Asthma Heterogeneity: Endotypes, Phenotypes and Choosing the Right Treatment Michael Wechsler, MD MMSc Director, NJH Cohen Family Asthma Institute Professor of Medicine National Jewish Health [email protected] Property of Presenter Not for Reproduction

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Asthma Heterogeneity: Endotypes, Phenotypes and
Choosing the RightTreatment
Michael Wechsler, MD MMScDirector, NJH Cohen Family Asthma
InstituteProfessor of MedicineNational Jewish Health
erty o
f Pres
enter
Not for
Rep
roduc
tion

Disclosures
Dr. Wechsler has received consulting honoraria from AstraZeneca, Boehringer Ingelheim, Glaxosmithkline, Novartis, Regeneron, Sanofi, Teva
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Asthma Defined
• Asthma is a heterogeneous disease, characterized by chronic airway inflammation and history of respiratory symptoms such as
• Wheeze
• Shortness of breath
• Chest tightness
• Cough that varies over time and in intensity
• Variable airflow limitation
Global strategy for asthma management and prevention. Global Initiative for Asthma website. https://ginasthma.org/wp‐content/uploads/2018/04/wms‐GINA‐2018‐report‐tracked_v1.3.pdf. Updated 2018. Accessed September 2018.
Healthy airway
Muscle
Normal bronchial tube lining
Asthma
Inflamed lining
Severe Asthma
Inflamed lining
Excess mucus
Severely tightened muscle
Tightened muscle
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Heterogeneity in Asthma—Not a New Concept
Spector SL, Farr RS. J Allergy Clin Immunol. 1976 May;57(5):499‐511.
.
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Asthma is Not a Clinically Homogeneous Condition
• Multiple areas of difference:• Clinical presentations• Physiological characteristics• Responses to therapy
• Time of asthma development is a key factor:• Children—relatively homogeneous with a strong personal and family allergic history of atopy
• Adults—very mixed group of patientsPropert
y of P
resen
ter
Not for
Rep
roduc
tion

Basis for Disease is Present Early and Evolves Throughout Life
Genetics
Proteins, biochemical pathways, cells
Physiology, symptoms
, environment
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Factors That Can Contribute to Uncontrolled Asthma
Uncontrolled AsthmaUncontrolled Asthma
•Cyclical nature of disease•Increased disease severity•Differing asthma phenotypes
Disease-Related Factors
•Medication under-prescribing•Failure to assess adherence•Failure to assess inhaler technique
•Misdiagnosis•Lack of asthma action plan•Absence of specialty care
Physician-Related Factors
•Passive smoking•Frequent exposure to traffic or air pollution
•Outdoor and indoor allergens
Environmental Factors•Comorbidities (eg, GERD rhinosinusitis, depression)
•Smoking•Obesity•Age •Psychosocial issues (eg, lower income, poor health literacy)
•Poor treatment adherence•Inadequate inhaler technique•Heterogeneity of treatment response
•Failure to follow self-management plan
•Side effects of other medications (eg, NSAIDs)
Patient-Related Factors
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

The Asthma Patient Population is Segmented Based on Disease Severity
Asthma Patient Population
Intermittent Mild Moderate Severe
Persistent Asthma
National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. National Heart, Lung, and Blood Institute website. https://www.nhlbi.nih.gov/files/docs/guidelines/asthsumm.pdf. Published October 2007. Accessed September 2018.
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Evolution of Asthma Classification
1980’s-1990’s
Inflammation
Early 2000’s
Identification of phenotypes and
clusters
Late 2000’s
Precision medicine:
identification of endotypes and mechanisms of
disease including T2 vs. non-T2
Present
Precision therapy by endotype
Desai M, Oppenheimer J. Ann Allergy Asthma Immunol. 2016;116(5):394-401.
1960’s-1970’s
Bronchoconstriction
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

1. Assess adherence and make sure it’s asthma
2. Characterize the asthma-what type of asthma is it?
3. Treat the Asthma
Approach to Asthma Mangement
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Asthma Phenotype vs Endotype
Phenotype
The set of observable characteristics of an
individual resulting from the interaction of its genotype with the
environment
Endotype
A specific biologic mechanism that explains observable properties of
an organism
Different asthma phenotypes and endotypes may respond differently to targeted therapies
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Understanding Severe Asthma Heterogeneity Through Phenotyping and Endotyping
1. Chung KF et al. Eur Respir J. 2014;43:343-373.
Severe Asthma Phenotype
and Endotype
GenesGene
expression
Airway epithelium,
smooth muscle
Environment:Infections/
Irritants
Patient factors
Comorbid disease
Environment: Allergies
Meds/Adherence
CytokinesImmune
cells
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Asthma Phenotypes
Kim H, et al. Allergy Asthma Clin Immunol. 2017;13:48.
Category PhenotypeTrigger‐induced asthma • Allergic
• Nonallergic• Aspirin‐exacerbated respiratory disease (AERD)• Infection• Exercise‐induced• Occupational
Asthma patient characteristics • Smoking• Obesity• Elderly• Black
Clinical presentation of asthma • Pre‐asthma wheezing in infants− Episodic (viral wheeze)− Multi‐trigger wheezing
• Exacerbation‐prone asthma• Asthma associated with apparent irreversible
airflow limitation
Category PhenotypeTrigger‐induced asthma • Allergic
• Nonallergic• Aspirin‐exacerbated respiratory disease (AERD)• Infection• Exercise‐induced• Occupational
Asthma patient characteristics • Smoking• Obesity• Elderly• Black
Category PhenotypeTrigger‐induced asthma • Allergic
• Non‐allergic• Aspirin‐exacerbated respiratory disease (AERD)• Infection• Exercise‐induced• Occupational
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Separation of Asthma Into Clinical Phenotypes
• Unbiased hierarchical cluster analysis• Clinical characteristics (gender, age of onset, severity)• Physiology (lung function, airway hyperresponsiveness)• Triggers (allergens, tobacco, occupation)• Sputum inflammatory cells (eosinophils, neutrophils)
• Sum total of characteristics are segregated into groups, with no single feature playing a predominant role in the classification Prop
erty o
f Pres
enter
Not for
Rep
roduc
tion

Asthma Cluster Approaches and Eosinophilic Inflammation1
1. Adapted from Haldar P et al. Am J Respir Crit Care Med. 2008;178:218-224.
Sym
ptom
s
Early Symptom Predominant
Early onset, atopic; normal BMI; high
symptom expression
Primary Care Asthma
Secondary Care Asthma
Eosinophilic Inflammation
Discordant Symptoms
Concordant Disease
Discordant Inflammation
Monitoring inflammation allows down-titration of CS
Symptom-based approach to therapy titration may be
sufficient
Monitoring inflammation allows targeted CS to lower
exacerbation frequencyBenign AsthmaMixed middle-aged
cohort; well-controlled symptoms and
inflammation; benign prognosis
Obese Noneosinophilic
Later onset, female preponderance; high symptom
expression
Inflammation PredominantLate onset, greater proportion of males; few daily symptoms but active eosinophilic inflammation
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

The Transition from Phenotyping and Endotyping to Genotyping
16
Personalized approach to asthmaDiagnosis
Refractory asthma?
Characterize subtype
Phenotype/Cluster approach
Endotypes (Th2 high vs. low) Genotype
GenderAge
ObesityEthnicity/RaceSmoking Hx
Early vs. Late Onset
Blood biomarkers
Sputum biomarkers
Other
IgEEosinophils
PeriostinCytokines
EosinophilsNeutrophilsCytokines
FeNO
TAILORED THERAPYDunn and Wechsler 2015
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Asthma is Not Just One Disease
Howard R, Rattray M, Prosperi M, Custovic A. Curr Allergy Asthma Rep. 2015;15(7):38. Lötvall J, Akdis CA, Bacharier LB, et al. J Allergy Clin Immunol. 2011;127(2):355‐60.
Asthma SyndromeSymptoms of asthma, variable airflow obstruction
Allergy Lung function
Exacerbations
Airway inflammatio
n
Wheeze, cough, other symptoms
Asthma Phenotype CharacteristicsBased on observable features with no direct relationship to a disease process (e.g., gender, age, obesity, ethnicity, smoking history, early vs. late onset, etc.)
Asthma EndotypesDistinct functional or pathophysiologic mechanisms that may be present in clusters of
phenotypes; identified by biomarkers (e.g., blood, sputum, urine, FeNO, exhaled breath)
Endotype 1 Endotype 2 Endotype 3 Endotype 4 Endotype 5
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Why Endotype?
To personalize therapy and maximize drug response
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Biomarkers to Identify Asthma PhenotypeCurrent
• Sputum eosinophils
• Circulating blood eosinophils
• Exhaled nitric oxide
• IgE
• Allergen skin testing
? Future
• Periostin
• Dipeptidyl peptidase‐4 (DPP‐4)
• Eosinophil peroxidase
• Urinary bromotyrosineIgE = Immunoglobulin E.
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Asthma Endotypes
• Type 2 asthma– Eosinophilic– High nitric oxide– High IgE– Mediated by IL‐4, IL‐5, and IL‐13
IL, interleukin; TNF, tumor necrosis factor.Chung KF, et al. Eur Respir J. 2014;43(2):343‐373; Kim H, et al. Allergy Asthma Clin Immunol. 2017;13:48.
• Non‐type 2 asthma– Neutrophilic– Mediated by IL‐1, IL‐6, IL‐17, and TNF
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Inflammatory, Immunologic, and Pathobiologic Features Leading to Severe Asthma
Israel E, Reddel HK. N Engl J Med 2017;377:965-976
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Inflammation, Endotypes, and Phenotypes in Severe Asthma are Heterogeneous
Gauthier M, et al. Am J Respir Crit Care Med. 2015;192:660–668; Fahy JV. Nat Rev Immunol. 2015;15:57–65; Wenzel SE. Nat Med. 2012;18:716‒725; Woodruff PG, et al. Am J Respir Crit Care. 2009;180:388–395; Dunican EM, Fahy JV. Ann Am Thorac Soc. 2015;12 Suppl 2:S144–S149; Peters MC, et al. J Allergy Clin Immunol. 2014;133:388–394; Volbeda F, et al. Thorax. 2013;68:19–24.
Eosinophilia (eosinophilic asthma)
Severe Asthma
Type 2‐high Type 2‐low IL‐4, IL‐13, IL‐5‐mediated IL‐6, IL‐17, TNF mediated
Allergic sensitization
Neutrophilia
Paucigranulocytic
Disease burden: Exacerbations, symptoms, airflow obstruction/FEV1 impairment
Early age of onset Later age of onset
Elevated FeNO
Chronic rhinosinusitis ± nasal polyps
Atopic dermatitis
Elevated IgE
Type 2 inflammation is prevalent in patients with uncontrolled persistent asthma, and these patients have the highest disease burden
Endotype
Phenotype
Comorbidities
Biomarker
Obesity, infections, smokers
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Targeted Pathways for Biologic TherapiesTargeted PathwaysIgE Inhaled allergens stimulate production of IgE by B lymphocytes and bind to mast
cellsdegranualationIL-5 Pro-eosinophilic cytokine; cytokine that regulates proliferation, maturation, migration, and
effector functions of eosinophilsIL-4
IL-13
Cytokine found in increased levels in airways and sputum of asthma patients and involved in eosinophil trafficking and B cell production of IgECytokine associated with eosinophil trafficking and production of eNO from epithelial cells
TSLP Novel target; epithelial-cell-derived cytokine; drives allergic inflammatory responses by activating dendritic cells and mast cells
Non-Type 2 Inflammatory Pathways IL-17 Cytokine produced by Th17 cells; plays important role in the immunologic responses seen in
asthmaCXCR2 Potent chemoattractant for neutrophils; under investigation in asthma and COPD
CXCR2, Chemokine receptor 2; IgE, Immunoglobulin E; Th2, T helper 2 cells; TSLP, Thymic stromal lymphopoietin
Wechsler ME. Respir Care. 2018 ;63:699-707.
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Novel Asthma Therapies Anti IL5: mepolizumab, reslizumab, benralizumab Anti IL4- R alpha/Anti IL13: dupilumab Anti IL13 lebrikizumab, tralokinumab Other Novel therapies:
• Anti TSLP• Anti IL33• Anti IL17• Anti IL6• Anti M1’• Anti Gata3 DNAzyme• TLR9 agonists• CRTH2 Antagonists• Antibiotics• Vitamin D
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

What is your approach to treating patients with severe asthma?
Treat with personalized approach Identify asthma type by phenotype or endotype Treat with the most appropriate therapeutic
strategy based on underlying asthmatic mechanism of inflammation
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

What can we achieve with biologics?
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

What can we achieve with biologics?
Reduced exacerbation Reduced steroid dose and side effects Improved symptoms and quality of life Disease modification to prevent asthma over long
term
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Which therapy is best for a specific patient? How do you choose between biologics?
George L, et al. Ther Adv Chronic Dis. 2016;7:34-51.
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Which therapy is best for a specific patient? How do you choose between biologics?
• Biomarkers help predict therapeutic responses Phenotype patients and choose most appropriate therapy Goal of personalized or “precision medicine” Potential need to measure different biomarkers to determine
endotype/phenotype
George L, et al. Ther Adv Chronic Dis. 2016;7:34-51.
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

BLOCKING EOSINOPHILS WITH ANTI IL5
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Eosinophilic asthma
• Asthma can be classified phenotypically as eosinophilic (40–60% of cases) or non-eosinophilic
• Symptom severity is increasedin eosinophilic asthma
• Interleukin-5 (IL-5) regulates proliferation, maturation, migration and effector functions of eosinophils
• IL-5 mRNA is increased in patients with asthma, correlates with asthma severity, and is inducible by allergen exposure
Corren J. Discov Med 2012;13:305–12Kouro T & Takatsu K. Int Immunol 2009;21:1303–9
Miranda C, et al. J Allergy Clin Immunol 2004;113:101–8Wenzel SE. Lancet 2006;368:804–13
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

epithelialcell
basophil
smoothmusclecell
mast cell
neutrophil
dendriticcell
macrophage
monocyte
eosinophil
endothelialcell
B cell neuronmyofibroblast
TH2
TH1TH0
IL-3, IL-6IL-8, ECPRANTESMBP
IL-8GM-CSF
IL-6IL-8LTECP
IL-3IL-4GM-CSFTNF-
IL-4TNF-
IL-4IL-5
IL-1IL-2IL-4IL-10IL-16 IL-4
RANTES
RANTESIL-3, IL-5GM-CSF
Eosinophilic cytokines contribute to the chronic inflammatory process
allergen/irritant
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

IL‐5
BenralizumabMepolizumabReslizumab
The targets: IL‐5 or eosinophils (IL‐5Rα)
Eosinophil
IL, interleukin
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Total exacerbations over time are reduced with mepolizumab vs. placebo
Pavord I, et al. Lancet 2012;380:651–9
Inclusion criteria • sputum eos >3%,• FeNO>50, • blood eos >300,• deterioration of
asthma after <25% reduction in ICS or OCS
• AND
>2 asthma exacerbations in previous year
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

MEPOLIZUMAB NEJM 2014
ORTEGA NEJM 2014 BEL NEJM 2014
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Reslizumab Effects on Exacerbations and Lung Function
Castro et al. Lancet Respir Med 2015; Epub ahead of print 36
1009080706050403020100
0 10 20 30 40 50 60 70 80
Pro
babi
lity
of n
ot h
avin
g C
AE
(%)
244 169 138 112 107 97 0 0 0PlaceboNumber at risk
245 207 177 158 146 136 1 0 0Reslizumab
0.40
0.30
0.20
0.10
00
LS m
ean
chan
ge fr
om b
asel
ine
in F
EV
1(L
)
4 8 1216202428323640444852 Endpoint
Visit (week)
PlaceboReslizumab
PlaceboReslizumab 3.0 mg/kg
Placebo; n=244Reslizumab 3.0 mg/kg; n=245HR 0.575 (95% CI 0.440–0.750)p<0.0001
††
†
*
†† † † † †
† †*
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Benralizumab and Exacerbations
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Reduction in ExacerbationEosinophils ≥300 cells per μL
Bleecker ER, et al. FitzGerald JM, et al.
(1.12‐1.58)
p<0.0001(0.60‐0.89)
(0.77‐1.12)
p=0.0018(0.48‐0.74)
p=0.0188(0.54‐0.82)
Percentage reduction relative to placebo‐45% ‐51%
Percentage reduction relative to placebo
‐36% ‐28%
FitzGerald J et al. Lancet Online Publishing, thelancet.com. September 2016.
Bleecker E et al. Lancet Online Publishing, thelancet.com. September 2016.
Annu
al asthm
a exacerbatio
n rate ra
tio (9
5% CI)
Annu
al asthm
a exacerbatio
n rate ra
tio (9
5% CI)
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

P NAIR ET AL, NEJM MAY 2017
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Does Broader Blockade of Type 2 Cytokines Improve Outcomes?
Dupilumab
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Anti IL4/13 and Asthma
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Dupilumab in Asthma
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Improvement in Lung Function, On Top ofCombination Rx
P < 0.001
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Dupilumab Significantly Lowers Rates of Severe Exacerbation in a Phase 3 Trial
Castro M, Corren J, Pavord ID, et al. N Engl J Med. 2018;378(26):2486‐2496.
• Phase 3, randomized, double‐blind, placebo‐controlled trial
• n=1902 patients ≥12 years of age with uncontrolled asthma stratified by baseline blood eosinophil level
• Randomized to receive add‐on SC dupilumab at a dose of 200 or 300 mg every 2 weeks or placebo for 52 weeks
• Primary outcomes: Annualized rate of severe asthma exacerbations and the absolute change from baseline to week 12 in FEV1 before bronchodilator use
Risk of Severe Asthma Exacerbations
0.1 0.25 0.50.751 1.5 2
DupilumabBetter
PlaceboBetter
A Dupilumab, 200 mg Every 2 Wk, vs. Matched PlaceboSubgroup No. of Patients Relative Risk vs. Placebo (95% Cl)
0.54 (0.43‐0.68)
0.33 (0.23‐0.45)0.56 (0.35‐0.89)1.15 (0.75‐1.77)
0.31 (0.19‐0.49)0.44 (0.28‐0.69)0.79 (0.57‐1.10)
0.52 (0.41‐0.66)
0.34 (0.24‐0.48)0.64 (0.41‐1.02)0.93 (0.58‐1.47)
0.31 (0.18‐0.52)0.39 (0.24‐0.62)0.75 (0.54‐1.05)
B Dupilumab, 300 mg Every 2 Wk, vs. Matched Placebo
Placebo DupilumabOverall 317 631Eosinophil count≥300 cells/mm3 148 264≥150 to <300 cells/mm3 84 173<150 cells/mm3 85 193
FENO≥50 ppb 71 119≥25 to <50 ppb 91 180<25 ppb 149 32
5
Subgroup No. of PatientsPlacebo Dupilumab
Overall 321 633Eosinophil count≥300 cells/mm3
≥150 to <300 cells/mm3
<150 cells/mm3
FENO≥50 ppb≥25 to <50 ppb<25 ppb
142 27795 17583 181
75 12497 186
144 3170.1 0.25 0.50.751 1.5 2
DupilumabBetter
PlaceboBetter
Relative Risk vs. Placebo (95%Cl)
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Dupilumab Significantly Improved Lung Function
Castro M, Corren J, Pavord ID, et al. N Engl J Med. 2018;378(26):2486‐2496.
Change in the Prebronchodilator FEV1 from Baseline over 52‐Weeks
The benefit of dupilumab on FEV1 was greatest among patients with a blood eosinophil count of ≥300 eos/cc at baseline
0.0
0.1
0.2
0.3
0.4
0 2 4 6 8 10 12 16 20 24 28 32 36 40 44 48 52
Week
Least‐Squares M
ean Ch
ange
from
Baseline in FEV
1 (liters)
No. at RiskDupilumab, 300 mgDupilumab, 200 mgPlacebo, 2.00 mlPlacebo, 1.14 ml
633631321317
625610313315
614613311307
612615313301
609604311305
598607309301
610611313307
611605310300
593601304303
596599296300
586589304290
579585301286
584590301289
584577297287
570581292288
562570290281
488477250240
Dupilumab, 300 mgDupilumab, 200 mgPlacebo, 2.00 mlPlacebo, 1.14 ml
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

BLOCKING IGE WITH OMALIZUMAB
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Omalizumab Blocks IgE Binding to Mast Cells
Mast cell
IgE molecule
FcRI receptor
Omalizumab Omalizumab
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

ExacerbationExacerbationReduces asthma exacerbations and
symptoms
Reduces asthma exacerbations and
symptoms
Release of IgE
Plasma cellPlasma cell
-switch-switch
AllergensAllergens
Mast cellsBasophilsMast cellsBasophils
OmalizumabOmalizumab
Binds to free IgE, reducing
cell-bound IgE
Binds to free IgE, reducing
cell-bound IgE
Reduces high-affinity
receptors
Reduces high-affinity
receptors
Reducesmediator release
Reducesmediator release
Allergic mediatorsAllergic
mediators
Allergicinflammation:
eosinophils and lymphocytes
Allergicinflammation:
eosinophils and lymphocytes
Omalizumab Mechanism of Action
B lymphocyteB lymphocyte
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

0.2
0.1
0.3
0.4
0
0.1
0.2
0.3
0.4
0.5
Study 1 Study 2
Mea
n ex
acer
batio
ns p
er p
atie
ntSummary of Reduction in
Asthma Exacerbationsin Pivotal Studies 1 and 2
0.2 0.2
0.4
0.3
0
0.1
0.2
0.3
0.4
0.5
Study 1 Study 2
Mea
n ex
acer
batio
ns p
er p
atie
nt
Stable Steroid Phase16 weeks
Steroid Reduction Phase12 weeks
P = 0.005 P <0.001 P = 0.004 P <0.001
Omalizumab PlaceboProp
erty o
f Pres
enter
Not for
Rep
roduc
tion

Different biomarkers and omalizumab response
Hanania NA et al. Am J Respir Crit Care Med. 2013;187:804‐811.
Effect of omalizumab based on Th2 biomarkers
Redu
ction in protocol‐d
efined
Asthm
a exacerba
tion rate (M
ean %, 95%
CI)
FeN0 Eosinophils Periostin<19.5 ppb ≥19.5 ppb <50 ng/mL ≥50 ng/mL<260/µL ≥260/µL
–16
–53
–9–32 –3 –30
40
20
0
–20
–40
–60
–80n = 193P=0.45*
n = 201P=0.001*
n = 383P=0.54*
n = 414P=0.005*
n = 279P=0.94*
n = 255P=0.07*
*Exacerbation reduction P‐values; omalizumab versus placebo in each biomarker subgroup.
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Propert
y of P
resen
ter
Not for
Rep
roduc
tion

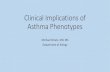
Tezepelumab treatment reduced the annualised AER vs placebo at Week 52
53
• Significant reduction in annualised AER for all tezepelumab treatment groups compared with placebo; P<0.001
***P<0.001, compared with placebo group. Sequential testing approach was used to adjust for the multiplicitycaused by the multiple dose‐placebo comparisons. The hierarchy was tezepelumab 280 mg, 210 mg, and70 mg vs placebo
Asthma exacerba
tion rate
(per patient‐year)
Treatment groupN=146N=145N=145N=148
0.0
0.2
0.4
0.6
61% 71% 66%
0.67
0.260.19 0.22
Percentage AER reduction vs placebo
*** *** ***
Placebo (N=148)Tezepelumab 70 mg Q4W (low dose) (N=145)
Tezepelumab 210 mg Q4W (medium dose) (N=145)Tezepelumab 280 mg Q2W (high dose) (N=146)
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Anti TSLP in Asthma (Corren 2017)
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Individualizing Asthma Therapy: Conclusions
• Response to asthma therapies is variable
• Need to understand who responds to what
• We now have multiple novel biologic therapies that may treat patients with severe eosinophilic asthma
• How will we decide which therapies work best in which patients?
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Treating Severe Asthmatics Now
• Do extensive workup• Endotype your patients
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Asthma Biomarkers
• IGE• FENO• EOS
– Sputum– Blood
• Periostin• DPP4 (Dipeptidyl Peptidase 4 / CD26;
an adipokine)Prop
erty o
f Pres
enter
Not for
Rep
roduc
tion

• Other factors influencing the decision: patient comfort with a new agent vs older treatment with more experience
Selecting Treatment for Severe Asthma: Anti-IgE Versus Anti‒IL-5
1. Papathanassiou E et al. Eur Clin Resp J. 2016;3:31813. 2. Magnan A et al. Allergy. 2016;71:1335-1344.
Head-to-head studies are needed
Anti-IgE or Anti‒IL-5 or Anti IL4/13
Patients with allergic noneosinophilic asthma
Anti-IgE or Anti IL4/13 if eNO high
Patients with allergic eosinophilic asthma
Patients with eosinophilic asthma who:• Are nonallergic
OR• Do not respond to anti-IgE treatment
OR• Are out of range of dosing
for anti-IgE treatment
Anti‒IL-5 or Anti iL4/13
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Conclusions
• Asthma is a spectrum of diseases, with different pathologic and clinical phenotypes
• There has been an increased understanding of the immunology of asthma, leading to new therapeutic options
• Defining phenotypes and endotypes in asthma is a young field, but it is making progress
• Tailoring treatment to phenotypes and endotypes is the ultimate goal Prop
erty o
f Pres
enter
Not for
Rep
roduc
tion

Conclusions
• Patients with severe asthma may require additional evaluation and referral
• Patients with allergic asthma not well controlled with high‐dose ICS and an additional controller can be considered for treatment with omalizumab
• Patients with severe eosinophilic asthma not controlled with ICS/LABA may benefit from an inhibitor of IL‐5 (mepolizumab, reslizumab, or benralizumab)
• Consider Dupilumab with eosinophilic or type 2moderate severe asthma or on systemic steroids
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Understanding Disease Mechanisms May Guide Therapy to a More Personalized Approach
Willis JC, Lord GM. Nat Rev Immunol. 2015;15(5):323‐329.
One Size Fits All Personalized MedicineStratified Medicine
• Evidence‐based• One treatment for all
• Evidence‐based• Different treatments for groups of patients
• Evidence‐based• Individualized treatment for each patient
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Providing Asthma Care is a Team Sport
Patient
Nurse Practitioner
AllergistPediatrician
Pulmonologist
Otolaryngologist
Pulmonary Rehabilitation Specialist
Case Manager
Immunologist
Primary care physician
School personnel
Pharmacist
Nurse/APN
Your Asthma Care Team. University of Rochester Medical Center website. https://www.urmc.rochester.edu/encyclopedia/content.aspx?contenttypeid=134&contentid=253. Accessed September 2018.
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

FUTURE QUESTIONS• How will clinicians and payers decide between different
biologics based on existing biomarkers?
• Can we use combinations of biologics?• Are there biomarkers that should be studied other than
blood eosinophils, IgE, FeNO?
• What are best therapies for nontype 2 severe asthma?• What about Asthma COPD overlap Syndrome???
63
Propert
y of P
resen
ter
Not for
Rep
roduc
tion

Drug Phase Dosing Frequency Route Exacerbation Reduction Rate
(vs. Placebo)
Increased FEV1 (vs. Placebo)
ReslizumabAnti IL5
Approve 2016 3.0 mg/kg Q4W IV 50-59% 110-126 ml
MepolizumabAnti IL5
Approved asthma 2015; Phase 3 COPD
100 mg Q4W Sub-Q 53% 98 ml
BenralizumabAnti IL5 Receptor
Approved asthma 2017; Phase 3 COPD
30 mg Q8W (first 3 doses every 4 weeks)
Sub-Q 36-55% (Q4W frequency)28-70% (Q8W frequency)
0-125 ml
OmalizumabAnti IgE
Approved asthma 2003; Approved urticaria
125mg –375mg (basedon weight/ IgE level)
Q2W or Q4W (depending on weight/ IgE level)
Sub-Q 33-75% NS
DupilumabAnti IL4 Receptor
Approved 2017 for Atopic Dermatitis;2018 for Asthma
200-300 mg Q2W Sub-Q 59.9-80.7% 390-430ml
TezepelumabAnti TSLP
Phase III for asthma
70‐280 mg Q2‐4 W Sub‐Q 61‐71% 110‐150 mlProp
erty o
f Pres
enter
Not for
Rep
roduc
tion

Thank [email protected]
Confidential – Not for DistributionDUP-14387
65
Propert
y of P
resen
ter
Not for
Rep
roduc
tion
Related Documents