Antibiotics

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Antibiotics

CONTENTS• History• Classification of antibiotics• Pharmacology of antibiotics• Prophylactic use of antibiotics.• Conclusion.• References

HISTORY

Origins of Antibiotics -Paul Ehrlich• The "dawn" of modern antimicrobial
Origins of Antibiotics -Paul Ehrlich• therapy began with the physician chemist
Paul Ehrlich (1854-1915).• He knew that arsenic could kill the
syphilis organism but it was toxic to humans He systematically tried many combinations of arsenics with organics until in the early 1900's the effective compound #606 called Sal arson was synthesized
• He coined the term selective toxicity, where a compound could be targeted against a microorganism but be less toxic to the host cells.

Origins of Antibiotics -Sir Alexander Fleming
• The next breakthrough came by accident.
• In 1928, Sir Alexander Fleming was working with Staphylococcus aureus cultures in his London laboratory
• A plate became contaminated with a mold, Penicillium.
• Where you or I may have discarded the plate.
• Fleming noted inhibition of the bacterial colonies near the mold colony.

Origins of Antibiotics –Penicillin
• Fleming extracted a compound from the mold that he called penicillin.
• High mortality from infections during WWII provided the incentive for both British and then American scientists to develop methods for large scale fermentation and extraction of penicillin from the fungus.
• The miracle drug was introduced on a large scale during the 1940's

CLASSIFICATION
1. Chemical structure2. Type of organisms
against which primarily active
3. Spectrum of Activity4. Type of Action5. Antibiotics are obtained
from6. Mechanism of action

1.Chemical structure
1. Sulfonamides and related drugs: Sulfadiazine and others, Sulfones—Dapsone (DDS), Paraaminosalicylic acid (PAS).
2. Diaminopyrimidines: Trimethoprim, Pyrimethamine. 3. Quinolones: Nalidixic acid, Norfloxacin, Ciprofloxacin etc.4. -lactamantibiotics: Penicillins,Cephalo-sporins,
Monobactams, Carbapenems.5. Tetracycline: Oxytetracycline, Doxycycline etc.6. Nitrobenzene derivative: Chloramphenicol.7. Amino glycosides: Streptomycin, Gentamycin, Neomycin etc.8. Macrolides antibiotics: Erythromycin, Roxithromycin,
Azithromycin etc.

9. Polypeptide antibiotics:Polymyxin-B, Colistin, Bacitracin, Tyrothricin.
10. Glycopeptides; Vancomycin, Teicoplanin11. Oxazolidinone: Linezolid.12. Nitro furan derivatives: Nitrofurantoin, Fura-zolidone.13. Nitroimidazoles:Metronidazole, Tinidazole.14. Nicotinic acid derivatives: Ionized, Pyra-zinamide,
Ethionamide.15. Polyene antibiotics: Nystatin, Amphotericin-B, Hamycin.16. Azoles derivatives: Miconazole, Clotrimazole, Ketoconazole,
Fluconazole.17. Others: Rifampin, Lincomycin, Clindamycin,
Spectinomycin, Sod. fusidate, Cycloserine, Viomycin, Ethambutol, Thiacetazone, Clofazimine, Griseofulvin

Antibacterial: Penicillin, Amino glycosides, Erythromycin etc.
Antifungal: Griseofulvin, Amphotericin B, Ketoconazole etc.
Antiviral: Idoxuridine, Acyclovir, Aman-tadine, Zidovudine etc.
Antiprotozoal: Chloroquine, Pyrimethamine, Metronidazoles, Diloxanide etc.
Antihelmintic:Mebendazole, Prantel, Niclosamide, Diethyl carbamazine etc.
2.Type of organisms against which primarily active

3.Spectrum of Activity
• BROAD SPECTRUM1. Tetracycline
2. Chloramphenicol
3. Amoxicillin
4. Cloxacillin
5. Amoxicillin + clavulanic acid
6. Amoxicillin + cloxacillin
7. Carbenicillin
8. Piperacillin
9. Gentamicin , Tobramycin
10. III Generation cephalosporin
11. Fluoroquinolones
12. Metronidazole
13. Ornidazole
14. Tinidazole
• NARROW SPECTRUM1. Penicillin G
2. Penicillin – V
3. Ampicillin
4. Ist and IInd generation cephalosporin
5. Nalidixic acid
6. Kanamycin
7. Streptomycin
8. Erythromycin
9. Roxithromycin
10. Azithromycin
11. Clindamycin
12. Lincomycin
13. Vancomycin
14. cotrimoxazole

Primarily bacteriostatic:Sulfonamides TetracyclineChloramphenicol Erythromycin,Ethambutol
Primarily bactericidal:Penicillin CephalosporinAmino glycosides VancomycinPolypeptides Nalidixic acidRifampin CiprofloxacinCo-trimoxazole
4.Type of Action

5.Antibiotics are obtained fromFungi:
PenicillinCephalosporin
Bacteria:Polymix BColistinBacitracinTryothricin
Actinomycetes:Amino glycosidesTetracyclineChloramphenicolMacrolides

6.Mechanism of action 1. Inhibit cell wall synthesis: Penicillin, Cephalosporin, Cycloserine,
Vancomycin, Bacitracin.2. Cause leakage from cell membranes: Poly-peptides—Polymyxins,
Colistin, Bacitracin. Polyenes—Amphotericin B, Nystatin, Hamycin.3. Inhibit protein synthesis: Tetracycline, Chloramphenicol,
Erythromycin, Clindamycin, Linezolid.4. Cause misreading of m-RNA code and affect permeability: Amino
glycosides—Streptomycin, Gentamycin etc. 5. Inhibit DNA gyrase: Fluroquinolones— Ciprofloxacin.6. Interfere with DNA function: Rifampin, Metronidazoles.7. Interfere with DNA synthesis: Idoxuridine, Acyclovir, Zidovudine. 8. Interfere with intermediary metabolism: Sulfonamides, Sulfones,
PAS, Trimethoprim, Pyrimethamine, Ethambutol.


I.CELL WALL INHIBITORS
• lactums. – E.g. Penicillins, Cephalosporins, Carbapenens,
Imipenins, meropenem, aztreonam.
• Other antibiotics inhibiting cell wall synthesis– E.g. Vancomycin, teicoplanin, daptomycin,
bacitracin, fosfomycin, cycloserine.

Mechanism of action
• Peptidoglycan composed of glycan chains, which are linear strands of two alternating amino sugars (N-acetyl glucosamine &N-acetyl muramic acid) that are cross linked by peptide chain .
• Biosynthesis of peptidoglycan involves 30 bacterial enzymes and is considered in 3 stages:-

• Stage -1:precursor formation 1. UDP-acetyl muramyl - penta-peptide (park
nucleotide) :-contain dipeptide D-alanyl-D-alanine note:-Cycloserine is a structural analog of D-alanine ,
so act as a competitive inhibitor2. UDP-acetyl glucosamine.
• Stage-2:- UDP-acetyl muramyl-pentapeptide &UDP-acetyl
glucosamine are linked to form long polymer

• Stage-3:-completion of crosslink , accomplished by a transpeptidation reaction
This step is inhibited by beta-lactum antibiotics & glycopeptide antibiotic vancomycin

lactums
• Most effective for head and neck infections.• This names refers to the lactum ring common to
these agents.• Basic structure consist of, a thiazolidine ring
connected to a lactum ring , to which is attached a side chain.
• The side chain determines many of antibacterial and pharmacological characteristics of a particular type of penicillin


a) Penicillins• Miracle drug.• Originally obtained from
penicillium notatum but now from a mutant of penicillium chrysogenum.
• Structure• The penicillins are
derivatives of a basic structure known as aminopenicillanicacid.

NATURAL PENICILLIN
Penicillin- G•Penicillin has a narrow spectrum of activity. It is primarily active against Gram positive
•Penicillin remains the antimicrobial of choice for streptococcal infections (e.g., Streptococcus pyogenes that causes "strep throat" or Streptococcus pneumoniae that causes meningitis and pneumonia.)

Preparation and Dosage Penicillin G – Acid labile.1. Sod. Penicillin G (Crystalline penicillin) Inj.
0.5 – 5MU im / iv 6-12 hrly.It is available as dry powder in vials to be dissolved in sterile water at the time of injection.
Repository penicillin G Injections.1. Procaine penicillin G.(Duracillin , wycillin)
0.5-1MU im 12-24 hrly as aqueous suspension. Fortified procaine Penicillin G. It contains 3 lac u procaine
penicillin and 1 lac u sod. Pen. G.2. Benzathine penicillin G. (Bicillin , Permapen )
0.6-2.4MU im every 2-4 weeks as aqueous suspension.

• Oral administration of penicillin G :-absorption is rapid, and maximal conc. In blood are attained in 30 to 60 minutes
• Parentral administration of penicillin G :-after intra muscular injection , peak conc. In plasma are reached with in 15 to 30 minutes this value declines rapidly since the half life of penicillin G is 30 minutes.
• Repositery penicillin shows longer duration of action as it resorbs very slowly
• Excreted mainly through kidney.

Semisynthetic Penicillins
• Produced to overcome the shortcomings of penicillin G like-
1. Poor oral efficacy.2. Susceptibility to penicillinase.3. Narrow spectrum of activity.4. Hypersensitivity.

Classification
1. Acid resistant alternative to Pen. G.• Phenoxymethyl Penicillin (Pen. V).2. Penicillinase resistant penicillins.
Methicillin, Oxacillin, Cloxacillin , dicloxacillin ,naficillin.3. Extended spectrum penicillins.a. Aminopenicillins: Ampicillin, Amoxycillin, Becampicillin.b. Carboxypenicillins: Carbenicillin, Ticarcillin.c. Ureidopenicillins: Piperacillin, Mezlocellin.d. Mecillinan.
** lactamase inhibitors: Clavulanic acid, sulbactam

1. Penicillin V: • Acid stable.• So better absorbed from G.I.T.• On an equivalent oral-dose basis penicillin V
yields plasma conc. 2-5 times greater than those provided by penicillin G
• Dose: 250-500mg - Adults60mg - Infants125-250mg – Children
6th hrly

• TRADE NAMES• Bistrepen, Fortified PP , Fortified Procaine
Peni Inj , Kaypen, Pencom, Penidure, Penivoral, Pentids , Bistrepen, Fortified PP , Fortified Procaine Peni Inj , Kaypen, Pencom, Penidure, Penivoral, Pentids

2.Penicillinase Resistant Penicillins
• Methicillin, Oxacillin, Cloxacillin , dicloxacillin ,naficillin.
• Indicated in infections caused by penicillinase producing staphylococci.
• Rapidly but incomplitely absorbed from GIT.(30 to 80%)
• Peak conc.in plasma attained in one hour• Rapidly excreted by kidney .• Half lives are all between 30 to 60 minutes.

Methicillin: Highly penicillinase resistant.
• Poor absorption so not given orally• MRSA has evolved. • MRSA contains an additional high
molecular weight PBP with a very low affinity for beta-lactum antibiotics.
• Vancomycin is drug of choice for such infection

Cloxacillin
• DOSAGE Children – 50-100 mg/kg/day(div 6 hr)• ROUTE Orally or IV• AVAILIBILITY AND TRADE NAMES• CAPSULES Klox, Clopen, Bioclox(250 mg,500mg)

• SYRUPS Klox, clopen (125 mg/5ml)
• INJECTIONS Klox, bioclox (inj 250 mg,500 mg vials)
• CAUTION Give oral preparation 1 h before food or 2h after
food

3.Extended Spectrum Penicillin
• Active against gram-ve bacilli as well.• Most common drugs – amoxycillin, ampicillin.• Both the drugs are susceptible to -lactamases.• Hence they are available in formulations with -
lactamase inhibitors.– Ampicillin – Sulbactam.– Amoxycillin - Clavulanic acid.

Extended spectrum penicillinAcid stable AMINOPENICILLINS
• Amphicillin (oral/parenteral)
• Bacampicillin (oral/parenteral)
• Talampicillin (oral/parenteral)
• Amoxycillin (oral/parenteral)
Acid labileAntipseudomonal penicillins
• Carbenicillin(parenteral)• Ticarcillin(parenteral)• Pipercillin(parenteral)• Mezclocillin(parenteral)• Azlocillin (parenteral)

Ampicillin
• Semisynthetic penicillin with extended spectrum against gram negative bacteria like E.coli, proteus, salmonella, shigella, H.influenzae besides gram positive bacteria
• Well absorbed orally
• INDICATION UTI, respiratory tract infection including bronchitis
sinusitis, otitis media, meningitis, gonorrhoea, bacillary dysentery, cholecystitis, SABE, septicemia

AmpicillinDOSAGE
• Orally adult = 500 mg 6 hrly children = 50-100 mg/kg/day 6 hrly(maximum 2-3
g/day)
• I.M/I.V100-200 mg/kg/day 6 hrly

• CAPSULES Roscillin, Biocillin, Ampicillin, Campicillin (250mg,500mg)
• DISPERSIBLE TABLETS Roscillin DT (125 mg), Ampicillin DT (250 mg),
Amp kid (125mg,250mg)

• SYRUPS Roscillin, Biocillin 125mg/5ml
• DROPS Biocillin, Roscillin, Aristocillin -100 mg/ml
• INJECTIONS Roscillin, Biocillin, Ampicillin, Aristocillin (250mg,
500mg vials)

Amoxicillin• Semisynthetic penicillin with extended spectrum against gram
negative e.g. E. coli, H. influenzae, N. gonorrhoea, Proteus and gram positive bacteriae.g. Staphylococcus, Strep. Pneumoniae, Strep. Viridans, Strep. Faecalis and anaerobes are Clostridium, Peptococcus.
• Well absorbed orally• Food does not interfere with absorption• Excreted unchanged in urine
• INDICATION Upper respiratory tract, urinary tract infection, meningitis,
skin and soft tissue infection, enteric fever, SABE, otitis media, sinusitis

Amoxicillin• DOSAGEAdult = 250 to 500 mg T.I.DChildren = 25 to 50 mg/kg/day (div 8-12 h)BRANDS AVAILABLEActimoxAdmoxinAmolinAmotexAmoxinatAtmox

• CAPSULES Novamox, Mox, Wymox, Blumox, Lamoxy (250mg,500mg)
• DISPERSIBLE TABLETS Novamox(125mg,250mg), Wymox(250 mg), Lamoxy(250 mg), Blumox(125mg,250mg,500mg), Blumox LB, Pressmox(250mg), Moxybiotic kid(125 mg,250mg)
• TABLETS Novamox LB(250 mg,500 mg), Mox (125 mg,250 mg,500 mg), Pressmox(125 mg,250 mg,500 mg)

• PEDIATRIC TABLET Wymox (125mg), Lamoxy(125mg)
• SYRUPS Novamox(125mg,250mg/5ml),
Mox(125mg,250mg/5ml), Wymox,Lamoxy,Blomox(125mg/ml)
• DROPS Novamox(100mg/ml)
• INJECTIONS Mox,Hipen(250mg,500mg)

Carboxypenicillins & ureidopenicillinsantipseudomonal penicillins
• Carbenicillin:-was first penicillin with activity against P.aeruginosa and some Proteus strains
• Drug may interfere with platelet function , and bleeding may occur because of abnormal aggregation of platelets
• Only used for the management of urinary tract infection caused by Proteus species

• Ticarcillin:-2-4 times more active against P.aerugenosa
• Mezlocillin:-more active against Klebsiella than carbanicillin and its activity against Pseudomonas is simillar to that of ticarcillin
• Pipercillin :-extend the spectrum to include P.aerugenosa , Enterobacteriaceae and many Bacteriod species

Amoxycillin + Clavulanic Acid (Coamoxiclav)
• MECHANISM OF ACTION Clavulanic acid is B- lactamase inhibitor.
Rapidly absorbs orally, bioavailability = 60 %
Metabolised and excreted in urine.
Gram +ve organisms areStaphylococci, S. aureus, S. pneumoniae, S. viridans, S. faecalis, and Gram –ve are E. coli, H. influenzae, N. gonohorrea, N. meningitis.
Anaerobes are Clostridium, Peptococcus, Peptostreptococcus.

DOSAGE
Adult = orally 500 mg amoxycillin + 125 mg clavulanic acid. T.I.D
Children <3 months: 30 mg/kg/day every 12 h,>3 months:20-40 mg/kg/day q. 8-12 h

• Tablets: Enhancin (375 mg=250 mg+125 mg)
Augmentin duo (625 mg=500 mg+125 mg), Clavam (1000 mg=875 mg+125 mg)
• Kid tab: Amox (200 mg), Clav (28.5 mg)

• Syrups : Enhancin, Moxclav, Clavam BD syrup 156.25 mg
(125 mg+31.25 mg)/5 ml Augmentin duo syrup 228.5 mg(200 mg+28.5
mg)/5 ml Enhancin DS 228.5 mg tab
• Injection Enhancin - 1.2 g(1000 mg+200 mg) Augmentin – 600 mg (500 mg+100mg) Clavan – 300 mg (250 mg+50 mg) inj vial

Amoxicillin + Cloxacillin
• INDICATIONS Lower respiratory tract, skin, urinary tract, post
operative infections. Osteomyelitis, gynaecological, septicemia,
bacterial endocarditis, brain abscess, meningitis.
• DOSAGEAdults = 500 mg to 1gm T.I.DChildren = 50 – 100 mg/kg of combination.

• AVAILIBILITY AND TRADE NAMES
Cap novaclox (amox 250 mg+clox 250 mg)Cap P mox kid tab (amox 125 mg+clox 125 mg)Tresmos kidtab, Cap, Pedclox,Novaclox LB,Redclox LB

b) Cephalosporins• The cephalosporins are closely related to the
penicillins.• They also have a beta lactam ring as part of the basic
structure (cephalosporanic acid).• The various cephalosporins differ from each other in
their side chains (R groups].

CephalosporinsExamples Useful Spectrum
First GenerationCefazolinCephradineCephalexinCefadroxilCephapirin
Is active against streptococciIs active against staphylococcus aureusIs not active against enterococci, Listeria, or MRSA
Second GenerationCefuroximeCefaclorCefonicidCefpodoximeCefprozilCefoxitinCefotetanCefmetazole
Expands first-generation spectrum to include greater gram-negative activity (Haemophilus influenzae, including ampicillin-resistant strains, and Escherichia coli, Neisseria, Klebsiella, Acinetobacter, Enterobacter, Gitrobacter, proteus, providencia, and moraxella.Is not as active against gram positive organisms as first-generation; not active against enterococci, Listeria, MRSA or PseudomonasHas spectrum similar to that of cefuroxime, but also active against Bacteroides fragilis, bacteroides spp., and other anaerobes.
Third GenerationCefotaximeCeftriaxoneCeftazidimeCefiximeCefoperazoneCeftibutenCeftizoximeCefdorenCefdinir
Achieves therapeutic concentrations in CSF, unlike first and second Gen.Is less active than first generation against gram-positive bacteria; less active than cefoxitin or cefotetan against anaerobes.Has expanded gram-negative spectrum compared with first and second generations, including Citrobacter, E coli, Klebsiella, Enterobacter, Pseudomonas aeruginosa, Proteus, Morganella, Providencia, Serratia, Neisseria Gonorrhoeae.Is not active against enterococci, Listeria, or MRSA.Is more effective than oral third-generation antibiotics (Cefixime, Cefpodoxime), which lack useful activity against most strains of Enterobacter and Pseudomonas and have limited antianaerobic activity.
Fourth GenerationCefepime
Compares with that of third generation but more resistant to some extended-spectrum -lactamases


c) Carbapenems• Imipenem & carbapenems.• Broad spectrum which includes g+ve cocci,
enterobacteriacea, Ps.aeruginosa, Listeria & anaerobes.
• Resistant to both lactamase& penicillinase producing staph.
• Limiting feature : rapid hydrolysis by dehydropeptidase I enzyme hence combined with cilastatitin(inhibit degradation of imipenem by renal tubular dipeptidase).
• Very effective against serious infections even in AIDS & NEUTROPENIC pts
• Dose: imipenem-cilastatin 0.5 gm I.v 6th hrly

II. PROTEIN SYNTHESIS INHIBITORS• Aminoglycosides• Tetracyclines• Chloramphenicol• Macrolides (erythromycin, clarithromycin &azithromycin)• Clindamycin• Pristinamycin(streptogramins)• Linezolid• SpectinAomycin• Polymyxin B & colistin• Vancomycin• Teicoplanin• Bacitracin • Lincosamides• Kitolides(telithromycin)• Mupirocin• Fusidic acid

a. Aminoglycosides
• Bactericidal.• Used primarily to treat infections caused by
aerobic gram-negative bacteria.• Mechanism of action:
– They bind to the ribosomes and cause misreading of the genetic code and therefore incorrect aminoacids are inserted into the peptide chain and faulty proteins are produced resulting in the death of the microorganism.

Mech. Of Resistance:i. Acquisition of cell membrane bound inactivating enzymes.ii. Mutation decreasing the affinity of ribosomal proteins that normally bind the aminoglycoside.iii. Decreased efficiency of the aminoglycoside transporting mechanism.

• Aminoglycosides are effective and often the drug of choice for serious odontogenic infections caused mainly by aerobic gram-ve rods.
• The margin between therapeutic dose and toxic dose is narrow.
• The drugs are – – Streptomycin.– Gentamycin.– Neomycin.– Kanamycin.– Tobramycin.– Amikacin. Etc.

Shared Toxicities:Ototoxicity- because of acculumation in endolymph and perilymph of the inner ear.-diffusion back into blood stream is slow – the half life of aminoglycoside are 5-6 times longer in the otic fluid than in plasma(all occur because of persistent elevated conc.of drug in plasma|)(hemodialysis is the treatment)
- Cochlear damage- Vestibular damage
Nephrotoxicity –because of accumulation in proximal tubular cells –alter structure and function of these cells – reduced excretion of drug –predisposes ototoxicity.
ca++shown to inhibit uptake and binding of aminoglycosideto renal brush boarder luminal membrene and supplemental dietery ca++attenuates nephrotoxicity.Neuromuscular blockade-inhibit prejunctional release of acetylcholineand intravenous adm.of calcium salt is prefered treatment for this toxicity

Precautions:Avoid during pregnancy because may accumulate in fetal plasma and amniotic fluid – can cause hearing loss in childhood
amino glycosides and penicillins must never be mixed in same bottle because penicillin inactivates the aminoglycoside to a significant degree.

StreptomycinOldest aminoglycoside.Its spectrum is relatively narrow, primarily aerobic G-ve bacilli.Some G+ve cocci, in high concentration.
ADRs:Vestibular disturbancesLowest nephrotoxicityPain at injected siteExofoliative dermatitis
Uses:TuberculosisSub Acute Bacterial Endocarditis (SABE)Plague

Gentamycin
• Most commonly used for acute infections.• More potent and cheapest.• Due to low therapeutic index it should be restricted
to serious gram-ve bacillary infections.• Dosage:
– 3.5mg /kg/day im either a single dose or divided into 3 doses - for an average adult with normal renal function.

Amikacin
• Outstanding feature – its resistant to bacterial aminoglycoside inactivating enzymes.
• Widest spectrum of activity.• However relatively higher doses are needed for
pseudomonas, proteus and staphylococcal infections.
• Dosage: – 15mg/kg/day in 1-3 doses.

Neomycin
• Wide spectrum, against most gram-ve bacilli and some gram+ve bacilli.
• Highly toxic to internal ear and kidneys.• Often used topically (sometimes in combination with
polymyxin, bacitracin) for infected wound, ulcers, burns etc.
• It is available as NEOSPORIN – Neomycin – 3400 I.u. – Polymyxin B 5000 I.u. – bacitracin 400 I.u. /gm

b. TETRACYCLINES History
• Discovered by systematic screening of soil specimens.• The first of these compounds , chlortetracyclines , was
introduced in 1948.• Chlortetracycline – by Streptomyces aureofaciens.• Oxytetracyclines – Streptomyces rimosus• Tetracyclines – produced semisynthetically from
chlortetracyclines• Demeclocyclines –mutant strain of Streptomyces
aureofaciens.• Methacyclines, doxycyclines, minocycline –
semisynthethic derivatives.

Chemistry
Congeners of polycyclic naphthacenecarboxamide.

Effects on micro-organism• Wide range of aerobic &anaerobic G+ve & G- ve bacteria• Also effective against micro-organism that are resistant to
cell wall active antimicrobial agents, such as - Rickettsia - Coxiella burnitti
- mycoplasma pneumoniae - chlamydia spp. - Legionella spp.
- Ureaplasma spp. - some atypical mycoplasma - plasmodium spp.
• Not active against fungi.

Effects on intestinal flora
• As many of tetracyclines are incompletely absorbed from GIT so higher concetration reached in bowel , therefore entric flora are markedly altered.
• Stools bacome softer and odorless and acquire a yellow-green colour.
• Super infection & pseudo membranous colitis may occur.

Distribution • Distribute widely throughout body and into
tissues and secretions.• Acculumate in the reticuloendothelial cells of the
liver, spleen and bone marrow and in bone,dentine and the enamel of unerupted teeth.
• Penetration of these drugs into most other fluid and tissue is excellent
• Conc.in synovial fluid and mucosa of maxillary sinus approach that in plasma
• Cross the placenta and enter the fetal circulation and amniotic fluids.
• Relatively higher conc.also found in breast milk.

Route of Administration and Dosage
• Oral Administration:-• TETRACYCLINE:- 1 -2g per day in adults 25-50mg/kg daily in 2-4
divided doses in children >8 yr.age
• DEMECLOCLCLINE:-150mg every 6 hourly or300mg every12 hourly
-6-12 mg /kg daily in 2-4 divided doses in children >8 yr.age

DOXYCYCLINE:-100mg every 12 hours during first 24 hours, followed by 100mg once a day ,or twice daily when severe infection is present.• 4-5mg /kg per day ,diveded into 2 equal doses given 12 every 12 hours the first day ,after which half this amount (2-2.5mg/kg)given as a single daily dose.
•MINOCYCLINE:-2OOmg initially ,followed by 100mg every 12 hours-4mg/kg initially ,followed by 2 mg/kg every 12 hours.
Gastrointestinal distress,nausea,and vomiting can be minimised by administration of tetracyclines with food ( but not dairy products)

PARENTERAL ADMINISTRATION:-
•DOXYCYCLINE:-because of local irritation and poor absorption ,intramuscular injection is not recommended-intravenous dose is 200mg in one or two infusions on the first day and 100mg on subsequent day-For children whose weight is <45 kg is 4.4mg/kg on first day after that it is reduced correspondingly
•MINOCYCLINE:-intravenously 200mg followed by 100 mg every 12 hours

•TETRACYCLINE FIBER (ACTISITE)
•DOXYCYCLINE POLYMER (ATRIDOX)
•MINOCYCLINE OINTMENT (PERIOCLINE)
LOCAL DELIVERY OF ANTIBIOTICS

• Delivery System Consists Of A Polymer, Ethylene Vinyl Acetate, 25% Saturated Tetracycline Hydrochloride
• Contains 12.7 Mg/9 Inches Of Tetracycline Hydochloride• The Fiber Releases Tetracycline At A Constant Rate For 14 Days• A Concentration More Than 150 Times That Achieved By
Systemic Tetracycline• Bactericidal Concentration Of Tetracycline• Fewer Side Effects• Best When Used In Combination With Scaling And Root Planing
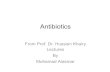
Tetracycline-Containing Fibers (Actisite)

Tetracycline fiber is packed into the periodontal pocket (a), secured with a thin layer of cyanoacrylate adhesive (b), and left
in place for 7 to 12 days.

• A Liquid Biodegradable Drug Delivery System That Hardens In The Periodontal Pocket And Gives A Controlled Release Of The Incorporated Agent
• Gel System• Incorporates Doxycycline 10%• Administered Via Syringe• Results As Monotherapy And In Conjunction With
Root Planing And Scaling Were Equivalent
• ↓ Probing Depth ,↓ Bleeding On Probing
Subgingival Delivery of Doxycycline (Atridox)

Atridox being placed into the pocket

• Sustained release form of 2% minocycline microspheres(arestin)for subgingival placements
• Adjunct to subgingival debridement. • The 2% minocycline is encapsulated into resorbable
microspheres in a gel carrier.• This system is a syringeable gel suspension delivery
formulation. • Improvement in probing depth, CAL and bleeding
index.
Subgingival Delivery System forMinocycline (Dentamycin,PerioCline,arestin)


Adverse drug reactions
TOXIC EFFECTS:-a)Gastrointestinal –epigastric burning and
distress ,abdominal discomfort ,nausea and vomiting,esophagitis and esophagial ulcer(Elmore and Rogge,1981),pseudomembranous colitis.
b)Photosensitivity :-demeclocycline, doxycycline to a lesser extend ,other derivatives may produce mild to severe photosensitivity.

C)Hepatic toxicity:-jaundice appears first followed by azotemia , acidosis ,irreversable shock.
d)Renal toxicity:-aggrevate uremia , Nephrogenic diabetes insipidus-demeclocycline so not used

• E)effects on teeth:-permanent brownish discolouration of teeth
• Highest effect when given to neonates and babies prior to first dentition.however may develop if drug is given between the age of 2 months and 5 years,when teeth are being calcified.
• This effect is due to its chelating property and formation of a tetracycline-calcium-orthophosphate complex.

• In pregnant ladies the period of greatest danger to the teeth is from mid pregnancy to about 4 to 6 months of a post natal period for the deciduous anterior teeth .
• In children from a few months to 5 years of age for permanent anterior teeth ,the period when the crown is being formed.
• However ,children up to 8 years age may be susceptible to this complication.

f) Miscellanous effects:-deposited in skeleton during gestation and throughout childhood - 40 % depression of bone growth.
• Thrombophlebitis• Vestibular toxicity-minocycline

c. CHLORAMPHENICOL1947, Streptomyces venezuelaeNitrobezene component: antibacterial activity, intense bitter taste.
MOA:acts primarly by binding reversibly to the 50s ribosomal subunit, near the site of action of macrolide antibiotic and clindamycin,which it inhibits competitively.Interfering ‘transfer’ of elongating peptide chains.
Uses:Never used for minor infectionsEnteric feverH.influenzae meningitisAnaerobic infectionsUTI

ADRs:Bone marrow depression :- present as anemia, leukopenia, or thrombocytopenia.HypersensitivityGray baby syndrome
- high dose ~100mg/kg, stops feeding, vomiting, hypothermic, abdomen distension, irregular respiration, gray cyanosis
- Blocks electron transport - ~25mg/kg/day
SuperinfectionsIrritative effects-nausea ,vomiting etc.

d. MACROLIDES
• Contains macrocyclic lactone ring with attached deoxy sugars.
• Effective against g +ve cocci and bacilli• Gram-ve bacteria and MRSA resist macrolides.

Erythromycin• Best known macrolide.• Bacteriostatic at low and cidal at high
concentrations.• Acts by interfering with proteins synthesis by
attaching to the 50s ribosomes.• Inactivated by gastric acids,thus administered as
entric coated tablets.absorbed from upper part of intestine.
• Its gram+ve antibacterial properties are similar to those of penicillins but erythromycin is not as effective as penicillins against anaerobes.
• Can be used in patients allergic to penicillins.

• DOSAGEChildren:30-50 mg/kg/day div.6-8 h(max dose
2g/day)• AVAILABILITY AND TRADE NAMESTABLETS – erythrocin(100,250,500mg),
althrocin(100,250,500mg), eltocin(250,500mg)
KID TAB – althrocin(125 mg)DISPERSIBLE – Althrocin(250 mg),eltocin(125
mg)DROPS –althrocin,erythrocin(100mg/ml)

Azithromycin • Spectrum – g+ve , g-ve aerobes & strict
anaerobes including actinobacillus actinomycetans, p. gingivalis.
• Oral absorption better than erythromycin.• Unique pharmacokinetic property-Good
tissue penetration –high drug conc.within cell (including phagocytes).tissue fibroblast act as a natural resorvior for drug and transfer of drug to phagocyte is easily accomplished.


Clindamycin
• It has reemerged as the most commonly used drug for serious odontogenic infections including osteomyelitis.
• It readily enters hard and soft tissues because of its relatively small molecular size.
• Its spectrum includes aerobic gram+ve bacteria and facultative and strict anaerobic bacteria.
• Dosage:– Adult – 150-450mg 6th hrly / orally.
300-900mg 8th hrly/ parenterally.Pediatric dosage – 10-20mg/kg/day in 3-4 doses.

VancomycinGlycopeptide antibioticDiscovered in 1956
MOA:Inhibiting cell wall synthesisDipeptide ‘D-alanyl D-alanine sequence
Spectrum:Very effective against MRSAStrep. viridansEnterococcusNo activity against G+ve bacteria

III.Agents affecting nucleic acids
• Quinolones.• Rifampicin.

QUINOLONES• Mechanisms of Action
• These agents interfere with the action of bacterial gyrase, one group of enzymes that helps to control the supercoiling of the DNA molecule

• The bacterial chromosome must be supercoiled so that it can fit in the bacterial cell (remember, bacteria do not have a nucleus)
• In the presence of quinolones, this supercoiling does not occur and the bacterial cells elongate and die.
• Eukaryotic cells do not contain
DNA gyrase,however they do
contain mechanistically simillar
type 2 DNA topoisomerase that
removes +ve supercoils to
prevents its tangling during
replication .quinolones inhibit
this only at much higher conc.

• The quinolones generally are affective for gram+ve and gram-ve aerobes including p.aeruginosa but are not useful for strict anaerobes.
• The quinolone antibiotics having one or more fluorin substitutes are called fluoroquinolones.

• They are classified as:• 1st generation fluoroquinolones.
– Norfloxacin. Ciprofloxacin.– Ofloxacin. Pefloxacin
• 2nd generation fluoroquinolones.– Lomeofloxacin. Gatifloxacin.– Levofloxacin. Sparfloxacin.
• 3rd generation– Moxifloxacin– 4th generation
G+ve cocci
G+ve cocci +anaerobes

Adverse effects• Gastrointestinal tract- nausea, vomiting etc.• Central nervous system – mild headache
and dizziness-NSAID drugs may potentiate this effect ,with seizures reported in patients receiving enoxacin and fenbufen.-because NSAID may augment displacement of GABA from its receptor by quinolones
• Arthralgia and joint swelling – not recommend in prepubertal children and pregnant women

Ciprofloxacin
• Most commonly used drug in head & neck infections.
• Oral absorption ranges from 50-90%.• It can pass into the most fluid compartments
and cross the placental barrier also.• Because of its increased side effects like GIT
upset, photosensitivity, xerostomia, insomnia, its use has become limited.

CiprofloxacinBroad spectrumMost susceptible: Aerobic G – ve bacilli, Neisseria,
enterobacteriaceaeWidely used in oral infections.
MOA:Inhibit bacterial DNA gyrase
Nicks double stranded DNA
Negative supercoiling
No replication/transcription

Ciprofloxacin
• Dosage:Children- 20-30 mg/kg/day div 12h(max dose
1.5g/day)orallyIV- 10-20 mg/kg/day div.12h(max dose 800
mg/kg)

• AVAILIBILITY AND TRADE NAMES• TABLETSCifran,ciplox,ciprobid,ciprolet(100,250,500,75
0 mg)• INJECTION20 mg/10 ml(50 ml,100ml,200ml)• SUSPENSIONCiprolar susp 125 mg/ml

Ofloxacin
• It is more potent than ciprofloxacin for gram+ve organisms.
• It is relatively lipid soluble, oral bioavailability is high and does not interfere with fluid.
• Ofloxacin is comparable to ciprofloxacin in the therapy of systemic mixed infections with less adverse effects.

Moxifloxacin
• Third genertion quinolones which provide good coverage against oral streptococci and anaerobes and has a good proven efficacy for acute sinusitis.

IV.INTERFERE WITH DNA FUNCTION
• Metronidazole • Bactericidal. They act by stimulating the production of
toxic metabolites which are able to kill susceptible bacteria.
• It is effective only against strict anaerobic bacteria including those in oral cavity.
• These drug can be useful adjunct to antibiotics with an aerobic spectrum in the treatment of mixed aerobic and anaerobic infections or for empirical treatment of stubborn odontogenic infections.
• Major side effect – Disulfiram reaction.• Pt. complains of nausea, headache, metallic taste.• CI in pregnant patients.

Metronidazole- Nitroimadazole, 1959- Broad Spectrum, against protozoa- Selectively toxic to anaerobic microorganisms
MOA: Enters cell by diffusion
DNA damage (cytotoxicity)
DNA helix destabilization
Strand breakage

Metronidazole
Uses:Anaerobic bacterial infectionsUlcerative gingivitis, trench mouthPseudomembranous enterocolitsAmoebiasisHelicobacter pylori gastritis/peptic ulcer
Doses:200-400 mg tab 8th hrly500 mg/100 ml i.v. infusion

Children – 30-50 mg/kg/day div. 6h PO/IV• AVAILIBILITY AND TRADE NAMES• TABLETSMetrogyl,aristogyl(200,400mg)• SUSPENSIONFlagyl, metrogyl suspension(200mg/5 ml),
aristogyl susp(100 mg/5ml)• INJECTIONMetrogyl, metronidazole IV (500mg/100 ml
infusion)

3 mix-MP (triple antibiotic paste)
developed by hoshino et alCompositionAntibiotics (3mix)
Ciprofloxacin200mgMetronidazole500mgMinocycline100mg
Carrier (MP)Macrogol ointmentPropylene glycol

• This triple antibiotic mixture has high efficacy. • In a recent preclinical study on dogs, the
intracanal delivery of a 20-mg/ml solution of these 3 antibiotics via a Lentulo spiral resulted in a
• greater than 99% reduction in mean colony-forming unit (CFU) levels,
• with approximately 75% of the root canal systems having no cultivable microorganisms present.

Subgingival Metronidazole• Topical medication containing oil
based metronidazole 25% gel• Applied in viscous consistency• Liquified by body heat• Again forms crystals with waterMetronidazole-benzoate→active
substance by esterases2 applications at 1 week
interval1.2 mm↓ probing depth,88%
↓ bleeding

PROPHYLACTIC USE OF ANTIBIOTICS






CONCLUSION Antibiotic selection remains as much an art as it is a
science.
Although antibiotics do not prevent all post operative infections, they can reduce the incidence significantly when administered correctly.
Future treatment strategies will not only include aggressive use of traditional management methods but also understanding normal immune system and associated defects, new antimicrobials.
Ultimately, we should provide a shorter course of treatment and improved outcomes for our patients.

REFERENCES• Medical pharmacology – Tripathi• Pharmacology by h.p.rang , m.m. dale, j.m.
ritter, p.k. moore- 5th edition• The pharmacological basis of therapeutics
by goodman & gilman-10th edition• Pharmacology and pharmacotherapeutics-r
s satoskar-18th edition

REFERENCES• Essentials of pharmacotherapeutics by f s k barab
-1st edition • Kayalvizhi. Role of antibiotics in paediatric
endodontics. ENDO (Lond Engl) 2010;4(1):41–48• Moloney J, Stasscn L. Antibiotics in odontogenic
infection lournal of the irish Dentol Association 2009; 55 (5): 242-245
• SEYMOUR R, HOGG SD. Antibiotics and chemoprophylaxis Periodontology 2000, Vol. 46, 2008, 80–108
• CIMS april july 2010
Related Documents