Assessing subtype and drug-resistance-associated mutations among antiretroviral-treated HIV-infected patients Rasool Hamkar a , Minoo Mohraz b , Shima Lorestani c , Arezoo Aghakhani d , Hong-Ha M. Truong e , Willi McFarland e , Mohammad Banifazl f , Ali Eslamifar d , Maryam Foroughi b , Atessa Pakfetrat g and Amitis Ramezani d Background: Several studies have reported an increasing number of therapeutic fail- ures with antiretroviral drugs in HIV-infected patients. The emergence of viral-resistant strains is a major problem for the medical management of infected individuals. The aim of this study is to determine viral subtypes and drug-resistance mutations among antiretroviral-treated HIV-infected patients. Methods: A total of 42 antiretroviral-treated but still viremic HIV-infected patients were enrolled. The HIV pol regions were amplified and sequenced to determine subtypes and antiretroviral-resistant mutations. Results: The subtype distribution was 48% A/D recombinants, 43% subtype B, 5% subtype A and 5% CRF01-AE recombinants. Drug-resistant mutations were most common in subtype B (53%) and A/D recombinant strains (44%). Virus samples from 19% of participants had no drug-resistant mutations; 2, 2 and 76% of samples carried one, two and at least three drug-resistant mutations, respectively. The prevalence of nucleoside transcriptase inhibitor mutations was 76%, with M184V and L74V present in 60 and 38% of samples, respectively. The prevalence of nonnucleoside transcriptase inhibitor mutations was 74%, with P225H present in 55% of study specimens. The prevalence of protease inhibitor mutations was 45%, with major mutation L90M seen in 33% and minor mutation A71V in 36% of samples. Of note, the P225H and A71V are ‘minor’ drug-resistance mutations conferring only minimal drug-resistance phenotypes in the absence of major mutations. Conclusion: Our study found a high prevalence of drug-resistant mutations in Iranian HIV-infected patients. Our data support the need for continued surveillance of resist- ance patterns to help guide therapeutic approaches and limit transmission of these variants. ß 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins AIDS 2010, 24 (suppl 2):S85–S91 Keywords: antiretroviral therapy, drug resistance, HIV a Tehran University of Medical Sciences, b Iranian Research Center for HIV/AIDS, Tehran, c School of Science, Islamic AZAD University, Qom, d Clinical Research Department, Pasteur Institute of Iran, Tehran, Iran, e University of California, San Francisco, California, USA, f Iranian Society for Support Patients with Infectious Diseases, Tehran, and g School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran. Correspondence to Amitis Ramezani, Clinical Research Department, Pasteur Institute of Iran, No. 69, Pasteur Avenue, Tehran 13164, Iran. Tel: +98 2166968852; fax: +98 2166465147; e-mail: [email protected] ISSN 0269-9370 Q 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins S85

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Assessing subtype and d
rug-resistance-associatedmutations among antiretroviral-treatedHIV-infected patients
Rasool Hamkara, Minoo Mohrazb, Shima Lorestanic,
Arezoo Aghakhanid, Hong-Ha M. Truonge,
Willi McFarlande, Mohammad Banifazlf, Ali Eslamifard,
Maryam Foroughib, Atessa Pakfetratg and
Amitis Ramezanid
aTehran UniversityUniversity, Qom,California, USA, f
University of Med
Correspondence t13164, Iran.
Tel: +98 2166968
ISS
Background: Several studies have reported an increasing number of therapeutic fail-ures with antiretroviral drugs in HIV-infected patients. The emergence of viral-resistantstrains is a major problem for the medical management of infected individuals. The aimof this study is to determine viral subtypes and drug-resistance mutations amongantiretroviral-treated HIV-infected patients.
Methods: A total of 42 antiretroviral-treated but still viremic HIV-infected patients wereenrolled. The HIV pol regions were amplified and sequenced to determine subtypes andantiretroviral-resistant mutations.
Results: The subtype distribution was 48% A/D recombinants, 43% subtype B, 5%subtype A and 5% CRF01-AE recombinants. Drug-resistant mutations were mostcommon in subtype B (53%) and A/D recombinant strains (44%). Virus samples from19% of participants had no drug-resistant mutations; 2, 2 and 76% of samples carriedone, two and at least three drug-resistant mutations, respectively. The prevalence ofnucleoside transcriptase inhibitor mutations was 76%, with M184V and L74V present in60 and 38% of samples, respectively. The prevalence of nonnucleoside transcriptaseinhibitor mutations was 74%, with P225H present in 55% of study specimens. Theprevalence of protease inhibitor mutations was 45%, with major mutation L90M seen in33% and minor mutation A71V in 36% of samples. Of note, the P225H and A71V are‘minor’ drug-resistance mutations conferring only minimal drug-resistance phenotypesin the absence of major mutations.
Conclusion: Our study found a high prevalence of drug-resistant mutations in IranianHIV-infected patients. Our data support the need for continued surveillance of resist-ance patterns to help guide therapeutic approaches and limit transmission of thesevariants. � 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins
AIDS 2010, 24 (suppl 2):S85–S91
Keywords: antiretroviral therapy, drug resistance, HIV
of Medical Sciences, bIranian Research Center for HIV/AIDS, Tehran, cSchool of Science, Islamic AZADdClinical Research Department, Pasteur Institute of Iran, Tehran, Iran, eUniversity of California, San Francisco,Iranian Society for Support Patients with Infectious Diseases, Tehran, and gSchool of Medicine, Mashhadical Sciences, Mashhad, Iran.
o Amitis Ramezani, Clinical Research Department, Pasteur Institute of Iran, No. 69, Pasteur Avenue, Tehran
852; fax: +98 2166465147; e-mail: [email protected]
N 0269-9370 Q 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins S85

S86 AIDS 2010, Vol 24 (suppl 2)
Introduction
The use of potent antiretroviral drugs controls HIVinfections by suppressing the viral replication in patientswith HIV infection [1,2], resulting in a reduction ofdisease progression and substantial increase in patientsurvival [3]. However, extensive genetic variation is aprominent feature of HIV, which causes the emergence ofresistance mutations to all currently used antiretroviraldrugs [4].
Studies have shown that 10% of patients who commenceHAART develop some form of genotypic drug resistanceafter 2 years, and almost 30% of patients develop viralfailure with one major resistance mutation within 6 yearsafter starting HAART [5], thereby representing a threat tothe control of transmitted multiple-class resistance [6,7].The selection of viral resistance strains is a major problemfor the medical management of infected individualsbecause it can limit therapeutic options, cause treatmentfailures and be transmitted. HIV drug resistancerepresents an important public health problem, particu-larly in areas where antiretrovirals have been widely usedfor many years [8–10] and where treatment optionsare limited.
Limited data are available on HIV-1 subtype distributionin the Middle East and North African region where the Band C subtypes are prevalent, with the exception ofLebanon where the subtype A is predominant [11].Subtype B of HIV is the predominant variant in Westerncountries; subtype A in central and western Africa;subtype C in eastern and southern Africa, India andChina; and CRF01-AE in Thailand and Southeast Asia[12–14]. The prevalence of resistant mutants variesgeographically, justifying the need for regional charac-terization and surveillance to determine circulatingsubtypes and mutants that influence the effectiveness ofantiretroviral treatment [15,16]. There are limited dataregarding resistance mutants in Iran. The aim of this studyis to determine subtype and drug-resistant mutationsamong antiretroviral-treated HIV-infected patients.
Methods
Overall study design, patients and methodsIn this cross-sectional study, 42 antiretroviral-treatedHIV-infected patients admitted to the Iranian ResearchCenter for HIV/AIDS from October to December 2009were enrolled. A questionnaire that gathered epidemio-logical, clinical and treatment data was completed byclinicians. This project was approved by Iranian ResearchCenter for HIV/AIDS ethics committee and informedconsent was obtained from patients prior to theirenrollment. All patients received antiretroviral treatmentfor at least 1 year and were on regimens containing one
protease inhibitor or one nonnucleoside transcriptaseinhibitor (NNRTI) in combination with two NRTIs.CD4þ cell count (cells/ml) was determined by flowcytometry. The HIV pol regions, which include viralprotease and reverse transcriptase genes, were amplifiedand sequenced for determining subtype and antiretro-viral-resistant mutations.
PCR algorithm and sequencingRNA extraction was performed following the manu-facturer’s instructions (AccuPrep Viral RNA Extraction,Bioneer Co., Deajeon, South Korea). Reverse-transcriptase PCR was carried out in four steps accordingto the Canadian National HIV and RetrovirologyLaboratories HIV drug-resistant mutant surveillanceprocedure. Nested PCR amplification was performedto yield a 684-base-pair (bp) product from the viralprotease region and a 724-bp product from the reversetranscriptase region. PCR products were purified usingthe High Pure PCR product purification kit (Qiagen,Hilden, Germany) and sequenced bidirectionally, usingrelated forward and reverse primers by the facility(Macrogen, Seoul, South Korea).
Subtypes and drug-resistance analysisSequences were edited by Bioedit software (version7.0.5.3) and the subtypes were determined usingnucleotide Basic Local Alignment Search Tool (BLAST)and Stanford University HIV Drug Resistance mutationsdatabases. Additional analysis was carried out fordetermining drug-resistant mutations using the above-mentioned database.
Phylogenetic analysisFor each HIV-1 isolate, viral protease and reversetranscriptase sequences were grouped. The resultingsequences were aligned with reference sequences ofvarious subtypes from the GenBank database (http://www.ncbi.nlm.nih.gov) using the CLUSTAL W pro-gram. Phylogenetic analysis was performed by theneighbor-joining method [17] with Kimura’s two-parameter correction [18] and a phylogenetic tree wasconstructed using the MEGA program, version 4 [19].Bootstrap resampling and reconstruction were carried out1000 times to confirm the reliability of the phylogenetictree [20]. The HIV-1 sequences used in this studywere deposited in GenBank under accession numbersGU724804–GU724845.
Results
Eighty-three percent of patients were men and 17% werewomen. The mean age was 38� 9 (range 13–56) years.The mean CD4þ cell count was 266� 146 (26–560) cells/ml. The HIV transmission risks were intrave-nous drug use (36%), infected blood and blood products

HIV drug-resistant mutations in Iran Hamkar et al. S87
Table 1. HIV subtypes in antiretroviral-treated HIV-infected patients stratified by transmission risk, Iran.
HIV subtype
Transmission risk A (%) A/D (%) B (%) CRF01-AE (%) Total
Injection drug use 2 (13) 5 (33) 7 (47) 1 (7) 15Multiple sexual partners 0 (0) 1 (33) 2 (67) 0 (0) 3HIV-positive husband 0 (0) 3 (60) 2 (40) 0 (0) 5Blood and blood products 0 (0) 5 (56) 4 (44) 0 (0) 9Tattooing 0 (0) 1 (100) 0 (0) 0 (0) 1Vertical 0 (0) 0 (0) 1 (100) 0 (0) 1Heterosexual contact and
injection drug use0 (0) 1 (100) 0 (0) 0 (0) 1
Unknown 0 (0) 4 (57) 2 (29) 1 (14) 7Total 2 (5) 20 (48) 18 (43) 2 (5) 42
(21%), HIV-positive husband (12%), multiple sexualpartners (7%), vertical transmission (2%), tattooing (2%)and heterosexual contact and injection drug use (2%)(Table 1). In 17% of patients, HIV transmission risk wasnot identified.
The viral loads of patients ranged from 150to 270 000 HIV-RNA copies/ml (mean� SD 21759�62049 copies/ml). Nearly all patients (n¼ 39) were usingthe lamivudine plus zidovudine plus nevirapine regimen.In the three other patients, the regimen was lamivudineplus zidovudine plus nelfinavir. According to guidelines,if nevirapine is not available or not tolerated, efavirenz ortenofovir is substituted. We recorded such changes.
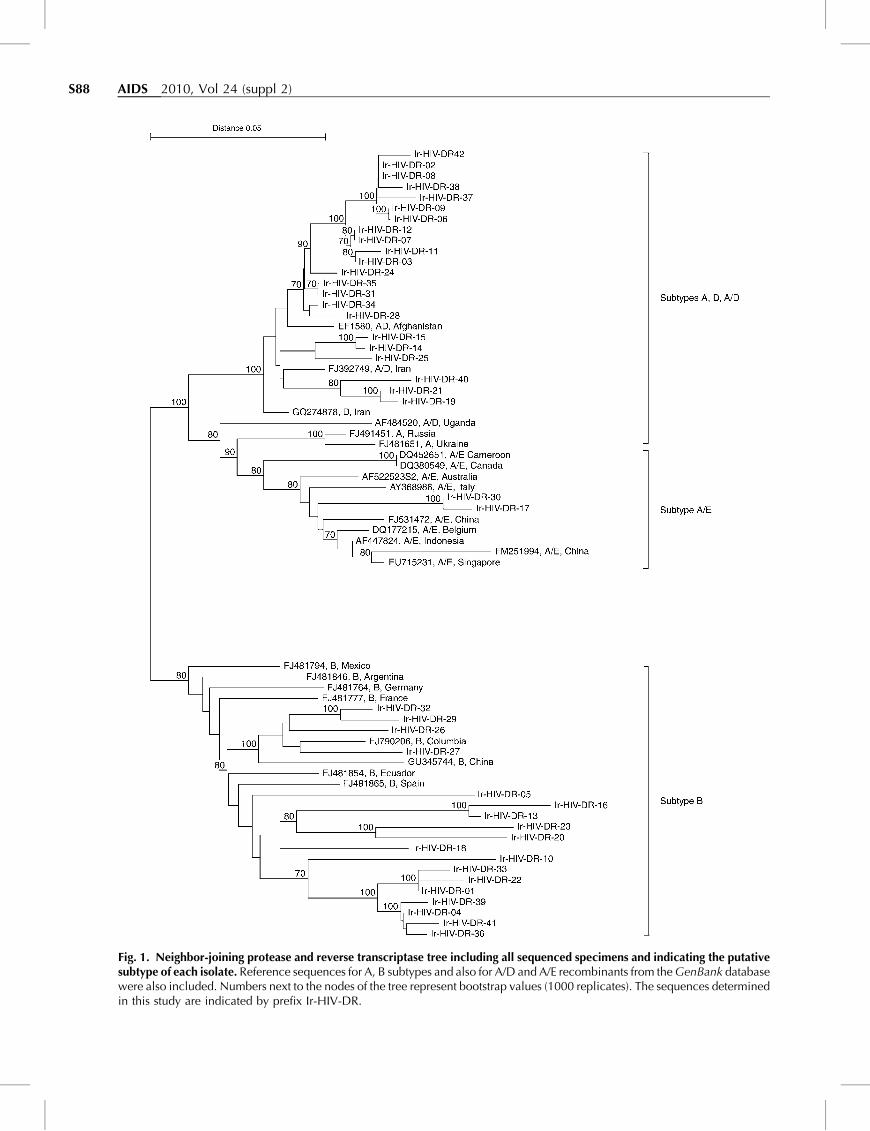
Sequencing of the samples revealed that 48% of strainswere subtype A/D recombinants, 43% subtype B, 5%subtype A and 5% CRF01-AE recombinants (Fig. 1). Thedistribution of HIV-1 subtypes in antiretroviral-treatedHIV-infected patients stratified by transmission risk isshown in Table 1.
Virus samples from 19% of participants had no drug-resistant mutations; 2, 2 and 76% of samples carried one,two and at least three drug-resistant mutations, respect-ively. Dual-class drug-resistant mutations were present in43% of participants (NRTI/NNRTI, 36%; NRTI/protease inhibitor, 5% and NNRTI/protease inhibitor,2%) and 36% had virus with triple-class drug resistance(NRTI/NNRTI/protease inhibitor).
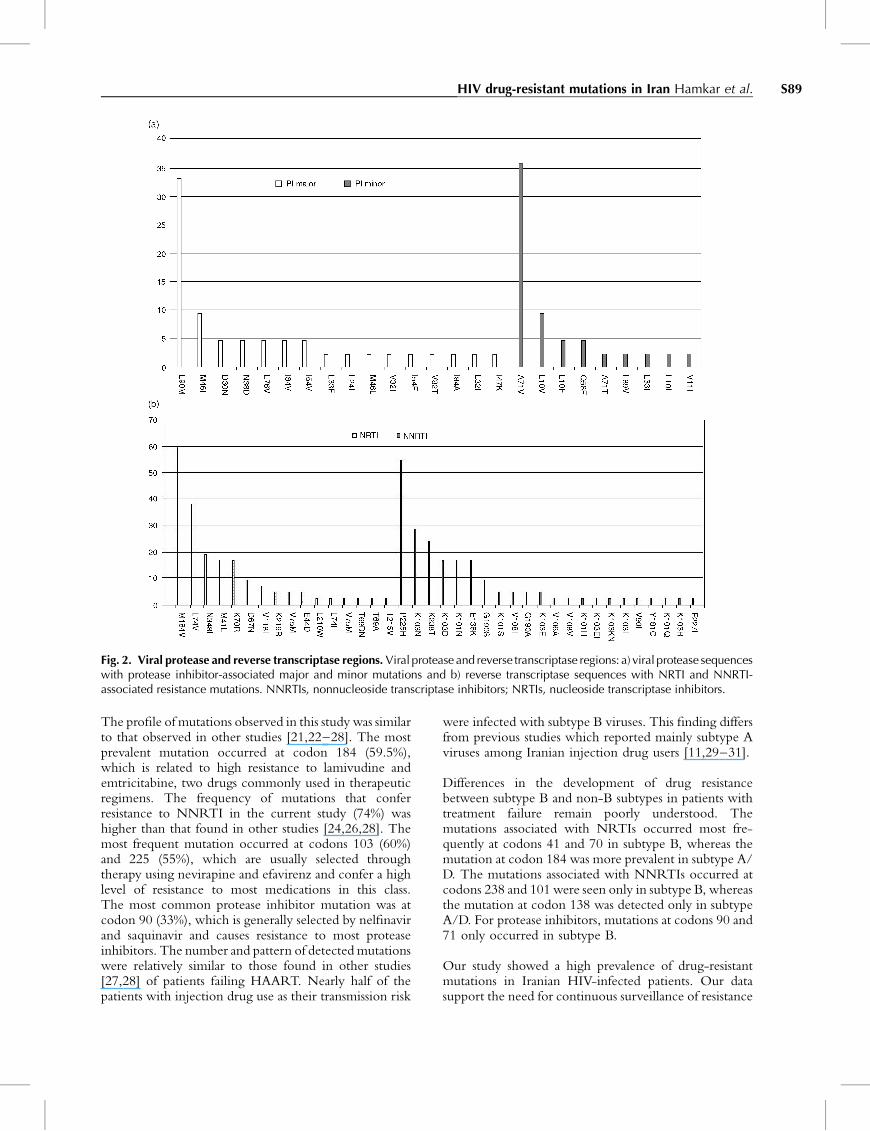
The prevalence of NRTI, NNRTI and protease inhibitormutations was 76, 74 and 45%, respectively. Thedistributions of major and minor drug-resistant mutationsin the viral protease and reverse transcriptase genes arepresented in Fig. 2(a and b). The most common proteaseinhibitor major mutations were L90M (33%), M46I(10%) and I84V, I54V, L76V, N88D, D30N (5% each).The most frequent protease inhibitor minor mutationswere seen at positions A71V (36%), L10V (10%), L10F(5%) and Q58E (5%) (Fig. 2a). The distribution ofresistance mutations in reverse transcriptase sequences was
as follows: M184V (60%), L74V (38%), N348I (19%),K70R (17%), M41L (17%) and D67N (10%) wereassociated with NRTI resistance; P225H (55%), K103N(29%), K238T (24%), K103D (17%), K101N (17%),E138K (17%) and G190S (10%) were associated withNNRTI resistance (Fig. 2b).
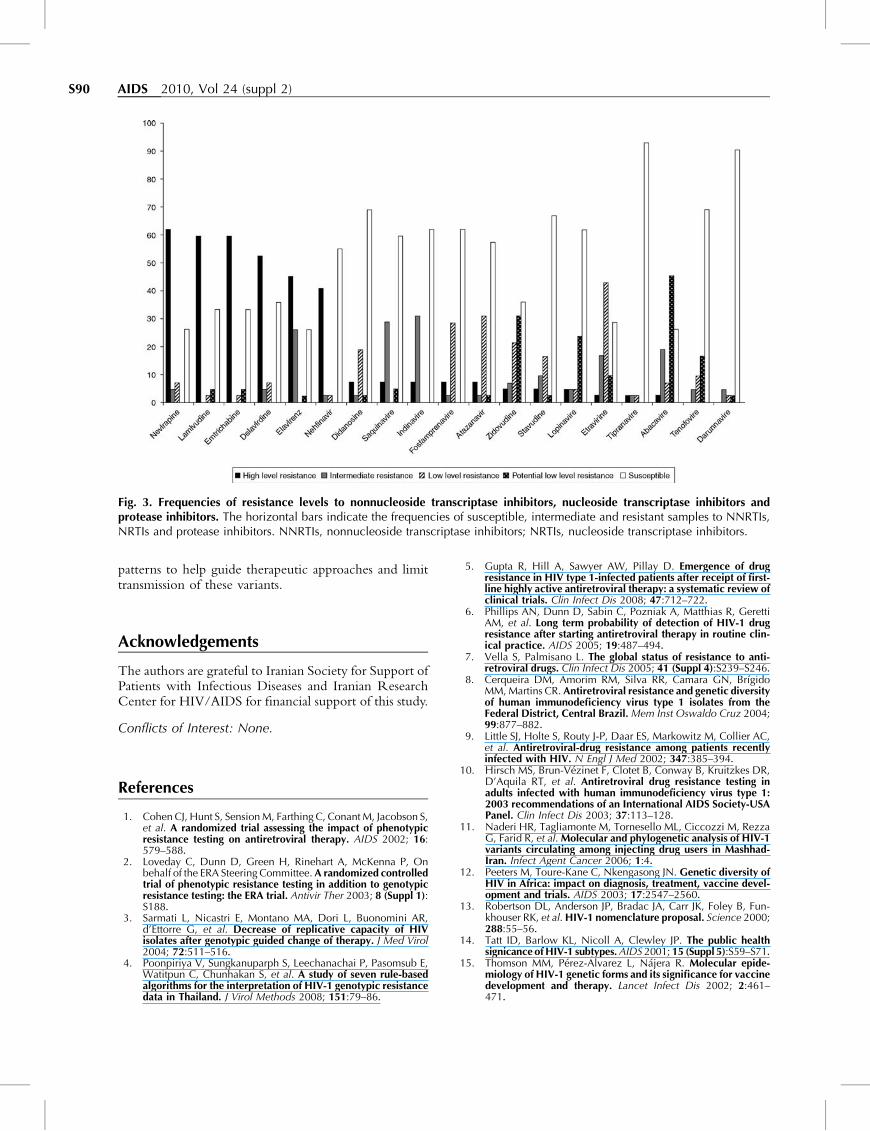
Drug-resistant mutations tended to be most common insubtype B (53%) and A/D recombinant strains (44%),although not statistically significant. No drug-resistantmutations were detected in subtype A. In the reversetranscriptase gene, NRTI-resistant mutations M41L andK70R appeared more prevalent in subtype B, whereas theM184V mutation appeared more frequently with subtypeA/D. NNRTI-resistant mutations K101N, K103D andK238T tended to be more frequently linked with subtypeB, whereas K103N and E138K mutations appeared morecommon with subtype A/D. In the viral protease gene,amino acid substitutions L90M and A71Vappeared moreoften with subtype B. NRTI drug resistance appearedmore common (76.2%) than resistance to other drugclasses (NNRTI 74% and protease inhibitor 45%). Thefrequency of resistance levels to NNRTI, NRTI andprotease inhibitor is shown in Fig. 3. Resistance tonelfinavir (41%, high-level resistance) and indinavir (31%,intermediate resistance) were most common among theprotease inhibitor. For NNRTI, the frequencies ofresistant isolates were 62% to nevirapine, 52% todelavirdine and 45% to efavirenz. For NRTI, thefrequencies of high-level resistance to lamivudine andemtricitabine were approximately 60% for both.
Discussion
The current study found that subtype A/D had thegreatest circulation in Iran, followed by subtype B. Thefrequency of mutations was high for all classes ofantiretrovirals in treated HIV-infected patients. NRTIresistance was most frequently detected, occurring in overthree quarters of the samples.
S88 AIDS 2010, Vol 24 (suppl 2)
Fig. 1. Neighbor-joining protease and reverse transcriptase tree including all sequenced specimens and indicating the putativesubtype of each isolate. Reference sequences for A, B subtypes and also for A/D and A/E recombinants from the GenBank databasewere also included. Numbers next to the nodes of the tree represent bootstrap values (1000 replicates). The sequences determinedin this study are indicated by prefix Ir-HIV-DR.
HIV drug-resistant mutations in Iran Hamkar et al. S89
Fig. 2. Viral protease and reverse transcriptase regions. Viral protease and reverse transcriptase regions: a) viral protease sequenceswith protease inhibitor-associated major and minor mutations and b) reverse transcriptase sequences with NRTI and NNRTI-associated resistance mutations. NNRTIs, nonnucleoside transcriptase inhibitors; NRTIs, nucleoside transcriptase inhibitors.
The profile of mutations observed in this study was similarto that observed in other studies [21,22–28]. The mostprevalent mutation occurred at codon 184 (59.5%),which is related to high resistance to lamivudine andemtricitabine, two drugs commonly used in therapeuticregimens. The frequency of mutations that conferresistance to NNRTI in the current study (74%) washigher than that found in other studies [24,26,28]. Themost frequent mutation occurred at codons 103 (60%)and 225 (55%), which are usually selected throughtherapy using nevirapine and efavirenz and confer a highlevel of resistance to most medications in this class.The most common protease inhibitor mutation was atcodon 90 (33%), which is generally selected by nelfinavirand saquinavir and causes resistance to most proteaseinhibitors. The number and pattern of detected mutationswere relatively similar to those found in other studies[27,28] of patients failing HAART. Nearly half of thepatients with injection drug use as their transmission risk
were infected with subtype B viruses. This finding differsfrom previous studies which reported mainly subtype Aviruses among Iranian injection drug users [11,29–31].
Differences in the development of drug resistancebetween subtype B and non-B subtypes in patients withtreatment failure remain poorly understood. Themutations associated with NRTIs occurred most fre-quently at codons 41 and 70 in subtype B, whereas themutation at codon 184 was more prevalent in subtype A/D. The mutations associated with NNRTIs occurred atcodons 238 and 101 were seen only in subtype B, whereasthe mutation at codon 138 was detected only in subtypeA/D. For protease inhibitors, mutations at codons 90 and71 only occurred in subtype B.
Our study showed a high prevalence of drug-resistantmutations in Iranian HIV-infected patients. Our datasupport the need for continuous surveillance of resistance
S90 AIDS 2010, Vol 24 (suppl 2)
Fig. 3. Frequencies of resistance levels to nonnucleoside transcriptase inhibitors, nucleoside transcriptase inhibitors andprotease inhibitors. The horizontal bars indicate the frequencies of susceptible, intermediate and resistant samples to NNRTIs,NRTIs and protease inhibitors. NNRTIs, nonnucleoside transcriptase inhibitors; NRTIs, nucleoside transcriptase inhibitors.
patterns to help guide therapeutic approaches and limittransmission of these variants.
Acknowledgements
The authors are grateful to Iranian Society for Support ofPatients with Infectious Diseases and Iranian ResearchCenter for HIV/AIDS for financial support of this study.
Conflicts of Interest: None.
References
1. Cohen CJ, Hunt S, Sension M, Farthing C, Conant M, Jacobson S,et al. A randomized trial assessing the impact of phenotypicresistance testing on antiretroviral therapy. AIDS 2002; 16:579–588.
2. Loveday C, Dunn D, Green H, Rinehart A, McKenna P, Onbehalf of the ERA Steering Committee. A randomized controlledtrial of phenotypic resistance testing in addition to genotypicresistance testing: the ERA trial. Antivir Ther 2003; 8 (Suppl 1):S188.
3. Sarmati L, Nicastri E, Montano MA, Dori L, Buonomini AR,d’Ettorre G, et al. Decrease of replicative capacity of HIVisolates after genotypic guided change of therapy. J Med Virol2004; 72:511–516.
4. Poonpiriya V, Sungkanuparph S, Leechanachai P, Pasomsub E,Watitpun C, Chunhakan S, et al. A study of seven rule-basedalgorithms for the interpretation of HIV-1 genotypic resistancedata in Thailand. J Virol Methods 2008; 151:79–86.
5. Gupta R, Hill A, Sawyer AW, Pillay D. Emergence of drugresistance in HIV type 1-infected patients after receipt of first-line highly active antiretroviral therapy: a systematic review ofclinical trials. Clin Infect Dis 2008; 47:712–722.
6. Phillips AN, Dunn D, Sabin C, Pozniak A, Matthias R, GerettiAM, et al. Long term probability of detection of HIV-1 drugresistance after starting antiretroviral therapy in routine clin-ical practice. AIDS 2005; 19:487–494.
7. Vella S, Palmisano L. The global status of resistance to anti-retroviral drugs. Clin Infect Dis 2005; 41 (Suppl 4):S239–S246.
8. Cerqueira DM, Amorim RM, Silva RR, Camara GN, BrıgidoMM, Martins CR. Antiretroviral resistance and genetic diversityof human immunodeficiency virus type 1 isolates from theFederal District, Central Brazil. Mem Inst Oswaldo Cruz 2004;99:877–882.
9. Little SJ, Holte S, Routy J-P, Daar ES, Markowitz M, Collier AC,et al. Antiretroviral-drug resistance among patients recentlyinfected with HIV. N Engl J Med 2002; 347:385–394.
10. Hirsch MS, Brun-Vezinet F, Clotet B, Conway B, Kruitzkes DR,D’Aquila RT, et al. Antiretroviral drug resistance testing inadults infected with human immunodeficiency virus type 1:2003 recommendations of an International AIDS Society-USAPanel. Clin Infect Dis 2003; 37:113–128.
11. Naderi HR, Tagliamonte M, Tornesello ML, Ciccozzi M, RezzaG, Farid R, et al. Molecular and phylogenetic analysis of HIV-1variants circulating among injecting drug users in Mashhad-Iran. Infect Agent Cancer 2006; 1:4.
12. Peeters M, Toure-Kane C, Nkengasong JN. Genetic diversity ofHIV in Africa: impact on diagnosis, treatment, vaccine devel-opment and trials. AIDS 2003; 17:2547–2560.
13. Robertson DL, Anderson JP, Bradac JA, Carr JK, Foley B, Fun-khouser RK, et al. HIV-1 nomenclature proposal. Science 2000;288:55–56.
14. Tatt ID, Barlow KL, Nicoll A, Clewley JP. The public healthsignicance of HIV-1 subtypes. AIDS 2001; 15 (Suppl 5):S59–S71.
15. Thomson MM, Perez-Alvarez L, Najera R. Molecular epide-miology of HIV-1 genetic forms and its significance for vaccinedevelopment and therapy. Lancet Infect Dis 2002; 2:461–471.
HIV drug-resistant mutations in Iran Hamkar et al. S91
16. Perrin L, Kaiser L, Yerly S. Travel and the spread of HIV-1genetic variants. Lancet Infect Dis 2003; 3:22–27.
17. SaitouN,Nei M. The neighbor-joiningmethod: a new method forreconstructing phylogenetic trees. Mol Biol Evol 1987; 4:406–425.
18. Kimura M. A simple method for estimating evolutionary ratesof base substitutions through comparative studies of nucleotidesequences. J Mol Evol 1980; 16:111–120.
19. Tamura K, Dudley J, Nei M, Kumar S. MEGA4: molecularevolutionary genetics analysis (MEGA) software version 4.0.Mol Biol Evol 2007; 24:1596–1599.
20. Felsenstein J. Confidence limits on phylogenesis: an approachusing the bootstrap. Evolution 1985; 39:783–791.
21. Varella RB, Ferreira SB, Castro MB, Tavares MD, Zalis MG.Prevalence of resistance-associated mutations in human immu-nodeficiency virus type 1-positive individuals failing HAART inRio de Janeiro, Brazil. Braz J Infect Dis 2008; 12:380–384.
22. Panos G, Charatsis G, Paparizos V, Kazantzi M, Falagas ME.Prevalence of genotypic resistance to nucleoside analogues,nonnucleoside analogues, and protease inhibitors in HIV-in-fected persons in Athens, Greece. AIDS Res Hum Retroviruses2008; 24:43–51.
23. Marconi VC, Sunpath H, Lu Z, Gordon M, Koranteng-Apeagyei K,Hampton J,etal.PrevalenceofHIV-1 drugresistanceafter failureof a first highly active antiretroviral therapy regimen in KwaZuluNatal, South Africa. Clin Infect Dis 2008; 46:1589–1597.
24. Torres Rivera B, Valles V, Rıos Olivares E. Prevalence ofprimary and secondary resistant mutations to antiretroviraldrug in a population of Puerto Rican infected with HIV. P RHealth Sci J 2002; 21:329–336.
25. McColl DJ, Chappey C, Parkin NT, Miller MD. Prevalence,genotypic associations and phenotypic characterization ofK65R, L74V and other HIV-1 RT resistance mutations in acommercial database. Antivir Ther 2008; 13:189–197.
26. Jlizi A, Ben Ammar El Gaaied A, Slim A, Tebourski F, BenMamou M, Ben Chaabane T, et al. Profile of drug resistancemutations among HIV-1-infected Tunisian subjects failing anti-retroviral therapy. Arch Virol 2008; 153:1103–1108.
27. Couto-Fernandez JC, Silva-de-Jesus C, Veloso VG, Rachid M,Gracie RS, Chequer-Fernandez SL, et al. Human immuno-deficiency virus type 1 (HIV-1) genotyping in Rio de Janeiro,Brazil: assessing subtype and drug-resistance associatedmutations in HIV-1 infected individuals failing highly activeantiretroviral therapy. Mem Inst Oswaldo Cruz 2005; 100:73–78.
28. Cavalcanti AM, Lacerda HR, Brito AM, Pereira S, Medeiros D,Oliveira S. Antiretroviral resistance in individuals presentingtherapeutic failure and subtypes of the human immunodefi-ciency virus type 1 in the Northeast Region of Brazil. Mem InstOswaldo Cruz 2007; 102:785–792.
29. Sarrami-Forooshani R, Das SR, Sabahi F, Adeli A, Esmaeili R,Wahren B, et al. Molecular analysis and phylogenetic char-acterization of HIV in Iran. J Med Virol 2006; 78:853–863.
30. Tagliamonte M, Naderi HR, Tornesello ML, Farid R, BuonaguroFM, Buonaguro L. HIV type 1 subtype A epidemic in injectingdrug user (IDU) communities in Iran. AIDS Res Hum Retro-viruses 2007; 23:1569–1574.
31. Soheilli ZS, Ataiee Z, Tootian S, Zadsar M, Amini S, Abadi K,et al. Presence of HIV-1 CRF35_AD in Iran. AIDS Res HumRetroviruses 2009; 25:123–124.
Related Documents











