Asthma and Co-Morbid Conditions Richard F. Lockey, M.D. Director, Division of Allergy and Immunology Department of Internal Medicine University of South Florida College of Medicine James A. Haley Veterans’ Hospital Tampa, Florida

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Asthma and Co-Morbid Conditions
Richard F. Lockey, M.D.
Director, Division of Allergy and Immunology
Department of Internal MedicineUniversity of South Florida College of
MedicineJames A. Haley Veterans’ Hospital
Tampa, Florida
Learning Objectives
• Physicians will gain additional insight about co-morbid conditions associated with asthma.
• Such familiarity will lead to better clinical outcomes and quality-of-life for patients with asthma.
• Treatment guidelines for asthma should address these co-morbid conditions.
1. Food2. Rhinosinusitis
a. Allergicb. Non-allergicc. Infectiousd. Nasal polyposise. Other
3. Gastroesophageal Reflux Disease (GERD)
4. Vocal Cord Dysfunction (VCD)
5. Obesity6. Osteopenia and
Osteoporosis
7. Psychological Problems8. Churg-Strauss Disease9. Sleep Apnea10. Pregnancy11. COPD versus Asthma12. Eczema13. Smoking Cessation14. Infection (Vaccination)15. Bronchiectasis and Cystic
Fibrosis16. Exercise-Induced Asthma17. Others- Endocrine,
Conjunctivitis,Congestive Heart Failure, Pulmonary Embolism, Medications
18. Primary Ciliary Dyskinesia
Introduction• Asthma is perhaps the most treatable of all
chronic diseases.• Continuous treatment necessary to
prevent symptoms and exacerbations. • For optimal outcomes, co-morbid
conditions must be identified and treated.• Co-morbid conditions and their diagnosis
and treatment should be included in asthma guidelines
Questions and procedures for patients with asthma (children and adults)
1. History + ask and think about co-morbid conditions
2. Risk factors for various co-morbid conditions (almost everyone has risk factors)
3. Complete physical examination4. Psychological profile5. Sleep profile6. Weight assessment
Questions and procedures for patients with asthma (children and adults)
7. Smoking (drinking and drug) assessment8. Diet – appropriate calcium and vitamin D.
Exercise (walk 1.5 miles) or stand (1.5 hours)
9. Spirometry and flow volume loop, as necessary
10. Dexa bone scan?11. Rhinoscopy, as indicated12. Vaccinations (flu, Pneumovax, Tdap,
? herpes zoster)13. Others as necessary
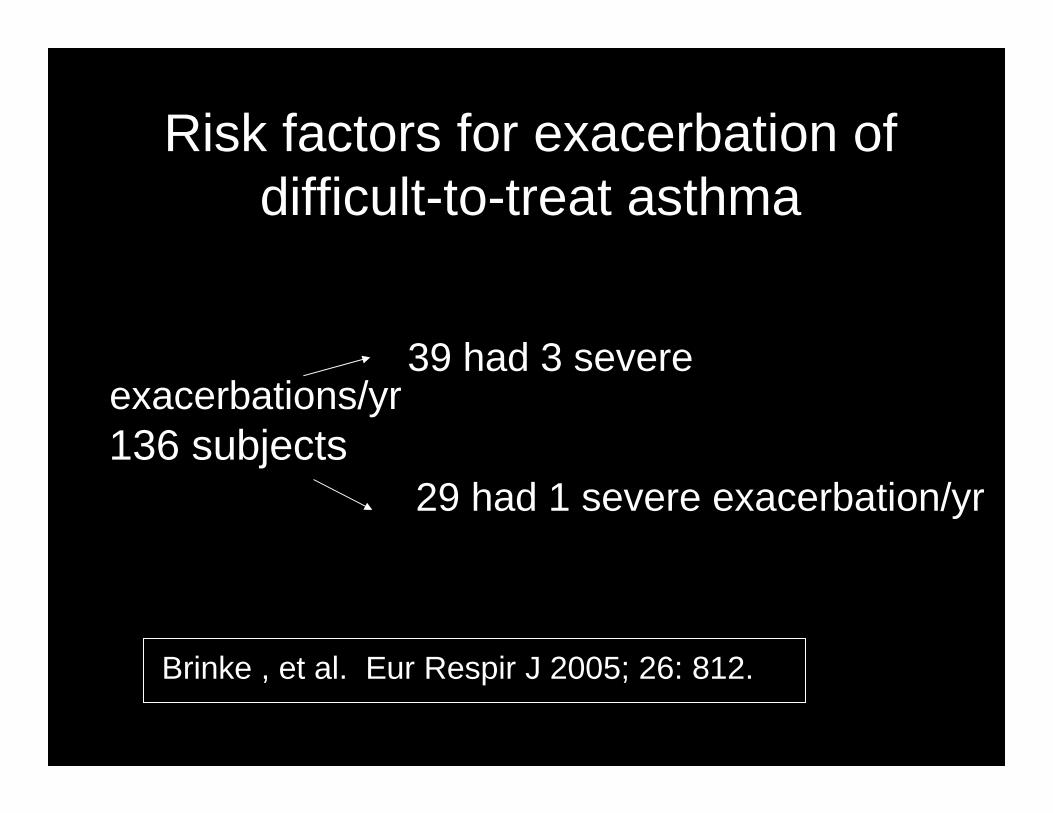
Risk factors for exacerbation of difficult-to-treat asthma
39 had 3 severe exacerbations/yr136 subjects
29 had 1 severe exacerbation/yr
Brinke , et al. Eur Respir J 2005; 26: 812.
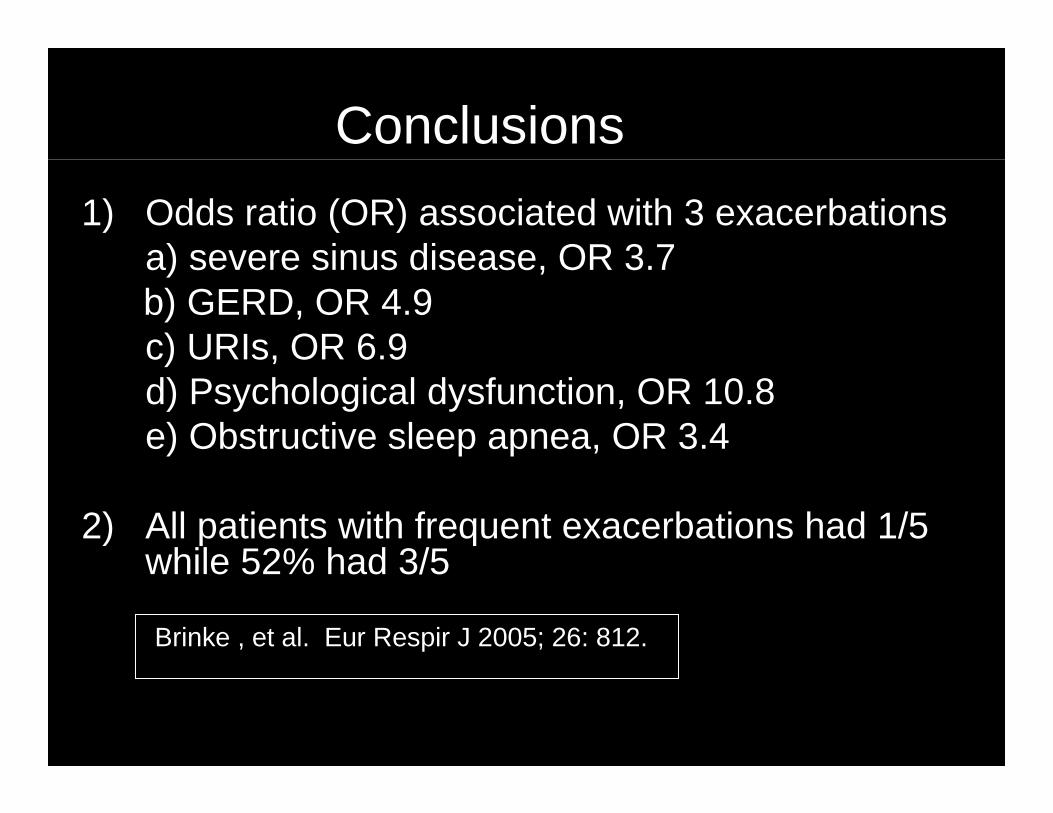
Conclusions
1) Odds ratio (OR) associated with 3 exacerbationsa) severe sinus disease, OR 3.7b) GERD, OR 4.9c) URIs, OR 6.9d) Psychological dysfunction, OR 10.8e) Obstructive sleep apnea, OR 3.4
2) All patients with frequent exacerbations had 1/5 while 52% had 3/5
Brinke , et al. Eur Respir J 2005; 26: 812.
Rhinosinusitis
Rhinosinusitis (Allergic, Nonallergic, Infectious) and AsthmaIncidence and Association
1. Rhinitis (all kinds) linked to sinusitis (rhinosinusitis) and to nasal polyps –all of which are co-morbid conditions of asthma
2. Up to 70% of patients with asthma alsopresent with rhinosinusitis.
Annesi-Maesano I. Allergy 1999;54 (suppl) 7-13
Rhinosinusitis (Allergic, Nonallergic, Infectious) and Asthma
Incidence and Association
3. Allergic rhinitis can be a precursor of asthma
4. Deterioration of rhinitis symptoms negatively impacts bronchial responsiveness and conversely adequate management of rhinitis improves asthma
5. Chronic sinus disease may be linked to severe asthma
Bachert C et al. In: Middleton 7th ed. Allergy: Principles and Practice, p 991
Rhinosinusitis (Allergic, Nonallergic, Infectious) and Asthma
Incidence and Association
6. Postulated that perennial allergic and non-allergic rhinitis rather than seasonal rhinitis predisposes to “sinusitis”
7. Controlling infectious sinusitis may decrease asthma medication needs
Moss MH et al. In: Middleton 6th ed. Allergy: Principles and Practice, 2003, p 1225
Nasal Polyps and Asthma1. Nasal polyps unusual in atopic patients.2. 40 – 80% of aspirin-exacerbated asthma
subjects have nasal polyps and 15% of polyp patients have aspirin-exacerbated asthma.
3. Nasal polyps in 37 – 48% of patients with cystic fibrosis (some patients have concomitant asthma)
4. Bronchial hypersensitivity exists in many patients with polyps.
Bachert C et al. In: Middleton 7th ed. Allergy: Principles and Practice, p 991
Gastroesophageal Reflux Disease
(GERD)
Atypical symptoms of GERD
• Chest pain• Hoarseness• Chronic cough• Sore throat• Wheezing
– 80% of subjects with asthma may have GERD
• Throat clearing(feels like “cotton-ball” which cannot clear)
• Globus• Laryngospasm• Dental erosion
-Mujica et al. Postgrad Med 1999-DeVault et al. Am J Gastroenterol 1999
Prevalence of GERD in Children
• Abnormal pH probes common and many such patients have no clinical symptoms
Chiquette et al. J Asthma 2002;39:135Khoshoo et al. Chest 2003;123:1008Sheikh et al. Pediatr Pulmonol 1999;28:181
Effect of GERD Rx on Asthma
• Decreased exacerbations or improved QOL– Littner MR Chest 2005;128:1128
– Sharma B et al. Journal of Gastroenterology2007;13:1706
– Khoshoo V et al. Journal of Pediatric Gastroenterology & Nutrition 2007;44:331
– Shimizu Y et al. Tohoku Journal of Experimental Medicine 2006;209:181
– Jiang SP et al. European Review for Medical & Pharmacological Sciences 2005;9:151
Effect of GERD Rx on Asthma
• Improved PEFR– Kiljander TO et al. Am J Respir Crit Care Med
2006;173:1091
Cochrane Data Base Review of GERD Treatment for Asthma in Adults
and Children (2006)• 12 randomized controlled trials of Rx for GERD in
adults and children• 2 independent reviewers• Interventions included proton pump inhibitors (6), H2
receptor antagonists (5), surgery and conservative management (1)
• Temporal relationship in 4 trials found between asthma and GERD
• Anti-reflux Rx did not consistently improve lung function, asthma symptoms, nocturnal asthma and medication use
• Conclusion: No overall improvement but subgroups may gain benefit; albuterol use may be decreased
GERD and Chronic Rhinosinusitis
• Upper respiratory symptoms frequent among subjects with symptomatic GERD Dx’d by esophageal study
• GERD associated with chronic rhinosinusitis in children and adults
-Theodoropoulos DS et al. Am J Resp Crit Care Med 2001;164:72-6-Barbero GJ. Otolaryngol Clin North Am 1996;29:27-38-Phipps CD et al. Arch Otolaryngol Head Neck Surg 2000;126:831-6-Ulualp SO et al. Am J Rhinol 199;13:197-202-DiBaise et al. Ann Int Med 1998;1291078-83

Vocal Cord Dysfunction (VCD)
Vocal Cord Dysfunction (VCD)Definition of VCD• Paradoxical adduction (closure) of the vocal
cords/ folds during inspiration and/or early expiration
• “Irritable larynx syndrome”• Episodic laryngeal dysfunction triggered by
irritant exposures or can occur spontaneously with variable clinical manifestations: chronic cough, frequent throat-clearing, globus pharyngeus, choking episodes, dysphonia, masquarades as asthma; exercise–induced asthma, or complicates asthma
-Mikita JA, et al., All Asthma Proc 2006;27:411.-Bahrainwala AH, et al., Curr Opin Pulm Med 2001;7:8.-Byrd RP, et al., Postgrad Med 2000;108:37.-Balkissoon R, In: Nonallergic Rhinitis, Baraniuk JN, Shusterman D (eds): Informa
Healthcare USA, Inc., New York, pp. 411, 2007.
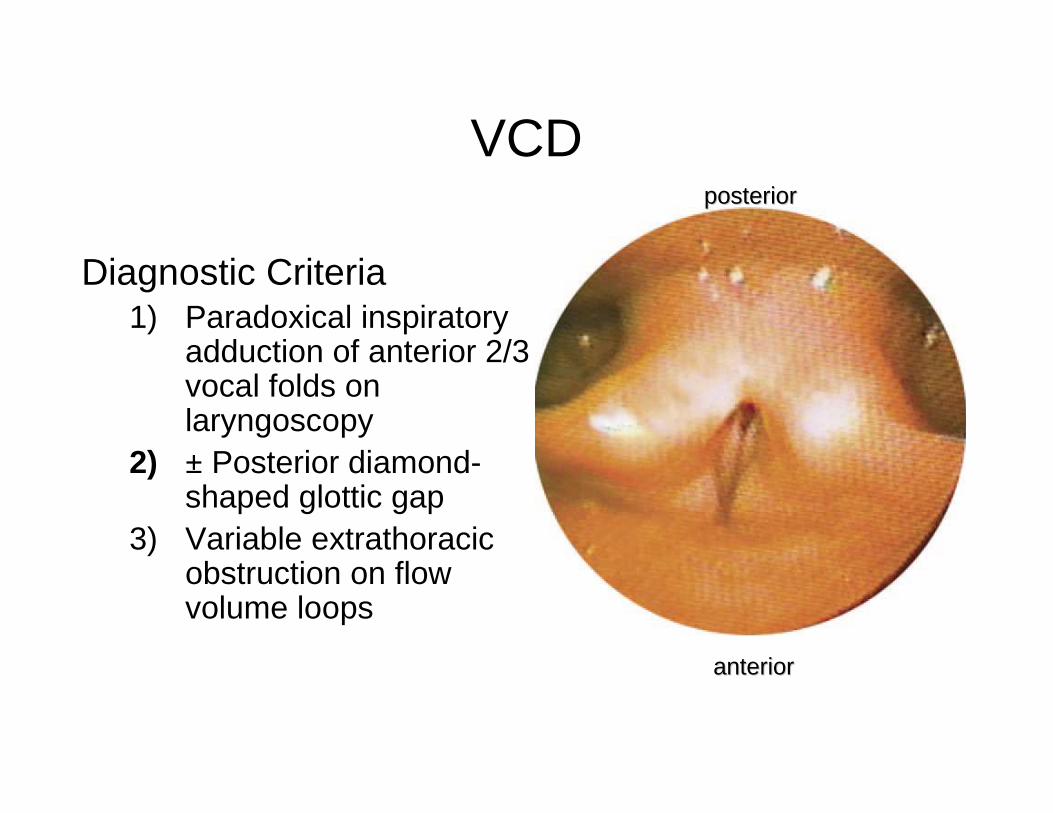
VCD
Diagnostic Criteria1) Paradoxical inspiratory
adduction of anterior 2/3 vocal folds on laryngoscopy
2) ± Posterior diamond-shaped glottic gap
3) Variable extrathoracic obstruction on flow volume loops
posteriorposterior
anterioranterior
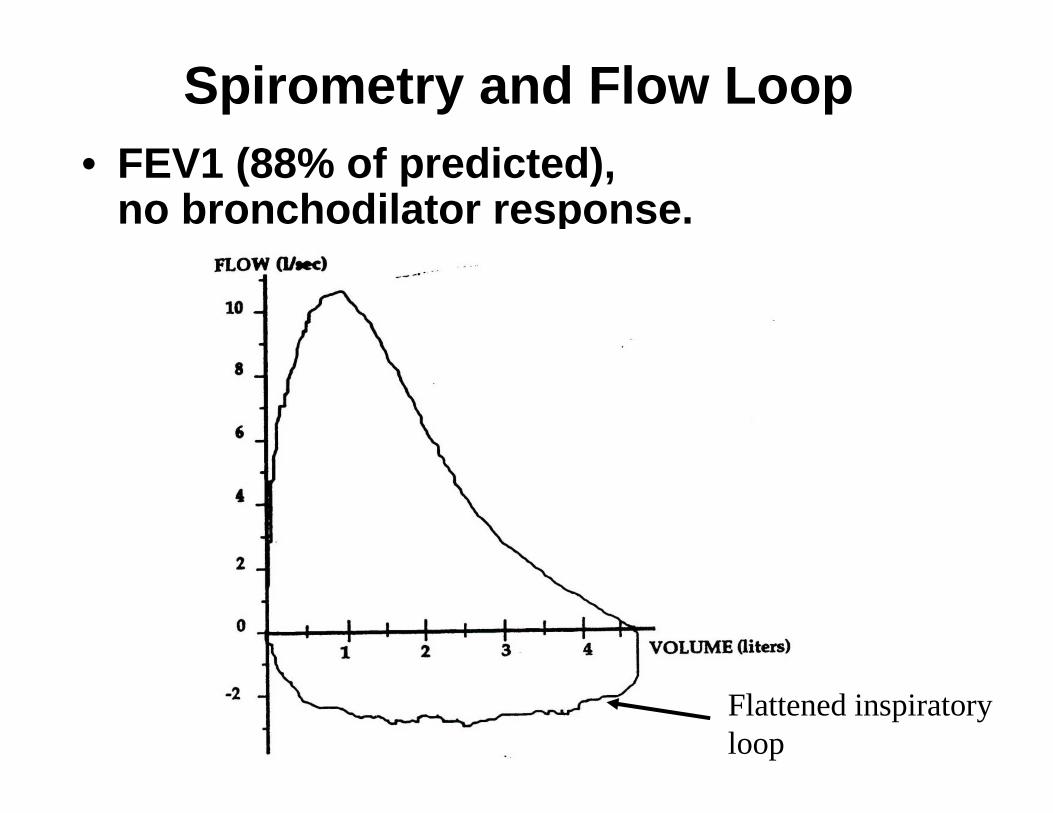
Spirometry and Flow Loop• FEV1 (88% of predicted),
no bronchodilator response.
Flattened inspiratory loop
Vocal Cord Dysfunction (VCD)
National Jewish Health95 subjects with asthma and/or VCDa. 42 had VCD aloneb. 53 had VCD with asthmac. 28% had been intubatedd. Misdiagnosed with asthma for average
of 4.8 yrse. “Very sick patients” with VCD
Newman AB et al. Am J Resp Crit Care Med 1995;152:1382

VCD: Treatment
• Multidisciplinary approach
• Treat underlying disorders; rhinitis, GERD/LPR, asthma
• Suppress cough: cough causes laryngeal injury• Speech pathology: throat relaxation, cough
suppression, throat clearing suppression, instruct on control of laryngeal responses to irritants and how to abort an acute attack
• Discontinue unnecessary medication
• Psychological support
Obesity
Asthma and ObesityObesity Increases the Incidence of Asthma• 17 prospective studies, 9 in adults and 8 in
children• Each involved several thousand subjects• Follow up periods of 2-21 years• Only 1 failed to show an increased
incidence of asthma in the obese• Obesity antedates asthma• Many controlled for exercise• Most show an effect of overweight as well
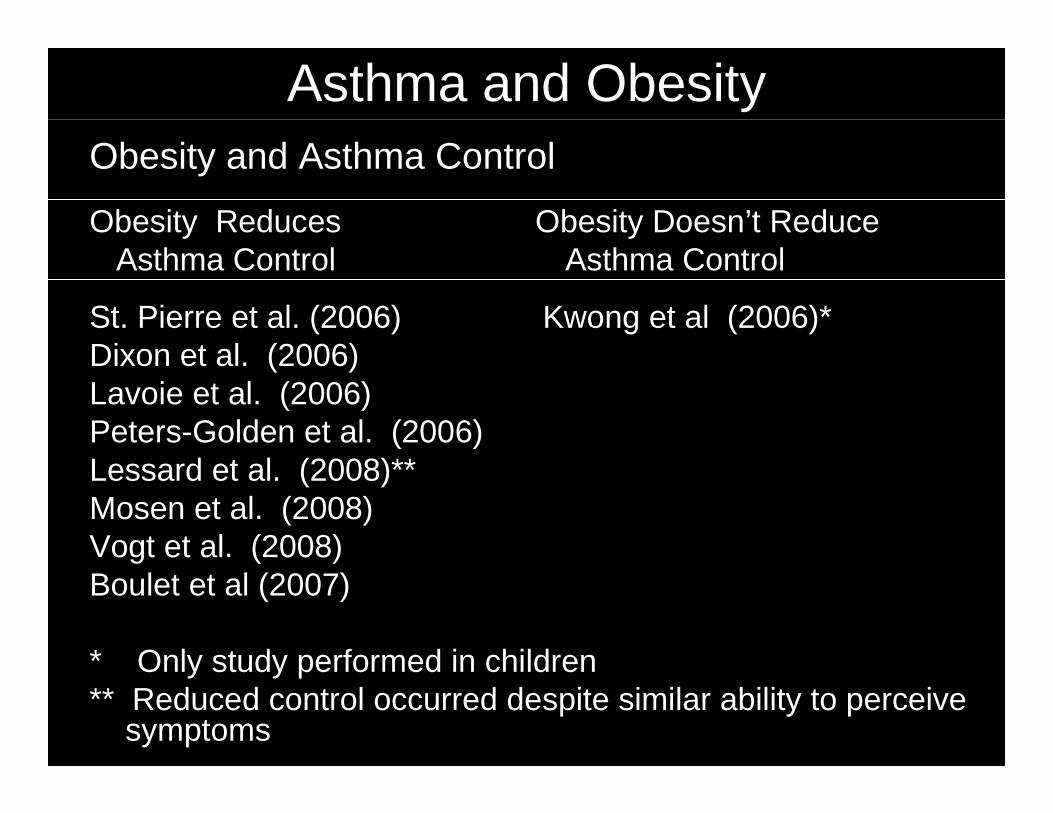
Asthma and Obesity Obesity and Asthma Control
Obesity Reduces Obesity Doesn’t ReduceAsthma Control Asthma Control
St. Pierre et al. (2006) Kwong et al (2006)*Dixon et al. (2006)Lavoie et al. (2006)Peters-Golden et al. (2006)Lessard et al. (2008)**Mosen et al. (2008)Vogt et al. (2008)Boulet et al (2007)
* Only study performed in children** Reduced control occurred despite similar ability to perceive
symptoms
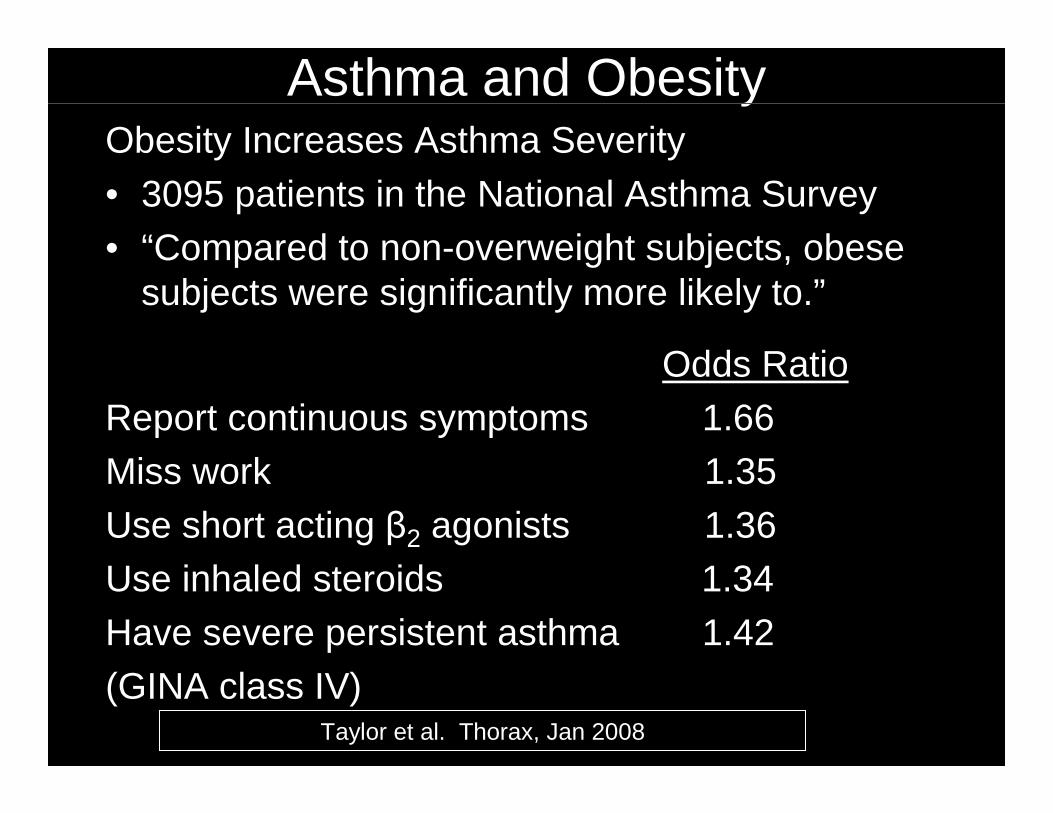
Asthma and ObesityObesity Increases Asthma Severity
• 3095 patients in the National Asthma Survey• “Compared to non-overweight subjects, obese
subjects were significantly more likely to.”
Odds RatioReport continuous symptoms 1.66Miss work 1.35
Use short acting β2 agonists 1.36Use inhaled steroids 1.34
Have severe persistent asthma 1.42(GINA class IV)
Taylor et al. Thorax, Jan 2008
Osteoporosis and Osteopenia
Osteoporosis and OsteopeniaInhaled Corticosteroid (ICS) Use and Bone
Mineral Density• One in three asthmatics in UK receive ICS
(majority beclomethasone in current study)– Approximately 30% receive more than 800
micrograms per day
• 2000 micrograms per day for 7 years or 1000 micrograms per day for 14 years would result in a decrease of 1 SD in bone mineral density (double the risk of fracture)
LancetLancet 2000;335:13992000;335:1399--403403
Osteoporosis and Osteopenia
Stratify Risk of Osteoporosis• High risk
– Chronic systemic corticosteroid (CS) (daily or qod)
– Systemic CS > 4 weeks continuously– Systemic CS bursts > 4 per 12 months– >2 other risk factors with chronic, moderate to
high dose inhaled corticosteroid
Ledford D et al. J Allergy Clin Immunol 1998;102(3):353-62
Psychosocial Problems
Psychosocial Problems
• Stress is linked to many diseases –asthma is no exception
• Stress may alter immune system in direction of Th2 response
• Depression particularly dangerous –especially for severe asthma
• Psychological problems are particularly dangerous for a patient with severe asthmaBloomberg GR, Chen E. Immunol Allergy Clin N Am 2005;25,83
Psychosocial Problems
• Stress associated with increased prevalence of asthma
• Stress associated with increased exacerbations
• ? whether asthmatic children have significantly more total anxiety disorders, lower self-esteem, greater functional impairment, past school problems, past psychiatric illnesses, and familial stress
-Guilbert T et al. In Middleton 7th ed. Allergy: Principles and Practice, 2009, pp 1319-1343-Wright RJ et al. Am J Respir Crit Care Med 2002;165:358-365-Sandberg S et al. Lancet 2000;356:982-987
Psychosocial ProblemsTreatment• Compliance is always a problem in
treatment, particularly those with psychological problems
• Compliance is always a suspected problem in patients with severe asthma
• Treat with prevention education, counseling, support, access to care and appropriate medications
- Guilbert T et al. In Middleton 7th ed. Allergy: Principles and Practice, 2009, p1333-National Asthma Education and Prevention Program. Expert Panel Report 3: Guidelines forthe diagnosis and management of asthma: clinical practice Guidelines. Bethesda (MD): NIH/National Heart, Lung, and Blood Institute 2007; August:4051
Asthma and Sleep Apnea
Asthma and Sleep Apnea
Definition
Obstructive Sleep Apnea Syndrome (OSAS) is:1. Complete or partial collapse of the
upper airways during sleep with consequent cessation of breathing despite ongoing respiratory effort plus coexistent daytime somnolence.
2. Coexistent daytime somnolence (disabling)
-Staevska MP, Baraniuk JN. Rhinitis and Sleep Apnea. In: Baraniuk J, -Shusterman D (eds). Nonallergic Rhinitis, 2007, Informa Healthcare, New York,449-472
Asthma and Sleep Apnea
Adult Symptoms
At least one of the following 3 observations:1. Patient complaints of unintentional sleep
episodes during wakefulness, daytime sleepiness, unrefreshing sleep, fatigue, or insomnia.
2. Patient wakes up at night with breath holding, gasping, or choking.
3. Bed partner observes symptoms of loud snoring and/or breathing interruptions.
-Staevska MP, Baraniuk JN. Rhinitis and Sleep Apnea. In: Baraniuk J, -Shusterman D (eds). Nonallergic Rhinitis, 2007, Informa Healthcare, New York,449-472
Asthma and Sleep ApneaSymptoms - Children1. The caregiver reports snoring and/or labored or
obstructed breathing during sleep.
2. The caregiver observes at least one of the following: - Paradoxical inward rib cage motion during
inspiration movement arousals- Diaphoresis- Neck hyperextension during sleep- Excessive daytime sleepiness, hyperactivity, or
aggressive behavior- Slow rate of growth- Morning headaches- Secondary enuresis
Staevska MP, Baraniuk JN. Rhinitis and Sleep Apnea. In: Baraniuk J, Shusterman D (eds). Nonallergic Rhinitis, 2007, Informa Healthcare, New York, 449-472
Conclusions
• HS a problem in primary school children• HS associated with significant risk factors• HS associated with sleep-disorder
breathing symptoms• HS associated with sleep-disordered
breathing symptoms and adverse neurobehavioral outcomes
HS = habitual snoring
Li AM, et al. Chest 2010;138(3):519-527
Asthma and Sleep ApneaPrevalence of Obstructive Sleep
Apnea-Hypopnea (OSAH) in Severe versus Moderate Asthma
1. 23 of 26 (88%) with severe asthma, 15 of 26 (58%) with moderate asthma, 8 of 26 (31%) controls without asthma had apnea-hypopnea index ≥ 15 events/hour.
Using more restrictive criteria, 50% severe, 23% moderate, and 12% (control) of subjects had obstructive sleep apnea (OSA).
2. No correlation between severity of sleep-disordered breathing and asthma severity.
Julien JY et al. J Allergy Clin Immunol 2009;124:371-6
Asthma and Sleep Apnea
1. Risk of sleep apnea increases with nasal obstruction, large adenoids and tonsils, and elongated face.
2. Rhinitis appears to increase the risk of obstructive sleep apnea.
3. Many other risk factors associated with sleep apnea include obesity, gastroesophageal reflux, endocrine problems, and others.
Asthma and Sleep Apnea
Treatment1. Recognition: look for signs and
symptoms. (Epworth Sleepiness Scale)2. Treat underlying disorders from upper
airway disease to obesity.3. Continuous Positive Airway Pressure
(CPAP)
Pregnancy
Pregnancy
Effect of Pregnancy on Asthma• Meta-analysis shows that one-third
improve, one-third stay the same, and one-third deteriorate.
• URIs the most common precipitants of severe asthma during pregnancy.
-Juniper EF, Newhouse MT. Effect of pregnancy on asthma: a systemic reviewand meta-analysis. In: Schatz M, Zeiger RS, Claman H, eds. Asthma andImmunologic diseases in pregnancy and early infancy. New York, Marcel Dekker; 1998:401
-Murphy VE et al. Obster Gynecol 2005;106:1046-1054
COPD versus Asthma
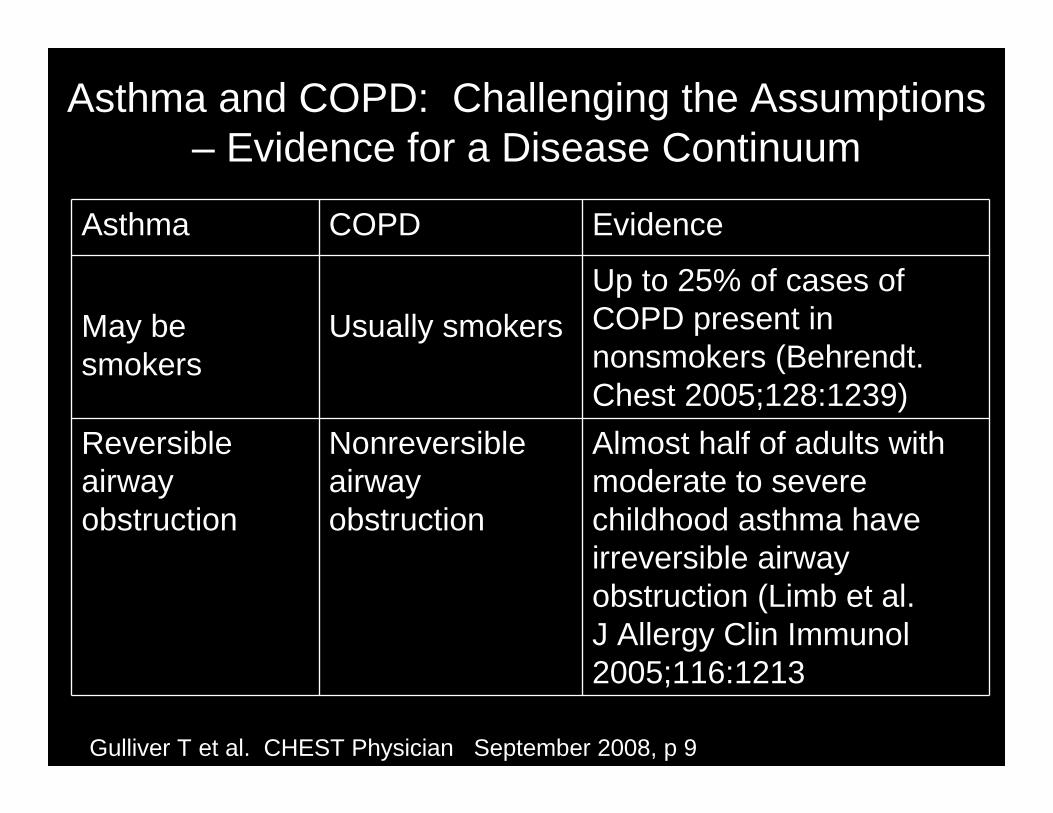
Asthma and COPD: Challenging the Assumptions – Evidence for a Disease Continuum
Asthma COPD Evidence
May be smokers
Usually smokersUp to 25% of cases of COPD present in nonsmokers (Behrendt. Chest 2005;128:1239)
Reversible airway obstruction
Nonreversible airway obstruction
Almost half of adults with moderate to severe childhood asthma have irreversible airway obstruction (Limb et al. J Allergy Clin Immunol 2005;116:1213
Gulliver T et al. CHEST Physician September 2008, p 9
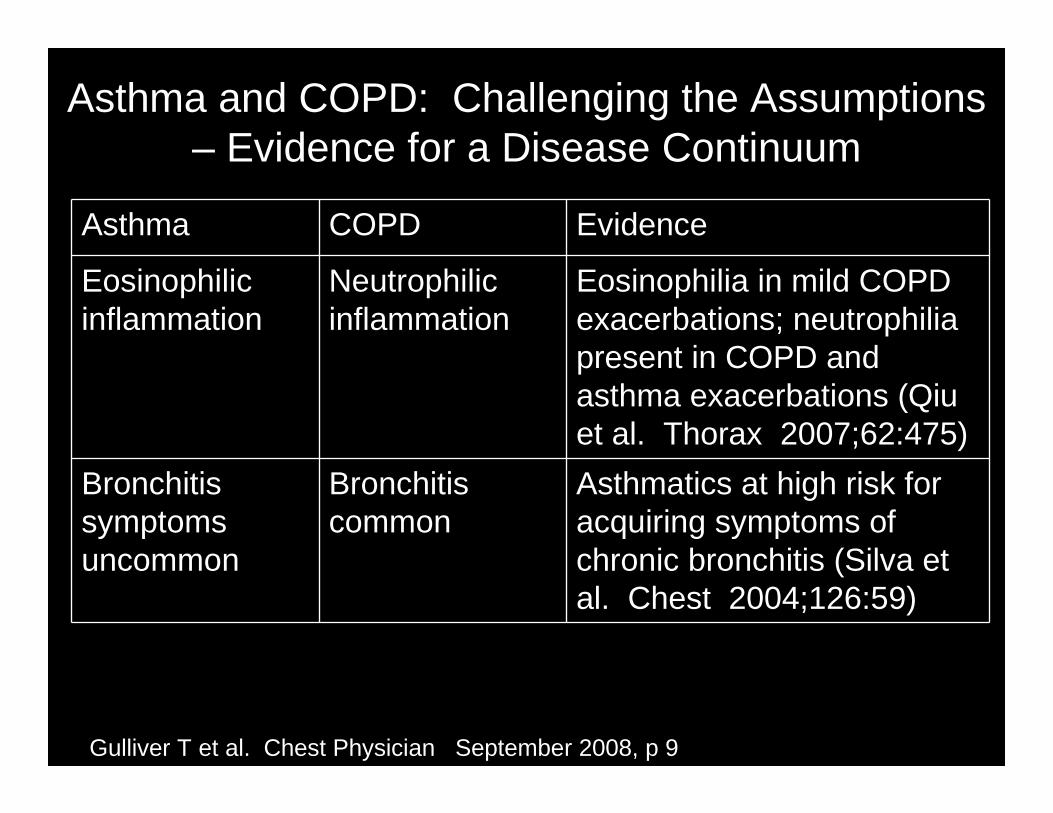
Asthma and COPD: Challenging the Assumptions – Evidence for a Disease Continuum
Asthma COPD Evidence
Eosinophilic inflammation
Neutrophilic inflammation
Eosinophilia in mild COPD exacerbations; neutrophilia present in COPD and asthma exacerbations (Qiu et al. Thorax 2007;62:475)
Bronchitis symptoms uncommon
Bronchitis common
Asthmatics at high risk for acquiring symptoms of chronic bronchitis (Silva et al. Chest 2004;126:59)
Gulliver T et al. Chest Physician September 2008, p 9
Smoking Cessation
Smoking Cessation and Asthma
• Active smoking and exposure to second-hand smoke trigger and aggravate asthma
• Studies link smoking with more frequent attacks, more severe symptoms, increased hospitalization rates, and declined lung function
Gritz ER et al. Gritz ER et al. Am J Prev Med 207;33(6S):S414Am J Prev Med 207;33(6S):S414--S422S422
Asthma and Infection (Vaccination)
Influenza Vaccine• An injectable trivalent, inactivated viral vaccine (TIV)
composed of seasonal H3N2, H1N1, and Influenza B• A live attenuated vaccine (LIAV) is also available• Studies show no increase in symptoms after
vaccination• Low to medium dose ICS does not affect vaccine
responsiveness– High dose ICS does decrease response to
Influenza B• Current evidence is conflicting on the effectiveness
of influenza vaccination in preventing morbidity and mortality in COPD and asthma
• Influenza vaccination is recommended in asthmatics and COPD based upon the known complications of influenza infection
CDC. MMWR: Recommendations and Reports 2009;58:1-52 (RR-8)
Streptococcus pneumoniae
• The risk of pneumonia is 11% to 17% in two studies of asthma.
• The Advisory Committee on Immunization Practices (ACIP) recommends all adults with asthma(19-64 yrs) receive the vaccine for S. pneumoniae (PPV-23).
--Talbot T et al. Talbot T et al. N Engl J Med N Engl J Med 2005;352:20822005;352:2082--9090--Juhn YJ et al. Juhn YJ et al. J Allergy Clin Immunol J Allergy Clin Immunol 2008;122:7192008;122:719--2323--Jung J et al. Jung J et al. J Allergy Clin Immunol J Allergy Clin Immunol 2010;125;2172010;125;217--2121
Pertussis
• 5,000-7,000 cases occur each year in the U.S. • Adults can serve as a reservoir for infection of
children due to waning immunity• Infection with B. pertussis can lead to
exacerbations of both asthma and COPD• A combination vaccine of tetanus, diphtheria,
and pertussis [Adacel (TdaP)] is recommended in these patients as a single dose vaccination for adults age 19-64– Vaccination has been shown to reduce the number of
cases by 44%
CDC. CDC. MMWR: Recommendations and Reports 1997;46:1-25(RR-7)CDC. MMWR: Recommendations and Reports 2006;55:1-37 (RR-17)
Herpes Zoster• Reactivation of Varicella Zoster leads to
significant morbidity in aging adults, and patients on high dose inhalational or oral steroids (>20mg/day prednisone) may be at higher risk.
• Zostavax has been shown to reduce the incidence of herpes zoster reactivation by 51.3% and post-herpetic neuralgia by 66.5%.
• Recommended for all adults (60 and older) as a single dose. Also recommended for all asthmatics and patients with COPD, 60 years and older if on >20mg/day of prednisone (or equivalent glucocorticosteroid).
CDC. MMWR: Recommendations and Reports 2008;57:1-30 (RR-5)
Bronchiectasis and Cystic Fibrosis
Bronchiectasis and Cystic Fibrosis
1. Bronchiectasis can be associated asthma, especially severe asthma. High resolution CT (HRCT) scans of severe asthmatics indicate bronchiectasis present in 40%.Many children with bronchiectasis confirmed by HRCT have asthma; spirometry does not necessarily correlate with the severity of symptoms.
-Gupta S et al. Chest 2009;136:152-Santamaria F et al. Chest 2006;130:480
Bronchiectasis and Cystic Fibrosis
2. Allergic bronchopulmonary aspergillosis has been estimated to occur in 1 to 2% of patients with chronic asthma and 1 to 50% of patients with cystic fibrosis.
3. Patients with cystic fibrosis can also have asthma which responds to asthma therapy.
-Vlahakis NE et al. Mayo Clin Proc 2001;76:930-Stevens DA et al. Clin Infect Dis 2003;37(suppl 3):s225
Asthma in Cystic Fibrosis
• Epidemiologic study of cystic fibrosis 1995
• 3,976 of 12,622 CF children and adults or 31% were receiving asthma treatment
Balfour-Lynn IM. J R Soc Med 2003;96(Suppl 43):30-34
Treat Co-Morbid Conditions and Reduce Asthma Morbidity and Mortality
1. How goes the nose, so goes the chest; Rx nasal disease, especially polyps
2. GERD in and of itself can be a severe and life-threatening as well as decrease quality of life. GERD can exacerbate asthma and asthma can exacerbate GERD. Rx appropriately.
3. Treat VCD or concomitant VCD.4. Overweight subjects refer to Weight
Watchers; encourage weight reduction.

Treat Co-Morbid Conditions and Reduce Asthma Morbidity and Mortality
5. Give calcium and vitamin D and encourage exercise for all patients. Look for and, where appropriate, decrease risk factors.
6. Psychiatric care, as necessary, as with any other disease.
7. Suspect, diagnose, and treat sleep apnea.
8. Give 24 hour access to all patients with asthma, particularly pregnant subjects.
Treat Co-Morbid Conditions and Reduce Asthma Morbidity and Mortality
9. Asthma and COPD can become the same disease.
10. Assist in smoking cessation.11. Bronchiectasis must be suspected in
severe asthma. So too, should other diseases such as ABPA, CF, etc.
Know when to refer for help, especially with co-morbid conditions.
Conclusions• Asthma is perhaps the most treatable of all
chronic diseases.It should be treated continuously to prevent symptoms and exacerbations.
• For optimal outcomes, co-morbid conditions must be identified and treated.
• Co-morbid conditions and their diagnosis and treatment should be included in asthma guidelines
Thank you!

Risk Factors for Fatal Asthma>> Asthma history
- Previous severe exacerbation (e.g., intubation or intensive care unit (ICU) admission for asthma)- Two or more asthma hospitalizations for asthma in the past year - Three or more emergency department (ED) visits for asthma in the past year- Hospitalization or ED visit for asthma in the past month
-Adapted from NIH/NHLBI National Asthma Education and Prevention Program. Expert Panel Report 3: guidelines for the diagnosis and management of asthma: Clinical practice guidelines. Bethesda (MD): 2007-Guilbert T et al. In Middleton 7th ed. Allergy: Principles and Practice, 2009, p 1323
Risk Factors for Fatal Asthma>> Asthma history
- Use of > 2 canisters per month of short-acting bronchodilators (SABA)- Difficulty perceiving asthma symptoms or severity of exacerbations- Other risk factors: lack of a written asthma action plan, sensitivity to Alternaria
-Adapted from NIH/NHLBI National Asthma Education and Prevention Program. Expert Panel Report 3: guidelines for the diagnosis and management of asthma: Clinical practice guidelines. Bethesda (MD): 2007-Guilbert T et al. In Middleton 7th ed. Allergy: Principles and Practice, 2009, p 1323
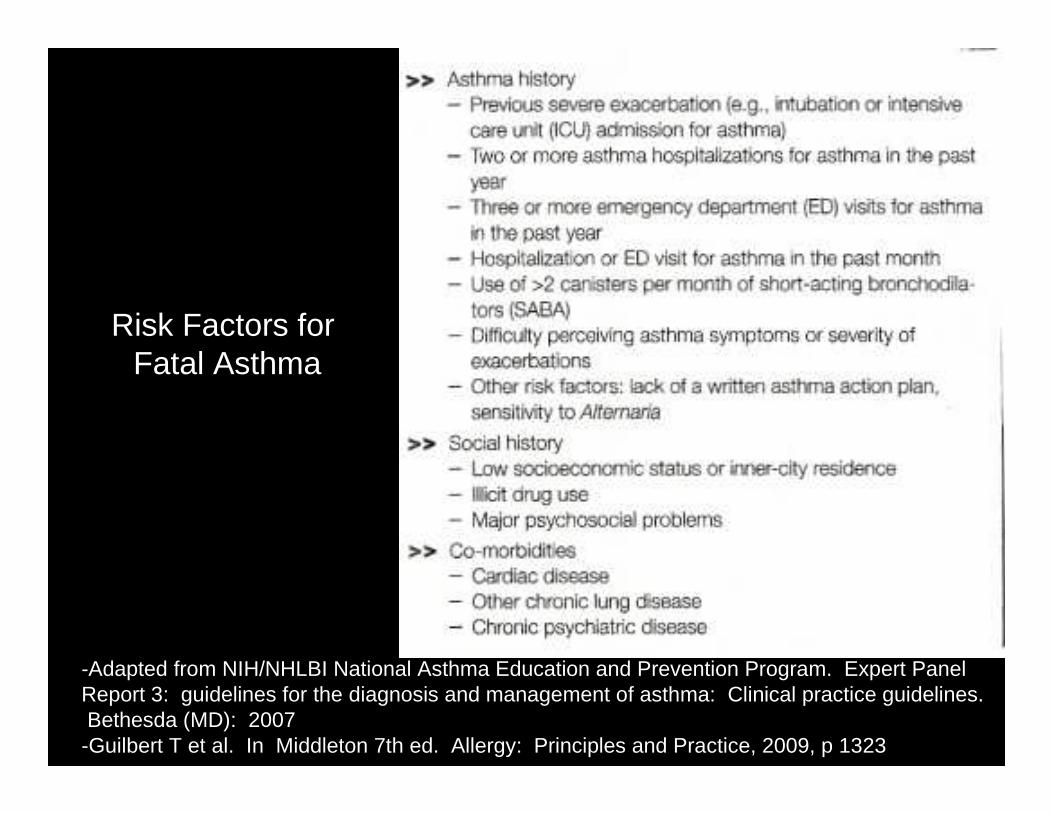
-Adapted from NIH/NHLBI National Asthma Education and Prevention Program. Expert Panel Report 3: guidelines for the diagnosis and management of asthma: Clinical practice guidelines. Bethesda (MD): 2007-Guilbert T et al. In Middleton 7th ed. Allergy: Principles and Practice, 2009, p 1323
Risk Factors for Fatal Asthma
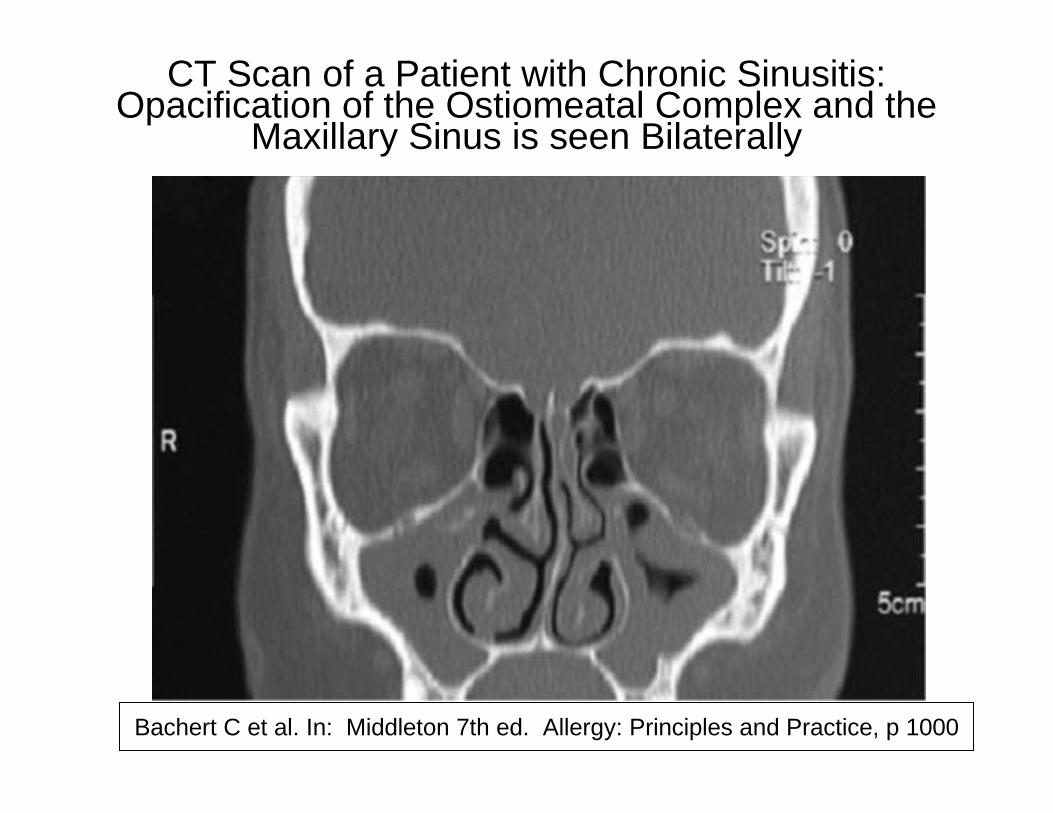
CT Scan of a Patient with Chronic Sinusitis: Opacification of the Ostiomeatal Complex and the
Maxillary Sinus is seen Bilaterally
Bachert C et al. In: Middleton 7th ed. Allergy: Principles and Practice, p 1000
Mass Psychogenic Illness Presenting as Acute Stridor in an Adolescent Female Cohort
• 14 subjects, 12 evaluated, all with inspiratory stridor over 10 months
• 14 to 18 yrs (9th to 12th grade)• School dance team• Polyurethane and paint temporally
involved in some but sentinel case presented before exposure
Powell SA, Nguyen CT, Gaziano J, Lewis V, Lockey RF, Padhya TA. Ann Otol Rhinol Laryngol 2007;116:525-531
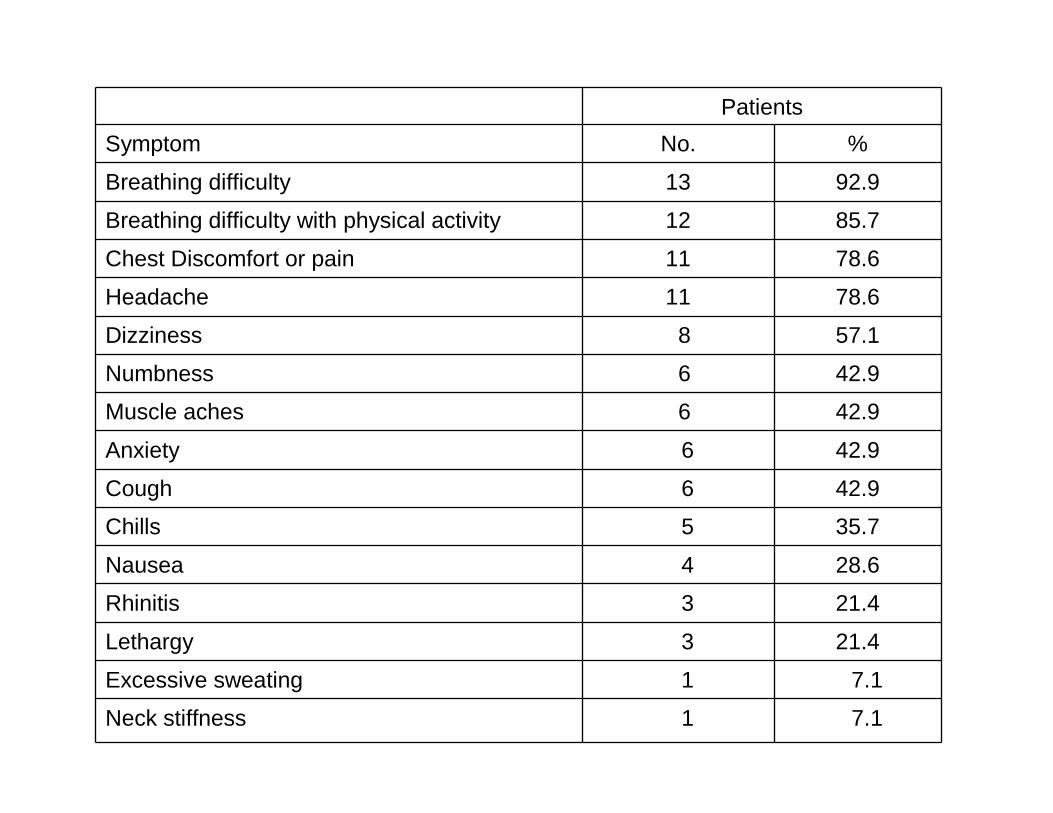
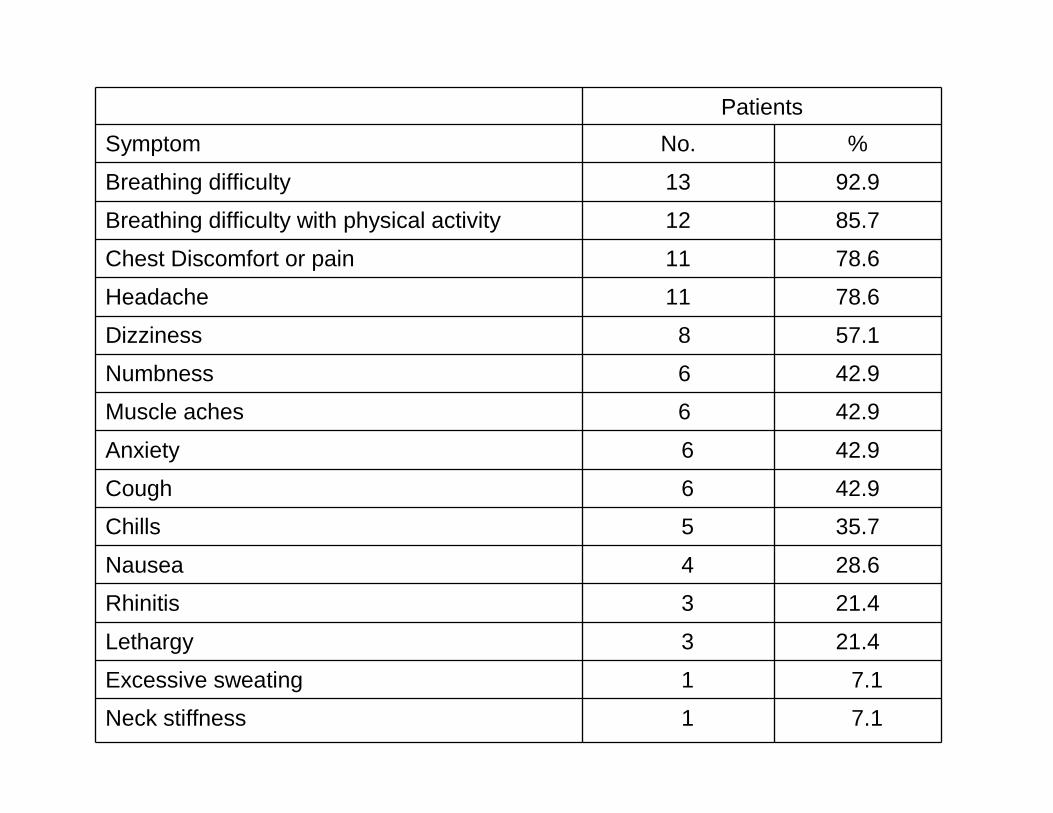
Breakdown of Additional Symptoms EncounteredPatients
Symptom No. %
Breathing difficulty 13 92.9
Breathing difficulty with physical activity 12 85.7
Chest Discomfort or pain 11 78.6
Headache 11 78.6
Dizziness 8 57.1
Numbness 6 42.9
Muscle aches 6 42.9
Anxiety 6 42.9
Cough 6 42.9
Chills 5 35.7
Nausea 4 28.6
Rhinitis 3 21.4
Lethargy 3 21.4
Excessive sweating 1 7.1
Neck stiffness 1 7.1Powell SA, Nguyen CT, Gaziano J, Lewis V, Lockey RF, Padhya TA. Ann Otol Rhinol Laryngol 2007;116:525-531
Mass Psychogenic Illness Presenting as Acute Stridor in an Adolescent Female Cohort
• 14 subjects, 12 evaluated, all with inspiratory stridor over 10 months
• 14 to 18 yrs (9th to 12th grade)• School dance team• Polyurethane and paint temporally
involved in some but sentinel case presented before exposure
Powell SA, Nguyen CT, Gaziano J, Lewis V, Lockey RF, Padhya TA. Ann Otol Rhinol Laryngol 2007;116:525-531
Breakdown of Additional Symptoms EncounteredPatients
Symptom No. %
Breathing difficulty 13 92.9
Breathing difficulty with physical activity 12 85.7
Chest Discomfort or pain 11 78.6
Headache 11 78.6
Dizziness 8 57.1
Numbness 6 42.9
Muscle aches 6 42.9
Anxiety 6 42.9
Cough 6 42.9
Chills 5 35.7
Nausea 4 28.6
Rhinitis 3 21.4
Lethargy 3 21.4
Excessive sweating 1 7.1
Neck stiffness 1 7.1Powell SA, Nguyen CT, Gaziano J, Lewis V, Lockey RF, Padhya TA. Ann Otol Rhinol Laryngol 2007;116:525-531

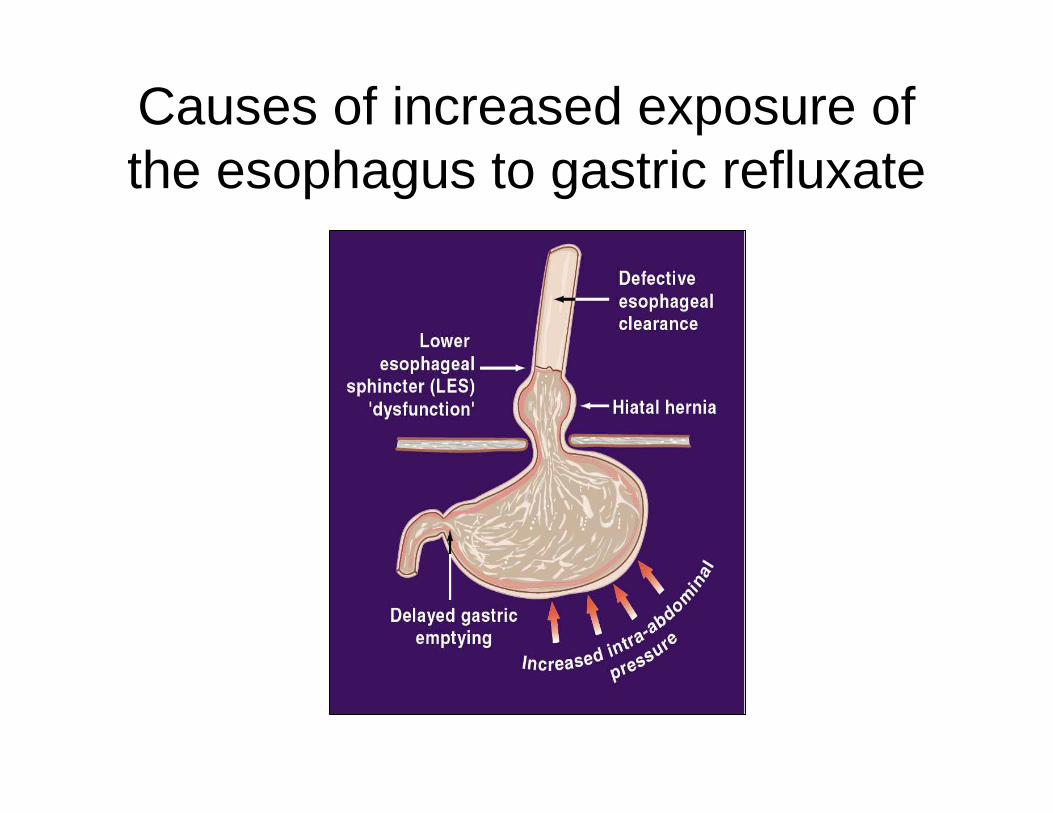
Causes of increased exposure of the esophagus to gastric refluxate
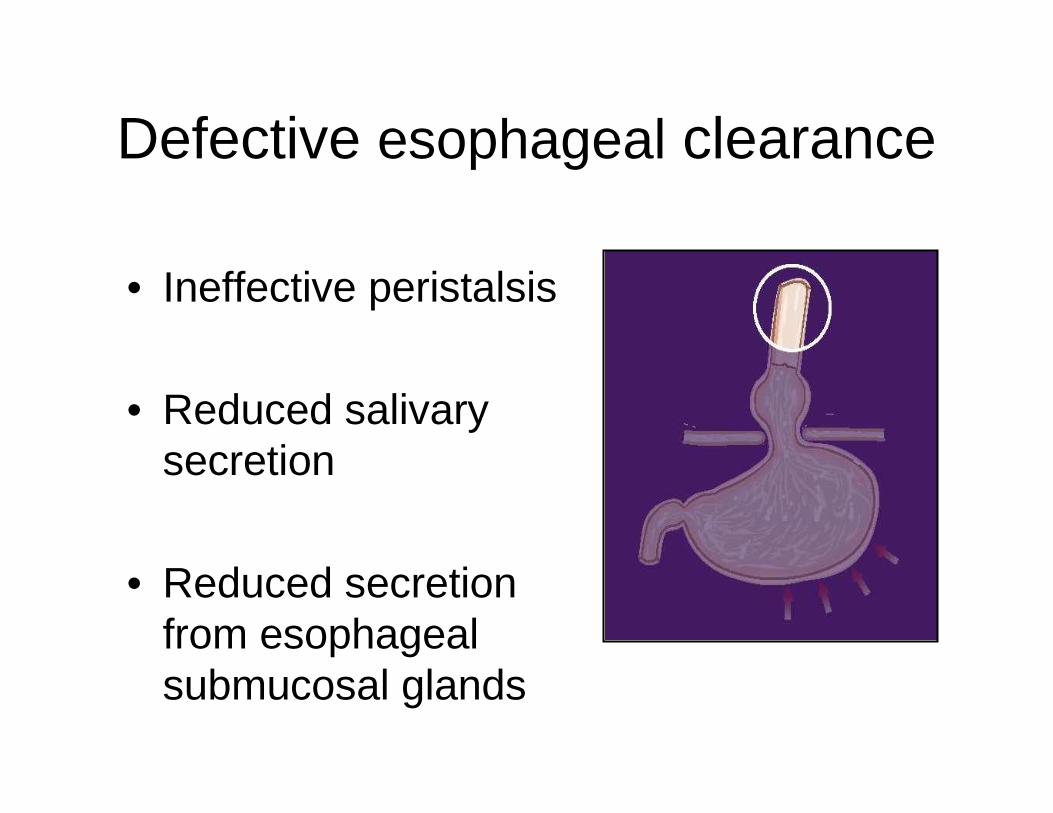
• Ineffective peristalsis
• Reduced salivary secretion
• Reduced secretion from esophageal submucosal glands
Defective esophageal clearance
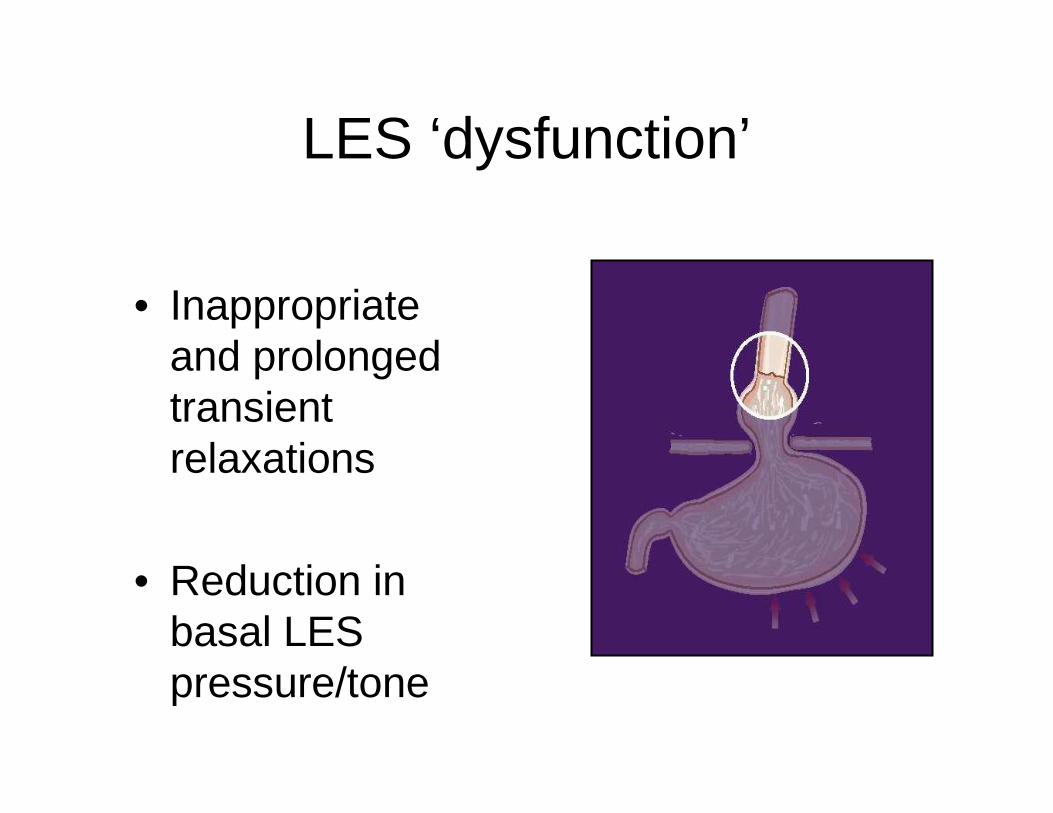
• Inappropriate and prolonged transient relaxations
• Reduction in basal LES pressure/tone
LES ‘dysfunction’
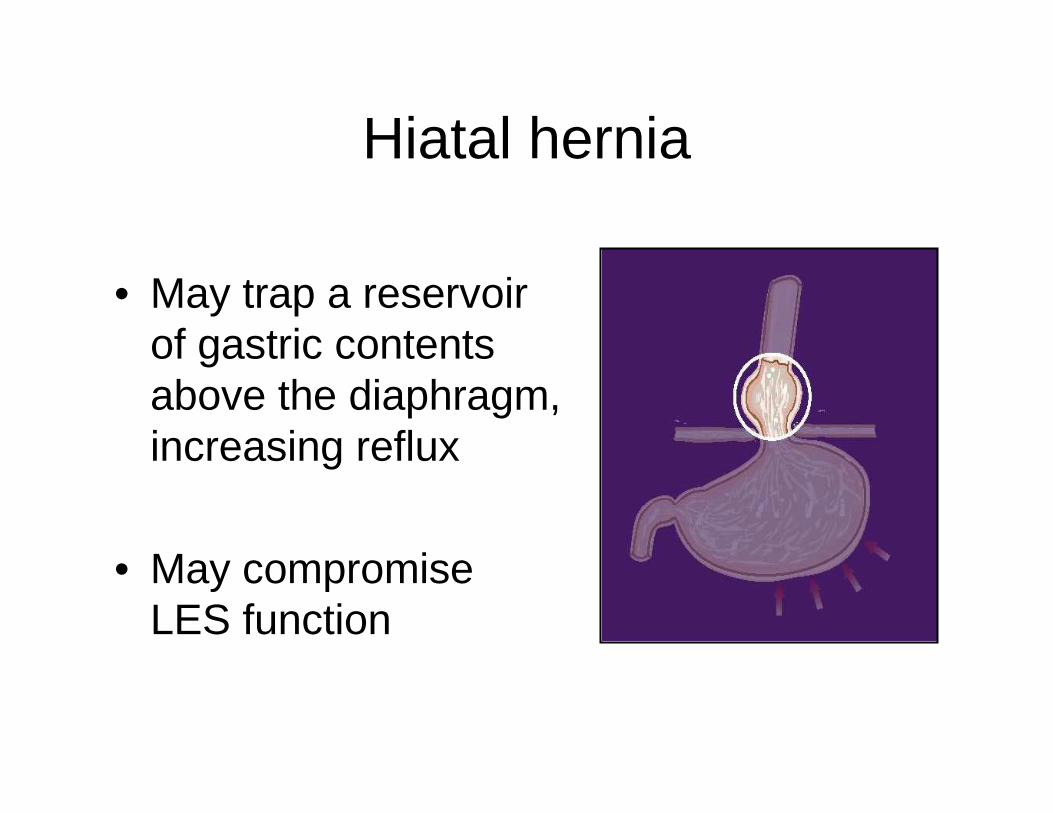
• May trap a reservoir of gastric contents above the diaphragm, increasing reflux
• May compromise LES function
Hiatal hernia
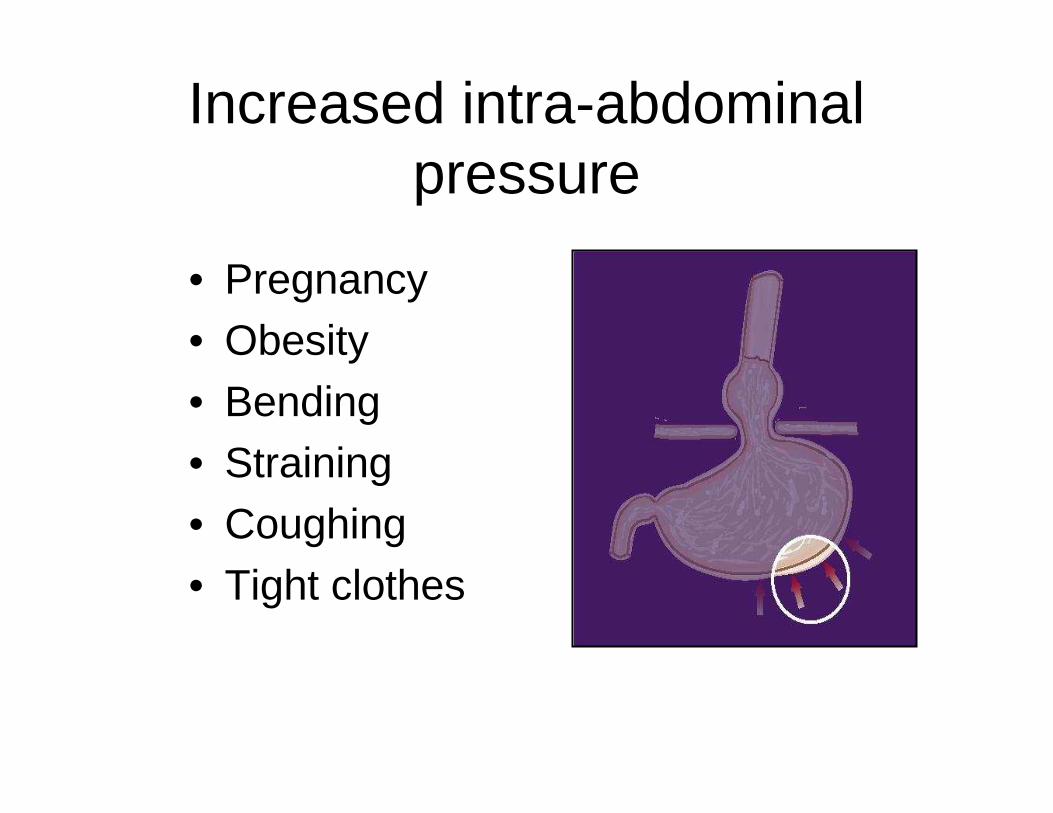
• Pregnancy• Obesity• Bending• Straining• Coughing• Tight clothes
Increased intra-abdominal pressure
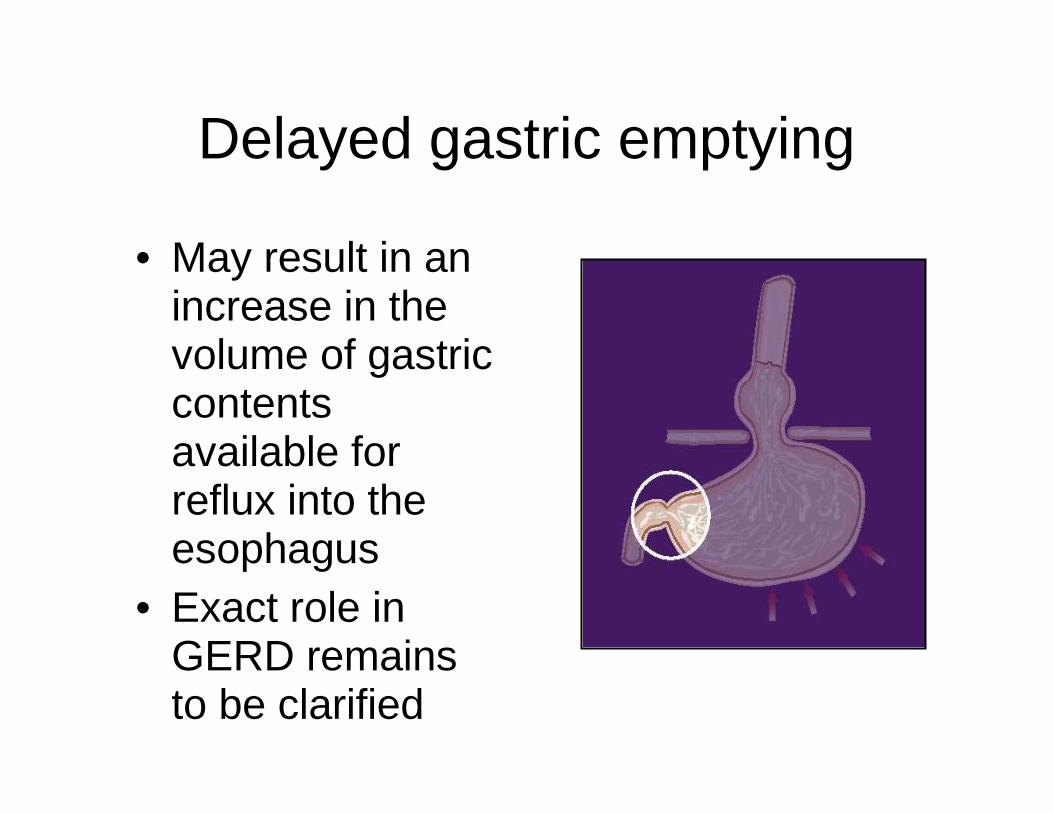
• May result in an increase in the volume of gastric contents available for reflux into the esophagus
• Exact role in GERD remains to be clarified
Delayed gastric emptying
Medications that may aggravate GERD symptoms by impairing LES
function• β-adrenergic
agonists• Theophylline• Anticholinergics• Tricyclic
antidepressants
• Progesterone
• α-adrenergic antagonists
• Diazepam• Calcium channel
blockers
Medications that may aggravate GERD symptoms by damaging the
esophageal mucosa• Tetracycline• Quinidine• Potassium chloride tablets• Iron salts• Aspirin and other NSAIDs• Bisphosphonates
Johnsson et al. Gullet 1992
Symptom patterns in GERD
• Reflux-related symptoms occur predominantly after meals
• Reflux-related symptoms are often triggered by– unusually large meals– fatty, spicy, or acidic foods– bending, stooping, or lying down– lifting, straining, or other strenuous activities
• The frequency of reflux-related symptoms varies widely
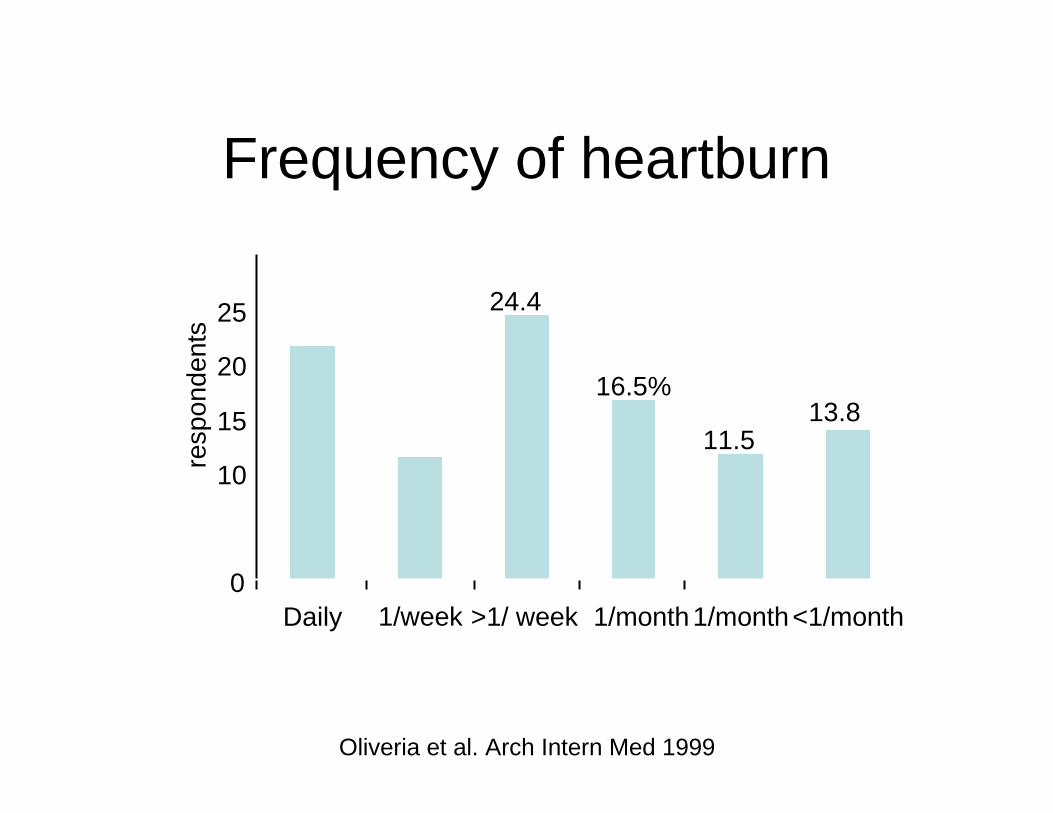
24.4%
>1/ week
Oliveria et al. Arch Intern Med 1999
0
5
10
15
20
25
30
21.5%
Daily
16.5%
>1/month
11.5%
1/month
13.8%
<1/month
Frequency of heartburn
% r
espo
nden
tsFrequency of heartburn
11.3%
1/week
• Esophageal– Barrett’s
esophagus– adenocarcinom
a
– stricture– ulceration
– bleeding
• Extra-esophageal– asthma
– reflux laryngitis– vocal cord
ulcers
– subglottic stenosis
– tracheal stenosis
Complications of GERD
Management
Medical Management of GERD• Oral antacids & alginates: minimally
effective• H2 blockers in divided doses: moderately
effective• PPIs once or twice daily: moderately to
highly effective– Some risk of bacterial overgrowth, decreased
absorption of B12, iron and calcium– Long term Rx necessary, usually 3-6 months
and often longer and often twice daily
• Prokinetic agents: questionably effective
Surgical Therapy for GERD1. Antireflux surgery, performed by an
experienced surgeon, is a maintenance
option for patients with documented GERD.a. Two published studies show
surgery more effective than medical
therapy. (One study compared antacids and lifestyle changes over 36-months. Second study compared surgery
versus
Surgical Therapy for GERD1. Antireflux surgery, performed by an
experienced surgeon, is a maintenance option for patients with documented GERD.b. Randomized trial 310 patients
initially controlled with omeprazole40 mg per day found surgery to be slightly superior (maintenance of esophagitis healing and symptoms) to omeprazole 20 mg per day at the end of 3 yr period.
Lundell L et al. Gastroenterology 1998;114:A207
Surgical Therapy for GERD1. Antireflux surgery, performed by an
experienced surgeon, is a maintenance
option for patients with documented GERD.c. If dose is titrated to 40-60 mg
perday of omeprazole medical and surgical treatments equal.
Additional Studies NeededThe American Lung Association Asthma Clinical Research Centers study entitled “Efficacy of Esomeprazole for Treatment of Poorly Controlled Asthma: A Randomized Controlled Trial” is under consideration for submission for publication. The Division at the University of South Florida is one of the 19 research centers for the study.
Snoring in Primary School Children
• Validated questionnaire completed by parents to assess sleep and day-time behaviors of Chinese children, 5-14 yrs
Li AM, et al. Chest 2010;138(3):519-527
• 6,349 / 9,172 questionnaires returned
• Habitual snoring (HS) 7.2%
• Male OR 2.5 (1.7-3.6), BMI z score OR 1.4 (1.1-1.6), maternal HS OR 3.4 (2.0-5.7), paternal HS OR 3.8 (2.7-5.5), allergic rhinitis OR 2.9 (2.0-4.2), asthma OR 2.4 (1.2-5.2), nasosinusitis OR 4.0 (1.5-10.6), tonsillitis OR 3.1 (1.9-5.1) in past 12 months independent risk factors associated with HS
Li AM, et al. Chest 2010;138(3):519-527
Results
Results (cont’d)
• HS associated with daytime, nocturnal, parasomniac, and sleep-related breathing symptoms
• Independent risk factor for parent-reported poor temper 1.9 (1.4-2.5), hyperactivity 1.7 (1.2-2.5), and poor school performance 1.7 (1.2-2.5)
Li AM, et al. Chest 2010;138(3):519-527
Do Inhaled Steroids Increase the Risk of Osteoporosis?
• Evidence-based answer:1) Conventional doses for asthma are not
associated with significant bone loss at 2 to 3 years follow-up (strength of recommendation: A
2) Higher doses may be associated with negative bone density changes in up to 4 years: C
3) Evidence lacking on whether nasal steroids increase risk.
4) Longer-term studies are necessaryGerayli F, Loven B. Gerayli F, Loven B. J Fam PractJ Fam Pract 2007;56:1312007;56:131--136136
Recommendations
• Encourage weight-bearing and aerobic exercise to all patients with asthma
Gerayli F, Loven B. J Fam Pract 2007;56:131-136
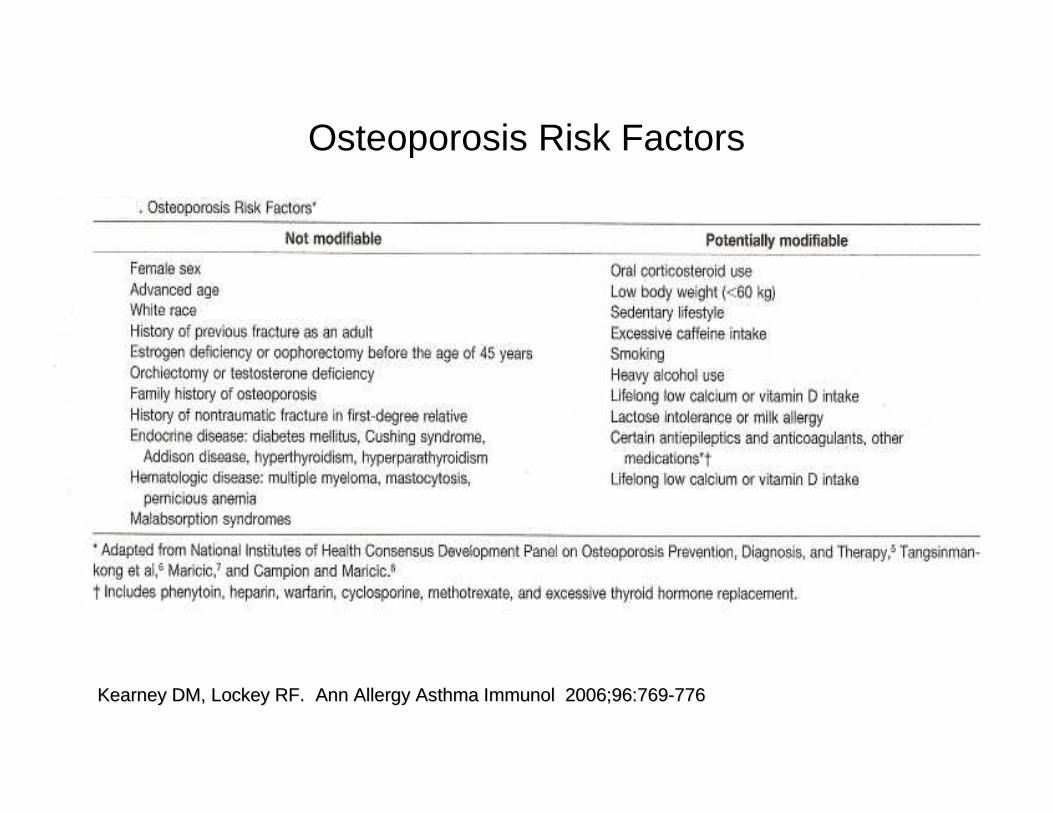
Osteoporosis Risk Factors
Kearney DM, Lockey RF. Kearney DM, Lockey RF. Ann Allergy Asthma ImmunolAnn Allergy Asthma Immunol 2006;96:7692006;96:769--776776
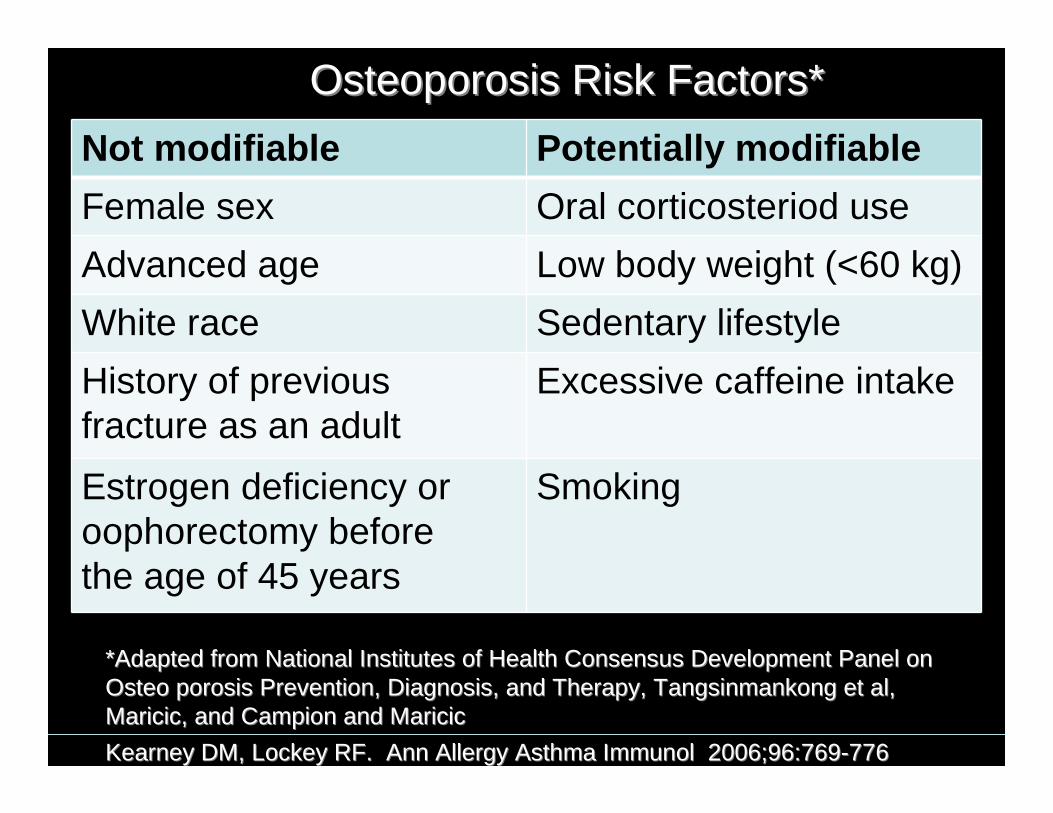
Not modifiable Potentially modifiable
Female sex Oral corticosteriod use
Advanced age Low body weight (<60 kg)
White race Sedentary lifestyle
History of previous fracture as an adult
Excessive caffeine intake
Estrogen deficiency or oophorectomy before the age of 45 years
Smoking
Osteoporosis Risk Factors*Osteoporosis Risk Factors*
Kearney DM, Lockey RF. Kearney DM, Lockey RF. Ann Allergy Asthma ImmunolAnn Allergy Asthma Immunol 2006;96:7692006;96:769--776776
*Adapted from National Institutes of Health Consensus Developmen*Adapted from National Institutes of Health Consensus Development Panel on t Panel on Osteo porosis Prevention, Diagnosis, and Therapy, TangsinmankongOsteo porosis Prevention, Diagnosis, and Therapy, Tangsinmankong et al, et al, Maricic, and Campion and MaricicMaricic, and Campion and Maricic
Not modifiable Potentially modifiable
Orchiectomy or testosterone deficiency
Heavy alcohol use
Family history of osteoporosis Lifelong low calcium or vitamin D intake
History of nontraumatic fracture in first-degree relative
Lactose intolerance or milk allergy
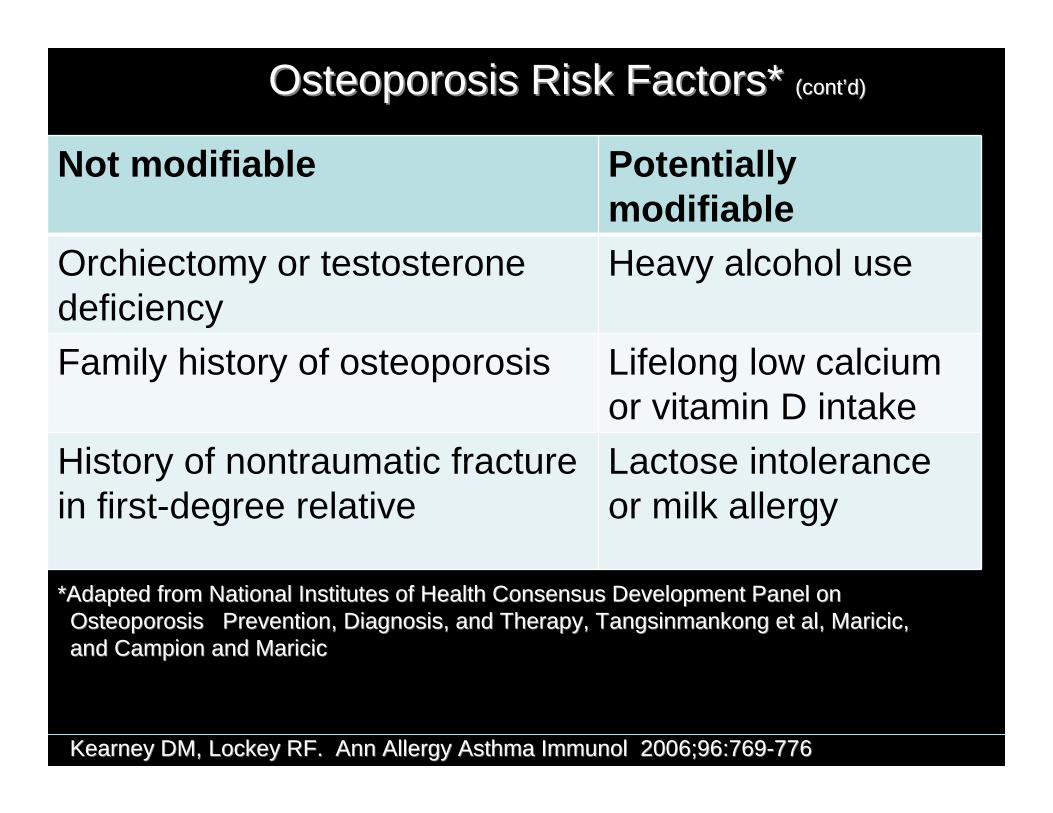
Osteoporosis Risk Factors* Osteoporosis Risk Factors* (cont(cont’’d)d)
*Adapted from National Institutes of Health Consensus Developmen*Adapted from National Institutes of Health Consensus Development Panel on t Panel on Osteoporosis Prevention, Diagnosis, and Therapy, TangsinmankOsteoporosis Prevention, Diagnosis, and Therapy, Tangsinmankong et al, Maricic, ong et al, Maricic, and Campion and Maricicand Campion and Maricic
Kearney DM, Lockey RF. Kearney DM, Lockey RF. Ann Allergy Asthma ImmunolAnn Allergy Asthma Immunol 2006;96:7692006;96:769--776776
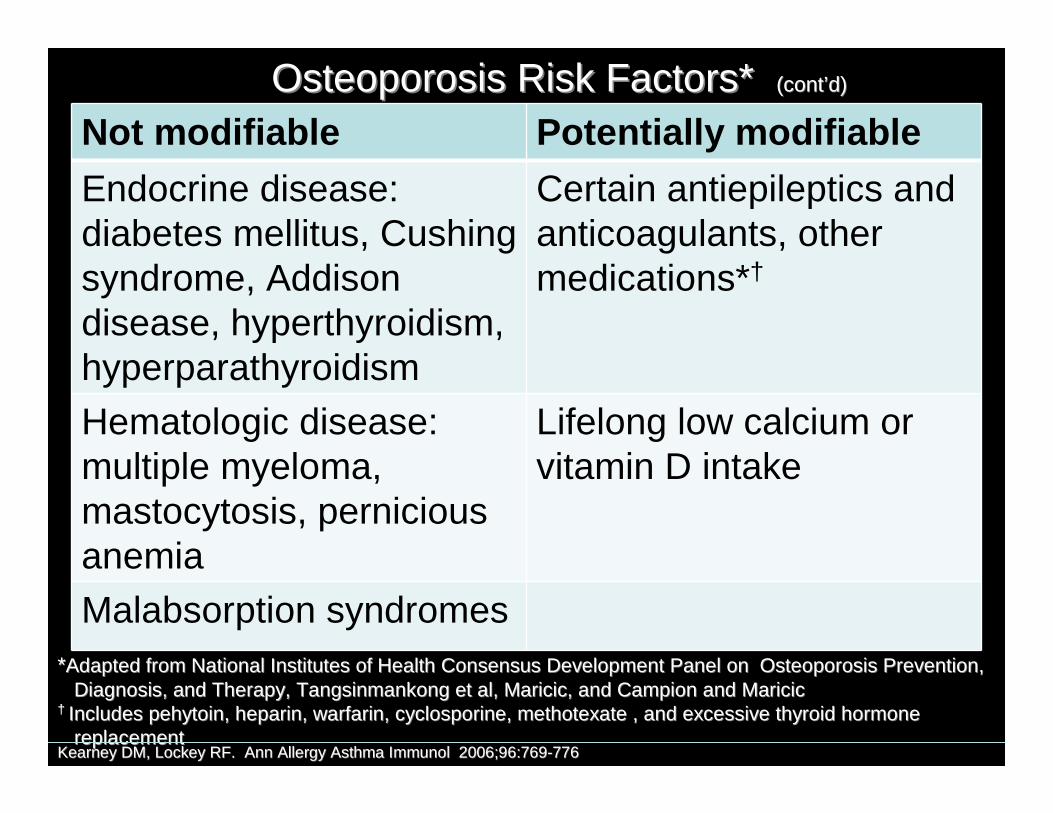
Not modifiable Potentially modifiable
Endocrine disease: diabetes mellitus, Cushing syndrome, Addison disease, hyperthyroidism, hyperparathyroidism
Certain antiepileptics and anticoagulants, other medications*†
Hematologic disease: multiple myeloma, mastocytosis, pernicious anemia
Lifelong low calcium or vitamin D intake
Malabsorption syndromes
Osteoporosis Risk Factors* Osteoporosis Risk Factors* (cont(cont’’d)d)
**Adapted from National Institutes of Health Consensus DevelopmentAdapted from National Institutes of Health Consensus Development Panel on Osteoporosis Prevention,Panel on Osteoporosis Prevention,Diagnosis, and Therapy, Tangsinmankong et al, Maricic, and CaDiagnosis, and Therapy, Tangsinmankong et al, Maricic, and Campion and Maricicmpion and Maricic
†† Includes pehytoin, heparin, warfarin, cyclosporine, methotexate Includes pehytoin, heparin, warfarin, cyclosporine, methotexate , and excessive thyroid hormone , and excessive thyroid hormone replacementreplacement
Kearney DM, Lockey RF. Kearney DM, Lockey RF. Ann Allergy Asthma ImmunolAnn Allergy Asthma Immunol 2006;96:7692006;96:769--776776
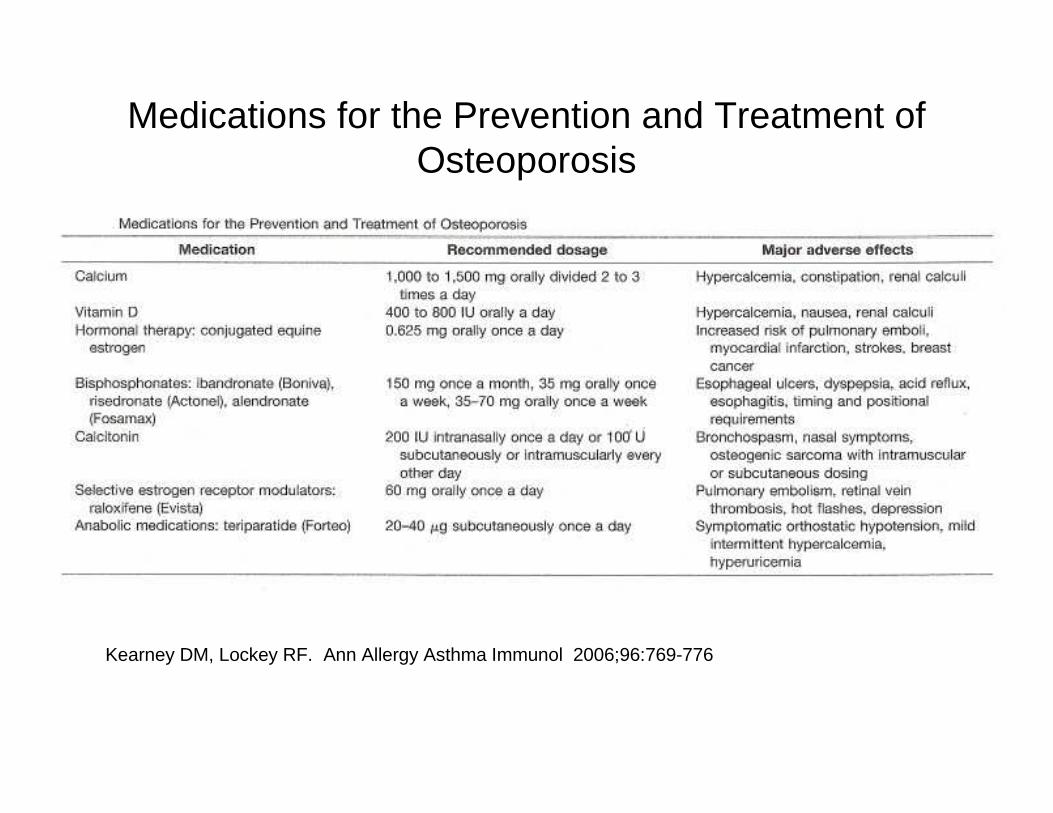
Medications for the Prevention and Treatment of Osteoporosis
Kearney DM, Lockey RF. Ann Allergy Asthma Immunol 2006;96:769-776
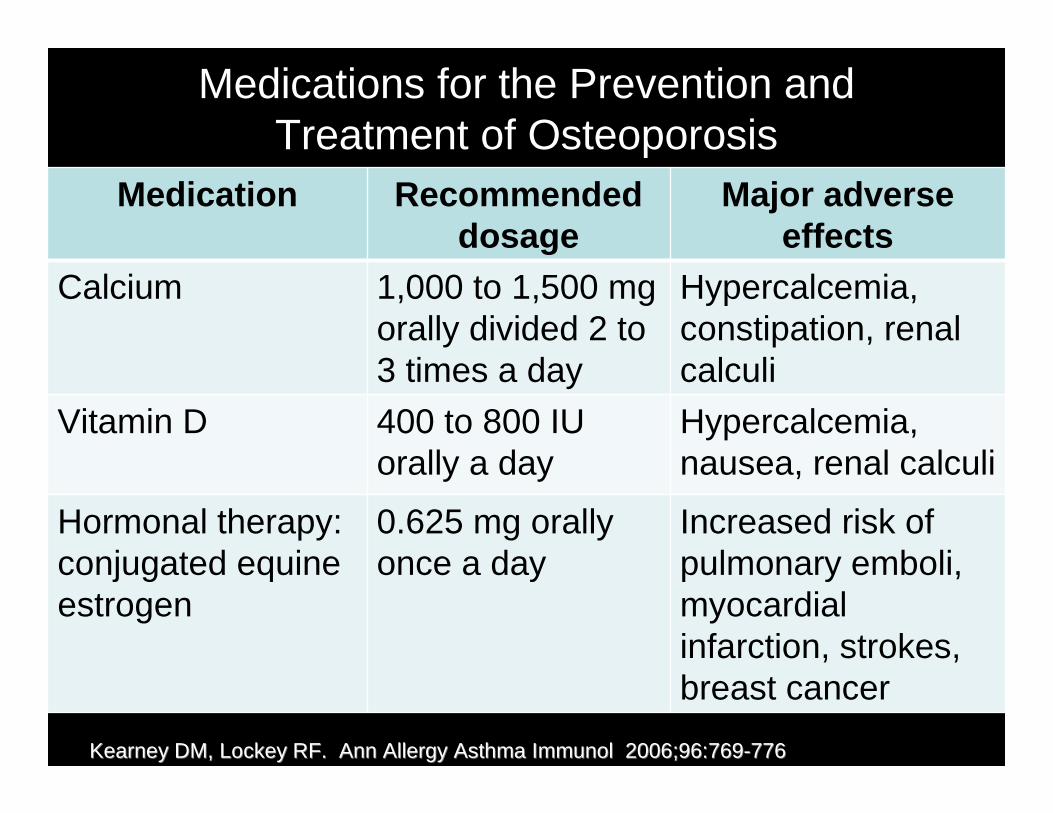
Medications for the Prevention and Treatment of Osteoporosis
Medication Recommended dosage
Major adverse effects
Calcium 1,000 to 1,500 mg orally divided 2 to 3 times a day
Hypercalcemia, constipation, renal calculi
Vitamin D 400 to 800 IU orally a day
Hypercalcemia, nausea, renal calculi
Hormonal therapy: conjugated equine estrogen
0.625 mg orally once a day
Increased risk of pulmonary emboli, myocardial infarction, strokes, breast cancer
Kearney DM, Lockey RF. Kearney DM, Lockey RF. Ann Allergy Asthma ImmunolAnn Allergy Asthma Immunol 2006;96:7692006;96:769--776776
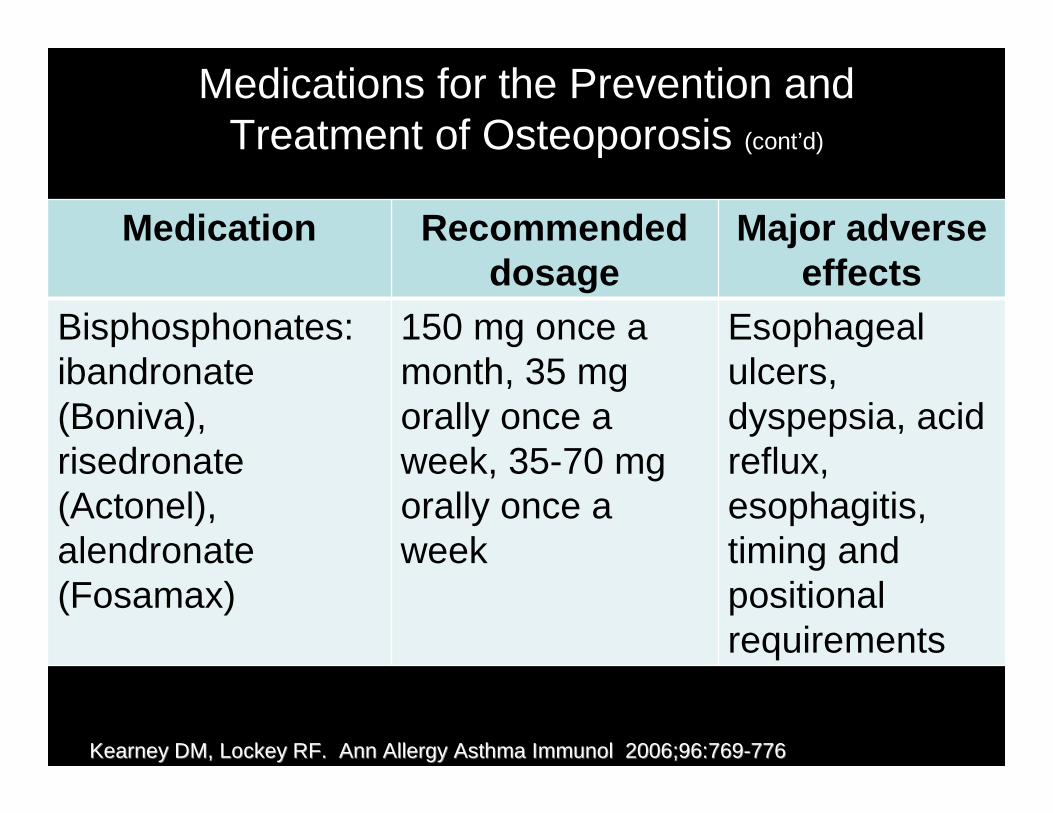
Medications for the Prevention and Treatment of Osteoporosis (cont’d)
Medication Recommended dosage
Major adverse effects
Bisphosphonates: ibandronate (Boniva), risedronate (Actonel), alendronate (Fosamax)
150 mg once a month, 35 mg orally once a week, 35-70 mg orally once a week
Esophageal ulcers, dyspepsia, acid reflux, esophagitis, timing and positional requirements
Kearney DM, Lockey RF. Kearney DM, Lockey RF. Ann Allergy Asthma ImmunolAnn Allergy Asthma Immunol 2006;96:7692006;96:769--776776
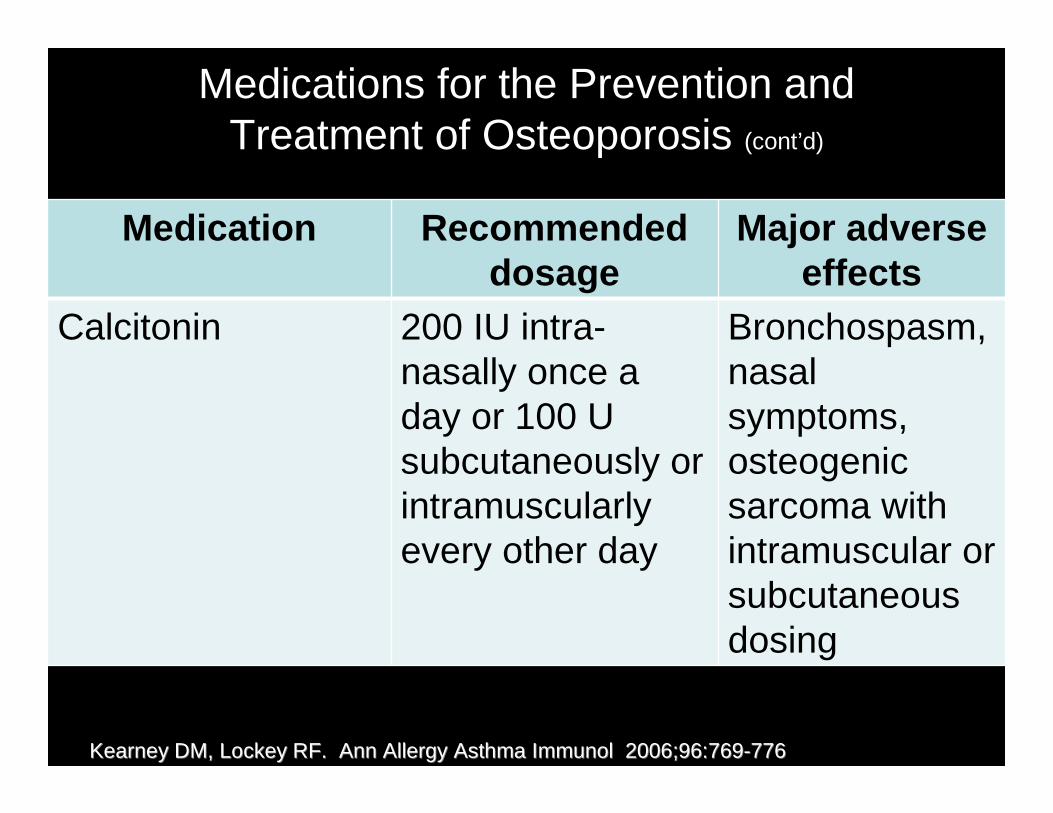
Medications for the Prevention and Treatment of Osteoporosis (cont’d)
Medication Recommended dosage
Major adverse effects
Calcitonin 200 IU intra-nasally once a day or 100 U subcutaneously or intramuscularly every other day
Bronchospasm, nasal symptoms, osteogenic sarcoma with intramuscular or subcutaneous dosing
Kearney DM, Lockey RF. Kearney DM, Lockey RF. Ann Allergy Asthma ImmunolAnn Allergy Asthma Immunol 2006;96:7692006;96:769--776776
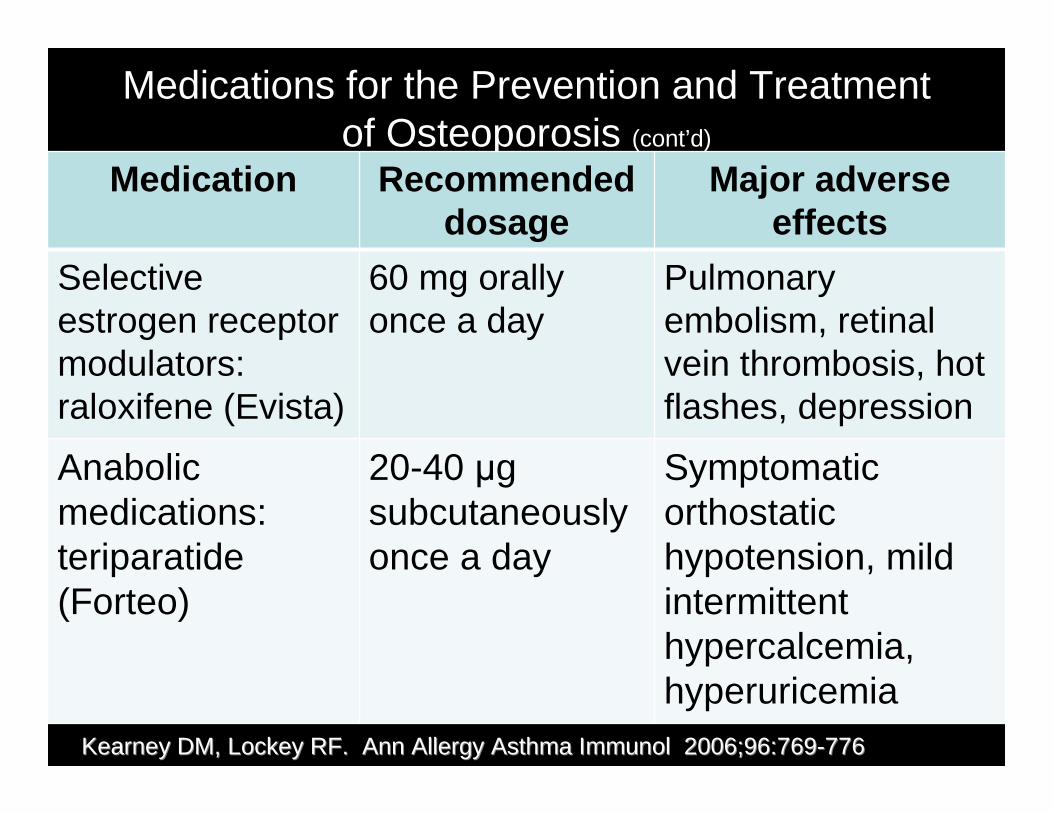
Medications for the Prevention and Treatment of Osteoporosis (cont’d)
Medication Recommended dosage
Major adverse effects
Selective estrogen receptor modulators: raloxifene (Evista)
60 mg orally once a day
Pulmonary embolism, retinal vein thrombosis, hot flashes, depression
Anabolic medications: teriparatide (Forteo)
20-40 µg subcutaneously once a day
Symptomatic orthostatic hypotension, mild intermittent hypercalcemia, hyperuricemia
Kearney DM, Lockey RF. Kearney DM, Lockey RF. Ann Allergy Asthma ImmunolAnn Allergy Asthma Immunol 2006;96:7692006;96:769--776776
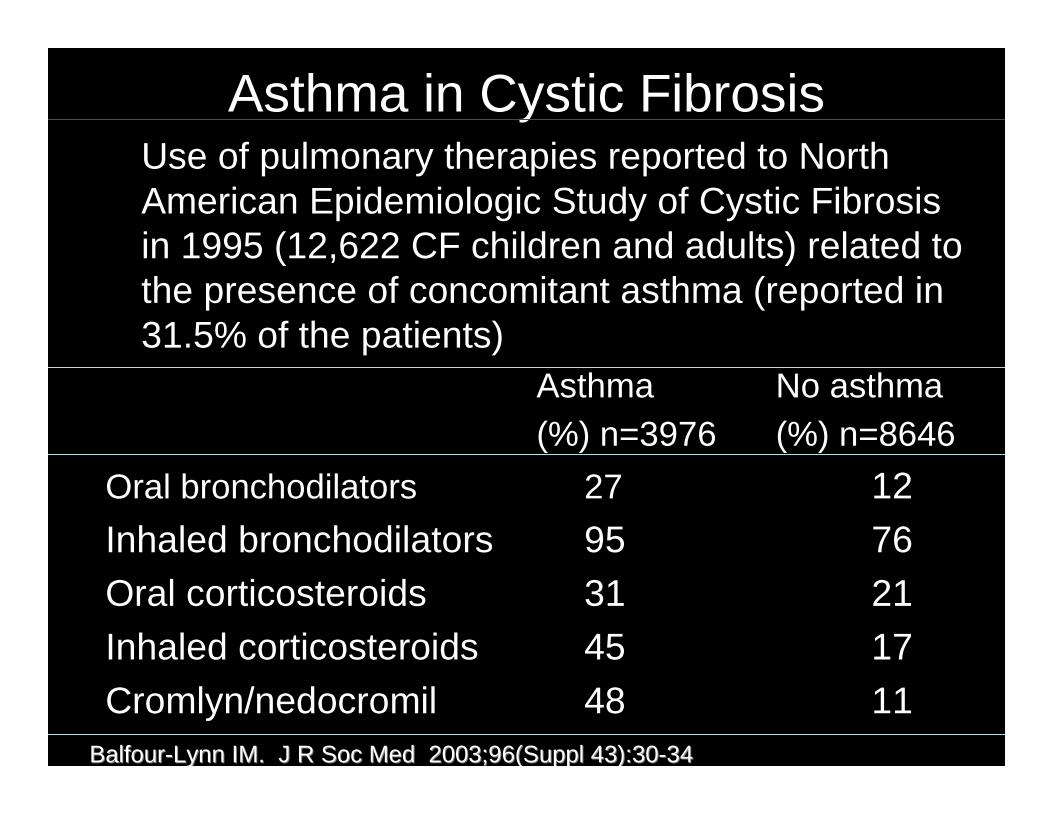
Asthma in Cystic FibrosisUse of pulmonary therapies reported to North American Epidemiologic Study of Cystic Fibrosis in 1995 (12,622 CF children and adults) related to the presence of concomitant asthma (reported in 31.5% of the patients)
Asthma No asthma(%) n=3976 (%) n=8646
Oral bronchodilators 27 12
Inhaled bronchodilators 95 76Oral corticosteroids 31 21Inhaled corticosteroids 45 17
Cromlyn/nedocromil 48 11BalfourBalfour--Lynn IM. Lynn IM. J R Soc MedJ R Soc Med 2003;96(Suppl 43):302003;96(Suppl 43):30--3434
Factors that Support Diagnosis of Cystic Fibrosis Asthma
• History of recurrent wheezing• Positive family history atopy in first degree
relative• Patient has history of atopy (eczema, hay
fever, food allergy)• Positive skin prick tests or serum
radioallergosorbent tests to aeroallergens (excluding Aspergillus)
BalfourBalfour--Lynn IM. Lynn IM. J R Soc MedJ R Soc Med 2003;96(Suppl 43):302003;96(Suppl 43):30--3434
Factors that Support Diagnosis of Cystic Fibrosis Asthma (cont’d)
• High serum IgE (excluding ABPA)• Physiology supportive (spirometry,
bronchodilator responsiveness, BHR)• Other diagnoses excluded (gastro-
oesophageal reflux, malacic airways, ABPA obliterative bronchiolitis)
• Response to anti-asthma medication
BalfourBalfour--Lynn IM. Lynn IM. J R Soc MedJ R Soc Med 2003;96(Suppl 43):302003;96(Suppl 43):30--3434
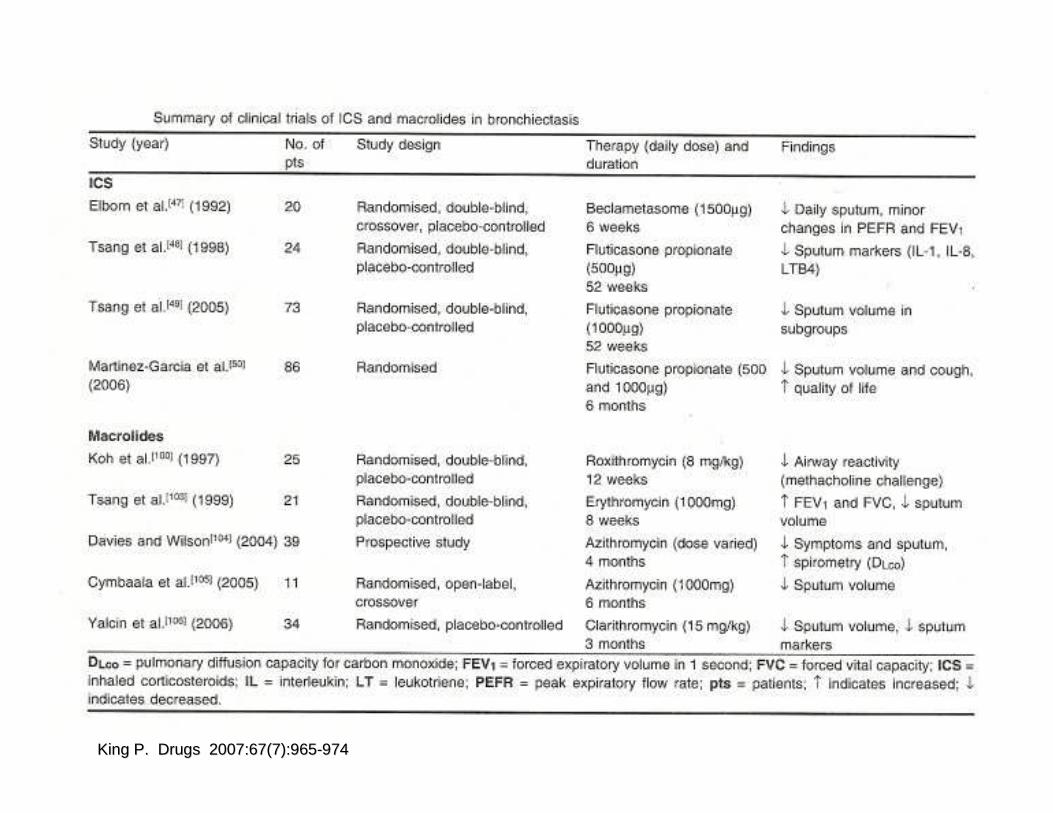
King P. King P. DrugsDrugs 2007:67(7):9652007:67(7):965--974974
Study (year) No. of pts
Study design Therapy (daily dose) and duration
Findings
ICS
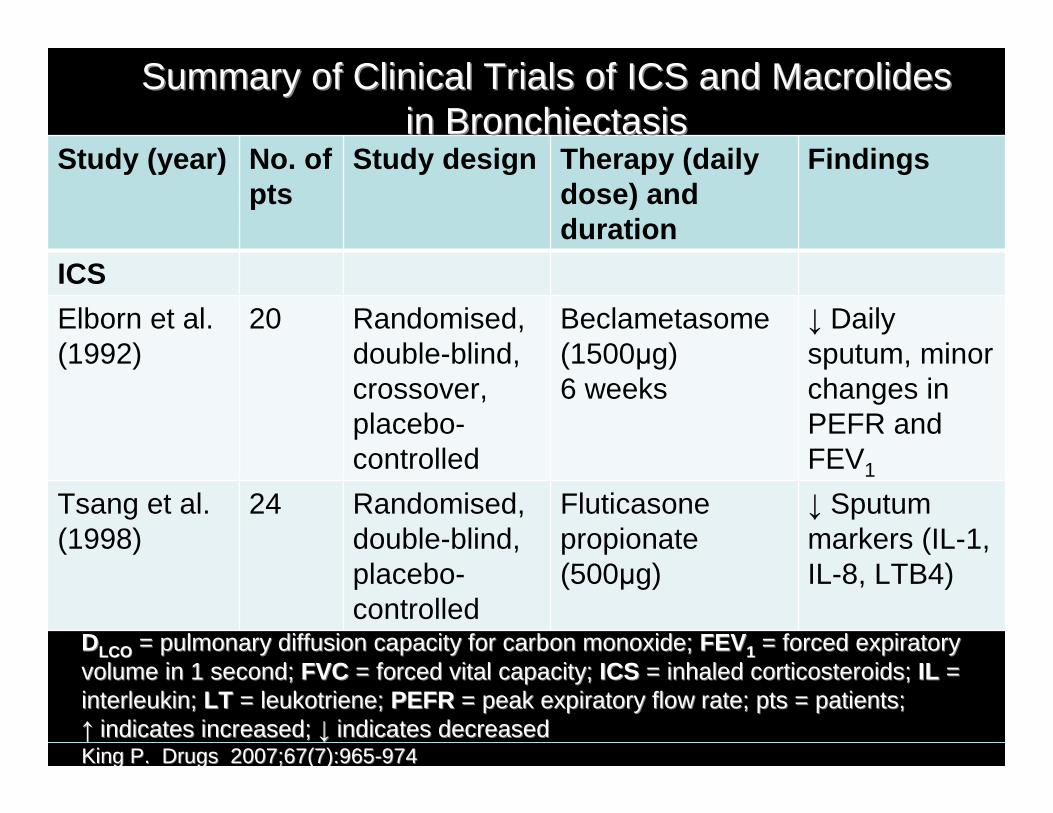
Elborn et al. (1992)
20 Randomised, double-blind, crossover, placebo-controlled
Beclametasome (1500µg) 6 weeks
↓ Daily sputum, minor changes in PEFR and FEV1
Tsang et al.(1998)
24 Randomised, double-blind, placebo-controlled
Fluticasone propionate (500µg)
↓ Sputum markers (IL-1, IL-8, LTB4)
Summary of Clinical Trials of ICS and Macrolides Summary of Clinical Trials of ICS and Macrolides in Bronchiectasisin Bronchiectasis
DDLCOLCO = pulmonary diffusion capacity for carbon monoxide;= pulmonary diffusion capacity for carbon monoxide; FEVFEV11 = forced expiratory = forced expiratory volume in 1 second; volume in 1 second; FVCFVC = forced vital capacity; = forced vital capacity; ICSICS = inhaled corticosteroids; = inhaled corticosteroids; ILIL = = interleukin; interleukin; LTLT = leukotriene; = leukotriene; PEFRPEFR = peak expiratory flow rate; pts = patients; = peak expiratory flow rate; pts = patients; ↑↑ indicates increased; indicates increased; ↓↓ indicates decreased indicates decreased King P. King P. DrugsDrugs 2007;67(7):9652007;67(7):965--974974
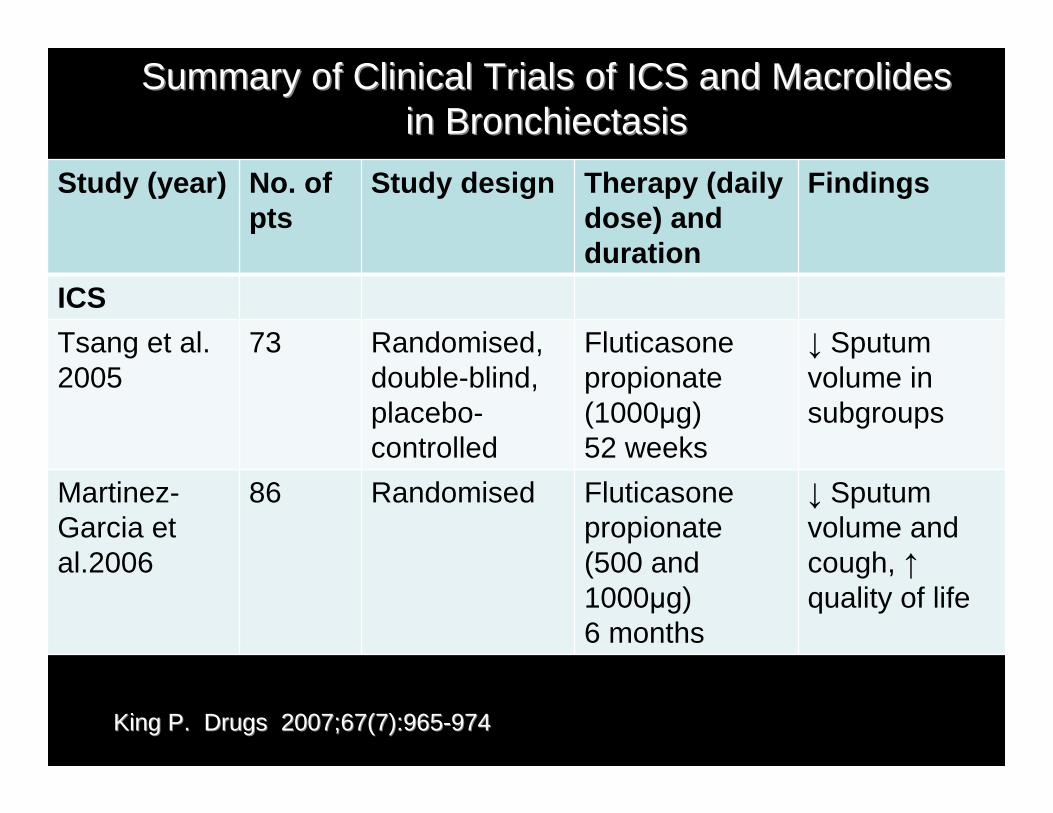
Study (year) No. of pts
Study design Therapy (daily dose) and duration
Findings
ICS
Tsang et al.2005
73 Randomised, double-blind, placebo-controlled
Fluticasone propionate (1000µg)52 weeks
↓ Sputum volume in subgroups
Martinez-Garcia et al.2006
86 Randomised Fluticasone propionate (500 and 1000µg)6 months
↓ Sputum volume and cough, ↑quality of life
Summary of Clinical Trials of ICS and Macrolides Summary of Clinical Trials of ICS and Macrolides in Bronchiectasisin Bronchiectasis
King P. King P. DrugsDrugs 2007;67(7):9652007;67(7):965--974974
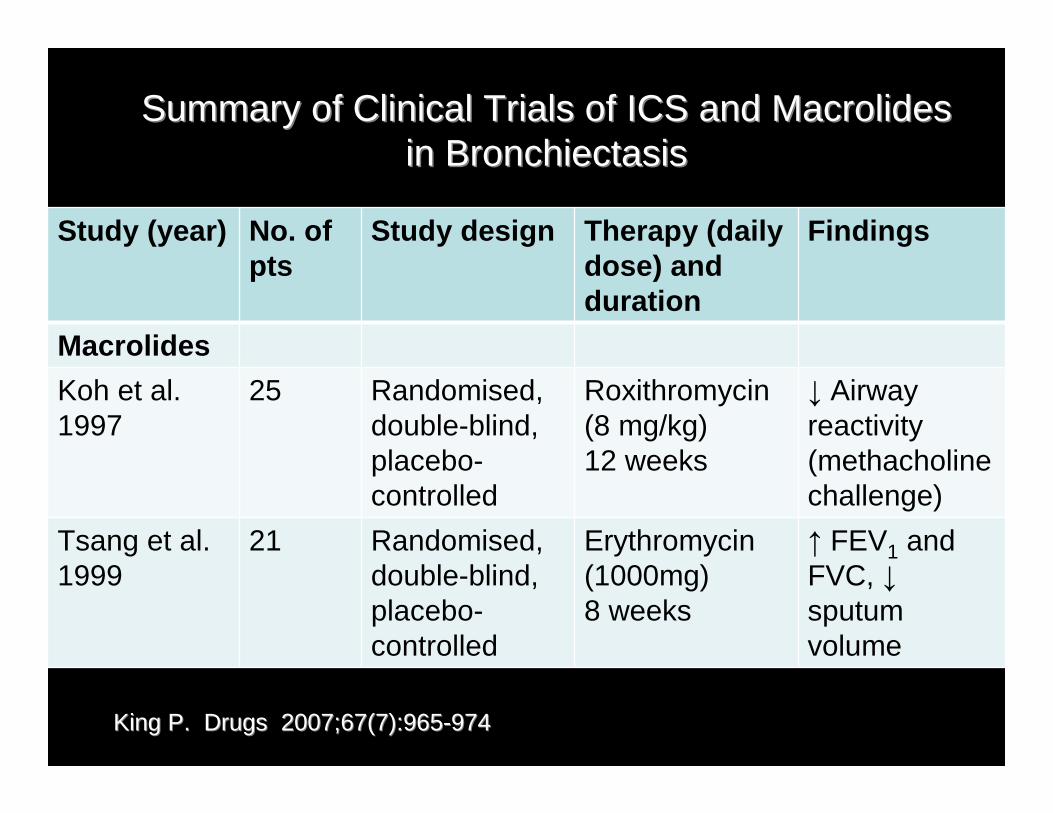
Study (year) No. of pts
Study design Therapy (daily dose) and duration
Findings
Macrolides
Koh et al.1997
25 Randomised, double-blind, placebo-controlled
Roxithromycin (8 mg/kg)12 weeks
↓ Airway reactivity (methacholine challenge)
Tsang et al.1999
21 Randomised, double-blind, placebo-controlled
Erythromycin (1000mg)8 weeks
↑ FEV1 and FVC, ↓sputum volume
Summary of Clinical Trials of ICS and Macrolides Summary of Clinical Trials of ICS and Macrolides in Bronchiectasisin Bronchiectasis
King P. King P. DrugsDrugs 2007;67(7):9652007;67(7):965--974974
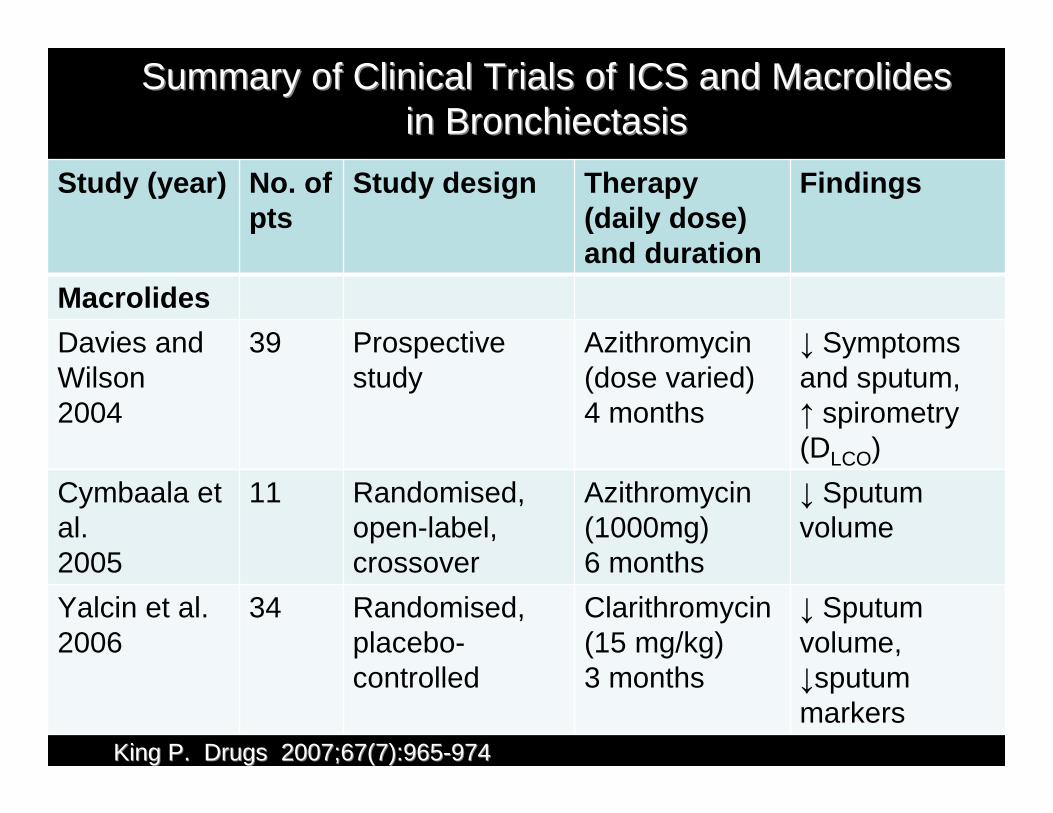
Study (year) No. of pts
Study design Therapy (daily dose) and duration
Findings
Macrolides
Davies and Wilson2004
39 Prospective study
Azithromycin (dose varied)4 months
↓ Symptoms and sputum, ↑ spirometry (DLCO)
Cymbaala et al.2005
11 Randomised, open-label, crossover
Azithromycin (1000mg)6 months
↓ Sputum volume
Yalcin et al.2006
34 Randomised, placebo-controlled
Clarithromycin (15 mg/kg)3 months
↓ Sputum volume, ↓sputum markers
Summary of Clinical Trials of ICS and Macrolides Summary of Clinical Trials of ICS and Macrolides in Bronchiectasisin Bronchiectasis
King P. King P. DrugsDrugs 2007;67(7):9652007;67(7):965--974974
Smoking Cessation and Asthma (cont’d)
• Secondhand smoke associated with increased symptoms, poor quality of life, reduced lung function, increased hospitalizations and emergency visits
• Effectiveness of treatment of asthma may be compromised by smoking
Gritz ER et al. Gritz ER et al. Am J Prev Med 207;33(6S):S414Am J Prev Med 207;33(6S):S414--S422S422
Asthma and Smoking
• Smoking asthmatics have increased numbers of neutrophils
• Increased levels of IL-8• Decreased numbers of eosinophils in
sputum • Smoking may shift the inflammatory
phenotype from eosinophilia towards neutrophilia
• Smoking may increase steroid-resistance in asthma
Hylkema MN. Hylkema MN. Eur Respir JEur Respir J 2007;29(3):4382007;29(3):438--445 445
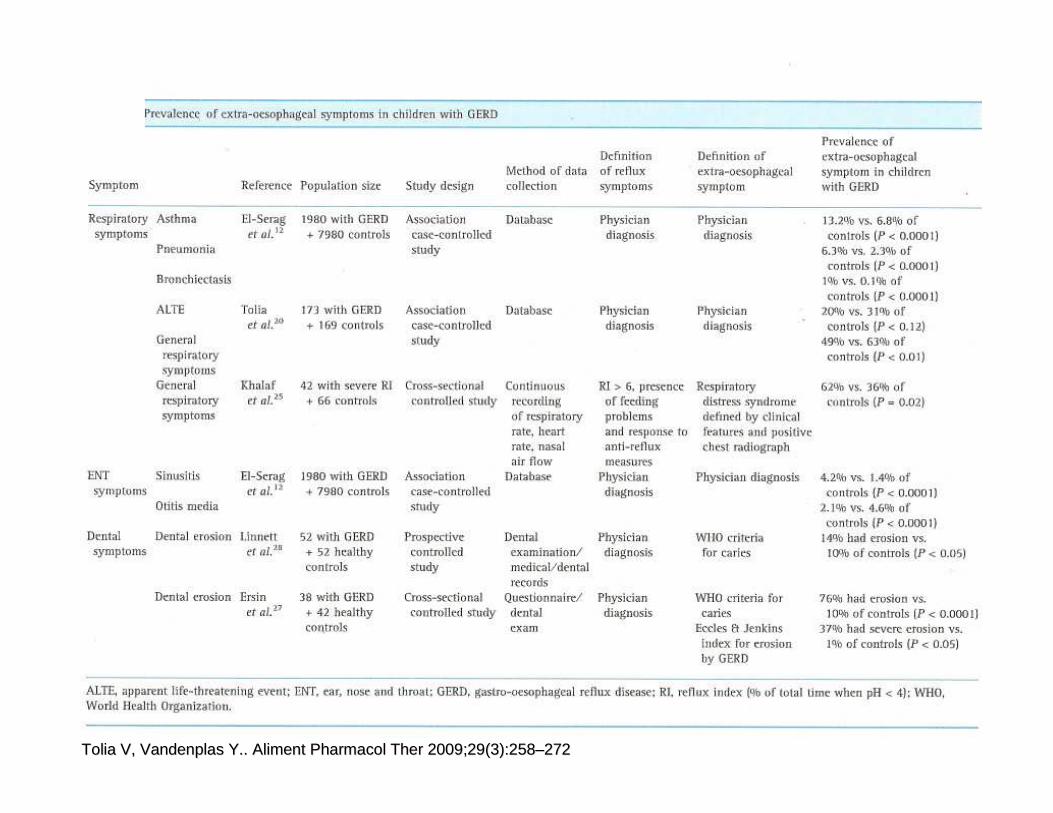
Tolia V, Vandenplas Y.. Aliment Pharmacol Ther 2009;29(3):258Tolia V, Vandenplas Y.. Aliment Pharmacol Ther 2009;29(3):258––272272
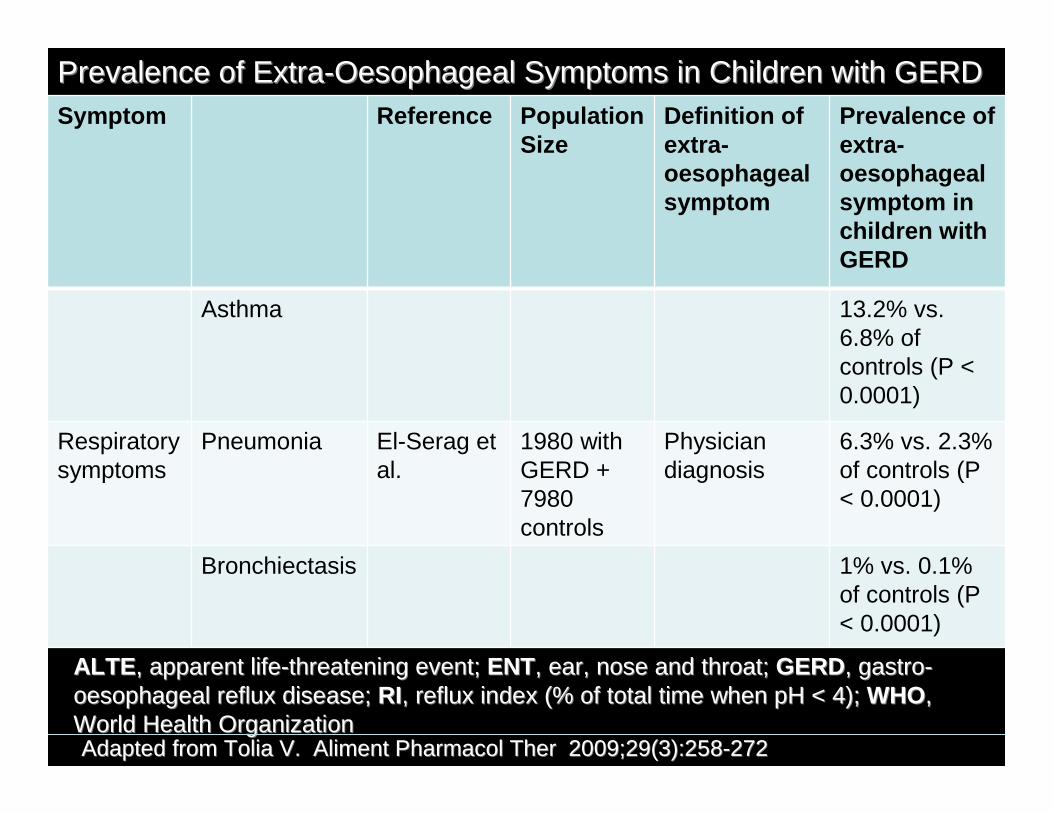
Symptom Reference Population Size
Definition of extra-oesophageal symptom
Prevalence of extra-oesophageal symptom in children with GERD
Asthma 13.2% vs. 6.8% of controls (P < 0.0001)
Respiratorysymptoms
Pneumonia El-Serag et al.
1980 with GERD + 7980 controls
Physician diagnosis
6.3% vs. 2.3% of controls (P < 0.0001)
Bronchiectasis 1% vs. 0.1% of controls (P < 0.0001)
Prevalence of ExtraPrevalence of Extra--Oesophageal Symptoms in Children with GERDOesophageal Symptoms in Children with GERD
ALTEALTE, apparent life, apparent life--threatening event; threatening event; ENTENT, ear, nose and throat; , ear, nose and throat; GERDGERD, gastro, gastro--oesophageal reflux disease; oesophageal reflux disease; RIRI, reflux index (% of total time when pH < 4); , reflux index (% of total time when pH < 4); WHOWHO, , World Health OrganizationWorld Health OrganizationAdapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--272272
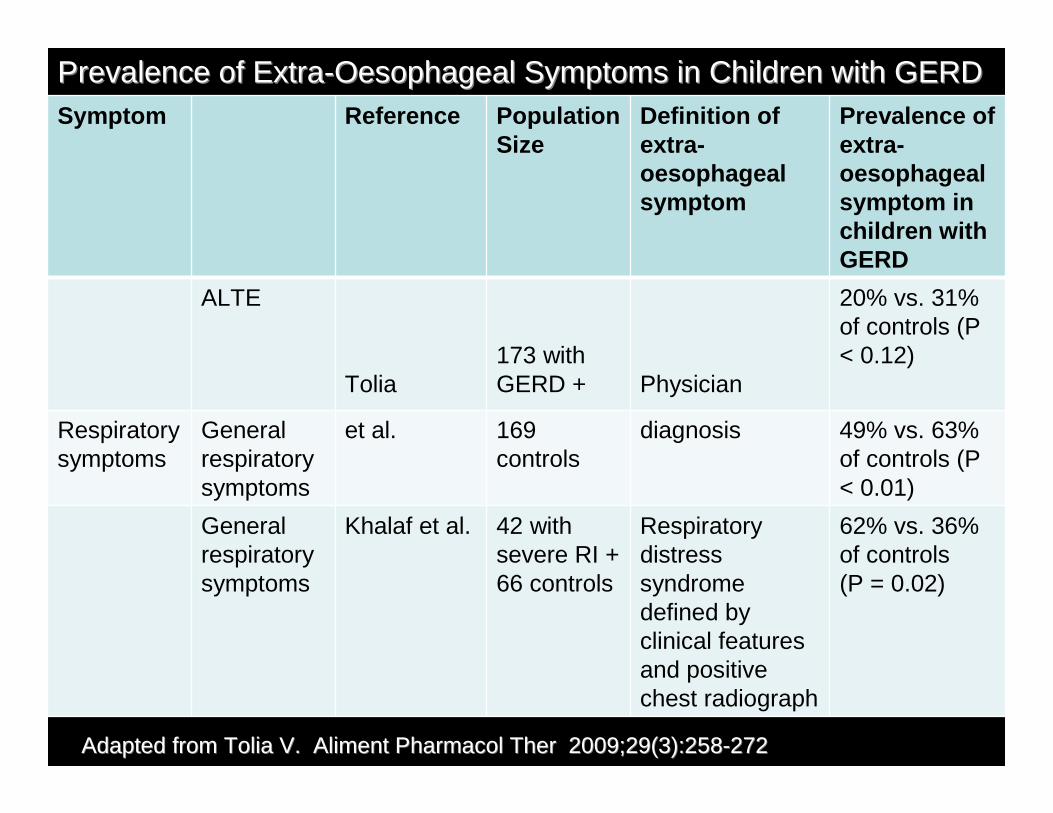
Symptom Reference Population Size
Definition of extra-oesophageal symptom
Prevalence of extra-oesophageal symptom in children with GERD
ALTE
Tolia173 withGERD + Physician
20% vs. 31% of controls (P < 0.12)
Respiratorysymptoms
General respiratory symptoms
et al. 169 controls
diagnosis 49% vs. 63% of controls (P < 0.01)
General respiratory symptoms
Khalaf et al. 42 with severe RI + 66 controls
Respiratory distress syndrome defined by clinical features and positive chest radiograph
62% vs. 36% of controls (P = 0.02)
Prevalence of ExtraPrevalence of Extra--Oesophageal Symptoms in Children with GERDOesophageal Symptoms in Children with GERD
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--272272
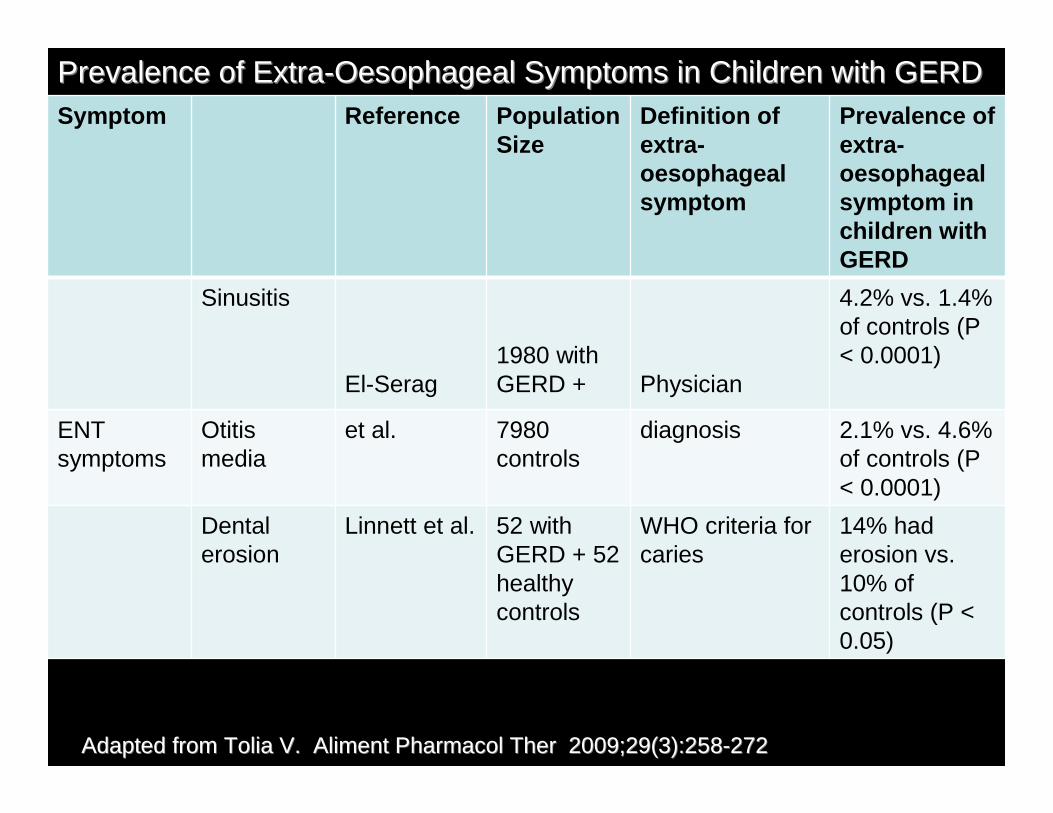
Symptom Reference Population Size
Definition of extra-oesophageal symptom
Prevalence of extra-oesophageal symptom in children with GERD
Sinusitis
El-Serag1980 with GERD + Physician
4.2% vs. 1.4% of controls (P < 0.0001)
ENTsymptoms
Otitis media
et al. 7980 controls
diagnosis 2.1% vs. 4.6% of controls (P < 0.0001)
Dental erosion
Linnett et al. 52 with GERD + 52 healthy controls
WHO criteria for caries
14% had erosion vs. 10% of controls (P < 0.05)
Prevalence of ExtraPrevalence of Extra--Oesophageal Symptoms in Children with GERDOesophageal Symptoms in Children with GERD
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--272272
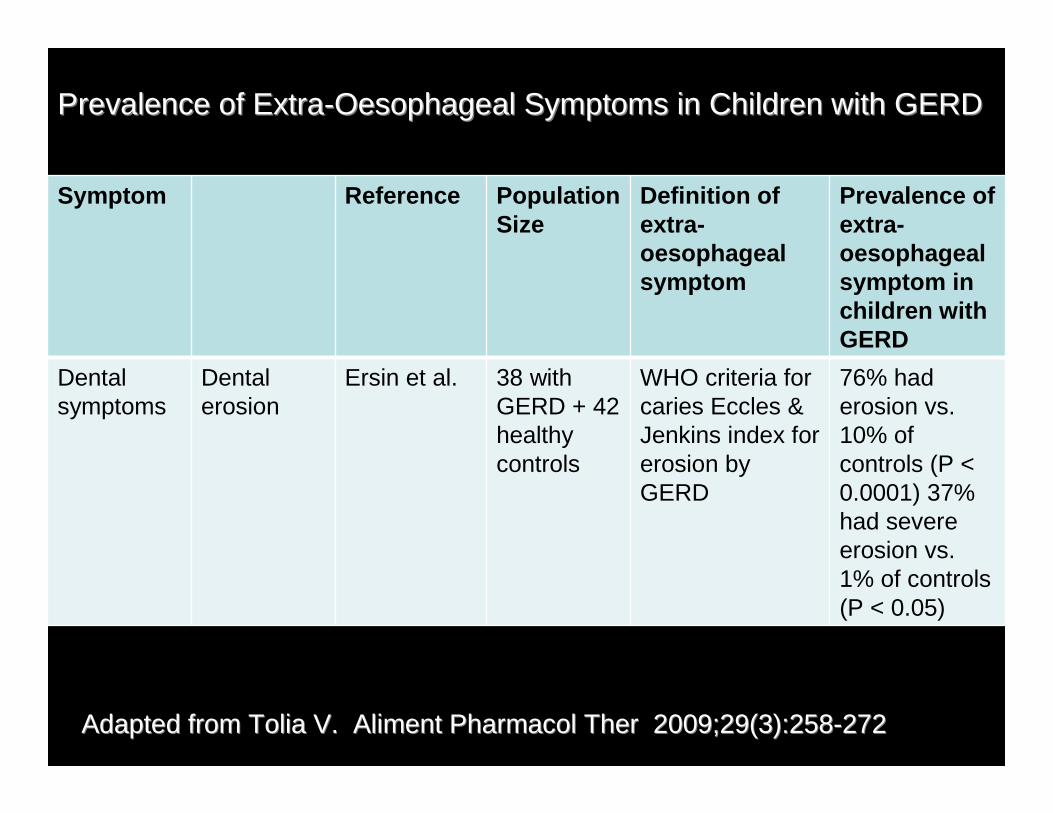
Symptom Reference Population Size
Definition of extra-oesophageal symptom
Prevalence of extra-oesophageal symptom in children with GERD
Dental symptoms
Dental erosion
Ersin et al. 38 with GERD + 42 healthy controls
WHO criteria for caries Eccles & Jenkins index for erosion by GERD
76% had erosion vs. 10% of controls (P < 0.0001) 37% had severe erosion vs. 1% of controls (P < 0.05)
Prevalence of ExtraPrevalence of Extra--Oesophageal Symptoms in Children with GERDOesophageal Symptoms in Children with GERD
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--272272
Tolia V, Vandenplas Y.. Aliment Pharmacol Ther 2009;29(3):258Tolia V, Vandenplas Y.. Aliment Pharmacol Ther 2009;29(3):258––272272
Tolia V, Vandenplas Y.. Aliment Pharmacol Ther 2009;29(3):258Tolia V, Vandenplas Y.. Aliment Pharmacol Ther 2009;29(3):258––272272
continuedcontinued
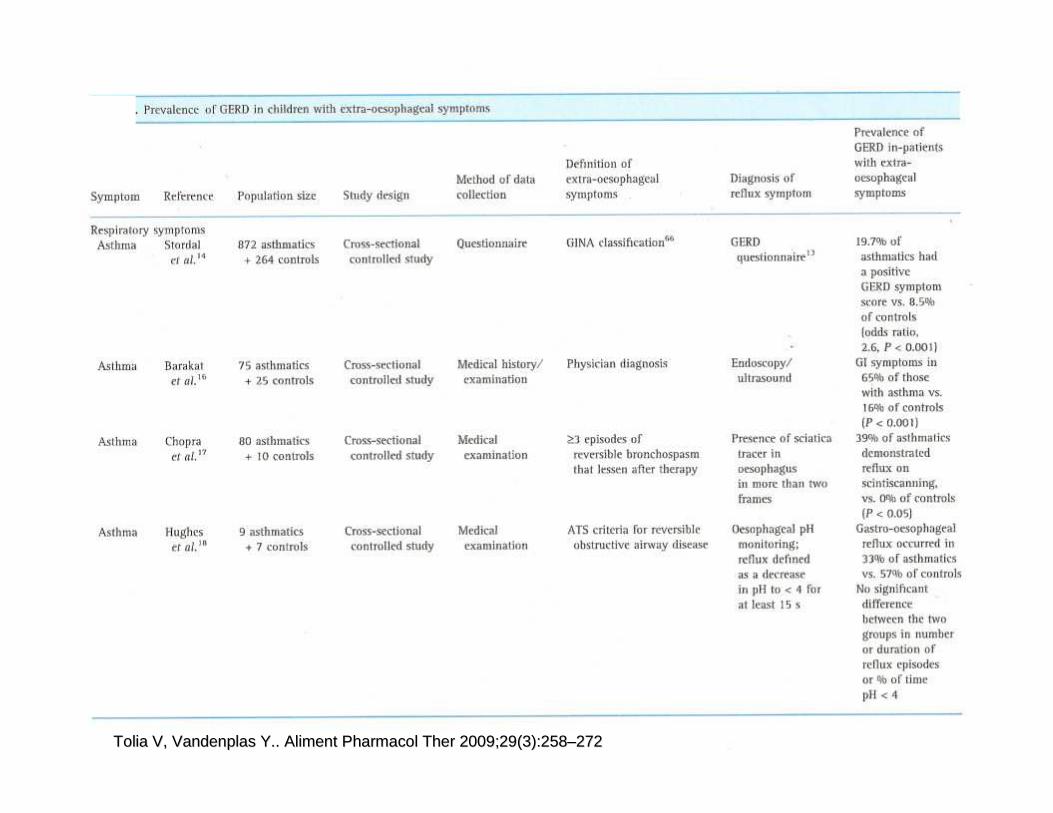
Symptom Reference Population size Diagnosis of reflux symptom
Prevalence of GERD in patients with extra-oesophageal symptoms
Respiratory symptoms
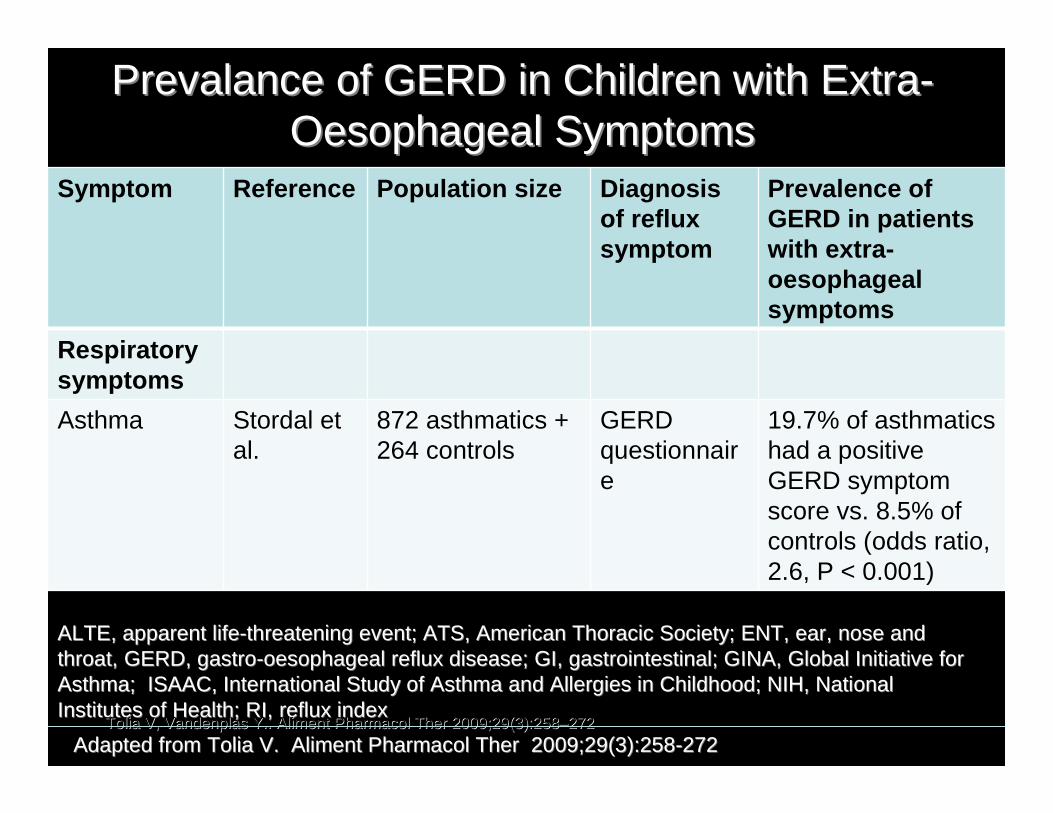
Asthma Stordal et al.
872 asthmatics + 264 controls
GERD questionnaire
19.7% of asthmatics had a positive GERD symptom score vs. 8.5% of controls (odds ratio, 2.6, P < 0.001)
Prevalance of GERD in Children with ExtraPrevalance of GERD in Children with Extra--Oesophageal SymptomsOesophageal Symptoms
ALTE, apparent lifeALTE, apparent life--threatening event; ATS, American Thoracic Society; ENT, ear, nosthreatening event; ATS, American Thoracic Society; ENT, ear, nose and e and throat, GERD, gastrothroat, GERD, gastro--oesophageal reflux disease; GI, gastrointestinal; GINA, Global Ioesophageal reflux disease; GI, gastrointestinal; GINA, Global Initiative for nitiative for Asthma; ISAAC, International Study of Asthma and Allergies in CAsthma; ISAAC, International Study of Asthma and Allergies in Childhood; NIH, National hildhood; NIH, National Institutes of Health; RI, reflux indexInstitutes of Health; RI, reflux index
Tolia V, Vandenplas Y.. Aliment Pharmacol Ther 2009;29(3):258Tolia V, Vandenplas Y.. Aliment Pharmacol Ther 2009;29(3):258––272272
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--272272
Symptom Reference Population size
Diagnosis of reflux symptom
Prevalence of GERD in patients with extra-oesophageal symptoms
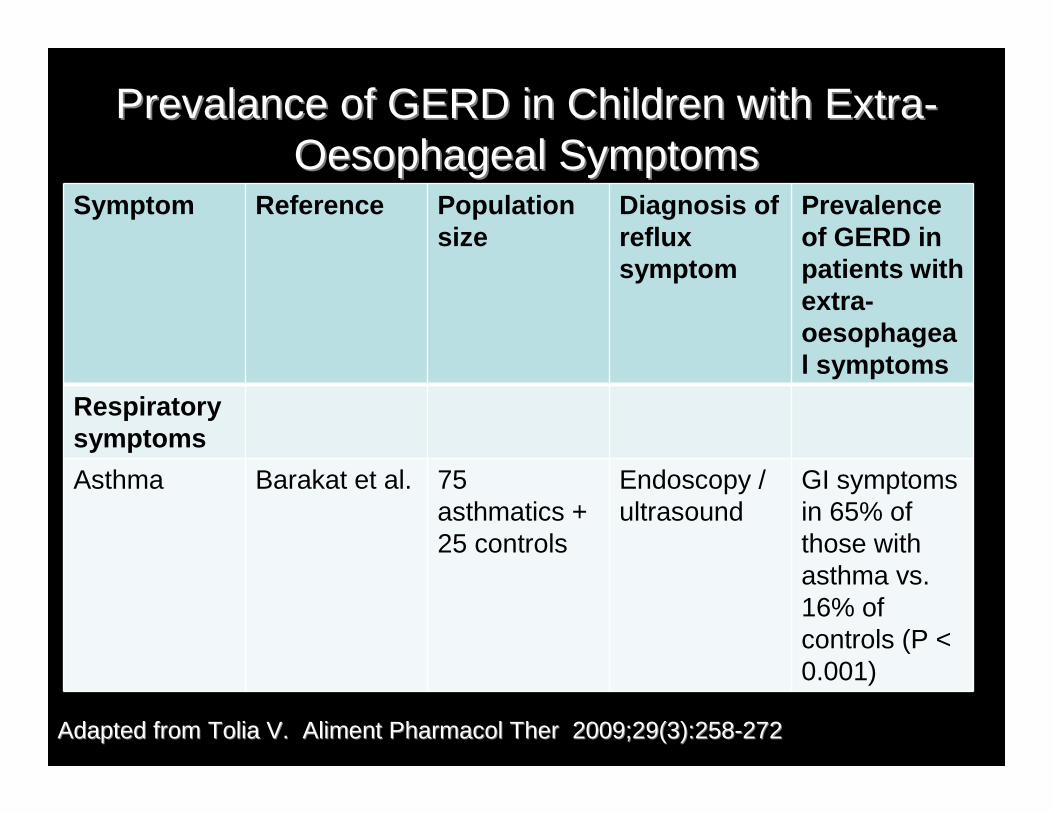
Respiratory symptoms
Asthma Barakat et al. 75 asthmatics + 25 controls
Endoscopy / ultrasound
GI symptoms in 65% of those with asthma vs. 16% of controls (P < 0.001)
Prevalance of GERD in Children with ExtraPrevalance of GERD in Children with Extra--Oesophageal SymptomsOesophageal Symptoms
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--272272
Symptom Reference Population size
Diagnosis of reflux symptom
Prevalence of GERD in patients with extra-oesophageal symptoms
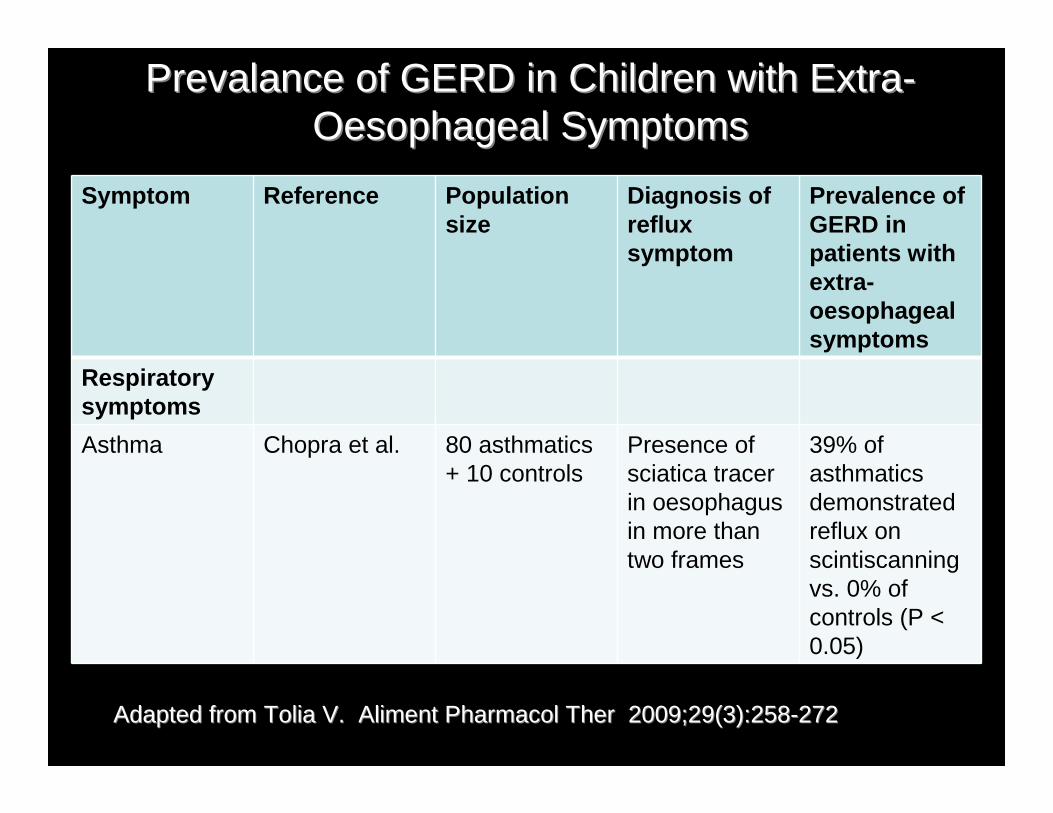
Respiratory symptoms
Asthma Chopra et al. 80 asthmatics + 10 controls
Presence of sciatica tracer in oesophagus in more than two frames
39% of asthmatics demonstrated reflux on scintiscanning vs. 0% of controls (P < 0.05)
Prevalance of GERD in Children with ExtraPrevalance of GERD in Children with Extra--Oesophageal SymptomsOesophageal Symptoms
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--272272

Symptom Reference Population size
Diagnosis of reflux symptom
Prevalence of GERD in patients with extra-oesophageal symptoms
Respiratory symptoms
Asthma Hughes et al.
9 asthmatics + 7 controls
Oesophageal pH monitoring; reflux defined as a decrease in pH to < 4 for at least 15 s
Gastro-oesophageal reflux occurred in 33% of asthmatics vs. 57% of controls. No significant difference between the two groups in number or duration of reflux episodes or % of time pH < 4
Prevalance of GERD in Children with ExtraPrevalance of GERD in Children with Extra--Oesophageal SymptomsOesophageal Symptoms
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--272272
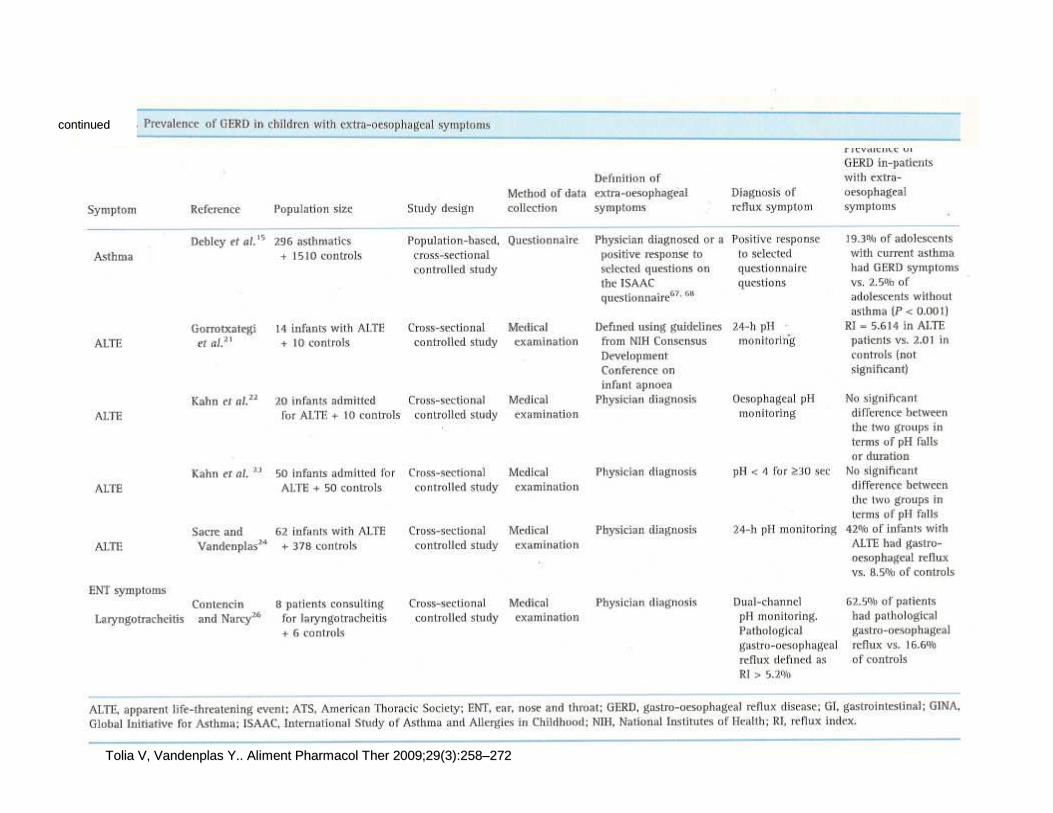
Symptom Reference Population size
Diagnosis of reflux symptom
Prevalence of GERD in patients with extra-oesophageal symptoms
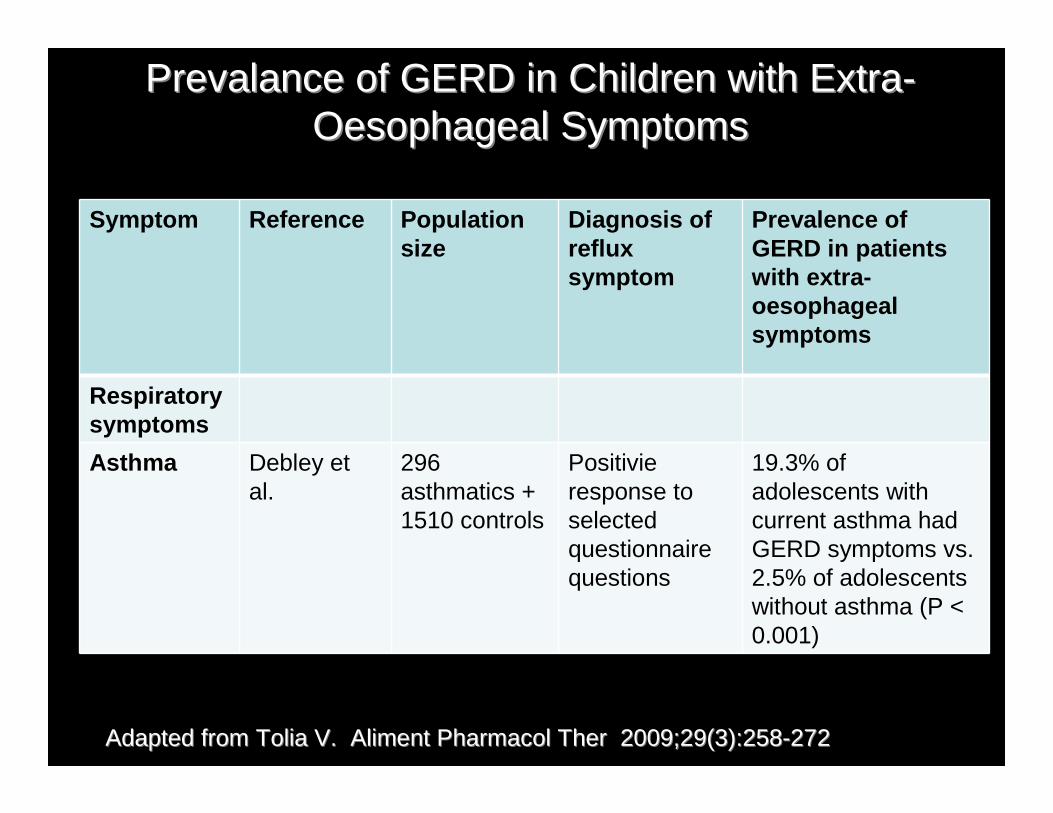
Respiratory symptoms
Asthma Debley et al.
296 asthmatics + 1510 controls
Positivie response to selected questionnaire questions
19.3% of adolescents with current asthma had GERD symptoms vs. 2.5% of adolescents without asthma (P < 0.001)
Prevalance of GERD in Children with ExtraPrevalance of GERD in Children with Extra--Oesophageal SymptomsOesophageal Symptoms
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--272272
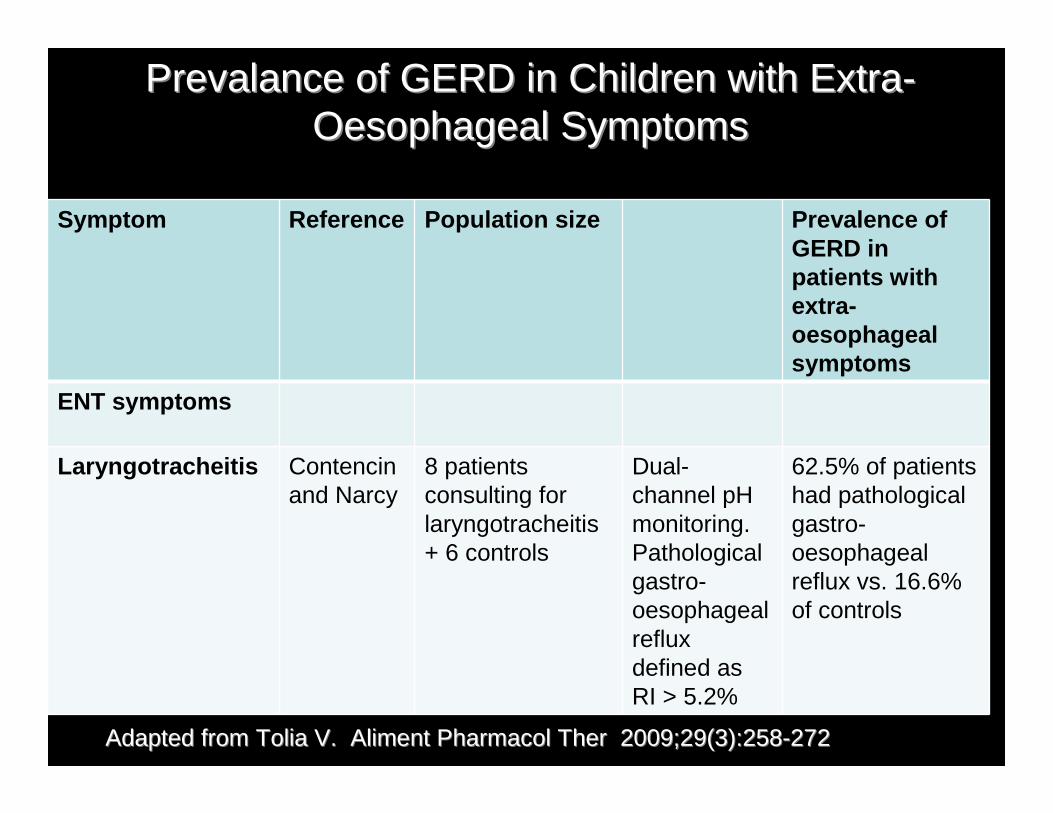
Symptom Reference Population size Prevalence of GERD in patients with extra-oesophageal symptoms
ENT symptoms
Laryngotracheitis Contencin and Narcy
8 patients consulting for laryngotracheitis + 6 controls
Dual-channel pH monitoring. Pathological gastro-oesophageal reflux defined as RI > 5.2%
62.5% of patients had pathological gastro-oesophageal reflux vs. 16.6% of controls
Prevalance of GERD in Children with ExtraPrevalance of GERD in Children with Extra--Oesophageal SymptomsOesophageal Symptoms
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--272272

Tolia V, Vandenplas Y.. Aliment Pharmacol Ther 2009;29(3):258Tolia V, Vandenplas Y.. Aliment Pharmacol Ther 2009;29(3):258––272272
Reference Pop.size
Study design
Definition of extra-oesophageal symptom
Drug and dosage
Outcome
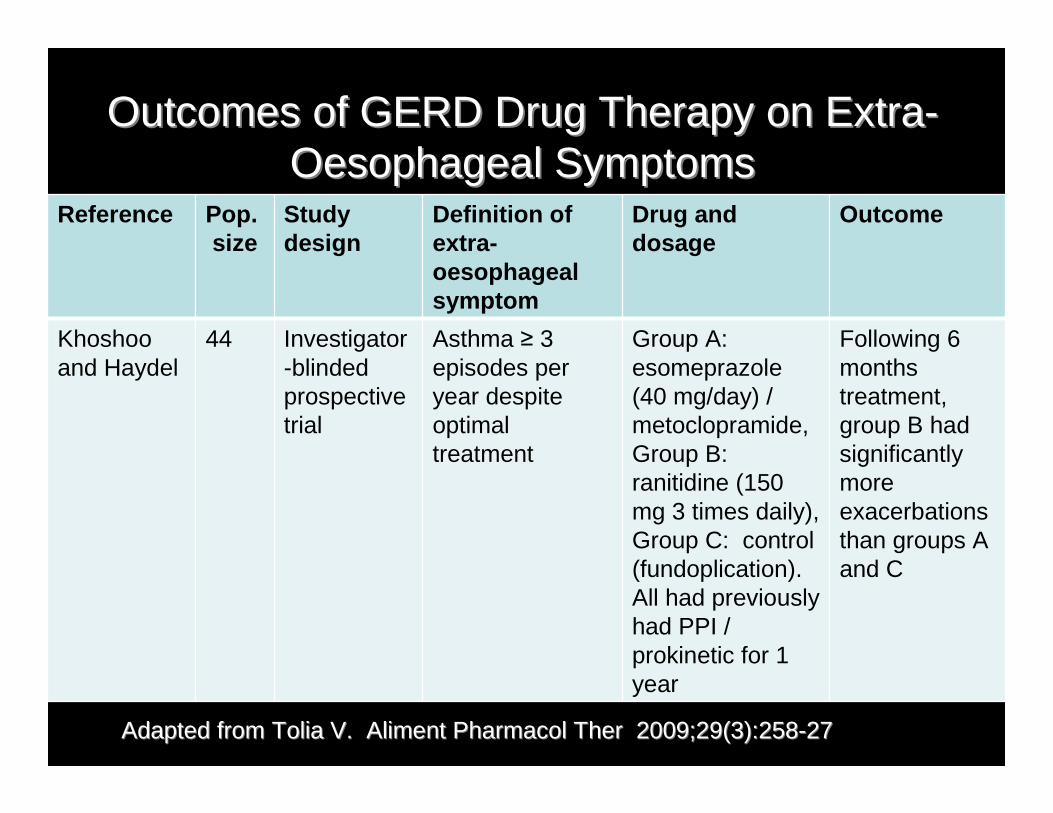
Khoshoo and Haydel
44 Investigator-blinded prospective trial
Asthma ≥ 3 episodes per year despite optimal treatment
Group A: esomeprazole (40 mg/day) / metoclopramide, Group B: ranitidine (150 mg 3 times daily), Group C: control (fundoplication). All had previously had PPI / prokinetic for 1 year
Following 6 months treatment, group B had significantly more exacerbations than groups A and C
Outcomes of GERD Drug Therapy on ExtraOutcomes of GERD Drug Therapy on Extra--Oesophageal SymptomsOesophageal Symptoms
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--2727
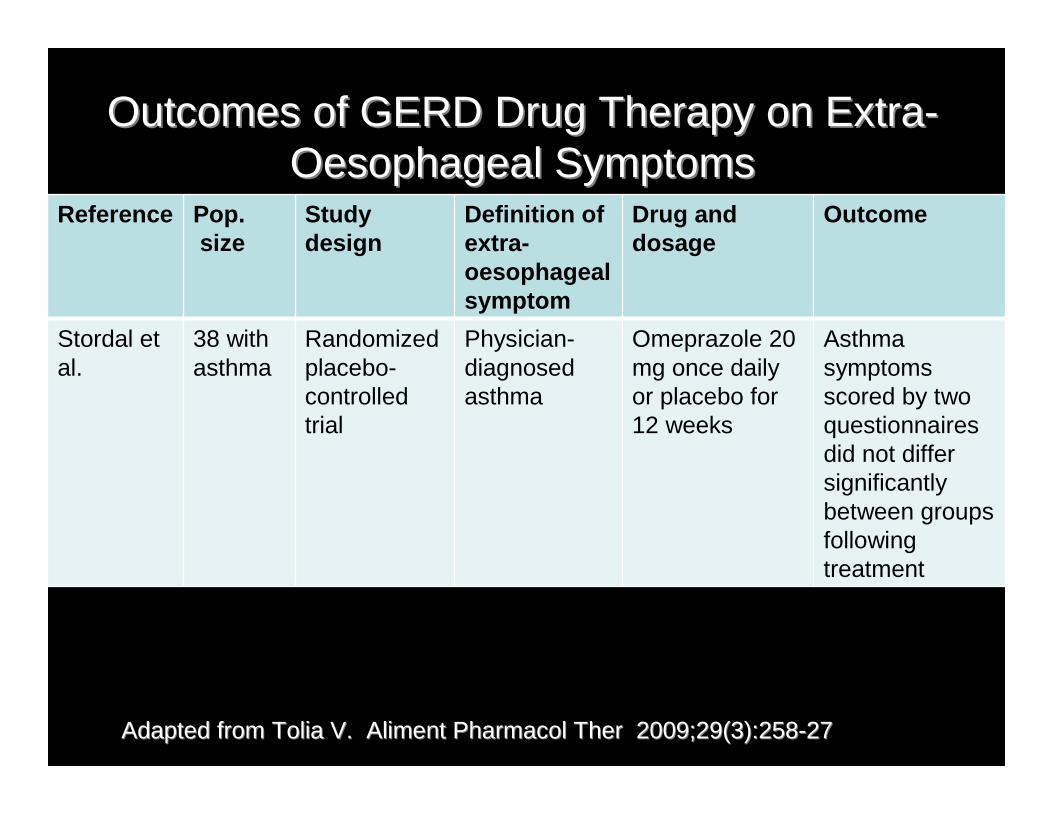
Reference Pop.size
Study design
Definition of extra-oesophageal symptom
Drug and dosage
Outcome
Stordal et al.
38 with asthma
Randomized placebo-controlled trial
Physician-diagnosed asthma
Omeprazole 20 mg once daily or placebo for 12 weeks
Asthma symptoms scored by two questionnaires did not differ significantly between groups following treatment
Outcomes of GERD Drug Therapy on ExtraOutcomes of GERD Drug Therapy on Extra--Oesophageal SymptomsOesophageal Symptoms
Adapted from Tolia V. Adapted from Tolia V. Aliment Pharmacol TherAliment Pharmacol Ther 2009;29(3):2582009;29(3):258--2727
Inhaled Budesonide in Smokers and Nonsmokers with Mild Persistent Asthma
• Lung function declines in smoking asthmatics quicker than nonsmoking asthmatics
• Benefits of budesonide are similar in both smokers and nonsmokers
O’Byrne PM et al. Chest 2009;136:1514-1520


Related Documents











