AOE Aseptic Non Union Aseptic Non-Union

Aseptic Non-Union
Feb 04, 2016
Aseptic Non-Union. AO Principles Course. Dr. Enrique Queipo de Llano Hospital Universitario de Málaga. Definition. No bone healing in the normal time Usually 6 a 8 months. Etiology. Do not blame the osteoblasts (Watson Jones). - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
AOEAOEAseptic Non Union
Aseptic Non-Union
AOEAOEAseptic Non Union
AO Principles Course
Dr. Enrique Queipo de Llano
Hospital Universitario de Málaga
AOEAOEAseptic Non Union
No bone healing in the normal time
Usually 6 a 8 months
Definition
AOEAOEAseptic Non Union
Do not blame the osteoblasts (Watson
Jones).
Fractures have a spontaneous tendency to heal. (Merle D’Aubigne).
Delayed or non-union is often multifactorial in nature.
Etiology
AOEAOEAseptic Non Union
Disturbed vascularity and instability are the most important factors leading to a non-union.
Etiology
AOEAOEAseptic Non Union
BiologicalCarpal scaphoidNeck of the femurTalusDevitalized fragments
Etiology (Vascularisation)
AOEAOEAseptic Non Union
Etiology (Instability)
Iatrogenic Insufficient orthopaedic treatment Incorrect osteosynthesis (unstable)
AOEAOEAseptic Non Union
Good reduction Contact between fragments Strict immobilization
Orthopaedic treatment
Conditions for a normal bone healing
AOEAOEAseptic Non Union
Anatomic reduction of articular fractures Good alignment of diaphyseal fractures Stable osteosynthesis Absolute asepsis
Surgical treatment
Conditions for a normal bone healing
AOEAOEAseptic Non Union
Non compliant patient The care plan has to be compatible
with the patient’s personality and life style.
Have to be controlled: Inappropriate weight bearing Smoking habit Improper diet Other shortcomings in behaviour
AOEAOEAseptic Non Union
Symptoms Abnormal mobility Abnormal mobility cannot be seen:
When there is an Internal Fixation Intramedullary nailDense fibrous callus
Pain and Limp A healed fracture does not hurt
AOEAOEAseptic Non Union
Radiology Sometimes difficult to see on the X-Rays
Reactive callus = Mechanical instability
Slight instability can be positive
AOEAOEAseptic Non Union
Delayed union In delayed union there are clinical and
radiological signs of prolonged fracture healing
It is important to establish the diagnosis Fracture instability Implant mobilization
To act to achieve a rapid bone healing
AOEAOEAseptic Non Union
Judet-Weber classification
A. Vital (Hypervascular) With biological reaction capacity
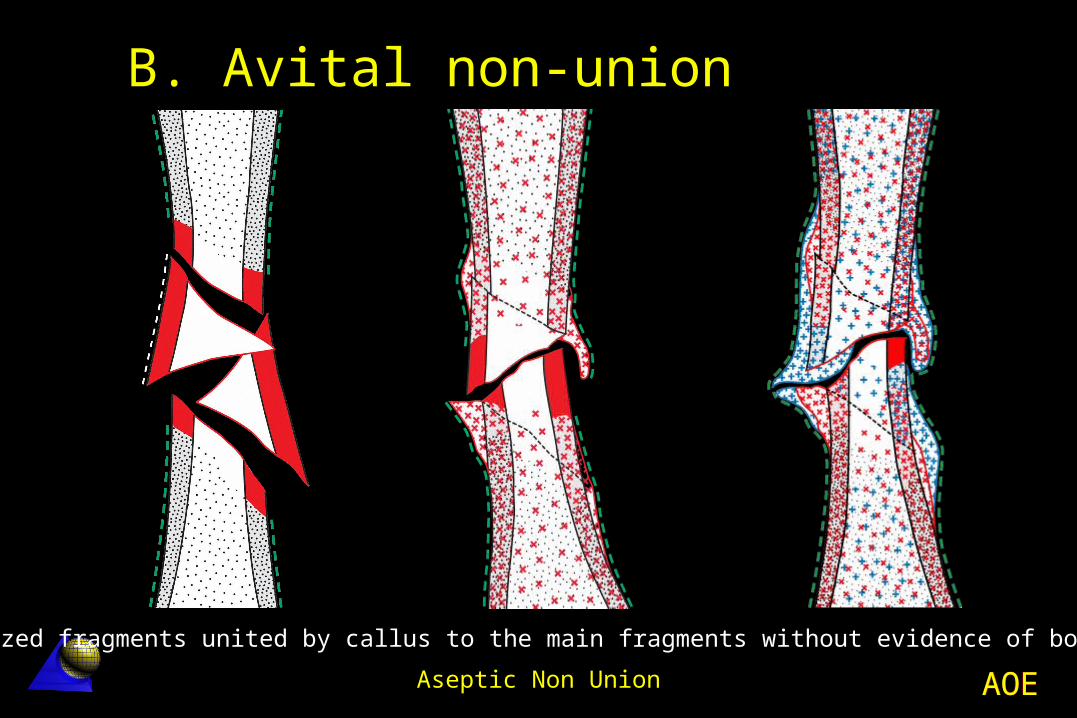
B. Avital (Avascular) Without biological reaction
capacity
AOEAOEAseptic Non Union
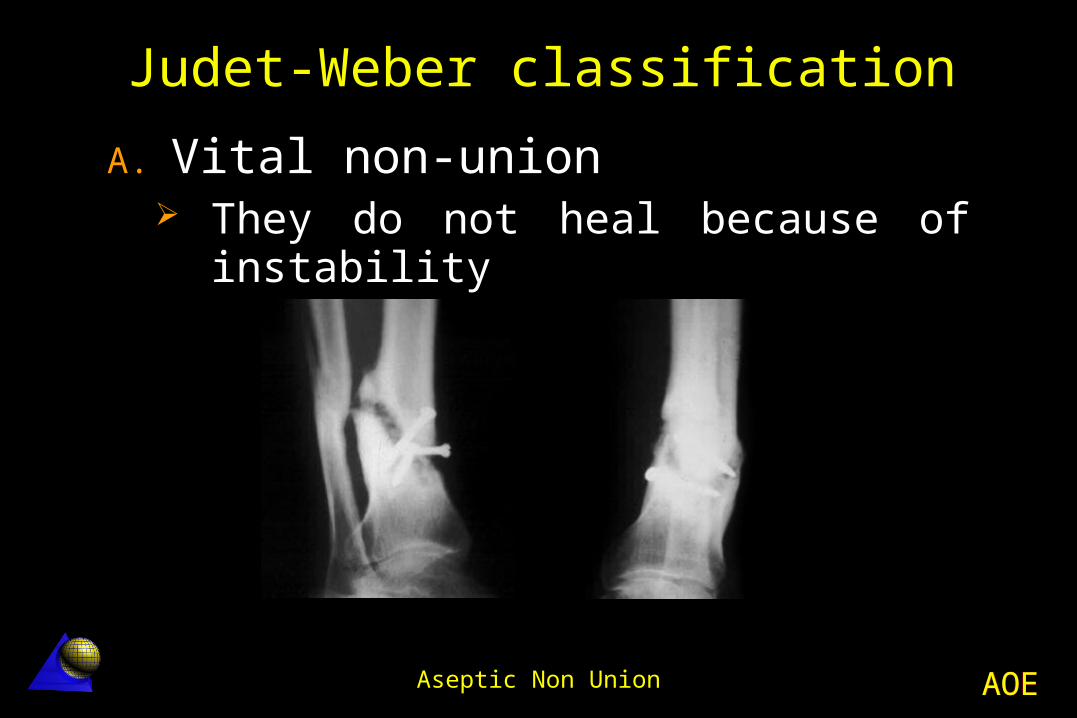
A. Vital non-union They do not heal because of
instability
Judet-Weber classification
AOEAOEAseptic Non Union
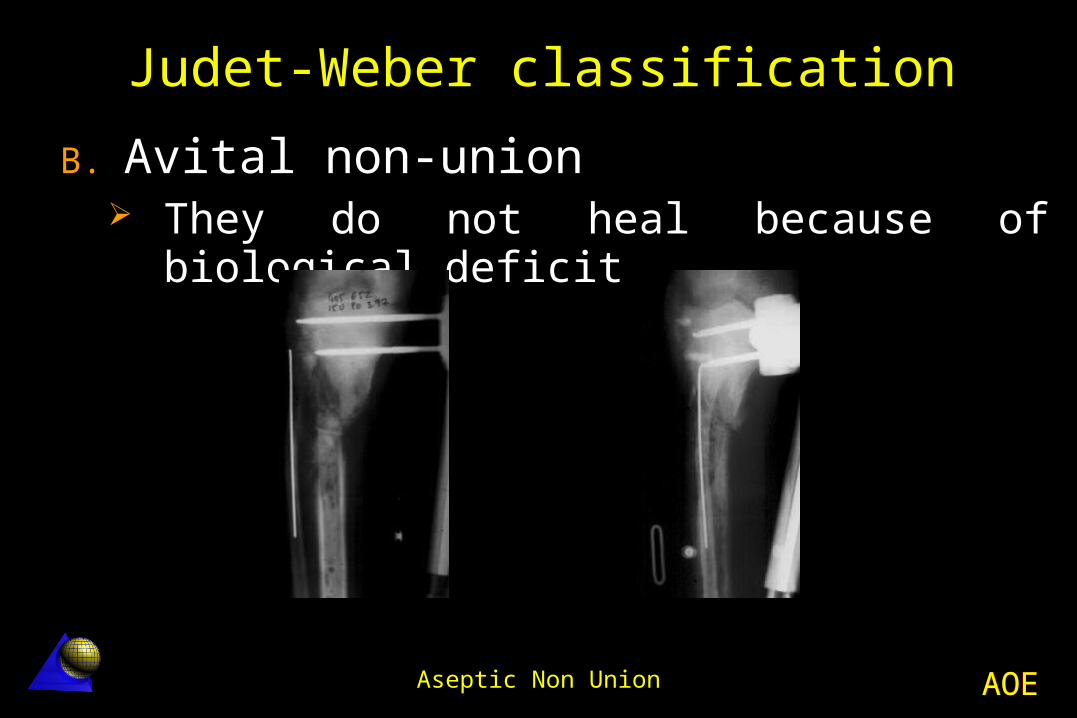
B. Avital non-union They do not heal because of biological
deficit
Judet-Weber classification
AOEAOEAseptic Non Union
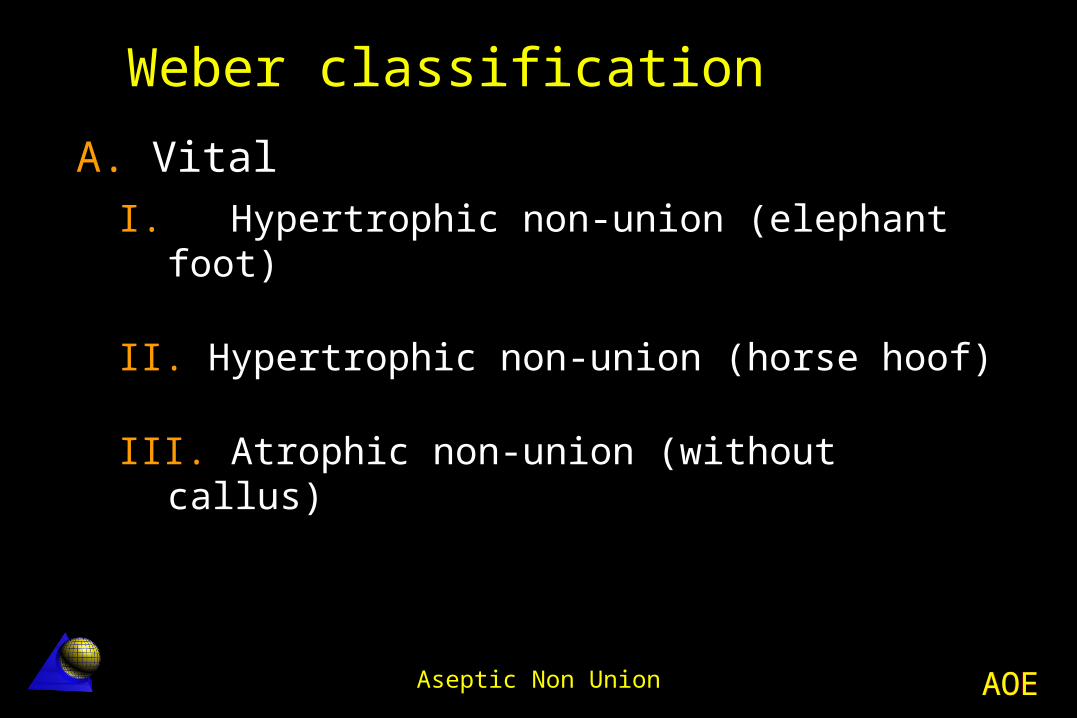
Weber classification
A. VitalI. Hypertrophic non-union (elephant
foot)
II. Hypertrophic non-union (horse hoof)
III. Atrophic non-union (without callus)
AOEAOEAseptic Non Union
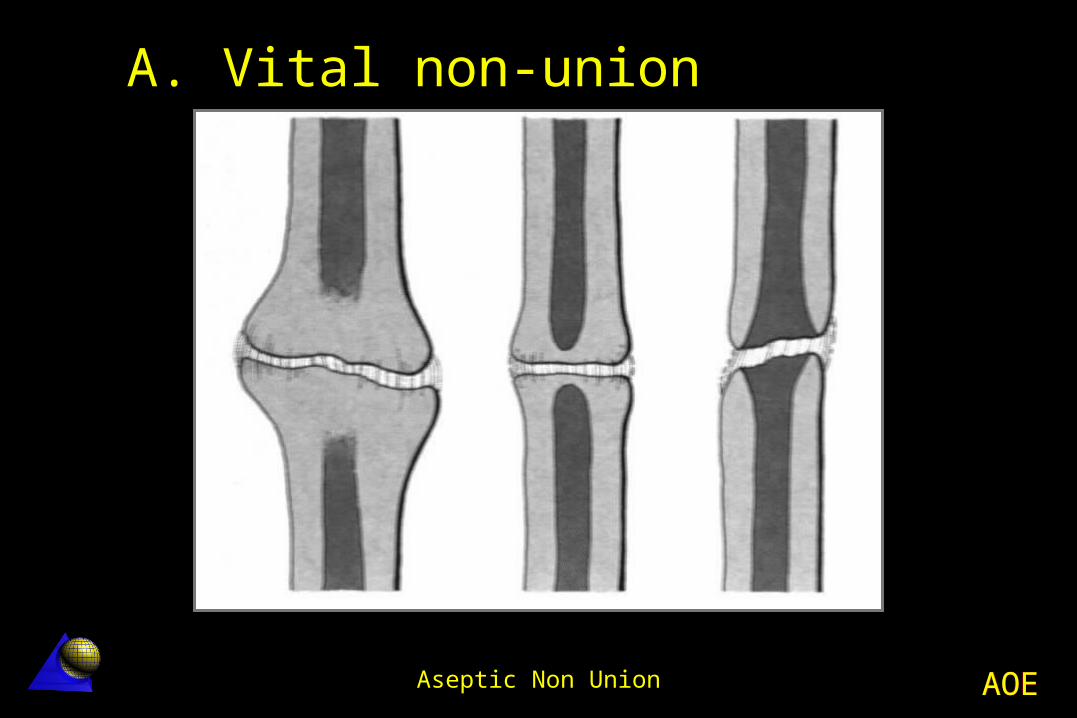
A. Vital non-union
AOEAOEAseptic Non Union
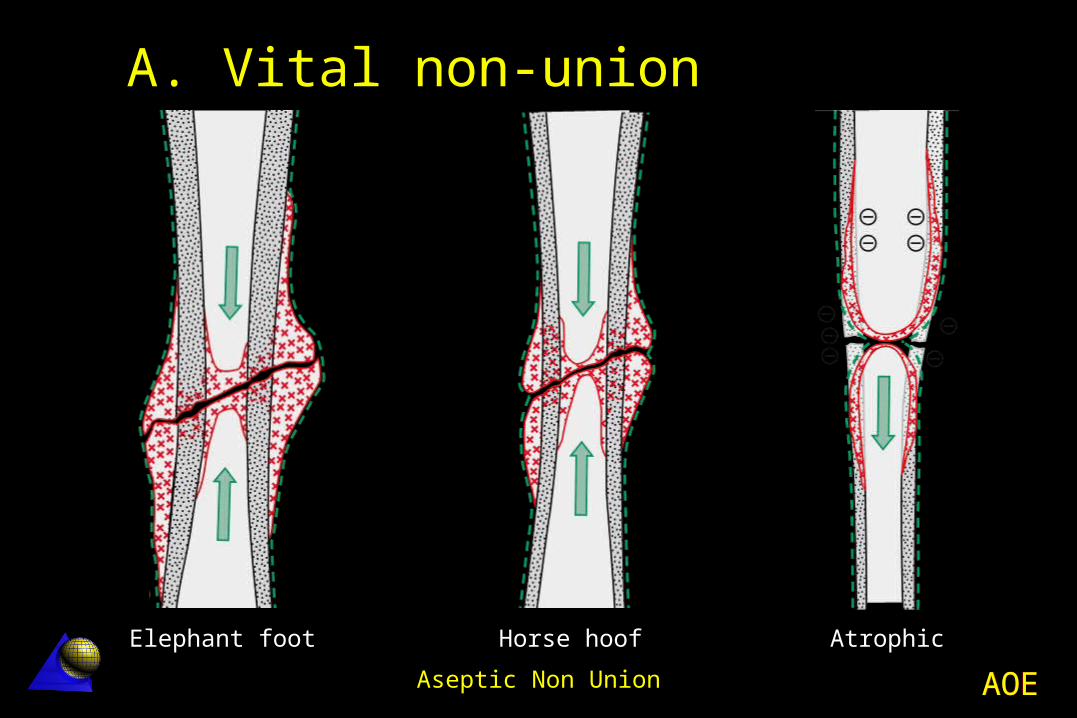
A. Vital non-union
Elephant foot Horse hoof Atrophic
AOEAOEAseptic Non Union
Hypertrophic non-union Hypertrophic non-union is frequently
localized in the lower extremities.
Its development largely depends on an impaired mechanical stability.
AOEAOEAseptic Non Union
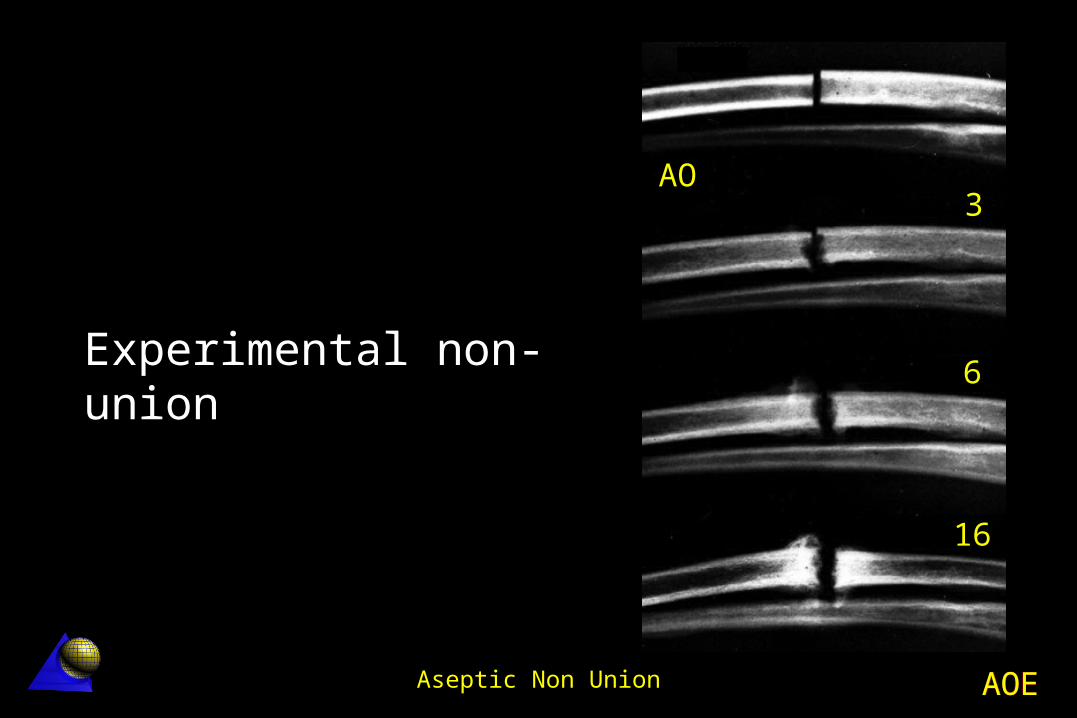
Experimental non-union
AO3
6
16
AOEAOEAseptic Non Union
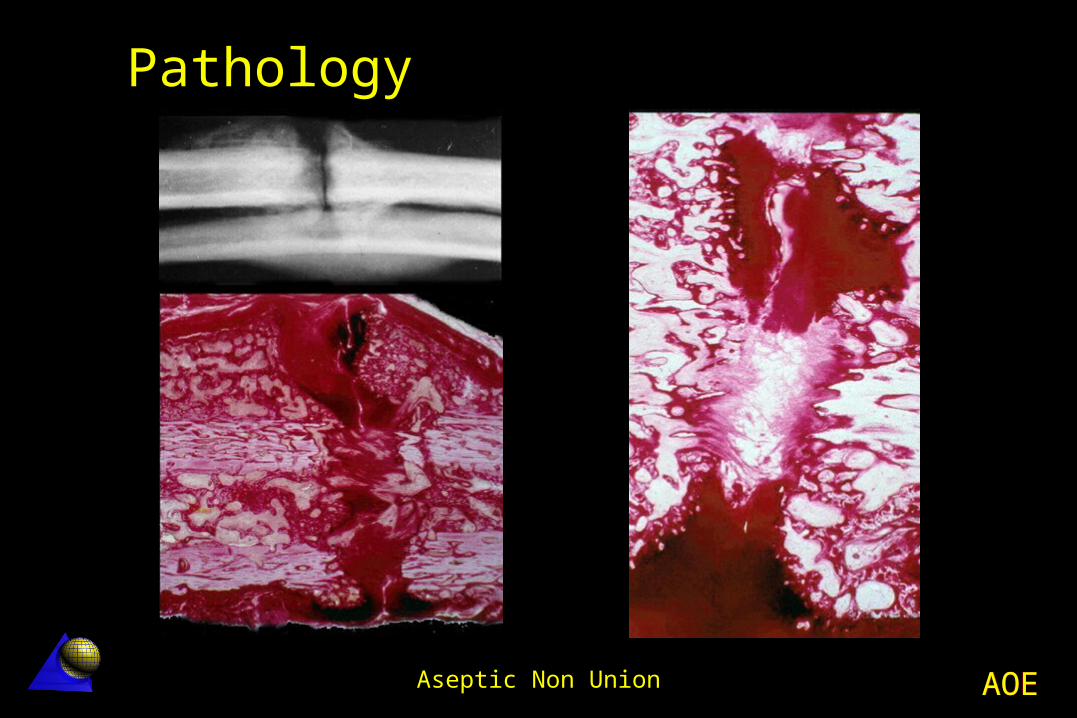
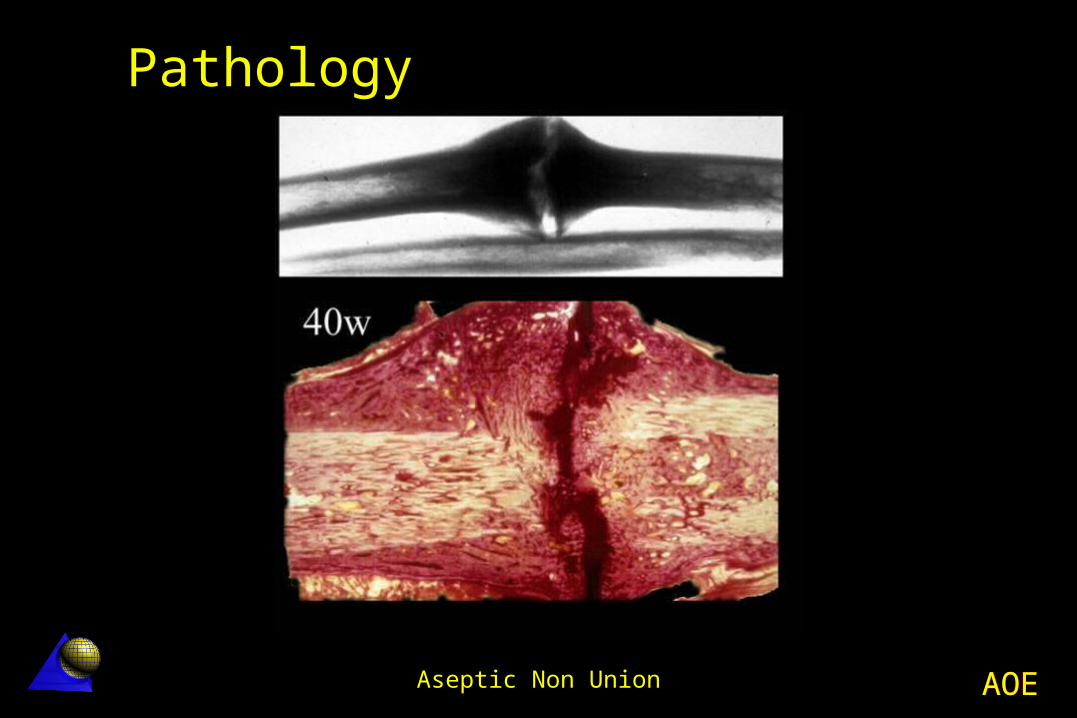
Pathology
AOEAOEAseptic Non Union
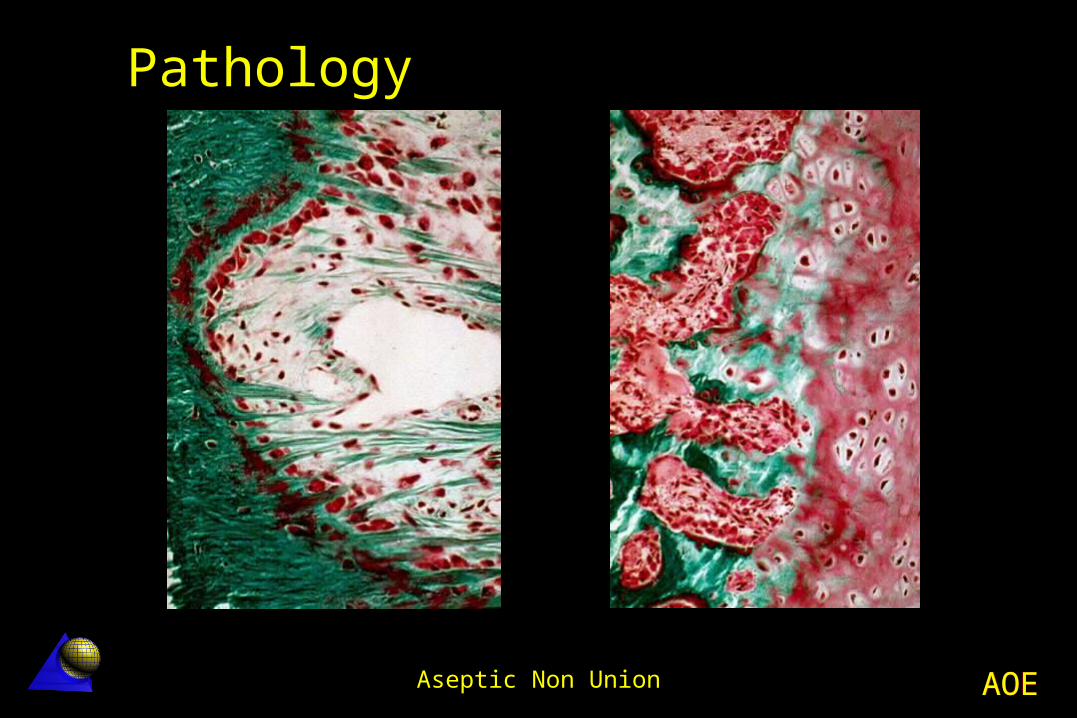
Pathology
AOEAOEAseptic Non Union
Pathology

AOEAOEAseptic Non Union
Pathology
AOEAOEAseptic Non Union
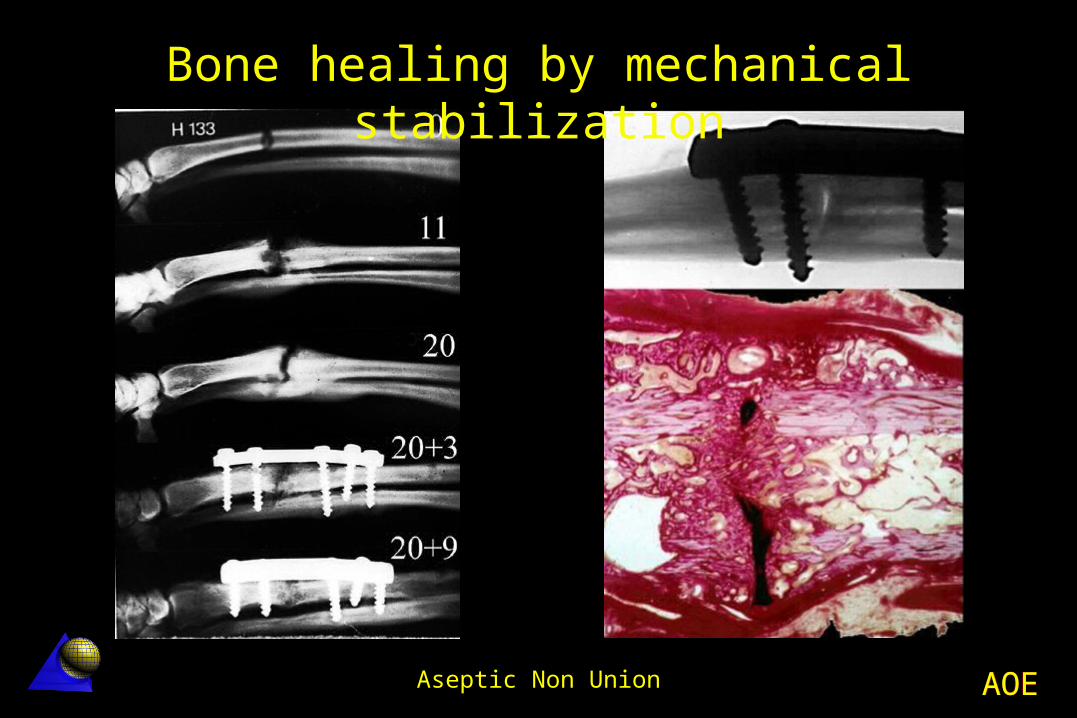
Bone healing by mechanical stabilization
AOEAOEAseptic Non Union
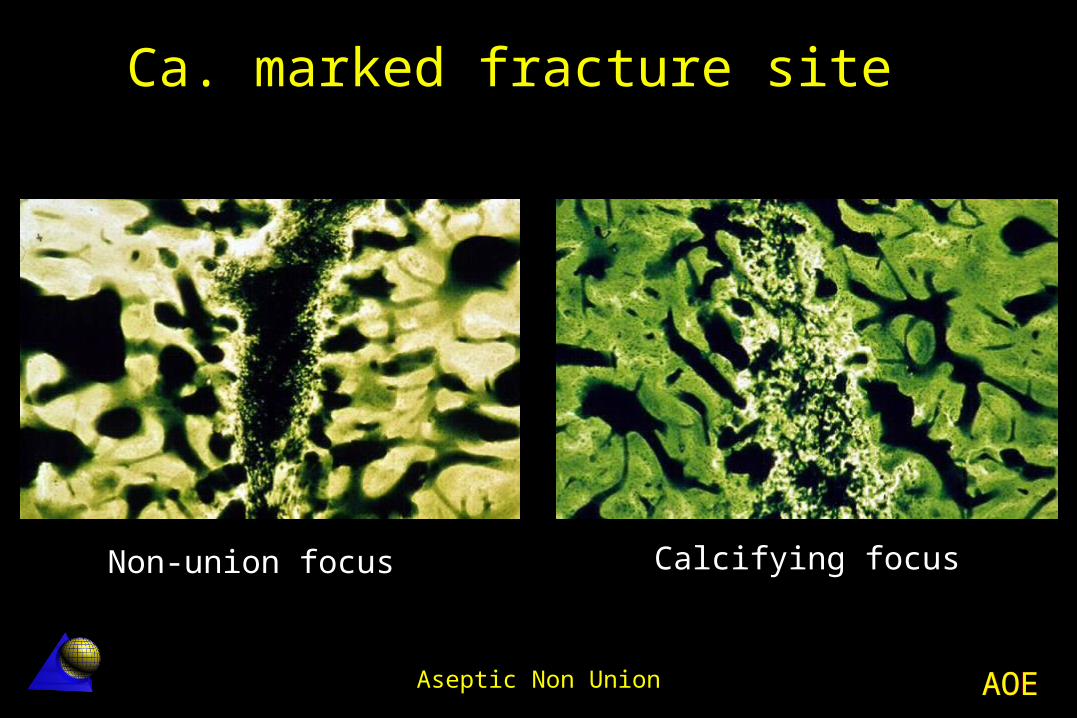
Ca. marked fracture site
Non-union focus Calcifying focus
AOEAOEAseptic Non Union
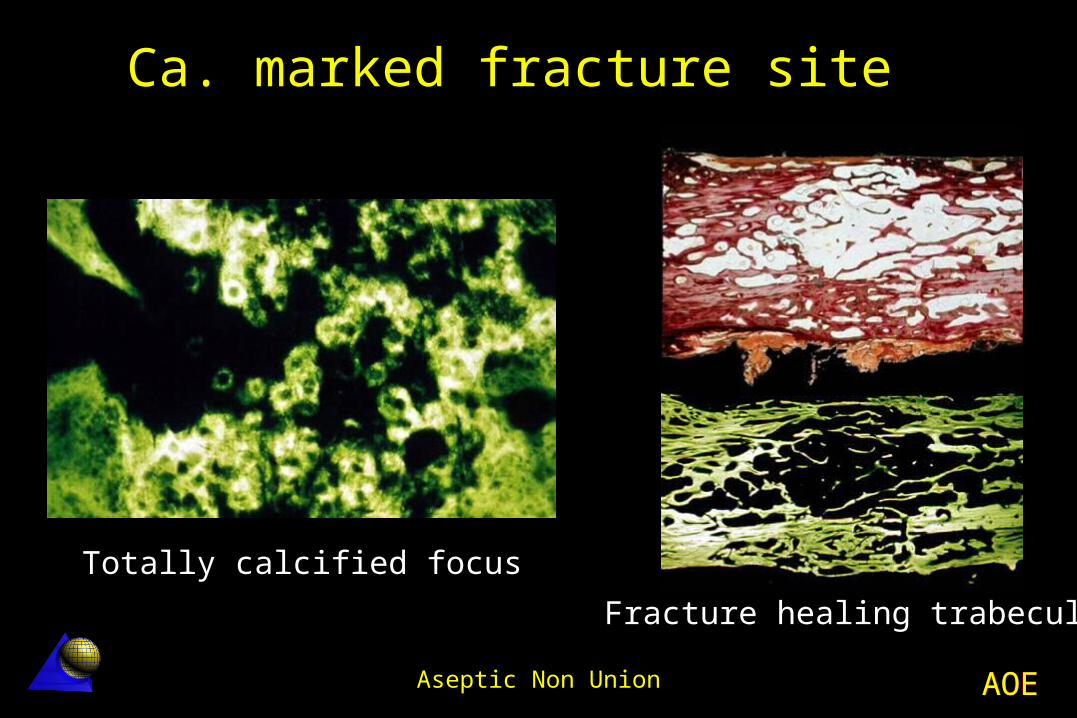
Totally calcified focus
Fracture healing trabeculae
Ca. marked fracture site
AOEAOEAseptic Non Union
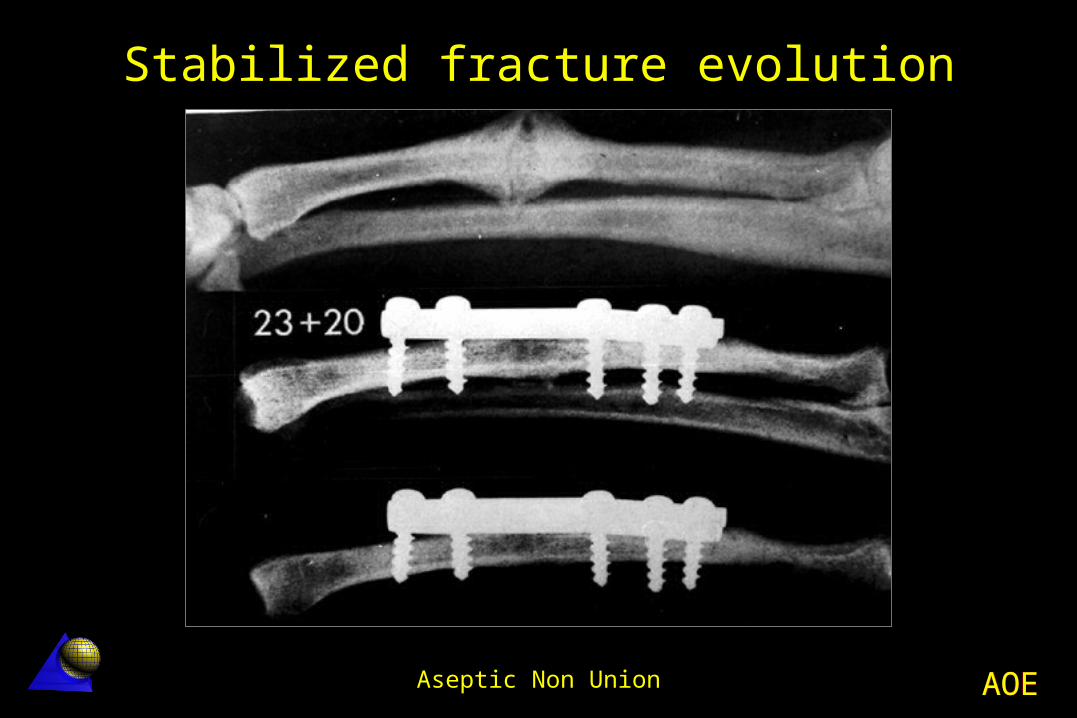
Stabilized fracture evolution Mechanical stability allows the fibrous
cartilage to calcify and finally ossify after vascular penetration.
Resection of an hypertrophic non-union must be regarded as an error.
AOEAOEAseptic Non Union
Stabilized fracture evolution

AOEAOEAseptic Non Union
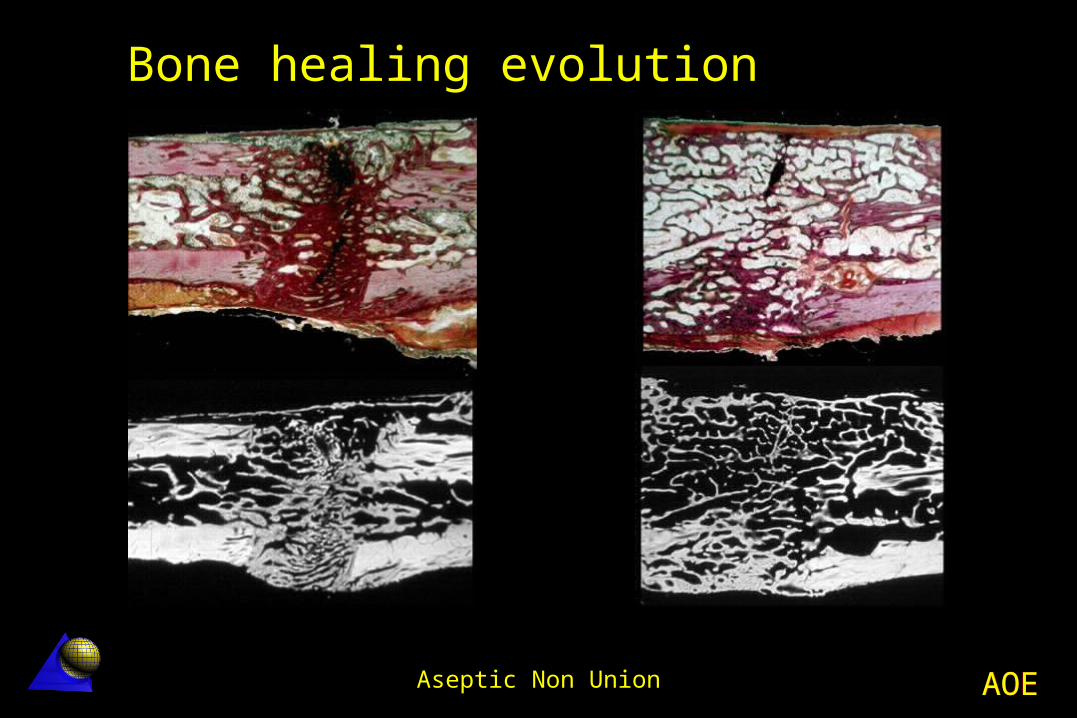
Bone healing evolution
AOEAOEAseptic Non Union
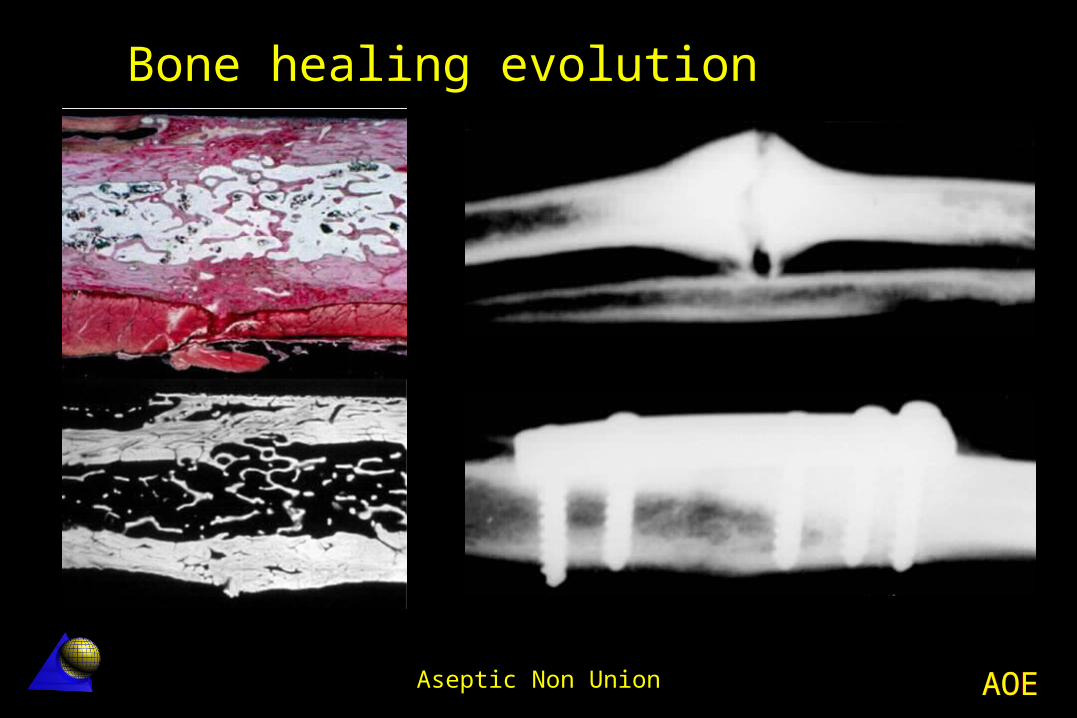
Bone healing evolution
AOEAOEAseptic Non Union
Bone healing evolution

AOEAOEAseptic Non Union
PO
Instability (non-union)
AOEAOEAseptic Non Union
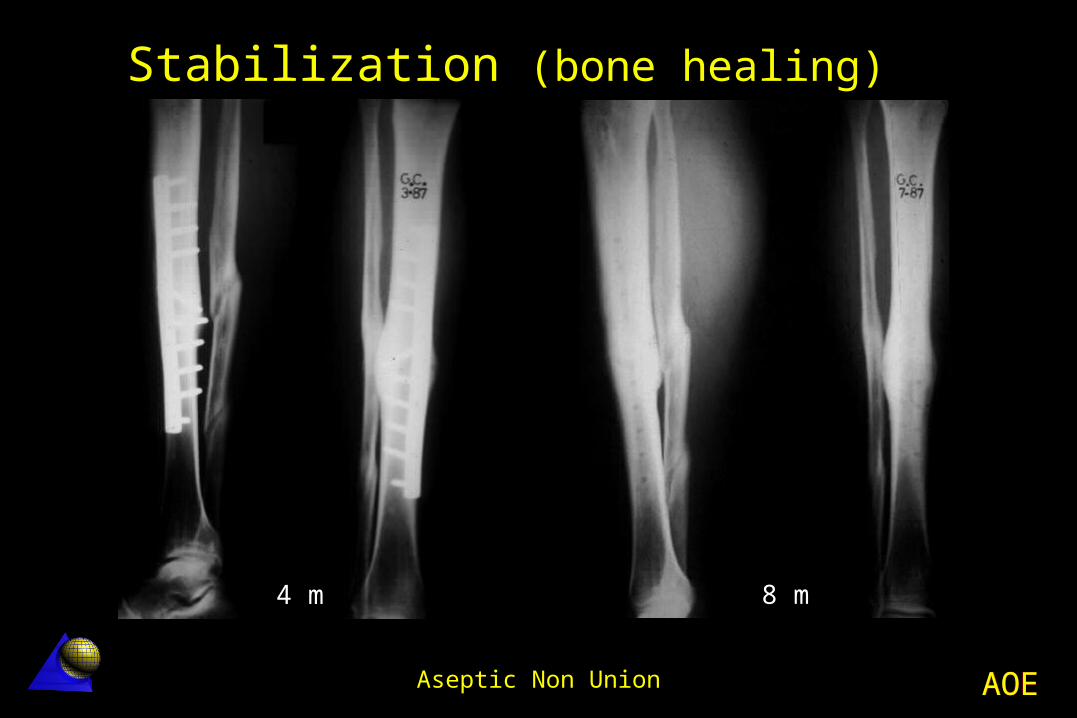
Stabilization (bone healing)
4 m 8 m

AOEAOEAseptic Non Union
“Elephant foot” non-union healed after plating stabilization
AOEAOEAseptic Non Union
B. Avital non-union
I. Dystrophic with intermediate wedge fragment
II. Necrotic with conminution
III. Bone loss
IV. Atrophic
Weber classification
AOEAOEAseptic Non Union
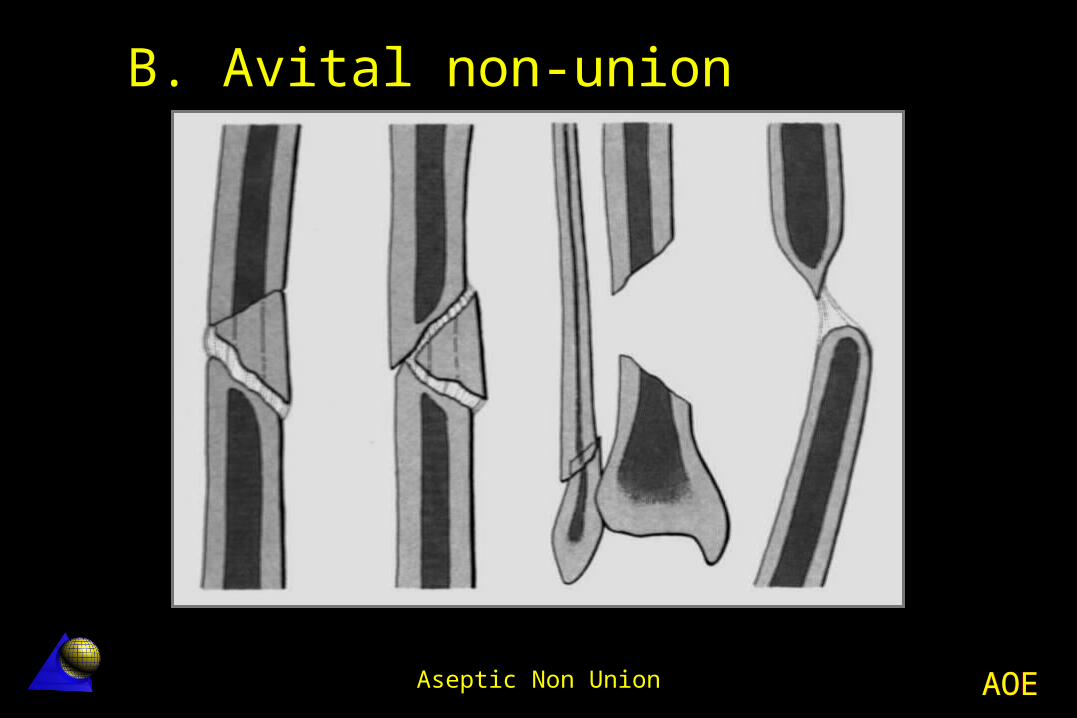
B. Avital non-union
AOEAOEAseptic Non Union
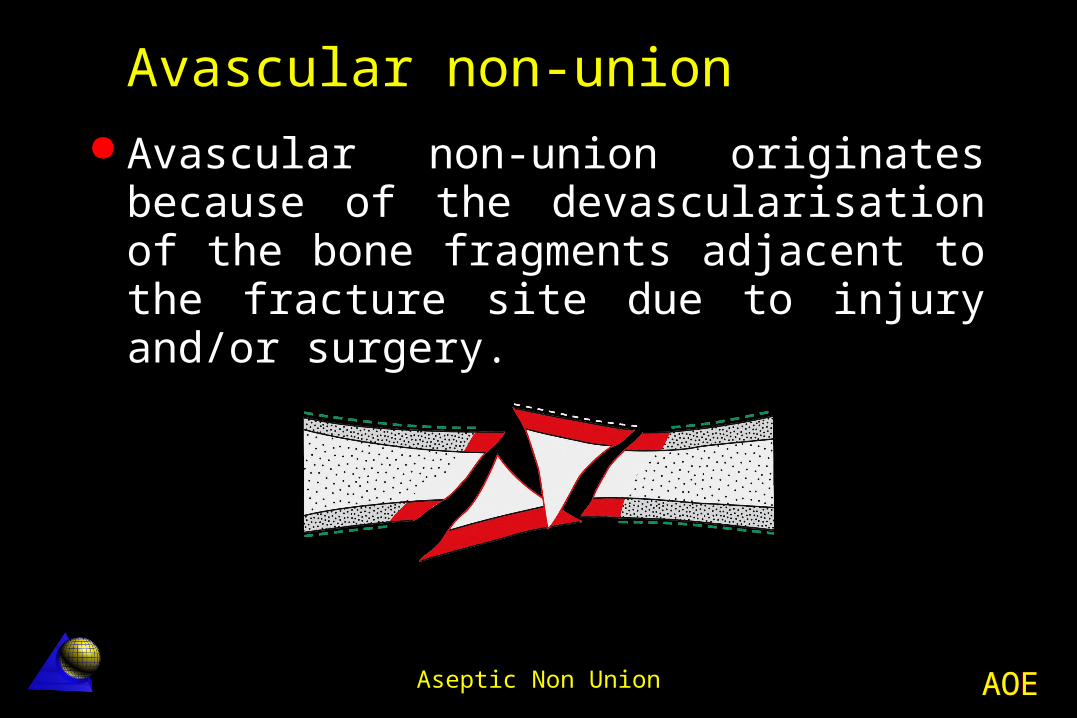
Avascular non-union Avascular non-union originates because
of the devascularisation of the bone fragments adjacent to the fracture site due to injury and/or surgery.
AOEAOEAseptic Non Union
Devitalized fragments united by callus to the main fragments without evidence of bone healing
B. Avital non-union
AOEAOEAseptic Non Union
Treatment of aseptic non-union
AOEAOEAseptic Non Union
To achieve a rapid bone healing with complete recovery of articular and muscular function.
Goal of the treatment
AOEAOEAseptic Non Union
To restore bone continuity If possible anatomically
To restore articular and muscular function
In the less possible time
Active treatment
AOEAOEAseptic Non Union
1. Vital Mechanical stabilization (osteosynthesis) Stable osteosynthesis
2. Avital Mechanical stabilization (osteosynthesis) Biological stimulation (autologous bone
grafting)
Treatment according to the type
AOEAOEAseptic Non Union
1. Pediculated vital bone grafts (decortication)
2. Autologous cancellous bone graft3. Bone transplants
Bone grafting
Fibula “pro tibia”Bone transportVascularised bone grafts
Bone loss
AOEAOEAseptic Non Union
Techniques for bone reconstruction
Diaphyseal non-union
AOEAOEAseptic Non Union
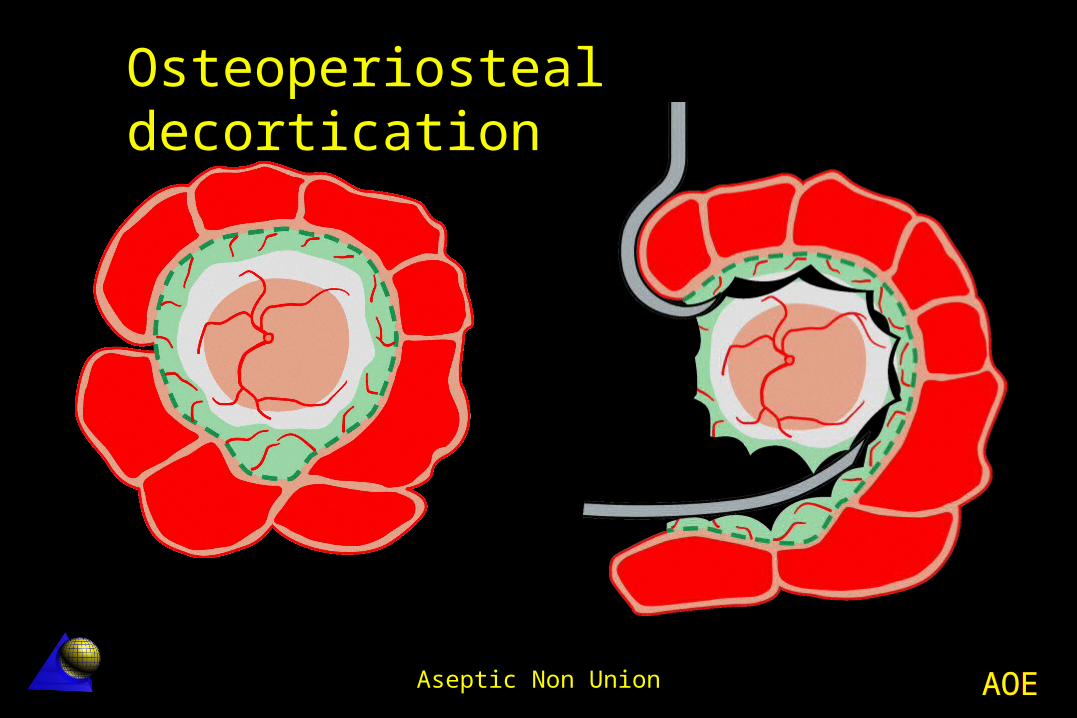
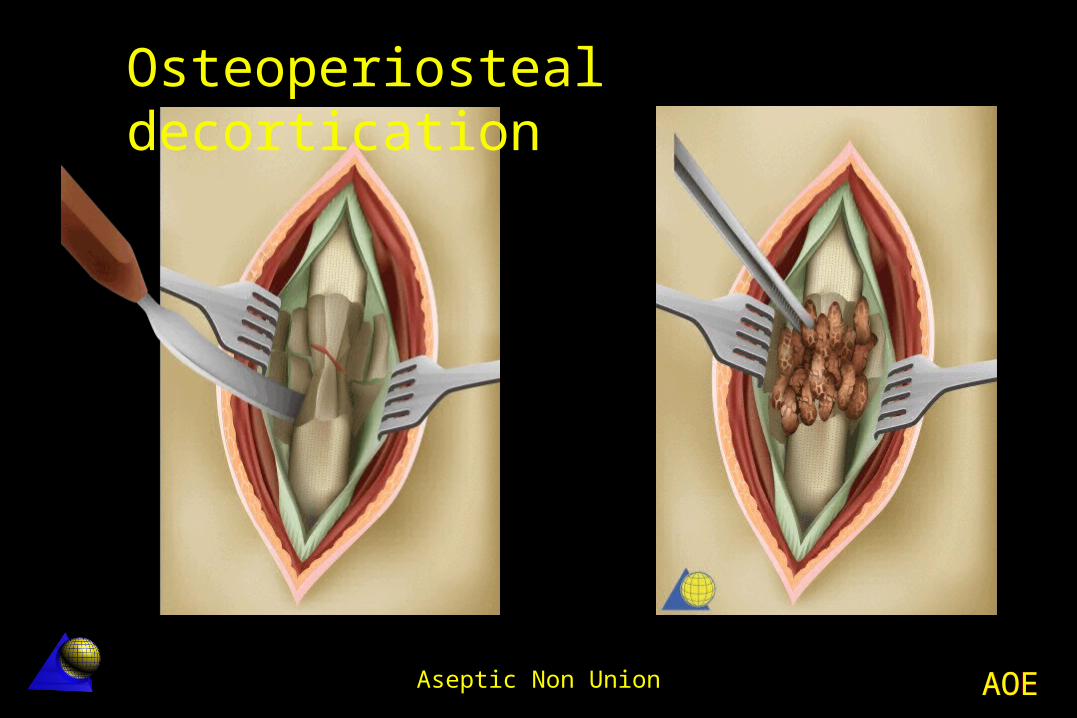
It is the simplest and most effective way to expose a non union without producing a substantial devascularization.
Judet osteoperiosteal decortication
This technique is used to enhance the healing response, creating a well vascularised that at the same time stimulates the bone healing process.
AOEAOEAseptic Non Union
Osteoperiosteal decortication
AOEAOEAseptic Non Union
Osteoperiosteal decortication
AOEAOEAseptic Non Union
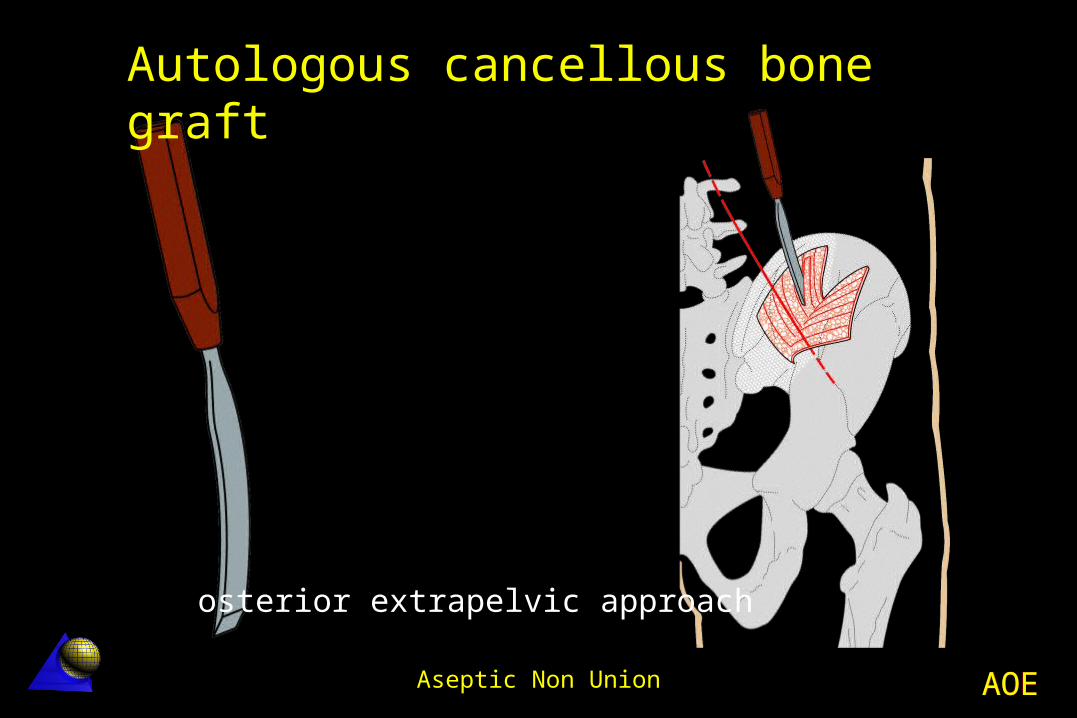
Cancellous autologous bone graft is the “gold standard” for both biological and mechanical purposes.
Autologous cancellous bone graft
It is osteogenic (a source of vital bone cells) It is osteoinductive (recruitment of local mesenchymal cells) It is osteoconductive (scaffold for ingrowth of new bone)
AOEAOEAseptic Non Union
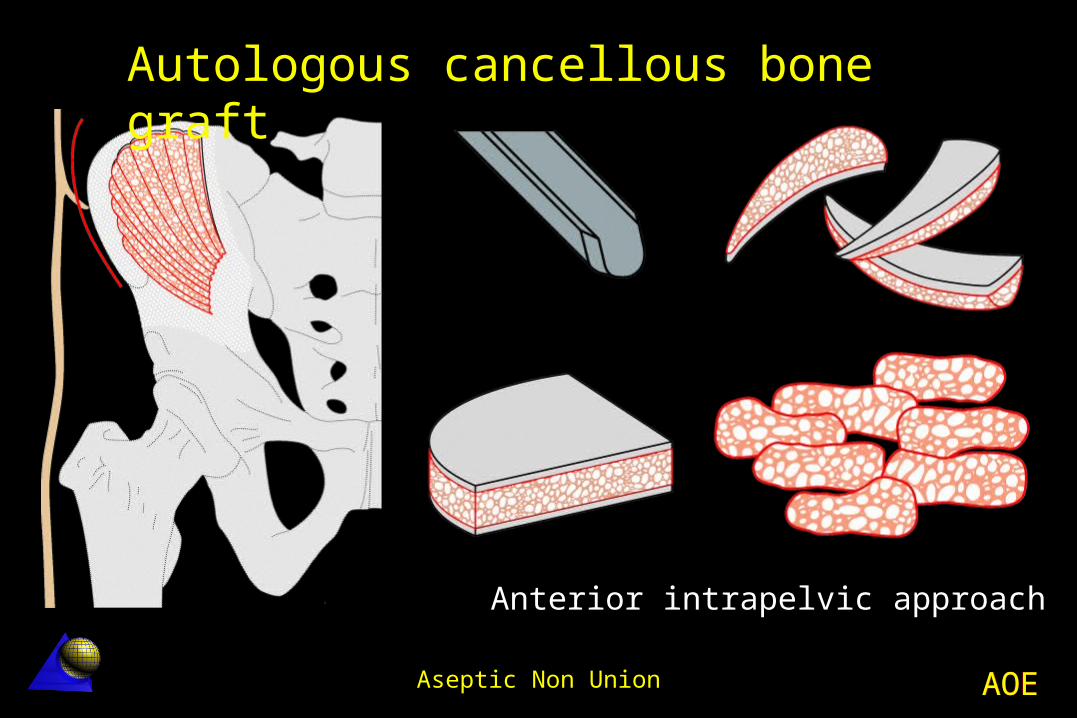
Anterior intrapelvic approach
Autologous cancellous bone graft
AOEAOEAseptic Non Union
Posterior extrapelvic approach
Autologous cancellous bone graft
AOEAOEAseptic Non Union
Poor vascularization Minimal callus formation Atrophic non-union
Cancellous autologous bone graft is: Osteogenic, osteoinductive and osteoconductive
Bone grafting indications
AOEAOEAseptic Non Union
Allografts and bone substitutes such as demineralized bone matrix, hidroxyapatite, tricalcium-phosphate, as welll as osteoinductive substances such as growth factors, bone morphogenetic proteins (BMPs), etc., are currently being intensively explored both experimentally and clinically, but have not yet proved to be significantly superior.
Allografts and bone graft substitutes
AOEAOEAseptic Non Union
All these substances require a vital environment in order to be effective.
In the absence of living cellular elements and blood supply there is no possibility of any healing.
Nothing is superior to autologous bone graft
Allografts and bone graft substitutes
AOEAOEAseptic Non Union
Osteogenesis by callus distraction (Ilizarov) and free vascularized bone graft should be taken into consideration when dealing with large (>4-6 cm) segmental bone defects.
Callus distractionFree vascularized bone grafts
AOEAOEAseptic Non Union
¡Mechanical stabilization is essential!
AOEAOEAseptic Non Union
Stabilization of a non-union provides the essential mechanical component to allow calcification of the fibrous cartilage within the non-union.
This prepares the field for development of a first bony bridge.
Stabilization
AOEAOEAseptic Non Union
Plating Intramedullary nailing External Fixation
Types of stabilization
AOEAOEAseptic Non Union
Plating The plate is probably the most adequate and
versatile tool for the stabilization of an aseptic non-union.
It allows in a single procedure : Interfragmentary compression Correction of any malposition Reconstructive measures (grafting
etc.)
AOEAOEAseptic Non Union
Plating techniques Tension band plating (on the convexity) Axial compression plating Buttress plate Lag screws and neutralization plate Bridge plate in segmental bone loss
AOEAOEAseptic Non Union
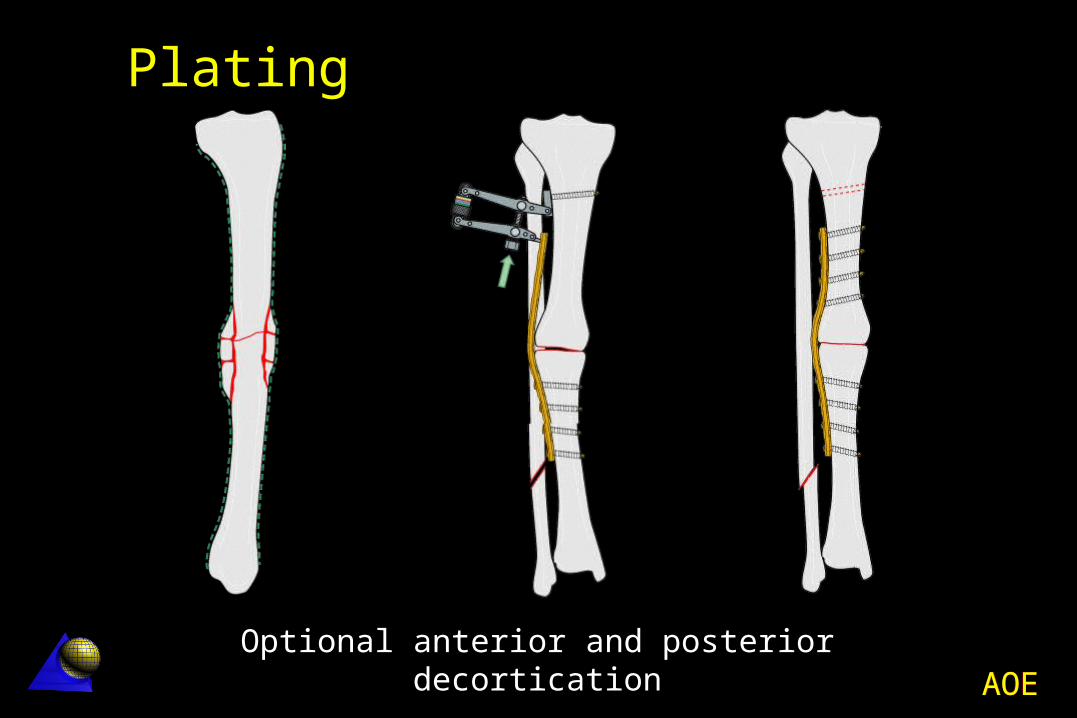
Plating
Optional anterior and posterior decortication
AOEAOEAseptic Non Union
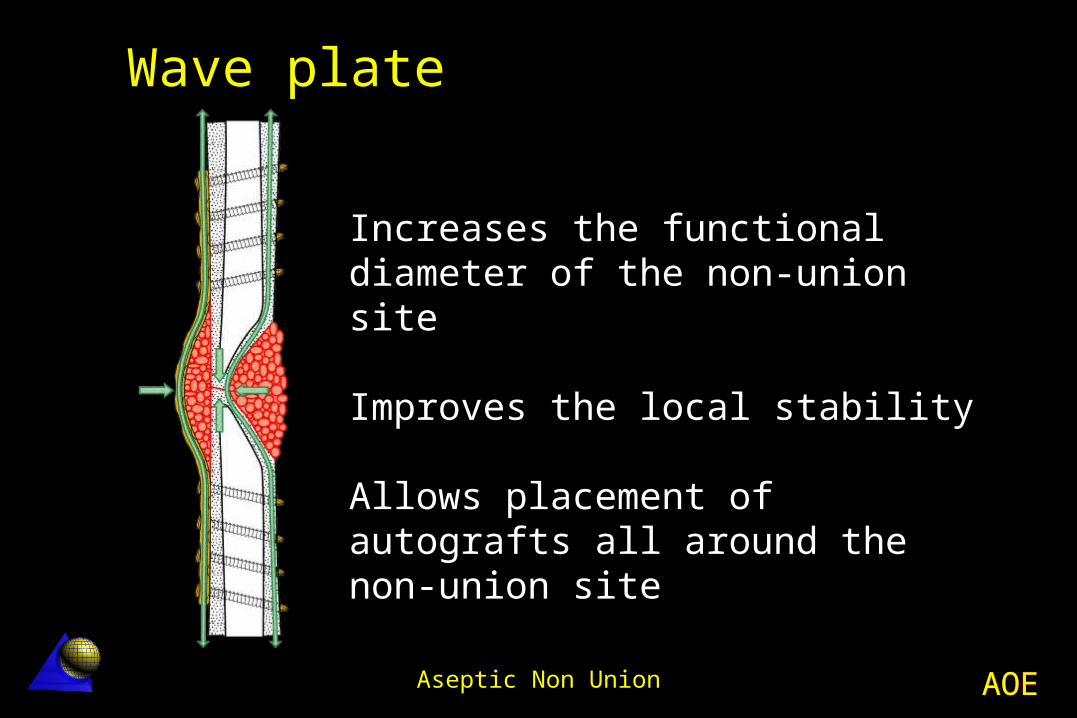
Wave plate
Increases the functional diameter of the non-union site
Improves the local stability
Allows placement of autografts all around the non-union site
AOEAOEAseptic Non Union
It is mainly indicated in diaphyseal non-unions of the lower extremity
Nailing has few advantages in the upper extremity and thin unreamed nails are not suitable, as they provide insufficient stability.
Intramedullary nailing
AOEAOEAseptic Non Union
Indications of intramedullary nailing Non displaced mid third femur and tibia
non-union Loose or broken nail
Over-ream not exposing the non-union site Introduction of a thicker and longer nail Dynamic interlocking (rotational stability) Increase of periosteal bone flow promotes union
AOEAOEAseptic Non Union
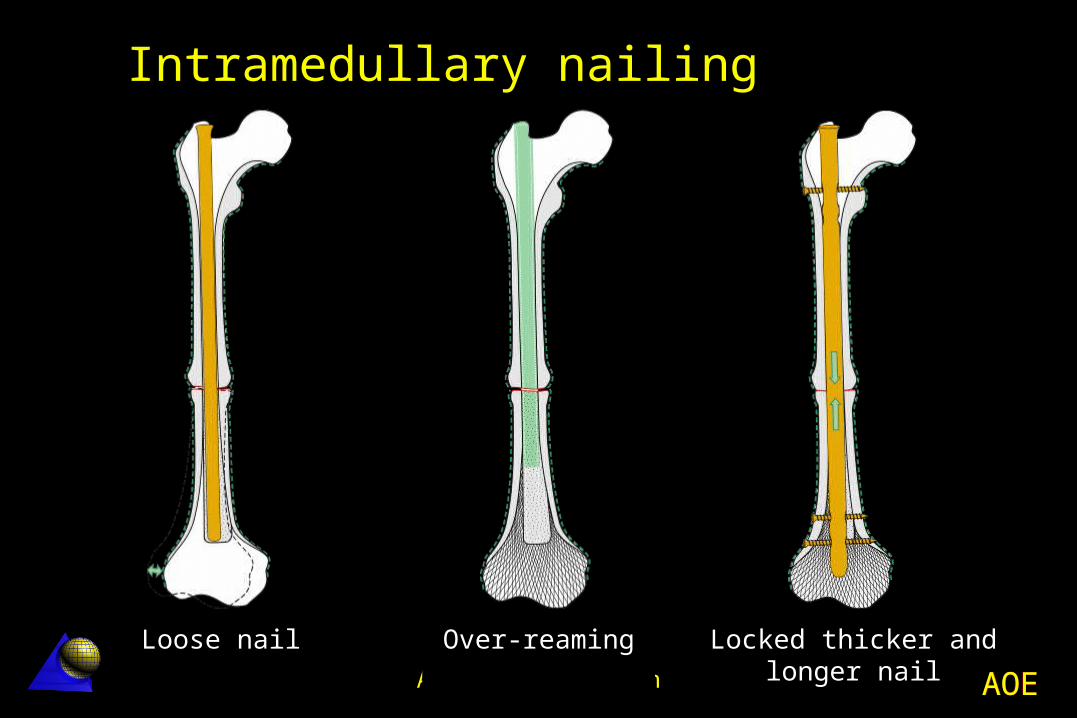
Loose nail Over-reaming Locked thicker and longer nail
Intramedullary nailing
AOEAOEAseptic Non Union
In most aseptic non-unions external fixation brings little advantage.
It may be applied in the presence of poor soft-tissue conditions or in complex multiplanar deformities near joints where a single-stage correction appears difficult and hazardous.
External Fixation
AOEAOEAseptic Non Union
Tibia non-union Poor skin coverage Suspicion of latent infection
Shortening with bone loss Callus distraction technique
Arthrodesis non-union Failed knee and ankle arthrodesis
Indications of External Fixation
AOEAOEAseptic Non Union
Bone reconstruction techniques
Methaphyseal non-union
AOEAOEAseptic Non Union
Limited local decortication avoiding devascularization of the joint fragment, correction of the deformities and mechanical adaptation of the main fragments with fixation by interfragmentary compression.
Usually one or two plates are used.
Bone grafting may be necessary.
Metaphyseal non-union
AOEAOEAseptic Non Union
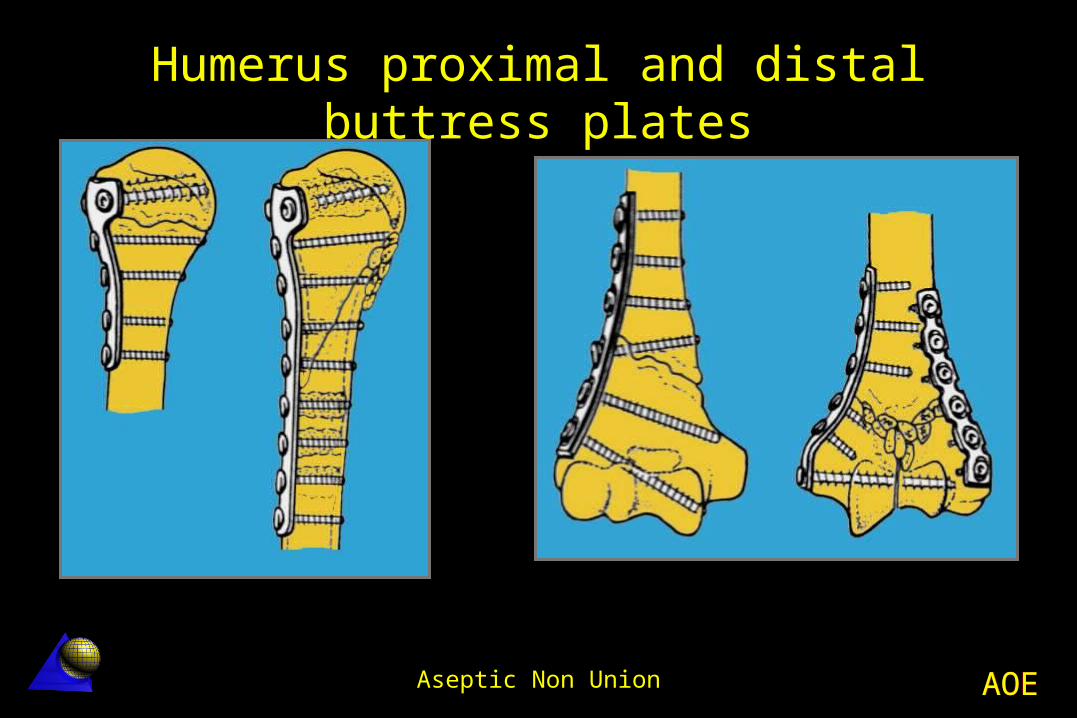
Indications Correct alignment of the articular
surfaces Articular fragment stable fixation
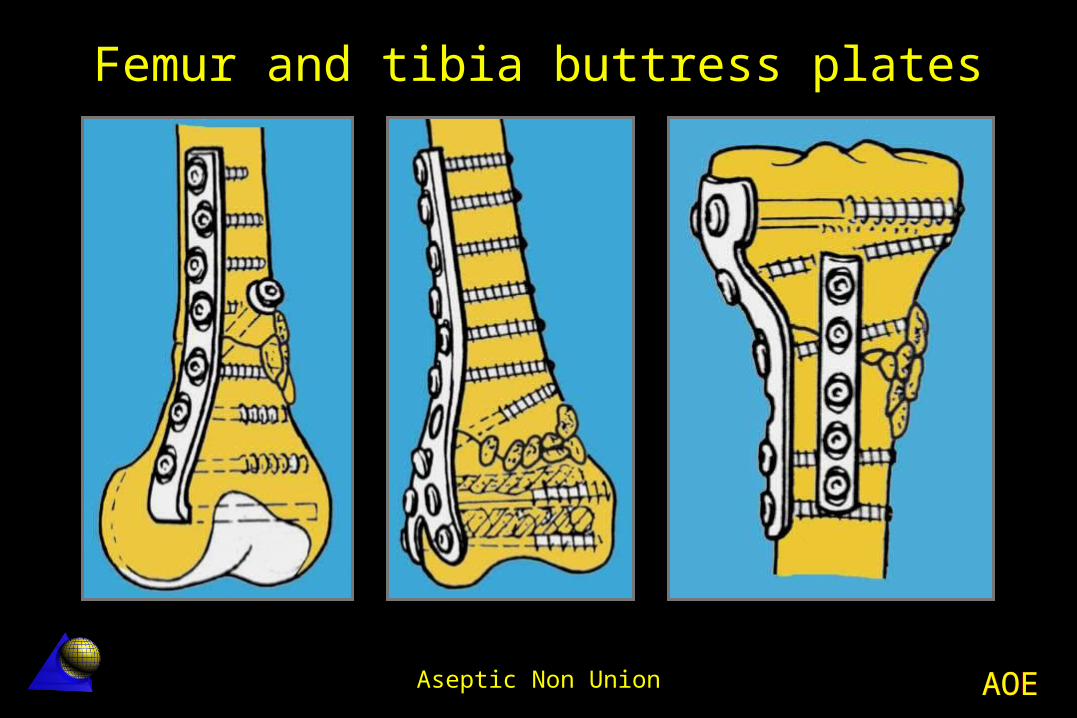
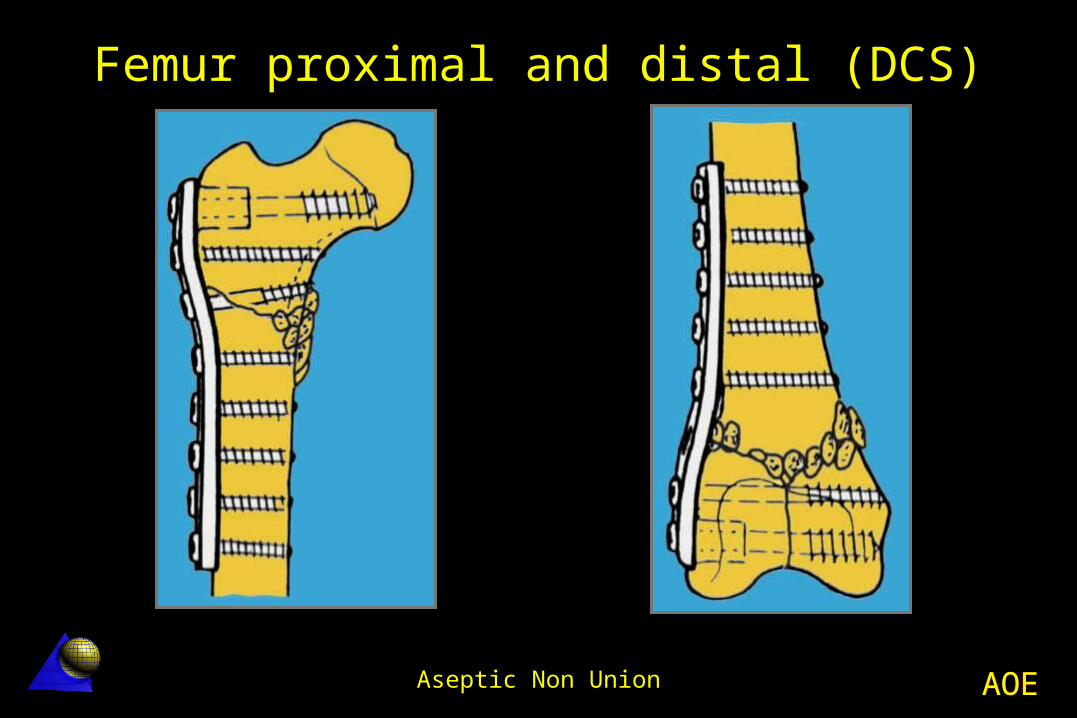
Angle plate Buttress plate
Active mobilization of a stiff joint Avoid forced mobilization before bone
healing
AOEAOEAseptic Non Union
Humerus proximal and distal buttress plates
AOEAOEAseptic Non Union
Femur and tibia buttress plates
AOEAOEAseptic Non Union
Femur proximal and distal (DCS)
AOEAOEAseptic Non Union
Adjuvant treatment
AOEAOEAseptic Non Union
Electromagnetic stimulation and, more recently, ultrasound, have been applied and advocated to stimulate bone healing.
They do appear to generate a certain physical (thermal) effect at the non-union site, but the final outcome is still questionable and real evidence is lacking.
Aseptic non-union
AOEAOEAseptic Non Union
Bone losses
AOEAOEAseptic Non Union
Bone transplant
1. Fibula “pro tibia”2. Bone transport3. Free vascularized bone grafts
AOEAOEAseptic Non Union
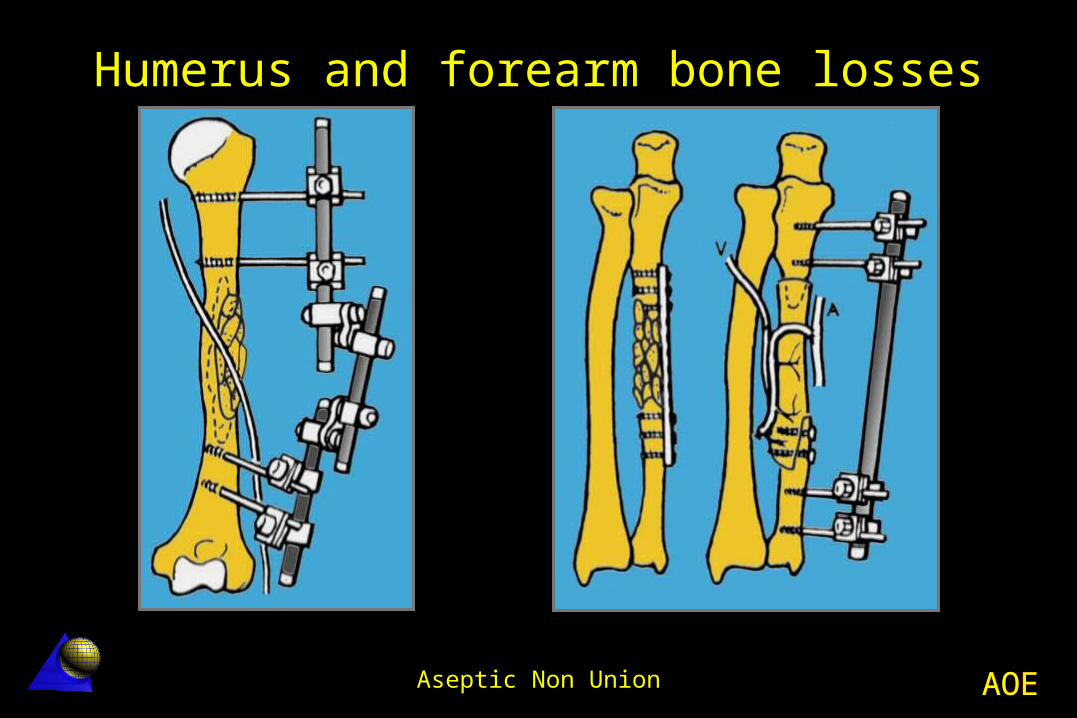
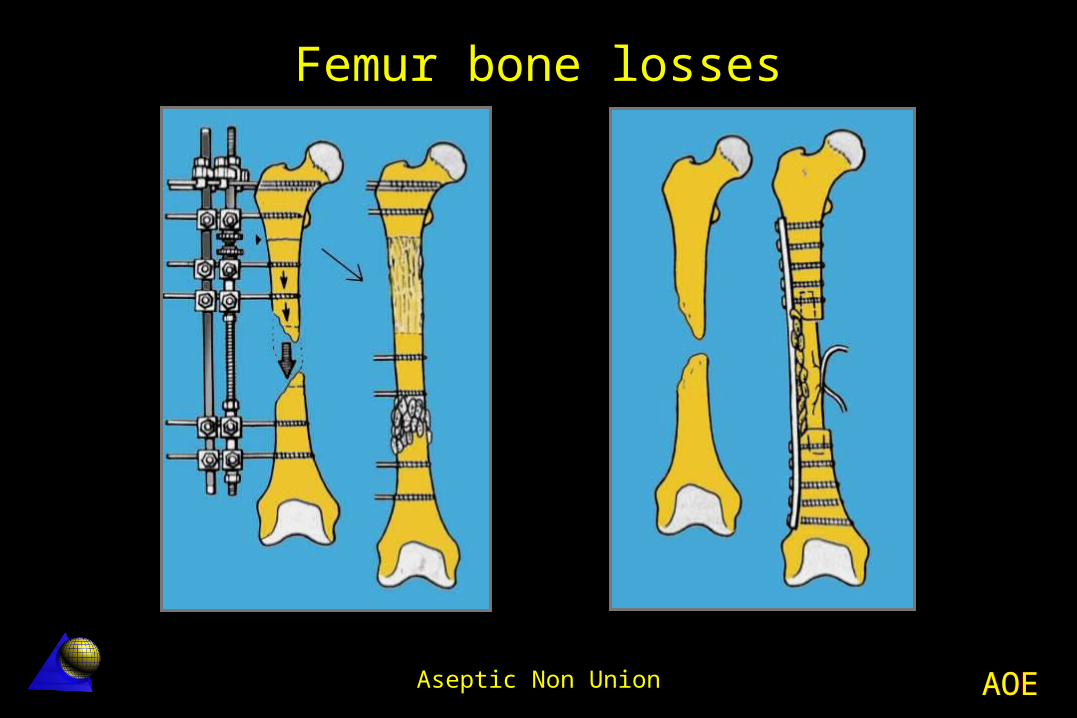
Bone losses (bridging techniques) Bridge plate
External Fixator Locked intramedullary nailing
Plus bone grafting Cortico-cancellousVascularized
AOEAOEAseptic Non Union
Humerus and forearm bone losses
AOEAOEAseptic Non Union
Femur bone losses
AOEAOEAseptic Non Union
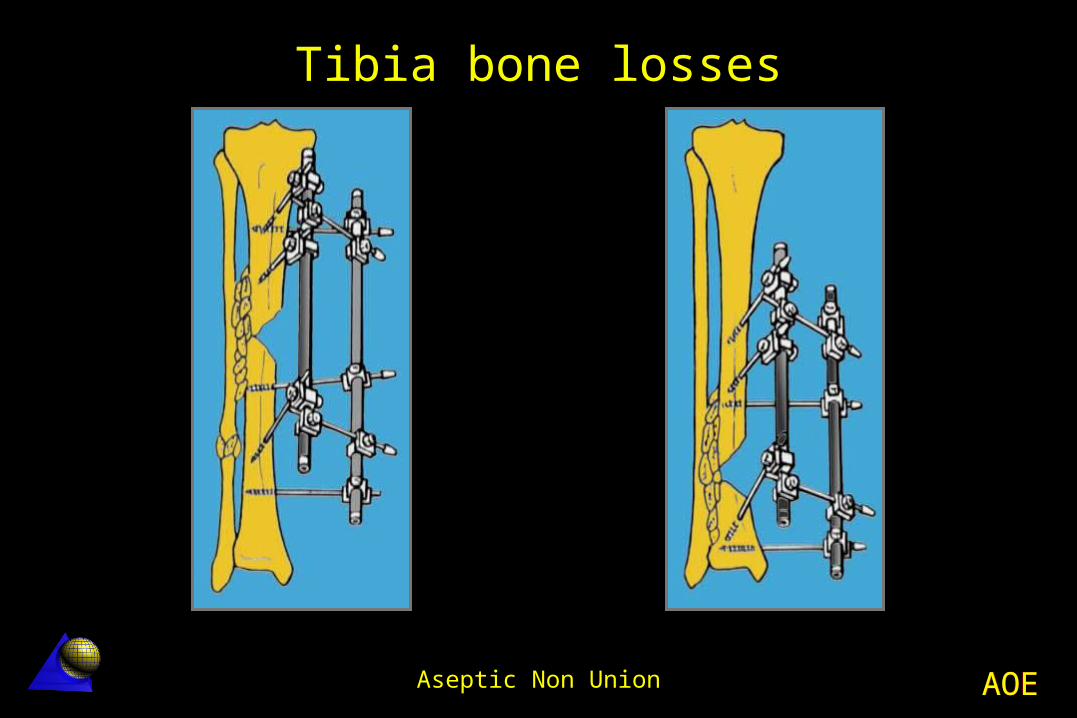
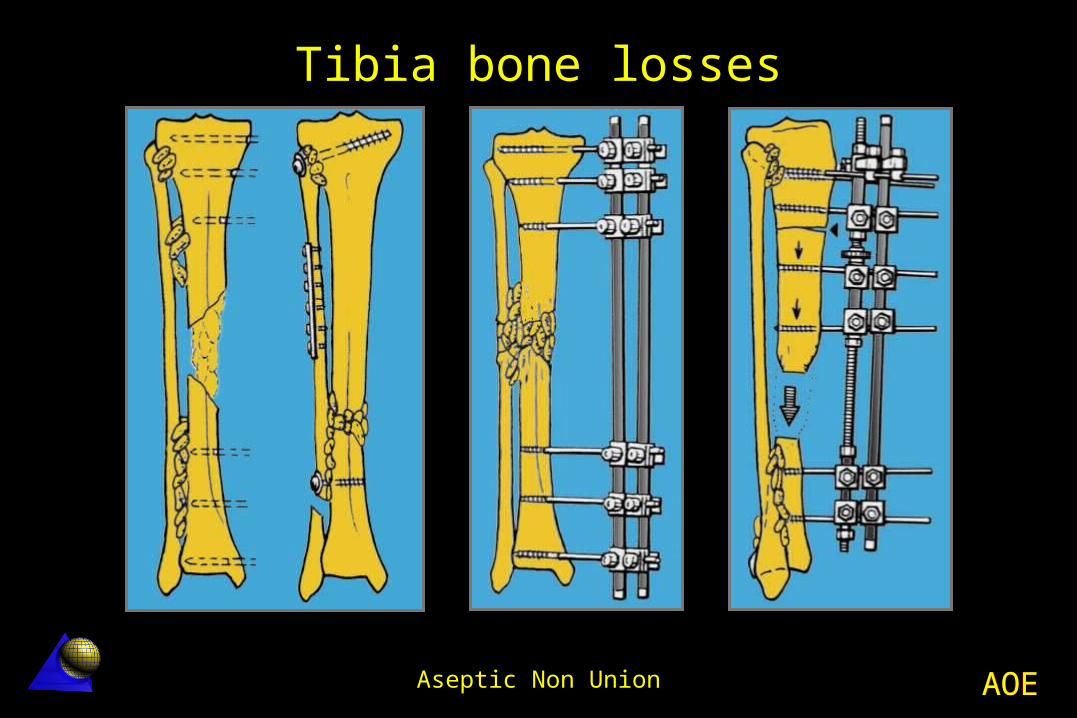
Tibia bone losses
Tibio fibular synostosis Fibula “pro tibia” Bone transport
Plus inter tibio-fibular grafting
AOEAOEAseptic Non Union
Tibia bone losses
AOEAOEAseptic Non Union
Tibia bone losses
AOEAOEAseptic Non Union
Aseptic Non-union Clinical Examples
AOEAOEAseptic Non Union
AO Principles Course
Dr. Enrique Queipo de Llano
Hospital Universitario de Málaga
AOEAOEAseptic Non Union
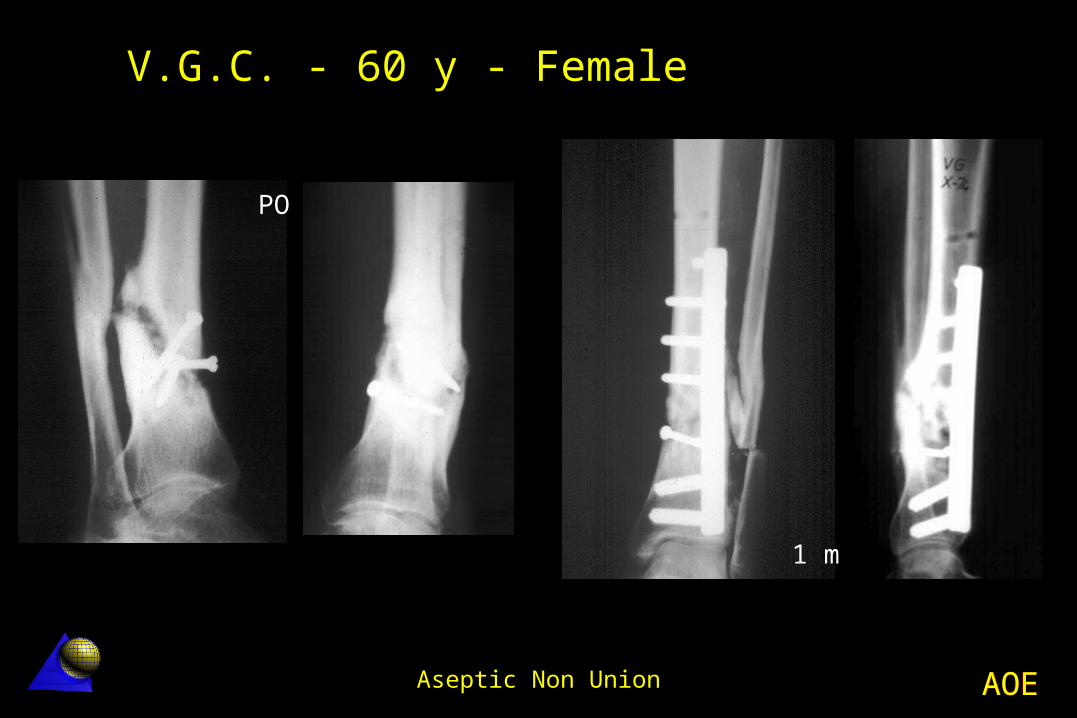
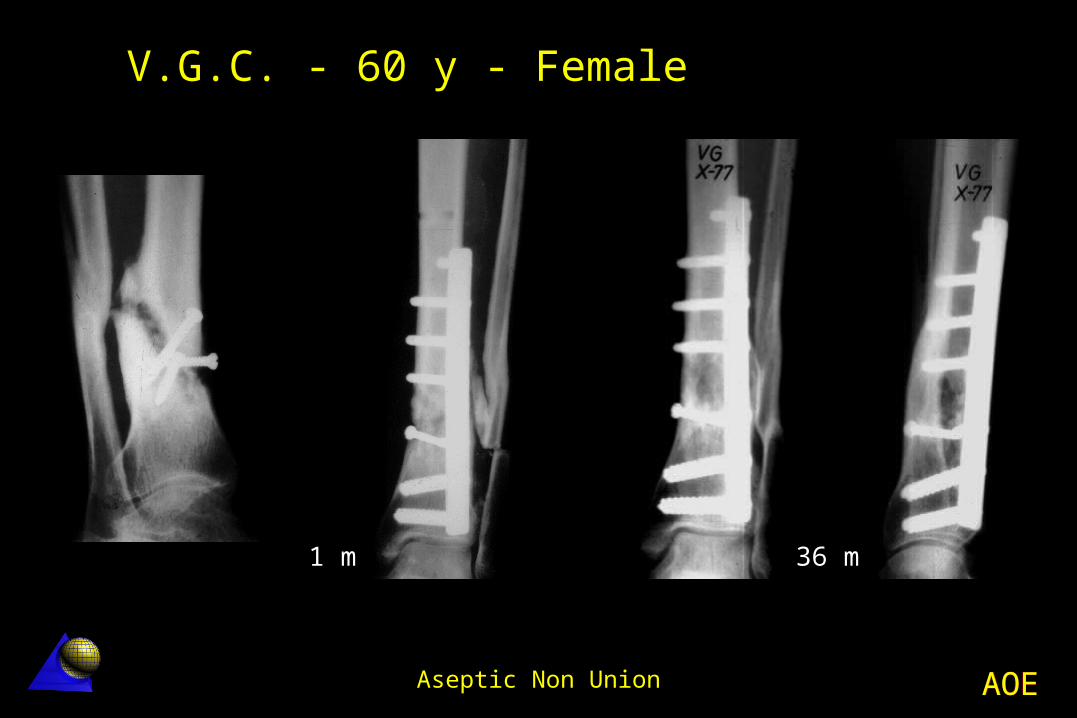
V.G.C. - 60 year old - Female Distal tibia non-union - 10-74
Distal tibia fracture no-union The fracture was treated in other Hospital
Simple screw fixation without IF compression No neutralization plate
Lag screw and DCP plating with deformity correction
Bone healing in 2 months
AOEAOEAseptic Non Union
V.G.C. - 60 y - Female
PO
1 m
AOEAOEAseptic Non Union
1 m 36 m
V.G.C. - 60 y - Female
AOEAOEAseptic Non Union
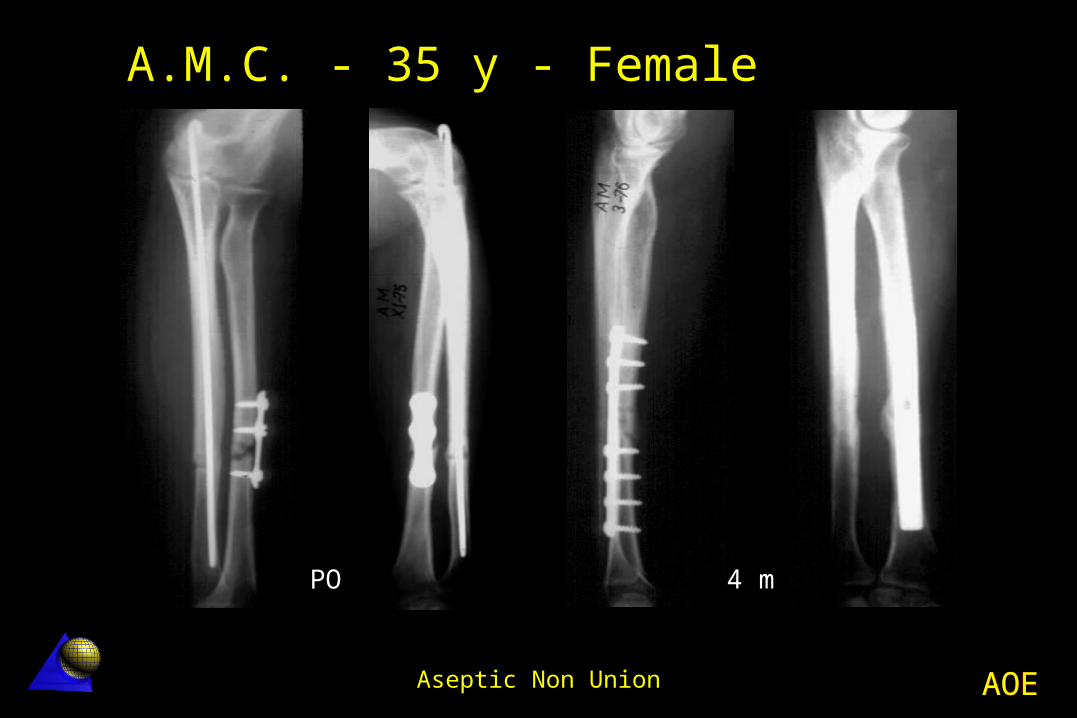
A.M.C. - 35 year old - FemaleRadius non-union - 11.75
Left forearm fracture (radius and ulna) Treated in other Hospital
Ulna nailing Plating of the radius with only three screws
Treatment Ulna nail removal (ulna fx. was healed) Radius DCP compression plating + Bone
grafting Bone healing in 3 months
AOEAOEAseptic Non Union
A.M.C. - 35 y - Female
PO 4 m
AOEAOEAseptic Non Union
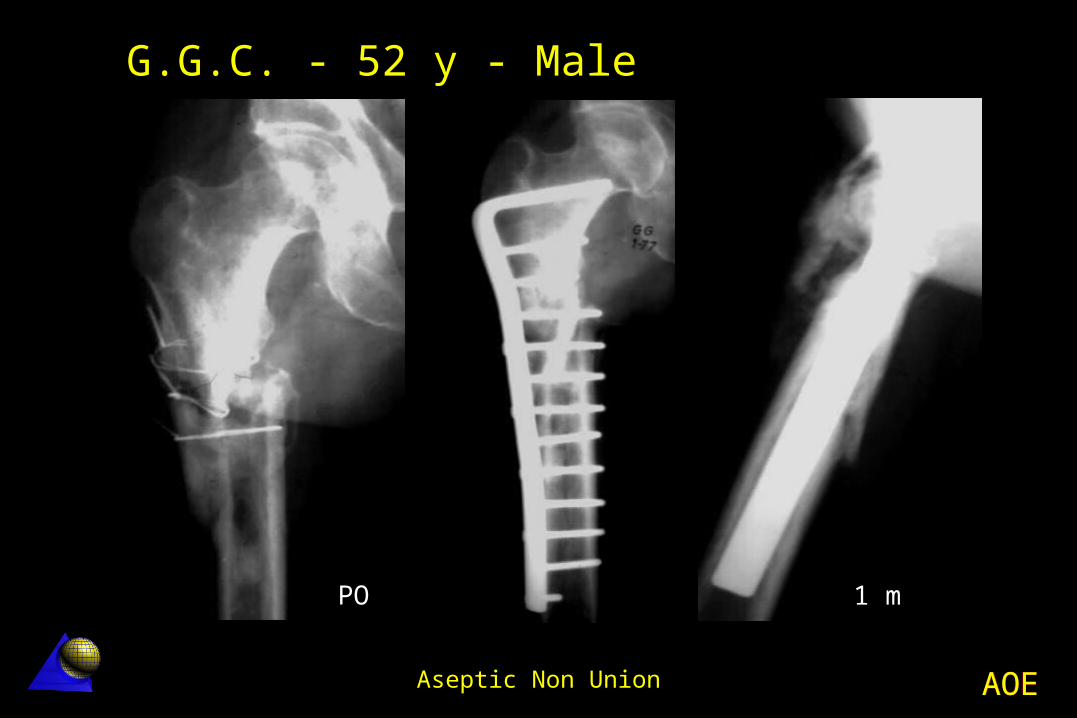
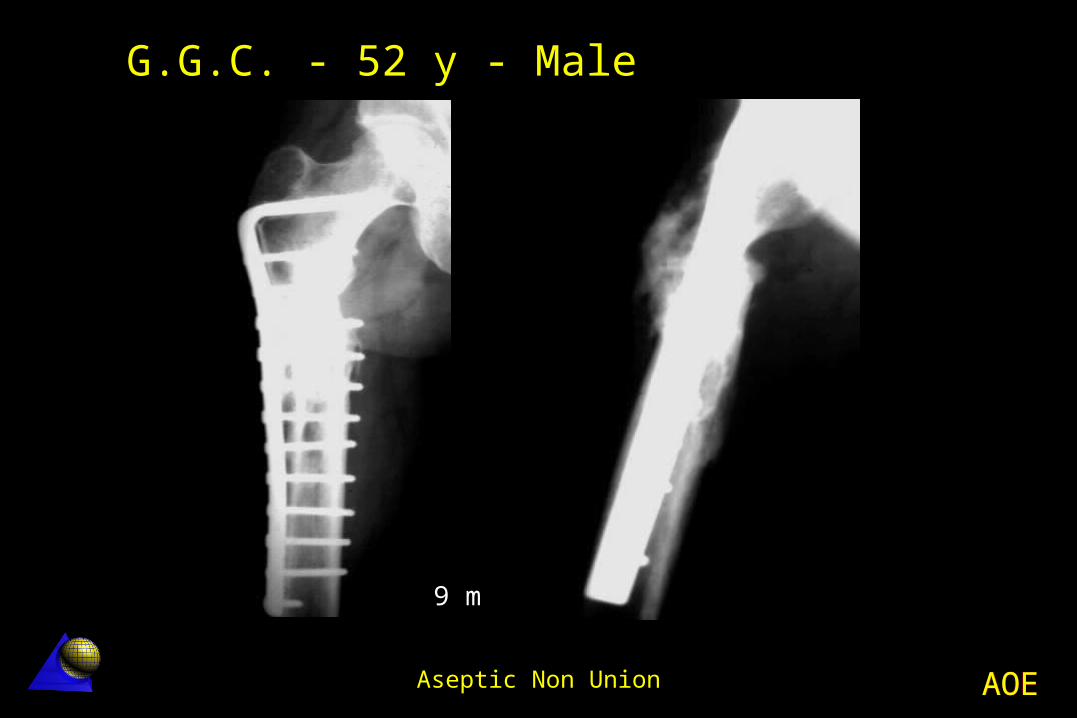
G.G.C. - 52 year old - MaleFemur non-union - 12.76 Sub-trochanteric fracture Incomprehensible wiring cerclage Treatment
Angle plate (95º) with axial compression fixation
Bone grafting Bone healing in 2 months
AOEAOEAseptic Non Union
G.G.C. - 52 y - Male
PO 1 m
AOEAOEAseptic Non Union
9 m
G.G.C. - 52 y - Male
AOEAOEAseptic Non Union
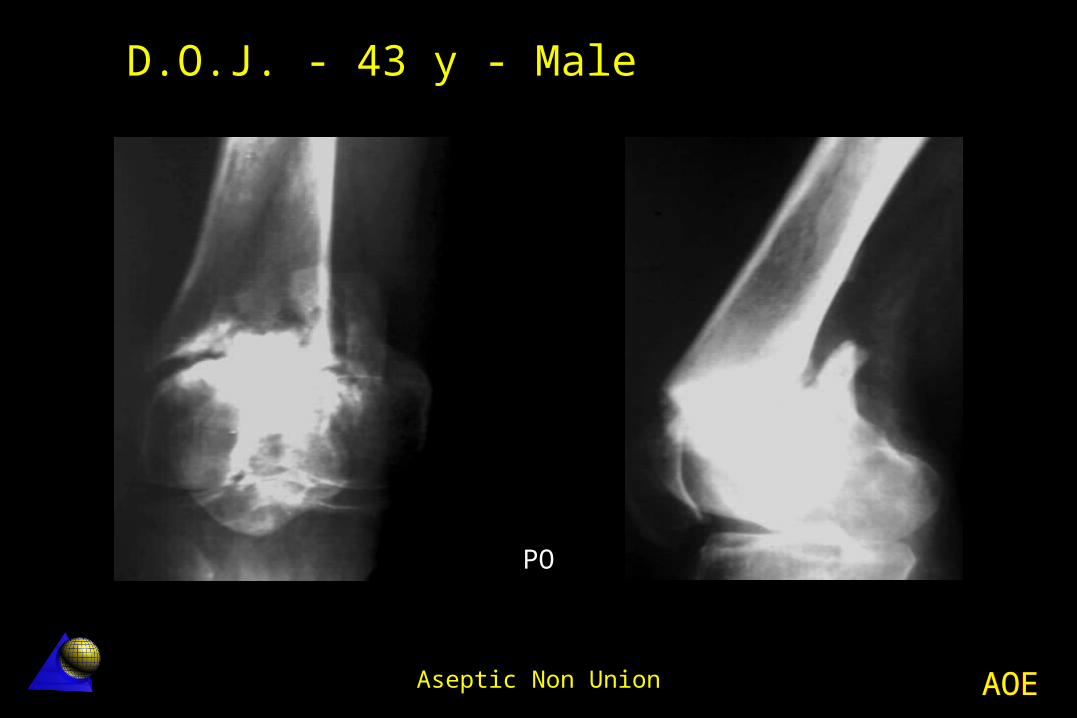
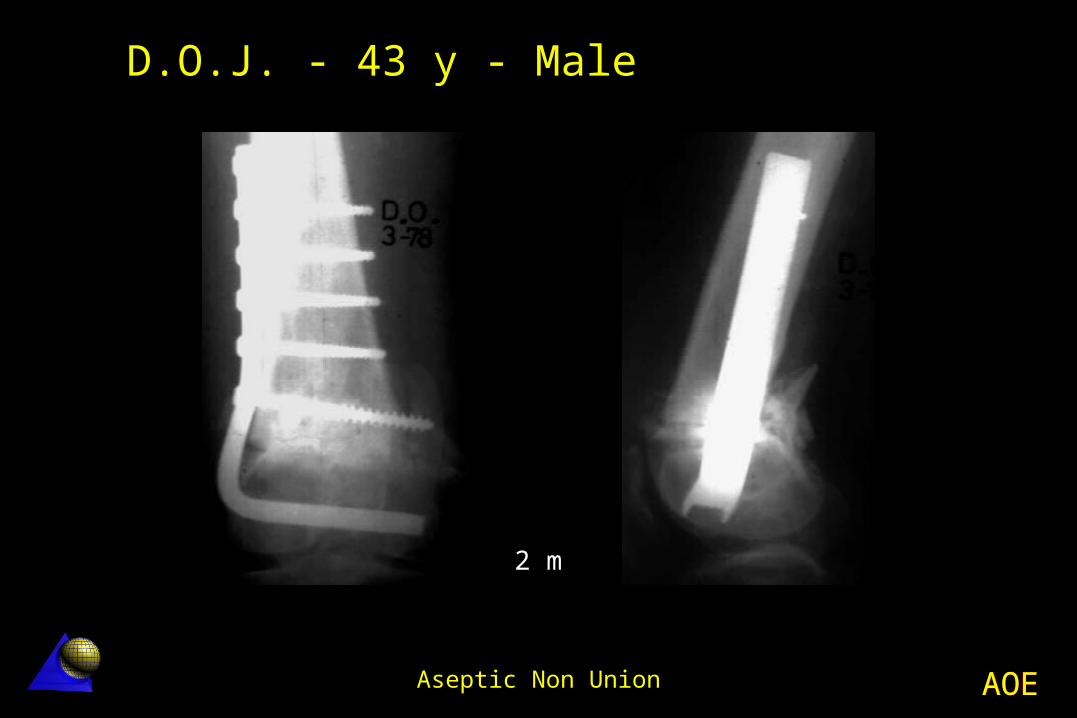
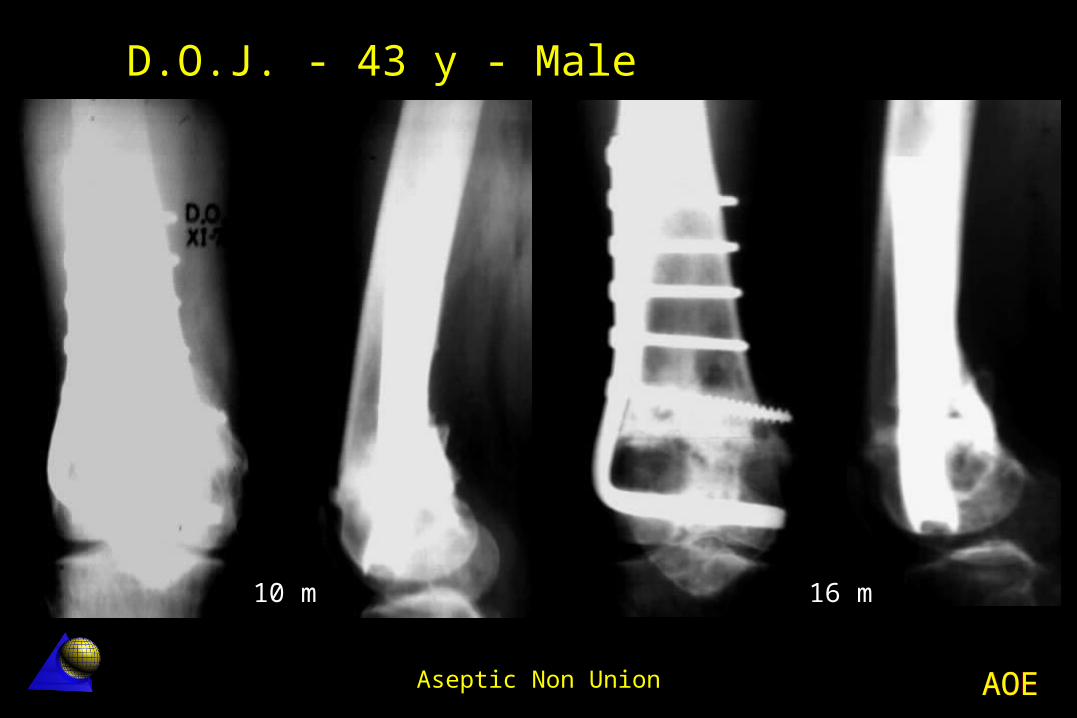
D.O.J. - 43 year old - MaleDistal femur non-union - 1.78 Distal femur metaphyseal non-union Previous orthopaedic treatment in
traction Angle plate (95º) fixation Bone healing in 3 months
AOEAOEAseptic Non Union
D.O.J. - 43 y - Male
PO
AOEAOEAseptic Non Union
2 m
D.O.J. - 43 y - Male
AOEAOEAseptic Non Union
10 m 16 m
D.O.J. - 43 y - Male
AOEAOEAseptic Non Union
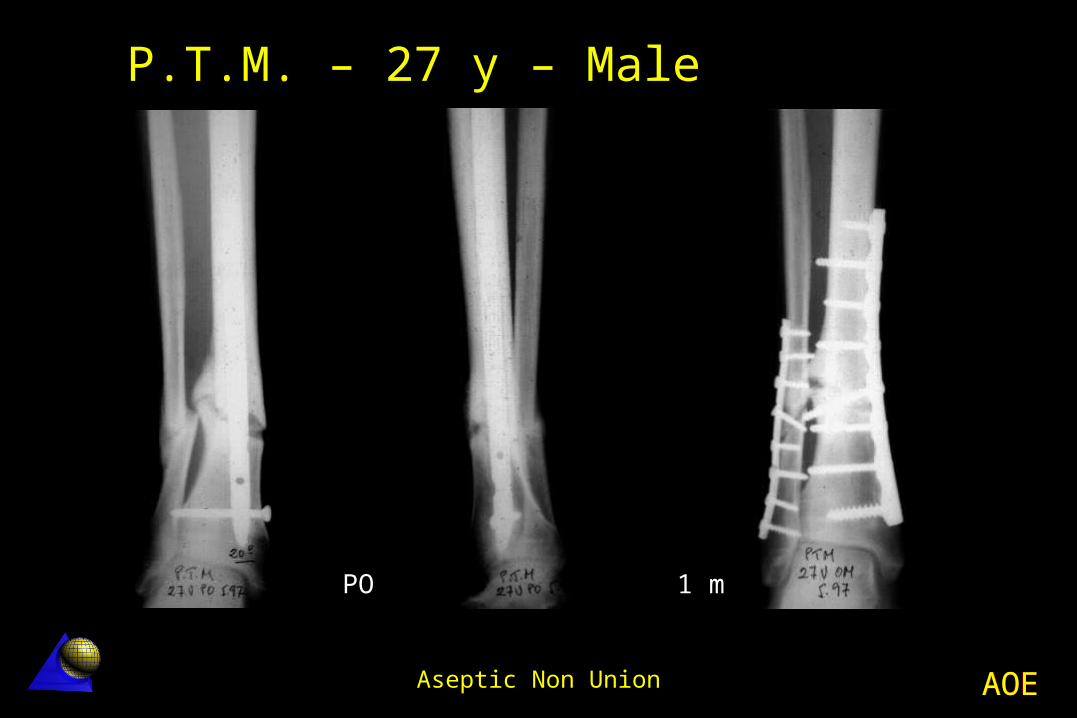
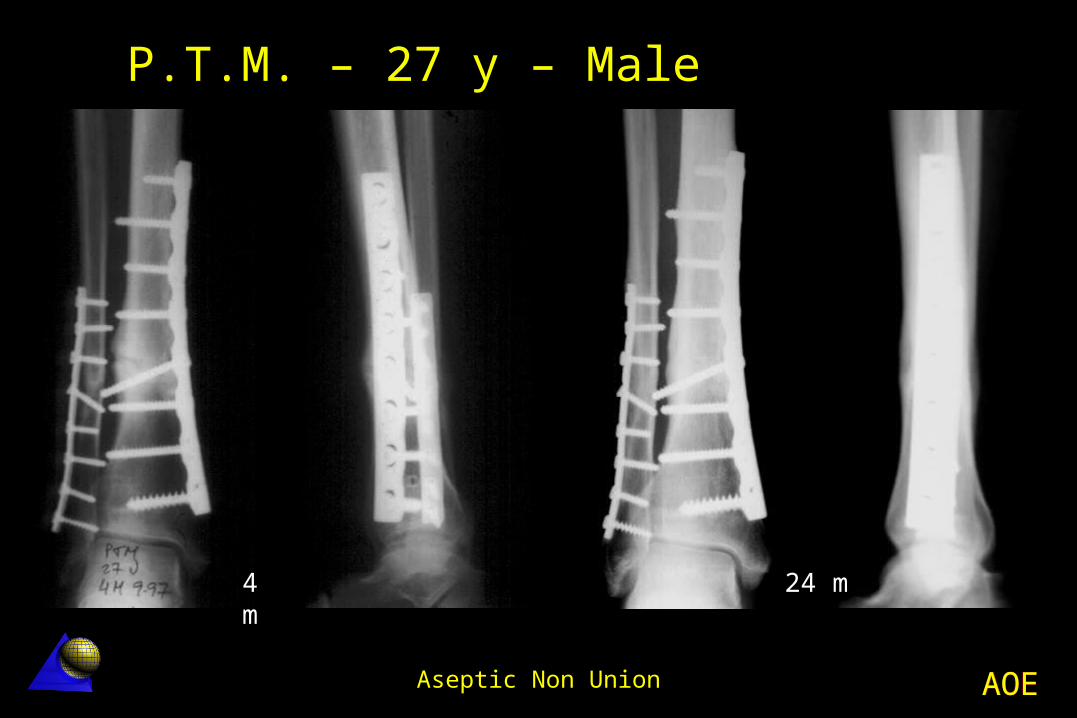
P.T.M. – 27 year old – MaleDistal de tibia non-union - 5.97
Distal de tibia fx. treated in another Hospital UTN nailing Technical defect (only one distal bolt)
Non-union with angular deformity Treatment
Decortication + Osteotomy LC-DCP tibia and fibula plate fixation
Excellent result
AOEAOEAseptic Non Union
P.T.M. – 27 y – Male
PO 1 m
AOEAOEAseptic Non Union
4 m
24 m
P.T.M. – 27 y – Male
AOEAOEAseptic Non Union
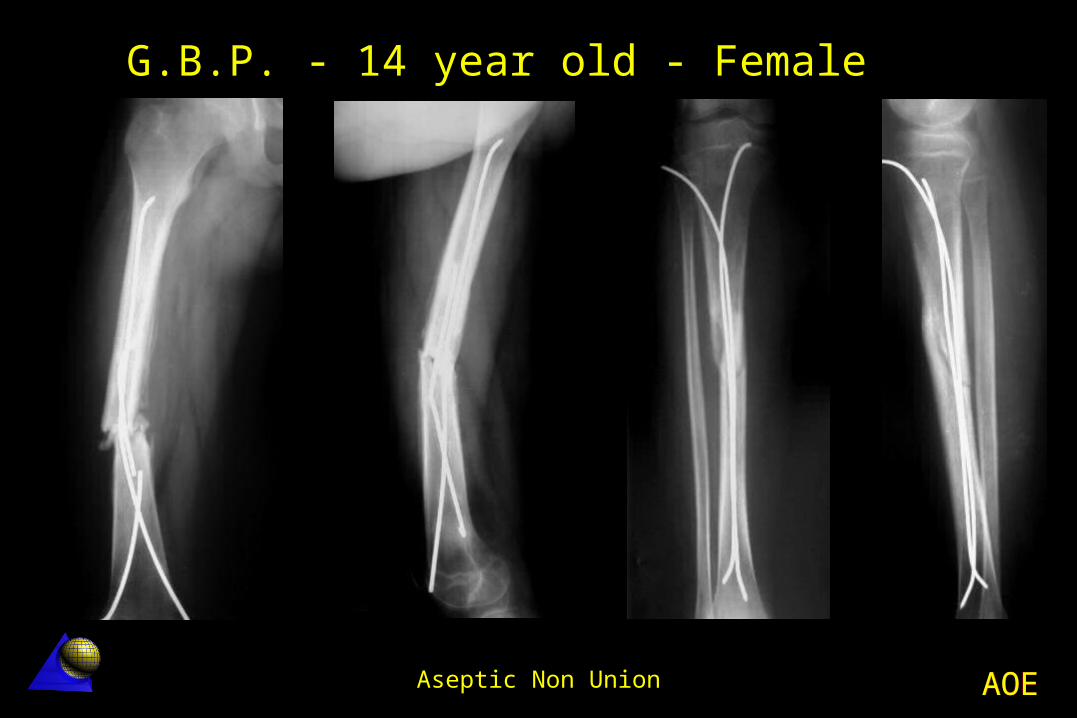
Motorcycle accident (Right femur and tibia fractures)
Treated in another Hospital Kirschner wire nailing of femur and tibia
At 6 months post-op Femur angulation with a broken K wire Femoral non-union Tibia fracture was healed
G.B.P. - 14 year old - FemaleFemur diaphysis non-union - 11.01
AOEAOEAseptic Non Union
Surgical treatment Femur and tibia nails removal Decortication + LC-DCP axial compression
plating Cancellous bone screws were used
(osteoporosis) Autologouu bone grafting
Excellent result at 12 and 24 months
G.B.P. - 14 year old - FemaleFemur diaphysis non-union - 11.01
AOEAOEAseptic Non Union
G.B.P. - 14 year old - Female

AOEAOEAseptic Non Union
0 m 0 m
Tibia healed. Decortication, axial compression plate fixation.
G.B.P. - 14 year old - Female

AOEAOEAseptic Non Union
3 m 6 m
G.B.P. - 14 year old - Female

AOEAOEAseptic Non Union
12 m
G.B.P. - 14 year old - Female

AOEAOEAseptic Non Union
24 m
G.B.P. - 14 year old - Female
AOEAOEAseptic Non Union
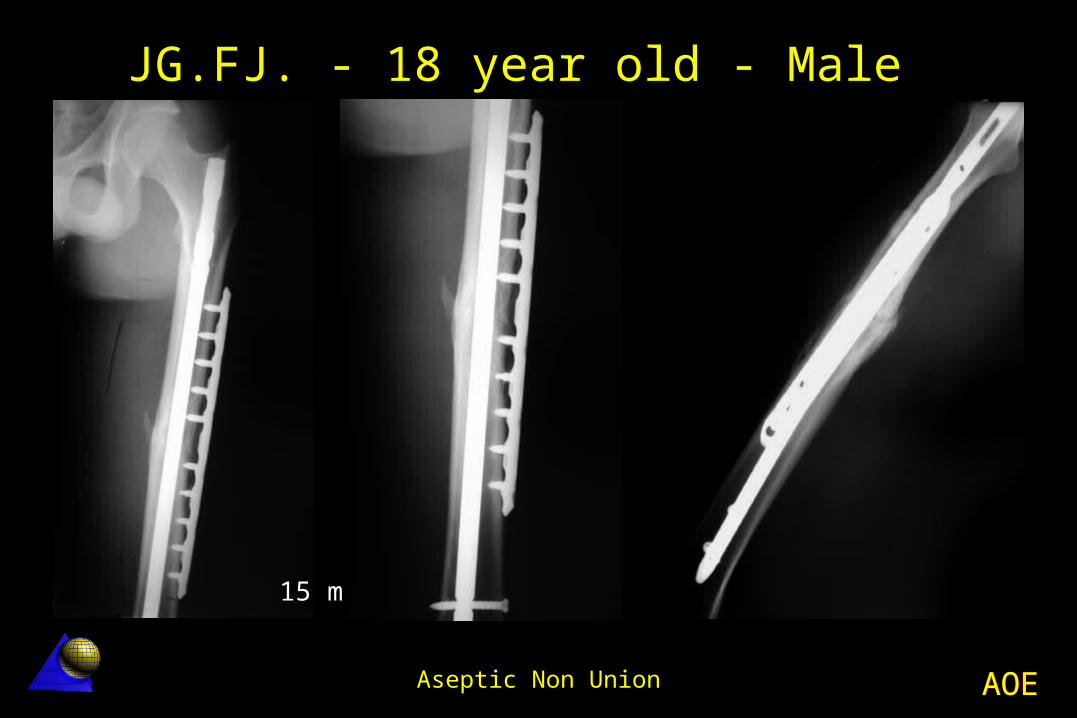
Left femur B2.2 fracture Operation: 6.5.02
UFN locked nailing with satisfactory reduction 9.02 - Small wedge resorption and instability 25.11.02 Operation
Decorticatión and LCP fixation without nail removal Bone grafting
Bone healing in 4 months (10 months since the accident)
Complete function at 12 months.
JG.FJ. - 18 year old - MaleMotorcycle accident - 5.5.02

AOEAOEAseptic Non Union
JG.FJ. - 18 year old - Male
PO0 m 6 s

AOEAOEAseptic Non Union
4 m 6 m
JG.FJ. - 18 year old - Male

AOEAOEAseptic Non Union
JG.FJ. - 18 year old - Male
6 m7 m

AOEAOEAseptic Non Union
JG.FJ. - 18 year old - Male
10 m 12 m
AOEAOEAseptic Non Union
JG.FJ. - 18 year old - Male
15 m
AOEAOEAseptic Non Union
L.S.C. - 27 year old - FemaleFemoral non-union - 5.89 Right femur transverse fracture
Primary reamed IM nailing No callus formation at 15 months Nail failure at 16 months Treatment
Nail removal without opening the fracture site
New reamed thicker nailing Bone healing in 2 months

AOEAOEAseptic Non Union
L.S.C. - 27 year old - Female
0 m 15 m

AOEAOEAseptic Non Union
L.S.C. - 27 year old - Female
16 m 24 m
AOEAOEAseptic Non Union
Fibula “pro tibia”
AOEAOEAseptic Non Union
P.A.R. - 10 year old - MaleAcute osteomyelitis secualae - 9.66 Diaphyseal segmental bone loss Fibula “pro tibia” proximal and distal Fibula tibialization Excellent result at 3 years.

AOEAOEAseptic Non Union
0 m 36 m
P.A.R. - 10 year old - Male
20 m
AOEAOEAseptic Non Union
G.S.A. - 15 year old - MaleRun over by a car – 3.97 Polytrauma patient Right tibia open IIIB fracture Peroneal muscles and nerve loss Extensive skin loss Immediate External Fixation Dorsalis free vascularized transfer
AOEAOEAseptic Non Union
Atrophic proximal tibia aseptic non-union
Osteoporotic bone Fibula “pro tibia” (lateral approach) Medial LC-DCP buttress plate fixation Autologous cancellous bone grafting
G.S.A. - 15 year old - MaleRun over by a car – 3.97

AOEAOEAseptic Non Union
G.S.A. - 15 year old - Male
PO 1 m 6 m 8 m

AOEAOEAseptic Non Union
G.S.A. - 15 year old - Male
12 m

AOEAOEAseptic Non Union
G.S.A. - 15 year old - Male
36 m

AOEAOEAseptic Non Union
G.S.A. - 15 year old - Male

AOEAOEAseptic Non Union
G.S.A. - 15 year old - Male
5 years

AOEAOEAseptic Non Union
G.S.A. - 15 year old - Male
5 years
AOEAOEAseptic Non Union
Related Documents