ATHABASCA UNIVERSITY UNIVERSITY OF CALGARY UNIVERSITY OF LETHBRIDGE A FACILITATOR TRAINING MANUAL FOR PARENTING IN EARLY RECOVERY FROM SUBSTANCE USE BY KAREN JANZEN A Final Project submitted to the Campus Alberta Applied Psychology: Counselling Initiative in partial fulfillment of the requirements for the degree of MASTER OF COUNSELLING Alberta June 2007

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ATHABASCA UNIVERSITY
UNIVERSITY OF CALGARY
UNIVERSITY OF LETHBRIDGE
A FACILITATOR TRAINING MANUAL FOR PARENTING IN EARLY RECOVERY
FROM SUBSTANCE USE
BY
KAREN JANZEN
A Final Project submitted to the
Campus Alberta Applied Psychology: Counselling Initiative
in partial fulfillment of the requirements for the degree of
MASTER OF COUNSELLING
Alberta
June 2007
i
ABSTRACT
Peardonville House initiated its Strengthening Mothers parenting program based on the belief
that recovery from substance use and the therapeutic needs of mothers and children are
optimally met in a professionally facilitated group format. The program is focused on
teaching mothers how to balance early recovery from substance use with the demands of
parenting. However, the Strengthening Mothers program has lacked a formal training
manual, limiting the effectiveness of the program facilitators. Within this applied project
document, the author describes the development of a treatment facilitator manual and
includes the manual as the product of this endeavour. The aim is to bridge various relevant
disciplines and provide facilitators with the necessary theoretical and practical knowledge to
conduct group sessions. The intent of the manual is to foster facilitator uniformity and to
establish an appropriate group framework, hence increasing the effectiveness of the
Strengthening Mothers parenting program at Peardonville House.
ii
ACKNOWLEDGEMENTS
I would like to acknowledge Gina Wong-Wylie for her considerable time and patience in
guiding me from beginning to end. Her support helped in my efforts towards bringing
research, form and understanding from a concept that has taken meaning in this project.
Along the way, she has helped me develop a deep sense of appreciation for the work of
research writing, and for those who engage in it regularly. Thanks so much Gina!
Carl, my soul-mate and rock! Your support and faith in me has been a powerful source of
support during this program. We did it! Also, to our amazing children Carly, Matt, Spencer,
Kaden, Madeleine, Ryder and the others, thanks for sharing mom time and making life
passionate. I love you lots! Lastly, to Pam, Laurie, Kim and Heather the gang at Peardonville
House who believed in me and took care of me and taught me about life. Much thanks.
iii
TABLE OF CONTENTS
CHAPTER I INTRODUCTION ............................................................................................1
PROJECT RATIONALE...............................................................................................2
PURPOSE......................................................................................................................3
OVERVIEW ..................................................................................................................4
CHAPTER II LITERATURE REVIEW ..............................................................................6
WOMEN AND SUBSTANCE USE .............................................................................6
PATH TO TREATMENT..................................................................................7
BARRIERS........................................................................................................8
BIOPSYCHOSOCIAL-SPIRITUAL PERSPECTIVE....................................11
PARENTING EDUCATION PROGRAMS................................................................14
GOALS OF PARENTING EDUCATION GROUPS .....................................16
GROUP PARENTING PROGRAMS .............................................................17
BRIDGING SUBSTANCE USE AND PARENTING................................................19
CONCLUSION............................................................................................................21
CHAPTER III FACILITATOR TRAINING MANUAL...................................................29
CHAPTER IV SYTHESIS AND IMPLICATIONS ...........................................................67
PROJECT IMPACT.....................................................................................................67
STRENGTHS ..............................................................................................................68
LIMITATIONS............................................................................................................69
HOW PROJECT MAY BENEFIT OTHERS..............................................................71
FUTURE DIRECTIONS FOR RESEARCH...............................................................71
CONCLUSION............................................................................................................72
1
CHAPTER I
Introduction
Parenting can afford some of the greatest rewards an individual will experience, but
also one of the most significant challenges. It is clear that strong families and effective
parenting are critical in raising emotionally healthy children (Kumpfer & Alvarado, 2003).
However, just what constitutes ‘strong’ families and ‘effective’ parenting is difficult to
explicitly define. Balancing early recovery from substance use and the complex role of
parenting is an exceptionally difficult undertaking. This phase presents a steep learning curve
for many women who may have not experienced positive parenting themselves. Many
women active in their addiction of substance use are unable to meet their children’s needs
physically and emotionally, despite loving their children and wanting the best for them.
Peardonville House is located in the Lower Mainland of British Columbia. It has
been in operation since 1987, offering women a holistic approach to recovery from substance
use. This program is unique in that women are permitted to bring their children, between
three months and six years of age, with them to the treatment facility. This accommodation
arrangement was instigated in 1991 in direct response to the recognition of the barriers that
women experience in seeking help for substance use (Valley Recovery Support Association,
1999). During the past 15 years Peardonville House has offered onsite childcare and parent
training components within their treatment program. The facility has solidified a partnership
with the Ministry for Children and Family Development (MCFD) to provide individual and
group parenting sessions, in addition to a hands-on component in the childcare centre, to
prepare women for their role of primary caregiver.

2
Project Rationale
This project was designed and initiated as a direct result of requests from
Peardonville House treatment program facilitators. The facilitators expressed the need for a
training manual which would provide information as to the theories and skills necessary to
meet the needs of their female clients during the group sessions. Peardonville House program
facilitators are trained in a variety of disciplines, including nursing, social work, early
childhood education, and child and youth care. While each facilitator’s background is unique,
all such disciplines are human service based, and thus provide some commonality. The
training manual is geared for facilitators with training in human services, with at least a four
year baccalaureate degree. A strong background in counselling, child growth and
development, and group process is helpful in assisting facilitators to carry out their work in
an effective manner. The facilitators expressed great interest in gaining a greater
understanding of substance use and the additional challenges that women face within the
parenting context.
I have been employed at Peardonville House for the past 15 years, working as a
parenting counsellor and group facilitator in the Strengthening Mothers program with the
mothers and their children. It is a privilege and an honour to work with such resilient
individuals. I have been able to see first hand the love that these women have for their
children, and their desire to parent effectively despite their substance use. As one of the
facilitators of a weekly parenting group, I have observed the need for concordant care
mediated through consistent facilitator training. Such guidance would enable a more
comprehensive psychoeducational program to be established, hence nurturing the confidence
and ability of mothers in our program to parent successfully. The aim of this project was thus
3
to develop a training manual designed to provide direction to facilitators as they assist
women to balance parenting and early recovery from alcohol and drug use.
Furthering the need for this endeavour, Cunningham, Bremner and Boyle (1995)
argue that offering psychoeducational support to parents in a group setting is more cost
effective than individual-based parent training and has been shown to have a better consumer
retention rate. Parents with children who have significant behaviour problems or who have
English as a second language tend to prefer group work to individual sessions (Cunningham,
Bremner, & Boyle). A key component of a successful parenting group is access to an
appropriate facilitator training manual. Training manuals provide uniformity across group
sessions, heighten effectiveness, and preserve a given set of philosophy and procedures
(Wideman, 2003). By designing a training manual, I am seeking to lay the foundation for a
more effective group parenting program aimed at women balancing parenting with early
recovery from substance use.
Purpose
The primary purpose of this project was the development of a manual aimed at
preparing facilitators to deliver a ten week parenting program to women in early recovery
from substance use at Peardonville House. Permission for this project was granted from the
Kinghaven/Peardonville House Society and they were in full support of this work. The
facilitator manual combines the fields of substance use and parenting, with a focus on the
needs of women. The delicate balance between recovery from substance abuse and the
challenges of parenting is also examined. There are many parent education programs which
focus on a single aspect of parenting, often based on the age of the child or the
socioeconomic status of the family. However, there is a paucity of compiled information and
4
program sessions focusing on parenting for women undergoing treatment. The material
covered in the sessions is discussed through the lens of substance use and touches on
reoccurring themes that, while not specific to parenting in recovery, are particularly common
withinin this group. These themes include parenting out of guilt, handling anger, building
trust and promoting attachment, and guiding and setting limits for children. The aim of the
program is for participants to learn strategies for effectively managing their recovery, while
simultaneously coping with the demands of parenting. Within the group parent education
sessions women can ask questions, share frustrations and ideas, and support each other.
Through the program, participants are supported and encouraged in their parenting roles.
They are also armed with new information and ideas as to interacting with their children.
The second key purpose of this project was to equip group facilitators with the ability
to organize and facilitate a group that will have uniformity, purpose, and usefulness to the
participants. The manual provides a series of tools to deal with group dynamics and
challenges that may erupt during sessions. Facilitators also have access to information as to
how to create a safe environment and develop group rules for conducting smooth group
sessions. The training manual thus enables facilitators to deliver effective psychoeducational
parenting groups with mothers in recovery from substance abuse.
Overview
The design of the treatment facilitator manual required an exploration of issues
surrounding women and substance use, as well as treatment and common barriers to
recovery. A review of these factors is provided in Chapter II, along with a discussion of the
biopsychosocial-spiritual perspective of treating women who use substances, as adopted in
the province of British Columbia (Resit et al., 2004). A literature review of available
5
parenting programs is also presented in Chapter II. All such findings contributed to the
development of the facilitator manual. The facilitator training manual itself is presented as
Chapter III. The final chapter of this project document, Chapter IV, presents a synthesis of
the material, in concert with a discussion of the strengths and weaknesses of the current
project, and implications for potential future research.
6
CHAPTER II
Literature Review
Women and Substance Use
Recent years have seen a growing recognition that women have different needs in
relation to the pattern of, and recovery from, substance use (Currie, 2001; Kaiser Foundation,
2002; Miller, 2001; Resit et al., 2004). Traditionally, drug and alcohol programs have used
male-based treatment approaches across the board (Brindis, Berkowitz, & Clayson, 1997). In
the 1970s, strong support emerged for the need take into account women’s differing
perspectives, but it waned in the 1980s and relevant literature was scant. Over the past
decade, however, a mounting resurgence of interest and sensitivity to gender differences has
emerged, highlighting the diverse pathways that women who use substances may utilize.
According to the Diagnostic and Statistical Manual of Mental Disorders (2000), ‘substance
abuse’ is defined as follows.
A maladaptive pattern of substance use leading to clinically significant
impairment or distress, as manifested by one (or more) of the following, occurring
within a 12-month period: i) recurrent substance use resulting in a failure to
fulfill major role obligations at work, school, or home…, ii) recurrent substance
use in situations in which it is physically hazardous, iii) recurrent substance-
related legal problems, iv) continued substance use despite having persistent or
recurrent social or interpersonal problems cause by or exacerbated by the effects
of the substance. (p. 199)
Within this project the term ‘substance use’ is adopted, encompassing the continuum
of use, abuse, and dependence (British Columbia Ministry for Children and Families, 1996).
7
‘Use’ refers to casual or initial use, whereas ‘abuse’ is recognized as harmful, and
‘dependency’ is evidenced by physiological and psychological determinants such as
cravings. The term substance abuse is intentionally avoided in this project, as substance use
is inclusive of behaviour that has not been recognized as harmful by the user. There is also
concern that the term abuse may convey a value judgement. The substances relevant to this
project are alcohol and psychoactive drugs (both legal and illegal). Psychoactive drugs
include narcotic analgesics (codeine, heroin, and morphine), psychomotor stimulants
(cocaine and amphetamines), benzodiazepines (Ativan), antipsychotics (both typical and
atypical), inhalants, marijuana, and alcohol.
Path to Treatment
The recognition of women’s distinctive needs in substance use recovery has been
associated with a shift towards a better understanding of women’s experiences of substance
use, on physical, psychological, and practical levels. It has been noted that women
experience the physical consequences of substance use differently from men, particularly in
three aspects. The first is childbearing, which includes potential harm to the foetus (Currie,
2001). Second, women have been documented to experience more severe health effects from
substance use than men, which results in greater damage to the body (Resit et al., 2004).
Third, women metabolize substances more slowly than men; as such, substances remain in
the body for longer. Resit and colleagues (2004) have also found that females progress more
quickly to addiction than males, even when using identical amounts of a given substance.
Other relevant differences between men and women include patterns of mental health
difficulties, which are at higher rates among women than men (Miller, 2001). In addition,
women who are substance users are more likely to have experienced violence, abuse, and
8
exploitation (Currie, 2001; Madden, 1996; Resit et al., 2004; Vimpani & Spooner, 2003).
Women also follow a distinct path to treatment, as they tend to seek help later than men due
to parenting and involvement in less violent crimes which results in less institutional restraint
and decreased opportunity for being exposed to treatment. These substance use factors need
to paired with data suggesting that women comprise the majority of heads of households
(Currie, 2001), and tend to be the primary caregivers to their children (Huebner, 2002). As
such, there is clearly an urgent need for specialized resources to address the requirements of
women, particularly mothers, who use substances.
Barriers
Researchers in the field of substance use have identified a number of barriers that
impede women who use substances from seeking treatment. In order to meet the needs of
women who use substances, an understanding of such barriers must be established and the
issues addressed. Four distinct categories of barriers have been delineated within the
literature, namely personal, relational, societal and structural barriers (Currie, 2001).
Personal barriers. Personal barriers to accessing treatment are women’s emotions
associated with substance abuse, such as fear, guilt, grief, and shame (Currie, 2001). Many
women at Peardonville are typical of those reflected in the literature; that is, they experience
feelings of shame, worthlessness, and guilt (Hazeldon Foundation, 1995). These emotions
can immobilize women and prevent them from seeking change. Fear of losing love and
support from significant others is a barrier for women seeking treatment. Lack of motivation
and treatment readiness also contributes to avoidance of treatment by women experiencing
substance use (Jessup, Humphreys, Brindis, & Lee, 2003). According to Prochaska,
9
DiClimente and Norcross (1992), treatment involves change, which requires both motivation
and awareness that the problem exists and has a significant negative impact on their lives.
Relational barriers. Relational barriers are seen as significant by women who
experience substance use issues (Currie, 2001). The greatest concern for a woman seeking
help is that she may lose her child into MCFD care, either temporarily or permanently
(Currie, 2001; Kaiser Foundation, 2002; Resit et al., 2004). Many women do not have an
understanding of the overarching guidelines of MCFD, which prioritize the birth family as
the preferred place for a child to live (Province of British Columbia, 1996). Women often
view the MCFD and social service agencies as ‘the enemy’ and respond with hostility and
mistrust towards those who are attempting to help (Miller, 2001). Some women have had
previous negative experiences with the MCFD, while others are aware of the frightening
experiences of their peers. Primal fears surrounding relationships for those seeking treatment
include a lack or withdrawal of familial and partner support (Jessup et al., 2003).
Societal barriers. Women who use substances face a variety of societal barriers,
including discrimination (Benjet, Azar, & Kuersten-Hagen, 2003; Resit et al., 2004), the
social stigma of being scrutinized more harshly than men in relation to parenting (Currie,
2001; Resit et al., 2004), are seen as having a ‘tainted’ history (Currie, 2001), and experience
punitive responses from institutions (Brindis et al., 1997; Jessup et al., 2003). These negative
attitudes and actions compound the difficulties experienced by women asking for help and
seeking treatment. Discrimination is not simply a matter of perception; it can come in
tangible forms such as having difficulty acquiring housing, and problems gaining and
sustaining employment. In addition, completing forms and receiving medical attention can be
a constant reminder to women about their substance use, although they may not have used
10
since entering treatment. Women have consistently reported receiving negative and
demeaning responses from public and private institutions when they reveal a substance use
problem. It is clear that the social stigma attached to women using substances has changed
little over the past several decades.
Structural barrier. Structural barriers are also in place in precluding women from
seeking treatment for recovery from substance use. The single greatest structural barrier
preventing women from obtaining treatment is a lack of available childcare (Currie, 2001,
Kaiser Foundation, 2002; Jessup et al., 2003; Madden, 1996; Resit et al., 2004). This is
reflected in the residential and day treatment programs available in British Columbia. Indeed,
Peardonville House is the only female residential treatment program in the province of
British Columbia that provides women with preschool-aged children aged three months to six
years, with onsite childcare. Miller (2001) notes the marked shortage of treatment facilities
geared towards accepting women and children. This places many women at a distinct
disadvantage, as they often have no available support or family members who can care for
their children while they attend a treatment facility. Organized provision of care can involve
lengthy wait lists, by which time the woman may not be ready to enter treatment. Other
structural barriers are transportation and associated costs of treatment that can prevent
women to accessing services, as many women are on fixed income assistance budgets which
do not include bus or taxi fares.
Additional barriers described in the literature include a lack of specific information
related to parenting and educating pregnant women, in concert with minimal specialized
support and treatment services for children (Currie, 2001; Miller, 2001). For instance, alcohol
and drug counselling focuses on recovery, and parenting is usually viewed in terms of how
11
the client was parented, rather than how the clients themselves parent (Hazeldon Foundation,
1995). Children living in families with substance users often have additional behavioural,
social, and academic challenges and would benefit from early intervention (Coyer, 2003).
Lack of knowledge and education can become another barrier, as some women have weak
parenting skills and a low understanding of child growth and development, and few effective
parenting strategies. The barriers described above are not static, nor do they operate in
isolation of each other. Rather, the complex interaction of these barriers can significantly
affect a woman’s ability to seek treatment.
Biopsychosocial-spiritual Perspective
In the province of British Columbia the most common approach to treating substance
abuse is the biopsychosocial-spiritual model (Resit et al., 2004). The biopsychosocial-
spiritual model takes into account the influences of various factors on substance use, and how
they are affected by use. The term ‘biopsychosocial’ was coined by a medical doctor, George
Engel, who conceptualized the mind and body as two interconnected systems (Taylor, 2002).
His model was then adapted for application within the field of substance use and addiction.
Within this model treatment is not only appropriate for addiction, which lies at one
end of the substance use continuum. Rather, seeking help at any point to reduce present and
future harm to self and others is desirable. The purpose of treatment is to address problematic
use of substances or behaviours sited at any location along this spectrum. The overall aim of
the biopsychosocial-spiritual model is to heal the person as a whole, and address the systems
(e.g., social, relational, and governmental) with which they come into contact (Health
Canada, 1999). The biopsychosocial-spiritual model does more than address substance use; it
involves an exploration of any other problems the person is experiencing that have
12
contributed to the substance use, or arisen from it. By understanding complex interaction of
biological, psychological, social, and spiritual factors acting on and within a client,
interventions can be tailored to meet the client’s needs.
The biopsychosocial-spiritual perspective aims to address each component that
comprises the individual, namely biological, psychological, social and spiritual factors. The
biological component is the physical aspect of the problem use, including physiological
predispositions and the effects of use on the nervous system, brain, and body (Inaba &
Cohen, 2004). Most effects are related to increased dependency and related behaviours,
which then affect withdrawal or reduction of use. The psychological component incorporates
a host of factors that contribute to developing problematic substance use. Substance use may
also develop into dependency. Contributing factors may be trauma, childhood difficulties,
abuse, and mental health issues, all of which leave individuals under-resourced to deal with
the challenge of dealing with substance use. Psychological effects of use which are
associated with increased dependency include the intense pleasure that using brings, as well
as stress, anxiety, and depression.
The third factor that affects the individual is the social component, including family,
friends, peers, coworkers and society in general. This factor encompasses societal attitudes,
beliefs, and expectations that can contribute to substance use, usually through peer pressure
and modeling. Another key issue which is associated with increased likelihood of substance
use is having difficulty relating to others. This can be due to being shy, having poor social
skills or underlying psychological problems. Individuals who are isolated from social
interaction may seek to replace it with substance use, which can rob them the opportunity to
develop socially and enrich their lives. Finally, the spiritual component of the
13
biopsychosocial-spiritual model refers to having meaning, purpose, and a connection in life.
Some individuals choose to address spiritual issues through substance use, instead finding
that it only brings increased alienation and confusion.
There are eight key implications of adopting the biopsychosocial-spiritual model. The
first is that substance use is seen as a complex interaction of biological, psychological, social,
and spiritual factors (Health Canada, 1999). Second, the biopsychosocial-spiritual model
views substance use as existing along a continuum of severity. The biopsychosocial-spiritual
model is based on the recognition that individuals can be located at different places along the
use continuum, ranging from mild to severe. Third, an individual is seen as developing a
pattern of use that is variable over time, and that may or may not progress to a fatal stage.
Fourth, the biopsychosocial-spiritual model recognizes that there is no one superior treatment
for all users. The four components of the model, the biological, psychological, sociological,
and the spiritual, will be different for each person in the development of misuse. According
to the biopsychosocial-spiritual model, abstinence is not necessarily the goal of treatment,
and thus harm reduction may be more appropriate for some individuals. Recovery may not
depend on total abstinence
The fifth implication of the biopsychosocial-spiritual model is that the population of
substance users is heterogeneous and cannot be stereotyped. Sixth, the biopsychosocial-
spiritual model requires the comprehensive and accurate matching of clients with the form of
treatment that best fits their needs, strengths, and situations, in order to produce a successful
outcome. This model thus also incorporates a proportion of individuals who recover from
serious use without any form of treatment. Seventh, according to the biopsychosocial-
spiritual model, some individuals need to abstain from substance use totally, while others can
14
learn moderation. Finally, spirituality is viewed as a component of a substance use problem.
While some aspects of substance use may be problematic, others may not. One major
advantage value of the biopsychosocial-spiritual model is its flexibility, and the
encompassing path it takes to individual treatment and recovery, which may or may not
include a reliance on a greater power than oneself.
Providing treatment from a biopsychosocial-spiritual perspective involves the
development of activities designed to care for each component of the individual, while taking
into consideration the interplay between these components. The perspective aims to address
both intra- and interpersonal aspects of an individual’s life and to restore ‘wholeness’ to the
individual.
Parenting Education Programs
Parent education is not a recent concept. It was first introduced in the United States,
and has received mounting attention, and spread around the globe since this time (Croake &
Glover, 1977). The first recorded group meeting of parents was held in 1815 in Maine. By
1820 mothers were meeting regularly in groups called ‘maternal associations’ to discuss
child-rearing ideas, usually centered on the religious and moral development of their children
(Sunley, 1955). The first parenting magazine, Mother’s Magazine, appeared in 1832, and by
1841 two further parenting magazines were in distribution. These publications became the
catalyst for a movement that has continued to flourish. In 1888 the Society for the Study of
Child Nature was established. This was the first of many formal organizations formed to
investigate parent education and child-rearing practices. There has been a rise in the variety
of parenting programs available, often designed to target specific age groups of children,
address a specific common concern, or based on parental characteristics such as marital or
15
socioeconomic status (Dembo, Sweitzer & Lauritzen, 1985). Programs are available for teen
parents, for parenting a child with special needs, for children with Attention Deficit
Hyperactivity Disorder (ADHD), for families facing mental health concerns, and for
parenting infants, preschoolers, tweens, and youths, to name only a few.
The parenting programs available ascribe to a range of different theoretical models
(Dembo et al., 1985). Behavioural programs are based on behavioural and social learning
principles. The goal of such programs is to introduce parents to behavioural techniques
including positive reinforcement, conditioning, and alternatives to punishment (Bunting,
2004). An example of a behavioural program that has had considerable success is the
Webster-Stratton parenting program, which focuses on the three components of parent, child
and teacher. Parents learn positive parenting and diminish punitive methods, negative
demands and criticism when responding to their child. Parents also learn to set limits
effectively and techniques to increase family communication and problem-solving. Through
this program children are expected to show an increase in social and emotional competence,
thereby reducing behavioural challenges. Teachers focus on strengthening classroom
management techniques and adapt their curriculum to encourage social and emotional
competence.
A second type of parenting program is relationship-based parenting programs. These
programs seek to provide parents with communication and active listening tools to use while
interacting with their children. The goal of these programs is to assist parents in
understanding their child’s perspective, hence illuminating the motives behind their
behaviour (Alaggia, 2001). This approach originates with Rogers’ (1957) client-centered
theory, which emphasizes the use empathy, congruence, and a genuine approach to resolve
16
problems. The outcomes of such programs include better communication strategies and
improved parent attitudes towards their child’s behaviour (Fennel & Fishel, 1998).
Another common parenting program is based on the cognitive-behavioural therapy
(CBT) framework. It combines behavioural techniques with cognitive strategies to help
parents restructure their thinking about themselves and their children (Bunting, 2004). CBT
is considered an effective intervention for dealing with children who have behavioural
problems (Rogers-Weise, 1992). A very different approach is adopted by Rational Emotive
Therapy parenting programs, which are designed to lower emotional stress through
challenging irrational beliefs and reinforcing rational beliefs. These techniques are thought to
improve decision-making and problem-solving skills. The programs discussed above are not
the only ones available, but they are the most commonly used. Often a given program may
draw on more than one theoretical style. Many programs operate on a weekly basis for two to
three hours, using a variety of teaching and training methods. There are many federal,
provincial, and private organizations and programs dedicated to supporting parents.
Goals of Parenting Education Groups
Parent education is operationally defined as an intentional learning opportunity
whereby parents can actively learn ideas about promoting positive communication,
attachment, parent-child relationships, and guiding and caring, for the purpose of promoting
healthy and positive outcomes of their children’s behaviour. The goal is for parents to
develop confidence and acquire information about positive ways to parent their children. All
parents are equipped with implicit beliefs, schemas, and personal experiences that provide
them with an interpretative perspective and understanding of child rearing (Rodrigo, Correa,
Maiquez, Martin, & Rodriguez, 2006). Parents use this implicit knowledge to guide their
17
interaction with their children. Parenting education is an opportunity to introduce to parents
new ways of relating and responding to their children. Through the education program
parents are encouraged to incorporate these new techniques into their mental schema and
their daily lives. It is clear that parenting programs have been instrumental in strengthening
parenting skills and have made a significant impact on children’s development and their
physical and emotional health (Patterson, Mackford, & Stewart-Brown, 2003). Bunting
(2004) cited a range of positive outcomes from parent education programs, including
strengthened relationships, decreased maternal stress and depression, improved maternal self-
esteem, and improved child behaviour. Clearly, the benefits encompass the entire family unit.
Yoshikawa (1995) also emphasized the benefit of parent training to reduce coercive
interactions and delinquency among children and youths.
Group Parenting Programs
There has recently been an explosion within the parent education industry in terms of
the number of programs and parenting groups aimed at providing early intervention (Day &
Davis, 1999). There has been a significant increase particularly in group parenting programs,
which appears to be the preferred method of delivery for many parents. Cunningham,
Bremner and Boyle (1995) conducted a random trial comparing group community-based
intervention with individual parent training. They found that immigrant families were more
likely to enrol in group parenting sessions than individual sessions. The group parenting
programs also showed greater overall improvements and better maintenance of those
improvements at a six month follow-up. This study also revealed that group parenting was
six times as cost effective as individual parenting sessions. Bunting (2004), in a review of
parenting programs, also found that positive results from group parenting programs were
18
more likely to be maintained over time. A study conducted by Rodrigo and colleagues (2006)
similarly demonstrated that group programs for parenting were effective in helping parents
change and increase their self-efficacy. In summary, the benefits of group parenting
programs include monetary savings, an enhancement in parent self-efficacy, and increased
participation due to client preference of the group format.
Group parenting programs offer parents the opportunity to come together, share their
experiences and learn from each other in a non-judgemental atmosphere (Rodrigo et al.,
2006). Groups can focus on a particular theme relating to the parent, such as being a teen
parent or of low socioeconomic status, or discuss a shared common issue such as child
autism or mental health issues. Researchers have also supported the adoption of a group
format for women receiving parenting assistance while in treatment. In a three year study
conducted by Brindis and associates (1997), using both quantitative and qualitative methods,
researchers concluded that a broad range of options responsive to the multiple needs of
women and their children should be made available. According to these researchers, the
earlier pregnant women entered treatment, the greater the birth weight of the child, and the
lower the amount of drugs transferred into the uterus. Brindis and colleagues also empirically
demonstrated that the majority of the children in the study scored within normal limits of
motor and psychomotor development. The authors strongly recommended that infant
education and parenting programs be included as part of every alcohol and drug treatment
program for women. Indeed, promising results such as these provide strong indications for
the need for more formal group parenting programs for women seeking treatment for
substance abuse.
19
In response to the available evidence, Miller (2001) has advocated that treatment
facilities for women should also provide accommodation for their children. He argued that
substance users have multiple barriers and often lack parenting skills. Women with substance
issues often adopt the same dysfunctional parenting strategies that they were exposed to as
children, and may not be aware of effects of their drug use on their own children. Provision
of parenting groups within treatment facilities rectifies a critical gap in treatment programs.
Many mothers enter treatment in order to get their child back from foster care or because
they want to parent their child full time. Offering a parenting program to clients in treatment
serves to reduce the likelihood of relapse (Catalano, 1999). Miller (2001) cites three markers
of success for treatment programs that serve women and children. These are: (1) removing
barriers to attendance by allowing women to attend treatment with their children; (2)
providing information about childcare and parenting skills as well as child growth and
development; and (3) offering support services to improve women’s confidence and self-
efficacy regarding parenting. The outcomes of treatment programs which incorporate group
parenting programs indicate that many clients can and do improve their lives and resume
their parenting role with increased confidence (Pepler, Moore, Motz, & Leslie, 2002).
Bridging Substance Use and Parenting
For many women motherhood is the only legitimate social role they ascribe to
(Hawley, Halle, Drasin, & Thomas, 1995). In their role as a mother, women who use
substances are often concerned about how their substance use may affect their child. This in
itself is a powerful motivating factor in bringing women forward to seek treatment. Since
these women most likely value mothering, facilitators are able to use this as an incentive to
20
encourage them to enter treatment, by providing effective parenting programs that will
increase their ability to care for their children and improve their confidence in parenting.
Women who use substances often lack parenting skills, limiting their ability
successfully deal with the daunting responsibility of raising children (Coyer, 2003; Miller,
2001). Many such women have experienced abuse and family dysfunction, where harsh
discipline or neglect is the norm (Huebner, 2002). Women in early recovery have the
formidable task of balancing their recovery from substance use with the demands of full time
parenting. Most are juggling many issues simultaneously (e.g., health, legal and relationship
problems) that cannot be put on hold until they have reached a more stable point (Hazeldon
Foundation, 1995). Recovery in itself requires a significant time commitment and a focus on
learning new ways of living, having fun, and recognizing potential triggers (Brindis et al.,
1997). Women in early recovery are focused on the steps it will take to remain clean and
sober. However, parenting active children requires time, patience, love, and routine. Women
benefit from having a greater understanding of child growth and development, which can
normalize a situation and help meet the needs of children regardless of age (Huebner, 2002).
Women in early recovery tend to be overwhelmed with what they are learning and the
challenges they face (Hazeldon Foundation, 1995). This means that parenting programs
delivered in this context must be presented in a simple manner, coupled with realistic
expectations. The literature review identified a series of common themes surrounding
parenting for women in early recovery, such as inconsistent parenting, parenting out of guilt
and shame, anger management, building trust, and setting limits (Huebner, 2002). Parenting
groups can generate discussion and share ideas related to these parenting topics with the goal
of increasing the parent’s skill set and confidence in parenting.
21
Conclusion
The path to treatment for women who use substances is complex and
multidimensional. Women are experience a variety of effects from substance use, including
physical, psychological, social, and relational outcomes (Currie, 2001). Physically, alcohol
and drugs create severe health problems for women, resulting in significant damage to their
bodies (Resit et al., 2004). Women can become psychologically dependent on substances and
a large proportion of women who use substances have mental health concerns (Miller, 2001).
Socially, women who use substances have often been ostracized from family, friends, and
society. In terms of relationships, many women fear losing their partner by seeking treatment
or have a lack of solid, caring relationships to help sustain them during treatment.
Women face a range of barriers when seeking help for substance use. These include
personal concerns, such as a lack of readiness for treatment (Jessup et al., 2003), and a fear of
losing their children to social services (Currie, 2001; Resit et al., 2004). A significant societal
barrier is the fact that women are viewed more harshly than men for using substances, while
structural barriers include a lack of child care (Madden, 1996). The issues are not static, nor
do they operate in isolation from each other.
A recent development is the adoption of the biopsychosocial-spiritual model, in
which four components (biological, psychological, social and spiritual) are seen as
composing the whole of the individual. Treatment according to the biopsychosocial-spiritual
model involves treating the entire person within their environmental milieu.
Parent education programs have been shown to be an effective method through which
parents can obtain support, ideas, and information as to how to raise their children. Groups
are often based on the ages of the children involved, a shared issue, or a parental feature (e.g.,
22
being a teen parent). According to the literature, the value of parent education programs is
evidenced through the measurable difference they can make by strengthening a family. For
organizations, group parenting programs are a cost effective and time saving means of
working with families, when compared with establishing individual parenting sessions.
Evidence suggests that there is a preference for group parenting programs over
individual parenting sessions (Cunningham, Bremner, & Boyle, 1995). This medium of
delivery has been shown to be effective for women undergoing treatment, who benefit from
learning parenting strategies and acquiring information about child growth and development,
hence improving their confidence in their role as parents. Treatment facilities appear to
provide an opportunity to offer parenting assistance to women as they embark on recovery,
and are learning to balance the demands of recovery with the challenges of parenting. It also
assists the women in networking and developing meaningful relationships, through which
they may develop a support system instead of solely relying on government and community
agency programs.
The following chapter incorporates the training manual for facilitators who deliver
the parenting program at Peardonville House. I have drawn on the literature regarding the
path that women take to treatment, and have utilized the biopsychosocial-spiritual model
when designing the activities aimed at helping women care for themselves and their children.
In the manual, I reflect on the concerns and issues typically experienced by women who use
substances, based on findings from available research and my professional experience with
this population. Within the training manual I suggest ways of increasing women’s confidence
in parenting while balancing the demands of early recovery. The manual contains substantial,
up to date information regarding child growth and development, and describes strategies for
23
parenting effectively with the aim of strengthening the family unit. Concerns addressed
include the key issues of parenting out of guilt and shame, increasing mother-child
attachment, building trust and setting limits for children. The intended goal of the program is
that the parent education group mothers will feel supported, informed, and encouraged in
their parenting.
24
References
Alaggia, R. (May, 2001). An overview of parenting programs for families of young children-
What works? Paper presented at the meeting of the Symposium conducted at the
meeting of the Parenting Alliance. Waterloo, ON.
American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental
Disorders 4th ed. Text Revision (4th ed.). Washington, DC: Author.
Benjet, C., Azar, S. T., & Kuersten-Hogan, R. (2003). Evaluating the parental fitness of
psychiatrically diagnosed individuals: Advocating functional contextual analysis of
parenting. Journal of Family Psychology, 17(2), 238-251.
Brindis, C., Berkowitz, G., & Clayson, Z. (1997). Option for recovery promoting perinatal
drug and alcohol recovery, child health, and family stability. Journal of Drug Issues,
27, 607-624.
British Columbia Ministry for Children and Families. (1996, May). The biopsychosocial
theory: A comprehensive descriptive perspective on addiction alcohol and drug
services. Retrieved May 19, 2006, from British Columbia Ministry for Children and
Families Adult Addictions Services Branch, Alcohol and Drug Services Web site:
http://www.health
services.gov.ca.bc.ca/mhd/pdf/biopsychosocial_theory_may_1996.pdf.
Bunting, L. (2004). Parenting programmes: The best available evidence. Child Care in
Practice, 10(4), 327-343.
Catalano, R. F. (1999). In Ashery, R.E. Robertson & K. L. Kumfer. Drug abuse prevention
though family interventions. Rockville, MD: DHSS, National Institute on Drug
Abuse.
Coyer, S. M. (2003). Women in recovery discuss parenting while addicted to cocaine.
American Journal of Maternal Child Nursing, 28(1), 45-49.
25
Croake, J. W., & Glover, K. E. (1977). A history and evaluation of parent education. Family
Coordinator, 26(2), 151-158.
Cunningham, C. E., Bremner, R., & Boyle, M. (1995). Large group parenting programs for
families of preschoolers at risk for disruptive behaviour disorders: Utilization, cost,
effectiveness and outcome. Journal of Child Psychology and Psychiatry, 36(7), 1141-
1159.
Currie, J. C. (2001). Best practices treatment and rehabilitation for women with substance
use problems. Retrieved March 21, 2003, from Canadian Government Web site:
http://www.hc-sa.gc.ca/hecs-sesc/cds/pdf/women-epdf
Day, C., & Davis, I. (1999). Community child mental health services: A framework of the
development of parenting initiatives. Clinical Child Psychology and Psychiatry, 4,
475-482.
Dembo, M. H., Sweitzer, M., & Lauritzen, P. (1985). An evaluation of group parent
education: Behavioural, PET, and Adlerian programs. Review of Educational
Research, 55(2), 155-200.
Fennel, D., & Fishel, A. (1998). Parent education: An evaluation of STEP on abusive parents'
perceptions and abuse potential. Journal of Child and Adolescent Psychiatric
Nursing, 11, 107-120.
Hawley, T., Halle, T., Drasin, R., & Thomas, N. (1995). Children of addicted mothers:
Effects of the "crack epidemic" on the caregiving environment and the development
of preschoolers. American Journal of Orthopsychiatry, 65, 364-379.
Hazeldon Foundation (1995). The Real Life Parenting Skills Program The Facilitator's
Guide. Center City, MN: Author.
Health Canada. (1999). Best practices: Substance abuse treatment and rehabilitation.
Retrieved October 12, 2006, from Health Canada Treatment and Publications Web
site: http:/www.hc.sc.gc.ca/ahc-asc/pubs/drugs/droges/bp-mp-abuse-
abus/index_e.html.
26
Health Canada. (2005). Literature Review Evaluation strategies in Aboriginal substance
abuse programs: A discussion. Retrieved September 12, 2006, from First Nations and
Inuit Health - Substance Use and Treatment of Addictions Web site: http://www.hc-
sc.gc.ca/fnih/spni/pubs/ads/literary_examen_review/index_e.html.
Huebner, C. E. (2002). Evaluation of a clinic-based parent education program to reduce the
risk of infant and toddler maltreatment. Public Health Nursing, 19(5), 377.
Inaba, D. S., & Cohen, W. E. (2004). Uppers, Downers, All Arounders: Physical and Mental
Effects of Psychoactive Drugs (5th ed.) Oregon: CNS Publishers.
Jessup, M. A., Humphreys, J. C., Brindis, C. D., & Lee, K. A. (2003). Extrinsic barriers to
substance abuse treatment among pregnant drug dependent women. Journal of Drug
Issues, 33(2), 285.
Kaiser Foundation. (2002). Introduction to Services. Retrieved August 5, 2005, from
http://www.kaiserfoundation.ca
Kumpfer, K. L., & Alvarado, R. (2003). Family-strengthening approaches for the prevention
of youth problem behaviours. American Psychologist, 58(6/7), 457.
Madden, R. G. (1996). Civil commitment for substance abuses by pregnant women? A view
from the front lines. Politics and the Life Sciences, 15, 56-59.
Miller, A. F. (2001). A critical need: Substance abuse treatment with children. Corrections
Today, 63, 88-91.
Patterson, J., Mackford, C., & Stewart-Brown, S. (2003). Parents' perceptions of the value of
the Webster-Stratton parenting programme: A qualitative study of a general practice
based initiative. Child Care, Health, and Development, 31(1), 53-64.
Pepler, D.J., Moore, T.E., Motz, M. & Leslie, M. (2002). Breaking the Cycle. A Chance for
New Beginnings. 1995-2000 Evaluation report. Toronto: Breaking the Cycle.
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of how people
change applications to addictive behaviours. American Psychologist, 47(9), 1102-
1114.
27
Province of British Columbia (1996). Child, Family, and Community Services Act. Victoria,
BC: Queen's Printer.
Resit, D., Marlatt, G. A., Goldnar, E. M., Parks, G. A., Fox, J., & Kang, S. (May, 2004).
Every door is the right door. A BC planning framework to address problematic
substance use and addiction. Retrieved October 27, 2004, from British Columbia
Ministry of Health Web site:
http://www.healthservices.gov.bc.ca/mhd/pdf/framework_for_substance_use_and_ad
diction_pdf.
Rodrigo, M. J., Correa, A. D., Maiquez, M. L., Martin, J. C., & Rodriguez, G. (2006). Family
preservation services on the Canary Islands: Predictors of the efficacy of a parenting
program for families at risk of social exclusion. European Psychologist, 11(1), 57-70.
Rogers, C. R. (1957). The necessary and sufficient conditions of therapeutic personality
change. Journal of Consulting Psychology, 21, 95-103.
Rogers-Weise, M. R. (1992). A critical review of parent training research. Psychology in the
Schools, 29, 229-236.
Sanders, M. R., Cann, W., & Markie-Dadds, C. (2003). The triple p-positive parenting
programme: A universal population-level approach to the prevention of child abuse.
Child Abuse Review, 12, 155-171.
Sunley, R. (1955). Early 19th century American literature on child rearing. In M. Mead & M.
Wolfenstein (Eds.), Childhood in Contemporary Cultures (pp. 150-167). Chicago, IL:
University of Chicago Press.
Taylor, G. J. (2002). Mind-body-environment: George Engel's psychoanalytic approach to
psychometric medicine. The Australian and New Zealand Journal of Psychiatry,
36(4), 449-457.
Valley Recovery Support Association. (1999). Breaking the Cycle of Addiction [Brochure].
Abbotsford, BC: Author.
28
Vimpani, G., & Spooner, C. (2003). Minimizing substance misuse by strategies to strengthen
families. Drug and Alcohol Review, 22, 251-254.
Wideman, M. (2003). Benefits and tops on writing successful manuals. Retrieved August 12,
2006, from www.maxwideman.com
Yoshikawa, H. (1995). Long-term effects of early childhood programs on social outcomes
and delinquency. The Future of Children, 5(3),51-71

29
CHAPTER III
Facilitator Training Manual
Strengthening Mothers:
Facilitator Training Manual for Parenting
in Early Recovery
for
Peardonville House
Developed by Karen Janzen, Master of Counselling Candidate,
Campus Alberta Applied Psychology
For full document see: DTPR Link to Final Project Provided here

Table of Contents
CHAPTER III ......................................................................................................................... 1
Facilitator Training Manual .................................................................................................. 1
Purpose..................................................................................................................................... 1
Program Philosophy ............................................................................................................... 2
Goals for the Mothers in the Group ...................................................................................... 2
Intended Audience .................................................................................................................. 3
Facilitators’ Guiding Assumptions........................................................................................ 5
Theoretical Considerations .................................................................................................... 6
Client-centered .................................................................................................................... 6
Ages and Stages: Developmental Theory.......................................................................... 7
Family Systems.................................................................................................................. 11
Strength-Based .................................................................................................................. 12
Play Therapy ..................................................................................................................... 12
Creating a Learner-centered Approach ............................................................................. 14
Multicultural Awareness ...................................................................................................... 14
Group Processes .................................................................................................................... 15
Expectations of Facilitators.................................................................................................. 16
1. Active Listening............................................................................................................. 16
2. Effective Communication ............................................................................................. 17
4. Promoting Participation ............................................................................................... 19
5. Being Flexible ................................................................................................................ 20
6. Setting Guidelines ......................................................................................................... 20
7. Confidentiality............................................................................................................... 21
8. Handling Challenging Situations................................................................................. 23
9. Exploring Values........................................................................................................... 26
Suggested Schedule ............................................................................................................... 28
Balancing Parenting with Early Recovery ......................................................................... 30
Evaluation of Program ......................................................................................................... 30
Linkage and Follow-Up ........................................................................................................ 31
Self-Care for Facilitators...................................................................................................... 32
Closing Thoughts .................................................................................................................. 32
Feedback: Strengthening Mothers Parenting Group ........................................................ 34
1
CHAPTER III
Facilitator Training Manual
Purpose
The purpose of this training manual is to equip facilitators with information and
strategies in order to deliver the group parenting program at Peardonville
House. After training is complete this manual can serve as an ongoing resource
for facilitators. The training manual is designed to assist in the delivery of a
weekly parenting program offered at Peardonville House. Peardonville House is
a ten week drug and alcohol residential treatment center that serves 25 women
and 8 children. The facility uses a revolving basis for entry, and thus the women
receiving treatment are at various stages of recovery. A unique feature of the
program is the attention given to parenting while in recovery. The women are
required to attend a weekly parenting group and individual sessions are
available if necessary. The mothers are given an opportunity to practice new
parenting techniques and spend time in the childcare center, where staff model
best practice caregiving.
The parenting group facilitators have a variety of educational backgrounds,
including social work, nursing, child and youth care, early childhood education,
and alcohol and drug counselling. This manual seeks to establish a modicum of
uniformity across sessions, and provide a common knowledge base regarding
parenting and issues common to early recovery from substance use.
The contents of this facilitator manual include a description of the program
philosophy, program goals, intended audience, facilitators’ objectives, means of
creating a learner-centered approach, information about multicultural
awareness, theoretical considerations, group processes, expectations of
facilitators, facilitators’ guiding assumptions, and key issues when balancing
parenting with early recovery.
2
Program Philosophy
The Peardonville House parenting program aims to strengthen the family unit.
We believe that the women who access our program love their children and
have the desire to be effective parents. These mothers want their children to be
happy and healthy.
We believe that balancing early recovery with parenting is paramount. Helping
mothers meet their own needs is an important step in assisting them to meet
their children’s needs.
We believe that all parents need encouragement and information. A supportive
parenting group can highlight a mother’s strengths and help her understand her
needs.
We believe that the women in our program need to be respected, valued, and
accepted for who they are. All the women have important contributions to make
to their families and to society.
We believe that each family is unique with their own cultural background and
experiences, and this fact needs to be honoured. We recognize that there is no
one right way to raise children; however, there are more appropriate and
effective ways to meet the developmental and emotional needs of children,
which we promote.
We believe that mothers in our group program know more about their children
than us. The facilitator is not seen as an expert, rather they are there to provide
information and guide the women through self-reflection and discovery.
Facilitators are also open to learning from the mothers.
Goals for the Mothers in the Group
� Gain confidence in her role as a mother
� Reflect on her life, her children, and her role as a parent
� Build on current parenting skills and learn and practice new ones
� Build self-efficacy and recognize her own strengths and abilities
� Share her knowledge and experiences with other members of the group
3
� Get to know other mothers and have fun while learning
� Make connections with others and see them as sources of support
Intended Audience
Peardonville House parenting program is specifically designed for women in
early recovery while in treatment for substance use. Women who are pregnant
or have children aged from newborn to 19 years of age will benefit from the
program. Some of the women will have their children with them at Peardonville
House, while other women will have their children living with family or in
foster care and may or may not have access or contact with them during their
stay. Most of the women have had previous contact with the Ministry of
Children and Family Development (MCFD) and many have Supervision Orders
attached to their intake file. This means that the MCFD has concerns about a
parent’s ability to protect her child due to her substance use and associated
behaviours. A Supervision Order is granted by a judge, with a list of
recommendations that need to be followed or the children can be removed from
her care. If removal occurs the children are typically placed with extended
family, but if this is not appropriate the children are placed in foster care.
Many of the women attending Peardonville House have not been involved in
full time parenting, as many have had their children removed to foster care.
Thus the learning curve experienced by these women is steep, as they need to
become reacquainted with their children and strengthen their attachment. These
mothers need to forge a bond with their children while undergoing intensive
treatment at Peardonville House. For other mothers, Peardonville represents a
stepping stone to receiving their children back from foster care. Attendance at
Peardonville demonstrates to the MCFD that, as a parent, they are taking steps
to address substance use and are seeking ways to strengthen their parenting
skills. Some mothers have been directly mandated by the courts to attend
Peardonville House, while others choose Peardonville as they can bring their
children with them. The courts look favourably upon women successfully
completing the Peardonville program, which is a testament to the program. The
reputation of the program can assist mothers in regaining care of their children.
Women in early recovery often face immediate parenting challenges that cannot
be set aside until they are more stable in recovery. Emotions are high, and
routines and expectations of being in a treatment facility, while simultaneously
parenting, are new and taxing. Furthermore, the women may still be
4
experiencing physiological changes from the cessation of substance use, such as
withdrawal symptoms or cravings. When a mother is engaged in substance use
it can become all-consuming and the physical care of her body is often
neglected, with medical and dental attention seldom sought. Chronic health
conditions as a result of using (e.g., HIV, AIDS or Hepatitis C) often require
immediate and intense treatment, which is difficult while these mothers are
struggling dealing with day-to-day concerns. In addition, these women are often
engaged in legal battles due to their behaviour while using, or are under
investigation from the MCFD. Housing and relationship problems are other
common concerns among this group of women.
Two vignettes are now presented to demonstrate the types of issues faced by
women in the Peardonville House program.
Vignette 1: Dorothy1
Dorothy is from Vancouver’s downtown Eastside. She is from a visible
minority culture, has mental health concerns, a myriad of learning disabilities,
and is an IV drug user. She was living on the streets until she discovered that
she was seven months pregnant, at which time she sought help. Dorothy has
three older children who were removed by the MCFD at birth. One child has
been adopted while the other two reside in foster care. She is not aware of their
current location. She is not in a relationship and has no family. Her son was
born premature and addicted, with a low birth weight. After spending three
months in hospital the baby was released into foster care. Dorothy was
permitted one visit per week for two hours duration. Upon her admission to
Peardonville House, her now six month old son was transferred to her care.
Dorothy is immediately thrilled, but soon becomes frustrated and overwhelmed
by the needs of her son. His sucking reflexes are poor and he needs to be fed
every four hours. He is not able to self-soothe so when he begins to cry, it
escalates for hours until he falls asleep from exhaustion. He is sensitive to light,
sound, and touch. Concurrently Dorothy is lowering her daily dose of
methadone to stay more alert, and is beginning to address the multiple years of
neglecting her body including Hepatitis C, HIV, and extensive dental work. The
Peardonville House physician is exploring medications to address bipolar
disorder and post-traumatic stress disorder.
1 The vignette is not based on a single individual but is representative of common issues facing women
attending Peardonville House.
5
Vignette 2: Sue1
Sue is the mother of a three year old boy and a five year old girl. The children
have witnessed violence and abuse from Sue’s multitude of partners. They have
lived in shelters, with Sue and her boyfriends, in foster care, and with extended
family. Sue has had a challenging past. She loves her children but says that they
are unmanageable and that they don’t listen to her. The children do not have a
routine in terms of eating and sleeping, and Sue states that they hit her. Sue has
bruises on her arms and legs from where her five year old has kicked her, and a
bite mark from her three year old. She believes in the adage “spare the rod and
spoil the child”. She was spanked as a child and feels that it did her no harm.
Facilitator Objectives
� To create an emotionally safe environment
� To encourage the women to actively participate in the group
� To facilitate group discussions
� To offer practical, positive and inexpensive ideas and approaches
� To offer support and normalize experiences through group sharing
� To provide information
� To practice problem-solving skills with the women
� To meet the needs of the group – this may include adapting the topic to
meet the current concerns of the group and ages of the children
� To be sensitive to the unique culture, background, and experiences of
each woman
Facilitators’ Guiding Assumptions
� The women love their children and want to be effective parents
� Assistance needs to begin based on the woman’s view of her own needs
� It is necessary to respect each woman’s choices and values
� It is necessary to practice self-reflection about our own class, race,
culture, and lifestyle and how this influences our work with these women
� It necessary to listen to differences

6
� It is necessary to acknowledge the inherent power of being in a facilitator
relationship with the women by being honest, clear, genuine and by
providing accurate information and support
Theoretical Considerations
The parenting program at Peardonville House draws from various theoretical
frameworks to assist the women to deal with parenting issues and concerns.
Parent education grounded in theory is not a new phenomenon. Its roots lie in
the United States more than a century ago. Current parenting groups have been
found to be effective in promoting attachment, reducing behavioural problems,
early intervention, and increasing confidence and skills in mothering.
Client-centered
The parenting program at Peadonville House is largely based on the work of
Carl Rogers (1957), who developed client-centered therapy. Rogers’ premise
was that living organisms that have a tendency to undertake healing and growth.
Rogers’ (1957) three basic tenets, which are seen as necessary and sufficient for
healing, are empathy, unconditional regard, and genuineness. Patterson (2004)
expanded on Rogers’ work, citing five skills that facilitators need to posses.
Respect for the client: Each client needs to be valued for who she is and viewed
as capable of making healthy choices.
Genuineness: The facilitator is real and genuine in their interactions with the
women. The facilitator does not come across as ‘knowing all the answers’ or
being ‘above’ the group, but as a willing learner within the group. The
facilitator can share personal experiences, for instance being frustrated with
their own children or how they handled a trying situation.
Empathy: The facilitator is attuned to the inner emotional world of the client
and responds to the individual at that level. This involves responding with
feeling and content to what is being said by the client.
Communication: The facilitator needs to be aware of both verbal and nonverbal
communication and know how to respond effectively. Nonverbal language is
often a more accurate predictor of behaviour than words.
7
Structuring: The facilitator needs to be able to structure the program to
provide opportunities for participants to share ideas, and to assist the women in
understanding group processes and conveying reasonable expectations.
Ages and Stages: Developmental Theory
Erik Erikson (1977) developed an eight stage psychosocial model of
development that he believed all individuals pass through in their life span.
Erikson (1977) describes development at each stage as a “crisis” or turning
point, where an individual can either move forward and master the
developmental stage, or fail to resolve the conflict and hence struggle with that
issue throughout life. The stages themselves provide a guideline for parents as
to developmental milestones. It is important to note that each child is unique
and may or may not fit uniformly within a given stage.
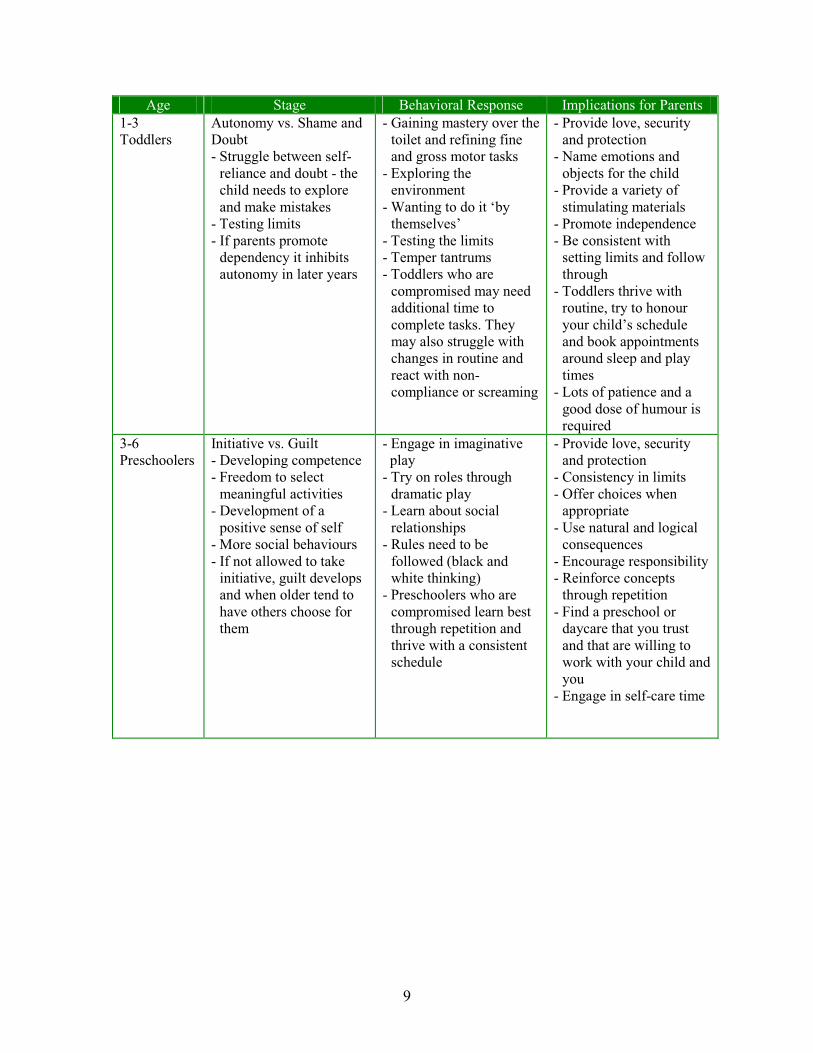
Erikson’s (1977) stages of psychosocial development are frequently referred to
in relation to parenting issues. His work provides a guideline for child growth
and development patterns, which can be used to normalize the behaviour of
children and help a mother understand how their child may respond and what
needs they may have. For instance, a mother may not understand that, at 18
months, her child may not have the words to express themselves. This
frustration can lead to biting, which is common among children of that age.
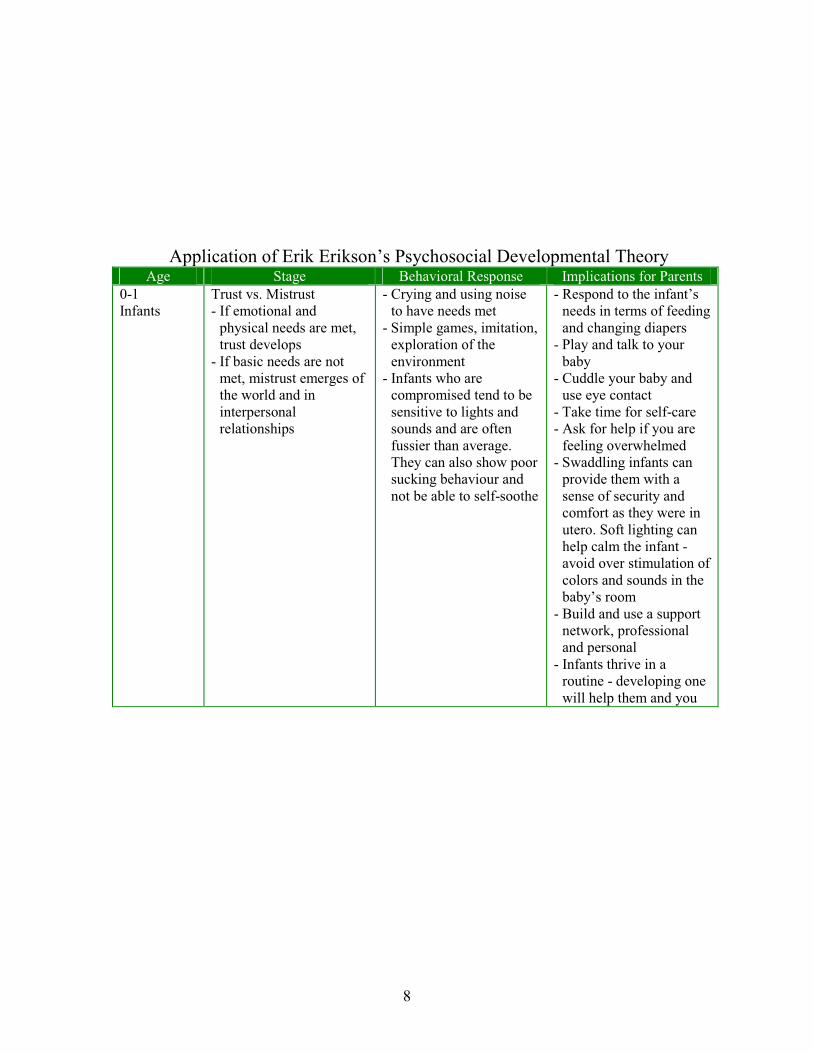
The following table describes Erikson’s Psychosocial Stages in the first and
second column (Corey, 2001 p.74-76). The third column provides common
behavioural responses from children and youth that characterize the
corresponding stage of development. While the last column gives implications
for parents as they guide and care for their child and youth from suggesting
practical ideas in caring for the child to self-care for the parent.
8
Application of Erik Erikson’s Psychosocial Developmental Theory Age Stage Behavioral Response Implications for Parents
0-1
Infants
Trust vs. Mistrust
- If emotional and
physical needs are met,
trust develops
- If basic needs are not
met, mistrust emerges of
the world and in
interpersonal
relationships
- Crying and using noise
to have needs met
- Simple games, imitation,
exploration of the
environment
- Infants who are
compromised tend to be
sensitive to lights and
sounds and are often
fussier than average.
They can also show poor
sucking behaviour and
not be able to self-soothe
- Respond to the infant’s
needs in terms of feeding
and changing diapers
- Play and talk to your
baby
- Cuddle your baby and
use eye contact
- Take time for self-care
- Ask for help if you are
feeling overwhelmed
- Swaddling infants can
provide them with a
sense of security and
comfort as they were in
utero. Soft lighting can
help calm the infant -
avoid over stimulation of
colors and sounds in the
baby’s room
- Build and use a support
network, professional
and personal
- Infants thrive in a
routine - developing one
will help them and you
9
Age Stage Behavioral Response Implications for Parents
1-3
Toddlers
Autonomy vs. Shame and
Doubt
- Struggle between self-
reliance and doubt - the
child needs to explore
and make mistakes
- Testing limits
- If parents promote
dependency it inhibits
autonomy in later years
- Gaining mastery over the
toilet and refining fine
and gross motor tasks
- Exploring the
environment
- Wanting to do it ‘by
themselves’
- Testing the limits
- Temper tantrums
- Toddlers who are
compromised may need
additional time to
complete tasks. They
may also struggle with
changes in routine and
react with non-
compliance or screaming
- Provide love, security
and protection
- Name emotions and
objects for the child
- Provide a variety of
stimulating materials
- Promote independence
- Be consistent with
setting limits and follow
through
- Toddlers thrive with
routine, try to honour
your child’s schedule
and book appointments
around sleep and play
times
- Lots of patience and a
good dose of humour is
required
3-6
Preschoolers
Initiative vs. Guilt
- Developing competence
- Freedom to select
meaningful activities
- Development of a
positive sense of self
- More social behaviours
- If not allowed to take
initiative, guilt develops
and when older tend to
have others choose for
them
- Engage in imaginative
play
- Try on roles through
dramatic play
- Learn about social
relationships
- Rules need to be
followed (black and
white thinking)
- Preschoolers who are
compromised learn best
through repetition and
thrive with a consistent
schedule
- Provide love, security
and protection
- Consistency in limits
- Offer choices when
appropriate
- Use natural and logical
consequences
- Encourage responsibility
- Reinforce concepts
through repetition
- Find a preschool or
daycare that you trust
and that are willing to
work with your child and
you
- Engage in self-care time
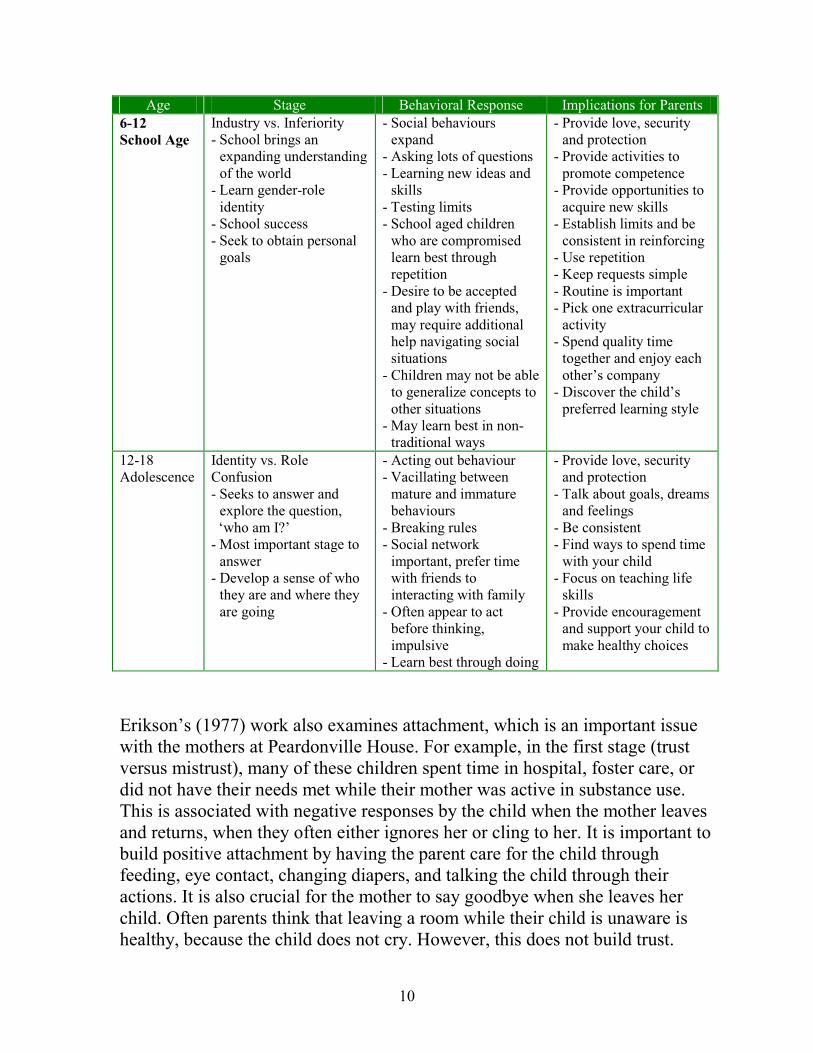
10
Age Stage Behavioral Response Implications for Parents
6-12
School Age
Industry vs. Inferiority
- School brings an
expanding understanding
of the world
- Learn gender-role
identity
- School success
- Seek to obtain personal
goals
- Social behaviours
expand
- Asking lots of questions
- Learning new ideas and
skills
- Testing limits
- School aged children
who are compromised
learn best through
repetition
- Desire to be accepted
and play with friends,
may require additional
help navigating social
situations
- Children may not be able
to generalize concepts to
other situations
- May learn best in non-
traditional ways
- Provide love, security
and protection
- Provide activities to
promote competence
- Provide opportunities to
acquire new skills
- Establish limits and be
consistent in reinforcing
- Use repetition
- Keep requests simple
- Routine is important
- Pick one extracurricular
activity
- Spend quality time
together and enjoy each
other’s company
- Discover the child’s
preferred learning style
12-18
Adolescence
Identity vs. Role
Confusion
- Seeks to answer and
explore the question,
‘who am I?’
- Most important stage to
answer
- Develop a sense of who
they are and where they
are going
- Acting out behaviour
- Vacillating between
mature and immature
behaviours
- Breaking rules
- Social network
important, prefer time
with friends to
interacting with family
- Often appear to act
before thinking,
impulsive
- Learn best through doing
- Provide love, security
and protection
- Talk about goals, dreams
and feelings
- Be consistent
- Find ways to spend time
with your child
- Focus on teaching life
skills
- Provide encouragement
and support your child to
make healthy choices
Erikson’s (1977) work also examines attachment, which is an important issue
with the mothers at Peardonville House. For example, in the first stage (trust
versus mistrust), many of these children spent time in hospital, foster care, or
did not have their needs met while their mother was active in substance use.
This is associated with negative responses by the child when the mother leaves
and returns, when they often either ignores her or cling to her. It is important to
build positive attachment by having the parent care for the child through
feeding, eye contact, changing diapers, and talking the child through their
actions. It is also crucial for the mother to say goodbye when she leaves her
child. Often parents think that leaving a room while their child is unaware is
healthy, because the child does not cry. However, this does not build trust.
11
Saying goodbye to the child with a hug and a kiss, letting them know a time that
they will be returning, and then returning at that time, engenders trust. We
actively encourage our mothers to follow through on their promises to their
children. If a mother tells their child that they will be back at a set time it is
appropriate to follow through with her to ensure she honours her word to her
child. It is through this congruence of words and actions that trust can emerge.
Family Systems
Family systems theorists view the entire family as the focus of the intervention
(Goldenberg & Goldenberg, 2000). Family members are invited to identify and
change problems in communication, and self-defeating and repetitive patterns
in relationships. Using this perspective, the family is viewed as being a living
organism that is larger then the sum of its members. A change in one member is
thus seen as having ramifications for the family as a whole. In this respect,
interactions are seen as circular rather than linear (i.e., A affects B, yet B also
influences A). According to this view the problems of one family member
cannot be understood independently of other members. The goal of the family
systems approach is to learn and implement new communication patterns.
The family systems approach has particular relevance to the women in our
program, both in reference to their family of origin (as a daughter) and their
own families (as a mother). The program seeks to assist women to learn new
patterns of communicating and responding with their children and significant
others. Family systems theories allow women to think of issues in terms of
systems or a multigenerational family. One feature of this approach is a move
away from blaming others, and beginning to take personal responsibility. This
is vital in our work, as we need the mothers to accept responsibility and start to
rebuild their lives. It is not uncommon for mothers who are involved with the
MCFD to blame the organization for ‘taking away their child’, or for the
women to blame others in their life for ‘making them this way’. Family systems
theories can help these women understand the system and their role within a
larger context. This perspective is also instrumental in assisting mothers to learn
new patterns of communication with significant family members, partners and
older children/youths. By choosing to seek treatment, these women’s decisions
have an impact on others. For some of our mothers this may mean choosing not
to go back into an unhealthy relationship, or that they may need to be
temporarily separated from their children in order to receive help. Mothers in
our program learn that their behaviours impact their children and others.
12
Strength-Based
The shift from a deficit perspective to the concept of a strength-based economy
has been adopted at Peardonville House and in our communities. A deficit
model focuses on what is wrong in an individual’s life, and what is not
happening. It tends to be associated with laying blame, and often creates a
dependency on outside resources and instils helplessness. In contrast, the
strength-based approach seeks to honour, value, and empower the individual,
reinforcing that their capabilities. It builds on the strengths and successes of the
individual and, most importantly, instils hope (Great Kids Inc. 2002).
Utilizing a strength-based model does not mean that concerns are not addressed.
Rather, multiple solutions, based on the strengths of the individual, are
developed (Rudolph & Epstein, 2000). This approach leads to the individual
being more cooperative, having high self-esteem and believing they are
capable.
The women at Peardonville have responded positively to the strength-based
approach. These women know their weaknesses all too well and are often
reminded of them when they meet with social workers and probation officers.
Operating from the strength-based perspective, the women that learn that we
believe in them and that are capable and worthy. We focus on what they are
doing well and use those factors to help them seek recovery in a way that makes
sense for them. In relating to their children, we look for ways to acknowledge
what they are doing well. This could be coming prepared for childcare, arriving
on time to pick them up, or how they handle a situation with their child. This
faith in their ability can be very powerful and is new to many of the women.
Play Therapy
Play is a child’s way of learning about the world and trying on roles. Play is a
safe way for children to deal with experiences that are confusing or scary to
them, as a means of helping them to resolve events. Gil (1991) suggests that
children will reveal their inner feelings when interacting with an empathetic,
supportive adult. The adult can then respond by reflecting the action, words,
and feelings of the child in a non-judgemental manner. The children that come
to Peardonville have, unfortunately, seen and experienced many traumatic
events, and thus the childcare staff encourage play and respond by reflecting the
child’s emotions back to them.
13
One example of a likely play scenario is children pretending that the ‘cops’ are
coming to take them to jail and take their kids to foster care, and so they had
better hide. One child declares that he’s going to ‘fight the pigs’ and not let
them come and take his kids. He then states that he needs a smoke or
something. Another example is a child pretending to not want to go near
another child. She states that ‘he likes to hit my mom and I don’t like him
except when he gives me candy’.
Many of the clients do not have a strong relationship with their children, and
many may have just had their children returned to them after a period in foster
care, and so do not really know their child. The mothers are thus often
interested in finding ways to enhance their relationship. One technique we
encourage is playing with their child. We have compiled a list of strategies to
use in order to initiate play with a purpose. Some of these ideas are as follows.
� Set aside some time every day for playing with your child with no
distractions
� Get down on the floor or be level with your child
� Use direct eye contact
� Let your child lead the play
� Take on the role or noises of the play
� Have fun and laugh
� Try not to do most of the talking
� Let your child know that you had fun spending time with them
We also encourage mothers to develop routines and rituals with their children.
This could be a special time set aside for reading books, going for walks, a
bathroom routine at night, or a snack time during the day. Building routines
allows children to predict what is coming next and is another way to promote
trust and build relationships.
14
Creating a Learner-centered Approach
The Peardonville House parenting program is based on participation. It
incorporates a set of learning principles, including that adults learn best when:
� The women have a voice in deciding what they will learn
� The program is relevant to their needs and what they want to learn
� The women see themselves as part of a caring and supportive group
� The women and their personal experiences and views are valued and
respected by everyone
� The program allows for the women to be themselves and to gain self-
confidence trying out new ideas and practicing new skills
� The positive is encouraged, such that the women are provided with a
great deal of positive reinforcement
� The program provides the opportunity for the women to learn through a
variety of media. This can include activities such as role playing, videos,
discussions, creation of collages and small group work. This is important
as many of the women do not have a formal education and may not know
how to read or write.
� Hands-on learning provides the greatest opportunity for remembering
Multicultural Awareness
Multicultural awareness includes learning to appreciate, value, and understand
cultures other than one’s own (Arthur & Collins, 2005). A broad definition of
culture encompasses more then the cultural group one belongs to, or an
individual’s ethnicity, but encompasses age, gender, sexual orientation,
socioeconomic status, and religious beliefs (Arthur & Collins, 2005). As a
facilitator it is important to be aware of your own biases and assumptions
concerning individuals from other backgrounds, and explore where these ideas
originated and if they are valid. It is vital to respect other cultures within the
group and to recognize and celebrate their differences as strengths which add to

15
the richness of the context. General knowledge about a cultural group can be
helpful, although there is a wide variance within a group, and the individual
may or may not choose to adhere to a specific cultural value.
Differences between individuals can also bring barriers, including distinct
languages, differences in values, different expectations, differences in parenting
practices, labelling, and stereotyping. It is common for differences to emerge in
parenting practices. Our cultural norms, and child welfare and protection
system is based on Western ideologies, which may sharply differ from other
cultures and create challenges for the women in the program. Many of the
women have faced labelling and stereotypical attitudes and comments about
their substance use from their families, communities and society. While we may
not be aware of the specifics of each individual culture, each woman can still be
treated with the dignity and respect that she deserves.
Group Processes
Group work is the preferred teaching method, compared to individual sessions,
for families looking for parenting education and support. Groups are cost
effective and have been shown to benefit members over a significant time span.
A group format allows participants to share their personal experiences with
each other and gain new ideas and learn new ways of doing things. Groups
provide a sense of identity and affiliation for their members.
The majority of the treatment provided at Peardonville House is offered via
groups. The parenting component is no exception, so it is important that the
details of group development be explored. Tuckman and Jensen (1977)
developed a well-known five stage plan for group development. It is important
to note that Peardonville operates on a continual intake basis. This means that
each of the 24 women are at a different place in the ten week cycle. This entails
a different set of group dynamics compared to one where all members begin
together, but the key traits of this five stage model have merit for our program.
Forming: The mothers are unsure of their role in the group at this time. They
are often unclear as to what to say and tend to volunteer and share only limited
information. The mothers will observe during this period, seeking to establish
whether it is safe to share personal information. During this stage the mothers
are developing relationships with other and the facilitator.
16
Storming: This stage is characterized by conflict and attempts to resist
authority. Individuals bend and mould ideas and attitudes to suit the group.
Conflict is present, but it may or may not surface. It is common for the women
to test the rules. As a result of the discomfort at this stage some women are
silent, while others dominate the conversation.
Performing: Not all groups reach this level but for those that do group identity
is strong, morale is high and loyalty is intense. The focus is on problem-solving
and group energy is on task. Roles are flexible and functional.
Adjourning: When the group terminates. For some women it can be a time of
‘mourning’ the loss of group membership. For women at Peardonville, it also
means that they have completed the 10 week program and are ready to leave the
facility. This can be a stressful time as the women are leaving a safe and
supportive environment and returning to the world.
Expectations of Facilitators
The expectations of facilitators will vary across individuals, groups, and from
session to session. This can be best summarized by the following eight methods
for facilitating. This list was generated by speaking with past and current
facilitators and identifying what they have deemed imperative to facilitating a
positive group experience.
1. Active Listening
Active listening means listening for the content and feeling of the message and
then reflecting it back to the speaker to show them that you have understood. It
does not involve providing advice or passing judgement, but reflects only the
message. Active listening helps the mothers to identify their own problems and,
in the process, build up their confidence. Active listening should mean the
women feel listened to and respected. This will validate what they are saying
and in turn will encourage further contributions. Modeling active listening will
encourage other women to do the same with other participants.
Ways to show active listening
� Look directly at the person who is talking
17
� Use minimal encouragers with the speaker. Examples of this are “oh”,
“hmm”. Nonverbal body communication can convey that you are
listening by leaning forward or nodding as they speak.
� Responding with content and feeling . This means not just saying, The
baby is keeping you up all night when a mother shares her feelings about
the incident, instead, say something like, When your baby is crying all
night, it can be overwhelming because you don’t know what to do. It’s
easy to get frustrated because the house-mom comes around to wake you
up early for breakfast and then you’re up for the day and busy.
� By using active listening the facilitator allows the mother time to identify
the problem without offering solutions, and follows the mother’s lead.
2. Effective Communication
As facilitators, our role is to get others talking and sharing their experiences
while minimizing our own contribution. There are issues to be aware of as we
communicate.
� Word selection
o Many of the women may not be familiar with the words and jargon
that you use. This can include speech such as, “Did your child have
a bm?” (bowel movement) or words like developmental or
normative.
o If the women do not understand what you are saying you are no
longer effectively communicating. Instead, use simple and
descriptive language and ask if the mothers understand you.
� Speak slowly and clearly
o Women in early recovery are still overwhelmed with what they are
learning (Hazeldon Foundation, 1995).
o Parenting issues are best approached in a simple way.
� Use of silence
o Silence can be a positive.
o A few moments of silence after you’ve asked a question allows the
women time to gather their thoughts and decide what to say.
18
o It is better to wait than to jump in immediately and take over.
Doing so sends the message that their ideas aren’t worth waiting
for and they will begin to wait for you to respond first.
� Body language
o Our body language conveys important messages.
o Pacing, fidgeting, or tapping can send the message that you are
bored or do not want to be there.
o Relaxing, laughing when appropriate, and sitting in an open and
comfortable manner sends the message to the women that you
want to be there and are interested in what they have to say.
3. Generating Discussion and Questioning
� Encourage discussion
o Ask open ended questions that can’t be answered with one word.
o Practice using “what and how” questions.
� What is your experience with this?
� How can you change this?
� Ask for details
o “Can you tell me what happened next?”
o “Tell me more about what that was like for you?”
� Ask people to brainstorm
o This means putting out an idea and asking the women say
whatever comes to mind. Nothing is evaluated or not included.
o “Is there anything we haven’t thought of yet?”
� Give positive feedback
o Acknowledge a woman’s participation
o “Great idea! I like how you dealt with that.”
o “Sounds like you got sharp problem-solving skills to figure that
one out”
� Refer to ideas the women have made
o This is one way to increase the woman’s self esteem and build
their confidence.
o “That sounds similar to what Kim was sharing with us last week.”
19
o “During the break, Sue was telling me about her son biting and
how she handled it, would you like to share your ideas with
Marg?”
� Open up questions and comments to the group
o “I’m interested to hear what others have to say.”
o “Who would like to respond?”
o “Does anyone have ideas about this to share?”
� Use first names
o Learning the names of the women and using them throughout the
sessions signals respect and promotes effective communication.
4. Promoting Participation
One of the key roles of facilitators is to encourage participation. Being in a
group may be a new experience for some of the women, or perhaps they have
had negative or embarrassing experiences of being in a group. Some women
may be frightened, shy, or not know how to respond in a group setting.
Some ways to involve parents are:
� Give parents a say in the program
o Ask the women what topics are important to them.
o Find out what kinds of activities they like to do and how they want
to learn.
o Have the women assist in setting up the schedule.
o Check with the women to see if and when they want a ‘smoke
break’.
� Get parents talking
o Use small group discussion and then bring it to the larger group.
o Ask questions.
o Use effective communication.
o Be interested.
o Have the women share their experiences. This is a great learning
tool for both them and the other group members.
o Get the parents to relate information in practical ways to their lives
and children.
20
� Encourage mutual support
o These women are together constantly while in treatment and share
many of the same life experiences. It is important to encourage
them to build up informal support from each other, particularly
after their stay at Peardonville House.
5. Being Flexible
The key role of a facilitator is to meet the needs of the women in the group. One
of the hallmarks of being an effective facilitator is being prepared to change the
topic and session plans to meet the needs of the group. This is a common
occurrence at Peardonville House. Many of the mothers are still operating in
crisis, and in concert with weak parenting skills they often need additional
support. If a parent is having a hard time managing her child in the dining room,
or if her child is biting another, it can be brought up as the topic for discussion
instead of what was planned for the day. If a woman is asked to leave, or
perhaps relapses, other mothers may well be upset and need debriefing about
the incident, especially if children are involved. Before the group can focus on
the topic for the week they may need to talk about the issue, so they find some
closure on the event. The facilitator can walk the mothers through such
experiences, providing a forum for sharing their thoughts and expressing their
fears, and then focusing on what they need to do to stay clean for in the present.
If you notice that the group is restless or not paying attention, stop and
comment on it. Ask the group if they are in need of a break or if they are bored
with the topic. Perhaps they don’t understand what the topic is about. Ask for
input. This will give them ownership of the program and make the time more
profitable for them.
If the discussion is lacking direction or rambling off topic, ask the group what
they want. Perhaps the topic is not a priority for them. For example, if you are
talking about health and safety with toddlers and most of the women have
children who are older, the topic will not appeal to them. With clients coming
and going, what you may have planned for one week may not work for the next.
6. Setting Guidelines
In order to ensure a group runs safely and smoothly, guidelines need to be set
very early, for everyone’s benefit. This is an opportunity to invite participation
from the women and ask them to share what they feel is important. In the first
21
session, ask the women how they can keep it a safe and respectful group and
what that means to them. Write down the responses from the women and post
them in the room. Also make copies for the women to take with them. Lastly,
add any other guidelines that you believe are necessary to run a safe and
effective group, as well as ramifications if the guidelines are broken. This will
need to be repeated throughout the sessions when new mothers join the group.
Some guidelines for modelling respect include:
� Let the group know if you need to miss a session
� The mothers should let you know if they are not coming to class. They
need a written excuse if they are unwell or at an appointment
� Begin and end the session on time
� Keep the break to ten minutes
� All members should not interrupt another speaker
� All members should respect someone’s ideas even if they differ from
their own
� All members should avoid laying blame or telling another what to do
� No inappropriate language (profanity, sexist or racist terminology)
� No passing notes or cross-talking when someone else has the floor
� Everyone should use “I” when speaking personally. For example “I feel
this way when you say that and I wonder if you feel that too?”
7. Confidentiality
A valuable exercise to conduct with the group is to explain the conditions
surrounding confidentiality and trust within the program. The women will have
been given this information as part of their orientation package and also have
signed a Release of Information to the MCFD, giving permission to speak with
the social worker. The policy and procedures about confidentiality and
reporting are also explained to the women upon arrival. It is important to clearly
delineate what this means with the mothers.
22
The release of information to the MCFD is typically a written overall report
about the mother, which includes a component on her parenting and ability to
meet the needs of her child. The mother is provided with a written copy of this
report before it is sent to the MCFD, in order to respect and involve the mother.
The mother is given the opportunity to respond or add her own thoughts and
sign the report. A copy of this is then sent to the MCFD, as well as the referring
alcohol and drug agency. This arrangement can initially seem threatening for
the client, and it has implications for how comfortable they feel sharing in the
group. It is important to reassure the mothers that nobody is perfect in their
parenting. It may be appropriate to share a personal example of how
challenging parenting is, even for the facilitators. It is very important to have a
discussion with the mothers and providing concrete examples for them to get a
fuller understanding of what confidentiality means, how Peardonville House
deals with parenting concerns, and what constitutes making a report.
Calls to the MCFD are only made after the mother has been informed, and after
a lengthy opportunity for change with the support of the staff. This is dependent
on the type of behaviour, its severity, and frequency. Any concerns are first
brought to the mother and discussed. Often by providing the mother with a
safety plan, such as calling a staff member when she is overwhelmed, or by
providing strategies for effective parenting, the situation can be resolved. If the
negative behaviour continues the mother will be invited to another meeting. At
this point all attendees will explore what is working and what isn’t, and another
opportunity for change is enacted. The mother is then informed that she will
now be monitored closely and also that further behaviour of this nature will lead
to a joint meeting attended by her social worker.
Encourage the women to keep the experiences that are shared in the group, ‘in
the room’. Discuss how this approach could benefit them, and what some of the
drawbacks might be to that guideline. Reviewing the parameters of
confidentiality is important, as is making the women aware of the types of
incidents that must be reported to MCFD. This is an important issue that
requires complete understanding by the client.
For example, it is not uncommon for women to become easily frustrated with
their children and spank them. This would not necessarily be grounds for
contacting the MCFD, but could be an opportunity to provide some other
alternatives that the parent can use.
23
Another example could be whereby, in sharing a personal experience, a parent
describes behaviours that include harming a child. A parent may also be seen
using harmful behavioural practices with her child. A meeting should be
arranged to address the concern and a plan for change suggested. A staff
member will then check in with the mother to see how the plan is working,
offer encouragement, debrief, and modify the plan as necessary. If the
behaviour continues, another meeting will be called to see what is preventing
positive change from occurring. At this time, the mother will be asked to
commit to healthier changes and will be notified that if positive change is not
evident then another meeting will be called with the social worker in
attendance. If the behaviour continues to persist, the client will be informed of
the need to involve her social worker and the call is placed in the presence of
the client.
Confidentiality is an important component of creating a safe environment for
sharing, and for building a trusting relationship. The mothers need to know the
circumstances under which phone calls to authorities will be made. The women
need to be aware of the parameters surrounding disclosing information, and the
mandatory informing of the MCFD. It is worthwhile to provide concrete
examples of this type of behaviour, such as sexually intrusive behaviour
towards a child, severe physical punishment, or being impaired by drug or
alcohol use that would prevent caring for a child.
Before any decision is made to involve or inform MCFD, attention is given to
the behaviour itself, its frequency, and severity. Reporting is imperative when
there is imminent danger to a child. In this situation, a staff member will remain
with the mother at all times, while the child will remain in childcare with staff
until the appropriate authorities come or the child leaves in an ambulance
accompanied by childcare staff.
8. Handling Challenging Situations
As a facilitator, there are a variety of challenging situations that you may face,
ranging from one woman monopolizing the conversation or giving advice, to an
emotional break-down, or a very quiet individual. Each of these situations is
unique and how you handle them will vary, yet there are some techniques that
you can use consistently.

24
Stay Calm: It is important to monitor your own responses. Take a breath and
speak in a slow, quiet, and calm voice. This will give you a moment to think
and will assist in calming the atmosphere.
Observe Factors: Consider any external factors that may be involved in the
situation. This can include a sensitive topic or lack of group safety.
Remain Respectful: Throughout an exchange it is crucial to respect the
individual or members who were disagreeing. It is important not to take sides or
pass judgement on those involved. This also includes not embarrassing anyone
by confronting them in front of the group.
Use Immediacy: This skill entails immediately exploring what you are noticing,
thinking, and/or feeling now. This can be offered as a tentative question
describing the atmosphere or with respect to the content of the discussion. Ask
the women what they see happening or how they are feeling as a result.
Focus on Commonalities: Finding ideas, beliefs, and values that are common
to the women in order to bind the group together.
Example: Disagreement
If two women are having a disagreement over a method of discipline, attention
can be drawn to how important and sensitive this topic is and how this topic
stirs up some strong emotional responses within us. “It sounds like this topic
brings out passionate responses within us.” “What type of discipline methods
bring out a strong response in you?” This can be related to how we were
parented and what was successful and what was not. It is helpful to look for
common themes among the mothers and focus on the idea that there are many
positive types of guiding and disciplining options available for mothers. You
should emphasize the importance of finding what works for each individual and
providing constancy when disciplining children.
Example: Handling Emotions
A woman begins to sob as she shares her stressful experiences as a single parent
with four children and being active in her addiction. Respond to the deep
feelings that are at the root of the behaviour. Acknowledge the belief or
behaviour, which in this case is the crying. “Some of us cry when we are
touched.” Look for common ground by asking, “How many of us have ever

25
cried about something that touched us deeply? What is happening inside you
when you cry? What would you like others to do when you cry?” Then
summarize the experience for everyone. “We’ve just had the experience of
being touched and of crying. We’ve thought of things that make us respond in
an emotional way and the response we want when we cry. What may we choose
to do the next time we cry or see someone cry?” It can be helpful to normalize
the emotion of crying and explore why people cry. Bring this to an end by
asking whether there is anything else to discuss, or whether you should continue
with the topic of stress in single parenting, or move on to a new topic. This puts
the group in control and leaves the decision-making to them.
Monopolizing Group Time: This is the woman who is enthusiastic and is quick
to respond to every question and comment. Facilitators should not embarrass
her in front of the group by asking her to speak less. Instead, encourage others
to respond and ask other people’s opinions. If necessary, speak to her privately
during the break or after group and offer to have an individual appointment.
This may lead to working out an arrangement where the facilitator uses a
‘signal’ as a visual sign to the client that it is time for someone else to share.
Another idea may be to use an object such as a talking feather or stick, such that
whoever has the object is the only person who may speak.
Argumentative: This is the woman who is naturally argumentative or feels
particularly passionate about the topic. Facilitators can select one good point
and encourage others to respond to it.
Slow Talker: This woman finds it challenging to speak as she is thinking, or
forgets what she is trying to say. As a facilitator, you can help by giving her
time to speak and summarizing what she has said. Thank her for contributing to
the discussion.
Side Conversation: These are women who talk about the topic separately or
who are chatting about other topics. Both are inappropriate and show a lack of
respect for the woman who is speaking. Facilitators can ask these women for a
response and to summarize what the last person has said. If this is happening
frequently, it may be helpful to remind the whole group about this particular
group guideline and see what can be done to minimize this. As a facilitator it is
important to take note of whether side conversations are due to the women
getting bored of the topic or needing a break.

26
Emotional: It is not uncommon to touch on sensitive issues that stir an
emotional response within the women. Facilitators can normalize the situation
and let the women know that crying is fine. It is useful to have tissue on hand
for use as required.
Rambler: This is the woman who easily goes off topic and on tangents while
talking. When there is a break or a breather, choose one comment that is in line
with the topic, respond, and then ask others to provide feedback. It can also be
helpful to summarize other important topics that she has brought up and let her
know that those are great topics to explore in future sessions.
Advice Giver: This is the woman who ‘knows all the answers’ and is willing to
share her opinions with everybody. Tactfully encourage others to share. It may
be appropriate to share some personal examples of not knowing all the answers,
or stating that there are many different ways to raise a child.
Quiet: This is the woman who listens carefully, yet rarely contributes to the
group. As a facilitator, you may want to include her by asking her if she has
anything to share with the group. It may work best to get to know her in the
break and indicate support for her sharing her experiences. Ask her if she would
be willing to share something she said in the break with the whole group, or ask
if you can make reference to what she said with the group yourself.
Definitely Not OK: This person states something that is clearly not correct. As
the facilitator, state that you understand what they are referring to, and then
provide the correct answer without passing judgement or making a big issue.
9. Exploring Values
Much of our lives and parenting experiences are based on our values. As
facilitators, you will be frequently be dealing with values judgements Values
are based on our core beliefs and are very important to us. Our values are
influenced by our life experiences and people in our lives. Values guide our
actions. Often disagreements are a result of a difference in values. Each person
has a unique set of values. People who share a cultural group or religious faith
may hold similar values which guide them in their behaviour.
Facilitators need to know what their personal values are. They need to
recognize that their values are not the only ones, or even necessarily the best
27
values, but their own. By knowing what you believe, you can be careful to not
promote your own values or look down on other people’s values.
The purpose of the parenting group is not to change someone’s values but to
acknowledge values and recognize the diversity in values, and to highlight the
role and impact that values have on the choices parents make. Exploring values
provides us with an opportunity to expand, question or confirm our values.
Due to its abstract nature many of the women will struggle with the concept of
values. It is therefore important to view values in ways that are concrete and
apply to their lives. Talking about values, women can make a connection
between what they believe and how their actions as parents reflect on their
values. It is helpful to discuss how values can evolve over our lifespan and how
we can hold conflicting values at the same time.
Questions to promote exploring values around parenting
Growing up, the way your parents treated you and the things they said and did
gave you messages about what they believed and the values they held.
� What messages did you receive from your parents?
� Which messages were positive?
� Which messages did you like?
� What messages do you give your children?
� What are some values that you would like your children to have?
� What can you do to encourage those values in your children?
� What hidden messages did your parents send you?
� What hidden messages are you sending your children?
You may want the mothers to write down a list of things that they value, where
each came from, and why it is important to them. For some mothers this may
not be possible due to illiteracy or it not being an optimal learning style for
them. Thus it is best to provide some expressive options for the women, such as
collage, drawing, talking in small groups, or finding objects to represent what
they value. Ask the women whether they can provide an example of how, over
28
their lives, a value has changed. Ask them to describe an example of a
conflicting value that they may hold, and discuss how they deal with it.
A common occurrence during group sessions is the conversation turning to how
the women’s substance use has affected their children. This tends to bring out
strong emotions, with the women talking about their feelings of guilt and
shame. While dealing with parenting issues and the effects of substance use on
their children requires honest answers, the associated feelings of guilt and
shame need to be minimized. While we cannot change the pattern of substance
use and behaviour while these women were pregnant or active in their
addictions, we can applaud their desire to give their children a stable, loving,
and healthy environment. It is important to recognize their efforts to seek help
and their desire for a positive change for their children in the present.
Suggested Schedule
Many formats have been found to be useful within the program. The following
option is commonly adopted by facilitators.
Check-in
� At the beginning of each session a check-in period is recommended
� This is a time when each woman can let the group know how she is
feeling and to explore immediate issues that are emerging for them
� During this time the facilitator should note how each woman is doing and
be made aware if one of the members is experiencing additional stress
� Note any concerns that have arisen during the week and that have been
brought forth by other staff
� During this time the group witnesses and validates each woman’s
experience
Example: Ask the woman to choose an animal the best reflects how they are
feeling today. Are they soaring like an eagle today or are they feeling like a pig
wallowing in mud or like a slow moving turtle?
29
Break
� Whenever possible group sessions should not extend longer than 50
minutes without taking a break
� Ask that the women come back promptly in ten minutes
Topic: Presentation, Exercises, and Discussions
� Process is an important ingredient of the program, thus information is
explored through group discussion as to its meaning and understanding
for each of the women
Homework:
� Homework assignments are at the discretion of the facilitator
� Women will sign up to be with their child in the childcare centre for
selected times in the morning to (a) observe staff, and (b) spend time with
their child. Ask the women to remember to journal the experience
afterward and share it in their time with their childcare staff person. The
staff may ask them to prepare something or be involved with the children
during their time in the centre
� Facilitators may ask the mothers to draw or create a collage describing
how they want to parent or what they want for themselves and their child
as they build a future together or find a song that best represents how
they feel about their child or what they would like to say to them
Closing Ritual:
� Find a ritual that works for the group. This may include using guided
imagery, meditation, a quote or song. A ritual that has been used with
success is referred to as ‘marbling out’ where a shiny rock is passed
around and the women share something about their experience that
morning.
This outline is designed to be a guide only. Some topics may need more time
depending on the needs of the clients, while if pressing concerns arise during
check-in, the group may instead choose to focus on that current issue.
30
Balancing Parenting with Early Recovery
The parent in early recovery from substance use still faces many issues, and
tends to be focused on what it takes to remain clean and sober each day.
Recovery needs to come first. Without that, no amount of parent training will
allow a woman to truly parent effectively. Some common themes that arise
during parenting sessions around substance use are as follows.
Shame and guilt: Acknowledge the women’s feelings of shame and guilt and
help them build a vision of hope for the future (Hazeldon Foundation, 1995).
Let them know that they cannot change the past, but acknowledge that they are
working to meet the needs of their child and be the best parent they can be right
now and for the future. Often this shame and guilt is evidenced in permissive
parenting and finding it hard to set limits to the child for fear of offending.
Parents may want to be friends with their child, or not want to upset their child
by setting boundaries. Inform them that children need limits and as a parent
providing limits demonstrates that you love your children.
Goals: In early recovery women often try to take on too much and try to solve
too many problems all at once (Hazeldon Foundation, 1995). This is a recipe for
failure. Encourage simple parenting plans built for success.
Self-care: Taking care of oneself allows a woman to take care of her children.
A woman who has time for exercise, have friends, and attend recovery meetings
is less stressed and can better handle her children’s needs (Hazeldon
Foundation, 1995).
Consistency and Time: Women need to know that effective parenting takes
time (Hazeldon Foundation, 1995). It takes time and consistency to bond with a
child.Rebuilding trust and handling anger also requires time and consistency.
Guiding and disciplining a child takes time and consistency. Encourage the
women to be patient and consistent with their efforts.
Evaluation of Program
The mothers are given the opportunity to provide feedback regarding the
Strengthening Mothers parenting course component at Peardonville House,
including overall effectiveness, content and facilitators. The evaluation form is
attached to the general program evaluation booklet distributed at Peardonville
31
House. Clients are given the option of completing the booklet themselves or
having a staff member from another department assist them such as in cases
where literacy is an issue. The results of the evaluation are confidential. They
are carefully reviewed by the management team and used to initiate change.
The evaluation form includes an informal suggestion box in which the clients
can make comments and propose ideas as to how to make the parenting sessions
meaningful for them. Clients are also encouraged to provide feedback to the
facilitators or their counsellor at any time during the program. The group
facilitators undertake one-on-one interviews with clients when feedback is
sought.
Linkage and Follow-Up
The mothers and children that attend Peardonville House are from throughout
the province of British Columbia. Towards the end of a mother’s stay at
Peardonville, time is spent developing an aftercare plan that the mother and
child can then take home and implement in their own community. Each mother
leaves with a series of recommendations and a progress report reflecting her
time at Peardonville House. Letters of support and acknowledgment to social
workers and courts are commonly provided. The aftercare plan includes a
referral to an alcohol and drug counsellor in her home community. It also
includes a biopsychosocial-spiritual perspective of care which can include
assistance with affordable housing, specialized counselling (e.g., for trauma,
eating disorders, or adult mental health), childcare, legal support, self-care,
spiritual refreshing or advocacy services. This may also include relocation of
the mother and child to a new community for safety reasons or simply for ‘a
fresh start’. Links to supportive care for the child within their home community
may include referrals to an Infant Development Program, Supported Childcare,
child and youth mental health, or art or play therapy. The process of linking the
mother to community support may begin at Peardonville House via phone calls
and the faxing of documentation, as this can allow the mother to have support in
place before she leaves Peardonville House.
According to present practice, follow-up consists of telephone calls from
counselling staff the first, third, and sixth months after leaving, and at the one
year mark. This follow-up provides the staff with an opportunity discover
details of the clients’ current situation, provide supportive counselling if
necessary, and share in the clients’ success.

32
Self-Care for Facilitators
Working with women in early recovery, all of whom are experiencing
heightened emotions, is taxing for facilitators. Often the women come to
Peardonville House with multiple needs and require a significant amount of
support. In order to maintain maximum effectiveness, it is essential that
facilitators take time to engage in self-care themselves, and build a supportive
network of colleagues. Having a support network of colleagues can also be
useful when coming up with ideas and to gain multiple perspectives on client
needs. Having a colleague group to rely on can also help generate relevant
topics and bring forth current research trends. As facilitators, caring for yourself
ensures that you have something left to give to the women.
Closing Thoughts
This training manual is designed to be a starting point for facilitators in
planning and implementing weekly parenting sessions with the women
attending Peardonville House. It provides the facilitator with ideas as to
organizing and guiding the group sessions as well as evaluation and prospective
research on efficacy of the program. Overarching guidelines and principles are
offered in order to facilitate healthy group processes.
The two hypothetical cases presented in this manual highlight the multiple
barriers that these women face as they parent while undergoing early recovery.
The purpose of providing the vignettes is to help those not directly working in
the field (who may facilitate sessions) or those who come in as guest speakers
understand common presenting situations. These cases should help such
individuals gain a better sense of the multiple challenges the mothers in this
program are facing. Use of the vignettes can assist the facilitator in selecting the
most meaningful parenting topics for the women. As illustrated by the two
vignettes, the most useful topics to the mother are bonding and attachment,
safety, nutrition, dealing with guilt and shame, communication, developing
boundaries, guiding and disciplining, developing a routine, and understanding
child growth and development. The vignettes also provide a snapshot of the
multiple and varied concerns clients are dealing with, while simultaneously
enrolled in a recovery and parenting program.
33
The information provided in this training manual should be useful to facilitators
as they plan their sessions, in their efforts to keep language clear and simple,
and use a variety of modalities to best meet the needs of the clients. Permeating
each topic and session is the need to support the women and focus on their
strengths and achievements, while reminding them that their recovery needs to
come first. Without recovery these mothers will not be able to parent
effectively.
The overarching purpose of the parenting groups is to create a positive
environment where mothers can share their stories and support each other. The
mothers should come away feeling supported and respected, with a new focus
on recognizing what they bring to parenting, and novel ways of strengthening
their parenting skills.
34
Feedback: Strengthening Mothers Parenting Group
Thank you for taking the time to complete this feedback questionnaire. Your
input is important to us and helps us find out information about how effective
our Strengthening Mothers Parenting courses are. This feedback allows us to
enhance our program and make it as meaningful as possible for you during your
stay with us. This form is confidential and your name is not attached to your
responses. If you require help completing this form please let your counsellor
know and she will assist you in doing so.
1. What pieces of the parenting group did you like best (give examples)?
2. How can the Strengthening Mothers parenting group be made better?
3. What topics did you feel were most helpful to you?
4. What other topics need to be included?
5. Which guest speakers did you benefit the most from?
6. How well did the facilitators prepare and guide the sessions? What
worked and what can be improved?
7. What are you taking away from this group?
8. How has your knowledge and skill set increased related to parenting?
9. Do you see yourself as a more confident parent?
10. Did the staff assist you in preparing you to return to your community
with your child and helping you connect with the support and services
you need?
11. How was your experience spending time in the childcare centre?
12. Thinking about your overall experience in the Strengthening Mothers
Parenting program, how would you rate it on a scale of 1-5?
1 2 3 4 5
poor needs help o.k. good excellent
35
References
Arthur, N., & Collins, S. (2005). Introduction to culture-infused counselling. In N. Arthur &
S. Collins (Eds.), Culture-infused counselling: Celebrating the Canadian mosaic (p.
3-49). Calgary, AB: Counselling Concepts.
Corey, Gerald (2001). Psychoanalytic therapy. In Theory and practice of counselling and
psychotherapy (6thed., chapter 4, p.74-76). Belmont, CA: Wadswoth Brooks/Cole.
Erikson, E. H. (1977). Identity and the life cycle. New York: International Universities Press.
Froberg, W. (1995). Helping your child through play. Parent Quarterly, 3-7.
Goldenberg, I., & Goldenberg, H. (2000). Family therapy: An overview. Belmont, CA:
Brooks/Cole-Wadsworth.
Gil, E. (1991) The healing power of play: Working with abused children. New York, NY:
Guildford Press.
Great kids, Inc. (2002). Retrieved September 30, 2006, from http:/www.greatkidsinc.org/
strength-based.htm
Hazeldon Foundation (1005). The Real Life Parenting Skills Program The Facilitator’s
Guide. Center City MN: Author.
Patterson, C. H. (2004). Do we need multicultural counseling competencies? Journal of
Mental health Counseling, 26(1), 67-73.
Rogers, C. R. (1957). The necessary and sufficient conditions of therapeutic personality
change. Journal of Consulting Psychology, 21, 95-103.
Rudolph, S. M., & Epstein, M. H. (2000). Empowering children and families through
strength-based assessment. Reclaiming Children and Youth, 8, 207-209.
Tuckman, B., & Jensen, M. (1977). Strategies of small group development. Group
Organizational Studies, 2, 419-427.
67
CHAPTER IV
Synthesis and Implications
Project Impact
Researchers have found that women in early recovery tend to have weak parenting
skills, and there is evidence that significant benefits are associated with increasing their
parenting skills while in treatment for substance use (Miller, 2001). Research conducted by
Brindis et al (1997) demonstrates the positive and longlasting value of parenting programs
for children of women in early recovery. This has an impact on future generations by giving
babies and young children a better start, thereby raising healthier children. Parenting
programs build capacity within the mother which translates into increasing protective factors
passed on to the children. The treatment program at Peardonville House includes a parenting
component, whereby women coming to treatment can bring their infants and preschool aged
children. During the time the mothers are receiving treatment, they are also involved in a
parenting group and hands-on sessions with their children to practice their newly acquired
skills. This manual presented as Chapter III is developed to enable effective and formalized
training of facilitators of the parenting groups at Peardonville House. The aim of this project
is to better equip facilitators to carry out Strengthening Mothers, a psychoeducational
parenting group with women in early recovery.
This facilitator manual is comprised of a number of elements which will enable
facilitators to offer a systematic and evidence-based parenting program to women in early
recovery. The program is based on a number of established theoretical perspectives,
including the client-centered approach, ages and stages theory, family systems theory, the
68
strength-based perspective, and play therapy. Facilitators may choose to align more closely
with one perspective or integrate several or all of the theories into their group sessions.
This project was designed to bring organization and uniformity to the parenting
program Stengthening Mothers’ at Peardonville House. The training manual will provide
facilitators with information and training on the necessary skills required to facilitate an
effective parenting group for women in early recovery. The women will also benefit from
this project, as they can share experiences and learn within a safe setting while acquiring
helpful parenting strategies and building their confidence in their ability to parent.
Strengths
The facilitator training manual developed for the Peardonville House group parenting
program has many strengths. First, the material has been gathered and compiled in a
sequential way in order to orientate a facilitator to the philosophy and audience, and to
review facilitator expectations. Included is a review of the theoretical orientations that
underlie the guidelines and information in the manual. This type of information has never
been presented in this manner to this group before, and thus will serve as a lens through
which the facilitator can interpret, consider, and deliver the parenting group sessions.
Second, the training manual is designed to provide a continuity of service to the
women in the program. The facilitators come from a diversity of backgrounds, and thus the
training manual provides uniformity, specific information on hosting groups, and insight into
the world of parenting in early recovery. Within the manual there is a degree of flexibility as
facilitators can choose to focus on various theories, such as the client centered or
psychosocial development theories of understanding child growth. Another avenue is
exploring family systems in relation to parenting and how each individual influences the
69
system as a whole. Attention is specifically given to the adoption of a strength-based
perspective in the Strengthening Mothers program, in addition to the premise that the
mothers should focus on interacting with their children. The mothers learn about the benefits
of play through enhancing their child’s development and begin to understand how it can be
used as a therapeutic tool to help their child interpret the world. The manual will thus
effectively prepare facilitators for planning and implementing meaningful parenting groups
for the women at Peardonville House.
Third, the manual specifically describes the mechanics of facilitating a group and
provides ways of handling challenging situations. This information was incorporated in order
to prepare the facilitators to more effectively interact with the mothers. The manual also
emphasizes the importance of using a variety of mediums in order to meet the needs and
learning styles of the women. This manual also demonstrates how to explore core values and
emphasize areas of commonality with the women in the groups.
Finally, the facilitator manual is written in a user-friendly format, with a focus on
practical ideas and examples focused particularly on women in early recovery at Peardonville
House. The facilitator training manual provides an opportunity for the facilitators to gain
confidence and competence in presenting and facilitating group parenting sessions.
Limitations
While the training manual effectively meets a specific need, and is representative of
the most vital component of the Peardonville House parenting program, there are certain
limitations in the design and use of the manual First, the manual provides a general overview
of issues that women may face while parenting in early recovery. Specific health issues,
disabilities, and legal concerns that are common to the women and influence their ability to
70
parent are not discussed in depth. This is simply because it is not possible to focus on each
possible area of concern or conflict that the women may experience.
Second, this manual is designed to be a general guide for facilitators in the
Peardonville House parenting program. The manual does not explicitly structure each
session. This was intentional, as the specifics of a given session will partly be determined by
the ages of the children involved, and needs of the women as a whole. The facilitators are
thus expected to use creative license to gather relevant material geared to meet the needs of
the mothers. For instance, if the mothers in a given group tend to have toddlers and have
experience biting issues recently, topics related to school-aged or teenage children will not be
as meaningful.
Third, the manual includes a section on cultural awareness, but does not describe in
depth the issues affecting any particular cultural group. The variety of cultural groups
represented at Peardonville House means that it would not be possible to address the types of
factors and variables inherent to each cultural group. Further work may be undertaken to this
component of the manual for future editions. Collecting information as to the cultural
background of the mothers at Peardonville House at intake would be a useful exercise, to see
which cultures utilize Peardonville House. This information would allow a systemic
investigation to be initiated into ways to increase the cultural awareness of the staff in the
program. Seeking feedback from the mothers is a helpful way to find out how to increase
cultural relevance for them, and identify which components of the program they prefer.
The manual and the group facilitation process does not specifically address issues
such as trauma and post traumatic stress disorder, which are known to be at high rates in this
population. However, by identifying and linking the mothers to specialized counselling and
71
resources within their own community (as one component of the plan of care package) these
needs can be addressed.
Finally, the manual has yet to be implemented and evaluated. The utility of the
manual and other apparent strengths and weaknesses may materialize as the manual becomes
operational. Feedback from the facilitators and the women will provide a starting point for
deciding what further changes need to be made.
How Project May Benefit Others
The training manual as presented here may be adapted to other community agencies
or day treatment programs that work with women in recovery. It provides a framework that is
portable and generalized, and can easily be adopted by those working with women in
recovery in a variety of settings. Some modifications would be necessary to target the
specific needs of other programs; however, this training manual offers a starting point.
Working with other agencies in providing resources enhances networking and ensures a
continuity of care for the women.
This training program may also be adapted for use at Kinghaven, the sister
organization Peardonville House which treats men in early recovery from substance use. The
facility is home to 55 men, many of which are fathers and who would benefit from learning
about parenting and exploring their role as a father and parent. The program could also be
expanded to be implemented with couples, who may both be in recovery and simultaneously
parenting or connected with their children in some capacity.
The manual was developed to be user friendly and to provide a compilation of
organizational ideas that can facilitate the creation of a successful parenting group. The
72
manual focuses on preparing facilitators with practical strategies to develop and deliver
sessions that will be meaningful for the women.
Future Directions for Research
The concept of women being able to bring children to treatment is relatively new, and
thus further research into the long-term effects of providing treatment for mothers and
children is needed. Positive findings would enable organizations to lobby for increased
funding to create more mother-child spaces. In particular, research examining services that
best meet the physical and psychological needs of the children while their mothers are in
treatment are urgently needed. There is also a need to confirm through research, the parenting
themes that women in early recovery are dealing with, as this will assist facilitators in
developing meaningful parenting sessions and guide the design of parenting programs for
women in early recovery. There is also an opportunity to investigate the efficacy of this
parenting program, in terms of its impact on women’s wellbeing, recovery, and ability to
parent. The evaluation process is at an early stage, but the results garnered will be compiled
and reviewed in order to identify possible additions to the program, hence maximizing its
effectiveness.
Conclusion
This applied project involved developing a training manual for facilitators delivering
the parenting program Strengthening Mothers at Peardonville House. The manual is also
provided as the product in this document. Facilitators utilizing this manual will be better
equipped to offer engaging group sessions based on theoretical principles and will
demonstrate strong communication skills. The manual was aimed to assist facilitators in
understanding dynamics of group processes, and necessary tools required to establish
73
successful parenting groups while the members are experiencing early recovery. This training
manual is designed to increase the skill levels of facilitators, improve their competence, and
enhance their confidence when delivering the group parenting program at Peardonville
House. In a parallel process, it is hoped that women partaking in the program will experience
enhanced competence and confidence in their mothering abilities.
74
References
Brindis, C., Berkowitz, G., & Clayson, Z. (1997). Option for recovery promoting perinatal
drug and alcohol recovery, child health, and family stability. Journal of Drug Issues,
27, 607-624.
Miller, A. F. (2001). A critical need: Substance abuse treatment with children. Corrections
Today, 63, 88-91.
Related Documents











