Are There Parallel Processes in Psychotherapy Supervision? An Empirical Examination Terence J. G. Tracey, Jamie Bludworth, and Cynthia E. Glidden-Tracey Arizona State University Parallel processes in supervision occur when (1) the therapist brings the interaction pattern that occurs between the therapist and client into supervision and enacts the same pattern but with the therapist trainee in the client’s role, or (2) the trainee takes the interaction pattern in supervision back into the therapy session as the therapist, now enacting the supervisor’s role. We examined these processes in the interactions of 17 therapy/supervision triads (i.e., supervisor, therapist/trainee, and client). Each session was rated for dominance and affiliation, and the similarity of these dimensions across equal status pairs (supervisor-therapist and trainee-client) was examined. It was hypothesized that if parallel process existed, there would be more similarity in dominance and affiliation between equal status pairs in contiguous sessions than would be true relative to general responses; the dominance and affiliation would be more closely matched than would be expected given general response tendencies. This was examined separately for each supervision triad using single-case randomization tests. Significant results were obtained for each dyad indicating the presence of parallel processes in each supervision triad. Addition- ally, the relation between parallel processes over the course of treatment and client outcome was examined using hierarchical Bayesian modeling. Results indicate that a positive client outcome was associated with increasing similarity of therapist behavior to the supervisor over time on both affiliation and dominance (increasing parallel process) and an inverted U pattern of high-low-high similarity of client behavior to trainee behavior over time. This study provides support for the existence of bidirec- tional parallel processes at the level of interpersonal interaction. Implications for therapist training and supervision are discussed. Keywords: parallel process, supervision, interpersonal behavior, interpersonal circumplex Psychotherapy supervision is a process whereby a clinical super- visor meets with a therapist/trainee to discuss the trainee’s work as a therapist with one or more clients with the goals of helping the client achieve good outcomes and the therapist increase therapeutic skills. Supervision is inherently a triadic process, involving a therapist meet- ing with a client which is then discussed in supervision with a supervisor. Most supervision involves discussion of the therapeutic work of one trainee with several clients, thus forming several triads, each involving the same supervisor and therapist but different clients. Research on the process aspect of therapy is extensive, and there is a growing body of research on the supervision process. However, there is relatively little on the overlap of these two domains and the inherent triadic nature of supervision. Parallel process as a supervision phe- nomenon and its use as a supervision tool are constructs that could be exhibited only in the triad of therapeutic supervision. The focus of the present study was on examining the processes of supervision and therapy conjointly. Specifically we sought to determine whether par- allel processes existed in supervision, and if so their relation to therapy outcome. Parallel process was first proposed in the psychodynamic liter- ature as the unconscious replication of the therapeutic relationship in supervision (Searles, 1955; Ekstein & Wallerstein, 1972). The therapist brings into the supervision session issues that arise in reaction to the client, by recreating the dynamic of the therapy session and enacting the client’s role with the supervisor. The supervisor in turn is then pulled into the role of the therapist, thus recreating the therapeutic relation in supervision but with the person who is both therapist and trainee switching roles from expert to help seeker. This process is considered to involve the underlying issues of power, authority, dependency, intimacy, and evaluation that are common across the master–apprentice relation- ship of supervision and the therapist– client relationship of psy- chotherapy (Doehrman, 1976; Grey & Fiscalini, 1987). Without endorsing unconscious determinants, parallel process is also rec- ognized as an important aspect of supervision in developmental (Loganbill, Hardy, & Delworth, 1987; Stoltenberg & Delworth, 1987) and interactional (Kell & Mueller, 1966; Mueller & Kell, 1972) models of supervision. A survey of both therapists and supervisors demonstrated that parallel process was recognized as part of supervision, and there were no differences in this recogni- tion across theoretical orientation (Raichelson, Herron, Primavera, & Ramirez, 1997). Very few denied its existence, but there were varying definitions of parallel process. This article was published Online First December 19, 2011. Terence J. G. Tracey, Jamie Bludworth, and Cynthia E. Glidden-Tracey, Counseling and Counseling Psychology, Arizona State University. Appreciation is expressed to Monica Adams, Tyler Barratt, Sara Dixon Staley, David Hauser, Jessica Rohlfing, and Brandon Yabko who served as raters in this study. Thanks also to the supervisors, therapists and clients who consented to be part of the study. Correspondence concerning this article should be addressed to Terence J. G. Tracey, 446 Payne Hall, MC-0811, Arizona State University, Tempe, AZ 85287-0811. E-mail: [email protected] Psychotherapy © 2011 American Psychological Association 2012, Vol. 49, No. 3, 330 –343 0033-3204/11/$12.00 DOI: 10.1037/a0026246 330

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Are There Parallel Processes in Psychotherapy Supervision?An Empirical Examination
Terence J. G. Tracey, Jamie Bludworth, and Cynthia E. Glidden-TraceyArizona State University
Parallel processes in supervision occur when (1) the therapist brings the interaction pattern that occursbetween the therapist and client into supervision and enacts the same pattern but with the therapist traineein the client’s role, or (2) the trainee takes the interaction pattern in supervision back into the therapysession as the therapist, now enacting the supervisor’s role. We examined these processes in theinteractions of 17 therapy/supervision triads (i.e., supervisor, therapist/trainee, and client). Each sessionwas rated for dominance and affiliation, and the similarity of these dimensions across equal status pairs(supervisor-therapist and trainee-client) was examined. It was hypothesized that if parallel processexisted, there would be more similarity in dominance and affiliation between equal status pairs incontiguous sessions than would be true relative to general responses; the dominance and affiliation wouldbe more closely matched than would be expected given general response tendencies. This was examinedseparately for each supervision triad using single-case randomization tests. Significant results wereobtained for each dyad indicating the presence of parallel processes in each supervision triad. Addition-ally, the relation between parallel processes over the course of treatment and client outcome wasexamined using hierarchical Bayesian modeling. Results indicate that a positive client outcome wasassociated with increasing similarity of therapist behavior to the supervisor over time on both affiliationand dominance (increasing parallel process) and an inverted U pattern of high-low-high similarity ofclient behavior to trainee behavior over time. This study provides support for the existence of bidirec-tional parallel processes at the level of interpersonal interaction. Implications for therapist training andsupervision are discussed.
Keywords: parallel process, supervision, interpersonal behavior, interpersonal circumplex
Psychotherapy supervision is a process whereby a clinical super-visor meets with a therapist/trainee to discuss the trainee’s work as atherapist with one or more clients with the goals of helping the clientachieve good outcomes and the therapist increase therapeutic skills.Supervision is inherently a triadic process, involving a therapist meet-ing with a client which is then discussed in supervision with asupervisor. Most supervision involves discussion of the therapeuticwork of one trainee with several clients, thus forming several triads,each involving the same supervisor and therapist but different clients.Research on the process aspect of therapy is extensive, and there is agrowing body of research on the supervision process. However, thereis relatively little on the overlap of these two domains and the inherenttriadic nature of supervision. Parallel process as a supervision phe-nomenon and its use as a supervision tool are constructs that could beexhibited only in the triad of therapeutic supervision. The focus of thepresent study was on examining the processes of supervision and
therapy conjointly. Specifically we sought to determine whether par-allel processes existed in supervision, and if so their relation to therapyoutcome.
Parallel process was first proposed in the psychodynamic liter-ature as the unconscious replication of the therapeutic relationshipin supervision (Searles, 1955; Ekstein & Wallerstein, 1972). Thetherapist brings into the supervision session issues that arise inreaction to the client, by recreating the dynamic of the therapysession and enacting the client’s role with the supervisor. Thesupervisor in turn is then pulled into the role of the therapist, thusrecreating the therapeutic relation in supervision but with theperson who is both therapist and trainee switching roles fromexpert to help seeker. This process is considered to involve theunderlying issues of power, authority, dependency, intimacy, andevaluation that are common across the master–apprentice relation-ship of supervision and the therapist–client relationship of psy-chotherapy (Doehrman, 1976; Grey & Fiscalini, 1987). Withoutendorsing unconscious determinants, parallel process is also rec-ognized as an important aspect of supervision in developmental(Loganbill, Hardy, & Delworth, 1987; Stoltenberg & Delworth,1987) and interactional (Kell & Mueller, 1966; Mueller & Kell,1972) models of supervision. A survey of both therapists andsupervisors demonstrated that parallel process was recognized aspart of supervision, and there were no differences in this recogni-tion across theoretical orientation (Raichelson, Herron, Primavera,& Ramirez, 1997). Very few denied its existence, but there werevarying definitions of parallel process.
This article was published Online First December 19, 2011.Terence J. G. Tracey, Jamie Bludworth, and Cynthia E. Glidden-Tracey,
Counseling and Counseling Psychology, Arizona State University.Appreciation is expressed to Monica Adams, Tyler Barratt, Sara Dixon
Staley, David Hauser, Jessica Rohlfing, and Brandon Yabko who served asraters in this study. Thanks also to the supervisors, therapists and clientswho consented to be part of the study.
Correspondence concerning this article should be addressed to TerenceJ. G. Tracey, 446 Payne Hall, MC-0811, Arizona State University, Tempe,AZ 85287-0811. E-mail: [email protected]
Psychotherapy © 2011 American Psychological Association2012, Vol. 49, No. 3, 330–343 0033-3204/11/$12.00 DOI: 10.1037/a0026246
330

The literature examining parallel process relies almost exclu-sively on case examples (e.g., DeLucia, Bowman, & Bowman,1989; McNeil & Worthen, 1989) or formal case studies (Alpher,1991; Doehrman, 1976; Friedlander, Siegel, & Brenock, 1989;Jacobsen, 2007; Lombardo, Greer, Estadt, & Cheston, 1997).However, case studies, even several, beg the question of general-izability. Does parallel process occur for all supervisions, or onlyfor certain select triads?
Given the noted variety of definitions of parallel process, wesought to focus on aspects that were most common across alldefinitions. The issues of power and intimacy have been noted tocharacterize the roles adopted in parallel process (Doehrman,1976; Grey & Fiscalini, 1987). These are the same two dimensionsthat underlie the interpersonal circle (Kiesler, 1983; Wiggins,1979). According to interpersonal theory, all behaviors can becharacterized in terms of the varying amounts displayed on theindependent dimensions of dominance and affiliation, with theinterpersonal circle representing the full range of blendings acrossthese two dimensions. While there is great commonality among thedifferent interpersonal circles, the version used in this study wasproposed by Strong (Strong, Hills, Kilmartin, et al., 1988; Strong,Hills, & Nelson, 1988), and it is presented in Figure 1. Forexample, behaviors high in dominance and moderately highin affiliation/friendliness would be “leading,” and behaviors low indominance (i.e., high in submission), and moderately low infriendliness would be “self-effacing.” The key to the interpersonalcircle is that the various blendings of the two underlying dimen-sions can be spatially represented as a circle, with behaviors closertogether more similar than those more distal.
Furthermore, these behaviors carry information regarding theinteraction desired by each participant (Kiesler, 1983; Tracey,1993). Each behavior is a statement about how the individualviews himself or herself relative to the other. If one person isdominant, the other is expected to respond as submissive to vali-date the relationship expectations of the first. If one acts friendly,the other person is also expected to be friendly in response. Eachinterpersonal behavior thus is an attempt to define how the other isto act: opposite on dominance and similar on affiliation. The extentto which the other participant responds with the behaviors ex-pected by the first is called complementarity, and it is related to
relationship quality (Dryer & Horowitz, 1997) and relationshipproductivity (Estroff & Nowicki, 1992). This model has been usedextensively to study interpersonal behavior in interaction (Strong,Hills, Kilmartin, et al., 1988; Tracey, 1994, 2004, 2005) as well asin therapy contexts (Tracey & Guinee, 1990; Tracey, Sherry, &Albright, 1999) and supervision (Friedlander et al., 1989; Tracey& Sherry, 1993).
In activating parallel process, the levels of dominance andaffiliation demonstrated by the therapist trainee in supervisionwould reflect the interpersonal style and expectations communi-cated by the client. The degree to which the supervisor comple-mented those behaviors demonstrated and expectations communi-cated by the client and reenacted by the therapist/trainee wouldinitially mimic the therapist’s response to the client (e.g., if theclient were cooperative, the complementary therapist would benurturant, or a noncomplementary therapist response would becritical or distrustful). Given the principle of complementarity,the trainee is likely to complement the client’s implicit expecta-tions, behaving in a manner consistent with what the client’sinterpersonal style typically elicits from other people. The therapisttrainee would enact the client’s role in the next supervision sessionwith the supervisor, in the complementary case acting in a morecooperative manner than usual. According to parallel processpredictions, the supervisor would, in response, enact a more nur-turant role than usual, similar to how the therapist trainee re-sponded to the client in the therapy session. So the dominance andaffiliation enacted in therapy would be brought to supervision butwith the roles reversed for the therapist/trainee.
An example of parallel process frequently experienced mayillustrate this process. A client comes into therapy seeking guid-ance because things are not going well in her relationships. Shedesires structure and direction from the therapist (client submissivebehavior). The therapist attempts to help the client by providingguidance (therapist dominant behavior). The client then starts tosee problems with each of the suggestions offered by the therapist(the common “Yes, but. . .” which is “distrustful” on the interper-sonal circle). The therapist over time starts to become subtly“critical,” complementing the behavior of the client. This patterncontinues over time, and the therapist comes into supervisioncomplaining about the client and how the therapist needs help anddirection because nothing is working (trainee increases his sub-missive behavior in parallel enactment of the client). As thesupervisor provides some direction (supervisor increases her dom-inance), the trainee also engages in “Yes, but. . .” (i.e., “distrust-ful” behavior). The supervisor also engages in more “critical”behavior than usual in response. The supervision interaction be-comes a relative replication of the therapy relationship, captured inthe relative amounts of dominance and affiliation exhibited by theparticipants. So parallel processes would be indicated by greatersimilarity between the interpersonal behaviors exhibited by bothparticipants in corresponding roles (help-seeker or expert) acrossthe dyads comprising each supervision triad, compared with eitherparticipant’s more typical behaviors. In other words, parallel pro-cess would be indicated in two similar ways within each supervi-sion triad. With respect to the client and trainee (equivalent help-seeker roles across therapy and supervision dyads), their behaviorsin respective therapy and supervision sessions will be more similarthan either would be to the other’s behavior generalized across allinteractions. For the therapist and supervisor (in equivalent expert
Self-Effacing
Self-Enhancing
Critical
Distrus�ul
Docile
Coopera�ve
Nurturant
Leading
Dominance
Affiliation
Figure 1. Complementarity of Interpersonal Communication RatingScales. Arrows indicate complementary scales. Reprinted from Tracey,T. J. G. (2005). Interpersonal rigidity and complementarity. Journal ofResearch in Personality, 39, 592–614.
331PARALLEL PROCESS

roles across the two dyads comprising one triad), their behaviors inconsecutive sessions will also be more similar than either partic-ipant’s behavior corresponding to that triad, compared with theother participant’s typical behavior across all clients or all trainees,respectively.
Many theorists view parallel process as arising in the therapeuticinteraction and then being transported “up” into supervision (e.g.,Searles, 1955). However, some theorists view the process as bidi-rectional, where not only does the therapist/trainee bring the ther-apy interaction into supervision, but the trainee/therapist alsobrings the supervision interaction back to therapy (Clarkson, 1994;Doehrman, 1976; Jacobsen, 2007). In this view, skillful supervi-sion occurs when the supervisor enacts the parallel of the therapistrole in therapy, but then deliberately alters this pattern in super-vision. This alteration of the pattern by selectively complementingonly certain behaviors of the client (or trainee in the client’s role)provides a model for the therapist to similarly engage in selectivecomplementarity with the client. So the therapist brings the clientinteraction into supervision by adopting the client (help-seeking)role, and the supervisor adopts the therapist (expert) role, thenalters it, helping the therapist then use this deliberate alteration insubsequent therapy interaction to communicate different expecta-tions and elicit alternative behaviors from the client.
Figure 2 depicts the bidirectional pattern of parallel processexamined in this study. The equivalent role of expert is seen asbeing shared by supervisor and therapist within the contexts ofsupervision and therapy, respectively (depicted by the upper arrowpointing from one session to the next consecutive session). Theequivalent role of help-seeker is seen as being shared by client andtrainee within the contexts of therapy and supervision, respectively(depicted by the lower arrow pointing from one session to the nextconsecutive session). Consecutive therapy and supervision ses-sions were coupled together to examine interactional influencefrom the therapy session to the subsequent supervision session(depicted by brackets labeled with numbers). Likewise, consecu-tive supervision and therapy sessions were coupled together toexamine interactional influence from the supervision session to thesubsequent therapy session (depicted by brackets labeled withletters).
The supervision transaction is expected to look increasinglysimilar to the therapy transaction over time if parallel process ispresent. Then if the client is to benefit, the supervisor deliberatelychanges this pattern to selective noncomplementary behavior insupervision, and the therapist learns to then apply it in therapy. Sothis conception of a bidirectional parallel process—where thesupervisor models how to alter an interaction, and the trainee/therapist carries this intentional strategy down to the therapy—suggests a curvilinear pattern of parallel processes being associ-ated over time with positive client outcomes. As the therapistapplies different behavior in the therapy session and the clientresponds, ideally complementing the new alternatives offeredby the therapist, there would be less carry over into the super-vision, and the participants could behave in manners moretypical of their own interpersonal styles and less representativeof the roles carried over from specific previous therapy ses-sions. The goals of this study were to examine the interactionpatterns of many different supervision triads to see if parallelprocesses occur in most, and also to examine whether thecurvilinear pattern of the presence of the parallel processeswould be related to client outcome.
Method
Sample
The sample was composed of 17 supervision triads (supervisor,trainee/therapist, and client) who met over the course of a semesterin a southwestern university counseling training clinic that serveda community population. These triads were composed of 17 clientsmeeting with seven different therapists, who in turn were super-vised by three different supervisors. The clients (13 female and 4male) had a mean age of 32.5 years (SD � 5.5). Thirteen of theclients were White, one was Native American, two were Latino/a,and one was biracial. The self-reported problems of the clientswere depression, interpersonal/relationship difficulties, and anxi-ety. Therapy was conducted by 7 female therapists (2 Latina and5 White) in their first practicum of a master’s degree counselingprogram. Each therapist met with two to three clients who agreed
Figure 2. Depiction of bidirectional parallel process in a supervision triad. Brackets indicate couplings oftherapy and supervision sessions. Numbered couplings represent pattern of influence wherein therapy interac-tions influence subsequent supervision interactions. Lettered couplings represent pattern of influence whereinsupervision interactions influence subsequent therapy interactions.
332 TRACEY, BLUDWORTH, AND GLIDDEN-TRACEY

to participate in the study. There were 3 female supervisors. Onesupervisor (supervisor X) was a White licensed psychologist with16 years of postdoctoral experience including 6 years of conduct-ing therapy and 10 years of supervision experience. This supervi-sor supervised 3 therapists with 3, 3, and 2 clients participating inthe study. The other 2 supervisors were advanced doctoral students(one Native American and one Latina) enrolled in a supervisionpracticum under the direction of the first supervisor. One of thesestudent supervisors (supervisor Y) had 1 trainee with 3 clientsparticipating and another with 2 clients. The other (supervisor Z)had two trainees each with 2 clients participating. All supervisorsendorsed an interpersonal model of psychotherapy, and the practi-cum class was structured along interpersonal theory lines using theTeyber (2006) text as a primary source.
Measures and Variables
Outcome Questionnaire-45. Outcome Questionnaire-45(OQ; Lambert et al., 1996) is 45-item measure of client distressthat was rationally created to assess three areas of distress: Symp-tom Distress, Interpersonal Relations, and Social Role Perfor-mance, as well as Total Distress. Participants respond to each itemusing a 5-point Likert-type format (0 � never, 4 � almost always).For the purpose of this study, only the total score was examined,summing the responses over all the items with higher scoresindicating greater distress. Psychometric properties of the instru-ment have been well supported in the literature (e.g., Bludworth,Tracey, & Glidden-Tracey, 2010; Burlingame, Lambert, Reisinger,Neff, & Mosier, 1995; Lambert et al., 1996; Mueller, Lambert, &Burlingame, 1998; Wells, Burlingame, Lambert, Hoag, & Hope,1996). In the present sample, internal consistency estimates of � �.90 were obtained for client ratings from the first session and � �.96 for client ratings over all sessions.
Interpersonal Communication Rating Scale. InterpersonalCommunication Rating Scale (ICRS, Strong, Hills, & Nelson,1988) is a manualized coding system based on Leary’s (1957)interpersonal circle. The ICRS provides definitions for the ratingof behavior into one of the eight types distributed around theinterpersonal circle (i.e., self-enhancing, critical, distrustful, self-effacing, docile, cooperative, nurturant, and leading), and at one offour levels of extremity. This system has been used extensivelyto study interpersonal behavior in interaction (Strong, Hills,Kilmartin, et al., 1988; Tracey, 1994, 2004, 2005) as well as intherapy contexts (Tracey & Guinee, 1990; Tracey, Sherry, &Albright, 1999). While the ICRS is typically used to ratespeaking turns, it was adapted in this context to provide thestructure with which to rate continuous behavior using thecomputer joystick apparatus.
Computer joystick apparatus and program. A computerjoystick apparatus and program (Sadler et al., 2007) was used torate the moment-by-moment interpersonal interaction of the par-ticipants. Specifically, the rater would push the joystick to thecorresponding section of the interpersonal circle using the ICRSdefinitions. The program would record the movements in twodimensions of dominance and affiliation (�1000 to �1000 units;extreme dominance � 1000, extreme submissiveness � �1000;extreme affiliation � 1000, and extreme hostility � �1000) twotimes every second. This rating was done separately for eachparticipant in a single triad; that is, each rater would use the
joystick to rate statements of only one participant at a time. Themoment–by-moment transcription of dominance and affiliationwas averaged to yield a mean dominance and a mean affiliationscore for each session.
Therapy sessions were rated by four advanced doctoral students.Raters were provided with copies of the ICRS manual and alsogiven practice in using the joystick to rate therapy tapes. Trainingreliability was estimated using a counseling audio tape not in-volved in the study. Each rater independently rated each of theparticipants on the training tape, such that each rater rated eachtape twice, once for the client and again for the therapist. Thepairwise reliability for the sequence ratings over the tape rangedfrom Intraclass Correlation Coefficient (ICC) � .67 to .92 with acollective ICC of .81. This level was judged to be sufficient.
The raters were then given access to the study audiotapes oftherapy sessions and rated one of the participants. Each participantin each tape was rated by at least two of the raters. Because thestudy used the mean dominance and affiliation scores for eachsession, these scores were examined for reliability of rating. Thepairwise ICC reliability estimates over all the study audiotapesranged from .79 to .93 with a collective ICC of .87. To furtherenhance the reliability of the data, we used the means of thedominance and affiliation scores across the raters to represent thedominance and affiliation for each participant for each session. Sofor each therapy session, we obtained the mean levels of clientdominance, client affiliation, therapist dominance, and therapistaffiliation.
Supervision sessions were rated identically but these super-vision sessions were rated by two different advanced doctoralstudents. The reliability for these raters was ICC � .88. Againthe means across the two raters were used as the measures ofsupervisor and trainee dominance and affiliation in this study.Because the trainee and supervisor would discuss several dif-ferent clients in each supervision session, we matched the clientwith the period in the supervision session where he or she wasbeing discussed. As such, the amount and sequencing of dis-cussion for each client could be determined, and this could beeasily matched with the moment-by-moment dominance andaffiliation ratings. In this manner, the mean dominance andmean affiliation ratings for both the supervisor and traineewhen talking about each client could be determined. So for eachclient discussed in each session, we obtained separate meanlevels of trainee dominance, trainee affiliation, supervisor dom-inance, and supervisor affiliation.
Behavioral dissimilarity. As noted, parallel process involvesan increase in behavioral similarity across the similar roles oftrainee with client and therapist with supervisor. To represent thissimilarity, the ratings on each participant of dominance and affil-iation from each therapy session were compared with the scoresfrom the subsequent supervision session segment in which thattherapy dyad was discussed. So for each pair of adjacent sessions,the client’s behavior in the preceding therapy session was com-pared with the trainee’s behavior in the subsequent supervision,and the therapist’s behavior in the preceding therapy session wascompared with the supervisor’s behavior in the subsequent super-vision session. Given that dominance and affiliation are orthogonalcomponents of the interpersonal circle, each was examined sepa-rately, and we used an absolute value of the difference (D) betweenthe either affiliation or dominance behavior scores for triad par-
333PARALLEL PROCESS

ticipants in equivalent roles to calculate behavioral similarity.Hence, the score is really one of dissimilarity, with greater scoresindicating greater differences in the behavior in question. Therewere four absolute value dissimilarity indices calculated: client-trainee dominance D (client dominance in the preceding therapysession minus trainee dominance in the subsequent supervisionsession when talking about the same client), client-trainee affilia-tion D (client affiliation in the preceding therapy session minustrainee affiliation in the subsequent supervision session whentalking about the same client), therapist-supervisor dominance D(therapist dominance in the preceding therapy session minus su-pervisor dominance in the subsequent supervision session whentalking about the same client), and therapist-supervisor affiliationD (therapist affiliation in the preceding therapy session minussupervisor affiliation in the subsequent supervision session whentalking about the same client).
Procedures
The training program where this study was conducted has asupervision practicum experience for the advanced doctoral stu-dents. Under the instructor’s guidance, advanced students super-vise two trainees who then see anywhere from 3 to 5 clients perweek over the span of a semester. At the start of the study,supervisors and supervisors-in-training were approached andasked to participate in a study on the supervision process whichwould involve audio recording their interaction with their trainees.Of the 4 supervisors approached, three agreed. The therapists whoworked with each of the consenting supervisors were then asked toparticipate by allowing their supervision and therapy sessions to beaudio recorded. Of the eight therapists approached, seven agreed toparticipate. Following this step, those clients assigned to theconsenting therapists who were not in major crisis or clearlypathological (as determined in the intake interview) were pro-vided with an information packet detailing participation. Allthat was required of the clients was allowing audio recording ofthe therapy sessions. Of the 38 clients approached, 17 consentedto be part of the study. All clients seen at the center wererequested to complete a symptom checklist (OQ-45) beforeintake and before their last session, regardless of their partici-pation in the study.
Therapy and supervision went on as usual with no experimentalintrusion. Sessions were audio taped and the middle 20 minutesfrom each therapy session were used to rate the behaviors of thetherapist and client as this provided enough data to rate but not toomuch to tax the raters. All supervision sessions were used to ratethe supervisor and trainee. To be included in the study, thereneeded to be audible tapes from contiguous sessions of the therapyand the supervision. If a client came in at the beginning of thesemester and then continued until the end, there could be a max-imum of 12 sessions. Many clients in the study started therapy midway through the semester and thus their number of sessions wascurtailed, and some ended before the end of the semester. Therewere several “holes” in the data set due to missed tapings, inau-dible tapes, or not having audible tapes from both the supervisionand therapy session in the same week (i.e., contiguous). A major-ity of the total possible session data were included in this study(62%), and these were distributed widely over the course oftreatment. There were holes also due to some clients not being
discussed in any given week in supervision. If a client was notdiscussed (or discussed for less than 5 minutes), these sessionsobviously could not be used to calculate the measures for thatclient. So overall, there was an irregular pattern of data acrosstime. However, in general, there were at least 4 paired sessions(supervision and therapy occurring within one week of eachother) for each dyad.
Results
Presence of Parallel Processes
It was hypothesized that parallel process would be indicated bylower dissimilarity (D) scores for each of the four dissimilarityindices within equivalent roles across the two dyads composing ofeach supervision triad relative to the amount of dissimilarity dem-onstrated between the members of the triad generally. We usedeach triad as its own control, looking for lower dissimilarity scoresthan would be demonstrated in a triad if the members acted as theytypically would. This acting in a manner typical across all recordedtransactions is what we defined as chance. Did a particular partic-ipant’s behavior with anyone (generalized across all triads) deviatefrom how the participants in a specific triad usually acted witheach other?
However, to examine this alteration from typical behavior, weneeded to compare the behaviors of each triad with the typicalpattern of behavior for members of that triad generalized across alltriads. The key was an intraindividual comparison. To do this, weadopted a single-case approach where each individual served as hisor her own control. To generate this self-as-control comparison,we used a single-case randomization analysis (Edgington, 1987,pp. 245–249). The patterns of each of the dissimilarity indices overthe course of treatment for each supervision triad were separatelycompared with distributions based on all the permutations of thesession behavior values of a particular individual in that specificrole (or a random sample of 1000 permutations if there were morethan 1000 permutations). As elaborated below, we calculated thedissimilarity indices derived from random pairings of one triadparticipant’s behavior within their shared triad to any behavior ofthe corresponding individual across all sessions recorded for thatindividual. The number of times those many comparison dissim-ilarities (1000 for each participant, in each role) were equal to orlower than the total dominance or affiliation dissimilarity indexobtained for a particular triad served as the numerator, which wasdivided by 1000. This ratio then served as an inferential probabilityvalue (i.e., p).
A crucial issue in the use of randomization tests is that anappropriate comparison distribution be selected (Levin &Wampold, 1999). Because we were testing whether each ofthe supervision dyad participants adjusted his or her behavior tothe behavior of the corresponding participant in the therapy dyad,we selected each participant’s typical behavior as the appropriatecomparison. Supervisor behavior with a specific trainee in discuss-ing a specific client was repeatedly compared with all behaviorsfrom that supervisor (i.e., including behavior discussing this andother clients, as well as behavior with other trainees). So what wetested were behaviors in key segments of sessions relative togeneral behavior patterns. For the trainee in the role of supervisee,the comparisons were behaviors demonstrated with the same su-
334 TRACEY, BLUDWORTH, AND GLIDDEN-TRACEY

pervisor, but in talking about all clients (both the same and otherclients). For the trainee in the role of therapist, the multiplecomparisons were made to all therapist behaviors demonstratedacross all participating clients. Finally, for the client, the compar-isons were drawn from all the behaviors demonstrated by all theparticipating clients seen by the therapist in the triad of interest. Inorder to use each person in the study as her or his own controlcompared with that same participant’s behavior of interest withineach triad of participation, these sets of multiple comparisons ofdissimilarities of dominance and affiliation behavior within andacross triads were conducted for every coupling of equivalent rolepairs across every supervision triad we studied.
To illustrate this randomization process, the client-trainee dis-similarity test will be described. Since this test is done separatelyfor each triad, the example of supervisor X meeting with therapistA, who met with client #1 will be used. The dominance dissimi-larity (D) indices for client (#1)-trainee (A) were calculated foreach of the five therapy and supervision sessions that were re-corded for this triad. The mean client-trainee dominance D wasthen calculated across the 5 sessions. This mean was then com-pared with the random distribution of all recorded and ratedbehaviors for that client-trainee pair. However, there were twoconceivable random distributions in this example, one based onclient behavior, the other on trainee behavior across all triads ofparticipation.
First, the client dominance ratings for each of the five sessionswere compared with the trainee dominance scores from five ran-domly drawn supervision sessions involving the same traineediscussing any client. We then calculated the mean client-traineedominance D from this pairing of the actual client with the randomtrainee behaviors. This procedure was repeated 1000 times (with-out replacement) thus providing a distribution of the mean dissim-ilarities between the client and random trainee behaviors againstwhich the actual client-trainee dissimilarity data for this triad couldbe compared. The number of times that the mean dissimilarityfrom the random data matched or was lower than the real data,divided by 1000, provided the probability value for the actualdominance data deviating from chance. A similar set of tests wasdone by calculating comparison dissimilarity indices, keeping thetrainee behavior constant and varying the client data. In this secondset of analyses on the same pair, the actual client dominance scoreover the five sessions was compared with five randomly drawntherapy sessions within this triad using the pool of all sessionsinvolving all the participating clients seen across all triads by thistherapist (therapist A). The mean dissimilarity was calculated forthis random pairing, and the process was repeated 999 more times.The number of times that the real mean dissimilarity was matchedor was lower in the random sample divided by 1000 yielded theprobability of actual deviating from chance.
So in this extended example with one equivalent roles pairwithin one triad, there were two randomization tests applied toeach dissimilarity index. This pattern of two tests for eachsupervision triad was replicated for each of the four dissimilar-ity indices (affiliation and dominance dissimilarities for client-trainee and therapist-supervisor pairs). So across the samplethere were two separate randomization tests on each of the fourdissimilarity indices calculated for each supervision triad, andthese were conducted separately (N � 1) for each equivalent
roles pair by interpersonal type within each client-therapist-supervisor triad.
The results of these tests are summarized in Table 1 for thedominance indices, and in Table 2 for the affiliation indices. Thetables summarize the equivalent roles being examined (therapistwith supervisor, or client with trainee) for each supervision triadand the comparison sets of this randomization test (varying ther-apist or supervisor in the therapist with supervisor comparison, oralternatively varying client or trainee in the client with traineecomparison). In addition, the tables summarize the mean dissim-ilarity D obtained using the actual data specific interactions amongthat triad, as well as the Random D (the mean dissimilarityobtained using the random permutations), and the p value of therandomization test.
As can be seen from Table 1, each comparison of the dominanceD and corresponding Random D indices was significant. Thedominance dissimilarity indices for each behavior-in-role compar-ison within a specific triad was significantly lower than expectedby chance in every case. So the dominance behavior of a particularclient and trainee in each week was more similar (i.e., less dis-similar) compared with either the dominance from the same traineein general across clients, or with the behavior of all clients inter-acting with the same therapist. There was clear parallel processwith each dyad in both role pairings for dominance.
Identical results were obtained when looking at affiliation be-haviors (Table 2). All tests were significant. For both dominanceand affiliation, there is a clear pattern characterized by the traineebehaving in supervision in ways that resemble more the client’sbehavior in the preceding therapy session compared with thetrainee’s behavior in general. There is also a pattern of the super-visor’s behavior matching the therapist’s behavior in the precedingtherapy session. While the absolute magnitude of the matching ofaffiliation and dominance between the equivalent roles variedappreciably across the different triads, the same relative pattern ofadapting interaction in a parallel manner was supported.
Relation of Parallel Process to Client Outcome
Based on theory (Doehrman, 1976; Kell & Mueller, 1966), weanticipated that there would be a curvilinear pattern, whereby thetherapist trainee brings in the dynamics of the therapist-clientinteraction into the earlier supervision sessions, and then the su-pervisor helps the trainee change this pattern which is then broughtdown to the later interactions of therapist and client. However,before examining this pattern, we reversed the association ofbehavior to take account of the bidirectional nature of supervision(Jacobsen, 2007). Instead of looking at the match between thepreceding therapy session and the subsequent supervision sessionas we did above, we reversed the direction by looking at the matchof the preceding supervision session with the subsequent therapysession to capture the pattern of the supervision leading to changein the subsequent therapy session. To represent this switch intemporal ordering, we reversed the role names. So instead ofreferring to therapist-supervisor dissimilarity (where we focusedon how much the supervisor matches the therapist’s behavior fromthe previous therapy session as given earlier), we adopted the termsupervisor-therapist dissimilarity to represent the amount of ther-apist dissimilarity in the therapy session from the behavior of thesupervisor in the previous supervision session. We also switched
335PARALLEL PROCESS

Table 1Summary of Randomization Tests on Dominance Dissimilarity (D) Across Each Supervision Triad
Therapist Client N
Comparison
Ses equivalent roles Distribution D Random D p
Supervisor XA 1 5 Therapist–supervisor Therapist 50.7 159.3a .009
Supervisor 50.7 199.1b .001Client–trainee Client 84.6 210.3c .001
Trainee 84.6 182.0d .001A 2 5 Therapist–supervisor Therapist 47.8 118.5 .011
Supervisor 47.8 152.6 .001Client–trainee Client 70.7 172.0 .002
Trainee 70.7 155.9 .003B 3 5 Therapist–supervisor Therapist 32.9 188.0 .024
Supervisor 32.9 173.5 .008Client–trainee Client 41.3 144.4 .010
Trainee 41.3 176.7 .001B 4 5 Therapist–supervisor Therapist 43.3 317.2 .015
Supervisor 43.3 263.5 .007Client–trainee Client 132.3 288.1 .001
Trainee 132.3 325.2 .008B 5 7 Therapist–supervisor Therapist 79.6 185.2 .043
Supervisor 79.6 221.9 .009Client–trainee Client 102.7 311.5 .003
Trainee 102.7 252.7 .001C 6 7 Therapist–supervisor Therapist 19.5 209.7 .021
Supervisor 19.5 188.3 .008Client–trainee Client 35.2 216.7 .002
Trainee 35.2 175.0 .001C 7 4 Therapist–supervisor Therapist 190.6 300.5 .030
Supervisor 190.6 257.3 .001Client–trainee Client 50.8 187.6 .041
Trainee 50.8 210.7 .001C 8 6 Therapist–supervisor Therapist 175.4 325.2 .012
Supervisor 175.4 277.4 .021Client–trainee Client 11.7 146.7 .005
Trainee 11.7 192.6 .001
Supervisor Y
D 9 8 Therapist–supervisor Therapist 132.3 288.5 .011Supervisor 132.3 243.2 .015
Client–trainee Client 223.7 321.7 .001Trainee 223.7 342.6 .001
D 10 6 Therapist–supervisor Therapist 141.6 295.6 .031Supervisor 141.6 274.0 .001
Client–trainee Client 337.9 445.6 .005Trainee 337.9 469.0 .001
E 11 7 Therapist–supervisor Therapist 40.7 221.3 .022Supervisor 40.7 199.7 .016
Client–trainee Client 91.0 217.6 .001Trainee 91.0 238.9 .001
E 12 7 Therapist–supervisor Therapist 46.7 167.9 .026Supervisor 46.7 212.5 .018
Client–trainee Client 88.2 245.6 .001Trainee 88.2 322.7 .010
E 13 7 Therapist–supervisor Therapist 62.7 248.3 .036Supervisor 62.7 197.7 .014
Client–trainee Client 182.3 330.9 .001Trainee 182.3 297.3 .031
Supervisor Z
F 14 9 Therapist–supervisor Therapist 24.2 245.3 .013Supervisor 24.2 164.5 .006
Client–trainee Client 102.6 200.1 .011Trainee 102.6 188.7 .001
336 TRACEY, BLUDWORTH, AND GLIDDEN-TRACEY

the naming of trainee-client dissimilarity in a similar manner tohelp clarify the order of events (i.e., matching of client behaviorsto the previous trainee behaviors in supervision.).
To detect any relation between the presence of parallel processand therapy outcome, we used the OQ-45 total scores from the firstand last sessions as indicators of outcome. Specifically we used asoutcome scores the residual gain score in the client post OQ-45after taking account of the client pre OQ-45 score. Lower valuesindicated less distress and thus a better outcome. This residual gainscore was the criterion in a multilevel model (i.e., hierarchicallinear model) of the dissimilarity indices over the course of treat-ment. We examined the four dissimilarity indices (the 2 interper-sonal behaviors of dominance and affiliation � 2 equivalent rolecomparisons of trainee with client and supervisor with therapist)separately as they varied over treatment. This was accomplishedby looking at the intercept (overall level association with out-come), linear trend (rising or lowering pattern of interpersonalsimilarity over time being associated with outcome), and thecurvilinear trend (a pattern of rising and lowering being associatedwith the outcome).
The ideal model for use in this investigation would have been afour-level hierarchical linear growth curve model, with sessioninteraction at level 1, dyad (with outcome) at level 2, therapist atlevel 3, and supervisor at level 4. However there were not enoughdata to support this model as there were only 17 dyads, 7 thera-pists, and 3 supervisors. We sought a simplified model, thereforewe examined three-level models with either therapist or supervisoras the top level, using HLM (Raudenbush, Bryk, & Congdon,2004). In each examination, the variance of the top level (eithertherapist or supervisor) was not significant; however, the power ofthis test is low due to the sample size. An examination of the ICCreliability estimates showed that the ICCs were all very low for thesupervisor level (ranging from .001 to .05) but more substantial forthe therapist level (ranging from .10 to .18). The low values for thesupervisor level indicated that there was not much variance at thislevel, and that it could be deleted. The ICCs at the therapist levelindicated that this level needed to be included.
However examining such a small data set using HierarchicalLinear Modeling (HLM) would result in tests of extremely low
power and thus questionable value. To obviate this, we adopted aBayesian estimation of the three-level hierarchical model usingMonte Carlo Markov Chain analysis (e.g., Gelman, Carlin, Stem,& Rubin, 1995; Ntzoufras, 2009) as implemented in the WinBugssoftware program. As Draper (1995) demonstrated, this Bayesianapproach is superior to typical HLM approaches in that the manyissues related to maximum likelihood estimation are avoided. It isalso very amenable to small sample sizes and levels with fewobjects (as is true in the present case). This approach fits aBayesian model to the data, and then creates data sets which arethen recreated using the output as input for the next iteration (in aMarkov Chain manner). With many iterations, the data reach anequilibrium point which indicates stable parameter estimates, aswell as estimates of precision (95% confidence bands). Generally,because this iterative Markov Chain process relies upon priordistributions, which typically are unknown, the estimates fromearly iteration tend to show great variability. To avoid reliance onthese poor initial estimates, a “burn in” number of iterations isoften used to start the process, but these burn in iterations arediscarded and not used as estimates of the model. In our analysis,a separate analysis was conducted on each of the four differenttypes of dissimilarity indices using a three-level hierarchical model(identical to one that would have been examined in HLM) with aburn in period of 1000 iterations and an analysis period of the next2000 iterations.
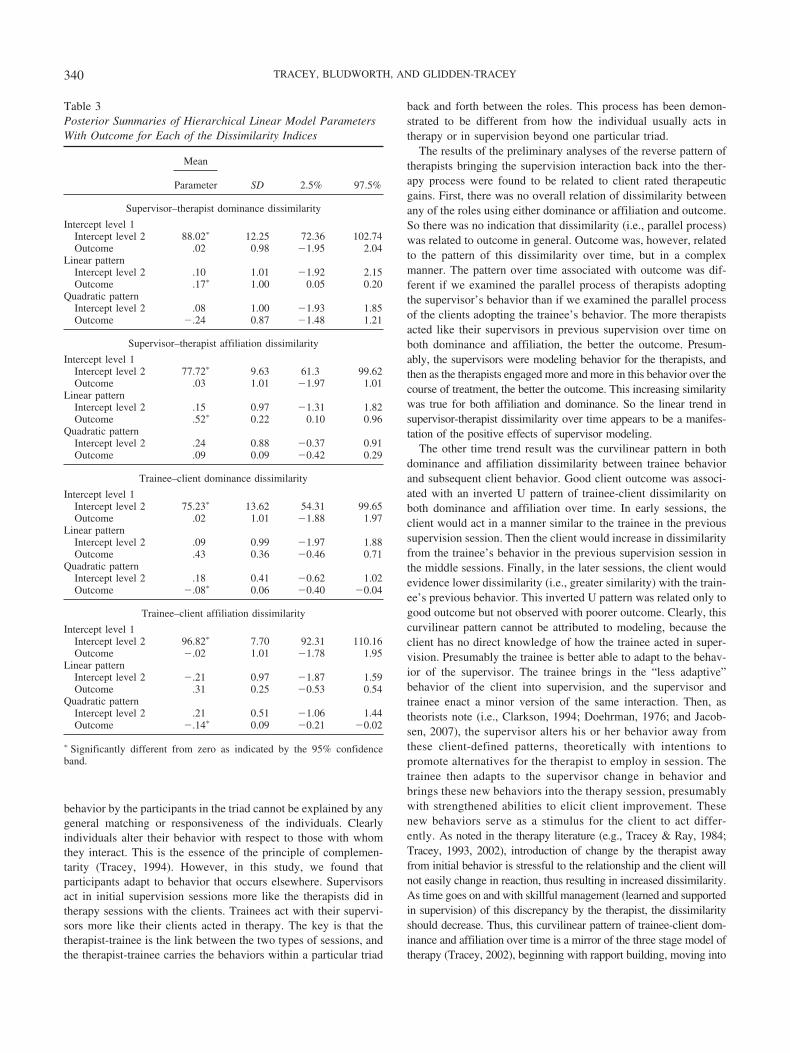
The results of the Bayesian hierarchical modeling are summa-rized in Table 3. Of interest were the terms that included theoutcome variable, because they tested variance in the pattern of thedissimilarity index as related to outcome. For the supervisor-therapist dominance D, there was a significant relation for theoutcome x linear pattern (parameter � .17; 95% band .05 to .20),indicating that better outcome (lower residual score) was associ-ated with lower dissimilarity (i.e., greater similarity) in supervisor-therapist dominance over time. Over time, the more the therapistacted like the supervisor did in the previous supervision session ondominance, the better the therapy outcome. None of the otherterms (except the overall intercept) were different from zero,including the hypothesized curvilinear terms.
Table 1 (continued)
Therapist Client N
Comparison
Ses equivalent roles Distribution D Random D p
F 15 3 Therapist–supervisor Therapist 21.0 145.6 .025Supervisor 21.0 21.99 .008
Client–trainee Client 30.7 157.6 .020Trainee 30.7 192.3 .010
G 16 6 Therapist–supervisor Therapist 50.4 188.8 .008Supervisor 50.4 225.5 .001
Client–trainee Client 105.1 310.0 .005Trainee 105.1 221.2 .001
G 17 7 Therapist–supervisor Therapist 33.0 172.3 .022Supervisor 33.0 205.4 .014
Client–trainee Client 81.7 191.7 .008Trainee 81.7 209.8 .001
a Mean dominance dissimilarity between therapist and supervisor when using random selection of therapist session values. b Mean dominancedissimilarity between therapist and supervisor when using random selection of supervisor session values. c Mean dominance dissimilarity between clientand trainee when using random selection of client session values. d Mean dominance dissimilarity between client and trainee when using random selectionof trainee session values.
337PARALLEL PROCESS

Table 2Summary of Randomization Tests on Affiliation Dissimilarity (D) Across Each Supervision Triad
Therapist Client N
Comparison
Ses equivalent roles Distribution D Random D p
Supervisor XA 1 5 Therapist–supervisor Therapist 20.3 162.3a .031
Supervisor 20.3 217.4b .004Client–trainee Client 10.7 225.6c .010
Trainee 10.7 177.2d .007A 2 5 Therapist–supervisor Therapist 120.5 189.7 .022
Supervisor 120.5 247.6 .019Client–trainee Client 8.7 187.2 .012
Trainee 8.7 245.6 .001B 3 5 Therapist–supervisor Therapist 88.7 221.3 .021
Supervisor 88.7 312.4 .001Client–trainee Client 175.9 337.0 .013
Trainee 175.9 315.2 .001B 4 5 Therapist–supervisor Therapist 91.6 234.2 .021
Supervisor 91.6 287.6 .036Client–trainee Client 145.4 322.7 .015
Trainee 145.4 289.7 .001B 5 7 Therapist–supervisor Therapist 185.3 287.2 .022
Supervisor 185.3 259.0 .029Client–trainee Client 56.0 189.7 .001
Trainee 56.0 224.3 .001C 6 7 Therapist–supervisor Therapist 57.6 197.2 .005
Supervisor 57.6 205.6 .001Client–trainee Client 39.7 225.7 .009
Trainee 39.7 186.2 .001C 7 4 Therapist–supervisor Therapist 99.2 321.2 .013
Supervisor 99.2 247.3 .001Client–trainee Client 91.3 298.2 .020
Trainee 91.3 267.3 .001C 8 6 Therapist–supervisor Therapist 15.4 211.3 .001
Supervisor 15.4 187.7 .031Client–trainee Client 305.6 425.2 .001
Trainee 305.6 381.2 .017
Supervisor Y
D 9 8 Therapist–supervisor Therapist 27.3 282.7 .001Supervisor 27.3 262.3 .001
Client–trainee Client 297.4 387.2 .031Trainee 297.4 426.7 .042
D 10 6 Therapist–supervisor Therapist 57.6 187.7 .001Supervisor 57.6 221.6 .001
Client–trainee Client 126.7 312.2 .005Trainee 126.7 252.3 .001
E 11 7 Therapist–supervisor Therapist 30.3 243.7 .001Supervisor 30.3 262.7 .001
Client–trainee Client 40.9 197.6 .012Trainee 40.9 228.9 .001
E 12 7 Therapist–supervisor Therapist 57.7 142.3 .019Supervisor 57.7 133.5 .021
Client–trainee Client 44.6 222.5 .001Trainee 44.6 182.7 .001
E 13 7 Therapist–supervisor Therapist 72.0 191.1 .016Supervisor 72.0 223.8 .010
Client–trainee Client 112.4 210.1 .001Trainee 112.4 189.7 .011
Supervisor Z
F 14 9 Therapist–supervisor Therapist 67.8 217.2 .001Supervisor 67.8 187.5 .030
Client–trainee Client 47.3 167.2 .009Trainee 47.3 221.2 .001
F 15 3 Therapist–supervisor Therapist 46.7 188.7 .012Supervisor 46.7 145.6 .001
338 TRACEY, BLUDWORTH, AND GLIDDEN-TRACEY

The results of the supervisor-therapist affiliation dissimilaritymirrored those of supervisor-therapist dominance. The primarysignificant result was the outcome by linear pattern term (param-eter � .52; 95% band .10 to .96). For supervisor-therapist affili-ation, the more the therapist acted in a manner similar to thesupervisor over time, the better the client outcome. As demon-strated earlier, none of the other terms except the trivial overallintercept term were different from zero. The linear trend by out-come relation shows that better outcome is associated with lowerdissimilarity on both affiliation and dominance over time.
For trainee-client dominance dissimilarity, the only substantiveterm that was significant was the quadratic trend by outcomeinteraction term (parameter � �.08; 95% band �.40 to �.04).There was an inverted U relation of dominance dissimilarity withoutcome, indicating that better outcome was associated with lowclient-trainee dissimilarity in the beginning and then increasingdissimilarity toward the middle and then decreasing at the end.Poorer outcome did not manifest this low, high, low pattern ofdominance dissimilarity. There was no linear pattern for trainee-client dominance with outcome as there was for supervisor-therapist dominance dissimilarity.
The results for trainee-client affiliation dissimilarity were iden-tical to those of the trainee-client dominance dissimilarity. Thequadratic pattern by outcome term was significantly different fromzero (parameter � �.14; 95% band �.21 to �.02). The invertedU pattern of trainee-client affiliation dissimilarity was associatedwith better outcome. There was no linear pattern of dissimilarityover time being related to outcome for the trainee-client affiliationdissimilarity either. So better outcome is associated with the in-verted U pattern of dissimilarity between the trainee and clientbehaviors for both affiliation and dominance.
Overall each of the tested dissimilarity indices was to some degreeassociated with client outcome, suggesting parallel processes, but thepatterns were varied across roles. Improved client outcomes wereassociated with a decreasing linear trend of supervisor-therapist dis-similarity over time (i.e., increasing similarity) on both dominanceand affiliation, and also with an inverted U trend of trainee-clientdominance and affiliation dissimilarity over time.
Discussion
The results of this study provide convincing support for thepresence of parallel processes in supervision where it was exam-ined independently in 17 different individual supervision triads.For each of the replicated single-case examinations, we foundsignificant evidence that participants altered their behavior fromtheir own general patterns in line with what would be predicted bythe theory of parallel processes in supervision. Therapists in therole of trainee altered their behavior away from their usual insupervision to act somewhat more like particular clients did in theprevious therapy session. This was also true for the supervisors,who would act somewhat like the therapists in the previous therapysessions with those particular clients. This pattern for therapist andsupervisor was found for both dominance and affiliation. So if aclient tended to act in a distrustful and self-effacing manner(submissive-critical) in the prior session and the therapist comple-mented this by acting in a critical manner in therapy, then thetherapist in the role of trainee would enact some of the distrustfulclient behavior in the subsequent supervision session. The super-visor would also demonstrate this parallel process by acting in amanner similar to how the therapist acted in the previous therapysession; in this example, the supervisor would become more crit-ical than typical. This is clear evidence for parallel process insupervision. Therapists bring the therapy interaction into supervi-sion and engage the supervisor into reenacting this process.
It is important to realize we focused only on changes in thepresence of dominance and affiliation behaviors, not their overallvalue. This means that we did not hypothesize or test that parallelprocess signifies that an individual would exactly match the be-havior of the other. If the therapist was acting in a hostile mannerin the session, our examination of parallel process does not meanthat the supervisor will adopt this same hostile manner in super-vision. We hypothesized therapists and supervisors acting in theirtypical manner but with minor shifts in their behavior in responseto the presentation of the other participant in the immediate inter-action, influenced also by transactions with other triad participantsin coupled sessions. Hence, the behavior changes are more subtleand nuanced, a matter of degree only. Further this shifting of
Table 2 (continued)
Therapist Client N
Comparison
Ses equivalent roles Distribution D Random D p
Client–trainee Client 37.5 233.4 .021Trainee 37.5 177.2 .001
G 16 6 Therapist–supervisor Therapist 18.9 149.7 .010Supervisor 18.9 230.0 .001
Client–trainee Client 50.6 194.2 .005Trainee 50.6 148.4 .018
G 17 7 Therapist–supervisor Therapist 66.4 186.4 .024Supervisor 66.4 201.7 .031
Client–trainee Client 11.1 145.6 .001Trainee 11.1 238.2 .001
a Mean affiliation dissimilarity between therapist and supervisor when using random selection of therapist session values. b Mean affiliation dissimilaritybetween therapist and supervisor when using random selection of supervisor session values. c Mean affiliation dissimilarity between client and traineewhen using random selection of client session values. d Mean affiliation dissimilarity between client and trainee when using random selection of traineesession values.
339PARALLEL PROCESS
behavior by the participants in the triad cannot be explained by anygeneral matching or responsiveness of the individuals. Clearlyindividuals alter their behavior with respect to those with whomthey interact. This is the essence of the principle of complemen-tarity (Tracey, 1994). However, in this study, we found thatparticipants adapt to behavior that occurs elsewhere. Supervisorsact in initial supervision sessions more like the therapists did intherapy sessions with the clients. Trainees act with their supervi-sors more like their clients acted in therapy. The key is that thetherapist-trainee is the link between the two types of sessions, andthe therapist-trainee carries the behaviors within a particular triad
back and forth between the roles. This process has been demon-strated to be different from how the individual usually acts intherapy or in supervision beyond one particular triad.
The results of the preliminary analyses of the reverse pattern oftherapists bringing the supervision interaction back into the ther-apy process were found to be related to client rated therapeuticgains. First, there was no overall relation of dissimilarity betweenany of the roles using either dominance or affiliation and outcome.So there was no indication that dissimilarity (i.e., parallel process)was related to outcome in general. Outcome was, however, relatedto the pattern of this dissimilarity over time, but in a complexmanner. The pattern over time associated with outcome was dif-ferent if we examined the parallel process of therapists adoptingthe supervisor’s behavior than if we examined the parallel processof the clients adopting the trainee’s behavior. The more therapistsacted like their supervisors in previous supervision over time onboth dominance and affiliation, the better the outcome. Presum-ably, the supervisors were modeling behavior for the therapists, andthen as the therapists engaged more and more in this behavior over thecourse of treatment, the better the outcome. This increasing similaritywas true for both affiliation and dominance. So the linear trend insupervisor-therapist dissimilarity over time appears to be a manifes-tation of the positive effects of supervisor modeling.
The other time trend result was the curvilinear pattern in bothdominance and affiliation dissimilarity between trainee behaviorand subsequent client behavior. Good client outcome was associ-ated with an inverted U pattern of trainee-client dissimilarity onboth dominance and affiliation over time. In early sessions, theclient would act in a manner similar to the trainee in the previoussupervision session. Then the client would increase in dissimilarityfrom the trainee’s behavior in the previous supervision session inthe middle sessions. Finally, in the later sessions, the client wouldevidence lower dissimilarity (i.e., greater similarity) with the train-ee’s previous behavior. This inverted U pattern was related only togood outcome but not observed with poorer outcome. Clearly, thiscurvilinear pattern cannot be attributed to modeling, because theclient has no direct knowledge of how the trainee acted in super-vision. Presumably the trainee is better able to adapt to the behav-ior of the supervisor. The trainee brings in the “less adaptive”behavior of the client into supervision, and the supervisor andtrainee enact a minor version of the same interaction. Then, astheorists note (i.e., Clarkson, 1994; Doehrman, 1976; and Jacob-sen, 2007), the supervisor alters his or her behavior away fromthese client-defined patterns, theoretically with intentions topromote alternatives for the therapist to employ in session. Thetrainee then adapts to the supervisor change in behavior andbrings these new behaviors into the therapy session, presumablywith strengthened abilities to elicit client improvement. Thesenew behaviors serve as a stimulus for the client to act differ-ently. As noted in the therapy literature (e.g., Tracey & Ray, 1984;Tracey, 1993, 2002), introduction of change by the therapist awayfrom initial behavior is stressful to the relationship and the client willnot easily change in reaction, thus resulting in increased dissimilarity.As time goes on and with skillful management (learned and supportedin supervision) of this discrepancy by the therapist, the dissimilarityshould decrease. Thus, this curvilinear pattern of trainee-client dom-inance and affiliation over time is a mirror of the three stage model oftherapy (Tracey, 2002), beginning with rapport building, moving into
Table 3Posterior Summaries of Hierarchical Linear Model ParametersWith Outcome for Each of the Dissimilarity Indices
Mean
SD 2.5% 97.5%Parameter
Supervisor–therapist dominance dissimilarity
Intercept level 1Intercept level 2 88.02� 12.25 72.36 102.74Outcome .02 0.98 �1.95 2.04
Linear patternIntercept level 2 .10 1.01 �1.92 2.15Outcome .17� 1.00 0.05 0.20
Quadratic patternIntercept level 2 .08 1.00 �1.93 1.85Outcome �.24 0.87 �1.48 1.21
Supervisor–therapist affiliation dissimilarity
Intercept level 1Intercept level 2 77.72� 9.63 61.3 99.62Outcome .03 1.01 �1.97 1.01
Linear patternIntercept level 2 .15 0.97 �1.31 1.82Outcome .52� 0.22 0.10 0.96
Quadratic patternIntercept level 2 .24 0.88 �0.37 0.91Outcome .09 0.09 �0.42 0.29
Trainee–client dominance dissimilarity
Intercept level 1Intercept level 2 75.23� 13.62 54.31 99.65Outcome .02 1.01 �1.88 1.97
Linear patternIntercept level 2 .09 0.99 �1.97 1.88Outcome .43 0.36 �0.46 0.71
Quadratic patternIntercept level 2 .18 0.41 �0.62 1.02Outcome �.08� 0.06 �0.40 �0.04
Trainee–client affiliation dissimilarity
Intercept level 1Intercept level 2 96.82� 7.70 92.31 110.16Outcome �.02 1.01 �1.78 1.95
Linear patternIntercept level 2 �.21 0.97 �1.87 1.59Outcome .31 0.25 �0.53 0.54
Quadratic patternIntercept level 2 .21 0.51 �1.06 1.44Outcome �.14� 0.09 �0.21 �0.02
� Significantly different from zero as indicated by the 95% confidenceband.
340 TRACEY, BLUDWORTH, AND GLIDDEN-TRACEY

conflict exploration, and ending with resolution and relationship clo-sure.
The results of this study support the bidirectional nature ofparallel processes depicted in Figure 2 and discussed in theliterature (Clarkson, 1994; Doehrman, 1976; Jacobsen, 2007).We found that therapists brought the dominance and affiliationinteraction pattern from therapy into supervision in the role oftrainee acting like client. Our results of the separate random-ization tests strongly support this first direction of parallelprocesses. Then our study supports the presence of a seconddirection of parallel process through examination of the extentto which trainees brought the pattern of dominance and affili-ation in supervision back into the therapy in the role of therapistacting like the supervisor. We found a significant relationship ofthis direction of parallel process with successful therapy outcome. Thelink was the therapist/trainee. Theoretically, the therapist is the me-dium of this process as he or she brings the therapy interaction process“up” into supervision and then brings the supervision interactionprocess “down” into therapy.
In their model of supervision, Stoltenberg and Delworth (1987)focus on the developmental level of the trainee. They proposed thatparallel process may occur in supervision with any level of trainee,but that it might be most pronounced in supervision involvingmore novice supervisors because the more novice supervisorswould be more prone to identify with the therapist consideringthere are fewer developmental differences between them. Thiscould account for the strength of our results with respect to thepresence of parallel process because two of our 3 supervisors werenovice supervisors enrolled in a supervision practicum. However,we still found strong presence of parallel process with our thirdsupervisor who had more than 10 years of supervision experience.So while the developmental level of some of the supervisors mayhave magnified the presence of parallel process, our results stillsupport its presence in general. Future research will further explorethe differences in parallel processes across supervisor develop-mental level.
This study is noteworthy in that it is the only one that examinesmore than one supervision triad. We recorded, rated, and analyzedinteractions of 17 triads. The amount of data coded and thenanalyzed was very large, and given the complexities involved, it isnot surprising that there are not any similar studies in the literature.However, there are several limitations in this study. While it is anasset that there were several clients, therapists, and supervisors, thenumbers of each are still limited. There were only 3 supervisors ofdiffering experience levels and 7 therapists meeting with only 17total clients. Further the supervision was nested, with one of thesupervisors serving in addition as the supervisor for the other 2who were supervisors in training. The extent to which these resultsgeneralize to a broader pool of supervisors beyond these three andwith respect to a pool of experienced supervisors remains to bedemonstrated. Also, all the therapists were beginning level traineesin their first practicum experience. It is not known if similar resultswould apply to therapist trainees further along in their develop-ment. The data used in rating the in-session therapy behaviorconsisted of only the middle 20 minutes of each therapy session.This was done to cut down on the amount of rating required, and wethought that this was representative enough of the interaction to yielda valid indication. But it still did not capture the entire interaction,which may have yielded different results. Finally, these results apply
only to dominance and affiliation. It makes sense to examine thesedimensions as they are the two basic dimensions of interpersonalinteraction (Wiggins, 1979), but these results may not apply to otherdimensions of interpersonal interaction.
There are several implications of the results of this study forsupervision in the training of therapists. Perhaps primary is toclarify the impact of the therapeutic process on the supervisionprocess and vice versa. How the client and therapist interact isbrought into supervision by the trainee. As such, the subtle alter-ations of the supervision process provide indications of the expe-riences of the therapist in therapy with a particular client. Bidirec-tional parallel processes provide the supervisor with anothervehicle, in addition to direct observation of therapy sessions andreview of case notes, in which to understand what is transpiring intherapy with this trainee and the client. The subtle alterations inhow both the trainee and the supervisor act when discussing aspecific client provide key information on the behavioral dynamicsof that particular therapy dyad. As these cues are recognized, thesupervisor can alter his or her behavior away from the pattern thatthe trainee is subtly structuring. Then the trainee can bring thisback “down” to the client, and in the process alter his or herbehavior in the therapy session to assist the client into alteringbehavior. Thus, the actual supervision interaction provides both adiagnostic cue regarding the therapy process as well as a potentialvehicle for affecting the therapy process.
One factor that supervisors can consider is their metacommuni-cation with the trainee regarding the parallel processes occurringacross therapy and supervision sessions. When aware of a parallelprocess, metacommunication (Beier & Young, 1984; Watzlawick,Beavin, & Jackson, 1967) involves the explicit discussion ofimplicit, or latent, patterns of communication. The supervisor maychoose to communicate with the trainee about how the trainee (inthe therapist role) and client are communicating, as well as how thetrainee and supervisor are communicating. In this way, the super-visor makes the implicit aspects of the parallel process moreexplicit for the trainee. The trainee then can make choices abouthow to best proceed based on the new understanding of theinteractional pattern at the both process and content levels ofinteraction. Of course, metacommunication as a supervision inter-vention requires the awareness by the supervisor of the parallelprocess, but has the advantages of not being a complement to aspecific eliciting behavior (Beier & Young, 1984) and creating acontext in which alternative responses to and for the client can besuggested and explored. Additionally, in some cases, metacommu-nication may be used by the supervisor as a behavioral model fortrainees regarding how to engage in communication with clientsthat helps make the implicit more explicit.
The evidence supporting parallel processes in supervision isgreatly strengthened by this investigation. While some theoristsview parallel process as an integral part of supervision and one thatrequires overt focus (Caligor, 1981; Doehrman, 1976), others seeit as important but not as primary (Clarkson, 1994). Morrissey andTribe (2001) argue that parallel processes exist in supervision, andthat they need to be recognized because the intentional use ofparallel processes can be among the most potent interventions insupervision. However they also note that it can be overused, andthat caution is warranted in its application. The results of this studywill help inform future theory and research continuing to elucidatethe extent to which the process of supervision replicates the
341PARALLEL PROCESS

process of therapy and vice versa, as well as the means by whichawareness of these parallel processes can be deliberately andappropriately used to facilitate the parallel goals of client improve-ment and trainee professional development.
References
Alpher, V. S. (1991). Interdependence and parallel processes: A case studyof structural analysis of social behavior in supervision and short-termdynamic psychotherapy. Psychotherapy, 28, 218–231. doi:10.1037/0033-3204.28.2.218
Beier, E. G., & Young, D. M. (1984). The silent language of psychother-apy. Chicago, IL: Aldine.
Bludworth, J., Tracey, T. J., & Glidden-Tracey, C. E. (2010). The bi-levelstructure of the Outcome Questionnaire-45. Psychological Assessment,22, 350–355. doi:10.1037/a0019187
Burlingame, G. M., Lambert, M. J., Reisinger, C. W., Neff, W. M., &Mosier, J. (1995). Pragmatics of tracking mental health outcomes in amanaged care setting. Journal of Mental Health Administration, 22,226–236. doi:10.1007/BF02521118
Caligor, L. (1981). Parallel and reciprocal processes in psychoanalyticsupervision. Contemporary Psychoanalysis, 17, 1–27.
Clarkson, P. (1994). On psychotherapy. London, United Kingdom: Whurr.DeLucia, J. L., Bowman, V. E., & Bowman, R. L. (1989). The use of
parallel process in supervision and group counseling to facilitate coun-selor and client growth. Journal for Specialists in Group Work, 14,232–238. doi:10.1080/01933928908412055
Doehrman, M. J. G. (1976). Parallel processes in supervision and psycho-therapy. Bulletin of the Menninger Clinic, 40, 9–104.
Draper, D. (1995). Inference and hierarchical modeling in the socialsciences. Journal of Educational and Behavioral Statistics, 20, 115–147.
Dryer, D. C., & Horowitz, L. M. (1997). When do opposites attract?Interpersonal complementarity vs. similarity. Journal of Personality andSocial Psychology, 72, 592–603. doi:10.1037/0022-3514.72.3.592
Edgington, E. S. (1987). Randomization tests. New York: Marcel Dekker.Ekstein, R., & Wallerstein, R. S. (1972). The teaching and learning of
psychotherapy (2nd. ed.). New York: International Universities Press.Estroff, S. D., & Nowicki, S. (1992). Interpersonal complementarity,
gender of interactants, and performance on puzzle and word tasks.Personality and Social Psychology Bulletin, 18, 351–356. doi:10.1177/0146167292183012
Friedlander, M. L., Siegel, S. M., & Brenock, K. (1989). Parallel processin counseling and supervision: A case study. Journal of CounselingPsychology, 36, 149–157. doi:10.1037/0022-0167.36.2.149
Gelman, A., Carlin, J. B., Stem, H. S., & Rubin, D. B. (1995). Bayesiandata analysis. New York: Chapman & Hall.
Grey, A. G., & Fiscalini, J. (1987). Parallel process as countertransference-countertransference interaction. Psychoanalytic Psychology, 4, 131–144.doi:10.1037/h0079131
Jacobsen, C. H. (2007). A qualitative single case study of parallel process.Counselling and Psychotherapy Research, 7, 26 –33. doi:10.1080/14733140601140410
Kell, B. L., & Mueller, W. J. (1966). Impact and change: A study ofcounseling relationships. Englewood Cliffs, NJ: Prentice Hall.
Kiesler, D. J. (1983). The 1982 interpersonal circle: A taxonomy forcomplementarity in human transactions. Psychological Review, 90, 185–214. doi:10.1037/0033-295X.90.3.185
Lambert, M. J., Hansen, N. B., Umpress, V., Lunnen, K., Okishi, J.,Burlingame, G. M., & Reisinger, C. W. (1996). Administration andscoring manual for the OQ-45.2. Salt Lake City, UT: American Profes-sional Credentialing Services.
Leary, T. (1957). The interpersonal diagnosis of personality. New York:Ronald.
Levin, J. R., & Wampold, B. E. (1999). Generalized single-case random-
ization tests: Flexible analysis for a variety of situations. School Psy-chology Quarterly, 14, 59–93. doi:10.1037/h0088998
Loganbill, C. R., Hardy, E. V., & Delworth, U. (1987). Clinical supervi-sion: A conceptual model. The Counseling Psychologist, 10, 3–42.doi:10.1177/0011000082101002
Lombardo, L. T., Greer, J., Estadt, B., & Cheston, S. (1997). Empower-ment behaviors in clinical training: An empirical study of parallelprocesses. The Clinical Supervisor, 16, 33– 47. doi:10.1300/J001v16n02_03
McNeil, B. W., & Worthen, V. (1989). The parallel process in psycho-therapy supervision. Journal of Counseling Psychology, 20, 329–333.
Morrissey, J., & Tribe, R. (2001). Parallel process in supervision. Coun-selling Psychology Quarterly, 14, 103–110. doi:10.180/09515070110058567
Mueller, R. M., Lambert, M. J., & Burlingame, G. M. (1998). Constructvalidity of the Outcome Questionnaire: A confirmatory factor analysis.Journal of Personality Assessment, 70, 248 –262. doi:10.1207/s15327752jpa7002_5
Mueller, W. J., & Kell, B. L. (1972). Coping with conflict: Supervisingcounselors and psychotherapists. New York: Appleton-Century-Crofts.
Ntzoufras, I. (2009). Bayesian modeling using WinBUGS. Hoboken, NJ:Wiley. doi:10.1002/9780470434567
Raichelson, S. H., Herron, W. G., Primavera, L. H., & Ramirez, S. M.(1997). Incidence and effects of parallel process in psychotherapy su-pervision. The Clinical Supervisor, 15, 37– 48. doi:10.1300/J001v15n02_03
Raudenbush, S., Bryk, A., & Congdon, R. (2004). HLM 6: Hierarchicallinear and nonlinear modeling. Lincolnwood, IL: Scientific SoftwareInternational.
Sadler, P., Ethier, N., Gunn, G. R., Duong, D., & Woody, E. (2007). Arewe on the same wavelength? Interpersonal complementarity as sharedcyclical patterns during interaction. Journal of Personality and SocialPsychology, 97, 1005–1020. doi:10.1037/a0016232
Searles, H. F. (1955). The informational value of the supervisor’s emo-tional experiences. Psychiatry, 18, 135–146. PMid:14384968.
Stoltenberg, C. D., & Delworth, U. (1987). Developmental supervision: Atraining model for counselors and psychotherapists. San Francisco: Jossey-Bass.
Strong, S. R., Hills, H., & Nelson, B. (1988). Interpersonal communicationrating scale (rev. ed.). Richmond, VA: Virginia Commonwealth University.
Strong, S. R., Hills, H. I., Kilmartin, C. T., DeVries, H., Lanier, K., Nelson,B. N., . . . Meyer, C. W. III, (1988). The dynamic relations amonginterpersonal behaviors: A test of complementarity and anticomplemen-tarity. Journal of Personality and Social Psychology, 54, 789–810.doi:10.1037/0022-3514.54.5.798
Teyber, E. (2006). Interpersonal process in psychotherapy: An IntegrativeModel (5th ed.). Belmont CA: Thomson Brooks/Cole.
Tracey, T. J., & Ray, P. B. (1984). The stages of successful time-limitedcounseling: An interactional examination. Journal of Counseling Psy-chology, 31, 13–27. doi:10.1037//0022-0167.31.1.13
Tracey, T. J., & Guinee, J. P. (1990). Generalizability of InterpersonalCommunications Rating Scale ratings across presentation mode. Journalof Counseling Psychology, 37, 330 –336. doi:10.1037/0022-0167.37.3.330
Tracey, T. J., & Sherry, P. (1993). Complementary interaction over time insuccessful and less successful supervision. Professional Psychology:Research and Practice, 24, 304–311. doi:10.1037/0735-7028.24.3.304
Tracey, T. J. (1993). An interpersonal stage model of the therapeuticprocess. Journal of Counseling Psychology, 40, 396–409. doi:10.1037/0022-0167.40.4.396
Tracey, T. J. (1994). An examination of the complementarity of interper-sonal behavior. Journal of Personality and Social Psychology, 67, 864–878. doi:10.1037/0022-3514.67.5.864
Tracey, T. J. G., Sherry, P., & Albright, J. M. (1999). The interpersonal
342 TRACEY, BLUDWORTH, AND GLIDDEN-TRACEY

process of cognitive-behavioral therapy: An examination of complemen-tarity over the course of treatment. Journal of Counseling Psychology,46, 80–91. doi:10.1037/0022-0167.46.1.80
Tracey, T. J. G. (2002). Stages of counseling and therapy: An examinationof complementarity and the working alliance. In Tryon, G. S. (Ed.),Counseling based on process research: Applying what we know (pp.265–297). Boston: Allyn & Bacon.
Tracey, T. J. G. (2004). Levels of interpersonal complementarity: A sim-plex representation. Personality and Social Psychology Bulletin, 30,1211–1225. doi:10.1177/0146167204264075
Tracey, T. J. G. (2005). Interpersonal rigidity and complementarity. Jour-nal of Research in Personality, 39, 592–614. doi:10.1016/j.jrp.2004.12.001
Watzlawick, P., Beavin, J. H., & Jackson, D. D. (1967). Pragmatics of
human communication: A study of interactional patterns, pathologies,and paradoxes. New York: Norton.
Wells, M. G., Burlingame, G. M., Lambert, M. J., Hoag, M. J., & Hope,C. A. (1996). Conceptualization and measurement of patient changeduring psychotherapy: Development of the Outcome Questionnaire andYouth Outcome Questionnaire. Psychotherapy: Theory, Research, Prac-tice, Training, 33, 275–283. doi:10.1037/0033-3204.33.2.275
Wiggins, J. S. (1979). A psychological taxonomy of trait-descriptive terms:The interpersonal domain. Journal of Personality and Social Psychol-ogy, 37, 395–412. doi:10.1037/0022-3514.37.3.395
Received June 24, 2011Revision received October 3, 2011
Accepted October 7, 2011 �
343PARALLEL PROCESS
Related Documents











