Association of Blood Pressure and Genetic Background With White Matter Lesions in Patients With Mild Cognitive Impairment Samantha Galluzzi, 1 Cristina Geroldi, 1,2 Luisa Benussi, 3 Roberta Ghidoni, 3 Cristina Testa, 1 Genoveffa Borsci, 1 Matteo Bonetti, 6 Dario Manfellotto, 4 Giuseppe Romanelli, 5 Roberto Zulli, 5 Giuliano Binetti, 3 and Giovanni B. Frisoni 1,2,4 1 LENITEM-Laboratory of Epidemiology, Neuroimaging and Telemedicine, 2 Psychogeriatric Unit, and 3 NeuroBioGenLab–Memory Clinic, IRCCS San Giovanni di Dio–Fatebenefratelli, Brescia, Italy. 4 AFaR, Associazione Fatebenefratelli per la Ricerca, Rome, Italy. 5 Institute of Internal Medicine, Department of Medical Sciences, University of Brescia, Italy. 6 Service of Neuroradiology, Istituto Clinico Citta ` di Brescia, Italy. Background. White matter lesions (WMLs) may contribute to cognitive deficits in patients with mild cognitive impairment (MCI), but their pathogenesis is complex. Fluctuations of blood pressure (BP) over 24 hours and genetic predisposition to develop vascular damage have been implicated. Methods. In 63 MCI patients 65 years old or older, BP was measured both clinically and with ambulatory BP monitoring. Patients were classified in two groups: no/very mild (n ¼ 34) and mild to severe (n ¼ 29) WMLs, based on a visual scale on magnetic resonance (mean age 71.8 6 4.7 vs 74.6 6 5.1, and female gender 53% vs 66%, respectively). The volume of WMLs was measured by a semi-automatic method, separately for periventricular caps and rim, periventricular confluent, subcortical punctate, and subcortical confluent. Polymorphisms of cystatin C (CST3) and cholesterol 24-hydroxylase (CYP46) genes, putative risk factors for cerebrovascular disease, were determined. Results. The prevalence of cerebrovascular risk factors was similar in the two MCI groups of different WML severity, as well as clinic and ambulatory BP. In patients with mild to severe, but not in those with no/very mild WMLs, the volume of periventricular confluent WMLs increased with increasing daytime systolic BP (regression coefficient .47, 95% confidence interval [CI], .13 to .71 vs .02, 95% CI, .32 to .36, p ¼ .003 for the difference between slopes). The volume of other WML subtypes was not associated with ambulatory BP. Participants carrying both CST3*B and CYP46*T alleles were overrepresented in the MCI group with mild to severe WMLs (43% vs 17%, p .03). Conclusions. BP and gene putative risk factors for cerebrovascular disease are differentially associated with WMLs in two MCI groups of different WML severity. WMLs might develop for the convergence of innate with acquired factors. Key Words: Blood pressure—White matter lesions—Mild cognitive impairment—Genotype—Cystatin c. M ILD cognitive impairment (MCI) is an etiologically heterogeneous syndrome of older persons that often precedes dementia. The most frequent causes of MCI are neurodegeneration due to Alzheimer’s disease (AD) (1) and white matter damage due to small vessel disease (2,3) that can be appreciated as white matter lesions (WMLs) on magnetic resonance (MR). A large body of evidence has shown that vascular risk factors, especially elevated blood pressure (BP), is associ- ated with the development of WMLs (4–6). In hypertensive patients, some factors seem to be associated with the presence of WMLs, such as the duration (7) and severity (8) of hypertension. In addition, studies on ambulatory BP monitoring evidenced the contribution of BP variability to cerebrovascular damage (9–11). In particular, steady and pulsatile components of daytime, nighttime, and 24-hour BP have gained interest in the prediction of WMLs (12). However, not all hypertensive persons develop WMLs, as suggested by clinical observations of elderly patients with a long history of hypertension, sometimes badly treated, who have only few or no WMLs. It is reasonable to hypothesize that other factors, such as genetic background, might facilitate the expression of WMLs, as suggested by genetic disorders leading to severe WMLs in the absence of vascular risk factors (13,14) and by a twin study finding that WMLs are highly heritable (15). Previous studies point to some genes as potential candi- dates for WMLs. The apoE e4 allele, the strongest risk fac- tor for AD, has been inconsistently found to be associated with WMLs (16–19). The cystatin C (CST3) gene encodes a protein implicated in the repair processes of the nervous system (20). Moreover, it has been found associated with amyloid deposits in cerebral amyloid angiopathy (21), a condition in which WMLs develop due to intimal thickening of the small vessels and ischemia of the surrounding white matter (22). The cholesterol 24-hydroxylase (CYP46) gene expresses a brain-specific enzyme involved in cholesterol metabolism and has been associated with brain amyloid load in AD (23). This literature suggests that genes might predispose to microvascular damage by either increasing 510 Journal of Gerontology: MEDICAL SCIENCES Copyright 2008 by The Gerontological Society of America 2008, Vol. 63A, No. 5, 510–517 by guest on March 1, 2016 http://biomedgerontology.oxfordjournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Association of Blood Pressure and GeneticBackground With White Matter Lesions inPatients With Mild Cognitive Impairment
Samantha Galluzzi,1 Cristina Geroldi,1,2 Luisa Benussi,3 Roberta Ghidoni,3 Cristina Testa,1
Genoveffa Borsci,1 Matteo Bonetti,6 Dario Manfellotto,4 Giuseppe Romanelli,5
Roberto Zulli,5 Giuliano Binetti,3 and Giovanni B. Frisoni1,2,4
1LENITEM-Laboratory of Epidemiology, Neuroimaging and Telemedicine, 2Psychogeriatric Unit, and3NeuroBioGenLab–Memory Clinic, IRCCS San Giovanni di Dio–Fatebenefratelli, Brescia, Italy.
4AFaR, Associazione Fatebenefratelli per la Ricerca, Rome, Italy.5Institute of Internal Medicine, Department of Medical Sciences, University of Brescia, Italy.
6Service of Neuroradiology, Istituto Clinico Citta di Brescia, Italy.
Background. White matter lesions (WMLs) may contribute to cognitive deficits in patients with mild cognitiveimpairment (MCI), but their pathogenesis is complex. Fluctuations of blood pressure (BP) over 24 hours and geneticpredisposition to develop vascular damage have been implicated.
Methods. In 63 MCI patients 65 years old or older, BP was measured both clinically and with ambulatory BPmonitoring. Patients were classified in two groups: no/very mild (n¼ 34) and mild to severe (n¼ 29) WMLs, based ona visual scale on magnetic resonance (mean age 71.8 6 4.7 vs 74.6 6 5.1, and female gender 53% vs 66%, respectively).The volume of WMLs was measured by a semi-automatic method, separately for periventricular caps and rim,periventricular confluent, subcortical punctate, and subcortical confluent. Polymorphisms of cystatin C (CST3) andcholesterol 24-hydroxylase (CYP46) genes, putative risk factors for cerebrovascular disease, were determined.
Results. The prevalence of cerebrovascular risk factors was similar in the two MCI groups of different WML severity,as well as clinic and ambulatory BP. In patients with mild to severe, but not in those with no/very mild WMLs, the volumeof periventricular confluent WMLs increased with increasing daytime systolic BP (regression coefficient .47, 95%confidence interval [CI], .13 to .71 vs .02, 95% CI,�.32 to .36, p¼ .003 for the difference between slopes). The volume ofother WML subtypes was not associated with ambulatory BP. Participants carrying both CST3*B and CYP46*T alleleswere overrepresented in the MCI group with mild to severe WMLs (43% vs 17%, p .03).
Conclusions. BP and gene putative risk factors for cerebrovascular disease are differentially associated with WMLs intwo MCI groups of different WML severity. WMLs might develop for the convergence of innate with acquired factors.
Key Words: Blood pressure—White matter lesions—Mild cognitive impairment—Genotype—Cystatin c.
M ILD cognitive impairment (MCI) is an etiologicallyheterogeneous syndrome of older persons that often
precedes dementia. The most frequent causes of MCI areneurodegeneration due to Alzheimer’s disease (AD) (1) andwhite matter damage due to small vessel disease (2,3) thatcan be appreciated as white matter lesions (WMLs) onmagnetic resonance (MR).
A large body of evidence has shown that vascular riskfactors, especially elevated blood pressure (BP), is associ-ated with the development of WMLs (4–6). In hypertensivepatients, some factors seem to be associated with thepresence of WMLs, such as the duration (7) and severity (8)of hypertension. In addition, studies on ambulatory BPmonitoring evidenced the contribution of BP variability tocerebrovascular damage (9–11). In particular, steady andpulsatile components of daytime, nighttime, and 24-hour BPhave gained interest in the prediction of WMLs (12).
However, not all hypertensive persons develop WMLs, assuggested by clinical observations of elderly patients witha long history of hypertension, sometimes badly treated,
who have only few or no WMLs. It is reasonable tohypothesize that other factors, such as genetic background,might facilitate the expression of WMLs, as suggested bygenetic disorders leading to severe WMLs in the absence ofvascular risk factors (13,14) and by a twin study finding thatWMLs are highly heritable (15).
Previous studies point to some genes as potential candi-dates for WMLs. The apoE e4 allele, the strongest risk fac-tor for AD, has been inconsistently found to be associatedwith WMLs (16–19). The cystatin C (CST3) gene encodesa protein implicated in the repair processes of the nervoussystem (20). Moreover, it has been found associated withamyloid deposits in cerebral amyloid angiopathy (21), acondition in which WMLs develop due to intimal thickeningof the small vessels and ischemia of the surrounding whitematter (22). The cholesterol 24-hydroxylase (CYP46) geneexpresses a brain-specific enzyme involved in cholesterolmetabolism and has been associated with brain amyloid loadin AD (23). This literature suggests that genes mightpredispose to microvascular damage by either increasing
510
Journal of Gerontology: MEDICAL SCIENCES Copyright 2008 by The Gerontological Society of America2008, Vol. 63A, No. 5, 510–517
by guest on March 1, 2016
http://biomedgerontology.oxfordjournals.org/
Dow
nloaded from

amyloid deposition in cerebral blood vessels or influencingbrain response to vascular damage.
The aim of this study is to evaluate the association ofambulatory BP and candidate genes for microvasculardamage with WMLs in MCI patients. BP will be measuredwith 24-hour ambulatory BP monitoring, daytime andnighttime BP will be studied separately, and pulse pressurewill also be addressed. The genetic predisposition todevelop WMLs will be assessed through polymorphismsof CST3, CYP46, and apoE genes. MCI patients rather thancognitively normal elders will be studied as the higherprevalence of WMLs in the former group may improve thepower to detect an association with BP.
MATERIALS AND METHODS
Population and Study DesignSixty-three consecutive patients seen at the Alzheimer’s
Unit of the IRCCS (Istituto di Ricovero e Cura a CarattereScientifico–Scientific Institute of Research and Care) SanGiovanni di Dio–Fatebenefratelli, Brescia, were recruited ina prospective study on the natural history of MCI. The studyprotocol was approved by the local ethics committee, and allparticipants signed an informed participation consent.
Inclusion criteria in the study were all of the following: (i)complaint by the patient or report by a relative or the generalpractitioner of memory or other cognitive disturbances; (ii)Mini-Mental State Examination (MMSE) (24) score of 24–27 or MMSE of �28 with low performance on the clockdrawing test (25) (score of 2/6 or lower); (iii) preservation ofinstrumental and basic activities of daily living. More detailshave been published elsewhere (26). Patients with history orneurological signs of major stroke have been excluded.From April 2002 through March 2005, 138 patients wereenrolled, and we selected for the present study those 100older than 65 years. Of these, 37 were excluded due toinvalid ambulatory BP measurements (n ¼ 7) or logisticproblems or refusal to perform the exam (n ¼ 30). Finally,63 MCI patients were included.
We divided the whole sample into two groups of differ-ent WML severity based on an exploratory analysis ofthe relationship between BP and WMLs assessed with avalidated visual rating scale (see MR Imaging, VisualAssessment). The analysis suggested a peculiar phenotypein which a sizeable subgroup (12 of 34, i.e., 35% of patients)had no or very mild WMLs even with high daytime systolicBP values (.135 mmHg). This observation was confirmedin the analysis of WML volumes, where a subgroup ofpatients had very low total and periventricular WMLvolumes even with extreme BP values. This observationencouraged us to isolate the group of patients with minimalor no WMLs to study possible differential associations ofBP variables and genetic background with WML severity.
Clinical AssessmentWe assessed vascular diseases and risk factors such as
hypertension, heart diseases, diabetes, and hyperlipidemia.Hypertension was defined as high values of 24-hour meanBP (systolic �135 or diastolic �85) (27) or antihypertensive
therapy. Heart diseases were defined as previous diagnosisand current treatment for coronary artery disease, primaryarrhythmias, or heart failure. Cardiovascular medicationswere recorded and coded according to the Anatomic,Therapeutic, and Chemical (ATC) classification system(C01–C08) (28). Diabetes and hyperlipidemia were definedas previous diagnosis and current treatment. Duration ofhypertension and diabetes was computed since the time offirst diagnosis.
Nonvascular physical diseases were ascertained throughhistory and clinical and instrumental exams. The number ofnonvascular physical diseases was computed as the sum ofthe following: peripheral venous, respiratory, hepatobiliary,renal, musculoskeletal, gastrointestinal, endocrine, and auto-immune diseases and malignancies.
BP MeasurementClinic BP measurement was obtained with the participant
seated after at least 2 minutes of rest using a traditionalsphygmomanometer from three consecutive measurementson both arms. The highest of the six measurements wasdefined as clinic BP.
Ambulatory BP monitoring was performed with anautomatic portable device (Schiller BR-102; Schiller AG,Baar, Switzerland). Measurements were obtained with anadult-size cuff place around the nondominant arm, unlessa right–left difference of systolic BP �10 mmHg wasdetected, in which case the cuff was placed around the armwith the higher measurement. The measurements were madeat fixed intervals of 20 minutes during daytime and nighttime.Data were considered to be adequate for analysis if at least70% of the 72 readings over the 24 hours were valid (29). The24 hours were divided into day and night based on patients’activity diaries. Daytime and nighttime BPs were the averageof the valid daytime and nighttime measurements. Pulsepressure was the average of the differences between 24-hoursystolic and diastolic values at each time point.
MR ImagingMR images were acquired at the Service of Neuroradi-
ology, Istituto Clinico Citta di Brescia, Brescia, using a 1.0Tesla Philips Gyroscan (Philips Medical Systems, Milan,Italy). Axial T2-weighted, proton density, fluid-attenuatedinversion recovery (FLAIR), and gradient echo 3D images(TR 20 ms, TE 5 ms, flip angle 308, field of view 220 mm,acquisition matrix 256 3 256, slice thickness 1.3 mm) wereacquired.
Visual AssessmentWMLs were assessed using the rating scale for age-
related white matter changes (ARWMC) (30) on T2-weighted and FLAIR MR images. WMLs were ratedseparately in frontal, parieto-occipital, temporal, infratento-rial areas and in basal ganglia on a 4-point scale. The totalscore is the sum of subscores for each area (score range 0–3)in the left and right hemisphere, ranging from 0 to 30.
MCI Groups of Different WML SeverityWMLs were considered as mild to severe when the
ARWMC scale total score was 4 or more, or when
511BP AND GENETIC BACKGROUND IN MCI
by guest on March 1, 2016
http://biomedgerontology.oxfordjournals.org/
Dow
nloaded from

beginning confluence of lesions (subscore 2) was observedin at least one area. Otherwise, WMLs were consideredabsent or very mild. Based on this criterion, patients weredivided into 34 with no/very mild WMLs and 29 with mildto severe WMLs. WML volume was computed with an in-home semiautomatic software. A description of images pre-processing, tracing, and volume computation is available athttp://www.centroalzheimer.it/public/additional_WMLvol.
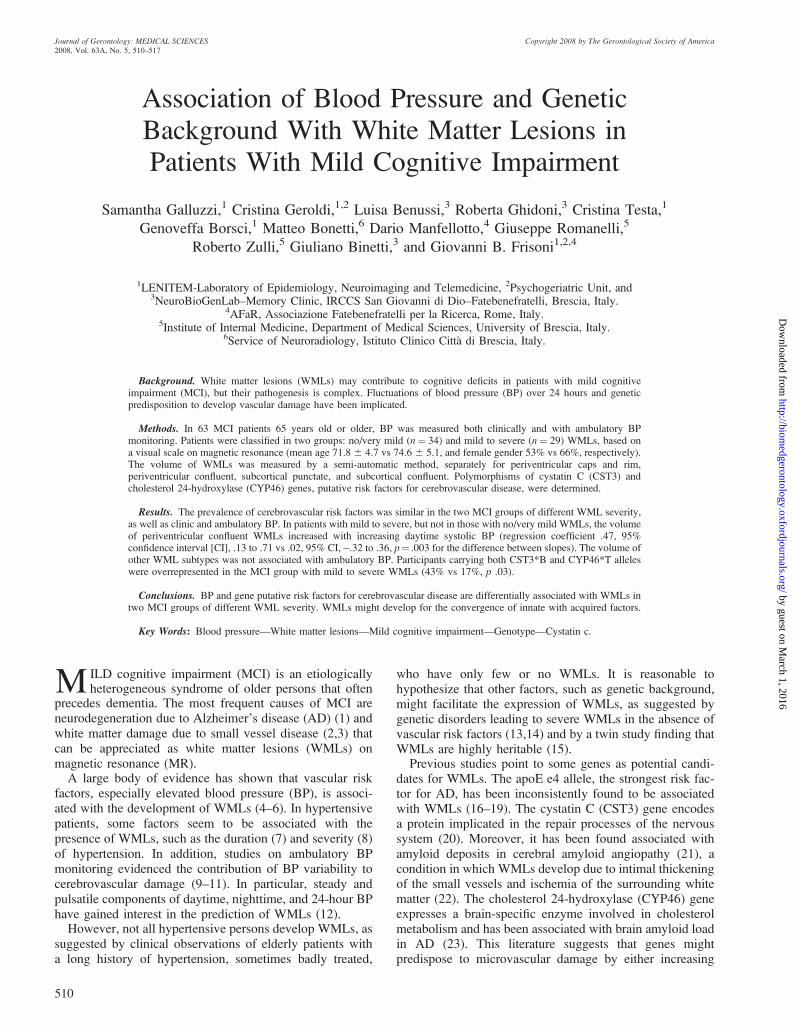
doc. WMLs were classified based on localization andmorphology, allowing differentiation of four subtypes ofWMLs: (i) periventricular caps and rim were symmetricaland regular caps around the horns of the lateral ventriclesand continuous lining surrounding the wall of lateralventricles (Figure 1a); (ii) periventricular confluent wereWMLs connected to the periventricular caps and rim butextending into deep white matter with irregular shape
Figure 1. Examples of definition of white matter lesion localization and morphology. a, Subcortical punctate (A) and confluent (B). b, Periventricular caps (A1),
caps and rim (A2), and confluent (B).
512 GALLUZZI ET AL.
by guest on March 1, 2016
http://biomedgerontology.oxfordjournals.org/
Dow
nloaded from

(Figure 1a); (iii) subcortical punctate were small (�5 mm)focal WMLS with regular shape located in deep whitematter (Figure 1b); (iv) subcortical confluent were large andirregular WMLs arising from confluence of multiple lesionslocated in the deep white matter not adjacent to lateralventricles (Figure 1b).
CovariatesThe total intracranial volume (TIV) was obtained by
manual tracing of coronal MRs using Display 1.3 tools(McConnel Brain Imagery Centre, Montreal NeurologicalInstitute, McGill University, Montreal, Canada). The brainvolume was the sum of gray and white matter volumesautomatically computed with statistical parametric mapping2 (http://www.fil.ion.ucl.ac.uk/spm/software/spm2/).
Genetic AnalysesBlood samples were available in 32 patients with no/very
mild and 28 with mild to severe WMLs. Genomic DNA wasextracted from whole-blood samples according to standardprocedures, and apoE genotyping was carried out by PCRamplification and HhaI restriction enzyme digestion. Thegenotype was resolved on 4% Metaphor Gel (BioSpa, Milan,Italy) and visualized by ethidium bromide staining (31). TheDNA was analyzed for CST3 and CYP46 polymorphisms aspreviously described (32,23). Two CST3 analyses weremissing because genotyping did not work.
Statistical AnalysisThe data were analyzed using SPSS version 13.0 (SPSS,
Chicago, IL). Sociodemographic, clinical, and geneticdifferences between the two MCI groups of differentWML severity were assessed with t test for continuousand with chi-square for categorical variables. The associa-tion between WML volume and BP variables was assessedwith multiple linear regression analysis adjusted for age,TIV, and brain volume. Generalized linear models (analysisof covariance [ANCOVA]) were built regressing each BPvariable on WMLs to assess the significance of thedifference between the regression coefficients of the twoMCI groups of WML severity. Age, TIV, and brain volumewere included as covariates.
RESULTS
Table 1 shows that patients with mild to severe WMLswere about 3 years older than those with no/very mildWMLs, whereas global cognitive performance was similar.There were no significant differences in vascular diseases,risk factors, or cardiovascular drug use, although diabeteswas about twice as frequent in the group with mild to severeWMLs (17% vs 9%). The number of nonvascular diseaseswas also similar, including renal diseases (3% vs 6%) andlevels of creatininemia (1.03 6 .20 mg/dL in both groups).In hypertensive patients, there was no correlation betweenduration of hypertension and WMLs (r ¼ .02, p¼ .92).
Table 2 shows that mean clinic and ambulatory BP valueswere not different in the two MCI groups. In those 18hypertensive patients with mild to severe and 17 with no/very mild WMLs, the mean clinic (systolic 156 6 16 vs148 6 27, p .25; diastolic 87 6 12 vs 84 6 10, p .56) andambulatory BP values (systolic 131 6 13 vs 129 6 16,p .72; diastolic 79 6 8 vs 79 6 9, p .96) were also similar,suggesting that hypertension was treated equally well inboth MCI groups with different WML severity. ApoEalleles had similar frequency in the two MCI groups. Analmost significant higher frequency of CST3*B carrierswas observed in MCI with mild to severe WMLs (46% vs23%, p .06). Participants carrying both the CST3*B andCYP46*T alleles were overrepresented in the MCI groupwith mild to severe WMLs (43% vs 17%, p .03). This resultremained significant when diabetic patients were not con-sidered in the analysis (44% vs 18%, p .046).
In the whole MCI sample (the two groups of differentWML severity being considered together), we did not findany association between total WML volume or WML
Table 1. Sociodemographic and Clinical Characteristics of
34 MCI Patients With No/Very Mild White Matter Lesions and
29 With Mild to Severe White Matter Lesions
White Matter Lesions
Variables
No/Very Mild
(N ¼ 34)
Mild to Severe
(N ¼ 29) p*
Sociodemographics
Age, y 71.8 þ 4.7 74.6 þ 5.1 .03
Gender, females 18 (53%) 19 (66%) .31
Education, y 7.3 þ 4.3 6.5 þ 3.1 .40
Cognition
MMSE 26.6 þ 1.5 27.1 þ 1.8 .27
Vascular diseases/RFs
Hypertension
Frequency 17 (50%) 18 (62%) .34
Duration, y 11.3 þ 10.6 12.3 þ 10.9 .82
Heart diseases
Arrhythmia 3 (33%) 2 (18%) .62
CAD 2 (17%) 2 (14%) 1.0
Heart failure 3 (33%) 2 (18%) .62
Diabetes
Frequency 3 (9%) 5 (17%) .32
Duration, y 18.0 þ 5.6 8.2 þ 5.4 .05
Hyperlipidemia 13 (38%) 8 (28%) .37
Cardiovascular drugs
ACE inhibitors 13 (38%) 13 (45%) .60
Ca antagonists 5 (15%) 5 (17%) .80
Diuretics 3 (9%) 4 (14%) .53
Beta blockers 4 (12%) 6 (21%) .33
Adrenergic block. 0 2 (7%) .12
Antiarrhythmics 3 (9%) 2 (7%) .78
Nitrates 5 (15%) 4 (14%) .92
Ca antagonistsy 3 (9%) 1 (3%) .38
Digitalis 0 1 (3%) .28
Physical comorbidity
(No. of nonvascular
physical diseases) 0.9 þ 1.0 0.7 þ 0.8 .45
Notes: *t or chi-square tests.yWith mainly cardiac effect (verapamil, diltiazem).
MCI ¼ mild cognitive impairment; MMSE ¼Mini-Mental State Examina-
tion; RFs ¼ risk factors; CAD ¼ coronary artery disease.
513BP AND GENETIC BACKGROUND IN MCI
by guest on March 1, 2016
http://biomedgerontology.oxfordjournals.org/
Dow
nloaded from

subtypes and BP. The relationship of BP variables with totalWML volume was significant for daytime systolic BP inMCI with mild to severe WMLs (Table 3, adjusted B¼ .38,95% CI, .02 to .66; p .03). No association was found for theother BP variables. When WML subtypes were taken intoaccount, the strongest association of daytime systolic BPwas found with periventricular confluent lesions. Theassociation was significant both within the group with mildto severe WMLs and between the two groups of WMLseverity (Table 3). Figure 2 illustrates the association ofdaytime systolic BP with WML subtype volumes in the twoMCI groups of different WML severity.
To rule out the possible confounding effect of higher,although statistically not significant, prevalence of diabetes inMCI with mild to severe WMLs, we repeated the analyses byexcluding diabetic patients (n¼ 8), but the results remainedunchanged. In particular, adjusted regression coefficients ofdaytime systolic BP on periventricular confluent WMLs were.37 (95% CI,�.04 to .67) in MCI with mild to severe and�.04(95% CI,�.39 to .32) in MCI with no/very mild WMLs ( p¼.009 for the difference between slopes).
DISCUSSION
The main finding of this study is that BP wasdifferentially associated with WMLs in MCI groups with
different WML load. In the group with greater WMLseverity, higher values of daytime systolic BP wereassociated with higher volume of periventricular confluentWMLs, whereas the other high and low values of BP wereassociated with a low burden of WMLs. The associationcannot be attributed to factors such as duration of hyper-tension or antihypertensive treatment, as these were equallydistributed in the two groups or to diabetes as the asso-ciation held also when the analyses were repeated afterexclusion of diabetic patients. Interestingly, the two MCIgroups had different genetic features, the one with greaterWML severity showing greater frequency of alleles with aputative detrimental effect on cerebral small vessels (CST3*Band CYP46*T alleles). Caps and rim, punctate, and sub-cortical confluent WMLs were never associated with BP.
Findings of the association between daytime systolic BPand WML severity and of different distribution of CST3 Band CYP46 T polymorphisms in MCI groups with differentWML load led us to speculate that this particular geneticprofile might carry an increased susceptibility to the detri-mental effects of BP on small vessels. Several observationssuggested that CST3 can exert a protective role on neurons:Different brain injuries, including ischemia, axotomy, sur-gery, and epilepsy, led CST3 expression levels to increase,both in activated glial cells and in neurons. We previouslydemonstrated that, in humans, the CST3 B allele was asso-ciated with reduced secretion of CST3 (33) and abnormalcortical rhythms in dementia and MCI (20). The CYP46T polymorphism was associated with increased cerebralb-amyloid load and cerebrospinal fluid levels of b-amyloidpeptides and phosphorylated s protein, as well as increasedrisk of AD in nondemented elderly persons (23), indicating
Table 2. Clinic and Ambulatory Blood Pressure (mmHg) and
Genetic Features of 34 MCI Patients With No/Very Mild White
Matter Lesions and 29 With Mild to Severe White Matter Lesions
White Matter Lesions
Variables
No/Very Mild
(N ¼ 34)
Mild to Severe
(N ¼ 29) p*
Blood pressure, clinic
Systolic 144 6 24 149 6 16 .31
Diastolic 82 6 10 83 6 11 .64
Pulse pressure 61 6 20 65 6 13 .34
Blood pressure, 24 h, daytime
Systolic 130 6 12 128 6 13 .43
Diastolic 79 6 9 79 6 9 .97
Pulse pressure 51 6 14 49 6 9 .42
Blood pressure, 24 h, nighttime
Systolic 125 6 16 120 6 17 .24
Diastolic 72 6 9 71 6 9 .47
Pulse pressure 52 6 13 49 6 12 .29
Apolipoprotein E
ApoE*2, alleles 1þ 2 (6%) 1 (4%) .64
ApoE*3, alleles 1þ 31 (97%) 27 (96%) .92
ApoE*4, alleles 1þ 13 (41%) 9 (32%) .50
Cystatin Cy
CST3*B, alleles 1þ 7 (23%) 13 (46%) .06
Cholesterol 24-hydroxylase
CYP46 T, alleles 1þ 28 (88%) 25 (89%) .83
Cystatin Cþ Cholesterol 24-hydroxylase
CST3*B CYP46*T, alleles 1þ 5 (17%) 12 (43%) .03
Notes: *t or chi-square test.yAvailable in 30 MCI patients with no/very mild white matter lesions and 28
with mild to severe white matter lesions.
MCI¼ mild cognitive impairment.
Table 3. Regression Coefficients (B) and 95% Confidence Interval
(CI) of Daytime Systolic Blood Pressure With Severity of White
Matter Lesions (WML) (Total and Subtypes) Volume in
34 Mild Cognitive Impairment (MCI) Patients With
No/Very Mild WMLs and 29 With Mild to Severe WMLs
No/Very Mild
WMLs (N ¼ 34)
Mild to Severe
WMLs (N ¼ 29)
Variables B 95% CI B 95% CI p*
Total volume �.14 �.46 to .21 .38y .02 to .66 .009
p ¼ .48 p ¼ .03
Periventricular caps and rim �.16 �.47 to .19 .12 �.26 to .47 .18
p ¼ .42 p ¼ .68
Periventricular confluent .02 �.32 to .36 .47y .13 to .71 .003
p ¼ .91 p ¼ .01
Subcortical punctate .12 �.23 to .44 .11 �.27 to .46 .49
p ¼ .51 p ¼ .50
Subcortical confluent �.18 �.49 to .17 .31 �.06 to .61 .05
p ¼ .36 p ¼ .10
Notes: No association was found between WML volume (total and subtypes)
and ambulatory blood pressure variables other than daytime systolic blood
pressure.
*On age-adjusted analysis of covariance. p denotes the difference between
slopes, that is, between B coefficients in those with no/very mild WMLs and
with mild to severe WMLs.ySignificant B of daytime systolic blood pressure with WML volume in
individual MCI group of WML severity. p Values (adjusted for age, brain
volume, and total intracranial volume) of B coefficients in individual MCI group
of different WML severity are shown.
514 GALLUZZI ET AL.
by guest on March 1, 2016
http://biomedgerontology.oxfordjournals.org/
Dow
nloaded from

a detrimental effect on the brain possibly mediated by b-amyloid. Our findings might suggest a synergistic inter-action of CST3 and CYP46. We hypothesize that decreasedproduction of CST3 together with increased amyloid pro-duction might result in an increased susceptibility to vas-cular damage.
The differential association of daytime systolic BP withWML subtypes deserves comment. There is much debatein the literature on the pathophysiology of WMLs. Somehistological data (34) and clinical studies (35) have
suggested that caps and rim lesions were caused by minorpathological changes of nonischemic origin and somepunctate WMLs may even correspond to no detectablechange on pathology (34,36). On the contrary, confluentWMLs seemed to have almost invariably a microvascularischemic origin (37). The present data supported the viewthat the pathophysiology of periventricular confluent wasdifferent from that of caps and rim and punctate lesions.Subcortical confluent WMLs showed a trend toward theassociation of BP with mild to severe WMLs, being
Figure 2. Association of daytime systolic blood pressure values with severity of white matter lesion (WML) subtypes in 34 mild cognitive impairment (MCI)
patients with no/very mild (open circles) and 29 with mild to severe (solid circles) WMLs.
515BP AND GENETIC BACKGROUND IN MCI
by guest on March 1, 2016
http://biomedgerontology.oxfordjournals.org/
Dow
nloaded from

significant only in the differential association between thetwo groups of WML severity.
This study has some methodological limitations. First, thesignificant associations of this study cannot be taken to pointto causal relationships due to the cross-sectional nature ofthe study and its design, which does not directly address thepathophysiological pathway leading from genes to BP toWMLs. Second, the small sample size prevented us fromadjusting analyses for potential confounders such ashypertension, which was slightly more prevalent in theMCI with mild to severe WMLs. Third, uncontrolledhypertension-related variables such as dipping (38) andBP variability (39), and other vascular risk factors such asplasma homocysteine levels and inflammatory markers(40,41) might be associated with WMLs. Fourth, the clinicalsetting where the study was carried out preventedgeneralizability before the results were replicated in a largepopulation-based sample of older persons. Last, wemeasured WMLs on conventional T2-weighted and FLAIRMR scans, which are known to capture only part of thephenotypic expression of WMLs. Novel MR techniquessuch as diffusion tensor imaging, sensitive to microstruc-tural changes of white matter axons invisible to traditionalimaging, might provide greater insight into the pathophys-iology of WMLs (42).
ConclusionOur study identified two MCI groups of different WML
load in which BP was differentially associated with WMLs.The different distribution of genes possibly involved inmicrovascular damage might underlie this differentialassociation. Further studies in larger samples of patientsare warranted to confirm these results.
ACKNOWLEDGMENTS
This study was funded in part by an ad hoc grant of the Italian Ministryof Health Ricerca Finalizzata ‘‘Decadimento cognitivo lieve non dementi-geno: stadio preclinico di malattia di Alzheimer e demenza vascolare.Caratterizzazione clinica, strumentale, genetica e neurobiologica e sviluppodi criteri diagnostici utilizzabili nella realta nazionale’’ (RA 00.61).
CORRESPONDENCE
Address correspondence to Giovanni B. Frisoni, MD, IRCCS Centro SanGiovanni di Dio–Fatebenefratelli, National Centre for Research and Careof Alzheimer’s and Mental Diseases, via Pilastroni 4, 25125 Brescia, Italy.E-mail: [email protected]
REFERENCES
1. Morris JC, Storandt M, Miller JP, et al. Mild cognitive impairmentrepresents early-stage Alzheimer disease. Arch Neurol. 2001;58:397–405.
2. DeCarli C, Miller BL, Swan GE, Reed T, Wolf PA, Carmelli D.Cerebrovascular and brain morphologic correlates of mild cognitiveimpairment in the National Heart, Lung, and Blood Institute TwinStudy. Arch Neurol. 2001;58:643–647.
3. Frisoni GB, Galluzzi S, Bresciani L, Zanetti O, Geroldi C. Mildcognitive impairment with subcortical vascular features: clinicalcharacteristics and outcome. J Neurol. 2002;249:1423–1432.
4. Breteler MM, van Swieten JC, Bots ML, et al. Cerebral white matterlesions, vascular risk factors, and cognitive function in a population-based study: the Rotterdam Study. Neurology. 1994;44:1246–1252.
5. De Leeuw FE, Barkhof F, Scheltens P. Alzheimer’s disease—oneclinical syndrome, two radiological expressions: a study on bloodpressure. J Neurol Neurosurg Psychiatry. 2004;75:1270–1274.
6. O’Rourke MF, Safar ME. Relationship between aortic stiffening andmicrovascular disease in brain and kidney: cause and logic of therapy.Hypertension. 2005;46:200–204.
7. de Leeuw FE, de Groot JC, Oudkerk M, et al. Hypertension andcerebral white matter lesions in a prospective cohort study. Brain.2002;125:765–772.
8. Sierra C, de La Sierra A, Mercader J, Gomez-Angelats E, Urbano-Marquez A, Coca A. Silent cerebral white matter lesions in middle-aged essential hypertensive patients. J Hypertens. 2002;20:519–524.
9. Yamamoto Y, Akiguchi I, Oiwa K, Hayashi M, Ohara T, Ozasa K. Therelationship between 24-hour blood pressure readings, subcorticalischemic lesions and vascular dementia. Cerebrovasc Dis. 2005;19:302–308.
10. Kukla C, Sander D, Schwarze J, Wittich I, Klingelhofer J. Changes ofcircadian blood pressure patterns are associated with the occurrence oflacunar infarction. Arch Neurol. 1998;55:683–688.
11. Sander D, Winbeck K, Klingelhofer J, Conrad B. Extent of cerebralwhite matter lesions is related to changes of circadian blood pressurerhythmicity. Arch Neurol. 2000;57:1302–1307.
12. van Boxtel MP, Henskens LH, Kroon AA, et al. Ambulatory bloodpressure, asymptomatic cerebrovascular damage and cognitive functionin essential hypertension. J Human Hypertens. 2006;20:5–13.
13. Chabriat H, Vahedi K, Iba-Zizen MT, et al. Clinical spectrum ofCADASIL: a study of 7 families. Cerebral autosomal dominant arterio-pathy with subcortical infarcts and leukoencephalopathy. Lancet. 1995;346:934–939.
14. Natte R, Maat-Schieman ML, Haan J, Bornebroek M, Roos RA, vanDuinen SG. Dementia in hereditary cerebral hemorrhage withamyloidosis-Dutch type is associated with cerebral amyloid angiopathybut is independent of plaques and neurofibrillary tangles. Ann Neurol.2001;50:765–772.
15. Atwood LD, Wolf PA, Heard-Costa NL, et al. Genetic variation inwhite matter hyperintensity volume in the Framingham Study. Stroke.2004;35:1609–1613.
16. Tian J, Shi J, Bailey K, Lendon CL, Pickering-Brown SM, Mann DM.Association between apolipoprotein E e4 allele and arteriosclerosis,cerebral amyloid angiopathy, and cerebral white matter damage inAlzheimer’s disease. J Neurol Neurosurg Psychiatry. 2004;75:696–699.
17. Wen HM, Baum L, Cheung WS, et al. Apolipoprotein E epsilon4 alleleis associated with the volume of white matter changes in patients withlacunar infarcts. Eur J Neurol. 2006;13:1216–1220.
18. Doody RS, Azher SN, Haykal HA, Dunn JK, Liao T, Schneider L.Does APO epsilon4 correlate with MRI changes in Alzheimer’sdisease? J Neurol Neurosurg Psychiatry. 2000;69:668–671.
19. Kuller LH, Shemanski L, Manolio T, et al. Relationship between ApoE,MRI findings, and cognitive function in the Cardiovascular HealthStudy. Stroke. 1998;29:388–398.
20. Babiloni C, Benussi L, Binetti G, et al. Genotype (cystatin C) and EEGphenotype in Alzheimer disease and mild cognitive impairment:a multicentric study. Neuroimage. 2006;29:948–964.
21. Levy E, Jaskolski M, Grubb A. The role of cystatin C in cerebralamyloid angiopathy and stroke: cell biology and animal models. BrainPathol. 2006;16:60–70.
22. Haan J, Maat-Schieman ML, Roos RA. Clinical aspects of cerebralamyloid angiopathy. Dementia. 1994;5:210–213.
23. Papassotiropoulos A, Streffer JR, Tsolaki M, et al. Increased brain beta-amyloid load, phosphorylated tau, and risk of Alzheimer diseaseassociated with an intronic CYP46 polymorphism. Arch Neurol.2003;60:29–35.
24. Folstein MF, Folstein SE, McHugh PR. ‘‘Mini-Mental State.’’ Apractical method for grading the cognitive state of patients for theclinician. J Psychiatr Res. 1975;12:189–198.
25. Shulman KI. Clock-drawing: is it the ideal cognitive screening test? IntJ Geriatr Psychiatry. 2000;15:548–561.
26. Rossi R, Geroldi C, Bresciani L, et al. Clinical and neuropsychologicalfeatures associated with structural imaging patterns in patients with mildcognitive impairment. Dement Geriatr Cogn Disord. 2007;23:175–183.
27. O’Brien E, Coats A, Owens P, et al. Use and interpretation ofambulatory blood pressure monitoring: recommendations of the Britishhypertension society. BMJ. 2000;320:1128–1134.
516 GALLUZZI ET AL.
by guest on March 1, 2016
http://biomedgerontology.oxfordjournals.org/
Dow
nloaded from

28. Nordic Council on Medicines. Guidelines for ATC Classification. Oslo:WHO Collaborating Centre for Drug Statistics Methodology; 1990.
29. Mancia G, Bombelli M, Lanzarotti A, et al. Systolic vs diastolic bloodpressure control in the hypertensive patients of the PAMELApopulation. Pressioni Arteriose Monitorate E Loro Associazioni. ArchIntern Med. 2002;162:582–586.
30. Wahlund LO, Barkhof F, Fazekas F, et al. European Task Force on Age-Related White Matter Changes. A new rating scale for age-related whitematter changes applicable to MRI and CT. Stroke. 2001;32:1318–1322.
31. Hixson JE, Vernier DT. Restriction isotyping of human apolipoproteinE by gene amplification and cleavage with HhaI. J Lipid Res. 1990;31:545–548.
32. Finckh U, von der Kammer H, Velden J, et al. Genetic association ofa cystatin C gene polymorphism with late-onset Alzheimer disease.Arch Neurol. 2000;57:1579–1583.
33. Benussi L, Ghidoni R, Steinhoff T, et al. Alzheimer disease-associatedcystatin C variant undergoes impaired secretion. Neurobiol Dis. 2003;13:15–21.
34. Fazekas F, Kleinert R, Offenbacher H, et al. Pathologic correlates ofincidental MRI white matter signal hyperintensities. Neurology. 1993;43:1683–1689.
35. Schmidt R, Enzinger C, Ropele S, Schmidt H, Fazekas F. AustrianStroke Prevention Study. Progression of cerebral white matter lesions:6-year results of the Austrian Stroke Prevention Study. Lancet. 2003;361:2046–2048.
36. Enzinger C, Smith S, Fazekas F, et al. Lesion probability maps of whitematter hyperintensities in elderly individuals: results of the Austrianstroke prevention study. J Neurol. 2006;253:1064–1070.
37. Pantoni L. Pathophysiology of age-related cerebral white matterchanges. Cerebrovasc Dis. 2002;13Suppl 2:7–10.
38. Sander D, Winbeck K, Klingelhofer J, Conrad B. Extent of cerebralwhite matter lesions is related to changes of circadian blood pressurerhythmicity. Arch Neurol. 2000;57:1302–1307.
39. Gomez-Angelats E, de La Sierra A, Sierra C, Parati G, Mancia G, CocaA. Blood pressure variability and silent cerebral damage in essentialhypertension. Am J Hypertens. 2004;17:696–700.
40. Hoshi T, Kitagawa K, Yamagami H, Furukado S, Hougaku H, Hori M.Relations of serum high-sensitivity C-reactive protein and interleukin-6levels with silent brain infarction. Stroke. 2005;36:768–772.
41. van Dijk EJ, Prins ND, Vermeer SE, et al. C-reactive protein andcerebral small-vessel disease: the Rotterdam Scan Study. Circulation.2005;112:900–905.
42. O’Sullivan M, Morris RG, Huckstep B, Jones DK, Williams SC,Markus HS. Diffusion tensor MRI correlates with executive dysfunc-tion in patients with ischaemic leukoaraiosis. J Neurol NeurosurgPsychiatry. 2004;75:441–447.
Received February 7, 2007Accepted August 16, 2007Decision Editor: Luigi Ferrucci, MD, PhD
517BP AND GENETIC BACKGROUND IN MCI
by guest on March 1, 2016
http://biomedgerontology.oxfordjournals.org/
Dow
nloaded from
Related Documents








![Galantamine for Alzheimer's disease and mild cognitive impairment … · [Intervention Review] Galantamine for Alzheimer’s disease and mild cognitive impairment Clement Loy1, Lon](https://static.cupdf.com/doc/110x72/5f171c96f6354220cc16d6f0/galantamine-for-alzheimers-disease-and-mild-cognitive-impairment-intervention.jpg)


