Case Report Antibody-Negative Relapse of Goodpasture Syndrome with Pulmonary Hemorrhage Charlene L. Rohm , 1 Sara Acree, 2 Aseem Shrivastava, 3 Asif A. Saberi, 3 and Louis Lovett 4 1 Department of Internal Medicine, WellStar Kennestone Regional Medical Center, Marietta, GA, USA 2 Department of Pathology, WellStar Kennestone Regional Medical Center, Marietta, GA, USA 3 Critical Care Medicine, WellStar Kennestone Regional Medical Center, Marietta, GA, USA 4 Department of Graduate Medical Education, WellStar Kennestone Regional Medical Center, Marietta, GA, USA Correspondence should be addressed to Charlene L. Rohm; [email protected] Received 27 November 2018; Revised 23 March 2019; Accepted 7 April 2019; Published 24 April 2019 Academic Editor: Andr´ e R. Simon Copyright © 2019 Charlene L. Rohm et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Goodpasture syndrome is a rare autoimmune disease comprising antiglomerular basement membrane (anti-GBM) crescentic glomerulonephritis and pulmonary capillaritis with circulating anti-GBM antibodies. Rarely, antibody-negative cases have been described. We report a young, African American adult woman admitted with flank pain and hematuria with laboratory testing and kidney biopsy demonstrating anti-GBM crescentic glomerulonephritis with elevated anti-GBM antibody levels. She received treatment but remained dialysis-dependent. She was seronegative and clinically stable until she presented 8 months later with dyspnea and hemoptysis requiring mechanical ventilation. Bronchoscopy revealed diffuse alveolar hemorrhage. She was treated for relapse of Goodpasture syndrome. However, anti-GBM antibodies were undetectable. is case emphasizes prompt diagnosis and treatment of Goodpasture syndrome to preserve renal function. Additionally, clinical manifestations of Goodpasture syndrome and its degree of activity do not necessarily correlate with the actual antibody titer on relapse. Clinicians should have enhanced awareness of this atypical presentation of a rare disease. 1. Introduction e estimated incidence of Goodpasture syndrome is one case per million per year [1]. It is mediated by anti-GBM antibody deposition on the alveolar and glomerular basement mem- brane confirmed by immunofluorescence. Most patients present with a combination of rapidly progressive glomer- ulonephritis (RPGN) and pulmonary hemorrhage with a positive anti-GBM antibody titer. However, few cases of antibody-negative relapse of Goodpasture syndrome have been reported. Given the rarity of this disease, both the correct diagnosis of Goodpasture syndrome and the recognition of a relapse are critical in initiating timely and effective treatment. is case describes a patient diagnosed with Goodpasture syndrome who was clinically stable until she re-presented 8 months later with an antibody-negative relapse of Good- pasture syndrome with pulmonary hemorrhage. 2. Case Presentation A 24-year-old African American woman presented to the emergency department (ED) with several months of recurrent nausea, flank pain, and hematuria. She previously sought care 2 weeks prior and was told she had a diagnosis of urinary tract infection (UTI) and was empirically treated with oral ciprofloxacin. However, a urine culture did not grow any organisms, and symptoms persisted despite completing a course of antibiotics. Her past medical history included UTIs for which she received empiric antibiotic treatment, although all urine cultures in her medical chart repeatedly showed no growth of organisms. She was not taking medications. Family history was not significant for any chronic medical illnesses. She smoked cigarettes but denied consuming alcohol or using illicit drugs. On presentation, vital signs were stable and physical examination was significant for bilateral flank pain. Hindawi Case Reports in Medicine Volume 2019, Article ID 2975131, 5 pages https://doi.org/10.1155/2019/2975131

Antibody-Negative Relapse of Goodpasture Syndrome with Pulmonary Hemorrhage
Feb 03, 2023
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Case Report Antibody-Negative Relapse of Goodpasture Syndrome with Pulmonary Hemorrhage
Charlene L. Rohm ,1 Sara Acree,2 Aseem Shrivastava,3 Asif A. Saberi,3 and Louis Lovett4
1Department of Internal Medicine, WellStar Kennestone Regional Medical Center, Marietta, GA, USA 2Department of Pathology, WellStar Kennestone Regional Medical Center, Marietta, GA, USA 3Critical Care Medicine, WellStar Kennestone Regional Medical Center, Marietta, GA, USA 4Department of Graduate Medical Education, WellStar Kennestone Regional Medical Center, Marietta, GA, USA
Correspondence should be addressed to Charlene L. Rohm; [email protected]
Received 27 November 2018; Revised 23 March 2019; Accepted 7 April 2019; Published 24 April 2019
Academic Editor: Andre R. Simon
Copyright © 2019 Charlene L. Rohm et al. *is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Goodpasture syndrome is a rare autoimmune disease comprising antiglomerular basement membrane (anti-GBM) crescentic glomerulonephritis and pulmonary capillaritis with circulating anti-GBM antibodies. Rarely, antibody-negative cases have been described.We report a young, African American adult woman admitted with flank pain and hematuria with laboratory testing and kidney biopsy demonstrating anti-GBM crescentic glomerulonephritis with elevated anti-GBM antibody levels. She received treatment but remained dialysis-dependent. She was seronegative and clinically stable until she presented 8months later with dyspnea and hemoptysis requiring mechanical ventilation. Bronchoscopy revealed diffuse alveolar hemorrhage. She was treated for relapse of Goodpasture syndrome. However, anti-GBM antibodies were undetectable. *is case emphasizes prompt diagnosis and treatment of Goodpasture syndrome to preserve renal function. Additionally, clinical manifestations of Goodpasture syndrome and its degree of activity do not necessarily correlate with the actual antibody titer on relapse. Clinicians should have enhanced awareness of this atypical presentation of a rare disease.
1. Introduction
*e estimated incidence of Goodpasture syndrome is one case per million per year [1]. It is mediated by anti-GBM antibody deposition on the alveolar and glomerular basement mem- brane confirmed by immunofluorescence. Most patients present with a combination of rapidly progressive glomer- ulonephritis (RPGN) and pulmonary hemorrhage with a positive anti-GBM antibody titer. However, few cases of antibody-negative relapse of Goodpasture syndrome have been reported. Given the rarity of this disease, both the correct diagnosis of Goodpasture syndrome and the recognition of a relapse are critical in initiating timely and effective treatment. *is case describes a patient diagnosed with Goodpasture syndrome who was clinically stable until she re-presented 8months later with an antibody-negative relapse of Good- pasture syndrome with pulmonary hemorrhage.
2. Case Presentation
A 24-year-old African American woman presented to the emergency department (ED) with several months of recurrent nausea, flank pain, and hematuria. She previously sought care 2weeks prior and was told she had a diagnosis of urinary tract infection (UTI) and was empirically treated with oral ciprofloxacin. However, a urine culture did not grow any organisms, and symptoms persisted despite completing a course of antibiotics. Her past medical history included UTIs for which she received empiric antibiotic treatment, although all urine cultures in her medical chart repeatedly showed no growth of organisms. She was not taking medications. Family history was not significant for any chronic medical illnesses. She smoked cigarettes but denied consuming alcohol or using illicit drugs. On presentation, vital signs were stable and physical examination was significant for bilateral flank pain.
Hindawi Case Reports in Medicine Volume 2019, Article ID 2975131, 5 pages https://doi.org/10.1155/2019/2975131
Laboratory studies included an antinuclear antibody (ANA), rheumatoid factor (RF), complement C3 and C4, human immunodeficiency virus 1 and 2 (HIV 1 and 2) antibody, antineutrophil cytoplasmic antibodies (ANCA), anti-double-stranded DNA (anti-dsDNA) antibodies, and anti-GBM antibodies. All were negative except for anti-GBM antibodies which reported positive 1week later with a titer level of 1.7 (<1.0 is normal). In the interim, a renal biopsy was performed due to rapidly declining renal function. Light microscopy showed necrotizing and crescentic glomerulo- nephritis with fibrocellular crescent formation (Figure 1(a)). Electron microscopy demonstrated widespread podocyte foot process effacement and linear deposits along the glo- merular basement membrane (Figure 1(b)) confirmed as IgG by immunofluorescence (Figure 1(c)). A diagnosis of anti-GBM crescentic glomerulonephritis was made.
Before the confirmatory diagnosis was made by renal biopsy, on day 1 of hospital admission, our patient was treated with methylprednisolone 1 g IV daily for 3 days and then prednisone 40mg by mouth daily for 1month. Once the renal biopsy confirmed anti-GBM crescentic glomeru- lonephritis along with serologies positive for anti-GBM antibody, intravenous cyclophosphamide and plasma ex- change were both initiated on day 9 of hospitalization. She received cyclophosphamide 1 g IV every 2weeks for 3 oc- currences. She received plasma exchange daily for 7 days then every other day for 3 occurrences. Plasma exchange was stopped once repeat testing for anti-GBM antibodies was undetectable on day 23. Due to rapidly progressing renal failure, she required initiation of hemodialysis on day 4 of admission and continued to require hemodialysis daily throughout her hospital stay. Our patient was discharged to home on day 28 with outpatient nephrology follow-up and hemodialysis three times a week. Anti-GBM antibody levels remained undetectable. Kidney transplant evaluation was initiated.
Eight months later, our patient presented to the ED with dyspnea and hemoptysis. She last received dialysis the day before admission and had not missed any dialysis sessions. Social history was notable for marijuana use daily for a week prior to admission. She appeared diaphoretic and drowsy with decreasing oxygen saturation despite supplemental oxygen. Physical examination was significant for tachycar- dia, tachypnea, reduced air movement in all lung fields, and dullness to percussion of the thorax. A portable chest ra- diograph showed diffuse bilateral patchy opacities (Fig- ure 2). A computerized tomography angiography (CTA) of
the chest with IV contrast confirmed diffuse bilateral con- solidations (Figure 3). Our patient required tracheal in- tubation and mechanical ventilation with admission to the intensive care unit (ICU).
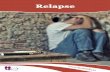
Our patient had a hemoglobin level of 6.4 g/dL, he- matocrit of 21%, and MCV of 95 fL which dropped to as low as a hemoglobin and hematocrit of 5.6 g/dL and 18%, re- spectively. *ree weeks prior to admission, hemoglobin was 8.7 g/dL and hematocrit was 26%. Flexible fiberoptic bronchoscopy was performed, and the bronchoalveolar la- vage (BAL) fluid was consistent with alveolar hemorrhage (Figure 4). *e lavage fluid was negative for malignant cells, bacterial, viral, or fungal organisms.
Repeat ANA, ANCA, and anti-dsDNA remained neg- ative. Unlike on initial presentation, repeat anti-GBM an- tibody levels were undetectable, which did not result until day 7 of the hospital stay. Given our patient’s history, a relapse of Goodpasture syndrome with pulmonary hem- orrhage was diagnosed. While the most likely diagnosis was a relapse of Goodpasture syndrome, acute heart failure was also included in the differential diagnosis. However, a transthoracic echocardiogram demonstrated a normal ejection fraction of 55–60%, normal left ventricular diastolic function, normal right ventricular systolic and diastolic function, mild tricuspid valve regurgitation with no other valvular abnormalities, an elevated pulmonary artery pres- sure of 50mmHg, and a normal central venous pressure. *ese findings were not suggestive of heart failure; rather, functioning of both left and right ventricles was intact, while the elevated pulmonary artery pressure was suggestive of a primary intrapulmonary process (pulmonary hemorrhage). Starting on day 1, she was treated with methylprednisolone 1 g daily for 5 days, and then changed to prednisone 40mg daily. Plasma exchange was also initiated on day 1 which she received daily for 5 occurrences. She was treated with mycophenolate 500mg IV every 12 hours for 5 days. She progressively improved clinically with resolved alveolar hemorrhage and was extubated on day 5. She was transferred to the medical ward in stable condition. On day 10, she was discharged to home with outpatient nephrology follow-up and continued dialysis.
Our patient was stable following her admission for Goodpasture syndrome relapse. She continued to have outpatient hemodialysis 3 times a week. She did not require outpatient oral steroids or immunosuppression. However, 9months later, we received the news that she had passed away from a drug overdose.
3. Discussion
Our patient’s urinalysis suggested a glomerulonephritis based on the presence of proteinuria, hematuria, and red cell casts. Subsequently, the diagnosis of RPGN was suspected because of rapidly progressive renal failure. RPGN com- prises 3 subtypes: immune-complex glomerulonephritis, pauci-immune glomerulonephritis, and anti-GBM glomer- ulonephritis (Goodpasture syndrome). Both anti-GBM and immune-complex glomerulonephritis demonstrate glo- merular staining for immunoglobulins, while pauci-immune
2 Case Reports in Medicine
glomerulonephritis has an absence or paucity of immunoglobulins.
Immune-complex glomerulonephritis is associated with systemic lupus erythematosus (SLE), immunoglobulin A (IgA) glomerulonephritis, IgA vasculitis, and postinfectious
glomerulonephritis. Our patient had negative ANA and anti-dsDNA antibodies, did not have symptoms suggestive of IgA vasculitis, and was previously healthy with no recent illnesses. Pauci-immune glomerulonephritis is associated with granulomatosis with polyangiitis, eosinophilic gran- ulomatosis with polyangiitis, and microscopic polyangiitis. Our patient had negative MPO-ANCA and PR3-ANCA levels which lower suspicion for their associated diseases.
While the best laboratory predictor of Goodpasture syndrome is serologic detection of anti-GBM antibodies, this serology takes several days to result. Rarely patients can have antibody-negative Goodpasture syndrome so that diagnosis is based on renal biopsy and clinical presentation. Our patient did have a positive anti-GBM antibody level. Light microscopy of her renal specimen showed that 95% of glomeruli had crescent formation. Immunofluorescence demonstrated linear deposits of IgG antibodies along the glomerular basement membrane, which is pathognomonic for anti-GBM glomerulonephritis. Based on our patient’s history and physical examination, urinary studies, rapidly progressive disease course, serologies, and renal biopsy, a
Figure 3: CTA of the chest with IV contrast reveals extensive bilateral consolidations.
Figure 4: Progressive increase in intensity of blood in sequential aliquots during BAL strongly suggests active alveolar hemorrhage.
(a) (b) (c)
Figure 1: (a) Light microscopy reveals glomeruli with cellular to focally fibrocellular crescent formation and underlying segmental tuft fibrinoid necrosis. Red blood cell casts are noted. *ere is severe mononuclear inflammation within the interstitium (H&E, 10x). (b) Electron microscopy demonstrates peripheral capillary loops of normal thickness and architecture with widespread effacement of the overlying foot processes. (c) Immunofluorescencemicroscopy shows strong linear staining along glomerular basementmembranes with IgG (4+) and kappa and lambda light chains (3-4+).
Figure 2: Portable chest radiograph demonstrates diffuse bilateral patchy opacities.
Case Reports in Medicine 3
diagnosis of anti-GBM glomerulonephritis (Goodpasture syndrome) was made.
Eight months later, our patient presented with dyspnea and hemoptysis. *e differential diagnosis for hemoptysis and dyspnea is broad, including infectious, immunological, or malignant etiologies. Given the hemoptysis, severe ane- mia, and chest imaging showing widespread opacities, there was a concern for hemorrhage. Our patient had no clinical history suggestive of an infectious process. Additionally, a BAL fluid analysis did not suggest an infection (no organism seen, rare WBCs, and no bacterial or fungal isolates). A respiratory infection panel which detects a variety of bacteria and viruses in the BAL fluid also returned negative. Negative ANA and anti-dsDNA antibody serologies ruled out rheumatologic disorders. Negative MPO-ANCA and PR3- ANCA serologies effectively ruled out ANCA-associated disorders.
Anti-GBM antibody levels were also undetectable. However, given our patient’s history of Goodpasture syn- drome, she likely had a relapse of Goodpasture syndrome with pulmonary hemorrhage.
Over 90% of patients with Goodpasture syndrome have circulating anti-GBM antibodies detectable by enzyme- linked immunosorbent assay (ELISA) [2]. ELISA for anti- GBM antibodies is highly sensitive (>95%) and specific (>97%) [2]. All positive results are confirmed by western blotting on collagenase-solubilized human GBM. *ese assays are rarely negative despite deposition of anti-GBM antibody in the kidney [2]. Although rare, the absence of circulating anti-GBM antibody in the setting of Goodpasture syndrome has been described [3–8]. A review of 6 reports revealed that each Goodpasture syndrome diagnosis had seronegative disease with diagnosis confirmed on renal biopsy. Database review shows that ELISA- and western blot-negative anti-GBM disease may occur in up to 2-3% of patients, requiring renal biopsy confirmation [2]. *erefore, while clinicians may rely on serological detection of cir- culating anti-GBM antibodies, the early renal biopsy dem- onstrating linear deposition of immunoglobulin along the GBM with crescentic glomerulonephritis remains the gold standard to diagnose Goodpasture syndrome.
*e average time to anti-GBM antibody result reporting for our patient was 7 days since this test was not done in- house. When our patient was first diagnosed with Good- pasture syndrome, she had an elevated anti-GBM antibody level of 1.7. During the subsequent hospital stay for relapse of Goodpasture syndrome, anti-GBM antibody was un- detectable by the same commercial ELISA kit BioPlex 2200 Vasculitis (Bio-Rad, Hercules, California). *is immuno- assay uses as antigen the extracted highly purified human alpha-3 chain of type IV collagen. An indirect fluorescent antibody (IFA) test was not performed. A western blot was not performed.
Prompt diagnosis and treatment of Goodpasture syn- drome is critical as it affects the disease course and prog- nosis. *e best predictor of outcomes for crescentic glomerulonephritis is based on serum creatinine and need for immediate hemodialysis. Levy et al. found that if
treatment is initiated when serum creatinine is<5.7mg/dL, patient and renal survival rates at 1 year are 100% and 95%, respectively [9]. Once serum creatinine is 5.7mg/dL or higher and without need for immediate dialysis, 1-year patient and renal survival decreased to 83% and 82%, re- spectively [9]. If treatment was initiated when patients presented with dialysis-dependent renal failure, 1-year pa- tient and renal survival was only 65% and 8%, respectively [9]. Our patient may have received an earlier diagnosis of Goodpasture syndrome had her prior urinalyses been more critically assessed for a glomerulonephritis rather than a UTI. Our patient had been told by prior physicians that her recurrent symptoms of nausea, flank pain, and hematuria were due to UTIs, despite multiple urine cultures demon- strating no growth of organisms and no resolution of symptoms with antibiotic treatment. She had incorrect di- agnoses of UTI in her past medical history. Her urinalysis showed significant amounts of red blood cells, protein, and red cell casts, which are all suggestive of glomerular disease. Specifically, she had a nephritic syndrome. Furthermore, an FENa of 2.8% and a BUN/Cr ratio of 7 suggested intrarenal damage. When presented with such urinary studies, glo- merulonephritis should be suspected. In the setting of a rapid decline in renal function, RPGN is likely. A renal biopsy should not be delayed. Unfortunately in our patient, treatment with plasma exchange and immunosuppression was not initiated until she had developed dialysis-dependent renal failure.
Patients with Goodpasture syndrome typically present with acute renal failure secondary to RPGN. *is can be associated with pulmonary hemorrhage. While most pa- tients present with a combination of RPGN and pulmonary hemorrhage, 30–40% present with an isolated renal in- volvement and 40–60% present with an isolated pulmonary hemorrhage [10, 11]. As in our patient, other cases of relapse with pulmonary hemorrhage have been reported [3, 4, 12–16]. Environmental factors such as cigarette smoking, drug use, and hydrocarbon solvents have been implicated in triggering pulmonary hemorrhage [3, 4, 12–16]. Our patient’s ongoing exposure to cigarettes plus her recent use of marijuana may have precipitated a Goodpasture relapse with pulmonary hemorrhage. Relapses resulting in pulmonary disease are strongly correlated with cigarette smoking, which causes inhalation injury leading to alveolar damage. It is possible that subjects with Good- pasture syndrome develop pulmonary hemorrhage when exposed to the right precipitant. Volatile hydrocarbons, cigarette smoking, concurrent infection, high concentration of inspired oxygen, and fluid overload have all been im- plicated [4].
In conclusion, Goodpasture syndrome is a rare syn- drome with variable patterns of presentation. Obtaining a kidney biopsy early and promptly initiating steroids and immunosuppression is critical in preserving renal function and minimizing morbidity and mortality. Goodpasture syndrome must also be considered despite the absence of anti-GBM antibody, as disease activity does not necessarily correlate with antibody titer.
4 Case Reports in Medicine
3.1. Learning Points
(i) Critically evaluate urinalysis. Consider glomerulo- nephritis in the setting of hematuria, proteinuria, and red cell casts.
(ii) Do not delay performing a renal biopsy to de- finitively diagnose Goodpasture syndrome. Mor- tality significantly increases once hemodialysis is required.
(iii) Isolated pulmonary hemorrhage can occur as the sole manifestation of relapse in Goodpasture syn- drome. *is can occur in the absence of detectable antibody levels.
(iv) Current evidence suggests that the clinical mani- festations of Goodpasture syndrome and its degree of activity do not necessarily correlate with the actual antibody titer.
Disclosure
*e case abstract has previously been presented at the So- ciety of General Internal Medicine Southern Regional Meeting in February 2017 in New Orleans, Louisiana, and at the Society of Hospital Medicine meeting in May 2017 in Las Vegas, Nevada. *e abstract has been published in the Journal of Hospital Medicine 2017. *is manuscript has not been published, accepted for publication, nor is it under editorial review for publication elsewhere.
Conflicts of Interest
All the authors declare that there are no conflicts of interest regarding the publication of this article.
Acknowledgments
We thank Dr. Salvatore Chillemi who was directly involved in the diagnosis, treatment, and management of this patient during her stay in the intensive care unit. We thank Dr. Harsharan Singh who assisted in the patient’s initial di- agnosis and provided the pathology images included in this report.
References
[1] W. Tang, S. P. McDonald, C. M. Hawley et al., “Anti- glomerular basement membrane antibody disease is an un- common cause of end-stage renal disease,” Kidney In- ternational, vol. 83, no. 3, pp. 503–510, 2013.
[2] A. D. Salama, T. Dougan, J. B. Levy et al., “Goodpasture’s disease in the absence of circulating anti-glomerular basement membrane antibodies as detected by standard techniques,” American Journal of Kidney Diseases, vol. 39, no. 6, pp. 1162–1167, 2002.
[3] K. Benz, K. Amann, K. Dittrich, C. Hugo, K. Schnur, and J. Dotsch, “Patient with antibody-negative relapse of Good- pasture syndrome,” Clinical Nephrology, vol. 67, no. 4, pp. 240–244, 2007.
[4] D. J. Serisier, R. C. Wong, and J. G. Armstrong, “Alveolar haemorrhage in anti-glomerular basement membrane disease
without detectable antibodies by conventional assays,” *o- rax, vol. 61, no. 7, pp. 636–639, 2006.
[5] M. Stolk, D. Carl, and H. D. Massey, “Antibody-negative Goodpasture’s disease,” Clinical Kidney Journal, vol. 3, no. 3, pp. 253–256, 2010.
[6] M. Borkum, G. L. Calligaro, and G. Symons, “A case of anti glomerular basement membrane (GBM) negative good- pasture’s disease,” Journal of Pulmonary & Respiratory Medicine, vol. 4, no. 6, p. 213, 2014.
[7] R. Fernandes, S. Freitas, P. Cunha, G. Alves, and J. Cotter, “Goodpasture’s syndrome with absence of circulating anti- glomerular basement membrane antibodies: a case report,” Journal of Medical Case Reports, vol. 10, no. 1, p. 205, 2016.
[8] M. A. Hellmann, T. M. Gerhardt, C. Rabe, S. Haas, T. Sauerbruch, and R. P. Woitas, “Goodpasture’s syndrome with massive pulmonary haemorrhage in the absence of circulating anti-GBM antibodies?,” Nephrology Dialysis Transplantation, vol. 21, no. 2, pp. 526–529, 2006.
[9] J. B. Levy, A. N. Turner, A. J. Rees, and C. D. Pusey, “Long- term outcome of anti–glomerular basement membrane an- tibody disease treated with plasma exchange and immuno- suppression,” Annals of Internal Medicine, vol. 134, no. 11, pp. 1033–1042, 2001.
[10] C. B. Wilson and F. J. Dixon, “Anti-glomerular basement membrane antibody-induced glomerulonephritis,” Kidney International, vol. 3, no. 2, pp. 74–89, 1973.
[11] F. Dammaco, S. Battaglia, L. Gesualdo, and V. Racanelli, “Goodpasture’s disease: a report of ten cases and a review of the literature,” Autoimmunity Reviews, vol. 12, no. 11, pp. 1101–1108, 2013.
[12] J. D. E. Castellon, P. A. Roche, A. E. Castellon, and C. M. Amada, “*e modifications produced in allergic alveolitis and in Goodpasture’s syndrome due to exposure to cigarette smoke,” Histology and Histopathology, vol. 6, pp. 535–547, 1991.
[13] G. J. Bombassei and A. A. Kaplan, “*e association between hydrocarbon exposure and anti-glomerular basement mem- brane antibody-mediated disease (Goodpasture’s syndrome),”…
Charlene L. Rohm ,1 Sara Acree,2 Aseem Shrivastava,3 Asif A. Saberi,3 and Louis Lovett4
1Department of Internal Medicine, WellStar Kennestone Regional Medical Center, Marietta, GA, USA 2Department of Pathology, WellStar Kennestone Regional Medical Center, Marietta, GA, USA 3Critical Care Medicine, WellStar Kennestone Regional Medical Center, Marietta, GA, USA 4Department of Graduate Medical Education, WellStar Kennestone Regional Medical Center, Marietta, GA, USA
Correspondence should be addressed to Charlene L. Rohm; [email protected]
Received 27 November 2018; Revised 23 March 2019; Accepted 7 April 2019; Published 24 April 2019
Academic Editor: Andre R. Simon
Copyright © 2019 Charlene L. Rohm et al. *is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Goodpasture syndrome is a rare autoimmune disease comprising antiglomerular basement membrane (anti-GBM) crescentic glomerulonephritis and pulmonary capillaritis with circulating anti-GBM antibodies. Rarely, antibody-negative cases have been described.We report a young, African American adult woman admitted with flank pain and hematuria with laboratory testing and kidney biopsy demonstrating anti-GBM crescentic glomerulonephritis with elevated anti-GBM antibody levels. She received treatment but remained dialysis-dependent. She was seronegative and clinically stable until she presented 8months later with dyspnea and hemoptysis requiring mechanical ventilation. Bronchoscopy revealed diffuse alveolar hemorrhage. She was treated for relapse of Goodpasture syndrome. However, anti-GBM antibodies were undetectable. *is case emphasizes prompt diagnosis and treatment of Goodpasture syndrome to preserve renal function. Additionally, clinical manifestations of Goodpasture syndrome and its degree of activity do not necessarily correlate with the actual antibody titer on relapse. Clinicians should have enhanced awareness of this atypical presentation of a rare disease.
1. Introduction
*e estimated incidence of Goodpasture syndrome is one case per million per year [1]. It is mediated by anti-GBM antibody deposition on the alveolar and glomerular basement mem- brane confirmed by immunofluorescence. Most patients present with a combination of rapidly progressive glomer- ulonephritis (RPGN) and pulmonary hemorrhage with a positive anti-GBM antibody titer. However, few cases of antibody-negative relapse of Goodpasture syndrome have been reported. Given the rarity of this disease, both the correct diagnosis of Goodpasture syndrome and the recognition of a relapse are critical in initiating timely and effective treatment. *is case describes a patient diagnosed with Goodpasture syndrome who was clinically stable until she re-presented 8months later with an antibody-negative relapse of Good- pasture syndrome with pulmonary hemorrhage.
2. Case Presentation
A 24-year-old African American woman presented to the emergency department (ED) with several months of recurrent nausea, flank pain, and hematuria. She previously sought care 2weeks prior and was told she had a diagnosis of urinary tract infection (UTI) and was empirically treated with oral ciprofloxacin. However, a urine culture did not grow any organisms, and symptoms persisted despite completing a course of antibiotics. Her past medical history included UTIs for which she received empiric antibiotic treatment, although all urine cultures in her medical chart repeatedly showed no growth of organisms. She was not taking medications. Family history was not significant for any chronic medical illnesses. She smoked cigarettes but denied consuming alcohol or using illicit drugs. On presentation, vital signs were stable and physical examination was significant for bilateral flank pain.
Hindawi Case Reports in Medicine Volume 2019, Article ID 2975131, 5 pages https://doi.org/10.1155/2019/2975131
Laboratory studies included an antinuclear antibody (ANA), rheumatoid factor (RF), complement C3 and C4, human immunodeficiency virus 1 and 2 (HIV 1 and 2) antibody, antineutrophil cytoplasmic antibodies (ANCA), anti-double-stranded DNA (anti-dsDNA) antibodies, and anti-GBM antibodies. All were negative except for anti-GBM antibodies which reported positive 1week later with a titer level of 1.7 (<1.0 is normal). In the interim, a renal biopsy was performed due to rapidly declining renal function. Light microscopy showed necrotizing and crescentic glomerulo- nephritis with fibrocellular crescent formation (Figure 1(a)). Electron microscopy demonstrated widespread podocyte foot process effacement and linear deposits along the glo- merular basement membrane (Figure 1(b)) confirmed as IgG by immunofluorescence (Figure 1(c)). A diagnosis of anti-GBM crescentic glomerulonephritis was made.
Before the confirmatory diagnosis was made by renal biopsy, on day 1 of hospital admission, our patient was treated with methylprednisolone 1 g IV daily for 3 days and then prednisone 40mg by mouth daily for 1month. Once the renal biopsy confirmed anti-GBM crescentic glomeru- lonephritis along with serologies positive for anti-GBM antibody, intravenous cyclophosphamide and plasma ex- change were both initiated on day 9 of hospitalization. She received cyclophosphamide 1 g IV every 2weeks for 3 oc- currences. She received plasma exchange daily for 7 days then every other day for 3 occurrences. Plasma exchange was stopped once repeat testing for anti-GBM antibodies was undetectable on day 23. Due to rapidly progressing renal failure, she required initiation of hemodialysis on day 4 of admission and continued to require hemodialysis daily throughout her hospital stay. Our patient was discharged to home on day 28 with outpatient nephrology follow-up and hemodialysis three times a week. Anti-GBM antibody levels remained undetectable. Kidney transplant evaluation was initiated.
Eight months later, our patient presented to the ED with dyspnea and hemoptysis. She last received dialysis the day before admission and had not missed any dialysis sessions. Social history was notable for marijuana use daily for a week prior to admission. She appeared diaphoretic and drowsy with decreasing oxygen saturation despite supplemental oxygen. Physical examination was significant for tachycar- dia, tachypnea, reduced air movement in all lung fields, and dullness to percussion of the thorax. A portable chest ra- diograph showed diffuse bilateral patchy opacities (Fig- ure 2). A computerized tomography angiography (CTA) of
the chest with IV contrast confirmed diffuse bilateral con- solidations (Figure 3). Our patient required tracheal in- tubation and mechanical ventilation with admission to the intensive care unit (ICU).
Our patient had a hemoglobin level of 6.4 g/dL, he- matocrit of 21%, and MCV of 95 fL which dropped to as low as a hemoglobin and hematocrit of 5.6 g/dL and 18%, re- spectively. *ree weeks prior to admission, hemoglobin was 8.7 g/dL and hematocrit was 26%. Flexible fiberoptic bronchoscopy was performed, and the bronchoalveolar la- vage (BAL) fluid was consistent with alveolar hemorrhage (Figure 4). *e lavage fluid was negative for malignant cells, bacterial, viral, or fungal organisms.
Repeat ANA, ANCA, and anti-dsDNA remained neg- ative. Unlike on initial presentation, repeat anti-GBM an- tibody levels were undetectable, which did not result until day 7 of the hospital stay. Given our patient’s history, a relapse of Goodpasture syndrome with pulmonary hem- orrhage was diagnosed. While the most likely diagnosis was a relapse of Goodpasture syndrome, acute heart failure was also included in the differential diagnosis. However, a transthoracic echocardiogram demonstrated a normal ejection fraction of 55–60%, normal left ventricular diastolic function, normal right ventricular systolic and diastolic function, mild tricuspid valve regurgitation with no other valvular abnormalities, an elevated pulmonary artery pres- sure of 50mmHg, and a normal central venous pressure. *ese findings were not suggestive of heart failure; rather, functioning of both left and right ventricles was intact, while the elevated pulmonary artery pressure was suggestive of a primary intrapulmonary process (pulmonary hemorrhage). Starting on day 1, she was treated with methylprednisolone 1 g daily for 5 days, and then changed to prednisone 40mg daily. Plasma exchange was also initiated on day 1 which she received daily for 5 occurrences. She was treated with mycophenolate 500mg IV every 12 hours for 5 days. She progressively improved clinically with resolved alveolar hemorrhage and was extubated on day 5. She was transferred to the medical ward in stable condition. On day 10, she was discharged to home with outpatient nephrology follow-up and continued dialysis.
Our patient was stable following her admission for Goodpasture syndrome relapse. She continued to have outpatient hemodialysis 3 times a week. She did not require outpatient oral steroids or immunosuppression. However, 9months later, we received the news that she had passed away from a drug overdose.
3. Discussion
Our patient’s urinalysis suggested a glomerulonephritis based on the presence of proteinuria, hematuria, and red cell casts. Subsequently, the diagnosis of RPGN was suspected because of rapidly progressive renal failure. RPGN com- prises 3 subtypes: immune-complex glomerulonephritis, pauci-immune glomerulonephritis, and anti-GBM glomer- ulonephritis (Goodpasture syndrome). Both anti-GBM and immune-complex glomerulonephritis demonstrate glo- merular staining for immunoglobulins, while pauci-immune
2 Case Reports in Medicine
glomerulonephritis has an absence or paucity of immunoglobulins.
Immune-complex glomerulonephritis is associated with systemic lupus erythematosus (SLE), immunoglobulin A (IgA) glomerulonephritis, IgA vasculitis, and postinfectious
glomerulonephritis. Our patient had negative ANA and anti-dsDNA antibodies, did not have symptoms suggestive of IgA vasculitis, and was previously healthy with no recent illnesses. Pauci-immune glomerulonephritis is associated with granulomatosis with polyangiitis, eosinophilic gran- ulomatosis with polyangiitis, and microscopic polyangiitis. Our patient had negative MPO-ANCA and PR3-ANCA levels which lower suspicion for their associated diseases.
While the best laboratory predictor of Goodpasture syndrome is serologic detection of anti-GBM antibodies, this serology takes several days to result. Rarely patients can have antibody-negative Goodpasture syndrome so that diagnosis is based on renal biopsy and clinical presentation. Our patient did have a positive anti-GBM antibody level. Light microscopy of her renal specimen showed that 95% of glomeruli had crescent formation. Immunofluorescence demonstrated linear deposits of IgG antibodies along the glomerular basement membrane, which is pathognomonic for anti-GBM glomerulonephritis. Based on our patient’s history and physical examination, urinary studies, rapidly progressive disease course, serologies, and renal biopsy, a
Figure 3: CTA of the chest with IV contrast reveals extensive bilateral consolidations.
Figure 4: Progressive increase in intensity of blood in sequential aliquots during BAL strongly suggests active alveolar hemorrhage.
(a) (b) (c)
Figure 1: (a) Light microscopy reveals glomeruli with cellular to focally fibrocellular crescent formation and underlying segmental tuft fibrinoid necrosis. Red blood cell casts are noted. *ere is severe mononuclear inflammation within the interstitium (H&E, 10x). (b) Electron microscopy demonstrates peripheral capillary loops of normal thickness and architecture with widespread effacement of the overlying foot processes. (c) Immunofluorescencemicroscopy shows strong linear staining along glomerular basementmembranes with IgG (4+) and kappa and lambda light chains (3-4+).
Figure 2: Portable chest radiograph demonstrates diffuse bilateral patchy opacities.
Case Reports in Medicine 3
diagnosis of anti-GBM glomerulonephritis (Goodpasture syndrome) was made.
Eight months later, our patient presented with dyspnea and hemoptysis. *e differential diagnosis for hemoptysis and dyspnea is broad, including infectious, immunological, or malignant etiologies. Given the hemoptysis, severe ane- mia, and chest imaging showing widespread opacities, there was a concern for hemorrhage. Our patient had no clinical history suggestive of an infectious process. Additionally, a BAL fluid analysis did not suggest an infection (no organism seen, rare WBCs, and no bacterial or fungal isolates). A respiratory infection panel which detects a variety of bacteria and viruses in the BAL fluid also returned negative. Negative ANA and anti-dsDNA antibody serologies ruled out rheumatologic disorders. Negative MPO-ANCA and PR3- ANCA serologies effectively ruled out ANCA-associated disorders.
Anti-GBM antibody levels were also undetectable. However, given our patient’s history of Goodpasture syn- drome, she likely had a relapse of Goodpasture syndrome with pulmonary hemorrhage.
Over 90% of patients with Goodpasture syndrome have circulating anti-GBM antibodies detectable by enzyme- linked immunosorbent assay (ELISA) [2]. ELISA for anti- GBM antibodies is highly sensitive (>95%) and specific (>97%) [2]. All positive results are confirmed by western blotting on collagenase-solubilized human GBM. *ese assays are rarely negative despite deposition of anti-GBM antibody in the kidney [2]. Although rare, the absence of circulating anti-GBM antibody in the setting of Goodpasture syndrome has been described [3–8]. A review of 6 reports revealed that each Goodpasture syndrome diagnosis had seronegative disease with diagnosis confirmed on renal biopsy. Database review shows that ELISA- and western blot-negative anti-GBM disease may occur in up to 2-3% of patients, requiring renal biopsy confirmation [2]. *erefore, while clinicians may rely on serological detection of cir- culating anti-GBM antibodies, the early renal biopsy dem- onstrating linear deposition of immunoglobulin along the GBM with crescentic glomerulonephritis remains the gold standard to diagnose Goodpasture syndrome.
*e average time to anti-GBM antibody result reporting for our patient was 7 days since this test was not done in- house. When our patient was first diagnosed with Good- pasture syndrome, she had an elevated anti-GBM antibody level of 1.7. During the subsequent hospital stay for relapse of Goodpasture syndrome, anti-GBM antibody was un- detectable by the same commercial ELISA kit BioPlex 2200 Vasculitis (Bio-Rad, Hercules, California). *is immuno- assay uses as antigen the extracted highly purified human alpha-3 chain of type IV collagen. An indirect fluorescent antibody (IFA) test was not performed. A western blot was not performed.
Prompt diagnosis and treatment of Goodpasture syn- drome is critical as it affects the disease course and prog- nosis. *e best predictor of outcomes for crescentic glomerulonephritis is based on serum creatinine and need for immediate hemodialysis. Levy et al. found that if
treatment is initiated when serum creatinine is<5.7mg/dL, patient and renal survival rates at 1 year are 100% and 95%, respectively [9]. Once serum creatinine is 5.7mg/dL or higher and without need for immediate dialysis, 1-year patient and renal survival decreased to 83% and 82%, re- spectively [9]. If treatment was initiated when patients presented with dialysis-dependent renal failure, 1-year pa- tient and renal survival was only 65% and 8%, respectively [9]. Our patient may have received an earlier diagnosis of Goodpasture syndrome had her prior urinalyses been more critically assessed for a glomerulonephritis rather than a UTI. Our patient had been told by prior physicians that her recurrent symptoms of nausea, flank pain, and hematuria were due to UTIs, despite multiple urine cultures demon- strating no growth of organisms and no resolution of symptoms with antibiotic treatment. She had incorrect di- agnoses of UTI in her past medical history. Her urinalysis showed significant amounts of red blood cells, protein, and red cell casts, which are all suggestive of glomerular disease. Specifically, she had a nephritic syndrome. Furthermore, an FENa of 2.8% and a BUN/Cr ratio of 7 suggested intrarenal damage. When presented with such urinary studies, glo- merulonephritis should be suspected. In the setting of a rapid decline in renal function, RPGN is likely. A renal biopsy should not be delayed. Unfortunately in our patient, treatment with plasma exchange and immunosuppression was not initiated until she had developed dialysis-dependent renal failure.
Patients with Goodpasture syndrome typically present with acute renal failure secondary to RPGN. *is can be associated with pulmonary hemorrhage. While most pa- tients present with a combination of RPGN and pulmonary hemorrhage, 30–40% present with an isolated renal in- volvement and 40–60% present with an isolated pulmonary hemorrhage [10, 11]. As in our patient, other cases of relapse with pulmonary hemorrhage have been reported [3, 4, 12–16]. Environmental factors such as cigarette smoking, drug use, and hydrocarbon solvents have been implicated in triggering pulmonary hemorrhage [3, 4, 12–16]. Our patient’s ongoing exposure to cigarettes plus her recent use of marijuana may have precipitated a Goodpasture relapse with pulmonary hemorrhage. Relapses resulting in pulmonary disease are strongly correlated with cigarette smoking, which causes inhalation injury leading to alveolar damage. It is possible that subjects with Good- pasture syndrome develop pulmonary hemorrhage when exposed to the right precipitant. Volatile hydrocarbons, cigarette smoking, concurrent infection, high concentration of inspired oxygen, and fluid overload have all been im- plicated [4].
In conclusion, Goodpasture syndrome is a rare syn- drome with variable patterns of presentation. Obtaining a kidney biopsy early and promptly initiating steroids and immunosuppression is critical in preserving renal function and minimizing morbidity and mortality. Goodpasture syndrome must also be considered despite the absence of anti-GBM antibody, as disease activity does not necessarily correlate with antibody titer.
4 Case Reports in Medicine
3.1. Learning Points
(i) Critically evaluate urinalysis. Consider glomerulo- nephritis in the setting of hematuria, proteinuria, and red cell casts.
(ii) Do not delay performing a renal biopsy to de- finitively diagnose Goodpasture syndrome. Mor- tality significantly increases once hemodialysis is required.
(iii) Isolated pulmonary hemorrhage can occur as the sole manifestation of relapse in Goodpasture syn- drome. *is can occur in the absence of detectable antibody levels.
(iv) Current evidence suggests that the clinical mani- festations of Goodpasture syndrome and its degree of activity do not necessarily correlate with the actual antibody titer.
Disclosure
*e case abstract has previously been presented at the So- ciety of General Internal Medicine Southern Regional Meeting in February 2017 in New Orleans, Louisiana, and at the Society of Hospital Medicine meeting in May 2017 in Las Vegas, Nevada. *e abstract has been published in the Journal of Hospital Medicine 2017. *is manuscript has not been published, accepted for publication, nor is it under editorial review for publication elsewhere.
Conflicts of Interest
All the authors declare that there are no conflicts of interest regarding the publication of this article.
Acknowledgments
We thank Dr. Salvatore Chillemi who was directly involved in the diagnosis, treatment, and management of this patient during her stay in the intensive care unit. We thank Dr. Harsharan Singh who assisted in the patient’s initial di- agnosis and provided the pathology images included in this report.
References
[1] W. Tang, S. P. McDonald, C. M. Hawley et al., “Anti- glomerular basement membrane antibody disease is an un- common cause of end-stage renal disease,” Kidney In- ternational, vol. 83, no. 3, pp. 503–510, 2013.
[2] A. D. Salama, T. Dougan, J. B. Levy et al., “Goodpasture’s disease in the absence of circulating anti-glomerular basement membrane antibodies as detected by standard techniques,” American Journal of Kidney Diseases, vol. 39, no. 6, pp. 1162–1167, 2002.
[3] K. Benz, K. Amann, K. Dittrich, C. Hugo, K. Schnur, and J. Dotsch, “Patient with antibody-negative relapse of Good- pasture syndrome,” Clinical Nephrology, vol. 67, no. 4, pp. 240–244, 2007.
[4] D. J. Serisier, R. C. Wong, and J. G. Armstrong, “Alveolar haemorrhage in anti-glomerular basement membrane disease
without detectable antibodies by conventional assays,” *o- rax, vol. 61, no. 7, pp. 636–639, 2006.
[5] M. Stolk, D. Carl, and H. D. Massey, “Antibody-negative Goodpasture’s disease,” Clinical Kidney Journal, vol. 3, no. 3, pp. 253–256, 2010.
[6] M. Borkum, G. L. Calligaro, and G. Symons, “A case of anti glomerular basement membrane (GBM) negative good- pasture’s disease,” Journal of Pulmonary & Respiratory Medicine, vol. 4, no. 6, p. 213, 2014.
[7] R. Fernandes, S. Freitas, P. Cunha, G. Alves, and J. Cotter, “Goodpasture’s syndrome with absence of circulating anti- glomerular basement membrane antibodies: a case report,” Journal of Medical Case Reports, vol. 10, no. 1, p. 205, 2016.
[8] M. A. Hellmann, T. M. Gerhardt, C. Rabe, S. Haas, T. Sauerbruch, and R. P. Woitas, “Goodpasture’s syndrome with massive pulmonary haemorrhage in the absence of circulating anti-GBM antibodies?,” Nephrology Dialysis Transplantation, vol. 21, no. 2, pp. 526–529, 2006.
[9] J. B. Levy, A. N. Turner, A. J. Rees, and C. D. Pusey, “Long- term outcome of anti–glomerular basement membrane an- tibody disease treated with plasma exchange and immuno- suppression,” Annals of Internal Medicine, vol. 134, no. 11, pp. 1033–1042, 2001.
[10] C. B. Wilson and F. J. Dixon, “Anti-glomerular basement membrane antibody-induced glomerulonephritis,” Kidney International, vol. 3, no. 2, pp. 74–89, 1973.
[11] F. Dammaco, S. Battaglia, L. Gesualdo, and V. Racanelli, “Goodpasture’s disease: a report of ten cases and a review of the literature,” Autoimmunity Reviews, vol. 12, no. 11, pp. 1101–1108, 2013.
[12] J. D. E. Castellon, P. A. Roche, A. E. Castellon, and C. M. Amada, “*e modifications produced in allergic alveolitis and in Goodpasture’s syndrome due to exposure to cigarette smoke,” Histology and Histopathology, vol. 6, pp. 535–547, 1991.
[13] G. J. Bombassei and A. A. Kaplan, “*e association between hydrocarbon exposure and anti-glomerular basement mem- brane antibody-mediated disease (Goodpasture’s syndrome),”…
Related Documents