Approved: 9 Jun 1999 1 DoD Health Care Provider’s Briefing: Anthrax Vaccine Immunization Program

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Approved: 9 Jun 1999 1
DoD Health Care Provider’s Briefing:
Anthrax Vaccine Immunization Program

Approved: 9 Jun 1999 2
Overview
• Anthrax is a biological weapon
• Anthrax is lethal
• Vaccine is safe and effective
• Immunization before exposure, along with wearing your mask, is critical
• This is a mandatory vaccination program, like all other force health protection vaccines

Approved: 9 Jun 1999 3
Threat
• Anthrax is one of the primary biological weapon (BW) threats
• Evidence of production and weaponization by other countries – Northeast Asia– Southwest Asia

Approved: 9 Jun 1999 4
Anthrax is an Ideal BW Agent
• Spores may survive > 40 years
• Aerosolized stable spore
• Efficient downwind spread
• Lethal dose could be inhaled with one deep breath
• Inhalational anthrax mortality reaches 100%

Approved: 9 Jun 1999 5
Microbiology of Anthrax
• Gram positive sporulating rod

Approved: 9 Jun 1999 6
Epidemiology of Anthrax
• Disease of herbivores
• Man infected via animal products
• Dramatic reduction in the U.S. since the early 1900s
• Still a problem in Asia and Africa

Approved: 9 Jun 1999 7
Pathogenesis• Spore enters skin, GI tract or lung
• Ingested by macrophages
• Transported to regional lymph nodes
• Germinate in regional nodes, mediastinum (inhalational)
• Local production of toxins
• Edema & necrosis
• Bacteremia & toxemia
• Seeding of other organ systems

Anthrax Toxin Effects
Increased Cyclic AMP
Macrophage Lysis
Edema Factor(EF)
MW 89,000
Protective Antigen(PA)
MW 83,000
Lethal Factor(LF)
MW 90,000
Local Edema

Approved: 9 Jun 1999 9
Cutaneous Anthrax
• > 95% of naturally occurring cases
• Spores enter breaks in skin after contact with contaminated animal products
• Papule - Vesicle - Ulcer - Eschar
• Up to 20% case fatality rate if untreated
• Mortality with treatment < 1%

Approved: 9 Jun 1999 10
Slide Of Cutaneous Ulcer

Approved: 9 Jun 1999 11
Gastrointestinal Anthrax
• Ingestion of insufficiently cooked meat from infected animals
• Nausea, vomiting, fever, abdominal pain
• Mortality may exceed 50% despite treatment

Approved: 9 Jun 1999 12
Inhalational Anthrax
• Incubation period 1-6 days
• Nonspecific symptoms– Malaise, fever, fatigue, cough, chest discomfort
• Terminal phase– Dyspnea, stridor, cyanosis, increased chest
pain, chest wall edema, followed by shock and death within 24-36 hours
• Meningitis seen in up to 50% of cases

Approved: 9 Jun 1999 13
Diagnosis of Inhalational Anthrax
• Initial symptoms nonspecific
• Development of respiratory distress– CXR with widened mediastinum– Usually no infiltrates
• Sputum not helpful
• Hemorrhagic pleural effusion or meningitis
• Swabs

Approved: 9 Jun 1999 14
CXR of Inhalational Anthrax

Approved: 9 Jun 1999 15
Inhalational Anthrax Treatment• Early IV antibiotics and intensive care required
– Mortality may still exceed 80%
• Penicillin - historical treatment
• Current treatment of choice:– Ciprofloxacin 400 mg IV q 8-12 h– Doxycycline 200 mg IV x 1 then 100 mg IV q 12 h
• Disease is not spread by respiratory secretions - no need for respiratory protection for health care providers– Use Standard Precautions

Approved: 9 Jun 1999 16
Post-Exposure Prophylaxis• Starting antibiotics within 24 hours after
aerosol exposure is expected to provide significant protection– Ciprofloxacin 500 mg po BID– Doxycyline 100 mg po BID
• Most effective when combined with vaccination
• Antibiotics are still indicated even when fully immunized

Approved: 9 Jun 1999 17
Anthrax Vaccine• Licensed since 1970 by the Food and Drug
Administration (FDA) – Not a new or experimental vaccine
• Sterile, cell-free (killed) bacterial vaccine – Contains predominately protective antigen from an
attenuated strain of Bacillus anthracis– Prepared from culture supernatant - there are no organisms
in the vaccine, cannot cause anthrax disease– Adsorbed to aluminum hydroxide– Contains 0.02% formaldehyde, 0.0025% benzethonium
chloride as preservatives• Manufactured by BioPort Corporation (formerly known as
Michigan Biologic Products Institute)

Approved: 9 Jun 1999 18
Vaccine Quality Control
• Each batch of any vaccine manufactured in the U.S. must meet FDA specifications and prescribed standards per 21 CFR 620– Potency, Sterility, Safety, Purity
• Testing done at manufacturer; results submitted to the FDA
• Prior to release, all stockpiled anthrax vaccine lots must pass supplemental testing

Approved: 9 Jun 1999 19
Handling Anthrax Vaccine• Vaccine must be refrigerated
• Store and maintain between 36 and 46 degrees F
• DO NOT FREEZE
• Once vial opened, use until expired– Discard if contaminated
• Reference USAMMA web site for guidance on questionable vaccine– http://www.medicine.army.mil/usamma/anthrax/
antxhome.htm
Approved: 9 Jun 1999 20
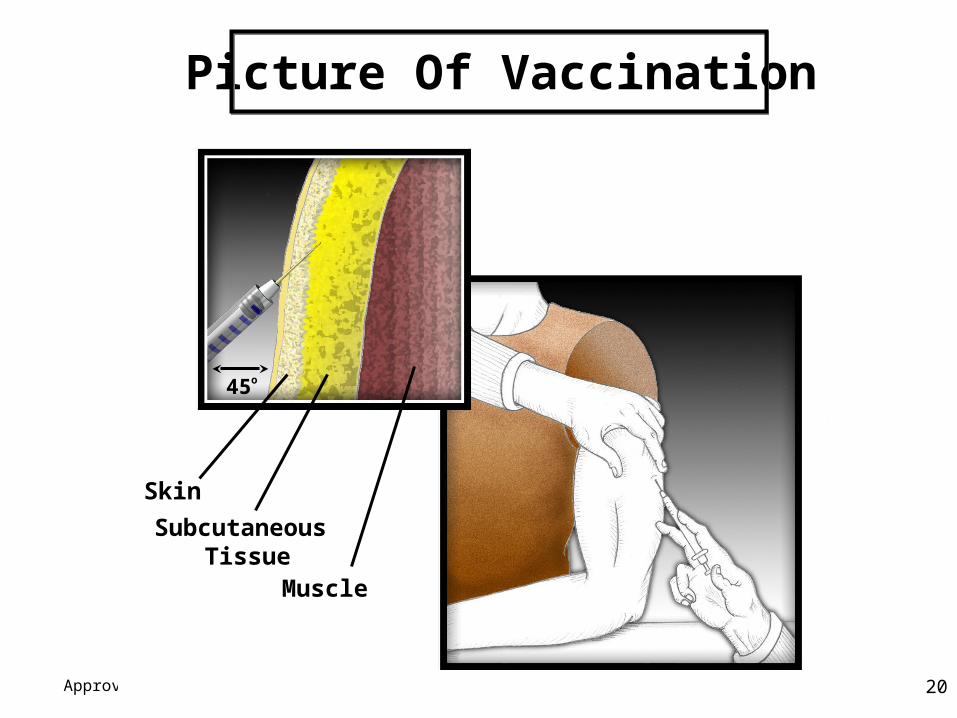
45 o
Picture Of Vaccination
Skin
Subcutaneous Tissue
Muscle

Approved: 9 Jun 1999 21
Vaccine Schedule
0
2 w
eek
s
4 w
eek
s
6 m
onth
s
12 m
onth
s
18 m
onth
s
5 months 6 months 6 monthsfrom 3rd
Dose 1 2 3 4 5 6
• 6 shots over 18 months, then annual booster

Approved: 9 Jun 1999 22
Standard Interval Between Doses
• Doses 1 & 2 - 2 weeks
• Doses 2 & 3 - 2 weeks
• Doses 3 & 4 - 5 months
• Doses 4 & 5 - 6 months
• Doses 5 & 6 - 6 months
Between Minimum Interval

Approved: 9 Jun 1999 23
Anthrax Vaccination Schedule
• The DoD policy is to adhere to the FDA approved vaccination schedule
• If documented gap after dose #1 is greater than two years, restart the series. Once given dose #2 or beyond, do not restart the series
• Late doses should be given ASAP - adjust timing of subsequent doses according to the standard interval schedule

Approved: 9 Jun 1999 24
Access to DoD Medical Treatment Facility (MTF)
• The following designated personnel may receive any dose at any MTF:– Active component – Reserve component (Must be in a duty status)– Emergency essential DoD civilian and contract
personnel– U.S. Coast Guard as applicable
• Mass immunizations require prior coordination with MTF

Approved: 9 Jun 1999 25
Response to Vaccine
• Anthrax vaccine, like other vaccines, stimulates your body to produce protective antibodies– Everyone has some antibody response after 2 doses– The full series is needed to obtain maximum and
on-going protection– Everyone gets some protection
• Even with a good antibody response, your defense system can be overwhelmed given sufficient number of spores

Approved: 9 Jun 1999 26
Animal Models For Human Protection
• Vaccine efficacy has been tested against numerous anthrax strains in animal studies– Guinea pigs and mice are poor animal models
for anthrax vaccine testing – Rabbits considered a more appropriate small
animal model
• Monkeys considered the best model for human response

Approved: 9 Jun 1999 27
Evidence Of Efficacy: Published Animal Trials
• 30 monkeys vaccinated twice– Challenged with aerosol at either 8, 16, 38, or
100 weeks later– 29 survived (1 died at 100 week challenge)
• 10 monkeys vaccinated once– Challenged with aerosol 6 weeks later– All survived
• Overall 98% vaccine protective efficacy

Approved: 9 Jun 1999 28
Vaccine Protection Against Different Strains
• Vaccine efficacy has been demonstrated against numerous anthrax strains in animal studies
• Biologic plausibility supports anthrax vaccine protection against all strains– Protective antigen is common to all anthrax
strains– Anthrax vaccine protection is expected against
diverse strains

Approved: 9 Jun 1999 29
Vaccine Efficacy - Inhalational Anthrax
• Human antibody response
• Animal protection data
• Compelling evidence that the vaccine series will be effective at preventing disease after an aerosol exposure

Approved: 9 Jun 1999 30
Record Keeping• Automated immunization tracking
– Service systems and DEERS central repository
• Written entries:– Health record (SF-601)– Adult Preventive and Chronic Care Flowsheet
(DD form 2766 or DD form 2766C)– Yellow Shot Card (PHS-731)
• Required documentation:– Date immunized, name of vaccine, manufacturer,
lot number, series number, dosage, provider name and MTF address

Approved: 9 Jun 1999 31
Adverse Reactions• Mild local reactions (30%)
– Redness, tenderness at site for up to 24-72 hours– Subcutaneous nodules (lumps)
• Moderate local reactions (4%)– Redness/hardness >5 cm, tenderness, itching for up to
24-72 hours• Severe local reactions rare (<1%) • Very rare systemic reactions occur (<0.2%)• Extremely rare systemic reactions (e.g., Guillain Barre
Syndrome) may occur with all vaccines

Approved: 9 Jun 1999 32
Adverse Event Reporting• FDA National Vaccine Adverse Event Reporting
System (VAERS)– FDA and DoD review 100% of adverse events reports
submitted to FDA– Anyone can submit a Form VAERS-1 – A Form VAERS-1 submission is REQUIRED for:
• Loss of duty > 24 hours
• Hospitalization
• Suspected vaccine lot contamination
– Form VAERS-1 may be obtained by calling: • 1-800-822-7967 or at www.fda.gov/cber/vaers.htm.

Approved: 9 Jun 1999 33
Reserve Component Adverse Event Procedures
• An individual experiencing a vaccine-associated adverse event in a non-duty status:– Seek medical evaluation at a DoD or civilian medical
treatment facility if necessary – Must report the event to their unit commander or
designated representative as soon as possible
• Form VAERS-1 is the same as Active Duty
• Commander will initiate Line of Duty and/or Notice of Eligibility

Approved: 9 Jun 1999 34
Contraindications• Hypersensitivity reaction to a previous dose
of anthrax vaccine or vaccine component• Younger than 18 or older than 65 • HIV positive • Temporary deferral
– Pregnancy– Active infection/illness with fever– Depressed immune response to include
corticosteroid or other immunosuppressive treatment

Approved: 9 Jun 1999 35
Pregnancy
• All vaccinations routinely deferred during pregnancy
• Before vaccination, ask all women if pregnant, defer vaccination if pregnant– Continue when no longer pregnant
• No reason to delay pregnancy or conception efforts after vaccination
• Breast feeding not a contraindication to vaccination

Approved: 9 Jun 1999 36
Conclusions
• Anthrax is a significant threat to our forces
• Anthrax vaccine is safe and effective
• Personal protective measures are still important
• Life saving benefit of anthrax vaccine make this a mandatory immunization program
• Vaccination is a crucial part of force health protection and readiness

Approved: 9 Jun 1999 37
Information Sources
• Chain of command
• Http://www.anthrax.osd.mil
• Http://www.defenselink.mil
• Http://www.cdc.gov
Related Documents