Presented by, Dr Saqba Alam J of IMAB. 2013, vol. 19, issue 4

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Presented by,
Dr Saqba Alam
J of IMAB. 2013, vol. 19, issue 4
The aim of oral anticoagulant therapy is
to reduce blood coagulability to an
optimal therapeutic range within which
the patient is provided some degree of
protection from thromboembolic events.
This is achieved at the cost of a minor risk
of haemorrhage.
Oral anticoagulant therapy is prescribed for :
prophylaxis and treatment of pulmonary embolism
venous thromboembolism
deep vein thrombosis, DVT
For the prevention of postoperative venous thromboembolism after orthopaedic surgical procedures as hip fracture and prosthetic total hip or knee joint replacement,thromboembolic complications associated with atrial fibrillation and/or prosthetic replacement of cardiac valves.

INDIRECT ACTING ANTICOAGS (Coumarin derivatives)
Acenocoumarol - derivative of coumarin
MOA vitamin K antagonist
Peak of action with oral intake occurs 12 h
after administration. After discontinuation, the action persists for 48 - 72 h.
Atrial fibrillation and mitral stenosis
history of embolism
age over 65
hypertension; diabetes or expressed left ventricular hypertrophy
intramural thrombus of the heart after a infarction or aneurysm (3-6 months)
artificial heart valves, with a limited left ventricular function
Coumarin derivative
MOA : Acts on extrinsic clotting pathway by preventing the reduction of vitamin K into its active form.
Depending on the reason for the anticoagulation (cardiovascular thrombo-embolic risk), the patient’s target INR therapeutic ranges will be different.
Patients with atrial fibrillation, DVT, or stroke have a target INR of 2.0 to 3.0, whereas after undergoing cardiac valve replacement surgery, patients have a target range of 2.5 to3.5.
Patients taking warfarin may require bridging anticoagulation around the time of major surgery.
This involves replacing the warfarin with unfractionated or low molecular weight heparin. Consultation with a cardiologist is particularly recommended if a patient with a coronary stent requires surgery.
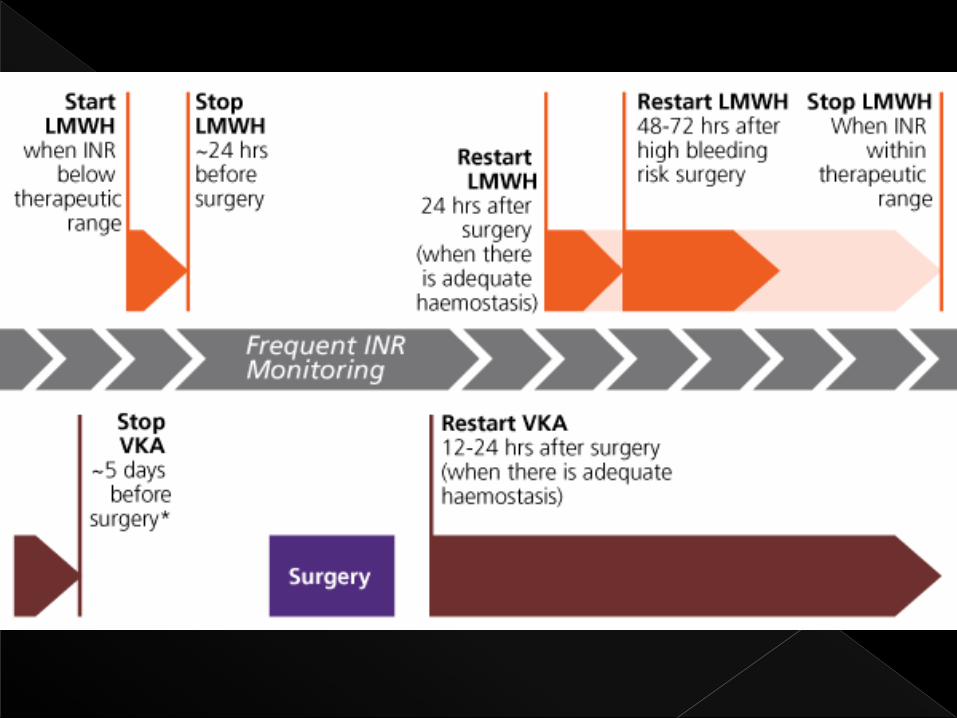

Bridging anticoagulation refers to giving a short-acting blood thinner, usually low-molecular-weight heparin given by subcutaneous injection for 10 to 12 days around the time of the surgery/procedure, when warfarin is interrupted and its anticoagulant effect is outside a therapeutic range.
Bridging anticoagulation aims to reduce patients' risk for developing blood clots, such as stroke, but may also increase patients' risk for developing potentially serious bleeding complications after surgery.

Dabigatran is a selective, reversible
direct thrombin inhibitor currently used in Europe and North America for stroke prevention in nonvalvular AF and in Europe for VTE prophylaxis in orthopedic patients.
Rapid onset of action.
It is able to provide stable anticoagulation at a fixed dose without the need for routine laboratory monitoring of INR and associated dosage adjustments.
No specific antidote or reversal agent exists.
However, owing to dabigatran’s short half-life (12-14 hours (14-17 hours in the elderly)), merely discontinuing the administration of the drug is thought to be sufficient to resolve minor bleeding in most circumstances.
Rivaroxaban is approved in Europe and North America as a highly selective Direct Factor Xa a Inhibitor.
MOA- Rivaroxaban interrupts the intrinsic and extrinsic pathway of the blood coagulation cascade, inhibiting both thrombin formation and development of thrombi. Rivaroxaban does not inhibit thrombin and no effects on platelets have been demonstrated.
It also provides stable anticoagulation at a fixed dose without the need for routine INR monitoring.
There is no specific reversal agent or antidote for rivaroxaban, but its short half-life means that the discontinuation of the drug is likely be adequate to correct most bleeding problems caused by its use.


Tests for anticoagulation assessment
The prothrombin time ratio (PTR), defined as the patient’s prothrombin time (PT) was used to monitor anticoagulant therapy for many years.
INR as an (ISI )index.
PT INR ratio INR =(PT test/PT normal)ISI
BY ( the International Committee on Thrombosis and Homeostasis 1985)
It is now widely used for monitoring anticoagulant therapy and dosage planning. The INR for a healthy patient is 1 and the therapeutic INR for those on anticoagulant therapy typically ranges from 2 to 4, depending on the reason for anticoagulation.

BCSH (British Committee for Standards in Haematology), the British Society for Haematology Committee, the British Dental Association (BDA), the National Patient Safety Agency (NPSA) presented a guideline in after reviewing in the year 2011, whose summary was…….
In pts with INR <4 (LOW) no need to discontinue oral
anticoags as the risk of thrombosis is increased.
GRADE A (LEVEL IB)
For patients stably anticoagulated on warfarin (INR
2-4) and who are prescribed a single dose of
antibiotics as prophylaxis against endocarditis,
there is no necessity to alter their anticoagulant
(grade C, level IV).
For patients who are stably anticoagulated on
warfarin, a check INR is recommended 72 hours
prior to dental surgery.
PTS with co-existing medical problems e.g. liver
disease, renal disease, thrombocytopenia .Such
patients may have an increased risk of bleeding.
NONE of these approaches is risk free
for the pt and the surgeon must make
a clinical judgement of the risk benefit
ratio between management
strategies and adverse complications.
Wahl reviewed 26 papers comprising 2014
dental surgical procedures in 774 patients
receiving continuous warfarin therapy,
THE CONCLUSION WAS….
Twelve patients (<2%) had postoperative
bleeding problems that were not controlled
by local measures
Major bleeding was rare (4/2012, 0.2%) for
patients with a therapeutic INR (<4)
undergoing dental surgery.THERE WERE NO
DEATHS……
The risk for FATAL pulmonary embolism
after discontinuing anticoagulant
therapy is 0.19 to 0.49 events per 100
person years for patients undergoing
anticoagulant therapy.
The case fatality rate from recurrent PE is
4% TO 9%

Specific consideration must be
given to the issue of whether oral
anticoagulant treatment should
be unaltered,modified, or
stopped according to possible
bleeding complications.
Hong C. et al. reported a study with 122
patients who had a total of 240 dental
extractions. 35 patients (29%) were on
concomitant medications thought to
potentate bleeding.7 patients were on
multiple antithrombotic
medications(excluding warfarin); 2 were
taking a combination of aspirin,cilastazol,
and nonsteroidal analgesic medication; 3
were on a combination of aspirin and
clopidogrel; and 2 were on acombination
of aspirin and enoxaparin.

The results of this retrospective study
suggest that the overall prevalence of
persistent bleeding after dental
procedures in patients on warfarin
therapy is low (2%).
Additionally, most complications
experienced were controlled with local
hemostatic measures
INR values should be obtained within 24 hours before the dental procedure. For patients with INR in the therapeutic range 2-4 or below, therapy need not be modified or discontinued for simple single dental extractions. More complicated and invasive oral surgical procedures for patients with an INR on the high end of the scale or greater than 3.5 should be referred to physician for dose adjust mentor therapy alteration before invasive dental procedures

(Ref : OCT 24,2003 GRACE REGISTRY EUR.HEART.J)
Local hemostatic measures are shown to
suffice to control the possible bleeding
secondary to dental treatments.

The risk of bleeding may be minimized by:
a.Pressure and Packing !!!....
b.The use of oxidized cellulose (Surgical) or collagen sponges and
c.sutures (grade B, level IIb).
d. 5% tranexamic acid mouthwashes used four times a day for 2 days (grade A, level Ib).
Ref : (Sept 2011Guidelines for the management of patients on oral anticoagulants requiring dental surgery
British Committee for Standards in Haematology)


.
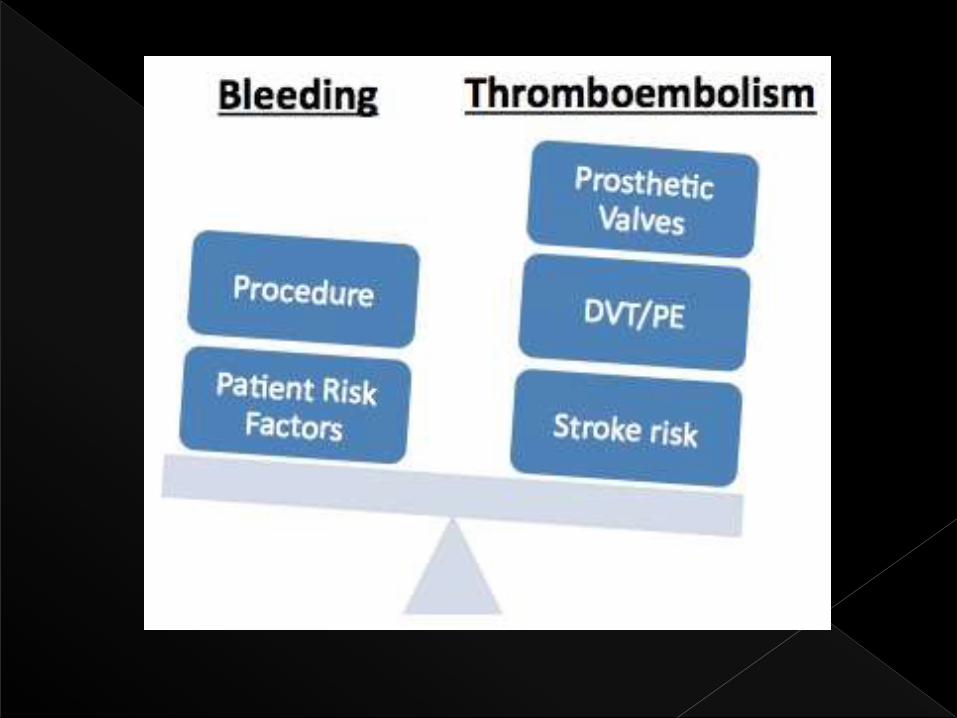
BLEEDING
VS
THROMBOSIS

It is necessary to carefully evaluate the
bleeding risk of the planned
treatment, as well as the thrombotic
risk of suppressing the anticoagulant
or antiplatelet medication, on an
individualized basis for each patient,
with a view to providing optimum and
personalized care.

THANK YOU !!
Related Documents











