1 Antibiotics and Patients: what can and must do the Pharmacist ? Jerome J. Schentag, Pharm D University at Buffalo [email protected] http://www.pharmacy-ce.com

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Antibiotics and Patients: what can and must do the Pharmacist ?
Jerome J. Schentag, Pharm DUniversity at Buffalo
[email protected]://www.pharmacy-ce.com

2
Antibiotic Classes
• Aminoglycosides• Beta Lactams• Fluoroquinolones• Macrolides• Glycopeptides• Streptogramins• Oxazolidinones

3
Antibiotic DevelopmentYear Antimicrobial 1930s Sulfonamides 1940s Penicillin G 1950s E-mycin, TCs, Chloramphenicol 1956-9 Vancomycin, Metronidazole 1961-4 Ampicillin, Methicillin, Nalidixic Acid 1968 Aminoglycosides, Cephalosporins 1970s Carbenicillin, 2nd Gen Cephs 1982-5 3rd Gen Cephs, Imipenem, BL/BLIs 1987 Ciprofloxacin and the FQs 1999 Streptogramins 2000 Oxazolidinones

4
Clinical Use of Antimicrobials
• Prophylaxis• Empirical Therapy• Known Pathogen Therapy• Switch Therapy/Streamlining• Emphasis on Clinically useful
information, from years of study

5
My Biases• One dose for all, must yield to one dose for each. This is
the emphasis on dosing to MICs and CCr• One drug for all, must yield to one drug for each. This is
the emphasis on selecting the most potent member of a therapeutic class for treatment of target pathogens.
• Cost of care is a much more important issue than cost of antibiotic, for reasons of efficacy, safety, and time of response vs drug dose and concentration.
• The most expensive regimen is the one that does not work the first time

6
The one that doesn’t work....
ABX A (Failure)More Tests and Procedures
Never less expensive...
A Second Course
More Expensive ABXCost of Other Care
INFECTION
ABX B (Success)$ (No additional cost,ultimately)
JA Paladino, 1997.

7
More of my Overall Biases...• Tobramycin over Gentamicin, for Safety reasons.• Ciprofloxacin among the FQs for situations that may
encounter Pseudomonas aeruginosa (Resistance issues)• 8-F or 8-Methoxy FQs for patients with Streptococcus
pneumoniae (resistance issues)• Less overall cephalosporin use, especially in settings of high
risk of MRSA and/or VREF• We need alternatives to Vancomycin, and we need them very
quickly...

8
BACTERIABACTERIA PATIENTPATIENT
AntibioticAntibiotic
Pharmaco-Dynamics
Resistance Pharmaco-kinetics
Toxicity
Infection
Host Defense

9
Killing a bacteria with an antibiotic
Toxic effect
minConcentration in non-target tissues
Dosage
therapeutic effects
MaxMICSerum
Concentration varying over time
Concentrationat the site of infection
adapted from W.A. Craig...

10
Model Antibiotics for Human PK/PD trials:
• Cefmenoxime• Cefepime• Vancomycin• Aztreonam• Synercid• Imipenem• Amikacin
• Ciprofloxacin• Grepafloxacin• Tobramycin• Piperacillin• Ceftazidime• Azithromycin• Linezolid

11
Antibiotic Monitoring
• Serum Concentration Target– assumes all pts with the same MIC, or at
least a low MIC covered by usual doses.• Antibiotic Effect Target
– Microbial Killing measured with gram stain or serial cultures
• Both Targets, the Strengths of Each
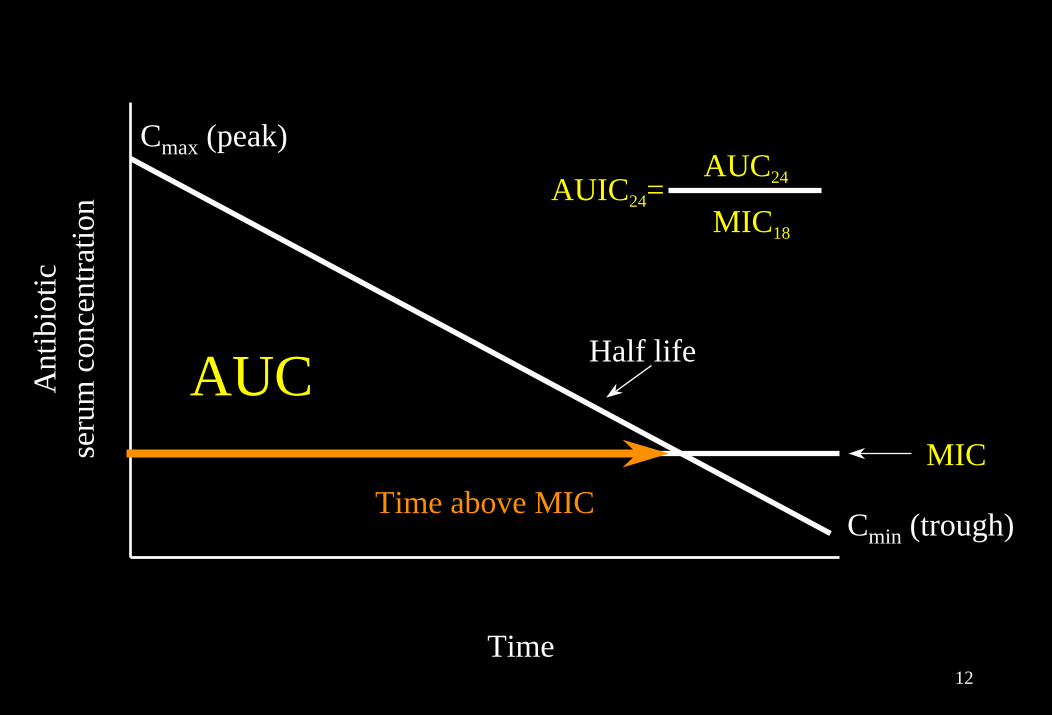
12
CCmaxmax (peak)(peak)
Time above MIC
Half lifeHalf life
Time Time
Ant
ibio
ticA
ntib
iotic
seru
m c
once
ntra
tion
seru
m c
once
ntra
tion
AUC
CCminmin (trough)(trough)
AUIC24=AUC24
MIC18
MIC

13
AUIC is a ratio, it does not have units1
• Mathematical derivation from integrated inverse ‘cidaltiters measured over time (Barriere et al, J AntimicrobChemother 16: 49-59, 1985)– The connection to measured ‘cidal activity in vivo led Forrest et
al to use SIT-1 in the 1993 paper discussing Ciprofloxacin (AAC 37: 1073-1081, 1993)
• AUIC is the Ratio of 24hr:– AUC: mcg x hr/ml (conc x time) to – MIC: mcg/ml x 18-24 hr incubation: mcg x hr/ml
• Therefore, use the 24hr mcg x hr/ml units for MIC as well as AUC, and units cancel out in AUIC calculations1. Mouton J., et al. Intl J Antimicrob Agents 19: 355-388, 2002

14
24
MIC=1.0
CSS = 4 mcg/mL
CFU Decline
Time, Hr
Broth (In Vitro)
AUC = 4x24 = 9624 hr AUIC = 96 1=96:
24
MIC=1.0
AUC = 96
CFU Decline
Time, Hr
Blood (In Vivo)
CSS = AUC 24 HR = 4.024 hr AUIC = 96 1=96
::
Hyatt et al, Clinical Pharmacokinetics28: 143-160, 1995

15
Pharmacokinetic/Pharmacodynamic Correlates of Cure for Different Classes of Antibiotics
Correlates of Successful Outcome
Drug ClassAminoglycosidesß-lactamsQuinolonesGlycopeptides
HumansCmax:MIC, AUICT>MIC, AUIC
Cmax:MIC, AUC:MIC, AUICMIC<1.0, T>MIC,
AUIC
In-VitroCmax:MICT>MIC
Cmax:MICT>MIC
AnimalsAUC:MIC
T>MICAUC:MICT>MIC,
AUC/MIC

16
Antibiotics for Study in Human LRTI
• Concentration Dependent Actions– Fluoroquinolones– Aminoglycosides– Carbapenems
• Concentration Independent Actions– Beta Lactams– Vancomycin– Macrolides– Linezolid

17
AUIC breakpoints in Mice and Man
AUIC Discussion
25-40 PD50 in animals; Some evidence for activity in mild infections inoutpatients with normal host defenses; peak:MIC ~ 3:1
125 Separates cure and failure in compromised patients; At 125,the AUC is 80% above MIC, and the peak:MIC ratio ~5:1;The threshold for avoiding resistance is an AUIC of 100
250 Maximal killing rate for concentration dependent ABX;peak:MIC ~ 10:1

18
Nosocomial Pneumonia, a Human Model for Studies of antibiotic PK/PD
• Precedent from Animal Models• Infection site concentration is equal to
the blood concentration, limiting the confusion over tissue penetration.
• low cure rate, rapid learning curve.• Easy access to tracheal organisms,
allowing time-killing studies in vivo

19
Advantages of Antibiotics
• You can isolate and study the bacterial “receptor” directly for conc/effect relationships
• Because testing of the individual sensitivity is easy, the correlation of in vitro Pharmacokinetics with in vivo Pharmacodynamics becomes feasible
• Gram stains, done serially, can tell you if you are eradicating the organism, or at least that you are reducing their numbers....

20

21
BACTERICIDAL ACTIVITY• Concentration-dependent killing
– the higher the drug concentration, the greater the rate and extent of activity
– aminoglycosides, quinolones, metronidazole• Minimal concentration-dependent killing
– saturation of killing rate occurs at low multiples of the MIC - usually 4-5X the MIC
– extent of killing dependent on time of exposure– β-lactams, vancomycin, clindamycin and macrolides

22
PHARMACOLOGY OF ANTIBIOTICS
• PHARMACOKINETICS– serum concentration profile– penetration to site of infection
• PHARMACODYNAMICS– relationship between serum concentration and the
pharmacological and toxicological effects• Both determine the time course of activity and the
clinical outcome of the patient

23
Applying AUICs to Empiric Therapy
• Measure or Calculate PK parameters (AUC)• Measure or default MICs
– Defaults in settings of breakpoints– Exact Values when available, and for streamlining
• Measure Antibiotic Endpoint as Bacterial Killing– Gram Stain pre vs post (i.e., Serial)
• The only true 10 minute determination of the correct dose– Culture
• Use culture positivity as an index of Low AUIC• Use early negative cultures to shorten duration of therapy

24
Case 03
• A 47 year old female with MS, was admitted from a nursing home in Respiratory distress with a temp of 104 oF; Intubated in ER. Her CXR was positive for a LLL infiltrate.
• Urine was packed with WBCs and bacteria.• Blood cultures have gram negative rods x2• Ht was 5’6”, weight 135 lbs, Cr was 1.0 mg/dl• She had multiple courses of TMP/SMX in the nursing
home, for frequent UTIs over 2 years.• What is the most likely pathogen in this case, and
what should be chosen for therapy?

The A.U.I.C. Program for Antimicrobial Dosing
ANTIBIOTIC UTILIZATION INFORMATION AND CONSULTATION ANTIBIOTIC UTILIZATION INFORMATION AND CONSULTATIONANTIBIOTIC UTILIZATION INFORMATION AND CONSULTATIONANTIBIOTIC UTILIZATION INFORMATION AND CONSULTATIONANTIBIOTIC UTILIZATION INFORMATION AND CONSULTATIONANTIBIOTIC UTILIZATION INFORMATION AND CONSULTATIONANTIBIOTIC UTILIZATION INFORMATION AND CONSULTATION
Version 1.0.0a
Copyright 1987–93, 1997–9 by The Clinical Pharmacokinetics Lab, Millard Fillmore Hospital, Buffalo, NY 14209, USA
Developed by: Martin Adelman, PhD and Jerome J Schentag, PharmD

26
Measures of Antimicrobial Action
• On the patient– Clinical Cure (contains no time sensitive information)– Rate of improvement in signs and symptoms– Daily symptom scoring and quantitative indices of
antimicrobial effects• Clinical Cure endpoint is not sensitive to:
– Rate of improvement over time– combination antibiotic effects vs single agents

27
Time to Eradication vs AUICGoss T et al. Ann Pharmacother 28: 863-868, 1994
% C
ultu
re p
ositi
ve%
Cul
ture
pos
itive
Cefmenoxime AUIC > 250Cefmenoxime AUIC > 250Ciprofloxacin AUIC > 250Ciprofloxacin AUIC > 250
6060
4040
2020
Differentiation of concentration and time dependent killing requires AUIC matching
100100
8080
00 2 4 6 2 4 6 88 10 12 1410 12 14
Days of treatmentDays of treatment
00
28
Trial Outcomes
• At similar AUIC, the antibiotic regimens tested performed similarly at EOT
• Most patients with AUICs above 125 were cured by the regimen that produced these values
• Daily scoring of these patients, to examine differences in speed of response vs antibiotic concentration in relation to MIC

Rs = 0.88
100 1000
Linezolid AUIC (SIT-1x24hr)
0
20
40
Line
zolid
60
80
100
%T>
MIC
Rayner et al. Clinical Pharmacokinetics 42: 1411-1423, 2003

30
Challenges in Antibiotic Monitoring
• AUIC values provide a precise means of expressing PK/PD changes in Exposure.
• Bacterial Eradication can be precisely monitored by serial cultures.
• We need an equally precise means of expressing and quantitating changes in the patients’ condition– This is the weak link in monitoring antibiotic therapy
at the moment.

31
Why standardize Antibiotic Activity Indices ?
• Endpoints for clinical trials
• Hypothesis testing in development of new antibiotics
• Development of drug monitoring strategies
• Facilitates computerization and automation, so it becomes the core of a dosing strategy to maximize efficacy and minimize resistance

32
Antibiotic Combinations
• Antibiotics are nearly always given in combination in the treatment of hospitalized patients
• Combinations broaden empiric spectrum and are felt to lower resistance. Some cases of Synergy are observed, although the normal effect appears to be additivity.
• Monotherapy is typical in outpatients, but the recent development of community resistance in S. pneumoniae, E. coli, and S. aureus suggests this is about to change
• A rational combination method is urgently needed both for the hospital and the community

33
Antibiotic CombinationsCompound AUC24
MIC P.aerug AUC/MIC
Ciprofloxacin 64 1.0 64
Pip-Tazo 1544 8.0 193
Total(Cipro+Pip-Tazo) 257

34
Synergy or Additivity between FQ and β-Ls?
• Additive in vitro, in most cases– in spite of different intra-cellular targets– in spite of different mechanisms of action
• First assessment is the action of each antibiotic alone vs the specific pathogen– Killing should appear conc dependent when most of the total
activity comes from the FQ– Killing should appear conc Independent when most of the
activity comes from the β-L

35
Ciprofloxacin with Pip/Tazo
• Depends on the absolute sensitivity of the organism to each antibiotic alone
• Best case is highly sensitive to ciprofloxacin, since that increases the speed of bacterial killing in vivo....

36
8C
once
ntra
tion
(µg/
ml) 40
30
20
10
016
Time (hrs)
0 24Cip MIC = 0.25 µg/ml
Pip AUIC = 40
Pip MIC = 32 µg/ml
Cip AUIC = 200
AUIC Total = 240DTE = 1 (Additive)DTE = 6 (Antagonism)
Pseudomonasaeruginosa, #1
Time (hrs)8
Con
cent
ratio
n (µ
g/m
l) 40
30
20
10
0160 24
Pip MIC = 4 µg/ml
Pip AUIC = 400
Cip AUIC = 40
AUIC Total = 440DTE = 6 (Additive)DTE = 2 (Synergy)
Cip MIC = 1 µg/ml
Pseudomonasaeruginosa, #2

37
Ciprofloxacin plus PiperacillinSynergy or Additivity?
OrganismP.aeruginosaP.aeruginosaE.cloacaeS.aureus
Predicted
DTE, Cip>32
115
MICCipro
1.00.25
0.1250.4
Predicted
DTE, Pip
776
>32
DTE(Actual)
6214
MICPip4.0
32.01.0
>256
Days to Eradication (DTE)

38
Ciprofloxacin with Pip-Tazo
• Piperacillin at maximal rate of bacterial killing will sterilize cultures in 4-6 days
• Ciprofloxacin at maximal rate of killing will sterilize cultures in 1 day
• Find pathogens where the predicted rate of sterilization is in excess of 7 days for either antibiotic alone, then optimize the other.

39
Ciprofloxacin with Pip-Tazo
• Depends on the absolute sensitivity of the organism to each antibiotic alone
• Best case is highly sensitive to ciprofloxacin, since that increases the speed of bacterial killing in vivo
• Must therefore optimize the dose of ciprofloxacin first, and then optimize the dose of piperacillin. Each of these can be done as AUICs for the pathogen in question

40
Antibiotic Combination effect in patient care
• Additivity is the usual situation in vivo
• AUIC values are additive• In vivo endpoint is more rapid
bacterial killing than expected by additive AUIC values alone.

41
Killing Curves Detect SynergyAs More Rapid Sterilization
1
4
3
5
7
6
2
Time
O
A+B
E
A
CFU
In Vitro100
30
Time
O
A+B
E
A
% C
ultu
re P
ositi
ve
In Vivo

42
Antibiotic Synergy
• Partly a matter of perspective• From the viewpoint of a β-lactam, synergy is
always possible, since they kill rather slowly on their own.
• Best partner antibiotic has concentration dependent killing– quinolones– aminoglycosides

43
Antibiotic Additions or Synergies
• Nosocomial Pneumonia is the best model for detecting the effects of synergy, as daily cultures can easily be performed.
• Once a bacteria is isolated, trach aspirate and BAL give the same information on the eradication of the pathogen, even though the original inoculum may be different
• Multiple organisms can be followed simultaneously

44
Impact of two drug regimens as calculated by A.U.I.C.
• AUIC24 values for each drug can be added to yield a total AUIC24 for the regimen
• True synergy would always speed organism eradication beyond the day predicted by the AUIC24 from additivity
• True synergy by this definition appears to be uncommon. Most interactions where the bacterial killing is measured are suggesting additive interaction

45
Principles of Combination Therapy
• Potentially synergistic combinations:– Tobramycin-Ceftazidime– Ciprofloxacin-Piperacillin
• Synergy can only be visualized when the MIC to both components is high, and therefore, the killing of the pathogen by either is rather slow

46
Strengths of these models
• Clinical data on bacterial killing rate are supportive of the findings in animal models
• Supportive of in vitro mechanisms and findings• Relevent to extracellular and probably also
intracellular pathogens• Relatively easy to use, since AUIC has a common
target for most clinical settings

47
CONCLUSIONS
• Utilizing pharmacokinetic and pharmacodynamic principles to optimize antibiotic dosing regimens will improve clinical outcomes and potentially decrease the development of resistance.
• Subsequent Presentations will demonstrate this premise for each of the major classes of antibiotics.
• AUIC plays a unique role in the implementation of antimicrobial pharmacodynamics at the bedside
Related Documents











