14/10/13 Approach to the adult with acute persistent v isual l oss ww w. upt oda te. com /con ten ts/ap proach -to-the-ad ult-with-acu te-persistent -visua l- loss?top icKey =PC%2F690 2&e lapsed TimeMs=0&sou rce=search_result&se arc… 1/1 7 Offic ial repr in t from UpToDate ® www.uptodate.com ©201 3 UpToDat e ® Author The llea Lev eque, MD, MPH Section Editor Jonathan Trobe, MD Deputy Editor H Nancy Sokol, MD Approach to the adult with acute persistent visual loss Disclosures All t opics are updated as new e v idence be comes available and our peer review process is complete. Literature review current through: Sep 2013. | This topic last updated: feb 11, 2013. INTRODUCTION — Acute vision loss is a frightening experience for patients and has the potential for long-term visual consequences. The many causes of acute vision loss and the time-sensitive need for evaluation and treatmen t pose diagno stic and thera peutic c hallenges. A carefu l hist ory is t he key to narro wing the d iff eren tial diagnosis and will allow f or a mor e fo cused physic al examination. Prompt diagnosis and treatment may influence the visual outcome. This topic will present an overview of the approach to patients with acute persistent visual loss. Transient visual loss, the diff ere ntial diagnosis of the red eye, and specific causes of acute vision loss are discussed separately. (See "Amaurosis fugax (transient monocular or binocular visual loss)" and "Evaluation of the red eye" .) DEFINITION OF TERMS — Acute transient visual loss (TVL) is defined as a sudden deficit in visual function in one or both eyes lasting les s t han 24 ho urs. It is caused by a t empor ary v ascular occlusion in the circulation to t he eye or visual cortex, or by neuronal depression after a seizure or migraine [ 1]. Acute persistent visual loss (PVL) may be defined as lasting at least 24 hours and is typically not caused by transient ischemia [ 2]. (See "Amaurosis fugax (transient monocular or binocular visual loss)" .) ETIOLOGY — To achieve clear vision, light must follow an unhindered path from the front to the back of the eye, traveling through the cornea, aqueous humor, lens, and vitreous humor to the retina ( figure 1). Refracted by the cornea and lens (and perhaps also by glasses or contact lenses), light is f ocused onto the retina where it is transformed into an electrochemical signal by photoreceptors and supporting cells. The signal is transmitted via the optic nerve through the visual pathways to the occipital lobes. Alterations in fun ction of any of the structure s along the v isual pathwa y may cause vision loss. Pathology can be broadly divided into three major anatomic categories (table 1): Media problems Retinal problems Neural visual pathway problems Media problems include keratopathy, hyphema, lens changes, vitreous hemorrhage, uveitis, and, endophthalmitis. Retina l dis ease includes v ascular occlus ion, retinal detachment, and acute maculopathy. Neural visual pathway malfunction may be subdivided into optic nerve, chiasmal, and retrochiasmal pathology. Media problems Keratitis — Keratitis is inflammation of the cornea due to trauma, abrasive exposure, allergy, or infection. It is marked by cloudiness, irregular ity, or loss of epithelial or sub-e pithelial cornea l ti ssues. Typically the eye i s t ear ing, red, and painful or irritated.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 1/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&searc…
Official reprint from UpToDate®
www.uptodate.com ©2013 UpToDate®
Author Thellea Leveque, MD, MPH
Section Editor Jonathan Trobe, MD
Deputy Editor H Nancy Sokol, MD
Approach to the adult with acute persistent visual loss
Disclosures
All topics are updated as new evidence becomes available and our peer review process is complete.
Literature review current through: Sep 2013. | This topic last updated: feb 11, 2013.
INTRODUCTION — Acute vision loss is a frightening experience for patients and has the potential for long-term
visual consequences. The many causes of acute vision loss and the time-sensitive need for evaluation and
treatment pose diagnostic and therapeutic challenges.
A careful history is the key to narrowing the differential diagnosis and will allow for a more focused physical
examination. Prompt diagnosis and treatment may influence the visual outcome.
This topic will present an overview of the approach to patients with acute persistent visual loss. Transient visual
loss, the differential diagnosis of the red eye, and specific causes of acute vision loss are discussed separately.
(See "Amaurosis fugax (transient monocular or binocular visual loss)" and "Evaluation of the red eye".)
DEFINITION OF TERMS — Acute transient visual loss (TVL) is defined as a sudden deficit in visual function in one
or both eyes lasting less than 24 hours. It is caused by a temporary vascular occlusion in the circulation to the eye
or visual cortex, or by neuronal depression after a seizure or migraine [ 1]. Acute persistent visual loss (PVL) may
be defined as lasting at least 24 hours and is typically not caused by transient ischemia [2]. (See "Amaurosis
fugax (transient monocular or binocular visual loss)".)
ETIOLOGY — To achieve clear vision, light must follow an unhindered path from the front to the back of the eye,
traveling through the cornea, aqueous humor, lens, and vitreous humor to the retina (figure 1). Refracted by the
cornea and lens (and perhaps also by glasses or contact lenses), light is f ocused onto the retina where it is
transformed into an electrochemical signal by photoreceptors and supporting cells. The signal is transmitted via the
optic nerve through the visual pathways to the occipital lobes.
Alterations in function of any of the structures along the visual pathway may cause vision loss. Pathology can be
broadly divided into three major anatomic categories (table 1):
Media problems
Retinal problems
Neural visual pathway problems
Media problems include keratopathy, hyphema, lens changes, vitreous hemorrhage, uveitis, and, endophthalmitis.
Retinal disease includes vascular occlusion, retinal detachment, and acute maculopathy.
Neural visual pathway malfunction may be subdivided into optic nerve, chiasmal, and retrochiasmal pathology.
Media problems
Keratitis — Keratitis is inflammation of the cornea due to trauma, abrasive exposure, allergy, or infection. It is
marked by cloudiness, irregularity, or loss of epithelial or sub-epithelial corneal tissues. Typically the eye is tearing,
red, and painful or irritated.

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 2/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&searc… 2
Loss of epithelial cells is demonstrated by corneal uptake of fluorescein dye, creating a focal or diffuse green glow
under a cobalt blue light. Deeper corneal disease may be visible as a focal or diffuse white opacity, or by dulling of
the usually distinct reflection of light off of the cornea (corneal light reflex). The most common causes of keratitis
are infection (viral, bacterial, fungal) and trauma. Both can also cause corneal edema.
Corneal edema — Corneal swelling results in loss of corneal clarity. Examination may reveal dulling of the
corneal light reflex or a frank grey or white color to the substance of the cornea.
A serious cause of sudden corneal edema is acute angle-closure glaucoma. The patient with severely elevated
intraocular pressure (IOP) typically has nausea, vomiting, and may see colored halos around lights. The eye istearing, red, and extremely painful, often with ipsilateral brow ache. In angle closure, the pupil may be fixed in a
mid-dilated position, and biomicroscopic (slit lamp) examination may reveal a shallow anterior chamber. IOP is
often dangerously elevated (usually 40 to 80 mmHg). If formal tonometry is not available, severely elevated IOP may
be suspected by noting hardness to palpation in comparison to the fellow eye. (See "Angle-closure glaucoma".)
Hyphema — A hyphema is blood in the anterior chamber. It may result from blunt trauma or may occur
spontaneously in a handful of conditions marked by abnormal growth or fragility of iris blood vessels (often in
chronic poorly controlled diabetes). Biomicroscopic examination reveals red blood cells circulating and/or layered in
the anterior chamber. Intraocular pressure may become dangerously elevated. (See "Traumatic hyphema:
Epidemiology, anatomy, and pathophysiology" and "Traumatic hyphema: Clinical features and management".)
Lens changes — Changes in the size, c larity, or positioning of the crystalline lens may alter the focus of light
onto the retina, resulting in visual disturbance. Trauma or a variety of congenital conditions can lead to lens
dislocation and resultant vision loss. Lens clouding (cataract) does not typically occur acutely, except in the setting
of trauma. (See "Ectopia lentis (dislocated lens) in children".)
Elevated blood glucose can cause increased lens tumescence, altering the refractive error. If the change is great
enough, patients may perceive vision loss. Vision impairment typically resolves within days to weeks of
normalization of blood glucose.
Vitreous hemorrhage — Bleeding into the vitreous humor can occur in the setting of trauma, spontaneous
retinal tear, spontaneous vitreous detachment, or in any condition with retinal neovascularization (as in poorly
controlled diabetes).
The reduction in vision is directly proportional to the amount of blood in the vitreous. If the hemorrhage is dense
enough, there may be a decreased red reflex (the reddish orange reflection off the subretinal layers when examining
the eye with an ophthalmoscope), or the retina may not be visible with ophthalmoscopy.
Uveitis — Uveitis is the general term for inflammation inside the eye. Inflammation of the anterior structures of
the eye typically are associated with red, painful light sensitivity, whereas isolated inflammation of intermediate and
posterior structures may be associated with normal general appearance of the eye with decrease in the red reflex
and/or patient complaint of new floaters. (See "Uveitis: Etiology, clinical manifestations, and diagnosis".)
The most important cause of acute persistent visual loss in this category is endophthalmitis. Endophthalmitis is a
serious bacterial or fungal infection of all intraocular tissues, caused by surface pathogens (usually in the setting of
recent ocular surgery) or blood-borne agents. (See "Bacterial endophthalmitis" and "Treatment of endogenous
endophthalmitis due to Candida species" and "Treatment of exogenous endophthalmitis due to Candida species"
and "Treatment of endophthalmitis due to molds".)
The eye is tearing, red, and painful. Biomicroscopic examination reveals white blood cells in the anterior chamber,
vitreous space, or both. A layer of pus, called a hypopyon, may collect in the anterior chamber. Corneal edema and
a decreased red reflex may also be present.
Retinal problems
Retinal artery occlusion — Thrombosis, embolism, or arteritis of the central retinal artery results in retinal

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 3/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&searc… 3
ganglion cell damage, leading to severe, sudden, painless, central or paracentral visual loss [3]. (See "Central and
branch retinal artery occlusion".)
Within minutes to hours of the occlusion, the only abnormality noted on ophthalmoscopy may be vascular
narrowing. An embolus is visible in about 20 percent of patients with central retinal artery occlusion (CRAO) [3].
After several hours, the inner layer of the retina becomes ischemic, turning milky white, except in the fovea, which
appears as a cherry-red spot. An afferent papillary defect is typically present. (See 'Physical examination' below.)
The presence of giant cell arteritis must be ruled out. (See 'Giant cell arteritis' below.)
Retinal vein occlusion — Thrombosis of the central retinal vein results in venous stasis, leading to disc
swelling, diffuse nerve fiber layer and pre-retinal hemorrhage, and cotton wool spots that create a dramatic
appearance, often called "the blood and thunder" fundus (picture 1). Depending upon the degree of ischemia or
presence of macular edema, there may be need for retinal laser to prevent further vision loss or intravitreal injections
of anti-VEGF agents or corticosteroids to recover vision [4]. (See "Retinal vein occlusion: Epidemiology, clinical
manifestations, and diagnosis" and "Retinal vein occlusion: Treatment".)
While vision loss may be severe, the onset is typically subacute in contrast to the sudden visual loss typical of
CRAO. When venous stasis is severe, infarction may occur due to slowed retinal blood flow on the arterial side. In
this setting, a relative afferent papillary defect is often present.
Retinal detachment — Detachment of the neurosensory retina may occur spontaneously or in the setting of trauma. The most common form is due to a tear or break in the retina. Patients may describe sudden onset of new
floaters or black dots in their vision, often accompanied by flashes of light (photopsias). In its early stages, a
detachment may present as a persistent missing portion of the monocular visual field. Once the macula (central
retina) has become involved, visual acuity will be severely compromised. (See "Retinal detachment".)
Retinal detachment is not painful and does not cause a red eye. There may be a dulling of the red reflex, and
ophthalmoscopic examination may reveal the retina to be elevated with folds. If the detachment is extensive, there
may be a relative afferent pupillary defect.
Acute maculopathy — Conditions that affect the macula are associated with a central blind spot (scotoma),
blurred vision, or visual distortion. Alteration of the macula due to fluid leakage, bleeding, infection, or other causescan occur de novo or as an acute worsening of a chronic disease (eg, new edema in previously dry diabetic
retinopathy, or new bleeding in previously dry macular degeneration). Diagnosis usually requires detailed
ophthalmoscopy with a high magnification lens through pharmacologically dilated pupils.
Optic nerve problems — Optic nerve lesions usually produce monocular visual loss. Optic neuritis is the most
common cause of optic nerve disease in younger adults, while ischemic optic neuropathy is the most common
etiology in older patients. Acute visual loss can also occur when orbital cellulit is spreads to infect and damage the
optic nerve. (See "Optic neuropathies" and "Orbital cellulitis", section on 'Extraorbital extension'.)
Ischemic optic neuropathy — Ischemic optic neuropathy is generally categorized as anterior (affecting the
optic disc) or posterior (retrobulbar) and as arteritic or nonarteritic. Infarction at the optic nerve head due to
thrombosis or transient hypotension leads to a superior or inferior altitudinal visual field defect, or diffusely reduced
vision.
An afferent pupillary defect is typically present (see 'Physical examination' below). In anterior optic neuropathy, the
optic disc is swollen, often accompanied by splinter hemorrhages (picture 2 and picture 3). If nerve damage occurs
posterior to the globe, no abnormalities may be seen on initial ophthalmoscopic exam. (See "Nonarteritic anterior
ischemic optic neuropathy: Clinical features and diagnosis".)
Giant cell arteritis must be ruled out. (See 'Giant cell arteritis' below.)
Optic neuritis — Inflammation of the optic nerve may be associated with a variety of conditions, most notably
multiple sclerosis. Optic neuritis is the presenting feature in 15 to 20 percent of patients with multiple sclerosis, and

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 4/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&searc… 4
it occurs at some time during the course of the disease in 50 percent of patients [ 5]. (See "Optic neuritis:
Pathophysiology, clinical features, and diagnosis".)
Affected patients note pain on eye movement, reduced visual acuity and washed out color vision. An afferent
papillary defect is typically present (see 'Physical examination' below), and the optic disc is either normal or
swollen.
Papilledema — Elevated intracranial pressure can lead to transient visual obscurations or mild persistent
blurred vision. Examination reveals bilateral optic nerve swelling without relative afferent papillary defect. (See
"Overview and differential diagnosis of papilledema".)
Chiasmal problems — Involvement of the chiasm is suggested by visual loss of any type associated with pituitary
dysfunction or by a monocular or bitemporal hemianopia.
Compressive chiasmal lesions typically cause gradual decline in vision, as they impinge upon the chiasm, optic
nerve, or optic tract. Peripheral vision loss is often asymptomatic until visual acuity is compromised; therefore,
most visual complaints are of gradual blurring or dimming of vision. Sudden chiasmal vision loss is less common
and implies a rapidly expanding mass or an infectious, vascular, or inflammatory cause.
Ophthalmic examination may reveal optic disc pallor if the process is longstanding. Optic disc swelling may result
from papilledema (with third ventricle obstruction) or from an infiltrative or inflammatory process.
Chiasmal visual field defects classically involve the temporal fields and respect the vertical midline in one or both
eyes. Defects of ocular motility, due to palsies of the third, fourth, or sixth cranial nerve, may accompany chiasmal
lesions that extend into the cavernous sinus.
Pituitary apoplexy is relatively rare, occurring predominantly in patients with preexisting adenoma (see "Causes of
hypopituitarism"). Emergency steroid and other hormonal replacement, and/or transsphenoidal surgery, is often
indicated. The clinical syndrome is characterized by the acute onset of visual loss, headache, ophthalmoplegia,
and altered mental status due to hemorrhage or infarction of the pituitary gland, resulting in rapid expansion into the
suprasellar space and cavernous sinuses. Clinical suspicion mandates MRI, as CT may miss the lesion [6].
Retrochiasmal disorders
Homonymous hemianopia — Brain lesions in the region of the optic tract, the lateral geniculate body, the
optic radiations, or the visual cortex produce a loss of vision on one side of both visual fields (figure 2). The visual
field defect is relatively symmetric and respects the vertical midline. No other abnormalities are seen on ophthalmic
examination. The most common cause is stroke or hemorrhage into a brain tumor. (See "Homonymous
hemianopia".)
Cortical blindness — Extensive bilateral damage to the cerebral visual pathways may result in complete loss
of vision. Rarely, patients may confabulate and deny blindness, exhibiting a condition known as Anton syndrome.
Other than blindness, no other abnormalities are seen on ophthalmic examination.
Psychogenic problems — Patients describing visual loss without an organic basis are said to have "functional"
visual loss. Patients who are purposely feigning blindness are malingerers, whereas those who truly perceive
blindness have a conversion disorder. (See "Somatization: Epidemiology, pathogenesis, clinical features, medical
evaluation, and diagnosis", section on 'Terminology'.)
The visual loss may be monocular or binocular, total or sub-total.
Malingerers have been known to pharmacologically alter pupillary function.
Once organic disease has been ruled out, sophisticated ophthalmic techniques and slights of hand may be required
for proper diagnosis.
APPROACH TO THE PATIENT — Health care providers in the urgent setting most often do not have the equipment

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 5/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&searc… 5
or expertise to perform a comprehensive ophthalmic examination. Key history and exam points can help determine
the general category, if not the specific etiology, of vision loss. A symptomatic approach to the differential diagnosis
is presented in a table (table 2) and in an algorithm (algorithm 1).
History — The history of present illness should include inquiry about the following:
Timing — A distinction must be made between sudden onset of visual loss and sudden discovery of
preexisting visual loss. If the normal eye is inadvertently covered, a longstanding or gradual loss of vision in
the other eye may be mistaken for acute loss.
Laterality — Bilateral loss often suggests a retrochiasmal visual pathway disorder.
Quality — Monocular loss of a portion of peripheral vision suggests subtotal retinal detachment, ischemic
optic neuropathy, or branch retinal vascular occlusion. However, patients with a homonymous visual field
defect often perceive vision loss only in the eye ipsilateral to the visual field cut.
Pain — Keratitis produces a sharp superficial pain, acute glaucoma produces a deep brow ache with nausea
and vomiting, endophthalmitis may also produce a deep boring pain, and optic neuritis produces pain worse
with eye movement. Other causes of vision loss are typically painless.
Redness — Patients with keratitis, acute glaucoma, and uveitis usually present with conjunctival hyperemia
(red eye).
Associated symptoms — Neurologic deficits can accompany a stroke (homonymous defect) or multiple
sclerosis (optic neuritis). Nausea and vomiting accompany severely elevated intraocular pressure.
Rhinorrhea is common when tearing is present. Some patients with monocular or binocular vision loss
complain of a vague sense of disorientation or difficulty with balance and depth perception.
Trauma — Mild trauma can cause keratitis or uveitis; more severe trauma can cause hyphema, vitreous
hemorrhage, traumatic cataract, retinal detachment, or traumatic optic neuropathy. Trauma with a sharp or
blunt object may produce a ruptured globe.
Elements of the past medical history should focus on the following:
Vascular disease — Patients with diabetes, coronary artery disease, hypertension, hypercoagulability, or
vascular risk factors are at increased risk for retinal vascular occlusion, ischemic optic neuropathy, or visual
pathway stroke. Patients with pre-existing diabetic retinopathy can experience a vitreous hemorrhage or
acute maculopathy.
Refractive status — Highly-nearsighted (myopic) eyes have a higher incidence of retinal tears, leading to
retinal detachment [7]. Patients who have had refractive surgery to correct for myopia still have increased
risk.
Contact lens wear — Contact lens wear is a risk factor for microbial keratitis, especially with soft lenses andwhen lenses are used improperly (poor hygiene, overnight wear, contaminated solutions) [8].
Eye surgery — Previous procedures may put certain patients at increased risk for uveitis, corneal edema,
acute glaucoma, maculopathy, or retinal detachment. Cataract surgery, the most commonly performed
ophthalmic procedure in Americans over age 65, can lead to retinal detachment in 0.6 to 1.7 percent of
patients during the first postoperative year [7]. In a systematic review of the literature, cataract surgery-
associated endophthalmitis was found to have an overall reported incidence of 0.13 percent, with a trend
toward significant increases over the past decade [9].
Medications — Many systemic medications are associated with ocular side effects. Most produce visual
symptoms gradually, associated with high dosages and/or with prolonged use. Medications that are

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 6/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&searc… 6
associated with acute visual loss include the following:
Anticholinergics: loss of accommodation, angle closure glaucoma
Bisphosphonates: uveitis
Digoxin: yellow vision
Rifabutin: uveitis
Sildenafil: blue vision, ischemic optic neuropathy
Sulfonamides: myopia
Topiramate: angle closure glaucoma.
Physical examination — The eye examination should include the following elements:
General inspection — noting erythema, tearing, light sensitivity
Visual acuity — to be tested with glasses, one eye at the time
Evaluation of extraocular movement
Confrontation visual fields
Pupils — symmetry, reactivity to light, pupillary reflex
Fluorescein application
Intraocular pressure testing (by tonometry or palpation)
Pen light or slit lamp exam (with examination for red-reflex symmetry) (see "Slit lamp examination")
Ophthalmoscopic examination
An afferent pupillary defect is demonstrated by shining a light alternately in one eye and then the other and finding
that the direct response to light is more sluggish in the affected eye. The room should be dark, and the patientshould fixate on a distant target to prevent miosis due to accommodation. (See "The detailed neurologic
examination in adults", section on 'Afferent pupillary defect'.)
The presence of an afferent pupillary defect is fairly specific for unilateral optic nerve pathology, and generally does
not occur with media or retinal problems.
Fluorescein staining is seen in keratitis, corneal abrasion, and corneal edema.
Abnormalities in the visual pathways posterior to the optic chiasm can be distinguished by the presence of a
homonymous visual field defect, often detectable with confrontation field testing (figure 2). Retrochiasmal tumors
may also cause palsy of the sixth cranial nerve. Alterations in the red reflex are seen in most media opacities and
in retinal detachment. More subtle retinal findings are best visualized with a detailed retinal examination followingpupil dilation with mydriatic eyedrops.
Patient triage — Appropriate management of acute persistent visual loss hinges on understanding the urgency for
treatment or referral to an ophthalmologist.
Immediate treatment is required for:
Acute central retinal artery occlusion (see "Central and branch retinal artery occlusion")
Intraocular pressure greater than 40 mmHg with eye pain (see "Angle-closure glaucoma")
Vision loss in the setting of suspected giant cell arteritis (see "Treatment of giant cell (temporal) arteritis")

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 7/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&searc… 7
Emergent referral is required for:
Infectious keratitis (See topics on specific infections, eg, herpes simplex type I, amoeba, fusarium)
Endophthalmitis (see "Bacterial endophthalmitis" and "Treatment of endogenous endophthalmitis due to
Candida species" and "Treatment of exogenous endophthalmitis due to Candida species" and "Treatment of
endophthalmitis due to molds")
Hyphema
Retinal detachment (see "Retinal detachment")
Urgent referral (within 24 to 48 hours) is appropriate for:
Non-infectious uveitis (see "Uveitis: Treatment")
Vitreous hemorrhage
Acute maculopathy
Central retinal vein occlusion
Optic neuritis (see "Optic neuritis: Prognosis and treatment")
Visual manifestations of intracranial pathology (stroke, tumor, bleed, or elevated intracranial pressure) should be
treated in the appropriate neurological or neurosurgical fashion.
Immediate treatment
Central retinal artery occlusion — Proposed treatments for central retinal artery occlusion (CRAO) are based
upon the principle that vision loss may be reversible if blood flow is restored quickly, before ganglion cell death
occurs. This window may be approximately 100 minutes, based on primate studies, although clinical observation
have found that some visual recovery may occur after as many as 48 hours of ischemia [10]. The effectiveness of
treatments for CRAO has not been established in randomized trials [11].
Proposed interventions are numerous, but most include an immediate attempt to lower the intraocular pressure with
digital massage, paracentesis, or pharmacologic agents. (See "Central and branch retinal artery occlusion".)
Giant cell arteritis — Giant cell arteritis (GCA) as the cause of CRAO or ischemic optic neuropathy is more
common in older patients (>50 years), women, and Caucasians. Patients may present with a temporal headache,
scalp tenderness, jaw claudication, fever, weight loss, fatigue, and/or night sweats. The reported incidence of ocular
involvement ranges between 14 and 70 percent [12]. An elevated erythrocyte sedimentation rate (ESR) or C-reactive
protein (CRP) may suggest the diagnosis, but the diagnostic gold standard is a temporal artery biopsy. (See
"Diagnosis of giant cell (temporal) arteritis".)
Patients with suspected GCA and ocular involvement are started on methylprednisolone 1000 mg IV daily for one to
three days, followed by prednisone 60 mg/d for two to four weeks. While cases of visual improvement following
treatment have been reported, vision loss is typically considered irreversible. (See "Treatment of giant cell
(temporal) arteritis".)
Acutely elevated intraocular pressure — Although the definitive treatment for angle-closure glaucoma is
laser or surgical peripheral iridotomy, initial treatment should be directed toward rapidly lowering the intraocular pressure. Irreversible vision loss may occur within hours if IOP remains above 40 mmHg. (See "Angle-closure
glaucoma".)
Initial management involves prompt administration of pressure-lowering eye drops. A possible regimen would be one
drop each, one minute apart, of [13]:
0.5% timolol maleate (Timoptic),
1% apraclonidine (Iopidine), and
2% pilocarpine (Isopto Carpine)
Systemic medications (oral or IV acetazolamide, IV mannitol, or oral glycerol or isosorbide) to control the
http://www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual-loss/abstract/13
http://www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual-loss/abstract/12
http://www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual-loss/abstract/11

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 8/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&searc… 8
intraocular pressure are often given. We suggest giving the patient two 250 mg tablets of acetazolamide in the office
[13]. Patients who are allergic to sulfa and sickle cell patients or those who are in crisis or have a hyphema and
elevated intraocular pressure should not be given acetazolamide.
Systemic medications other than oral acetazolamide should be administered under the guidance of an
ophthalmologist, since angle closure should be confirmed before they are given.
The eye pressure should be checked 30 to 60 minutes after giving pressure-lowering drops and oral acetazolamide.
Although no standard rate of reduction for intraocular pressure exists, one study identified a satisfactory reduction
as pressure less than 35 mmHg or a reduction greater than 25 percent of presenting pressure [14].
Emergent referral — Microbial keratitis can lead to permanent scarring or corneal perforation if not treated
promptly with appropriate topical antibiotics. Corneal biopsy or culture may be required to determine pathogen
sensitivity.
Endophthalmitis should be immediately treated with an intravitreal injection and occasionally with emergent
surgery. Collection of intraocular fluid is also performed to determine pathogen sensitivity. (See "Bacterial
endophthalmitis".)
Hyphema can induce dangerously high eye pressure and possible permanent corneal blood staining. It requires
detailed, often daily, examination to ensure that rebleeding does not occur. Surgical intervention is occasionally
required to clear the anterior chamber of blood.
Retinal detachment in which visual acuity is preserved should be surgically repaired immediately to prevent
extension of the detachment to the macula. Once the macula is involved in a retinal detachment, the prognosis for
a good visual outcome is less favorable. Macula-involving retinal detachments should be repaired within one week to
achieve the best possible visual outcome [15]. (See "Retinal detachment".)
SUMMARY
Acute persistent visual loss (PVL), defined as a sudden deficit in visual function in one or both eyes lasting
more than 24 hours, is distinguished from acute transient visual loss (amaurosis fugax). Whereas amaurosis
fugax is caused by only a few conditions (temporary vascular occlusion or temporary neuronal depression
related to seizure or migraine), the differential diagnosis of PVL is large. (See 'Definition of terms' above.)
Conditions that cause PVL can be divided into three categories: media problems, retinal problems, or neural
visual pathway problems. Media problems include keratitis, corneal edema, hyphema, lens changes,
vitreous hemorrhage, and uveitis. Retinal problems include vascular occlusion, retinal detachment, and acute
maculopathy. Neural visual pathway malfunction may be subdivided into optic nerve disease, chiasmal, and
retrochiasmal visual pathway pathology. (See 'Etiology' above.)
Healthcare providers in the urgent setting most often do not have the equipment or expertise to perform a
comprehensive ophthalmic examination. However, a thorough, focused history and initial eye examination
can help determine the general category, if not the specific cause, of vision loss (table 2 and algorithm 1).
(See 'History' above and 'Physical examination' above.)
Appropriate management of acute persistent visual loss depends on understanding the urgency for treatment
or referral to an ophthalmologist. (See 'Patient triage' above.)
The treatment of acute persistent visual loss depends on the specific diagnosis. The following causes require
immediate treatment: central retinal artery occlusion, giant cell arteritis, and acutely elevated intraocular
pressure. (See 'Immediate treatment' above.)
Use of UpToDate is subject to the Subscription and License Agreement.
http://www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual-loss/abstract/15

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 9/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&searc… 9
REFERENCES
1. Burde R, Savino P, Trobe J. Clinical Decisions in Neuro-ophthalmology, 3rd ed, Mosby, 2002.
2. Trobe JD. The Physician's Guide to Eye Care, 2nd ed, The Foundation of the American Academy of
Ophthalmology, San Francisco 2001.
3. Rumelt S, Brown GC. Update on treatment of retinal arterial occlusions. Curr Opin Ophthalmol 2003; 14:139.
4. London NJ, Brown G. Update and review of central retinal vein occlusion. Curr Opin Ophthalmol 2011; 22:159.
5. Balcer LJ. Clinical practice. Optic neuritis. N Engl J Med 2006; 354:1273.
6. Liu GT, Volpe NJ, Galetta SL. Vision loss: Disorders of the Chiasm. In: Neuro-Ophthalmology Diagnosis and
Management, WB Saunders Company, 2001.
7. Lois N, Wong D. Pseudophakic retinal detachment. Surv Ophthalmol 2003; 48:467.
8. Schein OD, Buehler PO, Stamler JF, et al. The impact of overnight wear on the risk of contact lens-
associated ulcerative keratitis. Arch Ophthalmol 1994; 112:186.
9. Taban M, Behrens A, Newcomb RL, et al. Acute endophthalmitis following cataract surgery: a systematic
review of the literature. Arch Ophthalmol 2005; 123:613.
10. Fraser S, Siriwardena D. Interventions for acute non-arteritic central retinal artery occlusion. Cochrane
Database Syst Rev 2002; :CD001989.
11. Hazin R, Dixon JA, Bhatti MT. Thrombolytic therapy in central retinal artery occlusion: cutt ing edge therapy,
standard of care therapy, or impractical therapy? Curr Opin Ophthalmol 2009; 20:210.
12. Rahman W, Rahman FZ. Giant cell (temporal) arteritis: an overview and update. Surv Ophthalmol 2005;
50:415.
13. Saw SM, Gazzard G, Friedman DS. Interventions for angle-closure glaucoma: an evidence-based update.
Ophthalmology 2003; 110:1869.
14. Choong YF, Irfan S, Menage MJ. Acute angle closure glaucoma: an evaluation of a protocol for acute
treatment. Eye (Lond) 1999; 13 ( Pt 5):613.
15. Ross WH. Visual recovery after macula-off retinal detachment. Eye (Lond) 2002; 16:440.
Topic 6902 Version 13.0
http://www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual-loss/abstract/15
http://www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual-loss/abstract/14
http://www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual-loss/abstract/13
http://www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual-loss/abstract/12
http://www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual-loss/abstract/11

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 10/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&sear… 10
GRAPHICS
Anatomy of the eye

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 11/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&sear… 1
Causes of acute persistent visual loss - Anatomic
Media problems
Keratitis
• Infectious or non-infectious
Corneal edema
• Acute glaucoma (primarily)
Hyphema
• Spontaneous or traumatic
Alterations in crystalline lens
• Thickening, clouding or dislocation
Vitreous hemorrhage
• Spontaneous or traumatic
Uveitis
Retina problems
Retinal vascular occlusion (CRAO, CRVO)
Retinal detachment
Acute maculopathy
Problems of the neural visual pathway
Optic neuropathy
• Ischemia, inflammatory, or infectious process
Papilledema
• Elevated intracranial pressureChiasmal disorders
• Pituitary apoplexy (primarily)
Retrochiasmal disorders
• Brain lesions in the visual pathway
Other considerations
Trauma as a cause of any of the above
Acute glaucoma
• Vision loss due to corneal edema and/or optic nerve ischemia in the setting of severely elevated
intraocular pressure
Functional visual loss
CRAO: central retinal artery occlusion; CRVO: central retinal vein occlusion.

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 12/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&sear… 12
Retinal vein occlusion
Courtesy of Don C Bienfang, MD.

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 13/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&sear… 13
Normal fundus appearance

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 14/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&sear… 14
Optic neuritis fundus
Papillitis: Note the absence of hemorrhages and exudates in thesetting of optic neuritis.
7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 15/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&sear… 15
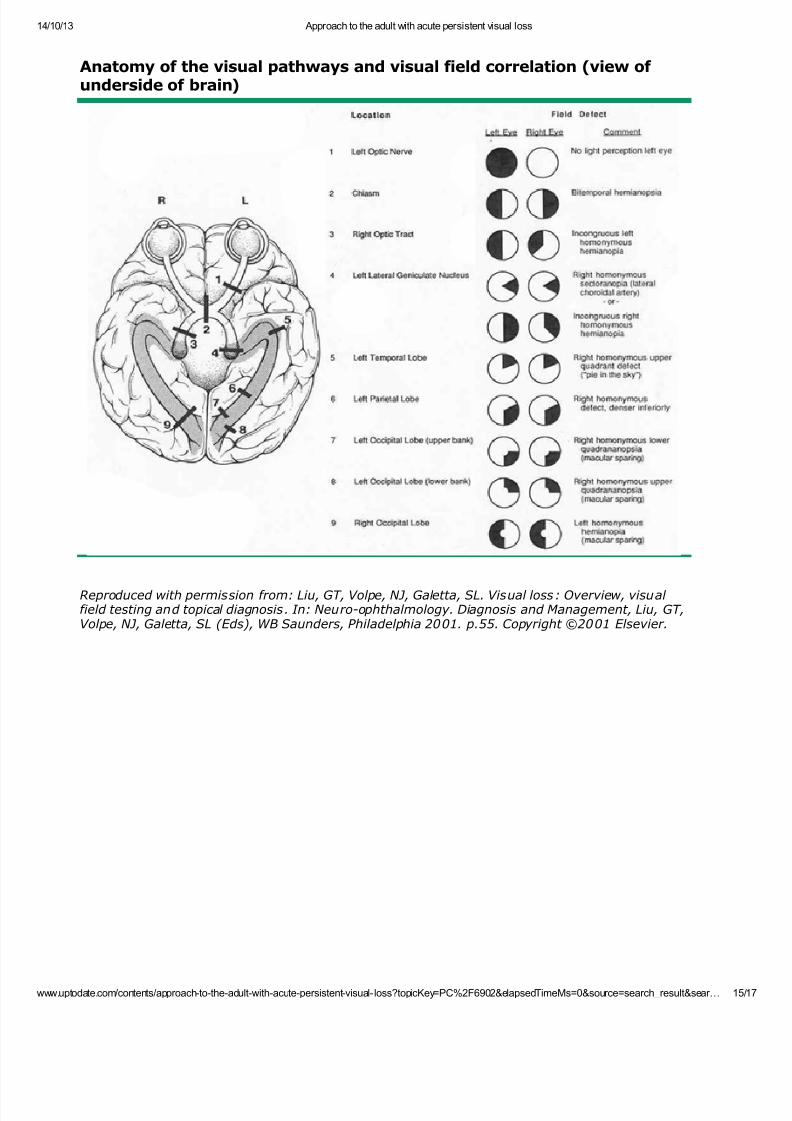
Anatomy of the visual pathways and visual field correlation (view of underside of brain)
Reproduced with permission from: Liu, GT, Volpe, NJ, Galetta, SL. Visual loss: Overview, visual field testing and topical diagnosis. In: Neuro-ophthalmology. Diagnosis and Management, Liu, GT,Volpe, NJ, Galetta, SL (Eds), WB Saunders, Philadelphia 2001. p.55. Copyright ©2001 Elsevier.

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 16/17
14/10/13 Approach to the adult with acute persistent visual loss
www.uptodate.com/contents/approach-to-the-adult-with-acute-persistent-visual- loss?topicKey=PC%2F6902&elapsedTimeMs=0&source=search_result&sear… 16
Causes of acute persistent visual loss - Symptomatic
Presentation Differential diagnosis
Unilateralpainless
Lens dislocation
Vitreous hemorrhage
Acute maculopathy
Retinal detachment
Retinal artery occlusion
Retinal vein occlusion
Ischemic optic neuropathy
Unilateral painful Corneal abrasion
Keratitis
Acute glaucoma
Hyphema
Endophthalmitis
Anterior uveitis
Optic neuritis
Bilateral painless Pseudotumor cerebri (variable symptoms)
Metabolic or toxic (hyperglycemia, methanol toxicity)
Homonymous field loss (chiasmal or retrochiasmal etiology)
Bilateral painful Keratitis from bilateral exposure (eg, contact lens, UV light, chemical,etc)
Adapted from Guluma, K. An Evidence-Based Approach to Abnormal Vision. Emergency MedicinePractice 2007; 9:1.

7/22/2019 Approach to the Adult With Acute Persistent Visual Loss
http://slidepdf.com/reader/full/approach-to-the-adult-with-acute-persistent-visual-loss 17/17
14/10/13 Approach to the adult with acute persistent visual loss
Considerations in diagnosing acute persistent visual loss*
* These are considerations only. Clinical picture must otherwise fit.Δ While corneal abras ion and keratitis are most common in patients who wear contact lenses,other sources of acute persistent visual loss should be considered if findings do not confirmabrasion or keratitis.
Related Documents











