Ventricular Function Assessment of mitral annular dynamics during diastole by Doppler tissue imaging: Comparison with mitral Doppler inflow in subjects without heart disease and in patients with left ventricular hypertrophy Leonardo Rodriguez, MD, Mario Garcia, MD, Miguel Ares, MD, Brian P. Griffin, MD, Satoshi Nakatani, MD, and James D. Thomas, MD Cleveland, Ohio The purpose of this study was to determine the normal pat- tern and magnitude of mitral annular velocities in diastole by Doppler tissue imaging (DTI) and to assess whether this is altered in patients with left ventricular hypertrophy. Mitral annulus velocities were measured by DTI. Peak and time- velocity integral were measured from the DTI tracings and the timing of the velocities in relation to electrocardiogram. DTI was compared with M-mode echo of the annulus and mitral inflow Doppler velocities, Integrated annular veloci- ties by DTI correlated with the annular displacement. Early diastolic velocities decreased with age and in patients with left ventricular hypertrophy. In the hypertrophy group, early diastolic velocities were significantly lower than normal even after correcting for age. Patients with left ventricular hypertrophy also showed a delay in peak early diastolic mi- tral annular velocity (5.5 ± 21 msec after the E wave). In conclusion, mitral annular velocity in diastole is readily re- corded by DTI. The magnitude and the pattern of these velocities are significantly altered by age and by left ventric- ular hypertrophy. This method provides a new insight into diastolic filling events and may prove useful in detecting abnormal diastolic function. (AM HEARTJ 1996;131:982-7.) Noninvasive evaluation of diastolic function is an important role of clinical echocardiography. Mitral inflow velocities are commonly used to evaluate From the Cardiovascular Imaging Center, Department of Cardiology, Cleveland Clinic Foundation. Supported in part by the Fondo de Inversiones Sanitarias, Spain, the Uehara Memorial Foundation, Tokyo, Japan, Grant-in-Aid 930133380 from the American Heart Association, and an equipment grant from Acu- son, Inc., Mountain View, Calif. Received for publication Aug'. 1, 1995; accepted Sept. 12, 1995. Reprint requests: Leonardo Rodriguez, MD, Desk F-15, Division of Cardi- ology, The Cleveland Clinic Foundation, 9500 Euclid Ave., Cleveland OH 44195. Copyright © 1996 by Mosby-Year Book, Inc. 0002-8703/96/$5.00 + 0 4/1/70745 diastolic function; these velocities are easily recorded and offer useful information about left ventricular filling. Important limitations exist, however, be- cause mitral inflow velocities depend on loading con- ditionsl; as a result, some patients with severe dias- tolic dysfunction may exhibit a pseudonormal pat- tern of filling. 2 Recently, a modified pulsed Doppler technique called Doppler tissue imaging (DTI) was developed, which allows measurement of the low velocities as- sociated with wall motion velocities. 3-5 This tech- nique has been used for annular velocity measure- ment in a normal population, 6 but the changes in annular velocities in pathologic conditions have not been described. Mitral annular velocities during di- astole and their relation to mitral inflow velocities may provide additional information about left ven- tricular filling and diastolic suction that is different from that available by other measurement modali- ties. The purpose of this study was to (1) validate DTI for assessing annular motion compared with M- mode annular displacement, (2) evaluate the char- acteristics of mitral annulus velocities and their changes with age in a population without heart dis- ease, (3) evaluate the impact of left ventricular hypertrophy on annular velocities, and (4) determine the relation in timing and magnitude between dias- tolic annular velocities and mitral Doppler inflow velocities. METHODS Patient population. We examined 23 participants with- out clinical or echocardiographic evidence of heart disease and 17 patients with concentric left ventricular hypertro- 982

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Ventricular Function
Assessment of mitral annular dynamics during diastole by Doppler tissue imaging: Comparison with mitral Doppler inflow in subjects without heart disease and in patients with left ventricular hypertrophy
Leonardo Rodriguez, MD, Mario Garcia, MD, Miguel Ares, MD, Brian P. Griffin, MD,
Satoshi Nakatani, MD, and James D. Thomas, MD Cleveland, Ohio
The purpose of this study was to determine the normal pat- tern and magnitude of mitral annular velocities in diastole by Doppler tissue imaging (DTI) and to assess whether this is altered in patients with left ventricular hypertrophy. Mitral annulus velocities were measured by DTI. Peak and time- velocity integral were measured from the DTI tracings and the timing of the velocities in relation to electrocardiogram. DTI was compared with M-mode echo of the annulus and mitral inflow Doppler velocities, Integrated annular veloci- ties by DTI correlated with the annular displacement. Early diastolic velocities decreased with age and in patients with left ventricular hypertrophy. In the hypertrophy group, early diastolic velocities were significantly lower than normal even after correcting for age. Patients with left ventricular hypertrophy also showed a delay in peak early diastolic mi- tral annular velocity (5.5 ± 21 msec after the E wave). In conclusion, mitral annular velocity in diastole is readily re- corded by DTI. The magnitude and the pattern of these velocities are significantly altered by age and by left ventric- ular hypertrophy. This method provides a new insight into diastolic filling events and may prove useful in detecting abnormal diastolic function. (AM HEART J 1996;131:982-7.)
Noninvasive evaluation of diastolic function is an important role of clinical echocardiography. Mitral inflow velocities are commonly used to evaluate
From the Cardiovascular Imaging Center, Department of Cardiology, Cleveland Clinic Foundation.
Supported in part by the Fondo de Inversiones Sanitarias, Spain, the Uehara Memorial Foundation, Tokyo, Japan, Grant-in-Aid 930133380 from the American Heart Association, and an equipment grant from Acu- son, Inc., Mountain View, Calif.
Received for publication Aug'. 1, 1995; accepted Sept. 12, 1995.
Reprint requests: Leonardo Rodriguez, MD, Desk F-15, Division of Cardi- ology, The Cleveland Clinic Foundation, 9500 Euclid Ave., Cleveland OH 44195.
Copyright © 1996 by Mosby-Year Book, Inc. 0002-8703/96/$5.00 + 0 4/1/70745
diastolic function; these velocities are easily recorded and offer useful information about left ventricular filling. Important limitations exist, however, be- cause mitral inflow velocities depend on loading con- ditionsl; as a result, some patients with severe dias- tolic dysfunction may exhibit a pseudonormal pat- tern of filling. 2
Recently, a modified pulsed Doppler technique called Doppler tissue imaging (DTI) was developed, which allows measurement of the low velocities as- sociated with wall motion velocities. 3-5 This tech- nique has been used for annular velocity measure- ment in a normal population, 6 but the changes in annular velocities in pathologic conditions have not been described. Mitral annular velocities during di- astole and their relation to mitral inflow velocities may provide additional information about left ven- tricular filling and diastolic suction that is different from that available by other measurement modali- ties.
The purpose of this study was to (1) validate DTI for assessing annular motion compared with M- mode annular displacement, (2) evaluate the char- acteristics of mitral annulus velocities and their changes with age in a population without heart dis- ease, (3) evaluate the impact of left ventricular hypertrophy on annular velocities, and (4) determine the relation in timing and magnitude between dias- tolic annular velocities and mitral Doppler inflow velocities.
METHODS Patient population. We examined 23 participants with-
out clinical or echocardiographic evidence of heart disease and 17 patients with concentric left ventricular hypertro-
982
Volume 131, Number 5
American Heart Journal l~ocir~guez et al. 983
phy (LVH). All patients were in sinus rhythm. Age was 42.3 ± 17.5 (mean -+ SD) years in the group without heart disease and 69.3 _+ 9.8 years in the LVH group (p < 0.0001). LVH was considered present when left ventricular wall thickness was ->12 mm. The cause of the LVH was systemic hypertension in 13 patients and aortic stenosis in 4. There were seven women in each group. All patients had normal systolic function without segmental wall motion abnormalities, and none had more than mild mitral regur- gitation by echocardiography.
Echocardiography. Images were taken with patients in the left lateral decubitus position by an Acuson 128 XP/10 (Mountain View, Calif.) with a multifrequency transducer equipped with DTI technology. DTI uses a modified wall filter and reduced gain to display myocardial velocity while avoiding blood flow detection. From the apical four-cham- ber view, a 10 mm sample volume was placed at the lateral mitral annulus, and spectral DTI was recorded on paper at a 100 mm/sec sweep speed. Meticulous care was taken to align the echo image to place the annular motion parallel to the DTI cursor. The spectral Doppler signal parameters were adjusted to obtain Nyquist limits between 15 and 20 cm/sec by using the lowest wall filter settings and the op- timal gain to minimize noise. From the DTI tracings the following measurements were obtained: peak velocity and time-velocity integral of annulus velocity during early fill- ing (Eann) and atrial contraction (Aann). The time intervals between the Q wave and the onset and the peak early di- astolic velocity were also measured. An M-mode echo of the lateral mitral annulus was also recorded from the apical window. From the M-mode tracings the early diastolic, atrial systolic, and total annular displacement were mea- sured. Mitral inflow velocities were recorded by standard pulsed-wave Doppler at the tips of the mitral valve. From the mitral inflow recordings peak early (E) and atrial (A) velocities and the time interval from the Q wave of the electrocardiogram to the onset and peak of the E wave were measured similarly to DTI measurements.
Data analysis. To validate DTI as a way to assess annu- lar motion, we compared the time-velocity integral of an- nular velocities with the M-mode excursion by using linear regression and analysis of the agreement in 10 patients. 7 Annular velocities and their ratios were expressed as mean _+ SD, and the group without heart disease and the LVH group were compared by unpaired t test. The relation of mitral annular velocities to both age and mitral inflow velocities was assessed by linear regression analysis. Analysis of covariance was used to determine the signifi- cance of LVH on mitral annulus velocities independent of the effect of age. A difference was considered significant at p < 0.05. Finally, the relation between the timing of annular motion and mitral inflow was compared by unpaired t test.
RESULTS
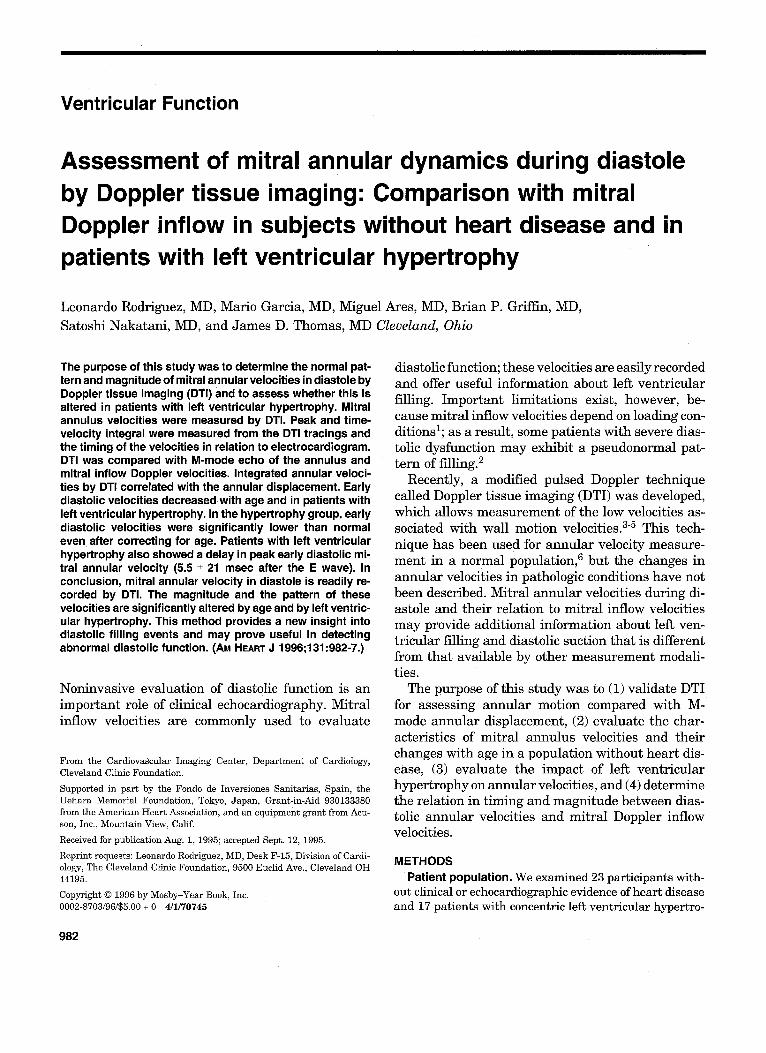
DTI spectral velocities were easily obtained from all patients. An example of a t rac ing of a subject wi thout hear t disease is shown in Fig. 1. Annu la r velocities showed three major distinctive waves: a
Fig. 1. Composite image showing recordings of M-mode echo of mitral annulus motion (top), mitral Doppler inflow (middle), and DTI of annular velocities (bottom).
positive wave toward the apex dur ing systole and two waves away from the t r ansducer dur ing diastole. The first diastolic wave occurred dur ing early filling, and the second corresponded to atrial contraction,
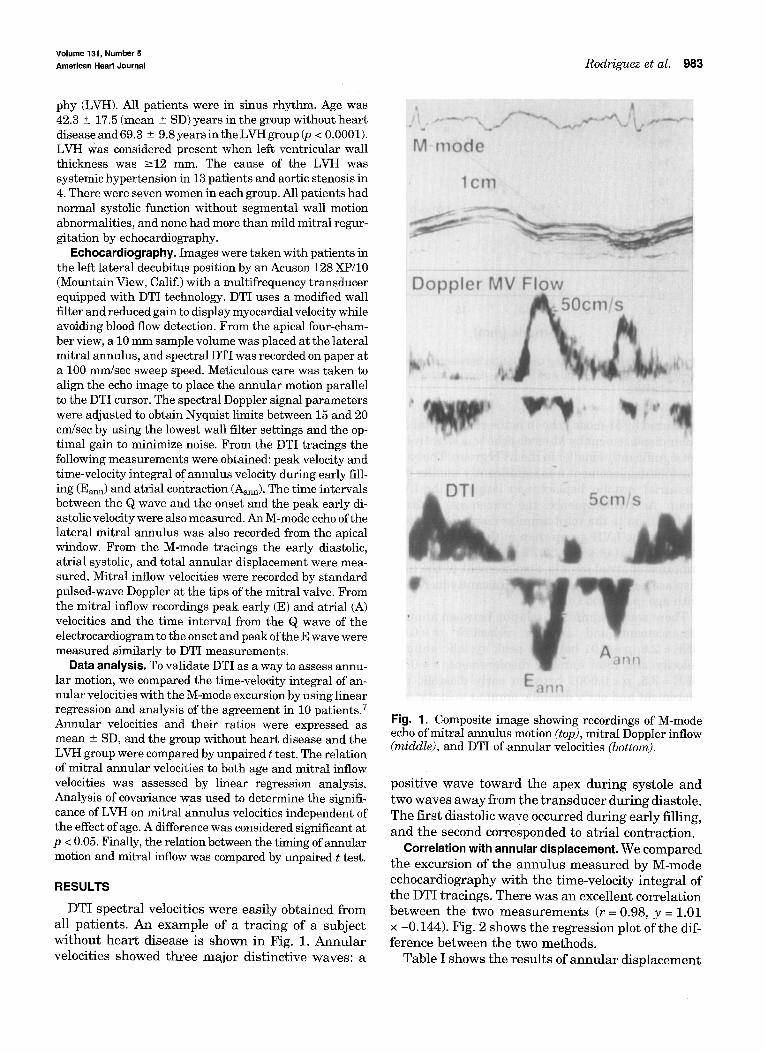
Correlation with annular displacement. We compared the excursion of the annulus measured by M-mode echocardiography with the time-velocity integral of the DTI tracings. There was an excellent correlation between the two measu remen t s (r = 0.98, y = 1.01 × -0.144). Fig. 2 shows the regression plot of the dif- ference between the two methods.
Table I shows the results of annu la r displacement
May 1996 984 Rodriguez et al. American Heart Journal
20
18
16
14
1 2
10,
~ 6 '
4,
2,
0 0
• "" " S y = 1.01x- 0.14 r= 0.98
I I 15 20
I I 5 lO
M - m o d e ( m m )
Fig. 2. Scatter plot showing correlation between annular excursion by M-mode echo and by time-velocity integral of DTI velocities.
m e a s u r e d by M-mode echo in bo th groups. Total an- nu la r d i sp lacemen t by M-mode echo was sl ightly bu t not s ignif icant ly smal le r in the LVH group. The ear ly diastolic d i sp lacement was s ignif icant ly smal le r and the a t r ia l systolic d i sp lacement l a rge r in the LVH group. As a consequence, the pe rcen tage of a t r ia l contr ibut ion to the to ta l a n n u l a r d i sp lacement was l a rge r in the LVH group t h a n in the g r o u p wi thou t h e a r t d isease (43.4% vs 30.7%, p = 0.0007). The con- t r ibu t ion of a t r ia l systolic d i sp lacement to the to ta l d i sp lacement of the annu lus s ignif icant ly increased wi th age (p = 0.0003).
There was a s ignif icant re la t ion be tween a n n u l a r d i sp lacemen t and a n n u l a r velocities ( r = 0 . 6 2 , SEE = 2.8, p = 0.01 be tween p e a k systolic a n n u l a r velocity and to ta l a n n u l a r d isplacement ; r = 0.73, SEE = 3.5, p < 0.0001 be tween ear ly diastolic dis- p l acemen t and ear ly diastolic a n n u l a r velocity; and r = 0.74, SEE = 1.8, p = 0.0008 be tween a t r ia l sys- tolic d i sp lacemen t and a t r ia l systolic a n n u l a r veloc- ity).
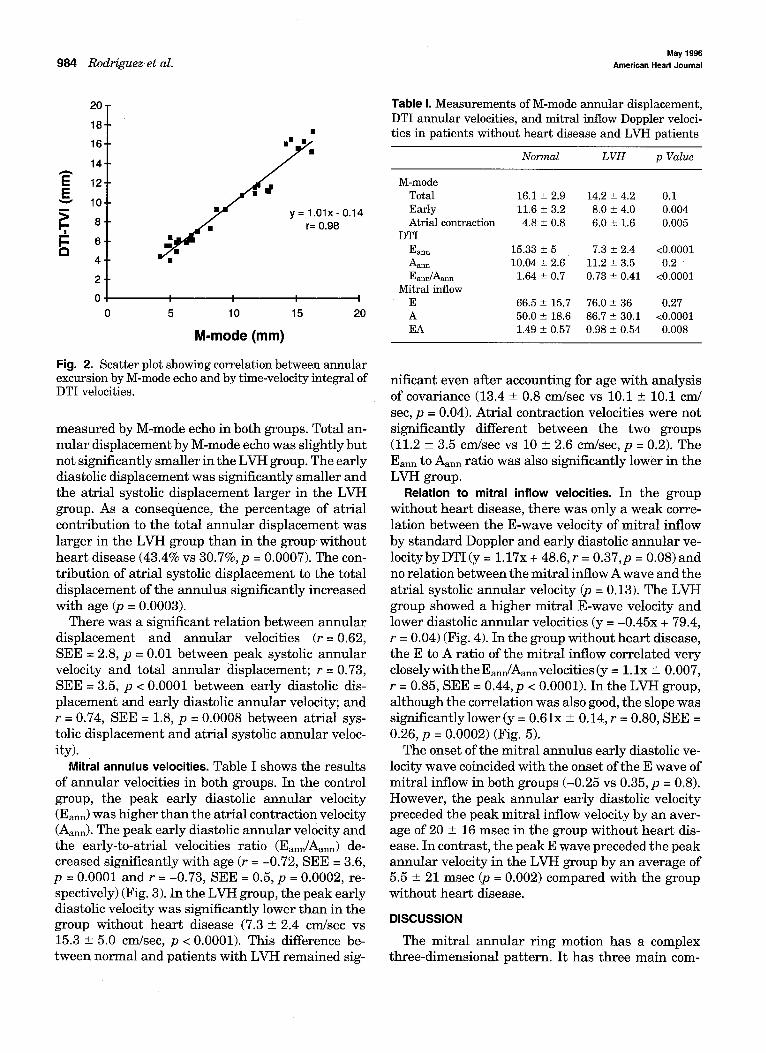
Mitral annulus velocities. Table I shows the resu l t s of a n n u l a r velocities in bo th groups. In the control group, the p e a k ear ly diastolic a n n u l a r velocity (Eann) was h igher t h a n the a t r ia l contract ion velocity (Aann). The p e a k ear ly diastolic a n n u l a r velocity and the ear ly- to-a t r ia l velocities ra t io (Eann/Aam~) de- c reased s ignif icant ly wi th age (r = -0.72, SEE = 3.6, p = 0.0001 and r = -0.73, SEE = 0.5, p = 0.0002, re- spectively) (Fig. 3). In the LVH group, the p e a k ear ly diastolic velocity was s ignif icant ly lower t h a n in the group wi thou t h e a r t disease (7.3 _+ 2.4 cm/sec vs 15.3 _+ 5.0 cm/sec, p < 0.0001). This difference be- tween no rma l and pa t i en t s wi th LVH r e m a i n e d sig-
Table I. Measurements of M-mode annular displacement, DTI annular velocities, and mitral inflow Doppler veloci- ties in patients without heart disease and LVH patients
Normal LVH p Value
M-mode Total 16.1 _+ 2.9 14.2 ± 4.2 0.1 Early 11.6 ± 3.2 8.0 ± 4.0 0.004 Atrial contraction 4.8 ± 0.8 6.0 ± 1.6 0.005
DTI Earm 15.33 ± 5 7.3 ± 2.4 <0.0001 Aann 10.04 ± 2.6 11.2 ± 3.5 0.2 Eann/Aarm 1.64 ± 0.7 0.73 ± 0.41 <0.0001
Mitral inflow E 66.5 ± 15.7 76.0 ± 36 0.27 A 50.0 -+ 18.6 86.7 ± 30.1 <0.0001 EA 1.49 _+ 0.57 0.98 _+ 0.54 0.008
nif icant even af ter account ing for age wi th ana lys i s of covar iance (13.4 _+ 0.8 cm/sec vs 10.1 _+ 10.1 cm/ sec, p = 0.04). Atr ia l contract ion velocities were not s ignif icant ly different be tween the two groups (11.2 _+ 3.5 cm/sec vs 10 _+ 2.6 cm/sec, p = 0.2). The Eann to Aann ra t io was also s ignif icant ly lower in the LVH group.
Relation to mitral inflow velocities. I n t h e g r o u p
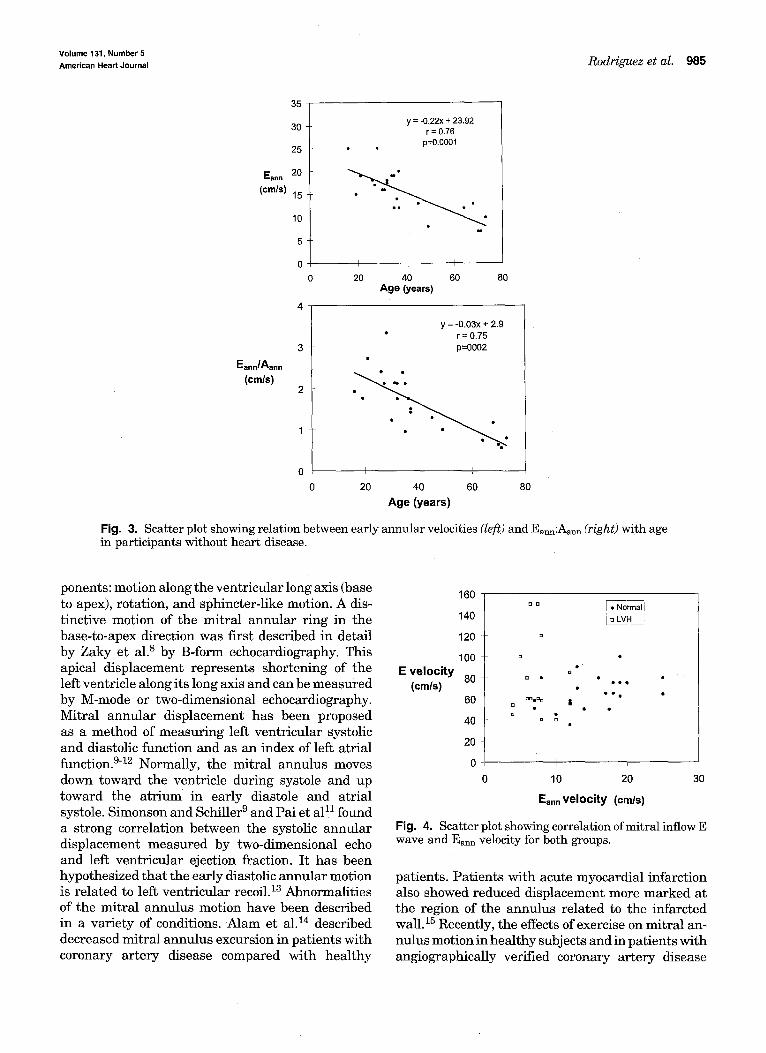
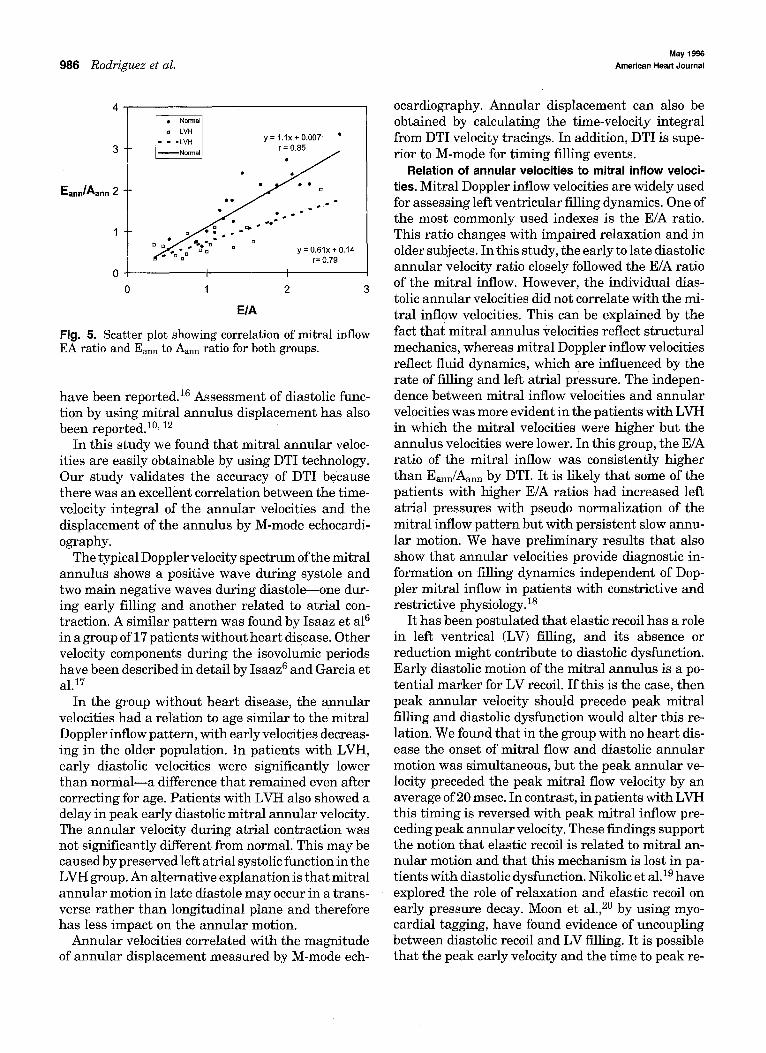
withou t h e a r t disease, t he re was only a w e a k corre- la t ion be tween the E-wave velocity of mi t r a l inflow by s t a n d a r d Doppler and ear ly diastolic a n n u l a r ve- loc i tyby DTI (y = 1.17x + 48.6, r = 0.37,p = 0.08) and no re la t ion be tween the mi t r a l inflow A wave and the a t r ia l systolic a n n u l a r velocity (p = 0.13). The LVH group showed a h igher mi t r a l E-wave velocity and lower diastolic a n n u l a r velocities (y = -0 .45x + 79.4, r = 0.04) (Fig. 4). In the group wi thou t h e a r t disease, the E to A ra t io of the mi t r a l inflow corre la ted very closely wi th the Eann/Aann velocities (y = 1. l x -+ 0.007, r = 0.85, SEE = 0.44, p < 0.0001). In the LVH group, a l though the corre la t ion was also good, the slope was s ignif icant ly lower (y = 0.61x _+ 0.14, r = 0.80, SEE = 0.26, p = 0.0002) (Fig. 5).
The onset of the mi t r a l annu lu s ear ly diastolic ve- locity wave coincided wi th the onset of the E wave of mi t r a l inflow in both groups (-0.25 vs 0.35, p = 0.8). However , the p e a k a n n u l a r ear ly diastolic velocity preceded the p e a k mi t r a l inflow velocity by an aver- age of 20 _+ 16 msec in the group wi thou t h e a r t dis- ease. In contras t , the p e a k E wave preceded the p e a k a n n u l a r velocity in the LVH group by an ave rage of 5.5 _ 21 msec (p = 0.002) compared wi th the group wi thou t h e a r t disease.
DISCUSSION
The mi t r a l a n n u l a r r ing mot ion has a complex th ree -d imens iona l pa t t e rn . I t ha s th ree m a i n com-
Volume 131, Number 5 American Heart Journal Rodriguez et al. 985
35
30
25
Eann 20
(cm/s) 15
10
5
0
3
Eann/Aann (cmls)
2
y = -0.22x + 23.92 r = 0.76
p=O.O001
I L. I 0 20 40 60 80
Age (years)
0 80
y = -O.03x + 2.9 • r = 0.75
p=O002
I : L
20 40 60
A g e (years)
Fig. 3. Scatter plot showing relation between early annular velocities (left) and Eam~:Aar~ (right) with age in participants without heart disease.
ponents: motion along the ventricular long axis (base to apex), rotation, and sphincter-like motion. A dis- tinctive motion of the mitral annular ring in the base-to-apex direction was first described in detail by Zaky et al. s by B-form echocardiography. This apical displacement represents shortening of the left ventricle along its long axis and can be measured by M-mode or two-dimensional echocardiography. Mitral annular displacement has been proposed as a method of measuring left ventricular systolic and diastolic function and as an index of left atrial function. 9-12 Normally, the mitral annulus moves down toward the ventricle during systole and up toward the atrium in early diastole and atrial systole. Simonson and Schiller 9 and Pai et al! 1 found a strong correlation between the systolic annular displacement measured by two-dimensional echo and left ventricular ejection fraction. It has been hypothesized that the early diastolic annular motion is related to left ventricular recoil. 13 Abnormalities of the mitral annulus motion have been described in a variety of conditions. Alam et al. 14 described decreased mitral annulus excursion in patients with coronary artery disease compared with healthy
160
140
120
100
E v e l o c i t y 80 (cmls)
6O
40
20
0
o
D
D o
o ~ • D o
o o
c]
• • e
• o e • |
0 10 20 30
Ean n v e l o c i t y (crn/s)
Fig. 4. Scatter plot showing correlation ofmitral inflow E wave and Eann velocity for both groups.
patients. Patients with acute myocardial infarction also showed reduced displacement more marked at the region of the annulus related to the infarcted wall.15 Recently, the effects of exercise on mitral an- nulus motion in healthy subjects and in patients with angiographically verified coronary artery disease
May 1996 986 Rodriguez et cd. American Heart Journal
4
y = 1.1x + 0.007 • 3 r = 0.85
Eann/Aann 21
y = 0,61x + 0.14 r= 0.79
0 I I
0 1 2 3
E/A
Fig. 5. Scatter plot showing correlation of mitral inflow EA ratio and Eann to Aann ratio for both groups.
have been reported. 16 Assessment of diastolic func- tion by using mitral annulus displacement has also been reported. 1°, 12
In this study we found that mitral annular veloc- ities are easily obtainable by using DTI technology. Our study validates the accuracy of DTI because there was an excellent correlation between the time- velocity integral of the annular velocities and the displacement of the annulus by M-mode echocardi- ography.
The typical Doppler velocity spectrum of the mitral annulus shows a positive wave during systole and two main negative waves during diastole--one dur- ing early filling and another related to atrial con- traction. A similar pattern was found by Isaaz et al6 in a group of 17 patients without heart disease. Other velocity components during the isovolumic periods have been described in detail by Isaaz ~ and Garcia et a]. 17
In the group without heart disease, the annular velocities had a relation to age similar to the mitral Doppler inflow pattern, with early velocities decreas- ing in the older population. In patients with LVH, early diastolic velocities were significantly lower than normal--a difference that remained even after correcting for age. Patients with LVH also showed a delay in peak early diastolic mitral annular velocity. The annular velocity during atrial contraction was not significantly different from normal. This may be caused by preserved left atrial systolic function in the LVH group. An alternative explanation is that mitral annular motion in late diastole may occur in a trans- verse rather than longitudinal plane and therefore has less impact on the annular motion.
Annular velocities correlated with the magnitude of annular displacement measured by M-mode ech-
ocardiography. Annular displacement can also be obtained by calculating the time-velocity integral from DTI velocity tracings. In addition, DTI is supe- rior to M-mode for timing filling events.
Relation of annular velocities to mitral inflow veloci- ties. Mitral Doppler inflow velocities are widely used for assessing left ventricular filling dynamics. One of the most commonly used indexes is the E/A ratio. This ratio changes with impaired relaxation and in older subjects. In this study, the early to late diastolic annular velocity ratio closely followed the E/A ratio of the mitral inflow. However, the individual dias- tolic annular velocities did not correlate with the mi- tral inflow velocities. This can be explained by the fact that mitral annulus velocities reflect structural mechanics, whereas mitral Doppler inflow velocities reflect fluid dynamics, which are influenced by the rate of filling and left atrial pressure. The indepen- dence between mitral inflow velocities and annular velocities was more evident in the patients with LVH in which the mitral velocities were higher but the annulus velocities were lower. In this group, the E/A ratio of the mitral inflow was consistently higher than Ea~m/Aann by DTI. It is likely that some of the patients with higher E/A ratios had increased left atrial pressures with pseudo normalization of the mitral inflow pattern but with persistent slow annu- lar motion. We have preliminary results that also show that annular velocities provide diagnostic in- formation on filling dynamics independent of Dop- pler mitral inflow in patients with constrictive and restrictive physiology, is
It has been postulated that elastic recoil has a role in left ventrical (LV) filling, and its absence or reduction might contribute to diastolic dysfunction. Early diastolic motion of the mitral annulus is a po- tential marker for LV recoil. If this is the case, then peak annular velocity should precede peak mitral filling and diastolic dysfunction would alter this re- lation. We found that in the group with no heart dis- ease the onset of mitral flow and diastolic annular motion was simultaneous, but the peak annular ve- locity preceded the peak mitral flow velocity by an average of 20 msec. In contrast, in patients with LVH this timing is reversed with peak mitral inflow pre- ceding peak annular velocity. These findings support the notion that elastic recoil is related to mitral an- nular motion and that this mechanism is lost in pa- tients with diastolic dysfunction. Nikolic et al. 19 have explored the role of relaxation and elastic recoil on early pressure decay. Moon et al., 2° by using myo- cardial tagging, have found evidence of uncoupling between diastolic recoil and LV filling. It is possible that the peak early velocity and the time to peak re-

Volume 131, Number 5 et al. 987 American Heart Journal l~oal%guez
flect two different phenomena: ventricular filling and restoring forces or elastic recoil. This interesting issue warrants further investigation.
In this study we specifically avoided patients with left ventricular systolic dysfunction because it is well known that this has an important influence on dias- tolic function and annular motion. Full delineation of the relation between annular motion and mitral flow in this important subgroup of patients would be a useful future study.
Study limitations. DTI, pulsed Doppler, and M-mode tracings cannot be obtained simultaneously, but me- ticulous care was taken to measure cycles with iden- tical R-R intervals. The LVH group comprised pa- tients who were relatively older, and it is therefore difficult to separate the effect of age from the one produce by LVH. However, a significant difference remains even after controlling for age with analysis of covariance. We compared annular velocities dur- ing diastole with mitral inflow Doppler. Because mi- tral inflow has important limitations for assessing diastolic function, a more definitive study will need direct measurement of left ventricular compliance with high-fidelity intracardiac pressure recordings.
Conclusions. Velocities of the mitral annulus can be easily obtained by using DTI technology and cor- relate well with absolute annular motion. Mitral an- nulus early diastolic velocity decreases with age and in patients with LVH. Early/late diastolic annular velocities closely correlate with the E/A ratio of mi- tral inflow. In patients without heart disease, mitral annular early diastolic peak velocity precedes peak mitral flow E wave, which suggests that LV elastic recoil contributes to diastolic motion of the mitral annulus. This relation is reversed in LVH patients. DTI of mitral annulus may be helpful in assessing diastolic function and in elucidating the mechanisms of LV filling.
REFERENCES
1. Choong CY, Abascal VM, Thomas JD, Guerrero JL, McGlew S, Weyman AE. Combined influence ofventricular loading and relaxation on the transmitral fiow velocity profile in dogs measured by Doppler echocardiography. Circulation 1988;78:672-83.
2. Appleton CP, Hatle LK, Popp RL. Relation oftransmitral flow velocity patterns to left ventricular diastolic function: new insights from a com- bined hemodynamic and Doppler echocardiographic study. J Am Coll Cardiol 1988;12:426-40.
3. Isaaz K, Thompson A, Ethevenot G, Cloes J, Brembilla B, Pernot C, Doppler echocardiographic measurement of low velocity motion of the left ventricular posterior wall. Am J Cardiol 1989;64:66-75.
4. Fleming AD, Xia X, McDicken WN, Sutherland GR, Fenn L. Myocar- dial velocity gradients detected by Doppler imaging. Br J Radio! 1994;67:679-88.
5. McDicken WN, Sutherland GR, Moran CM, Gordon LN. Colour Dop- pler velocity imaging of the myocardium. Ultrasound Med Biol 1992; 18:651-4.
6. Isaaz K, Munoz-del-Romeral L, Lee E, Schiller NB. Quantitation of the motion of the cardiac base in normal subjects by Doppler echocardiog- raphy. J Am Soc Echo 1993;6:166-76.
7. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;1:307-10.
8. Zaky A, Grabhorn L, Figembaun H. Movement of the mitral ring: a study in ultrasound cardiography. Cardiovasc Res 1967;1:121-31.
9. Simonson J, Schiller NB. Descent of the base of the left ventricle: an echocardiographic index of left ventricular function. J Am Soc Echo 1989;2:25-35.
10. Jones CJ, Song GJ, Gibson DG. An echocardiographic assessment of atrial mechanical behavior. Br Heart J 1991;65:31-6.
11. Pai RG, Bodenheimer MM, Pal SM, Koss JH, Adamick RD. Usefulness of systolic excursion of the mitral anulus as an index of left ventricular systolic function. Am J Cardiol 1991;67:222-4.
12. Alam M, Hoglund C. Assessment by echocardiogram of left ventricular diastolic function in healthy subjects using the atrioventricular plane displacement. Am J Cardiol 1992;69:565-8.
13. Jones CJ, Raposo L, Gibson DG. Functional importance of the long axis dynamics of the human left ventricle. Br Heart J 1990;63:215-20.
14. Alam M, Hoglund C, Thorstrand C, Hellekant C. Haemodynamic sig- nificance of the atrioventricular plane displacement in patients with coronary artery disease. Eur Heart J 1992;13:194-200.
15. Hoglund C, Alam M, Thorstrand C. Effects of acute myocardial infarc- tion on the displacement of the atrioventricular plane: an echocardio- graphic, study. J Int Med 1989;226:251-6.
16. Alam M, Hoglund C, Thorstrand C, Carlens Po Effects ofexercise on the displacement of the atrioventricular plane in patients with coronary artery disease. A new echocardiographic method of detecting reversible myocardial ischaemia. Eur Heart J 1991;12:760-5.
17. Garcia M, Rodriguez L, Homa D, Nakatani S, Griffin BP, Klein AL, Stewart WJ, Thomas JD. Intramyocardial motion assessment by Dop- pler ultrasound: characteristic findings in normal subjects [abstract]. J Am Soc Echo 1994;7:S14.
18. Garcia M, Rodriguez L, Ares MA, Griffin BP, Thomas JD, Klein A. Dif- ferentiation of constrictive pericarditis from restrictive cardiomyop- athy: assessment of left ventricular diastolic velocities in longitudinal axis by Doppler tissue imaging. J Am Coll Cardiol 1996;27:108-14.
19. Nikolic S, Yellin EL, Tamura K, Vetter H, Tamura T, Meisner JS, Frater RW. Passive properties of canine left ventricle: diastolic stiffness and restoring forces. Circ Res 1988;62:1210-22.
20. Moon MR, Ingels NB, Daughters GT, Stinson EB, Hansen DE, Miller DC. Alterations in left ventricular twist mechanics with inotropic stimulation and volume loading in human subjects. Circulation 1993; 89:142-50.
Related Documents











