Page 1 of 19 Antipsychotic Treatment for Borderline Personality Disorder: Are We Bordering the Line of Appropriate? Daniel Taylor, PharmD PGY2 Psychiatric Pharmacy Resident Central Texas Veterans Health Care System September 27, 2019 Learning Objectives: 1. Describe the pathophysiology of borderline personality disorder (BPD) 2. Identify current guideline recommendations for pharmacologic treatment of BPD 3. Explain the theoretical mechanism(s) of action for antipsychotic treatment in BPD 4. Assess the efficacy and safety of antipsychotic use for patients with BPD

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Page 1 of 19
Antipsychotic Treatment for Borderline Personality Disorder: Are We Bordering the
Line of Appropriate?
Daniel Taylor, PharmD
PGY2 Psychiatric Pharmacy Resident Central Texas Veterans Health Care System
September 27, 2019
Learning Objectives: 1. Describe the pathophysiology of borderline personality disorder (BPD) 2. Identify current guideline recommendations for pharmacologic treatment of BPD 3. Explain the theoretical mechanism(s) of action for antipsychotic treatment in BPD 4. Assess the efficacy and safety of antipsychotic use for patients with BPD

Page 2 of 19
Epidemiology: • Prevalence of BPD1-4
o Lifetime prevalence: 5.9% o Primary Care: 6% o Outpatient mental health clinics: 10% o Psychiatric inpatients: 15-28% o Female vs Male
▪ ~3:1 in clinical settings • Risk Factors for BPD5-9
o Environmental ▪ Childhood trauma/abuse – physical, sexual, emotional
o Genetic ▪ Increased risk noted in twin studies. ▪ Heritability of ~67% ▪ No specific causative gene identified. ▪ Epigenetic changes – DNA methylation abnormalities associated
with BPD. Pathophysiology:
• Structural Changes in the Brain10-11 – decreased brain volume o Amygdala – fear, emotional processing o Anterior Cingulate Cortex – emotion, impulse control, empathy o Hippocampus – learning and memory o Prefrontal Cortex – motivation, executive function
• Neurotransmitter effects in BPD12-13 o Serotonin – impulsive behavior & aggression regulation o Dopamine – emotion information processing, impulse control, cognition
▪ Proposed mechanism for antipsychotics in BPD is regulation of dopamine dysfunction.
o Acetylcholine – mood regulation o Norepinephrine – arousal, aggression, affective instability o Gamma-Aminobutyric Acid (GABA) – mood regulation
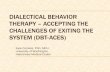
Co-morbid psychiatric disorders1,14
Figure 1: Commonly Co-Occurring Psychiatric Disorders

Page 3 of 19
Table 1: Diagnostic Criteria for BPD
DSM-IV-TR & DSM-V Criteria for Diagnosis of BPD15-16
A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked
impulsivity beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) of the following:
• Frantic efforts to avoid real or imagined abandonment. (Note: Do not include suicidal or self-mutilating
behavior covered in Criterion 5.)
• A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation
• Identity disturbance: markedly and persistently unstable self-image or sense of self
• Impulsivity in at least two areas that are potentially self-damaging (e.g., spending, sex, substance abuse,
reckless driving, binge eating). (Note: Do not include suicidal or self-mutilating behavior covered in Criterion 5.)
• Recurrent suicidal behavior, gestures, or threats, or self-mutilating behavior
• Affective instability due to a marked reactivity of mood (e.g., intense episodic dysphoria, irritability, or
anxiety usually lasting a few hours and only rarely more than a few days)
• Chronic feelings of emptiness
• Inappropriate, intense anger or difficulty controlling anger (e.g., frequent displays of temper, constant
anger, recurrent physical fights)
• Transient, stress-related paranoid ideation or severe dissociative symptoms
Table 2: Summary of BPD Treatment Guidelines17-20 APA 2001 WFSBP 2007 NICE 2009 NHMRC 2012
1st Line Treatment DBT/Psychodynamic therapy
Symptomatic Pharmacotherapy Recommendations
Affective Dysregulation
1st Line SSRI
SSRI
Pharmacotherapy not recommended
specifically for BPD
or its symptoms.
Antipsychotics: avoid medium/long-
term treatment
Consider drug
treatment for comorbid
conditions.
Short-term (< 1 wk)
sedative in crisis.
Evidence does not support the use of
pharmacotherapy
as first-line or sole treatment
for BPD.
May consider time-
limited use as adjunct to
psychotherapy for specific symptoms
• Avoid
polypharmacy, if possible
2nd Line Anger: Low-dose
antipsychotic Anxiety:
Clonazepam
MAOI
3rd Line MAOI Mood stabilizer
-
Impulsive Behavior
1st Line SSRI Mood stabilizer
2nd Line Low-dose FGA SGA
3rd Line Lithium
MAOI
-
4th Line SGA -
Cognitive-Perceptual
1st Line Low-dose FGA SGA
2nd Line Increase dose of FGA
SSRI or MAOI
FGA
Last-
Line
SGA or Clozapine -
DBT=dialectical behavioral therapy; FGA=first generation antipsychotic; SGA=second generation
antipsychotic; SSRI=selective serotonin reuptake inhibitor; MAOI=monoamine oxidase inhibitor

Page 4 of 19
Table 3: Cochrane Systematic Review and Meta-Analysis (2010); Cochrane Systematic Review (2015)21-22
Recommendations: Affective dysregulation: 1st line: mood stabilizers (topiramate, lamotrigine, valproate) 2nd line: SGAs (aripiprazole, olanzapine, quetiapine*), FGAs (haloperidol) Impulsive-behavioral dyscontrol: 1st line: mood stabilizers (lamotrigine, topiramate) Alternative: Antipsychotics (mixed results) • Aripiprazole: improvement on overall impulsivity • Flupentixol decanoate: favorable results • Olanzapine: unfavorable effects on self-mutilation and suicidal behavior Cognitive-perceptual symptoms: 1st line: SGAs (aripiprazole, olanzapine, quetiapine*) Interpersonal problems: Mood stabilizers (valproate, topiramate) Aripiprazole * Added based on Cochrane Systematic Review (2015)
Presenter Conclusions: • Mood stabilizers and second generation antipsychotics were found to be beneficial for
symptom clusters of BPD. • Large variation in outcome variables and rating scales used between studies. • Standardization of outcome measures, especially use of outcome measures specific to BPD,
would be beneficial for future studies and meta-analyses. • Longer study duration is necessary to evaluate long-term effectiveness of medications in
BPD. • Larger randomized, placebo-controlled studies are needed to better evaluate efficacy and
tolerability of BPD treatment.
FGA=first generation antipsychotic; SGA=second generation antipsychotic
Study Selection Process for Today’s Presentation: • Oral antipsychotic studies for patients with BPD • Published from 2014 to 2019

Page 5 of 19
Table 4: Comparison of Low and Moderate Dosages of Extended Release Quetiapine in Borderline Personality Disorder: A Randomized, Double-Blind, Placebo Controlled Trial.23 Black DW, Zanarini MC, Romine A, et al. Am J Psychiatry. 2014 Nov 1;171(11):1174-82.
Design 8 week, randomized, double-blind, placebo controlled trial
• Screening phase (weeks 1-2)
• Treatment phase (weeks 2-10)
• Discontinuation phase (week 11)
Objective To determine the efficacy of low and moderate dose quetiapine for symptoms of borderline personality disorder
Inclusion
Criteria
• Diagnosis of BPD (DSM-IV)
• Zanarini scale score > 9 at baseline
Exclusion
Criteria • Medically unstable
• Current major depressive disorder, post-traumatic stress disorder, panic disorder, or obsessive-compulsive disorder
• Current substance dependence or abuse
• Any psychotic disorder, primary neurological condition, or cognitive impairment
• Previous non-response to atypical antipsychotic
• Pregnant or lactating
• Could not begin psychotherapy during the study
Intervention • Quetiapine 150 mg/day, quetiapine 300 mg/day, or placebo for 8 weeks, followed by a
1-week discontinuation phase o Quetiapine 150 mg/day:
▪ Started at 50 mg/day
▪ Increased to 150 mg/day after 1 week o Quetiapine 300 mg/day
▪ Started at 50 mg/day ▪ Increased to 150 mg/day after 1 week
▪ Increased to 300 mg/day after 4 weeks
Assessment • Patients were evaluated at baseline and weekly using both clinician and patient rated scales
• Safety: electrolytes, glucose, lipids, and prolactin at baseline and week 10. UDS and
pregnancy test at baseline. Extrapyramidal symptoms (EPS) assessed by Abnormal Involuntary Movement Scale (AIMS), Barnes Akathisia Scale and Simpson-Angus Rating Scale.
Endpoints • Primary: Zanarini Rating Scale for BPD (ZAN-BPD) total score
• Secondary: ZAN-BPD Self-Report (SR), Borderline Evaluation of Severity Over Time (BEST),
Montgomery-Asberg Depression Rating Scale (MADRS), Overt Aggression Scale-Modified
(OAS-M), Young Mania Rating Scale, Global Assessment of Functioning (GAF), Barratt Impulsiveness Scale (BIS-11), Symptom Checklist 90 Revised (SCL-90-R), and Sheehan
Disability Scale
Statistical
Analysis • Sample size of 33 in each group required to provide power of 0.80
• Mixed-effects model for primary endpoint o Response: > 50% reduction in Zanarini scale total score
• Pearson’s chi square test for categorical baseline group differences
• Kruskal-Wallis test for dimensional baseline group differences
• Mean severity scores compared from baseline using analysis of variance
• Cox proportional hazards regression for time to response (primary endpoint) and to compare
adverse events between groups
Results • Enrollment: n=95
o Quetiapine 150 mg/d: 33 patients o Quetiapine 300 mg/d: 33 patients
o Placebo: 29 patients
o Mean age: 25 yrs o Female: n=67 (70%)

Page 6 of 19
• Psychiatric disorders: o Placebo: Mood disorder n=14 (48%); Anxiety disorder n=5 (17%); Substance Use
Disorder n=6 (21%) o Quetiapine ER 150 mg/day: Mood disorder n=25 (76%); Anxiety disorder n=5
(15%); Substance Use Disorder n=11 (33%)
o Quetiapine ER 300 mg/day: Mood disorder n=19 (58%); Anxiety disorder n=5 (15%); Substance Use Disorder n=13 (39%)
• Additional Psychotropic use:
o Use of benzodiazepines (< 1 mg lorazepam or equivalent) was allowed o Use of episodic anticholinergics was allowed for sleep
o Other psychotropic medications not allowed during study
• ZAN-BPD total score reduction:
o Quetiapine ER 150mg/day: - 9.8 points > quetiapine ER 300 mg/day -7.9 points > placebo -6.0 points
• Response Rate (> 50% reduction in ZAN-BPD total score):
o Quetiapine ER 150mg/day: 82% > quetiapine ER 300 mg/day 74% > placebo 48%
Quetiapine vs Placebo Effects on Endpoints (Mean Weekly Change)
Measure Quetiapine
150mg/d
P value Quetiapine
300mg/d
P value
ZAN-BPD Total Score
-0.79 0.031 -0.41 NS
ZAN-BPD Cognitive Disturbance
-0.63 0.023 -0.43 NS
ZAN-BPD Self-Rated
Total Score
-0.88 0.006 -0.87 0.007
ZAN-BPD Self-Rated Affective Disturbance
-0.70 0.040 -0.87 0.013
ZAN-BPD Self-Rated Cognitive Disturbance
-0.71 0.016 -0.73 0.013
ZAN-BPD Self-Rated
Disturbed Relationship
-0.86 0.002 -0.73 0.008
BEST Total Score
-0.85 0.009 -0.75 0.020
BEST Thoughts and Feelings
-0.90 0.004 -0.82 0.009
Overt Aggression Scale-
Modified
-0.82 0.014 -0.76 0.020
Young Mania Rating Scale -0.40 NS -0.50 0.019
Sheehan Disability Scale
Days Lost
-0.49 0.025 -0.54 0.012
Safety:
• Any adverse event: Not statistically significant between groups
o Quetiapine 150 mg/day: n=29 (88%) o Quetiapine 300 mg/day: n=30 (91%)
o Placebo: n=25 (86%)
• Increased risk for sedation (HR 2.16, p=0.021), change in appetite (HR 3.89, p=0.018),
and dry mouth (HR 16.77, p=0.007) for quetiapine 300 mg/d vs placebo.
• Increased risk for dry mouth (HR 9.32, P=0.034) with quetiapine 150 mg/d vs placebo
• Risk of discontinuation was higher, but not statistically significant, vs placebo
• No significant difference in weight gain, serum glucose level, or lipids.
• No serious adverse events occurred during study period.

Page 7 of 19
Author’s
Conclusions • Improvement in BPD symptoms (based on ZAN-BPD total score) was statistically significant
for low dose quetiapine ER vs placebo. Moderate dose quetiapine ER did not show a
statistically significant improvement in overall BPD symptoms. o Improvement was highest from weeks 2 to 6
• Both low- and moderate-dose quetiapine superior for symptoms of aggression compared to
placebo.
• No significant differences on impulsivity or depression between groups.
• Increased risk for sedation, appetite, and dry mouth with higher doses of quetiapine.
Presenter Comments &
Conclusions
Strengths:
• Randomized, double-blind, placebo controlled trial comparing multiple dosages of quetiapine
• Moderate sample size (n = 95)
• Use of validated rating scales
• Extended screening period Limitations:
• Dropout rate of 33%, although similar between groups
• Strict exclusion criteria
• Placebo arm did not meet power
• Funded by AstraZeneca
• Previous medication use not reported
Conclusion:
• Quetiapine ER 150 mg/day appears to improve overall symptoms of BPD in the short-term.
• Quetiapine ER 150-300 mg/day appears to improve symptoms of aggression, affective and cognitive disturbance, severity of symptoms, and days lost from work in the short-term.
• Quetiapine ER 300 mg/day appears to improve irritability, physical and verbal aggression.
Table 5: A Comparative Study on Olanzapine and Aripiprazole for Symptom Management in Female Patients with Borderline Personality Disorder.24 Shafti SS, Kaviani H. Bulletin of Clinical Psychopharmacology 2015;25(1):38-43.
Design 8 week, randomized, open-label study
Objective To compare the efficacy and safety of olanzapine vs aripiprazole with regard to management of BPD.
Inclusion
Criteria
• Diagnosis of BPD (DSM-IV TR)
• Female
Exclusion
Criteria
• Major depression, bipolar disorder, psychosis, substance dependence, mental retardation, or
neurological conditions
• Concurrent psychotropic medications or psychotherapy
Intervention • Olanzapine
o Initial: 2.5 mg/day; increased by 2.5 mg/day as needed or tolerated o Max dose: 10 mg/day
• Aripiprazole
o Initial: 2.5 mg/day; increased by 2.5 mg/day as needed or tolerated
o Max dose: 10 mg/day
• Dose established by week 4 continued for remainder of study
Assessment • Baseline and week 8
Endpoints • Primary: Brief Psychiatric Rating Scale (BPRS)
• Secondary: Clinical Global Impression-Severity (CGI-S), Buss-Durkee Hostility Inventory
(BDHI)
Statistical Analysis
• Student t-test to compare baseline characteristics
• BPRS, CGI-S, BDHI analyzed via paired t-test (within each group) and unpaired t-test
(between groups)
• Cohen’s d and effect size correlation to analyze effect size.
• Statistical significance: p<0.05

Page 8 of 19
Results • Enrollment: n=24 o Mean age:
▪ Olanzapine group: 28 years ▪ Aripiprazole group: 26.8 years
o Female: n=24 (100%)
• Mean dose:
o Olanzapine group: 6.4 mg/day o Aripiprazole group: 7.0 mg/day
Olanzapine vs Aripiprazole Effect on Endpoints
Intra-group analysis
Measure OLANZ
Baseline
OLANZ
Week 8
Mean
Reduction
P
value
ARIP
baseline
ARIP
Week 8
Mean
Reduction
P
value
BPRS 43.8 32.5 -25.7% 0.001 44.1 35.8 -18.8% 0.04
BDHI 59.7 50.7 -15% 0.04 58.3 51.1 -12.2% NS
CGI-S 3.5 2.8 -20.9% 0.03 3.36 2.7 -19.3% NS
Between-group analysis
Measure OLANZ Baseline
ARIP Baseline P value OLANZ Week 8
ARIP Week 8 P value
BPRS 44.1 43.8 NS 35.8 32.5 NS
BDHI 58.3 59.7 NS 51.1 50.7 NS
CGI-S 3.3 3.5 NS 2.7 2.8 NS
Safety: all adverse effects reported as mild and well-tolerated.
• Aripiprazole group (n=12)
o Tremor (n=1)
o Inner restlessness (n=2) o Akathisia (n=1)
o Headache (n=1) o Insomnia (n=1)
• Olanzapine group (n=12)
o Weight gain (n=3) o Somnolence (n=4)
o Dizziness (n=2)
o Tremor (n=2)
Author’s Conclusions
• Both olanzapine and aripiprazole improved overall symptoms of BPD, as measured by BPRS.
Between group analysis did not show a significant difference in effect between olanzapine and aripiprazole groups.
• Olanzapine had more improvement on “anger and hostility” and “overall illness severity” from
baseline to 8 weeks, although this was not statistically significant compared to aripiprazole.
• Side effect profiles differed between the two antipsychotics o Olanzapine was more likely to cause weight gain, somnolence, and dizziness.
o Aripiprazole was more likely to cause akathisia, headache, and insomnia.

Page 9 of 19
Presenter
Comments & Conclusions
Strengths:
• Patients were randomized
• Compared aripiprazole to most well-studied antipsychotic in BPD
• Not funded by manufacturer; authors report no conflicts of interest
• No dropouts
Limitations:
• Open-label design
• All female
• Lack of placebo group
• Baseline characteristics not well reported
• Concomitant psychotropic medications not well reported
• Small sample size (n=24) Conclusion:
• Olanzapine and aripiprazole doses of 2.5-10mg/day appear to be effective for the short-term
management of overall BPD symptoms.
• Olanzapine may have additional benefit on symptoms of “anger and hostility” and “overall
illness severity” compared to aripiprazole when used short-term.
• Generalizability to males limited due to all female study population. • Additional studies with larger sample sizes and placebo-control groups are needed to better
evaluate effects of olanzapine vs aripiprazole for treatment of BPD.
Table 6: Efficacy and Tolerability of Asenapine Compared with Olanzapine in Borderline Personality Disorder: An Open-Label Randomized Controlled Trial.25
Bozzatello P, Rocca P, Uscinska M, Bellino S. CNS Drugs. 2017 Sep;31(9):809-819.
Design 12 weeks, Open-label, Randomized, Controlled Clinical Trial
Objective To evaluate efficacy and tolerability of asenapine versus olanzapine for the treatment of BPD.
Inclusion
Criteria
• Diagnosis of BPD (DSM-V)
• Ages 18-55 years
Exclusion
Criteria • Diagnosis of dementia or other cognitive disorders
• Psychotic disorders, bipolar disorders, current major depressive episode and/or substance abuse
• Use of psychotropic medication and/or psychotherapy in 2 months before study
• Lack of adequate birth control (females)
Intervention • Asenapine 5-10 mg/day
o Asenapine titration: 5 mg/day for five days, then 10 mg/day if tolerated
• Olanzapine 5-10 mg/day o Olanzapine titration: 5 mg/day for five days, then 10 mg/day if tolerated
Assessment • At baseline, 6 weeks, and 12 weeks
Endpoints • Primary: Clinical Global Impression-Severity (CGI-S)
• Secondary: Borderline Personality Disorder Severity Index (BPDSI), Barratt Impulsiveness
Scale (BIS-11), Hamilton Depression Rating Scale (HAM-D), Hamilton Anxiety Rating Scale (HAM-A), Social Occupational Functioning Assessment (SOFAS), Overt Aggression Scale-
Modified (OAS-M), Self-Harm Inventory (SHI)
• Safety: Dosage Record and Treatment Emergent Symptom Scale (DOTES)
Statistical Analysis
• Intention-to-treat (ITT)
• One-way analysis of variance (ANOVA) to compare baseline mean scores between groups
• ANOVA repeated measures to compare score change at 12 weeks
• Bonferroni correction applied to correct for multiple comparisons
• LOCF
Results • Enrollment: n=51
o Asenapine: n=25 o Olanzapine: n=26
o Mean age: 24.7 years (range 18-51 years)

Page 10 of 19
Asenapine vs Olanzapine Effects on Endpoints
Measure Asenapine 5-10mg/d Olanzapine 5-10mg/d P value P value
Baseline 12 wks Baseline 12 wks Within Subject
Between Groups
CGI-S 4.00 3.70 4.20 3.90 0.012 NS
BPDSI Total
Score
55.59 51.35 53.37 49.12 0.001 NS
BPDSI- Affective Instability
8.21 4.58 7.54 6.86 0.001 0.001
BPDSI- Dissociation
2.37 2.36 2.49 1.67 0.001 0.021
HAM-A 17.30 17.00 18.50 16.40 0.0004 NS
HAM-D 12.90 12.80 15.70 15.70 NS NS
SOFAS 60.10 61.00 55.50 58.30 0.004 NS
OAS-M 5.50 5.20 5.20 4.80 NS NS
BIS-11 70.40 64.70 75.30 72.90 0.005 NS
SHI 7.90 6.90 10.30 8.80 0.004 NS
Safety:
• Discontinuation: o Asenapine: n=2
▪ Oral hypoesthesia: n=1 ▪ Anxiety (moderate): n=1
o Olanzapine: n=2
▪ Weight gain (> 3 kg): n=2
• Side effects: o Asenapine:
▪ Akathisia: n=2 ▪ Restlessness/anxiety: n=2
o Olanzapine group
▪ Somnolence: n=3 ▪ Fatigue: n=2
Author’s
Conclusions
• Both asenapine and olanzapine improved overall psychiatric symptoms.
• No significant difference between asenapine and olanzapine for overall psychiatric symptoms,
anxiety, or functioning.
• Asenapine was found superior to olanzapine in reducing affective instability.
• Olanzapine was found superior to asenapine in reducing dissociation/paranoid ideation,
although power was not met for this endpoint.
• Neither medication caused significant improvement for symptoms of depression.
• Asenapine was associated with a lower incidence of weight gain than olanzapine, but more common extrapyramidal symptoms (akathisia) and oral hypoesthesia.

Page 11 of 19
Presenter
Comments & Conclusions
Strengths:
• Intention-to-treat (ITT) analysis
• Moderate sample size (n=51)
• Compared asenapine to most well-studied atypical antipsychotic (olanzapine) for BPD
• Not funded by manufacturer; no author conflicts of interest
Limitations:
• Open-label design
• Lack of placebo group
• Strict exclusion criteria
• Previous pharmaco- and psychotherapy not assessed
• Drop-out rate (21.7%)
• Post-hoc power analysis Conclusion:
• Both asenapine and olanzapine appear to improve overall psychiatric symptoms in the short-
term.
• Asenapine appears to be more effective than olanzapine for symptoms of affective instability
in the short-term.
• Olanzapine may be more effective for cognitive-perceptual symptoms of BPD. • Validity of study results is limited by lack of placebo group.
Table 7: Real-world effectiveness of clozapine for borderline personality disorder: results from a 2-year mirror-image study.26
Rohde C, Polxwiartek C, Correl CU, Nielsen J. J Pers Disord. 2018 Dec;32(6):823-837.
Design Retrospective, observational, 2-year mirror-image study
Objective To identify the effectiveness of clozapine based on prescription database and hospitalization records.
Inclusion
Criteria
• Redeemed at least one prescription of clozapine between January 1995 and September 2012
Exclusion
Criteria • None listed
Exposure • Clozapine use (defined as redeeming at least one prescription based on prescription register
fill data). o Compared endpoints from 2-years before and after initial clozapine prescription.
o Post-mirror period was shortened if patient did not fill clozapine for > 3 months
Assessment • Danish Psychiatric Central Research Register (psychiatric admissions and diagnosis based on
ICD-8 and ICD-10 codes) o Data on all psychiatric admissions since 1969 and all outpatient contacts after 1994
• Danish National Patient Register from 1977 to obtain data on somatic admissions and
diagnoses (ICD-8 and ICD-10 codes)
• Danish National Prescription Register o Data on prescription-based medications and daily dose from 1995 onward
Endpoints • Psychiatric admissions
• Psychiatric bed-days
• Concomitant psychotropic medication use
o Lithium, Tricyclic antidepressants (TCAs), selective serotonin reuptake inhibitors
(SSRIs), Serotonin-Noradrenergic Reuptake Inhibitors (SNRIs), Mianserin, Mirtazapine, Moclobemide, Benzodiazepines (BZDs), First Generation Antipsychotics
(FGAs), and Second-Generation Antipsychotics (SGAs) o Calculated as Defined Daily Dose (DDD), excluding hospitalization days
• Serious side effects to clozapine
o Agranulocytosis, Cardiomyopathy, Myocarditis, Neuroleptic Malignant Syndrome,
Diabetes Mellitus Type 2
• Intentional self-harm or overdose.

Page 12 of 19
Statistical
Analysis • Paired t-test to compare psychiatric admissions, number of psychiatric bed-days, and total
DDD from before and after clozapine initiation.
o Wilcoxon-signed rank test for all BPD cohort (cohort did not satisfy parametric assumptions for paired t-test)
• McNemar’s exact test to compare concomitant medications and intentional self-harm or
overdose from before and after clozapine initiation.
• Linear regression model to adjust for decrease in available psychiatric beds in Denmark from
1995 to 2012.
• All analyses 2-sided; p<0.05 considered statistically significant
Results • Identified 1,107 patients with > 1 clozapine prescription
• Mean age: 36.34 years
• Female: n=675 (60.98%)
• Previously institutionalized (long-term): n=156 (14.09%)
• Mean follow up: 598.51 days
• Mean dose of clozapine 350.40 mg/day
Clozapine Effects on Endpoints
Measure Pre-Clozapine Post-Clozapine Mean difference P value
Psychiatric
Hospitalizations
All BPD pts
(n=1107)
2.54 2.00 -0.54 < 0.001
BPD specific pts (n=102)
2.02 1.33 -0.69 0.0067
Psychiatric
Hospitalizations for pts
admitted in Pre-Cloz Period
All BPD pts
(n=698)
4.04 2.70 -1.34 <0.001
BPD specific
pts (n=47)
4.38 2.51 -1.87 <0.001
Psychiatric
Bed-Days
All BPD pts
(n=1107)
56 4 - <0.001
Specific BPD
pts (n=102)
3 0 - 0.008
Psychiatric
Bed-Days for pts > 1 Bed-
Day in Pre-Cloz Period
All BPD pts
(n=770)
190.08 65.95 -124.12 <0.001
Specific BPD pts (n=52)
160.49 76.34 -84.15 0.006
Intentional
Self-Harm or Overdose
All BPD pts
(n=1107)
189 (17.07) 114 (10.30) - <0.001
Specific BPD pts (n=102)
19 (18.63) 14 (13.73) - NS
Concomitant Medication Use: All BPD pts (n=1107)
Medication Pre-Clozapine (%) Post-Clozapine (%) P value
Lithium 72 (6.50) 64 (5.78) NS
TCA 208 (18.79) 257 (23.22) <0.001
SSRI 368 (33.24) 380 (34.33) NS
Other Antidepressants 195 (17.62) 181 (16.35) NS
BZDs 664 (59.98) 751 (67.84) <0.001
FGAs Low-Potency 573 (51.76) 547 (49.41) NS
Mid-Potency 398 (35.95) 309 (27.91) <0.001
High-Potency 137 (12.38) 114 (10.30) 0.035
SGAs 448 (40.47) 407 (36.77) 0.001
*Specific BPD pts = without schizophrenia, schizoaffective disorder, or bipolar disorder

Page 13 of 19
Safety (n=1107)
Adverse Event Pre-Clozapine (%) Post-Clozapine
Agranulocytosis 0 (0) 0 (0)
Cardiomyopathy 5 (0.45) 2 (0.18)
Myocarditis 0 (0) 0 (0)
Neuroleptic Malignant Syndrome 4 (0.36) 0 (0)
Diabetes Type 2 14 (1.26) 19 (1.72)
Author’s Conclusions
• There were significant decreases in number of hospitalizations, as well as number of
psychiatric inpatient bed-days in the all BPD group and specific BPD group after initiation of clozapine.
o Clozapine in the specific BPD group showed a decrease in hospitalizations similar to
studies for bipolar disorder and schizophrenia.
• There was a significant decrease in intentional self-harm or overdose after initiation of clozapine in the all BPD group but not the specific BPD group. This may be due to the small
sample size of the specific BPD group.
• Use of BZDs and TCAs increased significantly. The use of all antipsychotics decreased significantly, except for low-potency FGAs.
• Rate of serious adverse effects was not significantly different after initiating clozapine.
Presenter
Comments & Conclusions
Strengths:
• Large overall sample size (n=1107) for all BPD patient group
• Not funded by manufacturer.
• Analyzed relevant clinical outcomes (hospitalizations, intentional self-harm)
• Analyzed concomitant medication use
Limitations:
• Data and conclusions based solely on ICD-8, ICD-10, and prescription refill data. o Unable to classify patients by specific symptomology or symptomatic benefits of
clozapine.
• Small sample size (n=107) for the specific BPD group based on type of study.
• Did not evaluate mild to moderate side effects of clozapine or reasons for discontinuation. Conclusion:
• Clozapine appears to decrease the risk of hospitalization for patients with BPD. However, the
sample size was small for patients with only BPD (without concomitant schizophrenia or
bipolar disorder).
• Unclear whether the magnitude of effect was due to improved symptomology from treating these other conditions or whether clozapine actually benefits BPD itself.
• Further study, preferably with randomized, double-blind, placebo-controlled trials is
warranted.

Page 14 of 19
Table 8: Comparison of Studies Evaluated23-26
Quetiapine (2014)
n=95
Olanzapine vs
Aripiprazole (2015) n=24
Asenapine vs
Olanzapine (2017) n=51
Clozapine (2018)
n=1107
Type of
Study
Randomized, double-
blind, placebo-controlled trial
Randomized, open-
label trial
Randomized, open-
label trial
Retrospective,
observational, mirror-image study
Treatment
Duration
8 weeks (tx phase) 8 weeks 12 weeks 2 years
Study
Population
Mean age: ~29 yrs
Female: 70% Psych. co-morbidities
included:
• Hx of mood,
anxiety, and/or SUD
Mean age: ~27 yrs
Female: 100% Psych. co-morbidities
included:
• Not defined
Mean age: ~25 yrs
Female: 63% Psych co-morbidities
included:
• Excluded most
co-morbid Axis I disorders
Mean age: ~36 yrs
Female: 61% Psych. co-morbidities
included:
• Not defined
Findings Significant
improvement in overall BPD symptoms with
low-dose quetiapine.
• Greatest improvement from
weeks 2 to 6.
Both low- and mod-
dose quetiapine improved symptoms of
aggression.
No significant
Improvement on impulsivity or
depression vs placebo.
Both olanzapine and
aripiprazole improved overall symptoms of
BPD.
Olanzapine >
aripiprazole on “anger and hostility” and
“overall illness severity” but not
statistically significant.
Both asenapine and
olanzapine improved overall psychiatric
symptoms.
Asenapine >
olanzapine for reducing affective instability.
Olanzapine >
asenapine for dissociation/paranoid
ideation
Neither medication improved symptoms of
depression.
Significant decrease in
psychiatric admissions and bed-days with
clozapine use.
No significant
difference in serious adverse events.
Strengths/ Limitations
Strengths: Randomized, double-
blind, placebo controlled trial
Moderate sample size
Use of validated rating
scales
Extended screening period
Limitations:
Dropout rate (33%)
Strict exclusion criteria
Funded by AstraZeneca
Previous medication
use not reported
Strengths: Patients were
randomized
Not funded by manufacturer
No dropouts
Limitations: Open-label design
All female
Lack of placebo group
Baseline characteristics not well reported
Small sample size
Strengths: Moderate sample size
Compared asenapine
to most well-studied atypical antipsychotic
for BPD
Not funded by
manufacturer
Limitations:
Open-label design
Lack of placebo group
Strict exclusion criteria
Drop-out rate (21.7%)
Strengths: Analyzed clinical
outcomes (e.g. hospitalizations)
Analyzed concomitant
medication use.
Limitations:
Analysis based on ICD, and prescription refill
data.
Small sample size for
the specific BPD group.
Did not evaluate mild to moderate side
effects or reasons for
discontinuation.

Page 15 of 19
Conclusions: A. There is some weak evidence for the use of specific atypical antipsychotics for the management of
overall BPD symptoms.
B. Atypical antipsychotics appear to be effective for the management of BPD symptoms, with variable
effects on specific symptom clusters based on the antipsychotic chosen. C. Antipsychotics may be useful for the treatment of BPD when first-line psychotherapies have failed or
are unavailable. Currently, available information provides evidence to support short-term antipsychotic treatment (< 12 weeks).
D. Evaluation of risks and benefits with initiation of antipsychotic therapy is pivotal to decide whether initiation of antipsychotic therapy is appropriate in patients with BPD. Patients should be informed of
current guideline recommendations and evidence with therapeutic options being offered.
E. More research is needed to evaluate the benefits of combination therapies, including psychotherapy plus pharmacotherapy or combination pharmacotherapy.
F. More long-term studies are needed to better evaluate the benefits and risks of continuing antipsychotic therapy when patients have experienced benefit.
G. Randomized, double-blind, placebo-controlled trials are needed to evaluate the benefit of clozapine
for the treatment of severe BPD.
References:
1. Grant BF, Chou SP, Goldstein RB, Huang B, Stinson FS, et al. Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: results from the Wave 2 National
Epidemiological Survey on Alcohol and Related Conditions. J Clin Psychiatry. 2008 Apr; 69(4): 533–
545. 2. Tomko RL, et al. Characteristics of borderline personality disorder in a community sample:
comorbidity, treatment utilization, and general functioning. J. Pers. Disord. 28. 734-750 (2014). 3. Zimmerman M, et al. The frequency of personality disorders in psychiatric patients. Psychiatr. Clin.
North Am. 31, 405-420 (2008). 4. Korzekwa MI, et al. Estimating the prevalence of borderline personality disorder in psychiatric
outpatients using a two-phase procedure. Compr. Psychiatry 49, 380-386 (2008).
5. Leichsenring F, Leibing E, Kruse J, New AS, Leweke F. Borderline personality disorder. Lancet. 2011 Jan 1;377(9759):74-84. doi: 10.1016/S0140-6736(10)61422-5.
6. Zanarini MC, et al. Reported pathological childhood experiences associated with the development of borderline personality disorder. Am J Psychiatry. 1997 Aug;154(8):1101-6.
7. Afifi TO, et al. Childhood adversity and personality disorders: results from a nationally representative
population-based study. J. Psychiatr. Res. 45, 814-822 (2011). 8. Torgersen S, et al. The Heritability of Cluster B Personality Disorders Assessed both by Personal
Interview and Questionnaire. J Pers Disord. 2012 Dec; 26(6): 848–866. doi: 10.1521/pedi.2012.26.6.848
9. Perez-Rodriguez MM, Bulbena-Cabré A, Bassir Nia A, Zipursky G, Goodman M, New AS. The
Neurobiology of Borderline Personality Disorder. Psychiatr Clin North Am. 2018 Dec;41(4):633-650. doi: 10.1016/j.psc.2018.07.012
10. Krause-Utz A, et al. The Latest Neuroimaging Findings in Borderline Personality Disorder. Curr Psychiatry Rep. 2014 Mar;16(3):438. doi: 10.1007/s11920-014-0438-z.
11. Pier KS, Marin LK, Wilsnack J, Goodman M. The Neurobiology of Borderline Personality Disorder. Psychiatric Times 2016; Vol 33, Issue 3. Retrieved from: https://www.psychiatrictimes.com/special-
reports/neurobiology-borderline-personality-disorder.
12. Gurvits IG, et al. Neurotransmitter dysfunction in patients with borderline personality disorder. Psychiatr Clin North Am. 2000;23(1):27-40.
13. Friedel RO. Dopamine dysfunction in borderline personality disorder: a hypothesis. Neuropsychopharmacology. 2004;29(6): 1029-39.

Page 16 of 19
14. Asherson P, et al. Differential diagnosis, comorbidity, and treatment of attention-deficit/hyperactivity
disorder in relation to bipolar disorder or borderline personality disorder in adults. Curr. Med. Res. Opin. 30, 1657-1672 (2014).
15. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington (VA): American Psychiatric Association; 2013.
16. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fourth
Edition, Text Revision. Washington, DC, American Psychiatric Association, 2000. 17. Oldham JM, Gabbard GO, Goin MK, Gunderson J, Soloff P, Spiegel D, et al. Practice Guideline for the
Treatment of Patients with Borderline Personality Disorder. American Psychiatric Association . Am J Psychiatry. 2001;158(10 Suppl):1-52.
18. Herpertz SC, Zanarini M, Schulz CS, Siever L, Lieb K, et al. World Federation of Societies of Biological
Psychiatry (WFSBP) Guidelines for Biological Treatment of Personality Disorders. The World Journal of Biological Psychiatry, 2007; 8(4): 212244.
19. National Collaborating Centre for Mental Health. Borderline personality disorder: the NICE GUIDELINE on treatment and management. National Clinical Practice Guideline No. 78. Leicester: British
Psychological Society & Royal College of Psychiatrists; 2009. 20. National Health and Medical Research Council. Clinical practice guideline for the management of
borderline personality disorder. Melbourne: National Health and Medical Research Council; 2012.
21. Lieb K, Völlm B, Rücker G, Timmer A, Stoffers JM. Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry. 2010 Jan;196(1):4-12.
22. Stoffers JM, Lieb K. Pharmacotherapy for borderline personality disorder--current evidence and recent trends. Curr Psychiatry Rep. 2015 Jan;17(1):534. doi: 10.1007/s11920-014-0534-0.
23. Black DW, Zanarini MC, Romine A, Shaw M, Allen J, Schulz SC. Comparison of low and moderate
dosages of extended-release quetiapine in borderline personality disorder: a randomized, double-blind, placebo-controlled trial. Am J Psychiatry. 2014 Nov 1;171(11):1174-82.
24. Shafti SS, Kaviani H. A Comparative Study on Olanzapine and Aripiprazole for Symptom Management in Female Patients with Borderline Personality Disorder. Bulletin of Clinical Psychopharmacology
2015;25(1):38-43. 25. Bozzatello P, Rocca P, Uscinska M, Bellino S. Efficacy and Tolerability of Asenapine Compared with
Olanzapine in Borderline Personality Disorder: An Open-Label Randomized Controlled Trial. CNS
Drugs. 2017 Sep;31(9):809-819. 26. Rohde C, Polcwiartek C, Correll CU, Nielsen J. Real-World Effectiveness of Clozapine for Borderline
Personality Disorder: Results From a 2-Year Mirror-Image Study. J Pers Disord. 2018 Dec;32(6):823-837.
27. Guy W: ECDEU Assessment Manual for Psychopharmacology: Publication ADM 76-338. Washington,
DC, US Department of Health, Education and Welfare.1976:534-7. 28. Barnes TR. A rating scale for drug-induced akathisia. Br J Psychiatry. 1989;154(5):672-6.
29. Barratt ES. Factor analysis of some psychometric measures of impulsiveness and anxiety. Psychol Rep. 1965;16:547-54.
30. Pfohl B, Blum N, McCormick B, et al. Reliability and validity of the Borderline Evaluation of Severity
Over Time (BEST): a self-rated scale to measure severity and change in persons with borderline personality disorder. J Pers Disord. 2009;23:281-93.
31. Arntz A, Van den Hoorn M, Cornelis J, et al. Reliability and validity of the borderline personality disorder severity index. J Pers Disord. 2003;17(1):45-59.
32. Ventura J, Green M, Shaner A, et al. Training and quality assurance with the Brief Psychiatry Rating Scale. “the drift busters”, Int J Psychiatr Res. 1993;3:221.
33. Buss AH, Durkee A. An inventory for assessing different kinds of hostility. J Consult Psychol.
1957;21:343-49. 34. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical
practice. Psychiatry (Edgmont). 2007 Jul;4(7):28-37. 35. Perez V, Barrachina J, Soler J, Pascual JC, Campins MJ, Puigdemont D, Alvarez E. The clinical global
impression scale for borderline personality disorder patients (CGI-BPD): a scale sensible to detect
changes. Actas Esp Psiquiatr. 2007 Jul-Aug;35(4):229-35. 36. Guy W. Dosage Record and Treatment Emergent Symptoms Scale (DOTES): ECDEU Assessment
Manual for Psychopharmacology-Revised, US Department of Health, Education and Welfare, Public

Page 17 of 19
Health Service, Alcohol, Drug Abuse, and Mental Health Administration, NIMH Psychopharmacology
Research Branch, Division of Extramural Research Programs. National Institute of Mental Health, Rockville, Md. 1976: 223-44.
37. Jones SH, Thomicroft G, Dunn G. A brief mental health outcome scale-reliability and validity of the Global Assessment of Functioning (GAF). Br J Psychiatry. 1995;166(5):654-9.
38. Hamilton M. The assessment of anxiety states by rating. Brit J Med Psychol. 1959;32(1):50-5.
39. Hamilton M. A rating scale for depression. J Neuro Neurosurg Psychiatry. 1960;23:56-62. 40. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J
Psychiatry. 1979;134(4):382-9. 41. Coccaro EF, Harvey PD, Kupsaw-Lawrence E, et al. Development of neuropharmacologically based
behavioral assessments of impulsive aggressive behavior. J Neuropsychiatry Clin Neurosci.
1991;3(2):S44-S51. 42. Sansone RA, Sansone LA. Measuring Self-Harm Behavior with the Self-Harm Inventory. Psychiatry
(Edgmont). 2010 Apr; 7(4): 16–20. 43. Sheehan DV, Harnett-Sheehan K, Raj BA. The measurement of disability. J Clin Psychopharm.
1996;11(S3):89-95. 44. Simpson GM, Angus JW. A rating scale for extrapyramidal side effects. Acta Psychiatr Scand.
1970;45(S212):11-9.
45. Goldman HH, Skodol AE, Lave TR. Revising Axis V for DSM-IV: a review of measures of social functioning. Am J Psychiatr. 1992;149(9):1148-56.
46. Derogatis LR. SCL-90-R, brief symptom inventory, and matching clinical rating scales. The use of psychological testing for treatment planning and outcome assessment. New York, NY: Lawrence
Erlbaum;1994:41-80.
47. Young RC, Biggs JT, Ziegler VE, et al. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. 1978;133:429-35.
48. Zanarini MC, Vujanovic AA, Parachini EA, et al. Zanarini Rating Scale for Borderline Personality
Disorder (ZAN-BPD): a continuous measure of DSM-IV borderline psychopathology. J Pers Disord.
2003;17(3):233-42.
49. Zanarini MC, Frankenburg FR. Self-Report Version of the Zanarini Rating Scale for Borderline
Personality Disorder. Belmont, Mass, McLean Hospital, 2008.

Page 18 of 19
Appendix A
Rating Scale Description • Abnormal Involuntary Movement Scale
(AIMS)27
• Clinician rated
• 10 items on 5 point Likert scale
• Used to assess for tardive dyskinesia
o Higher Score = More Severe
• Barnes Akathisia Scale28 • Subjective and Objective items on a 4-point Likert scale
• Global item on a 6-point Likert scale
• Used to assess drug induced akathisia
o Higher Score = More Severe
• Barratt Impulsiveness Scale – version 11 (BIS-11)29
• Self-report
• 30-items on 4 point Likert scale
• Used to assess motor impulsivity, cognitive impulsivity, lack of planning
• Borderline Evaluation of Severity Over Time (BEST)30
• Self-report
• 15 items on a 5-point Likert scale
• Used to measure BPD symptom severity and change o Higher Score = More Severe
o Final score which can range from 12 (best) to 72 (worst).
• Borderline Personality Disorder Severity
Index (BPDSI)31
• Clinician rated
• 8 items, scored 0-10 (0=never; 10=daily) and one item score
0-4 (identity)
• Semi-structured clinical interview to assess frequency and
severity of BPD symptoms. o Higher Score = More Severe
• Brief Psychiatric Rating Scale (BPRS)32 • Clinician rated
• 18 items on a 7-point Likert scale
• Used to assess psychotic symptoms
o Higher Score = More Severe
• Buss-Durkee Hostility Inventory
(BDHI)33
• Self-report
• 75 true/false items
• Used to measure changes in hostility and guilt
o Higher Score = More Severe
• Clinical Global Impressions Scale34 o CGI-S (severity)
o CGI-I (improvement)
• Clinician rated
• 3 items on 7 point Likert scale
• Higher Score = More Severe
• Clinical Global Impressions Scale
modified for borderline personality disorder (CGI-BPD)35
o CGI-BPD-S (severity) o CGI-BPD-I (improvement)
• Clinician rated:
• 10 items on 7 point Likert scale
o 9 items for 9 psychopathological domains of BPD o 1 item for global score
• Higher Score = More Severe
• Dosage Record and Treatment
Emergent Symptom Scale (DOTES)36
• 33 items on a 5-point Likert scale
• Used to assess for presence and intensity of side effects
o Higher Score = More Severe
• Covers 41 parameters, including posture, movement, and alertness
• Global Assessment of Functioning (GAF)37
• Clinician rated
• tracks psychological, social, and occupational functioning.
• Numeric scale (1 through 100) used by mental health clinicians and physicians to rate social, occupational, and psychological
functioning. o 100 is highest level of functioning; 0 is the least
functional

Page 19 of 19
• Hamilton Anxiety Rating Scale (HAM-A)38
• Clinician rated
• Scores severity of 14 anxiety symptoms over the last week
• Items scored 0-4; Total score range 0-56
• Used to assess symptoms of anxiety o Higher Score = More Severe
• Hamilton Depression Rating Scale
(HAM-D)39
• Clinician rated
• 17 items
o 8 items on a 5-point Likert scale and 9 items on a 3-
point Likert scale o Total score range 0-64
• Used to assess symptoms of depression
o Higher Score = More Severe
• Montgomery-Asberg Depression Rating Scale (MADRS)40
• Clinician rated
• 10 items on a 7-point Likert scale
• Used to measure severity of depression symptoms o Higher Score = More Severe
• 0 to 6 – normal /symptom absent 7 to 19 – mild depression 20
to 34 – moderate depression >34 – severe depression.
• Overt Aggression Scale-Modified
(OAS-M)41
• Clinician-rated scale
• 4 subscales for different types of aggression; scores are rated
0-4
• Used to track changes in aggression over time o Higher Score = More Severe
• Self-Harm Inventory (SHI)42 • Self-report scale to evaluate self-harm behaviors
• Scoring done by counting number of endorsed self-harm
behaviors
• Sheehan Disability Scale43 • Three self-rated items, on a scale of 0-10.
o 0 is unimpaired; 10 is highly impaired
• Used to measure functional impairment
• Simpson-Angus Scale44 • 10 items on a 5-point Likert scale
• Used to measure drug induced EPS symptoms
o Higher Score = More Severe
• Social Occupational Functioning Assessment (SOFAS)45
• Clinician rated scale
• Designed to evaluate patient impairment in social and occupational domains, independent of severity of patient
symptoms
• Score range 0-100 (higher score = better functioning)
• Symptom Checklist 90 Revised
(SCL-90-R)46
• Self-report
• 90 items on a 5-point Likert scale
• Used to measure current psychiatric symptoms
o Higher Score = More Severe
• Young Mania Rating Scale47 • Clinician rated
• 11 items; 4 items on 8-point Likert scale and 7 items on 4-point Likert scale.
• Used to assess severity of manic episode.
o Total scores of 0-60
o Higher Score = More Severe
• Zanarini Rating Scale for BPD (ZAN-BPD)48-49
o ZAN-BPD (clinician-rated) o ZAN-BPD SR (self-rated)
• Clinician rated and self-rated versions
• 9 items on a 5-point Likert scale
• Used to assess change in psychopathology of BPD o Higher Score = More Severe
Related Documents