CURICULUM VITAE M A : Prof.Dr.TAMSIL SYAFIUDDIN Sp.P (K) AT : Jln.KARSA No F 1 KOMPLEKS EKS KOWILHAN I SEI.AGUL MEDAN 20117 RJAAN : Guru Besar FK- UISU / FK- USU RIWAYAT PENDIDIKAN : okter Umum FK-USU Medan,1979 okter Spesialis I Paru FK-UI Jakarta, 1990 okter Spesialis II Paru, Konsultan Asma/PPOK, 1995 Pendidikan tambahan: - Pelatihan Kanker Paru, TSUKAGUCHI Hospital, Kobe- Japan 198 Pelatihan PPOK, AMAGASAKI Hospital, Kobe- Japan 1990 Pelatihan Respiratory Physiologi, ”JAPAN RESPIRATORY PHYSIOLOGIST CLUB”, Kyoto- Japan 1990 - Spirometry Training Course, Department of Respiratory Medic National University Hospital Singapore, Singapore 1997

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
CURICULUM VITAEN A M A: Prof.Dr.TAMSIL SYAFIUDDIN Sp.P (K)ALAMAT: Jln.KARSA No F 1 KOMPLEKS EKS KOWILHAN I SEI.AGUL MEDAN 20117PEKERJAAN : Guru Besar FK- UISU / FK- USU RIWAYAT PENDIDIKAN : -Dokter Umum FK-USU Medan,1979 -Dokter Spesialis I Paru FK-UI Jakarta, 1990 -Dokter Spesialis II Paru, Konsultan Asma/PPOK, 1995 Pendidikan tambahan: - Pelatihan Kanker Paru, TSUKAGUCHI Hospital, Kobe- Japan 1989 - Pelatihan PPOK, AMAGASAKI Hospital, Kobe- Japan 1990 - Pelatihan Respiratory Physiologi, JAPAN RESPIRATORY PHYSIOLOGIST CLUB, Kyoto- Japan 1990 - Spirometry Training Course, Department of Respiratory Medicine, National University Hospital Singapore, Singapore 1997
-
-Workshop of Bronchoscopy and Autofluorecent Bronchoscopy, RS Persahabatan Jakarta, Jakarta September 2005
-Training of the new interventional technique of bronchosfiberscopy (Optical Coherence Tommograhy) , Department of Thoracic Surgery, Tokyo Medical University Hospital,Tokyo - Japan 2007
-Workshop new technique of Bronchoscopy, Postgradute Medical Institute, Singapore General Hospital, Singapore 2009.- Workshop on Medical Thoracoscopy, The American College of Chest Physicians-The Indonesian Association of Pulmonologist, RS Persahabatan Jakarta, Jakarta November 1997
- Workshop on Reformation of Higer Education System,HEDS-JICA,Jakarta 1998
-Pulmonary Infections Course, Postgraduate Medical Institute, Singapore General Hospital, Singapore 2001
- Bronchoscopy &Thoracoscopy Workshop, Postgraduate Medical Institute, Singapore General Hospital, Singapore 2005 Workshop on Transbronchial Lung Biopsy and Trasbronchial Needle Aspiration PDPI Cabang Jakarta, RS Persahabatan Jakarta ,Jakarta Maret 1997 - Workshop on Respiratory Physiology and Its Clinical Application, RS Pusat Angkatan Darat Gatot Subroto Jakarta, Jakarta Juni 1997
-
Departemen PulmonologiFakultas KedokteranUniversitas Sumatera Utara2009Prof.Dr.Tamsil Syafiuddin,SpP(K)Dr.Bintang Sinaga, SpP Asthma
-
Tingkat kemampuan yang diharapkan dicapai pada akhir pendidikan dokter
Tingkat Kemampuan 1Dapat mengenali dan menempatkan gambaran-gambaran klinik sesuai penyakit ini ketika membaca literatur. Dalam korespondensi, ia dapat mengenal gambaran klinik ini, dan tahu bagaimana mendapatkan informasi lebih lanjut. Level ini mengindikasikan overview level.Bila menghadapi pasien dengan gambaran klinik ini dan menduga penyakitnya, Dokter segera merujuk.
Tingkat Kemampuan 2Mampu membuat diagnosis klinik berdasarkan pemeriksaan fisik dan pemeriksaanpemeriksaan tambahan yang diminta oleh dokter (misalnya : pemeriksaan laboratorium sederhana atau X-ray).Dokter mampu merujuk pasien secepatnya ke spesialis yang relevandan mampu menindaklanjuti sesudahnyaStandar Kompetensi Dokter , Konsil Kedokteran Indonesia, 2006
-
Tingkat Kemampuan 33a. Mampu membuat diagnosis klinik berdasarkan pemeriksaan fisik dan pemeriksaanpemeriksaan tambahan yang diminta oleh dokter (misalnya : pemeriksaan laboratorium sederhana atau X-ray). Dokter dapat memutuskan dan memberi terapi pendahuluan, serta merujuk ke spesialis yang relevan (bukan kasus gawat darurat).
3b. Mampu membuat diagnosis klinik berdasarkan pemeriksaan fisik dan pemeriksaanpemeriksaan tambahan yang diminta oleh dokter (misalnya : pemeriksaan laboratorium sederhana atau X-ray).Dokter dapat memutuskan dan memberi terapi pendahuluan, serta merujuk ke spesialis yang relevan (kasus gawat darurat)..Standar Kompetensi Dokter , Konsil Kedokteran Indonesia, 2006
-
Standar Kompetensi Dokter , Konsil Kedokteran Indonesia, 2006 Tingkat kemampuan4: Mampu membuat diagnosis klinik berdasarkan pemeriksaan fisik dan pemeriksaan tambahan yang diminta oleh dokter (misalnya: pemeriksaan laboratorum sederhana atau X-ray). Dokter dapat memutuskan dan mampu menangani problem itu secara mandiri hingga tuntas.
-
Levels of competenceStandar Kompetensi Dokter , Konsil Kedokteran Indonesia, 2006
-
Bronchiectasis 1 2 3A 3B 4COPD 1 2 3A 3B 4SARS 1 2 3A 3B 4Pneumonia 1 2 3A 3B 4Avian influenzae 1 2 3A 3B 4Lung abscess 1 2 3A 3B 4Pulmonary embolism 1 2 3A 3B 4Lung infarction 1 2 3A 3B 4Pleurisy TBC 1 2 3A 3B 4Pleurisy Cancer 1 2 3A 3B 4Pleurisy Lupus 1 2 3A 3B 4Pneumothorax 1 2 3A 3B 4Cystic fibrosis 1 2 3A 3B 4Aspiration pneumonia 1 2 3A 3B 4Standar Kompetensi Dokter , Konsil Kedokteran Indonesia, 2006
-
Diagnosis of Asthma
-
IDENTIFIKASI MASALAH/ANALISIS:MASALAH/DATA:PEMECAHAN MASALAH/RENCANA(Planning):KURIKULUM BERBASIS KOMPETENSI (Problem Based learning)
-
IDENTIFIKASI MASALAH/ANALISIS:DATA LAINRENCANA BERIKUT PF, Ro
BatukSesak napas Batuk darahNyeri dada
OBSTRUKTIFINFEKSI KEGANASANPENYAKIT ORGAN LAIN
MASALAH/DATA:PEMECAHAN MASALAH/RENCANA(Planning):Daftar keluhan Standar Kompetensi Dokter Indonesia
-
IDENTIFIKASI MASALAH/ANALISIS:DATA LAIN: Usia :Semua usia Riwayat Keluarga Riwayat Mengi Riwayat Obat (BD)RENCANA BERIKUTPem Fisik :Tanda Obtruktif: Eksirasi memanjang/MengiRO : NormalSpirometri : Tanda obstruktifBatukSesak napasBatuk darahNyeri dada
OBSTRUKTIF : ASMA, PPOKINFEKSIKEGANASANPENYAKIT ORGAN LAIN
MASALAH/DATA:PEMECAHAN MASALAH/RENCANA(Planning):
-
Recent issues in asthma managementThe Unmet Needs of asthma Theme of World Asthma Day 2005/2006 You can control your asthma Theme of World Asthma Day 2007/2008Adherence Self ManagementUUD No 29 / 2004 : Praktik Kedokteran CompetencyPharmacoeconomic consideration Quality of Life
-
Definition of asthma Chronic inflammatory disease of airways (AW) responsiveness of tracheobronchial tree Physiologic manifestation: AW narrowing relieved spontaneously or with BD Cster Clinical manifestations: a triad of paroxysms of cough, dyspnea and wheezing.
-
Asthma is an inflammatory diseases
-
Disease Pattern Episodic --- acute exacerbations interspersedwith symptom-free periods Chronic --- daily AW obstruction which may be mild, moderate or severe superimposed acute exacerbations Life-threatening--- slow-onset or fast-onset(fatal within 2 hours)
-
1. Warner O. Am J Resp Crit Care Med 2003; 167: 14651466. Bronchoconstriction Bronchial oedema Mucous hypersecretion Inflammatory cell recruitment eosinophilsAsthma symptoms: the tip of the iceberg1
-
Asthma Pathology and Therapy Evolution197519801985199019952000Large use of short-acting 2-agonists Fear of short-acting 2-agonistsSingle inhaler therapy ICS+LABAICS treatment introduced1972 Adding LAA to ICS therapy Kips et al, AJRCCM 2000 Pauwels et al, NEJM 1997 Greening et al, Lancet 1992
BronchospasmInflammationRemodelling
-
NormalAsthmaInflammation(+)() Bronchial hyperreactivity ( + )Bronchial hyperreactivity ( - ) Symptoms (+)Symptoms (-)TriggersBronchoconstriction ( - )Bronchoconstriction ( + )TriggersThe pathogenesis of asthma
-
Ig EAgYYMethyl transferasePhospholipidPhosphatidylethanolaminePhosphatidyl cholinePhospholipase A2Ca++HistaminCa++HistaminECF, NCFArachidonic acidlypoxygenasecyclooxygenase5-HETELeucotrienesLTB4LTC4LTD4LTE4ThromboxanesTXA2ProstaglandinsPGDPGF2Mediator release in asthma reactions
-
MBP, ECPEosinophilEpitheliumAIRWAY REMODELLING IN ASTHMADesquamations of epitheliumThickening of basement membraneIncrease in airway smooth muscle
-
Epithelial Damage P Jeffery, in: Asthma, Academic Press 1998
-
Basement Membrane ThickeningP Jeffery, in: Asthma, Academic Press 1998
-
P Jeffery, in: Asthma, Academic Press 1998
-
InflammationBronchial hyperreactivitySymptomsControllerRelieverMedicines and Pathogenesis of asthmaBronchoconstriction
-
Reliever:Controler:
-
Guidelines on Asthma Management: Past and Current TrendsLABA and ICSICSLABA+ICSGINA 1998 (adapted)GINA 2006Severe persistentModerate persistentMild persistent
Intermittent SABA / Rapid onset of action LABA ExacerbationStable condition Total controlPartially controlUncontrol
Old classification
New classification
-
Acute severe asthma:MANAGEMENT 11.Immediate Rx: O2 40-60% mask or cannula + SABA (salbutamol 5mg)/ nebulizer + ICS 200 mcg/ nebulizer or hydrocortisone 200mg IV. With lifethreatening features add 0.5mg ipratropium to nebulized 2 agonist + Aminophyllin 250mg iv over 20 min or salbutamol 250ug over 10 min.
2. Subsequent Rx: Nebulized SABA 6 hourly + ICS 200mcg or hydrocortisone 200mg 6 hourly IV + 40-60% O2.
-
MANAGEMENT 2
No improvement after 15-30 min: Nebulized 2 agonist every 15-30 min + Ipratropium.
Still no improvement: Aminophyllin infusion 750mg/24H (small pt), 1500mg/24H (large pt), or alternatively salbutamol infusion.
Monitor Rx: Aminophyllin blood levels + PEF after 15-30 min + oxymetry (maintain SaO2 > 90) + repeat blood gasesafter 2 hrs if initial PaO2 < 60, PaCO2 normal or raised andpatient deteriorates. Deterioration: ICU, intubate, ventilate + muscle relaxant.
-
ASTHMA MANAGEMENT: CLINICAL
QUICK RELIEVE MEDICATION
LONG TERM TREATMENT
-
Anti Inflammations is the mainstay therapy!
-
Inhalation therapy is the mainstay therapyBecause minimally side effect!
-
Controller: Anti inflammationbudesonide (Pulmicort) (Inflamid)beclomethasone dipropionate (Becotide) triamcinolone acetonidefluticasone(Flexotide)sodium chromoglicate (Intal)ketotifensodium nedocromil Inhaled Cortico SteroidNon steroid
-
Bronchodilator2 - agonist XanthinAnticholinergicReliever
-
BRONCHODILATORShort Acting 2 AGONIST (SABA):salbutamol/albuterol (Ventolin )terbutaline (Bricasma)procaterolfenoterolorciprenaline, etcANTICHOLINERGIC:atropine sulfate ipratropium bromidetiotropium bromideOTHER SYMPHATOMIMETIC: ephedrineadrenaline, etcXANTHINE:theophyllineaminophyllineLong Acting 2 AGONIST:(LABA)salmoterolformoterol
-
Combination therapy
SymbicortBudesonide + Formoterol
SeretideFluticasone + Salmoterol
-
The Beginning of Treatment
-
ExacerbationThe beginning of treatment?Stable condition x
-
Asthma management* Stable condition * Long-term therapy
-
Evaluations
-
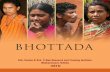
Inflammation can also be present during symptom-free periodsAdapted from Woolcock A. Clin Exp Allergy Rev 2001; 1: 6264. AHR is a marker of inflammationAHRRescue medication useImpaired am PEFImpaired FEV1Start of treatment% Reduction24618Rate of response of different measures of asthma control over 18 months of ICS treatmentNightsymptomsMonths
-
Peak flow meter600-700 0300( normal )Objective values
-
Peak Flow Meter /PEFR/APEMust be avilable
-
PEFR Monitoring:A Major Tool in Asthma Self-ManagementChronic DiseasesMonitorHypertension
Diabetes
AsthmaBlood pressure
Serum glucose
PEFR
-
Asthma Control Test Asthma Control Questionnaire Asthma Therapy Assessment Questionnaire Asthma Control Scoring System
-
5
-
5
-
5
-
5
-
5
-
Objective use of ACTACT is a scored tool which allows numerical targets to be set. Simple to complete 5 questions with a 5 point rating scale (max: 25)
19 or less = Uncontrolled asthma20-24 = Well controlled25 = Total Control
Improves patient / physician communication. Clear and concise questions that engage patients in a more open, candid discussionValidated using spirometry and specialist assessment
-
None (2 or less / week)NoneNoneNone (2 or less / week)NormalNoneDaytime symptomsLimitations of activitiesNocturnal symptoms / awakeningNeed for rescue / reliever treatmentLung function (PEF or FEV1)ExacerbationCONTROLLEDCharacteristicsMore than twice / weekAnyAnyMore than twice / week< 80% predicted or personal best (if known) on any dayOnce/more per yearPARTLY CONTROLLED3 or more features of partly controlled asthma present in any weekOne in any weekUNCONTROLLEDAsthma ClassificationGINA updated 2008Classification of Asthma Severity by Levels of Asthma Control(new classification)
-
The goal of asthma treatment
To achieve and maintainclinical controlQ o L
-
DIFFERENTIAL DIAGNOSIS
1. Upper airway obstruction glottic dysfunction.2. Acute LV failure pulmonary oedema.3. Pulmonary embolism.4. Endobronchial disease.5. Chronic bronchitis.6. Eosinophilic pneumonia.7. Carsinoid syndrome.8. Vasculitis.
-
DIAGNOSIS EXACERBATION : CLINICAL
Episodic asthma: Paroxysms of wheeze, dyspnoea andcough, asymptomatic between attacks.
Acute severe asthma: upright position, use accessory resp muscles, cant complete sentences in one breath, tachypnea > 25/min, tachycardia > 110/min, PEF 33-50% of pred or best, pulsus paradoxus, chest hyperresonant, prolonged expiration, breath sounds decreased, inspiratory andexpiratory rhonchi, cough.
-
Life-threatening features: PEF < 33% of pred or best,silent chest, cyanosis, bradycardia, hypotension, feeble respiratory effort, exhaustion, confusion, coma, PaO2 < 60,PCO2 normal or increased, acidosis (low pH or high [H+]).
Chronic asthma: Dyspnea on exertion, wheeze, chest tightness and cough on daily basis, usually at night and early morning; intercurrent acute severe asthma (exacerbations)and productive cough (mucoid sputum), recurrent respiratory infection, expiratory rhonchi throughout and accentuated on forced expiration.
-
Life is not problem to be solved, but a reality to be experienced ( Soren Kierkegaard)
-
Classification of Asthma Severity byClinical Features Before Treatment:(old classification)Intermittent:Symptoms less than once a weekBrief exacerbationsNocturnal symptoms not more than twice a month FEV1 or PEF 80% predicted PEF or FEV1 variability < 20%
Mild Persistent:Symptoms more than once a week but less than once a dayExacerbations may affect activity and sleepNocturnal symptoms more than twice a month FEV1 or PEF 80% predicted PEF or FEV1 variability < 20 30%GINA. 2006
-
Moderate Persistent:Symptoms dailyExacerbations may affect activity and sleepNocturnal symptoms more than once a weekDaily use of inhaled short-acting 2-agonist FEV1 or PEF 60-80% predicted PEF or FEV1 variability > 30%
Severe Persistent:Symptoms dailyFrequent exacerbationsFrequent nocturnal asthma symptomsLimitation of physical activities FEV1 or PEF 60% predicted PEF or FEV1 variability > 30%GINA. 2006
-
TERIMA KASIH, DOMO ARIGATOO GOZAIMASU
Related Documents