ANTIBIOTICS IN PEDIATRICS Presented by: Dr. pawan sinsinwar Guided by: Dr. kumar raghav Dr. shefali chaturvedi Dr. tarun sethi

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ANTIBIOTICS IN PEDIATRICS
Presented by:Dr. pawan sinsinwar
Guided by:Dr. kumar raghav
Dr. shefali chaturvediDr. tarun sethi
Antibiotics Act By Inhibition Of Protein
Synthesis•Tetracycline•Chloramphenicol•Aminoglycosides•Macrolides

TETRACYCLINES

From Actinomycetes
The tetracycline's still available in lndia for clinical use are: Tetracycline Oxytetracycline Demeclocycline Doxycycline Minocycline

Mechanism Of Action
1- Aminoglycosides2- Tetracycline3- Chloremphenicol4- Erythromycin

Broad-spectrum antibiotic
Promiscuous and often indiscriminate use has gradually narrowed the field of their usefulness.
1. Cocci 2. Most gram-positive bacilli 3. Gram-negative bacilli 4. Spirochetes, T. Pallidum 5. All rickettsiae (typhus, etc.) And chlamydiae are highly
sensitive. 6. Mycoplasma and actinomyces are moderately sensitive. 7. Entamoeba histolytica and plasmodia are inhibited at
high concentrations.
Antimicrobial Spectrum

The older tetracycline's are incompletely absorbed from GIT; absorption is better if taken in empty stomach.
Doxycycline and minocycline are completely absorbed irrespective of food.
Tetracycline's have chelating property-form insoluble and unabsorbable complexes with calcium and other metals.
Milk, iron preparations,nonsystemic antacids and sucralfate reduce their absorption.
Pharmacokinetics

They are concentrated in liver, spleen and bind to the connective tissue in bone and teeth.
Intracellularly, they bind to mitochondria.
Minocycline accumulates in body fat.

Most tetracycline's are primarily excreted in urine by glomerular filtration;
Doxycycline is an exception to this.
They are secreted in milk in amounts sufficient to affect the suckling infant.

1. Tetracycline: ACHROMYCIN, HOSTACYCLINE,RESTECLIN 250, 500 mg cap, 3% skin oint, 1% ear/eye drops and oint.
2. Oxytetracycline: TERRAMYCIN 250, 500 mg cap, 50 mg/ml in 10 ml vials inj;3% skin oint, 1% eye/ear drop and oint.
Preparations

3.Demeclocycline (Demethylchlortetracycline) LEDERMYCIN 150, 300 mg cap/tab.
4.Doxycycline: TETRADOX, BIODOXI, DOXT,NOVADOX 100 mg cap
5.Minocycline: CYANOMYCIN 50, 100 mg caps

Although tetracycline's are broad-spectrum antibiotics, they should be employed only for those infections for which a more selective and less toxic AMA is not available.
Clinical use declined due to fluoroquinolones and other efficacious AMAs.
Uses
The nature and sensitivity of the infecting organism cannot be reasonably guessed
Initial treatment of mixed infections
1. Empirical Therapy
(A) Venereal Diseases
(B) Atypical Pneumonia
(C) Cholera
(D) Brucellosis
(E) Plague
(F) Relapsing Fever
(G) Rickettsial Infections
2. Tetracyclines Are The First Choice

To Penicillin/Ampicillin To Ceftriaxone To Azithromycin For Pneumonia To Ceftriaxone/Azithromycin For Chancroid. To Streptomycin For Tularemia.
3. Tetracycline's Are Second Choice Drugs
(A) Urinary Tract Infections (B) Community Acquired pneumonia (C) Amoebiasis (D) As Adjuvant To Quinine Or Sulfadoxine (E) Acne Vulgaris (F) Chronic Obstructive Lung Disease
4. Other Situations In Which Tetracyclines May Be Used

Acute orofacial infections Chronic adult periodontitis Localized juvenile periodontitis Subgingivally
Dental use

Adverse Effects

Esophageal ulceration especially with doxycycline.
Intramuscular injection of tetracycline's are very painful; thrombophlebitis of the injected vein can occur, especially on repeated use
IRRITATIVE EFFECTS

1. Liver damage Fatty infiltration of liver and jaundice occur Pregnant women; can precipitate acute hepatic
necrosis which may be fatal.
2. Kidney damage In the presence of existing kidney disease. Except doxycycline, accumulate and enhance
renal failure. A reversible fancony syndrome llke condition is
produced by outdated tetracyclines
3. Phototoxicity
Dose Related Toxicity

4. Teeth and bones
Brown discoloration, ill-formed teeth, more susceptible to caries.
Tetracyclines have chelating property Calcium-tetracycline chelate gets deposited in
developing teeth and bone. Given from midpregnancy to 5 months of extra
uterine life, deciduous teeth are affected. 3 months and 6 years of age affect the crown
of permanent anterior dentition. Late pregnancy or childhood, temporary
suppression of bone growth. Deformities and reduction in height are a
possibility with prolonged use.
First, the ‘extrinsic theory’ (Berger et al. , 1989), Tetracycline attaches to the glycoproteins in acquired pellicles. This in turn etches the enamel, and demineralization/
remineralization cycles occur. It oxidizes on exposure to air or as a result of bacterial activity,
and so causes degradation of the aromatic ring, forming insoluble black quinone.
The second is the ‘intrinsic theory’ (Bowles and Bokmeyer, 1997; Bowles, 1998),
Where the tetracycline bound to plasma proteins is deposited in collagen rich tissues, such as teeth.
This complex oxidizes slowly over time with exposure to light. This deposition in teeth occurs solely within the dentin matrix as secondary and reparative dentin is formed
Mechanism of tetracycline staining

5. Antianabolic effect Reduce protein synthesis and have an overall catabolic
effect. They induce negative nitrogen balance and can
increase blood urea.
6. Increased intracranial pressure Noted in some infants.
7. Diabetes insipidus Demeclocycline antagonizes ADH action and reduces
urine concentrating ability of the kidney.
8. Vestibular toxicity Minocycline has produced ataxia, vertigo and
nystagmus, which subside when the drug is discontinued.

Resistance to tetracycline develops slowly in a graded manner.
Tetracycline concentrating mechanism becomes less efficient or the bacteria acquire capacity to pump it out.
Plasmid mediated synthesis of a 'protection‘ protein which protects the ribosomal binding site from tetracycline.
Resistance

Infrequent with tetracycline's.
Skin rashes, urticaria, glossitis, pruritus ani and vulvae, even exfoliative dermatitis have been reported.
Angioedema and anaphylaxis are extremely rare.
Hypersensitivity

The tetracycline should be discontinued at the first sign of superinfection and appropriate therapy instituted.
Doxycycline and minocycline are less liable to cause diarrhoea, because only small amounts reach the lower bowel
Superinfection
1. Not be used during pregnancy, lactation and in children.
2. Avoided in patients on diuretics: blood urea may rise in such patients.
3. Used cautiously in renal or hepatic insufficiency.
4. Never be used beyond their expiry date.
5. Do not mix injectable tetracycline's with penicillin-inactivation occurs.
6. Do not inject tetracycline's intrathecally.
Precautions

CHLORAMPHENICOL


Chemical structure

Mechanism Of Action
1- Aminoglycosides2- Tetracycline3- Chloremphenicol4- Erythromycin

Antimicrobial spectrum

Completely absorbed after oral administration,
Bound to plasma protein (approximately 60%) and widely distributed in body.
Crosses the blood-brain and placental barrier and shows its presence in csf, bile and milk.
It is conjugated with glucuronic acid in liver and excreted in urine.
Small amount is excreted in urine in unchanged form.
Pharmacokinetics

Because of Bone Marrow Toxicity its use is restricted to
the treatment of infection caused by S. Typhi And
Paratyphi
Other - H. Influenzae Meningitis, Urinary Tract
Infections, Anaerobic Infections Caused By Bacteroides Fragilis
And Locally In Eye And External Ear Infections.
Therapeutic Uses
Adverse Effects

Aminoglycosides
Bactericidal Antibiotics Various Streptomyces Species

Chemical structure

Act By Inhibiting Protein Synthesis Of Bacteria By Directly Combining With Ribosomes.
Other Aminoglycosides Bind To Additional Sites On 50s Subunit As Well As To 30s-50s Interface.
Mechanism of action

Mechanism Of Action
1- Aminoglycosides2- Tetracycline3- Chloremphenicol4- Erythromycin

Poorly absorbed after oral administration,
More active in alkaline ph
Excreted unchanged by glomerular filtration accumulation occurs in renal impairment.
Pharmacokinetics

All Aminoglycosides produce cochlear and vestibular damage (Ototoxicity) And Nephrotoxicity.
Reduce the acetylcholine release from motor nerve endings and cause neuromuscular blockade.
Adverse effects

STREPTOMYCIN
Used In All Tuberculosis Along With Antitubercular Drugs.
Other Indications: Tularemia, Plague, Brucellosis, Bacterial Endocarditis, Enterococcal Endocarditis.
Used concomitantly with Penicillin G for synergistic effect in the treatment of Enterococcal Endocarditis when other antibiotics are ineffective or contraindicated

Pain At Injection Site
Ototoxicity
Nephrotoxicity
Skin Rash
FeverExfoliative Dermatitis
Eosinophilia
Anaphylaxis Rarely
Optic Nerve Dysfunction
Adverse effects

AMIKACIN

From Streptomyces
Kanamyceticus.
Active Against Pseudomonas
Severe Ototoxicity And Nephrotoxicity
Replaced By Other
Aminoglycosides
Occasionally Used In
Multidrug Resistant Cases Of
Tuberculosis.
Kanamycin

From Streptomyces
Fradiae
Effective Against Most
Gram Negative
Bacilli And Some Gram
Positive Cocci.
High Ototoxicity
And Nephrotoxicity
,
Not Systemically Used Locally Skin And Eye
Infections.
Neomycin
Sulfonamides
Derivatives Of Sulfanilamide (P-
aminobenzene Sulfonamide)
First Antimicrobial Agents Effective Against Pyogenic
Bacterial Infections

Chemical structure

Sulfanilamide exhibits a structural similarity to para-amino benzoic acid (PABA).
WOODS AND FIELDS proposed theory that sulfonamides, inhibit bacterial FOLATE SYNTHETASE so folic acid is not formed which is needed for a number of metabolic reactions.
Causes FOLIC ACID deficiency and ultimately cause injury to the bacterial cell.
Mechanism of action


Bacteriostatic Antibacterial Activity Against Gram
Positive And Gram Negative Organisms ,
Certain Species Of Chlamydia
Infections Such As: Streptococci,
Staphylococci, Pneumococci, Gonococci,
Meningococci,.
Haemophilus Influenzae, Granulomatis, Vibrio
Comma, Vibrio Cholerae, E. Coli, Pasteurella Pestis,
Shigella
Antimicrobial spectrum

rapidly and completely
absorbed from GIT mainly in small
intestine
Binding with plasma proteins
differ considerably
among different groups.
The highly plasma protein
bound sulfonamides have longer
action.
Pharmacokinetics

I. Urinary Tract Infection
Ii. Acute Bacillary Dysentery Iii. Ulcerative Colitis
Iv. Streptococcal Pharyngitis, And
Tonsillitis.
V. Trachoma And Inclusion
Conjunctivitis:Vi. Chancroid
Vii. Meningococcal Meningitis.
Viii. Chloroquine Resistant Malaria Ix. Toxoplasmosis
X. Burns
Therapeutic uses
Adverse reactions
Allergic Symptoms Drug Fever, Skin Rash, Urticaria, Eosinophilia,
Photosensitization Reactions, Serum Sickness Like Syndrome.
Stevens- Johnson Syndrome And Exfoliative Dermatitis Are Also Common
With Longer Acting Agents Uncommon Allergic Reactions Acute Toxic Hepatitis, Toxic Nephrosis And
Acute Haemolytic Anaemia.
Renal Irritation And May Precipitate Renal Colic. Crystalluria, Haematuria And Albuminuria Can
Occur May Lead To Oliguria And Anuria.
Hematopoietic Toxicity Agranulocytosis, Thrombocytopenia And Rarely Aplastic
Anaemia Patients With G-6- Pd Deficiency,Cause Intravascular
Haemolysis.
The Other CNS Effects Include Depression, Confusion, Tinnitus,
Fatigue Etc.
Trimethoprim
Therapeutic usesInfection caused by salmonella typhi, klebsiella, enterobacter,pneumocystis carinii etc
And many other sulfonamide resistant strains of s. Aureus,strep. Pyogenes, shigella, e. Coli, h. Influenzae, meningococci and gonococci etc.
Effective as a second line agent in penicillin allergic patients where newer antibiotics are contraindicated or can’t be used.

UT IAcute
Cystitis
Bacterial Diarrhoea And
Dysentery.
Respiratory Tract Infection - Chronic
Bronchitis And Otitis Media Etc.
Typhoid.Nosocomial Infections
Chancroid
Sexually Transmitted
Diseases
Prophylaxis And Treatment HIV
Associated Infections
Prophylaxis - Organ
Transplantation
Patients Receiving
Immunosuppressants
The common indications are:

Quinolones


Quinolone Block bacterial DNA synthesis by inhibiting bacterial Topoisomerase II (DNA Gyrase)
and Topoisomerase IV
Inhibition of DNA gyrase prevents the relaxation of positively
supercoiled DNA that is required for normal transcription and
replication.
Mechanism of action

It is 4-QUINOLONE derivative effective against gram negative bacteria mainly E. Coli and Shigella.
Acts by inhibiting bacterial DNA GYRASE.
Used as urinary antiseptic and in diarrhea caused By E. Coli, Shigella,salmonella.
The side effects are GIT upset, Headache, Drowsiness, Vertigo, Visual Disturbances and on prolonged use can produce parkinsonism like symptoms.
In Individuals with G-6-PD deficiency can cause haemolysis.
Nalidixic acid
Quinolone AMAs having one or more fluorine substitutions, relatively broad spectrum of action and effective against gram positive And gram negative organisms.
They are highly effective against E. Coli, Klebsiella, Proteus Mirabilis, Shigella, Salmonella Species, H. Ducreyi Etc.
Fluoroquinolones

The presence of a 6-fluoro and 7- piperazine substitution greatly enhances their antimicrobial efficacy as compared to nalidixic acid.
The fluorine atom is responsible for increased potency against gram negative organisms and broadens the spectrum of their activity including gram positive organism.
Mechanism of action

After oral administration, well absorbed with the bioavailability Of 80 to 95 % and distributed widely in body fluids and tissues.
The fluoroquinolones are excreted mainly by tubular secretion and by glomerular filtration.
Pharmacokinetics

UTI
Dental UseNot indicated in acute
orofacial infectionsCiprofloxacin may be
used in rapidly progressive or
refractory periodontitis
Bacterial gastroente
ritis.
Typhoid fever.
Septicemia.
Otitis media.
Acute pneumonia
Ocular infections
Therapeutic uses

Fluoroquinolones are well tolerated.
Tendinitis is rarely reported in adults. Because of cartilage damage in children it must be used under close supervision.
Phototoxicity Reported With Pefloxacin, Lomefloxacin, Sparfloxacin And Ofloxacin.
Adverse effects

Most potent first generation fluoroquinolone,
Aerobic gram negative bacilli.
Higher concentration in the urine than plasma.
Produces rapid and complete clinical relief in nosocomial bronchopneumonia
Used prior to cardiac surgery and has attained levels higher than mics for at least 8 hours.
Ciprofloxacin
It is more potent than ciprofloxacin for gram positive organisms.
It also inhibits Mycobacterium tuberculosis and mycobacterium leprae and used as alternative in multidrug resistant therapeutic regimens.
It is also used in the treatment of chronic bronchitis and other ENT infections.
Ofloxacin
It is the levoisomer of ofloxacin and having better activity than ciprofloxacin and ofloxacin against s. Pneumoniae.
It is also used in chronic bronchitis, sinusitis, pyelonephritis, and other related infections of soft tissues.
Due to high oral bioavailability, patient can be shifted from Iv to oral therapy.
It can be administered just once a day regimen as an alternate to other fluoroquinolones in the treatment of respiratory infections.
Levofloxacin

It is less potent than ciprofloxacin
Primarily used in genitourinary tract infections.
It is not useful in respiratory and systemic infections due to gram positive cocci.
Norfloxacin
It is Difluorinated quinolone effective against gram positive bacteria, anaerobes and mycobacteria.
It is used in the treatment of pneumonia, chronic bronchitis, sinusitis etc.
Sparfloxacin

Macrolide antibiotics
Macrolides, as their name indicates are characterized by a large or macrocyclic lactone ring with attached sugar residue
First macrocyclic antibiotic From streptomyces erythreus.
Widely used antibiotic both in children as well as in adults.
It acts by binding with 50s ribosomal subunit of bacteria and inhibit protein synthesis.
Narrow spectrum, low concentration are bacteriostatic, however high concentrations are bactericidal.
Erythromycin

Mechanism Of Action
1- Aminoglycosides2- Tetracycline3- Chloremphenicol4- Erythromycin

The spectrum of activity also depends on the concentration of drug. It is more active in alkaline medium.
Effective against gram positive and few gram negative organisms
Also effective against penicillin resistant staphylococci, mycoplasma, campylobacter, legionella, gardnerella vaginalis are also highly sensitive.

Substitute to penicillin in allergic patients for upper respiratory tract infections, prophylaxis of rheumatic fever.
Atypical pneumonia due to mycoplasma pneumoniae,and whooping cough.
Wound and burn infections and severe impetigo not responding to topical antibiotics.
Therapeutic uses
Dental uses
Acute Orofacial Infection- Erythromycin
Acute Periapical Abscesses- Azithromycin
IE Prophylaxis

Gastrointestinal side effects like nausea, epigastric pain are common. Diarrhoea occurs occasionally.
Skin rashes, hypersensitivity reaction, hepatotoxicity Oral candidiasis, thrombophlebitis and fever have been reported.
Adverse effects

Azithromycin is an azalide antibiotic, a sub-class of the macrolides.
Azithromycin differs chemically from erythromycin in that a methyl substituted nitrogen atom is incorporated into the lactone ring.
oral administration, rapidly absorbed and widely distributed throughout the body.
Rapid distribution into tissues and high concentration within cells result in significantly higher azithromycin concentration is tissues than in plasma or serum.
Azithromycin

1. Lower respiratory tract infections:
2. Ear, nose and throat infections like tonsillitis, sinusitis, otitis media and pharyngitis.
3. Skin infections
Therapeutic uses

Adverse reactions include vomiting, dyspepsia, flatulence, jaundice, palpitations, chest pain. Allergic reactions include rash, photosensitivity and angioedema.
CNS side effects are headache, dizziness, vertigo and fatigue.
Adverse effect

Nitroimidazoles are imidazole heterocyclic compounds with a nitro group that have been used to combat anaerobic bacterial and parasitic infection .
Nitroimidazoles:
Anaerobic cocciAnaerobic gram –ve bacilli including bacteroidsAnaerobic spore-forming gram +ve bacilliAerobic and Facultative anaerobic bacteria
Metronidazole :

After entering the micro-organisms by
diffusion , its nitro group is reduced to
intermediate compounds which cause
cytotoxicity probably by damaging DNA.
Dose: 200,400 mg TDS
Mechanism of action
INDICATIONAmoebiasisAnaerobic
bacterial inf.Ulcerative Gingivitis
CONTRAINDICATION
In neurological
diseasesChronic
AlcoholismFirst
trimester of pregnancy
ADVERSE EFFECT
Anorexia, Nausea
Abdominal cramps
Metallic tasteHeadache ,
GlossitisRashes,
DizzinessSeizures,
Thrombophelbitis
Clinical Application
Non-indicated Cases for Antibiotic Prescription:
Acute Periapical Infection
Dry Socket Acute Pulpitis Chronic Marginal
Gingivitis Chronic Periodontitis
Indications for the Use of Antibiotics in Dentistry:
Oral infection accompanied by elevated body temperature,
Evidence of systemic spread, Facial cellulitis and/or
dysphagia. Periodontal abscess Acute nercotizing ulcerative
gingivitis Sinusitis Pericoronitis

Dental Procedures Requiring Antibiotic Coverage (2007
Guidelines) All dental procedures that involve manipulation
of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Suture removal
Extractions
Periodontal procedures (scaling, root planing, probing, surgery, recall maintenance)
Dental Procedures Requiring Antibiotic Coverage (2007 Guidelines)
Implant placement and reimplantation of avulsed teeth
Placement of orthodontic bands
Bacteremia is anticipated following invasive dental procedures
Infective endocarditis is an uncommon but life-threatening complication resulting from bacteremia
AAPD GUIDELINES 2012 ON ANTIBIOTIC PROPHYLAXIS

1. Prosthetic cardiac valve or prosthetic material used for cardiac valve repair
2. Previous IE
3. Congenital heart diseasea. Unrepaired cyanotic CHDb. Completely repaired defect with prosthetic material for 6months
after procedurec. Repaird CHD with residual defects
4. Cardiac transplant pts who develop cardiac valvulopathy
WHICH PATIENTS?

WHICH PROCEDURES? All dental procedures that involve
manipulation of gingival tissue
WHICH PROCEDURES DO NOT? LA through non-infected tissue, X-rays, Placement of removable prosthodontic or orthodontic
appliances, Placement of brackets, Shedding of deciduous teeth, Bleeding from trauma to the lips or oral mucosa

ABLE TO TAKE ORAL MEDS?-Amoxicillin 50mg/kg
UNABLE TO TAKE ORAL MEDS?-Ampicillin or Cefazolin 50mg/kg IV/IM
ALLERGIC TO PCN, ORAL?-Clindamycin 20mg/kg or Azithromycin/Clarithromycin 15mg/kg
ALLERGIC TO PCN, NON-ORAL?-Clindamycin 20mg/kg IV/IM
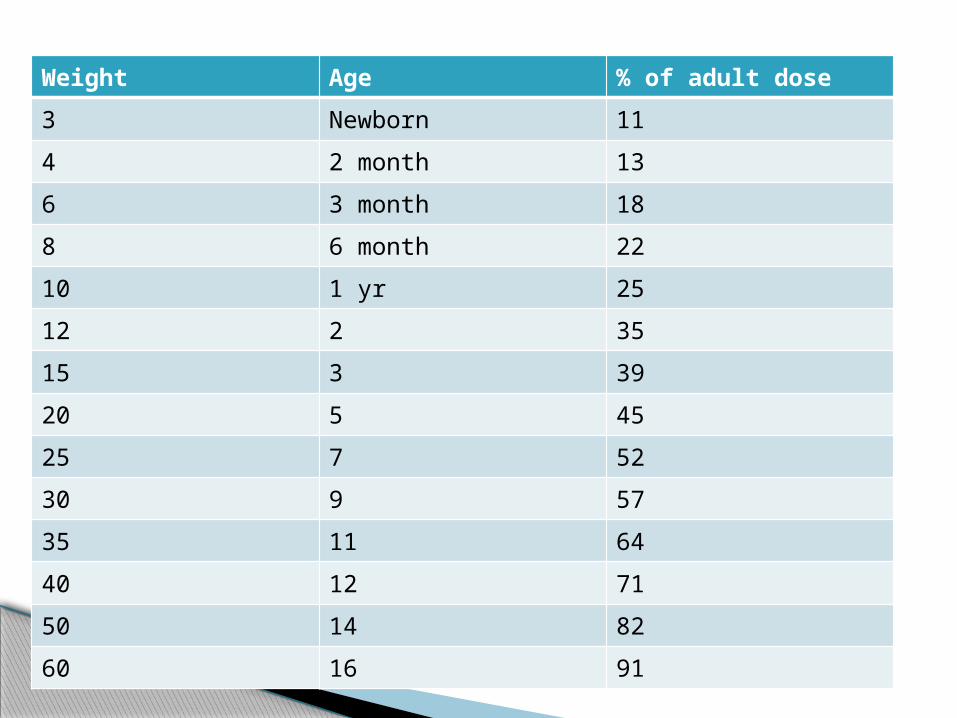
Weight Age % of adult dose
3 Newborn 11
4 2 month 13
6 3 month 18
8 6 month 22
10 1 yr 25
12 2 35
15 3 39
20 5 45
25 7 52
30 9 57
35 11 64
40 12 71
50 14 82
60 16 91

CONCLUSION: The role of antibiotics in odontogenic infections is of
paramount importance and one that cannot and
should not be neglected.
The fact that the microbial flora responsible for
odontogenic infections is a limited one only
emphasizes the need for proper antibiotic selection
and administration.
Too often in the look out for curing the infection, we
as dental practitioners tend to adopt a ‘shotgun
approach’ and prescribe unnecessary antibiotics.

1. St. Joseph Literature Review Some good stuff to know about kids‘ teeth.Wednesday, October 31, 2012 AAPD GUIDELINES ON ANTIBIOTICS Resident: Elliot Chiu
2. Laurence L. Brunton ,John S.Lazo ,Keith L. Parker; Goodman and Gilman’s The pharmacological basis of therapeutics; 11th edi,McGraw Hill,2006
3. KD Tripathi :Essentials of medical pharmacology; Jaypee brothers, 5th edi,2004
4. Naresh Kumar khanna; Principles of pharmacology for dental students, CBS publishers, 3rd edi,2010
5. Antibiotic & antimicrobial use in dental practice 2nd ed. by Michael G. Newman.
6. Tetracycline induced tooth discoloration Venkateswarlu M1 and Naga Sailaja R2
REFERENCES
Related Documents











