ARTHROSCOPIC GANGLIONECTOMY BY DIVYA SINGH, MD, AND RANDALL W. CULP, MD Ganglions are tbe most common sojt-tissne tumors seen and treated in the band and wrist. A wide variety of treatments bate been described including observation, aspiration, sclerotberapy, and open surgica! excision. /vrtbroscopic ganglion resection provides a minimally invasive means to safely resect dorsa l wrist gang lionJ while avoiding tbe requisite scar accompanying open resection . Artbro- scopic gang lionectomy allows a more complete examination of tbe wrist to include tbe etiology and location oftbe ganglions. and assode/ted intra-articular prob- lems. /vrtbroscopic resection is an approacb that preuents some of tbe complications of an open excision, and that may provide a lower recurrence rate. Copy rigbt © 2002 by the American ociety for SlIrgery of tbe Hand T he Greek term ganglion means knot of tissue, and an early description by Hippocrates refers to ganglions as containing mucoid flesh.v" Ganglions are defined as cyst-like masses closely asso- ciated with either joint or tendon sheaths that contain mucinous or jelly-like fluid. It has been estimated that over 25,000 resections are performed yearly for this most common soft-tissue tumor of the hand and wrist. A review of the literature in ganglion management shows a wide variety of treatment options. Observa- tion alone, which reflects the natural history of these cysts, includes a spontaneous resolution rate of 40% to 58%.5 Aspiration, with or without a cortisone in- jection, has a success rate of 36% to 85%.3,6-8 Open From the Philadelphia Hand Center, Department of Orthopedic Surgery, Thomas Jefferson University Hospital, Philadelphia, PA. Address reprint requests to Randall W. Cuip, MD, Philadelphia Hand Center, 700 Henderson Road, Suite 200, King of Prussia, PA 19406. E-mail: [email protected] Copyright © 2002 by the American Society for Surgery of the Hand 1531-0914/02/0201-0005$35.00/0 doi: 10.1053/jssh.2002.31118 surgical excision carries the risk for recurrence of 20% to 40%.2,3,5,9 The basis for a successful open surgical treatment is excision of a dorsal capsular window to include the ganglion stalk, which usually presents at the dorsal scapholunate and capsular area. Wrist arthroscopy has rapidly developed from a diagnostic to a therapeutic modality within the past decade. Initially described by Osterman and Ra- phael-? in 1995, arthroscopic ganglionectomy repre- sents a minimally invasive procedure with results equal to or superior to open procedures, with fewer risks and complications. As with open procedures, arthroscopic ganglionectomy allows for excision of the ganglion stalk based at the scapholunate ligament with a dorsal capsular window. ETIOLOGY M u lt iple theories have been advocated regarding the cause of ganglion cysts. Soren,? based on cross-sections of various-sized cysts, believed gangli- ons arise from a "mucoid degeneration process." Other investigators have suggested a I-way valve mechanism JOURNAL OF THE AMERICAN SOCIETY FOR SURGERY OF THE HAND' VOL. 2. NO. I, FEBRUARY 2002 33

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ARTHROSCOPIC
GANGLIONECTOMY
BY DIVYA SINGH, MD, AND RANDALL W. CULP, MD
Ganglions are tbe most common sojt-tissne tumors seen and treated in the bandand wrist. A widevariety of treatments bate been described includingobservation,aspiration, sclerotberapy, and open surgica! excision. /vrtbroscopic ganglionresection provides a minimally invasive means to safely resect dorsal wristganglionJ while avoiding tbe requisite scar accompanying open resection. Artbroscopic ganglionectomy allows a more complete examination of tbe wrist to includetbe etiology and location of tbe ganglions. and assode/ted intra-articular problems. /vrtbroscopic resection is an approacb that preuents some of tbe complicationsof an open excision, and that may provide a lower recurrence rate.
Copyrigbt © 2002 by the American ociety for SlIrgery of tbe Hand
The Greek term ganglion means knot of tissue,and an early description by Hippocrates refersto ganglions as containing mucoid flesh.v"
Ganglions are defined as cyst-like masses closely asso
ciated with either joint or tendon sheaths that containmucinous or jelly-like fluid. It has been estimated thatover 25,000 resections are performed yearly for thismost common soft-tissue tumor of the hand and wrist.
A review of the literature in ganglion managementshows a wide variety of treatment options. Observation alone, which reflects the natural history of these
cysts, includes a spontaneous resolution rate of 40% to58%.5 Aspiration, with or without a cortisone injection, has a success rate of 36% to 85%.3,6-8 Open
From the Philadelphia Hand Center, Department of OrthopedicSurgery, Thomas Jefferson University Hospital, Philadelphia, PA.Address reprint requests to Randall W. Cuip, MD, PhiladelphiaHand Center, 700 Henderson Road, Suite 200, King ofPrussia, PA19406. E-mail: [email protected]
Copyright © 2002 by the American Society for Surgery of the Hand1531-0914/02/0201-0005$35.00/0doi:10.1053/jssh.2002.31118
surgical excision carries the risk for recurrence of 20%to 40%.2,3,5,9 The basis for a successful open surgicaltreatment is excision of a dorsal capsular window toinclude the ganglion stalk, which usually presents atthe dorsal scapholunate and capsular area.
Wrist arthroscopy has rapidly developed from adiagnostic to a therapeutic modality within the pastdecade. Initially described by Osterman and Raphael-? in 1995, arthroscopic ganglionectomy represents a minimally invasive procedure with resultsequal to or superior to open procedures, with fewerrisks and complications. As with open procedures,arthroscopic ganglionectomy allows for excision of theganglion stalk based at the scapholunate ligamentwith a dorsal capsular window.
ETIOLOGY
M ultip le theories have been advocated regardingthe cause of ganglion cysts. Soren,? based on
cross-sections of various-sized cysts, believed ganglions arise from a "mucoid degeneration process." Otherinvestigators have suggested a I-way valve mechanism
JOURNAL OF THE AMERICAN SOCIETY FOR SURGERY OF THE HAND' VOL. 2. NO. I, FEBRUARY 2002 33

34 GANGLIONECTOMY' SINGH & CULP
when arthrographic, magnetic resonance imaging(MRI), and ultrasound studies showed communica
tion between the wrist joint and the ganglion via atract in 23% to 70% of patients. ll ,12
Some investigators have suggested that ganglionsoccur secondary to acute or chronic ligamentous stress.A history of previous trauma to the wrist is noted in10% to 50% of parienrs.t-'> Watson et aP4 reported
on 17 patients who developed rotary subluxation ofthe scaphoid after open ganglion excision.
Dorsal ganglions occur at the transition between
the dorsal scapholunate ligament and capsule. A com
plex series of cysts form a I-way valve, pumping fluidfrom the wrist joint to the primary ganglion. 1 1 It is
therefore critical to address the stalk and its sur
rounded capsule and not just the cyst because surgicalresection of the cyst alone yields a 30% to 60%recurrence rate.
CLINICAL PRESENTATION
G anglions occur primarily in the 2nd to 4thdecade of life, with a ratio of women to men
ranging from 2 to 4:1. 1,5 Symptoms depend on size
and location. Ganglions may appear suddenly or de
velop gradually over time. Typically measuring 1 to 2em in size, dorsal wrist ganglions usually present overthe dorsal scapholunate ligament area (Fig 1).
The most common presenting symptom is a dull
ache, which may be the result of compression of theposterior interosseous nerve's terminal branches.'? Pa
tients may also complain of the cosmetic deformity,pain with range of motion, or stiffness. Because of thesize of the ganglions, wrist extension activities may beproblematic.
J
FIGURE 1. Dorsal wrist ganglion. Reprinted with permissionfrom The Philadelphia Hand Center.
RADIOGRAPHIC EVALUATION
P lain radiographs are usually unremarkable. AnMRI can be obtained preoperatively to verify the
presence of a cystic mass and to rule out other diagnoses. It can also help to delineate the anatomicboundaries of the ganglion and its relationship to thescapholunate ligament.
INDICATIONS AND CONTRAINDICATIONS
T he primary indication for surgery is a symptomaticdorsal wrist ganglion. Patients should have com
plaints of pain that interferes with daily activities. Arthroscopic resection of occult dorsal ganglions has yet tobe reported on. Relative contraindications include recurrent ganglions, previous dorsal wrist open surgery, andinexperience of the surgeon in arthroscopic techniques.
TECHNIQUE
W rist arthroscopy is undertaken in the usualfashion with the patient in the supine position.
Either regional or a general anesthesia can be used. Atourniquet is used for better visualization. Traction of10 pounds through finger traps on the index and longfingers are used through a traction tower.
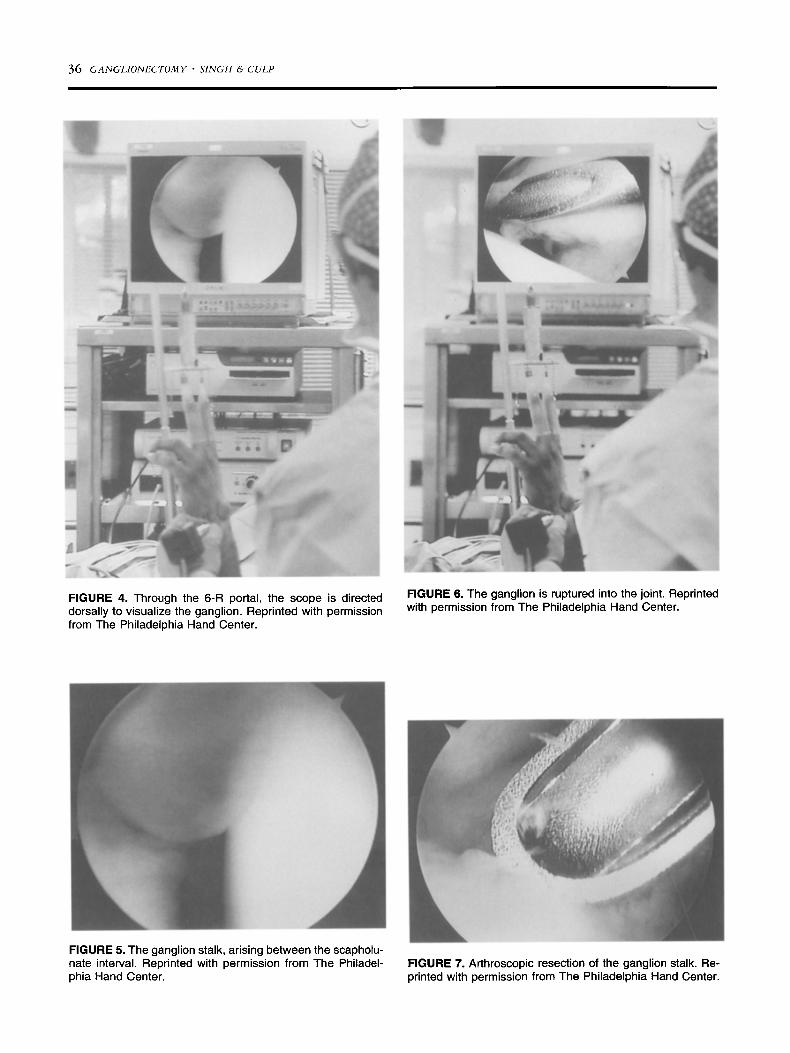
The standard arthroscopic portal landmarks(Lister's tubercle, extensor carpi ulnaris, 3-4 portal,6 radial [6R}, radial midcarpal) and ganglion aremarked and identified (Fig 2). The 6R portal is established first because the ganglion lies directly overthe 3-4 portal and the ganglion stalk is best visualizedfrom the ulnar side of the wrist (Fig 3). At this time,the proximal carpal row, intrinsic and extrinsic ligaments, and the triangular fibrocartilage complex areevaluated for concomitant pathology without disrupting the ganglion stalk. From the 6R portal, attentionis directed radially and dorsally. Gentle pressure withthe surgeon's thumb over the ganglions helps to visualize the stalk, which appears pearly gray and opalescent at the junction of the scapholunate ligamentand the dorsal capsule (Figs 4 and 5).
By using an 18-gauge needle through the 3-4portal, the ganglion stalk is ruptured into the joint asvisualized through the 6R portal (Fig 6). A 2.9-mmfull-radius resector placed into the 3-4 portal is usedto resect the ganglion stalk and a I-crrr' segment ofdorsal capsule (Fig 7). Decompression of the ganglionis noted by gelatinous material in the arthroscopic
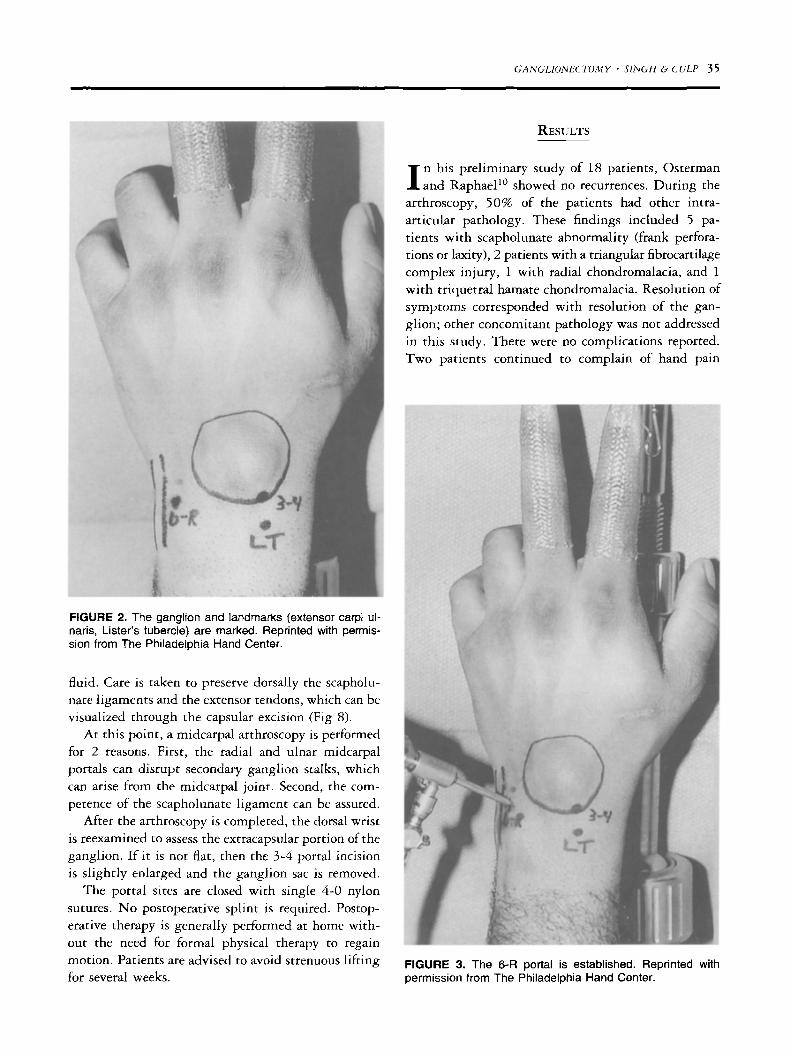
FIGURE 2. The ganglion and landmarks (extensor carpi ulnaris, Lister's tubercle) are marked. Reprinted with permission from The Philadelphia Hand Center.
fluid. Care is taken to preserve dorsally the scapholunate ligaments and the extensor tendons, which can bevisualized through the capsular excision (Fig 8).
At this point, a midcarpal arthroscopy is performedfor 2 reasons. First, the radial and ulnar midcarpalportals can disrupt secondary ganglion stalks, whichcan arise from the midcarpal joint. Second, the competence of the scapholunate ligament can be assured.
After the arthroscopy is completed, the dorsal wristis reexamined to assess the extracapsular portion of theganglion. If it is not flat, then the 3-4 portal incisionis slightly enlarged and the ganglion sac is removed.
The portal sites are closed with single 4-0 nylonsutures. No postoperative splint is required. Postoperative therapy is generally performed at home without the need for formal physical therapy to regainmotion. Patients are advised to avoid strenuous liftingfor several weeks.
GANGLIONECTOMY' SINGH & CULP 3S
RESULTS
I n his preliminary study of 18 patients, Ostermanand Raphael!" showed no recurrences. During the
arthroscopy, 50% of the patients had other intraarticular pathology. These findings included 5 patients with scapholunate abnormality (frank perforations or laxity), 2 patients with a triangular fibrocartilagecomplex injury, 1 with radial chondromalacia, and 1with triquetral hamate chondromalacia. Resolution ofsymptoms corresponded with resolution of the ganglion; other concomitant pathology was not addressedin this study. There were no complications reported.Two patients continued to complain of hand pain
FIGURE 3. The 6-R portal is established. Reprinted withpermission from The Philadelphia Hand Center.
36 GANGLIONECTOMY· SINGH & CULP
,
FIGURE 4. Through the 6-R portal, the scope is directeddorsally to visualize the ganglion. Reprinted with permissionfrom The Philadelphia Hand Center.
FIGURE 5. The ganglion stalk, arising between the scapholunate interval. Reprinted with permission from The Philadelphia Hand Center.
FIGURE 6. The ganglion is ruptured into the joint. Reprintedwith permission from The Philadelphia Hand Center.
FIGURE 7. Arthroscopic resection of the ganglion stalk. Reprinted with permission from The Philadelphia Hand Center.

A Area of Cyst (capsule) Resection B
GANGLIONECTOMY' SINGH & CULP 37
Area of Cyst (capsule) Resection
Area ofcyst, stalk,and capsuleresection
DorsalI +---If+- wrist
capsule
EDC
Area of ~ - ___cyst, stalk,
and capsuleresection
FIGURE 8. Area of cyst/dorsal capsule resection in the (A) sagittal and (8) coronal planes.
with strenuous use postoperatively. Osterman andCulp's prospective study now has over 80 patients,with only 1 recurrence reported.!?
A recent study performed by Luchetti et al.!? usinga modification of the technique described earlier,showed recurrence in 2 of 34 resections and residualpain in 3 of 34 (mean follow-up of 16 months).Included in their study were 3 patients with recurrences after open surgery, and 1 with a recurrence afteran arthroscopic treatment. The primary complicationin this study was dorsal wrist swelling in 8 patients(attributed to retained irrigation fluid) at the ganglionsite postoperatively. This fluid accumulation was treatedwith aspiration, with no further problems.
COMPLICATIONS
Complications from wrist arthroscopy in general arerelatively infrequent, with the incidence reported
around 2%.18 As in all arthroscopy, an understanding ofportal placement and relevant anatomy is necessary so asto prevent injury to tendons, neurovascular structures,and articular surfaces. 19 ,20 Forceful introduction of scalpels and trocars must be avoided. If the 6 ulnar or 1-2
portals are used, particular care must be taken to preventinjury to the ulnar sensory and superficial radial nerves.The radial artery can be damaged also, again, if the 1-2portal is not properly placed. Prolonged tourniquet timeand finger traction can damage the skin, ligaments, orperipheral nerves. Although not specifically reported, theextensor tendons and the dorsal scapholunate ligamentare at risk if the resection proceeds too far dorsally.
Recurrence is a concern with both open and arthro
scopic procedures. Any surgical procedure runs the riskfor scar formation and possible joint stiffness. Prolongedimmobilization of the wrist would increase this risk,
whereas the early mobilization postarthroscopy wouldtheoretically decrease scarring and stiffness.
TECHNICAL DIFFICULTIES
O ne advantage of arthroscopic ganglionectomy isvisualization of the ganglion stalk and ligamentous
pathology. If there is a technical or an anatomic problempreventing clear appreciation of the pathology, the surgeon may need to convert to an open procedure. Thepatient should be apprised of this possibility.

38 GANGLIONECTOMY' SINGH & CULP
DISCUSSION
I n summary, arthroscopic ganglionectomy is a reasonable procedure that improves on the results of
open ganglionectomy. Forty percent of ganglions will
have an intra-articular finding but, in most cases, anypreoperative symptoms disappear with ganglion resection alone. The advantages of the arthroscopic procedure include less scarring, faster mobilization, and a
better assessment of intra-articular pathology.
REFERENCES
1. Angelides AC. Ganglions of the hand and wrist. In: GreenDP, Hotchkiss RN, Pederson WC, eds. Green's OperativeHand Surgery. 4 th ed. Philadelphia: Churchill Livingstone,1999:2171-2183.
2. Angelides AC, Wallace PF. The dorsal ganglion of the wrist:Its pathogenesis, gross anatomy, and surgical treatment.J Hand Surg 1976;1:228-235.
3. Nelson CL, Sawmiller S, Phalen GS. Ganglions of the wristand hand. J Bone Joint Surg 1972;54A:1450-1464.
4. Soren A. Pathogenesis and treatment of ganglion. Clin Orthop 1966;48:173-179.
5. Carp L, Stout AP. A study of ganglion, with special referenceto treatment. Surg Gynecol Obster 1928;47:460-468.
6. Korman J, Pearl R, Hentz VR. Efficacy of immobilizationfollowing aspiration of carpal and digital ganglions. J HandSurg 1992;17A:1097-1099.
7. Richman JA, Gelberman RH, Engber WD, et al. Ganglionsof the wrist and digits: Results of treatment by aspiration andcyst wall puncture. J Hand Surg 1987;12A:1041-1043.
8. Zubowicz VN, Ishii CH. Management of ganglion cysts ofthe hand by simple aspiration. J Hand Surg 1987;12A:618620.
9. McEvedy BV. The simple ganglion: A review of treatmentand an explanation of the frequent failure of surgery. Lancet1954;1:135-136.
10. Osterman AL, Raphael J. Arthroscopic resection of dorsalganglion of the wrist. Hand Clin 1995;11:7-12.
11. Andren L, Eiken O. Arthrographic studies of wrist ganglions.J Bone Joint Surg 1971;53A:299-302.
12. Bianchi S, Abdelwahab IF, Zwass A, er al. Ultrasonic evaluation of wrist ganglia. Skeletal Radiol 1994;23:201-203.
13. McEvedy BV. Simple ganglia. Br J Surg 1962;49:585-594.14. Watson HK, Rogers WD, Ashmead D IV. Reevaluation of
the cause of the wrist ganglion. J Hand Surg 1989;14A:812817.
15. Dellon AL, Seif SS. Anatomic dissections relating the posterior interosseous nerve to the carpus, and the etiology ofdorsal wrist ganglion pain. J Hand Surg 1978;3:326-332.
16. Bienz T, Raphael JS. Arthroscopic resection of the dorsalganglia of the wrist. Hand Clin 1999;15:429-434.
17. Luchetti R, Badia A, Alfarano M, et al. Arthroscopic resectionof dorsal wrist ganglia and treatment of recurrences. J HandSurg 2000;25B:38-40.
18. Culp RW. Complications of wrist arthroscopy. Hand Clin1999;15:529-535.
19. Berger RA. Arthroscopic anatomy of the wrist and distalradioulnar joint. Hand Clin 1999;15:393-413.
20. Osterman AL. Atlas of right wrist arthroscopy. Hand Clin1995;11:103-113.
Related Documents











