ANTIBIOTICS 2015 IN ICU SAMIR EL ANSARY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ANTIBIOTICS2015 IN ICUSAMIR EL ANSARY

Critical Care Antibiotics

Definitions
• Minimum Inhibitory Concentration
– Antimicrobial concentration that inhibits visible microbial growth in artificial media
• Gram Stain
– Gram positive
– Gram negative
• Acid fast
• Problems with MIC:
•Fixed drug concentration•All or none parameter. Growth vs. no growth•Does not provide information on the time course of
antimicrobial activity•Drug concentrations change throughout the dosing
interval•Does not capture interpatient pharmacokinetic
variability•Does not provide info on post-antibiotic effects

Gram staining
FOR differentiating bacterialspecies into (gram-positive and gram-negative).
The name comes from its inventor, Hans Christian Gram.
Gram staining differentiates bacteria by the chemical and physical properties of their cell walls by detecting peptidoglycan, which is present in a thick layer in gram-positive bacteria.

Gram staining
In a Gram stain test, gram-positive bacteria retain the crystal violet dye, while a counterstain
(commonly safranin or fuchsine) added after the crystal violet gives all gram-negative
bacteria a red or pink coloring.

Acid-fastness
A physical property of certain bacteria (and, less commonly, protozoa), specifically their resistance to decolorization by acids during staining procedures.
The high mycolic acid content of certain Protozoa cell walls, and those of Mycobacteria, is responsible for the staining pattern of poor absorption followed by high retention. Usually used to identify mycobacteria.
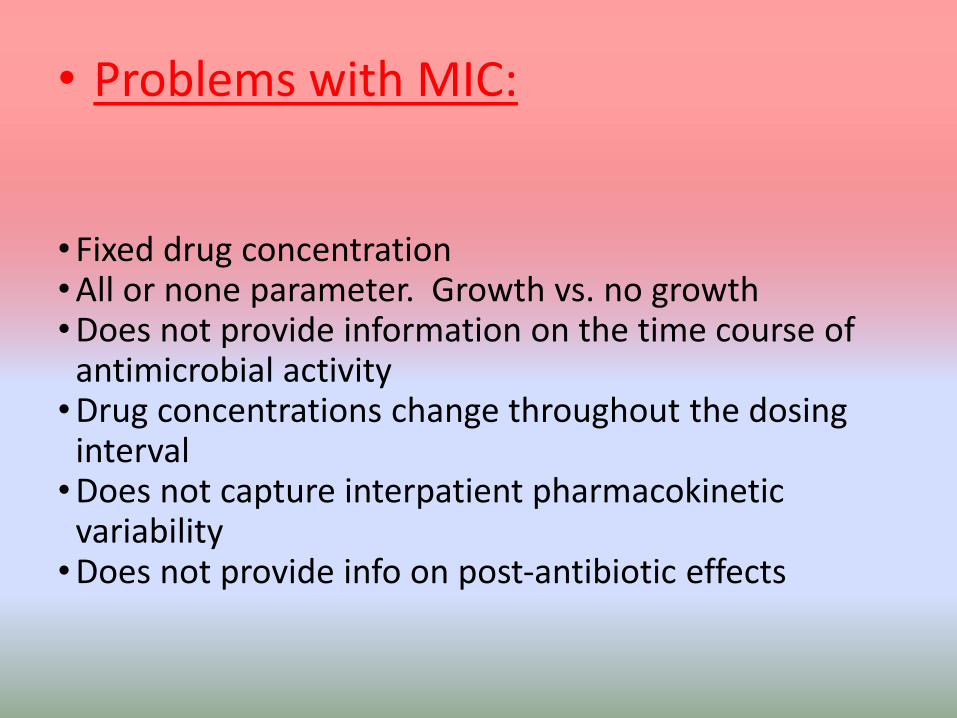
Pharmacodynamics
Time Dependent Killing
• Beta-Lactams– Penicillin
– Cephalosporins
– Piperacillin-Tazobactam
– Carbapenems
• Meropenem
• Ertapenem

• Pharmacokinetics versus pharmacodynamics
•Pharmacokinetics mathematically describe the relationship of antibiotic concentration to time.
• Aabsorption, distribution, metabolism, elimination, half-life, volume of distribution, and area under the concentration-time curve (AUC).

•Pharmacodynamics
•Describe the relationship of antibiotic concentration to pharmacologic effect or microorganism death.
• The three main pharmacodynamic parameters that are used are the
• peak to minimal inhibitory concentration ratio (peak/MIC), the AUC to MIC ratio (AUC/MIC)

•Pharmacodynamics
• The time the drug concentration remains above the MIC (T>MIC).
• Concentration independent antimicrobials include: beta-lactams, vancomycin, macrolides, aztreonam, carbapenems, clindamycin, tetracyclines, quinupristin/dalfopristin, flucytosine, and azole antifungals.

Pharmacodynamics
Concentration Dependent Killing
• Fluoroquinolones– Levofloxacin
– Ciprofloxacin
– Moxifloxacin
• Aminoglycosides– Amikacin
– Tobramycin
– Gentamicin
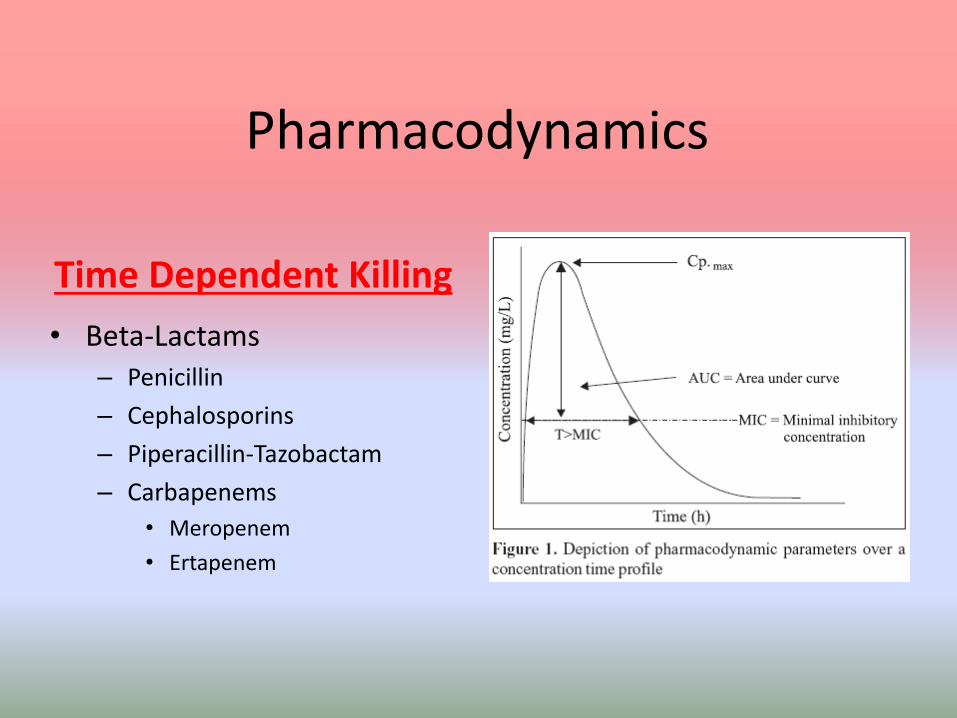
Pharmacodynamics
AUC/MIC Dependent Killing
• Vancomycin
• Linezolid
• Clindamycin
• Macrolides– Azithromycin
– Clarithromycin
– Erythromycin

Keys to Success
• Antibiotic covers potential infection/bacteria
• Dose of antibiotic is appropriate for treatment of infection and adjusted for renal/hepatic
impairment
• Antibiotic penetrates site of infection
• Antibiotic is being absorbed
• Adequate treatment duration

Risk Factors for Resistance
• Antimicrobial therapy in the preceding 90 days
• Current hospitalization of 5 days or more
• High resistance rates in the unit
• Residence in a nursing home or extended care facility
• Immunocompromised
• Home wound care
• Chronic dialysis
Gram Positive Agents
Vancomycin
Linezolid
Daptomycin
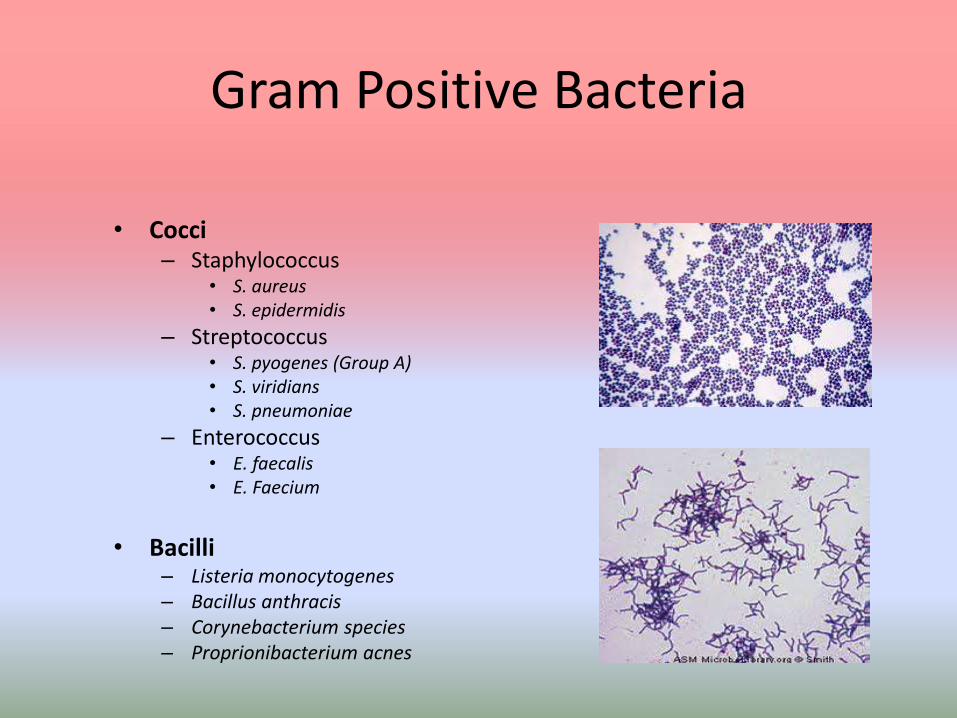
Gram Positive Bacteria
• Cocci– Staphylococcus
• S. aureus• S. epidermidis
– Streptococcus• S. pyogenes (Group A)• S. viridians• S. pneumoniae
– Enterococcus• E. faecalis• E. Faecium
• Bacilli– Listeria monocytogenes– Bacillus anthracis– Corynebacterium species– Proprionibacterium acnes

Vancomycin
• Spectrum of activity– Staph (MRSA, MSSA), strep, enterococcus, c. difficile colitis (oral)
• Mechanism of action– Inhibits synthesis of peptidoglycan/bacterial cell wall formation
• Dosing– Actual body weight– Loading dose = 25-30 mg/kg– Maintenance dose = 15-20 mg/kg– Usual Frequency = every 8-24h– Adjust dose for renal impairment

Vancomycin
• Adverse effects– Redman syndrome
– Thrombocytopenia
– Possible nephrotoxicity ??
– Ototoxicity (rare) Ototoxicity is not associated with trough concentrations.
• Monitoring– Goal Trough = 15-20 mcg/mL
– Bacteremia, endocarditis, osteomyelitis, meningitis, pneumonia
– Initial: trough before 4th or 5th dose
– Maintenance: trough once weekly

Vancomycin with Dialysis
• Continuous renal replacement therapy (CRRT)– 15mg/kg q24h– Hold dose if CRRT stopped > 8h– Trough before 4th or 5th dose
• Intermittent hemodialysis (iHD)– Pulse dosing with iHD– iHD removes ~25% of vancomycin– Goal Pre-iHD level < 24 mcg/mL– Initial dose = 15mg/kg x1 dose– Maintenance dose based on pre-iHD levels

Linezolid
• Spectrum of activity
– Staph (MSSA, MRSA), strep, VRE
• Mechanism of action
– Binds to bacterial ribosomes to inhibit protein synthesis
• Bacteristatic against staph, vre but cidalagainst strep pneumon
• Time dependent killing
Linezolid
• Adverse Effects– Myelosupression (pancytopenia, thrombocytopenia)
– GI upset
– Serotonin syndrome
• Drug interactions– Monoamine oxidase inhibitors (MAOI’s)
– Selective serotonin reuptake inhibitors (SSRI’s)
• Dosing– 600mg IV/PO q12h
Linezolid
• Clinical Pearls
– May be used for vancomycin failure or intolerance
– Oral & IV formulations
– Bacteriostatic
– No renal adjustment
– May have prescribing restrictions
– Expensive

Daptomycin• Spectrum of activity
– Staph (MSSA, MRSA), strep, enterococcus (VRE)
• Mechanism of action– Causes bacterial membranes to depolarize leading to inhibition of
protein, DNA, and RNA synthesis
• Typical Dosing– Adjust with renal impairment
– 4-6 mg/kg (actual weight) q24-48h
• Adverse Effects– Arthralgia
– Myalgia
– CPK elevations

Daptomycin• Clinical Pearls
– Not for treatment of pneumonia
– Can use doses of 8-10 mg/kg for severe infections
– Monitor CPK at baseline and weekly
– Can falsely elevate INR
– May have prescribing restrictions
– Takes 30-60 minutes to reconstitute
– Expensive

Gram Negative Agents
Aminoglycosides
Aztreonam

Gram Negative Bacteria
Cocci
• Neisseria gonorrhoeae
• Neisseria meningitidis
• Moraxella catarrhalis
Bacilli
• Pseudomonas aeruginosa
• Acinetobacter species
• Citrobacter species
• Enterobacter species
• Klebsiella pneumoniae
• E. Coli
• H. influenzae
• Proteus mirabilis
• S. maltophilia

Aminoglycosides
• Spectrum of activity
– Only gram negative, gram positive synergy
• Mechanism of action
– Bind bacterial ribosome and inhibit protein synthesis
• Adverse effects
– Nephrotoxicity
– Ototoxicity
– Prolonged neuromuscular blockade
Medications
Gentamicin Tobramycin Amkicacin
• Aminoglycoside antibiotics possess nondepolarizing neuromuscular blocking
activity, which is additive or synergistic with the effects of the nondepolarizing
neuromuscular blocking agents used in anesthesia .
• Aminoglycosides cause presynaptic inhibition of acetylcholine release and postsynaptic
reduction in sensitivity

Aminoglycosides
• Clinical Pearls– Used for
• Nosocomial infections• Double gram negative coverage • Endocarditis (synergy)
– Two dosing schemes• Traditional dosing• Extended interval dosing/once daily dosing
– Levels must be monitored• Traditional = peak & trough around 3rd dose• Extended interval = trough before 2nd dose
– Monitor Scr daily

Aztreonam• Class
– Monobactam
• Spectrum of activity‒ Gram positive: none‒ Gram negative: most, except S. maltophilia
• Mechanism of action– Inhibit cell wall synthesis
• Dosing– Usual: 1-2g IV Q8h– Meningitis: 2g IV Q6-8h
• Adverse effects (rare)– Transient eosinophilia– LFT elevations– Thrombocytopenia
**Can be used with
penicillin allergy**

Mixed Spectrum Agents
Cephalosporins
Piperacillin-Tazobactam
Carbapenems

Spectrum of Activity Primary Use
First GenerationCefazolin (Ancef) (IV)
Cephalexin (Keflex) (PO)
• Simple Gram (+) , simple gram (-) , no
anaerobes. No ceph gets enterococci.• Simple SSTI, surgical prophylaxis
Second GenerationCefotetan (Cefotan) (IV)
Cefoxitin (Mefoxin) (IV)
Cefuroxime (Ceftin) (IV)
Cefaclor (Ceclor) (PO)
Cefprozil (Cefzil) (PO)
• Same spectrum as 1st Generation
• Cefotetan and Cefoxitin cover anaerobes
• Surgical prophylaxis if anaerobes,
URTI, UTI
Third GenerationCeftriaxone (Rocephin) (IV)
Cefotaxime (Claforan) (IV)
Ceftazadime (Fortaz) (IV)
Cefpodoxime (Vantan) (PO)
Cefdinir (Omnicef) (PO)
Cefixime (Suprax) (PO)
• Better gram (-)
• Ceftazadime-pseudomonas • PNA, meningitis
Fourth Generation
Cefepime (Maxipime) (IV)
• Good gram (+), nosocomial gram (-)
including pseudomonas
• No anaerobes
• Sepsis, HAP, neutropenic fever
Fifth GenerationCeftaroline (Teflaro)
• MRSA, MSSA, E. faecalis, s.pneumoniae,
• Some gram (-), NO pseudomonas• Pneumonia, SSTI
Cephalosporins
• CABP pathogens, ceftaroline has activity against the Gram-positive organisms S.
pneumoniae, S. aureus and Streptococcus pyogenes, and Gram-negative species
(Haemophilus influenzae and CABP pathogens, ceftaroline has activity against the
Gram-positive organisms S. pneumoniae, S. aureus and Streptococcus pyogenes, and
Gram-negative species .
Cephalosporins
• Clinical Pearls
– Do not cover enterococcus (except ceftaroline)– ↑ gram negative coverage with higher generations– Used for surgical prophylaxis– Anaerobic coverage
• Cefoxitin• Cefotetan
– Pseudomonas coverage• Ceftazidime• Cefepime
Fluoroquinolines
Medications
Ciprofloxaci
nLevofloxacin Moxifloxacin
Gemifloxaci
n
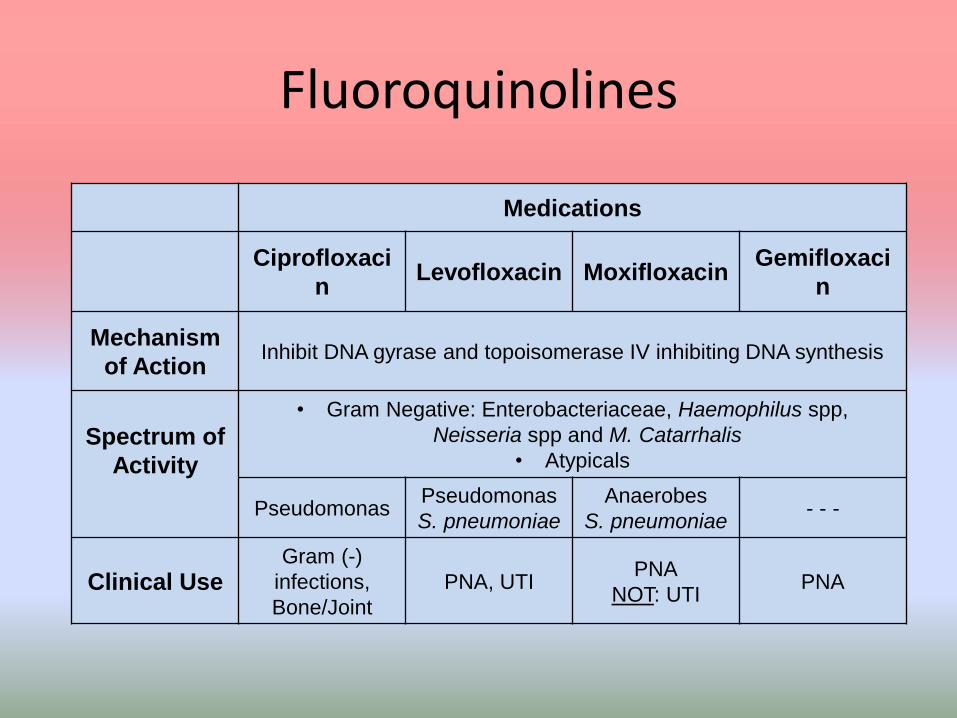
Mechanism
of ActionInhibit DNA gyrase and topoisomerase IV inhibiting DNA synthesis
Spectrum of
Activity
• Gram Negative: Enterobacteriaceae, Haemophilus spp,
Neisseria spp and M. Catarrhalis
• Atypicals
PseudomonasPseudomonas
S. pneumoniae
Anaerobes
S. pneumoniae- - -
Clinical UseGram (-)
infections,
Bone/Joint
PNA, UTIPNA
NOT: UTIPNA

Piperacillin-Tazobactam
• Spectrum of activity– Gram negative: P. aeruginosa, Enterbacteriaceae
– Gram positive: MSSA, Enterococci, Strep
– Anaerobes
• Mechanism of action– Inhibit cell wall synthesis
• Adverse effects– Gastrointestinal intolerance
– C. difficle colitis
– Interstitial nephritis

• Mechanism of Action:
• Inhibit mucopeptide synthesis in the bacterial cell wall, thus results in formation of defective cell walls and osmotically unstable organisms susceptible to cell lysis
•Tazobactam acts as a beta-lactamase inhibitor and inactivates both plasmid and chromosome mediated beta-lactamases

Carbapenems
Meropenem(Merem®)
Ertapenem (Invanz®)
Imipenem -Cilastatin
(Primaxin®)
Doripenem (Doribax®)
Mechanism of Action
Inhibit cell wall synthesis
Spectrum of Activity
Broad Spectrum: Gram (+), Gram (-), ESBL, Anaerobes NOT: MRSA
--NOT: Pseudomonas,
Enterococcus, Acinetobacter
-- --
Adverse Effects↓ PlateletsDrug Fever
Seizure↓ PlateletsDrug Fever
Common Use Meningitis Intra-abdominal Nocardia NOT: Pneumonia

Carbapenems
• Clinical Pearls
– First line agent for extended spectrum beta-lactamase(ESBL) producing bacteria
– Extended infusion meropenem• ↑ time above MIC
– Reserved for severe infections
– May have prescribing restrictions
Tigecycline
• Spectrum of activity– Enterococcus (including VRE), MSSA, MRSA, MRSE, anaerobes
– Not pseudomonas, proteus, providencia
• Mechanism of action– Binds to bacterial ribosomes to inhibit protein synthesis
• Dose– 100mg IV x 1 dose
– 50mg IV q12h
• Adverse effects– Nausea and vomiting
– Hyperbiliruminemia
•Tigecycline has a spectrum of activity that includes anaerobes, many gram-
positive cocci and gram-negative bacilli w/ the exception of
Pseudomonas, Proteus, and Providencia.
•N/V may occur in up to 2/3rds of patients

Tigecycline
• Clinical Pearls– No renal adjustment
– Hepatic dose adjustment (Child Pugh C)• 100mg IV x 1, then 25mg IV Q12h
– Used for resistant infections
– Do not use for • Ventilator associated pneumonia
• Bacteremia
– Can be used for • Intra-abdominal infections
• Skin & soft tissue infections

•All-cause Mortality: •An increase in all-cause mortality has been observed
•The cause of this mortality risk difference has not been established.
•Tigecycline should be reserved for use in situations when alternative treatments are not suitable.•Death resulted from progression of infection•Especially in ventilator associated pneumonia•Reserve for use when other agents are not an
option

Atypical Agents
Fluoroquinolones
Macrolides
Tetracyclines

Atypical Bacteria
Agents• Fluoroquinolones
– Levofloxacin– Ciprofloxacin– Moxifloxacin– Gemifloxacin
• Macrolides– Azithromycin– Erythromycin– Clarithromycin
• Tetracyclines– Tetracycline– Doxycycline– Minocycline
Bacteria
• Mycoplasma
• Legionella pneumoniae
• Chlamydia pneumoniae
• Richettsia
• Actinomyces
Commonly Encountered Infectious Disease Issues
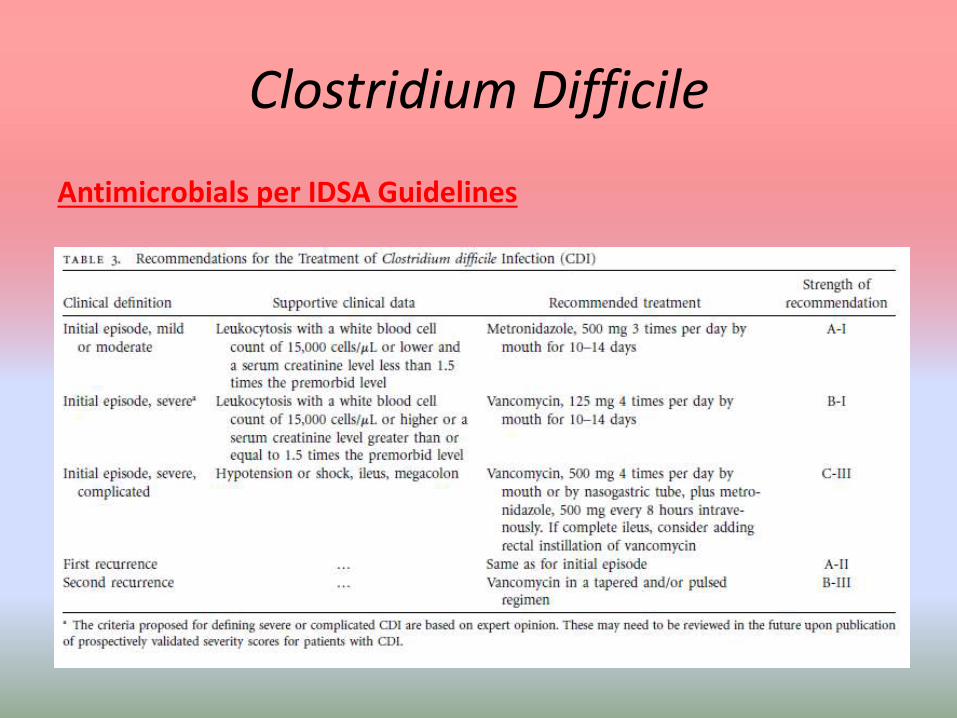
Clostridium Difficile
Antimicrobials per IDSA Guidelines

Clostridium Difficile
• IDSA Recommendations
– No probiotics - ↑ Bloodstream infections
– Stop causative antimicrobials
– Repeat testing during the same episode is discouraged
– Vancomycin taper after second reoccurrence
– Dual antimicrobials
• Ileus = IV metronidazole + vancomycin enema
**PO vancomycin is only used to treat c. diff infection**
• There is no evidence to support administration of combination therapy to patients with uncomplicated
CDI.
• Although hampered by its low statistical power, a recent trial did not show any trend toward better
results
when rifampin was added to a metronidazoleregimen.
• There is no evidence to support use of a combination of oral metronidazole and oral vancomycin.
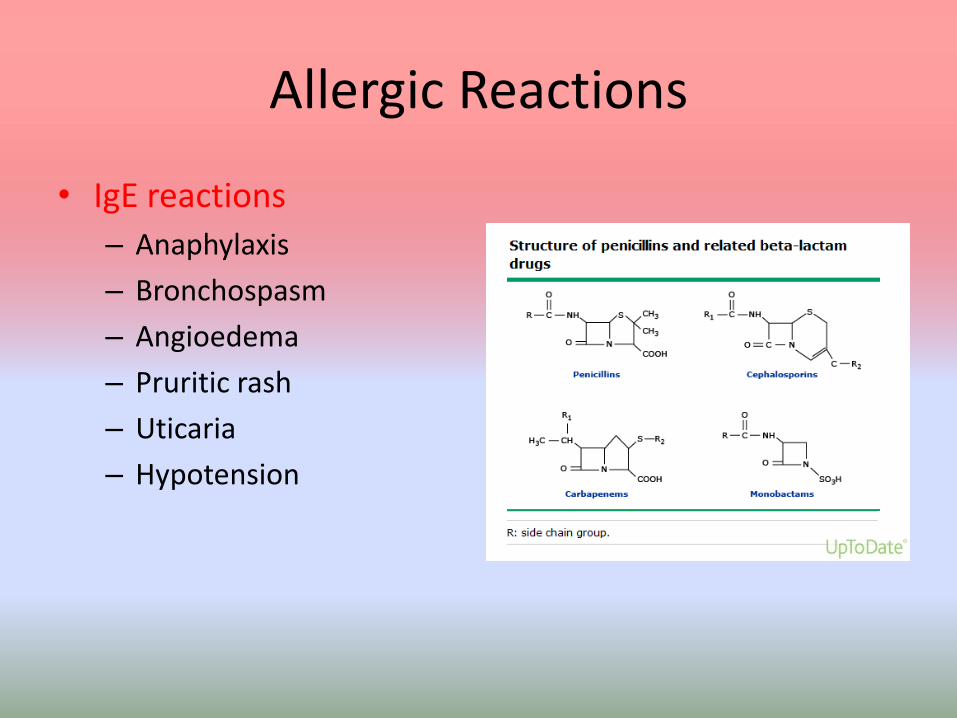
Allergic Reactions
• IgE reactions
– Anaphylaxis
– Bronchospasm
– Angioedema
– Pruritic rash
– Uticaria
– Hypotension
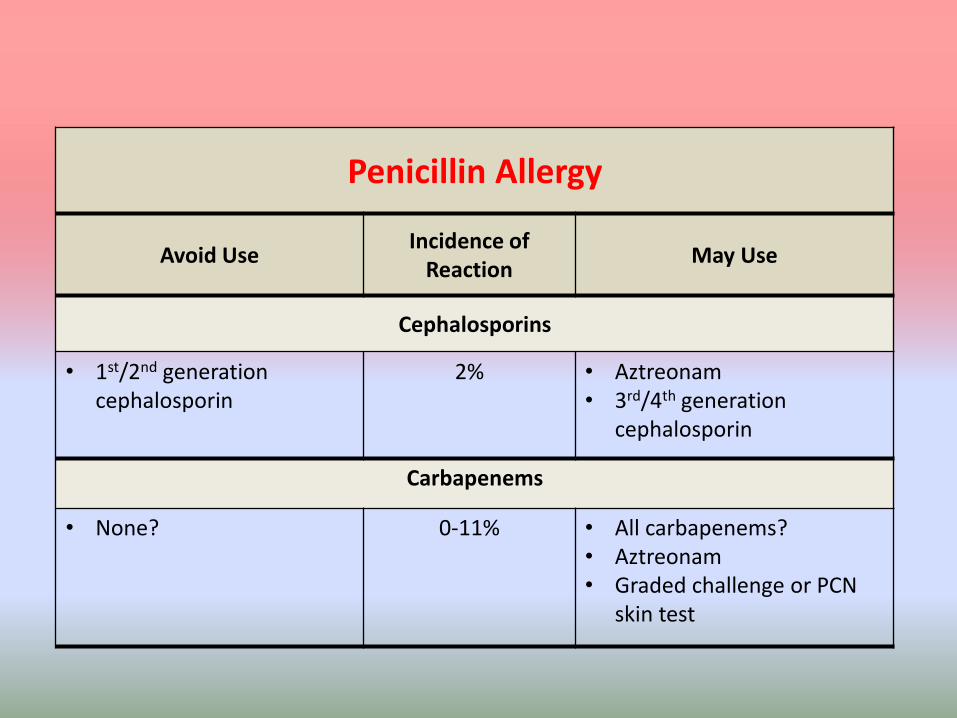
Penicillin Allergy
Avoid UseIncidence of
ReactionMay Use
Cephalosporins
• 1st/2nd generation cephalosporin
2% • Aztreonam• 3rd/4th generation
cephalosporin
Carbapenems
• None? 0-11% • All carbapenems?• Aztreonam• Graded challenge or PCN
skin test

•Penicillin-cephalosporin cross-reactivity studies that confirmed penicillin allergy by skin testing are superior
in design compared with those that diagnosed penicillin allergy by history alone.
•Another group of studies evaluated patients with positive penicillin skin tests (to penicilloyl polylysine
[PPL], penicillin G, and/or the minor determinant mixture [MDM]) who were challenged with
cephalosporins and found an overall reaction rate of 3.4 percent .
• If this analysis is limited to studies published after 1980 (when cephalosporins were no longer
contaminated with penicillin), the reaction rate is reduced to 2 percent.
•Thus, approximately 2 percent of patients with skin-test proven sensitivity to penicillin can be expected to
react to cephalosporins.
•Range for cephalosporin reaction was 0-12% reported in the literature.
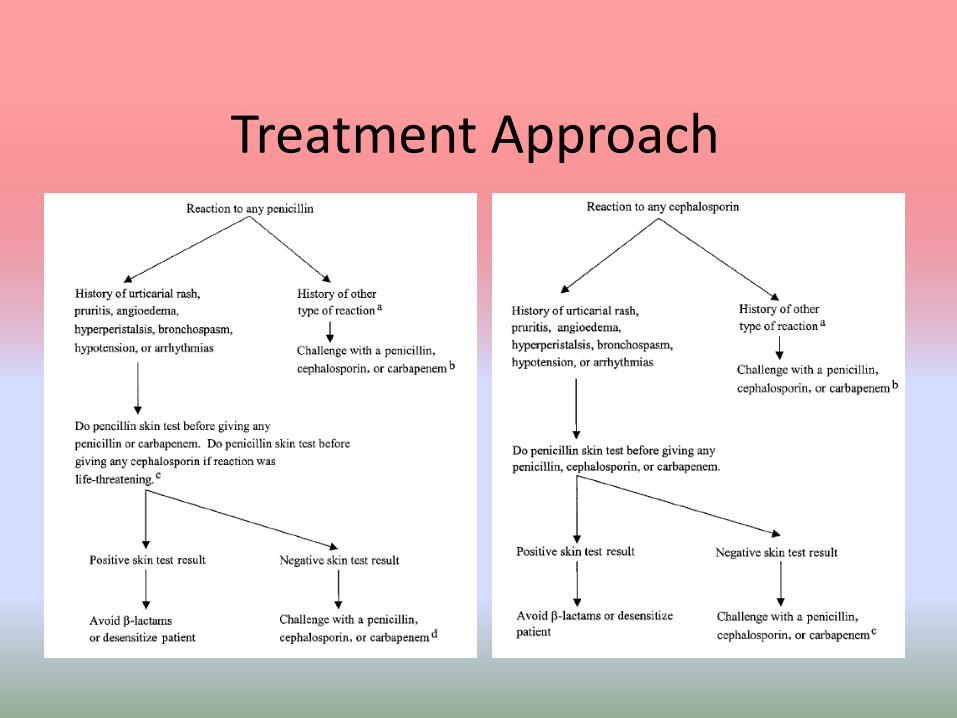
Treatment Approach
Related Documents