Archives ofDisease in Childhood 1992; 67: 115-119 A biotinidase Km variant causing late onset bilateral optic neuropathy V Th Ramaekers, T M Suormala, M Brab, R Duran, G Heimann, E R Baumgartner Abstract A patient with a newly recognised variant of biotinidase deficiency presented with acute loss of vision at the age of 10 years. Progressive bilateral optic neuropathy, spastic paraparesis, and a predominantly motor type neuropathy developed over the next five years. Metabolic investigations revealed biotin depletion causing multiple carboxylase deficiency. The basic defect was a biotin recycling disorder due to a mutant biotinidase with residual activity of 4-4% assayed routinely. Biocytin excretion in urine was only slightly increased. Further investigations on plasma biotinidase revealed biphasic kinetics with two different reduced values for maximum reaction velocity (Vmax) and two for the Michaelis constant (Km), one being almost normal and the other considerably raised. In contrast to this patient, two age matched children with partial bio- tinidase deficiency (2-8% and 2-9% of normal), but with a normal K. for biocytin, remained asymptomatic. After six months of oral substi- tution with 10 mg biotin per day the coeco- central and peripheral scotomata regressed, the pyramidal signs in the lower limbs dis- appeared, and further progression of the motor neuropathy arrested. We conclude that the differential diagnosis of unexplained bilateral optic neuropathy of juvenile onset, particularly when associated with upper and lower motor neuron disease, should include biotinidase deficiency. Department of Paediatrics and Ophthalmology, Technical University of Aachen, Germany V Th Ramaekers M Brab G Heimann Metabolic Unit, University Children's Hospital, Basel, Switzerland T M Suormala E R Baumgartner Metabolic Unit, University Children's Hospital 'het Wilhelmina Kinderziekenhuis', Utrecht, The Netherlands R Duran Correspondence to: Dr V Th Ramaekers, Department of Paediatrics, Technical University of Aachen, Pauwelsstrasse 30, D-5100 Aachen, Federal Republic of Germany. Accepted 25 July 1991 Biotinidase deficiency represents an autosomal recessive inborn error of biotin metabolism causing late onset, biotin responsive, multiple carboxylase deficiency. 1-3 Biotinidase acts by recycling biotin through liberation from bio- cytin (F-aminobiotinyl lysine) or from short biotinyl peptides formed during proteolytic degradation of the biotin dependent carboxyl- ases: propionyl-CoA carboxylase (PCC; EC 6.4.1.3), 3-methylcrotonyl-CoA carboxylase (MCC; EC 6.4.1.4), pyruvate carboxylase (PC; EC 6.4.1.1), and acetyl-CoA carboxylase (ACC; EC 6.4.1.2.). In biotinidase deficiency biocytin is lost in urine4 leading to progressive biotin depletion and subsequently to multiple car- boxylase deficiency.3 Biotinidase deficiency in its classical form usually presents during the first year of life with variable neurological signs (hypotonia, seizures, ataxia), dermatitis, alopecia, and recurrent infections. Metabolic acidosis and organic aciduria due to decreased activities of the biotin dependent carboxylases are inconsistently found. Despite rapid clinical and biochemical improvement after treatment with pharmaco- logical doses of biotin, neurological damage such as sensorineural hearing loss, optic atrophy, ataxia, and mental retardation has been reported to persist.3 5 6 Since the introduction of neonatal screening a number of children with partial biotinidase deficiency have been detected of whom most have remained clinically asympto- matic.7 8 In the present paper a new variant of biotinidase deficiency with delayed onset of symptomatology is described. In addition the effect of biotin treatment will be presented. Case report The patient was the single child of healthy non- consanguineous parents born in Poland after an uneventful pregnancy and delivery; his birth weight was 3250 g. Neurodevelopmental progress and growth in the first decade were reported to have been completely normal. At the age of 10 years the patient complained of acute visual loss during the course of a 'flu'-like illness. Bilateral optic atrophy was found and visual acuity was decreased to 20/100 with small bilateral coecocentral scotomata (see fig 1, upper section). Computed tomography, electro- encephalography, and routine laboratory in- vestigations gave normal results. He was treated empirically with parenteral vitamin B-12 but his vision continued to deteriorate. From the age of 14 he complained of fatigue, particularly after exercise, with weakness in the hands particularly when opening boxes or unscrewing bottles. Upon referral at the age of 15 years visual acuity was 20/200 on the right and 20/400 on the left and a mixed colour discrimination defect of red-green and blue-yellow type was found. Both optic discs showed appreciable temporal pallor with increased retinal transparency along the temporal arcuate fibre bundles. Coecocentral as well as peripheral scotomata had become en- larged (see fig 1, middle section). Other ocular findings were bilateral ptosis and mild chronic conjunctival injection. There was intense perspiration of the extremities but no signs of organ failure, alopecia, or dermatitis. Psychometric assessment showed a full scale intelligence quotient of 90. There were no cranial nerve abnormalities apart from mild ptosis and lack of facial expression. In the upper limbs considerable thenar muscle wasting with finger fasciculation was observed and grip was very weak. In the lower limbs there was distal muscle wasting with bilateral pes cavus and hammer toes. His gait was stiff and shuffling but he was not ataxic. Tendon reflexes in the 115 on June 1, 2021 by guest. Protected by copyright. http://adc.bmj.com/ Arch Dis Child: first published as 10.1136/adc.67.1.115 on 1 January 1992. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
Archives ofDisease in Childhood 1992; 67: 115-119
A biotinidase Km variant causing late onset bilateraloptic neuropathy
V Th Ramaekers, T M Suormala, M Brab, R Duran, G Heimann, E R Baumgartner
AbstractA patient with a newly recognised variant ofbiotinidase deficiency presented with acuteloss ofvision at the age of 10 years. Progressivebilateral optic neuropathy, spastic paraparesis,and a predominantly motor type neuropathydeveloped over the next five years. Metabolicinvestigations revealed biotin depletioncausing multiple carboxylase deficiency. Thebasic defect was a biotin recycling disorderdue to a mutant biotinidase with residualactivity of 4-4% assayed routinely. Biocytinexcretion in urine was only slightly increased.Further investigations on plasma biotinidaserevealed biphasic kinetics with two differentreduced values for maximum reaction velocity(Vmax) and two for the Michaelis constant(Km), one being almost normal and the otherconsiderably raised. In contrast to this patient,two age matched children with partial bio-tinidase deficiency (2-8% and 2-9% of normal),but with a normal K. for biocytin, remainedasymptomatic. After six months of oral substi-tution with 10 mg biotin per day the coeco-central and peripheral scotomata regressed,the pyramidal signs in the lower limbs dis-appeared, and further progression of themotor neuropathy arrested.We conclude that the differential diagnosis
of unexplained bilateral optic neuropathy ofjuvenile onset, particularly when associatedwith upper and lower motor neuron disease,should include biotinidase deficiency.
Department ofPaediatrics andOphthalmology,Technical University ofAachen, GermanyV Th RamaekersM BrabG HeimannMetabolic Unit,University Children'sHospital, Basel,SwitzerlandT M SuormalaE R BaumgartnerMetabolic Unit,University Children'sHospital 'het WilhelminaKinderziekenhuis',Utrecht,The NetherlandsR DuranCorrespondence to:Dr V Th Ramaekers,Department of Paediatrics,Technical Universityof Aachen, Pauwelsstrasse 30,D-5100 Aachen,Federal Republic of Germany.Accepted 25 July 1991
Biotinidase deficiency represents an autosomalrecessive inborn error of biotin metabolismcausing late onset, biotin responsive, multiplecarboxylase deficiency. 1-3 Biotinidase acts byrecycling biotin through liberation from bio-cytin (F-aminobiotinyl lysine) or from shortbiotinyl peptides formed during proteolyticdegradation of the biotin dependent carboxyl-ases: propionyl-CoA carboxylase (PCC; EC6.4.1.3), 3-methylcrotonyl-CoA carboxylase(MCC; EC 6.4.1.4), pyruvate carboxylase (PC;EC 6.4.1.1), and acetyl-CoA carboxylase (ACC;EC 6.4.1.2.). In biotinidase deficiency biocytinis lost in urine4 leading to progressive biotindepletion and subsequently to multiple car-boxylase deficiency.3
Biotinidase deficiency in its classical formusually presents during the first year of life withvariable neurological signs (hypotonia, seizures,ataxia), dermatitis, alopecia, and recurrentinfections. Metabolic acidosis and organicaciduria due to decreased activities of the biotindependent carboxylases are inconsistently
found. Despite rapid clinical and biochemicalimprovement after treatment with pharmaco-logical doses of biotin, neurological damagesuch as sensorineural hearing loss, optic atrophy,ataxia, and mental retardation has been reportedto persist.3 5 6 Since the introduction of neonatalscreening a number of children with partialbiotinidase deficiency have been detected ofwhom most have remained clinically asympto-matic.7 8 In the present paper a new variant ofbiotinidase deficiency with delayed onset ofsymptomatology is described. In addition theeffect of biotin treatment will be presented.
Case reportThe patient was the single child of healthy non-consanguineous parents born in Poland after anuneventful pregnancy and delivery; his birthweight was 3250 g. Neurodevelopmentalprogress and growth in the first decade werereported to have been completely normal. Atthe age of 10 years the patient complained ofacute visual loss during the course of a 'flu'-likeillness. Bilateral optic atrophy was found andvisual acuity was decreased to 20/100 withsmall bilateral coecocentral scotomata (see fig 1,upper section). Computed tomography, electro-encephalography, and routine laboratory in-vestigations gave normal results. He was treatedempirically with parenteral vitamin B-12 but hisvision continued to deteriorate. From the age of14 he complained of fatigue, particularly afterexercise, with weakness in the hands particularlywhen opening boxes or unscrewing bottles.Upon referral at the age of 15 years visual
acuity was 20/200 on the right and 20/400 on theleft and a mixed colour discrimination defect ofred-green and blue-yellow type was found. Bothoptic discs showed appreciable temporal pallorwith increased retinal transparency along thetemporal arcuate fibre bundles. Coecocentral aswell as peripheral scotomata had become en-larged (see fig 1, middle section). Other ocularfindings were bilateral ptosis and mild chronicconjunctival injection. There was intenseperspiration of the extremities but no signs oforgan failure, alopecia, or dermatitis.
Psychometric assessment showed a full scaleintelligence quotient of 90. There were nocranial nerve abnormalities apart from mildptosis and lack of facial expression. In the upperlimbs considerable thenar muscle wasting withfinger fasciculation was observed and grip wasvery weak. In the lower limbs there was distalmuscle wasting with bilateral pes cavus andhammer toes. His gait was stiff and shufflingbut he was not ataxic. Tendon reflexes in the
115
on June 1, 2021 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.67.1.115 on 1 January 1992. Dow
nloaded from
http://adc.bmj.com/
-
Ramaekers, Suormala, Brab, Duran, Heimann, Baumgartner
c
0
2o-
0
0
._
._o
0CD
0
00
-
a
0E
.x
0
0
00co
06E
-ill
4
06i
I4v3
o.D.
o.D.
o.0.
....4 I
4- 11
13.
4
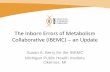
Figure I Visualfields. Top: initial examination at the age of 10years in Poland showed an enlarged blind spot extendinginto the central visualfield. Middle: at the age of 15years the visualfields demonstrated enlarged coecocentral scotomas withwedgelike extensions into the temporal visualfield breaking through to the periphery. Bottom: six months after treatment with10 mg biotinlday the visualfields had improved with reduction ofdepth and extent ofthe coecocentral scotomas and opening upofthe peripheral visualfield borders. The roman numbersfrom 0 to IV represent the identification bordersfor differently sizedobject, from the size of 1116 mm2 (0) to 16 mm2 (IV) respectively. Increasing light intensity is indicated by arabic numbersfrom I to 4. The most important scotomas have been shaded by a grey-white scale.
upper limbs were normal but in the legs theywere symmetrically exaggerated with extensorplantar responses and ankle clonus. There wasslight reduction of vibration sense distally in thelower limbs.
Electroneuromyography in median, tibial,and common peroneal nerves was consistentwith severe neuroaxonal denervation. Motorand sensory conduction velocities were normal.Sensory nerve action potentials derived fromthe sural and median nerve were normal.Audiometry, brain stem and sensory evokedresponses were also normal. The normalelectroretinogram excluded any defects at thelevel of the retinal photoreceptor-ganglioncell unit. The pattern visual evoked response(stimulus size=80 minutes of arc) was extin-guished on the right and equivocal on the left.Brightness stimuli showed plump responseswith diminished amplitudes and prolongedlatencies. The findings on electroretinographyand from evoked visual responses suggested
severe axonal fibre loss and conduction distur-bance.
In peripheral nerve, measurements of neuro-filament density indicated shrinking of axons ofmyelinated nerve fibres but the ultrastructure ofnon-myelinated nerve fibres appeared normal.A muscle biopsy specimen showed light micro-scopic changes indicative of a slowly progressiveneurogenic muscle atrophy.
Despite normal macroscopic appearance ofskin and hair, microscopy of a skin biopsyspecimen showed chronic inflammatory changescharacteristic of chronic dermatitis. On lightmicroscopy a conjunctival biopsy specimenshowed extensive inflammatory changes consis-tent with chronic conjunctivitis.Computed tomography, magnetic resonance
imaging, electroencephalography, cardiac func-tion, analysis of protein in the cerebrospinalfluid, and routine laboratory tests gave normalresults. The first screening of urinary organicacid excretion showed a moderately raised
116
on June 1, 2021 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.67.1.115 on 1 January 1992. Dow
nloaded from
http://adc.bmj.com/
-
A biotinidase Km variant causing late onset bilateral optic neuropathy
excretion of 3-OH-isovaleric acid and a trace of3-OH-propionate (courtesy of Dr Lehnert,Freiburg). A colorimetric screening test forbiotinidase was positive. Neurological assess-ment, ophthalmological and neurophysiologicalexamination in both parents gave normal results.Other family members were not available forophthalmological studies.
EFFECT OF BIOTIN TREATMENTBefore detection of the metabolic inborn errorthe patient's diet was normally balanced andwas lacking food substances rich in biotin. Afterconfirmation of partial biotinidase deficiencydaily substitution with 10 mg biotin was started.After six months on biotin treatment the coeco-central scotomata regressed and peripheralvisual fields showed recovery to near normal(fig 1, bottom section). Colour discriminationhad also improved. These clinical findingscould be substantiated by examination of hisvisual evoked responses. While pattern visualevoked response (representing the central 5-10°of arc) remained unaltered, the brightnessstimuli demonstrated appreciable recovery ofamplitudes and latencies. Subjective improve-ment with less fatigue over the daytime andafter exercise was reported by the patient. Afterbiotin supplementation further deterioration ofthe motor neuropathy arrested. Eight monthsafter biotin supplementation the pyramidalsigns in the lower limbs had disappeared.
Special biochemical studiesMETHODSBiochemical data obtained in the patient werecompared with those of two age matched girlswho had residual biotinidase activities of 2-8%and 2-9% of mean normal (table 1). In contrastto the patient these 15 year old girls appearedperfectly healthy and were neurologicallynormal.8
Informed consent was obtained from theparents and patient before the samples of blood,cerebrospinal fluid, and urine were collected.Organic acids were quantified using gaschromatography/mass spectrometry. Biotinconcentrations were determined in plasma andurine samples by a microbiological assay usingLactobacillus plantarum-ATCC 8014.9 Biocytin
concentrations in urine were measured by amodified high performance liquid chromato-graphy (HPLC).4 8 The activities of biotindependent mitochondrial carboxylases (PCC,MCC, PC) in lymphocytes were measuredbefore and after in vitro activation of apo-carboxylases with excess of biotin as describedpreviously.'0 ACC activity was assayed inlymphocytes by measuring the citrate activatedincorporation of ['4C]-bicarbonate into malonyl-CoA. " Biotinidase activity in plasma wasmeasured colorimetrically using 0-15 mmol/lbiotinyl-p-aminobenzoate as substrate. 2 Kineticstudies on biotinidase were performed by asensitive HPLC method that uses the naturalsubstrate biocytin.8 Plasma from one of the girlswith partial biotinidase deficiency was analysedin the same set of assays as that of the patient.To measure the maximum reaction velocity(Vmax) and Michaelis constant (Km) for bio-tinidase initial velocities were measured usingseveral biocytin concentrations varying from0-00125 to 2-0 mmol/l assay mixture. Theresults were plotted using Eadie-Hofstee re-ciprocal plots, from which the respective Vmaxand Km values were derived.
ResultsBefore biotin treatment organic acid analysisshowed only moderate abnormalities in urinewith a slight rise of 3-OH-isovalerate of 30[tmol/mmol creatinine (normal 8±4 ,tmol/mmol)and a trace of 3-OH-propionate. Plasma concen-trations of 3-OH-isovalerate (9 ,tmol/l), 3-OH-propionate (12 [imol/1), and 3-OH-butyrate (44[imol/l) were also moderately increased. Thelatter organic acids, except for 3-OH-butyrate,are not normally detectable in plasma. However,in cerebrospinal fluid the concentration of 3-OH-isovalerate was 250 .tmol/l, that is, 27 timesthe concentration in plasma. Plasma and cere-brospinal fluid lactate and pyruvate wereall within the normal range. Tiglylglycine,methylcitrate, and 3-methyl-crotonylglycinewere not detected in any of the body fluidsinvestigated. Prompt response to biotin supple-mentation was shown after 24 hours by nor-malisation of 3-OH-isovalerate concentrationsin plasma (1 ,umol/l) and urine (9-7 iimollmmolcreatinine). After four weeks a repeated lumbarpuncture showed return of the 3-OH-isovalerate
Table I Biotinidase activity -in plasma and kinetic parameters for plasma biotinidase calculated from Eadie-Hofsteereciprocal plots presented in figure 2
Subject Activity Kinetic parameters` Factorst(nmollmin/ml plasma)*
(nmol/minlml plasma) (x 10 6 molIl)
Patient 0 275 0-101-=V,,m, 5 56= KmI F=24952-38='Vmax..2 1000=Km2 p
-
Ramaekers, Suormala, Brab, Duran, Heimann, Baumgartner
concentration in the cerebrospinal fluid to thenormal range. Plasma biotin concentrationsbefore biotin treatment were undetectable (table2). The mitochondrial carboxylase activities inlymphocytes of the patient were appreciablydecreased (12-20% of mean normal values), andACC activity was within the normal range.Biotin responsiveness could be demonstrated invitro by the normalisation of the carboxylaseactivities after preincubation with excess biotin.In the two girls with partial biotinidase defic-iency the mitochondrial carboxylases were onlymoderately decreased to 30-58% ofmean normalvalues.Compared with controls and the girls with
partial biotinidase deficiency the urinary biocytinexcretion in the patient before and during biotin
Table 2 Biotin concentrations in plasma and biotin and biocytin concentrations in urine
Subject Biotin Plasma Urine (nmollmmol creatinine)treatment biotin
(nmolll)* Biotin Biocytin
Patientt Nil
-
A biotinidase Km variant causing late onset bilateral optic neuropathy 119
organic aciduria and macroscopic skin or hairabnormalities were absent. Another surprisingfinding was the absence of hearing abnor-malities, whereas the majority of symptomaticpatients who were diagnosed late suffered fromhearing loss. It should be emphasised that thehistory of our patient did not show any-evidenceof increased dietary intake of free biotin thatmight explain the delayed onset of clinicalsymptoms. Biotin treatment in our patient ledto considerable improvement of the optic neuro-pathy, disappearance of pyramidal signs, andarrest of progression of the neuropathy. How-ever the long term outcome is not yet known. Inother patients with delayed onset of biotinsupplementation there was prompt reversal ofthe metabolic derangement and of most clinicalsymptoms with the exception of optic atrophyand hearing abnormalities which persisted insome of them. The selective vulnerability of thecentral nervous system in biotinidase deficiencyhas been observed previously in a single caseresembling Leigh's disease. This phenomenonwas attributed to earlier depletion of biotinstores in the brain than in other tissues,'6 whichwas confirmed by postmortem enzyme studiesof brain, liver, and kidney." In the presentpatient the 27-fold higher 3-OH-isovalerateconcentration in cerebrospinal fluid comparedwith plasma supports this hypothesis.The relationship between the unusual clinical
course in our patient and the enzymatic findingsis not understood. To our knowledge similarbiphasic kinetics have never been observed inplasma of other patients with complete orpartial biotinidase deficiency. In our patientbiocytin excretion was significantly lower thanin patients with complete biotinidase deficiencyindicating a considerable recycling of biotin. Onthe other hand, biotin recycling in our patientwas more severely compromised than in thegirls with similar residual biotinidase deficiencybut a normal Km value. This is reflected by his2-4 fold higher excretion of biocytin comparedwith the girls with partial deficiency.8 Theabsence of symptoms in these two 15 year oldgirls suggests that residual biotinidase activityas low as 2-3% with normal Km maintainsbiotin concentrations high enough to result insufficiently active carboxylases avoiding patho-genic consequences.' However, in our patientsimilar residual activity in combination with anabnormal Km does not allow sufficient recyclingof biotin to prevent neurological abnormalities.
Further investigations are needed to clarifythe molecular basis of the biphasic kinetics ofthis biotinidase Km variant. It is of interest thatbiotinidase activity in the patient's parents wasnormal in contrast to the intermediate activityobserved in parents of patients with complete orpartial biotinidase deficiency.7 8
In conclusion we recommend looking for Km
variants in biotinidase deficient patients with anunusual clinical course. Disorders of biotinmetabolism should be included in the differen-tial diagnosis of patients presenting with un-explained sudden visual failure as early detectionand biotin supplementation will prevent visualor neurological deterioration. The basic screen-ing for disorders of the biotin cycle shouldinclude both urinary organic acid analysis aswell as the colorimetric biotinidase assay onplasma by using three different substrate con-centrations. Testing of biotinidase activity atdifferent substrate concentrations will roughlydetect biotinidase Km variants.
Part of this work was supported by the Deutsche ForschungsGemeinschaft (German Research Foundation). The biochemicalpart of the work was supported by the Swiss National ScienceFoundation grant No 3.871-0.88. We thank Ms J Engler and hergroup (Department of Vitamin and Nutrition Research, FHoffmann-La Roche and Co Ltd, Basel, Switzerland) for thebiotin determinations in plasma and urine. Last but not least wearemost grateful to DrJ Wilson (consultant paediatric neurologist,Hospital for Sick Children, London), for his expert advice andhelp in preparing the manuscript.
1 Sweetman L, Nyhan WL. Inheritable biotin-treatable dis-orders and associated phenomena. Annu Rev Nutr 1986;6:317-43.
2 Wolf B, Grier RE, Allen RJ, Goodman SI, Kien CL.Biotinidase deficiency: the enzymatic defect in late-onsetmultiple carboxylase deficiency. Clin Chim Acta 1983;131:273-81.
3 Wolf B, Heard GS. Disorders of biotin metabolism. In:Scriver CR, Beaudet AL, Sly WS, Valle D, eds. Themetabolic basis of inherited disease. New York: McGraw-Hill, 1989:2083-103.
4 Suormala TM, Baumgartner ER, Bausch J, Holick W, WickH. Quantitative determination of biocytin in urine ofpatients with biotinidase deficiency using high-performanceliquid chromatography (HPLC). Clin Chim Acta 1988;177:253-70.
5 Wolf B, Heard GS, Weissbecker KA, Secor McVoy JR, GrierRE, Leshner RE. Biotinidase deficiency: initial clinicalfeatures and rapid diagnosis. Ann Neurol 1985;18:614-7.
6 Wastell HJ, Bartlett K, Dale G, Shein A. Biotinidasedeficiency: a survey of 10 cases. Arch Dis Child 1988;63:1244-9.
7 Secor McVoy JR, Levy HL, Lawler M, et al. Partialbiotinidase deficiency: clinical and biochemical features.J Pediatr 1990;116:78-83.
8 Suormala TM, Baumgartner ER, Wick H, Scheibenreiter S,Schweitzer S. Comparison of patients with complete andpartial biotinidase deficiency: biochemical studies.J Inherited Metab Dis 1990;13:76-92.
9 Frigg M, Brubacher G. Biotin deficiency in chicks fed awheat-based diet. IntJ Vitam Nutr Res 1976;46:314-21.
10 Suormala TM, Wick H, Bonjour JP, Baumgartner ER. Rapiddifferential diagnosis of carboxylase deficiencies and evalu-ation of biotin responsiveness in a single blood sample. ClinChim Acta 1985;145:151-62.
11 Baumgartner ER, Suormala TS, Wick H, et al. Biotinidasedeficiency: a cause of subacute necrotizing encephalomye-lopathy (Leigh syndrome). Report of a case with lethaloutcome. Pediatr Res 1989;26:260-6.
12 Knappe J, Brummer W, Biederbick K. Reinigung undEigenschaften der Biotinidase aus Schweinenieren undLactobacillus casei. Biochemische Zeitschrift 1963;338:599-613.
13 Ziegler K. Misuse of nonlinear Scatchard plots. TrendsBiochem Sci 1989;14:314-7.
14 Singh G, Lott MT, Wallace DC. A mitochondrial DNAmutation as a cause of Leber's hereditary optic neuropathy.N EnglJ' Med 1989;320:1300-5.
15 Wallace DC. Maternal genes: mitochondrial diseases. In:McKusick VA, Roderick TH, Mori J, Paul NW, eds. Birthdefects original article series. Medical and experimentalmammalian genetics: a perspective. New York: Alan R Liss,1987;23:137-90.
16 Baker H, Frank 0, DeAngelis B, Feingold S. Vitamins inhuman blood and cerebrospinal fluid after intramuscularadministration of several B-vitamins. Nutrition ReportsInternational 1983;27:661-70.
on June 1, 2021 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.67.1.115 on 1 January 1992. Dow
nloaded from
http://adc.bmj.com/
Related Documents