Dr. Agh Pakniyat ASTHMA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr. Agh Pakniyat
ASTHMA

EPIDEMIOLOGY
• children than adults, in females than males, and in blacks than whites or Hispanics.
• more prevalent in the impoverished and in those residing in nonmetropolitan locales.
• Factors that contribute to asthma morbidity and mortality :
inadequate patient and physician assessment of an acute episode resulting in under treatment
overuse of prescribed or over-the-counter medications leading to delays in seeking treatment
failure of physicians to consider previous ED visits,hospitalizations, or life-threatening episodes of asthma
failure to initiate corticosteroid therapy early in the course of an exacerbation.
Socioeconomic factors, environmental influences, and overreliance on emergency facilities for all asthma care are also contributing factors.
PATHOPHYSIOLOGY
• Increased expiratory resistance:
Airway inflammation
Bronchospasm
Mucosal edema
Mucous plugging
Smooth muscle hypertrophy
• Consequences:
Air trapping
Airway remodeling
Increased dead space
Hyperinflation

Pollen
Dust mites
Molds
Animal dander
Other environmental allergens
Viral upper respiratory infections
Occupational chemicals
Tobacco smoke
Environmental change
Cold air
Exercise induced
Emotional factors
Menstrual associated
Drugs:
Aspirin
NSAIDs
β-blockers
Triggers:

• Mast cell stabilizers (e.g., beta-agonists) are
more effective in the early asthmatic
response but are of less use later in the
course of an exacerbation. Anti-inflmmatory
therapy (e.g., corticosteroids, LT antagonists)
is more effective in the late asthmatic
response.


ASPIRIN-EXACERBATED RESPIRATORY DISEASE
(AERD) :
nasal polyps
eosinophilic sinusitis
asthma
and sensitivity to cyclooxygenase (COX)-1
inhibitor drugs (e.g., aspirin)
adult>pedi
Femal>male
average age of onset is 34 years, frequently after a
viral respiratory illness.

• acute asthma symptoms occur within 3 hours,
• accompanied by profuse rhinorrhea,
conjunctival injection, periorbital edema, and
occasionally a scarlet flshing of the head and
neck

AERD RX :
oblock synthesis of LTs (e.g.,
zileuton)
oblock specifi LT receptors (e.g.,
zafilukast, montelukast).
• AERD is not reported after administration of COX-2 inhibitors.
Most patients with AERD can tolerate up to 500 mg of acetaminophen safely, but 28 to 34% experience mild respiratory reactions when administered 1000 to 1500 mg. Reactions to acetaminophen tend to be milder than those to NSAIDs.

EXERCISE-INDUCED ASTHMA (EIA):
Prophylaxis :short-acting inhaled beta-agonist
Pretreatment with cromolyn, LT antagonists (montelukast), and inhaled parasympatholytics is also effective.
Breathing through the nose may allow warming and humidification of cool dry air during exercise.
Long-acting beta-agonists are usually effective, but tachyphylaxis and loss of efficacy may occur if these agents are used regularly
MENSTRUATION-ASSOCIATED ASTHMA
• Perimenstrual reductions in peak expiratory
flew rates (PEFRs) of 35 to 80% are reported.
• Estradiol inhibits eosinophil degranulation
and suppresses LT activity.
• Progesterone may also have bronchodilator
and antiinflmmatory activity, and the rapid
decline in progesterone levels before
menstruation may contribute to increased
bronchospasm.
• Rx: LT antagonists, long-acting beta-agonists,
and oral contraceptives.

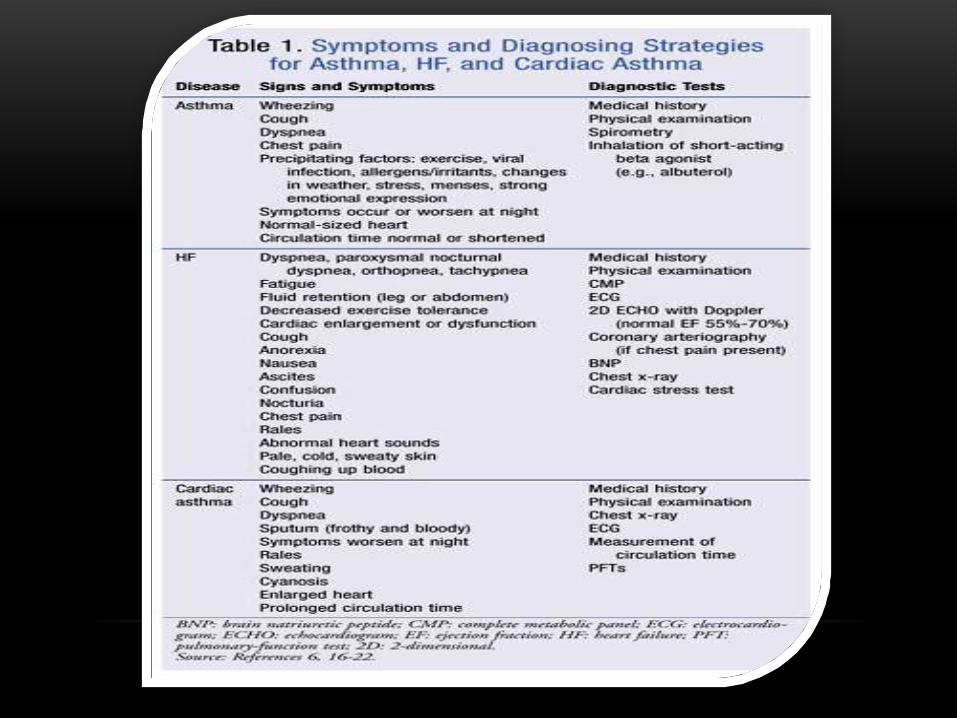
DIAGNOSTIC STRATEGIES
• PFT
• Therefore routine PFT should be part of ED assessment and monitoring.
• The forced expiratory volume in 1 second from maximal inspiration (FEV1) or the PEFR in liters per second, starting with fully inflted lungs and sustained for at least 10 msec, may be used.
• Any patient not able to perform a pulmonary function study should be considered to have severe airway obstruction.
ABG;hyperventilation leads to a modest fall in the
partial pressure of carbon dioxide in arterial blood (Paco2). As airway obstruction increases, the Paco2 normalizes (PFT values 15-25% predicted) and then increases (PFT values <15% predicted) with worsening hypoxemia.
ABG determination is rarely clinically useful in acute asthma exacerbations unless oxygen saturation cannot be obtained reliably via pulseoximetry.
ABG sampling should be limited to a subset of patients with predicted PFT values of less than 30%, whose clinical course is perplexing, and for whom capnographyis not available.
• Laboratory studies rarely are helpful in evaluating the patient with an acute asthma attack.
• Leukocytosis
• In the older asthmatic with cardiovascular comorbidities, measurement of the B-type natriuretic peptide (BNP) level may reveal unrecognized congestive heart failure.
• Serum electrolytes are not primarily altered unless the patient is taking corticosteroids or diuretics or has cardiovascular disease and is receiving aggressive beta2-agonist therapy.
CXR :
complicating cardiopulmonary process,
such as pneumonia, pneumothorax,
pneumomediastinum, or congestive
heart failure.
patients who do not respond to
optimal therapy and require
hospital admision.
First presentation
ECG :
• If :chest pain or a history of significant cardiovascular disease, in whom the asthma attack may be a physiologic stress test.
continuous cardiac monitoring :
Older patients, especially those with coexistent heart disease or with severe exacerbation
severe hypoxemia
intubation is contemplated.
o Transient changes in severe asthma :
Right axis deviation
Right bundle branch block
Abnormal P-waves
Nonspecific ST–T-wave changes:severe right ventricular strain pattern that reverses with improvement in airflw.
• cytokine profies in the blood
• evaluation of LTE4 in the urine
• monitoring of exhaled pentane, hydrogen peroxide, NO, or carbon monoxide levels
exhaled NO, a marker of airway inflmmation.


MANAGEMENT OF ACUTE EXACERBATION:
PRE HOSPITAL :
• Recognize the “quiet chest” as respiratory distress.
• increased use of inhaled beta2-agonists
• early administration of systemic corticosteroids (not simply doubling the dose of current ICSs)

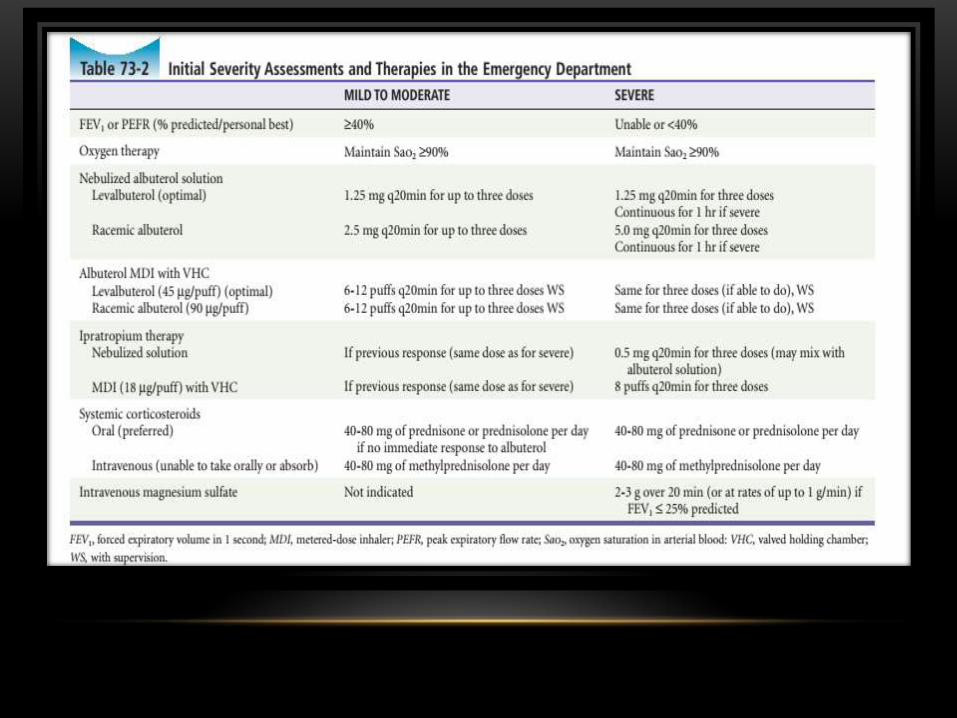
MANAGEMENT OF ACUTE ASTHMA IN
THE EMERGENCY DEPARTMENT
•Oxygen Administration:
Goal : arterial oxygen saturation above 90% (above 95% in pregnant women and those with coexistent heart disease).
Humidification of the inspired air oxygen mixture is not essential.
ADRENERGIC MEDICATION:
•Guidelines for chronic
use of inhaled beta2-
agonists,, recommend
limited daily use in a
rescue-only mode.
SHORT-ACTING INHALED BETA2-AGONIST
CHOICE AND ADMINISTRATION SCHEDULE.• more beta2-selective
In chronic asthma, levalbuterol provides a better therapeutic index
An MDI plus a valved holding chamber (“spacer”) provides similar bronchodilation and side effects, even in severe asthma, when compared with wet nebulization.
Epinephrine is used cautiously in patients older than 40 years or those with suspected cardiovascular disease, (average 1.5 µg/min with a range of 0.5-13.3 µg/min)
The PFT response to the initial bronchodilator therapy over the initial 15 to 60 minutes is a better predictor of the need for hospitalization than is the severity of an exacerbation.
Subcutaneous adrenergic agents = aerosol delivery.
(1 : 1000 solution 0.2 to 0.5 mL q 20 to 30 minutes up to 3 dose).
LONG-ACTING BETA2-AGONISTS
(LABAS) AND ACUTE DISEASE.
• It has an onset of action of 20 minutes and thus is not a rescue medication.
• contraindicate chronic use in patients of all ages without concomitant use of an asthma controller medication such as an ICS

SYSTEMIC CORTICOSTEROIDS IN THE EMERGENCY
DEPARTMENT
moderate to severe attacks
experiencing an incomplete response to initial beta-agonist
therapy
taking oral corticosteroids or ICSs
• Oral 60 mg
• Im 40-80 mg
• may decrease admissions only in severe mode
• Continuing therapy with oral prednisone or prednisolone is given in
an adult dose of 40 to 80 mg/day, usually as a single dose.

Side effects :
1. reversible increases in glucose (important in diabetics)
2. decreases in potassium
3. fluid retention with weight gain
4. mood alterations including rare psychosis,
5. Hypertension
6. peptic ulcers,
7. aseptic necrosis of the femur
8. and rare allergic reactions.
Evidence suggests that treating both systemically and via airway with corticosteroids in acute disease is more effective than either treatment method alone.
An acceptable regimen is 40 to 60 mg of prednisone (or equivalent) in single daily dose for a total of 5 to 10 days. Dose tapering for patient was already receiving systemic steroid.
• An alternative approach, if compliance or inability to obtain oral corticosteroids is an issue, is to give an equally efficacious single depot dose of dexamethasone 10 mg, triamcinolone diacetate 40 mg, or methylprednisolone 160 mg before ED discharge.
addition of inhaled high-dose budesonide (400 µg, two puffs twice per
day)

• The maximum effect with inhaled ipratropium is in 30 to 120minutes, with the effect lasting up to 6 hours. it should not be used alone for therapy of acute asthma attacks.
Ipratropium may be more effective in :
• patients older than 40 years,
• bronchospasm secondary to beta blocking agents
• psychological factors contribute to their disease.
Magnesium adjunctive administration in severe asthma attacks (FEV1 <25% predicted) improves airflow obstruction and decreases the need for hospital admission
administer 2 to 3 g of intravenous magnesium sulfate over 20 minutes or at rates of up to 1 g/min to patients with severe refractory asthma while continuing aggressive inhalation therapy.
• Side effects :warmth, flushing, sweating, nausea and emesis, muscle weakness and loss of deep tendon reflexes, hypotension, and respiratory depression.
• Methylxanthines:
• Not recommended in acute asthma.
• Leukotriene Modifirs:
Zafilukast (20 mg twice a day) and montelukast (10 mg
daily) are rapid-acting, safe, oral asthma controller drugs
that are potent and highly selective antagonists of type 1
cysteinyl LT receptors.
Consider Antibiotic

PREGNANCY AND ACUTE ASTHMA:
• The effect of pregnancy on asthma is unpredictable.
• severity = risk of severe exacerbation.
• Obesity and female fetal sex =increased risk of exacerbation.
• severe asthma =gestational diabetes and delivery before 37 weeks.
• The hyperventilation of pregnancy is compensated for by a metabolic acidosis. Typical pregnant patients have ABGs with a pH of 7.40 to 7.45, Po2 of 106 to 110, and Pco2 of 28 to 32 mm Hg;therefore when ABG values in a pregnant patient are interpreted, a normal Pco2 actually represents hypercarbia. Maternal hypoxemia quickly results in fetal hypoxemia. PEFR remains unchanged during pregnancy, and monitoring in the ED is strongly recommended.
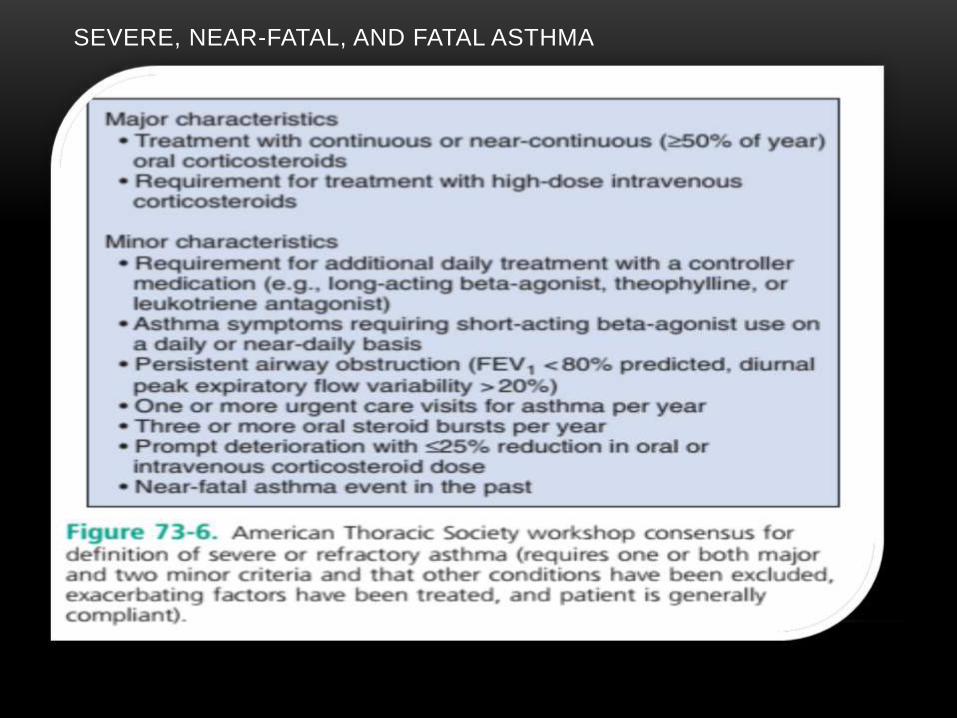
SEVERE, NEAR-FATAL, AND FATAL ASTHMA
•

Clinical features of severe asthma ;
• lesser prevalence of atopy
• a history of aspirin sensitivity
• higher incidence of sinusitis
• use of nasal corticosteroids (suggesting involvement of the upper as well as the lower respiratory tract).
• associated with menses.
Status asthmatics : severe bronchospasm that does not respond to aggressive therapies within 30 to 60 minutes.
Near fatal asthma :respiratory arrest or evidence of respiratory failure (Paco2 above 50 mm Hg).
o Slow-onset near fatal asthma: several days
o Rapid-onset near-fatal asthma: 3 hrs
It is interesting to note that the hypercapnia in rapid-onset near-fatal asthma is more responsive to therapy than that in the slow-onset type, and these patients require shorter durations of mechanical ventilation
CLINICAL APPROACH TO THE CRITICALLY ILL
ASTHMATIC
Alterations in consciousness
and bradypnea indicate
hypercarbia and impending
respiratory arrest.
• Persistent elevations of arterial lactate levels are
often associated with a poor prognosis. An elevated
lactic acid level is not predictive of respiratory failure
in critically ill asthmatics, and blood lactate levels are
not generally prognostic.
NONINVASIVE STRATEGIES.
continuously nebulized beta and anticholinergic agents
If parenteral adrenergic therapy is desired, terbutaline is preferred because of its beta2 selectivity.
Intravenous magnesium sulfate or beta-agonists (where available) may be of benefi.
Oral prednisone 60 mg or intravenous methylprednisolone 125 mg
Helium:
Mixture of helium and oxygen (80:20, 70:30, 60:40)Less dense than airDecrease airway resistance.Decrease in respiratory exhaustionNot currently recommended for routine use
Noninvasive positive-pressure ventilation may benefit carefully selected patients
May improve oxygenation and decrease respiratory fatigue
Can only be used in an alert patient
Should not replace intubation
Not currently recommended for routine use

INTUBATION AND VENTILATOR
STRATEGY
• Indications for intubation in the asthmatic patient :
• coma, altered consciousness, cardiac or respiratory arrest, paradoxical breathing pattern, refractory hypoxemia, and failure of NIPPV.
• threshold levels for intubation based on ABG results, but there is no evidence that ABG results provide better guidance regarding need for intubation than does overall clinical assessment.
• Rapid sequence intubation
Lidocaine to attenuate airway reflexesEtomidate or ketamine as an induction agentSuccinylcholine should be administered to achieve paralysis.A large endotracheal tube > 7 mm should be used to facilitate ventilation.May need to mechanically exhale for the patient
Permissive hypercapnia

• Ketamine (1-2 mg/kg) is the preferred agent for induction in rapid sequenceintubation of the asthmatic patient.
•Bronchodilator and an anesthetic agentUseful as an induction agent during intubation
•Contraindications:HTNCoronary diseasePreeclampsiaIncreased intracranial pressure

ADMISSION CRITERIA
MEDICAL WARDS
• PEFR < 40% and minimal air movement
Persistent respiratory distress:
Factors that should favor admission:
Prior intubation
Recent ED visit
Multiple ED visits or hospitalizations
Symptoms for more than 1 wk
Failure of outpatient therapy
Use of steroids
Inadequate follow-up mechanisms
Psychiatric illness
Observation Unit
PEFR > 40% but < 70% of predicted
Patients without subjective improvement
Patients with continued wheeze and diminished air movement
Patients with moderate response to therapy and no respiratory distress
Discharge CriteriaPEFR > 70% should be > 300Patient reports subjective improvementClear lungs with good air movementAdequate follow-up within 48–72 hr
PEARLS AND PITFALLS
Altered mental status in asthma equals ventilator
failure.
Patients should be able to demonstrate the
correct use of their inhaler or
nebulizer:Discharge with a peak flow meter
If no signs or symptoms of dehydration, no
evidence that IVF will clear airway secretions.
Antibiotics should generally be reserved for
patients with purulent sputum, fever, pneumonia,
or evidence of bacterial sinusitis.



Related Documents







![[Obese asthma patients have poorer asthma control.]](https://static.cupdf.com/doc/110x72/633532d03e69168eaf073f49/obese-asthma-patients-have-poorer-asthma-control.jpg)


