Application of Metabolomics to Diagnosis of Insulin Resistance Michael V. Milburn and Kay A. Lawton Metabolon Inc., Durham, North Carolina 27713; email: [email protected], [email protected] Annu. Rev. Med. 2013. 64:291–305 The Annual Review of Medicine is online at med.annualreviews.org This article’s doi: 10.1146/annurev-med-061511-134747 Copyright c 2013 by Annual Reviews. All rights reserved Keywords biomarkers, biochemistry, diabetes, prognostics, diagnostics Abstract Metabolomics, the global interrogation of the biochemical components in a biological sample, has become an important complement to ge- nomics and proteomics to aid in the understanding of pathophysiology. Major advantages of metabolomics are the size of the metabolome rela- tive to the genome or proteome and the fact that it provides a view of the existing biochemical phenotype. As such, metabolomics is fast becoming an important discovery tool for new diagnostic and prognostic biomark- ers. Although many methods exist for performing metabolomics, rela- tively few have led to successful development of new diagnostic tests. This review will aid the reader in understanding various metabolomic methods and their applications, as well as some of their inherent ad- vantages and disadvantages. In addition, we present one example of the application of metabolomics to the identification of new fasting blood biomarkers for the diagnosis and monitoring of insulin resistance. 291 Annu. Rev. Med. 2013.64:291-305. Downloaded from www.annualreviews.org by Dr. Michael Milburn on 01/18/13. For personal use only.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ME64CH21-Milburn ARI 12 December 2012 20:6
Application of Metabolomicsto Diagnosis of InsulinResistanceMichael V. Milburn and Kay A. LawtonMetabolon Inc., Durham, North Carolina 27713; email: [email protected],[email protected]
Annu. Rev. Med. 2013. 64:291–305
The Annual Review of Medicine is online atmed.annualreviews.org
This article’s doi:10.1146/annurev-med-061511-134747
Copyright c© 2013 by Annual Reviews.All rights reserved
Keywords
biomarkers, biochemistry, diabetes, prognostics, diagnostics
Abstract
Metabolomics, the global interrogation of the biochemical componentsin a biological sample, has become an important complement to ge-nomics and proteomics to aid in the understanding of pathophysiology.Major advantages of metabolomics are the size of the metabolome rela-tive to the genome or proteome and the fact that it provides a view of theexisting biochemical phenotype. As such, metabolomics is fast becomingan important discovery tool for new diagnostic and prognostic biomark-ers. Although many methods exist for performing metabolomics, rela-tively few have led to successful development of new diagnostic tests.This review will aid the reader in understanding various metabolomicmethods and their applications, as well as some of their inherent ad-vantages and disadvantages. In addition, we present one example of theapplication of metabolomics to the identification of new fasting bloodbiomarkers for the diagnosis and monitoring of insulin resistance.
291
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
INTRODUCTION TO GLOBALMETABOLOMICS
Over the past decade, “omics” technolo-gies have become key to discovering novelbiomarkers. Biomarkers can be nearly any-thing that distinguishes one individual fromanother. They can be based on a diagnostictest (e.g., cholesterol measurements), physicalcharacteristic (e.g., body mass index), genetics(e.g., single nucleotide polymorphisms), orother distinguishing characteristics (e.g., diet).Discovery technologies such as transcriptomics(profiling mRNA), proteomics (profilingproteins), and others (e.g., genome wideassociation studies) start with an idea of thebiomarker type needed to determine a con-dition, disease, or health risk. Unfortunately,general screening methods for biomarker dis-covery have been challenging, with few successstories. Biomarker validation is a relativelynew and evolving concept. The challenges aremathematical, technological, and/or statistical(insufficient number of well-characterizedsamples). One technology with promise toovercome these issues is metabolomics, whichprofiles biochemicals and metabolites. This re-view introduces applications of metabolomicsin the diagnosis of insulin resistance.
The goal of metabolomics is to measureall of the small molecules (i.e., biochemicals,metabolites) in a sample. As such, it is groundedin biochemistry and provides a snapshot ofthe biochemical or metabolic status of thesubject under investigation. The developmentof metabolomics as a tool to leverage the largebody of available biochemical knowledge hasbeen a major challenge. Most laboratories havefocused on targeted metabolomic analysis,specializing in the measurement of 20–100different metabolites which, most often, arewithin a common class of compounds. Forexample, a number of companies and academiclabs have developed methods for detectinglipid compounds. Although lipids representonly a subset of the total biologically relevantmetabolites, these data have proven useful forbiomarker discovery efforts (1).
Other groups have focused on methods totruly investigate all of the small molecules insamples. “Global” or “unbiased” metabolomicshas been plagued by difficulties stemmingfrom the diverse physical properties of smallmolecules. These properties can vary greatly,with significant differences in solubilities andwith molecular weights ranging from 20 to>1,500 Da. It is therefore difficult to develop asingle chromatography method to separate allof the compounds and even more difficult toanalyze individual compounds without chro-matographic separation. Further complicationsarise if studies are expected to be completedwithin a clinically useful turnaround time.These issues are currently being addressedthrough advanced multisystem approacheswhere the best separation and detectioninstrument technologies are developed to runin tandem. This approach allows for a com-prehensive solution achieved by combiningprinciples offered by various best-in-breedtechnologies. As this new technology developsand its use in biomarker detection studiesincreases, it is rapidly becoming clear thatmetabolomics will likely have a high impact inthe diagnosis of disease, identification of drugtargets, evaluation of the effects of drugs, andselection of patients most likely to respond todrug therapy (i.e., personalized medicine).
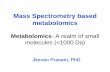
To develop a viable technology platformthat harnesses the power of metabolomicsrequires engineering a system of chro-matographic separation coupled to massspectrometry (2–4). One such metabolomicsanalysis process operates in essentially foursteps (Figure 1). Step one is extraction of thesmall molecules from the biological sample.Step two is the chromatography coupled withmass spectrometry and data collection. Stepthree is the automated and manual qualitycontrol (QC) analysis of the data. Step fouris the statistical and biological interpretationof the data. Numerous methods of analyzinga wide range of very polar to nonpolar com-pounds from as little as 50 μl of blood plasmahave been published (5–7). For the case study
292 Milburn · Lawton
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
Generation of data
UHPLC-MS/MS (+ESI)UHPLC-MS/MS (+ESI)UHPLC-MS/MS (–ESI)UHPLC-MS/MS (–ESI)
GC-MS (+EI)GC-MS (+EI)
Sample preparation
Biochemicalextraction
Biochemicalextraction
Metabolic pathwaysAnalytics
Figure 1Data-generation steps of a global metabolomics method as applied to a biological sample. The three steps are (1) biochemicalextraction, (2) multiple chromatography and mass spectrometry analysis, and (3) unbiased global informatics methods to reduce the rawmachine data to the biochemicals in the sample and determine the relative concentration of each biochemical in each sample. Inaddition, a quality-control step is performed on the data prior to statistical analysis and biological interpretation.
presented in this review, the extracted sampleswere split into four aliquots for differentchromatography and mass spectrometry (MS)platforms, two ultra-high-performance liquidchromatography (UHPLC) methods and onegas chromatography (GC) method, with onealiquot held in reserve (4). These three chro-matography and MS systems complement oneanother in the range of biochemicals measuredand provide an enhanced biochemical coverageof each sample (4). Approximately 70%–80%of the biochemicals are measured on more thanone platform, with 30%–40% measured onall three platforms. For compounds observedon multiple platforms, the chromatography/analytical system with the best analyticalcharacteristics (e.g., fewest interfering peaks orhighest signal to noise) is generally used for theanalysis of that compound. In general, the GCmethod provides better separation of moleculesthat tend to be more difficult to separate usinga typical reverse-phase liquid chromatography(LC) method (e.g., carbohydrates).
Following acquisition of the raw data fromthe instruments, a suite of software meth-ods (3, 8–14) automatically integrates each ionacross retention time and then uses that ionic
information, which may include additionalMS/MS fragmentation information and reten-tion time, to identify the compound. After acompound is identified in a sample, one of thecharacteristic and stronger ions is used to deter-mine a relative concentration of that compoundin each sample. This chemo-centric approachassures that the compound will be representedonly once in the subsequent statistical analysis.When the software has finished analyzing thesamples, all of the data are loaded into a visualuser interface that allows manual curation of thedata. For QC purposes, a scientist visually in-spects how well each compound was identifiedand verifies that only those compounds with thehighest degree of confidence are included in thefinal data set used for statistical analysis (14).
After QC curation, a variety of statisticalapproaches can be applied to the final dataset, including ANOVA, t-tests, Random Forest,Principal Component Analysis, etc. The goalof these statistical treatments is to identify thebiochemicals that best represent the most sig-nificant changes in concentration between thegroups in the study. One advantage of biochem-istry is that multiple compounds in a particularbiochemical pathway may often be significantly
www.annualreviews.org • Metabolomics and Insulin Resistance 293
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
altered, giving an even higher degree of con-fidence to the importance of that biochemicalchange. In this respect, it is important to pointout that most statistical treatments assume in-dependent variables when, in fact, we know thatcertain biochemicals are related to the same orsimilar pathways. Consequently, knowledge ofthe biochemical context can enable the iden-tification of and increase confidence in thecandidate biomarkers.
INTRODUCTION TOBIOMARKER DISCOVERYAND VALIDATION
Biomarker discovery typically involves, asa first step, the deployment of a discoverytechnology. Whether that technology isgenomics/transcriptomics, proteomics, meta-bolomics, or something else, the process startswith an unmet need and an idea of the type ofbiomarkers that are required (single nucleotidepolymorphisms, proteins, biochemicals, etc.).Clinical biomarker discovery studies usuallyinvolve (a) the identification of the appropriatestudy populations, using a “gold standard” testto distinguish individuals with the disease fromthe nondisease individuals; (b) the determina-tion of the availability of appropriate sampletypes in sufficient numbers with the necessarymeta-data for the desired study population;and, in many cases, (c) the development ofclinical research agreements with academicand/or healthcare organizations.
For example, insulin resistance (IR) isa well-studied condition that can lead to anumber of increased health risks, includingdiabetes, cardiovascular disease, and metabolicdiseases. However, no simple fasting bloodtests currently exist for IR or the assessment ofthe degree of IR. The current gold-standardtest—namely, the hyperinsulinemic clamp(HI clamp)—is invasive, time-consuming,expensive, and rarely used outside of a clinicalresearch setting. Currently available index testshave limitations in terms of time, invasiveness,complexity, and performance. New biomarkersthat can be developed into a new diagnostic
test are needed to better manage this growingconcern in humans and companion animals. Ifdetermining insulin sensitivity and identifyinginsulin-resistant subjects is the clinical test idea,then the next step is to perform a feasibilitystudy to determine whether it is possible toseparate the case from the control groupsusing the chosen technology and to identifycandidate biomarkers that contribute to theseparation. These proof-of-concept studies aretypically simple in design and relatively small(<30 subjects per group).
As with many initial research studies, abiomarker feasibility study can produce mixedresults even if well designed and sufficientlypowered. Analysis of these initial studies can beconfounded by the unforeseen impact of age,gender, or other differences (e.g., diet, medi-cations, lifestyle) between the groups. A fur-ther important consideration for “omics-based”studies is that when a very large number of mea-surements (e.g., 1 million SNPs) are made ononly a small number of subjects (e.g., 50 individ-uals per group), the probability of separating thegroups by chance alone is enormous and oftenleads to false discovery. As a result, more thanone feasibility study may be necessary to fullydemonstrate the proof-of-concept and becomesufficiently confident in the data to invest the re-sources necessary for the larger studies that areessential for biomarker validation. Each subse-quent study design can be adjusted to take intoaccount the confounding variables uncoveredin prior studies.
Once it seems reasonable that the sampletype for the biomarker is suitable (blood, urine,etc.), and the biomarker(s) from the feasibil-ity study meets minimum performance crite-ria, then larger, well-powered discovery studiesare warranted. These studies should focus onclinical utility and contain sufficient numbers ofsubjects to not only assess the reproducibility ofthe biomarker candidates uncovered in the fea-sibility study, and uncover additional biomark-ers, but also provide an independent test set ofsubjects. That is, the clinical study populationshould be large enough to be divided into a “dis-covery validation set” (or “training set”) and a
294 Milburn · Lawton
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
“test set,” the latter of which is composed ofsubjects who have not been used to discoverthe biomarkers. A schematic of the diagnosticdevelopment from discovery study through val-idation and commercial formatting of the testis exemplified in Figure 2.
Another important consideration inbiomarker discovery and validation is thedemographic suitability of the subjects in thediscovery population relative to those for whomthe test will be applied. For instance, usingonly European populations for the discoveryand development of the biomarkers may bea concern if the test will also be employed inJapan.
In addition to biomarker diagnostic perfor-mance validation, the laboratory assays used tomeasure the biomarkers must undergo analyt-ical validation. Although analytical assay de-velopment and validation entail significantlyless risk than developing the biomarker, thesesteps can be equally time consuming. Sufficientnumbers of samples from the test populationare necessary to confirm the laboratory per-formance of the analytical assays. In addition,the assay throughput requirements or the as-say setting (e.g., hospital, point-of-care, cen-tral laboratory) often require specific formatsfor the biomarker measurement and may differfrom the discovery assays. For example, genechips are often used for the discovery analysis ofgenetic biomarkers, but to satisfy the through-put, cost, and quantitation requirements, othermethods, such as PCR-based assays, have beendeveloped.
ADVANTAGES OFMETABOLOMICS FORBIOMARKER DISCOVERY
The word “metabolomics” (or “metabo-nomics”) first appeared in journal articles in2000. Only a few metabolomics papers werepublished that year, but in 2009 >1,300 pub-lished scientific papers reported metabolomicsresults. In fact, metabolomics publications areone of the fastest-growing areas of scientificpublications in the past few years. Although
Diagnostic development process
Clinical samples
Biomarker discovery platform
Statistical analysis
Quantitative assay
Statistical analysis
Commercial format
30candidate biomarkers
38diagnostic markers
Commercial test3 analytes
Figure 2Process flow using “omics” technologies for biomarker discovery andvalidation. The initial work begins with decisions on the types of samples to beanalyzed for the biomarker discovery study, number of subjects and samplesrequired, and the relevant case and case controls that will be used. Many ofthese decisions are based on the types of technologies employed to analyze thesamples. Other decisions depend more on how the ultimate biomarker ordiagnostic test will be used clinically. After the samples are received, then thediscovery technology can be employed and analyzed. The analysis of “omics”technologies is beyond the scope of this review but can involve complexmultivariate analysis and methods to control for false discovery. Ultimately, theaim of the discovery study is to develop a shorter list of candidate biomarkersthat can be further validated with independent assays and preferablyindependent cohorts of samples. Rarely is the discovery technology itselfemployed on an individual basis, although some technologies are moving inthis direction. In most cases, the assay to validate a biomarker is a more specificquantitation of the analyte under strict clinical protocols. Ultimately, theseassays will be further validated in the clinic to determine their clinical utility.Furthermore, many standard clinical measurements can be used in theperformance evaluation of the new biomarkers; this explains the additionaleight candidate markers in the figure, bringing the total biomarkers evaluatedin this example to 38.
www.annualreviews.org • Metabolomics and Insulin Resistance 295
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
analytical chemists and biochemists havebeen identifying small molecules in biologicalsamples since long before 2000, as a robust,nontargeted discovery tool the technology isnew and rapidly evolving. In addition to theincreasing number of publications in the pastfew years, several significant biomarker reportsusing metabolomics have been published thatinclude supporting validation data for thesediscoveries (5, 15, 16).
Because metabolomics analysis is basedon measuring the small molecules (i.e., bio-chemicals or metabolites of molecular weights<1,500 Da) in a biological sample, the in-terpretation of the resulting data is basedon biochemistry. This provides a significantadvantage. Relative to molecular biology andproteomics, biochemistry is a mature, highlydeveloped field of science. In fact, many of theNobel Prizes in Medicine before the 1960swere awarded in biochemistry. Today, weroutinely depend on metabolite-based diseasediagnosis. For instance, high glucose in urinewas one of the earliest tests for diabetes, andcholesterol is used to measure the risk of heartdisease. Metabolic panels of fatty acids, bileacids, sugars, creatine, creatinine, urea, etc. areroutinely used clinically to assess organ functionor risk for many diseases as well as for diseasediagnosis. Clearly, the field of metabolomics ispositioned to take advantage of this repositoryof biochemical pathway knowledge.
The major challenge for metabolomics hasbeen to develop a technology that can extract,identify, and quantitate the entire spectrumof the small molecules (<1,500 Da) in anybiological sample, unlike profiling DNA, RNA,or protein (see Figure 3). The exact number ofsmall molecules in biological samples is a hotlydebated subject. Some databases of metaboliteslist as many as 6,000 comprising the humanmetabolome. However, a deeper evaluation ofthese metabolites reveals that several thousandmolecules can simply be grouped as differentcombinations of complex lipids or smallpeptides (17, 18). From a primary metabolismstandpoint, and disregarding the combinations
of complex lipids or peptides as well as xenobi-otic metabolites from drugs, diet, and the like,it is very likely that <3,000 human metabolitesare significant for understanding metabolismand metabolic effects. Importantly, in anyone sample matrix (i.e., blood, urine, tissue,etc.) there will always be dramatically fewermetabolites than the total number synthesizedin the entire organism.
Most importantly, this number (<3,000metabolites) is much smaller than the numberof molecules involved in other “omics” tech-nologies, such as genomics (>30,000 genes)or proteomics (>100,000 proteins). This dif-ference may represent a significant advantagefor metabolomics in biomarker discovery. Asmaller number of total observed measure-ments for any individual allows the applicationof more robust statistical testing methodologiesand results in fewer false discoveries. Falsediscovery (19) represents a severe limitationfor generally profiling genes and proteins.The underlying math is simple. As the totalnumber of observations per individual subjectincreases, the likelihood of separating groupsof individuals purely by chance increasessignificantly. For instance, in a study of twogroups of 100 subjects, the likelihood of sepa-rating the groups by random measurements issignificantly higher if one is measuring 100,000variables per individual than if one measures1,000 variables per individual.
Another important advantage of metabolo-mics, especially for developing tests thatrely on noninvasive types of samples, is thatessentially any type of sample can be analyzed.Metabolites can be routinely measured inurine, feces, sweat, saliva, blood, tissue, etc.,which can often be challenging sources forobtaining genetic or protein information. Anumber of papers have been published recentlydescribing the use of metabolomics assessmentof more creative sample types for disease(20–22).
Many biological effects of drugs and diseaseresult from the overall health of an individual,as well as his or her environment, lifestyle, and
296 Milburn · Lawton
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
Any sample type
Condensed andinformation rich
Bridge betweengenome and phenotype
Translatable
OH
OH
O
NH2
OH
OH
OH
HO
OH
O
HOH
H
H
L-threonineGlucose Cholesterol
Metabolism advantages
DNA
RNA
Proteins
Biochemicals
Mechanistic insightinto phenotype
Metabolomics analysis
Figure 3Progression of genes to metabolites and how each step fits into the “omics” technologies. In contrast to>30,000 genes and >100,000 possible transcripts and proteins, metabolites represent a far smaller totalnumber, totaling <3,000. The consequence is that a discovery study in metabolomics is likely to be fraughtwith far fewer false discovery effects than these other technologies. In addition, nearly any type of samplewill contain biochemicals (sweat, saliva, urine, feces, etc.). Perhaps the most striking difference is how closelythe measurements of metabolites reflect the current phenotype of the test subject as compared to genomicsand proteomics. This is likely why metabolomics results can be much more practical at solving metabolismand mechanism problems.
diet. Although genetics can play an importantpart in predisposing an individual to drugside effects or disease, the biochemistry ofan individual is likely a more informativemeasurement of the individual’s current state
and condition. Combining genetic predis-position with the environmental and healthstatus measurements that can be achieved withmetabolomics will likely be a very importantbiomarker discovery method of the future.
www.annualreviews.org • Metabolomics and Insulin Resistance 297
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
THE NEED FOR SIMPLE INSULINRESISTANCE BIOMARKERS
Insulin resistance (IR) is a well-established riskfactor for type 2 diabetes (T2D) and cardio-vascular disease (CVD) progression (23–29).IR and compensatory hyperinsulinemia areoften associated with obesity. When coupledwith beta-cell dysfunction, IR is a major patho-physiological determinant of hyperglycemia(impaired fasting glycemia and impaired glu-cose tolerance) and T2D (30, 31). Conditionsassociated with high CVD risk, such as hy-pertension, dyslipidemia, and atherosclerosis,have also been associated with IR (30–33).
Although IR plays a central role in thedevelopment of numerous diseases, it is notreadily detectable using many of the clinicalmeasurements for prediabetic conditions. IRdevelops prior to the onset of hyperglycemiaand is associated with increased production ofinsulin. Over decades, the ability of the cell torespond to insulin decreases, and the subjectbecomes resistant to the action of insulin.Eventually the beta cells of the pancreas cannotproduce sufficient insulin to compensate forthe decreased insulin sensitivity. The betacells begin to lose function and apoptosis istriggered. Beta-cell function may be decreasedas much as 80% in prediabetic subjects. Asbeta-cell function decreases, the productionof insulin decreases, resulting in lower insulinlevels and high glucose levels in diabetic sub-jects. Vascular damage is associated with theincrease in IR and the development of T2D.
Unfortunately, traditional clinical fastingplasma measurements do not assess IR directly.The gold standard for assessing IR is the HIclamp. This involves glucose and insulin infu-sions and requires insertion of two cathetersinto the patient, who must remain immobi-lized in the clinic for up to six hours (34). Asa result, the procedure is typically performedonly in a research setting, and the associatedcost and time constraints severely limit its clin-ical utility. Fasting insulin and derived indices(HOMA, QUICKI) have been used to assess IR(35), but owing to the complicated calculations
required, these have not been widely adoptedin routine clinical practice. The identificationof novel biomarkers to detect subjects at riskof IR and to stratify the risk of progression toT2D and/or CVD in subjects with IR, in orderto implement effective strategies for preventionas well as to monitor treatment response, re-mains an unmet need. Furthermore, a test forIR could be particularly useful in identifyingpatients who have significant IR levels despitenormal A1C levels.
Biomarker Discovery for IR Using aGlobal Metabolomics Analysis
Pilot studies had demonstrated the feasibilityof identifying IR biomarkers, so biomarker dis-covery and validation studies were designed.The first step was to identify a sufficiently largecohort of nondiabetic subjects in whom the HIclamp had been performed and for whom fast-ing blood plasma samples were available formetabolomic analysis. The RISC (Relationshipof Insulin Sensitivity to Cardiovascular Risk)cohort, subjects of a large, observational lon-gitudinal study initiated to address how IR maycontribute to progression to T2D and CVD,met these criteria. The cohort included a spec-trum of insulin sensitivity as determined by theHI clamp (36, 37). The study design for the dis-covery and validation of the IR biomarkers withthe RISC cohort is illustrated in Figure 4.
As previously reported, for biomarkerdiscovery, fasting blood plasma samples col-lected at baseline from 399 subjects from theRISC study, all of whom were nondiabeticand clinically healthy, were analyzed usingmetabolomics (38). Roughly half the subjectswere male and half were female; all werematched to age and body mass index (BMI).Each subject had his or her insulin sensitivityassessed using the HI clamp, which resulted ina measured insulin-mediated glucose disposalrate, MFFM (expressed as μmol × min−1 kgFFM−1, where FFM refers to fat-free mass).The measured MFFM values ranged from highto low and included a spectrum of insulin
298 Milburn · Lawton
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
Training set
894 subjects
Test set
383 subjects
RISC cohort
2,327 subjects
Measure IR using “gold standard”
Hyperinsulinemic clamp at baseline
Validation study
1,277 subjects
Discovery study
399 subjects
Figure 4Experimental design schema illustrating theidentification of a sufficiently large cohort, in thiscase the Relationship between Insulin Sensitivityand Cardiovascular Disease (RISC) Study, on whichthe hyperinsulinemic clamp test has been performedto serve as the biomarker discovery and validationcohort. The large number of subjects is partitionedinto a smaller discovery study comprising 399subjects and an independent validation studycomprising a training set and a test set of subjects.IR, insulin resistance.
sensitivity from very insulin sensitive (highMFFM) to insulin resistant (low MFFM). Subjectswith <45 μmol × min−1 kg FFM−1 belongedto the bottom tertile of the cohort analyzed andwere defined as being insulin resistant whereasthe top two tertiles (MFFM >45 μmol ×min−1 kg FFM−1) were defined as being insulinsensitive (38).
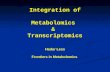
A total of 471 metabolites were measured inthe blood plasma samples collected from the399 subjects and analyzed for IR biomarkers(38). The authors assessed the ability to clas-sify subjects as insulin sensitive or insulin resis-tant, with Random Forest analysis performedusing the entirety of the screening data (i.e.,471 compounds). Figure 5 shows the resultingImportance Plot, which ranks the classifiers bytheir contribution to the separation of the sub-jects into groups. This result did not changewhen normalizing the M value for kilograms ofbody weight rather than kilograms of FFM. Aseparate univariate correlation analysis of thescreening data identified the correlation of themetabolites to the glucose disposal rate.
From these analyses, a panel of 30 candi-date biomarkers was identified for further assay
development and evaluation (38). The candi-date markers from this analysis are summa-rized in Table 1. For biomarker success, it wasvery important that two completely indepen-dent statistical treatments, in this case RandomForest and correlation analysis, resulted in thesame top-performing metabolites and furtherconfirmed the likely importance of these bio-chemicals as biomarkers for IR.
Since the initial analyses were based on dataobtained from the nontargeted biochemicalprofiling technology, targeted isotopic dilutionassays were developed for the panel of the 30best candidate biomarkers to provide abso-lute quantitative results (38). These analysesshowed a high correlation between the resultsfrom the screening platform and the quantita-tive targeted assay. Further, whether measuredby the screening platform or the targetedisotopic dilution assay, the biomarker α-HBwas consistently higher, and the biomarkerslinoleoyl-lysoglycerophosphocholine (L-LPC)and oleate were lower, in insulin-resistantsubjects than in insulin-sensitive subjects (p< 0.0001 for both the screening and targeteddata). Thus, the targeted assay data validatedthe screening data in the test cohort.
Developing an IR Biomarker Panelinto a Diagnostic Test
After the development and analytical validationof quantitative assays for the selected biomarkercandidates, the next steps in developing thebiomarkers into a clinically useful diagnostictest include (a) biomarker selection and algo-rithm development, (b) validation in an inde-pendent set of clinically relevant samples, and(c) demonstration of the clinical utility of thetest.
The 30 biomarkers identified by RandomForest and Lasso Regression analyses as impor-tant to build models to predict IR (defined bythe bottom tertile of M values in the cohort) arelisted in Table 1 (38). These cross-validatedbiomarkers were used to classify individualsas insulin resistant (bottom tertile MFFM) ornormally insulin sensitive (top two-thirds
www.annualreviews.org • Metabolomics and Insulin Resistance 299
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
α-hydroxybutyrate
X-12,063
Glycine
Phosphate
1-palmitoyl-GPE
Mannose
Hippurate
Catechol sulfate
Trigonelline
Urate
Adrenate (22:4 n6)
X-8,889
3-phenylpropionate
2-oleoyl-GPC
X-4,055
Creatine
Decanoyl-carnitine
X-11,793
Eicosenoate (20:1 n9 or 11)
Cysteine
Glutamate
Octanoyl-carnitine
Isoleucine
X-11,421
Linoleoyl-LPC
X-13,431
X-7,888
X-11,537
α-ketobutyrate
1-oleoyl-GPC
Mean decrease accuracy2 3 4 5
Predicted
Actual
> 45 MFFM
> 45 MFFM
≤ 45 MFFM
≤ 45 MFFM
201 60
36 102
% correct 76%
Figure 5The results of Random Forest analysis of the previously reported (38) discovery study cohort. TheImportance Plot shows the top-ranked biomarkers identified in the initial study. The inset table shows theresults of the classification of subjects as being insulin sensitive (>45 M-ffm) or insulin resistant (≤45 M-ffm)using the biomarkers. The prediction accuracy of the separation of the top two-thirds, which are theinsulin-sensitive subjects, from the bottom tertile, which represents the insulin-resistant subjects, is ∼75%.
MFFM). Samples from 90% of the subjects wereused to build the model, and samples from theremaining 10% were used to test the predictivepower of the model. These analyses identifiedbiomarkers that are positively or negativelycorrelated with estimated M and ranked thebiomarkers of most use to estimate M. Thesebiomarkers are useful for determining insulinsensitivity and diagnosing IR. As shown in
Table 2, 164 subjects were classified as insulinresistant and 235 subjects were classified asinsulin sensitive. These results indicate asensitivity of ∼85%, a specificity of ∼91%,and an overall prediction accuracy of ∼76%(38).
Next, an independent validation of thebiomarkers was conducted using the targetedassays on fasting plasma samples from a
300 Milburn · Lawton
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
Table 1 Biomarker candidates
2-hydroxybutyrate Linoleic acid Stearate3-hydroxybutyrate Linolenic acid Threonine3-methyl-2-oxo-butyric acid Margaric acid Isovalerylcarnitine3-phenylpropionate Octanoyl carnitine Linoleoyl-LPCCatechol sulfate Oleic acid 1,5-anhydroglucitolCreatine Oleoyl-LPC Stearoyl-LPCDecanoyl carnitine Palmitate 1-palmitoyl-GPEDocosatetraenoic acid Palmitoleic acid OctanoylcarnitineGlutamic acid Palmitoyl-LPC alpha-ketobutyrateGlycine Serine Cysteine
validation set of subjects. Samples from thesesubjects were also from the RISC cohort (36,37) but had not been analyzed in the discoverystudy. The validation study comprised 1,277fasting plasma samples obtained at baselinefrom the RISC participants, with 894 subjectsamples included in the training set and 383subject samples in the test set (Figure 4).Continuous regression and logistic regressionanalyses were carried out to generate candidatediagnostic algorithms to estimate the M value.Shown in Figure 6 is the spectrum of insulinsensitivity and the associated change in theselected biomarkers and comparisons with themeasured M value, insulin, and BMI.
It is important in the development of anynew test to benchmark the performance ofthe new analytes to previously used analytes.Part of the reason is to better understand theperformance differences, both biologically andanalytically. There may be simple analyticaladvantages for some biomarkers over others.BMI has been shown previously to be corre-lated with insulin, and using BMI or insulinwith new analytes could improve the overallaccuracy of IR assessment.
Analytical/Clinical ValidationAfter the diagnostic biomarkers and algorithmsare validated and the clinical utility is demon-strated, the diagnostic test itself must be analyt-ically validated before it can be used clinically.Figure 7 illustrates the prototype developmentand design control activities that precede clin-ical and analytical validation, or final productvalidation for an MS-based diagnostic test.
As demonstrated by this case study, a non-targeted metabolomics analysis has utility forthe discovery of new biomarkers and furthersupports the increased application of this newtechnology for biomarker discovery. Usingmetabolomics, several novel IR biomarkers,including α-HB, oleate, and L-LPC, wereidentified and validated, and a specific diag-nostic assay and algorithm for fasting bloodsamples were developed for the assessmentof IR in nondiabetic indiviuals. Furthermore,these biomarkers and test, used alone andin combination with additional biomarkersidentified in this work, are likely to provideclinically useful diagnostic tests for identifyingand managing IR and its associated disorders,such as T2D, CVD and the like.
Table 2 Classification of insulin-resistant (IR) subjects by hyperinsulinemic (HI) clamp and byusing IR biomarkers
Number determined byHI clamp
Number predicted bybiomarkers
Insulin resistant 138 (true positive) 164Insulin sensitive 261 (true negative) 235
www.annualreviews.org • Metabolomics and Insulin Resistance 301
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
Linoleoyl-LPC
Mic
rogr
ams/
mL
Insulin sensitivityIM
10
50
20
30
40
IS0
IR
BMI
kg/m
2
Insulin sensitivityIM
20
25
45
30
35
40
IS
15
IR
50
M-wbm
GD
R, m
g/kg
/min
Insulin sensitivityIM
5
25
30
10
15
20
IS
0
IR
Oleate
Mic
rogr
ams/
mL
Insulin sensitivityIM
100
500
200
300
400
IS
0
IR
600
α-hydroxybutyrate
Mic
rogr
ams/
mL
Insulin sensitivityIM
2
12
14
4
6
8
10
IS0
IR
Insulin
Mic
roU
/mL
Insulin sensitivityIM
50
250
100
150
200
IS
0
IR
300
Figure 6Association of insulin, body mass index (BMI), and insulin resistance (IR) biomarkers with various levels ofinsulin sensitivity. The box plots represent three categories of insulin sensitivity classification—insulinsensitive (IS) (M-wbm >7.5 mg/kg/min), intermediate (IM) (M-wbm >5.6 and <7.5 mg/kg/min), andinsulin resistant (IR) (<5.6 mg/kg/min)—based on the gold-standard test of IR, the hyperinsulinemic clamp.GDR (glucose disposal rate): M-wbm 5.6 mg/kg/min reflects the bottom tertile of insulin sensitivity in theentire baseline population used in training and test sets (n = 1277). In the box plots, the top and bottom ofthe box represent the 75th and 25th percentile, respectively; 75% of the data points lie within the boxedregion. The top and bottom bars (“whiskers”) represent the entire spread of the data points, excluding“extreme” points, which are indicated with circles. The solid line in the box indicates the mean value andthe + indicates the median value.
302 Milburn · Lawton
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
Instrument qualification(Process validation)
Mass spectrometry instrument,software, refrigerators/freezers,
centrifuges, etc.
Clinical validationFinal validation cohort sample analysis
Finalize coefficients for diagnostic algorithm
Methods development(Extraction and liquid chromatography/
mass spectrometry procedure)
Validation SOP/method performance
(Stability testing; quality control preparation)
Stock verification(Stock quality controls
match unlabeled standard)
Stock stability(1 month, 3 month, 6 month, etc.)
Sample analysis SOP(Acceptance criteria, monitoring performance)
Execute analytical validation(Running test samples,
extract reference materials)
Doc
umen
t sta
ndar
dop
erat
ing
proc
edur
es (S
OPs
)
Figure 7Prototype workflow describing the development and design control activities that are necessary for finalvalidation of a multi-analyte diagnostic test. In this example, the test methods are based on liquidchromatography–mass spectrometry. A central requirement of design control is the development anddocumentation of standard operating procedures for each aspect of the diagnostic test.
CONCLUSIONS ANDACKNOWLEDGMENTS
Metabolomics offers a number of advantagesthat enable biomarker discovery and diagnostictest development. Profiling biochemicals inblood is relatively straightforward and is lesslikely than other “omics” technologies to beaffected by false discovery. Profiling biochem-icals facilitates understanding of metabolismand the effects of disease on metabolic pheno-type, as well as drug alterations of metabolismin the liver, kidney, testes, and other organs,which also affect metabolic phenotype. Under-standing the mechanisms of disease and drugeffects will provide a wealth of potential newbiomarkers.
Routine metabolomics could become thediscovery method of choice, not only for diag-
nostic biomarker discoveries based on lifestyleand diet, but also for segregating biomarkers ofpopulation genetic differences in drug responseand toxicity. One of the most exciting recentdevelopments in metabolomics with potentialto impact diagnostics is the new understandingof the penetrance of an individual’s geneticson metabolite levels in the blood (39, 40). Thelargest challenge to this growing technologyis the early stage of the technology itself; fewgroups have developed fully validated globalmetabolomics methods, and many have verylimited experience in using and understandingthe data. It is hoped that as the importance ofmetabolomic studies is realized, a renaissance ofbiochemical learning will inspire a new breed ofscientists who are as well versed in biochemistryas they are in molecular biology and genetics.
www.annualreviews.org • Metabolomics and Insulin Resistance 303
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
DISCLOSURE STATEMENT
M.V.M. and K.A.L. are employees of Metabolon, Inc.. The authors have no other relevant af-filiations or financial involvement with any organization or entity with a financial interest in orfinancial conflict with the subject matter or materials discussed in this article apart from thosedisclosed.
LITERATURE CITED
1. German JB, Gillies LA, Smilowitz JT, et al. 2007. Lipidomics and lipid profiling in metabolomics. Curr.Opin. Lipidol. 18:66–71
2. Ryals J, Lawton K, Stevens D, et al. 2007. Metabolon, Inc. Pharmacogenomics 8:863–663. Dehaven CD, Evans AM, Dai H, et al. 2010. Organization of GC/MS and LC/MS metabolomics data
into chemical libraries. J. Cheminform. 2:94. Evans AM, Dehaven CD, Barrett T, et al. 2009. Integrated, nontargeted ultrahigh performance liquid
chromatography/electrospray ionization tandem mass spectrometry platform for the identification andrelative quantification of the small-molecule complement of biological systems. Anal. Chem. 81:6656–67
5. Scalbert A, Brennan L, Fiehn O, et al. 2009. Mass-spectrometry-based metabolomics: limitations andrecommendations for future progress with particular focus on nutrition research. Metabolomics 5:435–58
6. Romisch-Margl W, Prehn C, Bogumil R, et al. 2012. Procedure for tissue sample preparation and metabo-lite extraction for high-throughput targeted metabolomics. Metabolomics 8:133–42
7. Lee Do Y, Bowen BP, Northen TR. 2010. Mass spectrometry-based metabolomics, analysis of metabolite-protein interactions, and imaging. BioTechniques 49:557–65
8. Bryan K, Brennan L, Cunningham P. 2008. MetaFIND: a feature analysis tool for metabolomics data.BMC Bioinform. 9:470
9. Bowen BP, Northen TR. 2010. Dealing with the unknown: metabolomics and metabolite atlases. J. Am.Soc. Mass Spectrom. 21:1471–76
10. Dunn WB, Bailey NJ, Johnson HE. 2005. Measuring the metabolome: current analytical technologies.Analyst 130:606–25
11. Thielen B, Heinen S, Schomburg D. 2009. mSpecs: a software tool for the administration and editing ofmass spectral libraries in the field of metabolomics. BMC Bioinform. 10:229
12. Xia J, Psychogios N, Young N, et al. 2009. MetaboAnalyst: a web server for metabolomic data analysisand interpretation. Nucleic Acids Res. 37:W652–60
13. Cloarec O, Dumas ME, Craig A, et al. 2005. Statistical total correlation spectroscopy: an exploratoryapproach for latent biomarker identification from metabolic 1H NMR data sets. Anal. Chem. 77:1282–89
14. DeHaven CD, Evans AM, Dai H, et al., eds. 2012. Software techniques for enabling high-throughputanalysis of metabolomic datasets, metabolomics. doi: 10.5772/31277. http://www.intechopen.com/books/metabolomics/software-techniques-for-enabling-high-throughput-analysis-on-metabolomic-datasets
15. Brindle JT, Antti H, Holmes E, et al. 2002. Rapid and noninvasive diagnosis of the presence and severityof coronary heart disease using 1H-NMR-based metabonomics. Nat. Med. 8:1439–44
16. Sreekumar A, Poisson LM, Rajendiran TM, et al. 2009. Metabolomic profiles delineate potential role forsarcosine in prostate cancer progression. Nature 457:910–14
17. Kopka J, Schauer N, Krueger S, et al. 2005. [email protected]: the Golm Metabolome Database.Bioinformatics 21:1635–38
18. Wishart DS, Tzur D, Knox C, et al. 2007. HMDB: the Human Metabolome Database. Nucleic Acids Res.35:D521–26
19. Benjamini Y, Hochberg Y. 1995. Controlling the false discovery rate: a practical and powerful approachto multiple testing. J. R. Stat. Soc. Ser. B 57:289–300
20. Barnes VM, Teles R, Trivedi HM, et al. 2010. Assessment of the effects of dentifrice on periodontaldisease biomarkers in gingival crevicular fluid. J. Periodontol. 81:1273–79
21. Ohta T, Masutomi N, Tsutsui N, et al. 2009. Untargeted metabolomic profiling as an evaluative tool offenofibrate-induced toxicology in Fischer 344 male rats. Toxicol. Pathol. 37:521–35
304 Milburn · Lawton
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64CH21-Milburn ARI 12 December 2012 20:6
22. Wetmore DR, Joseloff E, Pilewski J, et al. 2010. Metabolomic profiling reveals biochemical pathways andbiomarkers associated with pathogenesis in cystic fibrosis cells. J. Biol. Chem. 285:30516–22
23. Ginsberg H, Olefsky JM, Reaven GM. 1974. Further evidence that insulin resistance exists in patientswith chemical diabetes. Diabetes 23:674–78
24. Harris MI. 1995. Epidemiologic studies on the pathogenesis of non-insulin-dependent diabetes mellitus(NIDDM). Clin. Invest. Med. 18:231–39
25. Lyssenko V, Jonsson A, Almgren P, et al. 2008. Clinical risk factors, DNA variants, and the developmentof type 2 diabetes. N. Engl. J. Med. 359:2220–32
26. Reaven GM. 1998. Insulin resistance and human disease: a short history. J. Basic Clin. Physiol. Pharmacol.9:387–406
27. Reaven GM, Olefsky JM. 1978. The role of insulin resistance in the pathogenesis of diabetes mellitus.Adv. Metab. Disord. 9:313–31
28. Shen SW, Reaven GM, Farquhar JW. 1970. Comparison of impedance to insulin-mediated glucose uptakein normal subjects and in subjects with latent diabetes. J. Clin. Invest. 49:2151–60
29. Warram JH, Martin BC, Krolewski AS, et al. 1990. Slow glucose removal rate and hyperinsulinemiaprecede the development of type II diabetes in the offspring of diabetic parents. Ann. Int. Med. 113:909–15
30. Abdul-Ghani MA, DeFronzo RA. 2009. Pathophysiology of prediabetes. Curr. Diabetes Rep. 9:193–9931. DeFronzo RA. 2009. Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for
the treatment of type 2 diabetes mellitus. Diabetes 58:773–9532. Reaven GM. 1999. Insulin resistance: a chicken that has come to roost. Ann. NY Acad. Sci. 892:45–5733. Reaven GM, Chen YI, Coulston AM, et al. 1983. Insulin secretion and action in noninsulin-dependent
diabetes mellitus. Is insulin resistance secondary to hypoinsulinemia? Am. J. Med. 75:85–9334. DeFronzo RA, Tobin JD, Andres R. 1979. Glucose clamp technique: a method for quantifying insulin
secretion and resistance. Am. J. Physiol. 237:E214–2335. Muniyappa R, Lee S, Chen H, et al. 2008. Current approaches for assessing insulin sensitivity and resistance
in vivo: advantages, limitations, and appropriate usage. Am. J. Physiol. Endocrinol. Metab. 294:E15–2636. Hills SA, Balkau B, Coppack SW, et al. 2004. The EGIR-RISC STUDY (The European group for
the study of insulin resistance: relationship between insulin sensitivity and cardiovascular disease risk): I.Methodology and objectives. Diabetologia 47:566–70
37. Ferrannini E, Balkau B, Coppack SW, et al. 2007. Insulin resistance, insulin response, and obesity asindicators of metabolic risk. J. Clin. Endocrinol. Metab. 92:2885–92
38. Gall WE, Beebe K, Lawton KA, et al. 2010. alpha-Hydroxybutyrate is an early biomarker of insulinresistance and glucose intolerance in a nondiabetic population. PLoS One 5:e10883
39. Gieger C, Geistlinger L, Altmaier E, et al. 2008. Genetics meets metabolomics: a genome-wide associationstudy of metabolite profiles in human serum. PLoS Genet. 4:e1000282
40. Suhre K, Shin SY, Petersen AK, et al. 2011. Human metabolic individuality in biomedical and pharma-ceutical research. Nature 477:54–60
www.annualreviews.org • Metabolomics and Insulin Resistance 305
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64-frontmatter ARI 18 December 2012 10:19
Annual Review ofMedicine
Volume 64, 2013Contents
Abiraterone and Novel Antiandrogens: Overcoming CastrationResistance in Prostate CancerR. Ferraldeschi, C. Pezaro, V. Karavasilis, and J. de Bono � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 1
Antibody-Drug Conjugates in Cancer TherapyEric L. Sievers and Peter D. Senter � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �15
Circulating Tumor Cells: From Bench to BedsideMarija Balic, Anthony Williams, Henry Lin, Ram Datar, and Richard J. Cote � � � � � � � � �31
Cytokines, Obesity, and Cancer: New Insights on Mechanisms LinkingObesity to Cancer Risk and ProgressionCandace A. Gilbert and Joyce M. Slingerland � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �45
Glioblastoma: Molecular Analysis and Clinical ImplicationsJason T. Huse, Eric Holland, and Lisa M. DeAngelis � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �59
Harnessing the Power of the Immune System to Target CancerGregory Lizee, Willem W. Overwijk, Laszlo Radvanyi, Jianjun Gao,
Padmanee Sharma, and Patrick Hwu � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �71
Human Papillomavirus Vaccines Six Years After ApprovalAlan R. Shaw � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �91
Reduced-Intensity Hematopoietic Stem Cell Transplants forMalignancies: Harnessing the Graft-Versus-Tumor EffectSaar Gill and David L. Porter � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 101
The Need for Lymph Node Dissection in NonmetastaticBreast CancerCatherine Pesce and Monica Morrow � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 119
The Role of Anti-Inflammatory Drugs in Colorectal CancerDingzhi Wang and Raymond N. DuBois � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 131
The Human Microbiome: From Symbiosis to PathogenesisEmiley A. Eloe-Fadrosh and David A. Rasko � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 145
The Rotavirus Saga RevisitedAlan R. Shaw � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 165
v
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64-frontmatter ARI 18 December 2012 10:19
Staphylococcal Infections: Mechanisms of Biofilm Maturation andDetachment as Critical Determinants of PathogenicityMichael Otto � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 175
Toward a Universal Influenza Virus Vaccine: Prospects and ChallengesNatalie Pica and Peter Palese � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 189
Host Genetics of HIV Acquisition and Viral ControlPatrick R. Shea, Kevin V. Shianna, Mary Carrington,
and David B. Goldstein � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 203
Systemic and Topical Drugs for the Prevention of HIV Infection:Antiretroviral Pre-exposure ProphylaxisJared Baeten and Connie Celum � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 219
Hyperaldosteronism as a Common Cause of Resistant HypertensionDavid A. Calhoun � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 233
Mechanisms of Premature Atherosclerosis in RheumatoidArthritis and LupusJ. Michelle Kahlenberg and Mariana J. Kaplan � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 249
Molecular Mechanisms in Progressive Idiopathic Pulmonary FibrosisMark P. Steele and David A. Schwartz � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 265
Reprogrammed Cells for Disease Modeling and Regenerative MedicineAnne B.C. Cherry and George Q. Daley � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 277
Application of Metabolomics to Diagnosis of Insulin ResistanceMichael V. Milburn and Kay A. Lawton � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 291
Defective Complement Inhibitory Function Predisposesto Renal DiseaseAnuja Java, John Atkinson, and Jane Salmon � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 307
New Therapies for GoutDaria B. Crittenden and Michael H. Pillinger � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 325
Pathogenesis of Immunoglobulin A Nephropathy: Recent Insightfrom Genetic StudiesKrzysztof Kiryluk, Jan Novak, and Ali G. Gharavi � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 339
Podocyte Biology and Pathogenesis of Kidney DiseaseJochen Reiser and Sanja Sever � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 357
Toward the Treatment and Prevention of Alzheimer’s Disease:Rational Strategies and Recent ProgressSam Gandy and Steven T. DeKosky � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 367
Psychiatry’s Integration with Medicine: The Role of DSM-5David J. Kupfer, Emily A. Kuhl, Lawson Wulsin � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 385
vi Contents
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.

ME64-frontmatter ARI 18 December 2012 10:19
Update on Typical and Atypical Antipsychotic DrugsHerbert Y. Meltzer � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 393
Ataluren as an Agent for Therapeutic Nonsense SuppressionStuart W. Peltz, Manal Morsy, Ellen M. Welch, and Allan Jacobson � � � � � � � � � � � � � � � � � � 407
Treating the Developing Brain: Implications from Human Imagingand Mouse GeneticsB.J. Casey, Siobhan S. Pattwell, Charles E. Glatt, and Francis S. Lee � � � � � � � � � � � � � � � � � � 427
Genetic Basis of Intellectual DisabilityJay W. Ellison, Jill A. Rosenfeld, and Lisa G. Shaffer � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 441
Sickle Cell Disease, Vasculopathy, and TherapeuticsAdetola A. Kassim and Michael R. DeBaun � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 451
Duty-Hour Limits and Patient Care and Resident Outcomes: CanHigh-Quality Studies Offer Insight into Complex Relationships?Ingrid Philibert, Thomas Nasca, Timothy Brigham, and Jane Shapiro � � � � � � � � � � � � � � � � � 467
Quality Measurement in HealthcareEliot J. Lazar, Peter Fleischut, and Brian K. Regan � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 485
Indexes
Cumulative Index of Contributing Authors, Volumes 60–64 � � � � � � � � � � � � � � � � � � � � � � � � � � � 497
Article Titles, Volumes 60–64 � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 501
Errata
An online log of corrections to Annual Review of Medicine articles may be found athttp://med.annualreviews.org/errata.shtml
Contents vii
Ann
u. R
ev. M
ed. 2
013.
64:2
91-3
05. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
by D
r. M
icha
el M
ilbur
n on
01/
18/1
3. F
or p
erso
nal u
se o
nly.
Related Documents