Aortic Dissection and Dissecting Aortic Aneurysms E. STANLEY CRAWFORD, M.D., LARS G. SVENSSON, M.D., JOSEPH S. COSELLI, M.D., HAZIM J. SAFI, M.D., and KENNETH R. HESS, M.S. Operation was employed in the treatment of 546 patients for complications of aortic dissection during the 32-year period of 1956-1988. Current concepts and operative techniques evolved during this period. Fortunately, about half the patients were treated during the latter 4 years, as modern therapy became standardized. The cumulative survival rate was 86% for all patients and 94% for those treated during recent years. Patho- logic processes and requirements of operation became clearer by treating 174 patients who had had 198 previous operations by the time of referral. Reoperation was required for compli- cations of operations now considered outdated, heart opera- tions in patients with ascending aortic dilatation, and progres- sive dilatation of residual segments of the aorta. The 546 pa- tients were followed, and a total of 838 operations were finally employed, resulting in total aortic replacement in 18, near total replacement in 41, entire thoracic aorta in 22, near total tho- racic aorta in 33, and the entire thoracoabdominal aorta in 148 patients. Long-term survival in 439 patients after final opera- tion was 66% and 44% at 5 and 10 years, respectively, despite the fact that the median age at first admission was 59. Opera- tive treatment appears to be well-established for this disease. T n HE SERIOUSNESS of aortic dissection and dis- secting aortic aneurysm has been generally ac- cepted. Earlier studies of untreated patients with acute dissection indicated that, in most cases, death occurred within 3 months.' Even among survivors, few patients survived the chronic phase more than 5 years because of rupture of fusiform aneurysms of the false lumen.'-3 With the development of operative techniques and their increasing application, mortality from early operation has steadily decreased and long-term survival has increased."9 Due to continued refinements in con- cepts, techniques of operation, and general supportive Presented at the 108th Annual Meeting of The American Surgical Association, San Francisco, California, May 2-4, 1988. Reprint requests and correspondence: E. Stanley Crawford, M.D., Department of Surgery, The Methodist Hospital, 6535 Fannin Street, Houston, TX 77030. Submitted for publication: May 18, 1988. From the Baylor College of Medicine and The Methodist Hospital, Houston, Texas measures, early survival from operation is now about 90%. 10-18 This report is concerned with the senior author's ob- servations in 614 patients personally treated during the period of 1956-1988. The relevance of this experience lies in the fact that it extends throughout much of the period during which surgical treatment was developing and consists, in large measure, of patients from a wide referral base who were highly selected because of prob- lems such as early and late complications of operations performed at the time, recurrence and progression of disease or conditions in the region of previous opera- tions, extensive aortic dilatation, the frequency of com- plications due to the disease, and the high incidence and nature of associated disease. Although this nonpopulation-based group of patients may not represent the true spectrum of complications in its natural setting, an intermittent review of this special group of patients with their frequently unique and exag- gerated features has permitted a better understanding of the pathologic features of the disease processes. This has provided the opportunity to better appreciate the thera- peutic requirements for both its prevention and treat- ment. Application of this knowledge in the latter part of the series, a period of general progress in the treatment of cardiovascular disease, has improved the results. This presentation is intended to summarize and emphasize some of the more important findings in a detailed study of these cases. Patients and Methods The records of all 614 patients with aortic dissection studied between 1956 and 1988 were reviewed, late fol- 254

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Aortic Dissection and Dissecting Aortic Aneurysms
E. STANLEY CRAWFORD, M.D., LARS G. SVENSSON, M.D., JOSEPH S. COSELLI, M.D.,HAZIM J. SAFI, M.D., and KENNETH R. HESS, M.S.
Operation was employed in the treatment of 546 patients forcomplications of aortic dissection during the 32-year period of1956-1988. Current concepts and operative techniques evolvedduring this period. Fortunately, about half the patients weretreated during the latter 4 years, as modern therapy becamestandardized. The cumulative survival rate was 86% for allpatients and 94% for those treated during recent years. Patho-logic processes and requirements of operation became clearerby treating 174 patients who had had 198 previous operationsby the time of referral. Reoperation was required for compli-cations of operations now considered outdated, heart opera-tions in patients with ascending aortic dilatation, and progres-sive dilatation of residual segments of the aorta. The 546 pa-tients were followed, and a total of 838 operations were finallyemployed, resulting in total aortic replacement in 18, near totalreplacement in 41, entire thoracic aorta in 22, near total tho-racic aorta in 33, and the entire thoracoabdominal aorta in 148patients. Long-term survival in 439 patients after final opera-tion was 66% and 44% at 5 and 10 years, respectively, despitethe fact that the median age at first admission was 59. Opera-tive treatment appears to be well-established for this disease.
Tn HE SERIOUSNESS of aortic dissection and dis-secting aortic aneurysm has been generally ac-cepted. Earlier studies of untreated patients
with acute dissection indicated that, in most cases, deathoccurred within 3 months.' Even among survivors, fewpatients survived the chronic phase more than 5 yearsbecause of rupture of fusiform aneurysms of the falselumen.'-3 With the development ofoperative techniquesand their increasing application, mortality from earlyoperation has steadily decreased and long-term survivalhas increased."9 Due to continued refinements in con-cepts, techniques of operation, and general supportive
Presented at the 108th Annual Meeting of The American SurgicalAssociation, San Francisco, California, May 2-4, 1988.
Reprint requests and correspondence: E. Stanley Crawford, M.D.,Department of Surgery, The Methodist Hospital, 6535 Fannin Street,Houston, TX 77030.Submitted for publication: May 18, 1988.
From the Baylor College of Medicine andThe Methodist Hospital, Houston, Texas
measures, early survival from operation is now about90%. 10-18
This report is concerned with the senior author's ob-servations in 614 patients personally treated during theperiod of 1956-1988. The relevance of this experiencelies in the fact that it extends throughout much of theperiod during which surgical treatment was developingand consists, in large measure, of patients from a widereferral base who were highly selected because of prob-lems such as early and late complications of operationsperformed at the time, recurrence and progression ofdisease or conditions in the region of previous opera-tions, extensive aortic dilatation, the frequency of com-plications due to the disease, and the high incidence andnature of associated disease.Although this nonpopulation-based group of patients
may not represent the true spectrum ofcomplications inits natural setting, an intermittent review of this specialgroup of patients with their frequently unique and exag-gerated features has permitted a better understanding ofthe pathologic features of the disease processes. This hasprovided the opportunity to better appreciate the thera-peutic requirements for both its prevention and treat-ment. Application of this knowledge in the latter part ofthe series, a period of general progress in the treatmentof cardiovascular disease, has improved the results. Thispresentation is intended to summarize and emphasizesome of the more important findings in a detailed studyof these cases.
Patients and Methods
The records of all 614 patients with aortic dissectionstudied between 1956 and 1988 were reviewed, late fol-
254
AORTIC DISSECTION
low-up was updated (99% completed), and pertinent in-formation was added to the data base stored on com-
puter and analyzed. In 82 patients, operation was notperformed initially in 35 who had acute and 47 who hadchronic dissection. Of the former, seven were Type I,
with dissection involving most of aorta, and three were
Type II, with dissection limited to ascending aorta. Sixof these ten patients died before operation could be per-
formed. The remaining four patients had repair per-
formed at other institutions and were immediately re-
ferred for possible further treatment. These patients didnot need another operation and were treated medically.
Twenty-five patients had acute Type III (limited toaorta beyond left subclavian artery) dissections. Ofthese, 19 were in good condition, the dissection was notcomplicated, and they were treated medically as a defin-itive form of therapy. Medical treatment failed in twopatients, both of whom had successful descending tho-racic aortic replacement. The remaining six Type IIIpatients experienced pain and had dilated descendingthoracic aortas, but were treated medically because ofadvanced age and associated cerebrovascular, cardiopul-monary, and renal disease that posed prohibitive opera-
tive risks. Three patients experienced rupture in the hos-pital, and operation was successful for one patient, whoremained in the hospital on a respirator for 1 year be-cause ofcomplications related to obstructive pulmonarydisease. The other patients died later, after transfer backto nursing homes.Of the 47 patients with chronic dissection not treated
initially by operation, one with rupture died beforeoperation could be performed, 31 (with dilatation lessthan 6 cm in diameter) did not need operation, and for15 who had severe associated risks for treatment of dif-fuse disease as above, operation was not recommended.These 47 patients were treated medically and followed.Twelve of the 31 patients who did not need surgery
initially were later treated by operation, and eight ofthose for whom surgery was not recommended died ofassociated disease or rupture. Thus, of these 82 patientson whom operation was not performed initially, 68(83%) were not treated surgically and are not consideredfurther in the study. The 14 patients (17%) ultimatelytreated by operation are included.
Surgically Treated Patients
Operation was ultimately employed in the treatmentof 546 patients with aortic dissection by 838 aorticoperations, 198 performed elsewhere before referral and640 at our institution (Tables 1 and 2). There were 127females (23%) and 419 males (77%) in the series, whoseages ranged from 13 to 87 years (median 59). Ninety-sixpatients (18%) had Marfan syndrome. Hypertension waspresent in 406 (74%).
TABLE 1. Aortic Operations Performedfor Aortic Dissectionor Aneurysm (546 Patients)
Prior Author TotalOperations Operations Operations
ASC 105 143 248ASC/ARCH 3 98 101ASC/ARCH/DES 0 3 3ASC/DES 0 1 1ARCH 1 10 11ARCH/DES 0 6 6DES 37 170 207DES/TAA 0 3 3DES/AAA 2 8 10TAA 6 169 175TAA/AAA 0 9 9AAA 44 20 64
Total 198* 640 838
ASC = ascending aorta.DES = descending aorta.TAA = thoracoabdominal aorta.AAA = abdominal aorta.ARCH = aortic arch.* 174 patients had prior aortic operations.
In 221 patients, the dissecting process involved theentire aorta, was limited to the ascending aorta in 67,and involved the descending thoracic and abdominalaorta in 258 patients. These cases therefore may be clas-sified as DeBakey types 1, 2, and 3, respectively. Whentreated at our institution, the dissecting process wasacute in 133 (24%) and chronic in 413 (76%) patients.Dissection was frequently superimposed upon pre-exist-ing aneurysms, more commonly in the ascending aortaand arch, but also in some patients with aneurysms lo-cated in the descending thoracic or thoracoabdominalaortic segments. The latter lesions were not always iden-tified as such before operation, which was performedbecause leakage or rupture of a regular aneurysm wassuspected. A tear was not present in a small number ofthese cases, in whom the dissected space was simplyfilled with clot.
Aortic specimens were available for histologic exami-nation in 372 patients. The aortic media was abnormalin all specimens, with degeneration of the media in 355of these patients and aortitis in 17. Atherosclerosis, pri-marily intimal, was superimposed upon the medial
TABLE 2. Ratio ofAortic Operations to Patient (546 Patients)
Number Number ofPer Patient Patients
1 3222 1713 404 115 2
255VOl. 208 * NO. 3
CRAWFORD AND OTHERS
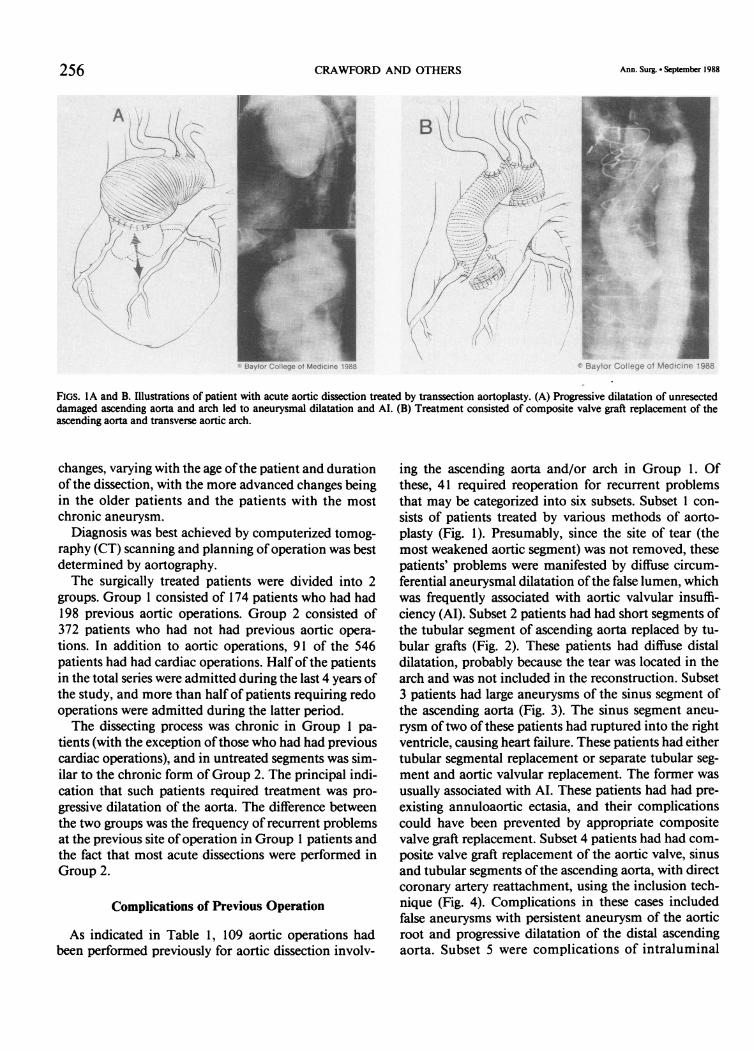
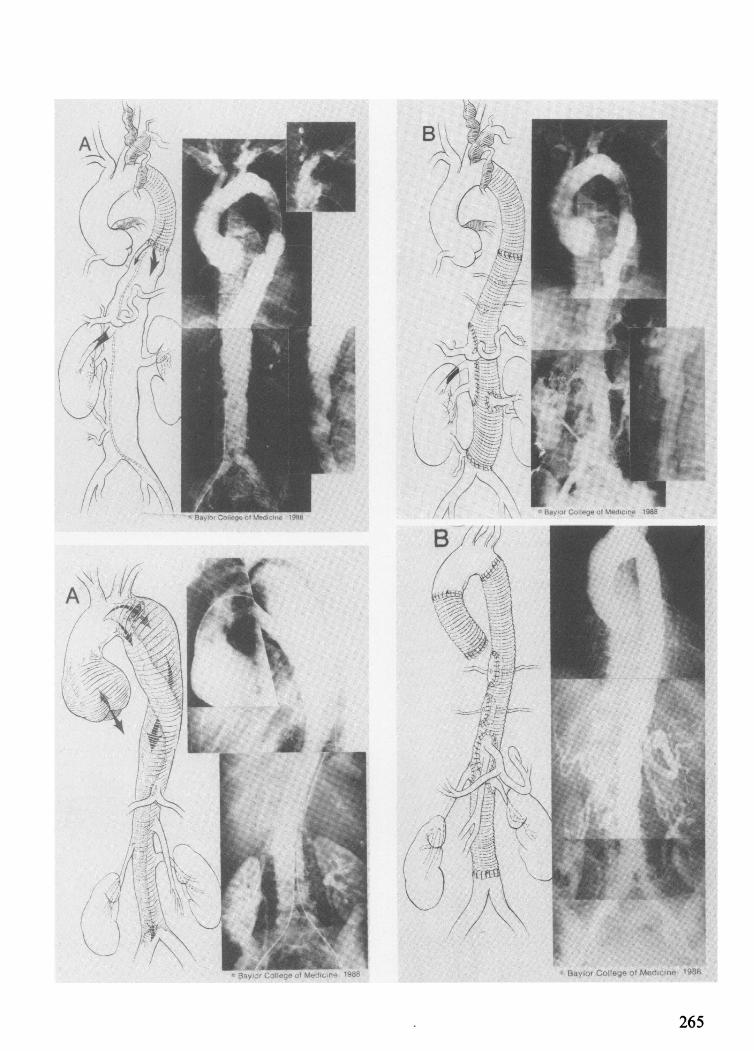
FIGS. IA and B. Illustrations of patient with acute aortic dissection treated by transsection aortoplasty. (A) Progressive dilatation of unresecteddamaged ascending aorta and arch led to aneurysmal dilatation and AI. (B) Treatment consisted of composite valve graft replacement of theascending aorta and transverse aortic arch.
changes, varying with the age ofthe patient and durationof the dissection, with the more advanced changes beingin the older patients and the patients with the mostchronic aneurysm.
Diagnosis was best achieved by computerized tomog-raphy (CT) scanning and planning of operation was bestdetermined by aortography.The surgically treated patients were divided into 2
groups. Group 1 consisted of 174 patients who had had198 previous aortic operations. Group 2 consisted of372 patients who had not had previous aortic opera-tions. In addition to aortic operations, 91 of the 546patients had had cardiac operations. Half of the patientsin the total series were admitted during the last 4 years ofthe study, and more than half of patients requiring redooperations were admitted during the latter period.The dissecting process was chronic in Group 1 pa-
tients (with the exception ofthose who had had previouscardiac operations), and in untreated segments was sim-ilar to the chronic form of Group 2. The principal indi-cation that such patients required treatment was pro-gressive dilatation of the aorta. The difference betweenthe two groups was the frequency of recurrent problemsat the previous site of operation in Group 1 patients andthe fact that most acute dissections were performed inGroup 2.
Complications of Previous Operation
As indicated in Table 1, 109 aortic operations hadbeen performed previously for aortic dissection involv-
ing the ascending aorta and/or arch in Group 1. Ofthese, 41 required reoperation for recurrent problemsthat may be categorized into six subsets. Subset 1 con-sists of patients treated by various methods of aorto-plasty (Fig. 1). Presumably, since the site of tear (themost weakened aortic segment) was not removed, thesepatients' problems were manifested by diffuse circum-ferential aneurysmal dilatation ofthe false lumen, whichwas frequently associated with aortic valvular insuffi-ciency (Al). Subset 2 patients had had short segments ofthe tubular segment of ascending aorta replaced by tu-bular grafts (Fig. 2). These patients had diffuse distaldilatation, probably because the tear was located in thearch and was not included in the reconstruction. Subset3 patients had large aneurysms of the sinus segment ofthe ascending aorta (Fig. 3). The sinus segment aneu-rysm oftwo of these patients had ruptured into the rightventricle, causing heart failure. These patients had eithertubular segmental replacement or separate tubular seg-ment and aortic valvular replacement. The former wasusually associated with AI. These patients had had pre-existing annuloaortic ectasia, and their complicationscould have been prevented by appropriate compositevalve graft replacement. Subset 4 patients had had com-posite valve graft replacement of the aortic valve, sinusand tubular segments ofthe ascending aorta, with directcoronary artery reattachment, using the inclusion tech-nique (Fig. 4). Complications in these cases includedfalse aneurysms with persistent aneurysm of the aorticroot and progressive dilatation of the distal ascendingaorta. Subset 5 were complications of intraluminal
256 Ann. Surg * September 1988

AORTIC DISSECTION 257
FIGS. 2A and B. This patient had treatment ofacute dissection by limited graft replacement ofthe proximal tubular segment ofthe ascending aorta.
(A) Progressive dilatation ofdistal ascending aorta and arch occurred over a 3-year period because the site oforigin was not replaced. (B) Treatmentconsisted of graft replacement of distal ascending aorta and aortic arch.
grafts that included perigraft leakage and aneurysms,
graft stenosis, and hemolysis (Fig. 5). Subset 6 consistedof patients with perigraft infection (Fig. 6). The intervalbetween the original operation and our redo operationvaried from 65 days to 25 years (median 4.2 years).Common to both groups ofpatients was aortic dissec-
tion occurring as a complication of previous cardiacoperations. Ninety-one patients in this series of 546cases had had previous cardiac operations, 37 had coro-
nary artery bypass graft (CAB), 48 had aortic valve re-
placement (AVR), and six had both. Twenty-seven ofthe former and 20 of the latter two groups of patientsentered 3 months to 8 years later with aortic dissectionof the ascending aorta of either DeBakey type 1 or 2(Figs. 7 and 8). The dissection process was acute in 12patients (26%) and chronic in 35 (74%). The operativefindings in these cases were consistent with dissectionsuperimposed upon pre-existing fusiform aneurysm of
FIG. 3. Illustrations of limited separate graft replacement of tubular segment of aorta and valve replacement of aortic valve at time of acutedissection. (A) Rupture of enlarged residual sinus segment aneurysm into right ventricle that caused heart failure from large left to right shunt. (B)Treatment consisted of composite valve graft replacement of valve and entire ascending aorta and closure of fistula.
Vol. 208 * No. 3

*' Baylor College of Medicine 1987
4 Baylor College of Medicine 1987
258
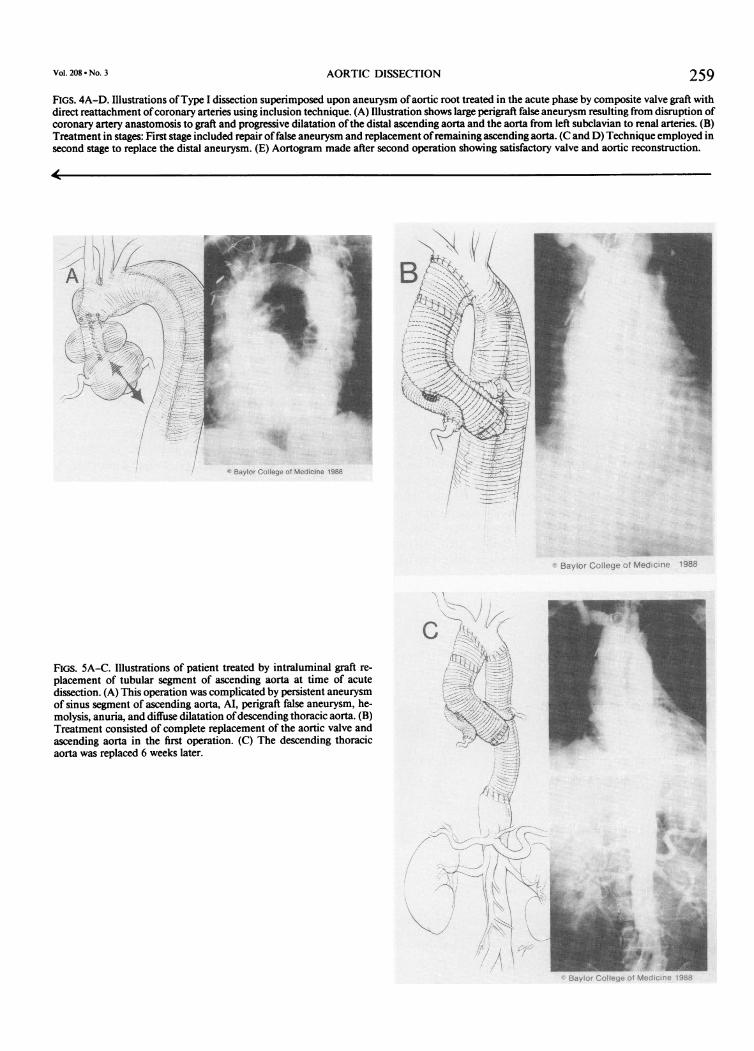
Vol. 208 * No. 3 AORTIC DISSECTION 259FIGS. 4A-D. Illustrations ofType I dissection superimposed upon aneurysm ofaortic root treated in the acute phase by composite valve graft withdirect reattachment ofcoronary arteries using inclusion technique. (A) Illustration shows large perigraft false aneurysm resulting from disruption ofcoronary artery anastomosis to graft and progressive dilatation ofthe distal ascending aorta and the aorta from left subclavian to renal arteries. (B)Treatment in stages: First stage included repair of false aneurysm and replacement ofremaining ascending aorta. (C and D) Technique employed insecond stage to replace the distal aneurysm. (E) Aortogram made after second operation showing satisfactory valve and aortic reconstruction.
* Baylor College of Medicine 1986
FIGS. 5A-C. Illustrations of patient treated by intraluminal graft re-placement of tubular segment of ascending aorta at time of acutedissection. (A) This operation was complicated by persistent aneurysmof sinus segment of ascending aorta, AI, perigraft false aneurysm, he-molysis, anuria, and diffuse dilatation ofdescending thoracic aorta. (B)Treatment consisted of complete replacement of the aortic valve andascending aorta in the first operation. (C) The descending thoracicaorta was replaced 6 weeks later.

CRAWFORD AND OTHERS
)
W Baylor College of Medicine 1988
FIGS. 6A and B. Illustrations of patient who developed infection of ascending aortic graft employed for treatment of aortic dissection. Thiscomplication was associated with development of aorto-right ventricular fistula and heart failure. (A) Diagram and aortogram made beforeoperation showing defect. (B) Method of repair using cardiopulmonary bypass, profound hypothermia, and circulatory arrest to enter chest andviable muscle flaps and permanent antibiotic suppressive treatment to control infection.
the ascending aorta. A review of available operative re-ports indicated the presence of aortic dilatation and ex-cess bleeding at either aortotomy or graft anastomosissites. Of interest is the fact that the ascending aorta hadnot been visualized before operation in most patients,despite cardiac catheterization and cine angiography.Thus, in the 229 patients who required operation for
dissection of the ascending aorta and/or arch as theirfirst operation by us, 88 (38%) were in-patients who had
either aortic dissection operations that now may be con-sidered outdated or underlying aortic disease that hadprogressed or was overlooked or, more commonly, ig-nored at the time of cardiac operation.
Patient Characteristics
Due to the complex nature of the clinical problemsand the need for multiple operations in these patients,
FIGS. 7A and B. Illustrations ofaortic dissection occurrence superimposed upon aortic dilatation present at time ofcoronary artery bypass grafting.(A) Drawing and angiogram showing nature and extent ofdissecting process 3 years after operation. (B) Results oftreatment. The chest was openedwith the circulation arrested, the entire ascending aorta was replaced with a graft, and patent coronary artery grafts were attached to the graft.
260 Ann. Surg * September 1988

AORTIC DISSECTION
College of Medicine 1988
ioGS. 8A and B. Illustrations of dissection occurring in an aneurysm of the ascending aorta that was present at the time ofAVR but not detecteduntil time of operation. (A) Drawing and aortogram showing size of aneurysm at time of second operation 3 years later. (B) Drawing andpostoperative aortogram made after second operation.
they were reclassified into two groups for analysis, with229 patients requiring proximal operations at the as-cending aorta and/or aortic arch level, and 317 patientsrequiring more distal operations of the descending tho-racic aorta and/or the thoracoabdominal aortic seg-ments at the time of admission as their first operation.The respective 29 and 25 preoperative, operative, andpostoperative variables are presented in Tables 3 and 4.These include clinical manifestations, associated dis-eases, operative events, postoperative morbidity andmortality, and period of treatment. Symptoms weregraded from 1 to 4, based on the degree of severity.Patients with Grade 1 were asymptomatic; those withGrade 2 had mild symptoms, including occasional pain,cough, hoarseness (paralyzed left vocal cord), and dys-phagia; those with Grade 3 experienced continuouspain; and finally, those with Grade 4 experienced acuteonset of pain, heart failure, neurologic deficits, hypoten-sion, anuria, or bowel ischemia.As previously indicated, the disease was frequently
diffuse and involved both aortic regions under this clas-sification. Operation, replacing only a localized seg-ment, was necessary at the time of admission in somecases. In others, long segments, even the entire aorta,needed replacement. Operative treatment was fre-quently staged in the latter, removing the most life-threatening segment first; and then, at a later date, theremaining diseased segment was replaced. Because theremaining aneurysmal segment posed risk of ruptureand death, this postoperative variable (residual aneu-rysm) was thought to be possibly a significant factor toconsider in the period during which these patients weretreated. Thirty-eight per cent of the patients requiringascending and/or arch operation were treated during
the last 2 years, and one half of those requiring distaloperation were treated during the past 4 years (Tables3 and 4).
Variables examined but not included in the analysisbecause they had no clinically significant effect on mor-tality on univariate analysis or because the numberswere too small included: 1) etiologic factors: infection/mycotic aneurysm, aortitis, false aneurysm, inflamma-tory aneurysm, previous use of steroids, and histology ofaortic wall; 2) associated disease: diabetes, cancer, diver-ticular disease, hiatus hernia, peptic ulcer, gout, pre-vious gastrointestinal (G.I.) surgery, occlusion of the ca-rotid-subclavian arteries, mesenteric, renal, aorto-iliac,or femoro-popliteal arteries, and gallstones; 3) operative:aortic cross-clamp times, profound hypothermia, circu-latory arrest times, cardiopulmonary bypass time, atrio-femoral bypass, use of intraluminal shunt, time for uri-nary clearance of dye, type of previous cardiac or vascu-lar operation, mitral valve replacement, pacemakerinsertion, both combined distal and proximal repair,and combined carotid, innominate or subclavian by-pass.
Indications for Operation
Ascending aortic operation was recommended at thetime of admission in all patients with acute dissectionthat involved the ascending aorta to prevent or treatcardiac complications (i.e., rupture, tamponade, AI, andaorto-cardiac chamber fistulae). Medical therapy wasemployed in patients with uncomplicated acute dissec-tion arising distal to the left subclavian artery. Operativetreatment was employed in the latter for complicationsincluding vessel obstruction, persistent pain, aortic dila-tation greater than 5.5 cm, and rupture when a favorable
Vol. 208 * No. 3 261
262 CRAWFORD AND OTHERS Ann. Surg. September 1988
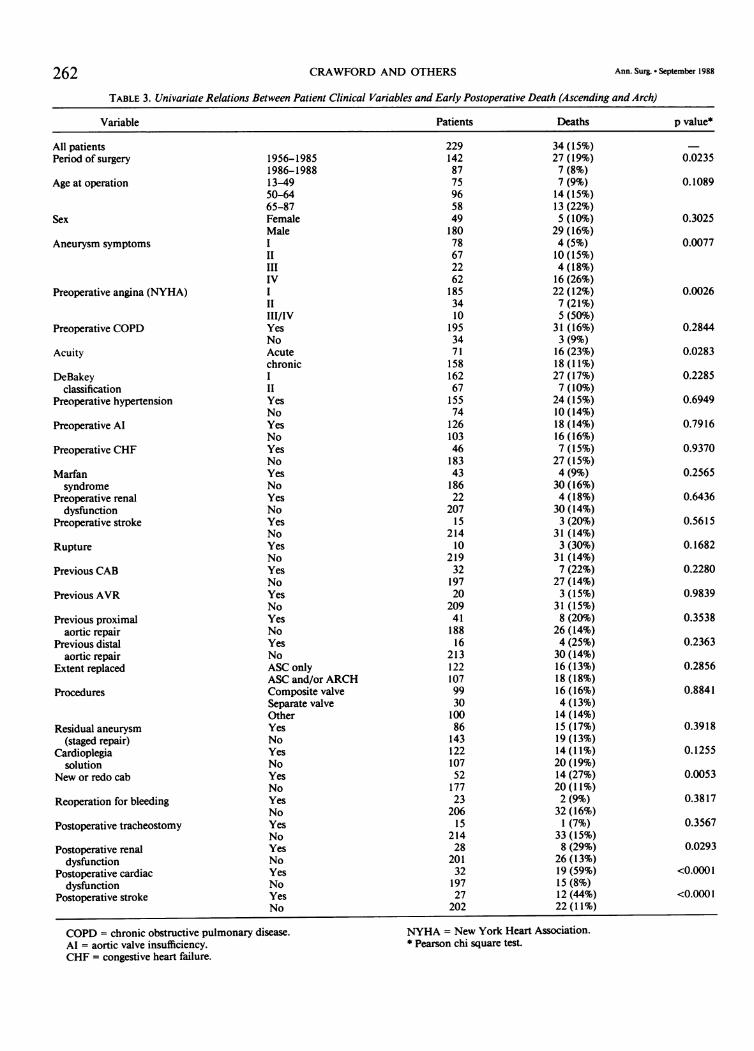
TABLE 3. Univariate Relations Between Patient Clinical Variables and Early Postoperative Death (Ascending and Arch)
Variable Patients Deaths p value*
All patients 229 34 (15%)Period of surgery 1956-1985 142 27 (19%) 0.0235
1986-1988 87 7 (8%)Age at operation 13-49 75 7 (9%) 0.1089
50-64 96 14 (15%)65-87 58 13 (22%)
Sex Female 49 5 (10%) 0.3025Male 180 29 (16%)
Aneurysm symptoms I 78 4 (5%) 0.0077II 67 10 (15%)III 22 4 (18%)IV 62 16 (26%)
Preoperative angina (NYHA) I 185 22 (12%) 0.0026II 34 7 (21%)III/IV 10 5 (50%)
Preoperative COPD Yes 195 31 (16%) 0.2844No 34 3 (9%)
Acuity Acute 71 16 (23%) 0.0283chronic 158 18 (11%)
DeBakey I 162 27 (17%) 0.2285classification II 67 7 (10%)
Preoperative hypertension Yes 155 24 (15%) 0.6949No 74 10 (14%)
Preoperative Al Yes 126 18 (14%) 0.7916No 103 16 (16%)
Preoperative CHF Yes 46 7 (15%) 0.9370No 183 27 (15%)
Marfan Yes 43 4(9%) 0.2565syndrome No 186 30 (16%)
Preoperative renal Yes 22 4 (18%) 0.6436dysfunction No 207 30 (14%)
Preoperative stroke Yes 15 3 (20%) 0.5615No 214 31 (14%)
Rupture Yes 10 3 (30%) 0.1682No 219 31 (14%)
Previous CAB Yes 32 7 (22%) 0.2280No 197 27 (14%)
Previous AVR Yes 20 3 (15%) 0.9839No 209 31 (15%)
Previous proximal Yes 41 8 (20%) 0.3538aortic repair No 188 26 (14%)
Previous distal Yes 16 4 (25%) 0.2363aorticrepair No 213 30(14%)
Extent replaced ASC only 122 16 (13%) 0.2856ASC and/or ARCH 107 18 (18%)
Procedures Composite valve 99 16 (16%) 0.8841Separate valve 30 4 (13%)Other 100 14 (14%)
Residual aneurysm Yes 86 15 (17%) 0.3918(staged repair) No 143 19 (13%)
Cardioplegia Yes 122 14 (11%) 0.1255solution No 107 20 (19%)
New or redo cab Yes 52 14 (27%) 0.0053No 177 20(11%)
Reoperation for bleeding Yes 23 2 (9%) 0.3817No 206 32 (16%)
Postoperative tracheostomy Yes 15 1 (7%) 0.3567No 214 33 (15%)
Postoperative renal Yes 28 8 (29%) 0.0293dysfunction No 201 26 (13%)
Postoperative cardiac Yes 32 19 (59%) <0.0001dysfunction No 197 15 (8%)
Postoperative stroke Yes 27 12 (44%) <0.0001No 202 22 (11%)
COPD = chronic obstructive pulmonary disease. NYHA = New York Heart Association.AI = aortic valve insufficiency. * Pearson chi square test.CHF = congestive heart failure.

AORTIC DISSECTION 263TABLE 4. Univariate Relations Between Patient Clinical Variables and Early Posloperative Death Distal Aorta
Variable Patients Deaths p value*
All patientsPeriod of surgery
Age at operation
Sex
Aneurysm symptoms
Preoperative angina(NYHA)
Preoperative COPD
Acuity
DeBakeyclassification
Preoperative hypertension
Marfansyndrome
Preoperative renaldysfunction
Preoperative neuromusculardysfunction
Rupture
Previous CAB
Previous AVR
Previous proximalaortic repair
Previous distalaortic repair
Extent replaced
ProceduresTemporary bypassSimple X-clamp
Residual aneurysm(staged repair)
Reoperation for bleeding
Postoperative tracheostomy
Postoperative renaldysfunction
Postoperative cardiacdysfunction
Postoperativeneuromusculardysfunction
* Pearson chi-square test.DES = descending aorta.
1956-19831984-198813-4950-6465-87FemaleMale
IVIIIV
II/III/IVYesNoAcutechronicIIIIYesNoYesNoYesNoYesNoYesNoYesNoYesNoYesnoYesNoDESTAA
YesNoYesNoYesNoYesNoYesNo
YesNo
3171581598112411278
239671356055
3001784
23362
25559
2582516653
26437
2938
30924
29311
30634
28363
25469
248162155
8723052
26524
29319
29873
24414
303
51266
41 (13%)33 (21%)8 (5%)5 (6%)14 (11%)22 (20%)7 (9%)
34 (14%)2 (3%)6 (4%)15 (25%)18 (33%)
39 (13%)2 (12%)16 (19%)25 (11%)22 (35%)19 (7%)2 (3%)
39 (15%)32 (13%)9 (14%)2 (4%)
39 (15%)8 (22%)
37 (12%)3 (38%)
38 (12%)4 (17%)37 (13%)
1 (9%)40 (13%)2 (6%)
39 (14%)4 (6%)37 (15%)10 (14%)31 (13%)23 (14%)18 (12%)
1 1(13%)30 (13%)11(21%)30 (11%)9 (38%)
32 (11%)4 (21%)37 (12%)13 (18%)28 (11%)7 (50%)
34 (11%)
<0.000 1
0.0178
0.2301
<0.0001
0.8826
0.0515
<0.000 1
0.0155
0.8484
0.0294
0.0938
0.0360
0.5708
0.6991
0.1947
0.0819
0.6626
0.4930
0.9246
0.0534
<0.000 1
0.2767
0.1572
<0.0001
0.044911 (22%)30(11%)
TAA = thoracoabdominal aorta.COPD = chronic obstructive pulmonary disease.
outcome was thought possible. The majority of our pa-tients with acute type III dissections had these compli-cations at the time of entry and were thus treated surgi-cally. Diffuse aortic dilatation or rupture resulting from
dissection superimposed on pre-existing fusiform aneu-
rysm was the most common indication in this group.Consequently, most patients were treated by graft re-
placement of long aortic segments of either the descend-
Vol. 208 * No. 3

Ann. Surg. September 1988CRAWFORD AND OTHERS
B
FIGS. 9A and B. (A) Drawing and aortogram showing typical aneurysm limited to the descending thoracic segment of the distal diffuse dissectingprocess. (B) Drawing and aortogram show result of our preferred method of treatment of either acute or chronic dissection at this level, whichconsists of insertion of a regular tube graft with sutures.
ing thoracic or both descending thoracic and abdominalaorta.The indications for operative treatment in the pa-
tients with chronic dissection again varied with the seg-
ment involved. Operation was considered indicated inpatients with chronic dissection of the ascending aortaand arch who had persistent or new cardiac complica-tions, those who had complications of previous ascend-ing aortic and heart operations, and in those associatedwith dilatation more than 6 cm in diameter. The indica-tion for elective distal operation in patients with chronicdissection was progressive dilatation greater than 6 cm(Fig. 9). Urgent operation was indicated for aneurysmalsymptoms and rupture. Operation was usually staged inpatients with diffuse disease ofthe aorta (involvement ofboth proximal and distal segments) by removing themost life-threatening segment first, and then the other ata later date, 6 weeks to 3 months (Figs. 4-5, 10-12). Thespecific indications for reoperation for the ascendingaorta and arch have been described and illustratedabove. The indications for reoperation in distal seg-
ments of the aorta were false aneurysm, inappropriateprevious operation, and progressive dilatation of distalsegments (Fig. 10).
Operative Techniques
The operative techniques employed in these patientswere those that were available at the time of their re-
spective operations and varied with the aortic segmentinvolved in the operation, the stage of disease, the com-plications produced by the disease or previous aortic or
cardiac operation, and the period of treatment as pre-
viously described. Our current methods of proximaloperation became standardized by early 1985 after re-
view of the problems that recur after operation for dis-section or cardiac operations. These techniques were
first reported in 1985 and again in 1986.1617In brief, theprinciples oftreatment include complete replacement ofthe entire tubular segment of ascending aorta in all pa-tients with proximal acute dissection. Replacement was
extended into transverse aortic arch in patients whosesite of origin was located in the arch and also whenindicated for brachiocephalic arterial involvement. Re-placement was extended proximally to include the sinussegment of aorta and valve in patients with pre-existingaortic dilatation and in those patients with acute dissec-tion in whom the proximal aortic wall did not allow theperformance of a secure anastomosis. Attempts were
FIGS. lOA and B. Illustrations of patient with progressive dilatation of distal aorta and visceral arterial obstruction present after proximal graftreplacement for acute dissection in a patient with Takayasu's aortitis. (A) Location and extent of previous graft, current dilatation, visceralobstruction, and small vessel aneurysms characteristic ofthis form of aortitis. (B) Drawing and aortogram showing method oftreatment. The smallaneurysms were replaced later.
FiGS. 11A and B. Illustrations of patient with Marfan syndrome whose cardiovascular manifestations included fusiform aneurysm of aortic rootwith AI and diffusely dilated dissection of the distal aorta treated in stages. (A) Drawing and aortogram showing nature, location, and extent ofdisease. (B) Drawing and aortogram showing grafts in place and functioning.
264
Li)1
ft
265
4
..:Ie
II I.. i

6 Baylor College of Medicine 1987
1 Baylor College of Medicine 1987
FIGS. 12A-C. Illustrations of patient with diffuse chronic dissectinganeurysm involving the entire aorta, which was treated in stages. (A)Drawing and aortogram show extent ofaneurysm. (B) Ascending aortaand arch were replaced at first operation and the descending thoracicaorta at second operation. (C) The remaining aorta was replaced atthird operation. Reconstruction in our 18 patients requiring total aor-tic replacement for chronic dissection was performed in two stages inmost and was dependent upon physiologic events of operation.

TABLE 5. Aortic Dissection 30-Day Survival According to Acuity, Location ofOperation, and Period ofAuthors' Treatment (First Operation)
Acute Chronic
Location Period Patients Survival Patients Survival
ASC/ARCH 56-85 47 33 (70%) 95 82 (86%)86-88 24 22 (92%) 63 58 (92%)
DES 56-83 22 11 (50%) 60 51 (85%)84-88 19 16 (84%) 61 61 (100%)
TAA/AAA 56-83 12 5 (42%) 64 58 (91%)84-88 9 8 (89%) 70 66 (94%)
ASC = ascending aorta.ARCH = aortic arch.DES = descending aorta.
TAA = thoracoabdominal.AAA = abdominal aorta.
made to redirect flow distally into true lumen by obli-teration of false channels using Teflon.T felt in patientswith acute dissection. Distal flow was re-established inboth distal channels in patients with chronic dissection.When the sinus segment of aorta and valve were pre-
served in patients with acute dissection, the proximaldissection channel was obliterated proximally by sand-wiching the dissected walls between strips of Teflon felt.When the sinus segment was replaced, the coronary ar-teries, when involved, were reattached to the graft, usingaorto-distal coronary artery vein bypass grafts. The cor-onary arteries were reattached by small Dacron.T grafts(modified Cabrol technique) in patients with chronicdissection requiring sinus segment replacement (Fig.5)." Cardiopulmonary bypass and cold dilute oxygen-ated blood potassium cardioplegia were employed in85% of cases during the last 2 years. During this time,profound hypothermia and circulatory arrest were alsoemployed in all patients with acute dissection, as well asin all patients in whom the arch was replaced regardlessof acuity.'2"18 Hypothermic arrest was produced by fem-oral vein-femoral artery bypass perfusion in the groinbefore chest entry in patients with large aneurysms, inthose with contained ruptured false aneurysms, and inthose with infection to prevent fatal hemorrhage and tolimit the needs of exposure.'1'7
Prealbuminized knitted dacron grafts or woven da-cron composite valve-grafts were sutured in place, usingpolypropylene in the former and dacron sutures in thelatter. At this level, intraluminal grafts and inclusiontechniques were abandoned.
In the 229 patients who had either ascending aorta(122) or ascending aorta and aortic arch replacement( 107) as their first operation, composite valve grafts wereused in 99 and separate valve and graft in 30. The aorticvalve was retained in 100 who had various operations,including closure of false aneurysm and simple graftreplacement of tubular segments of the ascending aorta(Table 3).
As our first operation in 317 patients, distal operationofthe descending thoracic aorta or both descending tho-racic and abdominal aorta were replaced by dacrongrafts sutured in place using inclusion technique (Table4). Visceral arteries were reattached in the latter patients(Figs. 11 and 12). Intercostal and lumbar arteries werealso reattached in the latter cases when the disease waschronic. Attempts to reattach these vessels in patientswith acute dissection were usually unsuccessful andwere associated with bleeding. Profound hypothermiaand circulatory arrest were employed when proximalexposure ofthe distal transverse aortic arch was impossi-ble for clamping, in those with large aneurysms, thosewith contained rupture, in some who developed eitherpulmonary artery or aortic lacerations during operation,and in other cases where both proximal and distal aorticsegments required simultaneous replacement.'5 The lat-ter operations were performed through posterolateralincisions, with hypothermia being obtained by femoralvein-femoral artery cardiopulmonary bypass.
Various methods were employed to prevent paraple-gia.'9 These included surface hypothermia, profoundhypothermia, and temporary bypass with and withoutsomatosensory-evoked potential monitoring. Thesemethods were no more effective in preventing paresisthan simple aortic cross-clamping combined with proxi-mal blood pressure control using pharmacologicalagents.
Statistical Methods
Standard methods were employed, using the BMDPstatistical software package (BMDP Statistical SoftwareIncorporated, Los Angeles, CA). Univariate (Pearsonchi square test, BMDP4F) and multivariate (stepwiselogistic regression, BMDPLR) analyses were usedto identify statistically significant clinical predictorsof early mortality. Kaplan-Meier survival curves, cor-responding Cox-Mantel log-rank tests (BMDP1 L),
267Vol. 208 - No. 3 AORTIC DISSECTION
CRAWFORD AND OTHERS Ann. Surg. - September 1988
REPAIR OF AORTIC DISSECTIONTHIRTY-DAY MORTALITY
30-Day Mortality (%) Number of Patients
ASCENDING/ARCH DISSECTIONTHIRTY-DAY MORTALITY
30-Day Mortality (%)
56-79 1980 1981 1982 1983 1984 1985 1986 1987'
546 Patients Total Year of Surgery * Includes Jan. Feb. 1988
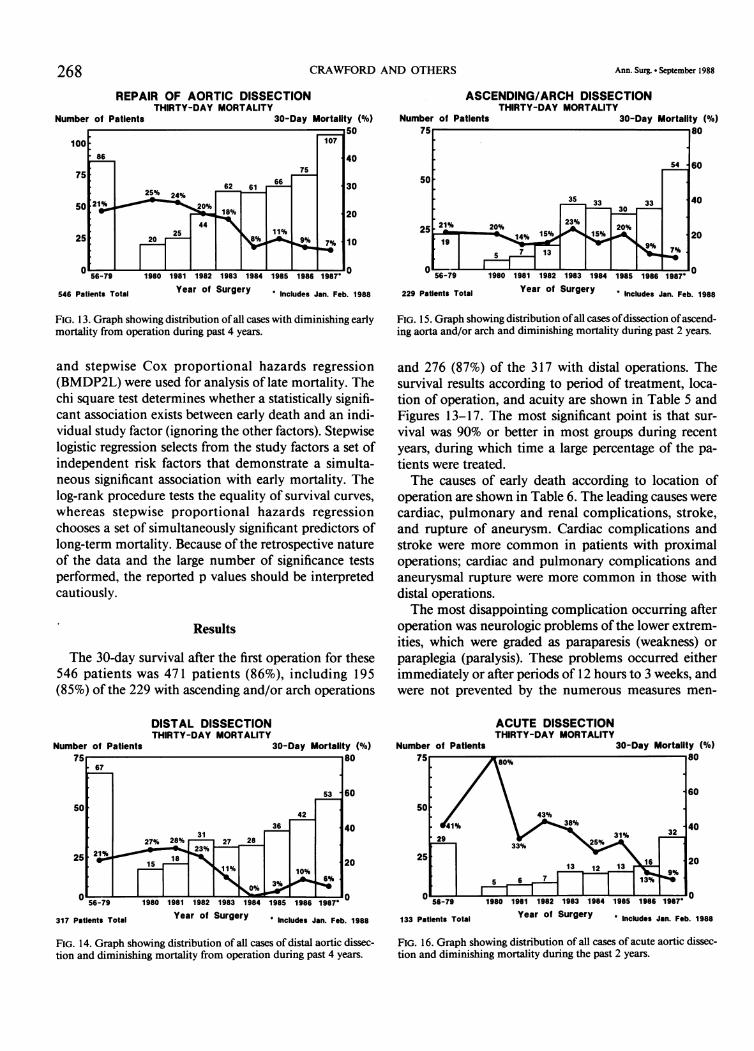
FIG. 13. Graph showing distribution of all cases with diminishing earlymortality from operation during past 4 years.
and stepwise Cox proportional hazards regression(BMDP2L) were used for analysis of late mortality. Thechi square test determines whether a statistically signifi-cant association exists between early death and an indi-vidual study factor (ignoring the other factors). Stepwiselogistic regression selects from the study factors a set ofindependent risk factors that demonstrate a simulta-neous significant association with early mortality. Thelog-rank procedure tests the equality of survival curves,whereas stepwise proportional hazards regressionchooses a set of simultaneously significant predictors oflong-term mortality. Because of the retrospective natureof the data and the large number of significance testsperformed, the reported p values should be interpretedcautiously.
Results
The 30-day survival after the first operation for these546 patients was 471 patients (86%), including 195(85%) of the 229 with ascending and/or arch operations
229 Patients Total Year of Surgery ' Includes Jan. Feb. 1988
FIG. 15. Graph showing distribution ofall cases ofdissection ofascend-ing aorta and/or arch and diminishing mortality during past 2 years.
and 276 (87%) of the 317 with distal operations. Thesurvival results according to period of treatment, loca-tion of operation, and acuity are shown in Table 5 andFigures 13-17. The most significant point is that sur-vival was 90% or better in most groups during recentyears, during which time a large percentage of the pa-tients were treated.The causes of early death according to location of
operation are shown in Table 6. The leading causes werecardiac, pulmonary and renal complications, stroke,and rupture of aneurysm. Cardiac complications andstroke were more common in patients with proximaloperations; cardiac and pulmonary complications andaneurysmal rupture were more common in those withdistal operations.The most disappointing complication occurring after
operation was neurologic problems ofthe lower extrem-ities, which were graded as paraparesis (weakness) orparaplegia (paralysis). These problems occurred eitherimmediately or after periods of 12 hours to 3 weeks, andwere not prevented by the numerous measures men-
DISTAL DISSECTIONTHIRTY-DAY MORTALITY
30-Day Mortality (%)
ACUTE DISSECTIONTHIRTY-DAY MORTALITY
- 56-79
317 Patients Total
1980 1981 1982 1983 1984 1985 1986 1987'
Year of Surgery * Includes Jan. Feb. 1988
FIG. 14. Graph showing distribution of all cases of distal aortic dissec-tion and diminishing mortality from operation during past 4 years.
133 Patients Total Year of Surgery * Includes Jan. Feb. 1988
FIG. 16. Graph showing distribution of all cases of acute aortic dissec-tion and diminishing mortality during the past 2 years.
268
Number of Patients
Number of Patients75 80
67
53 160so
4236 40
3127% 28%.. 27 28
21% , 23%25 &wo
is is 2011% 10%N
3%6%
.,,,O%--L-0 ---- ----- ---- ---- ---- 0
AORTIC DISSECTION
Number of Patients
CHRONIC DISSECTIONTHIRTY-DAY MORTALITY
75. 75 80
.57 5
50~~~~~~~~~~3 6
37 ~~~~~~40
25 20%11% 19 i~12
7% ----L
0~~~~~~~~~~~~~~
30-Day Mortality (%)
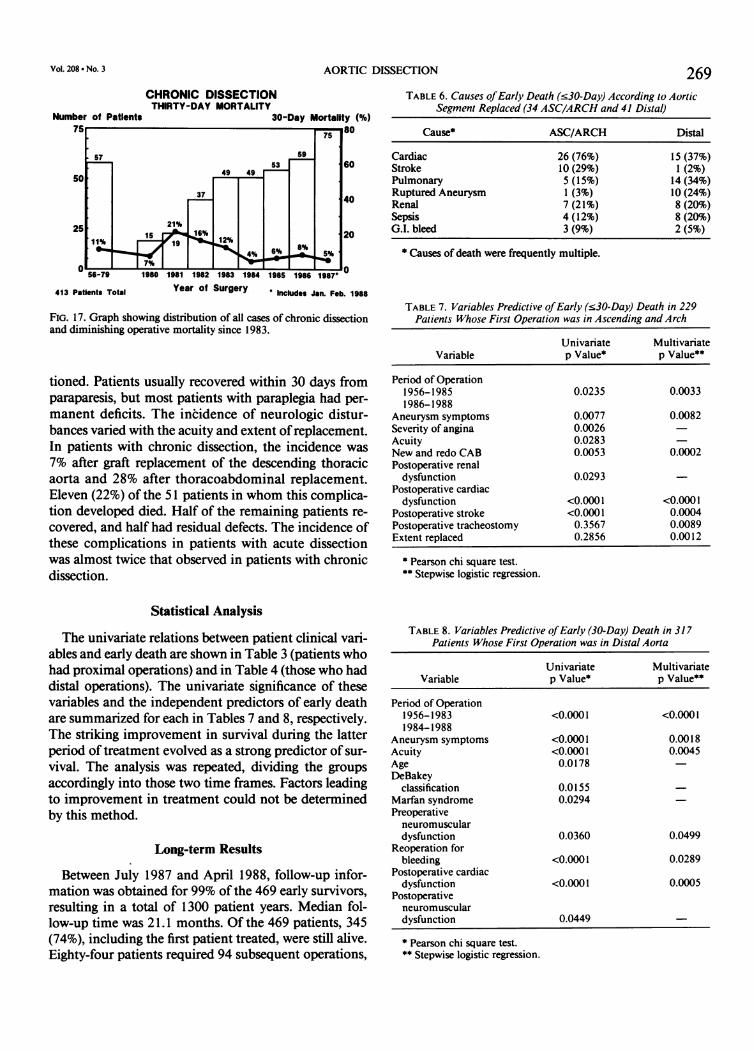
269TABLE 6. Causes ofEarly Death (.30-Day) According to Aortic
Segment Replaced (34 ASC/ARCH and 41 Distal)
Cause* ASC/ARCH Distal
Cardiac 26 (76%) 15 (37%)Stroke 10 (29%) 1 (2%)Pulmonary 5 (15%) 14 (34%)Ruptured Aneurysm 1 (3%) 10 (24%)Renal 7 (21%) 8 (20%)Sepsis 4 (12%) 8 (20%)G.I. bleed 3 (9%) 2 (5%)
* Causes of death were frequently multiple.
56-79 1980 1981 1982 1983 1984 1985 1986 1987
413 Patients Total Year of Surgery Includes Jan. Feb. 1988
FIG. 17. Graph showing distribution of all cases of chronic dissectionand diminishing operative mortality since 1983.
tioned. Patients usually recovered within 30 days fromparaparesis, but most patients with paraplegia had per-
manent deficits. The incidence of neurologic distur-bances varied with the acuity and extent ofreplacement.In patients with chronic dissection, the incidence was
7% after graft replacement of the descending thoracicaorta and 28% after thoracoabdominal replacement.Eleven (22%) of the 51 patients in whom this complica-tion developed died. Half of the remaining patients re-
covered, and half had residual defects. The incidence ofthese complications in patients with acute dissectionwas almost twice that observed in patients with chronicdissection.
TABLE 7. Variables Predictive ofEarly (.30-Day) Death in 229Patients Whose First Operation was in Ascending and Arch
Univariate MultivariateVariable p Value* p Value**
Period of Operation1956-1985 0.0235 0.00331986-1988
Aneurysm symptoms 0.0077 0.0082Severity of angina 0.0026Acuity 0.0283New and redo CAB 0.0053 0.0002Postoperative renal
dysfunction 0.0293Postoperative cardiac
dysfunction <0.0001 <0.0001Postoperative stroke <0.0001 0.0004Postoperative tracheostomy 0.3567 0.0089Extent replaced 0.2856 0.0012
* Pearson chi square test.** Stepwise logistic regression.
Statistical Analysis
The univariate relations between patient clinical vari-ables and early death are shown in Table 3 (patients whohad proximal operations) and in Table 4 (those who haddistal operations). The univariate significance of thesevariables and the independent predictors of early deathare summarized for each in Tables 7 and 8, respectively.The striking improvement in survival during the latterperiod of treatment evolved as a strong predictor of sur-
vival. The analysis was repeated, dividing the groups
accordingly into those two time frames. Factors leadingto improvement in treatment could not be determinedby this method.
Long-term Results
Between July 1987 and April 1988, follow-up infor-mation was obtained for 99% of the 469 early survivors,resulting in a total of 1300 patient years. Median fol-low-up time was 21.1 months. Of the 469 patients, 345(74%), including the first patient treated, were still alive.Eighty-four patients required 94 subsequent operations,
TABLE 8. Variables Predictive ofEarly (30-Day) Death in 317Patients Whose First Operation was in Distal Aorta
Univariate MultivariateVariable p Value* p Value*5
Period of Operation1956-1983 <0.0001 <0.00011984-1988
Aneurysm symptoms <0.0001 0.0018Acuity <0.0001 0.0045Age 0.0178DeBakey
classification 0.0155Marfan syndrome 0.0294Preoperativeneuromusculardysfunction 0.0360 0.0499
Reoperation forbleeding <0.0001 0.0289
Postoperative cardiacdysfunction <0.0001 0.0005
Postoperativeneuromusculardysfunction 0.0449
* Pearson chi square test.** Stepwise logistic regression.
Vol.208 -No. 3
270 CRAWFORD AND OTHERS
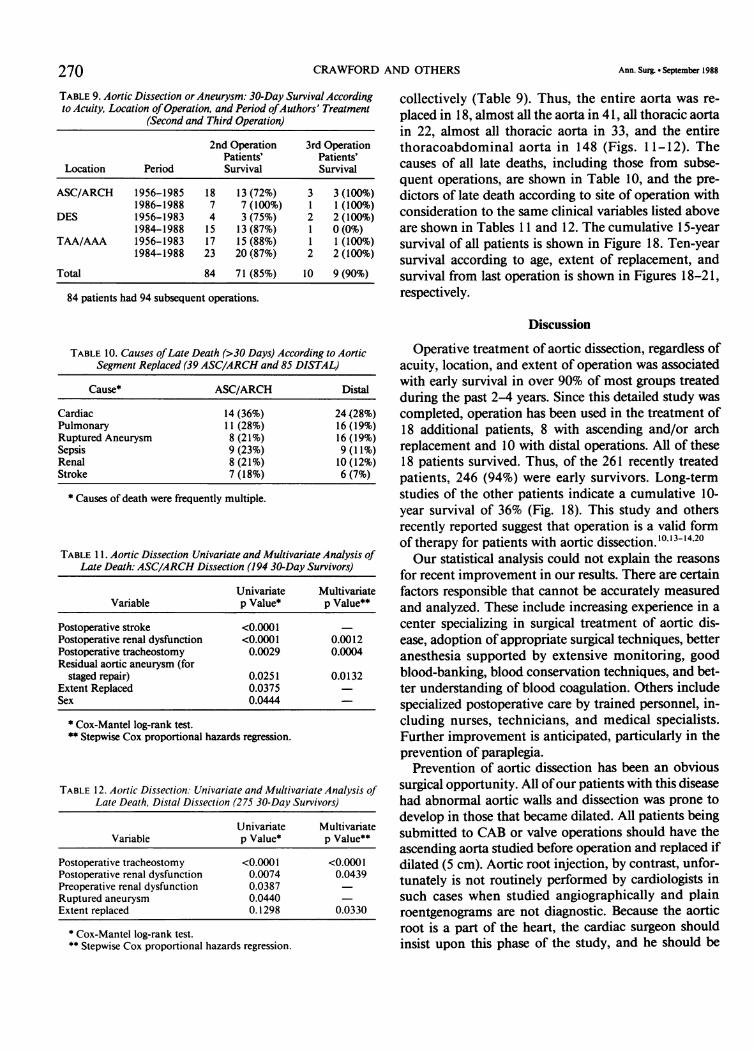
TABLE 9. Aortic Dissection or Aneurysm: 30-Day Survival Accordingto Acuity, Location ofOperation, and Period ofAuthors' Treatment
(Second and Third Operation)
2nd Operation 3rd OperationPatients' Patients'
Location Period Survival Survival
ASC/ARCH 1956-1985 18 13 (72%) 3 3 (100%)1986-1988 7 7 (100%) 1 1 (100%)
DES 1956-1983 4 3 (75%) 2 2 (100%)1984-1988 15 13 (87%) 1 0 (0%)
TAA/AAA 1956-1983 17 15 (88%) 1 1 (100%)1984-1988 23 20 (87%) 2 2 (100%)
Total 84 71 (85%) 10 9 (90%)
84 patients had 94 subsequent operations.
TABLE 10. Causes ofLate Death (>30 Days) According to AorticSegment Replaced (39 ASC/ARCH and 85 DISTAL)
Cause* ASC/ARCH Distal
Cardiac 14 (36%) 24(28%)Pulmonary 11 (28%) 16 (19%)Ruptured Aneurysm 8 (21%) 16 (19%)Sepsis 9 (23%) 9 (11%)Renal 8 (21%) 10 (12%)Stroke 7 (18%) 6 (7%)
* Causes of death were frequently multiple.
TABLE 1 1. Aortic Dissection Univariate and Multivariate Analysis ofLate Death: ASC/ARCH Dissection (194 30-Day Survivors)
Univariate MultivariateVariable p Value* p Value**
Postoperative stroke <0.0001Postoperative renal dysfunction <0.0001 0.0012Postoperative tracheostomy 0.0029 0.0004Residual aortic aneurysm (for
staged repair) 0.0251 0.0132Extent Replaced 0.0375Sex 0.0444
* Cox-Mantel log-rank test.** Stepwise Cox proportional hazards regression.
TABLE 12. Aortic Dissection: Univariate and Multivariate Analysis ofLate Death, Distal Dissection (275 30-Day Survivors)
Univariate MultivariateVariable p Value* p Value**
Postoperative tracheostomy <0.0001 <0.0001Postoperative renal dysfunction 0.0074 0.0439Preoperative renal dysfunction 0.0387Ruptured aneurysm 0.0440Extent replaced 0.1298 0.0330
* Cox-Mantel log-rank test.** Stepwise Cox proportional hazards regression.
Ann. Surg * September 1988
collectively (Table 9). Thus, the entire aorta was re-placed in 18, almost all the aorta in 41, all thoracic aortain 22, almost all thoracic aorta in 33, and the entirethoracoabdominal aorta in 148 (Figs. 1 1-12). Thecauses of all late deaths, including those from subse-quent operations, are shown in Table 10, and the pre-dictors of late death according to site of operation withconsideration to the same clinical variables listed aboveare shown in Tables 11 and 12. The cumulative 15-yearsurvival of all patients is shown in Figure 18. Ten-yearsurvival according to age, extent of replacement, andsurvival from last operation is shown in Figures 18-21,respectively.
Discussion
Operative treatment of aortic dissection, regardless ofacuity, location, and extent of operation was associatedwith early survival in over 90% of most groups treatedduring the past 2-4 years. Since this detailed study wascompleted, operation has been used in the treatment of18 additional patients, 8 with ascending and/or archreplacement and 10 with distal operations. All of these18 patients survived. Thus, of the 261 recently treatedpatients, 246 (94%) were early survivors. Long-termstudies of the other patients indicate a cumulative 10-year survival of 36% (Fig. 18). This study and othersrecently reported suggest that operation is a valid formof therapy for patients with aortic dissection. 10,13-14.20Our statistical analysis could not explain the reasons
for recent improvement in our results. There are certainfactors responsible that cannot be accurately measuredand analyzed. These include increasing experience in acenter specializing in surgical treatment of aortic dis-ease, adoption of appropriate surgical techniques, betteranesthesia supported by extensive monitoring, goodblood-banking, blood conservation techniques, and bet-ter understanding of blood coagulation. Others includespecialized postoperative care by trained personnel, in-cluding nurses, technicians, and medical specialists.Further improvement is anticipated, particularly in theprevention of paraplegia.Prevention of aortic dissection has been an obvious
surgical opportunity. All ofour patients with this diseasehad abnormal aortic walls and dissection was prone todevelop in those that became dilated. All patients beingsubmitted to CAB or valve operations should have theascending aorta studied before operation and replaced ifdilated (5 cm). Aortic root injection, by contrast, unfor-tunately is not routinely performed by cardiologists insuch cases when studied angiographically and plainroentgenograms are not diagnostic. Because the aorticroot is a part of the heart, the cardiac surgeon shouldinsist upon this phase of the study, and he should be

Vol. 208 - No.3 AORTIC DISSECTION 271
AORTIC DISSECTION AND ANEURYSMAll Patients
15 Year SurvivalT: Total Patients (N=546); S: 30-Day Survivors (N=469)
10
>o-_ SS+~~654%76)ae60.72w
Total -
20 Survivors
o l I I I I I I I I I I I -1 I I
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years After Surgery
FIG. 18. Fifteen-year survival of all patients and all survivors of firstoperation.
AORTIC DISSECTION AND ANEURYSMAll 30-Day Survivors
10-Year Survival According to Age1: 13-49 (N=144); 2: 50-64 (N=190); 3: 65-87 (N=135)
100123%(55)
>'x123w'9N p=0.007080 13 (;6_ _' 7417%(20
7914%(79) %%
60- . 8..(
44t113%(40* Age0 -- 13-49 ...........
20 -50-64 32125%16..... 65-87
0 1 2 3 4 5 6 7 8 9 10
Years After Surgery
FIG. 19. Ten-year survival of first operation survivors, according toage.
AORTIC DISSECTION AND ANEURYSMAll 30-Day Survivors
10-Year Survival According to Extent GroupA: Asc/Arch (N=194); D: Distal (N=275)
10080%(123) p=0.1499
55*2%(151)56718%(23)60 G4O5W(54)40 - Group
Ascending/Arch 2120 Distal
C * I I I0 1 2 3 4 5 6 7 8 9 10
Years In Surgery
FIG. 20. Ten-year survival of first operation survivors, according toextent of resection.
AORTIC DISSECTION AND ANEURYSMAll Patients
10-Year Survival from Date of Last Aortic OperationT: Total Patients (N=546); S: 30-Day Survivors (N=439)
10060;- 7272%(284)
80!557) <644112%(7)40 -
CS (-,'>40 Group ------
cn -- Total 3N111%(7)20 Survivors
o0 I I
0 1 2 3 4 5 6 7 8 9 10
Years After Surgery
FIG. 21. Ten-year survival from date of last aortic operation of allpatients and those who survived for 30 days.
aware that aortic replacement in such patients does notadd significant risk to the heart operation. Moreover,dissection also occurs more frequently in dilated distalaortas, and operation should be considered when distaldilatation exceeds twice the proximal uninvolved aorta.
AcknowledgementsGrateful acknowledgment is given to Barbara Brooks for continuous
follow-up and recording of all the data on computer, Carol Pienta forproduction ofillustrations, and Harriet Schubb for editorial assistance.
References1. Anagnostopoulos CE, Prabhakar MJS, Kittle CF. Aortic dissec-
tions and dissecting aneurysms. Am J Cardiol 1972; 30:263-273.
2. Bickerstaff LK, Pairolero PC, Hollier LH, et al. Thoracic aorticaneurysms: a population-based study. Surgery 1982; 92:1103-1108.
3. Crawford ES, DeNatale RW. Thoracoabdominal aortic aneurysm:Observations regarding the natural course ofthe disease. J VascSurg 1986; 3:578-582.
4. DeBakey ME, Cooley DA, Creech 0, Jr. Surgical considerations ofdissecting aneurysm ofthe aorta. Ann Surg 1955; 142:586-612.
5. Bahnson HT, Spencer FC. Excision ofaneurysm of the ascendingaorta with prosthetic replacement during cardiopulmonary by-pass. Ann Surg 1960; 151:879-890.
6. Crawford ES. Thoraco-abdominal and abdominal aortic aneu-rysm involving renal, superior mesenteric, and celiac arteries.Ann Surg 1974; 179:763-772.
7. Crawford ES, Crawford JL, Stowe CL, Safi HJ. Total aortic re-placement for chronic aortic dissection occurring in patientswith and without Marfan's syndrome. Ann Surg 1984;199:358-362.
8. Crawford ES, Stowe CL, Crawford JL, et al. Aortic arch aneurysm:

272 CRAWFORD AND OTHERS Ann. Surg. * September 1988
a sentinel of extensive aortic disease requiring subtotal andtotal aortic replacement. Ann Surg 1984; 199:742-752.
9. Crawford ES, Walker HSJ III, Saleh SA, Normann NA. Graftreplacement aneurysm descending thoracic aorta: results with-out bypass or shunting. Surgery 1981; 89:73-85.
10. DeBakey ME, McCollum CH, Crawford ES, et al. Dissection anddissecting aneurysms ofthe aorta: twenty-year follow-up of fivehundred twenty-seven patients treated surgically. Surgery 1982;92:1118-1134.
11. Cabrol C, Pavie A, Mesnildrey P, et al. Long-term results withtotal replacement of the ascending aorta and reimplantation ofthe coronary arteries. J Thorac Cardiovasc Surg 1986; 91:17-25.
12. Griepp RB, Stinson EB, Hollingsworth JF, et al. Prosthetic re-placement of the aortic arch. J Thorac Cardiovasc Surg 1975;70:1051-1063.
13. Miller DC, Mitchell RS, Oyer PE, et al. Independent determinantsof operative mortality for patients with aortic dissections. Cir-culation 1984; 70:1/153-164.
14. Haverich A, Miller DC, Scott WC, et al. Acute and chronic aorticdissections: determinants of long-term outcome for operativesurvivors. Circulation 1985; 72:11/22-34.
15. Crawford ES, Coselli JS, Safi HJ. Partial cardiopulmonary bypass,hypothermic circulatory arrest, and posterolateral exposure forthoracic aortic aneurysm operation. J Thorac Cardiovasc Surg1987; 94:824-827.
16. Crawford ES, Coselli JS, Safi HJ. Treatment dissection of ascend-ing aorta and aortic arch based upon a study ofpatients requir-ing reoperation. Contemp Surg 1986; 29:13-31.
17. Crawford ES, Crawford JL, Safi HJ, Coselli JS. Redo operationsfor recurrent aneurysmal disease of the ascending aorta andtransverse aortic arch. Ann Thorac Surg 1985; 40:439-455.
18. Cooley DA, Livesay JJ. Technique of "open" distal anastomosisfor ascending and transverse arch resection. Cardiovasc Dis1981; 8:421-426.
19. Crawford ES, Mizrahi EM, Hess KR, et al. The impact of distalaortic perfusion and somatosensory evoked potential monitor-ing on prevention of paraplegia after aortic aneurysm opera-tion. J Thorac Cardiovasc Surg 1988; 95:357-367.
20. Kouchoukos NT, Marshall WG, Jr, Wedige-Stecher TA. Eleven-year experience with composite graft replacement ofascendingaorta and aortic valve. J Thorac Cardiovasc Surg 1986;92:691-705.
DISCUSSION
DR. MICHAEL E. DEBAKEY (Houston, Texas): I am sure that youappreciate the fact that I take great pride in Stanley's presentation-greater pride than anyone else. His perseverance, his dedication, andhis creative abilities have resulted in great improvement in the treat-ment of this highly fatal disease.
This disease is highly fatal ifnot treated, and even with good medicalmeasures, which consist essentially in maintaining the blood pressureat the lowest level possible, it still has an extremely poor prognosis.Therefore, the ability to achieve a 30 or 40% survival rate of 10 or 15years means that these patients not only live longer but most ofthemlead a reasonably normal life.
I would like to emphasize a few points that Stanley made about thelong-term effects.
(Slide) This patient is still alive 24 years after treatment; in fact Italked with him yesterday. I heard from him about I year ago and hada report from his physician. He has had some cardiac problems,namely coronary disease, but he still is able to work in his garden andenjoy life reasonably well, nearly 25 years since his operation.
(Slide) This slide exemplifies one ofthe reasons for early failure thatwe did not recognize, that is, ifthere is any question about aortic valveincompetence and the inability to preserve that valve satisfactorily byrepair, it is best to put in a valve. We did not place a valve in thispatient, and you see 6 years later he required valve replacement. He isstill living today, nearly 20 years after the original operation.
(Slide) This slide exemplifies one of the cases that Dr. Crawfordshowed, a patient who had been operated on elsewhere, but in whomall the dissected part ofthe aneurysm had not been removed. To someextent this is the result ofconcern about the coronary arteries, the ostiaof the coronary arteries. Six years later an extensive aneurysm haddeveloped involving the proximal portion that was not resected at thetime it should have been even though valve replacement was done.Therefore, a second operation had to be performed, and 7 years afterthat operation, the patient is doing well.
(Slide) This slide exemplifies another point that Dr. Crawford made,that is, the condition will progress ifone is not careful and may result inrupture of a distal aneurysm. It is therefore important that these pa-tients be observed carefully and closely because one of the results ofanalysis of our experience is the fact that next to cardiac reasons, thehighest incidence of late deaths was rupture of a distal aneurysm thathad not been taken care ofearlier. The original operation for a Type IIIdissection was limited to the descending thoracic aorta. Six years later,however, a large aneurysm of the entire abdominal aorta developed,and a second operation of resection and graft replacement with at-tachment to the previous graft was performed; the aortogram showsgood function 1 I years later and 17 years after the original operation.
This is also an example of Type III dissection with extension belowthe diaphragm in a 46-year-old woman. After resection ofthe dissectedsegment arising just below the origin of the left subclavian artery, aDacron graft was attached proximally and then distally to the normallumen after the false lumen was obliterated by suture closure withTeflon baffles of the inner and outer layers. The postoperative aorto-gram shows good function with no evidence of aneurysmal formationdistally 23 years later.
(Slide) This last slide illustrates that if one can remove the entireaneurysm, as was done in this patient, the prognosis is good. Thispatient was operated on 28 years ago. He was 14 years old then and hada Type III dissection. You can see the technique that was used then totry to avoid ischemic changes. Fortunately, he did not have any, and heis leading a normal life now 28 years after his operation; therefore, in acertain proportion of patients, long-term survival is possible. Indeed,in an analysis of 527 cases reported several years ago, there was anoverall survival rate of 57% for 5 years, 32% for 10 years, and 5% for 20years. With the technical advances and indications that Dr. Crawfordhas provided, we can expect not only the mortality rate to be lower, butthe number of long-term survivors to improve.
DR. FRANK C. SPENCER (New York, New York): I rise primarily tocompliment Drs. Crawford and DeBakey on their spectacular accom-plishments with aortic aneurysms over the last 20 years. It is a particu-lar credit to Dr. DeBakey, for Dr. Crawford was one of his early facultyappointments, coming to Houston after finishing his residency at theMassachusetts General Hospital in Boston. Over the past several years,especially in the past 10 years, Dr. Crawford's publications have be-come the landmark references for complex aortic aneurysms. Withthoracoabdominal aneurysms, his concepts have been particularlyfundamental, lowering operative mortality rates from a range of30-40% to 10-15%.
Just this past week in New York we admitted a patient on my servicewith a dissecting aneurysm with the Marfan syndrome. She had pre-viously been operated on under emergency circumstances with a com-plex conduit reconstruction of the aortic root. After reviewing theaortogram (and Dr. Crawford is not acquainted with the patient yet),which shows a dissection extending down to the bifurcation of theabdominal aorta, and considering the possibilities, I said, "This is avery nice case for Dr. Crawford. I will be talking to him in San Fran-cisco!"
In comparing our limited experiences with the extensive ones pre-sented by Dr. Crawford, two questions arise. In the past 2 years over 40patients have been operated on at New York University with ascendinganeurysms involving the arch, 22 ofwhom had acute dissections. Themortality rate was about 15% in both groups, a total of six deaths. This
Related Documents











