Antibiotic Use in Hospital Admissions Extra Information Clinical Outcome IDAP Other Death 4 (7%) 17 (7%) Readmission 10 (18%) 50 (20%) Escalation 1 (2%) 8 (3%) Disease-specific complication 0 (0%) 2 (1%) Statistical tests: Two sample t- test Weekend admissions, Night admission, Given antibiotic, Composite Outcome Two Sample Wilcoxon ranksum Mann -Whitney test Age, Charlson Index, Antibiotic quantification, Length of Stay Accompanying Information - Design of Data Entry Form and Dataset Nicola Fawcett – Research Fellow, Dept Micro/ID, John Radcliffe Hospital [email protected] Some of this may be very basic, some very complicated! Apologies if bits are very basic/grannies sucking eggs etc. AIM:

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Antibiotic Use in Hospital Admissions
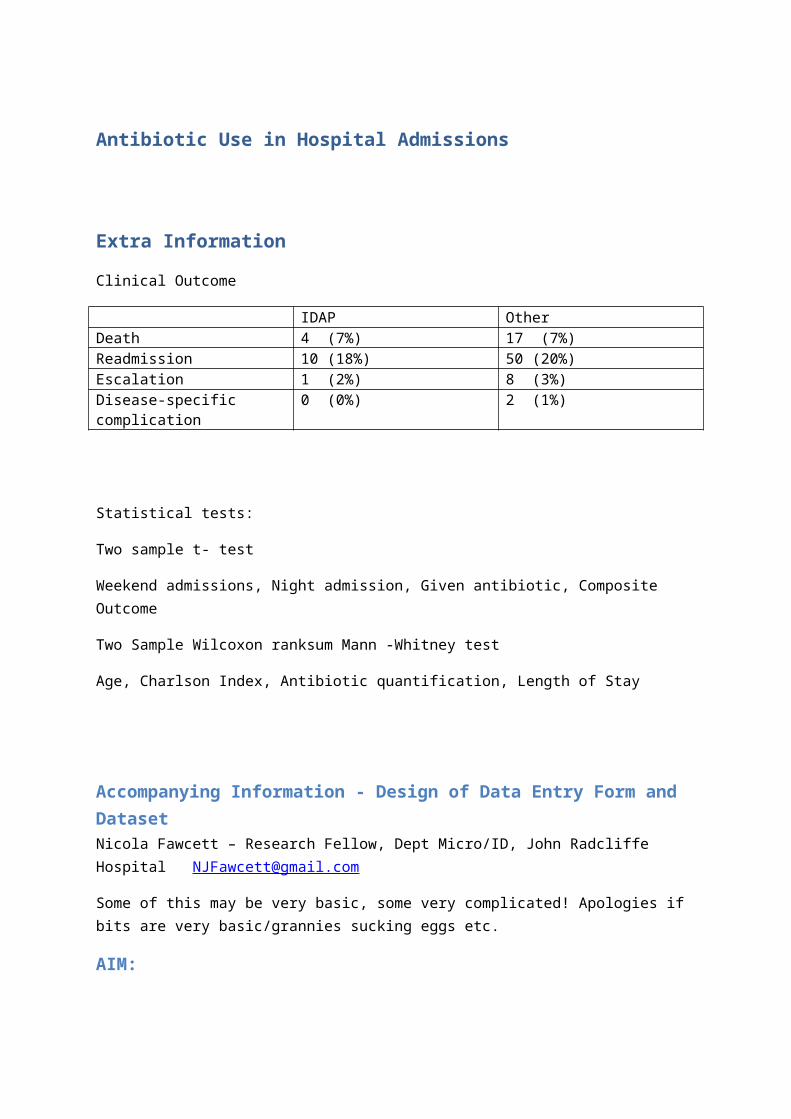
Extra Information
Clinical Outcome
IDAP OtherDeath 4 (7%) 17 (7%)Readmission 10 (18%) 50 (20%)Escalation 1 (2%) 8 (3%)Disease-specific complication
0 (0%) 2 (1%)
Statistical tests:
Two sample t- test
Weekend admissions, Night admission, Given antibiotic, Composite Outcome
Two Sample Wilcoxon ranksum Mann -Whitney test
Age, Charlson Index, Antibiotic quantification, Length of Stay
Accompanying Information - Design of Data Entry Form and DatasetNicola Fawcett – Research Fellow, Dept Micro/ID, John Radcliffe Hospital [email protected]
Some of this may be very basic, some very complicated! Apologies if bits are very basic/grannies sucking eggs etc.
AIM:
Collect data on antibiotic use in hospital admissions which allows us to assess:
1) Quantity a. Common measure, b. enabling:intervention with clinicians (metric they understand)c. enabling economic analysis (Lengths of treatment and cost of abx)d. enabling publication/comparison with other studiese. ‘baseline’ for further studies
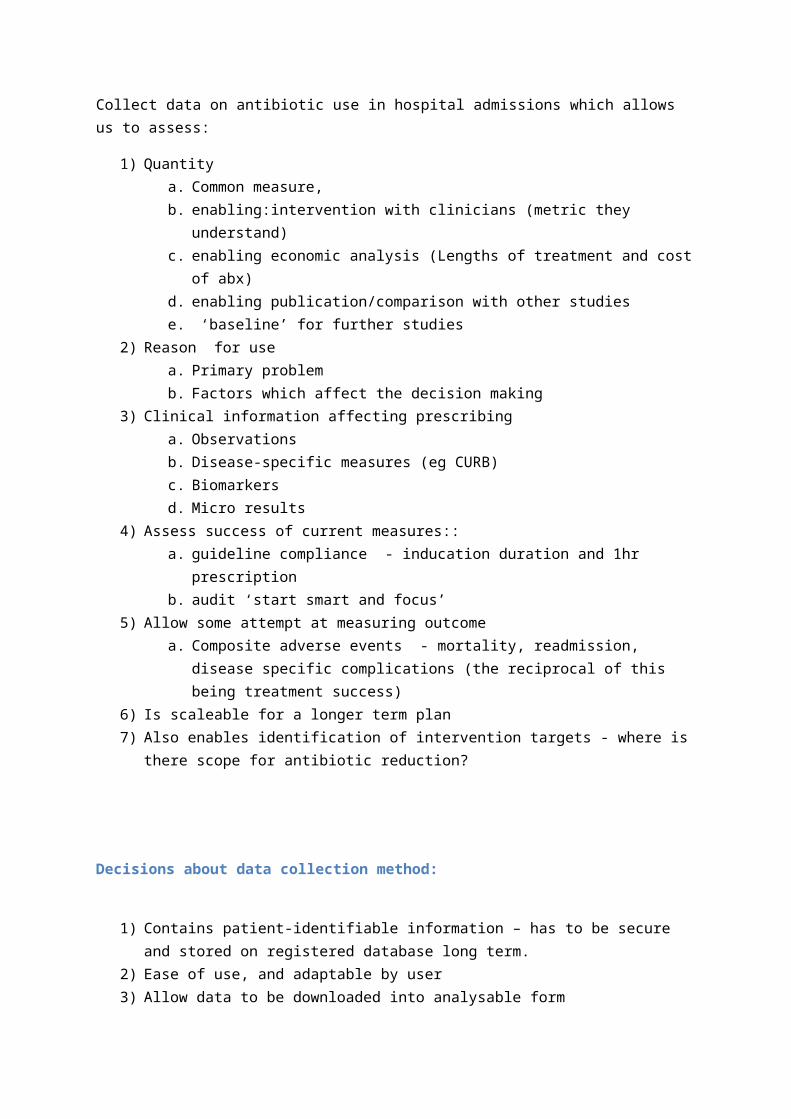
2) Reason for use a. Primary problemb. Factors which affect the decision making
3) Clinical information affecting prescribinga. Observationsb. Disease-specific measures (eg CURB)c. Biomarkersd. Micro results
4) Assess success of current measures::a. guideline compliance - inducation duration and 1hr prescriptionb. audit ‘start smart and focus’
5) Allow some attempt at measuring outcomea. Composite adverse events - mortality, readmission, disease specific complications
(the reciprocal of this being treatment success) 6) Is scaleable for a longer term plan 7) Also enables identification of intervention targets - where is there scope for antibiotic
reduction?
Decisions about data collection method:
1) Contains patient-identifiable information – has to be secure and stored on registered database long term.
2) Ease of use, and adaptable by user3) Allow data to be downloaded into analysable form
Epi-info:
1) For patient-identifiable information – NHS computers best used – but often do not allow installation of nontrusted applications.
2) Epi-info does not install on your computer. It runs as a .exe file straight from the folder in which you save it – as such can be run from a USB stick, or c drive, or even online drive (though this does slow things down)
3) Allows user editing of form 4) Can save data as a Microsoft access file, or longer term, to an sql database5) Developed and supported by the CDC Atlanta with good ongoing development - likely to be
an ongoing viable solution, also FREE, can be easily downloaded.
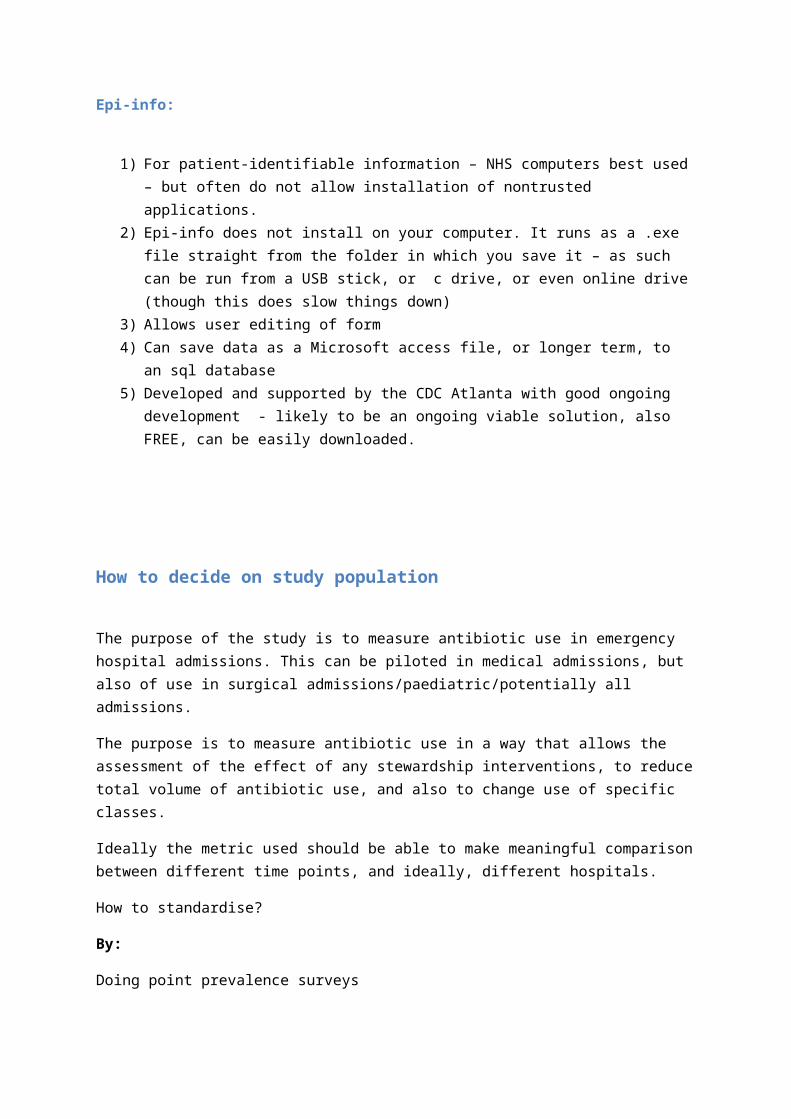
How to decide on study population
The purpose of the study is to measure antibiotic use in emergency hospital admissions. This can be piloted in medical admissions, but also of use in surgical admissions/paediatric/potentially all admissions.
The purpose is to measure antibiotic use in a way that allows the assessment of the effect of any stewardship interventions, to reduce total volume of antibiotic use, and also to change use of specific classes.
Ideally the metric used should be able to make meaningful comparison between different time points, and ideally, different hospitals.
How to standardise?
By:
Doing point prevalence surveys
Standardising per patient admission
Standardising per patient bed day
Per patient admission under certain teams
Choosing a particular patient subset (eg all patients with a diagnosis of UTI)
The choice:
For purposes of audit and intervention – measure antibiotic use in the group you want to intervene on, in a metric that they will understand, believe and feel fairly reflects their practice.
IE. Measure hospital-wide – and then report the characteristics of the hospital, or choose a particular subset.
Medicine also uses a significant proportion of the total antibiotic use in the hospital setting, treats the elderly patients at highest risk of resistant infection and often uses antibiotics inappropriately. Surgical admissions are another group worth considering.
Metrics
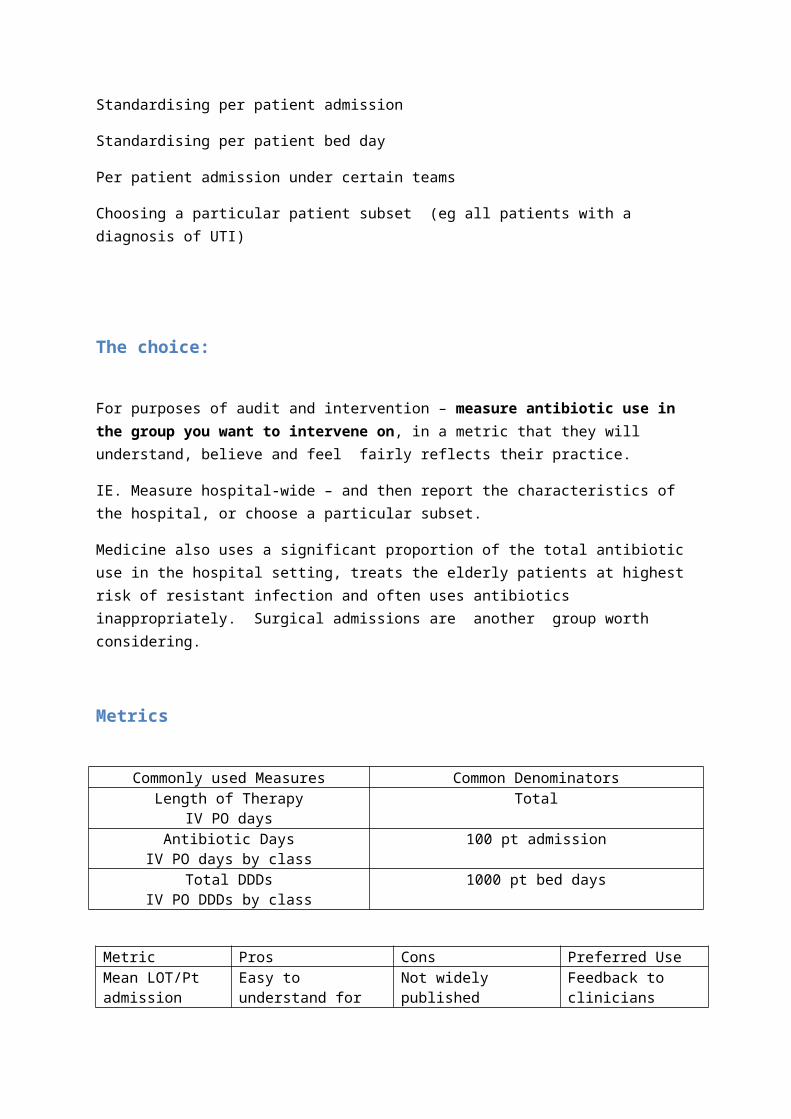
Commonly used Measures Common DenominatorsLength of Therapy
IV PO daysTotal
Antibiotic DaysIV PO days by class
100 pt admission
Total DDDsIV PO DDDs by class
1000 pt bed days
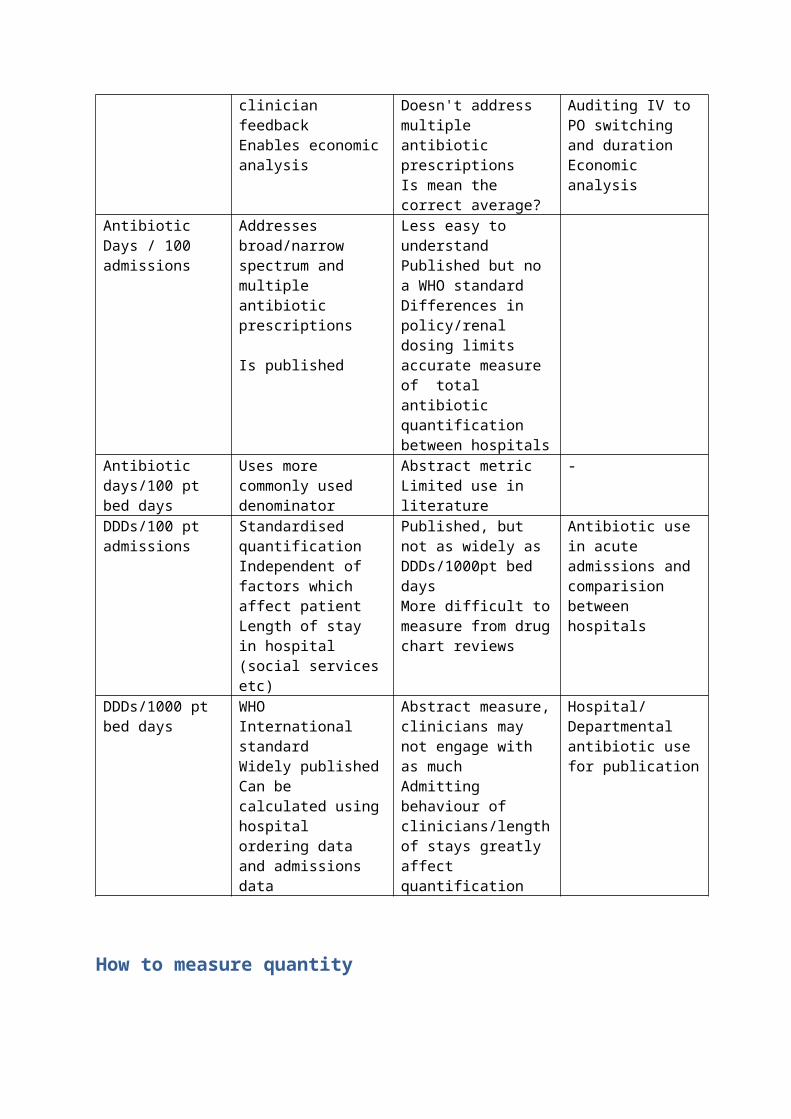
Metric Pros Cons Preferred UseMean LOT/Pt admission
Easy to understand for clinician feedbackEnables economic analysis
Not widely publishedDoesn't address multiple antibiotic prescriptionsIs mean the correct average?
Feedback to cliniciansAuditing IV to PO switching and durationEconomic analysis
Antibiotic Days / 100 admissions
Addresses broad/narrow spectrum and multiple antibiotic prescriptions
Is published
Less easy to understandPublished but no a WHO standardDifferences in policy/renal dosing limits accurate measure of total antibiotic quantification between hospitals
Antibiotic days/100 pt bed days
Uses more commonly used denominator
Abstract metricLimited use in literature
-
DDDs/100 pt admissions
Standardised quantificationIndependent of factors which affect patient Length of stay in hospital (social services etc)
Published, but not as widely as DDDs/1000pt bed daysMore difficult to measure from drug chart reviews
Antibiotic use in acute admissions and comparision between hospitals
DDDs/1000 pt bed days
WHO International standardWidely publishedCan be calculated using hospital ordering data and admissions data
Abstract measure, clinicians may not engage with as muchAdmitting behaviour of clinicians/length of stays greatly affect quantification
Hospital/ Departmental antibiotic use for publication
How to measure quantity
I’ve done a bit of basic modelling and found that slight changes in how the patient’s length of stay is managed has much more effect on measured antibiotic use per bed day than managing to reduce your antibiotic use by a third (ie. Increase your average LOS by a day and you’ll probably have as much effect as reducing your antibiotic use by a quarter…). Given that hospitals and especially
medicine face very different pressures in terms of LOS and it’s very dependent on external factors eg. availability of community beds, and the possibility that one 3 month admission can completely skew this data -
Antibiotic use per patient admission will not be affected by this.
As such whilst my method of analysis/reporting will be DDDs/100 pt admissions (publishable) average days of antibiotic therapy po and iv (easy to understand and relevant to clinicians for feedback/behaviour change) and classes of antibiotic (broad vs narrow)
However important to record data in such a way that allows you to report the following:
DDD/1000 pt bed days
DDD/100 pt admissions to hospital
Days of therapy/1000pt bed days Iv and PO
Days of therapy/100 pt admissions IV and PO
DDDs of a particular antibiotic class
Method of entering antibiotic data:
Days of therapy is easy to record – total days, and then total days of a specific antibiotic. For means of sensitivity – I have entered partial days.
Eg. ciprofloxacin 500mg bd for 7 doses = 3.50 days.
Co –amoxiclav 625mg tds for 7 doses = 2.33 days (2 decimal places)
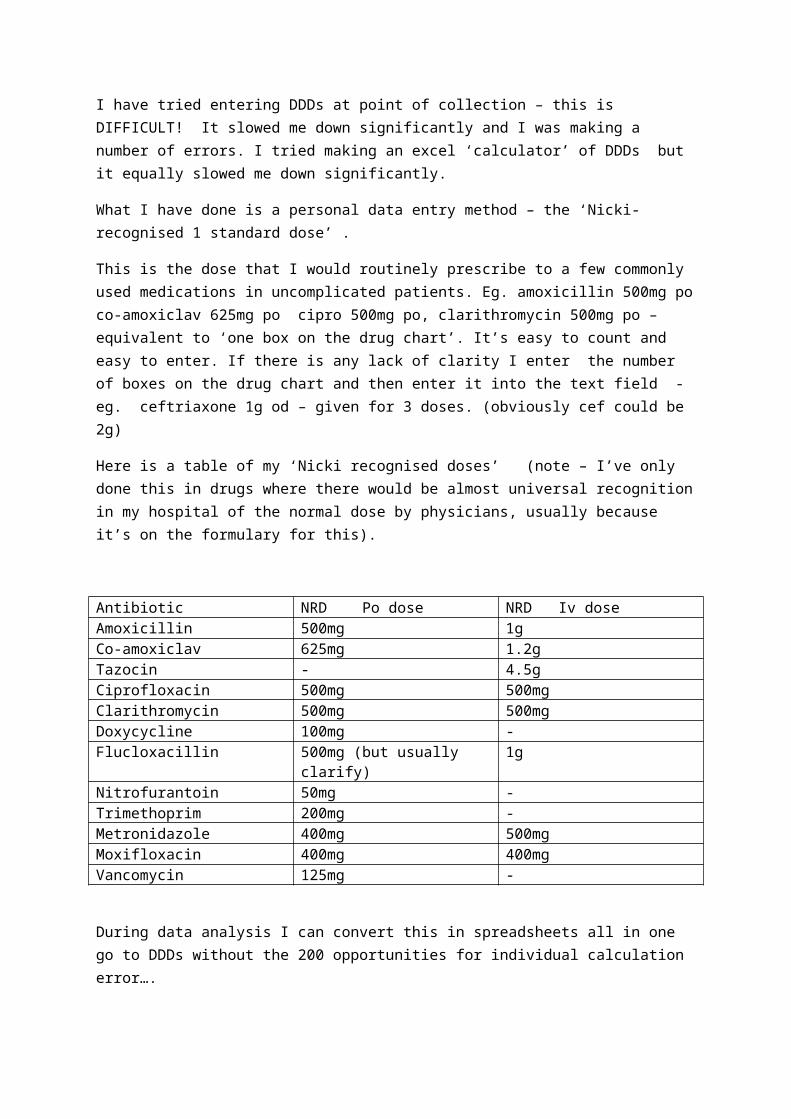
I have tried entering DDDs at point of collection – this is DIFFICULT! It slowed me down significantly and I was making a number of errors. I tried making an excel ‘calculator’ of DDDs but it equally slowed me down significantly.
What I have done is a personal data entry method – the ‘Nicki-recognised 1 standard dose’ .
This is the dose that I would routinely prescribe to a few commonly used medications in uncomplicated patients. Eg. amoxicillin 500mg po co-amoxiclav 625mg po cipro 500mg po, clarithromycin 500mg po – equivalent to ‘one box on the drug chart’. It’s easy to count and easy to enter. If there is any lack of clarity I enter the number of boxes on the drug chart and then enter it into the text field - eg. ceftriaxone 1g od – given for 3 doses. (obviously cef could be 2g)
Here is a table of my ‘Nicki recognised doses’ (note – I’ve only done this in drugs where there would be almost universal recognition in my hospital of the normal dose by physicians, usually because it’s on the formulary for this).

Antibiotic NRD Po dose NRD Iv doseAmoxicillin 500mg 1gCo-amoxiclav 625mg 1.2gTazocin - 4.5gCiprofloxacin 500mg 500mgClarithromycin 500mg 500mgDoxycycline 100mg -Flucloxacillin 500mg (but usually clarify) 1gNitrofurantoin 50mg -Trimethoprim 200mg -Metronidazole 400mg 500mgMoxifloxacin 400mg 400mgVancomycin 125mg -
During data analysis I can convert this in spreadsheets all in one go to DDDs without the 200 opportunities for individual calculation error….
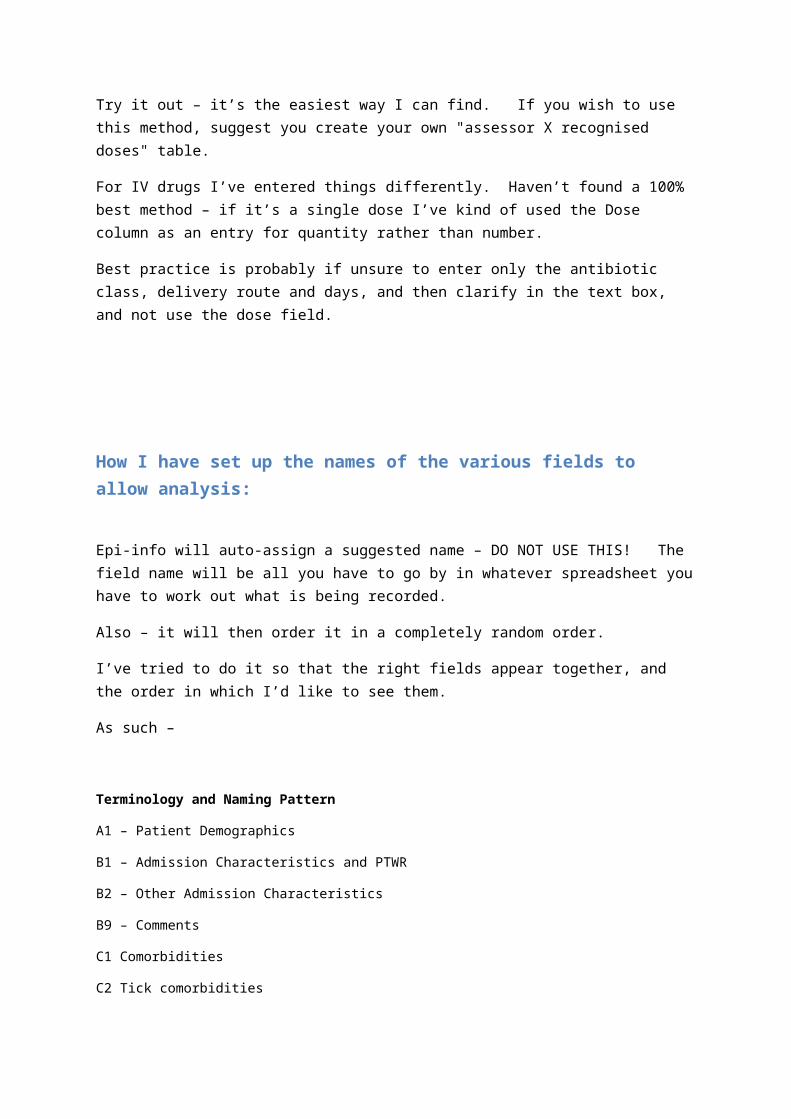
Try it out – it’s the easiest way I can find. If you wish to use this method, suggest you create your own "assessor X recognised doses" table.
For IV drugs I’ve entered things differently. Haven’t found a 100% best method – if it’s a single dose I’ve kind of used the Dose column as an entry for quantity rather than number.
Best practice is probably if unsure to enter only the antibiotic class, delivery route and days, and then clarify in the text box, and not use the dose field.
How I have set up the names of the various fields to allow analysis:
Epi-info will auto-assign a suggested name – DO NOT USE THIS! The field name will be all you have to go by in whatever spreadsheet you have to work out what is being recorded.
Also – it will then order it in a completely random order.
I’ve tried to do it so that the right fields appear together, and the order in which I’d like to see them.
As such –
Terminology and Naming Pattern
A1 – Patient Demographics
B1 – Admission Characteristics and PTWR
B2 – Other Admission Characteristics
B9 – Comments
C1 Comorbidities
C2 Tick comorbidities
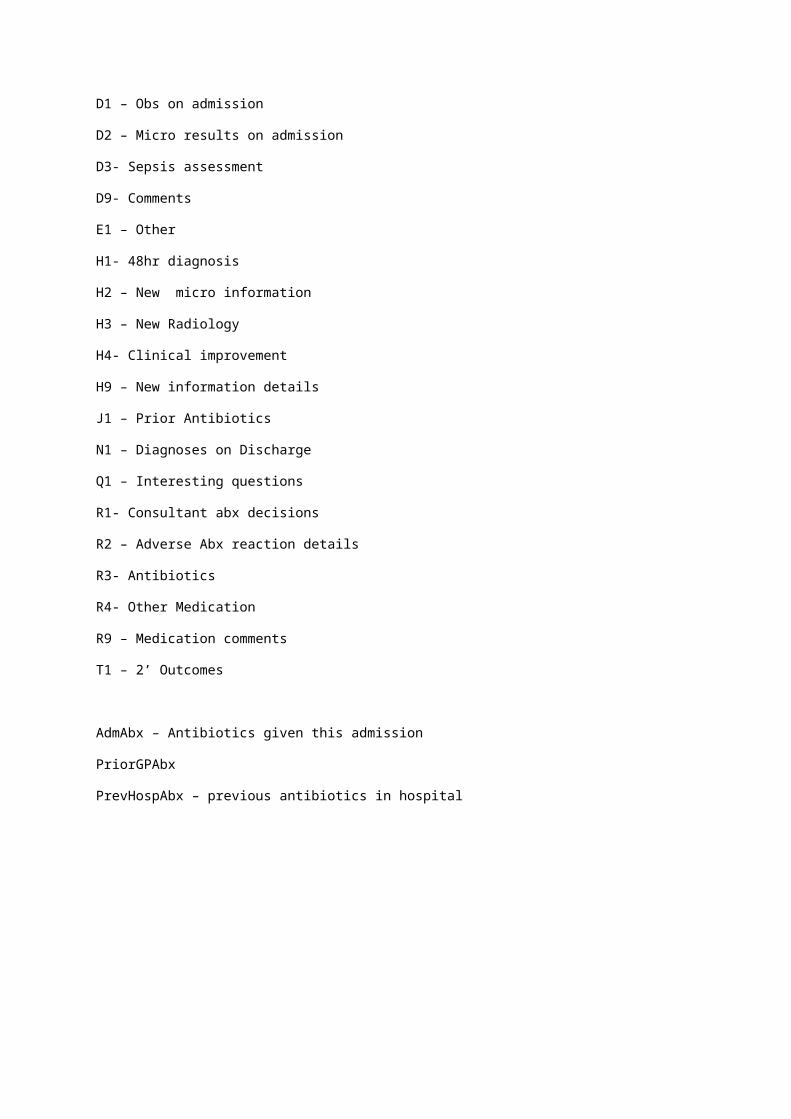
D1 – Obs on admission
D2 – Micro results on admission
D3- Sepsis assessment
D9- Comments
E1 – Other
H1- 48hr diagnosis
H2 – New micro information
H3 – New Radiology
H4- Clinical improvement
H9 – New information details
J1 – Prior Antibiotics
N1 – Diagnoses on Discharge
Q1 – Interesting questions
R1- Consultant abx decisions
R2 – Adverse Abx reaction details
R3- Antibiotics
R4- Other Medication
R9 – Medication comments
T1 – 2’ Outcomes
AdmAbx – Antibiotics given this admission
PriorGPAbx
PrevHospAbx – previous antibiotics in hospital
Streamlining Workflow/Maximising Efficiency.
What are we interested in?
Antibiotic use
Is there any point in collecting detailed physiological information on patients who are admitted with clear NSTEMIs? Maybe, but it falls out of the remit of the audit, and I cannot see myself ever using the data.
I also want to capture the subtle change between DR A who says - oooh, elderly patient confused, no objective markers of infection - give co-amox, and Dr B who says – hmmm, hold antibiotics.
As such – just collecting data on patients started on antibiotics could miss this.
My hybrid system is to look at all patients is to look at all the patients who are started on antibiotics, or you could feasibly see a doctor starting antibiotics on.
I had a long chat with a couple of our Consultants, and we felt that you could divide the patients up into
Definitely not infection
Definitely infection – and/or started on antibiotics (interested)
‘Grey area’ patients – ‘possible infection’
There may be a degree of intra-operator variance on this- however I can give a brief description on how to decision make:
Defining infection/possible infection/not infection
Infection:Infection is the primary differential Diagnosis. Eg. Green sputum productive cough consolidation – diagnosis on PTWR – pneumonia. Red leg, pyrexia high CRP – cellulitis.
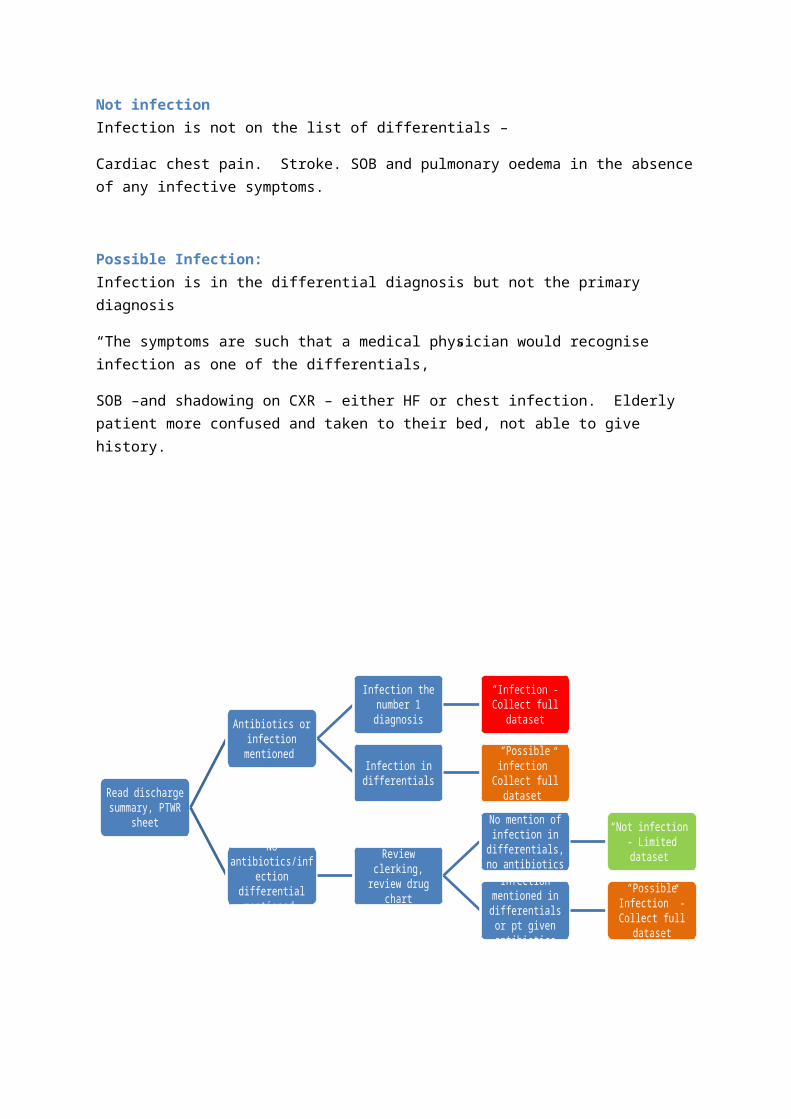
Not infection Infection is not on the list of differentials –
Cardiac chest pain. Stroke. SOB and pulmonary oedema in the absence of any infective symptoms.
Possible Infection:Infection is in the differential diagnosis but not the primary diagnosis
“The symptoms are such that a medical physician would recognise infection as one of the differentials, ”
SOB –and shadowing on CXR – either HF or chest infection. Elderly patient more confused and taken to their bed, not able to give history.
DATA COLLECTION: What to collect and where:
ALL Medical Admission will be collected including same day discharges and ambulatory care (provision of ambulatory care will differ between hospitals).
In All those with category “Not Infection”
Limited dataset – basic information plus diagnosis on admission/discharge and length of stay. If you can get date MFFD as well that would be ideal.
All those with category “Infection” or “Possible Infection”
Full data set including bloods and obs, presence or absence of cultures, and questions of interest.
Read discharge summary, PTWR sheet
Antibiotics or infection mentioned
Infection the number 1 diagnosis
“Infection”- Collect full dataset
Infection in differentials
“Possible infection” Collect full dataset
No antibiotics/infection
differential mentioned
Review clerking, review drug chart
No mention of infection in
differentials, no antibiotics
“Not infection” - Limited dataset
Infection mentioned in differentials or pt given antibiotics
“Possible Infection” - Collect full dataset

All those with clinical bacteraemia
Record antibiotic use previously in more detail in the tables
Acceptable Abbreviations:
COPD, IECOPD, NIECOPD, MI, ACS
Symptoms of Respiratory Infection – RespSx,
Acute Functional Decline in the Elderly with No Symptoms Localising Infection – AFDENSLI
Charlson Index Guidance/ What qualifies:
I note that the interpretation of pulmonary disease/etc in comorbidities will be subject to interpretation by many physicians.
I have proceeded to record CI as per OUH coding guidance to ensure that in future studies the recording of comorbidities happens in a standardised way that is in keeping with current procedures in the hospital. Whilst the coding guidance isn’t perfect, at least it’s standardised and recognised!
This should ensure that if we use the hospital database in future, for time series, the data collection method should be the same.
I’ve included my guide to the charlson index on a separate spreadsheet.
For full guidance on what qualifies – please see the Charlson Index Sheet
Note on comorbidities recording :
Record of charlson index by tickbox - represents ADMISSION comorbidities, but includes all diagnoses made by the posttake ward round.
After this point – any new comorbidities (eg has an in-hospital stroke on day 30) should be put in the text box with a note - as this should not figure on our admission CI figures.
However if we compare to hospital coding at a later timepoint this is discharge coding - and may continue information about things that developed during the admission, so we do need to know what happened.
Eg. 84yr female comes in with pneumonia. Has dementia, osteoporosis and ckd. 15 days into hospital stay has a stroke. Record:
Tick boxes – dementia , ckd. Text box: alzheimers dementia, ckd, osteoporosis in hospital – cva
Advice for starting out
Computer I think the best solution is to get a hospital –configured laptop. This enables you to access patient data, and also save your information on hospital drives.
a. Suggest you contact hospital IT and ask for the specifications of the computers that they set up for their staff/ email them to you.
b. Ask the dept. who does the order purchasing, and give them the specs of the computer
c. When it arrives, ask hospital IT to set it up like they would one of their own. If you can get them to add the encryption they would normally use this massively helps in terms of data protection issues.
Necessary softwareMicrosoft Access (should come with Microsoft Office) database management, Excel for easy to understand analysis, and Epi-Info, downloaded from website
Necessary Paperwork1) Audit approval – this allows you to collect the patient-identifiable information and
sometimes to get assistance with data collection. As we’re auditing against a fairly broad set of guidelines (SSAF) it allows us to actually collect quite a broad range of information. Suggest finding out from the hospital who you need to contact and ask and why. I’ve included a copy of my audit proposal at the bottom of this
2)
Learning the software:
Epi-Info I learnt my slightly budget epi-info skills from their website tutorials/guides
https://docs.google.com/file/d/0B1mGcf7b92K6R2dSQm54UTZHQ1U/edit?pli=1
http://wwwn.cdc.gov/epiinfo/html/tutorials.htm
http://wwwn.cdc.gov/epiinfo/user-guide/index.htm
http://www.phconnect.org/group/epiinfo/forum/topics/epi-info-7-quick-start-guide
The quick start guide is pretty good.
Probably the best way to learn how to edit forms is to try making a practice form or two, read the 'quick start guide' and then editing mine. (I started with a cake survey of the lab...)

Microsoft Access In terms of access, you shouldn't need advanced skills - simply creating a basic database, relationships and queries.
The Oxford computing services have some decent training resources at:
http://portfolio.it.ox.ac.uk/resource/course-pack/access-fundamentals-using-database/2007
http://portfolio.it.ox.ac.uk/categories/databases
Supplementary material
1) Audit Proposal
Project Title
Antibiotic Use in Hospital Admissions – Start Smart and Focus Guideline
Project Type
Audit
Re-audit
Service Evaluation
Patient Survey
Reason for audit
Please tick all that apply
NICE/ Standards
Policy/ Guideline
Project Lead
Contact Details
Name:
Dr Nicola Fawcett
Job Title: Registrar Acute/General Medicine
Address:
Dept Microbiology Level 7 John Radcliffe Hospital
Telephone/Bleep number: 22194
Email: [email protected]
Date: 07/02/2013 Fax:
Project Owner (if
Name: Dr Nicola Jones Job Title: Consultant Micro/ID and lead in Antimicrobial Stewardship
Lead is not permanent staff) Telephone/Bleep number:
Details and Objectives of the audit
Evidence base to be audited against
Details of what guideline or evidence is being measured
Department of Health Advisory Committee on Antimicrobial Resistance and Healthcare – Start Smart and Focus Guideline
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_131181.pdf
“
Subject
Further details of what is to be audited
We will audit the compliance to the start smart and focus guidelines in sequential medical admissions
From the guideline:
1) All patients with evidence/suspicion of infection should be started on prompt antimicrobial therapy
2) By 48hrs the antimicrobial prescribing decision should be made- De-escalate IV antibiotics to PO if appropriate- Stop antibiotics in the absence of infection- Review the duration of therapy- Review narrowing from broad to narrow spectrum therapy- Consider outpatient antimicrobial therapy
Objectives
How does this audit fit Trust objectives (eg monitors NICE guidance, relates to incident trend.)?
From the Department of Health Guidance Document:
1)There should be an ongoing programme of audit, revision and update monitored by the Antimicrobial Stewardship Committee/Management Team.It is recommended that a multi-disciplinary quality improvement/audit programme for antimicrobial stewardship should be developed and sustained in every acute Trust.
Regular (at least annual) feedback of adherence to prescribing standards should be provided to the Trust Board (as part of the annual infection control committee prescribers, lead clinicians and microbiologists, nurses, pharmacists and the DIPC.
2)It is recommended that as a minimum, providers should monitor adherence to Start Smart – then Focus, in particular, evidence of an Antimicrobial Stewardship review at 48 hours of all patients on intravenous antibiotics 48 hours after admission.
3)The Antimicrobial Stewardship Committee/Management Team and the DIPC should review antibiotic consumption trends regularly (at least annually).
4)Organisations should consider formal investigation of cases of repeated non-compliance (without clinical justification) or inappropriate prescribing, particularly when these result in an adverse patient outcome (e.g. development of an HCAI, prolonged length of stay, etc.)
5)It is important for providers to monitor patient outcome to ensure that qualitative or quantitative alterations (changing, reducing, restricting) to antimicrobial prescribing do not have unintended detrimental effects for example increased time to clinical cure, increased mortality, increased readmission rate
Participants
Who/ which area/clinical unit is involved in collecting the data or providing data?
Collecting Data- Infection Control, and Dept. of Microbiolog/ID, and antimicrobial stewardship programme - Dr Nicola Fawcett- Registrar Acute/General Medicine, working with the stewardship programme.
Providing data –
Acute/General Medicine Department – list of sequential medical admissions.
Medical Records – providing patient notes
Comparators
Criteria
What is to be measured?
1) All patients with evidence/suspicion of infection should be started on antibiotics:- Antimicrobial prescription (drug chart)- Clinical diagnoses and differential diagnoses - categorised into infection/possible infection- Clinical information recorded in notes which provides objective clinical evidence of possible
infection (observations, presence of possible infection on radiology reports, biochemical tests – White cell count and CRP)
2) 48hr antimicrobial prescribing decision- Record in notes of formal decision,- Whether the patient fulfilled criteria for de-escalation (clinical improvement, able to take oral
therapy)- Whether there was de-escalation by 48hrs from iv to po therapy- Whether patient fulfilled criteria for narrowing antibiotic cover (new microbiology/clinical results)- Whether they were switched to narrow spectrum cover- Whether their duration was reviewed appropriately
3) With regards the Trust objectives outlines in 4) and 5)- Development of Healthcare associate infection- Length of stay, Clinical cure rate,30 day mortality, Readmission rate
Standards
What standard has been set to achieve?
No formal standards were set in the guidance document.
This is the first round of our audit – we aim to achieve 80% compliance.
We expect the first round of audit to show compliance below this level, and will be feeding back the results of the audit to the general medical physicians, with the aim to re-audit and achieve this compliance .
This audit will form the basis for a regular audit cycle, as recommended in the guidelines.

Ethical Considerations
Ethical issues
Consider patient information/ sensitivity Data source
There will be no direct patient contact – all information will be recorded from clinical notes. We will not record patient name. We will be recording clinical data and hospital number, and we will be storing the data directly onto the secure hospital infection control drive, which is resctricted access, and accessible only through hospital computers with password protection.
User involvement
Are patients involved in the project design?
How will patients be informed of findings?
The Author of the guideline recommending the regular audit activity is the Advisory Committee on Antimicrobial Resistance, and this includes a patient representative/lay member.
There are no plans to directly inform patients of the findings, but the body of data will go towards informing the Department of Health about antimicrobial prescribing in secondary/tertiary care.
Methodology
Method
How is the audit to be carried out? (E.g. case note review, patient or staff questionnaire, observation, etc.)
Case note review
Sample
What will the sample size be?
Population?
1 week of sequential medical admissions – approximately 600 patients.
Resource implications
Medical records?
Questionnaires?
Postage?
1 full time data collection Doctor - provided by stewardship programme.
Medical records – likely to need to find approximately 50-100 notes for review of patients with adverse 30 day outcome (readmission, mortality of estimated 10%)
Timescales
Data Collection starts Date: Feb 2013 (aim 16th Feb 2013)
Data collection ends Date: Feb 2013 (aim 23rd Feb 2013)
Report due Date: March 2013
When will the audit report and any follow up be presented?
Division/Directorate Governance meeting (All projects)
Date: April 2013 – Infection Control
Trust Clinical Audit Committee
(as appropriate)
Date: If required
Other Please state: ………………………Date:.
Responsibilities
Presentation of Report Dr N Fawcett
Dissemination of report
Dr N Fawcett and Infection Control/Dept Microbiology
Implementation of Action Plan
Antimicrobial Stewardship team, Infection Control/Dept Microbiology
Assurance
Approved by
(Clinical Director
or designate)
I confirm that this project is appropriate, has been quality assured and is to be added to the Trust Clinical Audit programme
Signature
This should be sent electronically from outbox of Approver
Name: Job Title:
Date Email:
Send completed form to [email protected]
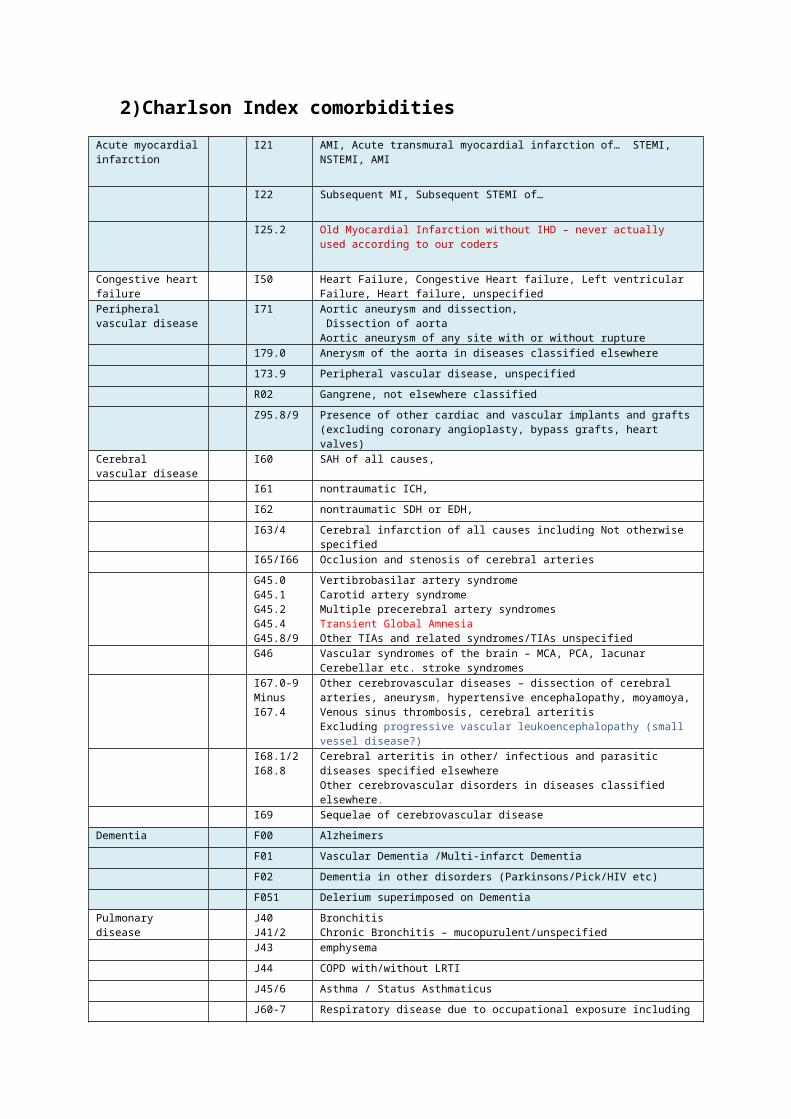
2)Charlson Index comorbidities Acute myocardial infarction
I21 AMI, Acute transmural myocardial infarction of… STEMI, NSTEMI, AMI
I22 Subsequent MI, Subsequent STEMI of…
I25.2 Old Myocardial Infarction without IHD – never actually used according to our coders
Congestive heart failure
I50 Heart Failure, Congestive Heart failure, Left ventricular Failure, Heart failure, unspecified
Peripheral vascular disease
I71 Aortic aneurysm and dissection, Dissection of aortaAortic aneurysm of any site with or without rupture
179.0 Anerysm of the aorta in diseases classified elsewhere173.9 Peripheral vascular disease, unspecifiedR02 Gangrene, not elsewhere classifiedZ95.8/9 Presence of other cardiac and vascular implants and grafts (excluding coronary
angioplasty, bypass grafts, heart valves)Cerebral vascular disease
I60 SAH of all causes,
I61 nontraumatic ICH,I62 nontraumatic SDH or EDH,I63/4 Cerebral infarction of all causes including Not otherwise specifiedI65/I66 Occlusion and stenosis of cerebral arteriesG45.0G45.1G45.2G45.4G45.8/9
Vertibrobasilar artery syndromeCarotid artery syndromeMultiple precerebral artery syndromesTransient Global AmnesiaOther TIAs and related syndromes/TIAs unspecified
G46 Vascular syndromes of the brain – MCA, PCA, lacunar Cerebellar etc. stroke
syndromesI67.0-9Minus I67.4
Other cerebrovascular diseases – dissection of cerebral arteries, aneurysm, hypertensive encephalopathy, moyamoya, Venous sinus thrombosis, cerebral arteritisExcluding progressive vascular leukoencephalopathy (small vessel disease?)
I68.1/2I68.8
Cerebral arteritis in other/ infectious and parasitic diseases specified elsewhereOther cerebrovascular disorders in diseases classified elsewhere.
I69 Sequelae of cerebrovascular diseaseDementia F00 Alzheimers
F01 Vascular Dementia /Multi-infarct DementiaF02 Dementia in other disorders (Parkinsons/Pick/HIV etc)F051 Delerium superimposed on Dementia
Pulmonary disease J40J41/2
BronchitisChronic Bronchitis – mucopurulent/unspecified
J43 emphysemaJ44 COPD with/without LRTIJ45/6 Asthma / Status AsthmaticusJ60-7 Respiratory disease due to occupational exposure including pneumoconiosis
(incl TBpneumoconiosis) farmers/bird fanciers lung etc etc except chemicals/gas/vapors and pneumonitis due to liquids/vomit/solids
Connective tissue disease 1
M32M33.2M34M353
SLE incl Drug-induced SLEPolymyositisSystemic Sclerosis and all forms of CREST/etcPMR(excepting other vasculitides!)
M05.01,23,8
Systemic Rheumatoid - Feltys,Rheumatoid lung disease, vasculitis, multiorgan involvement etc. (excluding seropositive rheumatoid arthritis unspecified)
M060063069
Rheumatoid arthritis, Rheumatoid nodule, Seronegative Rheumatoid, (excepting Adult onset stills, rheumatoid bursitis, inflammatory polyarthropathy, rheumatoid, unspecified) )
Peptic ulcer disease K25K26K27K28
Peptic/Gastric/Duodenal/Jejunal ulcer, acute/chronic, with/without perforation/haemorrhage
(excludes GORD, oesophagitis, gastritis)Liver disease(Nonsevere)
K70.2/3 Alcoholic cirrhosis, fibrosis and sclerosis, (excludes alcoholic liver disease, alcoholic hepatitis,)
K717 Toxic liver disease with fibrosis/cirrhosis (excludes toxic liver disease with other sequelae incl. hepatitis)
K73 Chronic hepatitis of multiple causesK74.2-6 Hepatic fibrosis/sclerosis
Fatty liver diseaseBiliary CirrhosisOther inflammatory liver diseasesK75 not included – autoimmune hepatitis , and K76 –infarction, necrosis, other inflammatory liver diseases, liver disorders in diseases classified elsewhere – hepatorenal and portal HTN – severe liver disease )
Severe liver disease K72.1K72.9
Chronic Hepatic FailureHepatic failure, unspecified(does not include K72- hepatic failure not otherwise specified/, acute and subacute hepatic failure)
K76.6K76.7
Portal hypertensionHepatorenal syndrome (does not include – hepatic veno-occlusive disease)
Diabetes 1 E101.5,9E111.5.9E131.5.9E141.5.9
Insulin-Dependent Diabetes/Type I DiabetesNIDDM/ T2DM/Other/ Unspecified Diabeteswith ketoacidosis, peripheral circulatory complications/ without complications (excepting malnutrition-related diabetes)
Diabetes with complications 2
E102.3.4E112.3.4E132.3.4E142.3.4
Diabetes etc with coma, renal, ophthalmic, neurological, multiple or other/unspecified complications
Hemiplegia or paraplegia
G81G82.0-2G04.1
HemiplegiaParaplegia (spastic/flaccid) (excludes tetraplegia)Tropical spastic paraplegia
Renal disease 2 N01N03N05.2-6N07.2-4
Rapidly Progressive Nephritic syndromeChronic Nephritic SyndromeUnspecified Nephritic SyndromeHereditary Nephropathy (excluding – haematuria, Nephrotic syndrome, isolated proteinuria with specified morphological lesion, glomerular disorders in other diseases – diabetes, endocrine, CTD)
N18N19
Chronic Renal Failure, CKDUnspecified Renal Failure(would not include these in absence of specifying renal failure - TIN, reflux uropathy, hydronephrosis, drug induced nephropathy, Acute Renal Failure-
N17)N25 Renal osteodystrophy
Cancer C0-9 Cancer!C4 except C4.2 Excluding – malignant neoplasm of skin (if not specified as melanoma, kaposi’sC7 except C7.7-9 Secondary malignant neoplasm of… goes under metastatic cancerC88.3, 88.7 88.9
A few haematological malignancies which are felt to be nonmetastatic or not specified enough - (malignant immunoproliferative disease/other/unspecified/small intestine)
C9 Except - panmyelosis
Metastatic cancer C7.7-9C80
Secondary neoplasmHaematological malignancy all causes (except a few which go into plain cancer -see above)
HIV B20, B21, B22, B23, B24
HIV comprehensive

3) Epi-info Information
Epi-Info Supplementary Material
Tips 1) Name your fields well! I’ve already pre-named the fields in my template, but if you want to
change or use an alternative naming system, if you make sure you’re systematic and consistent it will make your life much easier. Mine isn’t perfect but hopefully it’s not awful…
2) If you’re entering a large volume of text – choose the multiple lines field3) Avoid copy/pasting to create new fields – it gets very confused4) Create a ‘messing around with’ form to try out how your edits work5) Don’t use the Date/Time function – it gets MASSIVELY confusing. It’s also not that easy to
enter. Whilst in an ideal world it would be great, most of the calculations we do are based on day, or on hour, but you hardly ever need the two together, and the payoff for easy use of your data is more than worth it.
6) Use the ‘data dictionary’ function to check your field names
A few notes on form design I’ve learnt
Good/bad data management practice in rather prolonged youtube comedy skit:
http://www.youtube.com/watch?v=N2zK3sAtr-4
1) Name your fields well!! It streamlines analysis massively. Using the key above means you can slot in extra fields and they come out in the right place. I tend to name all labels/boxes/things I’m never going to analyse starting with z so they don’t clutter up my form.
2) Setting the tab order – Epi info allows you do really quick data entry by pressing tab to go through fields. Get it right and you’ll be really speedy. Read about how to set this
3) Creating automatic entry- (ie when you get to a field it auto-fills) - can be created using the code function in epi-info - check it out – it’s like very basic logic code and fairly easy to create. Eg. click B1ConsPTWR – before – then ASSIGN field B1ConsPTWR = “MRConsultant”.
4) Creating ‘skip’ fields. More logic! You may want to forego this as you can get it wrong and create frustration for yourself. I’ve got a couple of examples in the code already. Eg IF Field1 = No then GOTO Field 3 Other GOTO Field 2. See how you get on/if you want to try.
5) Don’t copy/paste to create new fields- it gets confused! Best way is to select the fields you want to repeat, and right click and create template. Then drag this in.
6) If you want to edit your form before you start collecting data, no problem. If you want to edit it after collecting data, this can be a problem. Epi-info doesn’t allow you to edit the names of existing field if you’ve collected data. If you’ve collected data on a form it also doesn’t allow you to edit details of new fields once you’ve created them.
7) My solution is – do a few test runs, get the form working well. You’ll find a few things you need to edit. Go into create form - open the form – go to the menu bar –Tools- and select- delete data table. Close the form and close form editor. Reopen it and you can now edit the fields. When you then open up the form in ‘Enter Data’ you’ll get an error message the first time. Don’t worry. Close it and reopen it and it’ll work the second time.
8) The ‘create table’ feature is quite powerful but quite difficult to get used to – have a play around with it in another form before you try and create one on your full form and cause problems
9) When creating drop down lists (‘legal values’) always consider the possibility the information may not be availiable and make it very clear from your choices what is actually happening. Eg. recording of sepsis – if you just have - Sepsis status: ‘no sepsis, sepsis, severe sepsis,septic shock’ if there’s nothing in the notes – what do you do? Leaving blank could mean – I forgot to enter this, or that there was nothing in the notes about it. Also, they might have been erroneous in their assessment. So instead say: Sepsis (recorded in notes) ‘not recorded, no sepsis, sepsis, etc) Also consider having ‘other’ fields.
10) The ‘command’ button which can make text pop up (eg list adverse reaction descriptions) – can be useful – but the text it displays has to be on one line without spaces between lines as it doesn’t like these.
How epi-info saves your data in files and backing up
Epi-info is very helpful in how it saves your data. If you go to the downloaded epi-info folder, and go into the ‘project’ folder, you’ll see each new project you create will have it’s own separate folder, together with the form, and an access database file. These can be copied/pasted, dragged, dropped and still work fine.
I’d suggest collecting your data on a fast, easy to access place- if your trust is happy, on an encrypted laptop should be fine. Then to save it to a trust password protected drive of your choice regularly
(like after ever y significant day of data entry) with a date. Eg AbxAuditProject1 20130702 (year 2013 month july 2nd - if you do it in reverse order it ‘autosorts’ to date order)
Epi info and spreadsheets
Epi-info will save each page of the form as a separate spreadsheet, and each table you create in the form as another spreadsheet.
Each list of ‘drop down options menu’ (called ‘legal values’) that you create – epi-info will create ANOTHER spreadsheet!
If you then edit or re-use the saved legal values – it’ll create ANOTHER spreadsheet and link it to your existing legal values.
This leaves you with loads of spreadsheets you’re never going to want to use, or to mess around with!
Focus on the FormOne1 FormOne2 etc
To link the spreadsheets (so you can compare data on Page 1 with the table on page 2 etc)
Each new entry (new patient) will have a unique identifier ‘globalrecordid’. When you create a related spreadsheet, this spreadsheet will automatically then create an ‘FKEy’ which is identical to the Globalrecord ID.
The best thing in access is to learn about relationships, and how to create them, using the process:
To link to other tables –
Key: GlobalrecordID (on master form) - FKey (on linked spreadsheet)
(Don’t use GlobalrecordID –GlobalrecordID – it doesn’t work!)
How it records data in numeric form
Checkboxes; Unchecked = “0” Checked = “-1”.
Radio buttons: Unchecked - no value Option 1 = “0” Option 2 = “1” Option 3 =”2” (ARGH! I KNOW! Best to know this now, rather than when you’ve assumed that 1 =1 and 2=2 though…)

Other random bits
If you’ve got long descriptives of categories, you can use the comment legal function.
Eg. Nursing home resident
Y- Yes
N – No
Unk- I literally have no idea as this was not recorded in the notes
Whilst you can select the very long sentence from dropdown, it will record the data as Y N and Unk only.
Related Documents











