Assessment of Paediatrics Guidelines V1.1 August 2020 Page 1 of 36 Assessment of Paediatrics Guidelines Version : 1.1 First Issues: 01/08/2020 Revision Date: 01/08/2021

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 1 of 36
Assessment of Paediatrics Guidelines
Version : 1.1
First Issues: 01/08/2020
Revision Date: 01/08/2021
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 2 of 36
DOCUMENTATION INFORMATION
Version Date
01/08/2020
Version Number:
V1.1
Status:
Approved
Next Revision Date:
01/08/2021
Developed by:
Kay Bagridge, Samantha Day, Sarah Collins
Key Contact:
Kay Bagridge
Approved by:
CLG
Date Approved:
01/08/2020
Version Control
Version No:
Description Version Date Author
1.1 New Document 01/08/2020 Kay Bagridge, Samantha Day
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 3 of 36
This document is controlled and maintained on behalf of The Partnership of East London
Cooperatives:
Distribution List
All NELFT & PELC Clinical Staff
Related Documents
HI guidelines/flowchart
CONTENTS:
Section Page
1. Introduction 4 2. Aims and objectives 4 3. Roles and responsibilities 4 4. Main body of the document (process) 6 4.1 Special Considerations for Paediatric Patients 6-7 4.2. Initial Primary Assessment of the Paediatric Patient 7 4.2.1. PAT – Appearance – TICLS (“Tickles”) 8 4.2.2. PAT – Work of Breathing 9 4.2.3. PAT – Circulation to Skin 9 4.2.4. PAT - Conclusions 9 4.3. Initial Secondary Assessment of the Paediatric Patient 9 4.4 Full Assessment / Consultation 11 4.4.1. Presenting Complaint 11 4.4.2 History of Presenting Complaint 11
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 4 of 36
4.4.3. Past Medical History 12 4.4.4. Pregnancy History 12 4.4.5. Birth History 12 4.4.6 Family History 12 4.4.7 Social History 12 4.4.8 Immunisation History 12 4.4.9. Allergies 12 4.4.10. Parents / Carers and Consent 12 4.4.11. Examination 12 4.4.12 Diagnostic Tests 12 4.4.13. Impression 12 4.4.14. Plan 12 4.5 Common Childhood Illnesses 12-22 4.5.1 - 4.5.36 Details of individual conditions 12-22 4.6 Paediatric Injuries 22 5. Consent 22-23 6. Implementation process 23 7. Monitoring arrangements 23 8. Equality statement 24 9. External references 24-25 10. Training 25 Stakeholder form 26 Equality Impact Assessment (EqIA) 27 Approval checklist 29
Leadership Team approval checklist 30 Addendum
1. Introduction This SOP details the clinical assessment of paediatric patients presenting to the Walk in Centre. This SOP incorporates the previously ratified clinical policies for the assessment of paediatric patients at the Walk in Centre into a single umbrella guideline. Patients presenting to the Walk in Centre are seen, assessed and treated by autonomous Nurse Practitioners or Emergency Care Practitioners who will make diagnostic decisions based upon their consultation, clinical examination and interpretation of diagnostic tests.
2. Aims and objectives The NHS Constitution safeguards the enduring principles and values of the NHS; it sets out the rights to which patients, public and staff are entitled, and pledges which the NHS is committed to achieve. NHS bodies and local authorities are required by
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 5 of 36
law to take account of this Constitution in their decisions and actions; therefore all policy/procedural documents should consider and take into account the NHS Constitution pledges – NHS Constitution click here The Trust acknowledges the significance of National Health & Clinical Excellence (NICE) guidance. The Trust strives to provide high quality care that consistently improves by taking account of best practice. In order to achieve this, National Health & Clinical Excellence (NICE) Guidance must be disseminated, reviewed and where appropriate, implemented within the Trust. The Trust is therefore committed to ensuring National Health & Clinical Excellence (NICE) Guidance is disseminated, reviewed and where appropriate implemented within the Trust. The aim and objective of this procedural guideline is to ensure that the assessment of paediatric patients is completed in a consistent and clinically appropriate manner based upon recent clinical evidence. To ensure that patients receive a comprehensive clinical assessment based upon their individual needs. Clinicians are responsible for obtaining a clinical history and making diagnostic decisions facilitated by a medical consultation model. This procedural guideline aims to support a consistent approach in the clinical assessment of paediatric patients.
3. Roles and responsibilities
4.1 Chief executive
The Chief executive has accountability for ensuring the provision of high quality, safe and effective services within the Trust.
4.2 Senior Leadership Team (SLT) Responsible for the approval of all trustwide procedures/guidelines/protocols. 4.3 Directors
All directors are responsible for the implementation of this procedure into practice within their service areas and taking appropriate action should any breach of this procedure arise.
4.4 Assistant Directors
All assistant directors have a delegated responsibility for ensuring that this procedure/guideline is known to all staff and that its requirements are followed by all staff within their area.
4.5 Operational leads
Responsible for:
• bringing to the attention of their staff the publication of this document • providing evidence that the document has been cascaded within their team or
department
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 6 of 36
• ensuring this document is effectively implemented • ensuring that staff have the knowledge and skills to implement the procedure
and provide training where gaps are identified
4.6 Clinicians It is the duty and responsibility of all clinicians to be conversant and competent in the management of conditions detailed within this procedural guideline.
Clinicians will also be responsible for undertaking and documenting a full clinical history ensuring that the clinical records comply with Trust and professional standards for record keeping. It is the responsibility of the Operational Lead to ensure that clinical staffs are adequately trained and competent to treat the conditions detailed within this procedural guideline. A written record of assessed clinical competencies will be kept. It is the responsibility of the organisation to provide financial support for training and development to support clinical staff to practice at an advanced level.
4.7 Authors Responsible for writing the procedure/guideline, sending out for consultation and making all amendments prior to final sign off.
4.8 Quality and Patient Safety Responsible for: • Quality checking all documents to ensure both statutory and Trust requirements are met (this is to be carried out via stakeholder consultation) • publishing approved/ratified/amended documents on NELFT’s intranet Communicating newly approved/ratified/amended documents to Communications for publication in the Trust weekly newsletter
4.9 Communications
Publishing an article in the Trust weekly newsletter indicating all newly approved/ratified/amended documents
4. Process Children are brought to any healthcare setting by parents / carers for many reasons, however the most significant reasons can be summarised as follows:- • Acute Illness • Chronic Illness • Delay in reaching developmental milestones • Advice on nutrition, immunization, growth, normal variations • Recognition of syndrome complex • Reassurance of normality.
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 7 of 36
However, all paediatric patients will undergo the same initial process to establish their individual health care needs. Individual health needs will be identified by utilization of a medical model which supports effective communication for the paediatric patient, parent / carer and clinician. Communication is therefore vital, at appropriate levels and must be accurate, resulting in improved health outcomes. Clinicians will undertake consultations based upon a medical framework model which will support diagnostic decision making. Clinical records will be written up reflecting the consultation model and include the following elements:- • Initial concept of the problem • Information gathered to provide clinical assessment • Physical examination • Interpretation of examination findings / diagnostic tests • Explanation of findings • Education / treatment • Discharge advice / referral Clinicians will undertake a holistic approach when assessing individual health needs to ensure that all paediatric patients are discharged safely from the service. It will be the responsibility of the clinician to take into account any previous past medical history and social circumstances as an integral part of their clinical assessment. Specific examination and conditions affecting paediatric patients, where different to adults, will be detailed individually in the following clinical guideline. Management of individual conditions will be discussed separately, however all paediatric patients will undergo a similar initial process to establish their individual need and a working diagnosis. Reference will be made to ‘Adult’ clinical guidelines / policies, where appropriate, to avoid unnecessary repetition, as will references to Patient Group Directions, be made for similar reasons. 4.1. Special Considerations for Paediatric Patients Definition The definition of a paediatric patient is complex and varies from the differing viewpoints of the persons / agencies involved in their health and social care. Paediatric patients are often defined, medically as those patients who have not reached puberty. However, ‘puberty’ is not a single moment event, it occurs over a period of time. Furthermore, physical (as well as mental / emotional) development continues beyond puberty and indeed, in some respects, beyond the legal definition of childhood. Legally, within the UK, paediatrics, or children, are defined as such until they reach the age of 18 years. There are seven ages of children: 1. Newborn / neonate first 28 days of life 2. Infant 1 month to 12 months 3. Toddler 1 year to 3 years

Assessment of Paediatrics Guidelines V1.1 August 2020 Page 8 of 36
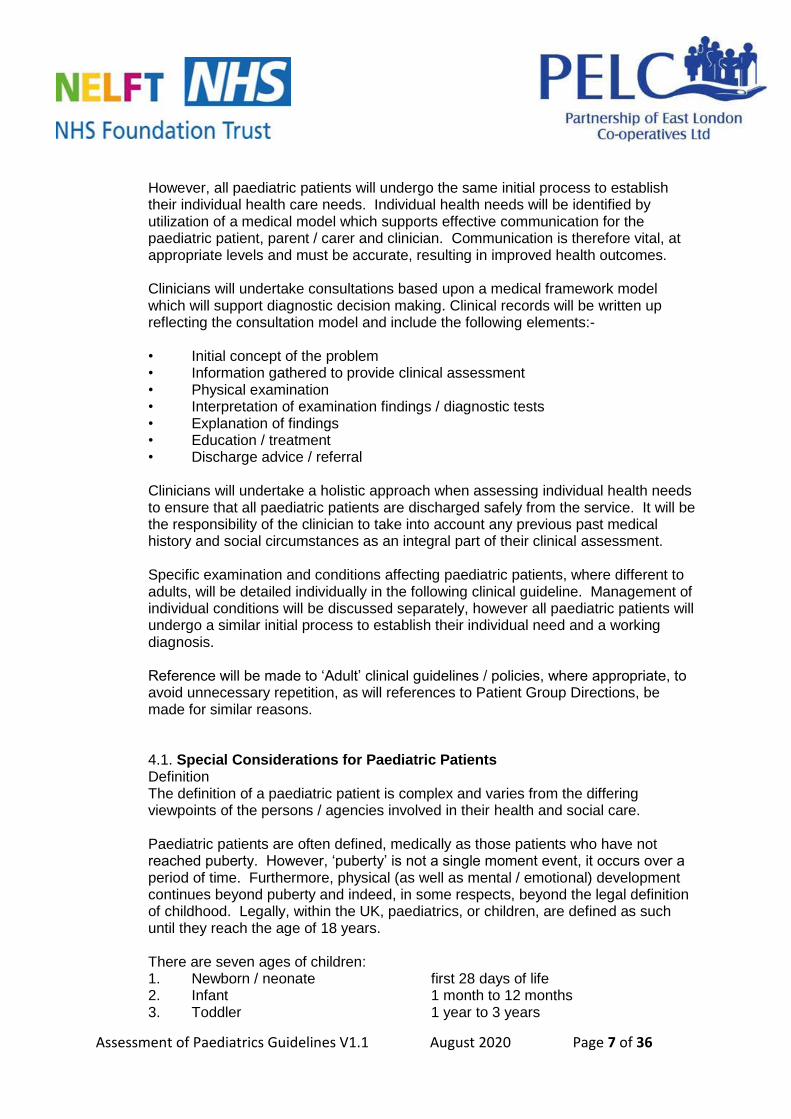
4. Pre-school 3 to 5 years 5. Schoolchild 5 to 18 years 6. Child 0 to 18 years 7. Adolescent early 10 to 14 years late 15 to 18 years It must be remembered that children are not little adults and the spectrum of diseases they suffer from are different, as is their physical anatomy. Children respond differently to disease and injury, both physically and psychologically. Young children, especially pre-verbal, have limited ability to express themselves. With children, there is never just ‘one patient.’ The parent / carer are also very much a ‘patient’, if only in the ‘emotional’ or ‘psychological’ sense; and must be treated as well. A very anxious parent / carer will almost invariably lead to a very anxious child, which makes for a much harder assessment. A parent’s / carer’s perspective of the child’s problem may differ from that of the clinician; however “a smart mother makes often a better diagnosis than a poor doctor.” (August Bier, 1861-1949.) Remember to always consider the environment ensuring safety for the child and siblings, if appropriate. It is well known that children can ‘compensate’ very well, which means that the normal signs that an adult might show of a steadily deteriorating condition are not always visible, hence initially all paediatric patients should be triaged / assessed as soon as is possible. It is well known that subtle clues missed during such an initial assessment can lead to the child de-compensating rapidly and showing signs of a life threatening nature within a few minutes (an adult might take one or more hours to gradually develop these signs – children usually do not, they take minutes!) 4.2 Initial Primary Assessment of the Paediatric Patient Using the Paediatric Assessment Triangle (PAT) to develop an early general impression:-
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 9 of 36
This PAT system can be used ‘from across the room’ without the need for any equipment or even to ‘lay hands on’ the child. 4.2.1 PAT - Appearance – TICLS (“tickles”)
Characteristic Features to look for
Tone Moving or vigorously resisting examination?
Good muscle tone or limp, listless or flaccid?
Interactiveness How alert? How readily does a stimulus distract?
Grabs for a toy / hand / instrument when offered?
Uninterested in playing / interacting?
Consolability Can be consoled / comforted?
Crying and agitation unrelieved by gentle reassurance?
Look / Gaze Fixes gaze on face?
‘Nobody – home’, glassy eyed stare?
Speech / Cry Cry, strong and spontaneous or weak and high pitched?
Speech content – age appropriate or confused / garbled?
Appearance Work of Breathing
Circulation to skin
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 10 of 36
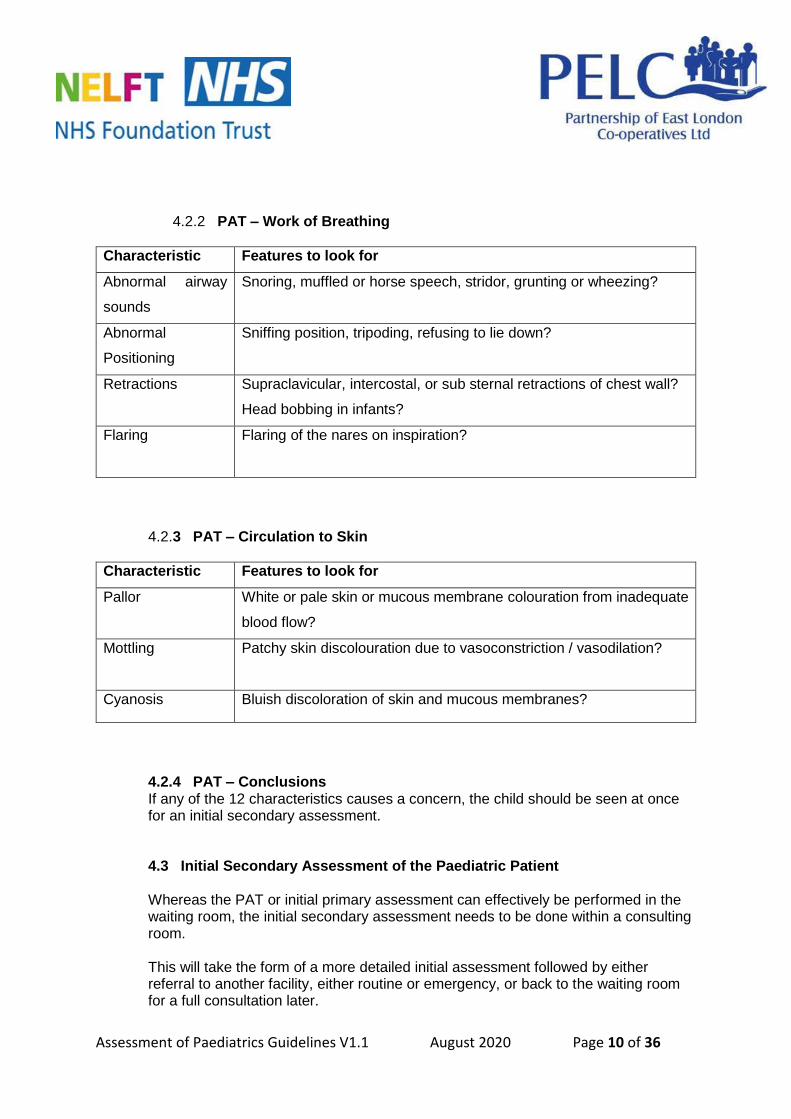
4.2.2 PAT – Work of Breathing
Characteristic Features to look for
Abnormal airway
sounds
Snoring, muffled or horse speech, stridor, grunting or wheezing?
Abnormal
Positioning
Sniffing position, tripoding, refusing to lie down?
Retractions Supraclavicular, intercostal, or sub sternal retractions of chest wall?
Head bobbing in infants?
Flaring Flaring of the nares on inspiration?
4.2.3 PAT – Circulation to Skin
Characteristic Features to look for
Pallor White or pale skin or mucous membrane colouration from inadequate
blood flow?
Mottling Patchy skin discolouration due to vasoconstriction / vasodilation?
Cyanosis Bluish discoloration of skin and mucous membranes?
4.2.4 PAT – Conclusions If any of the 12 characteristics causes a concern, the child should be seen at once for an initial secondary assessment. 4.3 Initial Secondary Assessment of the Paediatric Patient Whereas the PAT or initial primary assessment can effectively be performed in the waiting room, the initial secondary assessment needs to be done within a consulting room. This will take the form of a more detailed initial assessment followed by either referral to another facility, either routine or emergency, or back to the waiting room for a full consultation later.
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 11 of 36
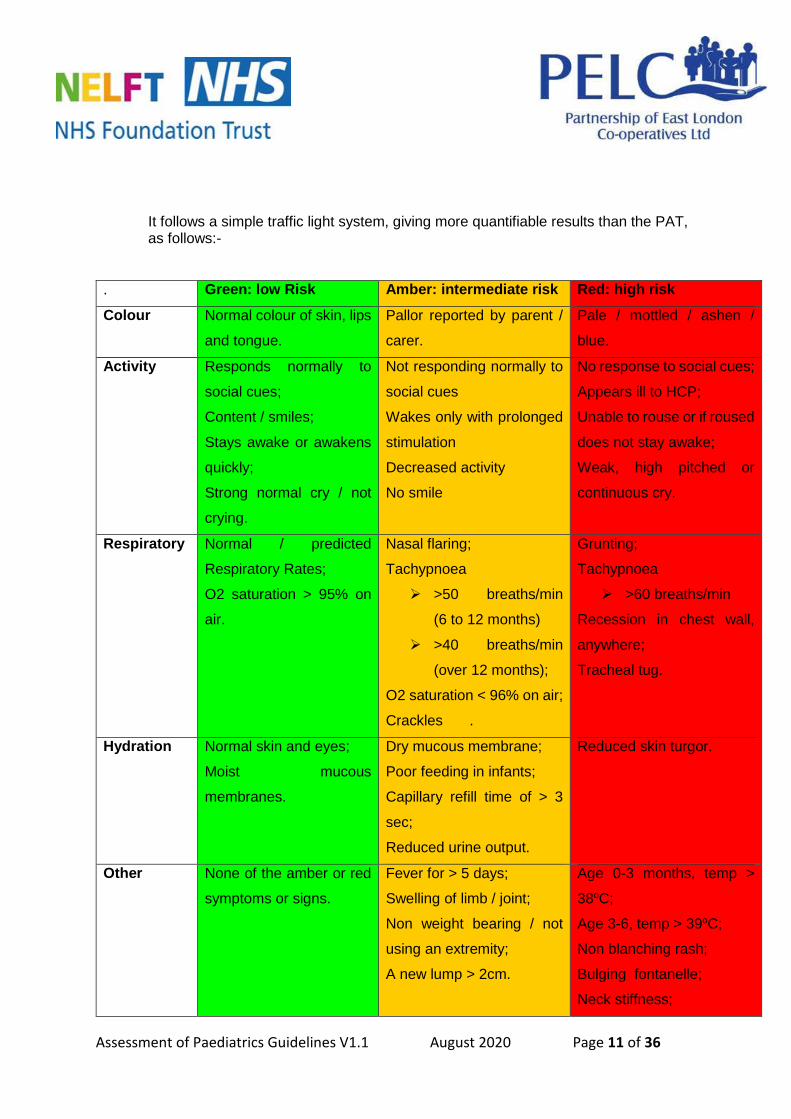
It follows a simple traffic light system, giving more quantifiable results than the PAT, as follows:-
. Green: low Risk Amber: intermediate risk Red: high risk
Colour Normal colour of skin, lips
and tongue.
Pallor reported by parent /
carer.
Pale / mottled / ashen /
blue.
Activity Responds normally to
social cues;
Content / smiles;
Stays awake or awakens
quickly;
Strong normal cry / not
crying.
Not responding normally to
social cues
Wakes only with prolonged
stimulation
Decreased activity
No smile
No response to social cues;
Appears ill to HCP;
Unable to rouse or if roused
does not stay awake;
Weak, high pitched or
continuous cry.
Respiratory Normal / predicted
Respiratory Rates;
O2 saturation > 95% on
air.
Nasal flaring;
Tachypnoea
>50 breaths/min
(6 to 12 months)
>40 breaths/min
(over 12 months);
O2 saturation < 96% on air;
Crackles .
Grunting;
Tachypnoea
>60 breaths/min
Recession in chest wall,
anywhere;
Tracheal tug.
Hydration Normal skin and eyes;
Moist mucous
membranes.
Dry mucous membrane;
Poor feeding in infants;
Capillary refill time of > 3
sec;
Reduced urine output.
Reduced skin turgor.
Other None of the amber or red
symptoms or signs.
Fever for > 5 days;
Swelling of limb / joint;
Non weight bearing / not
using an extremity;
A new lump > 2cm.
Age 0-3 months, temp >
38oC;
Age 3-6, temp > 39oC;
Non blanching rash;
Bulging fontanelle;
Neck stiffness;
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 12 of 36
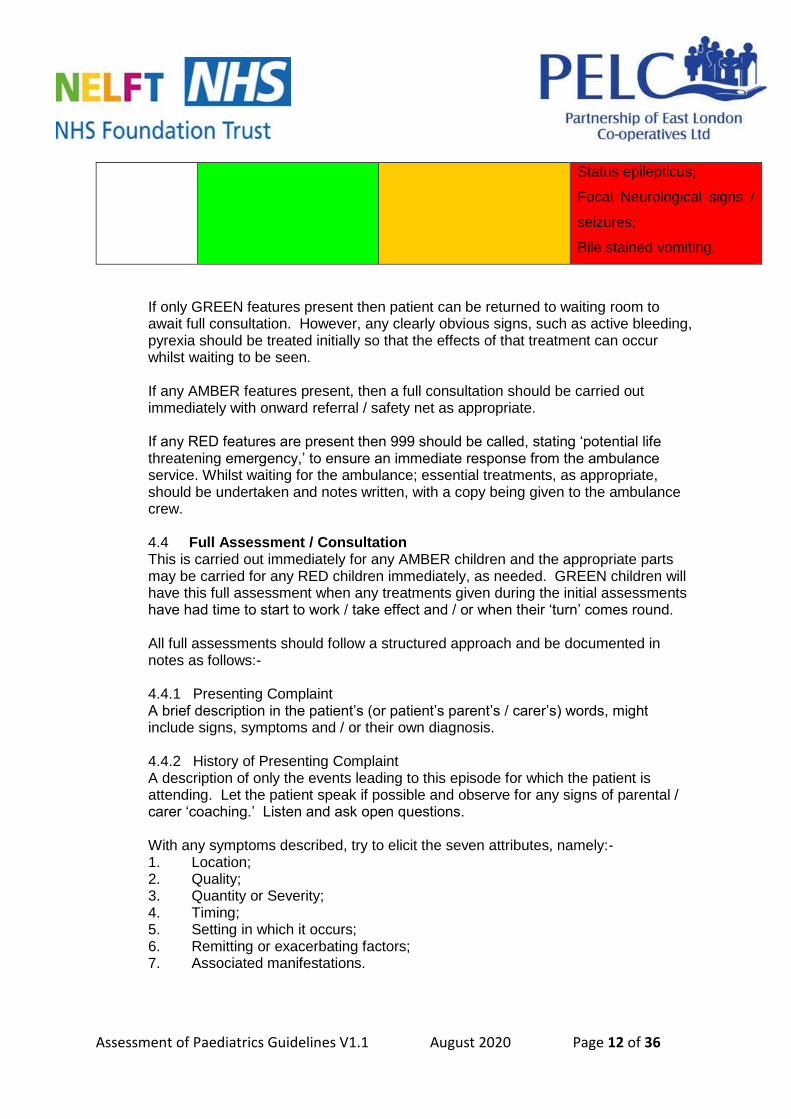
Status epilepticus;
Focal Neurological signs /
seizures;
Bile stained vomiting.
If only GREEN features present then patient can be returned to waiting room to await full consultation. However, any clearly obvious signs, such as active bleeding, pyrexia should be treated initially so that the effects of that treatment can occur whilst waiting to be seen. If any AMBER features present, then a full consultation should be carried out immediately with onward referral / safety net as appropriate. If any RED features are present then 999 should be called, stating ‘potential life threatening emergency,’ to ensure an immediate response from the ambulance service. Whilst waiting for the ambulance; essential treatments, as appropriate, should be undertaken and notes written, with a copy being given to the ambulance crew. 4.4 Full Assessment / Consultation This is carried out immediately for any AMBER children and the appropriate parts may be carried for any RED children immediately, as needed. GREEN children will have this full assessment when any treatments given during the initial assessments have had time to start to work / take effect and / or when their ‘turn’ comes round. All full assessments should follow a structured approach and be documented in notes as follows:- 4.4.1 Presenting Complaint A brief description in the patient’s (or patient’s parent’s / carer’s) words, might include signs, symptoms and / or their own diagnosis. 4.4.2 History of Presenting Complaint A description of only the events leading to this episode for which the patient is attending. Let the patient speak if possible and observe for any signs of parental / carer ‘coaching.’ Listen and ask open questions. With any symptoms described, try to elicit the seven attributes, namely:- 1. Location; 2. Quality; 3. Quantity or Severity; 4. Timing; 5. Setting in which it occurs; 6. Remitting or exacerbating factors; 7. Associated manifestations.
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 13 of 36
4.4.3 Past Medical History This needs to include chronic conditions (whether or not any treatment is being received,) other acute issues (i.e. not those causing the presentation today,) previous hospitalisations, previous infectious diseases and previous injuries. 4.4.4 Pregnancy History Most relevant for children aged under 2 years. Note any variations from the norm. 4.4.5 Birth History Most relevant for children aged under 2 years. Gestation period, type of delivery, analgesia or other drugs used during labour. Note any periods in special care or neonatal intensive care. 4.4.6 Family History Any medical conditions with immediate blood family, i.e., parents, grandparents, uncles, aunts, siblings. 4.4.7 Social History Household set up, number of siblings and adults / other family members. Recent travel overseas. Recent illness of other household members. 4.4.8 Immunisation History Is it up to date (UTD), if not, what is missing and why? 4.4.9 Allergies Not just drugs allergies, but also food allergies, contact allergies; sometimes worth noting immediate blood family allergies. 4.4.10 Parent / Carer and consent Who is with the child, if anyone? Is it an appropriate adult and can informed consent be gained from the patient (if Fraser competent) or from the parent / carer? If relevant, it is also worth noting here if the child uses alcohol, tobacco or other recreational drugs. Smoking by other household members should be noted as well. 4.4.11 Examination The relevant area should be examined and the findings documented. 4.4.12 Diagnostic Tests If appropriate, diagnostic tests should be completed and documented or attached to patient notes. 4.4.13 Impression The Clinician’s impression of the diagnosis or various differential diagnoses’ should be listed. 4.4.14 Plan The treatment to be initiated or the referral to be made should be documented, together with appropriate safety netting.
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 14 of 36
4.5 Common Childhood Illness The list below is not exhaustive, but details some of the more common illnesses and their usual treatments. Some of the conditions listed are technically symptoms of illness, rather than illnesses themselves, but it is often the symptom that causes the child to present for treatment. Often there is no treatment for the condition, but there are symptom relieving treatments available and these are listed where appropriate.- 4.5.1 Asthma Within the walk in centre, asthma presentations will usually be acute exacerbations, rather than queries regarding long term chronic disease management (these queries should be referred back to the GP.) Acute exacerbations will usually result in a red traffic light (see above) which will require immediate treatment, which should follow the patient group directions for salbutamol. 4.5.2 Catarrh This is uncomfortable as it is an excess of mucus in the nose and throat. It may result from a common cold, measles, hayfever, or sinusitis. It could also result from an allergy. The child will have a running nose, cough, may vomit and have ongoing nasal congestion. They may be irritable. Babies may not feed well. Try to ascertain the cause and treat as needed as the child can get very run down and tired. 4.5.3 Chicken Pox This is dealt with in the Skin Conditions Guidelines. 4.5.4 Cold Sores This is dealt with in the Skin Conditions Guidelines. 4.5.5 Conjunctivitis This is dealt with in the Ophthalmic Guidelines. 4.5.6 Cradle cap This is dealt with in the Skin Conditions Guidelines. 4.5.7 Croup Coup in an infection normally resulting from a common cold or bronchitis. It causes a swelling at the back of the throat along with difficulties in breathing. It usually occurs in young children up to around the age of 6. Older children have wider air passages and the condition is less serious and known as laryngitis. Croup can attack at night and can come on rapidly lasting a couple of hours. It will be noticed by a distinctive bark or croaking cough. There may be a shortness of breath or inspiratory stridor. If croup has not triggered a RED response on the traffic light system then treatment is usually symptomatic and, if appropriate, for the underlying condition. 4.5.8 Deafness This is dealt with in the Ear, Nose and Throat Guidelines. 4.5.9 Earache
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 15 of 36
This is dealt with in the Ear, Nose and Throat Guidelines. 4.5.10 Eczema This is dealt with in the Skin Conditions Guidelines. 4.5.11 Fever Due to their immature immune systems and under developed hypothalamus (until around the age of six years,) children are very likely to develop a fever or pyrexia with any infection, from any cause (e.g. bacterial, viral, and fungal.) A fever is the most common reason parents / carers will present a child for health care intervention. Determining the cause of the fever is useful, as it can allow treatment of the cause to initiated, however a diagnosis of pyrexia of unknown origin can sometimes be the only diagnosis given and requires onward referral for further investigation along with a PEWS score. The mainstay of treatment is administration of analgesia for comfort and symptom control. Administration of medication specifically as an antipyretic is no longer recommended (see Paediatric pyrexia NICE guidance), Encourage maintenance of clear fluid intake and remove excess clothing. Follow the patient group directions for paracetamol and ibuprofen. Seek the advice of a paediatrician at an acute hospital, or send direct to A&E if a medical emergency or ‘red’ (or potentially amber) PEWS score/sepsis red flags 4.5.12 Fifth Disease (Erythema Infectiosum) Fifth disease is caused by a virus, human parvovirus B19. It is sometimes called “slapped cheek” disease because of the appearance of the rash. Signs and symptoms of fifth disease may include: - • Flu-like symptoms (e.g., runny nose, sore throat, mild body weakness and joint pain, fever) may be present about 7 days before onset of rash • Raised, red rash that first appears on child’s cheeks • The lace-like rash spreads to the rest of the body after 1 – 4 days, first on torso and arms, and then on to the rest of the child’s body • After the rash fades, it may continue to re-appear for 1 – 3 weeks when child is exposed to sunlight or heat (e.g., bathing). Treatment is supportive only and the main concerns are:- • Pyrexia which should be treated by removing excessive clothing. • Dehydration, treated with fluids orally. If any complications occur, discuss with a paediatrician at an acute hospital. 4.5.13 Gastro Intestinal Conditions 4.5.13.1 Campylobacteriosis Campylobacter bacteria are a common cause of gastrointestinal infection in both children and adults, often in the summer and autumn. There are several types of campylobacter bacteria that cause illness. The most common cause of illness in humans is Campylobacter jejuni. Signs and symptoms of campylobacteriosis may include: • Abdominal pain and cramping • Diarrhoea (may be bloody)
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 16 of 36
• Nausea and vomiting • Malaise • Fever Illness usually lasts 2 – 5 days and is highly infectious. See Diarrhoea and Vomiting guidelines. 4.5.13.2 Constipation Constipation begins once a baby is onto solid foods. To avoid constipation the child should be eating a healthy diet which includes fresh fruit and vegetables and a good daily intake of water. If the child is constipated it can be very painful. They will have hard pebble-like stools, pain in the lower stomach and there may be blood in the nappy or underwear due to straining. Ensure the child eats food containing fibre (wholemeal bread, fruit, and bran cereals). Continual constipation should be referred to G.P. Occasional constipation should, if possible be relieved by dietary means, but if necessary over the counter medicines can be used with pharmacist advice. 4.5.13.3 Diarrhoea This is caused by an irritation of the intestines – frequent watery stools will be passed which can lead to dehydration and should be taken seriously in young children. Less than 5 years old, with diarrhoea, especially if accompanied by vomiting should be seen by a Paediatrician if it occurs for over 12 hours; 5 years and over, the period is 24 hours. Parents / carers should be encouraged to give them frequent little and often amounts of clear liquid, but avoiding acidic drinks. Food or milk should be avoided until they feel better and then introduce simple foods such as plain/dry and soups. High levels of hand/toilet hygiene for child and parent / carer must be stressed. Avoid anti-diarrhoea treatments. 4.5.13.4 E. Coli (Escherichia Coli): Diarrhoea Illness and Haemolytic Uremic Syndrome There are many strains of E. coli bacteria and most of them are harmless. Others cause diarrhoea when a toxin is produced by the bacteria. Signs and symptoms of E. coli infection may include:- • Loose, watery diarrhoea than may change to bloody diarrhoea • Mild to severe abdominal cramps • Vomiting • Fever (usually less than 38.5°C) Most people with E. coli infections recover completely within 5 – 7 days. Very young children and the elderly are more likely to develop severe illness and haemolytic uremic syndrome (HUS). HUS is an acute disease characterized by haemolytic anaemia, acute renal failure (uraemia), and a low platelet count. Symptoms of HUS may include: - • Decreased urine output • Irritation • Fatigue • Pale skin Recovery is usually spontaneous but child may need hospitalization and dialysis during acute illness. About 5 – 10% of people who develop HUS will die. Children
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 17 of 36
between the ages of 6 months and 4 years are most likely to develop HUS. If HUS is suspected, refer to a paediatrician at an acute hospital, via A&E if a medical emergency. 4.5.13.5 Food Poisoning See Diarrhoea guidelines above. 4.5.13.6 Vomiting Nearly all children will get diarrhoea (see guideline above) and will vomit at some stage. Parents / cares are usually very concerned; however this is usually not a cause for concern in its own right. Always bear in mind that it could be a symptom of a more serious underlying condition (including medical emergencies.) Points to consider are: - • The illness will most probably be brief • It could however make the child dehydrated (watch this carefully, especially with babies) – at least x3 wet nappies/urine with no urine for >8hrs = Paediatric ED for assessment. • When dehydrated babies and children first become irritable then loose interest and become lethargic. Their eyes can be sunken and skin very dry. You may be able to pinch some skin and instead of it bouncing back, it will remain upright. • Most mild dehydration can be treated at home – make sure the child is given plenty of fluids. They may not readily accept it but always make sure it is regularly offered; moisten their lips. • In more severe cases a rehydration fluid can be given – which can be bought over the counter from a pharmacist. It contains a mixture of salt and sugars which is dissolved in water. • If in any doubt always discuss with the on call paediatrician at an acute hospital. 4.5.14 German measles This is dealt with in the Skin Conditions Guidelines. 4.5.15 Glue Ear This is dealt with in the Ear, Nose and Throat Guidelines. 4.5.16 Hayfever This is similar to asthma except that it is an allergy whose reaction occurs in the nose and eyes. It will cause sneezing, a runny nose, itchy and watery eyes. Spring and summer are the worst months for hayfever and is due to pollen from flowers and grasses. Some hayfevers are all year round and are due to pets or house dust and mites. Treatment is usually limited in the acute phase to symptomatic relief from over the counter medicines. However see the Patient Group Direction on Chlorphenamine. 4.5.17 Hand, foot and mouth disease. Hand, foot, and mouth disease is caused by a coxsackie virus. It occurs mainly in the summer and early autumn and is most common in children under 10 years of age. Signs and symptoms of hand, foot, and mouth disease usually start suddenly and may include: -
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 18 of 36
• Fever • Sore throat • Headache • Small painful blisters inside the mouth on tongue and gums (last 4 to 6 days) • Blisters may appear on the palms of child’s hands, on their fingers, and on the soles of their feet for 7 to 10 days It is possible to have the infection and not have any symptoms. Treatment is supportive only and the main concerns are:- • Dehydration, treated with fluids orally. Sepsis should always be excluded. If any complications occur, discuss with a paediatrician at an acute hospital. 4.5.18 Head Lice Head Lice are tiny parasitic insects which live on human hair. They are irritating but can be eradicated and are not serious. Detector combs can be bought from the chemist – wet comb the child’s hair twice a week. There is also over the counter louse repellent spray and medicated shampoo, but this must not be used if your child has asthma or under the age of 2. The spray / shampoo kills the lice not the nits (louse eggs,) so two treatments must be applied one week apart, as all eggs hatch within seven days. DO NOT use either of the above unless the child has head lice. The child will be scratching their scalp, there will be redness on the back of the neck, and nits will be seen while combing the hair (tiny white pearl like eggs at the root of the hair). 4.5.19 Heat Rash This is dealt with in the Skin Conditions Guidelines. 4.5.20 Impetigo This is dealt with in the Skin Conditions Guidelines. 4.5.21 Influenza Influenza (the flu) is a respiratory illness caused by Influenza A and Influenza B viruses. Influenza season in the U.K. is usually November through April. Signs and symptoms of influenza may include: - • Fever • Cough, sneezing, runny nose • Headache • Body aches and pain • Exhaustion • Sore throat • Nausea, vomiting, and diarrhoea are more common in children than adults. Influenza is most serious for babies less than 2 years of age and those with chronic illnesses. Treatment is supportive only and the main concerns are: • Persistent pyrexia >38’ • Dehydration, treated with fluids orally. If any complications occur, discuss with a paediatrician at an acute hospital.
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 19 of 36
4.5.22 Laryngitis This is dealt with in the Ear, Nose and Throat Guidelines. 4.5.23 Measles This is dealt with in the Skin Conditions Guidelines. 4.5.24 Meningitis Meningitis is rare but it is dangerous and although the HIB vaccine protects against one type of bacterial meningitis, there are several forms of the disease which do not have vaccines. However, if it is detected and treated early, the majority of children who contract meningitis make a full recovery. The symptoms in babies are as follows: - • persistent high temperature • refusing feeds, vomiting, high-pitched moaning cry • convulsions • difficult to wake • pale, blotchy or mottled skin, non- blanching rash of any description • bulging of the fontanelle (the soft spot on top of the head) The symptoms in toddlers and older children are as follows: • headache • vomiting • high temperature • neck stiffness (often shown as reluctance to put chin on chest) • pain in the joints • drowsiness • confusion • dislike of bright lights (photophobia) • rash of purple spots or bruises (press a glass over the rash to see if it turns white. If it doesn’t, it could be meningitis.) Remember, not all symptoms appear at one time. This is a medical emergency and should be referred to A&E via 999. 4.5.25 Molluscum Contagiosum Molluscum contagiosum is a viral infection of the skin infection caused by a poxvirus. Signs and symptoms of molluscum contagiosum may include: - • Tiny painless bumps on the skin that grow over several weeks • Bumps become small, waxy, pinkish-white, raised lesions which may have a small crater in the centre of them • Bumps may become swollen and red as part of the body’s response to the virus. In children, the bumps most often appear on the face, body, legs, and arms. Without treatment, the infection usually lasts 6 months to 2 years. Treatment is usually painful (hence often not done in children) and patients should be referred to their own G.P. for follow up if they wish. 4.5.26 Mouth Ulcers
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 20 of 36
Ulcers can occur due to stress, a physical injury such as biting the cheek or from an infection. Children can be stressed if they are to embark on something unusual or something they feel uncomfortable with – sometimes the beginning of school. In these cases ulcers are small creamy-white lumps in the mouth anywhere on the tongue, gums or lining of the mouth. They will disappear but may be painful and can easily reoccur. If the inside of the mouth is injured through a bite or knock, even a rough tooth rubbing against the side of the mouth can cause an ulcer. Ulcers can appear as a red/yellow indented sore. These will again be painful but will clear up within a fortnight. If an infection is present – may be due to a cold sore or virus – the ulcer will look like white blisters which may also cause a fever. Nothing can really be done about ulcers – they are painful and may cause a lack of appetite – over the counter treatments are available depending upon the age of the child. Salt water mouth washes can be helpful, but only if child is old enough to know not to swallow. 4.5.27 Mumps Mumps is caused by a virus and lasts about ten days. The child will feel unwell for a day or two before any major symptoms appear. The symptoms will be: - • Pain when chewing or swallowing acidic liquids – fruit juices • Pain around the ear • Headaches • Fever • Chills • Poor appetite / difficulty in swallowing • Swelling starting under the jaw by the ear and may be on one side or both Treat is support only, pyrexia control and fluids (not acidic, i.e. Water only) if complications occur then refer to paediatrics at acute hospital or A&E if medical emergency. 4.5.28 Nose Bleeds (Epistaxis.) This is dealt with in the Ear, Nose and Throat Guidelines. 4.5.29 Ringworm This is dealt with in the Skin Conditions Guidelines. 4.5.30 Roseola Infantum (“Sixth Disease”) An acute rash disease caused by a virus. There are many viruses that can cause roseola. The most common virus is human herpesvirus-6 virus. Signs and symptoms of roseola may include: - • Fever (usually ≥ 39.5°C) appears suddenly and lasts 3 – 5 days • Febrile seizures may occur • Swelling of eyelids may occur • Rash usually develops as fever is resolving • Rosy – pink rash develops first on neck and chest, and then spreads to rest of the body
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 21 of 36
• The spots (rash) turn white if you gently press on them and they may have a lighter colour ring around them • Rash usually lasts 1 – 2 days Roseola occurs most commonly between the ages of 6 months and 2 years. It is rarely seen after 4 years of age. Treatment is supportive only and the main concerns are:- • Pyrexia which should be treated with an over the counter anti-pyretic and • Dehydration, treated with fluids orally. If any complications occur, discuss with a paediatrician at an acute hospital. 4.5.31 Scabies This is dealt with in the Skin Conditions Guidelines. 4.5.32 Sore Throat This is dealt with in the Ear, Nose and Throat Guidelines. 4.5.33 Streptococcal Infections: Scarlet Fever and Strep. Throat This is dealt with in the Ear, Nose and Throat Guidelines. 4.5.34 Teething A baby’s teeth will come through at about 6 months. By the time they are 18 months they will usually have a set of first teeth. Some children’s teeth are a little later, some earlier. As the teeth come through the baby will dribble a lot more and want to bite everything in sight. They may be irritable and become more ‘clingy’ than usual. Over the counter preparations are available, a pharmacist will advise on a soothing gel to rub on the babies teeth or give them a teething object that will be a comfort. Some of these can be left in the fridge and the coolness provides further comfort. Occasionally a mild fever can be caused with redness of the cheeks or cheek, depending on where the tooth is cutting. This can be treated with an over the counter analgesic. . 4.5.35 Tonsillitis This is dealt with in the Ear, Nose and Throat Guidelines. 4.5. 36 Whooping Cough This is a viral infection. Whooping Cough begins like a common cold and cough. The cough gradually gets worse and coughing bouts begin. These are exhausting and can make it difficult to breathe and cause airway compromise and vomiting. The child may also have a slight fever, runny nose, aches and pains and feel generally run down. They may also be very tired as coughing may keep them awake at night. Whooping Cough can be very dangerous in babies – it is rare however as immunisation in now routine. A severe attack can damage the lungs and cause bronchial infections. Vomiting can also cause dehydration.
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 22 of 36
Any child suspected of whooping cough should be referred to paediatrics at an acute hospital or to A&E if a medical emergency. 4.5 37 Urinary Tract Infection in Children and Young Adults
Urinary tract infection is a common bacterial infection in infants, children and young
people. A urinary tract Infection is defined by a combination of clinical features and
the presence of bacteria in the urine. Around 1 in 10 girls and 1 in 30 boys will have
had a urinary tract infection by the age of 16 years.
Making the diagnosis can be difficult because the presenting symptoms or signs
(fever, irritability and vomiting) are non-specific and are commonly seen in many
childhood viral illnesses, particularly in younger children. A severe infection can make
a child extremely unwell and sometimes have serious consequences; even minor
infections can be distressing. Repeated episodes of acute urinary tract infection are
distressing to infants, children and young people, and their parents or carers.
Although most infants, children and young people recover promptly from a urinary
tract infection and have no long-term complications, there is a small subgroup at risk
of significant morbidity.
Prompt and accurate diagnosis of urinary tract infection is essential, and it is
important to recognise and treat recurrent infection.
The following guidance should be followed: NICE 2018
Training and Competencies
The quality standard should be read in the context of national, local guidelines and
current PGD on training and competencies. All healthcare practitioners involved in
assessing, caring for and treating infants, children and young people with a urinary
tract infection should have sufficient and appropriate training and competencies to
deliver the actions and interventions described in the quality standard.
Statement 1. Infants, children and young people presenting with unexplained fever of
38°C or higher have a urine sample tested within 24 hours
Statement 2. Infants, children and young people with a urinary tract infection have
risk factors for urinary tract infection and serious underlying pathology recorded as
part of their history and examination.
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 23 of 36
Statement 3. Infants, children and young people with a urinary tract infection caused
by coliform bacteria have results of microbiology laboratory testing differentiated by
Escherichia coli (E. coli) or non-E. coli organisms.
Statement 4. Children and young people who have had a urinary tract infection are
given information about how to recognise re-infection and to seek medical advice
straight away.
If a urine sample cannot be obtained then a referral to acute services or own GP
should be made within the 24 hour time frame recommended.
All urine samples that are tested at the WIC via dipstick method to be documented
and a copy of the results provided to the patient to give to own GP.
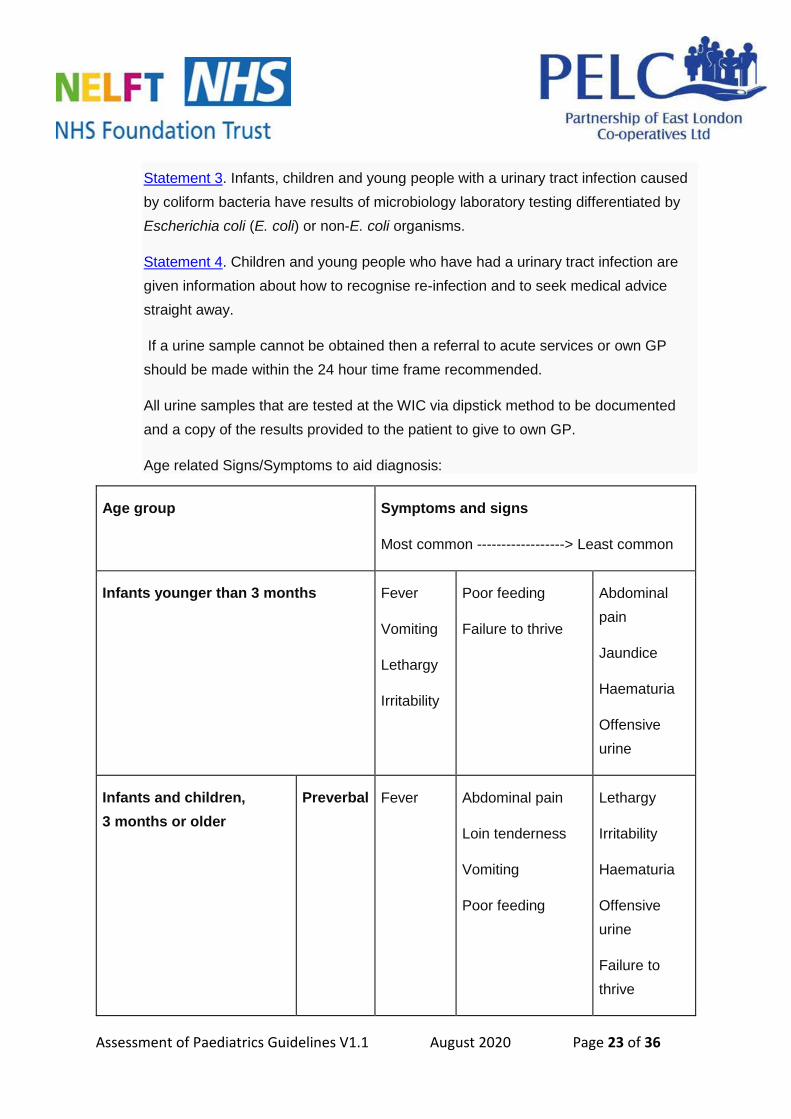
Age related Signs/Symptoms to aid diagnosis:
Age group Symptoms and signs
Most common ------------------> Least common
Infants younger than 3 months Fever
Vomiting
Lethargy
Irritability
Poor feeding
Failure to thrive
Abdominal
pain
Jaundice
Haematuria
Offensive
urine
Infants and children,
3 months or older
Preverbal Fever Abdominal pain
Loin tenderness
Vomiting
Poor feeding
Lethargy
Irritability
Haematuria
Offensive
urine
Failure to
thrive
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 24 of 36
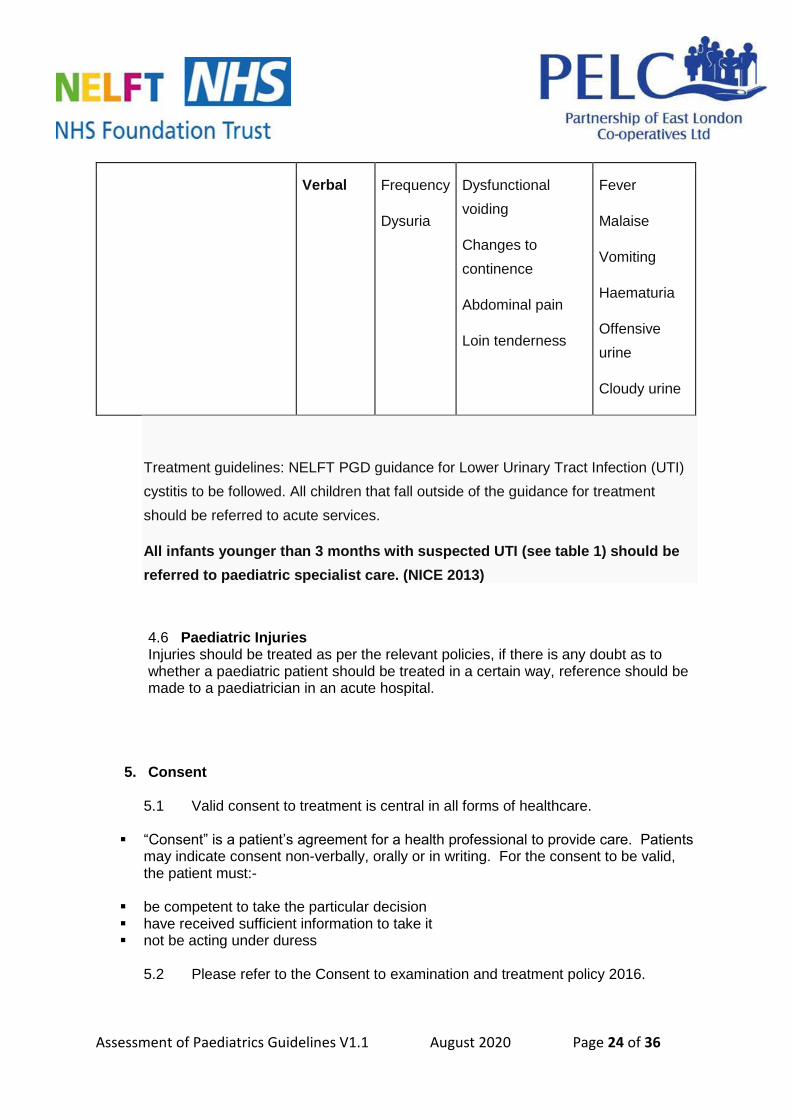
Verbal Frequency
Dysuria
Dysfunctional
voiding
Changes to
continence
Abdominal pain
Loin tenderness
Fever
Malaise
Vomiting
Haematuria
Offensive
urine
Cloudy urine
Treatment guidelines: NELFT PGD guidance for Lower Urinary Tract Infection (UTI)
cystitis to be followed. All children that fall outside of the guidance for treatment
should be referred to acute services.
All infants younger than 3 months with suspected UTI (see table 1) should be
referred to paediatric specialist care. (NICE 2013)
4.6 Paediatric Injuries Injuries should be treated as per the relevant policies, if there is any doubt as to whether a paediatric patient should be treated in a certain way, reference should be made to a paediatrician in an acute hospital.
5. Consent
5.1 Valid consent to treatment is central in all forms of healthcare.
“Consent” is a patient’s agreement for a health professional to provide care. Patients may indicate consent non-verbally, orally or in writing. For the consent to be valid, the patient must:-
be competent to take the particular decision have received sufficient information to take it not be acting under duress
5.2 Please refer to the Consent to examination and treatment policy 2016.
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 25 of 36
5.3 If there is any indication that the patient may lack mental capacity to consent a mental capacity assessment must be carried out. Please refer to your specific business unit mental capacity act policies.
5.4 Consent and access to treatment for children and young people: please refer
to the Consent to examination and treatment policy 2016.
6. Implementation process
6.1 Staff will be made aware of any new approved policies/procedures/guidelines
via the Trust weekly newsletter. Quality and patient safety team will be responsible for ensuring newly approved documents are sent to the communications team in order for them to insert into the Trust weekly newsletter.
6.2 All senior managers/heads of service/team leaders need to ensure new policies and procedures are placed on team meeting agendas for discussion. There is an expectation that the team leader will develop local systems to ensure their staff are instructed to read all relevant policies and to identify any outstanding training deficits.
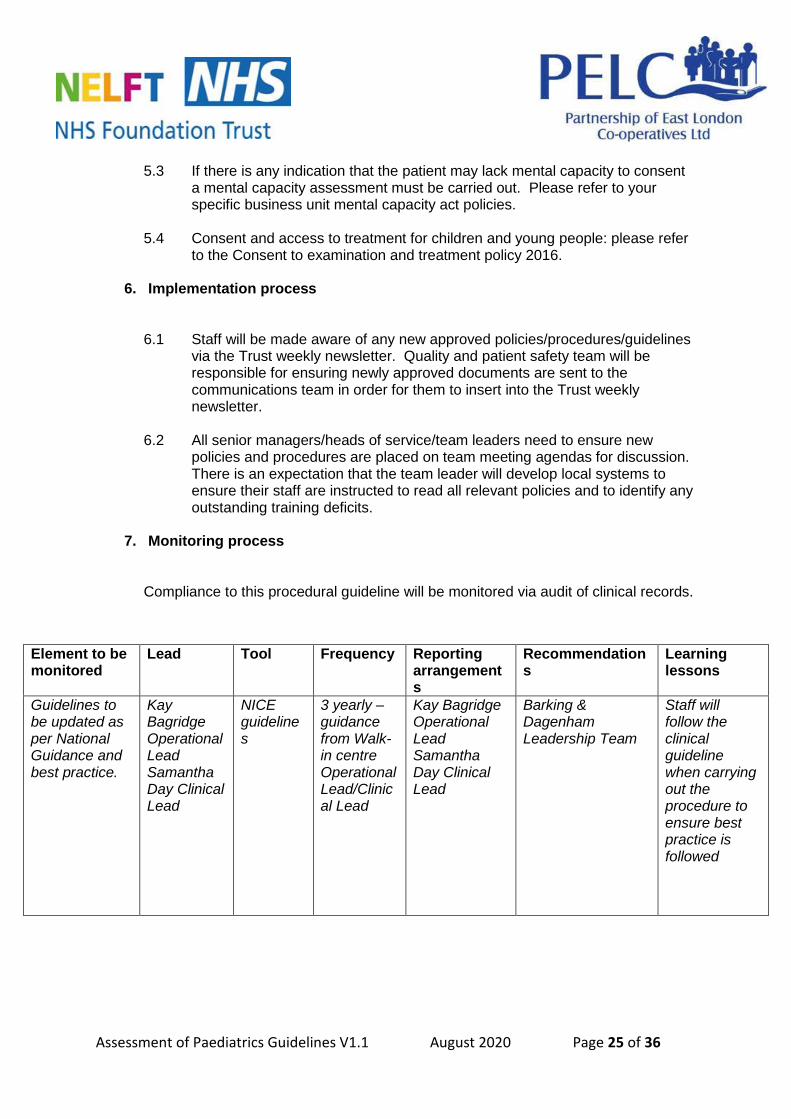
7. Monitoring process
Compliance to this procedural guideline will be monitored via audit of clinical records.
Element to be monitored
Lead Tool Frequency Reporting arrangements
Recommendations
Learning lessons
Guidelines to be updated as per National Guidance and best practice.
Kay Bagridge Operational Lead Samantha Day Clinical Lead
NICE guidelines
3 yearly – guidance from Walk-in centre Operational Lead/Clinical Lead
Kay Bagridge Operational Lead Samantha Day Clinical Lead
Barking & Dagenham Leadership Team
Staff will follow the clinical guideline when carrying out the procedure to ensure best practice is followed
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 26 of 36
8. Equality statement
This procedure/guideline reflects the organisation’s determination to ensure that all parts of our community have equality of access to services and that everyone receives a high standard of service as a service user, a carer or employee. This procedure/guideline anticipates and encompasses the Trust’s commitment to prevent discrimination on any illegal or inappropriate basis and recognise and respond to the needs of individuals based on good communication and best practice. We recognise that some groups of the population are more at risk of discrimination or less able to access to services than others and that services can often unintentionally put barriers in place that can limit or prevent access. The organisation is continually working to prevent this from happening.
9. External references BC Centre for Disease Control (2009), electronic resource - http://www.bccdc.ca/NR/rdonlyres/8061A728-C969-4F38-9082-B0296EF2A128/0/Epid_GF_childhood_quickguide_may_09.pdf&sa=U&ei=3fvZT9uBDu_B0gWq0-SiBA&ved=0CBEQFjAA&usg=AFQjCNFF_lws-facIsdHYi5iUtQ75RmknA/ accessed 13th June 2012 Bickley, L.S., (2009) Bates’ guide to Physical Examination and History Taking, 10th Ed., Wolters Kluwer, Philadelphia. BNF (2019), electronic resource - http://www.medicinescomplete.com/mc/bnf/current/ accessed December 2018. BNF for Children 2011–2012 (2011), electronic resource - http://www.medicinescomplete.com/mc/bnfc/current/ accessed December 2018. Chamley, C.A., Carson, P., Randall, D. and Sandwell, M. (2005) Developmental Anatomy and Physiology of Children, Churchill Livingstone, Edinburgh Dieckmann, R.A. (ed.) (2006) Pediatric Education for Prehospital Professionals, 2nd Ed., Jones and Bartlett Publishers, Sudbury Dundee University (2012), electronic resource - http://gptraining.dundee.ac.uk/docs/Educators%20Page/Common%20Childhood%20Illness.ppt#256,1,Common Childhood Illness/ accessed 13th June 2012. Egton Medical Information Systems Limited (2012), electronic resource - http://www.patient.co.uk/ accessed 13th June 2012. Gill, D. and O’Brien, N., (2007) Paediatric Clinical Examination Made Easy, 5th Ed., Churchill Livingstone, Edinburgh. Hopcroft, K., and Forte, V., (2014) Symptom Sorter, 5th Ed., Radcliffe Publishing, Oxford. Moulton, C. and Yates, D., (1999) Emergency Medicine, 2nd Ed., Blackwell Science, Oxford.
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 27 of 36
Munro, J. and Edwards, C.R.W., (eds.) (1995) Macleod’s Clinical Examination, 9th Ed., Churchill Livingstone, Edinburgh NHS Evidence (2012), electronic resource - https://www.evidence.nhs.uk/ accessed December 2018.
Fever in under 5s: assessment and initial management – NICE (Aug 2018) NICE (2013) urinary Tract Infection in Children and Young Adults https://www.nice.org.uk/guidance/qs36 accessed 09th August 2017 Patient Group Directions for the supply and administration of Antibiotics 10-2018-04 2019 10.Training
All staff undertaking autonomous clinical consultations will have skills in advanced assessment. Competency is assessed and maintained through completion of a specific clinical competency framework supported by additional training where identified. Where appropriate training is provided to use the necessary Patient Group Directions. Training will be accessed via the Training and Education Department and recorded within the practitioner’s file.
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 28 of 36
Stakeholder form
Stakeholder title
Date sent to Stakeholders C
om
men
ts
rece
ived
Retu
rned
,
no
co
mm
en
ts
No
t re
turn
ed
Equality and Diversity Manager
Leadership Team – Basildon and Brentwood Locality
Leadership Team – Barking and Dagenham Locality
Leadership Team – Havering Locality
Leadership Team – Redbridge Locality
Leadership Team – Thurrock Locality
Leadership Team - Waltham Forest Locality
Leadership Team - MHIPAD
Chief Nurse Group
Compliance Team (QPS) [email protected]
Consultant in Old Age Liaison Psychiatry and Associate Medical Director Stephen.O'[email protected]
Head of Health and Safety
Head of Information Governance
Associate Director of Human Resources [email protected]
Director of Nursing (Clinical Effectiveness – [email protected]
Director of Nursing (Patient Safety, BTUH Health Economy) – [email protected]]
Director of Nursing (Patient Experience) [email protected]
Associate Director of Nursing Quality & Patient Safety [email protected]
Finance [email protected]
Performance [email protected]
Estates – Havering/Basildon/Thurrock [email protected]
Interim Head of Estates (WF/Red/B&D) [email protected]
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 29 of 36
Communication team [email protected]
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 30 of 36
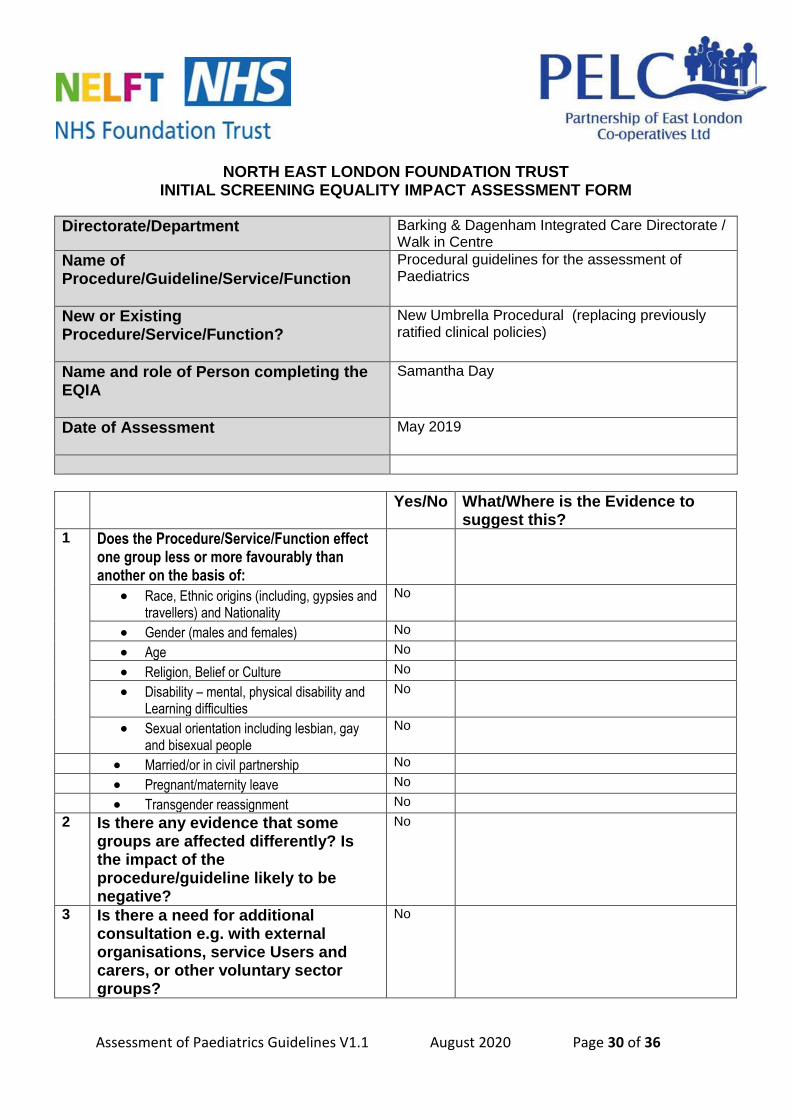
NORTH EAST LONDON FOUNDATION TRUST INITIAL SCREENING EQUALITY IMPACT ASSESSMENT FORM
Directorate/Department
Barking & Dagenham Integrated Care Directorate / Walk in Centre
Name of Procedure/Guideline/Service/Function
Procedural guidelines for the assessment of Paediatrics
New or Existing Procedure/Service/Function?
New Umbrella Procedural (replacing previously ratified clinical policies)
Name and role of Person completing the EQIA
Samantha Day
Date of Assessment
May 2019
Yes/No What/Where is the Evidence to suggest this?
1 Does the Procedure/Service/Function effect one group less or more favourably than another on the basis of:
Race, Ethnic origins (including, gypsies and travellers) and Nationality
No
Gender (males and females) No
Age No
Religion, Belief or Culture No
Disability – mental, physical disability and Learning difficulties
No
Sexual orientation including lesbian, gay and bisexual people
No
Married/or in civil partnership No
Pregnant/maternity leave No
Transgender reassignment No
2 Is there any evidence that some groups are affected differently? Is the impact of the procedure/guideline likely to be negative?
No
3 Is there a need for additional consultation e.g. with external organisations, service Users and carers, or other voluntary sector groups?
No
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 31 of 36
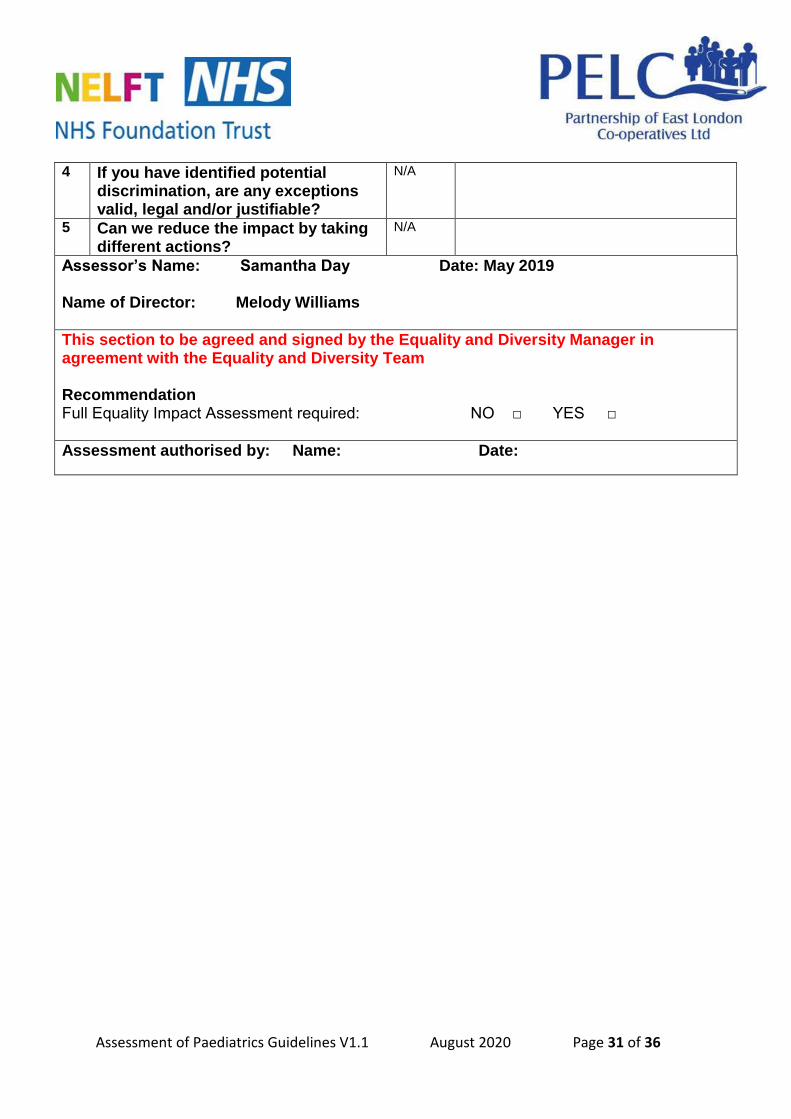
4 If you have identified potential discrimination, are any exceptions valid, legal and/or justifiable?
N/A
5 Can we reduce the impact by taking different actions?
N/A
Assessor’s Name: Samantha Day Date: May 2019 Name of Director: Melody Williams
This section to be agreed and signed by the Equality and Diversity Manager in agreement with the Equality and Diversity Team Recommendation Full Equality Impact Assessment required: NO □ YES □
Assessment authorised by: Name: Date:
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 32 of 36
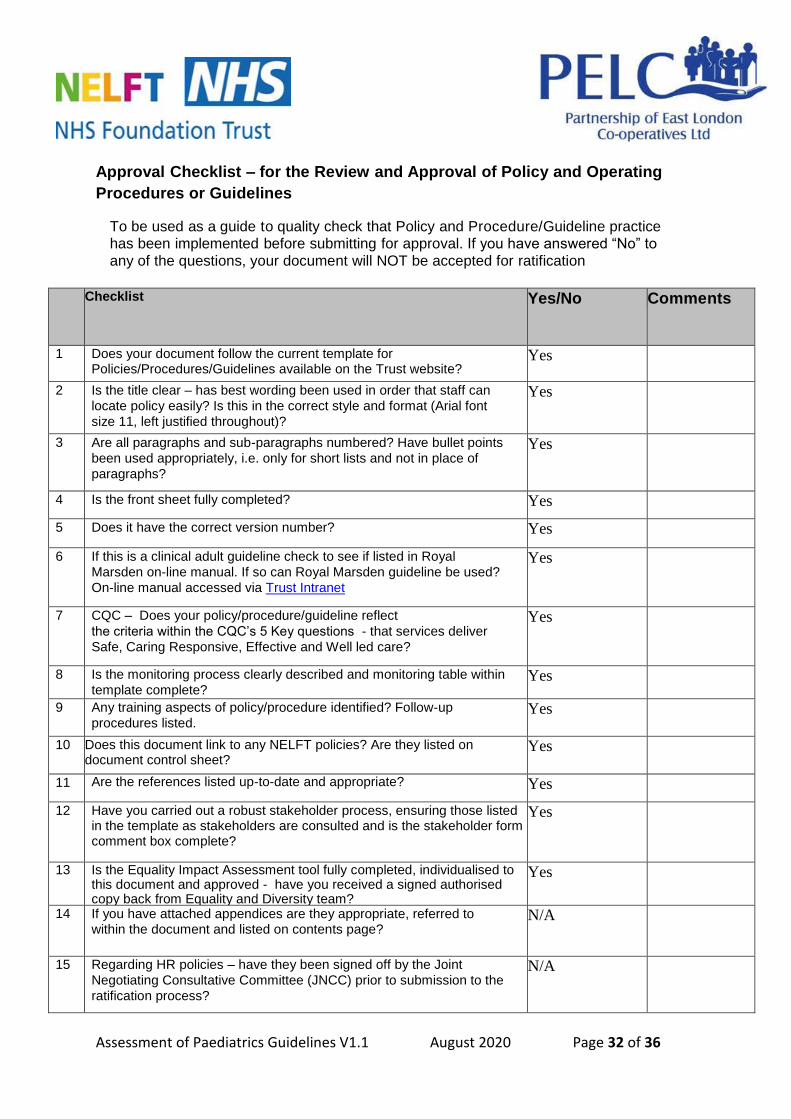
Approval Checklist – for the Review and Approval of Policy and Operating
Procedures or Guidelines
To be used as a guide to quality check that Policy and Procedure/Guideline practice has been implemented before submitting for approval. If you have answered “No” to
any of the questions, your document will NOT be accepted for ratification
Checklist
Yes/No Comments
1 Does your document follow the current template for Policies/Procedures/Guidelines available on the Trust website?
Yes
2 Is the title clear – has best wording been used in order that staff can
locate policy easily? Is this in the correct style and format (Arial font
size 11, left justified throughout)?
Yes
3 Are all paragraphs and sub-paragraphs numbered? Have bullet points
been used appropriately, i.e. only for short lists and not in place of
paragraphs?
Yes
4 Is the front sheet fully completed? Yes
5 Does it have the correct version number? Yes
6 If this is a clinical adult guideline check to see if listed in Royal
Marsden on-line manual. If so can Royal Marsden guideline be used?
On-line manual accessed via Trust Intranet
Yes
7 CQC – Does your policy/procedure/guideline reflect
the criteria within the CQC’s 5 Key questions - that services deliver
Safe, Caring Responsive, Effective and Well led care?
Yes
8 Is the monitoring process clearly described and monitoring table within
template complete? Yes
9 Any training aspects of policy/procedure identified? Follow-up
procedures listed. Yes
10 Does this document link to any NELFT policies? Are they listed on document control sheet?
Yes
11 Are the references listed up-to-date and appropriate? Yes
12 Have you carried out a robust stakeholder process, ensuring those listed in the template as stakeholders are consulted and is the stakeholder form comment box complete?
Yes
13 Is the Equality Impact Assessment tool fully completed, individualised to this document and approved - have you received a signed authorised copy back from Equality and Diversity team?
Yes
14 If you have attached appendices are they appropriate, referred to within the document and listed on contents page?
N/A
15 Regarding HR policies – have they been signed off by the Joint
Negotiating Consultative Committee (JNCC) prior to submission to the
ratification process?
N/A
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 33 of 36
16 16
Finally have you carried out a final proof-read, checked all spellings and ensured your document is accurate and ready for publication?
Yes
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 34 of 36
LEADERSHIP TEAM APPROVAL SHEET
Procedure/Guideline title:
Assessment of Paediatrics
Author: Kay Bagridge Samantha Day Sarah Collins Nurse Practitioner
Assistant/Associate Director approval
Sangita Lall
Once the form has been agreed/not agreed for ratification by Leadership team it should be sent to [email protected] as confirmation of approval
Meeting Date of meeting
Chair name and title Signature of LT Chair
Ap
pro
ved
?
Y /
N
Reason for non-approval
Leadership Team
Assessment of Paediatrics Guidelines V1.1 August 2020 Page 35 of 36

Addendum
Date Section Change Agreed by
Related Documents











