STUDY PRO T O COL Open Access A comparison of rigid tape and exercise, elastic tape and exercise and exercise alone on pain and lower limb function in individuals with exercise related leg pain: a randomised controlled trial Melinda M Franettovich Smith 1* , Sonia S Coates 1 and Mark W Creaby 2 Abstract Background: Exercise related leg pain (ERLP) is a common lower limb overuse injury characterised by pain located betwee n the knee and ankle that occurs during activit y. The high incidence of the condition, subsequ ent interfere nce with participation in physical activity and substantial recovery time, highlights a need for effective interventions. Whilst many interventions have been described for the management of ERLP, currently there is a lack of high quality evidence for an effective intervention for the condition. Methods/Design: A single -blinde d randomised controlled clinical trial will be condu cted in a commu nity setting. Forty-five female volunteers aged between 18 and 40 years with a history of insidious onset of pain located between the knee and ankle of at least one month duration that is aggravated by weight bearing activities will be recruited for the study. Suitable participants will be randomly allocated to one of three treatment groups for the 6 week intervention period : (i) exercise only, (ii) rigid anti-prona tion tape and exercise, (iii) elastic anti-pr onation tape and exercise. Outcomes will be measured at baseline, 1, 2 and 6 weeks using primary outcome measures of usual and worst pain visual analogue scale and global perceived improvement. Secondary outcome measures will include Foot and Ankle Ability Measure, Patient Specific Functional Scale and amount of activity in the previous week. In addition, participants will be contacted by phone to obtain primary and secondary outcome measures at 12, 18, 24 and 30 weeks. Discussion: This article describes a single-blinded randomised controlled clinical trial that will utilise high quality methodologies in accordance with CONSORT guidelines. The results of this study will contribute to the limited knowledge regarding effective interventions for the management of ERLP. Trial registration: Australian New Zealand Clinical Trials Registry (ACTRN12613000914763 ) Keywords: Shin pain, Medial tibial stress syndrome, Anti-pronation Background Exercise related leg pain (ERLP) is a lower limb overuse injury characterised by pain located between the knee and ankle that occurs during activity. The condition encom- passes the clinical and pathological features of several commo nly used labels such as shin splints, medial tibial stress syndrome, periostitis, stress fractures, tendinopa- thies and compartment syndrome [1]. ERLP is particu- larly common in running populations with 13 to 20% of runnin g injur ies presenting to sports medicine clinics attributed to ERLP [ 1]. Incidence of ERLP has also been reported to be higher in females than males [2-6]. Signif icant burden is associated with the condit ion with 40-60% of runne rs reporting that ERLP caused a reduc - tion in running or an interr uption to training [7,8]. Furthermore, the condition is associated with lengthy recovery periods in both runners and military personnel [9,10]. Given the high incidence of the condition, subse- quent interference with participation in physical activity and subst antial recovery time, effective interventions for management of ERLP are required. * Correspondence: [email protected] 1 School of Physiotherapy, Australian Catholic University, Brisbane, Australia Full list of author information is availa ble at the end of the artic le © 2014 Franettovich Smith et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated. Franettov ich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328 http://ww w.biomedc entral.com/ 1471-2474/15/328

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
STUDY PROTOCOL
ed
rk
Keywords: Shin pain, Medial tibial stress syndrome, Anti-pronation
Franettovich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328http://www.biomedcentral.com/1471-2474/15/328for management of ERLP are required.1School of Physiotherapy, Australian Catholic University, Brisbane, AustraliaFull list of author information is available at the end of the articleBackgroundExercise related leg pain (ERLP) is a lower limb overuseinjury characterised by pain located between the knee andankle that occurs during activity. The condition encom-passes the clinical and pathological features of severalcommonly used labels such as shin splints, medial tibialstress syndrome, periostitis, stress fractures, tendinopa-thies and compartment syndrome [1]. ERLP is particu-larly common in running populations with 13 to 20% of
running injuries presenting to sports medicine clinicsattributed to ERLP [1]. Incidence of ERLP has also beenreported to be higher in females than males [2-6].Significant burden is associated with the condition with40-60% of runners reporting that ERLP caused a reduc-tion in running or an interruption to training [7,8].Furthermore, the condition is associated with lengthyrecovery periods in both runners and military personnel[9,10]. Given the high incidence of the condition, subse-quent interference with participation in physical activityand substantial recovery time, effective interventions* Correspondence: [email protected]
Background: Exercise related leg pain (ERLP) is a common lower limb overuse injury characterised by pain locatedbetween the knee and ankle that occurs during activity. The high incidence of the condition, subsequent interferencewith participation in physical activity and substantial recovery time, highlights a need for effective interventions. Whilstmany interventions have been described for the management of ERLP, currently there is a lack of high quality evidencefor an effective intervention for the condition.
Methods/Design: A single-blinded randomised controlled clinical trial will be conducted in a community setting.Forty-five female volunteers aged between 18 and 40 years with a history of insidious onset of pain located betweenthe knee and ankle of at least one month duration that is aggravated by weight bearing activities will be recruited forthe study. Suitable participants will be randomly allocated to one of three treatment groups for the 6 week interventionperiod: (i) exercise only, (ii) rigid anti-pronation tape and exercise, (iii) elastic anti-pronation tape and exercise. Outcomeswill be measured at baseline, 1, 2 and 6 weeks using primary outcome measures of usual and worst pain visualanalogue scale and global perceived improvement. Secondary outcome measures will include Foot and Ankle AbilityMeasure, Patient Specific Functional Scale and amount of activity in the previous week. In addition, participants will becontacted by phone to obtain primary and secondary outcome measures at 12, 18, 24 and 30 weeks.
Discussion: This article describes a single-blinded randomised controlled clinical trial that will utilise high qualitymethodologies in accordance with CONSORT guidelines. The results of this study will contribute to the limitedknowledge regarding effective interventions for the management of ERLP.
Trial registration: Australian New Zealand Clinical Trials Registry (ACTRN12613000914763)A comparison of rigid taptape and exercise and exlower limb function in inrelated leg pain: a randomMelinda M Franettovich Smith1*, Sonia S Coates1 and Ma 2014 Franettovich Smith et al.; licensee BioMthe Creative Commons Attribution License (htdistribution, and reproduction in any mediumDomain Dedication waiver (http://creativecomarticle, unless otherwise stated.Open Access
e and exercise, elasticrcise alone on pain andividuals with exerciseised controlled trial
W Creaby2ed Central Ltd. This is an Open Access article distributed under the terms oftp://creativecommons.org/licenses/by/4.0), which permits unrestricted use,, provided the original work is properly credited. The Creative Commons Publicmons.org/publicdomain/zero/1.0/) applies to the data made available in this
-
Franettovich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328 Page 2 of 10http://www.biomedcentral.com/1471-2474/15/328Several interventions have been described for themanagement of ERLP such as load management, low-energy laser treatment, stretching exercises, strengthen-ing exercises, compression stockings, leg braces, pulsedelectromagnetic fields, ice massage, ultrasound, ionto-phoresis, phonophoresis, and extracorporeal shockwavetherapy. Whilst many of these interventions have beeninvestigated in the literature, a recent systematic review[11] has reported a lack of evidence for an effective inter-vention for the condition. Despite the lack of researchevidence, there appears to be consensus among clinicalopinion pieces and review articles for the use of relativerest (load modification, alternative training), NSAIDS andice in the acute phase of ERLP [1], and following this, thecommencement of strengthening exercises for the calf andintrinsic foot muscles as well as more proximal musclesincluding the abdominals and gluteals with the aim ofimproving endurance and running mechanics [1,12,13].To further develop the evidence base from expert opinionand anecdotal reports, Winters and colleagues [11] havesuggested that it may be important to first understand theaetiological factors contributing to the condition.A systematic review and meta-analysis by Newman
et al. [14] suggests that the aetiology of ERLP is likelymultifactorial. The authors reported evidence forseveral contributing factors: previous history of the condi-tion (relative risk (RR) 3.74), female gender (RR 1.71),decreased running experience (standardised mean dif-ference (SMD) -0.74), higher body mass index (SMD0.24), history of orthotic use (RR 2.31) and >10 mmvertical displacement of the navicular from a subtalarneutral position to bodyweight supported stance (RR 1.99),commonly termed navicular drop [15]. Of these factorshowever only body mass index and navicular drop arepotentially modifiable. Based on these findings, it isconceivable that interventions which reduce body massindex or reduce navicular drop may have the potentialto influence pain and function in individuals with ERLP.Navicular drop provides an indication of the vertical
mobility of the midfoot, which can also be measured bydorsal arch height difference [15]. Interventions whichhave demonstrated effectiveness in reducing verticalmobility of the midfoot include taping and exercise.Anti-pronation taping techniques, such as the low-Dyeand augmented low-Dye (ALD), have consistently dem-onstrated reductions in vertical mobility of the midfootand increased medial longitudinal arch height immedi-ately following application, during walking and jogging,and following 20mins of jogging [16,17]. Of interest, theALD taping technique has also demonstrated maintenanceof an increase in medial longitudinal arch height followingremoval of tape after two weeks of continual wear [18].
Importantly, these biomechanical effects have beendemonstrated in ERLP populations [17-19], howeverthe efficacy of the ALD in the management of pain andfunction has not been evaluated. These anti-pronationtaping techniques have traditionally in the past beenapplied using a rigid (inelastic) sports tape, however inrecent times, and at least since the 2008 OlympicGames, there has been increasing popularity in the useof elastic tapes, such as Kinesio tape , Dynamic Tape,KT-Tape, SpiderTech and Cure Tape [20]. The rea-sons underlying the increasing popularity of elastictaping are not known. The elastic nature of the tapeand alternate fabrication with more waterproof mate-rials may lead to increased comfort. It is also conceiv-able that the elastic recoil in the tape may providemechanical assistance or resistance (deceleration oracceleration) to movement, therein reducing the loaddemands on musculotendinous units while also per-mitting full range of motion to occur. Neverthelessdespite their growing utility in the clinical setting, nostudy to date has evaluated the efficacy of an elastictaping technique in the management of ERLP.Plantar intrinsic foot muscle training consisting of sub-
maximal flexion of the metatarsophalangeal and proximalinterphalangeal joints to raise medial longitudinal archheight has also demonstrated reductions in verticalmidfoot mobility. Mulligan et al. [21] reported that afour week program consisting of three minutes daily ofthis plantar intrinsic foot muscle exercise, which pro-gressed from sitting to bilateral and single leg stance,produced a reduction in navicular drop. This reductionin navicular drop was evident at conclusion of the pro-gram and was maintained another four weeks followingcessation of the program. This training program, how-ever, was evaluated in an asymptomatic population andhas not been investigated in individuals with ERLP. Inaddition, there is evidence that during functional tasksmotion of the foot is related to more proximal motionat the hip, suggesting that a whole limb approach tocontrol midfoot mobility may be warranted. Specifically,increased navicular drop has been reported to be relatedto increased hip internal rotation during a single-legsquat [22] and moderate to strong correlations havebeen reported between frontal and transverse planemovements of the hip and frontal plane movement ofthe foot during walking [23,24]. This evidence suggeststhat strengthening exercises for the hip abductor andexternal rotator muscles may also have the potential toinfluence foot mobility, however this has not beeninvestigated.The current lack of evidence for effective interventions
for the management of ERLP warrants the conduct offurther high quality randomised controlled trials. A rea-sonable rationale for the development of an effective
intervention may be one based on current clinical expertopinion and addressing identified risk factors for the
-
Recruitment of participantsFemale volunteers will be recruited from paid advertise-ments in local community newspapers, supplementedby regular postings of advertisements on noticeboardswithin the University and wider community (e.g. gym-nasiums, sporting clubs, health clinics). Each potentialparticipant who responds to advertisements will undergoa screening process (via phone or email) to determineeligibility. Eligible volunteers will be provided with aninformation sheet thoroughly explaining the study andinformed written consent to participate in the study willbe obtained. Once eligibility has been determined and theinformed consent process completed, participants will beassigned an identification number. Enrolled participantswill attend a baseline testing session at which an assessorblinded to group allocation will obtain demographic infor-mation (age, weight, height), clinical characteristics ofERLP (nature, location, duration, onset, previous treat-ment), exercise history (intensity, duration and modalityof current participation, and participation prior to the
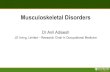
Figure 1 Flow chart of participants through study.
Franettovich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328 Page 3 of 10http://www.biomedcentral.com/1471-2474/15/328condition. As previously discussed, there appears to be ageneral consensus that advocates relative rest followedby strengthening exercise(s) for the management ofERLP. Whilst several risk factors for the condition havebeen identified, foot mobility is one of two modifiablefactors. Anti-pronation taping and plantar intrinsic footmuscle training have demonstrated the ability to reducefoot mobility, however, no scientific study has evaluatedthe effectiveness of either intervention in the manage-ment of pain and function in ERLP.
MethodsAimThe aim of this project is to compare the effectivenessof (i) lower limb muscle training alone, (ii) lower limbmuscle training and rigid anti-pronation taping, and (iii)lower limb muscle training and elastic anti-pronationtaping, for the management of ERLP.
Study designA randomised controlled clinical trial will be conductedin a community setting over a 12 month period. TheAustralian Catholic University Human Research EthicsCommittee has granted ethical approval and all partici-pants will provide informed written consent prior tocommencement in the trial. An individual independentto the trial will perform the computer-generated ran-domisation sequence and preparation of envelopes con-taining the group allocation. The physiotherapist willcommunicate with participants regarding group alloca-tion; due to the nature of the intervention it will not bepossible to blind the treating physiotherapist or the par-ticipants. An assessor blinded to group allocation willperform outcome measurements at all time points. Dataentry and statistical analysis will be performed by ablinded assessor. Figure 1 provides an overview of thestudy protocol.
Eligibility criteriaFemale volunteers will be eligible for participation in thetrial on the basis of the following criteria: age 18 to40 years, insidious onset of pain unrelated to any trau-matic event, pain located between the knee and ankle ofat least one month duration that is aggravated by weightbearing activities such as running, hopping or jumping,and worst pain over the previous week of at least 30 mmon a 100 mm visual analogue scale. Volunteers will beexcluded from the trial in the presence of any of the fol-lowing: a history of surgery to the lower limb, a cardiaccondition, a known allergy to adhesive strapping tape,or symptoms of radiculopathy or other neurological in-volvement. Extensive previous exposure to either taping
technique will also exclude volunteers from participationin order to prevent bias to one intervention.onset of ERLP), and perform outcome measurements.At the conclusion of baseline outcome measurements,
-
Franettovich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328 Page 4 of 10http://www.biomedcentral.com/1471-2474/15/328the participant will be notified of group allocation bythe treating physiotherapist and the intervention willcommence.
RandomisationFor group allocation, a computer-generated table ofrandom numbers (in three blocks) will be used for therandomisation sequence. An individual not otherwiseinvolved in the study will place the randomisationsequence in a series of consecutively numbered opaqueenvelopes, and sign across the seal of the envelope.Allocation will be concealed from the outcome assessorfor the duration of the trial.
InterventionThe interventions will be performed by one of two regis-tered physiotherapists (Physiotherapy Board of Australia),each with at least 10 years of experience in musculoskel-etal physiotherapy. In addition, both physiotherapists willhave completed two comprehensive training sessionstogether for explanation and discussion of the standar-dised intervention protocol for the trial. A detailed writtenprotocol outlining trial procedures will be provided totreating physiotherapists. This will include standardisedinstructions for participant advice, application of both therigid and elastic taping techniques, prescription of thelower limb muscle training exercises, and recording oftreatment. Over a six week intervention period partici-pants will receive one of three treatments: (i) lower limbmuscle training alone, (ii) combined intervention of rigidtape and lower limb muscle training, (iii) combined inter-vention of elastic tape and lower limb muscle training.
Lower limb muscle training aloneParticipants in this group will receive advice and edu-cation and will be prescribed an exercise program toperform at home. At the completion of the baseline out-come measurements, the physiotherapist will provide astandardised information sheet with advice and educa-tion regarding ERLP, as well as load management. Partic-ipants will be advised not to start any new activities ortreatments for the duration of the study, encouraged tocontinue to wear current footwear (including orthoticuse) and participate in activities that do not provokesymptoms and to avoid activities that aggravate symp-toms either during or following the activity; as treatmentprogresses, this may include a return to participation inactivities that previously aggravated symptoms.At the end of week 1, the participant will attend a
thirty minute physiotherapy session where advice andeducation information will be reviewed with the patientand training in the exercise program will commence.
The exercise program will include two exercises: (i) theplantar intrinsic foot muscle exercise [21] (Figure 2), and(ii) hip abductor and external rotator muscle exercise(Figure 3). The difficulty of both exercises can be in-creased from non-weightbearing, to double-limb weight-bearing and then single-limb weightbearing (Figures 2and 3). A rating scale to assess the intrinsic foot muscles[21], based on unsteadiness of navicular height duringsingle-limb stance, will be used to decide the difficultyof the exercises prescribed at the first session: non-weightbearing exercises will be prescribed for a rating ofpoor stability; double limb weightbearing exercises willbe prescribed for a rating of fair stability, and single-limb weightbearing will prescribed for a rating of goodstability. Participants will be instructed how to performthe exercises at each level of difficulty, and will beencouraged to increase the difficulty of the exerciseswhen full repetitions are achieved (3 minutes for intrin-sic foot muscles, 3 20 second holds for gluteal mus-cles). Participants will be instructed to perform theexercises daily and record the exercises they completedand their difficulty level in a training diary for the dur-ation of week 2 of the trial. At the end of week 2, theparticipant will attend a thirty minute physiotherapysession to reinforce advice and education, review theexercise program and progress exercises as able. Partici-pants will be instructed to perform the exercises dailyand record the exercises they completed and their diffi-culty level in a training diary for a further 4 weeks. Tocheck exercise progression and encourage compliance,the treating physiotherapist will contact participantsweekly by telephone. At conclusion of the 6 week inter-vention, participants will be encouraged to continue pre-scribed exercises and load management strategies andthis self management will be recorded in follow-up ques-tionnaires at 12, 18, 24 and 30 weeks.
Combined rigid anti-pronation taping and lower limbmuscle trainingParticipants will receive advice and education, be pre-scribed an exercise program and wear rigid ALD taping[25] (Figure 4). At the completion of the baseline out-come measurements, the physiotherapist will provide astandardised information sheet, as described above. Fol-lowing this, ALD taping will be applied using a rigidsports tape (38 mm zinc oxide adhesive, LeukosportBDF) and the appropriate skin checks made and warn-ings given. Participants will be re-taped half way throughweek 1; no advice or education regarding the exerciseswill occur during this session. Participants will beinstructed to remove the tape and any tape residue thenight prior to attending the testing session. At the endof week 1, the participant will attend a thirty minutephysiotherapy session where advice and education will
be reinforced, the ALD tape re-applied and training inthe exercise program commenced. The exercise program
-
Figure 2 Plantar intrinsic foot muscle training. Plantar intrinsic foot muscle training will be performed as described by Mulligan et al. [21].Active intrinsic foot muscle exercises may be commenced in a non-weight bearing sitting position (A). The patient is instructed to increase themedial longitudinal arch by gently supinating the foot and approximating the head of the first metatarsal towards the heel, without flexing thetoes. This position should be held for 5 seconds and then slowly released back to a relaxed state. Patients should aim to perform up to 3 minutesof this exercise daily. Exercises can then be progressed to functional weight bearing positions, for example double-limb stance (B) and single-limbstance (C). For further progression, a small knee bend (D) and/or heel raise (E) can be added to these functional positions.
Figure 3 Hip abductor and external rotator muscle training. For the non-weight bearing and weight bearing exercises, the patient will performa 20 second hold and aim to perform 3 repetitions, daily. The non-weight bearing exercise (A) will be performed in side-lying with the treatment limbuppermost and both limb flexed to 45 at the hip and 90 at the knee. Ideally the patients back and plantar surface of the foot are placed against a wallfor control of position and movement. The patient raises the top limb off the other, such that the hip is in ~30 abduction/external rotation beforereturning to the starting position. The weight bearing exercise (B) is performed with the patient standing side-on to a wall with body rotated slightlyto face into the wall. The leg closest to the wall is flexed at the knee so that the foot is off the ground, and the hip is in neutral flexion/extension. Thefoot of the leg closest to the wall is tucked behind the knee of the outer leg. The standing leg knee should be bent slightly. The patient is instructed tosqueeze the bottom together and hold this throughout the movement, then turn the knee of the standing leg out without moving the foot or pelvis.The bent leg is held against the wall for balance only.
Franettovich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328 Page 5 of 10http://www.biomedcentral.com/1471-2474/15/328
-
niqeewit
Franettovich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328 Page 6 of 10http://www.biomedcentral.com/1471-2474/15/328Figure 4 Rigid anti-pronation taping technique (ALD). The ALD techThe ALD comprises of a low-Dye technique (A) with the addition of thrare anchored to the lower third of the leg. The technique is completedwill include the same two exercises as described above:(i) intrinsic foot muscle exercise, and (ii) hip abductorand external rotator muscle exercise. Participants will beinstructed to perform the exercises daily and recordtheir performances in a training diary for the duration ofweek 2 of the trial. Participants will be re-taped half waythrough week 2; no advice or education regarding theexercises will occur during this session. Participants willbe instructed to remove the tape and any tape residuethe night prior to attending the testing session. At theend of week 2, the participant will attend a thirty minutephysiotherapy session to reinforce advice and education,review the exercise program and progress exercises asable. Participants will be instructed to perform the exer-cises daily and record in a training diary for a further4 weeks. To check progress and encourage compliance,the treating physiotherapist will contact participantsweekly by telephone. No taping will be applied duringthese final 4 weeks of the intervention.
Elastic anti-pronation taping and lower limb muscletrainingParticipants will receive advice and education, be pre-scribed an exercise program and wear an elastic anti-pronation taping [26] (Figure 5). At the completion of thebaseline outcome measurements, the physiotherapist willprovide advice and education regarding the condition and
the malleoli (D).ue will be applied following guidelines previously described [25].reverse-6 techniques (B) and two calcaneal sling techniques (C) thath circumferential lock off strips from the proximal anchor to just aboveload management. Following this, elastic anti-pronationtaping will be applied using an elastic tape (50 mm &75 mm, Beige Dynamic Tape) and the appropriate skinchecks made and warnings given. Participants will bere-taped half way through week 1; no advice or educationregarding the exercises will occur during this session. Par-ticipants will be instructed to remove the tape and anytape residue the night prior to attending the testing ses-sion. At the end of week 1, the participant will attend athirty minute physiotherapy session where advice andeducation will be reinforced, the elastic tape re-appliedand training in the exercise program will commence. Theexercise program will include the same two exercises asdescribed above: (i) intrinsic foot muscle exercise, and (ii)hip abductor and external rotator muscle exercise. Partici-pants will be instructed to perform the exercises daily andrecord their performances in a training diary for the dur-ation of week 2 of the trial. Participants will be re-tapedhalf way through week 2; no advice or education regardingthe exercises will occur during this session. Participantswill be instructed to remove the tape and any tape residuethe night prior to attending the testing session. At the endof week 2, the participant will attend a thirty minutephysiotherapy session to reinforce advice and education,review the exercise program and progress exercises asable. Participants will be instructed to perform the exer-cises daily and record in a training diary for a further
-
Figure 5 Elastic anti-pronation taping technique. The elasticanti-pronation taping technique will be applied following Dynamic Tapeguidelines for the plantar fascia and anti-pronation techniques [26]. Foreach technique a double layer of 50 mm Dynamic Tape will be used.The plantar fascia technique (A) is applied by cutting out a small wedgefrom one end of the double layered tape to allow it to conformto the proximal phalanx of the first toe. With the foot and ankle in fullplantarflexion, inversion, adduction and flexion of the first toe, the tape isapplied from the plantar surface of the first toe, along the medial plantaraspect of the foot, onto the medial aspect of the calcaneus, around thecalcaneus to cross the lateral aspect obliquely, continuing under theplantar aspect of the foot to emerge under the navicular and finallylifting the navicular to anchor the tape on the dorsum of the foot.The anti-pronation technique (B) is then applied with the foot and anklein full dorsiflexion, inversion, and adduction. The double layered tape isapplied from the plantar surface of the foot between the first and secondmetatarsals, courses over the dorsum of the foot from medial to lateral,under the plantar aspect of the foot on a diagonal course to the navicular,lifting the navicular and coursing across the anterior talocural joint toanchor on the lateral aspect of the mid-shin region. The anti-pronationtechnique is then repeated with one layer of 75 mm Dynamic Tape (C).
Franettovich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328 Page 7 of 10http://www.biomedcentral.com/1471-2474/15/3284 weeks. To check progress and encourage compliance, thetreating physiotherapist will contact participants weeklyby telephone. No tape will be applied during these final4 weeks of the intervention.
Outcome measurementsA blinded assessor will perform tests of foot mobilityand other outcome measurements at baseline and then atfollow-up sessions occurring at 1, 2, and 6 weeks. Partici-pants will also be contacted by email or phone to obtainquestionnaire outcome measurements only at 12, 18, 24and 30 weeks. At the completion of the test sessions,assessor blinding will be evaluated via a questionnaire.Biomechanical effectiveness of the intervention will be
evaluated by measuring vertical mobility of the midfoot.These measures will be performed at baseline and thenat follow-up sessions occurring at 1, 2, and 6 weeks. Inaddition to these measurements by the assessor, thetreating physiotherapist will also obtain a measurementof foot mobility before and after each application of tapeto ensure consistency of application of the intervention.Measurement of vertical mobility of the midfoot will beperformed using two custom made platforms and modi-fied callipers with the participant in two positions (i)standing on both feet with equal weightbearing and, (ii)sitting with legs relaxed over the edge of a plinth. Dorsalarch height difference will be calculated by subtractingthe dorsal arch height in standing from the dorsal archheight in non-weight bearing. This measurement hasbeen described in detail previously and demonstrateshigh inter- and intra-rater reliability [15].
Visual Analogue ScaleUsual and worst pain over the preceding week will beobtained using two separate 100 mm visual analoguescales (VAS). The reliability and validity of the VAS iswell established [27]. Each VAS will consist of a 100 mmhorizontal line with the text no pain at the 0 mm markand worst pain imaginable at the 100 mm mark. Partici-pants will be instructed to place a single vertical mark onthe horizontal line that represents the level of their pain.
Foot and Ankle Ability MeasureFunction will be measured using the Foot and AnkleAbility Measure (FAAM) which provides an indicationof participation in usual activities [28]. The FAAM is aset of eight (8) items that are each scored by the partici-pant from 4 to 0, with a score of 4 indicating no diffi-culty with the functional task and 0 indicating that theparticipant is unable to perform the task. Thus, thegreater the FAAM score, the higher the level of function.
The validity, reliability and responsiveness of the FAAMhas been previously demonstrated [28].
-
Franettovich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328 Page 8 of 10http://www.biomedcentral.com/1471-2474/15/328Patient Specific Functional ScaleThe Patient Specific Functional Scale (PSFS) provides amethod for eliciting, measuring and recording descrip-tions of patients disabilities that are most relevant tothem. Participants will be asked to identify up to five (5)important activities that they are having difficulty withor are unable to perform. The current level of difficultyassociated with each activity is then marked on an 11-point scale, where 0 is unable to perform activity and10 is able to perform activity at the same level as beforethe injury or problem. This scale has been shown tohave excellent test-retest reliability, sensitivity to change,and validity [29].
Global perceived effectGlobal perceived effect will be measured with a 6-pointLikert scale with categories: completely recovered, muchimproved, improved, no change, worse and much worse.Such retrospective assessment scales have been shownto be more sensitive to change and more correlated withpatients satisfaction with change than serial assessmentscales that include a baseline measurement, such as theVAS [30]. This outcome measure will be performed ateach of the follow-up sessions, but not at baseline.
Amount of activity performed in the previous weekThe physical activity level of participants will be quantifiedusing a physical activity questionnaire which has previ-ously demonstrated moderate to high reliability [31]. Theparticipant will record the amount of time spent in occu-pational, household, and leisure activities of moderate,hard and very hard intensities during the previous week.The total time for each intensity level of activity is thenmultiplied by the metabolic equivalents of the activitiesand summed to give an overall caloric output. This canthen be standardised to body weight to allow comparisonbetween and within individuals over time.A further questionnaire regarding any adverse re-
sponses and perception of comfort of the taping inter-ventions, as well as whether participants have soughtany treatment outside the study, will be administered atfollow-up sessions at 1, 2 and 6 weeks.
Sample size considerationsSample size calculations [32] indicate that 10 partici-pants per group will be sufficient to detect (i) a clinicallysignificant improvement of 20 mm in pain severity [33]based on a standard deviation of 12.7 mm [34], power of0.80 and alpha level 0.05 and (ii) a clinically significantimprovement of 9 points [28] on the FAAM based on astandard deviation of 26.7 [28], power of 0.80 and alphalevel of 0.05. To account for potential dropout, 15 par-
ticipants per group will be recruited, with a total samplesize of 45.Planned statistical analysisData processing, data entry and data analysis will be per-formed by an assessor who is blinded to group alloca-tion. The primary analysis of the data will be performedon an intention-to-treat basis. SPSS software (version21.0) will be used for statistical procedures. Demo-graphic data, clinical characteristics of pain and physicalactivity level at baseline will be examined for compar-ability across the three intervention groups. To evaluatethe effect of the interventions on pain and function(VAS, FAAM, PSFS, Physical activity level) a two-wayrepeated measure analysis of variance with betweensubject factor of intervention group and within subjectfactor of test session, will be performed. Global perceivedeffect will be dichotomised to either success (completelyrecovered, much improved, improved) or no success(no change, worse, much worse) and expressed as rela-tive risk reduction and numbers needed to treat. For allstatistical procedures age, weight and height will beincluded as covariates and alpha level will be set at 0.05.
DiscussionThis study will be the first randomised controlled trial toevaluate the effectiveness of anti-pronation taping andlower limb muscle training for ERLP. As there is cur-rently a lack of evidence for effective interventions forERLP [11], the results of this study will provide evidenceto inform healthcare providers in the management ofthe condition. For example, if this study identifies oneintervention to be superior to the others, this interven-tion can be recommended in preference to others. Alter-natively, if no differences are identified between thethree intervention groups, then taping would be consid-ered to have no additional benefit over exercise aloneand it would therefore be recommended that clinicianscould focus on exercise alone rather than additionaltaping. An important feature of this study is the inclusionof a follow-up at 12, 18, 24 and 30 weeks. Accordingly, thisstudy will provide an evaluation of both the short and longterm effectiveness of an intervention for ERLP.The three intervention groups evaluated in this study
were selected to target a reported risk factor for the condi-tion (increased foot mobility) as well as to reflect clinicalpractice. Clinical opinion pieces and review articles advo-cate the reduction of pain through relative rest (loadmodification, alternative training), NSAIDS and ice in theacute phase of ERLP, and following this, the commence-ment of strengthening exercises [1,12,13]. Therefore, weselected a lower limb muscle training intervention whichconsisted of advice and education on ERLP and load man-agement, followed by strengthening exercises. For com-parison, we included a combined intervention of taping
and lower limb muscle training. This was selected toreflect a tissue stress model approach to management
-
Franettovich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328 Page 9 of 10http://www.biomedcentral.com/1471-2474/15/328whereby the short term use of external devices (such astaping) is advocated to alleviate tissue stress and thenfollowed by conventional physical therapy modalities suchas muscle strengthening exercises [35,36].The rigid anti-pronation taping technique (ALD) selected
for this randomised controlled trial is a well-establishedand described technique which has previously demon-strated biomechanical effectiveness in ERLP populations. Astrength of this randomised controlled trial is the inclusionof a comparative elastic anti-pronation taping technique.Despite a rapid uptake of these tapes clinically, there is lim-ited evidence as to their biomechanical or clinical efficacy,and specifically, no study has investigated an elastic tapingtechnique in an ERLP population. In addition to evaluatingthe clinical efficacy of the rigid and elastic anti-pronationtaping techniques, this study may also enable somecomparisons to be made between them, including inci-dence of adverse responses and perceptions of comfort.The lower limb muscle training selected for this ran-
domised controlled trial includes two exercises; oneaimed at the plantar intrinsic foot muscle and one aimedat the external rotator and abductor muscles of the hip.Plantar intrinsic foot muscle training was included inthis study as previous evidence has reported effective-ness to influence vertical mobility of the midfoot [21], afactor that has been prospectively identified as a contrib-uting to the development of ERLP [14]. Whilst there isno study to date that has investigated the use of hipexternal rotator and abductor muscle training on footposture or mobility, there is theoretical evidence thatsupports the rationale for its inclusion. Aligning with akinetic chain approach to lower limb function, frontaland transverse plane hip motion has been shown to bestrongly correlated to frontal plane foot motion duringwalking [23,24], and increased navicular drop has alsobeen shown to be related to increased hip internal rota-tion during a single-leg squat [22]. This is supported bythe finding of altered proximal control of gait, specific-ally the gluteus medius (abductor and external rotator ofthe hip), in individuals with ERLP [34]. The non-weightbearing hip rotation exercise was selected because it is arelatively simpler task with less body segments to control.It is also a commonly prescribed exercise for gluteus med-ius clinically and previous fine-wire investigations havereported higher gluteal-to-TFL muscle activation com-pared with other hip exercises [37]. The weight bearingexercise progression was selected to increase complexityand to facilitate relevance to the functional tasks of walk-ing and running. Specifically it was chosen as it closelyresembles the midstance position of these activities and hasbeen used in previous studies to target gluteal strengtheningin other lower limb overuse conditions [38,39].
This randomised controlled trial is registered with
the Australian New Zealand Clinical Trials Registry(ACTRN12613000914763) and will comply with the CON-SORT statement. Previous randomised controlled trials inERLP populations have exhibited high risk of bias [11] andtherefore this study has been designed with considerationto minimise these limitations. Specifically this study designincorporates a random sequence generation and concealedallocation to minimise selection bias, blinding of the out-come assessor to group allocation to minimise detectionbias and blinding of the investigators responsible for dataprocessing and statistical analysis to minimise possible biasassociated with their anticipated outcomes. Unfortunately,due to the nature of the interventions, blinding of par-ticipants and the treating physiotherapist to preventperformance bias is not possible. Finally, to ensure highmethodological quality, outcome measures with estab-lished reliability and validity have been selected. A limi-tation of the methodology is the recruitment of femaleparticipants of less than 40 years of age; therefore theresults of this study may not be generalizable to male and/or older populations with ERLP. This limitation, however,should be considered in light of evidence that femalegender has been reported as a risk factor in ERLP [14] andhigher incidence of ERLP has been reported in bothfemales and the 1840 years age group [2-6,40].
AbbreviationsALD: Augmented low-Dye; ERLP: Exercise related leg pain; FAAM: Foot andAnkle Ability Measure; PSFS: Patient Specific Functional Scale; RR: Relative risk;SMD: Standardised mean difference; VAS: Visual analogue scale.
Competing interestsThe authors declare that they have no competing interests.
Authors contributionsMS conceived the trial and is chief investigator on the research grants. MS, SOand MC planned and designed the trial. MS was responsible for registering thetrial and writing the manuscript. SO and MC edited and reviewed the manuscript.All authors have read and approved the final manuscript.
AcknowledgementsThis study is funded by an Australian Catholic University Health FacultyResearch Grant and Australian Catholic University Early Career ResearcherGrant.
Author details1School of Physiotherapy, Australian Catholic University, Brisbane, Australia.2School of Exercise Science, Australian Catholic University, Brisbane, Australia.
Received: 18 February 2014 Accepted: 19 September 2014Published: 2 October 2014
References1. Reinking MF: Exercise Related Leg Pain (ERLP): a Review of The Literature.
N Am J Sports Phys Ther 2007, 2(3):170180.2. Reinking MF, Hayes AM: Intrinsic factors associated with exercise-related
leg pain in collegiate cross-country runners. Clin J Sports Med 2006,16(1):1014.
3. Willems TM, De Clercq D, Delbaere K, Vanderstraeten G, De Cock A,Witvrouw E: A prospective study of gait related risk factors forexercise-related lower leg pain. Gait Posture 2006, 23(1):9198.4. Yates B, White S: The incidence and risk factors in the development ofmedial tibial stress syndrome among naval recruits. Am J Sports Med2004, 32(3):772780.
-
control in individuals with exercise related leg pain. Med Sci Sports Exerc2010, 42(3):546555.
35. Vicenzino B: Foot orthotics in the treatment of lower limb conditions: amusculoskeletal physiotherapy perspective. Man Ther 2004, 9(4):185196.
36. McPoil TG, Hunt GC: Evaluation and management of foot and ankledisorders: present problems and future directions. J Orthop Sports PhysTher 1995, 21(6):381388.
37. Selkowitz DM, Beneck GJ, Powers CM: Which exercises target the glutealmuscles while minimising activation of the tensor fascia lata?Electromyographic assessment using fine-wire electrodes. J Orthop SportsPhys Ther 2013, 43(2):5464.
38. Vicenzino B, Collins N, Crossley K, Beller E, Darnell R, McPoil T: Foot orthosesand physiotherapy in the treatment of patellofemoral pain syndrome: arandomised clinical trial. BMC Musculoskelet Disord 2008, 9:27.
39. Crossley K, Bennell K, Green S, Cowan S, McConnell J: Physical therapy forpatellofemoral pain - a randomized, double-blinded, placebo-controlledtrial. Am J Sports Med 2002, 30(6):857.
Franettovich Smith et al. BMC Musculoskeletal Disorders 2014, 15:328 Page 10 of 10http://www.biomedcentral.com/1471-2474/15/3285. Bennett JE, Reinking MF, Pluemer B, Pentel A, Seaton M, Killian C:Factors contributing to the development of medial tibial stress syndromein high school runners. J Orthop Sports Phys Ther 2001, 31(9):504510.
6. Sallis RE, Jones K, Sunshine S, Smith G, Simon L: Comparing sports injuriesin men and women. Int J Sports Med 2001, 22(6):420423.
7. Reinking MF, Austin TM, Hayes AM: A survey of exercise-related leg painin community runners. Int J Sports Phys Ther 2013, 8(3):269276.
8. Reinking MF, Austin TM, Hayes AM: Exercise-related leg pain in collegiatecross-country athletes: extrinsic and intrinsic risk factors. J Orthop SportsPhys Ther 2007, 37(11):670/678.
9. Moen MH, Bongers T, Bakker EW, Zimmermann WO, Weir A, Tol JL, Backx FJG:Risk factors and prognostic indicators for medial tibial stress syndrome.Scand J Med Sci Sports 2012, 22(1):3439.
10. Moen MH, Rayer S, Schipper M, Schmikli S, Weir A, Tol JL, Backx FJG:Shockwave treatment for medial tibial stress syndrome in athletes;a prospective controlled study. Br J Sports Med 2012, 46(4):253257.
11. Winters M, Eskes M, Weir A, Moen MH, Backx FJG, Bakker EWP: Treatment ofmedial tibial stress syndrome: a systematic review. Sports Med (Auckland,NZ) 2013, 43(12):13151333.
12. Locke S: Exercise-related chronic lower leg pain. Aust Fam Physician 1999,28(6):569573.
13. Galbraith RM, Lavallee ME: Medial tibial stress syndrome: conservativetreatment options. Curr Rev Musculoskelet Med 2009, 2(3):127133.
14. Newman P, Witchalls J, Waddington G, Adams R: Risk factors associatedwith medial tibial stress syndrome in runners: a systematic review andmeta-analysis. Open Access J Sports Med 2013, 4:229241.
15. McPoil TG, Cornwall MW, Abeler MG, Devereaux KJ, Flood LJ, Merriman SE,Sullivan S, van Der Laan MJ, Villadiego TA, Wilson K: The optimal methodsto assess the vertical mobility of the midfoot: navicular drop versusdorsal arch height difference? Clin Res Foot Ankle 2013, 1:1.
16. Franettovich M, Chapman A, Blanch P, Vicenzino B: A physiological andpsychological basis for anti-pronation taping from a critical review ofthe literature. Sports Med (Auckland, NZ) 2008, 38(8):617631.
17. Franettovich M, Blanch P, Vicenzino B: Initial neuromotor and posturaleffects after continual use of augmented low-Dye taping. Athlet TrainingSports Health Care 2011, 3(1):2128.
18. Franettovich M, Chapman A, Blanch P, Vicenzino B: Continual use ofaugmented low-Dye taping increases arch height in standing but doesnot influence neuromotor control of gait. Gait Posture 2010, 31(2):247250.
19. Franettovich M, Chapman AR, Blanch P, Vicenzino B: Augmented low-Dyetape alters foot mobility and neuromotor control of gait in individualswith and without exercise related leg pain. J Foot Ankle Res 2010, 3:5.
20. Williams S, Whatman C, Hume PA, Sheerin K: Kinesio taping in treatmentand prevention of sports injuries: a meta-analysis of the evidence for itseffectiveness. Sports Med (Auckland, NZ) 2012, 42(2):153164.
21. Mulligan EP, Cook PG: Effect of plantar intrinsic muscle training on mediallongitudinal arch morphology and dynamic function. Man Ther 2013,18(5):425430.
22. Nguyen A-D, Shultz SJ, Schmitz RJ, Luecht RM, Perrin DH: A preliminarymultifactorial approach describing the relationships among lowerextremity alignment, hip muscle activation, and lower extremity jointexcursion. J Athlet Training 2011, 46(3):246256.
23. Barton CJ, Levinger P, Crossley KM, Webster KE, Menz HB: The relationshipbetween rearfoot, tibial and hip kinematics in individuals withpatellofemoral pain syndrome. Clin Biomech 2012, 27(7):702705.
24. Souza TR, Pinto RZ, Trede RG, Kirkwood RN, Fonseca ST: Temporal couplingsbetween rearfoot-shank complex and hip joint during walking. Clin Biomech2010, 25:745748.
25. Franettovich M, Chapman A, Vicenzino B: Tape that increases mediallongitudinal arch height also reduces leg muscle activity: a preliminarystudy. Med Sci Sports Exerc 2008, 40(4):593600.
26. Dynamic tape - The Biomechanical Tape. [http://www.dynamictape.com.au]27. Price DD, McGrath PA, Rafii A, Buckingham B: The validation of visual
analogue scales as ratio scale measures for chronic and experimentalpain. Pain 1983, 17:4556.
28. Martin RL, Irrgang JJ, Burdett RG, Ped C, Conti SF, VanSwearingen JM:Evidence of validity for the Foot and Ankle Ability Measure (FAAM).Foot Ankle Int 2005, 26(11):968983.29. Chatman AB, Hyams SP, Neel JM, Binkley JM, Stratford PW, Schomberg A,Stabler M: The patient-specific functional scale: measurement propertiesin patients with knee dysfunction. Phys Ther 1997, 77(8):820829.40. Orava S, Puranen J: Athletes' leg pains. Br J Sports Med 1979, 13(3):9297.
doi:10.1186/1471-2474-15-328Cite this article as: Franettovich Smith et al.: A comparison of rigid tapeand exercise, elastic tape and exercise and exercise alone on pain andlower limb function in individuals with exercise related leg pain: arandomised controlled trial. BMC Musculoskeletal Disorders 2014 15:328.
Submit your next manuscript to BioMed Centraland take full advantage of:
Convenient online submission
Thorough peer review
No space constraints or color gure charges
Immediate publication on acceptance
Inclusion in PubMed, CAS, Scopus and Google Scholar
Research which is freely available for redistribution30. Fischer D, Stewart AL, Bloch DA, Lorig K, Laurent D, Holman H: Capturingthe patient's view of change as a clinical outcome measure. JAMA 1999,282(12):11571162.
31. Sallis JF, Haskell WL, Wood PD, Fortmann SP, Rogers T, Blair SN, PaffenbargerRSJ: Physical activity assessment methodology in the five-city project.Am J Epidemiol 1985, 121(1):91106.
32. Faul F, Erdfelder E, Lang A-G, Buchner A: G*power 3: a flexible statisticalpower analysis program for the social, behavioural and biomedicalsciences. Behav Res Methods 2007, 29(2):175191.
33. Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W: Minimal clinicallyimportant changes in chronic musculoskeletal pain intensity measuredon a numerical rating scale. Eur J Pain 2004, 8(4):283291.
34. Franettovich M, Chapman AR, Blanch P, Vicenzino B: Altered neuromuscularSubmit your manuscript at www.biomedcentral.com/submit
AbstractBackgroundMethods/DesignDiscussionTrial registration
BackgroundMethodsAimStudy designEligibility criteriaRecruitment of participantsRandomisationInterventionLower limb muscle training aloneCombined rigid anti-pronation taping and lower limb muscle trainingElastic anti-pronation taping and lower limb muscle training
Outcome measurementsVisual Analogue ScaleFoot and Ankle Ability MeasurePatient Specific Functional ScaleGlobal perceived effectAmount of activity performed in the previous week
Sample size considerationsPlanned statistical analysis
DiscussionAbbreviationsCompeting interestsAuthors contributionsAcknowledgementsAuthor detailsReferences
Related Documents