Antiseptic solution in Operating theatre Patricia Kan

Antiseptic solution in Operating theatre Patricia Kan.
Mar 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Antiseptic solution in Operating theatre
Patricia Kan

Antiseptic solutions in operating theatre
Joseph Lister (1827-1912)• Hospitalism: outcomes
of pyaemia, septicaemia, erysipelas, hospital gangrene and tetanus
• One of the giants of infection control
• Laid down the principles of antisepsis in surgery
• In late 1800s, he started to use carbolic acid to clean the operation site before incision.

Topical antiseptic solution in OT
• 1. Preoperative skin preparation
• 2. Regional anaesthesia (epidural, spinal, etc)
• 3. Central line insertion
• 4. Hand hygiene

• Topical antiseptic are antimicrobial agents that kill, inhibit or reduce the no. of microorganisms on the skin.
• Human skin is colonized by a wide variety of microorganisms that may provide a protective mechanism to the host, but also a source of infection.

Normal skin flora
– Transient: • contracted from the environment or from other pe
ople• thrive in the environment of sweat, dirt and oil• can be easily removed by soap and water.
– Resident: • live in the skin pores and stratum corneum• continually work towards the skin surface• Difficult to remove and require antimicrobial agent
s with residual action to be effective
• Topical antiseptic are active against both resident and transient flora by both mechanical and chemical action.
• Apply enough pressure and friction to remove dirt, debris and microbes. (except superficial malignancy, areas of carotid plaque)
• Common antiseptics: Alcohol, Iodine and iodophors, Chlorhexidine
Alcohol
• Protein coagulation and denaturation• Alcohol-mediated disruption of cytoplas
mic integrity, cell lysis and interference with cellular metabolism
• 100% alcohol is not effective– it deprives bacterial cell walls of water– induce the formation of impermeable protei
n layers which prevent the alcohol from penetrating in to the cell
• Alcohol is defined by FDA as having one of the following active ingredients:– Ethyl alcohol, 60-95% by volume in aqueou
s solution– Isopropyl alcohol, 50-91.3% by volume in a
queous solution
• Most common concentration: 70%– Effective, less dessicating, less expensive

Advantages
• Onset of action is most rapid, 10-15 sec• Broad antimicrobial spectrum:
– Excellent bactericidal effect on G+, G- – Effective against tubercle bacillus, fungi and virus
(certain enveloped viruses: HSV, HIV, influenza virus, RSV)
– Not sporicidal, poor activity against certain nonenveloped viruses (e.g. poliovirus, enterovirus, HAV, rotavirus)
• Alcohol antiseptic has been used since 1930s and there have been no reports of alcohol resistant bacterial strains
Disadvantages• No residual activity• Effectiveness is reduced by organic materials
such as blood, mucus, excreta• Volatility and Flammability﹡• Drying of skin, allergic contact dermatitis
– Emollients, may enhance the antimicrobial activity• Toxic reactions have been reported in
children after sponge bathing with isopropyl alcohol to reduce fever (1950-60s). The vapors may be absorbed through the lungs and cause acute poisoning.

Iodine and iodophors

Iodine and iodophors• Tincture of iodine was used as early as 1839 by
French war surgeon who treated battle wound during the Civil War
• Action:– Iodine molecules rapidly penetrate the cell wall of
microorganisms– inactivate cell s by forming complex with amino acid and
unsaturated fatty acids – Impaired protein synthesis, alteration of cell membrane
• Most effective concentration is 1-2%• Cause stinging and irritation, discoloration• Must be removed with 70% alcohol after drying

• Iodophors: solutions in which iodine is chemically bound to polymer carrier (complexing agents of high molecular weight) e.g. polyvinylpyrrolidone– Povidone-iodine = Betadine
• Water soluble, less staining, less irritating to skin, eye and mucous membrane
• Allows slow and continuous release of free iodine which determines the antimicrobial activity
• 10% povidone-iodine contains 1% iodine
• Onset: – iodophors require ~2 min of contact time to a
llow release of free iodine– after dried
• Broad spectrum of bactericidal activity– Effective against G+, G-, tubercle bacillus , f
ungi, virus and certain spore forming bacteria (e.g. clostridia, Bacillus spp.)
– Not sporicidal in concentration used in antiseptic

• Rapidly neutralized in the presence of organic materials such as blood, mucus, sputum, urine, faeces, etc
• Antimicrobial activity is affected by – pH (~6)– temperature (esp sporicidal activity is markedly temper
ature-dependent, ↑temp → ↑activity)– exposure time, conc of total available iodine, etc
• Greater activity when the cpd is in dry state• Some residual effect
– If washed away, 30-60 min (except 1 study: 6 hrs)– Bacteriostatic effect as long as on the skin

To dry or not to dry???• Wipe the skin dry after apply the antiseptic agent to all
ow adherence of disposable adhesive drapes• Kutarski, Grundy. To dry or not to dry? An assessment
of the possible degradation in efficiency of preoperative skin preparation caused by wiping skin dry. Annuals of the Royal College of Surgeons of England (1993) vol 75, 181-185.– Skin flora were obtained from subjects at 5, 30, 60 and 120 m
in– No significant difference in the reduction of baseline count of
skin flora between wiping the agent off after 30 sec of application and leaving it to dry
– Author suggested a longer period of application time may be worthwhile , particularly where infection would prove disastrous, e.g. implanting prostheses

Povidone-iodine related chemical burns
• 24/F, R hand flexor tendon repair (2hrs)– Preparation ran down the patient’s arm and
absorbed by the padding under the tourniquet cuff

• 45 yrs old, epidural anaesthesia for femoro-popliteal bypass graft, gauze soaked in povidone-iodine antiseptic solution and was then covered with occlusive transparent waterproof dressing
blistered area in the shape
of the gauze at the back
• PI after closed and prolonged exposure can damage the skin– over bony prominence, pressure points, underneath
an area constricted with a tourniquet dressing or bandage
• Recommendations:– Skin must not be abraded excessively before the
final skin preparation solution is applied– The agent should not be allowed to pool and
become trapped under the tourniquet or the torso of the patient
– The agent should be allowed to dry before the patient is draped.
Transcutaneous iodine absorption
• Topical application of PI in burn patients – renal failure, metabolic acidosis, hypernatraemia, hyperosmolari
ty, hypothyroidism
• Hypothyroidism in infants– Skin is very thin and permeable– High plasma iodine conc transient inhibition of thyroid hormo
ne production, ↓serum thyroxine level (Wolff-Chaikoff effect)– Usu lasts only 48hrs, even if the plasma iodine level remain high – Prolonged hypothyroidism esp in preterm infants– Recommendations:
• Avoid iodine containing antiseptic in infants<3mths old• Iodine should be washed off with sterile saline solution

Chlorhexidine gluconate
CHG 0.05% aqueous
CHG 0.05% aqueous (25ml)
CHG 0.015% + cetrimide 0.15%
Chlorhexidine gluconate (CHG/ Hibitane)
• Cationic bisbiguanide • Action:
– attachment, disruption of cytoplasmic membranes– precipitation of cellular contents
• Broad antimicrobial spectrum– Good activity against G+– Less activity against G-, fungi– Poor activity against tubercule bacilli– Not sporicidal– In vitro activity against enveloped virus (HSV, HIV, CMV, influenz
a, RSV)– Less activity towards non-enveloped virus (rotavirus, adenovirus,
enterovirus)
• Introduced to Europe in 1950s and US in 1970s– Bacterial resistance not common, limited to some resist
ant strains of Pseudomonas, Proteus, Staphylococcus aureus
• Antimicrobial activity is not affected by the presence of organic material
• ∵cationic activity reduced by natural soaps, ino∴rganic anions, nonionic surfactants, hand cream containing anionic emulsifying agents
• pH dependent (5-8), if pH above 9 precipitation of active component
• Onset: 3-5 min• Good residual activity
– It binds to skin and mucous membrane and remain active for at least 6 hrs
• Not absorbed through skin , low irritancy potential
• Should not come into contact with eyes, meninges (neurotoxic), middle ear (ototoxicity)
Allergy/ Anaphylaxis to chlorhexidine
• Most of the case reports from Japanese literature
• Application to skin, mucous membrane, chlorhexidine-sulphadiazine-coated central venous catheter
• (In our ICU, the antibiotic-coated central venous catheter is minocycline/ rifampicin coated)

Summaryagent mechanis
m of action
G+ G- MTB Fungi
virus
Rapidity of action
Residual activity
Alcohol Denature
protein
+++ +++ ++ ++ ++ Rapid
10-15 s
none
CHG Disrupt cell membrane
+++ ++ - + ++ Intermediate
3-5 min
+++
Iodine/
iodophor
Oxidation/ substitution by free iodine
+++ ++ ++ ++ ++ Intermediate
2 min
some

Alcohol based antiseptic solution

Alcohol based antiseptic solution
• low concentration (0.5-1%) CHG is added to alcohol (70%)
• Combination of Alcohol and PI
• Advantages:– Rapid action of alcohol– Persistent action of CHG– Decrease the drying time

Operating theatre fire and alcohol based antiseptics
Case reports• Barker S, Polson J. Fire in the operating room: a case report and lab
oratory study. Anesth. Analg. 2001; 93: 960-5• Fong E, et al. Diathermay and alcohol skin preparations – potential d
isastrous mix. Burns 2000; 26: 673-5• Chang BW, et al. Patient fire safety in the operation room. Plast. Rec
onstr. Surg. 1994; 93: 519-21• Magruder G, et al. Fire prevention during surgery. Arch. Ophthalmol.
1970; 84: 237• Briscoe C, et al. Infammable antiseptics and theatre fires. Br. J. Surg.
1976; 63: 981-3• Nicholson M. Comments. Anesth. Analg 1972; 51: 646• Waitemata Distric Health Board. Report into operating theatre fire ac
cident, 17 Aug 2002. Witemata Distric Health Board Final Report. New Zealand; Waitemata Hospital, 2002.
• Toother R, et al. Surgical fires and alcohol-based skin preparations. ANZ J Surg.2001: 74: 382-385 ………………………………..
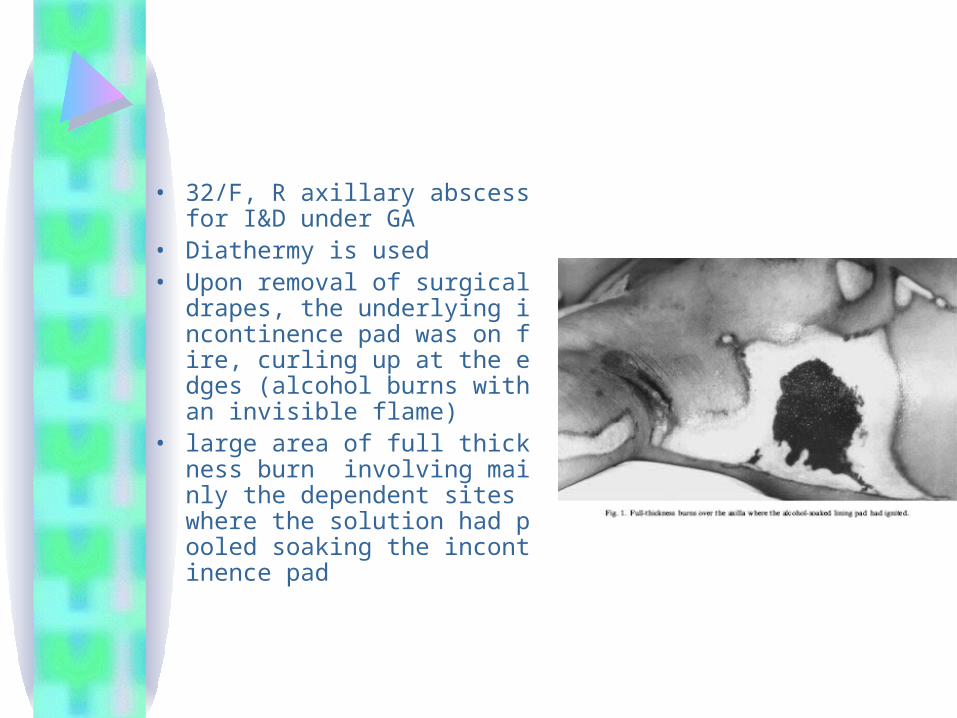
• 32/F, R axillary abscess for I&D under GA
• Diathermy is used• Upon removal of surgical dra
pes, the underlying incontinence pad was on fire, curling up at the edges (alcohol burns with an invisible flame)
• large area of full thickness burn involving mainly the dependent sites where the solution had pooled soaking the incontinence pad

• 17/F, LSCS under epidural anaesthesia• 0.5% CHG with 70% alcohol was used to prepare the abdomen• Diathermy was used• “woomph” noise was heard• Patient complained of heat and the anaesthetist felt the heat an
d saw a flame/shimmer• Fire was put out with fire and CS completed with birth of a healt
hy baby• The mother suffered 12-16% full thickness burns to her inner thi
ghs and both flanks • due to pooling of alcohol-based skin antiseptic underneath the a
dhesive surgical drapes which produced alcohol vapour which was ignited by a spark from diathermy
• No oxygen supplement is given
Recommendations• Alcohol-based solutions are not recommended for s
kin preparation in the presence of ignition source ( electrocautery unit, laser)
• Any alcohol based solution should be clearly labelled• Run-off and pooling of alcohol based antiseptic should
be avoided by– Using minimum amount necessary– Allowing solution to dry completely prior to draping – Preparation that contains dye are recommended because they
make it easier to see what skin has been painted less likely to use excessive amt and pooling
– Temporary absorptive sheets around the surgical site while using alcohol based solution and removed after use

• The drying time for skin preparation might need to be longer than the manufacturer’s recommendation (usu 2-3 min), 5 min might be preferable
• Electrosurgical instruments should be used on the lowest power setting to minimize the risk of sparking and excessive temperatures
• Don’t put diathermy and laser foot pedals side by side• Don’t leave diathermy in the quiver each time after use• The creation of oxygen rich atmosphere should be avoid
ed – Not to create O2 tents by placing drapes over nasal cannula or
oxygen mask– In event of fire , oxygen and nitrous oxide supply should be ceas
ed immediately

Alcohol vs non-alcohol based antiseptics ??

1. Surgical site infection (SSI)
• An audit of pre-operative skin preparative methods practised by the surgeons in Northern Ireland in 2005
CDC guideline for prevention of surgical site infection, 1999
• Use an appropriate antiseptic agent for skin preparation. Category IB (Strongly recommended for implementation and supported by some experimental, clinical or epidemiological studies and strong theoretical rationale)
• ….The iodophors, alcohol-containing products and chlorhexidine gluconate are most commonly used agents….
• ….No studies have adequately assessed the comparative effects of these preoperative antiseptics on SSI risk in well-controlled, operation specific studies….

The Cochrane Database of Systematic Reviews Preoperative skin antiseptic for preventing surgical wound infections after clean surgery (2004)
• There is insufficient evidence from randomised trials to support or refute the use of antiseptic preparation of skin at operative sites, or of one antiseptic over another.
• Only one RCT (Berry 1982) demonstrated a significant difference in infection rates between two different antiseptics (in favour of CHG over iodine)

Berry A, et al. A comparison of the use of povidone-iodine and chlorhexidine in the prophylaxis. J. of Hospital infection 1982; 3 (1): 55-63.
• 371 clean operations• Results:
– Gp1. povidone-iodine 10% in alcohol• 28/176 , 15.9%
– Gp2. chlorhexidine 0.5% in spirit• 8/195, 4.1%
• Limitation: – Lack of extensive FU, underestimate the infection
rates
• Hibbard, et al. Analyses comparing the antimicrobial activity and safety of current antiseptic agents: A Review. J. of infusion nursing 2005, 28 (3): 194-207.– CHG+IPA provided the best immediate, persistent, cumu
lative antimicrobial activity• Ostrander, et al. Efficacy of surgical preparation solutions in
foot and ankle surgery. J. Bone joint Surg Am 87: 980-985, 2005.– ChloraPrep ( 2% chlorhexidine and 70% IPA) was most
effective for eliminating bacteria from the forefoot prior to surgery, when compared with DuraPrep (0.7% iodine + 74% IPA) or 3% chloroxylenol
• Bibbo C, et al. Chlorhexidine provided superior skin decontamination in foot and ankle surgery. Clinical orthopaedics and related research 438: 204-208, 2005.
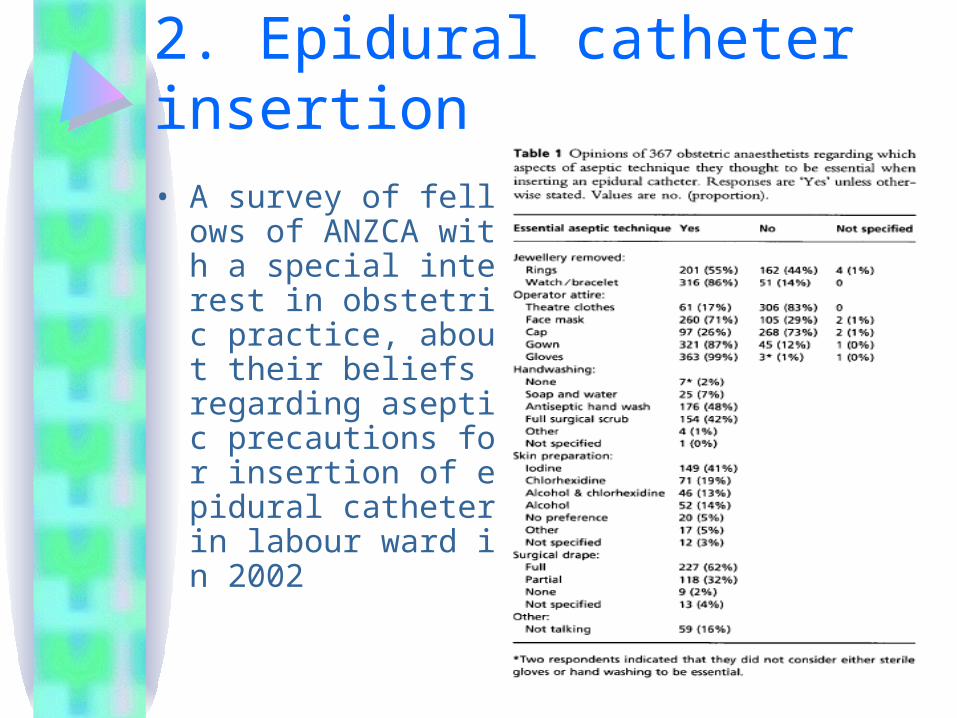
2. Epidural catheter insertion• A survey of fellows of
ANZCA with a special interest in obstetric practice, about their beliefs regarding aseptic precautions for insertion of epidural catheter in labour ward in 2002
• Mechanisms of epidural infection:– Skin flora introduced either at the time of puncture or b
acterial migration along a catheter or needle tract(soiling of the back by amniotic fluid, urine and feces during labour and delivery ↑catheter contamination)
– Contamination of drug or material– Haematogenous spread from another site of infection– Catheter colonization arising from clinicians’ and nurse
s’handling of syringes and solutions, via catheter hub

Clevenot D, et al. Critical review of the literature concerning the comparative use of two antiseptic soultions before intravascular or epidural catheterization. Ann Fr Anesth Reanium 2003 Nov; 22(9): 787-97
• Chlorhexidine in alcoholic solution seems more efficient than povidone iodine in aqueous solution in the clinical setting.
• The place of povidone iodine in alcoholic solution, whose performances on the healthy skin are similar to those of alcoholic chlorhexidine, is being in evaluation.

Birnbach, et al. Comparison of povidone iodine and DuraPrep (iodophor in IPA) for skin disinfection prior to epidural catheter insertion in parturients. Anesthesiology 2003; 98(1): 164-9.


• Explanation:– Alcohol provides rapid antisepsis– Long lasting effect:
• Duraprep, when placed on skin, produces a film of disinfectant
• This film resists being washed away by fluids and blood
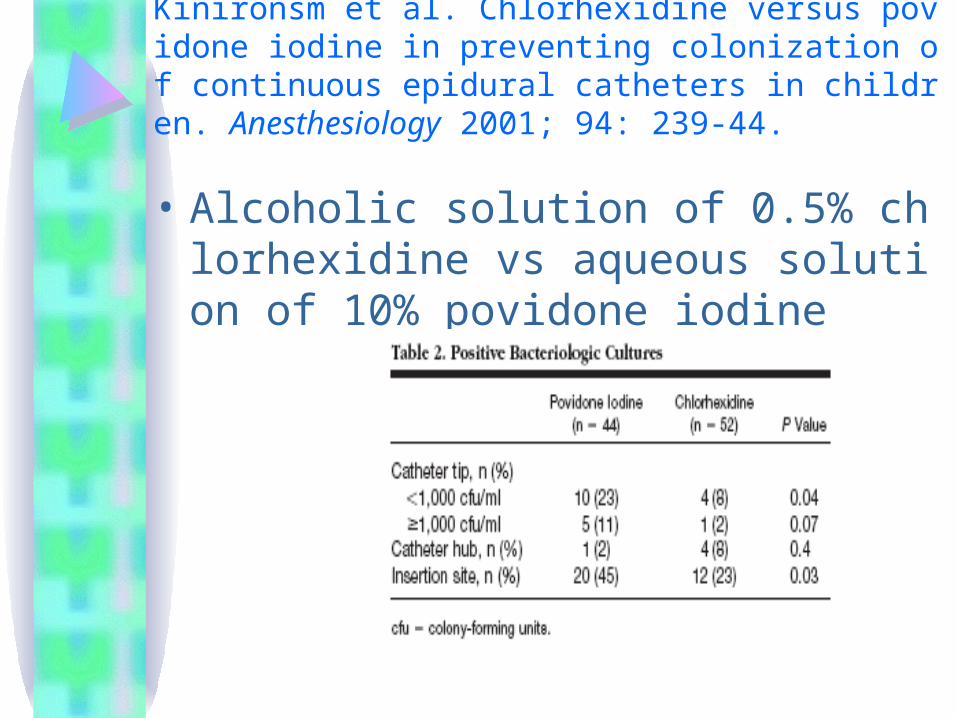
Kinironsm et al. Chlorhexidine versus povidone iodine in preventing colonization of continuous epidural catheters in children. Anesthesiology 2001; 94: 239-44.
• Alcoholic solution of 0.5% chlorhexidine vs aqueous solution of 10% povidone iodine

• Catheter inserted after skin preparation with chlorhexidine were one sixth as likely and less quickly colonized as catheters inserted after skin preparation with povidone iodine
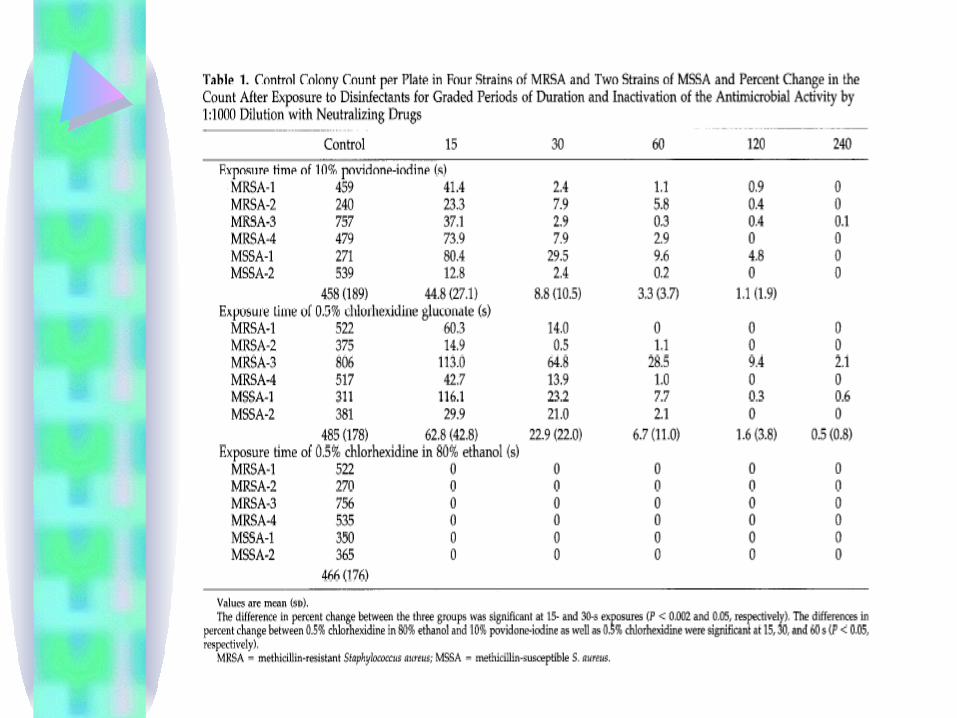
Sakuragi, et al. Bactericidal activity of skin disinfectants on MRSA. Anesth Analg 1995; 81: 555-8.
• Most frequently detected organism in the normal human skin flora is S. epidermidis (65-69%).
• The prevalence of S. aureus is 1-2% but is the most common organism in epidural abscess.
3. Central line insertion
• Two main routes by which intravascular devices become contaminated
• Intraluminal contamination:– consequence of improper handling of the catheter
hub at the time of connection and disconnection of the administration set
– Most common origin after the first week of catheter placement
– To prevent this, strict asepsis must be observed in hub and fluid handling

• Extraluminal contamination:– Bacterial invasion from the catheter entry si
te along the external surface of the catheter
– Bacteremia during the week following catheter placement
– Prevented by appropriate skin disinfection and the adoption of maximal antiseptic barriers at the time of catheter insertion

Chaiyakunapruk, et al. Chlorhexidine compared with povidone-iodone solution for vascular catheter-site care: A Meta-analysis. Ann Intern Med 2002; 136: 792-801.

• The overall risk ratio for catheter colonization in chlorhexidine group compared with povidone-iodine is 0.49
Chlorhexidine rather than povidone-iodine can reduce the risk for catheter-related bloodstream infection by approximately 50% in hospitalized patients who require short-term catheterization.
• Subset analyses of aqueous and nonaqueous solutions showed similar effect sizes, but only the subset analysis of the five studies that used alcoholic solution produced a statistically significant reduction in catheter-related bloodstream infection.
• Few studies used chlorhexidine aqueous solution

Parienti, et al. Alcholic povidone-iodine to prevent central venous catheter colonization: A randomized unit-crossover study. Crit care med 2004; 32(3): 708-713.

CDC guidelines for the prevention of intravscular catheter-related infections, 2002
• Disinfect clean skin with an appropriate antiseptic before catheter insertion and during dressing changes
• Although a 2% chlorhexidine based preparation is preferred, tincture of iodine, an iodophor, or 70% alcohol can be used.
• Allow the antiseptic to remain on the insertion site and to air dry before catheter insertion
• Allow povidone iodine to remain on the skin for at least 2 min or longer if it is not yet dry before insertion
• Do not apply organic solvents (e.g. acetone and ether) to the skin before insertion of catheter or during dressing changes
NICE (National Institute for Clinical Excellence) guideline for infection control, 2003
• Catheter site care:– An alcoholic chlorhexidine gluconate soluti
on should be used to clean the catheter site during dressing changes, and allowed to air dry.
– An aqueous solution of chlorhexidine gluconate should be used if the manufacturer’s recommendation prohibit the use of alcohol with the product.

Conclusion
• Skin antisepsis plays an important role in infection control and prevention of nosocomial infection (e.g. surgical site infection, epidural infection, catheter related infection, etc)
• An understanding of the properties of different antiseptic solutions is needed to facilitate the selection and proper use of them.

• It should be remembered that antiseptic solution is only a small part of infection control.
• Aseptic techniques such as cap, gowning, glove, mask, proper scrubbing, etc are also very important.

Best antiseptic solution???

My opinion• Ideal antiseptic solution does not exist• The current evidence seems to favour the
alcohol based antiseptic solution (esp alcoholic chlorhexidine)
• If alcohol based solution is avoided in view of OT fire, povidone-iodine is an alternative.
• The effect of aqueous chlorhexidine is unsure as most of the studies involve alcoholic chlorhexidine.

The End
Thanks
Related Documents











