1396 Architecture of the Atrial Musculature In and Around the Triangle of Koch: Its Potential Relevance to Atrioventricular Nodal Reentry DAMIAN SANCHEZ-QUTNTANA. M.D.. D. WYN DAVIES, M.D..* SIEW YEN HO. PH.D..*=f= PAUL OSUZLOK, M.B..t and ROBERT H. ANDERSON, M.D.** From Ihe Departamento de Anatomia Humana. Facultad de Medicina. Universidad de Exlremadtiia. Badajoz. Spain; **Depaiiment olPaedialrics. Imperial College School of Medicine at National Heart and Lung Institute. London. United Kingdom; *Depanmenl ot Cardiology. St. Mary's Hospital. London. United Kingdom; and iDepartmenl ol Cardiology. Our Lady's Hospital for Sick Children. Crumlin, Ireland Atrial Fibers. Introduction: Recent studies suggest that atrial fibers in the approaches to the AV node form part of the dual pathways recognized electrophysiologically in patients with AV nodal reentrant tachycardia (AVNRT). Our aim was to determine, hy gross dissection, the arrangement of the superficial musculature in the area of the triangle of Koch In normal hearts and in hearts with documented AVNRT. hoping to ascertain anatomic features that might con- tribute to the dehate. Methods and Results: We used blunt dissection to study the architecture of the superficial atrial musculature in 16 autopsied hearts from adults who died of noncardiac disease. A well-defined pattern of architecture of muscle fihers was found in the region of the triangle of Koch, showing marked variations in 7 of the 16 specimens. The relationship of these fibers to tbe histologically specialized AV node was confirmed by histology in tbree cases. Two hearts from patients with known AVNRT, treated hy ahlation in one, were examined further histologically. These sections showed that the site of ablation was well distant from the histologically discrete AV node. Conclusion: The variahility in the arrangement of the superficial atrial nmscle fihers in the area of the triangle of Koch may be one of the factors infiuencing the route for imputses entering the AV node, tesions that ablate nodal reentry are within these atrial fibers ratber than tbe histologi- cally specialized AV node. (J Cardiovasc Electrophysiol, Vol. 8, pp. 1396-1407, December 1997) atrium, atrioventricular node, catheter ablation, conduction, electrophysiology Introduction In 1909. Koch' described the landmarks of a triangular area situated between the lower atria! septum and the tricuspid valve. He showed that it contained the airial components of the histo- During ihls invesiigation. Dr. Sanchez-Quiniana was^ supported by Grain DGICYT (PRy5-()57) Iroin Ihe Spiinish govL-rnmenl ajid JiiiUii of Exircmiidura. Drs, Ho and Anderson are suppttried by (he British Hean roimdaiion, together wiih ihe Josoph Levy Foundation. Address tor correspondeiiL-e: Siew Yen Ho, Ph.D., FRCPath. De- partment of Paediatrics. Imperial College School of Medieine at Naiional Heart and Lung Institute. Dovehouse Si.. London .SW3 6LY. United Kingdom. F:ix: 44-171-3518230: E-mail; yen.ho® ic.;ie.uk Manusiiripi received 15 August 1997; Accepted for piiblieation 8 October 1997. logically specialized AV conduction axis. This re- gion has been described as being uniform in size in adult humati hearts.- Its boundaries are tbe tendon of Todaro (the fibrous commissure of tbe valves guarding the openings of the inferior caval vein and the coronary sinus) and the at- tachment of tbe septal leaflet of the tricuspid valve tbat converge at its apex, with tbe orifice of the coronary sinus fVirming the base.-' Current inter- est in intervention or treatment of arrhythmias, es- pecially AV nodal reentrant tachycaidia (AVNRT) and common atrial llutler, is rLx:used on the envi- rons of tbis area. Both surgical and catheter abla- tion techniques make use of the anatomic land- marks of tbe triangle of Koch in attempting to divide the presumptive reentrant pathways. The

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1396
Architecture of the Atrial Musculature In and Aroundthe Triangle of Koch: Its Potential Relevance to
Atrioventricular Nodal Reentry
DAMIAN SANCHEZ-QUTNTANA. M.D.. D. WYN DAVIES, M.D..*SIEW YEN HO. PH.D..*=f= PAUL OSUZLOK, M.B..t
and ROBERT H. ANDERSON, M.D.**
From Ihe Departamento de Anatomia Humana. Facultad de Medicina. Universidad de Exlremadtiia. Badajoz. Spain;**Depaiiment olPaedialrics. Imperial College School of Medicine at National Heart and Lung Institute. London.
United Kingdom; *Depanmenl ot Cardiology. St. Mary's Hospital. London. United Kingdom;and iDepartmenl ol Cardiology. Our Lady's Hospital for Sick Children. Crumlin, Ireland
Atrial Fibers. Introduction: Recent studies suggest that atrial fibers in the approaches to theAV node form part of the dual pathways recognized electrophysiologically in patients with AVnodal reentrant tachycardia (AVNRT). Our aim was to determine, hy gross dissection, thearrangement of the superficial musculature in the area of the triangle of Koch In normal heartsand in hearts with documented AVNRT. hoping to ascertain anatomic features that might con-tribute to the dehate.
Methods and Results: We used blunt dissection to study the architecture of the superficial atrialmusculature in 16 autopsied hearts from adults who died of noncardiac disease. A well-definedpattern of architecture of muscle fihers was found in the region of the triangle of Koch, showingmarked variations in 7 of the 16 specimens. The relationship of these fibers to tbe histologicallyspecialized AV node was confirmed by histology in tbree cases. Two hearts from patients withknown AVNRT, treated hy ahlation in one, were examined further histologically. These sectionsshowed that the site of ablation was well distant from the histologically discrete AV node.
Conclusion: The variahility in the arrangement of the superficial atrial nmscle fihers in the areaof the triangle of Koch may be one of the factors infiuencing the route for imputses entering theAV node, tesions that ablate nodal reentry are within these atrial fibers ratber than tbe histologi-cally specialized AV node. (J Cardiovasc Electrophysiol, Vol. 8, pp. 1396-1407, December 1997)
atrium, atrioventricular node, catheter ablation, conduction, electrophysiology
Introduction
In 1909. Koch' described the landmarks of atriangular area situated between the lower atria!septum and the tricuspid valve. He showed thatit contained the airial components of the histo-
During ihls invesiigation. Dr. Sanchez-Quiniana was supported byGrain DGICYT (PRy5-()57) Iroin Ihe Spiinish govL-rnmenl ajid JiiiUiiof Exircmiidura. Drs, Ho and Anderson are suppttried by (he BritishHean roimdaiion, together wiih ihe Josoph Levy Foundation.
Address tor correspondeiiL-e: Siew Yen Ho, Ph.D., FRCPath. De-partment of Paediatrics. Imperial College School of Medieine atNaiional Heart and Lung Institute. Dovehouse Si.. London .SW36LY. United Kingdom. F:ix: 44-171-3518230: E-mail; yen.ho® ic.;ie.uk
Manusiiripi received 15 August 1997; Accepted for piiblieation 8October 1997.
logically specialized AV conduction axis. This re-gion has been described as being uniform in sizein adult humati hearts.- Its boundaries are tbetendon of Todaro (the fibrous commissure of tbevalves guarding the openings of the inferiorcaval vein and the coronary sinus) and the at-tachment of tbe septal leaflet of the tricuspid valvetbat converge at its apex, with tbe orifice of thecoronary sinus fVirming the base.-' Current inter-est in intervention or treatment of arrhythmias, es-pecially AV nodal reentrant tachycaidia (AVNRT)and common atrial llutler, is rLx:used on the envi-rons of tbis area. Both surgical and catheter abla-tion techniques make use of the anatomic land-marks of tbe triangle of Koch in attempting todivide the presumptive reentrant pathways. The
Sanchez-Quiiitana, et at. Atrial Fibers 1397
anatomic substrates of these pathways, however,are controversial. Soine have proposed that the sub-strates for AVNRT are provided by anatomicallyspecialized tracts, despite the lack of anatomic ev-idence in the human for tbe existence of such tracts.In this respect, although it is well recognized thatthe general pathways for conduction follow pref-erentially the alignment of myocardial fibers, tbereis very little information on anisotropic propaga-tion in tbe environs of the AV node.' - To the bestof our knowledge, no systematic investigation hasbeen made of tbe geometric arrangement of thosemuscular fibers that form the approaches to theAV node. Tbe purpose of this study was twofold.First, we aimed to elucidate any variations in thearrangement of the superficial atrial muscular fibersin and around the triangle of Koch in tbe normalbeart. Second, we analyzed these findings in rela-tion to histologic observations made in twohearts from patients with previously diagnosedAVNRT. treated by ablation in one. By clarifyingthe architecture of the alrial musculature in andaround tbe triangle of Koch, our study sets thescene for future experimental studies.
Materials and Methods
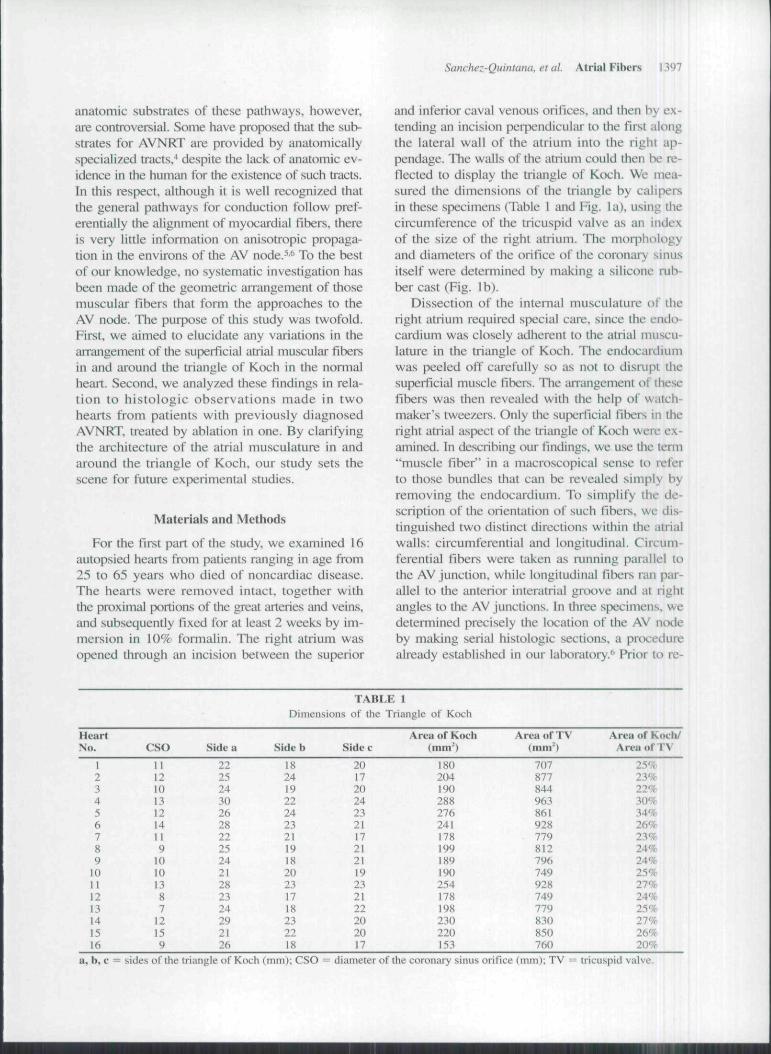
For tbe first part of the study, we examined 16autopsied hearts from patients ranging in age from25 to 65 years who died of noncardiac disease.The hearts were removed intact, together withthe proximal portions of the great arteries and veins,and subsequently fixed for at least 2 weeks by im-mersion in 10% formalin. Tbe right atrium wasopened through an incision between the superior
and inferior caval venous orifices, and then by ex-tending an incision perpendicular to the first alongthe lateral wall of the atrium into the right ap-pendage. The walls of the atrium could tben be re-flected to display the triangle of Koch. We mea-sured the dimensions of the triangle by calipersin these specimens (Table 1 and Fig. la), using thecircumference of the tricuspid valve as an indexof the size of the right atrium. The morphologyand diameters of the orifice of the coronary sinusitself were detennined by making a silicone aib-ber cast (Fig. Ib).
Dissection of tbe intemal musculature of tberigbt atrium required spiecial care, since the endt>cardium was closely adherent to tbe atrial muscu-lature in the triangle of Koch. The endocardiumwas peeled off carefully so as not to disrupt tiiesuperficial muscle fibers. The arrangement of thesefibers was then revealed witb the help of watch-maker's tweezers. Only the superficial fibers in theright atrial aspect of tbe triangle of Koch were ex-ainined. In describing our findings, we use the tcmi"muscle fiber" in a macroscopical sense to referto those bundles that can be revealed simply byremoving tbe endocardium. To simplify the de-scription of the orientation of sucb fibers, we dis-tinguished two distinct directions within the atrialwalls: circumferential and longitudinal. Circum-ferential fibers were taken as running parallel totbe AV juncfion. while longitudinal fibers ran par-allel to tbe anterior interatrial groove and at rightangles to tbe AV junctions. In tbree specimens, wedetennined precisely the location of tbe AV nc>deby making serial histologic sections., a prtxedurealready established in our laboratory/' Prior to re-
HeartNo.
1234567S910111213141516
eso111210131214It9101013871215')
Sidt.' a
22252430262822252421282324292\26
TAIII
Dimensions of the
Side 1)
1824192224232119182023171823
IS
Side (.'
20172024232117212119232122202017
.E 1
Triangle of Koch
Area of Koch(mm')
1802041902882762411781991891902541781982302201,'53
Area or TV(mm*)
707877844963861928779812796749928749779830850760
Area of Kocli/Area of TV
25'*23%22%30%34%26%23%24%24%25%27%24%25%27%26%20%
coronary sinus orifice (mm); TV = iricuspid valve.
1398 Journal of Cardiovascular Electrophysiology Vot. 8. No. 12. December 1997
b)
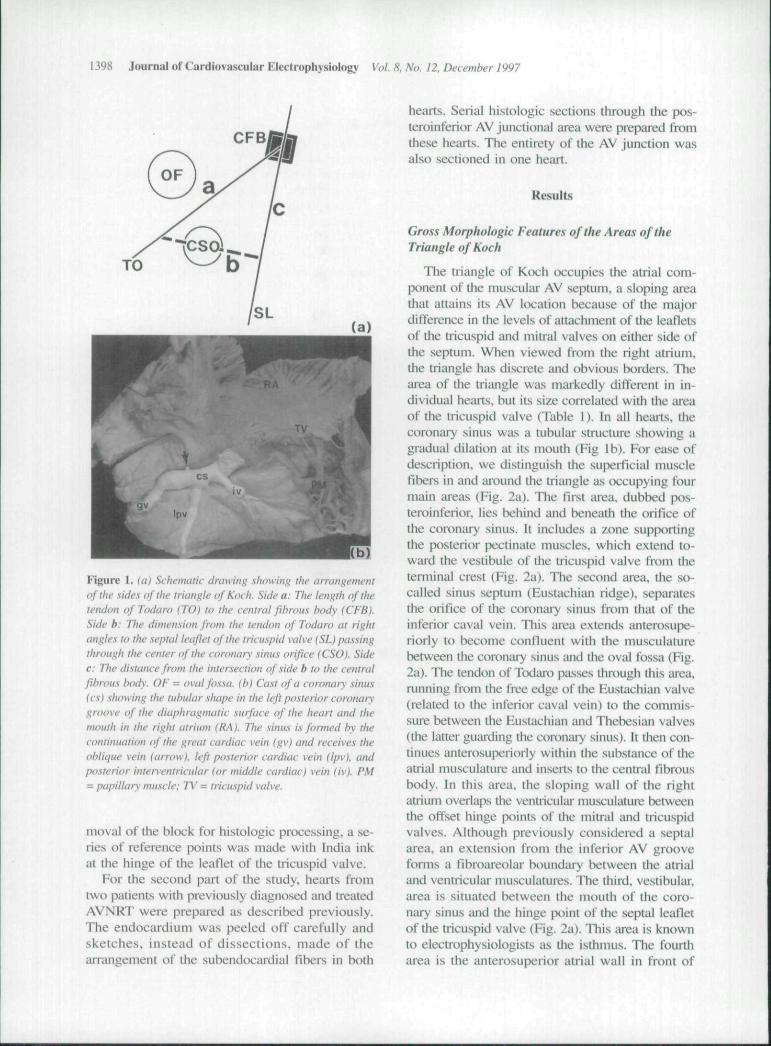
Figure 1. (a) Sctiematic drawing sttowing rtie arrangementofthe .Kide.s of ihe triangle ofKocti. Side a: Ttie tength of ttietendon of Todaro (TO} to the central fibrous body (CFB).Side b: Ttie dimension from ttie tendon of Todaro at rightangtes to ttie septat teaJJet of ttie tricuspid valve (SL) paswingthrough the center ofthe coronary sinus orifice (CSO). Sidec: The distance from the intersection of side b to the centratfibrous tiody. OF = ovat fossa, (b) Ca.st of a coronary sinus(cs) showing the tiitnilar stiape in ttw left posterior coronarygroove of ttte diaphragmatic surface of ttie heart and ttiemouth in the right atrium (RA). The sinus is formed by thecontinuation ofthe great cardiac vein (gv) and receives theotytique vein (arrow), left posterior cardiac vein (tpv). andpo.sterior interventricutar (or middte cardiac) vein (iv). PM= papittary muscte: TV = trtcuspUi vatve.
moval ofthe block for histologic processing, a se-ries of reference points was made with India inkat the hinge of the leaflet of the tricuspid valve.
For the second part of the study, hearts fromtwo patients with previously diagnosed and treatedAVNRT were prepared as described previously.The endocardium was peeled off carefully andsketches, instead of dissections, made of thearrangement of the subendocardial fibers in both
hearts. Serial histologic sections through the pos-teroinferior AV junctional area were prepared fromthese hearts. The entirety of the AV junction wasalso sectioned in one heart.
Results
Gross Morphologic Features ofthe Areas oftheTriangle of Koch
The triangle of Koch occupies the atrial com-ponent of tbe muscular AV septum, a sloping iireathat attains its AV location because of the majordifference in the levels of attachment of the leafletsof the tricuspid and mitral valves on eitber side oftbe septum. When viewed from tbe right atrium,the triangle bas discrete and obvious borders. Thearea of the triangle was markedly different in in-dividual heails, but its size correlated with the areaof tbe tricuspid valve (Table 1). In all bearts, thecoroniiry sinus was a tubular structure showing agradual dilation at its mouth (Fig Ib). For ease ofdescription, we distinguisb tbe superficial musclefibers in and around the triangle as occupying fourmain aieas (Fig. 2a). Tbe first area, dubbed pos-teroinferior, lies behind and beneath the orifice ofthe coronary sinus. It includes a zone supportingthe [xisterior [pectinate muscles, wbicb extend to-ward the vestibule of the tricuspid valve from theterminal crest fFig. 2a). Tlie second area, the so-called sinus septum (Eustachian ridge), separatesthe orifice of the coronary sinus lrom tbat of theinferior cava! vein. This area extends anterosupe-riorly to become contluent with tbe musculaturebetween the coronary sinus and the oval fossa (Fig.2a). The tendon of Todaro passes througb this area,running from the free edge of tbe Eustachian valve(related to the interior caval vein) to the commis-sure between the Eustachian and Thebesian valves(the latter guiirding the coronary sinus). It then con-tinues anterosuperiorly within the substance of theatrial musculature und in.seils lo the central fibrousbody. In this area, the sloping wall of the rightatrium overlaps the ventricular musculature betweenthe offset binge points of Ihe mitral and tricuspidvalves. Altbough previously considered a septalarea, an extension from the inferior AV groovefomis a ftbroareolar boundai-y between tbe atrialand ventricular musculatures. Tbe tbird, vestibular,area is situated between the mouth of the coro-nary sinus and tbe hinge point ofthe septal leafletofthe tricuspid valve (Fig. 2a). This area is knownto electrophysiologists as the isthmus. Tbe fourtharea is the anterosuperior atrial wall in front of
Sanchez-Quintana, et al. Atrial Fibers 1399
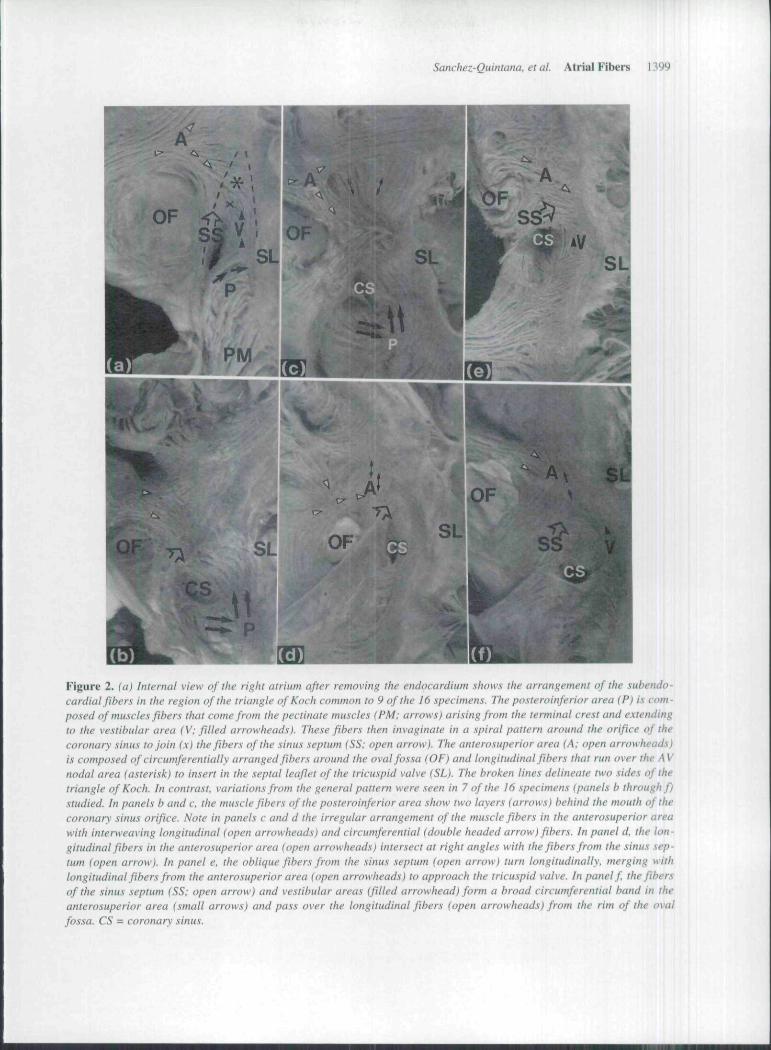
Figure 2. (a) internal view of the right atrium after removing the endocardium shows the arrangement of the subendo-cardial fibers in the region of the triangle of Koch common to 9 of the 16 specimens. The posteroinferior area (P) is com-posed of muscles fibers that come from the pectinate muscles (PM; arrows) arisitigftom the terminal crest and extendingto the vestibular area (V: filled arrowheads). These fibers then invaginate in a spiral pattern around the orifice of thecoronary sinus to join (x) the ftbers of the sinus septum (SS: open arrow}. The anterosuperior area (A: open arrowheads)is composed of circumferentially arranged fibers around the oval fossa (OF) and longitudinal fibers that run over the AVnodal area (asterisk) to insert in the septal leaflet of the tricuspid valve (SL). The broken lines delineate two sides of thetriangle of Koch. In contrast, variations from the general pattern were seen in 7 of the 16 specimens {panels b through f)studied. In panels b and c. the muscle fibers of the posteroinferior area show two layers (arrows) behind the mouth of thecoronary sinus orifice. Note in panels c and d the irregular arrangement of the muscle fibers in the anterosuperior areawith interweaving longitudinal (open arrowheads) and circumferential (double headed arrow) fibers. In panel d. the lon-gitudinal fibers in the anterosuperior area (open arrowheads) intersect at right angles with the fibers from the sinus .xep-tum (open arrow}. In panel e. the oblique fibers from the sinus septum (open arrow) turn longitudinally, merging withlongitudinal fibers from the anterosuperior area (open arrowheads) lo approach the tricuspid valve. In patwl f the fibersof the sinus septum (SS: open arrow) and vestibular areas (filled arrowhead) form a broad circumferential band in theanterosuperior area (small arrows) and pass over the longitudinal fibers (open arrowheads) from the rim of the ovalfossa. CS = coronary sinus.
1400 Journal of Cardiovascular Electrophysiology Vot. S. No. 12, December 1997
the oval fossa. Its musculature consists of the an-terosuperior rim of the oval fossa and the musclebundles extending from the medial walJ ofthe rightatrium (Fig. 2a). This last area is also the so-calledaortic mound, reflecting its important relationshipwith the noncoronary sinus of the aortic valve. Thecompact AV ntxle is located towiird the apex of thetriangle of Koch, deep beneath the intersection ofsinus septal, vestibular. and anterosuperior areas.'
Muscular Architecture ofthe Triangle of Koch
TTie superficial muscle fibers were arranged inrelatively precise pattems within the different ar-eas. In 9 ofthe 16 specimens (56%). the arrange-ment of fibers was remiirkably similar. In the pos-teroinferior area, the muscle fibers ran longitudi-nally from the thick pectinate muscles extendingfrom the temiinal crest and passed directly to thevestibule of the tricuspid valve (Fig. 2a). The si-nus septum, in contrast, was made up of circum-ferential muscle fibers that entered the septal areahaving encircled the oval fossa, becoming obliqueat the level of the tendon of Todaio. The vestibu-lar area was formed by circumferential musclefibers running parallel to the line of insertion ofthe tricuspid valve, these fibers being continuouswith the longitudinal fibers of the pectinate mus-cles in the pt>stei"CJinferior zone. The fibers also in-vaginated in a spiral pattem around the orifice ofthe coronary sinu.s and extended anterosuperiorlyto join with the fibers of the sinus septum (Fig.2a). TTie anterosuperior area was made up of twogroups, one of circumferentially arranged fibersrelative to the tricuspid orifice that passed anteriorto the oval fossa, and the second a series of lon-gitudinal fibers that nui from the aortic mound overthe site of the AV node to insert at the attach-ment of the septal leaflet of the tricuspid valve.
Within this general pattem of arrangement,changes in the direction of muscle fibers were ob-sei-ved. mainly in the posteroinferior and antero-superior areas (Fig. 2. panels b through f). In theposteroinferior area, in three specimens we notedtwo discrete arrays of fibers arising from the pecti-nate muscles. The more superficial of these fibersdirectly encircled the orifice of the coronary si-nus, while the other deeper fibers were longitudi-nally or obliquely ananged (Fig. 2, panels b andc). The overall myoarehitecture within the heartsvaried much more in the anterosuperior area. In thespecimen shown in Figure 2d. the muscle fibersoriginating from the anterosuperior aspect of theseptum took a predominantly longitudinal route. As
the fibers approached the apex of the nodal trian-gle, they were crossed by fibeni from the area ofthe sinus septum. In one further specimen (Fig. 2e),the anterosuperior muscle fiber's showed a prefer-entially longitudinal anangement over the AV mxieand connected directly to the tricuspid ring at rightangles to the fibei-s from the vestibular area. In stilltwo other specimens, the fibers from the sinus sep-tum joined with the fibers of the posteR>inferior andvestibular aix;as (Fig. 20. forming a broad circum-ferential band that coursed over the longitudinalfibers of the anterosuperior iirea as they passed to-ward Ihe septal leaflet of the tricuspid valve.
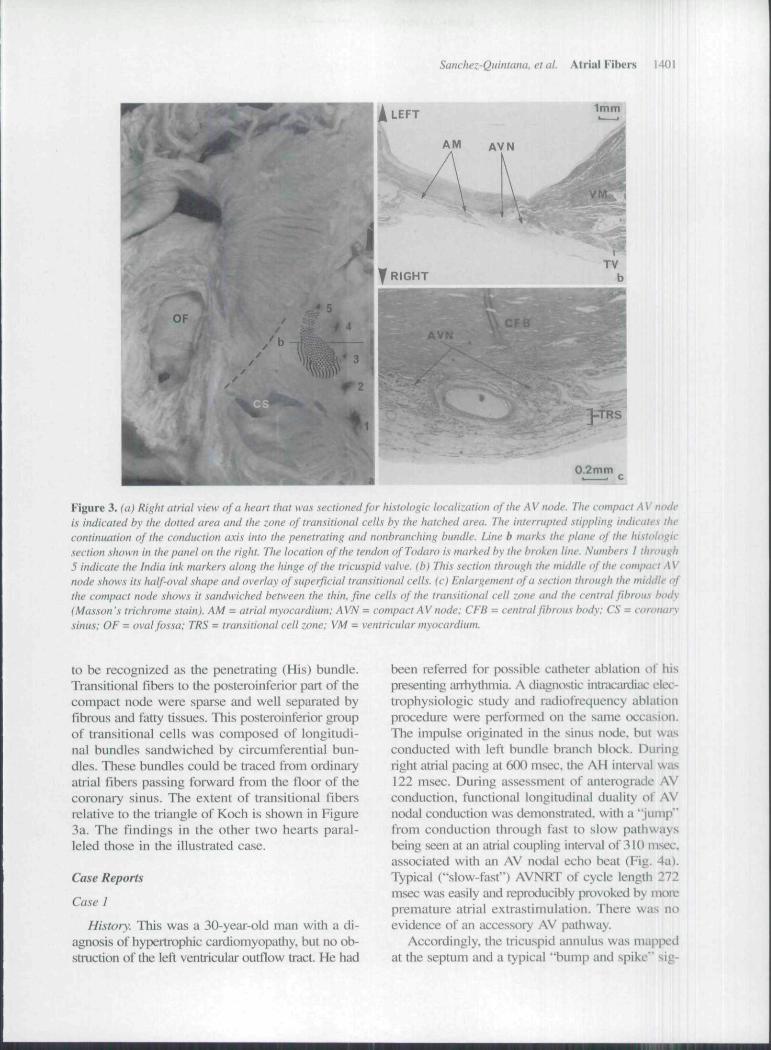
Examination of the sections from iUl three heartsstudied histologicaily confirmed the aiTangementof the subendocardial fibers. Using the markersmade with India ink. the histologicaily distinctcompact AV node in the heart illustrated in Figure3 was located in the triangle of KtK-h between lev-els 3 and 4. It measured 5.25 mm in length. 2.5 to3.5 mm wide, and 0.7 to 1 mm thick. Ltx:ated onthe sloping upper margin of the ventricular sep-tum, but within the atrial myocardium, it was ad-herent to the slope of the central fibrous body suchthat, when viewed in cross section, its right mar-gin was nearer to the hinge of the tricuspid valve.Us left margin, more superiorly situated, facedthe atrial septum (Fig. 3b). The posterior pari ofthe compact node diverged into rightward and left-ward extensions of 2 mm to either side of the nodalartery. The body and anterior parts of the compactnode were continuous with an antemsuperior groupof cells transitional histologically between those t)fthe compact node and the working atrial fibers.These transitional cells extended as superficial anddeep layers. Tlie su|x;rficial layer of the transitionalcells were interposed between the right margin ofthe compact node and the ordinary working fibersof the atrial myocardium approaching the nodefrom the sinus septum and the antcrosujKiior area(Fig. 3. panels b and c). There were 3 to 5 layersof these fibers, which were widely separated byfatty and fibrous tissue. The histologically transi-tional cells in the middle of the atrial septum im-mediately overlying the compact ntxlal mass wereorientated cireuniferentially. but were arranged inlongitudinal sheets .separated by thin fibrous tis-sue. The deep transitional fibers, which inteiposedbetween the compact node and ihe left side ofthe atdal septum, were arranged in bundles takinglongitudinal and circumferential orientations. Tliesewere the last fibers to make contact with the com-pact node before the conduction axis became com-pletely surrounded by fibrous tissue, permitting it
Sanchez-Quintana. etal. Atrial Fibers 1401
1mm
RS
0.2mm
Figure 3. ia) Right atrial view of a heart that was sectioned for histologic localization of the AV node. The cunifHict AV nodeis indicated by the dotted area atid the zotie of tratisitional cetts by the hatched area. The interrupted stippling indicates thecontinuation of the conduction axis into the penetrating and nonbranching bundle. Line b marks the plane of the histologic.section .shown in the panel on the right. The location of the tetidon of Todaro is marked by the broken line. Numbers I through5 indicate the India ink markers along the hinge of the tricuspid valve, (b) This section through the middle of the compact AVnode .shows its half-oval shape and overlay of superficial transitional cetts. (c) Enlargement of a section through the middle ofthe compact node shows it sandwiched between the thin, fme cells of the transitional celt zone and the centrat fibrous body(Masson's trichrome stain). AM = atrial myocardium; AVN = compact AV node: CFB = central fibrous body; CS = coronarysinus: OF = oval fossa; TRS = transitionat cett zone; VM = ventricular myocardium.
to be recognized as the penetrating (His) bundle.Transitional ftbers to the posteroinferior patt of tliecompact node were sparse and well sepiirated byfibrous and fatty tissues. This posteroinferior groupof transitional cells was cotnposed of longitudi-nal bundles sandwiched by circutnferential bun-dles. These bundles could be traced frotn ordinaryatrial fibers passing forward from the tloor of thecoronary sinus. The extent of transitional fibersrelative to the triangle of Koch is shown in Figure3a. The findings in the other two hearts paral-leled those in the illustrated case.
Case Reports
Case 1
History. This was a 30-year-old man with a di-agnosis of hypertrophic cardiomyopathy. but no ob-struction of the left ventricular outflow tract. He had
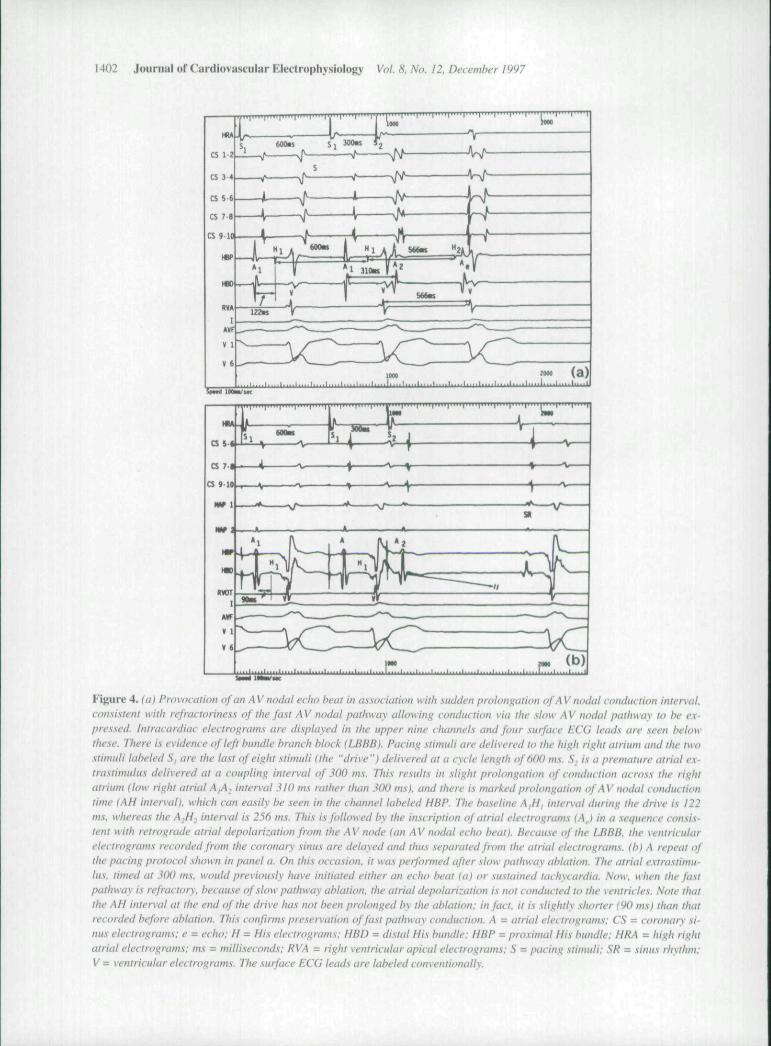
been referred for possible catheter ablation of hispresenting arrhythmia. A diagnostic intracanJiac elec-trophysiologic study and radiofrequency ablationptocedure were performed on the same cx:casion.The impulse originated in the sinus ntxle. but wasconducted with left bundle branch block. Duringright atrial pacing at 600 msec, tlie AH interval was122 m.sec. During assessment of anterograde AVconduction, functional longitudinal duality of AVnodal conduction was demonstrated, with a "Jump"frt)m conduction through fast to slow pathwaysbeing seeti at an atrial coupling interval of 310 msec,associated witli an AV ntxlal echo beat (Fig. 4a).Typical ("slow-fast") AVNRT of cycle length 272msec was easily and reproducibly pn.)voked by morepremature atrial extrastimulation. Theie was noevidence of an accessory AV patliway.
Accordingly, the tricuspid annulus was mappwdat the septum and a typical "bump and spike" sig-
1402 Journal of Cardinva-scular Electrophysidlo^y Vot. 8, No. t2, Decemt)er 1997
MU
css«
CS 7.
CS 9.10
IV 1
no
tWTI
S V
-A v-
4 V
.1....[...,I....I. rFigure 4. foj Provocation of an A V nodat ectut t)eat in association with sudden proloni'ation of A V nodal conduction intervat.consistent with reftactoriness of ttie fast A V nodat pattiway attowing conduction via ttie .sh)w A V nodat pathway to be e.K-pressed. Intracardiac electrograms are displayed in the upper nine channels and four surface ECC leads are seen belowthese. There is evidence of left bundle branch t-tlock (LBBB). Pacing stimuti are delivered to ttie high right atrium and ttie twostimuti labeled S, are ttie tast of eight stimuli (the "drive ") delivered at a cycte tength of 6{H) ms. S. is a premature atriat ex-trastimidus delivered at a coupttng intervat of 300 ms. Ttvs results in slight prolongation of conduction across the rightatriutn (low right atrial A^_, intervat 3W ms ruther than 300 ms), and there is marked prolongation ofAV nodat conductiontime (AH intervat). which can easity be seen in the channet tatwled HBP. The tyasetine A,H, inten'at during the drive is 122ms. whereas ttie A,H, intervat is 256 ni.'i. This is fottowed tyy ttie inscription of atriat electrograms M,J ('/' a .sequence con.\ls-tent with retrograde atriat depolarization from the A V node (an A V nodat echo beat). Because of the LBHB, ttie ventricutarelectrograms recorded from the coronary sinus are detayed and thus separated from the atriat etectrograms. (b) A repeat ofttw pacing protocot stiown In panet a. On ttiis occasion, it was perfonned after stow patttway abtatton. Tlie atriat e.xtrastimu-tus. timed at .^00 ms, woutd previousty tiave initiated eittier an ectio beat (a) or .su.stained tactnvardta. Now, when the fastpathivay is refractory, tjecaii.se of stow pathway abtalion. ttie atriat depotarization is not conducted to ttie ventrtctes. Note thatthe AH interval at the end of ttie drive has not been prolonged by the ablation: in fact, it is stightty stwrter (90 ms) than ttiatrecorded before ablation. This confirms pre.servatton offa.st pathway conduction. A = atriat etectrograms: CS = coronary st-nus etectrograms; e = echo: H = His etectrograms: HBD = distat His bundle: HBP - pro.ximat His bundte: HRA = high rigtuatrial electrograms: ms = mittiseconds: RVA = rigtit ventricular apicat etectrograms: S = pacing .stimuti: SR = sinus rhxthm:V = ventricutar electrograms. The surface ECG teads are labeted conventionatty.
Sanchez-Quintana, et at. Atrial Fibers 1403
nal'- idenfified. One pulse of 90 seconds of ra-diofrequency energy was delivered, stalling at 30W and increasing to 35 W according to imped-ance measurements. Only one junclional ectopicbeat was seen during delivery of energy. After de-livery of the energy, the anterograde conductioncurve was redefined. The effective refractory pe-riod of the anterograde fast AV nodal pathway wasunchanged but, because of successful ablation ofthe slow pathway, more closely coupled atrial de-polarizations were not conducted to the ventricles{Fig. 4b). The velocity of conduction through thefast pathway (AH interval) was not prolonged bythe delivery of radiofrequency energy, confirm-ing safe ablation of the slow pathway and preser-vation of normal conduction via the fast pathway.The patient remained free from palpitafions, butdied suddenly 12 months later.
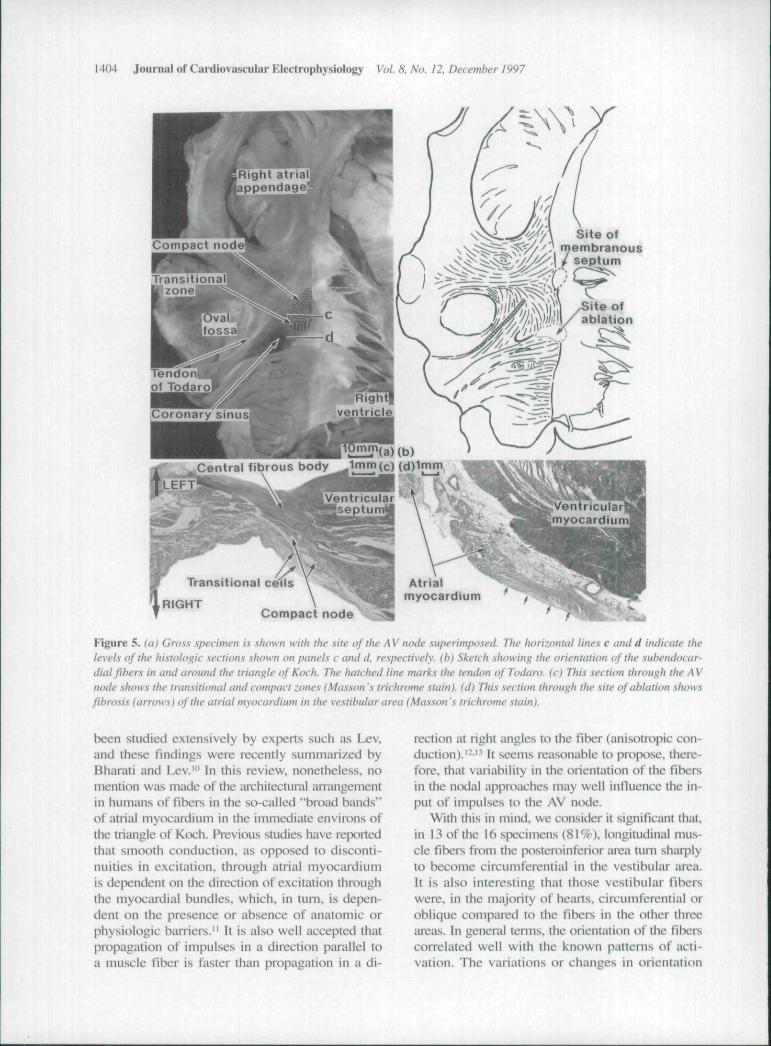
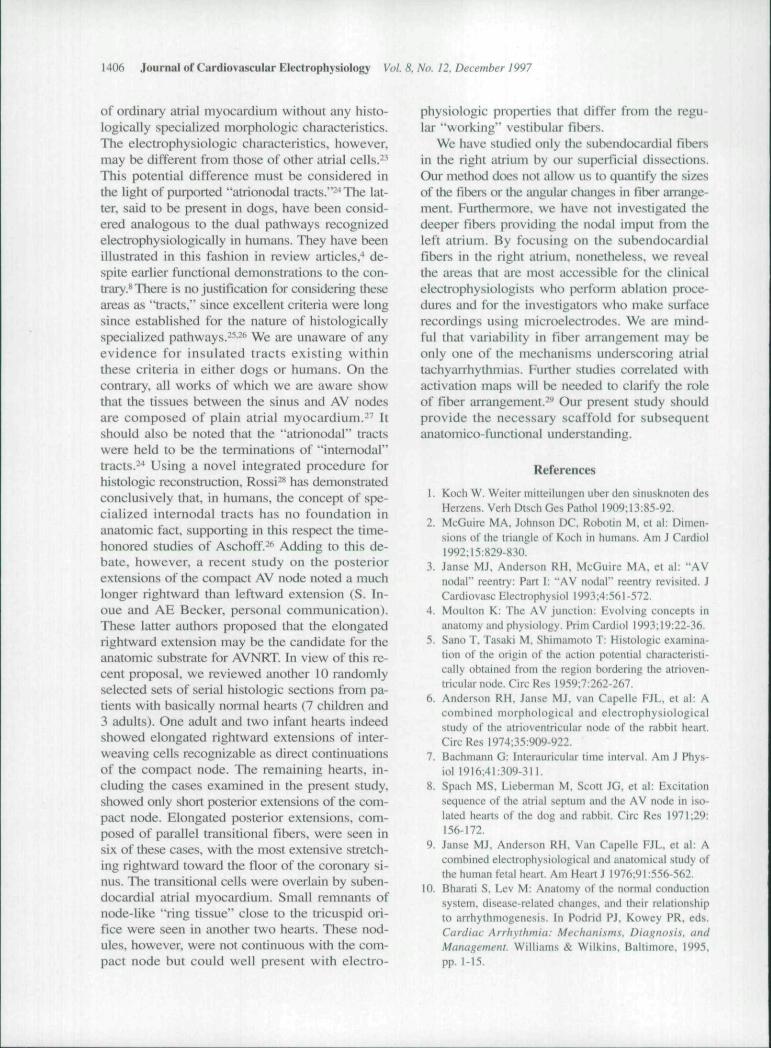
Grass examittation of the heart. The heartweighed 55i) g. It was hyperttophied. showing dif-fuse fibrosis of the ventricular myocardium andfeatures of hypertrophic caidiomyopathy. The fibersin the vestibular area were continuous with theposterior pectinate muscles and passed in circum-ferential orientation anterosuperiorly over the iireaof the compact node, joining with the longitudinalfibers that descended from the anterior limb of theoval fossa (Fig. 5). A white, ovoid lesion mea-suring 8 X 1 4 mm was located at the base of thetriangle of Koch, inferior to the mouth of the coro-nary sinus (Fig. 5a). On histologic examination,the lesion was shown to be an area of fibrous tis-sue involving the full thickness of the right atrialwall imtnediately posterior to the sU)ping crest ofthe muscular ventricular septum. This vestibularwall overlaid the deep invagination of the tissuesof the pt>steromedial AV groove, the fibroareolarplane containing the artery to the AV node. Thenodal artery was not damaged by the lesion. Thedepth of the lesion was mainly limited by the fi-broareolai' tissue plane, although it penetrated about1 mm deep into the ventricular myocardium im-mediately heneath. The coinpact AV ntxic was nor-mal, and its posterior bifurcafion was limited to 1mm on the right and 0.75 mm on the left. Themost postetior pail of the histoiogically special-ized compact AV node and its transifional cellswas situated 2 mtn anterosuperior to the fibroustissue at the site of ablation.
Case 2
History. This boy was diagnosed as having di-abetes mellitus at the age of 8 years and was started
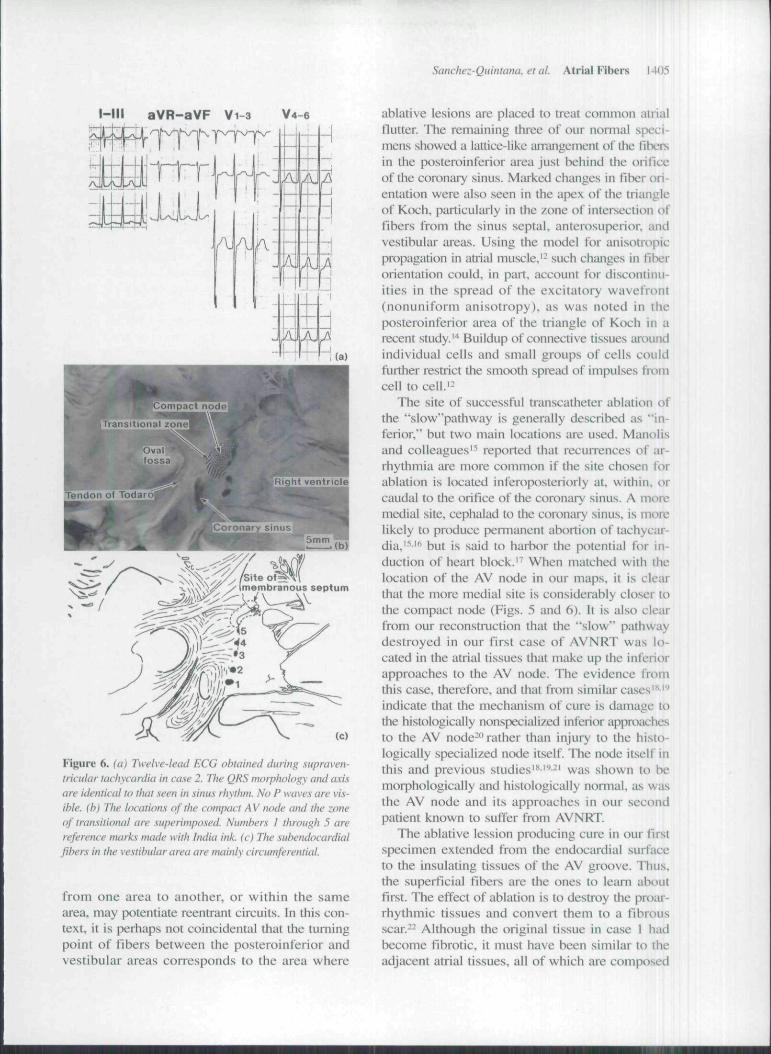
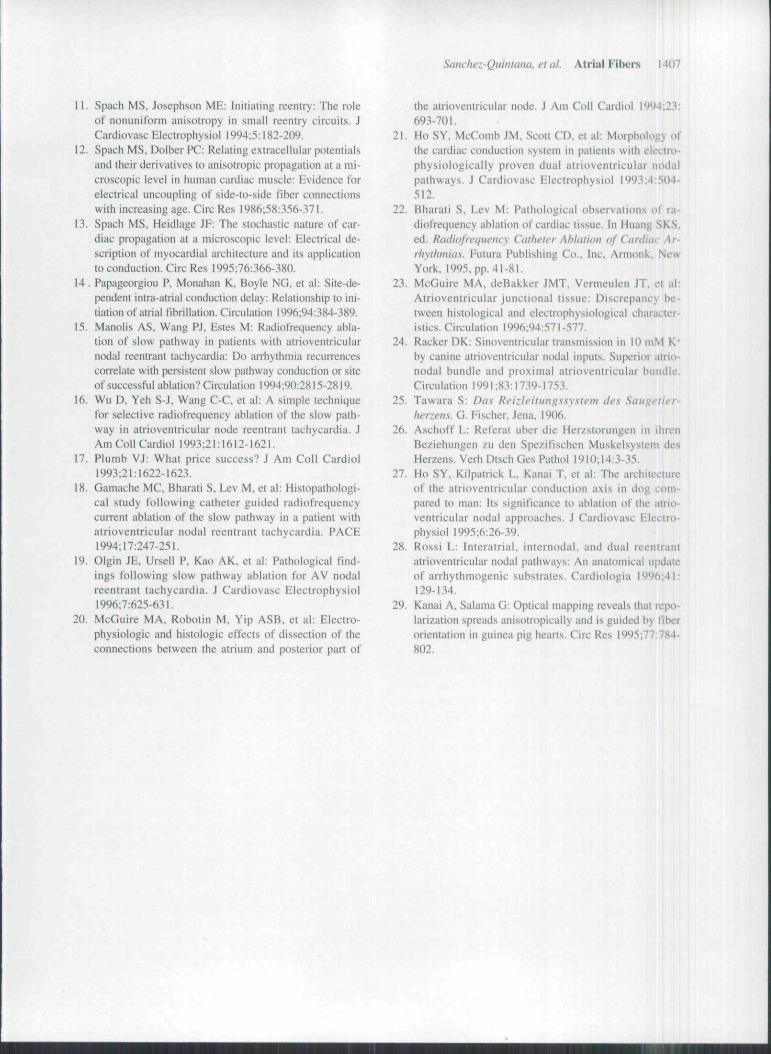
on insulin. At around the same time, he complainedof palpitations. Serial ECGs obtained during sinusrhythm showed no evidence of preexcitatit)n. Thetracings showed a consistent morphology duiingtachycardia (Fig. 6a), having narrow complexes,absent P waves, and, at times, terminal notchingof the QRS complex. The rate was 170 beats/minand was typical of AVNRT He was treated ini-tially with digoxin. Two years later, his treatmentwas changed to flecainide when episodes ofsupraventricular tachycardia recurred. Although heremained well, he was complaining of briefepisodes of tachycardia when he was last tieviewed7 weeks prior to dying suddenly while playingfootball.
Grit.'is examination of the heart. The heart wasstmcturally normal and weighed 2(X) g. The suhen-docardial fibers were orientated longitudinally inthe vestibular area overlying the AV septum (Fig.6, panels b and c).
Histologic exatninatio/h The posterior sectionsshowed a tongue of atrial myocatdium from thevestibular area invaginating toward the ventricularseptum behind the hinge of the septal leaflet. Se-rial sections showed fibrous tissue separating theatrial from the ventricular myocardium. Thecompact AV node had a flat cross-sectional ap-pearance and a short posterior bifurcation. Tran-sitional fibers from the middle and left sides of theseptum made contact with the compact node. Noaccessory connections wete foutid anywhere witliinthe AV junctions.
Discussion
Studies from the time of Bachmann' have shownthat the mode of conduction of impulses withinthe muscular walls of the atriums reflects thearrangement of well-developed tnuscular bun-dles. Pi'evious experimental studies"^" have demt>n-strated two broad bands of atrial approaches to theAV node, one from the inferior region beneath theorifice of the coroniiry sinus (the vesiibular area)and the other comprising the union of a middleband (the sinus septal area) and an anterosuperiorband. These approaches leHect the geometry of theright atrium produced by the orifices of the cavatveins, the coronary sinus, and the oval fossa (Fig.1). Although these activation maps have pro-vided classic models of dual input to the nodal areain animals''-^ and in fetal hearts,'' to the best ofour knowledge, no detailed examination has beentnade of the orientation of the atrial fibers withinthem. The histology of the nodal approaches has
1404 Journal of Cardiovascular Elei-trophysiology Vot. 8, No. 12, December 1997
Site of?, membranous
Site ofablation
Central fibrous body^imm(c) (d)immLEFT
ntrtcular '•' V - ,
JF Transitional cells
U RIGHTCompact node
ventricularImyocardium
Atrialmyocardium
Figure 5. (a) Gross specimen is .ihown with the site of the A V node superimposed. Ttie horizontat tines c and d indicate thetevets of the histotogic sections shown on panets c and d. respectivety. (b) Sketch showing tlie orientation of the sut>endocar-dial fibers in and around the triangle of Koch- The hatctied line marks the tendon of Todaro. (c) This .section through ttie AVnode shows ttie transititmat and compact zones (Masson 's trichrome stain), (d) This section through ttie site ofahtation showsfibrosis (arrows) of the atriat myocardium in the vestibutar area (Ma.sson 's trichrome .stain).
been studied extensively by experts such as Lev.and these findings were recently summarized byBharati and Lev.'" In this review, nonetheless, nomention was made of the iirchitectunil arrangementin humans of fibers in the so-called "broad bands"of atiial tnyocaidium in the immediate environs ofthe uiangie of Koch. Previous studies have reportedthat smooth conduction, as opposed to disconti-nuities in excitation, through atrial myocardiumis dependent on the direction of excitation throughthe myocardial bundles, which, in turn, is depen-dent on the presence or absence of anatomic orphysiologic barriers." It is also well accepted thatpropagation of impulses in a direction parallel toa muscle fiber is faster than propagation in a di-
rection at right angles to the fiber (ani.sotropic con-duction).'-" It seems reasonable to propose, there-fore, that variability in the orientation of the fibersin the n(xlal approaches may well iiilluence the in-put ol' impulses t(» the AV ncxie.
Witli this in mind, we consider it significant ihat,in 13 of the 16 spccimen.s (81 %), longitudinal mus-cle fibers from the posteroinferior area tum sharplyto become circumferential in the vestibular area.It is also interesting that those vestibular fiberswere, in the majority of heaiis. circumferential oroblique compared to the tlbers in the other threeitreas. In genenil tenns. the orientation of the fiberscorrelated well with the known pattems of acti-vation. The variations or changes in orientation
Sanchez-Quintana. et al. Airial Fibers I41).'S
l-in aVR-aVF Vi-3 V4-6
ompact node• • •nsitional zone
tc)
Figure 6. (a) Twelve-lead ECG obtained during .supraven-tricular tachycardia in case 2. The QRS morphology and axisare identical to that seen in sinus rhythm. No P waves are vis-ible, (h) The locations of the compact A V node and the zoneof transitional are superimposed. Numbers I through 5 arereference mitrks made with India ink. (c) Tlie .subendocardialfibers in the vestibular area ate mainly circumferential.
from one area to another, or within the samearea, may potentiate reentrant circuits. In this con-text, it is perhaps not coincidental that the turningpoint of fibers between the posteroinferior andvestibular areas corresponds to the area where
ablative lesions are placed to treat common atrialflutter. The remaining three of our normal speci-mens showed a lattice-like arrangement of the fibersin the posteroinferior ;irea just behind the orificeof the coromiry sinus. Miuked changes in fiber ori-entation were also seen in the apex of the triangleof Koch, particularly in the zone of intersectit)n offibers from the sinus septal, anterosuperior, andve.stibiihir iireas. Using the model for anisotropicpropagation in atrial muscle,'- such chiuiges in filx rorientation could, in part, account for discontinu-ities in the spread of the excitatory wavefront(nonuniform anisotropy), as was noted in theposteroinferior area of the triangle of Koch in arecent .study.' Buildup of connective tissues aroundindividual cells and small groups of cells couldfurther restrict the smooth spread of impulses fromcell to cellJ-
The site of successful transcatheter ablation ofthe "slow"pathway is generally described as "in-ferior," but two main !(x:ations are used. Manotisand colleagues'^ reported that recurrences ot" ar-rhythmia are more common if the site chosen forablation is located inferoposteriorly at. within, orcaudal to tlie orifice of the coronaiy sinus. A moremedial site, cephalad to the coronary sinus, is morelikely to produce permanent abortion of tachyciir-dia,'^"' but is said to harbor the potential for in-duction of heart block.'^ When matched with thelocation of the AV node in our maps, it is clearthat the more medial site is considerably closer tothe compact node (Figs. 5 and 6). It is also clearfrom our reconstaiction that the "slow" pathwaydestroyed in our first case of AVNRT was lo-cated in the atrial tissues that make up the inferiorapproaches to the AV node. The evidence fromthis case, therefore, and that from similar cases'"'"*indicate that the mechanism of cure is damage tothe histologically nonspeci;ili/.ed inferior appn>achesto the AV node-" rather than iiijui-y to the histo-logically specialized node itself. The node itself inthis and previous studies'"'"-' was shown to bemorphologically and histologically normal, as wasthe AV node and its approaches in our secondpatient known to suffer from AVNRT
The ablative lession producing cure in our firstspecimen extended from the endocardial surfaceto the insulating tissues of the AV groove. Thus,the superficial fibers are the ones to learn aboutfu?>t. The effect of ablation is to destroy the proar-rhythmic tissues and convert them to a fibrousscar.-- Although the original tissue in case I hadbecome fibrotic, it must have been similar to theadjacent atrial tissues, all of which are composed
1406 Journal of Cardiovascular Electrophysiology Vol. 8, No. J2, December 1997
of ordinary atrial myocardium without any histo-logically specialized morphologic characteristics.The electrophysiologic characteristics, however,may be different from those of other atrial cells.-'This potential difference must be considered inthe light of purported "atriontxial tracts."--* The lat-ter, said to be present in dogs, have been consid-ered analogous to the dual pathways recognizedelectrophysiologicaliy in humans. They have beenillustrated in this fashion in review articles,^ de-spite earlier functional demonstrations to the con-trary.** There is no justificafion for considering theseareas as "tracts," since excellent criteria were longsince established for the nature of histologicallyspecialized pathways. ^-*' We are unaware of anyevidence for insulated tracts existing withinthese criteria in either dogs or humans. On thecontrary, all works of which we are aware showthat the tissues between the sinus and AV nodesare composed of plain atrial myocardium.-' Itshould also be noted that the "atrionodal" tractswere held to be the tenninations of 'intemodal"tracts. " Using a novel integrated procedure forhistologic reconstruction, Rossi-** has demonstratedconclusively that, in humans, the concept of spe-cialized internodal tracts has no foundation inanatomic fact, supporting in this respect the time-honored studies of Aschoff.- Adding to this de-bate, however, a recent study on the posteriorextensions of the compact AV node noted a muchlonger rightward than leftward extension (S. In-oue and AE Becker, personal communication).These latter authors proposed thai the elongatedrightward extension may be the candidate for theanatomic substrate for AVNRT In view of this re-cent proposal, we reviewed another 10 randomlyselected sets of serial histologic sections from pa-tients with basically normal hearts (7 children and3 adults). One adult and two infant hearts indeedshowed elongated rightward extensions of inter-weaving cells recognizable as direct continuationsof the compact node. The remaining hearts, in-cluding the cases examined in the present study,showed only short posterior extensions of the com-pact node. Elongated po.sterior extensions, com-posed of parallel transitional fibers, were seen insix of these cases, with the most extensive stretch-ing rightward toward the floor of the coronary si-nus. The transitional cells were overlain by suben-docardial atrial myocardium. Small remnants ofnode-like "ring tissue" close to the tricuspid ori-fice were seen in another two hearts. These nod-ules, however, were not continuous with the com-pact node but could well present witb electro-
pbysiologic properties that differ from the regu-lar "working" veslibular fibers.
We have studied only the subendocardial fibersin the right atrium by our supeiUcial dissections.Our method does not allow us to quantity the sizesof the fibers or the iuigular changes in fiber arrange-ment. Furthermore, we have not investigated thedeeper fibers providing the nodal imput from theleft atrium. By focusing on the subendocardialfibers in the right atrium, nonetheless, we revealthe areas that are most accessible for tbe clinicalelectrophysiologists who perform ablation proce-dures and for the investigators who make surfacerecordings using microelectrodes. We are mind-ful that variability in fiber arrangement may beonly one of the mechanisms underscoring atrialtachyarrhythmias. Further studies correlated withactivation maps will be needed to clarify the roleof fiber arrangement.-'' Our present study shouldprovide the necessary scaffold for subsequentanatomico-functional understanding.
References
1. Koch W. Weiter mitteilungen uber den sinusknoten desHerzens. Verh Dtsch Ges Pathol 1909:13:85-92.
2. McGuire MA, Johnson DC, Robotin M. et al: Dimen-sions of the triangle ot" Koch in humans. Am J Cardiol1992:15:829-830.
3. Janse MJ, Anderson RH, McGuire MA, et al: "AVnodal" reentry: Part I: "AV nodal" reenlry revisited. JCardiovasc Eleclrophysiol 1993;4:561-572.
4. Moulton K: The AV junction: Evolving concepts Inanatomy and physiology. Prim Cardiol 1993:19:22-36.
5. Sano T. Tasaki M, Shimamoto T: Histologic examina-tion of the origin of the action ptitential characteristi-cally obtained from the region bordering the atrioven-tricular node. Circ Res 1959:7:262-267.
6. Anderson RH. Janse MJ. van Capelle FJL. et al: Acombined morphological and electrophysiologicalstudy of tbe atrinventricular node of the rabbit bean.Circ Res 1974:35:909-922.
7. Bacbmann G: Interauricular time interval. Am J Phys-io! 1916:41:309-311.
8. Spach MS, Lieberman M. Scott JG, et al: Excitationsequence of tbe atrial septum and the AV node in iso-lated hearts of tbe dog and rabbit. Circ Res 1971:29:156-172.
9. Janse MJ. Anderson RH. Van Capetle FJL. et al: Acombined electrophysiological and anatomical study ofthe human fetal heart. Am Heart J 1976:91:556-562.
10. Bharati S, Lev M: Anatomy of the normal conductionsystem, disease-related changes, and their relationshipto arrhythmogenesis. In Podrid PJ, Kowey PR, eds.Cardiac Arrhythmia: Mechanisms. Diagnosis, andManagement, Williams & Wilkins, Baltimore, 1995.pp. M5.
Sanchez-Quintana. el at. Atrial Fibers 1401
11. Spach MS. Josephson ME; Initiating reentry: The roleof nonuniform anisoEropy in small reentry circuits. JCardiovasc Electropliy.siol 1994:5:182-209.
12. Spach MS. Dolber PC: Relating extracellular potentialsand their derivatives to anisotropic propagation at a mi-croscopic level in human cardiac muscle: Evidence forelectrical uncoupling of side-to-side fiber connectionswith increasing age. Circ Res l986;58:356-37 i.
13. Spach MS. Heldlage JF: The stochastic nature of car-diac propagation at a microscopic level: Electrical de-scription of myocardial architecture and its applicationto conduction. Circ Res I995;76:366-38O.
14. Papageorgiou P. Monahan K. Boyle NG. et al: Site-de-pendent intra-atrial conduction delay: Relationship to ini-tiation of atrial fibrillation. Circulation 1996:94:384-389.
15. Miinolis AS. Wang PJ. Estes M: Radio!requency abla-tion of slow pathway in patients with atrioventricularnodal reentrant tachycardia: Do arrhythmia recurrencescorrelate with persistent slow pathway conduction or siteof successful ablation? Circulation I994;9():2815-28I9.
16. Wu D, Yeh S-J, Wang C-C. et al: A simple techniquefor .selective radiofrequency ablation of the slow path-way in atrioventricular node reentrant tachycardia. JAm Coil Cardiol 1993:21:1612-1621.
17. Plumh VJ: What price success? J Am Coll Cardiol1993:21:1622-1623.
18. Gamache MC, Bharati S, Lev M, et al: Histopathologi-cal study following catheter guided radiofrequencycurrent ablation of the slow pathway in a patient withatrioventricular nodal reentrant tachycardia. PACE1994:17:247-251.
19. Olgin JE. Ursell P. Kao AK. et al: Pathological find-ings following slow pathway ablation for AV nodalreentrant tachycardia. J Cardiovasc Elcctropbysiol1996:7:625-631.
20. McGuire MA. Robotin M. Yip ASB. et al: Electro-physiologic and histologic effects of dissection of theconnections between the atrium and posterior part of
the atrioventricular node. J Am Coll Cardiol 1994:23:693-701.
21. Ho SY. McComb JM. Scott CD. et al: Morphology ofthe cardiac conduction system in patients with electro-physiologically proven dual atrioventricular nodalpathway.s. J Cardiovasc Electrophysiol 1993:4:504-512.
22. Bharati S. Lev M: Pathological observations of ra-diofrequency ablation of cardiac tissue. In Huang SKS.ed. Radiofrequency Catheter Abtatiim of Cardiac Ar-rhyttviitas. Futura Publishing Co.. Inc. Armonk. NewYork. 1995. pp. 41-81.
23. McGuire MA. deBakker JMT. Vermeulen JT. ct al:Atrioventricular junctional tissue: Discrepancy be-tween histological and electrophysiological character-istics. Circulation 1996:94:571-577.
24. Racker DK: Sinoventricular transmission in 10 inM K*by canine atrioventricular nodal inputs. Superior atrio-nodal bundle and proximal atrioventricular bundle.Circulation 1991:83:1739-1753.
25. Tawara S: Das Reizteitungssystem ties Saugetier-tierzens. G. Fischer. Jena. 1906.
26. Aschoff L: Referat uber die Herzstorungen in ihrenBeziehungen zu den Spezifischen Muskelsystem desHerzens. Verh Dtsch Ges Pathol 1910:14:3-35.
27. Ho SY. Kilpatrick L. Kanai T. et al: The architectureof the atrioventricular conduction axis in dog com-pared to man: Its significance to ablation ofthe atrio-ventricular nodal approaches. J Cardiovasc Electro-physiol 1995:6:26-39.
28. Rossi L: Interatrial. internodai. and dual reentrantatrioventricular nodal pathways: An anatomical updateof arrhythmogenic substrates. Cardiologia I996;41:129-134.
29. Kanai A. Salama G: Optical mapping reveals that repo-larization spreads anisotropically and is guided by fiberorientation in guinea pig hearts. Circ Res 1995;77:784-802.

Related Documents











