarrhythmic drugaccording to underlying pathology
Eur Heart J 2013;31:2369-2429
(?)
Treatment of AF:Non-pharmacologic Options
Treatment of AF:Non-pharmacologic Options
� Rate control
� Ablate and pace
� Surgical
� Cox-MAZE procedure
� Radiofrequency catheter ablation
� Pulmonary vein isolation
� Extended LA ablation

Cox J L Europace 2003;5:S20-S29
Surgical procedure for AF: Standard Maze-III Surgical procedure for AF: Standard Maze-III
Angiogram of a Left Inferior Pulmonary Vein Depicting the Source and Exit of Ectopic Activity.
Haïssaguerre M et al. N Engl J Med 1998;339:659-666.

Initiation of Focal AFInitiation of Focal AF
Haissaguerre et al. NEJM 1998;389:659-66
AF Ablation: Targeting and isolating pulmonary veinsAF Ablation: Targeting and isolating pulmonary veins
Ames A , Stevenson W G Circulation 2006;113:e666-e668a

Electroanatomic map with an integrated computed tomographic image of the left atrium and pulmonary veins (viewed from the back) showing the lesion set created for ablation of paroxysmal
atrial fibrillation.
Calkins H Circulation. 2012;125:1439-1445
AF Ablation: Creating PVIAF Ablation: Creating PVI
Tung R et al. Circulation 2012;126:223-229

Ablation of Persistent AF: Additional lesions requiredAblation of Persistent AF:
Additional lesions required
Tung R et al. Circulation 2012;126:223-229
Efficacy of Antiarrhythmic Drugs versus Catheter AblationEfficacy of Antiarrhythmic Drugs versus Catheter Ablation
Me
ta-a
na
lyze
d p
rop
ort
ion
o
f p
ati
en
ts (
%)
Drugs (N=34 studies) Ablation (N=63 studies)
Treatment
success
Recurrent
AF
Single-
procedure
success
off AAD
Multiple-
procedure
success
off AAD
Single-
procedure
success
on AAD or
uncertain
Multiple-
procedure
success
on AAD or
uncertain
Patients
requiring
repeat
ablation
0
10
20
30
40
50
60
70
80
90
Calkins H: Circ Arrhy Electrophysiol 2009;2:349
N= 6589 N=6936

AF Ablation ComplicationsAF Ablation Complications� Mortality
� Death overall 0.7%
� Procedure-related 0%
� Vascular access <1%
� Periprocedural events
� TIA/Stroke 0.5%
� Cardiac tamponade 0.8%
� Pericardial effusion 0.6%
� PV stenosis 1.6%
� LA-esophageal fistula 0%
� Total= 4.9%
Calkins H: Circ Arrhy Electrophysiol 2009;2:349

SummarySummary
� AF is a common disorder whose incidence is expected to rise dramatically
� Stroke prevention is a critical component of management in patients with AF
� Anticoagulation is underutilized
� Even when utilized, current anticoagulant characteristics limit the ability to maintain patients within target range
� Emerging anticoagulant agents without some of these limitations may improve stroke prevention
� Rate control vs rhythm management based on clinical assessment
� AF ablation is a Rx option for highly symptomatic patients
Related Documents











