Vaginal bleeding in 2 nd Half of pregnancy (Ante-partum hemorrhage) Yahyia Al-Abri 90440

approach to patient vaginal bleeding in 2nd half of pregnancy
Jan 22, 2018
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Vaginal bleeding in 2nd Half of pregnancy
(Ante-partum hemorrhage)
Yahyia Al-Abri
90440

Objectives
• Antepartum hemorrhage – Definition
– Causes
• Case scenario
• Placenta previa
• Placental abruption
• Vasa previa
• Uterine rupture
Definition
• Bleeding from or in to the genital tract, occurring from 24 + weeks of pregnancy and prior to the birth of the baby. (Royal College of Obstetricians
and Gynecologists )
• Uterine bleeding after 20 weeks of gestation that is unrelated to labor and delivery. (UPTODATE)
Causes
Common
– Abruptio placentae
– Placenta previa
– Preterm labor
Uncommon
– Uterine rupture
– Vasa previa
– Cervical lesion (cervicitis, polyp, ectropion, cervical cancer)
– Other:coagulopathy.
Hacker and moore
Case scenario
• H is 30 years old lady pramigarvida at 30 week of gestation she presented to the A/E with P/V bleeding.– LMP: 11/5/2016– EDD: 15/2/2017– Admission : 09/12/2016
– The bleeding started 1 hour ago low in amount. She noted the bleeding while she was passing urine. She had two episodes in less than 24 hours.
– no abdominal pain– no dysuria– No fever– No other complain– good fetal movements
Case scenario
• Past medical:– GDM on Insulin (N15/8 units, R5/5 units) and Metformin 500 mg BID.– No HTN – No bleeding disorder
• Family history not remarkable • Gyne
– Regular period every 28 days bleeding for 4 -5 days– Never used of contraceptive – No pap smear done
• Obstetric – Planed pregnancy .Anomaly scan on 13/10/2016 no gross anomaly
seen
• Family history:- mother diabetic
Case scenario
• On examination:– Looks well.
– Vitally stable.• T: 36.5
• P: 88
• BP: 130/80
• saturation 98%
– Patient abdomen: soft, relaxed uterus, no tenderness.
– Patient cervix : no bleeding, os closed.
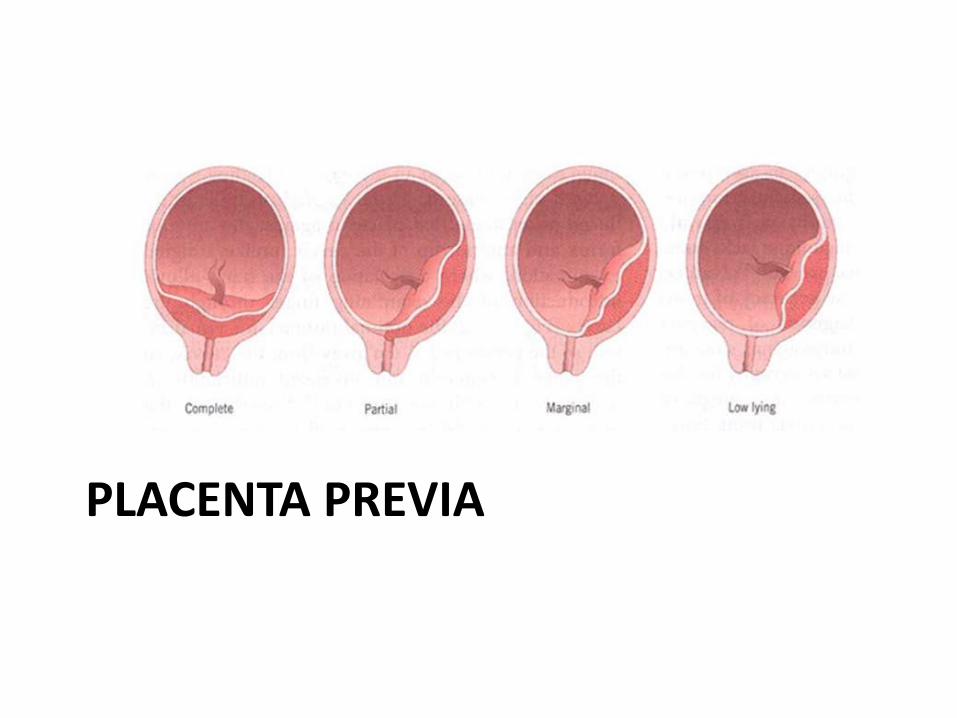
PLACENTA PREVIA
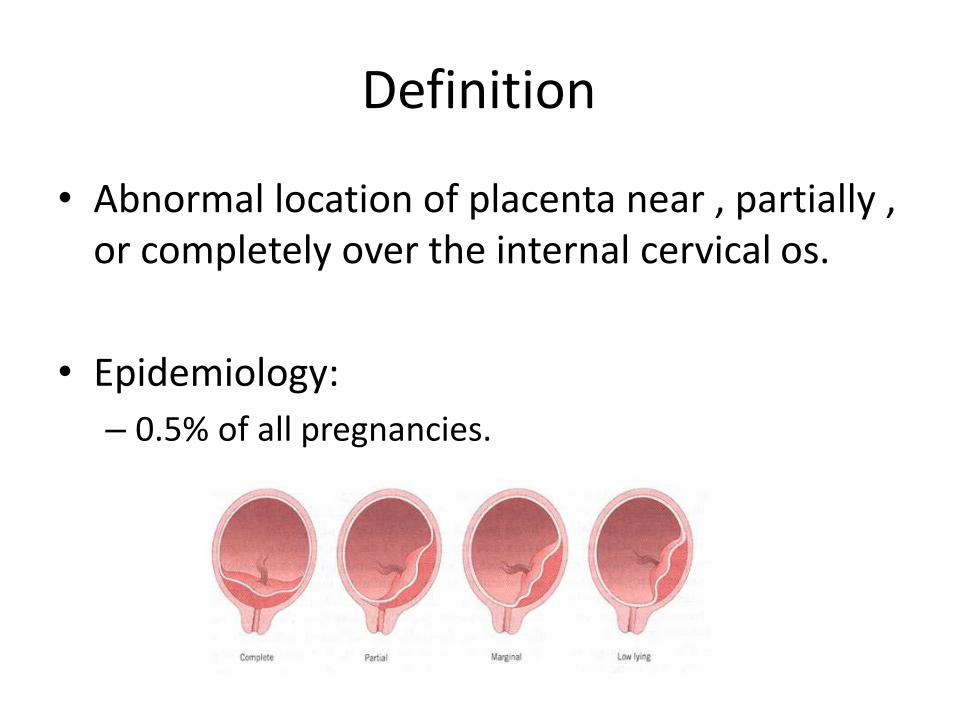
Definition
• Abnormal location of placenta near , partially , or completely over the internal cervical os.
• Epidemiology:
– 0.5% of all pregnancies.
Risk factors
– Multiparty.
– Increasing maternal age.
– History of prior placenta previa.
– Multiple gestation
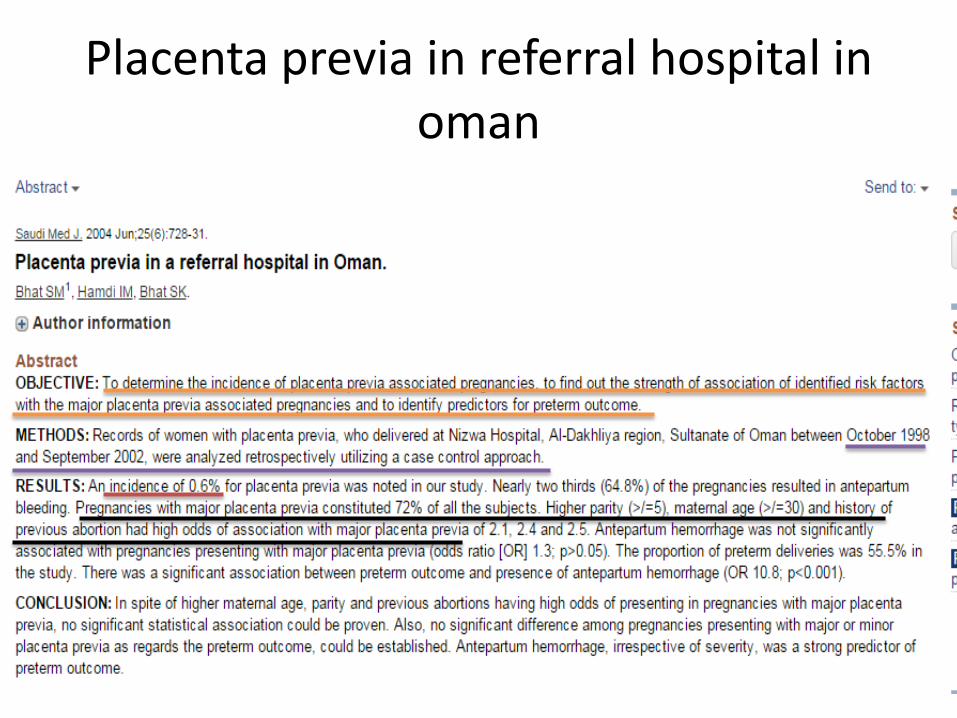
Placenta previa in referral hospital in oman
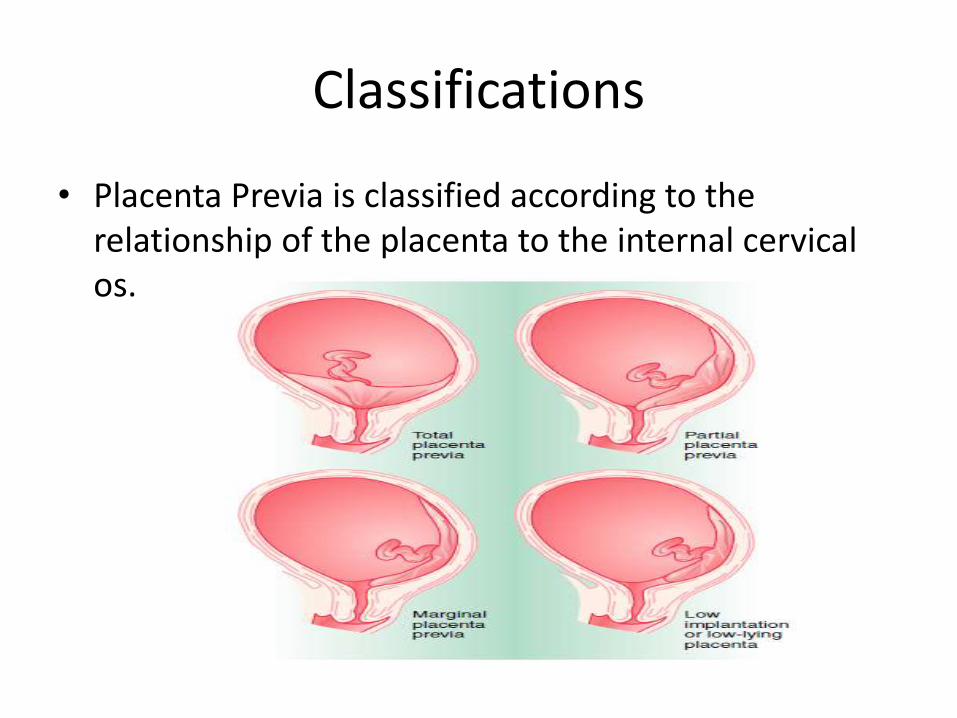
Classifications
• Placenta Previa is classified according to the relationship of the placenta to the internal cervical os.
Clinical features
• PAINLESS bright red vaginal bleeding (recurrent)
• Shock/anemia correspond to degree of apparent blood loss.
• Uterus soft and non-tender
• Malpresentation, failure of the fetal head to engage.
• FHR usually normal
Do NOT perform a vaginal exam until placenta previa has been ruled out by U/S
Investigations(laboratory)
• CBC ( hemoglobin, platelet).
• Coagulation profile(INR/aPTT).
• Blood group type and Cross match.
• CTG ( fetal monitoring )
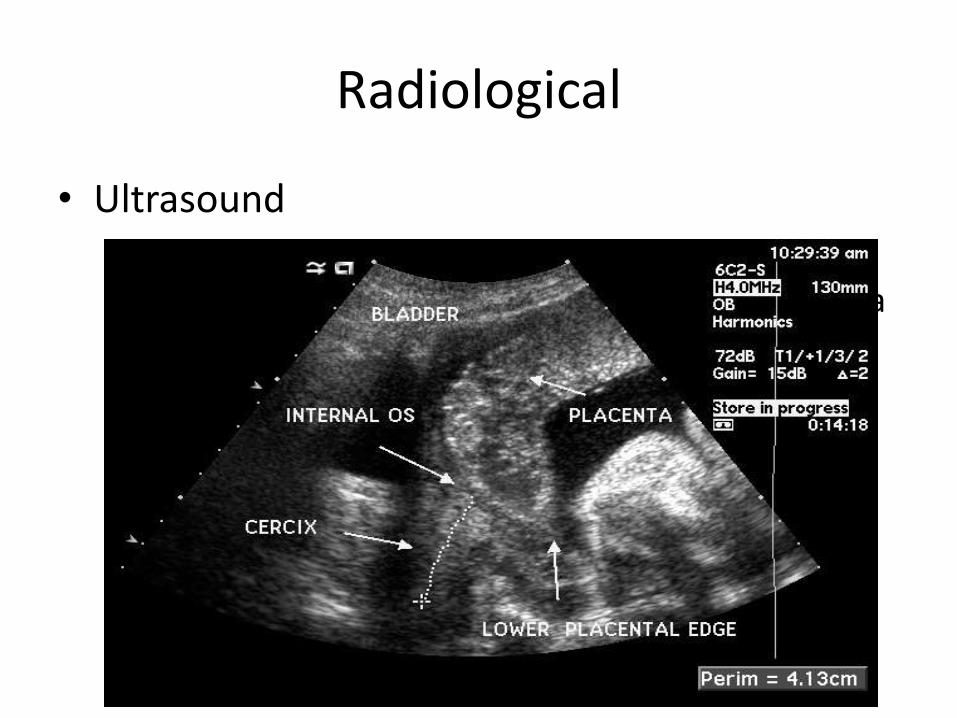
Radiological
• Ultrasound
– Transvaginal U/S is more accurate than transabdominal U/S at diagnosing placenta previaat any gestational age.
Placenta previa
• Treatment:
– Asymptomatic placenta previa:
1. monitor placental position with ultrasound examination as an outpatient
2. avoid vaginal intercourse, digital examination, avoid exercise
3. Advise to seek immediate medical attention if contractions or vaginal bleeding occur
4. Delivery by C-section at 37 weeks
Management
• Symptomatic
• Stabilize and monitor– Maternal stabilization: large bore IV lines with
hydration, O2 for hypotensive patients.
– Maternal monitoring: vitals, urine output, blood loss.
– CTG.
– U/S assessment: • Determine fetal viability.
• Placental status/position.

Management
GA <37 weeks and minimal bleeding: • Expectant management
• Admit to hospital• Limited physical activity, no douches,
enemas, • Consider corticosteroids for fetal lung
maturity• Delivery when fetus is mature or
hemorrhage is excessive
GA ≥37 weeks, and/or bleeding is excessive:
• Delivery must be accomplished by• C-section regardless of gestational
age!
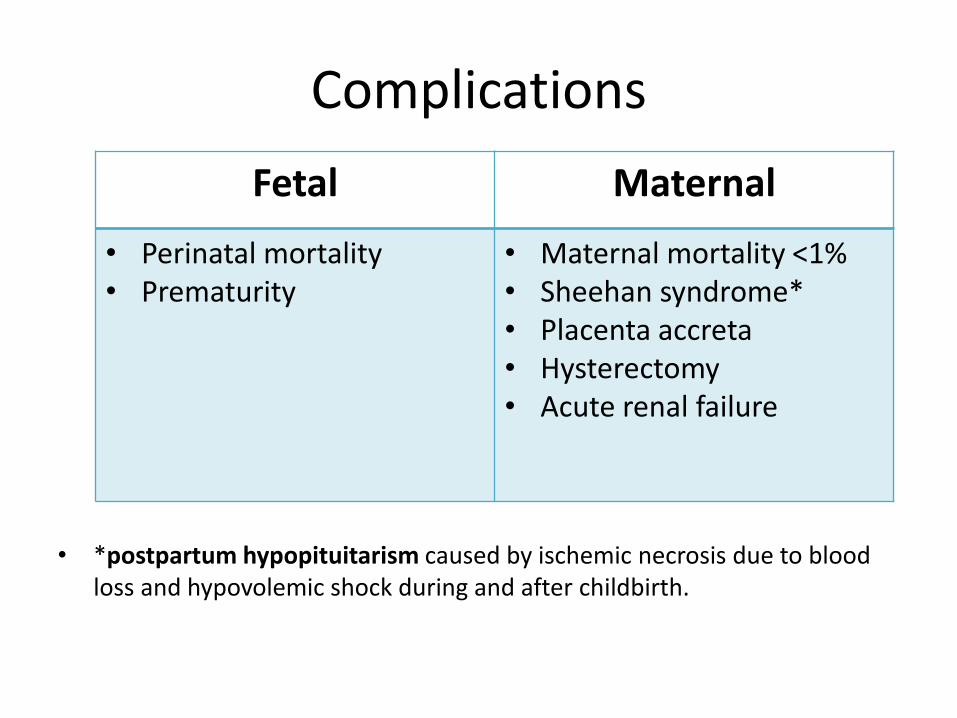
Complications
• *postpartum hypopituitarism caused by ischemic necrosis due to blood loss and hypovolemic shock during and after childbirth.
Fetal Maternal
• Perinatal mortality • Prematurity
• Maternal mortality <1%• Sheehan syndrome*• Placenta accreta• Hysterectomy • Acute renal failure
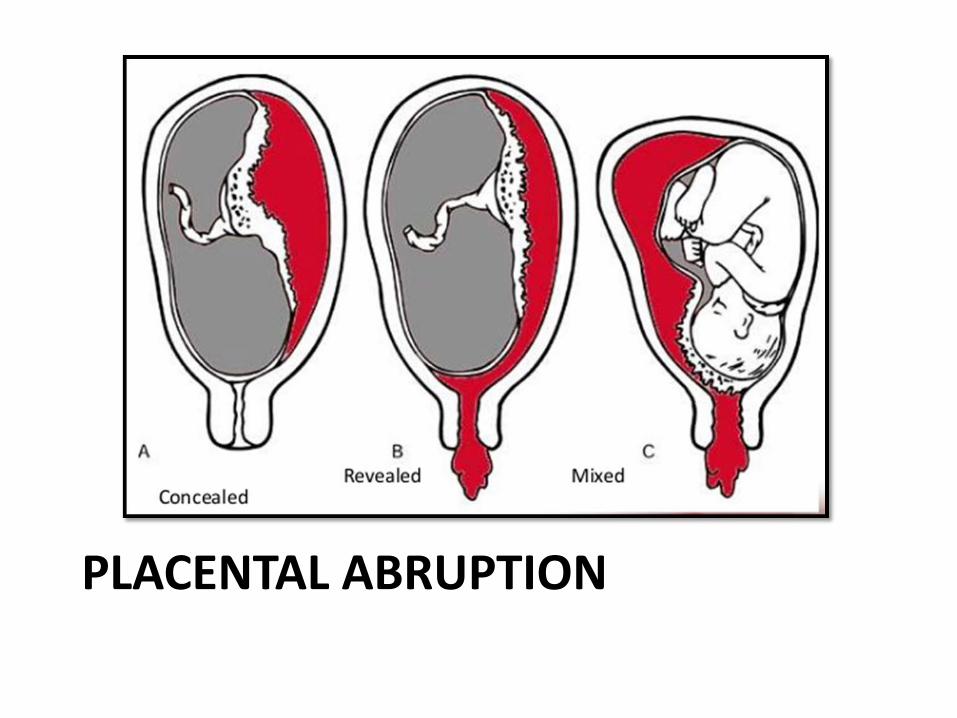
PLACENTAL ABRUPTION
Definition
• Premature separation of normal implanted placenta from the uterine wall before the delivery of the fetus.
• Epidemiology :
– 0.5% to 1.5% of all pregnancies.
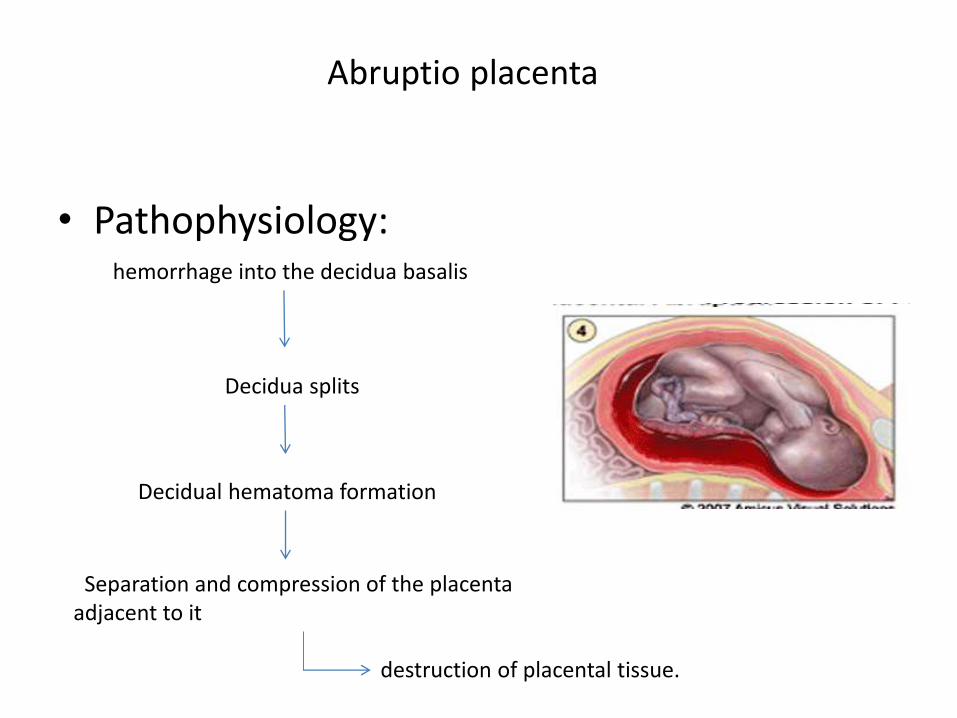
Abruptio placenta
• Pathophysiology:hemorrhage into the decidua basalis
Decidua splits
Decidual hematoma formation
Separation and compression of the placenta adjacent to it
destruction of placental tissue.
Perinatal mortality in Oman
Risk factors
• Maternal hypertension (most common factor).
• History of placental abruption in a prior pregnancy.
• Trauma.
• Premature rupture of membranes.
• Short umbilical cord.
• Smoking.
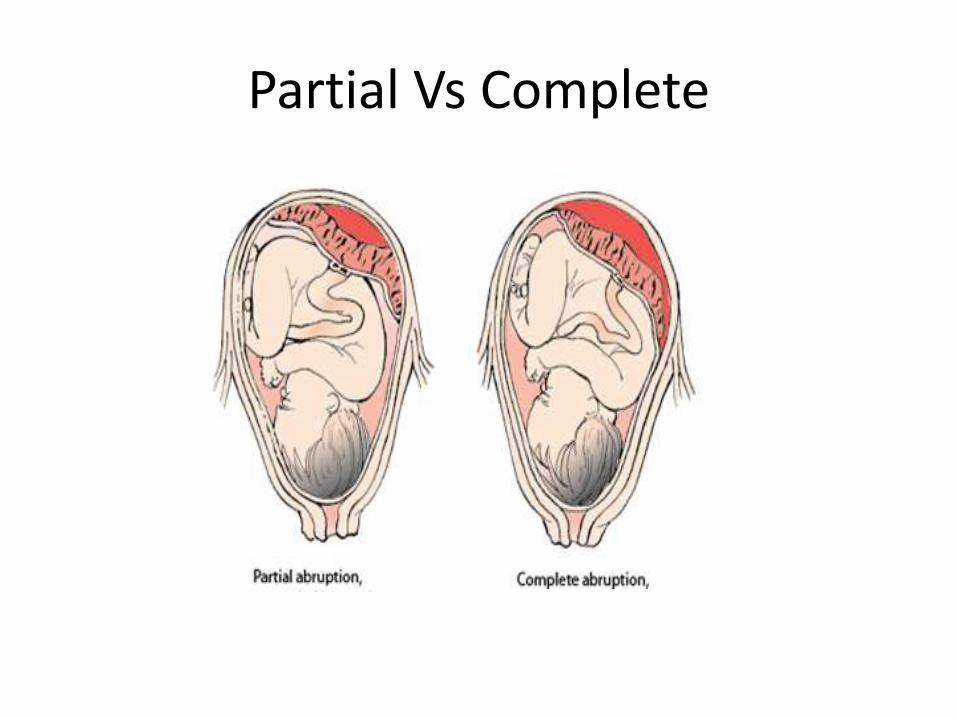
Partial Vs Complete
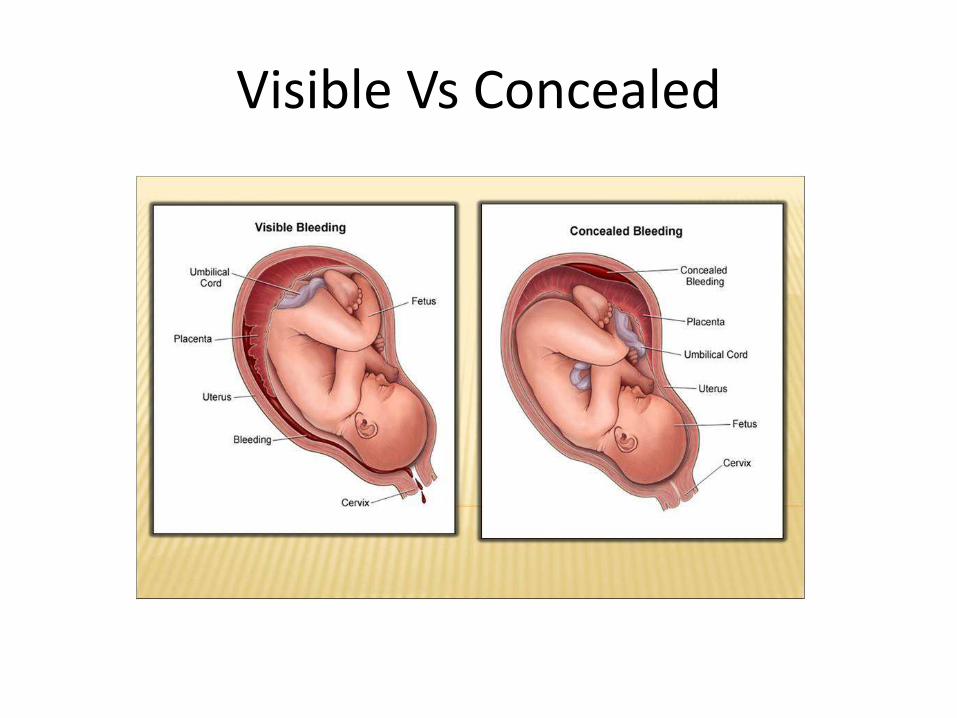
Visible Vs Concealed
Clinical features
• PAINFUL (80%) vaginal bleeding
– bleeding not always present if abruption is concealed.
• Pain
– sudden onset, constant, localized to lower back and uterus.

Clinical features
• O/E
– General condition depends on the amount of bleeding (shock/anemia out of proportion to apparent blood loss)
– Uterus is Hard and Tender
– nonreassuring FH, reduced or absent fetal movements, fetal distress
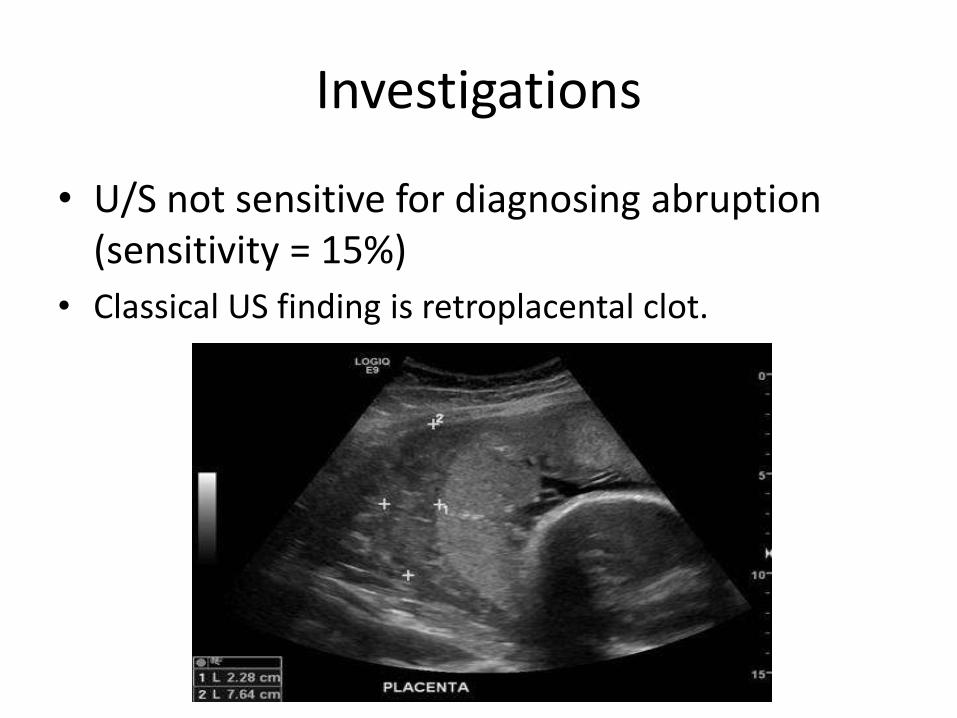
Investigations
• U/S not sensitive for diagnosing abruption (sensitivity = 15%)
• Classical US finding is retroplacental clot.
Management
• Stabilization & monitoring :
– Maternal stabilization: large bore IV with hydration, O2 for hypotensive patients.
– Maternal monitoring: vitals, urine output, blood loss.
– CTG.
– Blood products on hand, because of DIC risk.
Management
• Mild abruption– GA <37 weeks: use serial Hct to assess concealed
bleeding, deliver when fetus is mature or when hemorrhage is excessive.
– GA ≥37 weeks: stabilize and deliver.
• Moderate to severe abruption– Immediate delivery.
– Vaginal delivery if no contraindication and no evidence of fetal or maternal distress OR fetal demise.
– C/S if there is fetal or maternal distress.
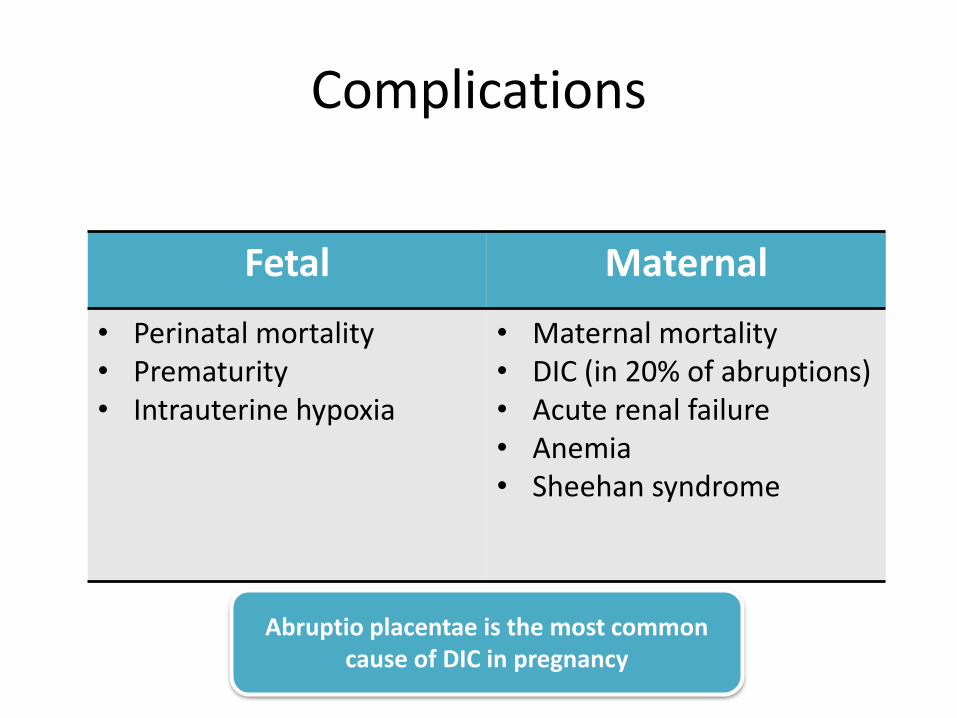
Complications
Fetal Maternal
• Perinatal mortality• Prematurity• Intrauterine hypoxia
• Maternal mortality• DIC (in 20% of abruptions)• Acute renal failure• Anemia• Sheehan syndrome
Abruptio placentae is the most common cause of DIC in pregnancy
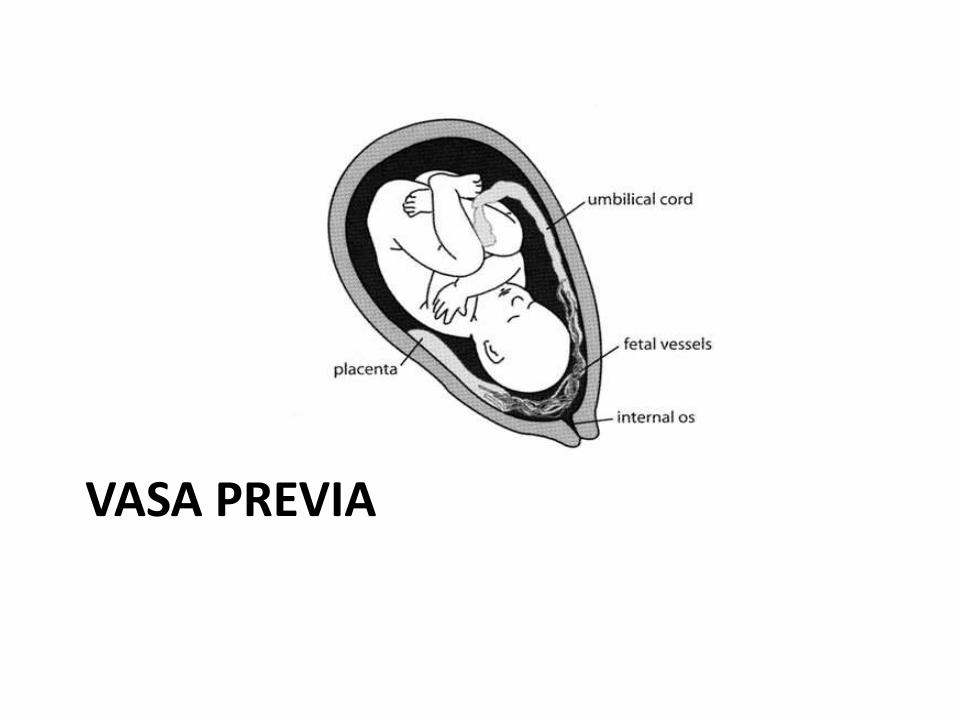
VASA PREVIA
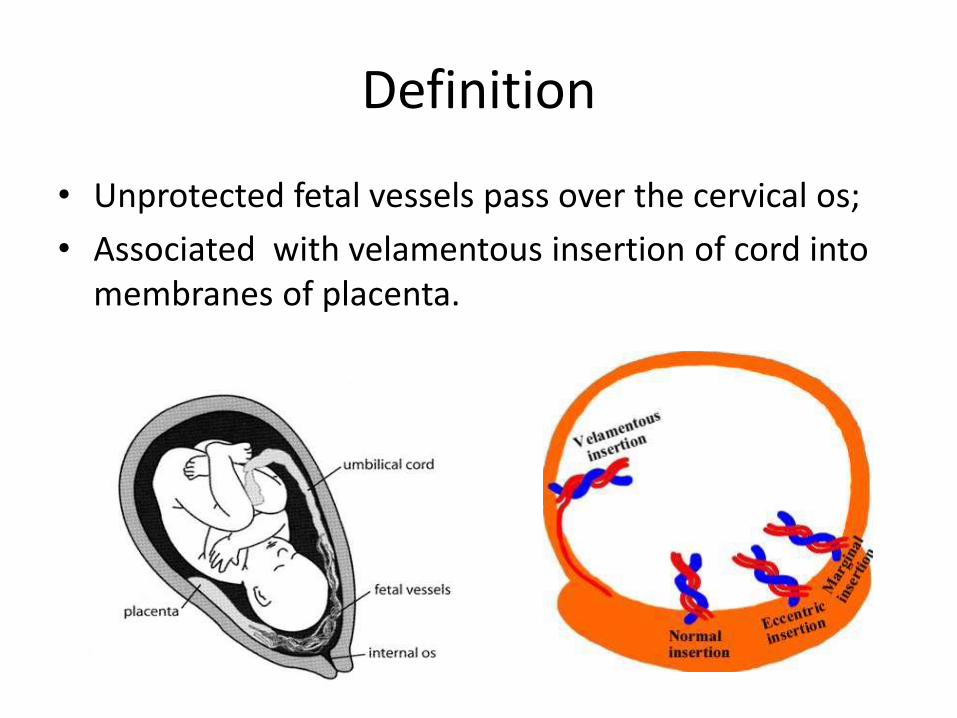
Definition
• Unprotected fetal vessels pass over the cervical os;
• Associated with velamentous insertion of cord into membranes of placenta.
Clinical Features
• PAINLESS vaginal bleeding .
• Fetal distress.
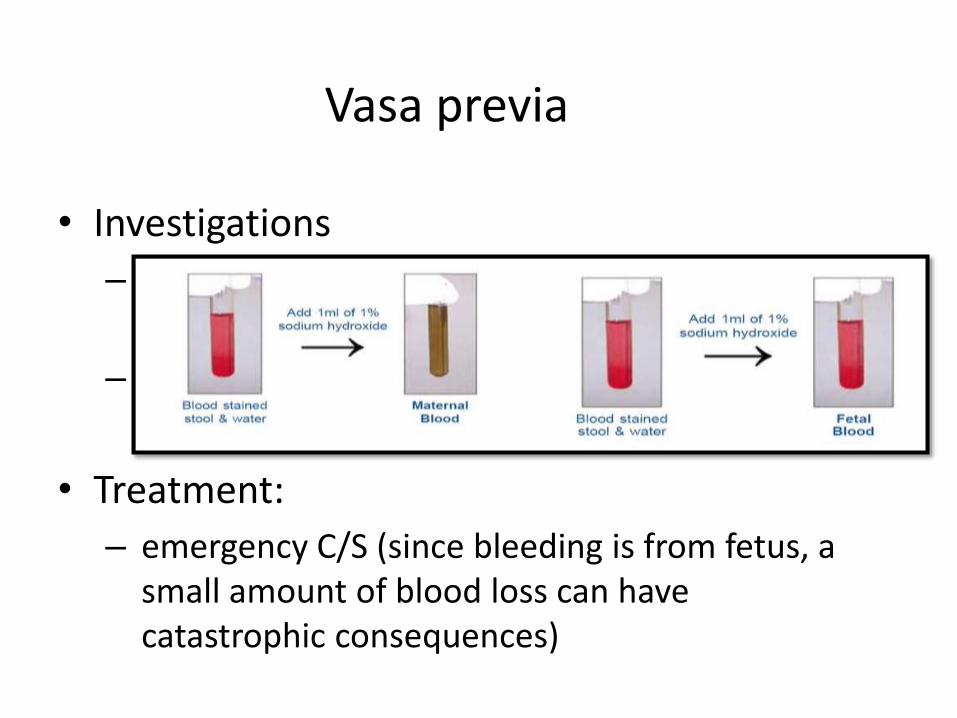
Vasa previa
• Investigations
– Apt test (alkai denaturation test) to determine if the source of bleeding is fetal.
– TVS examination with color Doppler
• Treatment:
– emergency C/S (since bleeding is from fetus, a small amount of blood loss can have catastrophic consequences)
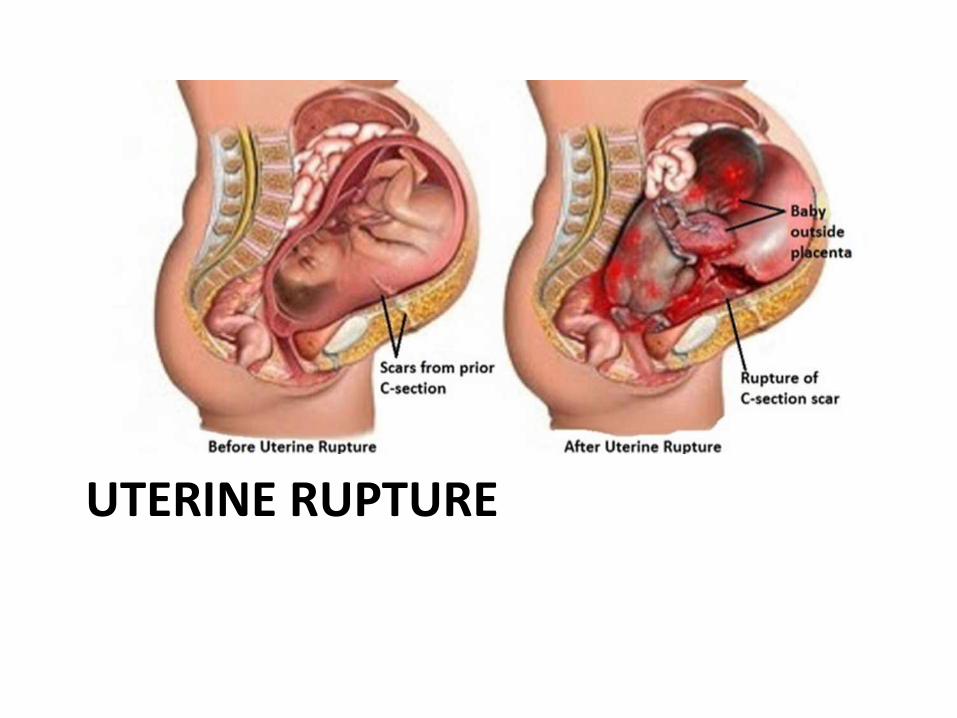
UTERINE RUPTURE
Definition
• Complete separation of the uterine musculature through all of its layers, with all or a part of the fetus being extruded from the uterine cavity.
• Epidemiology:
– 0.5% of all pregnancies.
– A prior uterine scar is associated with 40% of cases.
Risk factors
• Previous C\S (types and number).
• Previous uterine myomectomy.
• Congenital uterine anomalies.
• Multiparty.
• Fetal macrosomia.
• Labor induction.
• Uterine instrumentation\ trauma.
Clinical features
• highly variable.
– Sudden onset of intense abdominal pain.
– Vaginal bleeding.
– Shock (Profound maternal tachycardia and hypotension)
– Fetal parts may be more easily palpated abdominally.
Management
• Immediate laparotomy
• In most cases, total abdominal hysterectomy is the treatment of choice.
• Debridement of the rupture site and primary closure may be considered in women of low parity who desire more children.
• fluid and blood transfusion

Case scenario
• last scan 10/12/16
– active, cephalic, liquor normal, placenta posterior up, no signs of placental separation or retroplacental clots.
• Hb-9.7
• Coagulation : normal
Case scenario
• Glycosylated Haemoglobin = 5.9
• Urine MCS = Normal
• Group: O Rh Positive
• Antibody Screen: No atypical antibodies detected.

Case scenario
• Started on dexa prophylaxis and blood sugar monitoring.
• CTG and fetal heart monitoring at least once daily /or as indicated
• Rest
no more p/v spotting upon admission
References
• Hacker and Moore’s obstetrics and gynecology.
• Toronto Notes 2015.
• www.uptodate.com
• www.ncbi.nlm.nih.gov
• Medscape.com

Related Documents











