Assessing market incentive policies in Kenya with a food security and nutrition perspective: a macro- microsimulation approach Ramos, M.P Custodio, E Jiménez, S Mainar-Causapé, A Boulanger, P Ferrari, E EUR 30034 EN

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Assessing market incentive policies in Kenya with a food security and nutrition perspective: a macro-microsimulation approach
Ramos, M.P Custodio, E
Jiménez, S
Mainar-Causapé, A
Boulanger, P
Ferrari, E
EUR 30034 EN

This publication is a Technical report by the Joint Research Centre (JRC), the European Commission’s science and knowledge service. It aims
to provide evidence-based scientific support to the European policymaking process. The scientific output expressed does not imply a policy position of the European Commission. Neither the European Commission nor any person acting on behalf of the Commission is responsible for the use that might be made of this publication. For information on the methodology and quality underlying the data used in this
publication for which the source is neither Eurostat nor other Commission services, users should contact the referenced source. The designations employed and the presentation of material on the maps do not imply the expression of any opinion whatsoever on the part of the European Union concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of
its frontiers or boundaries. Contact information
Name: Emanuele Ferrari Address: Calle Inca Garcilaso, Seville Email: [email protected]
Tel.: +34 954 488461 EU Science Hub
https://ec.europa.eu/jrc
JRC119390 EUR 30034 EN
PDF ISBN 978-92-76-14654-4 ISSN 1831-9424 doi:10.2760/925912
Luxembourg: Publications Office of the European Union, 2020
The reuse policy of the European Commission is implemented by the Commission Decision 2011/833/EU of 12 December 2011 on the reuse of Commission documents (OJ L 330, 14.12.2011, p. 39). Except otherwise noted, the reuse of this document is authorised under the Creative Commons Attribution 4.0 International (CC BY 4.0) licence (https://creativecommons.org/licenses/by/4.0/). This means that reuse
is allowed provided appropriate credit is given and any changes are indicated. For any use or reproduction of photos or other material that is not owned by the EU, permission must be sought directly from the copyright holders.
All content © European Union, 2020, except cover photos [image #1, Fruit and Vegetable Market © derejeb – stock.adobe.com]; [image #2, Small squared fields at sunset, Great Rift Valley, Kenya © malajscy – stock.adobe.com].
How to cite this report: Ramos, MP; Custodio, E; Jiménez, S; Mainar-Causapé, A; Boulanger, P; and Ferrari, E. Improving food security and nutrition indicators in Kenya through market incentives: a macro-microsimulation approach, EUR 30034 EN , Publications Office of the European Union, Luxembourg, 2020, ISBN 978-92-76-14654-4, doi:10.2760/925912, JRC119390.

1
Contents
1. Introduction ......................................................................................................................................................................................................................................................... 3
2. Methodological Approach .......................................................................................................................................................................................................................... 6
2.1. Food security and nutrition indicators ..................................................................................................................................................................... 6
2.1.1. Food security .................................................................................................................................................................................................................... 7
2.1.1.1. Indirect outcomes .................................................................................................................................................................................................... 7
2.1.1.2. Direct outcomes-Food consumption ............................................................................................................................................................ 7
2.1.2. Nutrition ............................................................................................................................................................................................................................... 8
2.2. Modelling .................................................................................................................................................................................................................................... 8
2.2.1. CGE model for Kenya ............................................................................................................................................................................................... 10
2.2.2. Non-parametric MS approach ............................................................................................................................................................................ 10
2.3. Data sources and treatments .................................................................................................................................................................................... 11
2.3.1. Kenya SAM (2014) and CGE simulations .................................................................................................................................................... 11
2.3.2. Kenya Integrated Household Budgetary Survey (2015/2016) ...................................................................................................... 13
2.3.3. Kenya Food Composition Tables (2018) ...................................................................................................................................................... 14
3. Results ................................................................................................................................................................................................................................................................. 15
3.1. Food Security and Nutrition Indicators in Kenya: descriptive analysis ............................................................................................ 15
3.1.1. Food Security ................................................................................................................................................................................................................. 15
3.1.2. Nutrition ............................................................................................................................................................................................................................ 19
3.2. Fertiliser policy reform: macro-micro simulations results ....................................................................................................................... 20
3.2.1. Food access .................................................................................................................................................................................................................... 21
3.2.2. Food consumption ...................................................................................................................................................................................................... 23
3.2.2.1. Calories ....................................................................................................................................................................................................................... 23
3.2.2.2. Macronutrients ....................................................................................................................................................................................................... 25
4. Conclusions ...................................................................................................................................................................................................................................................... 31
References ................................................................................................................................................................................................................................................................. 32
List of abbreviations and definitions ........................................................................................................................................................................................................ 35
List of figures .......................................................................................................................................................................................................................................................... 36
List of tables ............................................................................................................................................................................................................................................................ 37
Annexes ....................................................................................................................................................................................................................................................................... 38
Annex 1. Table A.1. Atwater conversion factors ....................................................................................................................................................................... 38
Annex 2. Table A.2. Consumption prices variation by food item (SAM code) from the CGE mode simulations – All scenarios. ................................................................................................................................................................................................................................................................................. 38
Annex 3. Table A.3. Fertiliser scenario - Quantities variations by food item and households from the CGE mode simulations. ................................................................................................................................................................................................................................................................................. 40
Annex 4. Table A.4. Fertiliser scenario + subsidy Remove scenario- Quantities variations by food item and households from the CGE mode simulations. .................................................................................................................................................................................................................... 42

2
Annex 5. Table A.5. Fertiliser scenario + Market Access- Quantities variations by food item and households from the CGE mode simulations. ....................................................................................................................................................................................................................................... 44
Annex 6. Table A.6. Fertiliser scenario + Extension scenario- Quantities variations by food item and households from the CGE mode simulations. ............................................................................................................................................................................................................................. 46
Annex 7. Table A.7. Food matching between Kenya SAM 2014 and KIHBS 2015/2016SAM ..................................................................... 48

1
Acknowledgements
The estimation of households' nutrient apparent consumption was done in collaboration with the Statistics Division at the Food and Agricultural Organization of the United Nations. We would like to thank Ana Moltedo, Cristina Alvarez and Talent Manyani for their invaluable contribution and technical advice in the construction of a nutrition conversion table to convert food quantities into nutrients.
Authors
Maria Priscila Ramos, IIEP-Baires (UBA-CONICET)
Estefania Custodio, JRC Seville
Sofía Jimenez Calvo, JRC Seville and Universidad de Zaragoza
Alfredo Mainar-Causapé, JRC Seville
Pierre Boulanger, JRC Seville
Emanuele Ferrari. JRC Seville

2
Abstract
Kenya, such as other African countries, is particularly concerned about the achievement of the Sustainable Development Goal #2 (SDG #2: zero hunger), and its associated consequences for the society. Empirical evidence about food security and nutrition in Kenya accounts for deficiencies in food access, food sufficiency and food quality at the household level. These deficiencies are among others the causes of all forms of malnutrition (stunting, wasting and overweight), which can lead to cognitive impairment, limited immunity to diseases, low educational performance, increased risk of chronic disease and even mortality cases of children in this country.
To solve the food security and nutrition problems in Kenya is a challenging issue because of the different dimensions to be tackled (economic, environmental, educational, health and sanitation) and also because of the heterogeneity that characterizes households (income and food expenditure, education level of households’ head, regional sanitation coverage, access to potable water / waste water system, etc.).
In the recent past, the Government of Kenya supported the construction of a roughly €1.1 billion fertilizer plant in Eldoret in the framework of a fertilizer cost reduction strategy aiming at stabilizing fertilizer prices and making fertilizer more accessible through local manufacturing, blending and bulk procurement. Increasing the domestic production of fertilizers should reduce the price of fertilizer, making them more accessible for farmers. Co-authors of this report, employing the STatic Applied General Equilibrium for DEVelopment (STAGE-DEV) Computable General Equilibrium (CGE) model, calibrated on a Social Accounting Matrix Kenya 2014, evaluated the impact on food security of the creation of the fertiliser plant together with three additional policy scenarios (market access, extension and subsidies removal). For the purpose of this study, we developed a macro-micro simulation model, based on the previously developed CGE and policy scenarios and on microsimulations using the Kenya Integrated Household Budged Survey 2015/2016.
The objective is to produce new set of food security indicators using macro-micro model linkages and it is purely methodological. The policy results, which should be taken with some caution, are discussed in terms of initial economic (per capita income), food security (household dietary diversity and dietary energy consumption) and children’s nutritional (stunting, wasting) status at the household level. Furthermore, national results are disaggregated by metropolitan areas (Nairobi and Mombasa) and the rest of urban and rural zones of the country.
Main results suggest that increasing fertilizers’ availability coupled with increasing market access through the improvement of infrastructures and the reduction of transport costs (market access scenario) will increase overall purchasing power. Supporting pro-poor growth, this development will benefit the most those households with lower diet diversity and higher stunting rates. This policy scenario also leads to the largest increases in diet energy consumption, with similar distributive results as for the purchasing power impact. Increasing fertilizers’ availability paired with improving crops productivity in agricultural practices (extension scenario) leads to the largest increase in energy consumption, particularly from fats in the diet, among households with low diet diversity. Average protein and carbohydrate consumption at national level increase the most within the market access scenario.
The results confirm the findings of the previous report. Increasing fertilizer availability in Kenya is not enough to improve food security in the country. The contribution of complementary policies, such as increasing the market access for fertilizers and agriculture by improving the rural infrastructure or improving the extension services to train small-holder farmers about fertilizer and land use, that give farmers better access to input and output markets is needed.

3
1. Introduction
During the last fifteen years, Kenya has made steady progress towards the Sustainable Development Goal #2 (SDG Goal #2), which aims at ending hunger and all forms of malnutrition, one of the top priorities of the Kenyan food and nutritional agenda. The 2018 Global Nutrition Report shows that the country is on course to meet the global nutrition targets for stunting (a measure of growth retardation), wasting (severe thinness, a form of acute malnutrition), and overweight in children (Global Nutrition Report, 2018) although stunting is still high and overweight among adolescents and adults an increasing concern. Moreover, the Global Report on Food Crises (FSIN 2019) identified Kenya as a country experiencing severe food insecurity problems.
Although the World Bank reclassified Kenya’s economy as lower-middle income in 2014, poverty, food insecurity, and malnutrition high (WFP, 2018).
In relation to malnutrition, stunting has decreased in Kenya significantly from 40% to 26% in the 2000 to 2014 period. However, progress has been uneven, with regions like Coast, Eastern or Rift Valley still with very high levels of stunting at 30% or above (National Bureau of Statistics Kenya, 2014). Stunting or growth retardation has been related to impaired cognitive development, poor immunity to disease, poor educational performance and lower work productivity in adulthood (Dewey and Bequm, 2011).
Regarding acute malnutrition, the last demographic and health survey (DHS) conducted in Kenya in 2014 showed that wasting was no longer a public health problem at national level (with an estimated prevalence of 4%). However, it was still a great concern in the North Eastern province (estimated at 13%), and in recent years some counties of the arid and semi/arid lands of Kenya surpassed the 15% wasting prevalence, which is considered the emergency threshold according to the World Health Organization (WHO) (National Bureau of Statistics Kenya, 2014). Wasting is characterized by extreme weight loss and, in its severe form, can lead to death
While the overweight estimates in children below 5 years has also decreased from 8% to 4% between 2000 and 2014, the overweight among female school-age children and adolescents aged 5 to 19 years has increased from 7 % to 16%, and among female adults from 22% to 34% in the same period. Overweight and obesity are associated with non-communicable diseases like diabetes, coronary heart disease and stroke (WHO, 2003).
The United Nations Children's Fund (UNICEF) malnutrition framework (UNICEF and WHO, 2010) defines the immediate causes of children's malnutrition as the inadequate dietary intake and the presence of disease at individual level. These, in turn, are affected by the underlying causes measured at household level that can be aggregated in the categories of food insecurity, inadequate caring practices and an unhealthy environment. The basic causes of malnutrition encompass structural causes at the population level, including poverty, low educational coverage, unemployment, etc. (Bhutta et al., 2013).
Current dietary intakes in Kenya provide evidence of inadequate consumption among adults of several food groups like vegetables, fruits, nuts and seeds or meat, and of nutrients like calcium, iron, folic acid or omega 3 fatty acids (Global Nutrition Report, 2018). Moreover, only 22% of children aged 6 to 24 months receive an adequate diet in terms of quantity and quality (National Bureau of Statistics Kenya et al., 2015). Diet inadequacy can be the result of inappropriate caring practices and/or food insecurity at household level as underlying causes.
In relation to food insecurity, in January 2018 it was estimated that 2.35 million people were acutely food insecure in Kenya. The most severe conditions existing the arid and semi-arid drought-prone north, which accounts for 80 percent of the country’s landmass and is often disrupted by local conflicts. Between 2016 and 2018, three consecutive poor rainy seasons affected agricultural productivity and caused livestock emaciation and animal deaths, leading to severe shortages of livestock products. Fall armyworm infestations and locust invasions also caused substantial destruction of crop, pasture and browse. Furthermore, the proportion of Kenyans living on less than the international poverty lined, although it has declined over the last decade is still high at 36% overall, and it can raise to 80% in the north-eastern parts of the country (FSIN, 2019).
The Kenya Agriculture Research Institute attributes the food insecurity problems in the country, among other factors, to the frequent droughts in most counties and to increasing food prices. Global food prices get high, but also the costs of domestic food production are elevated, mainly due to the high costs of inputs (especially fertilizers) that coupled with the low purchasing power of large proportions of the population have an important impact on the food insecurity of the Kenyan families (Kenya Agricultural Research Institute, 2012).
One of the economic issues related to food security and malnutrition is food access, which includes enough supply, affordability of food and adequate chain of food distribution. Even when the econometric literature finds a positive correlation between improving commercialization of food items and nutrition in Sub-Saharan Africa (SSA), there are not yet robust econometric results proving this link (Carletto et al., 2017). In the particular case of Kenya there is only weak econometric evidence showing that the improvement of retail distribution of food (i.e., supermarkets) has an impact on the composition of the consumption basket at the household level. The effect observed was a switch from unprocessed foods to highly processed foods consumption, being the former relatively healthier than the latter, so a deterioration of diet quality (nutrition) is expected (Demmler et al., 2018). Nevertheless, when there are farmers who benefit from a better

4
chain of distribution of their food production through supermarkets, their income increases leading to an improvement in the food access dimension (income effect) (Chege et al., 2015). Here we refer to two different dimensions of the problem, the quality of food consumption in nutritional terms and the quantity of food access when the real farmer's income increases.
Furthermore, there are several studies suggesting the impact of increasing income on the intake of macronutrients and micronutrients in other SSA countries. Concerning particular macronutrients such as protein from animal sources, econometric estimations of six SSA countries (excluding Kenya) suggest that the demand of meat and fish displays high-income elasticities, thus growth or policies that impact income could particularly change the composition of the consumption households baskets and thus improve the nutritional content of their diets in terms of animal protein. However, the choice of the policy is not negligible since it could mean either an increase in highly processed foods or an increase in unprocessed foods depending on the change in relative prices (Desiere et al., 2018).
Ecker et al. (2010) find that deficiencies in micronutrient intake (Vitamin A, iron and zinc) in East African countries are highly and positively correlated with caloric deficiency and suggests that improving purchasing power through public policies could tackle both economic and nutritional issues.
Finally, considering that poverty is one of the main basic causes of malnutrition (Akombi et al., 2017), improvement of economic and welfare conditions of households through public policies related to food security can be one of the appropriate means to tackle food security and nutritional problems in Kenya1. The policies that address the underlying or basic causes of malnutrition are defined as nutrition sensitive. They are directed to the pathways by which agriculture or other sectors can influence nutrition There is evidence that such nutrition-sensitive interventions in agriculture have the potential to enhance the scale and effectiveness of nutrition-specific interventions (which target the immediate causes of undernutrition: inadequate diet and disease) (Ruel et al., 2013). A study in Kenya shows that in some rural areas, although household heads are aware of their diet deficiencies thanks to nutrition education interventions (nutrition specific), the resource constraints (income) and the change in relative prices of food highly determine the caloric intake and the degree of dietary diversity in their households (Byrd et al., 2017).
The Kenya Ministry of Devolution and Planning has designed a working agenda to ensure progress in the attainment of SDG Goal #2 that includes fast track interventions to enhance high quality and quantity of food production, access and availability through increased agricultural productivity. The Kenyan government has been implementing projects related to irrigation; interventions to transform agriculture from subsistence to productive commercial farming; subsidization of fertilizers and seeds; construction and renovation of fresh-produce markets; and provision of extension services to improve horticultural and livestock farming, among others (Kenya Ministry of Devolution and Planning, 2017).
The Joint Research Centre (JRC),is committed under the Administrative Arrangement JRC №33272-2013-10 DEVCO 325863 between DG Development And Cooperation – Europeaid and DG Joint Research Centre (DG JRC) to provide support for: i) improvement of information systems on agriculture, nutrition and food security, ii) policy and economic analysis to support policy decision-making process and iii) scientific advice on selected topics concerning sustainable agriculture and food and nutrition security. In the framework of this commitment, the Economics of Agriculture Unit (JRC.D.4) of the Sustainable Development directorate is responsible to elaborate the methodology and tools to provide macroeconomic analysis of the national and regional economic systems related to: sustainability of policies in the sectors of agriculture, social transfer and fight against food and nutrition insecurity.
In this context, in 2017 the JRC analysed the impacts of the construction of a new fertilizer plant on the agricultural sector and the rest of the Kenyan economy (Boulanger P et al, 2017). Boulanger et al. (2017) calibrated a tailored version of a single-country Computable General Equilibrium (CGE) model to an original 2014 Social Accounting Matrix (SAM) for Kenya. In the main scenario, the new fertilizer factory increases domestic fertilizer production by 100%. They also took into account as main constraints poor infrastructure and lack of extension services, and tested different scenarios. Results suggested that in order to increase agricultural production and reduce rural poverty the increase in fertilizers availability should be coupled with other policies related to increasing market access and improving rural infrastructures. However, Boulanger et al. (2017) treated the food security and nutrition dimensions only peripherally and using aggregated national food consumption data compiled using the Kenya food balance sheet.
Thus, the aim of this study is to bring an in-depth perspective of the food security and nutrition dimensions into the former fertilizers policy analysis. And more specifically, to evaluate the impact of the fertiliser policy reform on food access, food consumption, and malnutrition by geographical areas and according to the degree of malnutrition measured at the household level.
For that purpose, we used food consumption and nutrition data collected at the household level instead of the aggregated information at national level provided by food balance sheets. Given the heterogeneity across households, concerning their food security and nutrition related characteristics and also the multi-dimensionality of food insecurity and malnutrition causes (economic and non-economic), we developed a macro-micro simulation model for Kenya. The methodology
1 Other sectors to be addressed for the improvement of nutrition are health, wash and education.

5
combines the policy simulations from the STatic Applied General Equilibrium for DEVelopment (STAGE-DEV) Computable General Equilibrium (CGE) model (Boulanger et al., 2017) calibrated on the Kenyan Social Accounting Matrix (SAM) for 2014 (Mainar-Causapé et al., 2018), with microsimulations using non-parametric regressions of food security and nutritional indicators computed based on the Kenya Integrated Household Budgetary Survey (KIHBS) 2015/2016 (KNBS, 2018).
The rest of this report is organised as follows. Section 2 presents and justifies our methodological approach in terms of food security and nutritional indicators to be used, macro-micro simulation modelling and data sources and treatments. Section 3 discusses the results, first concerning the current food security and nutrition situation in Kenya and then the fertiliser policy simulations results in terms of food access, quantity and quality of food consumption at national level and across economic and nutritional characteristics of households. Finally, in Section 4 we conclude and set the possible extensions of future research in this multi-disciplinary field.

6
2. Methodological Approach
Three aspects are essential for the definition and the implementation of our methodological approach to evaluate the impact of the fertiliser policy reform in Kenya on food security and nutrition aspects. The first, the definition of the food security and nutrition indicators used in the analysis and the data availability to construct them (subsection 2.1). The second, the linkage of the CGE and the microsimulation approaches introducing the selected food security and nutrition indicators (subsection 2.2). The third, the evaluation of the data sources available and their treatments for the implementation of the complete methodology (subsection 2.3).
All these methodological aspects and decisions are described below.
2.1. Food security and nutrition indicators
In 2012, the Committee on World Food Security defined food and nutrition security as "Food and nutrition security exists when all people at all times have physical, social and economic access to food, which is safe and consumed in sufficient quantity and quality to meet their dietary needs and food preferences, and is supported by an environment of adequate sanitation, health services and care, allowing for a healthy and active life". (Committee on World Food Security, 2012: 8).
The definition is broad and, at the time being, there is no single indicator that can provide the comprehensive picture of the food security and nutrition situation of a given context. Rather, a set of suitable indicators are needed to describe each of the dimensions in an integrative way.
According to previous literature and limited by the data available in the KIHBS 2015/16, we constructed the food security and nutrition indicators as described below. Although they do not cover all aspects of the food security and nutrition dimensions, they provide a first look from the food security and nutrition perspective
Table 1. Food security and nutrition indicators at the household level.
Dimension Outcomes Measured by Indicators used in this study:
Indirect outcomes
Food access Food expenditure Total food expenditure in the household and food expenditure per capita
Household dietary diversity Household Consumption and Expenditure Surveys Dietary Diversity Score (HCES-DDS)
Food security
Direct outcomes-Food consumption
In terms of calories Total calories consumed Dietary Energy Consumption (DEC) per capita
In terms of macronutrients
Caloric contribution of the different macronutrients (in Kcal)
Caloric contribution of proteins to total calories per capita (in Kcal and %)
Share of the caloric contribution of each macronutrient (in %)
Caloric contribution of fats to total calories per capita (in Kcal and %) Caloric contribution of carbohydrates to total calories per capita (in Kcal and %).
Nutrition Wasting Weight for height z score (WHZ) in children below 5 years of age
Wasting defined as WHZ<-2
Overweight Overweight defined as WHZ>+2
Minimum weight for height z score registered in the household

7
Stunting (HAZ<-2)
Height for age z score (HAZ) in children below 5 years of age
Stunting defined as HAZ<-2
Minimum height for age z score registered in the household
Proportion of stunted children below 5 years of age suffering in the house
2.1.1. Food security
Food security can be measured at household level by direct outcomes of food consumption or by indirect outcomes related to food access, availability and stability (IPC Global partners, 2012). In this study, we used selected direct and indirect outcomes, based on available data, as described below.
2.1.1.1. Indirect outcomes
Based on the available data in KIBHS 2015/16 we decided to use food access as the indirect outcome to proxy food insecurity, using for that purpose the indicators described below.
Food expenditure: The food expenditure is computed at the household level and per capita according to the household composition. The KIHBS 2015/16 provides the expenditure data for each food item. This information offers us the proportion of income expended in food but also, and more specifically, the possibility to compute the expenditure shares by food item in each household. The latter allows computing the consumption effect when the prices of food items change due to a policy reform. This indicator is a measure of change in the purchasing power of food and thus can be a good indicator to evaluate food access, although its interpretation may vary depending on the context (rural or urban).
Household dietary diversity score: One of the indicators used as proxy of food security is the Household Dietary Diversity Score (HDDS) (Swindale & Bilinsky, 2006). The HDDS is computed based on the food consumed at the household in the previous 24 hours (Kennedy et al., 2007; 2010). However, as many household consumption and expenditure surveys collect food consumption data for reference periods longer than 24 hours, the Food and Agriculture Organization of the United Nations (FAO) has proposed the use of an alternative household dietary diversity indicator, the so-called household consumption and expenditure surveys dietary diversity score (HCES-DDS). This indicator can be used for longer reference periods (seven days, two weeks, twelve months, etc.), (Moltedo et al., 2018). As the KIHBS 2015/16 collects the food consumption data for a 7 days period this is the indicator we use for the analysis. The HCES-DDS is computed as a simple unweighted count of food groups consumed by a household during the period of recall, based on the following 16-food group classification: 1. Cereals, 2. Root tubers, 3. Vitamin A rich vegetables, 4. Dark green leafy vegetables, 5. Other vegetables, 6. Vitamin A rich fruits, 7. Other fruits, 8. Organ meat, 9. Flesh meat, 10. Egg, 11. Fish, 12. Pulses, 13. Diary, 14. Oils, 15. Sweets and 16. Miscellaneous (Moltedo et al., 2018).
2.1.1.2. Direct outcomes-Food consumption
The direct outcomes of food consumption in this report are defined in terms of calories and macronutrients as described below.
Calories: to evaluate the quantity of food consumed we calculated the total calories consumed using the Dietary Energy Consumption (DEC) per day per capita indicator.
The first step was to construct the Kenya Nutrient Conversion table (Kenya NCT) in which the 210 food items reported in the KIHBS 2015/16 were matched with the raw forms of the food items from the 2018 Kenya Food Consumption Table (FCT), the FCT KEN2018 (see section 2.3 for detailed description of these datasets). This was done in collaboration with the FAO statistical division. In the cases where direct matching (one food item of the KIHBS 2015/2016 matching with a single food item from the FCT KEN2018) was not possible, the average of the pertinent food items from the FCT KEN2018 was used.
We then computed the DEC by multiplying the daily quantities of all foods consumed in the household (edible portions in grams) as reported in the KIHBS 2015/16 by the kilocalories per gram for each food item as described in the Kenya NCT. Note that the quantities consumed per household were declared for 7 days so all variables were converted per day (divided by 7) and per capita (dividing by household size) in the analysis.

8
Macronutrients: to assess the diet in terms of macronutrients we calculated the calories obtained from each of the energy-yielding macronutrients (fat, proteins and carbohydrates) per day and per capita following the methodology described in the ADePT-FSM software (Moltedo et al., 2014; 2018).
We calculated the nutrient contents of all food items based on the Kenya NCT 2018 nutrition values. These are expressed as grams (g) of nutrients per 100 grams edible portion on a fresh basis, thus we converted quantities in grams using the refuse factor and the density factor.
Once the macronutrients quantities provided by each food item was known, we used the Atwater conversion factors (Table A.1 in the Annexes) to convert them to kilocalories, and thus obtain the caloric contribution of each macronutrient.
In order to infer the potential access to a balanced diet in terms of quality, the shares in the caloric contribution of each macronutrient to the total energy consumed in the household were also calculated.
2.1.2. Nutrition
Nutritional outcomes, by definition, are assessed at the individual level, and one of the most widespread methodologies to do so is anthropometry (systematic body measurements). The KIHBS 2015/2016 collected anthropometric data (weight and height) of children below five years of age that we used to calculate the nutrition indicators described below.
Nutrition indicators were calculated in two steps. In the first step, we calculated the individual nutrition indicators of all children below five, and in a second step, those indicators were aggregated at the household level to obtain a household nutrition indicator.
Step 1: Calculation of individual nutrition indicators for children under 5 years
Wasting/Overweight: is calculated by comparing the weight of the measured child with the mean of the weight of children with same sex and height from the reference population. The number of standard deviations from that mean is then computed (z-score) and reflects how much the child deviates from the mean of the reference population. When the z-score for weight for height (WHZ) is below -2 the child is identified as being wasted (suffering wasting), and below -3 severely so. When the WHZ is above +2 (for children under five years) the child is identified as having overweight.
Stunting: the z scores are calculated by comparing the height of the measured child with the mean of the height of children with same sex and age from the reference population. When the z-score for height for age (HAZ) is below -2 the child is identified as being stunted (suffering stunting), and below -3 severely stunted.
We calculated these indicators with the Anthro Software and using the WHO Child Growth Standards 2006 as the reference population (WHO, 2019).
Step 2: Computation of household nutrition indicators
In order to have meaningful nutrition indicators at household level we constructed the following indicators:
Household minimum WHZ: from the WHZ computed for all children under five in the household we selected the lowest one and defined it as the household minimum WHZ, using it as proxy of the presence of wasting (negative values below -2).
Household minimum HAZ: from the HAZ computed for all children under five in the household we selected the lowest one and defined it as the household minimum HAZ, and we used it as proxy of the presence of stunting (negative values below -2) in the household.
Household proportion of stunted children: we calculated the proportion of stunted children under five out of all children under five living in the household.
2.2. Modelling
In order to achieve the objectives of this report, we will take advantages from the top-down combination of two approaches: a General Equilibrium (GE) Approach and a Micro-Simulations (MS) one using household surveys (Chen & Ravaillon, 2004) for food security and nutritional purposes.
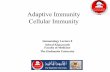
Figure 1 presents a simplified scheme of the top-down macro-microsimulation approach, with the data requirements in
each of the steps, models’ linkage and outputs.

9
Figure 1. Macro-micro top-down methodology scheme.
The GE models allow evaluating the consequences of a policy shock (or even an exogenous shock as a change in international prices of agricultural commodities) over macroeconomic variables as well as by agent and sectors.
Nevertheless, the computation of distributional welfare effects due to the changes in goods' and factors' prices is challenging and sometimes more information that the one available is required. Therefore, such a policy shock becomes a weakness of the GE models. The same is true to measure the change in food consumption patterns and nutritional security status, since the nature of these problems requires the consideration of the heterogeneity of households (and individuals) across different regions of an economy (Akombi et al., 2017; Ecker et al., 2010) and the multi-dimensionality of their causes.
The households are heterogeneous in terms of income and food expenditure and on the gender, economic activity and education level of the household's heads (Chiputwa & Qaim, 2016), among others. Moreover, the communities and regions where they live differ in terms of the environment and climate, the hygiene and sanitation coverage (access to potable water / waste water system) (Ecker et al., 2010) and on the implementation of public policies sensitive to food security and nutrition problems (Breisinger & Ecker, 2014; Desiere et al., 2018; Akombi et al., 2017). Consequently, in order to tackle the food security and nutrition problems with a multi-dimensional perspective, it is necessary to conduct a case-by-case study, by considering these differences across households and regions.
To solve previous limitations of GE models, MS approaches help to better exploit the information about household heterogeneity (preferences and endowments) in a sampled population, and then complement the GE results. These combined approaches have been applied since the beginning of the current century to evaluate poverty consequences of different policies (trade liberalization, subsidies, land use, transfers programs, etc.) testing different ways of integration (bottom-up, top-down, etc.). No significant differences for results appear when full employment is assumed (Cockburn et al., 2014); however, when the change employment/unemployment also matters, welfare impact could be underestimated (Debowicz, 2016). In the case of this research, we will extend the MS approaches to evaluate the change in the food and nutritional situation of households in Kenya using the indicators presented previously.
We further describe the computable GE model for Kenya (Aragie et al., 2017) and its link to the non-parametric MS approach (Deaton, 1989; 1997).

10
2.2.1. CGE model for Kenya
We will use a single-country, multi-product static Computable General Equilibrium (CGE) model, called STAGE-DEV (Aragie et al., 2017). Like any other CGE model, it simulates the variation in economy-wide (e.g., national/regional welfare and gross domestic product) and sector (e.g., production, consumption and trade quantities and prices at the product level) variables resulting from policies scenarios (e.g., agricultural policy reforms). Changes in the consumption patterns resulted from the simulated scenarios will also affect the use of production factors (labour, capital, land and livestock) and their reallocation across sectors.
The richness of this CGE model are the main features and stylized facts that characterize the Kenyan economy (also applied to other SSA countries) to properly model agriculture and food security issues. For instance, the dual roles of semi-subsistent agricultural households, (which play the non-separable double role of producers and consumers) is a key behaviour to evaluate food availability and nutrition. Moreover, factors' market characteristics also are well represented, such as structural rigidities in labour market and factor segmentation; high unemployment/under employment, particularly in rural areas; the use of time in non–productive activities; and migration from rural to urban areas.
When evaluating agricultural policy scenarios (e.g., subsidies on fertilizers) in Kenya with this CGE model, the change in domestic prices, consumed quantities and factor remuneration changes will be the link with the second approaches in our combined top-down methodology. Those changes in prices and consumed quantities will allow assessing the food security impact and its distribution among households based on their income and considering different criteria: national vs. regional; urban vs. rural; and by children nutritional statuses (e.g., households with the presence of stunting or wasting/overweight for at least one of their children).
The following MS approach will be used for food security and nutritional outcomes under the simulated agricultural policy scenarios.
2.2.2. Non-parametric MS approach
In this report, we will apply a non-parametric approach (Deaton, 1989; 1997) to evaluate the change in nutritional status at the household level. This approach has been particularly used to evaluate poverty impact and distributional effect of a policy reform. In this sense, based on the micro data from household surveys in Kenya, we are able to compute the welfare effect as a decomposition of the consumption and the income effects of each scenario. Thus, we get the average welfare impact for all Kenya households and its distribution across standards of living, according to the data available.
In the particular case of the nutritional concerns of agricultural policy reforms, we have to distinguish the measurement of the different dimensions of the food and nutritional security issue discussed before.
First, concerning an equal and stable accessibility in the base of the affordability of food, food access, we compute the food consumption effect (fce) at the household (h) level following the same procedure of a poverty analysis. More precisely, given the expenditure shares of each food item (i) at the household level (Θh,i), we compute the change in the purchasing power of food as a consequence of prices variation (pi) under an agricultural policy reform. Formally, equation (1) shows the way to compute the food consumption effect to each household.
𝑓𝑐𝑒ℎ = σ 𝜃ℎ.𝑖𝑖 ∗ 𝑝𝑖 (1)
Second, as described in section 2.1, in order to measure food consumed in terms of calories or macronutrients, we also need to take into account the change in quantities consumed at the household level when the same policy reform is simulated. For this purpose, we converted all consumed quantities of each food item into calories and then, we added them to compute calories consumed at the household level. The change in calories consumed at the household level per day (dech) is computed as shown in the equation (2), where qh,i represents the percentage change in the consumed edible quantities in grams for each household and each food item per day, Ki, corresponds to caloric value (kilocalories per 100g of food item) provided for each food item.
𝑑𝑒𝑐ℎ = σ 𝐾𝑖 ∗ 𝑞ℎ,𝑖𝑖,𝑗 (2)
Knowing the size of each household, it would be possible to compute it also per capita following the country measurements.
Third, to measure the change in food consumption in qualitative terms (naj,h) we will compute the change in each type of macronutrient (j) consumed at the household level (h). In order to isolate the macronutrient effect due to consumed

11
quantities change, we compute the contribution in calories of each macronutrient in the total calories consumed per day and per person (γi,j). This indicator changes when the scenario also affects total calories and composition of the diet.
𝑛𝑎𝑗,ℎ = σ 𝛾𝑖.𝑗 ∗ 𝑞ℎ,𝑖𝑖 (3)
Similar indicators could be built for micronutrients (e.g., iron, zinc, vitamin A, etc.), which depends on data treatment and compatibility in terms of food items from different datasets.
After microsimulations of the food and nutritional security indicators detailed in equations (1) to (3), we will run non-parametric regressions of those food security results in terms of economic and food security statuses (e.g., the per capita expenditure (in log) distribution as an economic welfare measure of households), and also in terms of other nutritional indicators (e.g., children under malnutrition conditions denoted by the Z scores of stunting and wasting/overweight) to all households, but also exclusively to rural vs. urban (Metropolis and other urban). Non-parametric regressions fit a local relationship between two variables, e.g. the change in DEC per capita (y- variable) and the log of per capita expenditure (x- variable).
2.3. Data sources and treatments
The combination of the macro-micro approaches requires matching at least three different sources of data with different levels of aggregation (SAM of Kenya, KIHBS, and FCT KEN) to make them compatible at the product, sector and regional levels. Thus, databases involved in this report are:
the Social Accounting Matrix (SAM) of Kenya, 2014 (Mainar-Causapé et al., 2018) which is the calibration base for the Kenya CGE model, and the changes in food prices and quantities from the CGE simulations;
the Kenya Integrated Household Budgetary Survey (KIHBS), 2015/2016 which provides the consumption quantities by item, source of origin, total and food expenditure by item and other characteristics at the household and member levels to build nutrition indicators (KIBHS, 2018);
the Kenya Food Composition Tables (FCT KEN2018), which describes the content of foods in terms of nutrients and energy allowing for the calculation of nutritional indicators when combined with the quantities consumed in each household (FAO/Government of Kenya, 2018).
2.3.1. Kenya SAM (2014) and CGE simulations
The CGE approach is calibrated on the Social Accounting Matrix (SAM) for Kenya in 2014 (Mainar-Causapé et al., 2018) . The SAM provides national information disaggregated in nine regions (2 cities and 7 agro-ecological zones).
Moreover, the 666 consumed items by the Kenyan households are aggregated in 50 products and services in the SAM (Table 2). Regarding food and nutritional purposes, we will concentrate this work particularly on 210 items of those 666 from the KIHBS, which correspond to 20 food items from the Kenya SAM. Then, based on the Kenya FCT 2018 we could match each of the 210 items with their nutritional contribution in terms of calories and macronutrients (proteins, fats, carbohydrates).
Furthermore, the SAM presents the information for 35 production factors, 30 types of labours by skills and jobs location, 2 types of lands depending on irrigation (irrigated, non-irrigated area), 2 capitals specific for agriculture (agricultural) and non-agriculture (non-agricultural) sectors and 1 livestock. These factors refer to the sources of households' income in the
survey such as they are detailed in Table 2. These households also receive transfers and rents as part of their incomes.
Even when the SAM displays the private Kenyan agents (24) by quintiles and regions, which is already a large degree of detail, the use of the household’s survey data expands the possibilities to provide the results based on other characteristics of the households that make them heterogeneous within each of the 24 agents’ categories (poor-rich, male-female head, by different nutritional indicators scores, etc.).
Table 2. Mapping between macro-micro models’ data.
STAGE-DEV Kenya SAM 2014 KIHBS survey 2015/2016
Regions r=9 47 districts

12
2 cities
7 agro-ecological zones
Commodities c=50 666 consumption items
20 agri-products 210 food consumption items
3 extractives (fishing, forestry and mining)
14 manufactured goods including food
13 services
Factors f=35
30 labours (3 skills*9 r +RW) 63 ISIC R3 (4 digit)
2 lands (irr, nir) 2 accounts (land and subsoil rents)
external regional data for irrigation
2 capital (ag, na) net benefits 118 ISIC R3 (4 digit) +5 (1 digit)
1 livestock -
other sources (transfers, res/com, rents, etc)
Households h=24 21773 original households
Q5 in cities, RU/UR in agro-eco regions
After consumption and income treatment 21,625 households. After nutrition treatment 7,530
According to the growth projections of the Government of Kenya, the economy should achieve an ambitious growth target. The government is pursuing macroeconomic policies that should benefit key economic sectors. Among them, agriculture should grow by an annual average of about 6.4%. The government prepared a set of policies to achieve the target. These policies will prioritise the implementation of the fertilizer cost reduction strategy, to increase the access of Kenya’s livestock products to regional and international markets, and to support to extension services among others. Boulanger et al., 2017 started from this list of priorities and from a recent piece if news related to the government funding of a brand-new plant to produce fertilisers domestically, to develop a modelling framework using a general equilibrium approach, taking into account the specificities of the Kenyan economy. A main policy scenario and three additional ones inspect the possible impacts of the new fertilizer factories on the Kenyan economy.
Fertiliser scenario: the main scenario simulated the increase (100%) in the Fertiliser domestic production because of a construction of a new fertiliser plant funded by the Kenyan government in the framework of a fertilizer cost reduction strategy. The fertiliser scenario is considered as the central scenario, on top of which we add:
o Subsidy scenario: The Government of Kenya is using an input subsidy programs (National Accelerated Agricultural Inputs Access Program, NAAIAP) to subsidize fertilizers. Subsidies were successful in increasing the fertilizer use but they represent a financial burden on the Kenyan government of almost €27 million yearly. Further, the increase in fertilizer use is sustained by imports and a significant amount of subsidies is paid to import fertilizers. On top of the increase of domestic production, we model a removal of subsidies on fertilisers, to simulate the possible impact of government savings due to subsidy removal.
o Market Access scenario: One of the key issues about the fertilizer use in Kenya is the difficulty to access fertilizer outlets because of poor infrastructure (such as road network) or weakly organized distribution

13
channels. This is reflected in high fertilizers prices due to high trade margins. An improvement in market access due to public investment in infrastructure is simulated reducing trade and transportation margins by 30% on all domestically traded commodities
o Extension scenario: access to extension services is another constraint that limits Kenya's agricultural potential. Access of extension services for farmers shall improve sharing knowledge, technologies and agricultural information, promoting household food and nutrition security by increasing income and reducing poverty. The main benefit of extension services is a more conscious use of fertilizers and seeds with better farming practices. To simulate the impacts of improved to access to extension services, productivity of fertilizer and seed use and labour use by 3%. The government pay the cost to reach more farmers with an additional expenditure in this sector.
Among macroeconomic, sector and households’ results, we have extracted the percentage change in food items’ prices and the consumed quantities variations by food item and for every type of household of each agro-ecological zone under each of the four scenarios described above. These food prices and quantities variations allow for microsimulations at the household level and thus concerning food access, sufficiency and adequacy, on which we are interested (see tables in the Annexes).
Since food security and nutrition variables may greatly differ between rural and urban areas, we have stratified the analysis by areas of residence as follows:
Metropolitan: comprising the two cities of Nairobi and Mombasa;
Other urban: other communities defined as urban in the KIHBS;
Rural: communities defined as rural in the KIHBS.
2.3.2. Kenya Integrated Household Budgetary Survey (2015/2016)
In the framework of our top-down macro-micro simulation approach, the MS one requires household micro data for Kenya and for that we have used the KIHBS for 2015/2016 which is the most recent national household budget survey available. This survey provides the information for 21,773 households (1,131 clusters with 10 households each, 1,834 clusters with 9 households each, 2,190 clusters with 8 households each and 16,618 clusters with 7 households or less).
Among all data collected by the survey during 12 months, we use the household characteristics: location by county (47), urban/rural stratification, number of members, and household composition by age and gender, general health characteristics and nutrition (anthropometric data for children under five years old), household income, expenditure and food consumption by item (210 food items). Among food items we have to eliminate those which are not really food and also those which are related to food consumed away from home (restaurants, bar, canteens, etc.).
When the purpose of combining macro-micro models is to evaluate poverty impact, we generally need two kinds of information: households’ expenditure by item and households’ income by sources. For our purpose, we focus only on the expenditure data to compute the consumption budget shares by food item.
However, in order to address food and nutritional issues related to consumption patterns at the household level, we also need some extra information provided by the KIHBS.
Concerning households’ questionnaires, we have particularly used quantities consumed in the household during the last 7 days (Questionnaire Q1C, SECTION T:4-11.). The KIHBS 2015/16 reports food consumption by source of origin, thus we summed the quantities of food coming from the four sources (purchases, own stock, own production, gifts and other sources) to obtain the total quantity of food consumed in the household before calculating nutrient contents as described in the section 2.1.
After all this treatment and cleaning processes of the data, the sample reduced to 21,625 households.
Another section of the survey collects information on the demographic structure of the household, family ties and sex and age of all family members (Questionnaire 1A, SECTION B: 4-5). This information we used to calculate the adult male equivalents (AME).
Children under five years living in the surveyed households were measured, and anthropometric measurements compiled in section F (Questionnaire 1A, SECTION F: 28). We used these data (age, sex, weight, and length/height of children < 5 years old) to calculate the individual nutrition indicators: wasting (acute malnutrition), stunting (chronic malnutrition) and overweight. In order to compute the malnutrition indicators at household level (as described in section 2.1) we had to merge the household and the children's datasets.

14
2.3.3. Kenya Food Composition Tables (2018)
The Food Composition Tables (FCTs) are essential tools for the calculation of nutritional indicators, as they provide the nutrient content in the food items consumed.
The 2018 is the most updated version of the Kenya Food Composition Table and provides information in a large array of nutrients (energy, macronutrients, main minerals and vitamins, amino acids, fatty acids classes, oxalates and phytate) to determine nutrition adequacy and diet formulation. It displays a larger list of products and with greater detail to the previous 1993 FCT (FAO, 2018).
As described in section 2.1 in order to obtain the nutrient content of the food items collected in the KIHBS survey it was necessary to construct a country specific Nutrient Content Table (NCT), the Kenya NCT, to match food items from the survey (in quantities ) to food items in the FCT (providing calories and nutrients). This is an elaborate process requiring technical expertise. For this exercise, we counted with the experience of Ana Moltedo, Cristina Alvarez, and Talent Manyani from the Statistical Division of the FAO.
In particular, it is essential this compatibility and matching between all these databases in terms of product/sector and regional levels in order to undertake the macro-micro simulations to evaluate the food security and nutritional impact of an agri-policy reform.

15
3. Results
We first describe the current food security and nutritional statuses of households in Kenya, at both national and regional levels (subsection 3.1). Once the current picture is known, we discuss the results of fertiliser policy reforms in terms of food access and food consumption quantitatively and qualitatively (subsection 3.2).
3.1. Food Security and Nutrition Indicators in Kenya: descriptive analysis
According to the chosen food security and nutrition indicators (subsection 2.1) and the data availability (subsection2.3), we describe current situation in Kenya. This picture will be useful to understand the food access and food consumption results of macro-micro simulations concerning the fertilisers' policy reform in this country.
3.1.1. Food Security
3.1.1.1. Food Access (Food expenditure and HCES-DDS)
As described in section 2.1 for the food access dimension we built two indicators using household's survey data: the food expenditure and the diet diversity at the household (HH) level.
Our sample is 21,625 households at the national level, which are geographically decomposed by 1,003 households in the Metropolis (Nairobi and Mombasa), 13,036 households in rural areas and 7,586 households in other urban areas. On average, at the national level, the size of households is around four persons while the factor of Adult Male Equivalent (AME) is lower than that denoting the diverse composition in terms of ages and gender. As it is normal in big cities, households have fewer household members than in the rest of the country. Concerning food expenditure, the share spent in food is around 60% of the total expenditure at the national level, while it decreases in the Metropolis to 40%. However, the amount spent per day per capita in food (deflated) in Nairobi and Mombasa almost double the amount in rural areas. In all regions of the country, more than half of households spend less than the mean in food per capita per day. Diet diversity is
also slightly greater in big cities than in the rest of the country, but the gap across regions is less remarkable (Table 3).
Table 3. Descriptive statistics of the population of Food Access indicators (national and regional).
National Rural Metropolis Other Urban
N= 21,625 60% 5% 35%
Mean p50 sd mean p50 sd mean p50 sd mean p50 sd
HH size 4.28 4 2.52 4.67 4 2.53 2.98 3 1.9 3.79 3 2.44
Food Expenditure (share) 0.56 0.56 0.19 0.64 0.65 0.17 0.4 0.4 0.14 0.49 0.49 0.18
Food Expenditure (per day per capita)
125 97 186 108 84 178 193 161 132 145 115 202
HCE-DDS 10 11 3 10 10 3 11 12 3 11 11 3
At the national level, households spend around 20% of food expenditure on bread and cereal, then 10% on meat and other
10% on milk, cheese and eggs (Table 4). Thus, a decrease in prices of this food could have a considerable improvement in
purchasing power (food access measure).
Table 4. Descriptive statistics of Food Expenditure shares by main food groups as collected in the KIHBS 2015/16 survey (national).
mean p50 Sd
Bread and Cereal 0.21 0.19 0.11
Meat 0.10 0.08 0.10
Fish and seafood 0.06 0.04 0.06
Milk, cheese and eggs 0.10 0.08 0.08
Oils and fats 0.03 0.02 0.03

16
Fruits 0.05 0.03 0.05
Vegetables 0.07 0.06 0.05
Roots and tubers 0.03 0.02 0.04
Sugar, jam, honey, chocolate 0.05 0.04 0.04
Food products n.e.c. Spices and Misc. 0.01 0.00 0.01
Coffee, tea and cocoa 0.01 0.01 0.01
Mineral water, soft drinks, fruit and vegetable juices 0.03 0.02 0.03
Spirits 0.12 0.09 0.11
Beer 0.12 0.08 0.11
Wine 0.11 0.09 0.09
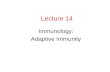
Figure 2 panel (a) evidences that the degree of the diet diversity in households (HCE DDS) increases with the level of
livelihood. This positive relation is supported at national and at geographical disaggregation. Comparing results by income distribution, we find that poor households in Metropolis have a lower HCE DDS than poor households in the rest of the country, while for rich households the degree of diet diversity is greater for those who live in Metropolis than in the rest of the country. Panel (b) shows that, on average, poor households spend a greater proportion of their income on food than rich households. This gap is particularly large on bread and cereal, milk, cheese and eggs, while the consumption share of meat is the highest for all households with very low difference across percentiles.
Figure 2. HCE DDS (national and regional) and national food consumption shares (by food groups) across percentiles of expenditure per capita.
(a) HCE-DDS (b) Food Consumption shares
Differences in food expenditure shares (total and by food item) are key parameters to explain the consumption effect when food prices change, and the degree of diet diversity at the household level complements that information. Both indicators will be used to run microsimulations of the fertiliser policy reforms and non-parametric regressions of these food access indicators changes.
3.1.1.2. Food consumption (Calories and macronutrients)
The current food consumption situation in Kenya at the household level is computed in quantitative and qualitative terms.
The size of the sample used to compute the daily DEC per capita and macronutrients intakes (Fat, Protein, Carbohydrate)
per capita is the same as before at the national level and regions. Table 5 describes these indicators in kilocalories and for
89
10
11
12
13
HC
E D
DS
0 20 40 60 80 100Percentiles of Expenditure per AME (log)
National Metropolis
Rural Other Urban
0
.02
.04
.06
.08
Food C
onsum
ption s
hare
s
0 20 40 60 80 100Percentiles of Expenditure per AME (log)
Bread and Cereals Coffee, tea and cocoa
Food products n.e.c.Spices & Miscellaneous Fruits
Meat Milk, cheese and eggs
Oils and fats Roots and tubers
Sugar, jam, honey, chocolate

17
macronutrients, also in shares of total kilocalories consumed per capita. The national average of daily energy consumed per capita is 2,656 kcal, being the median value lower than the mean (right-skewed distribution).2
Table 5. Descriptive statistics of DEC (kcal.) and Macronutrients intakes (kcal. and shares) per capita (national and regional).
National Rural Metropolis Other Urban
N= 21,625 60% 5% 35%
mean p50 sd mean p50 sd mean p50 sd mean p50 sd
DEC (kcal.) 2266 2027 1202 2271 1995 1235 2273 2122 1131 2248 2039 1176
Fat (kcal.) 485.9 413.6 315.6 450 376 297 557 504 343 512 442 324
share 0.21 0.2 0.08 0.2 0.19 0.07 0.24 0.24 0.08 0.22 0.22 0.08
Protein (kcal.) 261.9 229.2 154.5 263 227 158 264 234 149 258 230 149
share 0.11 0.11 0.03 0.11 0.11 0.02 0.11 0.11 0.03 0.11 0.11 0.03
Carbohydrate (kcal.) 1514.3 1361 811.4 1554 1375 846 1444 1360 716 1474 1340 789
share 0.67 0.68 0.25 0.69 0.70 0.09 0.65 0.64 0.55 0.66 0.67 0.14
Concerning macronutrients intakes per capita, the shares of caloric intake provided by fats, proteins and carbohydrates
within the total caloric intake are 21%, 11% and 67% respectively and on average at the national level (Table 5). Those
values fall within the ranges suggested by the FAO and the WHO for a balanced diet to avoid related diseases (WHO, 2003), and 46% of households (national level) take a balanced diet for the three macronutrients. Nevertheless, around 3% of household (national level) do not meet the recommendations for any of the three macronutrients. Then there are some particular cases where household do not meet at least one of these requirements. For instance, 21%, 29% and 6% of the households do not meet the minimum percentage recommended by FAO for fats, proteins and carbohydrates respectively
(Table 6) (WHO, 2003). We can also observe that within households with at least one stunted child the proportions of
households falling to meet the below thresholds of calories provided by proteins and fats are higher (33.7% and 24.4% respectively) that the percentage among all households at national level (29.7% and 20.8% for proteins and fats respectively).
Table 6. Proportion of the households within, below or above the ranges of population macronutrient intake goals3 by region in Kenya
National Metropolis Other Urban Rural Min HAZ <=-2
A balanced diet 45.8% 45.6% 46.1% 45.7% 43.1%
A diet that does not meet any of the three recommended goals for energy-supplying macronutrients
2.6% 5.9% 3.5% 1.8% 0.9%
Dietary energy provided by protein below the lower recommended threshold (10%)
29.7% 30.3% 30.5% 29.1% 33.7%
Dietary energy provided by fat below the lower recommended threshold (15%)
20.8% 11.1% 16.8% 23.9% 24.4%
Dietary energy provided by carbohydrate below the lower recommended threshold (55%)
5.6% 10.9% 7.8% 3.9% 2.4%
2 For the computation of the DEC we only consider food consumed at home. Tobacco and other stimulants were
deleted as well as food consumed in restaurants and canteens. 3 The ranges of population nutrient intake goals for energy-supplying macronutrients are expressed as
percentage of total energy: fat (15-30%), carbohydrate (55-75%) and protein (10-15%)

18
Dietary energy provided by protein above the upper recommended threshold (15%)
6.8% 8.9% 6.9% 6.6% 5.5%
Dietary energy provided by fat above the upper recommended threshold (15%)
9.9% 19.6% 12.7% 7.6% 6.2%
Dietary energy provided by carbohydrate above the upper recommended threshold (55%)
13.9% 9.5% 12.3% 15.3% 17.5%
Even when there is a positive association between the energy availability at the household level (DEC) and the HDDS-HCE, it is not always direct and the socioeconomic status (e.g., per capita income) determines a greater dietary diversity of a
household (Donini et al., 2016). Figure 3 displays positive relation between the daily DEC per capita and the degree of diet
diversity at household level (i.e., the same relation is observed in terms of percentiles of expenditure per capita for this
sample). In terms of macronutrients’ composition of the diet, panel (b) in Figure 3 shows that the proportion of carbohydrates decreases with the degree of diet diversity, while fats and proteins proportion increase, suggesting that the diversification of the diet is related to the incorporation of protein and fat rich foods, probably in replacement of starchy staples.
Figure 3. DEC per capita and % of Macronutrients in total energy consumed per capita.
(a) DEC per capita (b) % of Macronutrients
0
1000
2000
3000
4000
DE
C p
er
AM
E
0 2 4 6 8 10 12 14 16HCE_DDS
0.2
.4.6
.8
% o
f M
acro
nutr
ients
0 2 4 6 8 10 12 14 16HCE_DDS
Fat Protein
Carbohydrate

19
3.1.2. Nutrition
Since child growth is a particular worry at international level, we are particularly concerned to evaluate agricultural policies that could indirectly affect stunting in children. Anthropometric indicators based on height, weight, age and sex for children allows monitoring the prevalence and changes in trends of under-nutrition in children (underweight, wasting and stunting) and overweight.
According to the WHO (2010), the stunting status is measured as the percentage of children with a low height for age. This indicator can provide different information: (i) the cumulative effects of under-nutrition (and health problems) since and even before birth and (ii) the persistence of poor environmental conditions that restrict potential growth for children. We calculated the proportion of stunted children at the household level.
The empirical evidence highlights that even when the stunting in pre-school children in developing countries displays a decreasing trend according to De Onis et al. (2012), its prevalence remains a worry problem particularly in Africa (e.g., 43.4% in Eastern Africa). Consequently, a direct and indirect (i.e., agricultural reform) intervention is needed to accelerate the reduction of malnutrition in children.
In the case of Kenya, the KIHBS for 2015/2016 provides the information to compute the percentage of children with low height for age for selected households. A sub-sample of 7,530 households was complete for anthropometric measures to
compute the minimum HAZ and the proportion of stunted children per household. According to this sub-sample (Table 7) 31% of households present at least one stunted child (min HAZ lower than -2). Moreover, 10% of them display up to 50% of stunted children and 19% more than 50% of children with growth retardation or stunting in the house. Even if on average this pattern for stunting is similar between rural and urban/peri-urban areas, one third of this sample of households are rural, which means a greater number of rural families with stunted children.
Table 7. Proportion of households with children under 5 years old with stunting or wasting (N=7, 530 households).
Proportion
Stunting
(min) height for age z score < -2 0.31
up to 50% 0.10
more than 50% 0.19
Wasting
(min) weight for height z score < -2 0.15
Note: proportions computed at the household level using min HAZ for stunting, min WHZ for wasting
Around 30% of the households with children under five years of age had at least one child with stunting. In 10% of the households between 10% and 50% of the children in the household suffered stunting, and in 19% of the households more than 50% of the children under five showed stunting.
Concerning wasting (low weight for height), 15% of the households has at least one wasted child (min z score <-2). The percentage of households with children under 5 years old with wasting is lower compared to the proportion of households with stunting.
These malnutrition indicators computed at household level will be the ones used in the presentation of microsimulation results concerning different scenarios of agricultural policy reforms.

20
3.2. Fertiliser policy reform: macro-micro simulations results
According to the results of the CGE simulations of fertiliser policy reforms in Kenya (Boulanger et al., 2017), we run microsimulations for food access, food sufficiency and nutrient adequacy indicators using the treated data from the KHIBS 2015/2016 and the FCT KEN2018 described before. Then, we estimate non-parametric regressions of the change in those indicators and the initial characteristics of households, such as expenditure per capita, DEC per capita, HCE-DDS, and nutritional status for children under 5 years old – stunting and wasting/overweight.
In order to understand the changes in food security indicators at the household level, it is necessary to revised first the changes in prices and consumed quantities that come from the simulated scenarios. First is better to look at the changes in
food prices and consumed quantities under each scenario. Table 8 presents prices changes by food groups according to
the household survey classification. Among the four simulated scenario the Market Access and the Extension display the greatest prices variations; however, changes in prices differ leading to changes in the composition of consumption basket. For instance, while the greatest decrease is for Vegetables under the Market Access scenario, it does for Milk, Cheese and Eggs under the Extension one.
Table 8. Percentage changes in food prices under each scenario (mean and sd).
% Change in Prices
Fertilizer Removal Subsidies Market Access Extension
Mean SD Mean SD Mean SD Mean SD
Bread and Cereal -0.11 0.02 -0.08 0.03 -1.10 0.61 -0.42 0.18
Meat -0.03 0.04 -0.02 0.02 -0.17 0.09 -0.18 0.19
Fish and seafood -0.01 0.00 0.03 0.00 -0.03 0.01 -0.17 0.01
Milk , cheese an -0.06 0.00 0.00 0.00 -0.39 0.01 -0.49 0.01
Oils and fats -0.11 0.00 -0.10 0.01 -0.97 0.04 -0.27 0.01
Fruits -0.14 0.00 -0.09 0.00 -0.93 0.00 -0.41 0.00
Vegetables -0.10 0.00 -0.07 0.00 -1.57 0.00 -0.53 0.00
Roots and tubers -0.08 0.00 -0.05 0.00 -0.95 0.00 -0.39 0.00
Sugar, jam, hone -0.07 0.02 -0.04 0.02 -0.29 0.23 -0.33 0.03
Food products n. -0.01 0.00 -0.03 0.00 0.06 0.00 0.05 0.00
Coffee, tea and -0.05 0.00 -0.01 0.00 -0.33 0.00 -0.34 0.00
Mineral water, -0.05 0.00 -0.01 0.00 -0.33 0.00 -0.34 0.00
Spirits -0.05 0.00 -0.01 0.00 -0.33 0.00 -0.34 0.00
Beer -0.05 0.00 -0.01 0.00 -0.33 0.00 -0.34 0.00
Wine -0.05 0.00 -0.01 0.00 -0.33 0.00 -0.34 0.00
These changes in prices lead to changes in consumed quantities in the CGE simulation and according to the demand specification for each household type and products in the Kenya CGE model. Changes in consumed food quantities that will
affect calories and macronutrients intakes are presented in Table 9.
Table 9. Percentage changes in consumed quantities under each scenario (mean and sd).
% Change in Consumed Quantities
Fertilizer Subsidies Removal Market Access Extension
Mean SD Mean SD Mean SD Mean SD
Bread and Cereal 0.24 0.14 0.16 0.12 1.36 1.25 0.97 0.50
Meat 0.09 0.17 0.04 0.11 0.06 0.25 0.52 0.66
Fish and seafood 0.20 0.10 0.08 0.10 0.00 0.26 0.78 0.18
Milk, cheese an 0.25 0.12 0.07 0.10 0.44 0.17 1.54 0.54
Oils and fats 0.24 0.12 0.21 0.13 1.46 0.75 0.78 0.22

21
Fruits 0.44 0.25 0.29 0.19 1.53 0.78 1.37 0.50
Vegetables 0.31 0.15 0.21 0.14 3.01 1.70 1.58 0.57
Roots and tubers 0.32 0.16 0.21 0.14 1.72 0.88 1.39 0.45
Sugar, jam, hone 0.23 0.16 0.13 0.14 0.34 0.62 1.08 0.34
Food products n. -0.04 0.15 -0.01 0.12 -0.08 0.43 0.02 0.64
Coffee, tea and 0.20 0.11 0.07 0.10 0.38 0.18 1.18 0.34
Mineral water, 0.17 0.11 0.04 0.10 0.37 0.18 1.09 0.36
Spirits 0.23 0.10 0.08 0.10 0.40 0.16 1.23 0.29
Beer 0.20 0.11 0.07 0.10 0.37 0.19 1.19 0.34
Wine 0.15 0.11 0.02 0.11 0.34 0.16 1.04 0.37
In the following subsections, we compare and discuss the performance of the four scenarios on fertilisers according to three mentioned dimensions of the food security and nutrition problem.
3.2.1. Food access
In order to evaluate the change in the households’ food access and affordability we compute the traditional food consumption effect. Given the composition of each household basket of food (food expenditure shares), it measures the consequences in the food purchasing power for each household when food prices change as a result of scenarios of fertiliser policy reforms.
Figure 4 presents the households’ change in purchasing power of food at the national level across percentiles of per capita
expenditure (panel (a)), percentiles of DEC per capita (panel (b)), dietary diversity (HCE DDS, panel (c)) and considering anthropometric indicators of children under 5 years old: the percentage of malnourished children for stunting (panel (d)); the minimum value of the z score for stunting (height for age) and the minimum value of the z score for wasting/overweight (weight for height).
Figure 4. Food Consumption effect (% change in purchasing power of food).
(a) By Percentiles of Expenditure per capita (b) By Percentiles of DEC per capita
(c) By HCE-DDS (d) By proportion of stunted children
0.2
.4.6
Change (
%)
in F
ood P
urc
hasin
g P
ow
er
0 20 40 60 80 100Percentiles of per capita Expenditure (log)
Fertiliser Subsidy Removal
Market Access Extension
0.1
.2.3
.4.5
Ch
an
ge
(%
) in
Fo
od
Pu
rch
asin
g P
ow
er
0 20 40 60 80 100Percentiles of DEC per capita (log)
Fertiliser Subsidy Removal
Market Access Extension
0.1
.2.3
.4.5
Ch
an
ge
(%
) in
Fo
od
Pu
rch
asin
g P
ow
er
0 5 10 15HCE_DDS
Fertiliser Subsidy Removal
Market Access Extension
0.2
.4.6
.8
Change (
%)
in F
ood P
urc
hasin
g P
ow
er
0 .2 .4 .6 .8 1
Proportion of -5y stunted children
Fertiliser Subsidy Removal
Market Access Extension

22
(e) By min HAZ – stunting (f) By min WHZ – wasting
On average at the national level, the Fertiliser scenario displays a positive food access effect for all households in Kenya; however, the elimination of subsidies reduces this effect even when the net effect remains positive. When combining the Fertiliser with the Market Access or the Extension scenarios, the food consumption effects become greater, being preferable the former than the latter. This ranking of scenarios prevails under any of food security characteristics and anthropometric measures of households.
Panel (a) displays a pro-poor food consumption effect under the Extension and the Market Access scenarios, which is an expected result in order to improve food security in terms of the food access dimension. This positive food consumption effect declines with the level of livelihood.
According to the daily energy consumed per capita, the panel (b) shows that food purchasing power increases with the level of DEC per capita for households based on initial distribution. This is not a contradictory result with panel (a) since poor households not necessary display an appropriate diet, but sometimes very high in calories and not correctly balanced in terms of nutrients.
Considering current diet diversity of households, panel (c) tells that purchasing power would increase with the level of diet diversity measured by the HCE DDS; however, these relations displays an inverted U-shape form. Since an average level of diet diversity (HCE DDS = 8) the size of the food consumption effect becomes smaller and relatively flat compared to the first half of the distribution.
Finally, taking into account anthropometric indicators of children under 5 years old, we can say that households with greater percentage (almost 80%) of stunted children (panel (d)) or at least a child with stunting or severe stunting (z values lower than -2 and -3 respectively, panel (e)) and/or at least one child with wasting or severe wasting (z value lower than -2 or -3 respectively, panel (f)) would improve their food access conditions due to a slightly greater food purchasing power. This result is particularly remarkable under the Market Access scenario, since the Extension scenario (and others) displays lower but similar distributive effects across z scores of stunting and wasting.
Table 10 presents the average food consumption effects decomposed by Metropolis (Nairobi and Mombasa), rural and
other urban areas and by the initial households’ characteristics concerning the percentage of stunted children under 5 years old. The same pattern prevails confirming that the Market Access scenario leads to the greatest food consumption effect across main regions and children’ nutritional characteristics mentioned before. Rural regions comparatively benefit the most under any of scenarios, and the same is true for households with up to 50% children under stunting.
Table 10. Average Food Consumption Effect by regions (metropolis, rural and other urban) and stunting
categories.
Regions
Stunting Categories
(% of stunted children)
Metropolis Rural Other Urban 0% Up to 50% More than 50%
Fertiliser 0.03 0.06 0.04 0.05 0.06 0.06
Subsidy Removal 0.02 0.03 0.03 0.03 0.03 0.03
Market Access 0.30 0.54 0.42 0.51 0.56 0.54
Extension 0.15 0.27 0.20 0.25 0.28 0.27
Note: Metropolis concerns Nairobi and Mombasa, Other Urban refers to urban and peri-urban areas except Nairobi and Mombasa, and Rural refers all rural areas in the country
0.2
.4.6
Ch
an
ge
(%
) in
Fo
od
Pu
rch
asin
g P
ow
er
-5 0 5HAZ (min)
Fertiliser Subsidy Removal
Market Access Extension
0.2
.4.6
Ch
an
ge
(%
) in
Fo
od
Pu
rch
asin
g P
ow
er
-5 0 5WHZ (min)
Fertiliser Subsidy Removal
Market Access Extension

23
These results are desired and encourage for the implementation of Market Access and Extension agricultural policies since they could have positive impact on households with malnourished children in order to improve their food access.
3.2.2. Food consumption
3.2.2.1. Calories
Concerning the caloric intake, we measure the change in the DEC per capita at the household level under each of the fertiliser scenarios. The results of non-parametric regressions of the change in DEC per capita are also performed across expenditure per capita, household diet diversity and children’s nutrition characteristics of households.
Figure 5. DEC per capita effect (% change in DEC per capita).
(a) By percentiles of per capita Expenditure (b) By HCE DDS
(c) By min HAZ (stunting) (d) By min WHZ
Such as for food access, the Fertiliser scenario displays an average increase (0.25%) in the daily energy consumed per capita
(Figure 5); however, the elimination of Subsidies reduces that increase in the dietary energy consumption for all
households. In contrast to the food access and affordability, the changes in DEC per capita are not systematically greater under the Market Access improvement than under the Extension scenario, which are the scenarios that display greater positive variations. Results between these two scenarios differ throughout the households’ income, diet and nutrition characteristics.
Panel (a) shows the poorest households display the greatest changes in DEC per capita under the Extension scenario, while under the Market Access scenario households in the middle of the income distribution do. This result is completed with panel (b), which considers the degree of diet diversity per households. For households with lower HCE DDS (up to 7), the Extension scenario would allow increasing the DEC per capita, while for households with higher HCE DDS (from 8 to 16) the Market Access scenarios allows reaching that levels of DEC per capita increase. Finally, when considering children with
0.5
11.5
Change (
%)
in D
EC
per
capita
0 20 40 60 80 100Percentiles of per capita Expenditure (log)
Fertiliser Subsidy
Market Extension
0.5
11
.5
Ch
an
ge
(%
) in
DE
C p
er
ca
pita
0 5 10 15HCE_DDS
Fertiliser Subsidy
Market Extension
.2.4
.6.8
11.2
Change (
%)
in D
EC
per
capita
-5 0 5Min HAZ (z score)
Fertiliser Subsidy
Market Extension
0.5
11
.5
Ch
an
ge
(%
) in
DE
C p
er
ca
pita
-5 0 5Min WHZ (z score)
Fertiliser Subsidy
Market Extension

24
malnutrition problems as nutritional characteristics of households, panel (c) displays systematic greater changes in DEC per capita throughout the distribution under the Market Access scenario. This scenario also displays greater changes in daily calories consumed per capita in households where children display overweight (panel (d)), whereas the Extension scenario would allow greater change in DEC per capita in households where children display more severe stunting problems (panel (c)).
Table 11 displays the average DEC per capita effects of each fertiliser scenario geographically decomposed - Metropolis
(Nairobi and Mombasa), Rural and Other Urban regions - and also by stunting categories according to the initial nutritional status of households’ children under 5 years. Such as for national results in previous figures, the improvement of Market Access conditions allows for the greatest increase in the daily consumption of calories per capita in any region; however, in rural areas the increase in DEC per capita is larger than in the rest of the country under any scenario. Even we find different patterns of results between urban areas: the change in DEC per capita in Metropolitan areas is lower than in other urban zones. Finally, concerning the comparison across stunting categories, we find that the Market Access scenario allows for the greatest change in DEC per capita for households without stunting and with more than 50% of children under five years stunted. Nonetheless, the change in DEC per capita becomes the largest under the Extension scenario to all households with at least one stunted child.
Table 11. Average DEC per capita effect by regions (metropolis, rural and other urban) and stunting
categories.
Regions
Stunting Categories
(% of stunted children)
Metropolis Rural
Other
Urban 0% Up to 50% More than 50%
Fertiliser 0.12 0.31 0.18 0.26 0.27 0.28
Subsidy Removal 0.06 0.22 0.08 0.17 0.18 0.18
Market Access 0.58 1.28 1.22 1.21 1.17 1.23
Extension 0.52 1.22 0.97 1.10 1.16 1.15
Summarising the findings, we can say that the Market Access and the Extension scenario would particularly increase calories consumed in households that live in rural areas and where stunting affects children under 5 years old. Although these results inform on the food sufficiency impact of fertiliser scenarios according to economic and current food security and nutritional status of households, they remain incomplete in terms of quality of households’ diet addressing nutritional problems. Consequently, we analyse in the next subsection the change in the macronutrients’ composition of these increases in daily energy consumption per capita.

25
3.2.2.2. Macronutrients
All fertiliser reforms allow increasing the consumption of all macronutrients on average. However, this increase in macronutrients consumption differs across households according to their income, energy consumption, diet diversity and children’ nutritional characteristics.
Figure 6 shows that all fertiliser scenarios display a pro-poor result concerning fats (panel (a)), proteins (panel (b)) and
carbohydrates (panel (c)) intakes per capita, being the Market Access scenario the one that allows for the greatest variations.
Looking at the details of variation across macronutrients, we find that for poorest households the greatest increase in macronutrients intakes comes from proteins, while for middle-income households it comes from carbohydrates. These results should be compared with the initial macronutrient deficits across households.
Figure 6. Macronutrients effect (% change in Daily Macronutrients per capita) across percentiles of
expenditure per capita.
(a) Fats (b) Proteins
(c) Carbohydrates
0.5
11.5
Change (
%)
in F
AT
inta
kes
0 20 40 60 80 100Percentiles of per capita Expenditure (log)
Fertiliser Subsidy
Market Extension
0.5
11
.5
Ch
an
ge
(%
) in
PR
O in
take
s
0 20 40 60 80 100Percentiles of per capita Expenditure (log)
Fertiliser Subsidy
Market Extension
0.5
11.5
Change (
%)
in C
AR
inta
kes
0 20 40 60 80 100Percentiles of per capita Expenditure (log)
Fertiliser Subsidy
Market Extension

26
Figure 7 presents the change in macronutrients intakes across percentiles of DEC per capita. The change in consumption
patterns at the household level under all scenarios allows increasing all macronutrients consumption. On average, the change in macronutrients consumption is greater for carbohydrate (panel (c)) intakes and looking at the DEC per capita distribution these macronutrients changes benefits those households in the right tale of the distribution when Market Access conditions improve. Regarding proteins (panel (b)), the Extension scenario leads to a slightly greater increase for households with low DEC per capita (left tale of distribution). For these last households (with lower DEC per capita) the Extension scenario would be preferred for the increase in all macronutrients.
Figure 7. Macronutrients effect (% change in Daily Macronutrients per capita) across percentiles of DEC per
capita.
(a) Fats (b) Proteins
(c) Carbohydrates
.2.4
.6.8
11
.2
Ch
an
ge
(%
) in
FA
T in
take
s
0 20 40 60 80 100Percentiles of DEC per capita (percentiles)
Fertiliser Subsidy
Market Extension
.2.4
.6.8
11
.2
Ch
an
ge
(%
) in
PR
O in
take
s
0 20 40 60 80 100Percentiles of DEC per capita (percentiles)
Fertiliser Subsidy
Market Extension
0.5
11.5
Change (
%)
in C
AR
inta
kes
0 20 40 60 80 100Percentiles of DEC per capita (percentiles)
Fertiliser Subsidy
Market Extension

27
According to the current households’ diet diversity based on the HCE-DDS indicator, Figure 8 shows that for those
households with lowest degree of diet diversity, the Extension scenario would lead to the greatest increase in all macronutrients’ intakes. The Market Access scenario allows for the greatest increase in all macronutrients’ consumption for households with medium-high degree of diet diversity. The gap between these two scenarios disappears when approaching the highest values of the HCE-DDS.
Comparing the changes across macronutrients and the level of diet diversity, we find (panel (b)) that protein intakes display the greatest increase (1.1%) in households where there is a very low HCE-DDS (Extension scenario), while for households with high values of the HCE-DDS carbohydrates increase more (around 1%) than other macronutrients.
Figure 8. Macronutrients effect (% change in Macronutrients per day per person) according to HCE DDS (diet
diversity indicator).
(a) Fats (b) Proteins
(c) Carbohydrates
0.5
1
Ch
an
ge
(%
) in
FA
T in
take
s
0 5 10 15HCE_DDS
Fertiliser Subsidy
Market Extension
0.5
11.5
Change (
%)
in P
RO
inta
kes
0 5 10 15HCE_DDS
Fertiliser Subsidy
Market Extension
0.5
11.5
Change (
%)
in C
AR
inta
kes
0 5 10 15HCE_DDS
Fertiliser Subsidy
Market Extension

28
Considering the minimum HAZ score for households with children under five years (Figure 9), we find that the increase in
macronutrients intakes (particularly fats and proteins) increase the most for HAZ values lower than -2, which means at least one stunted child in the house. For fats change the gap between the Market Access and the Extension scenario is imperceptible but for protein and carbohydrates, the greatest increase appears under the Market Access scenario. For carbohydrates, even if the Market Access scenario allows greatest changes on average, the Extension scenario allows for relatively more increase for households with stunted children.
Figure 9. Macronutrients effect (% change in Daily Macronutrients per capita) with respect to the min z score
(stunting in U5y children per household).
(a) Fats (b) Proteins
(c) Carbohydrates
.2.4
.6.8
11.2
Change (
%)
in F
AT
inta
kes
-5 0 5Min HAZ (z score)
Fertiliser Subsidy
Market Extension
.2.4
.6.8
11.2
Change (
%)
in P
RO
inta
kes
-5 0 5Min HAZ (z score)
Fertiliser Subsidy
Market Extension
.2.4
.6.8
11.2
Change (
%)
in C
AR
inta
kes
-5 0 5Min HAZ (z score)
Fertiliser Subsidy
Market Extension

29
Across z scores related to wasting/overweight (Figure 10), we find that the Market Access scenario leads to the greatest
increase in all macronutrients’ intakes in households with children with overweight. Nevertheless, the Extension scenario is the one that allows the largest increase for macronutrients intakes in households where children display wasting. Finally, under any of the scenarios the increase in all macronutrients intakes is greater for households that display cases of overweight than those showing cases of wasting among the children under five in the house.
Figure 10. Macronutrients effect (% change in Daily Macronutrients per capita) with respect to the min WHZ
score (wasting in U5y children per household).
(a) Fats (b) Proteins
(c) Carbohydrates
.2.4
.6.8
11
.2
Ch
an
ge
(%
) in
FA
T in
take
s
-5 0 5Min WHZ (z score)
Fertiliser Subsidy
Market Extension0
.51
1.5
Cha
ng
e (
%)
in P
RO
in
takes
-5 0 5Min WHZ (z score)
Fertiliser Subsidy
Market Extension
.2.4
.6.8
11.2
1.4
1.6
Change in C
arb
ohydra
te inta
kes
-5 -2.5 0 2.5 5Min WHZ (z-score)
Fertiliser Subsidy Removal
Market Access Extension

30
Table 12 summarises the average change in macronutrients intakes under all scenarios by regions and percentage of
stunted children under 5 years old at the household level. Changes in macronutrients intakes are bigger under the Market Access improvement and the Extension of services related to the fertiliser use than others. Among the three macronutrients analysed we find that the average increase is greater for carbohydrates closely followed by proteins and particularly under the Market Access scenario. Rural households are those who benefit the most of this increase in macronutrients intakes and those households who displays more than 50% of their children with stunting problems. Fats intakes displays greater variations under the Extension scenario, and the distributive effect across regions and stunting categories remains the same as for proteins and carbohydrates.
Table 12. Average Macronutrient (Fats, Proteins and Carbohydrates) effect by region (metropolis, rural and
other urban) and stunting categories.
Regions
Stunting Categories
(% of stunted children)
Metropolis Rural Other Urban 0% Up to 50% More than 50%
Fat Fertiliser 0.12 0.32 0.18 0.26 0.28 0.28
Subsidy Removal 0.06 0.23 0.08 0.17 0.18 0.19
Market Access 0.54 1.17 1.10 1.10 1.09 1.14
Extension 0.51 1.23 0.94 1.10 1.17 1.15
Protein Fertiliser 0.11 0.30 0.17 0.25 0.27 0.27
Subsidy Removal 0.05 0.22 0.06 0.16 0.18 0.18
Market Access 0.54 1.29 1.15 1.19 1.18 1.24
Extension 0.52 1.20 0.96 1.09 1.15 1.14
Carbohydrate Fertiliser 0.11 0.31 0.19 0.26 0.27 0.27
Subsidy Removal 0.06 0.22 0.08 0.16 0.18 0.18
Market Access 0.60 1.30 1.26 1.23 1.17 1.24
Extension 0.52 1.22 0.99 1.10 1.17 1.16

31
4. Conclusions
Kenya, such as other African countries, is particularly concerned about the achievement of the Sustainable Development Goal #2 (SDG #2: zero hunger). Empirical evidence about food security and nutrition in Kenya accounts for deficiencies in food access, sufficiency and an inadequate diet in terms of daily per capita calories and nutrients intakes. These nutritional deficiencies are, among others, the causes of all forms of malnutrition in young population (e.g. stunting, wasting and overweight), that can lead to impaired cognitive development, limited immunity to diseases, low educational performance, increased risk to chronic diseases, and even mortality cases of children in this country.
Food and nutrition security problems are challenging issues due to the multi-dimensionality of causes to be tackled, and also because of the heterogeneity across households concerning: their income and food expenditure, education level of households heads, regional sanitation coverage, environment (access to potable water / waste water system/health system), as well as public policies with direct or indirect impact on the households nutritional status.
In the framework of this study, we focused on the economic factors affecting food security and malnutrition, and more specifically on the impact of a series of policy developed around the construction of a new fertilizer plant funded by the Kenyan government on the food security and malnutrition dimensions in Kenya.
We developed a macro-micro simulation approach to evaluate this set of policies simulated by four scenarios. Results focus on food access and affordability, and calories and macronutrient consumption as a first consideration of food adequacy. The criteria provided by the literature and the data availability concerning consumption and nutrition have been key for choosing feasible and pertinent food security and nutritional indicators.
The food security and nutrition macro-micro simulations results of the scenarios were discussed in terms of households' expenditure and their initial food security and nutrition conditions such as the daily calories consumption per capita, the diet diversity score and the percentage of children’s malnutrition (stunting and wasting) in the household. Main results suggest that improved market access (better roads and consequently lower costs to move commodities around the country) allow for the largest average improvement of the food access and affordability dimension, with a pro-poor result, greater impact on rural areas and benefiting the most those households with malnourished children (either wasted or stunted). The reduction in trade costs also leads to the greatest increase of daily energy and macronutrients consumption per capita across levels of livelihood and in households with stunted children. Nevertheless, improving productivity in agricultural practices (Extension scenario) also allows for an increase in all macronutrients' intakes, although average increases are greater for carbohydrates than for fats or proteins. Important to say, poor households would benefit from a relatively greater increase in all macronutrients' intakes. An encouraging result is that the Extension scenario would allow increasing macronutrients intakes (greater average variation for proteins) in households with relatively low diet diversity and with children suffering from wasting. Decomposing national results by main population subgroups shows highest impact for rural areas in all food security and nutrition dimensions, and lowest one for the Metropolis even if they remain positive in all the populations sub-groups analysed.
These results contribute to the discussion on how different agricultural and rural development policies in Kenya can contribute to tackle the SDG Goal #2. Nonetheless, we are aware that there is not a unique policy instrument but a set of tools that would be required to cover all households suffering food consumption and nutrition deficiencies in Kenya.

32
References
Akombi, B., Agho, K., Merom, D., Renzaho, A., & Hall, J. (2017). Child malnutrition in sub-Saharan Africa: A meta-analysis of demographic and health surveys (2006-2016). PloS one, 12(5), e0177338.
Aragie, E., Dudu, H., Ferrari, E., Mainar-Causapé, A., McDonald, S., & Thierfielder, K. (2017). Stage-Dev a variant of the stage model for developing countries. Joint Research Centre (Seville site), EUR 28627 EN.
Bhutta, Z. A., Das, J. K., Rizvi A,, Gaffey, M. F., Walker, N., Horton, S., Webb, P., Lartey, A., Black R. E, the Lancet Nutrition Interventions Review Group & the Maternal and Child Nutrition Study Group (2013).. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet 2013, 382(9890), 452-477, http://dx.doi.org/10.1016/S0140-6736(13)60996-4, published online June 6.
Boulanger, P., Dudu, H., Ferrari, E., Mainar-Causapé, A., & Proietti, I. (2017). Boosting the fertilizer production in Kenya: a CGE analysis. Joint Research Centre (Seville site), EUR 28695 EN.
Breisinger, C. & Ecker, O. (2014). Simulating economic growth effects on food and nutrition security in Yemen: a new macro-micro modeling approach. Economic Modelling, 43, 100-113.
Byrd, K., Williams, A., Dentz, H. N., Kiprotich, M., Rao, G., Arnold, C. D., Null, A. C., Dewey, K. G., & Stewart, C. P. (2017). Differences in complementary feeding practices within the context of the wash benefits randomized, controlled trial of nutrition, water, sanitation, and hygiene interventions in rural Kenya. The FASEB Journal, 31(1 supplement), 165-1.
Carletto, C., Corral, P., & Guelfi, A. (2017). Agricultural commercialization and nutrition revisited: Empirical evidence from three African countries. Food Policy, 67, 106-118.
Chege, C. G., Andersson, C. I., & Qaim, M. (2015). Impacts of supermarkets on farm household nutrition in Kenya. World Development, 72, 394-407.
Chen, S. & Ravallion, M. (2004). Welfare impacts of china's accession to the world trade organization. The World Bank economic review, 18(1), 29-57.
Chiputwa, B. & Qaim, M. (2016). Sustainability standards, gender, and nutrition among smallholder farmers in Uganda. The Journal of Development Studies, 52(9), 1241-1257.
Cockburn, J., Savard, L., & Tiberti, L. (2014). Macro-micro models. In Handbook of Microsimulation Modelling. Emerald Group Publishing Limited, 275-304.
Committee on World Food Security (2012). Coming to Terms with Terminology. Technical report, Committee on World Food Security, Final report 2012/39, Rome, October 15-20.
De Onis, M., Blossner, M., & Borghi, E. (2012). Prevalence and trends of stunting among preschool children, 1990-2020. Public health nutrition, 15(1), 142-148.
Deaton, A. (1989). Household survey data and pricing policies in developing countries. The World Bank Economic Review, 3(2), 183-210.
Deaton, A. (1997). The analysis of household surveys: a microeconometric approach to development policy. The World Bank.
Debowicz, D. (2016). Does the microsimulation approach used in macro–micro modelling matter? An application to the distributional effects of capital outflows during Argentina's Currency Board regime. Economic Modelling, 54, 591-599.
Demmler, K. M., Ecker, O., & Qaim, M. (2018). Supermarket shopping and nutritional outcomes: A panel data analysis for urban Kenya. World Development, 102, 292-303.
Desiere, S., Hung, Y., Verbeke, W., & D’Haese, M. (2018). Assessing current and future meat and fish consumption in Sub-Sahara Africa: Learnings from FAO Food Balance Sheets and LSMS household survey data. Global food security, 16, 116-126.
Dewey KG and Bequm K. Long-term consequences of stunting early in life. Matern Child Nutr 2011. Oct; 7 Suppl 3:5-18.
Donini, L. M., Dernini, S., Lairon, D., Serra-Majem, L., Amiot, M.-J., Del Balzo, V., Giusti, A.-M., Burlingame, B., Belahsen, R., Maiani, G., Polito, A., Turrini, A., Intorre, F., Trichopoulou, A., & Berry, E. M. (2016). A consensus proposal for nutritional indicators to assess the sustainability of a healthy diet: the Mediterranean diet as a case study. Frontiers in nutrition, August 29, 3-37.
Ecker, O., Weinberger, K., & Qaim, M. (2010). Patterns and determinants of dietary micronutrient deficiencies in rural areas of East Africa. African Journal of Agricultural and Resource Economics, 4(2), 175-194.
FAO/Government of Kenya (2018). Kenya Food Composition Tables. Rome & Nairobi: The Food and Agriculture Organization of the United Nations & The Ministry of Health, Republic of Kenya & The Ministry of Agriculture and Irrigation, Republic of Kenya. ISBN: 978-92-5-130445-7. Available at: http://www.fao.org/3/I8897EN/i8897en.pdf

33
Food Security International Network (FSIN), 2019. Global Report on Food Crises 2019. Joint analysis for better decisions. Rome April 2019.
Global Nutrition Report (2018). Available at: https://globalnutritionreport.org/reports/global-nutrition-report-2018/
Integrated Food Security Phase Classification (IPC) Global Partners (2012). IPC Technical Manual Version 2.0. Evidence and Standards for Better Food Security Decisions. Rome: The Food and Agriculture Organization of the United Nations. Available at: http://www.ipcinfo.org/fileadmin/user_upload/ipcinfo/docs/IPC-Manual-2-Interactive.pdf
Kennedy, G., Ballard, T., & Dop, M.C. (2010). Guidelines for Measuring Household and Individual Dietary Diversity. Rome: Nutrition and Consumer Protection Division, FAO. ISBN: 978-92-5-106749-9 Available at: http://www.fao.org/3/a-i1983e.pdf
Kennedy, G. L., Pedro, M. R., Seghieri, C., Nantel, G., & Brouwer, I. (2007). Dietary diversity score is a useful indicator of micronutrient intake in non-breast-feeding Filipino children. The Journal of nutrition, 137(2), 472-477.
Kenya Agricultural Research Institute (2012). Food Security Report 2012. Available at: http://www.foodsecurityportal.org/kenya/food-security-report-prepared-kenya-agricultural-research-institute
Kenya Ministry of Devolution and Planning, Implementation of the Agenda 2030 for Sustainable Development in Kenya, June 2017). Available at https://www.un.int/kenya/sites/www.un.int/files/Kenya/vnr_report_for_kenya.pdf
Kenya National Bureau of Statistics (2018). Basic Report on the 2015/2016 Kenya Integrated Household Budget Survey. March. ISBN: 978-9966-102-03-4. Available at: https://sun-connect-news.org/fileadmin/DATEIEN/Dateien/New/KNBS_-_Basic_Report.pdf
Kenya National Bureau of Statistics, Ministry of Health/Kenya, National AIDS Control Council/Kenya, Kenya Medical Research Institute, National Council for Population and Development/Kenya, & ICF International (2015). Kenya Demographic and Health Survey 2014. Rockville, MD, USA: Kenya National Bureau of Statistics, Ministry of Health/Kenya, National AIDS Control Council/Kenya, Kenya Medical Research Institute, National Council for Population and Development/Kenya, and ICF International. Available at: https://dhsprogram.com/publications/publication-FR308-DHS-Final-Reports.cfm
Maclean, W., Harnly, J., Chen, J., Chevassus-Agnes, S., Gilani, G., Livesey, G., & Warwick, P. (2003). Food energy methods of analysis and conversion factors, FAO Food and Nutrition paper, 77.
Mainar-Causapé, A., Boulanger, P., Dudu, H., Ferrari, E., McDonald, S., & Caivano, A. (2018). Social accounting matrix of Kenya 2014. Joint Research Centre (Seville site), EUR 29056 EN.
Ministry of Devolution and Planning, 2017. Implementation of the Agenda 2030 for Sustainable Development in Kenya. Nairobi, Kenya June 2017.
Moltedo, A., Troubat, N., Lokshin, M., & Sajaia, Z. (2014). Analyzing food security using household survey data: streamlined analysis with ADePT software. The World Bank. Available at: http://documents.worldbank.org/curated/en/488671468168574663/Analyzing-food-security-using-household-survey-data-streamlined-analysis-with-ADePT-software
Moltedo, A., Alvarez, C., Troubat, N., & Cafiero, C. (2018). Optimizing the use of ADePT-Food Security Module for Nutrient Analysis. ADePT-FSM Version 3. Rome: FAO Statistics Division (ESS), January. Available at: http://www.fao.org/fileadmin/templates/ess/foodsecurity/Optimizing_the_use_of_ADePT_FSM_for_nutrient_analysis.pdf
Ruel, M.T., Alderman, H., & the Maternal and Child Nutrition Study Group (2013). Nutrition-sensitive interventions and programmes: how can they help to accelerate progress in improving maternal and child nutrition? Lancet 2013, Maternal and Child Nutrition 382(9891): 536-551, https://doi.org/10.1016/S0140-6736(13)60843-0.
Swindale, A., & Bilinsky, P. (2006). Household dietary diversity score (HDDS) for measurement of household food access: indicator guide. Washington, DC: Food and Nutrition Technical Assistance Project, Academy for Educational Development.
UNICEF & WHO (2010). Indicators for assessing infant and Young child feeding practices. Part 2. Measurement. WHO library cataloguing-in publication data, 2010.
Weisell, R., & Dop, M. C. (2012). The adult male equivalent concept and its application to Household Consumption and Expenditures Surveys (HCES). Food and nutrition bulletin, 33(3_suppl2), S157-S162.
WHO (2010). Nutrition Landscape Information System (NLIS) country profile indicators: interpretation guide. Technical report, Geneva: World Health Organization.
WHO (2003). Diet, nutrition and the prevention of chronic diseases: report of a joint WHO/FAO expert group. WHO Technical Report Series 916. Geneva: World Health Organization.
WHO (2019). The WHO Child Growth Standards. Available from: http://www.who.int/childgrowth/en/ accessed February 15.

34
World Food Program, WFP, 2018. Kenya WFP country brief, November 2018. Available from https://reliefweb.int/report/kenya/wfp-kenya-country-brief-november-2018

35
List of abbreviations and definitions
AME Adult Male Equivalent
CGE Computable General Equilibrium
DEC Dietary Energy Consumption
DHS Demographic and Health Survey
FAO Food and Agriculture Organization of the United Nations
FCT Food Composition Table
GE General Equilibrium
HAZ Height for Age Z score
HCES-DDS Household consumption and expenditure surveys dietary diversity score
HDDS Household Dietary Diversity Score
HH Household
KIHBS Kenya Integrated Household Survey
MS Micro-Simulations
NCT Nutrient Conversion Table
SAM Social Accounting Matrix
SDG Sustainable Development Goal
SSA Sub-Saharan Africa
STAGE-DEV STatic Applied General Equilibrium for DEVelopment
UNICEF United Nations Children's Fund
WHO World Health Organization
WHZ Weight for Height Z score

36
List of figures
Figure 1. Macro-micro top-down methodology scheme. ............................................................ 9
Figure 2. HCE DDS (national and regional) and national food consumption shares (by food groups) across
percentiles of expenditure per capita. .............................................................................. 16
Figure 3. DEC per capita and % of Macronutrients in total energy consumed per capita. ....................... 18
Figure 4. Food Consumption effect (% change in purchasing power of food). ................................... 21
Figure 5. DEC per capita effect (% change in DEC per capita). .................................................... 23
Figure 6. Macronutrients effect (% change in Daily Macronutrients per capita) across percentiles of
expenditure per capita. ............................................................................................... 25
Figure 7. Macronutrients effect (% change in Daily Macronutrients per capita) across percentiles of DEC per
capita. ................................................................................................................. 26
Figure 8. Macronutrients effect (% change in Macronutrients per day per person) according to HCE DDS (diet
diversity indicator). ................................................................................................... 27
Figure 9. Macronutrients effect (% change in Daily Macronutrients per capita) with respect to the min z score
(stunting in U5y children per household). ........................................................................... 28
Figure 10. Macronutrients effect (% change in Daily Macronutrients per capita) with respect to the min WHZ
score (wasting in U5y children per household). .................................................................... 29

37
List of tables
Table 1. Food security and nutrition indicators at the household level. ............................................ 6
Table 2. Mapping between macro-micro models’ data. ............................................................ 11
Table 3. Descriptive statistics of the population of Food Access indicators (national and regional). ............ 15
Table 4. Descriptive statistics of Food Expenditure shares by main food groups as collected in the KIHBS
2015/16 survey (national). ........................................................................................... 15
Table 5. Descriptive statistics of DEC (kcal.) and Macronutrients intakes (kcal. and shares) per capita (national
and regional). ......................................................................................................... 17
Table 6. Proportion of the households within, below or above the ranges of population macronutrient intake
goals by region in Kenya .............................................................................................. 17
Table 7. Proportion of households with children under 5 years old with stunting or wasting (N=7, 530
households). .......................................................................................................... 19
Table 8. Percentage changes in food prices under each scenario (mean and sd). ............................... 20
Table 9. Percentage changes in consumed quantities under each scenario (mean and sd). .................... 20
Table 10. Average Food Consumption Effect by regions (metropolis, rural and other urban) and stunting
categories. ............................................................................................................. 22
Table 11. Average DEC per capita effect by regions (metropolis, rural and other urban) and stunting
categories. ............................................................................................................. 24
Table 12. Average Macronutrient (Fats, Proteins and Carbohydrates) effect by region (metropolis, rural and
other urban) and stunting categories. ............................................................................... 30

38
Annexes
Annex 1. Table A.1. Atwater conversion factors
Kcal/gram
Protein 4
Fat 9
Carbohydrate 4
Fiber 2
Alcohol 7
Source: Maclean W et al. (2003).
Annex 2. Table A.2. Consumption prices variation by food item (SAM code) from the CGE mode simulations – All scenarios.
SAM food codes Fertiliser Fertiliser + Remove Subsidy Fertiliser + Market Access Fertiliser + Extension
c_bake -0.080 -0.047 -0.239 -0.349
c_beef -0.105 -0.031 -0.352 -0.553
c_bevt -0.084 -0.034 -0.351 -0.425
c_dair -0.106 -0.034 -0.382 -0.590
c_fish -0.087 -0.040 -0.165 -0.252
c_frui -0.204 -0.142 -0.892 -0.535
c_goat -0.086 -0.022 -0.380 -0.649
c_maiz -0.210 -0.129 -1.079 -0.816
c_meat -0.045 -0.027 -0.226 -0.183
c_ogrn -0.189 -0.111 -1.032 -0.724
c_oils -0.117 -0.113 -0.953 -0.289
c_oliv -0.111 -0.036 -0.294 -0.424
c_omfd 0.033 0.005 -0.115 0.147
c_poul -0.177 -0.100 -0.265 -0.723
c_rice -0.095 -0.117 -2.426 -0.136
c_root -0.128 -0.091 -0.916 -0.487
c_vege -0.133 -0.100 -1.527 -0.607

39
c_whea -0.114 -0.121 -1.127 -0.372

40
Annex 3. Table A.3. Fertiliser scenario - Quantities variations by food item and households from the CGE mode simulations.
NA MO HR MN MS CO AN AS TU
Q1 Q2 Q3 Q4 Q5 Q1 Q2 Q3 Q4 Q5 RU UR RU UR RU UR RU UR RU UR RU UR RU UR
FERTILISER
c_maiz 0.017 0.096 0.113 0.149 0.126 0.114 0.144 0.212 0.207 0.262 0.372 0.366 0.766 0.030 0.183 0.026 0.168 0.081 0.173 0.223 0.159 0.132 0.292 0.250
c_whea -0.021 0.067 0.078 0.099 0.085 0.064 0.086 0.147 0.129 0.163 0.235 0.154 0.369 -0.005 0.154 -0.008 0.118 0.040 0.127 0.169 0.098 0.062 0.204 0.122
c_rice -0.028 0.061 0.071 0.089 0.076 0.054 0.074 0.134 0.113 0.143 0.207 0.111 0.287 -0.012 0.148 -0.015 0.108 0.031 0.117 0.159 0.085 0.047 0.186 0.096
c_ogrn 0.009 0.089 0.105 0.138 0.117 0.102 0.131 0.198 0.190 0.239 0.342 0.318 0.677 0.022 0.176 0.018 0.157 0.072 0.163 0.211 0.145 0.116 0.272 0.221
c_root -0.025 0.116 0.136 0.173 0.148 0.116 0.155 0.256 0.229 0.290 0.417 0.301 0.695 0.000 0.258 -0.005 0.205 0.074 0.218 0.290 0.174 0.117 0.354 0.229
c_oils -0.027 0.092 0.108 0.136 0.117 0.089 0.120 0.203 0.178 0.226 0.326 0.217 0.516 -0.006 0.211 -0.010 0.163 0.055 0.174 0.233 0.135 0.086 0.281 0.171
c_frui 0.022 0.145 0.171 0.225 0.191 0.170 0.217 0.321 0.312 0.394 0.561 0.543 1.142 0.042 0.280 0.037 0.254 0.121 0.263 0.339 0.239 0.197 0.442 0.372
c_vege -0.020 0.112 0.132 0.168 0.144 0.114 0.151 0.248 0.223 0.283 0.406 0.303 0.691 0.003 0.246 -0.002 0.198 0.074 0.210 0.278 0.170 0.117 0.342 0.228
c_beef -0.044 0.117 0.136 0.170 0.147 0.108 0.146 0.256 0.220 0.279 0.403 0.241 0.598 -0.015 0.274 -0.021 0.206 0.064 0.222 0.298 0.166 0.099 0.355
c_dair -0.037 0.100 0.116 0.146 0.126 0.093 0.126 0.219 0.189 0.240 0.346 0.210 0.517 -0.012 0.234 -0.017 0.176 0.056 0.189 0.255 0.143 0.086 0.304 0.172
c_poul 0.006 0.133 0.156 0.203 0.173 0.149 0.192 0.293 0.279 0.352 0.502 0.452 0.971 0.027 0.267 0.022 0.233 0.103 0.243 0.316 0.213 0.166
c_oliv -0.034 0.102 0.119 0.150 0.129 0.096 0.130 0.224 0.195 0.356 0.226 0.548 -0.010 0.236 -0.015 0.180 0.059 0.193 0.259 0.147 0.091 0.311 0.182
c_goat -0.049 0.090 0.105 0.130 0.112 0.163 0.301 0.140 0.386 -0.024 0.224 -0.028 0.160 0.174 0.237 0.123 0.063 0.275 0.130
c_fish -0.049 0.091 0.106 0.131 0.113 0.077 0.108 0.199 0.165 0.209 0.304 0.145 0.395 -0.023 0.225 -0.028 0.161 0.043 0.175 0.238 0.124 0.064 0.277 0.133

41
c_meat -0.044 0.042 0.048 0.057 0.050 0.026 0.040 0.091 0.066 0.084 0.124 0.001 0.075 -0.027 0.121 -0.030 0.075 0.009 0.085 0.119 0.049 0.010 0.128
c_bake -0.053 0.087 0.102 0.125 0.108 0.072 0.101 0.192 0.156 0.198 0.288 0.120 0.350 -0.027 0.221 -0.032 0.155 0.038 0.170 0.232 0.117 0.056 0.267 0.118
c_bevt -0.050 0.090 0.104 0.129 0.111 0.075 0.106 0.197 0.161 0.205 0.298 0.136 0.379 -0.024 0.223 -0.029 0.159 0.041 0.173 0.236 0.121 0.061 0.273 0.127
c_omfd -0.121 0.035 0.039 0.034 0.033 -0.018 -0.004 0.074 0.013 0.020 0.039 -0.264 -0.371 -0.090 0.168 -0.094 0.066 -0.037 0.086 0.136 0.006 -0.072 0.108 -0.113

42
Annex 4. Table A.4. Fertiliser scenario + subsidy Remove scenario- Quantities variations by food item and households from the CGE mode simulations.
NA MO HR MN MS CO AN AS TU
Q1 Q2 Q3 Q4 Q5 Q1 Q2 Q3 Q4 Q5 RU UR RU UR RU UR RU UR RU UR RU UR RU UR
FERTILISER +
REMOVE SUBSIDY
c_maiz -0.053 0.038 0.050 0.077 0.056 0.048 0.075 0.147 0.127 0.171 0.240 0.169 0.473 -0.026 0.132 -0.038 0.103 0.012 0.125 0.142 0.096 0.059 0.192 0.139
c_whea -0.057 0.036 0.047 0.073 0.053 0.044 0.070 0.141 0.120 0.162 0.229 0.151 0.440 -0.029 0.130 -0.041 0.098 0.008 0.121 0.138 0.091 0.053 0.185 0.128
c_rice -0.058 0.035 0.046 0.071 0.051 0.042 0.068 0.139 0.117 0.159 0.224 0.144 0.425 -0.030 0.129 -0.042 0.097 0.007 0.120 0.136 0.088 0.050 0.182 0.124
c_ogrn -0.060 0.033 0.044 0.068 0.049 0.039 0.064 0.134 0.112 0.152 0.215 0.130 0.399 -0.033 0.127 -0.044 0.093 0.004 0.117 0.132 0.084 0.045 0.176 0.115
c_root -0.112 0.044 0.060 0.094 0.066 0.047 0.086 0.198 0.157 0.216 0.305 0.141 0.519 -0.065 0.197 -0.084 0.136 -0.007 0.175 0.198 0.117 0.051 0.258 0.146
c_oils -0.081 0.045 0.060 0.094 0.067 0.054 0.089 0.185 0.154 0.210 0.296 0.182 0.554 -0.044 0.173 -0.059 0.128 0.007 0.160 0.182 0.116 0.064 0.242 0.161
c_frui -0.074 0.065 0.085 0.130 0.096 0.085 0.129 0.240 0.212 0.285 0.401 0.307 0.817 -0.033 0.210 -0.051 0.169 0.027 0.204 0.231 0.161 0.106 0.316 0.242
c_vege -0.100 0.045 0.061 0.096 0.068 0.051 0.089 0.196 0.158 0.217 0.307 0.162 0.544 -0.057 0.190 -0.075 0.135 -0.001 0.172 0.194 0.119 0.057 0.256 0.155
c_beef -0.167 0.015 0.026 0.047 0.025 -0.004 0.029 0.146 0.084 0.127 0.182 -0.087 0.121 -0.112 0.186 -0.132 0.094 -0.055 0.141 0.159 0.060 -0.025 0.186
c_dair -0.140 0.014 0.024 0.042 0.023 -0.001 0.027 0.127 0.075 0.113 0.161 -0.064 0.121 -0.093 0.159 -0.111 0.083 -0.045 0.122 0.138 0.054 -0.018 0.163 0.019
c_poul -0.100 0.045 0.061 0.096 0.068 0.051 0.089 0.196 0.159 0.218 0.307 0.162 0.545 -0.057 0.190 -0.074 0.135 -0.001 0.172 0.195 0.119 0.057
c_oliv -0.139 0.015 0.025 0.044 0.025 0.000 0.029 0.129 0.077 0.165 -0.057 0.134 -0.092 0.160 -0.110 0.084 -0.043 0.124 0.139 0.056 -0.016 0.165 0.023
c_goat -0.147 0.009 0.017 0.033 0.016 0.060 0.136 -0.103 0.047 -0.100 0.154 -0.117 0.073 0.114 0.128 0.042 -0.031 0.146 -0.005
c_fish -0.136 0.017 0.028 0.047 0.028 0.004 0.033 0.134 0.083 0.123 0.175 -0.042 0.163 -0.090 0.162 -0.107 0.088 -0.040 0.127 0.143 0.060 -0.010 0.172 0.033

43
c_meat -0.085 0.007 0.012 0.022 0.011 -0.004 0.012 0.071 0.039 0.060 0.086 -0.051 0.046 -0.057 0.092 -0.067 0.045 -0.029 0.069 0.078 0.028 -0.015 0.090
c_bake -0.132 0.021 0.031 0.053 0.032 0.009 0.040 0.141 0.092 0.134 0.191 -0.018 0.207 -0.086 0.166 -0.104 0.093 -0.036 0.132 0.149 0.067 -0.003 0.182 0.047
c_bevt -0.140 0.015 0.024 0.043 0.024 -0.001 0.028 0.128 0.076 0.114 0.163 -0.061 0.126 -0.093 0.160 -0.111 0.083 -0.044 0.123 0.138 0.055 -0.017 0.164 0.021
c_omfd -0.164 -0.004 0.002 0.011 -0.002 -0.032 -0.009 0.086 0.026 0.051 0.075 -0.197 -0.128 -0.115 0.141 -0.132 0.052 -0.071 0.093 0.104 0.016 -0.062 0.108 -0.061

44
Annex 5. Table A.5. Fertiliser scenario + Market Access- Quantities variations by food item and households from the CGE mode simulations.
NA MO HR MN MS CO AN AS TU
Q1 Q2 Q3 Q4 Q5 Q1 Q2 Q3 Q4 Q5 RU UR RU UR RU UR RU UR RU UR RU UR RU UR
FERTILISER +
MARKET ACCESS
c_maiz 0.362 0.405 0.475 0.624 0.525 0.523 0.593 0.702 0.792 0.941 1.361 1.798 3.153 0.301 0.741 0.386 0.692 0.447 0.467 0.795 0.684 0.855 0.962 1.040
c_whea 0.382 0.419 0.493 0.649 0.546 0.548 0.622 0.734 0.832 0.991 1.430 1.905 3.353 0.319 0.756 0.403 0.717 0.468 0.490 0.822 0.715 0.891 1.006 1.104
c_rice 0.910 0.825 0.981 1.351 1.126 1.239 1.433 1.640 1.930 2.361 3.344 4.864 8.896 0.802 1.169 0.883 1.410 1.045 1.139 1.570 1.572 1.880 2.229 2.884
c_ogrn 0.344 0.390 0.458 0.599 0.504 0.499 0.564 0.669 0.753 0.892 1.293 1.693 2.955 0.284 0.726 0.369 0.667 0.426 0.444 0.769 0.654 0.820 0.919 0.976
c_root 0.486 0.580 0.679 0.879 0.741 0.716 0.806 0.965 1.074 1.263 1.840 2.344 4.039 0.395 1.128 0.535 0.992 0.615 0.633 1.150 0.947 1.200 1.327 1.342
c_oils 0.426 0.499 0.585 0.760 0.640 0.624 0.703 0.839 0.938 1.106 1.608 2.069 3.581 0.348 0.956 0.464 0.854 0.535 0.552 0.988 0.822 1.038 1.154 1.187
c_frui 0.444 0.536 0.627 0.811 0.684 0.657 0.738 0.886 0.983 1.155 1.684 2.131 3.659 0.360 1.054 0.492 0.918 0.564 0.579 1.065 0.870 1.105 1.219 1.217
c_vege 0.839 0.840 0.992 1.335 1.118 1.174 1.344 1.563 1.804 2.178 3.114 4.342 7.800 0.721 1.363 0.850 1.435 0.996 1.064 1.624 1.510 1.844 2.133 2.547
c_beef 0.133 0.331 0.378 0.436 0.376 0.263 0.270 0.374 0.347 0.348 0.570 0.325 0.216 0.067 0.935 0.225 0.569 0.238 0.203 0.702 0.392 0.571 0.532
c_dair 0.132 0.296 0.338 0.396 0.340 0.248 0.258 0.350 0.334 0.344 0.552 0.380 0.379 0.074 0.810 0.208 0.508 0.223 0.195 0.623 0.363 0.521 0.496 0.164
c_poul 0.060 0.241 0.272 0.301 0.261 0.155 0.148 0.227 0.185 0.158 0.292 -0.021 -0.373 0.009 0.754 0.143 0.414 0.145 0.107 0.522 0.247 0.387
c_oliv 0.077 0.254 0.288 0.324 0.280 0.177 0.175 0.257 0.221 0.355 0.076 -0.190 0.025 0.767 0.159 0.437 0.164 0.129 0.546 0.275 0.419 0.370 -0.019
c_goat 0.130 0.295 0.337 0.394 0.338 0.330 0.546 0.372 0.363 0.073 0.808 0.207 0.506 0.193 0.621 0.361 0.518 0.492 0.159
c_fish -0.001 0.194 0.216 0.219 0.194 0.074 0.054 0.122 0.057 -0.001 0.071 -0.364 -1.015 -0.047 0.706 0.088 0.334 0.078 0.032 0.435 0.148 0.272 0.188 -0.284

45
c_meat 0.021 0.131 0.147 0.158 0.138 0.073 0.066 0.110 0.080 0.057 0.122 -0.090 -0.365 -0.008 0.432 0.072 0.225 0.070 0.046 0.287 0.123 0.201 0.162
c_bake 0.044 0.229 0.258 0.280 0.244 0.134 0.124 0.200 0.152 0.117 0.235 -0.109 -0.538 -0.006 0.741 0.129 0.393 0.127 0.088 0.499 0.221 0.357 0.293 -0.131
c_bevt 0.112 0.281 0.321 0.370 0.319 0.223 0.229 0.317 0.294 0.295 0.483 0.274 0.180 0.057 0.795 0.191 0.483 0.202 0.172 0.596 0.332 0.485 0.452 0.100
c_omfd -0.032 0.170 0.188 0.179 0.160 0.035 0.007 0.070 -0.006 -0.079 -0.039 -0.534 -1.333 -0.075 0.682 0.060 0.294 0.045 -0.005 0.392 0.098 0.215 0.118 -0.386

46
Annex 6. Table A.6. Fertiliser scenario + Extension scenario- Quantities variations by food item and households from the CGE mode simulations.
NA MO HR MN MS CO AN AS TU
Q1 Q2 Q3 Q4 Q5 Q1 Q2 Q3 Q4 Q5 RU UR RU UR RU UR RU UR RU UR RU UR RU UR
FERTILISER +
EXTENSION
c_maiz 0.373 0.452 0.501 0.599 0.563 0.569 0.660 0.768 0.819 0.973 1.382 1.754 2.793 0.493 1.026 0.547 0.802 0.560 1.094 0.586 0.878 0.660 1.151 1.038
c_whea 0.196 0.316 0.337 0.364 0.369 0.337 0.389 0.464 0.452 0.515 0.741 0.765 0.940 0.330 0.887 0.386 0.569 0.367 0.874 0.337 0.591 0.330 0.741 0.442
c_rice 0.102 0.244 0.251 0.240 0.266 0.215 0.245 0.304 0.258 0.273 0.403 0.242 -0.039 0.245 0.813 0.301 0.447 0.265 0.758 0.205 0.439 0.156 0.524 0.128
c_ogrn 0.336 0.423 0.467 0.550 0.523 0.521 0.604 0.705 0.743 0.878 1.249 1.549 2.408 0.459 0.997 0.514 0.753 0.520 1.048 0.535 0.819 0.591 1.065 0.914
c_root 0.395 0.574 0.621 0.695 0.685 0.650 0.751 0.888 0.894 1.036 1.484 1.669 2.321 0.609 1.510 0.700 1.030 0.682 1.523 0.657 1.088 0.679 1.385 0.976
c_oils 0.222 0.396 0.418 0.437 0.453 0.401 0.461 0.556 0.523 0.586 0.849 0.792 0.812 0.409 1.174 0.486 0.717 0.451 1.136 0.396 0.733 0.366 0.906 0.452
c_frui 0.403 0.565 0.614 0.696 0.680 0.653 0.755 0.890 0.907 1.056 1.509 1.743 2.504 0.603 1.449 0.689 1.012 0.677 1.476 0.662 1.076 0.697 1.377 1.022
c_vege 0.447 0.599 0.655 0.755 0.729 0.710 0.822 0.966 0.998 1.170 1.669 1.990 2.967 0.643 1.484 0.729 1.070 0.725 1.531 0.725 1.148 0.779 1.480 1.170
c_beef 0.487 0.674 0.734 0.836 0.814 0.784 0.907 1.069 1.093 1.275 1.822 2.122 3.079 0.721 1.715 0.822 1.207 0.810 1.752 0.797 1.287 0.844 1.650
c_dair 0.437 0.591 0.645 0.741 0.717 0.697 0.807 0.948 0.977 1.144 1.632 1.933 2.859 0.634 1.476 0.719 1.056 0.714 1.518 0.710 1.131 0.760 1.456 1.136
c_poul 0.519 0.654 0.721 0.850 0.808 0.804 0.932 1.089 1.147 1.356 1.929 2.391 3.717 0.709 1.541 0.794 1.164 0.803 1.620 0.826 1.264 0.913
c_oliv 0.334 0.512 0.550 0.605 0.605 0.563 0.649 0.772 0.764
1.261 1.359 1.785 0.540 1.395 0.626 0.921 0.602 1.390 0.566 0.965 0.569 1.218 0.791
c_goat 0.473 0.619 0.678 0.789 0.757
1.052
1.762 2.134 3.236 0.667 1.504 0.752 1.103
1.563 0.761 1.190 0.827 1.539 1.257
c_fish 0.229 0.431 0.453 0.466 0.489 0.425 0.488 0.592 0.546 0.605 0.880 0.771 0.684 0.443 1.312 0.530 0.783 0.487 1.260 0.418 0.794 0.373 0.975 0.437

47
c_meat 0.110 0.235 0.244 0.241 0.260 0.218 0.249 0.306 0.269 0.292 0.428 0.314 0.142 0.238 0.752 0.289 0.428 0.259 0.710 0.211 0.426 0.173 0.516
c_bake 0.289 0.477 0.508 0.545 0.555 0.503 0.579 0.694 0.669 0.760 1.096 1.104 1.307 0.498 1.359 0.584 0.862 0.552 1.334 0.501 0.890 0.484 1.112 0.637
c_bevt 0.335 0.513 0.551 0.607 0.606 0.564 0.651 0.774 0.766 0.881 1.265 1.366 1.798 0.541 1.396 0.627 0.923 0.603 1.392 0.567 0.967 0.571 1.221 0.795
c_omfd -0.014 0.244 0.229 0.144 0.222 0.107 0.114 0.175 0.041 -0.025 0.001 -0.589 -1.862 0.220 1.121 0.309 0.464 0.221 0.958 0.075 0.399 -0.080 0.411 -0.381

48
Annex 7. Table A.7. Food matching between Kenya SAM 2014 and KIHBS 2015/2016SAM
SAM codes Food groups Food items
c_bake Bread and cereals Biscuits …
Brown bread
Cakes
Other bread
Pasta (spaghetti, macaroni, noodles e.g., indomie)
Wheat buns/scones
White bread
Sugar, jam, honey, chocolate Chewing gum
Chocolate bar
Honey
Jaggery (nguru)
Jam
Marmalade
Other sugar (confectionary)
Sugar
Sugar-icing
Sweets
c_beef Meat Beef - without bones
c_bevt Beer Beer (lagers touts)
Other beers
Traditional beer
Coffee, tea and cocoa Cocoa and cocoa products
Coffee
Other coffee, tea and cocoa
Soya drink
Tea leaves
Mineral water, soft drinks, fruit and vegetable juices Energy/Health drink
Fruit juice
Mineral water
Other drinks
Sodas
Squashes
Vegetable juice
Spirits Brandy
Chang'aa
Other spirits

49
Rum
Vodka
Whisky
Wine Fortified wines
Sparkling wines (e.g., champagne)
Wine (e.g., cider, king fisher, etc)
c_dair Milk, cheese and eggs Camel milk
Cheese
Condensed/powder milk
Eggs - exotic/kienyenji
Fresh flavoured packeted cow milk
Fresh packeted cow milk
Fresh unpacketed cow milk / fresh cream
Goat milk
Milk sour - packeted mala
Milk sour - unpacketed mala
Other
UHT- long life milk
Yoghurt
Oils and fats Butter
c_fish Fish and seafood Dried/Smoked fish (Excluding Omena)
Fresh fish
Frozen fish fillets
Omena
Other fish
Prawns/Other sea foods
c_frui Fruits Apples
Avocado
Coconut
Grape fruit
Grapes
Guavas
Lemons
Lime
Loquats
Mangoes
Melons
Oranges

50
Other fruits/Berries
Passion
Paw paws
Peaches
Pears
Pineapples
Plums
Ripe bananas
Strawberries
Tangerines
Tree tomato
Sugar, jam, honey, chocolate Sugar cane
c_maiz Bread and cereals Fortified maize flour
Green maize
Green maize- loose
Maize flour - loose
Maize flour - sifted
Maize grain - loose
Popcorn
c_meat Meat Beef - with bones
Beef brawn
Camel meat
Canned beef/Ham/Salami
Meat paste for hamburger
Minced meat
Mutton/Goat meat
Other Meats products
Pork
Pork Brawn/Bacon
Rabbit meat
Sausages/Smokies/Hot dog
Tinned /Packeted soups (meat)
c_ogrn Bread and cereals Baby food cereals (tinned)
Barley and other cereals
Breakfast cereal/Oats
Cassava flour
Fortified porridge flour
Millet flour

51
Millet grain
Mixed porridge flour
Other grain/Flour
Sesame Seeds/Simsim
Sorghum flour
Sorghum grain
Soya flour
c_oils Bread and cereals Beans
Cashew nuts
Chicken peas
Cowpeas
Dolicos (Njahi)
Green grams
Groundnuts
Macadamia
Other grams
Peas
Oils and fats Cooking fat
Cooking oil (Salad)
Fortified cooking fat
Fortified margarine
Ghee
Lard (From butcheries)
Margarine
Other oils and fats
Peanut butter
c_omfd Bread and cereals Other pulses
Tinned beans
Tinned pulses
Fish and seafood Tinned fish
Food products n.e.c. spices & miscellaneous Baking powder /Bicarbonate
Chilli sauce
Common salt
Crisps
Food seasoning (e.g., royco, knorr, etc,)
Ginger-tangawizi
Magadi (sodium bicarbonate)
Mustard

52
Other food n.e.c./ Spices
Pickles
Pilau masala
Tomato sauce
Vinegar
Yeast
Meat Offals (liver and kidney)
Offals (matumbo)
Milk, cheese and eggs Baby milk - tinned
c_poul Meat Chicken meat (broiler kienyeji)
c_rice Bread and cereals Aromatic unbroken rice (pishori/basmati/etc.)
Broken white rice (aromatic or non-aromatic)
Brown rice
Non aromatic (unbroken), white rice
c_root Roots and tubers Arrow roots-nduma
Cassava
Dried cassava
Other roots and tubers
Potatoes (Irish)
Sweet potato
Yams
c_vege Vegetables Aubergines-eggplant (biringanya)
Beetroot
Broccoli radish
Cabbages
Capsicums (pilipili hoho)
Carrots
Cooking bananas
Coriander leaves (dania)
Courgettes/Squash/Marrow
Cucumber
French beans
Kale-Sukuma wiki
Lettuce celery
Mushrooms and Asian vegetables
Onion - bulbs
Onion - leeks
Other vegetables (specify)

53
Peas (garden, snap, snow)
Pepper - pilipili
Pumpkins/Butter nut
Runner/Broad bean
Spinach
Tinned/packeted vegetables
Tomatoes
Traditional vegetables
Turnips
c_whea Bread and cereals Fortified wheat flour
Wheat flour-brown
Wheat flour-white
Wheat grain
Vegetables Baby and sweet corn

GETTING IN TOUCH WITH THE EU
In person
All over the European Union there are hundreds of Europe Direct information centres. You can find the address of the centre nearest you at: https://europa.eu/european-union/contact_en
On the phone or by email
Europe Direct is a service that answers your questions about the European Union. You can contact this service:
- by freephone: 00 800 6 7 8 9 10 11 (certain operators may charge for these calls),
- at the following standard number: +32 22999696, or
- by electronic mail via: https://europa.eu/european-union/contact_en
FINDING INFORMATION ABOUT THE EU
Online
Information about the European Union in all the official languages of the EU is available on the Europa website at: https://europa.eu/european-union/index_en
EU publications
You can download or order free and priced EU publications from EU Bookshop at: https://publications.europa.eu/en/publications. Multiple copies of free publications may be obtained by contacting Europe Direct or your local information centre (see https://europa.eu/european-union/contact_en).

KJ-N
A-3
00
34
-EN-N
doi:10.2760/925912 ISBN 978-92-76-14654-4
Related Documents