Assessment and Care of the Stroke Patient Megan McHugh, MS, RN, CCRN, CNRN Stroke Coordinator MedStar Georgetown University Hospital

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Assessment and Care of the Stroke Patient
Megan McHugh, MS, RN, CCRN, CNRN
Stroke Coordinator
MedStar Georgetown University Hospital

Goals:
• What is Stroke?
• Stroke Statistics
• Types of stroke
• Imaging Basics
• Cerebrovascular correlations
• Common deficits
• Hyperacute stroke care/tPA
• Acute stroke care
• Deficits

What is Stroke?
Abrupt and dramatic development of a focal neurologic deficit caused by an occlusion or
hemorrhage of a vessel feeding the brain

Stroke Statistics
• Incidence • 795,000 new cases annually in the United States
• 610,000 are first strokes
• 185,000 are recurrent strokes
• 4th leading cause of death
• Prevalance • Symptomatic Stroke
• Men – 2.7% >= 18 years, 3.8% of black men
• Women – 2.5% >= 18 years have had a stroke
• Silent Stroke increases with age
• Age 55-64 11%
• Age 85+ 43%

Stroke Statistics
• Mortality • 5.5% of all deaths in the US.
• 12.6% off all stroke patients die within 30 days
• 8.1% of ischemic stroke patients
• 44.6% of hemorrhagic stroke patients
• Disability • Survivors:
• 15-30% totally disabled
• 20% institutionalized at 3 months
• Only 50-70% regain functional independence
• Expense • Direct medical cost of stroke in 2007 was $25 billion
• Direct and indirect cost in 2007 $41 billion
• Individual lifetime cost $140,000

Transient Ischemic Attack
(TIA) Definition
• Acute, neurological event that reduces blood flow to a portion of the brain
• Symptoms correlate with the region of the brain affected
• Two definitions: Time vs. Tissue • Time: Temporary weakness/numbness or visual
changes caused by vascular disease that resolves within 24 hours
• Tissue: No permanent damage, e.g. resolved symptoms with normal MRI
• One third of patients whose symptoms resolve have MRI scans positive for an acute stroke!!!

TIA Statistics
• 15% of all strokes heralded by TIA
• Risk of stroke
• Within 2 days: 3-10%
• Within 90 days: 9-17% (one study showed 20%)
• Death within one year: 12-13%

Classification of Strokes
Stroke
Ischemic 87%
Thrombotic
Large vessel 20%
Small vessel (lacunar) 25% Embolic
20%
Cryptogenic 30%
Hemorrhagic 13%
ICH 10%
SAH 3%

Stroke Recognition
• Sudden:
• Weakness or numbness
• Trouble speaking or understanding
• Trouble seeing in one or both eyes
• Trouble walking, loss of balance or coordination
• Severe headache

Ischemic Stroke

How a clot forms
Courtesy Genetech

Infarct versus Penumbra
Penumbra
Infarct

Stages of Infarction (R MCA)

Lacunar stroke

Hemorrhagic Stroke
• 15-20%
• Intracerebral
Within the brain
parenchyma
• Subarachnoid
• Aneurysm
• Vascular malformations

Subarachnoid Hemorrhage

Types of Stroke: Summary
• Clots can form in an artery or travel from someplace else
• Blood vessels that burst inside the brain tissue cause intracerebral hemorrhages
• Blood vessels that burst in the subarachnoid space cause subarachoid hemorrhage
• Clots in the venous drainage system can lead to either type of stroke

Anatomy: Lobes of the Brain

Anatomy: Homunculus

Imaging 101
• MRI and CT are looking from the bottom up
• The left side of the image is the right side of the brain
• The right side of the image is the left side of the brain

Imaging basics: CT
• Best for showing acute blood
• Normal for 12-24 hours post stroke
• Important: CT read as “negative for acute stroke” that was done less than 24 hours after last normal does NOT mean they didn’t have a stroke!

Imaging Basics: MRI
• DWI (Diffusion weighted image) positive in seconds, stays positive for about two weeks.
• Areas of restricted diffusion, e.g. ischemia are bright (“light-bulb”)
• Flair (Fluid Attenuated Inversion Recovery) is positive in 6-12 hours, lasts forever
• Ischemia is bright, fluid is dark.
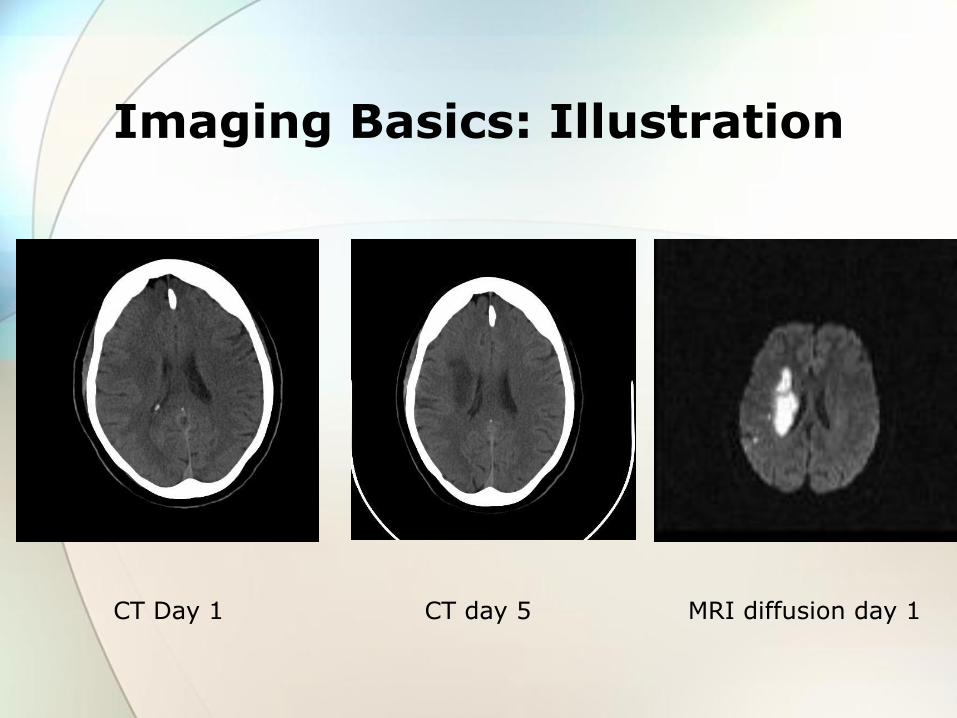
Imaging Basics: Illustration
CT Day 1 CT day 5 MRI diffusion day 1

Blood Supply of the Brain

Arterial supply

Blood Supply of the Brain
• Three come in: Basilar (Vertebrobasilar) formed from L and R vertebral
L & R Internal carotids
• Circle of Willis (the “beltway”)
• Six go out (three per side): ACA – anterior cerebral artery
MCA – middle cerebral artery
PCA – posterior cerebral artery

Incoming
B
C C
Circle of Willis

Outgoing
M M
ACOM
PCOM PCOM
95 North
270
Rt. 66
95 South
Rt. 4
Rt. 50

Complete
M M
ACOM
PCOM PCOM
C C
B

Circle of Willis

Cerebrovascular Anatomy
PCA PCA
MCA MCA
ACA ACA
PCOM PCOM
ACOM

Vascular Territories
ACA
PCA
MCA MCA

Examples
•Occlusion: •ACA
•collateral circulation •MCA •PCA •Carotid •Basilar
•PICA

ACA Occlusion
M M
ACOM
PCOM PCOM
C C
B
270
66

ACA Occlusion

Symptoms, by Vessel Insufficiency: ACA
• Personality change
• Confusion
• Incontinence
• Leg weakness greater than arm weakness
• Difficulty tracking
• Motor/sensory changes on opposite side of body

MCA Occlusion
M M
ACOM
PCOM PCOM
C C
B

Right MCA occlusion
MRI Day 2

L MCA Completed Infarct
CT Day 1 CT Day 5

Symptoms, by Vessel Insufficiency: MCA
• Middle cerebral artery
Motor/sensory changes on opposite side of body
Arm weakness greater than leg weakness
Same side visual changes
Left—speech
Right—knowing where body parts are

PCA Occlusion
M M
ACOM
PCOM PCOM
C C
B

PCA Occlusion

Symptoms, by Vessel Insufficiency: PCA
Opposite-side sensory loss
Same-side vision loss
Left—communication
Right—knowing where body parts are
Graying of vision

R Carotid Occlusion
M M
ACOM
PCOM PCOM
C C
B

R Carotid Occlusion
MRI

Symptoms, by Vessel Insufficiency
• Carotid artery
Opposite motor/sensory loss
Amaurosis fugax (fleeting blindness)
Right—knowing where body parts are
Left—speech

R Basilar Occlusion
M M
ACOM
PCOM PCOM
C C
B

PICA Occlusion
• Largest branch off vertebral
• One of the three main arterial supplies for the cerebellum
• Other two are SCA and AICA
QuickTime™ and a decompressor
are needed to see this picture.
Quic kTime™ and a decompress or
are needed to see th is p ic ture.

Dizziness
Nausea and vomiting
Ataxia
Dysarthria
Dysphagia
Eye movement
Facial weakness
Hearing loss
Symptoms, by Vessel Insufficiency: Vertebrobasilar

Clinical Presentation: Summary
• Determined by region of vascular insufficiency

Clinical Presentation: Right Hemisphere
Neglect—body part or loss of function not acknowledged
Flat or bland affect
Apraxia—partial or complete inability to execute purposeful movement
Left hemiplegia/hemisensory loss

Speech changes—expressive, receptive, global aphasia
Right hemiplegia/hemisensory loss
Clinical Presentation: Left Hemisphere

• Brain stem
Hemiplegia/quadriparesis
Loss of sensory in ½ of body or all four limbs
Dysarthria
Dysphagia
Ataxia
Nausea and vomiting
Cranial nerve changes
Clinical Presentation: Brain Stem

Stroke Treatments: Ischemic
•Geared towards the cause:
•Ischemic: •Dissolve the clot (tPA) • <3 hours (FDA)
• <4.5 hours (ECASS 3 trial, AHA)
•Retrieve the clot
•Manipulate blood pressure
•Remove the clot/plaque surgically (CEA)
•HOB flat, SBP up to 220 mmHg • to increase perfusion to penumbra
• SBP < 185 mmHg for tPA

Stroke Treatment: Hemorrhagic
• Intracerebral hemorrhage
• Subarachnoid hemorrhage
• Main differences
• BP parameters
• HOB flat or elevated
• No antithrombotics or anticoagulation
• Coagulopathy

Stroke Treatments
• Blood pressure manipulation • Can be elevated to keep vessels open
• Can be lowered to prevent more bleeding
• Brain perfusion manipulation • HOB flat increases perfusion
• HOB elevated increases drainage and lowers ICP

Signs and symptoms reveal location:
• Sudden weakness or numbness
• Sudden loss of vision
• Sudden difficulty speaking or understanding
• Sudden dizziness or loss of balance
• Sudden severe headache
“Sudden” is the key!

Common Deficits
• Aphasia
Expressive aphasia – can understand what you are saying but cannot get the right words out, speaking gibberish, or mute
Receptive aphasia – cannot understand what is being said to them; likened to being in a foreign country where you don’t know the language
Can have both expressive and receptive aphasia
Give pt time to try to communicate – remember they may be very frustrated

Common Deficits
• Swallowing difficulties
May silently aspirate, without even a cough
Common cause of increased mortality
Swallow screen by the nurse and full evaluation help identify these patients so that we can feed safely and reduce risk.
Well-meaning family need education about aspiration pneumonia so they understand why we may delay starting feedings
Aspiration precautions for all: Sit up 90 degrees to feed, small spoonfuls, correct consistency, don’t rush, stop if coughing

Common Deficits
• Hemiplegia
Most often one side of the face/arm/leg weak or flaccid
Can easily dislocate a shoulder if you pull on it repositioning the patient; often develop shoulder pain even without overt injury
Prop weak arm up on a pillow, hand above heart to reduce dependent edema

Common Deficits
• Neglect
Pt may be unaware of the weak side of the body
May not look towards that side, may not see that side
May not know that there is a problem, so they try to get out of bed and fall
Pay attention to the patient – try to feed them and address them from the bad side to help in recuperation

Care goals:
• Prevent secondary injury/ infections • Prevent pressure ulcers by frequent
repositioning • Prevent edema by elevating flaccid
extremities on pillows • Prevent aspiration pneumonia by swallow
screens, aspiration precautions • Prevent contracture by doing range of motion
exercise every shift in weak limbs • Prevent falls: patients with symptoms of
neglect/ visual cuts are at very high risk

Remember the Basics
• Infection
• DVT
• Pneumonia
• Bowel/bladder care
• Constipation
• Incontinence

Remember the Basics
• Mobility
• Falls
• contractures
• Skin care
• Avoid breakdown
• Detect dysphagia
• Swallow assessment
• Nutritional compromise

Complications of Stroke

Summary
• Care is the KEY to RECOVERY
• Symptoms determined by vessel(s) affected
• In-hospital care is only the beginning
• Rehab and improvement continue for many months


References Revised and updated recommendations for the establishment of primary stroke centers: a summary statement from the Brain Attack Coalition (2010). Stroke (41) 2402-2448. Retrieved from http://stroke.ahajournals.org
Heart Disease and Stroke Statistics 2011 Update: A Report from the American Heart Association. Retrieved from http://circ.ahajournals.org
Expansion of the Time Window for Treatment of Acute Ischemic stroke with Intraveious Tissue Plasminogen Activator: A science advisory from the American Heart Association/ American Stroke Association (2009)
Comprehensive Overview of Nursingand Interdisciplinary Care of the Acute Ischemic Stroke Patient: A scientific statement from the American Heart Association (2009)
Related Documents