WHO/CDS/CSR/DRS/2001.10 ORIGINAL: ENGLISH DISTRIBUTION: GENERAL Antibiotic resistance: synthesis of recommendations by expert policy groups Alliance for the Prudent Use of Antibiotics World Health Organization ANTIBIOTIC RESIST ANCE: SYNTHESIS OF REC OMMENDA TIONS BY EXP ERT POLICY GR OUPS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Copies can be obtained from the CDS Information Resource CentreWorld Health Organization, 1211 Geneva 27, Switzerland
fax: +41 22 791 42 85 • email: [email protected]
WHO/CDS/CSR/DRS/2001.10ORIGINAL: ENGLISHDISTRIBUTION: GENERAL
Antibiotic resistance:synthesis ofrecommendations byexpert policy groupsAlliance for the PrudentUse of Antibiotics
World Health Organization
ANTIBIO
TIC RESISTANCE: SYN
THESIS O
F RECOM
MEN
DATIO
NS BY EXPERT PO
LICY GRO
UPS
WHO/CDS/CSR/DRS/2001.10ORIGINAL: ENGLISHDISTRIBUTION: GENERAL
Antibiotic resistance:synthesis ofrecommendationsby expert policy groupsAlliance for the Prudent Use of AntibioticsJL Avorn, JF Barrett, PG Davey, SA McEwen,TF O’Brien and SB LevyBoston, MA, United States of America
World Health Organization
A BACKGROUND DOCUMENT FOR
THE WHO GLOBAL STRATEGY
FOR CONTAINMENT OF
ANTIMICROBIAL
RESISTANCE

© World Health Organization 2001
This document is not a formal publication of the World Health Organization (WHO), and all rights are reserved by the Organiza-tion. The document may, however, be freely reviewed, abstracted, reproduced and translated, in part or in whole, but not for sale orfor use in conjunction with commercial purposes.
The views expressed in documents by named authors are solely the responsibility of those authors.
The designations employed and the presentation of the material in this document, including tables and maps, do not imply theexpression of any opinion whatsoever on the part of the secretariat of the World Health Organization concerning the legal status ofany country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines onmaps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended byWHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietaryproducts are distinguished by initial capital letters.
Designed by minimum graphicsPrinted in Switzerland
Acknowledgements
The World Health Organization (WHO) and the Alliance for the Prudent use of Antibiotics (APUA)acknowledge the United States Agency for International Development (USAID) for their concern aboutthe issue of antibiotic resistance and their support in producing this report.
Stuart B. Levy, President of APUA, ensured that the report was accurate and comprehensive and that itwould benefit both Ministers of Health and health care workers at the local level who can make a differ-ence.
Kathleen Young, the Executive Director of APUA, recognized the contribution that APUA could make tosupport WHO’s Global Strategy through this project. She designed the initial format and assured thequality of the report.
Barbara Souder, the Project Director, coordinated all aspects of this report and Margaret Kruse, a scientistand writer, acted as chief technical writer and production engineer.
APUA gratefully acknowledges the assistance of its support staff: Sarann Bielavitz, for summarizing thereports by the expert policy groups; Brian Price for the graphics; Jennifer Mills-Knutsen for administrativecoordination; and Ellen Wells for bibliographic and editorial assistance.
Julia J. Chuang, from Scientific Information Resources, Bristol-Myers Squibb, United States, is gratefullyacknowledged for her research work on Chapter IV.

Contents
iii
WHO/CDS/CSR/DRS/2001.4 DRUG RESISTANC IN MALARIA
List of acronyms v
Executive Summary 1
Introduction Stuart B. Levy 11
Chapter I Improve and expand surveillance Thomas F. O’Brien 15
Chapter II Increase awareness: optimize patient and provider behaviour Jerry L. Avorn 33
Chapter III Strengthen sanitation, infection control, and regulatory measures Peter G. Davey 39
Chapter IV Encourage research and product development John F. Barrett 53
Chapter V Improve antibiotic use in animals Scott A. McEwen 65
Conclusion Stuart B. Levy 81
References 83
Some useful web sites 87
Appendix A Summaries of reports by expert policy groups (1987–2000) 89
Appendix B Local action around the world 125
Appendix C About the authors 153


List of acronyms
AHRQ Agency for Healthcare Researchand Quality, United States
AIDS Acquired Immune DeficiencySyndrome
AIEPI Integrated Management of Child-hood Diseases, Pan AmericanHealth Organization
APO Audit Project OdenseAR antimicrobial/antibiotic resistanceARM antimicrobial resistance manage-
ment/manager/monitorASM American Society for MicrobiologyBBSRC Biotechnology and Biological
Sciences Research Council, UnitedKingdom
BSAC British Society for AntimicrobialChemotherapy
CA-SFM Comite de l’Antibiogramme de laSociété Française de Microbiologie,France
CDC Centers for Disease Control andPrevention, United States
CEM/NET Centro de Epidemiologia Molecu-lar, Portugal/Network for Epide-miological Tracking of AntibioticResistant Pathogens, United States
CISET Committee on InternationalScience Engineering and Technol-ogy, United States
CMO Chief Medical OfficerCNS central nervous systemCPD continuing professional develop-
ment, United KingdomDANMAP Danish Integrated Antimicrobial
Resistance Monitoring andResearch Program
DDA Department of Drug Administra-tion, Nepal
DDD defined daily doseDHHS Department of Health and Human
Services, United StatesDoD Department of Defense, United
States
DTC Drug and Therapeutic Committee,Viet Nam
DVA Department of Veterans’ Affairs,United States
EARS European Antimicrobial ResistanceSurveillance
EMEA European Medicines EvaluationAgency
ENT ear, nose, and throatEPA Environmental Protection Agency,
United StatesESBIC European Society for Biomodu-
lation and ChemotherapyESCMID The European Society for Clinical
Microbiology and InfectiousDiseases
EU European UnionFDA Food and Drug Administration,
United StatesFESCI Federation of the European
Societies for ChemotherapyGAARD Global Advisory on Antibiotic
Resistance DataGAO General Accounting Office,
United StatesGPs General PractitionersHACCP Hazard Analysis, Critical Control
Point, United KingdomHCFA Health Care Financing Adminis-
tration, United StatesHELICS Hospitals in Europe Link for
Infection Control through Surveil-lance
HGOH Hospital Gynecology-ObstetricHanoi, Viet Nam
HIV Human Immunodeficiency VirusHMG His/Her Majesty’s GovernmentHMO Health Maintenance Organization,
United StatesHRSA Health Resources and Services
Administration, Department ofHealth and Human Services,United States
v
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
vi
ICARE Intensive Care AntimicrobialEpidemiology, Centers for DiseaseControl and Prevention, UnitedStates
ICU intensive care unitID infectious diseaseIDSA Infectious Diseases Society of
AmericaIMF International Monetary FundIND investigational new drugIOM Institute of Medicine, United
StatesISC International Society of Chemo-
therapyKOL key-opinion-leaderMDRTB multidrug-resistant tuberculosisMIC minimal inhibitory concentration,
testing methodMRC Medical Research Council,
EnglandMRSA methicillin-resistant Staphylococcus
aureusMSH Management Sciences for Health,
Boston, United StatesNAO National Audit Office, United
KingdomNARMS National Antimicrobial Resistance
Monitoring System, United StatesNATAC National Antibiotic Therapeutic
Advisory Committee, NepalNCCLS National Committee for Clinical
and Laboratory Standards, EuropeNEPI Network for
Pharmacoepidemiology, SwedenNHS National Health Service, United
KingdomNIAID National Institute of Allergy and
Infectious Diseases, United StatesNIBSC National Institute for Biological
Standards and Control, UnitedKingdom
NICE National Institute for ClinicalExcellence, Great Britain
NICE Nosocomial Infection Control inEurope
NIH National Institutes of Health,United States
NINSS Nosocomial Infection NationalSurveillance Scheme
NISS Nosocomial Infection SurveillanceSystem
NME new molecular entityNSG National Steering Group
NNISS National Nosocomial InfectionsSurveillance System
OIE Office International des EpizootiesOTA Office of Technology Assessment,
United States CongressOTC over the counterPAHO Pan American Health Organiza-
tionPCR polymerase chain reactionPHCP/GTZ Primary Health Care Project/
Deutsche Gessellschaft fürTechnische Zusammenarbeit
PHLS Public Health Laboratory Service,England and Wales
PHON Pharmaceutical Horizon of NepalPRP penicillin-resistant pneumoniaPRSP penicillin-resistant Streptococcus
pneumoniaeQC quality controlRCCDC Regional Center of Communicable
Disease Control, Malmo, SwedenR&D research and developmentRTI respiratory tract infectionSIGN Scottish Intercollegiate Guideline
NetworkSMA Scottish Microbiology AssociationSMAC Standing Medical Advisory
Committee, United KingdomSRH Smolensk Regional Hospital,
RussiaSTD sexually transmitted diseaseSTRAMA Swedish Strategic Program for the
Rational Use of AntimicrobialAgents and Surveillance ofResistance
TB tuberculosisTIGR The Institute for Genomic
Research, Maryland, United StatesTSN The Surveillance Network,
California and Virginia, UnitedStates
USAID United States Agency for Interna-tional Development
USDA Department of Agriculture, UnitedStates
UTI urinary tract infectionVRE vancomycin-resistant enterococciWB World BankWHO World Health OrganizationWMA Welsh Microbiological AssociationWP Working PartyWTO World Trade Organization

1
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Executive Summary
APUA also collected information from their in-ternational chapters about experiences at the locallevel; these reports, reflecting the views of APUAChapters and not necessarily reflecting nationalpolicy, are included in Appendix B.
After review, analysis and update, and with ad-ditional insights from the authors of the individualchapters of this review, the key recommendationsemanating from the 25 expert reports are summa-rized below under the following headings:
• Increase awareness of the antibiotic resistanceproblem
• Improve surveillance of antibiotic resistance
• Improve antibiotic use in people
• Regulate antibiotic use in animals
• Encourage new product development
• Increase resources to curb antibiotic resist-ance in the developing world
• Increase funding for surveillance, research andeducation.
Under each heading recommendations havebeen organized on the basis of the suggested levelof decision-making necessary for implementationof the intervention i.e., “who can do what”.
A more detailed analysis of these recommenda-tions is provided by the author of each chapter.
Increase awareness of the antibioticresistance problem
For real reforms in the use of antibiotics to occur,individuals in the general public and in publichealth and provider groups at the international,national, and local levels must take ownership ofthe problem and provide leadership to reverse thispublic health crisis.
International organizations
• Obtain worldwide commitments to establishprudent antibiotic use policies.
In the not too distant past, antibiotics could becounted on to treat a bacterial infection. Those daysare almost gone, as bacteria have emerged that areresistant to each of the antibiotics currently on themarket. Deaths have occurred as a result of untreat-able bacterial infections. This trend is expected tocontinue unless the problem of antibiotic resist-ance can be curbed. In response to this threat, theWorld Health Organization (WHO) has workedwith many partners, including the Alliance for thePrudent Use of Antibiotics (APUA), to develop theWHO Global Strategy for Containment of Anti-microbial Resistance (26).
As part of the development process of the WHOGlobal Strategy, WHO commissioned a series oftechnical reviews. APUA responded to WHO’srequest to review reports on antibiotic resistanceprepared by prestigious scientific and governmen-tal organizations over the last two decades. The pur-pose of this review is to identify areas of consensusin the experts’ recommendations in the selectedreports, update the findings, consider the barriersto concerted action and suggest ways to move fromrecommendations to action.
Twenty-five expert reports (1–25—see Table 1,Table 3 and Appendix A) compiled by scientificand medical authorities were selected for this re-view by APUA because they are highly referencedin the literature and reflect extensive deliberationsby a wide variety of key expert policy groups. Indeveloping this synthesis, APUA consulted fivemedical and scientific experts on antibiotic resist-ance who reviewed relevant sections of the reports.Their reviews are presented in Chapters I–V andcover the major areas of intervention, i.e., surveil-lance, education of patient and provider behaviour,prevention (including sanitary and infection con-trol), research and product development, and anti-biotic use in animals. Each author focused on thosereports with extensive subject matter related to theirarea of investigation. In addition to summarizingfindings from the expert policy reports, updatedinformation, references and authors’ insights wereadded.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
2
National and municipal organizations
• Publicize the outcomes of programmes from othercountries: Communicate global trends in antibi-otic resistance with potential local impact, suchas the results of the European Union’s legisla-tion against use of antibiotics in growth promo-tion. Collect and publicize the economicconsequences, or lack thereof, of Denmark andSweden’s complete ban on growth promoters.
• Educate the general public: The United Kingdom’scampaign to “cherish and conserve your naturalflora” pointed out the beneficial aspects of bac-teria which can be obliterated by excessive anti-biotic use. A campaign about proper antibioticuse should be aimed at young children, theparents of young children, workers in day carecentres, schoolteachers, those who work in agri-culture, and policy-makers in all areas.
• Promote communication: Facilitate communicationamong academic institutions, government agen-cies, those who pay for health care, and pharma-ceutical manufacturers to reduce the extent towhich such groups act at cross purposes in rela-tion to antibiotic use and infection control.Provide materials to support intervention pro-grammes and utilize communication tools suchas the media and the Internet.
• Evaluate the curricula of universities: Undergraduate,postgraduate and continuing education pro-grammes at veterinary, medical, pharmacy, andnursing schools should be evaluated to ensurethat prudent antimicrobial use and resistance aregiven high priority. Courses should makestudents more aware of how to evaluate promo-tional materials and what questions to ask dur-ing a sales presentation.
Health care institutions
• Use effective teaching methods for educating pre-scribers:
— Use group problem-solving sessions, roleplaying, lectures.
— Focus on clinical issues one at a time.— Use an educational outreach worker for train-
ing at the office.— Use opinion leaders or district-level staff as
trainers. — Repeat sessions to reinforce message.— Apply community-based case management
interventions.
Health care workers
• Educate the general public:
— Physicians: Discuss proper antibiotic usewith all patients.
— Veterinarians: Discuss ways to minimize an-tibiotic use with animal owners, such as im-proved farm hygiene and alternatives toantibiotics as growth promoters.
Improve surveillance of antibioticresistance
The urgent recommendation for surveillance ofantimicrobial resistance and plans for performingsurveillance have been elaborated upon over the pasttwo decades. Over that same period a succession ofunexpected, new and life-threatening resistanceproblems have emerged and spread throughout theworld. These global outbreaks have had littlemonitoring to support their ultimately failed con-tainment. Only inadequate and fragmentarysurveillance systems exist today.
National and municipal organizations
• Coordinate local surveillance networks: Public healthdepartments can take the initiative to contactmedical centres and develop a surveillance net-work. If an existing privately-initiated networkexists, the public health department should sup-port and help that network to grow.
• Recruit leaders for surveillance networks: The publichealth department cannot pay for all the par-ticipants that a surveillance network requires. Ithas to find leaders within the network and usetheir help to motivate all the participants to worktogether on the surveillance network.
• Support a reference laboratory: The public healthdepartment should support a reference labora-tory, hitherto lacking in many surveillance net-works. The network initiator’s laboratory maybecome the reference laboratory. With proper sup-port, the reference laboratory can appreciably im-prove the performance of the network’s laboratoriesand connect, integrate, and interpret their data.
• Share results of surveillance with international organi-zations.
• Monitor resistance in food animals: Undertake regu-lar monitoring for resistant bacterial pathogensand commensals in food-producing animalpopulations and animal-based food products.
3
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
• Monitor sentinel human populations: Evaluate theusefulness of monitoring sentinel humanpopulations (e.g. farm and abattoir workers) andpeople in the community for infection and/orcolonization with resistant bacteria.
Health care institutions
• Develop local surveillance networks: Medical centrescan support data gathering within their centreand join or start a local surveillance network.
• Maintain a laboratory with adequate quality assuranceand trained technicians.
Health care workers
• Initiate a local surveillance network: A microbiologistor infectious disease specialist can initiate anantimicrobial resistance surveillance network;most of the networks started in various coun-tries began in this way. The leadership and in-terest of these individuals and their colleaguescan keep these networks functioning.
Pharmaceutical companies
• Undertake post-marketing surveillance to detect emer-gence of resistance to new antibiotics.
• Support surveillance networks: Support the work ofa local surveillance centre through funding and/or surveillance projects.
Improve antibiotic use in people
National and municipal organizations
• Enforce the prudent use of antibiotics: For example,the United States federal government couldadopt a strategy making the implementation ofstate policies to curb the misuse of antimicro-bial drugs mandatory before states could receivefederal funds earmarked for public health.
• Create national and regional guidelines: Nationalstandards and guidelines should be created forcommunity infection control management withthe following features:— A requirement that every district health
authority should have at least one commu-nity infection control nurse.
— The ability to be adapted at the local level.— An implementation protocol that includes
who is being targeted; how to stage the im-plementation; how to manage the support-
ers and detractors; how to reach goals, andways to build on existing audit systems.
• Update guidelines based on surveillance data: Regu-larly update guidelines for antimicrobial usebased on resistance surveillance data.
• Eliminate financial incentives that promote the misuseof antibiotics: In countries where governmentssubsidize the purchase of antimicrobial drugs,legislative or regulatory changes in these subsi-dies could lead to a decline in the use of thedrugs. Governments could investigate the effectof changes in reimbursement on the prudent useof antibiotics and on surveillance of prescribingor resistance; for example, the United StatesCongress Office of Technology Assessment(OTA) identified a potential problem with Med-icaid and Medicare reimbursement policies.
• Monitor advertising: Develop and enforce ethicalstandards concerning advertising of antibioticsto the general public to counteract the strongcommercial pressures from manufacturers to in-crease utilization of antibiotics and antibacterials.
• Consider the impact of new drugs on resistance duringthe drug approval process: Consideration of resist-ance issues should be required prior to drugapproval for human, animal, or plant use.
• Limit general access to new drugs.
• Establish post-marketing surveillance accords withproducers to ensure early detection of emergingresistance to new drugs.
Health care institutions
• Establish an Infection Control Committee for surveil-lance of infection; identification of outbreaks;implementation of effective control measures(e.g., hand washing); sterilization and disinfec-tion of equipment and supplies.
• Establish a Drugs and Therapeutics Committee to evalu-ate antibiotic use data, resistance patterns,efficacy and cost; make recommendations forproper antibiotic use that are appropriate to aparticular clinical setting and population.
• Establish guidelines for appropriate antibiotic use: Formaximum benefit, such guidelines should be:
— Based on evidence.— Relevant and appropriate to the clinical and
microbiological issues of a given population.— Developed with the involvement of the prac-

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
4
titioners (and potentially the patients) whowill be using them.
— Disseminated not simply via printed memo-randa, but rather through the use of inter-active strategies oriented to changebehaviour.
• Appoint an antimicrobial resistance monitor to:— Serve as a local resource to follow the cur-
rent literature on antibiotic resistance.— Analyse local data.— Propose and implement strategies for con-
trol and resistance.— Work with clinicians on the care of specific
patients.• Reduce the spread of infection: Adopt Centers for
Disease Control and Prevention (CDC) recom-mendations for isolation of patients colonizedwith resistant bacteria.
• Create pharmacy reports: Hospitals should produceregular reports about pharmacy supplies to wardsor clinics in the format of defined daily dose(DDD) per 1000 beds. Review the pharmacyreports periodically with the laboratory resultsto detect problems of resistance early.
• Establish and disseminate essential drugs lists: Basedon those such as the World Health Organiza-tion Model List of Essential Drugs, to helpsimplify antibiotic choices for practitioners aswell as make them more clinically appropriateand cost-effective.
• Educate employees: Promote education about theantibiotic resistance problem through:— Providing ongoing supervision and monitor-
ing of practice.— Instituting regular audit and feedback of
prescribing patterns.— Teaching through the development of group
processes.— Developing standardized treatment guide-
lines.— Using problem-oriented training.— Providing targeted in-service training of
health workers.
• Maintain a laboratory: with adequate quality assur-ance and trained technicians. Use sterile sup-plies and sterile procedures: Gloves and gownsare important pieces of protective equipment.
Health care workers
• Prescribe antibiotics prudently through:— Avoiding antibiotics for simple coughs and
colds.— Avoiding using antibiotics for the treatment
of viral sore throat.— Limiting antibiotic use in uncomplicated
cystitis in healthy women to three days.— Limiting telephone prescription of antibiot-
ics to exceptional cases only.— Avoiding using broad-spectrum antibiotics
when narrower-spectrum agents would workas well.
— Basing the antibiotic prescription on micro-biological culture results whenever possible.
— Modifying the regimen over time as required.— Considering cost-effectiveness in choosing an
antibiotic regimen.
• Improve hygiene: Perform regular hand washing.Failure to cleanse hands after each patient con-tact spreads infection.
Improve antibiotic use in animals
Antibiotics are used not only to combat bacterialinfections in animals but also as growth promotersin animals raised for meat (referred to as food ani-mals). In some countries, about 50% of total anti-microbial production by weight is used in animalagriculture. As in people, the excessive antibioticuse in animals provides intensive training insurvival-of-the-fittest to the resident bacteria. Areservoir of antibiotic resistance is building in thebacteria associated with animals which may betransferred to the bacteria living in humans.
National and municipal organizations
• Increase awareness of the antibiotic resistance problem:Make veterinarians and animal owners aware ofantibiotic resistance impact on humans, and ofthe costs of resistance to themselves, their fami-lies and animals, and to the public. People needgood reasons to modify their behaviours andthese should be provided to them.
• Regulate antibiotic prescriptions for animals: Evaluatethe impact of making all systemic veterinaryantimicrobials available by prescription only. Ifsufficient evidence exists that profits from salesnegatively impact on prescribing, take appropri-ate countermeasures. Address the reluctance orinability to regulate prescribing practices ofveterinarians at the national level.

5
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
• Restrict growth promoter use in animals: Stop usingantimicrobials of a similar class to those usedfor treating humans as growth promoters inanimals.
• Regulate antibiotic use in animals: Establish a regu-latory system to oversee the authorization, dis-tribution, sale and the use of antimicrobials infood-producing animals. Establish a system tomonitor the type and quantity of antimicrobialsgiven to food animals, similar to that forhumans.
• Set a risk standard for resistance: Identify the publichealth risks from antibiotic resistance that areacceptable to society. If acceptable levels formicrobial risks (or “risk standards”) can be agreedupon internationally, quantitative risk assess-ment could be used to identify resistance thresh-olds, beyond which public health impactsbecome unacceptable. If antibiotic resistanceincreases above levels of concern, then incremen-tal interventions up to withdrawal of the drugfrom the market should be considered.
• Consider human and non-human uses simultaneously:A single, multidisciplinary government commit-tee should oversee the regulation of anti-microbials in both human and non-humanfields.
• Monitor advertising: Advertising and promotion ofanimal health products should comply withnational guidelines and codes of practice.
Veterinarians
• Promote the prudent use of antibiotics in animals, inaccordance with similar strategies for humans.Recommended dosages should be optimal fortherapy and minimize the development ofresistance. Prophylactic use should be regularlyassessed for effectiveness and need.
• Develop local guidelines for antibiotic use: Locally de-rived treatment guidelines should include a listof antimicrobials for conditions commonly pre-sented in various species, and offer a rationaltreatment choice based on scientific data. Theseguidelines should address the use of antibioticsimportant to humans such as fluoroquinolones.
Food animal producers
• Improve farm hygiene: Develop and implementstandards of practice to ensure that antimi-
crobials are not used as a substitute for good farmhygiene.
• Reduce use of antibiotics as growth promoters: Reduceexposure of animals to low doses of antimi-crobials for long periods of time (i.e., growthpromoters and prophylactics) if such uses selectfor resistance to drugs used in human medicine.
• Improve animal husbandry: Encourage farmingpractices that reduce the need for prophylacticand therapeutic use of antibiotics. Alternativeways to reduce infectious disease in animals, suchas improved vaccination programmes, enhancedbiosecurity measures, and reduced housingdensity should be promoted when appropriate.This could, however, increase the cost of foodproduction in some countries.
Researchers
• Risk-benefit analysis of growth promoter use: Evalu-ate the nature and magnitude of the impact ofantimicrobial growth promoters and use the in-formation to assist in risk-benefit assessmentsof each use.
• Environmental impact: Conduct pilot studies toassess the extent of environmental contamina-tion by antimicrobial residues and resistantorganisms that enter the soil or water fromhuman and animal waste.
• Food processing and distribution methods: Evaluatethe effect of current food processing and distri-bution methods on the emergence and spreadof resistant organisms.
Encourage new product development
As the current tools used against bacteria becomeless effective, protecting the public from bacterialinfections requires new tools. Pharmaceutical com-panies and related industries must be encouragedto pursue research and development of new pre-ventative and curative measures (such as vaccinesand antibiotics) and new screening and surveillancemethods.
National and municipal organizations
• Provide incentives to industry:— Create policies that give pharmaceutical
companies an extended patent life in ex-change for increased restrictions on the salesof antimicrobials.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
6
— Provide incentives to companies to invest inresearch and development so as to removethe need to re-coup their investment in apredictably poor selling, but medicallyneeded agent.
— Streamline the regulatory process for drugsand products that are critically needed orwhich address infection solutions withoutundermining resistance solutions.
— Provide a mechanism for a government ornot-for-profit organization to assume theleadership (and risk) in developing an essen-tial infectious disease therapy product(vaccine or drug or diagnostic test) if pharma-ceutical industries choose not to do so.Thiswould be analogous to the strategy of indus-try licensing-in from academia by establish-ing the option for the reverse process to occur(license from the industrial concerns).
— Encourage pharmaceutical companies thathad developed antibiotics but never commer-cially exploited them to pursue more anti-microbial research and development if theirearlier antibiotics (now without patent pro-tection) were given extra legal protection,either under patent law or a legal regime likethe Orphan Drug Act.
— Introduce joint funding arrangementschemes for research work between govern-mental agencies and industry.
• Protect intellectual property rights: International lawshould provide intellectual property protectionrights and enforcement to encourage industryto invest in antibiotic research, development, anddelivery in developing countries.
• Facilitate networking: Encourage partnerships be-tween industry, academia, and government tobetter exploit existing and new technologies tocombat antimicrobial resistance (drugs, vaccines,diagnostics).
Pharmaceutical companies
• Increase research and development in several areas:
— Vaccine research and drug discovery.— Pharmacokinetics, pharmacodynamics, and
dosage regimens in relationship to antimi-crobial resistance emergence probability.
— Basic research into the identification andfunction of novel genes to provide industrywith new, defined targets for therapeutic in-tervention.
— Screening methods.— Surveillance tools, including computer pro-
grams for data management and reporting.
Increase resources to curb antibioticresistance in the developing world
Antibiotic-resistant bacteria are found in industrial-ized and developing countries alike and with inter-national travel, can pass easily from country tocountry.
International organizations
• Share results of surveillance internationally: Interna-tional cooperation is needed to disseminate theresults of surveillance among all countries, sothat even those without the infrastructure canuse the results to conduct risk assessment, makepolicy and manage risk.
• Secure technical and financial support for developingcountries: Investigate methods for mandatingtechnical or financial support from industrial-ized countries to developing countries.
• Invest in a worldwide vaccine strategy to reduce antibi-otic use and combat antimicrobial resistance bypreventing infectious diseases in humans.
• Ensure the availability of vaccines and quality drugs:— Initiate major worldwide programmes relat-
ing to formulation and delivery of vaccines.— Strengthen national and international capac-
ity to ensure the availability and quality ofanti-infective drugs.
• Facilitate communication among the countries of theworld:— Introduce a global alert system requiring
national governments to inform worldwidehealth authorities about outbreaks of resist-ant infections.
— Develop a global web site similar to theNosocomial Infection Control in Europeweb site at http://helics.univ-lyon1.fr.
• Safeguard privacy and human rights: Internationalhuman rights law must be taken into accountto set effective public health policies.
• Promote appropriate international laws: Consulta-tions with experts in international law is impor-tant when devising a global strategy for curbingantibiotic resistance.
7
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
National and municipal organizations
• Decrease risk of infectious disease by:— Improving the quality of life and health with
widespread immunizations.— Improving sanitation and water supply
systems.— Emphasizing alternate methods of infection
control, such as bednets in areas at risk formalaria.
• Ensure antibiotic availability: Availability of appro-priate antibiotics for treatment of infections willcontain the spread of infection in general andresistant strains in particular.
• Share resources with other countries: Industrializedcountries should help developing countries builda quality infrastructure to address health needsin the long term, including investment inresearch and development.— Provide support to invest in diseases in the
developing world.— Assist in implementing preventive strategies
through improving social infrastructure andimproving sanitation and water supply sys-tems in developing countries.
— Support developing countries in creatingreliable supply systems.
Increase funding for surveillance, researchand education
Increasing understanding of the bacterial responseto antibiotics and increasing operational researchinto interventions to deal with the antibiotic re-sistance are two major recommendations to helpcurb the antibiotic resistance problem.
National and municipal organizations
• Increase funding for a surveillance network: Publichealth departments need funding to build a sur-veillance network.
• Increase funding for research: Basic and clinicalresearchers need funding to identify new anti-bacterial targets and to better understand anti-biotic resistance mechanisms.
• Increase funding for education: Health care provid-ers and the general public need to be educatedabout the antibiotic resistance problem.
TABLE 1. REPORTS BY EXPERT POLICY GROUPS (1987–2000)
Year Study nature, location,(ref no.) Document title Organization and time Conclusions
1987 Reviews of Infectious National Institutes Six Task Forces, comprised of A global, standardized surveillance system is(1) Diseases Antibiotic Use of Health (NIH), representatives from different recommended as the best way to track
and Antibiotic Resistance Fogarty Center disciplines and countries, studied emerging resistance patterns. ExpandedWorldwide Sponsored by (USA) various aspects of antibiotic studies of the mechanisms of multidrugthe Fogarty International resistance between 1983 and resistance are supported. The authors alsoCenter, NIH 1986. encourage the expansion of central
surveillance systems and the developmentof vaccines and more rapid diagnostic tests.
1990 Healthy People 2000: Public Health Convened consortium in 1987 The keys to meeting the government’s(2) National Health Promotion Service (PHS) with 300 national organizations. objectives on infectious diseases include
and Disease Prevention. (USA) The 2000 Consortium was public education about hygiene andFull Report, With facilitated by the National infection control, education of health careCommentary Academy of Sciences and the providers about disease epidemiology and
Institute of Medicine to assist disease prevention, research on thethe PHS to convene 8 regional improvement of immunizations, diagnostichearings and take testimony techniques and therapies, as well asfrom over 750 individuals. Over immunization and efforts to maintain safe10,000 people responded to the food and water supplies.review and comment period.
1992 Emerging Infections: Institute of Between February 1991 and Surveillance is crucial to the detection and(3) Microbial Threats to Health Medicine (IOM) July 1992, a multidisciplinary control of infectious diseases. Coordinated
in the United States (USA) committee convened to identify efforts of public and private organizations,significant emerging infectious individuals and government agencies mustdiseases and develop recom- be expanded and improved.mendations on how to deal withthem.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
8
Year Study nature, location,(ref no.) Document title Organization and time Conclusions
1994 Addressing Emerging Centers for Disease Plan developed by CDC in The creation of a comprehensive strategy is(4) Infectious Disease Threats: Control and partnership with representatives necessary to address the threat of emerging
A Prevention Strategy for Prevention (CDC) from public and private health infectious diseases. To be most effective,the United States (USA) organizations at the local, state, such a strategy should be integrated with
national and international plans for reform of the larger health carelevels. system.
1995 WHO Scientific Working World Health Summary of International Heavy usage of antimicrobial agents, poor(5) Group on Monitoring and Organization Workshop held by WHO, Geneva, infection control standards, and
Management of Bacterial (WHO) Switzerland Nov. 29-Dec. 2, 1994. environmental contamination withResistance to Antimicrobial antimicrobial-resistant pathogens are keyAgents areas of concern.
1995 Impacts of Antibiotic- Office of Review of scientific literature, Infection control, the optimal use of existing(6) Resistant Bacteria Technology exploration of biological antibiotics, and the development of new
Assessment (OTA) mechanisms behind ABR, and antibiotics should be the primary(USA) research into availability of new approaches to antibiotic resistance.
antibiotics.
1995 Infectious Disease – National Science Report from the CISET Working In order for a global surveillance network to(7) A Global Health Threat and Technology Group on Emerging and Re- be realized, it is necessary to coordinate,
Council (USA) emerging Infectious Diseases strengthen and link existing systems.Convened December 1994. Electronic links would enhance the surveil-
lance capabilities of the US government’sfield stations.
1995 Report of the ASM Task American Society Report of a workshop held on The Task Force stresses the immediate need(8) Force on Antibiotic for Microbiology July 6, 1994. for surveillance of resistance in humans and
Resistance (ASM) animals. They also advise the more prudentuse of antibiotics in human and veterinarymedicine; improved hospital infectioncontrol and guidelines; improvement ofinfection control curricula for all health careprofessionals; better consumer education;and more basic research.
1997 The Medical Impact of the World Health Report of WHO Meeting When creating any public health policies(9) Use of Antimicrobials in Organization Berlin, Germany regarding the use of antimicrobials in
Food Animals (WHO) Oct. 13–17, 1997. livestock production, it is necessary to takeinto account the benefits to productionversus the potential risks to human health.More prudent use of antibiotics is the keyrecommendation, especially when viablealternatives exist.
1997 America’s Vital Interest in Institute of Report of a workshop conducted The improvement of global health, security(10) Global Health Medicine (IOM) in November of 1995. and economic viability depends on
(USA) collaborations among US government healthagencies, as well as partnerships with USindustry, academia and non-governmentalorganizations, other governments and NGOs.
1997 New and Reemerging American Society Analysis of documents on The report recommends increased funding(11) Infectious Diseases: A Global for Microbiology emerging infectious diseases. for research efforts to develop improved
Crisis and Immediate Threat (ASM) diagnostic tests, new antibiotics, andto the Nation’s Health. The vaccines.Role of Research.
1997 Resistant Organisms: Global Royal Society of Proceedings of a conference The abatement of the problem of antibiotic(12) Impact on Continuum Medicine sponsored by 3M Health Care resistance can only be achieved through
of Care (UK) and Regent Medical, London cooperation of prescribers, patients,September 27, 1996. government, pharmaceutical, and
agricultural industries. Surveillance, infectioncontrol, and improved prescribing practicesare all important components of anycollaborative effort.
9
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Year Study nature, location,(ref no.) Document title Organization and time Conclusions
1997 Joint Committee on the Society for Health Publication in Infection Control Antibiotic resistance must be considered a(13) Prevention of Antimicrobial Care Epidemiology and Hospital Epidemiology, global health problem. Responsibility lies
Resistance: Guidelines for of America and Vol.18, No.4, pp. 275–291. with all hospital personnel to controlthe Prevention of Antimi- Infectious Diseases infections and use antibiotics properly, tocrobial Resistance in Society of America help prevent its further spread.Hospitals
1997 Antibiotic Resistance: CIBA Foundation Proceedings of a Symposium Reversal of antibiotic resistance and return of(14) Origins, Evolution, (International and (#207) held at the Ciba susceptible organisms are possible. These
Selection, and Spread Scientific Charity) Foundation, London goals can be achieved through theJuly 16–18, 1996. implementation of rational use guidelines for
new antimicrobials and through thecooperation of prescribers and consumers.
1998 The Current Status of Anti- World Health Report of WHO Workshop (held Europe’s disparate surveillance networks(15) microbial Resistance Organization in collaboration with the Italian would benefit from a pan-European
Surveillance in Europe (WHO) Associaizone Culturale Microbio- coordinating group. Such a group could helplogia Medica) Verona, Italy, to standardize surveillance methodologiesDecember 12, 1997. at the local, national and international levels.
1998 Emerging Infectious Centers for Peer-review Journal: Proceedings Basic research is crucial to the control of(16) Diseases Special Issue Disease Control of the International Conference emerging and reemerging infectious
and Prevention on Emerging Infectious Diseases, diseases. Improvements in hygiene and(CDC) (USA) Atlanta, GA, March 1998. immunization can be very effective methods
of infection control, although often difficultto implement because of human nature.
1998 Preventing Emerging Centers for An evaluation and update of Implementation of guidelines from(17) Infectious Diseases: Disease Control Preventing Emerging Infectious Preventing Emerging Infectious Diseases
A Strategy for the and Prevention Diseases. resulted in decreases in the prevalence of21st Century (CDC) (USA) certain infectious organisms. The authors
expect this follow-up plan to be successful inpreparing the US public health infrastructureto respond to infectious diseases, whetherthey are familiar, of unknown origin, or theresult of bioterrorist attacks.
1998 Antibacterial Drugs in Food and Drug The criteria are suggestions for The criteria are meant to keep the(18) Animal Feeds. Human Administration complying with regulations agricultural industry within what are thought
Health Safety Criteria, (FDA) (USA) mandated by Congress and the to be safe levels of antimicrobial use in food-Guideline 18. Food and Drug Administration. producing animals.
1998 The Path of Least Department of Review of case studies, review The prescription of antibiotics often depends(19) Resistance Health (UK) of the basis and impact of on the attitudes and expectations of patients;
resistance, commission of an the practitioner’s decision must take intoindependent review of evidence. account the greater effect of the prescription,
in terms of increased selection for resistance.A combined approach of practitioner andpublic education is recommended.
1998 Antimicrobial Resistance British Medical Peer Review Journal Cooperation on the part of medical(20) (Entire Journal for Journal (7 editorials and 4 papers). professionals, politicians, the pharmaceutical
September 5, 1998 devoted industry, and patients is necessary to improveto Antimicrobial Resistance) the problem of antibiotic resistance.
1998 Resistance to Antibiotics House of Lords Between July 1997 and March The problem of antibiotic resistance must be(21) and other Antimicrobial (UK) 1998, Sub-Committee members more widely recognized as a serious threat
Agents conducted interviews at the in order to be adequately addressed.Public Health Laboratory Service Continuing professional education wouldand with individual experts in help to achieve such recognition. Locally-the US and UK. They also created antibiotic formularies andgathered evidence from the guidelines, and improved access to micro-agricultural and pharmaceutical biological testing, when practical, are otherindustries, international and important tools for practitioners. The authorsregional health organizations urge caution in the use of antibiotic classesand professional medical and that are prescribed in both human andscientific societies. veterinary medicine.
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
10
Year Study nature, location,(ref no.) Document title Organization and time Conclusions
1998 Antimicrobial Resistance: Institute of Report of a workshop conducted The participants stress the need for national(22) Issues and Options Medicine (IOM) in July of 1997. and global surveillance of antibiotic
(USA) resistance in animals and humans; for moreprudent use of antibiotics, especially in thearea of food production; improved hospitalinfection control and guidelines; patienteducation; continuing education forpractitioners; and more basic research fornew antibiotics and diagnostic tests.
1998 Protecting the Crown Center for Science Compilation of statistics and The authors recommend changes on the part(23) Jewels of Medicine: in the Public information from other of public and private institutions, as well as
A Strategic Plan to Preserve Interest scientific sources. consumers, to prevent the further spread ofthe Effectiveness of (USA) antibiotic resistance. Prevention of infectiousAntibiotics diseases is emphasized over the develop-
ment of new drugs.
1999 The Agricultural Use of General Review consisting of interviews Despite 20 years of discussion among(24) Antibiotics and Its Accounting with representatives from govt government agencies, consensus on the
Implications for Human Office (GAO) agencies, agricultural industry subject of antibiotic use in agriculture hasHealth (USA) and agricultural associations; not been reached. The report recommends
also scientific review, and restriction of antibiotics as growth promotersconsultations with experts. in animals.May 1998–April 1999.
1999 The Use of Drugs in Food National Research The Committee reviewed major The committee’s greatest concern is the(25) Animals: Benefits and Risks Council classes of drugs used in food potential for development of resistance to
(USA) animals; reviewed scientific antibiotics used in human medicine due toliterature; heard testimony on misuse of antibiotics in food animals. Toanimal drug-related issues and avoid any increase in such development, thereviewed relevant federal committee recommends the development ofregulations. new antimicrobials, with possible restrictions
of their use to either human or animalmedicine.
11
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
IntroductionStuart B. Levy
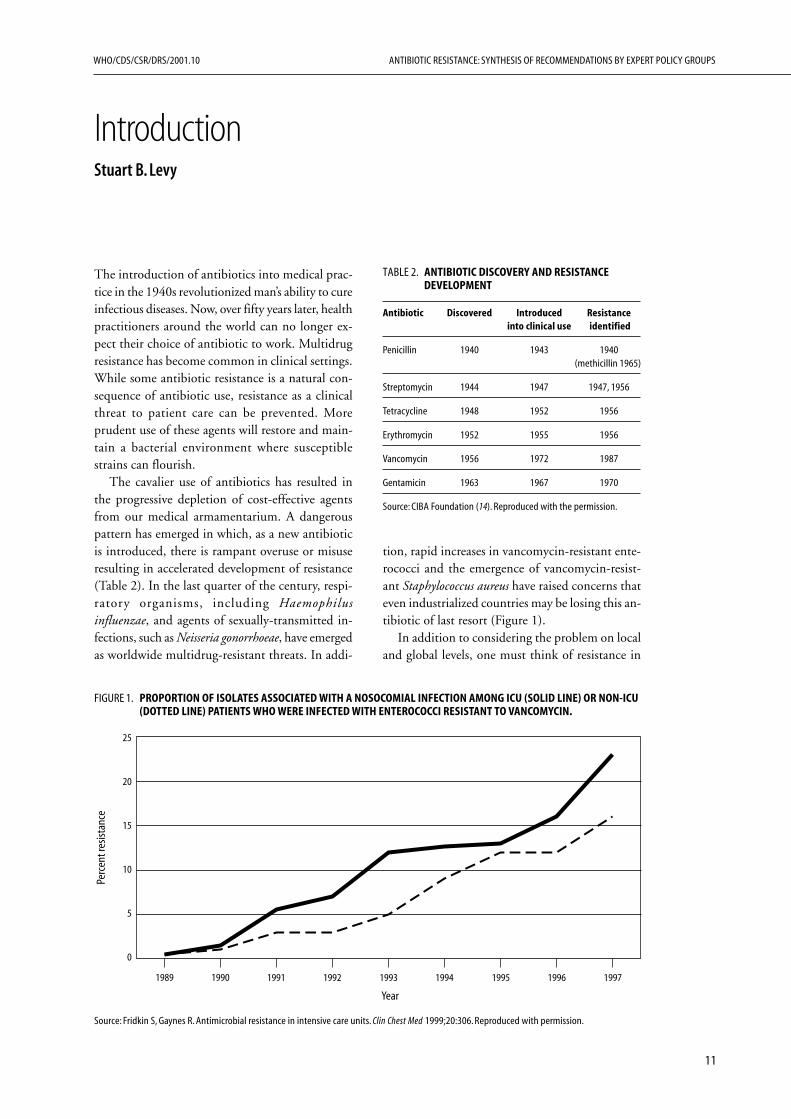
tion, rapid increases in vancomycin-resistant ente-rococci and the emergence of vancomycin-resist-ant Staphylococcus aureus have raised concerns thateven industrialized countries may be losing this an-tibiotic of last resort (Figure 1).
In addition to considering the problem on localand global levels, one must think of resistance in
The introduction of antibiotics into medical prac-tice in the 1940s revolutionized man’s ability to cureinfectious diseases. Now, over fifty years later, healthpractitioners around the world can no longer ex-pect their choice of antibiotic to work. Multidrugresistance has become common in clinical settings.While some antibiotic resistance is a natural con-sequence of antibiotic use, resistance as a clinicalthreat to patient care can be prevented. Moreprudent use of these agents will restore and main-tain a bacterial environment where susceptiblestrains can flourish.
The cavalier use of antibiotics has resulted inthe progressive depletion of cost-effective agentsfrom our medical armamentarium. A dangerouspattern has emerged in which, as a new antibioticis introduced, there is rampant overuse or misuseresulting in accelerated development of resistance(Table 2). In the last quarter of the century, respi-ratory organisms, including Haemophilusinfluenzae, and agents of sexually-transmitted in-fections, such as Neisseria gonorrhoeae, have emergedas worldwide multidrug-resistant threats. In addi-
FIGURE 1. PROPORTION OF ISOLATES ASSOCIATED WITH A NOSOCOMIAL INFECTION AMONG ICU (SOLID LINE) OR NON-ICU(DOTTED LINE) PATIENTS WHO WERE INFECTED WITH ENTEROCOCCI RESISTANT TO VANCOMYCIN.
Source: Fridkin S, Gaynes R. Antimicrobial resistance in intensive care units. Clin Chest Med 1999;20:306. Reproduced with permission.
1989 1990 1991 1992 1993 1994 1995 1996 1997
25
20
15
10
5
0
Perc
ent r
esist
ance
Year
TABLE 2. ANTIBIOTIC DISCOVERY AND RESISTANCEDEVELOPMENT
Antibiotic Discovered Introduced Resistanceinto clinical use identified
Penicillin 1940 1943 1940(methicillin 1965)
Streptomycin 1944 1947 1947, 1956
Tetracycline 1948 1952 1956
Erythromycin 1952 1955 1956
Vancomycin 1956 1972 1987
Gentamicin 1963 1967 1970
Source: CIBA Foundation (14). Reproduced with the permission.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
12
terms of the broader environment in whichmicrobes live. Antibiotic resistance is an ecologicalproblem reflecting the fact that antibiotics aresocietal drugs. Antibiotic use affects not only theindividual, but also the individual’s environmentof microorganisms, which is shared with the rest ofsociety. Susceptible strains are removed and resistantstrains replace them. Thus, any national or localstrategy to curb antibiotic resistance must stress theprudent use of antibiotics so as to allow restorationof the susceptible flora in a particular community.Recognizing the role that microbial ecology playsin housing and propagating resistant pathogens andcommensal organisms will help enormously indeveloping guidelines for antibiotic use. The micro-biologist and clinician, working together as a team,can determine appropriate use in their facility orcommunity.
Selection of reports for this review
As part of the process of development of the WHOGlobal Strategy for Containment of AntimicrobialResistance (26), a series of technical reviews werecommissioned. The Alliance for the Prudent Useof Antibiotics (APUA) responded to WHO’srequest and reviewed reports on antibiotic resistanceprepared by prestigious scientific and governmentalorganizations over the last two decades. Twenty-five expert reports (1–25), compiled by scientificand medical authorities, were selected for this reviewby APUA because they are highly referenced in theliterature and reflect extensive deliberations by awide variety of key expert policy groups. There areother excellent policy reports which have not beenreviewed but which could supplement thoseconsidered here, such as those from Canada,Australia, Finland and Denmark.
The review process
In developing this synthesis, APUA consultedfive medical and scientific experts on antibioticresistance who reviewed relevant sections of theselected expert reports. Their reviews are presentedin Chapters I–V and cover the major areas ofintervention: Chapter I. Improve and ExpandSurveillance; Chapter II. Increase Awareness:Optimize Patient and Provider Behaviour; ChapterIII. Strengthen Sanitation, Infection Control, andRegulatory Measures; Chapter IV. EncourageResearch and Product Development; and ChapterV. Improve Antibiotic Use in Animals. Each author
focused on those reports with extensive subjectmatter related to their area of investigation (seeTable 3). For example, only McEwen (Chapter V)reviewed those reports written specifically onantibiotic use in animals and plants. O’Brienreviewed additional reports (27,28,29,30,31)because they were exclusively about surveillance andintroduced important data and principles revisitedin later reports. In addition to summarizing find-ings from the expert policy reports, updatedinformation, references and the author’s insightswere added where considered appropriate andrelevant by the author. The Summary of Reports,with key conclusions from each, is presented in theExecutive Summary Table 1 together with the KeyRecommendations synthesized under a series ofheadings:
• Increase awareness of the antibiotic resistanceproblem
• Improve surveillance of antibiotic resistance
• Improve antibiotic use in people
• Improve antibiotic use in animals
• Encourage new product development
• Increase resources to curb antibiotic resist-ance in the developing world
• Increase funding for surveillance, research andeducation.
Each set of recommendations is categorized bythe levels of decision-making necessary to initiateaction. A resumé of each of the expert reports re-viewed, prepared by APUA, is contained in Ap-pendix A.
In addition, APUA collected information fromtheir international chapters about a number of cur-rent national and local initiatives, as an illustrationof the power of local movements. Each of theseprogrammes chose a particular feature of the anti-biotic use and resistance problem and put togethera team to address it. Their reports, reflective ofAPUA Chapters but not necessarily reflecting na-tional policy, are included in Appendix B.
Conclusion—A manageable approach atthe local level
Although concerned scientists and prestigious studygroups have met to document the problem of anti-microbial resistance and suggest solutions, the keyplayers who can impact the problem have some-how not been engaged. This review highlights the

13
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
TABLE 3
General review Control & prevention
Public healthReference Trends in Causes & Antimicrobial Economic promotion & PublicNo. (year of publication) diseases & mechanisms use in animals cost of prevention policyShort title resistance of resistance & plants resistance strategies strategies Surveillance
1. (1987) Antibiotic use and anti-biotic resistance worldwide:report of a study sponsored bythe Fogarty International Centerof the National Institutes ofHealth, 1983–1986 x x x x x
2. (1990) Healthy People 2000:National Health Promotion andDisease Prevention x x x
3. (1992) Emerging Infections:Microbial Threats to Health inthe United States x x x x
4. (1994) Addressing emerginginfectious disease threats: Aprevention strategy for theUnited States x
5. (1995) WHO Scientific WorkingGroup on Monitoring andManagement of Bacterial Resis-tance to Antimicrobial Agents x x
6. (1995) Impacts of Antibiotic-resistant bacteria x x x x x x x
7. (1995) Infectious Disease–A Global Health Threat x x x
8. (1995) Report of the ASM TaskForce on Antibiotic Resistance x x x
9. (1997) The Medical Impact ofthe Use of Antimicrobials inFood Animals x
10. (1997) America’s vital interestin global health: Protecting ourpeople, enhancing our economy,and advancing our interests x
11. (1997) New and Re-emergingInfectious Diseases: A GlobalCrisis and Immediate Threat tothe Nation’s Health x x
12. (1997) Resistant organisms :Global Impact on Continuumof Care x x
13. (1997) SHEA Position Paper onPrevention of AntimicrobialResistance in Hospitals x x x
14. (1997) Antibiotic Resistance:Origins, Evolution, Selectionand Spread x x x x x x x
15. (1998) The Current Status ofAntimicrobial ResistanceSurveillance in Europe x
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
14
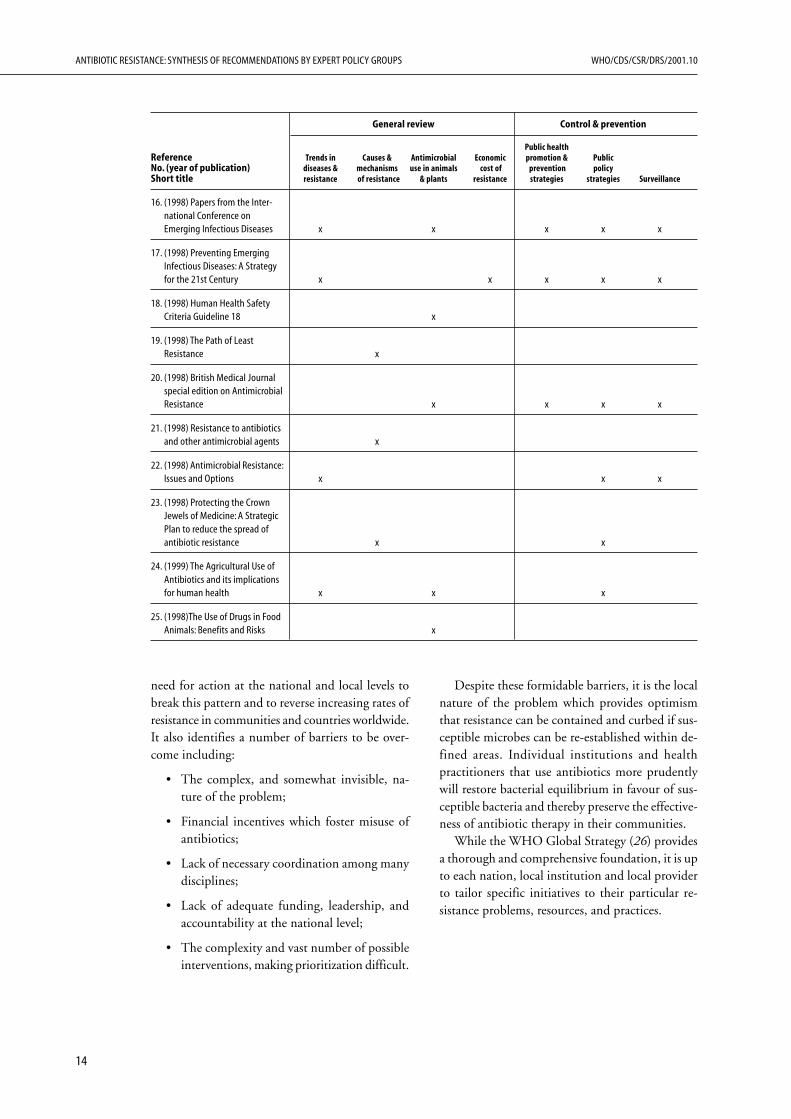
need for action at the national and local levels tobreak this pattern and to reverse increasing rates ofresistance in communities and countries worldwide.It also identifies a number of barriers to be over-come including:
• The complex, and somewhat invisible, na-ture of the problem;
• Financial incentives which foster misuse ofantibiotics;
• Lack of necessary coordination among manydisciplines;
• Lack of adequate funding, leadership, andaccountability at the national level;
• The complexity and vast number of possibleinterventions, making prioritization difficult.
Despite these formidable barriers, it is the localnature of the problem which provides optimismthat resistance can be contained and curbed if sus-ceptible microbes can be re-established within de-fined areas. Individual institutions and healthpractitioners that use antibiotics more prudentlywill restore bacterial equilibrium in favour of sus-ceptible bacteria and thereby preserve the effective-ness of antibiotic therapy in their communities.
While the WHO Global Strategy (26) providesa thorough and comprehensive foundation, it is upto each nation, local institution and local providerto tailor specific initiatives to their particular re-sistance problems, resources, and practices.
General review Control & prevention
Public healthReference Trends in Causes & Antimicrobial Economic promotion & PublicNo. (year of publication) diseases & mechanisms use in animals cost of prevention policyShort title resistance of resistance & plants resistance strategies strategies Surveillance
16. (1998) Papers from the Inter-national Conference onEmerging Infectious Diseases x x x x x
17. (1998) Preventing EmergingInfectious Diseases: A Strategyfor the 21st Century x x x x x
18. (1998) Human Health SafetyCriteria Guideline 18 x
19. (1998) The Path of LeastResistance x
20. (1998) British Medical Journalspecial edition on AntimicrobialResistance x x x x
21. (1998) Resistance to antibioticsand other antimicrobial agents x
22. (1998) Antimicrobial Resistance:Issues and Options x x x
23. (1998) Protecting the CrownJewels of Medicine: A StrategicPlan to reduce the spread ofantibiotic resistance x x
24. (1999) The Agricultural Use ofAntibiotics and its implicationsfor human health x x x
25. (1998)The Use of Drugs in FoodAnimals: Benefits and Risks x

15
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
CHAPTER I
Improve and expand surveillanceThomas F. O’Brien
The groups made generally similar recommen-dations over the two decades, although some of theirmore recent reports have commented on how littlethese recommendations have been implemented.An obstacle may be that surveillance of resistance,as noted, requires an unusual degree of coopera-tion and integration between the efforts of care-givers and public health workers. Caregivinginstitutions are the predominant producers andusers of resistance surveillance data, but publichealth leadership and support is needed to inte-grate the data into larger systems and to collabo-rate in understanding and containing resistance.
Synthesis and summary
Do we need surveillance of antimicrobial resistance?
The groups were nearly all emphatic about the needfor surveillance of antimicrobial resistance, asreflected in their statements:
• “without reliable information … it would beimpossible to find solutions”(2)
• “more systematic surveillance on a much largerscale is needed to provide explanations orremedies”(4)
• The US should “take the lead in promoting thedevelopment and implementation of a compre-hensive global infectious diseases surveillancesystem.”(5)
• “Distribute …software in laboratories to enablethem to monitor their own results for test qual-ity, for infection control problems and for localtrends in resistance, and to enable them also tomerge their results into same-format, isolate-based databases for detailed national and inter-national surveillance of resistance.”(6)
• “There is an urgent need for effective domesticsurveillance of antibiotic resistance in animalsand humans.”(7)
• “A surveillance system is essential for understand-ing the spread of antibiotic-resistant bacteria and
Abstract
Expert groups advising on control of antimicrobialresistance have repeatedly emphasized the need forsurveillance of resistance. This chapter reviews thediscussions and recommendations on surveillanceof resistance in reports issued by sixteen such groupsover the past two decades.
The problem of antimicrobial resistance is enor-mous because of the magnitude of the intercon-necting global bacterial populations it involves. Itis intricate because of the diversity of resistancegenes and genetic vectors responding to differingusage of antimicrobial agents on different parts ofthose populations in different parts of the world. Itis also peculiarly circular since an attempt to cureone patient may eventually prevent cure of another.
For these reasons, as reflected in these reports,resistance presents different problems to a remark-ably wide range of caregivers, policy-makers, andresearchers, and they need different kinds of infor-mation from surveillance. The reports identifyneeds for local information to guide local selectionof agents for individual patients, infection controlin the hospital, public health in the community,and local antimicrobial usage strategy. Differentanalyses are needed at the national level to over-view resistance epidemiology and to set drug policy.Global detection and tracing of emerging problemsare also needed.
The reports recognize that information for sur-veillance of resistance must ultimately begin withdata from microbiology laboratories and that theselaboratories need to be increased and improved.They look to advancing information technology tolink clinical laboratories in networks guided byreference laboratories that would work to bothgenerate and improve the data. They also seek tointegrate this information with additional patientinformation, including patient antimicrobial usage,in order to make better systems for the manage-ment of local resistance. Such data from multiplecentres would also provide more detailed under-standing of the relationship of antimicrobial use tothe spread of resistance.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
16
planning interventions so as to preserve theefficacy of currently available antibiotics.”(9)
• “Establish a system for monitoring bacterialresistance and antibiotic usage.”(10)
• “Redressing these deficits”[in surveillance] “iscrucial in global and national public health terms,and the most powerful case possible must bemade for urgent and substantial response.”(12)
• “Systematic collection of epidemiological dataon resistance should be initiated imme-diately…The costs to the NHS are likely to bemodest compared with many other actions.”(13)
• “Comprehensive surveillance is required to meas-ure the public health impact of antimicrobialresistance and of interventions (including thoseproposed in this report) to minimize antimicro-bial usage.”(14)
• “A critical elemental in addressing the environ-mental impact of antimicrobial resistance iseffective surveillance…With respect to antimi-crobial impact on the environment, surveillanceinvolves not only data on bacterial pathogens,but also data on other microorganisms that arepart of the affected ecosystem.”(15)
• “Surveillance of antibiotic resistance (AR) is criti-cal to provide early warning of emerging prob-lems, monitor changing patterns of resistance,and target and evaluate prevention and controlmeasures.”(16)
What kind of surveillance do we need?
Systems for surveillance of antimicrobial resistancehave many common and interrelated elements,which are mentioned frequently in the reviewedreports. Any one system will be a blend of and abalance between these elements. Report numbersreferenced below for each element do not cite all ofthe reports that touched upon that element, butonly some that are representative or most pertinent.
Antimicrobial resistance is an enormously com-plex subject, dealt with by microbiologists, clini-cians, epidemiologists, pharmacists, basic researchscientists, infection control workers and publichealth workers, etc. They see the problem in dif-ferent ways and, as members of these expert groups,have wanted different kinds of information fromsurveillance of it. Nonetheless, a general consensusabout the elements of surveillance emerges fromthese reports, and their differences often seem com-plementary.
Clinical microbiology laboratory information
The essential basic element of surveillance is infor-mation from microbiology laboratories. Antimicro-bial resistance is ultimately about different kindsof bacteria and their susceptibility to differentantimicrobial agents. Microbiology laboratories arethe only source of such information, and most of itis generated by routine clinical microbiology labo-ratories.
The immediate users of such data from anymicrobiology laboratory are health care workers inthe hospital and the community it serves. They needthis level of surveillance information to treat indi-vidual patients, to update local treatment guide-lines, to observe effects of their local interventionsand to detect, monitor, and contain local spread ofresistant strains (3,6,12,14,15).
The most direct, responsive, and useful way ofproviding local health care workers with the sur-veillance information they need is to file the datafrom their clinical microbiology laboratory in auser-friendly, local electronic database, which theycan query instantly, repeatedly, and in specific de-tail, as problems arise. The World Health Organi-zation (WHO) provides free software for such adatabase (WHONET) and additional software(BACLINK) to translate data into the databasefrom existing local computerized laboratory report-ing systems that lack database capability (6,7,15).
The need for antibiotic use data. In addition to resist-ance data there is need for health institutions andgovernments to collect and review antibiotic usedata. This would allow more precise analyses ofrelationships between antibiotic use and resistance.Much of the antibiotic use data reside within phar-maceutical companies which should be encouragedto share this information with public health agen-cies. Also, governments could set up their own sys-tems and requirements to collect the use data fromhealth care providers and institutions. In addition,post-marketing resistance surveillance should beroutine to detect resistance trends.
Problems with quality of clinical microbiology laboratoryinformation. Several of the groups recognized prob-lems with the existing quality of clinical microbi-ology laboratory data. Quality of testing may beuneven in many laboratories, and there is often noprogramme for quality assurance. These limitationsmay represent lack of funding, supplies, trainingor oversight. Many regions lack microbiology labo-

17
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
ratories altogether, and where they do exist theirservices may be underutilized or improperlyutilized. Information is further diminished if alaboratory reports only the interpretations of sus-ceptibility tests without their actual measurements(12,16).
Recognition of these limitations has promptedrecommendations in the reports reviewed fordevelopment, support, training, improvement andquality assurance oversight of clinical microbiol-ogy laboratories, and for more of them in someplaces. Their improvement is seen as essential for acomprehensive surveillance system and, not inci-dentally, to improve care for the many patientswhose individual treatment is being directly affectedby tests done in those laboratories (6,12).
Problems with analysis of clinical laboratory information.Another limitation of using only clinical microbi-ology laboratory reports, cited by several of thereports, is that it relates to an uncertain populationbase. Prevalence of resistance is commonly expressedas a percentage derived from the number of resist-ant isolates as the numerator with the number ofboth resistant and susceptible isolates as thedenominator.
This is adequate for many practical uses of sur-veillance information, including many at the locallevel such as infection control. It can, however,allow a sampling bias that overstates resistance byignoring susceptible strains obscured by successfultreatment without culture, or by more culturing inplaces where there is more resistance. It also limitsmore formal epidemiological studies of resistanceand its contribution to disease burden (14).
The reports that mention this need for moreappropriate denominators do not specify how toget them. Presumably, the microbiology databaseswould have to be linked to other databases con-taining demographics, diagnoses, etc., which couldbetter characterize the patients. The microbiologydatabases could also be linked with pharmacydatabases in order to identify those patients whowere treated for infection without being culturedbefore treatment. Advances in informatics are nowbeginning to make this a real possibility (14).
Members of some groups wanted to specify inadvance which bacterial pathogens should be in-cluded in surveillance, presumably to minimizework or data storage costs. We have been repeat-edly surprised in recent decades, however, byresistance problems emerging in species where theyhad not been expected (e.g., enterococci). We have
also come to recognize the importance of earlydetection of such new problems (called “alert or-ganism surveillance” or “exception reporting” in onereport). Over the same period, moreover, the costsof data storage and management have plummetedto near trivial levels (7,14).
A similar question about what to include in thedatabase further illustrates differences in viewpoint.Those investigating the evolution or ecology ofantimicrobial resistance see resistance as epidemicsof resistance genes through vast populations of bac-teria that rarely infect. They want surveillance toelucidate and trace how resistance genes emerge,get into vectors and become linked under selectionand co-selection in reservoirs of environmental orcolonizing bacteria before finally entering a patho-genic strain that may infect someone. Theirdenominators are bacterial populations. They thinkthat everything important for resistance happensin the bacteria before the infection begins and theepidemiologists start to count people for theirdenominators.
Advancing information technology has the po-tential to accommodate such diverse views. It canfacilitate entry of data that is well characterized, sothe database can be broadly inclusive at little costand still allow subsequent analyses of any selectedsubsets of the data to be sharply defined. Yourpathogens need not interfere with my commensals,and we may both learn how they interact (4,12,15).
The roles of microbiology referencelaboratories
The reviewed reports identified multiple roles inresistance surveillance for microbiology referencelaboratories (6,14,15).
Surveillance by the reference laboratory. Reference labo-ratories can themselves do surveillance of antimi-crobial resistance. The usual way is for a networkof clinical laboratories to collect designated typesof bacteria from among those they routinely iso-late and ship them to the reference laboratory. Thereference laboratory then retests the susceptibilityof those isolates and may also repeat their identifi-cation.
Reference laboratory surveillance has the poten-tial to test the isolates by more uniform methodol-ogy and against more agents. Testing against moreagents can distinguish fine differences betweenagents and discriminate more resistance pheno-types. Having all of the isolates in one laboratory

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
18
also makes it easier to use newer methods to inves-tigate their genetic relatedness and the molecularbases of their resistance phenotypes.
The limitations of this model of reference labo-ratory surveillance is that it is expensive and there-fore can sample only a tiny fraction of a network’sclinical isolates. It is best at answering selected ques-tions or providing general overviews of specificproblems. Its information on population denomi-nators for the isolates it tests is no greater and maybe less than that of the network clinical laborato-ries that contributed them. It also lacks the detailneeded for surveillance at the local level. Localinfection control needs to know the locations ofthe last hundred patients who had methicillin-resistant Staphylococcus aureus (MRSA), and not justof the two whose isolates were sent to the referencelaboratory.
It would be valuable, however, for local surveil-lance to know both the locations of their last hun-dred patients with MRSA, from their own localdatabase, and also how their local testing of thetwo MRSA isolates sent to the reference laboratorycompared to its testing of them. It would addition-ally be useful for them to know how their two iso-lates related to the MRSA sent in from other centres.Conversely, it would be useful for the reference labo-ratory to know whether the two isolates they testedfrom that centre represented only a few such iso-lates at that centre or an extensive outbreak.
For such reasons, the value of integrating thedata from routine clinical laboratories and the datafrom reference laboratories on the isolates they haveboth tested was recognized by several of the groupsreviewed, and characterized as “cross-validating” byone of them. It does not appear to have been muchexploited yet (14). Most existing reference labora-tory surveillance has been proprietary, its largebudgets supported mostly by pharmaceutical com-panies seeking information on particular issues.Cross-validation has thus not been a priority.
It would seem easy, however, to extend the analy-ses of databases of such proprietary systems to cross-validation and to other questions framed by publichealth concerns. There will undoubtedly be a needalso to develop antimicrobial resistance referencelaboratories in the public health sector, not only todo some specialized or “cross-validating” surveil-lance, but to also have multiple other roles in coor-dinating multi-centre surveillance networks, asdiscussed below.
Reference laboratory roles in coordinating multi-centre sur-veillance networks. Organizing networks of medicalcentres and merging their individual susceptibilitytest databases can generate a national resistancesurveillance database without great expense. Theorganized network can then serve as a base for col-laborative programmes that use continuing qualitycontrol and benchmarking analyses of the shareddata to improve its quality, use, and interpretationboth locally and nationally.
Several of the groups discussed the roles that acentral reference laboratory could play in organiz-ing and coordinating such a surveillance network.It could take the initiative in recruiting and settingup the network. It could train participants in useof the network software. It could develop or be thenetwork distribution point for proficiency testingand other quality assurance programmes for net-work laboratories. It could give network laborato-ries training courses shaped, in part, by problemsseen in the results of such quality testing resultsand in the analyses of the data flowing through thenetwork (6,14).
To the extent that a network reference labora-tory also conducted surveillance projects on thereference laboratory model sketched above, it wouldhave the opportunity to further improve routinenetwork data by the kind of cross-validation men-tioned above. Finally, the reference laboratorywould take the lead in the continuing analysis oftotal network data and in improving the local analy-ses ongoing at each centre in the network (14).
Active surveillance. “Active surveillance” is a termsometimes used in descriptions of epidemiologicalstudies. Within the context of studies of resistancethe term may be applied at a number of levels, forexample: the identification and recruitment of apatient or study population; the collection ofscreening or diagnostic specimens; the performanceof non-routine testing; and/or the in-depth analy-sis of data. Used in this sense, active surveillancecan often be accomplished within, and be a valu-able complement to, routine clinical practices. Forsome purposes, however, it may also requirespecial studies.
Special studies. Special studies to provide moresurveillance information than is in routine clinicalisolate data usually undertake to obtain additionaldesignated specimens for culture, or additional cat-egories of patient information, or to perform moreelaborate isolate testing or data analysis.

19
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Such studies might, for example, survey resist-ance of E. coli from stools of untreated healthypeople, of S. pneumonia in nasopharyngeal swabsfrom children in a day-care centre, or the urinaryisolates of all untreated women presenting withsymptoms of urinary tract infection.
Alternatively, they might seek to record all diag-noses, or extensive demographic data or all antimi-crobial therapy in a given population of patients.They might also perform extensive analyses of thegenotypes of isolates of one species or of the link-ages of different antimicrobial resistance phenotypesin different bacterial species in various collectionsof isolates.
Because such special studies have usually beenlabour intensive, requiring extra effort and fund-ing, they have tended to be fragmentary and diffi-cult to sustain. They do, however, have the potentialto enhance the information obtained from surveil-lance and improve its epidemiological foundation,especially if they can be linked to one another andto more routine surveillance to develop new kindsof cross-validation (14).
Advancing information technology has the po-tential to eliminate the extra effort required for someof these studies and so make them more widelyutilized. Data on patients’ demographics and useof antimicrobials are increasingly being filed in elec-tronic reporting systems, along with their microbi-ology test results. Downloading all three into acommon database would routinize and so makewidely available analyses previously kept rare by theneed for tedious chart review.
Participants interconnected in existing surveil-lance networks may also be better organized, if notalready self-selected, to collaborate in ongoingprojects requiring collection and culturing of ad-ditional specimens.
Information systems for surveillance
Many of the reviewed reports emphasized howessential for the surveillance of antimicrobial re-sistance are computerized information systems, butfew explored their specifications. The needs seemobvious and advancing information technologyshould be making it easier to meet them(3,5,6,7,13,14).
Software exists now, as mentioned above, to putany laboratory’s susceptibility test results and somebasic demographics of the cultured patients into adatabase dedicated to that application. If softwarewith the same or easily matched codes and file for-
mat is used by all the laboratories in a network,merging their databases, after ‘hashing’ for confi-dentiality, into a database network costs almostnothing.
Further development of such software couldincrease its usefulness for infection control datamanagement. Downloading discharge data on eachpatient’s diagnoses and pharmacy data on eachpatient’s antimicrobial usage into additional fieldsin the same database would make it possible toanalyze what kinds of isolates preceded or followedwhat kinds of antimicrobial therapy in patients withwhat kinds of diagnoses (7,14).
Downloading pharmacy data on antimicrobialusage by each patient at each medical centre in amulti-centre resistance network would also allowthe network to capture that data for the whole net-work, as it does the resistance data, by merging thedatabases of all the centres. This could be one com-ponent of a national system for surveillance of an-timicrobial usage. Such surveillance has beenstrongly recommended in several of the recent re-viewed reports, but none of them has offered muchdetail on how to do it (12,16).
Information technology now makes it easier toimplement such integrated information systems. Atype of software called a data conversion utility fa-cilitates matching of data fields and translation ofcodes between the various electronic systems thatreport and store relevant data sets in different medi-cal centres and a common database that can analyzeall of their interrelationships. An example wouldbe BACLINK, which facilitates translations of datafrom various microbiology reporting systems intocommon WHONET files.
Research on surveillance data
We can picture how resistance genes may emerge,insert into genetic vectors and spread under selec-tion in one or many strains and species throughthe world’s interconnecting bacterial populations.The picture we have, however, is projected largelyfrom expectations based on the well-studied mo-lecular details of those genes and vectors. Plasmidscan transfer, and resistance genes should move inand out of integrons, etc., but only rarely have webeen able to observe them actually doing thosethings in the real world. The microbes’ resistancesystem is operating all around us, but we cannotobserve its workings or the rates at which changesoccur. If we could, we might manage it better.
The kind of systematic surveillance of resistance

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
20
recommended by many of these reports, coupledwith advancing molecular technology, should makeit possible to do at least some surveillance at themolecular level. We should be able to trace line-ages of resistance genes, genetic vectors, and strainsof bacteria in different circumstances and underdiffering selection. The goal would be to improveour ability to predict what will happen and tointervene and avert problems (3,4,6).
Research and surveillance are each recommendedin nearly all of the reviewed reports, but only a fewmake a connection between them. We need researchon how best to do surveillance. We need furtherdevelopment of surveillance software and researchon how to use it fully. We also need to developsurveillance linked to molecular technology as aresearch tool to elucidate the real world popula-tion biology and detailed epidemiology of antimi-crobial resistance.
What have been the barriers to the implementationof surveillance?
The urgent recommendation for surveillance ofantimicrobial resistance and basic plans for how todo it were made nearly two decades ago (2,3). Itsurgency has been reemphasized and elaboratedupon by each of the expert groups that has metsince. Over that same period, a succession of unex-pected, new, and very damaging resistance prob-lems have emerged and spread throughout theworld. These global outbreaks, one after another,have had only the sketchiest of monitoring to sup-port the ultimately failed attempts at containment.As nearly all of the recent reports agree, only inad-equate and fragmentary surveillance systems existtoday.
The reports reviewed do not examine thereasons why prior reports’ recommendations forsurveillance of antimicrobial resistance had beenso little implemented, except for one that discussesbarriers and resources in one country (13). Thenature of antimicrobial resistance, the types of rec-ommendations made, and the experiences of thosesurveillance systems that have been started may,however, suggest some of the barriers.
Compared to other medical problems beingbrought to the attention of the public and publichealth officials, antimicrobial resistance is an ex-tremely diffuse subject and difficult to describe. Itis not in one organ or one type of patient but car-ried by all of us and in the environment. It is not adisorder in people as much as it is a disorder of the
world’s huge but invisible bacterial populations.Attempts to cure people drive a process that ulti-mately prevents cure of other people. The fact thatit is confusing may have been a barrier to focusingattention on recommendations to contain resist-ance.
The recommendations for surveillance made inthese reports require perhaps unprecedented coop-erative activity in any country between a smallnumber of public health officials and large num-bers of diverse groups of health care workers. Anti-microbial resistance is a public health problem.Most of the people who are causing it, trying tocope with it, and generating nearly all of the infor-mation on it, however, are providing services toindividual patients. They produce, own, and havethe most immediate and varied uses for the datathat will have to be recycled into public health sur-veillance if there is to be any.
The two parties need to help each other. Thepublic health official on whose desk the recommen-dations arrive may not have a detailed grasp of theworkings of the microbiologists, pharmacists, in-fection control workers, and clinicians in the medi-cal centres and the communities they serve.Conversely, it may not occur often to these busymulti-specialty local health care providers that theyare in part public health workers.
Most of the antimicrobial resistance surveillancenetworks that have gotten started in various coun-tries over the last decade or so were initiated by amicrobiologist or infectious disease specialist. Heor she began to file and analyse local susceptibilitytest results in a database in his or her own medicalcentre, then persuaded colleagues at other centresto do the same. Occasional funds and/or occasionalsurveillance projects from pharmaceutical compa-nies helped. The leadership and interest of theseindividuals and their colleagues have kept many ofthese networks functioning, and some have grownto include thirty or more centres.
Less often, a public health department has takenthe initiative to contact medical centres and begindevelopment of a surveillance network. What seemsto have worked best has been when a public healthdepartment has established a relationship with oneof the beginning privately-initiated networks. Intwo such examples some relationship had existedfrom the beginning, and the public health divisionhad later expanded its support when it came torealize the value of the growing network.
When a public health department has come tosupport a surveillance network, substantial im-

21
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
provements have followed. Presumably two thingshave happened. The first is that the network hadbeen built with participants who were motivated,in that they had been self-selected by their interestand belief that a network could help their worklocally.
The second is that the public health departmentcould begin to support a reference laboratory, hith-erto lacking in those networks. In each of these twocases the network initiator’s laboratory became thereference laboratory. With this support, it couldbegin to perform the reference laboratory functionsdescribed above, and the networks improved ap-preciably.
Each of the two parties has its own barrier. Thepublic health department needs to be given fund-ing and accountability to build a surveillance net-work. The public health department, however,cannot begin to pay all the participants that a net-work needs. Therefore, it has to exercise real lead-ership in finding leaders within the network, and,with their help, motivate all the participants to worktogether on the network.
Similarly, none of the participants in the net-work would be able to fully support a reference labo-ratory. Yet, the improvements in the network fromsuch a laboratory can enhance the work of the par-ticipants. Cooperative mutual barrier removalbetween public health and local health care may bethe most important process in implementingsurveillance of antimicrobial resistance.
Governments and their public health agenciesneed to take the lead in removing these barriersand in encouraging clinical laboratories to partici-pate fully in surveillance networks. They have rarelydone this because they have been slow to see theepidemic nature and the menace to health of anti-microbial resistance and thus slow to see it as apublic health responsibility, deserving priority andadequate support.
Authors’ notes on reports
(27) WHO International Collaborative Study ofAntibiotic Sensitivity Testing (1968–1970)
This study, carried out in 16 laboratories in differ-ent parts of the world, was set up in response to arecommendation of the WHO Expert Committeeon Antibiotics.(1961) It was sponsored by WHO,initiated at a meeting in Geneva and coordinatedby the Karolinska Institute in Stockholm, withfinancial support for meetings and administrativework provided by WHO.
The study compared, in multiple countries ingreat quantitative detail, both broth dilution andagar diffusion methods for antimicrobial suscepti-bility testing. It essentially began the developmentof the framework for standardizing and interpret-ing test results and comparing results from differ-ent countries, which are essential prerequisites forsurveillance of resistance, especially for internationalsurveillance of resistance.
Its 90 page report, published as a supplement toACTA Pathologica et Microbiologica Scandinavia(Section B 1971, Supplement No. 217) did not usethe word “surveillance” which may not then havebeen applied to antimicrobial resistance, but forwhich the study began to build a foundation. It did,however, begin by listing as one of three purposes forstandardizing the measurement of the sensitivityof microorganisms to antibiotics (along withrational use and evaluation of new agents) as “forepidemiological studies.”
(28) WHO Scientific Working Group on AntimicrobialResistance, Geneva, 23–27 November 1981.WHO/BVI/PHA/ANT/ 82.1
The Working Group outlined the current situationof antimicrobial resistance. It emphasized that theincreasing frequency of acquired resistance to anti-biotics among bacteria of medical importance is aworldwide health problem that demands interna-tional attention. Its report concluded that withoutreliable information about the susceptibility toantibiotics of important bacteria, it would be im-possible to find solutions to the problems createdby antibiotic resistance.
The Working Group therefore recommendedpromotion of surveillance activities at both nationaland international levels and suggested that WHOcould play an important role in promoting theseactivities. It stressed the necessity of extending theWHO activities in establishing a system for sur-veillance of antibiotic resistance, and concluded thatthere was a need for unification of methodologyused for the surveillance.
(29) WHO Consultation Group for Surveillance ofAntimicrobial Resistance, Geneva, 22–26November 1982. WHO/BVI/PHA/ ANT/ 82.5
This meeting was convened to respond to the rec-ommendations on surveillance of the previous year’sScientific Working Group (above). Its purpose wasto discuss the approaches to and objectives of na-tional and international surveillance of antibiotic

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
22
resistance, and to make recommendations as to howsuch a surveillance programme might be designedand implemented on a global scale.
The plan proposed was to:
1. Develop systems to produce reliable data onresistance in all parts of the world.
2. Develop systems to ensure that the data areof good quality and comparability.
3. Analyse the resulting data in many differentuseful ways on a continuing basis.
4. Use the analyses to monitor, understand andcontrol the spread of resistance.
The Consultation Group identified three gen-eral sources of data for surveillance. One was thesusceptibility test result data generated in enormousvolume by the world’s clinical microbiology labo-ratories. A second was the more specialized datagenerated by reference laboratories. A third wouldcome from special studies with epidemiologicallyplanned sampling not just of selected patientpopulations but also of healthy people in differentsettings and of the environment. The group em-phasized that planning in advance to integrateanalyses of data from these three general sourceswould allow cross-referencing enhancement of thevalue of each.
The report made general recommendations formethods of susceptibility testing, and also for qual-ity control of that testing and for what anti-microbials to test, drawing upon an earlier WHOreport on “Guidelines for Antimicrobial Testing
(WHO, Ref, LAB/79.3 in Annex)”. It pointed outthe need to record the actual measurements of sus-ceptibility, such as diameters of zones of inhibitionaround susceptibility test discs or minimal inhibi-tory concentrations, rather than the interpretivecategories derived from them.
The Consultation Group also examined in somedetail the management of the data from suchsurveillance. It recognized that nearly a dozen cat-egories of data, such as type of sample, date ofsample, and the identified species and susceptibil-ity measurements of each isolate were recorded inmost laboratories.
Planning in advance a common software formatfor filing the data in these categories and commoncodes for the terms and measurements of that datawould thus greatly simplify the merging, manag-ing and analysis of data from many laboratories andsources.
The report noted also that once such data areelectronically filed, it is easy and cheap to ana-lyse and reanalyse it in many ways to fully extractfrom it practical understanding of the emergenceand spread of resistance. For illustration, it sketchedout nine different types of such analyses. It wenton to explain how results from these analyses couldbe extrapolated to insights about prevalence orresistance in different places and different sub-populations, about prevalence of resistance genesand about the evolution and epidemiology ofresistance plasmids. It summarized this with atable (below) offering three examples of the kindsof observations that might be made from such
Level Observation Use
Local Frequency of resistance to each antibiotic Aid selection of antibiotics for individual patients
Frequency of resistance to each combination Identify cross-infecting strains, locally endemic resistance plasmidsof antibiotics
Local trends in resistance Aid re-evaluation of local antibiotic usage and infection controlpractices
National More resistance to one antibiotic than usual Decrease use of the antibiotic, introduce alternative agentsin other countries
Variation in antibiotic resistance in different Seek regional differences in usage, vehicles of resistance spread,regions of the country e.g., food or water, hygienic practices
General level and trend of national resistance Review, revise national antibiotic usage strategy to increase itsoverall in comparison with other countries effectiveness, reduce resistance
Global Global trends in resistance to various antibiotics, Guide development, use of new antibiotics, ways of preservingprevalence of different genera older ones. Compare countries’ practices
Early detection of new resistance to an antibiotic Global warning to detect, contain, treat the emerging strain,in a particular strain in a particular area examine circumstances preceding emergence
Global trends in prevalence of distinctive Detection, prevention of international spread of particular resistancecombinations of resistance or resistance genes plasmids of resistant strains

23
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
surveillance at each of three levels, local, national,and global, and then of the kind of correspondingpractical responses that might be made by caregiversand policy-makers at each level.
Even though this Consultation Group was meet-ing within about a year after the introduction ofthe IBM personal computer (PC), at a time whenapplications of the PC were only beginning, thegroup noted its potential significance. “Now, how-ever, rapid improvement and reduced costs of smallcomputer technology may soon make it possibleto enter the data directly on cassette tape or disc atthe testing laboratory.” They further observed thatthis would make possible local analysis of the datafor local management of resistance at each medicalcentre in addition to the more centralized multi-centre analysis, which was all that had been practi-cal previously with the big, expensive mainframecomputers.
(1) Antibiotic Use and Antibiotic ResistanceWorldwide, A study sponsored by the FogartyInternational Center of the National Institutes ofHealth, 1983–1986
Nearly all reference to surveillance of antimicro-bial resistance in this study performed by five taskforces comprised of international experts was in thereport of Task Force 2, entitled “Resistance of Bac-teria to Antibacterial Agents.” The 13 members ofthat Task Force came from 5 continents, with only2 of its members from the same country. Many ofthe members brought available data on resistancefrom their own medical centres, from colleagues intheir countries, or from published literature. Datawere also presented from a computerized and iso-late-based international surveillance system sup-ported by the US Food and Drug Administration(FDA), which was then ongoing but discontinuedlater when FDA found an international study in-appropriate.
The work of Task Force 2 was to piece togetherfrom this available information an overview of thecurrent distribution and apparent trends of anti-microbial resistance throughout the world. Theirparticular emphasis was to try to integrate what datathey had with growing understanding of the mo-lecular basis of resistance and of its spread, so as tobe able to interpret one in terms of the other. Theirreport attempts to do this by examining resistanceto agents grouped according to their being inacti-vated by the same families of resistance mechanisms.
The first recommendation of Task Force 2 was:“The available data on global prevalence of resist-
ance to antibacterial agents were barely adequateto sketch ranges and suggest trends. More system-atic surveillance on a much larger scale is neededto provide explanations or remedies. The WorldHealth Organization has developed detailed rec-ommendations for such surveillance and is nowbeginning integrated surveillance programmes inseveral regions of the world…This initiative shouldbe exported and expanded.”
Their second recommendation began by notingthe growing understanding of the genetic elementsof resistance. It then stated: “What are particularlyneeded now are broadly based studies of the de-ployment of these genetic elements in naturalpopulations of bacteria that will provide an expla-nation of the phenomena observed in surveillanceand suggest practical strategies for containment andreduction of resistance.”
(3) Emerging Infections. Microbial Threats to Healthin the United States. Report of the Institute ofMedicine. National Academy Press (1992)
This report called attention to a whole group ofrecently observed or recently worsening infectiousdisease problems by creating a new category forthem, Emerging Infections, and setting forth theirspecial features and similarities and the growingseriousness of their threat to human health. It am-plified the perceived importance of antimicrobialresistance by including it in this category of Emerg-ing Infections.
The report repeatedly emphasizes the impor-tance of surveillance for the control of all emergingdiseases. They constitute such a large and diverseset of problems, however, that the report did notattempt to delineate the special needs for the sur-veillance of each, let alone for antimicrobial resist-ance, which probably differs most from the othersin surveillance methodology. Surveillance of resist-ance is, however, mentioned in several places.
1. Additional resources are recommended for theCenters for Disease Control and Prevention(CDC) to enhance its National Nosocomial In-fections Surveillance System (NNISS) in fiveways. The first is to “include data on antiviraldrug resistance.” The fifth is “to determine thereliability of antimicrobial susceptibility testingperformed in NNISS member hospitals.” Nodescription is given of the current status ofNNISS data on antimicrobial resistance.
2. Under “Agricultural Conditions and Practices”is the somewhat tentative sentence: “It is con-

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
24
ceivable that surveillance of feedlot animals forthe development of resistant organisms mightbe a means of early warning for the emergenceof newly drug-resistant pathogens.”
3. In a section on Access to Surveillance Informa-tion, emphasizing that access to surveillancedatabases is needed by many types of health careworkers and researchers, it is noted that thereare now no such databases for many problems,including antimicrobial resistance.
4. In a later section is a recommendation that theUS Public Health Service develop a comprehen-sive, computerized infectious disease databasethat includes all of these components andensure appropriate access to it.
5. It later recommends that the US “take the leadin promoting the development and implemen-tation of a comprehensive global infectiousdiseases surveillance system.” Another sentencelater in the report says that: “Should a globalinfectious diseases surveillance system be put inplace, such as the one suggested in this report,tracking antimicrobial resistance worldwide maybe possible.”
(5) WHO Scientific Working Group on Monitoringand Management of Bacterial Resistance toAntimicrobial Agents. Geneva (1994).WHO/CDS/BVI/ 95.7
This Working Group added several new insights.Meeting at this time, they were able to look backand recognize that resistance had worsened greatlyover the previous decade due to an array of surpris-ing new problems, which they reviewed in detail.They warned also that this was happening at a timewhen pharmaceutical companies, represented at themeeting, appeared to have under development fewnew antimicrobials to address these new problems.
For surveillance of resistance, a particular insightand emphasis of this group was the primary im-portance of local surveillance linked to local man-agement of resistance for each medical centre andits community. The group introduced the idea of alocal antimicrobial resistance management (ARM)team comprised, to the extent available, of infec-tion control workers, microbiologists, pharmacistsand infectious disease clinicians. They would worktogether, applying their diverse skills to the ongo-ing analyses of local resistance data, to treat patientsand retard spread of resistance optimally within thespecial circumstances of their time and place.
The report noted that such local monitoring andmanagement was now possible because local resist-ance databases could be maintained on localpersonal computers. Previously, local results had tobe sent to a single remote centre for multi-centreanalysis on a mainframe computer, with standard-ized printed overview results returned to the centrelater. In contrast, local databases can be queriedlocally, frequently and very specifically on an adhoc basis as specific local problems arise. The tech-nology was seen capable of inverting the older “top-down” surveillance into a “bottom-up” model. Inthis newer “grass roots” model, actively used localdatabases could, if they shared common file for-mats and codes, be easily merged without loss ofdetail to produce higher level regional, national orinternational databases, as an inexpensive byproduct.
Software dedicated to supporting such local butcombinable antimicrobial resistance databases wasdemonstrated for the Group. This shareware, calledWHONET, had been developed to meet the needsset forth by the WHO Consultation Group forSurveillance of Resistance of 1982 (see above).
Another emphasis of this Scientific WorkingGroup relating to surveillance was the need to buildprofessional infrastructure to support the monitor-ing and management of resistance. Well-trainedmicrobiologists in adequately supported microbi-ology laboratories were essential because they werethe ultimate source of all of the surveillance dataand its quality, and of the information for treatingindividual patients. The microbiologists, in addi-tion to infection control workers, infectious dis-ease clinicians and pharmacists, would constitutethe ARM teams.
The report made separate recommendations foreach of three levels of organization. Those relatedto surveillance of resistance are quoted verbatimbelow.
Recommendations for WHO
Improve systems for surveillance of antimicrobialresistance.
• Assist nations in assessing status and specificneeds of their laboratories for performing ad-equate identification and susceptibility testingof bacterial pathogens.
• Distribute and facilitate the installation ofWHONET software in laboratories to enablethem to monitor their own results for test qual-ity, for infection control problems, and for local
25
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
trends in resistance, and to enable them to mergetheir results into same-format isolate-baseddatabases for detailed national and internationalsurveillance of resistance.
• Assist laboratories, through WHO RegionalOffices, in the development of quality controland quality assurance programmes to help im-prove the accuracy of antimicrobial susceptibil-ity testing methods.
• Provide support and facilitate coordinationbetween reference laboratories for better straintyping and other specialized procedures inorder to better characterize the epidemiology ofresistance.
• Encourage the prompt reporting of culture andresistance data and analyses to clinicians, infec-tion control personnel, and public healthauthorities, and prompt transmission of selectedisolates to reference laboratories when appropri-ate.
• Call attention to patterns of resistance inspecies of bacteria that may represent emergingepidemics, such as vancomycin-resistantenterococci, penicillin-resistant pneumococci,fluoroquinolone-resistant Shigella, multi-resist-ant Salmonella typhi, and others less obvious.
• Develop an action plan for appropriate responseto outbreaks of resistant organisms.
• Identify funding sources to help implement theabove recommendations.
Recommendations for individual countries
Same as for WHO plus:
• Encourage medical centre laboratories to developisolate-based computer databases of their sus-ceptibility test measurements in a common fileformat, such as WHONET, which can easily bemonitored at each centre and aggregated into anational surveillance database.
• Designate one or more laboratories to help otherlaboratories install and use the common soft-ware, to provide them with test strains and othersupport for improving their testing, and to man-age and share with them their shared surveil-lance database.
• Assess the quality, geographic distribution andprofessional microbiological support of existingmicrobiology laboratories, improve them where
needed, and open new laboratories inunderserved areas.
• Integrate the work and data of reference labora-tories with that of other laboratories monitor-ing the spread of resistance.
Recommendations for local hospitals and referencelaboratories
• Develop a plan to monitor and control resist-ance.
• Implement a user-friendly, multi-analysis isolate-based computer system, such as WHONET,which allows detailed monitoring of local resist-ance and flags isolates or clusters of isolates thatmay represent emerging outbreaks of resistantstrains.
• Appoint an antimicrobial resistance manager(ARM) responsible for monitoring and inter-preting local resistance and local antimicrobialuse and for alerting and working with infectioncontrol, pharmacy, administrators and cliniciansto refine and optimize antimicrobial therapy andto focus containment efforts.
(8) Report of The ASM Task Force on AntibioticResistance (1995)
This report emphasized the need for surveillanceof resistance in the US. It pointed out that: “Thereis currently no national or global surveillance sys-tem for monitoring antibiotic resistance in animalsor humans. In fact, the amount being expended istotally inadequate.” It reviewed available figuresfrom 1992 and could find, outside of private-sec-tor investment in proprietary systems, only $55,455from all sources dedicated to antibacterial and an-tiviral drug resistance, out of a total of $76.4 mil-lion of federal, state and local funds for surveillanceactivities of all kinds.
The first recommendation of the report is for aNational Antimicrobial Surveillance System. It be-gins with a list of things the surveillance systemshould do. The first block of suggestions includesfocus on prevalent pathogens from clinical diseasecases and routine isolates, attention to upward“creep” of minimal inhibitory concentration (MIC)levels, monitoring of animal products at the super-market level, inclusion of Salmonella as reflectingantimicrobial usage in the animal world and Shig-ella usage in the developing world, and monitor-ing of soil waste on farms.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
26
The list further includes use of concurrentpatient demographic profiles, the ability to flagorganisms with certain phenotypic or genotypicresistance patterns for further study at referencelaboratories and for molecular typing, and the useof surveillance to target areas for intervention orepidemiological investigation, mostly at the localbut also at national or international levels. It alsosuggests devising different benefits for different setsof participants, making data available to pharma-ceutical companies and having a system that couldbe modified to address new areas of concern.
Under “monitoring of organisms”, the reportdiscusses how to update the list of pathogens tomonitor, frequency of analyses, the need forsignificant numbers of isolates, and the need toinclude species that may not be pathogens but maybe a source of transfer of resistance genomes toprevalent human pathogens.
Sections on geographic representation discusschoosing participant laboratories by US populationdistribution, suggesting one site per one to twomillion people with stratification by medical cen-tre size, type, and services, and with supporting helpfrom local and state laboratories, possibly in coor-dinating data from laboratories supporting com-munity practices.
A section on methods recommends followingEurope’s National Committee for Clinical andLaboratory Standards (NCCLS) documents, usingwhere possible the disc-diffusion method with al-ternative special tests including molecular testing,some at reference laboratories, guided by expertadvisory panels and with rigid quality control. Italso states that: “all data should be expressed asquantitative endpoints regardless of method. Thisdictates measurement of disc diffusion tests bycalipers to the nearest whole millimeter and the useof MIC endpoints in micrograms per millimeterfor dilution methods.” “Qualitative interpretationsshall be applied objectively by computer programsbased on current NCCLS tables. Similarly, qualitycontrol guidelines found in the NCCLS tablesshould also establish the validity of each partici-pant’s/ referee’s data.”
A section on data entry and analyses emphasizesthat all surveillance systems need well-structuredcomputer systems. It cites the CDC’s NNISS andthe WHO’s WHONET as examples of such soft-ware used for resistance surveillance, available andmodifiable. It also suggests that networks using suchsystems or others such as CDC’s sexually transmit-ted disease programme, Veteran Administration
(VA) networks, or SCOPE (Surveillance and Con-trol of Pathogens of Epidemiologic Importance,Medical College of Virginia and University of Iowa)might serve as working models and that these in-ternational programmes might provide possiblecollaborations. Another section sketches guidelinesfor analysis of and access to the data, which wouldbe audited by the oversight panel or study admin-istrators.
A section on organization of the surveillancesystem recommends that funding should be soughtfrom all parties that would benefit from the sys-tem, including CDC, FDA, NIH, USDA, VA,DoD, pharmaceutical and health supply industries,drug and health care delivery companies, academicinstitutions, professional societies, and universitymedical centres. An oversight panel should includerepresentatives of the organizations plus membersof the scientific community who are experts onantimicrobial resistance, specialists in infectiousdiseases and in vitro susceptibility testing or expe-rienced in multi-laboratory surveillance, hospital/health care epidemiologists, and computer andstatistical analysts conversant with antimicrobialissues. Location of the programme within CDCwould allow integration with other surveillanceactivities.
A final section on immediate recommendationscalls for an expert panel to develop a surveillanceprotocol and establish an annual budget, for whichthe ASM outline might serve as a preliminary ortentative plan. Federal funding should be immedi-ately identified, with federal agencies and othersources involved in funding decisions. It calls alsofor appropriate expertise in statistical and compu-ter support and for an immediate search for earlierresistance surveillance databases from the US orworldwide surveillance, if available.
(7) Report of the US National Science andTechnology Council Committee on InternationalScience, Engineering, and Technology WorkingGroup on Emerging and Reemerging InfectiousDiseases. Washington (1995)
This US government interagency Working Group,chaired by the Undersecretary for Global Affairs ofthe Department of State and established under theaegis of the Committee on International ScienceEngineering and Technology (CISET) of PresidentClinton’s National Science and Technology Coun-cil, had members representing more than 17 dif-ferent Government agencies and departments. Its
27
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
charge was to review and make recommendationson the US role in detection, reporting and responseto outbreaks of new and re-emerging infectiousdiseases.
The Working Group considered the entire rangeof emerging infections and emphasized the impor-tant role of surveillance for the whole group. The 2of its 19 recommendations that mention surveil-lance for antimicrobial resistance specifically arereproduced below.
• Assisting WHO to establish surveillance of antibioticresistance and drug use, as a first step towards thedevelopment of international agreements on antibi-otic usage.
WHONET, an international reporting systemfor antibiotic resistance, provides WHO with astarting point for this significant work. Takingadvantage of its overseas networks US Agencyfor International Development (UASID) canprovide support for surveillance of drug resist-ance that hinders the treatment of internation-ally important diseases. In addition CDC cancontribute technical support and data manage-ment resources (5).
• Identifying and strengthening WHO CollaboratingCentres that serve as unique reference centres fordiseases whose re-emergence is feared.
WHO Collaborating Centres operated in theUnited States by Government agencies or byAmerican universities require support to buildor rebuild their capacity to serve as referencelaboratories within a larger, more active infec-tious diseases network (8).
(6) Report of the Office of Technology Assessment ofthe Congress of The United States on Impacts ofAntibiotic Resistant Bacteria (1995)
The report does not use the word “recommend”,that presumably being the prerogative of the Con-gress, but instead presents “issues and options”,usually expressed as “the Congress could.” Underthe first of these in its summary (A. Surveillance) itsays that “Congress could support the establishmentof a national surveillance system, including pro-viding funding.”
It goes on to explain: “A surveillance system isessential for understanding the spread of antibiotic-resistant bacteria and planning interventions so asto preserve the efficacy of currently available anti-biotics. Because of these public health considera-tions, and the likelihood that a surveillance system
would decrease medical costs, including costs tomedicare, Congress could consider funding anationwide surveillance system.”
“The features of the current, limited systems canbe incorporated and combined to produce a sys-tem of desired size, complexity and cost. It may beadvantageous to begin with a less complex system(such as some of the operating systems describedin this report), and then add more features. Anysystem must have a strong advisory group that in-cludes diagnostic laboratory and computer experts,clinicians, hospital administrators, pharmaceuticalcompany researchers, academic scientists, and fed-eral and state regulatory and health officials. Theadvisors could work to assure that the surveillancesystem collects and disseminates the informationin the forms for its best use.”
(13) Society for Healthcare Epidemiology of Americaand Infectious Disease Society of America JointCommittee on the Prevention of AntimicrobialResistance: Guidelines for the Prevention ofAntimicrobial Resistance in Hospitals. (SHEAPosition Paper) (1997)
The first two of the report’s seven recommenda-tions for hospitals large and small are: “Establish asystem for monitoring bacterial resistance and anti-biotic usage” and “Establish practice guidelines andother institutional policies to control the use ofantibiotics, and respond to data from the monitor-ing system.”
(15) WHO Workshop on the Current Status ofAntimicrobial Resistance Surveillance in Europe.Verona (1997). WHO/EMC/BAC/98.1
Participants in resistance surveillance networks inEurope filled out questionnaires in advance, andtheir responses constitute the descriptions printedin this report. Twenty-nine surveillance activitiesor networks are described, approximately half ofwhich targeted a single bacterial species. In theworkshop the participants reviewed, elaboratedupon and discussed these systems.
They found need to improve communicationof results to decision-makers; to improve and har-monize quality assurance standards throughoutEurope; to have adequate support for microbiol-ogy and epidemiology training, laboratory infra-structure, data analysis and communication; andto provide adequate funding for regional partner-ships. Lack of funding was the principal obstaclefor existing systems. They concluded that further

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
28
discussions were necessary to develop collaborationbetween existing programmes.
(22) Antimicrobial Resistance: Issues and Options.Institute of Medicine Workshop Report (1998)
The report’s section on surveillance begins by stat-ing that its purpose is to provide information foraction and that the information is “for several pur-poses at every level where health care is provided.Each level has different needs and all are critical.”Examples are given of the many kinds of questionsthat need to be asked and a review of the problemsthat have historically restricted efforts to monitorantimicrobial resistance.
The report makes the statement in its summarythat: “No country, including the United States, hasa reliable, longitudinal, full-service antimicrobialresistance surveillance programme with comprehen-sive focus, nor is there a comprehensive databasefor monitoring trends in antimicrobial usage.”
A section on characteristics of an ideal resist-ance surveillance system indicates that it should beprospective, active, timely and affordable, with thebroadest possible access. It should also provideaccurate incidence and prevalence rates, exclude re-peat isolates, distinguish infecting and colonizingorganisms, and categorize data by location as wellas by hospital or community, urban or rural. Inaddition, it should gather information on antimi-crobial use and treatment outcomes (especially fail-ure); detect new resistance markers; and use reliable,standardized test methods on appropriate specimenswith validation. It should be a national networkrepresenting inpatients and outpatients in allregions with all participating laboratories compu-terized to collect, process, and report electronic datacontinuously, with all such databases integratednationally, and regional and local data made avail-able to practitioners. A separate section reempha-sizes the need for local-level surveillance.
A section follows which describes several exist-ing national surveillance systems, including: CDC’s,The Surveillance Network (TSN), Canada’s, Ice-land’s, and as international systems CEM/NET,WHO initiatives, and SENTRY. This partially over-laps with a lengthier inventory added as AppendixA.
Another section points out that surveillance dataare laboratory-dependent. It proceeds to give anoverview, based on extensive experience with qual-ity control surveying largely in the US, of the kindsof problems encountered in laboratory susceptibil-
ity testing. It emphasizes that there are few labo-ratories, even when central laboratories are in-cluded, where testing cannot stand improvement,and an alarming number where improvement isessential. The need to improve is not just for sur-veillance, but for the patients whose therapy is be-ing guided by these tests.
In addressing what is needed the report sum-marizes why no single global or national antimi-crobial resistance surveillance system has thequalities outlined here. Few of the multiple exist-ing surveillance activities have been longitudinaland as a group they are almost totally uncoordi-nated and unstandardized, so the magnitude andimpact of resistance remain poorly understood and,“…the most powerful case possible must be madefor urgent and substantial response.”
The report refers to the ASM Task Force of 1995(see above), the recommendations of which it in-cludes as Appendix B. It comments that eventhough those recommendations are straightforward,their elaboration and implementation will requiremuch coordination and compromise. “No singlesystem is likely to be able to perform the full rangeof necessary surveillance, so that harmonization ofmultiple systems and guidelines for the productionof comparable data will be ongoing challenges.”“Real partnerships will be essential as people andinstitutions with varying priorities try to achievegoals that may be similar in many ways but diver-gent in others.”
(21) The British House of Lords Select Committee onScience and Technology Report on Resistance toAntibiotics and Other Antimicrobial Agents.London (1998)
Chapter 5 of the report is on surveillance. Its first9 paragraphs are on general reporting requirementsfor infections and on liaison between agencies. Para-graphs 10–13 emphasize importance of informa-tion technology, citing NNISS and Intensive CareAntimicrobial Epidemiology (ICARE). Paragraphs14–17 discuss recent problems with professionalinfrastructure and its funding in the UK, includ-ing declining financial support for the Public HealthLaboratory Service (PHLS).
The last 5 paragraphs cover a national strategyfor surveillance. Many groups agree that there isno adequate systematic surveillance of resistance inthe UK now. Costs for such a system would bemodest but no source has provided funding. Thereneeds to be a consensus with PHLS, NHS,

29
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
academia and clinicians. The British Society forAntimicrobial Chemotherapy (BSAC) has set up aWorking Party on Resistance Surveillance, whichhas proposed a multi-level approach and is seekingcollaborative arrangements. The Minister for Pub-lic Health said, “We support a strategic approachto this,” but was unable to make any commitmentas to resources.
In concluding their report, the Committee de-clares surveillance of resistance to be vital to thefight against resistance. It makes multiple recom-mendations for surveillance, most of which are ad-dressed to specific agencies or organizations in theUK about resource allocation rather than to ele-ments of system design. It does, however, stress theimportance of information technology in speedingup exchange of compatible data locally, nationally,and internationally. It also expresses approval of theUK’s NNISS system, hopes that it can acquire dataon use of antimicrobials, and suggests it considerthe ICARE model.
(19) Report of the British Department of HealthStanding Medical Advisory Committee Subgroupon Antimicrobial Resistance: The Path of LeastResistance (1998)
This incisive and comprehensive report visualizesa multi-level surveillance system that integratesmultiple methods of surveillance, “each cross-vali-dating the other.” It summarizes and critiques whatexists at each level in the UK now and makes real-istic suggestions about their improvement. It is ex-tracted, at times nearly verbatim, below.
“Alert organism surveillance,” the detection oforganisms with significant new features, has a roleas an early warning system. It is in place now onlyto the extent that such isolates find their way toreference laboratories.
Reference laboratory elaboration of species orof resistance mechanisms is often elegant now, butinterpretations of epidemiological significance arebeset by sampling problems and lack of a denomi-nator.
Sentinel laboratory monitoring, meaning theprospective collection of selected organisms for test-ing with standard methodology by a central labo-ratory, offers a high level of control but also lacks adenominator population and can test only smallnumbers of isolates.
Special surveys are a good tool, particularly ifthey have prospective selection with a clinical casedefinition in a defined population, but cannot be
performed for every organism and the costs areconsiderable.
Compilation of routine susceptibility testingdata can be a measure of public health impact be-cause these data do have a population denomina-tor, but there remains the problem of non-standardtesting methodology. Such routine data representa huge untapped source of inexpensive, accessibleresults, which could be analyzed at local, national,and regional levels to give a measure of the publichealth impact of antimicrobial resistance. The sys-tem envisaged is one fed by regular downloads fromlaboratory computers of routine susceptibility dataon a wide range of organisms and specimen types.The aim would be to encompass the whole; anessential facet would be linking the data to popula-tion denominators. Although this is a new area ofwork, the burden on individual laboratories wouldbe relatively low. Electronic downloading of datadirectly from microbiology computer systems is theideal, and has been done in other places.
(30) Report from the American Academy ofMicrobiology: Antimicrobial Resistance, AnEcological Perspective (1999)
This report seeks to take a broad, ecological viewof antimicrobial resistance and its distribution inthe environment. This emphasis is given to muchof the discussion and to most of the recommenda-tions for future scientific research. The ecologicalapproach is reflected in the section on surveillanceby the statements that “with respect to antimicro-bial impact on the environment, surveillanceinvolves not only data on bacterial pathogens butalso data on other microorganisms that are part ofthe affected ecosystem.” The report also states “Dif-ferent types of surveillance are needed for each com-ponent of the biosphere.”
In discussing different existing types of surveil-lance it mentions sentinel surveillance for detectingrare or important events. An ecological dimensionmight be added to this if instead of noting onlystrains categorized resistant by existing clinicalbreakpoints resistance could also be defined bylower “thresholds” of change in susceptibility thatwould “provide a selective advantage to a microor-ganism or risk for evolution toward greater resist-ance.”
The report continues its discussion of resistancesurveillance methods by recognizing that specialstudies conducted with prospectively definedpopulations, e.g., surveying pharyngeal carriage of

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
30
pneumococci in a defined group of children, isdesirable but expensive because the survey has topay for the culturing.
The same is true for surveillance of clinical iso-lates by sending them to a remote reference labora-tory for uniform testing.
It acknowledges that the bulk of surveillance datawill thus come from clinical isolate susceptibilitytest results downloaded from routine clinical labo-ratory files. This approach has the potential disad-vantage of variable test quality, but it costs little, isrich in local epidemiological detail, and so supportslocal management of resistance while being a com-ponent of regional or national surveillance. Analy-sis of the resulting stream of test results, moreover,“can serve to continuously improve the quality ofthe laboratory sampling and testing.”
Implicit, but not stated in this discussion, aretwo ways to enhance the value of such clinicalisolate data for generating ecological or environ-mental insights. One would be to not screen outnon-pathogens from surveillance databases, as issometimes suggested, but only exclude them fromparticular analyses. The other, as supported abovefor many other reasons, would be to file only fullrange measurements of isolate susceptibility (inhi-bition zone diameters or full-range MICs) ratherthan just the interpretive categories derived fromthose measurements. This would allow continuousmonitoring of the small increments in resistance(e.g., creeping resistance by accumulating mutationsto fluoroquinolones) that may “provide a selectiveadvantage….or risk evolution toward greater resist-ance.”
(31) US Interagency Task Force for a Public HealthAction Plan to Combat Antimicrobial Resistance(2000)
Based on a public meeting held in Atlanta, Geor-gia, in July 1999, with representatives of CDC,FDA, NIH, AHRQ, USDA, DoD, DVA, EPA,HCFA, and HRSA and many other groups, the planlists issues, goals and actions that apply mostly tohuman (as opposed to non-human, such as agri-cultural) antimicrobial resistance (AR) issues. Foreach action item “coordinator” and “collaborator”agencies/departments are specified. Its ExecutiveSummary lists under 4 major headings 11 toppriority action items to combat antimicrobial re-sistance. The first of the 4 headings is “Surveillance”,with 2 priority items under it:
“With partners design and implement a nationalAR surveillance plan that defines, national, regional,state and local surveillance activities; the roles ofclinical, reference, public health, and veterinarylaboratories; and is consistent with local or nationalsurveillance methodology and infrastructure thatcurrently exist or are being developed”.
“Develop and implement procedures for moni-toring patterns of antimicrobial drug use in humanmedicine, in agriculture, and in consumer prod-ucts.”
The section on surveillance in the report states:“At present the United States lacks a coordinatednational plan for AR surveillance” and “ImprovedAR surveillance depends upon enhanced epidemio-logic and laboratory capabilities at local, state andnational levels, use of standardized and reliable labo-ratory testing methods, and enhanced use ofinformatics.”
The remainder of the section is an extensiveoutline of the general needs for developing andimplementing such a comprehensive system. Thefirst block deals largely with allocation of generalcategories of tasks to specific coordinators and col-laborators.
The second block is on the development ofstandards and methodologies. It includes “stand-ardized laboratory methodologies and data elementsthat allow susceptibility test results and AR sur-veillance data to be compared across geographicjurisdictions. Similarly, use standardized definitionsand methodology to create an electronic surveil-lance system that health care institutions can useto compare AR data from other local facilities.”
It also calls for development of “standards forreporting quantitative data (e.g., MICs or zone di-ameters) in ways that will detect decreased suscep-tibility.” This is necessary because numerical ARtest results reported non-quantitatively (e.g., as sus-ceptible, intermediate or resistant) as “susceptible”may mask an emerging AR problem (i.e., microbeswith a small decrease in susceptibility may still beclassified as susceptible).
A block is devoted to the need, little mentionedin previous reports, to allow the data within such asurveillance system to comply with patient confi-dentiality policy. Subsequent sections recommendwork to ensure that this is possible and to developnew policy if needed.
Other recommendations follow, such as: “Linkhuman drug-use data to clinical information (e.g.,diagnosis, severity of illness and outcome). “Workwith accrediting agencies to address antimicrobial

31
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
drug-use monitoring as part of quality control as-surance in health care delivery systems.” “Evaluatethe performance of licensed, automated AR test-ing devices in the context of changing resistancepatterns and update their labeling where appropri-ate (e.g., changes in quantitative resistance that maymake a test result invalid).”
Under a section on state health and agriculturalagencies is the recommendation that they “main-tain the capacity to test the drug-susceptibility pat-terns of resistant organisms of public healthimportance, especially for drug-microorganismcombinations for which testing methods are notroutinely available at hospital and commercial labo-ratories.”
A section on dissemination of surveillance datarecommends: “Provide an accessible, centralizedsource of AR data from major surveillance systems
involving animal and human populations. In con-sultation with stakeholders determine how to re-port AR data in a way that is useful to interestedparties (e.g., clinicians, public health officials,veterinarians, and researchers). Include sufficientdetail in surveillance reports to permit local analy-sis and comparison with trends in drug use andmedical and agricultural practices.”
A final section on monitoring AR in agriculturalsettings recommends expansion of the NationalAntimicrobial Resistance Monitoring System(NARMS) and extension of its sampling to moni-tor transmission of resistant infections. It also rec-ommends monitoring of fruit and vegetableproduction and of environmental contaminationby antimicrobial drug residues and drug-resistantorganisms that enter the soil from human and ani-mal waste.

CHAPTER II
Increase awareness: optimize patientand provider behaviourJerry L. Avorn
• Minimal or nonexistent training of children atall levels of education in relation to health hab-its
• Aggressive marketing of antibiotics andantibacterials to both physicians and patients
• Inadequate or nonexistent continuing educationrequirements concerning infection control andantibiotic utilization for most health profession-als.
This chapter reviews the barriers for changingphysician and patient behaviour and suggestseffective intervention strategies.
Disincentives and barriers to overcome
A number of specific problems have been identi-fied that present obstacles to the development anddissemination of effective programmes of prescriberand patient education concerning the prudent useof antibiotics (7,21,22,39). These include:
• Inadequate support for publicly financed edu-cational programmes for either professionals orlay people
• Strong commercial pressures from manufactur-ers to increase utilization of antibiotics andantibacterials
• Low levels of literacy in the developing world,limiting the impact of verbally-based public edu-cation messages
• Fear of litigation in the United States which en-courages the practice of “defensive medicine”,often leading to prescription of an antibioticwhen one may not be necessary
• Pressures to shorten the length of a physicianvisit, which in turn increases pressure for anti-biotic utilization as a time-efficient means ofending the visit
• Poor regulation in the developing world of claimsmade in promotional materials for antibiotics
• Physicians’ desire for autonomy, which can make
Abstract
Considerable evidence points to widespread prob-lems in knowledge, attitudes, and behaviour relat-ing to antibiotic use among both patients andprescribers in the industrialized and the develop-ing worlds (19,32,33,34). Such evidence is drawnfrom numerous sources:
• Inappropriate patterns of antibiotic use for avariety of specific clinical conditions:
— Use of antibiotics to treat symptoms that areclearly viral in nature
— Reliance on excessively broad-spectrum an-tibiotics when narrower-spectrum agentswould be more appropriate
— Errors in the timing and duration of antibi-otic prophylaxis at the time of surgery
— Poor adherence by patients to prescribedantibiotic regimens, including prematurecessation of therapy and “hoarding” antibi-otics for future unsupervised use
• In the developing world, widespread use of an-tibiotic injections when not clinically indicated
• Erroneous responses by patients and physiciansto surveys concerning antibiotic knowledge andattitudes
• Under-use by physicians and consumers ofproven non-antibiotic means of infection con-trol, such as hand washing
• Growing consumer demand for “antibacterial”cleaning preparations which can actually increasebacterial resistance
• Low levels of use of products that can providesafe, effective alternatives to antibiotic use tocombat infection, such as condoms, bednets inmalaria-prone areas, vaccines.
The causes of such educational and behaviouraldeficits have also been well identified (8,35–38).They include:
• Inadequate training of health professionals inrational antibiotic use (and non-use)
33
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
34
them disinclined to accept guidelines or antibi-otic restrictions.
Educational strategies which have beenshown to be ineffective
One approach stands out as having remarkably lit-tle effect in altering antibiotic use. This approach,the simple dissemination of printed guidelines oreducational messages, without other reinforcement,is unfortunately among the most commonly used.This has now been studied in a variety ofrandomized controlled trial settings with strikinglyconsistent results: physicians who are mailed printedinformation on proper prescribing, but who do notreceive any other kind of intervention, in generaldo not change their practice any more than physi-cians randomized to a control group (40). The factthat this finding has been so consistently reportedmakes it even more disturbing that this approachis probably the single most frequently employedstrategy for changing antibiotic prescribing.Another common approach, that of having anexpert lecture a passive audience with minimalopportunity for interaction, has also been report-edly shown to result in little or no change in medi-cation use behaviour.
Fortunately, other methods of improving anti-biotic utilization have been well studied and foundto reliably improve the appropriateness of prescrib-ing. These are described in the section that follows.While the term “appropriate antibiotic use” will beused consistently, it should be pointed out that suchbroadly-defined education would also include suchtopics as the appropriate use of vaccines and theuse of alternative methods of infection control, suchas hand washing.
Strategies which have been demonstratedto be effective in improving theappropriateness of antibiotic use
Most studies and published recommendations haveconsidered education and behaviour change inter-ventions separately by the audience targeted:patients, prescribers, or (in the developing world)non-physician drug vendors. These categories willbe used in the sections which follow. However, it isevident that the ideal approach would constitute acombination strategy aimed at both the prescrib-ers and the users of antibiotics. In fact, somerecent research has shown that such a “double-barrelled” targeting of both audiences can producea synergistic effect much greater than that achieved
by addressing either audience separately.Another overarching principle evident in many
studies and policy recommendations on improve-ment of medication use is the concept that educa-tion/behaviour change interventions should betailored to the specific circumstances and needs ofthe audience, rather than presenting a “one size fitsall” formula which may not resonate with the indi-vidual experience of the targeted prescriber orpatient.
Ideally, programmes to change behaviour ofpatients, physicians, or lay caregivers should begrounded in solid behavioural science theory andexperience, as well as (equally practically) the theoryand experience of marketing (41). Specific theo-ries relevant to the reduction in antibiotic misuseinclude the PRECEDE model, which considersfactors that encourage or prevent behaviour change,and the Transtheoretical Model, which takes intoaccount the various cognitive and behavioural stagesassociated with adopting changes in a specific area(42,43).
While it is not easy to reduce inappropriate an-timicrobial use, some encouraging data exists aboutthe efficacy of some programmes in improvingproblematic practices. Overall, there is good newsabout the efficacy of such programmes in improv-ing drug use. In a review of 59 studies of interven-tions to improve medication use (primarilyantibiotics) in the developing world, Ross-Degnan(44) found that among studies which had an evalu-ation design adequate to permit comparison ofoutcomes, 43% of studies had an impact classifiedas “large” (>25% improvement compared to con-trols), and 36% had a moderate impact (10–25%improvement compared to controls). Only 21% ofthe studies had low or no impact (<10% improve-ment). The most common approach in this lattergroup of minimal impact was the dissemination ofprinted materials recommending rational utiliza-tion.
Interventions directed at prescribers
In that review (44), the following types of inter-ventions were found to produce significant im-provements in prescribing, as measured inrandomized intervention trials:
• Multiple training modalities applied together(group problem-solving, role playing, lectures,opportunity to practice skills)
• Focusing on one clinical issue at a time

35
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
• Training at the work site
• Use of opinion leaders or district-level staff astrainers
• Repeated sessions focusing on reinforcement ofthe message
• Community-based case management interven-tions (their use in acute respiratory infectionsand diarrhoea was so effective that a mortalitybenefit could be demonstrated).
Administrative interventions were found to workwell in improving antibiotic utilization if they hadthe following attributes:
• Were based on group process
• Involved ongoing supervision and monitoringof practice
• Provided regular audit and feedback of prescrib-ing patterns.
In a similar evaluation, Laing and Hogerzeil (un-published) reviewed the experience of a number ofprogrammes in the developing world and concludedthat the following strategies had strong records ofsuccess in improving prescribing of antibiotics andother drugs:
• The development and effective dissemination oflists of essential drugs and standardized treat-ment guidelines
• The creation and empowerment of pharmacyand therapeutics committees in hospitals
• Problem-oriented training
• Targeted in-service training of health workers.
In addition to these observations about effec-tive strategies, consensus has also developed con-cerning the clinical content of programmes toimprove antibiotic use. Some of these are quitestraightforward, such as the basic British recom-mendations advocated as a simple starting-pointfor reducing inappropriate antibiotic use (20):
• Avoid antibiotics for simple coughs and colds
• Do not use antibiotics for the treatment of viralsore throat
• Limit antibiotic use in uncomplicated cystitis inhealthy women to three days
• Limit telephone prescription of antibiotics toexceptional cases only.
Other recommended content areas for such an-
tibiotic education programmes are equally straight-forward, and contain messages such as the follow-ing:
• Do not use broad-spectrum antibiotics whennarrower-spectrum agents would work as well
• Base the antibiotic prescription on cultureresults whenever possible
• Modify the regimen over time as required
• Consider cost-effectiveness in choosing an anti-biotic regimen.
In the industrialized world, computers have beenput to good use in guiding choices of antibioticsfor hospitalized patients. In one system, a compu-ter “consultant” is given all pertinent facts concern-ing a patient’s infection and clinical condition, andthen offers antibiotic recommendations. These havebeen found to have a very high degree of clinicalaccuracy when compared with the “gold standard”recommendations of infectious disease specialists(45).
The ordering of all medications, including anti-biotics, on computer terminals will become com-mon in many institutions in the industrializedworld over the next few years. Initial experiencewith such systems in hospitals where they are al-ready in place indicates that they can be used togood advantage in reducing antibiotic utilizationby reminding the ordering physician at the time theorder is being written that such a choice is not inconformance with available evidence and/or insti-tutional guidelines, and offering more reasonablealternatives. Such systems can also be used to flagorders which require further consultation or ap-proval by an infectious disease consultant (46,47).
Other educational approaches less dependent ontechnology have also been demonstrated to beeffective in improving antibiotic use. In the 1980s,researchers in the United States began to apply thepowerful behaviour change interventions employedby the pharmaceutical industry, but put in the serv-ice of restrained prescribing rather than promotionof sales of a given product. In this approach, whichcame to be known as “academic detailing,” clini-cian/educators were trained from a medical schoolbase to become expert in the drug therapy requiredfor specific conditions, and also received trainingin strategies of “social marketing” and behaviourchange. These educational outreach workers werethen sent to visit with physicians in their offices ata convenient time, much as industry sales repre-sentatives do. They presented the need for appro-

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
36
priate prescribing in terms which were concise,clinically relevant, and behaviourally appropriate;the presentation was supplemented by engaging,well-designed, graphic print materials. Initially, sucheducational outreach workers were primarily phar-macists, but this role has also been filled effectivelyby physicians, nurses, and—in the developingworld—by lay people as well. The communicationis designed to be interactive rather than didactic,which offers the educator an opportunity to un-derstand the specific informational and attitudinalsituation of the targeted prescriber and to modifythe educational session accordingly. Following itsinitial demonstration in the United States, thisapproach has spread throughout the world, and hasbeen found to be equally effective in both industri-alized countries and the developing world. In April1997, a four-day conference in Chiang Mai, Thai-land, focused on improving medications in thedeveloping world; a number of such successful pro-grammes were described in detail. Cost-benefitanalyses have demonstrated that such programmescan save more than twice their expenses in terms ofreduction of unnecessary prescribing (44).
Education of students in the healthprofessions
Current training about rational antibiotic use iswidely regarded as inadequate in most pre-profes-sional settings throughout the world. More relevantand critical education about infection control andtreatment has been called for not just for medicalstudents, but also for students of nursing, phar-macy, and veterinary medicine. Beyond the spe-cific scientific content in pharmacology andmicrobiology that must be taught, students alsoneed to be taught to critically evaluate promotionalmaterials for medications to become more “mediasavvy” in evaluating printed advertisements andprepared to ask the right questions during sales pres-entations for antibiotics. Problem-based educationhas been found by many health professions educa-tors to be a useful and powerful method of com-municating such information.
Interventions directed at patients,families, and consumers
The patient is a vital link in the pathway of antibi-otic utilization; it is often patient demand whichtriggers inappropriate antibiotic prescribing in thefirst place. Because of this, and because of the cen-
tral role played by the patient (or parent of apediatric patient) in the implementation of antibi-otic regimens, strategies directed at consumers canbe of particular importance in reducing antibioticuse (48). Such education can take numerous forms:
• In pediatrics, caregivers can be educated to rec-ognize patterns of symptoms that can indicatewhether a child should be brought in for medi-cal care and potentially for an antibiotic prescrip-tion. Such education encourages appropriateutilization and discourages inappropriate use.
• Better recognition of the symptoms of malariacan allow for earlier referral to a health care pro-fessional, earlier diagnosis, and treatment.
• Education about the non-drug management ofroutine diarrhoea in children (e.g., with oral re-hydration solutions) can replace unnecessary re-ferrals to scarce medical resources, as well asinappropriate requests for antibiotics.
• In adults, conditions susceptible to such educa-tion about appropriate health-seeking behaviourinclude viral upper respiratory symptoms, vagin-itis, and recognition of the early symptoms ofHuman Immunodeficiency Virus (HIV), amongothers.
Public education programmes have focused onbroad themes, such as the lack of utility of antibi-otics in viral conditions and the need to adherecarefully to the prescribed regimen if an antibioticis ordered, rather than starting or stopping therapyon an as-needed basis.
A particularly interesting approach has beentaken in the United Kingdom to encourage thepublic to “cherish and conserve your natural flora,”pointing out the beneficial aspects of bacteria whichcan be obliterated by excessive antibiotic use. Othergroups have advocated the education of the publicconcerning the risks of unnecessary antibiotic usein animals and agriculture as well as humans; theAlliance for the Prudent Use of Antibiotics (APUA)has been particularly active in this regard.
Other audiences for interventions
Beyond the obvious targets of physicians and pa-tients, other important groups have been identi-fied as appropriate audiences for education aboutantibiotic use, including workers in day care cen-tres, schoolteachers, those who work in agriculture,and policy-makers in all these areas as well as healthcare.

37
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
System-wide interventions
In addition to strategies directed at prescribers andpatients, a number of effective educational strate-gies have targeted the health care delivery systemitself, whether in the form of governmental healthcare services or private sector health practices orsystems. This section will not deal with regulatoryapproaches to improve the antibiotic use, whichare discussed elsewhere in this report (See ChapterIII). Rather, it will focus on means of educatingthe participants and leaders of such systems in or-der to encourage them to adopt more enlightenedpolicies at a systems level (31,49).
• The creation of drugs and therapeutics commit-tees (or pharmacy and therapeutics committees)can be a very useful strategy at the level of indi-vidual health centres as well as at the level ofnational health care programmes. Such groupscan evaluate all available evidence concerningutilization data, resistance patterns, efficacy, andcost, in order to make recommendations forproper antibiotic use which are appropriate to aparticular clinical setting and population.
• Dissemination of essential drug lists, such asthose promulgated by the World Health Organi-zation (WHO), can help simplify antibioticchoices for practitioners as well as make themmore clinically appropriate and cost-effective.
• Facilitation of communication among academicinstitutions, government agencies, those who payfor health care, and pharmaceutical manufac-turers can sometimes reduce the extent to whichsuch entities act at cross purposes in relation toone another in relation to antibiotic use andinfection control.
• Beyond the drug lists themselves, guidelines forthe use (or non-use) of antibiotics in particularsituations can improve the rationality of prescrib-ing. For maximum benefit, such guidelinesshould be:
— Evidence-based— Appropriate to the clinical and microbiologi-
cal issues relevant to a given population— Developed with the involvement of the prac-
titioners (and potentially the patients) whowill be using them
— Disseminated not simply via printed memo-randa, but rather through the use of interac-tive strategies oriented to changes in behaviour,as described elsewhere in this section.
A number of strategies for improving the knowl-edge base of physicians and the public concerningantibiotic use have pointed to the need for capac-ity building on a number of fronts to make suchprogrammes possible. Such infrastructure require-ments fall into several categories. First among theseis the capacity to devise, validate, and modify evi-dence-based guidelines on rational antibiotic use,since this is necessary to provide the content neededto drive any educational programme. These pro-grammes can be governmentally sponsored, as isthe case with the British National Institute for Clini-cal Excellence (NICE), or the guidelines develop-ment process of the US Agency for Health CarePolicy and Research before it was disbanded underpolitical pressure several years ago. Similar activi-ties have been conducted by the US Centers forDisease Control and Prevention as well as WHO,and antibiotic guidelines have been widely dissemi-nated in Australia. In addition, professional socie-ties have also developed their own evidence-basedguidelines for appropriate antibiotic use. These haveincluded the American Society for Microbiology,and a variety of specialty societies (e.g., the Ameri-can Heart Association guidelines for the use of pro-phylactic antibiotics in patients with valvular heartdisease, or the American College of Gastroenterol-ogy recommendations concerning regimens for theeradication of H. pylori infection).
WHO has identified a number of other infra-structure-related issues that bear directly on thecapacity to mount successful educational pro-grammes concerning antibiotics. These include:
• Control of the promotional activities of drugmanufacturers
• Training of a new category of health professional,the antimicrobial resistance manager/monitor(ARM), to serve as a local resource to follow thecurrent literature on antibiotic resistance,analyse local data, propose and implement strat-egies for control and resistance, and work withclinicians on the care of specific patients
• Development and enforcement of ethical stand-ards concerning advertising of antibiotics
• Analysis of data on local resistance patterns
• Communication of global trends in antibioticresistance with potential local impact
• Development of information systems to moni-tor and feed back data on utilization and resist-ance patterns.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
38
Similarly, the US Agency for InternationalDevelopment (USAID) (39) has also focused onthe need to build local capacity in developing coun-tries to provide the infrastructure needed to encour-age rational antibiotic use. This includes trainingof personnel and creation of systems to:
• Perform surveillance
• Manage data
• Conduct educational programmes
• Choose which antibiotics to purchase
• Develop policies concerning regulation, reim-bursement, and financing of antibiotic purchases
• Provide unbiased drug information
• Establish field sites for innovative demonstra-tion projects (e.g., tuberculosis surveillance andcontrol)
• Train microbiology laboratory personnel
• Prepare training and advocacy materials forlocal government officials on the burden ofdisease related to resistance and the need forspecific programmes to combat it
• Develop and enforce quality control standardsfor drug manufacturing and microbiology labo-ratories.
Internet access makes it possible for patients andpractitioners throughout the world to have instan-taneous access to current information about medi-cations, patterns of resistance, and other datarelevant to appropriate antibiotic use. One suchguide has been made available on the Internetthrough WHO (http://www.who.int). For otherrelevant web sites see the section, Some Useful WebSites.
Conclusions
Just as considerable progress has been made inmicrobiology and clinical infectious diseases in thelast two decades, similar progress has been madeduring this period in understanding why antibiot-ics are misused by prescribers and by patients, and,equally important, which strategies are most effec-tive in preventing such misuse. Rigorous data areavailable describing the effect of such innovativeprogrammes in patient and caregiver education,computer-based prescribing guidelines, academicdetailing of prescribers, and community-orientededucational programmes; such studies have amplydemonstrated their utility and, for some, even theircost-effectiveness. Similarly consistent data are avail-able describing the poor track record of many con-ventional practices in changing practice patterns,such as the mailed transmission of expert guide-lines. It is unfortunately true that such older, con-ventional practices remain the norm, while moreinnovative programmes, though becoming morewidely adopted each year, still form the minorityof intervention programmes. This is probably thecombined result of habit and tradition, as well asthe lower costs required to conduct programmesthat are print-only in nature, and skepticism con-cerning the cost-effectiveness of more interactiveperson-based programmes. As the stakes becomehigher each year in terms of the clinical and eco-nomic consequences of antibiotic misuse, it is tobe hoped that educational interventions in thisarena are subjected to the same critical evaluationand evidence-based use as are the medicationswhose utilization they attempt to improve.
39
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
CHAPTER III
Strengthen sanitation, infection control,and regulatory measuresPeter G. Davey
• Failure to cleanse hands after each patient con-tact
• Limited use of gloves and gowns
• Lack of sterile supplies and poor sterilizationpractices
• Increased movement of patients within and be-tween hospitals.
There is a broad consensus among the expertpolicy groups (see Table B) on the need to establishan infection control programme in order to moreeffectively control hospital infections. Elements ofsuch a programme identified in the reports are:• Surveillance of infection
• Identification of outbreaks
• Implementation of effective control measures(e.g., hand washing, gowns)
• Sterilization and disinfection of equipment andsupplies.
Most of the reports reviewed recommendedsome form of a committee or programme to be re-sponsible for the improvement of infection con-trol. The general statements about infection controlimprovements within hospitals need to be supple-mented by the specific recommendations for im-provement of infection control which wereaddressed in some of the previous expert reports(see Tables C and D). Developing countries in par-ticular face the challenge of improving their publichealth infrastructure, community sanitation andhealth education in order to decrease the emergenceand spread of infections. This is a priority need inorder to decrease the spread of resistant organisms.All countries could improve education of health careand day care workers (5,49). The previous expertreports also make strong recommendations aboutmandating hospital infection control within pur-chasing and commissioning agreements (see TablesC and D).
Abstract
Governmental and private health management sys-tems, at national, regional, and local levels providethe basis for the delivery of health care. These sys-tems are critical to the curtailment of antimicro-bial resistance because they help determine theavailability and usage of antimicrobials. They alsoplay a role in developing and enforcing programmesto reduce the spread of microbial infections,whether in hospitals or in the community.
Limiting microbial infections is a key step to-wards the goal of reducing the current prevalenceof antimicrobial-resistant organisms. The respon-sibility of carrying out the daily routines of infec-tion control and sanitation programmes falls tohospital management and health care providers.These routines range from proper hand washing toreporting surveillance data.
This chapter reviews the expert groups’ (1,5,6,7,11,13,19,20,21,22,24) findings and strategies re-lating to 1) sanitation and infection control, and2) government and health system regulation. Thisreview outlines what is covered in previous expertpolicy reports, and provides guidelines from theexpert policy groups on a global strategy. The re-view also designates specific programme compo-nents and models that countries might consider indeveloping their national strategies for infectioncontrol and regulation of antibiotics. Areas of con-cern from previous reports and additional recom-mendations from the expert policy reports arenoted.
I. Sanitation and infection control
Control and prevention of microbial infections andimproved sanitation in the health care setting areimperative to decrease the spread of resistantorganisms and minimize the need for antibiotics.As cited in the expert reports reviewed (1,5,6,7,11,13,19,20,21,22,24) (Table A), the major fac-tors contributing to the spread of infection andantibiotic resistance transfer in health care settingsare:

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
40
Other national models for antibiotic resistanceintervention
Several programmes and guidelines related to healthcare management and the control of infections havebeen developed after most of the policy reports werepublished. Since infection control is a key strategyin containing antibiotic resistance, local govern-ments and professional societies could consideradapting the following programmes to their ownneeds, within the limits of available resources (otherexamples of local initiatives are outlined in Appen-dix B).
• The epic project: Developing National Evidence-Based Guidelines for Preventing Healthcare-Associated Infections. The epic project hasdeveloped guidelines, approved by the UKDepartment of Health, which include the fol-lowing topics: standard principles (hospital en-vironmental hygiene, hand hygiene, the use ofpersonal protective equipment, and the use anddisposal of sharps); short-term indwelling urethralcatheters in acute care; and central venous cath-eters. The guidelines are targeted at the UnitedKingdom and are thought to be practical andaffordable within that context. However, thestructure of the guidelines would facilitateadaptation to other countries, including devel-oping countries. The second phase of the epicprogramme will concentrate on control of in-fection in the community. More information canbe found at the following web site: http://www.epic.tvu.ac.uk/
• The HELICS project: (Hospitals in Europe Linkfor Infection Control Through Surveillance).HELICS has produced infection control recom-mendations for hospitals in the EuropeanUnion (EU), annexes describing various nationalinfection control programmes, and the currentnational policies concerning antibiotic resistancefrom each EU member state. This informationcan be found at the Nosocomial Infection Con-trol in Europe web site (http://helics.univ-lyon1.fr).
Summary and conclusions: infection controlexperiences
The statements about hospital infection from thevarious expert reports discuss important actions atthe local and national level to curb antibiotic re-sistance. This author suggests that they should befollowed by these specific actions:
• Adapt for local use the HELICS Methodology for Measur-ing the Status Quo for National Initiatives in InfectionControl
This is consistent with the recommendationfrom the WHO Scientific Working Group (5):“Develop methods and standards for evaluatinghospital infection and antimicrobial resistancecontrol programmes, leading ultimately tonational accreditation systems.”
• Adapt the epic Evidence Based Guidelines (http://helics.univ-lyon1.fr) for implementation in other coun-tries
The evidence reviewed in these guidelines is acomprehensive review of the published worldliterature. However, there may be existing localguidelines that could be reviewed and incorpo-rated into country-specific guidelines. Thesewould also need to take account of existing clini-cal practices and facilities.
• Encourage governments to accept accountability forinfection control at the national level by making hospi-tal management accountable for local implementation
This direction is consistent with the recommen-dation from the WHO Scientific WorkingGroup (5): “Link the prevention and control ofantimicrobial resistant organisms in hospital tonational and local quality assurance efforts.”
The concept of clinical governance is having con-siderable impact in the United Kingdom. TheUK Government has put infection control andantimicrobial resistance into the list of nationalpriorities for public health, and used initiativeson clinical governance to make it clear to hospi-tal management that they are responsible foraction in their hospitals. This approach is nowbeing extended to managers responsible for com-munity health services.
• Emphasize the importance of infection control in thecommunity
In addition to the recommendations of theWHO Scientific Working Group (5), develop-ment of related interventions to contain anti-microbial resistance in the community includeeducational programmes and hygienic standardsfor day care and extended-care facilities, andpromotion of hygiene in the community, includ-ing safe water and food hygiene.
As noted in the UK House of Lords report (21),infection control beyond the hospital is an areaof particular weakness. Communities should
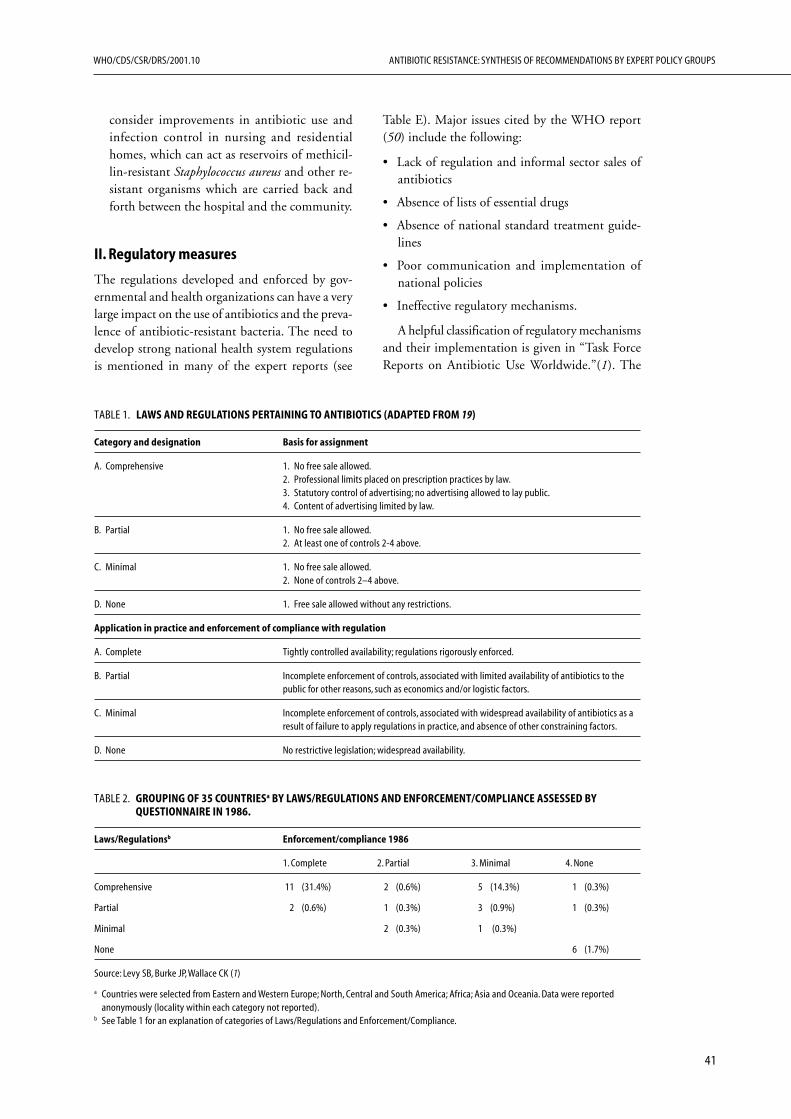
41
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
consider improvements in antibiotic use andinfection control in nursing and residentialhomes, which can act as reservoirs of methicil-lin-resistant Staphylococcus aureus and other re-sistant organisms which are carried back andforth between the hospital and the community.
II. Regulatory measures
The regulations developed and enforced by gov-ernmental and health organizations can have a verylarge impact on the use of antibiotics and the preva-lence of antibiotic-resistant bacteria. The need todevelop strong national health system regulationsis mentioned in many of the expert reports (see
TABLE 1. LAWS AND REGULATIONS PERTAINING TO ANTIBIOTICS (ADAPTED FROM 19)
Category and designation Basis for assignment
A. Comprehensive 1. No free sale allowed.2. Professional limits placed on prescription practices by law.3. Statutory control of advertising; no advertising allowed to lay public.4. Content of advertising limited by law.
B. Partial 1. No free sale allowed.2. At least one of controls 2-4 above.
C. Minimal 1. No free sale allowed.2. None of controls 2–4 above.
D. None 1. Free sale allowed without any restrictions.
Application in practice and enforcement of compliance with regulation
A. Complete Tightly controlled availability; regulations rigorously enforced.
B. Partial Incomplete enforcement of controls, associated with limited availability of antibiotics to thepublic for other reasons, such as economics and/or logistic factors.
C. Minimal Incomplete enforcement of controls, associated with widespread availability of antibiotics as aresult of failure to apply regulations in practice, and absence of other constraining factors.
D. None No restrictive legislation; widespread availability.
TABLE 2. GROUPING OF 35 COUNTRIESa BY LAWS/REGULATIONS AND ENFORCEMENT/COMPLIANCE ASSESSED BYQUESTIONNAIRE IN 1986.
Laws/Regulationsb Enforcement/compliance 1986
1. Complete 2. Partial 3. Minimal 4. None
Comprehensive 11 (31.4%) 2 (0.6%) 5 (14.3%) 1 (0.3%)
Partial 2 (0.6%) 1 (0.3%) 3 (0.9%) 1 (0.3%)
Minimal 2 (0.3%) 1 (0.3%)
None 6 (1.7%)
Source: Levy SB, Burke JP, Wallace CK (1)
a Countries were selected from Eastern and Western Europe; North, Central and South America; Africa; Asia and Oceania. Data were reportedanonymously (locality within each category not reported).
b See Table 1 for an explanation of categories of Laws/Regulations and Enforcement/Compliance.
Table E). Major issues cited by the WHO report(50) include the following:
• Lack of regulation and informal sector sales ofantibiotics
• Absence of lists of essential drugs
• Absence of national standard treatment guide-lines
• Poor communication and implementation ofnational policies
• Ineffective regulatory mechanisms.
A helpful classification of regulatory mechanismsand their implementation is given in “Task ForceReports on Antibiotic Use Worldwide.”(1). The

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
42
report reviewed policies about antibiotics in thirty-five countries and found that only eleven (31%)had comprehensive laws and regulations that werecompletely enforced (Tables 1 and 2). This evidencesupports the need for more effective regulatorymechanisms. The data in “Task Force Reports” arenearly fifteen years old; nonetheless, there is broadconsensus among the experts on the need to ad-dress the five problems listed above (see Table E).There is also broad historical consensus in supportof effective national regulation of antibiotic qual-ity, dissemination, and promotion.
Elements of a national policy to combat antibioticresistance
Additional regulatory recommendations proposedin the recent WHO report (50) are also repeatedlysuggested by previous expert reports (see Table F)and suggest a basic framework that each countryshould establish to minimize the emergence andspread of antibiotic resistance in their country:
• Adopt the WHO model legal framework forantimicrobial licensing, sale, supply, distribution,and promotion
• Introduce legal requirements for collection ofdata on antimicrobial production, distribution,sales, and consumption in human, veterinary,and agricultural use
• Introduce formal training for personnel in anti-microbial dispensing outlets and registrationschemes for such outlets.
Additionally, the WHO document (50) makesthe following recommendation: “identify and elimi-nate economic incentives (i.e., reimbursement prac-tices) that encourage inappropriate antimicrobialuse.” This recommendation was apparently over-looked by the other expert policy groups and is onlyendorsed by one of the other documents (6, TableF). Nonetheless, it is an important global issue anda key consideration for national governmentsattempting to control antibiotic use.
Finally, the importance of involving inter-national organizations is noted in the WHOrecommendation: “Target advocacy for actionencouraging prudent use of antimicrobials amongrelevant organizations, such as the World TradeOrganization, the World Bank and the Interna-tional Monetary Fund” (50).
Additional issues concerning government and healthmanagement systems
Additional specific issues and recommendationsfrom individual expert reports fall into two mainareas (detailed in Tables G and H). The first areaconcerns suggestions for additional legislation toimprove the prudent use of antimicrobials, for ex-ample, granting antimicrobial use licenses contin-gent upon implementing antimicrobial-usemonitoring programmes, or, where applicable,adjusting subsidies for antibiotics to encourage amore prudent use (20,51).
The second area concerns legal issues that mayimpact implementation of infection control or an-timicrobial use measures. One example is improv-ing personal human rights laws, especially indeveloping countries, so that they have a positiveimpact on a population’s public health (19,51). Thedocument by Fidler (51), is a particularly rich sourceof issues about legislation, encompassing trade regu-lations, patient rights, data privacy, and patent pro-tection.
Another example is creating economic incentivesfor pharmaceutical companies to develop new an-timicrobial medications (51). The listed statementsalso include good practice guidelines for antimi-crobial use, such as assisting poorer countries togain supplies of appropriate antimicrobials, as wellas creating international alert systems concerningantimicrobial resistance (7,49,51).
Conclusions: Regulatory measures
In the management of distribution, availability anduse of antimicrobials, several factors—legal, eco-nomic, and scientific—should be considered, assummarized below:
• Development of guidance documents by governmentand health systems on policies for antimicrobial use
Local ownership of guidelines adds to their suc-cess. Guidelines can be applied to infection con-trol and can also be part of general antibioticpolicies, where local microbial epidemiology canjustify variations in prescribing and where thereare legitimate concerns about the selection pres-sures created by uniform national prescribingpolicies. These guidance documents should bereadily adaptable for use in developing countries.
• Assessment of policies, laws, and regulations and theirimplementation
The 1987 report by the US Department ofHealth and Human Services (1) could be up-
43
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
dated. The original report did not reveal theidentity of the countries that submitted data.This author would query whether secrecy aboutsuch an important global issue either necessaryor justifiable.
• Review opportunities for improving prudent use of an-tibiotics by changing the licensing process
Extend patents in exchange for industry supportof programmes to limit the use of antibioticsand support license extension of older drugs withactivity against resistant pathogens through fasttracking or orphan drug programmes.
• Investigate the effect of changes in reimbursement poli-cies on prudent use of antibiotics and on surveillance ofprescribing or resistance
This is an important recommendation in “Con-taining Antimicrobial Resistance”(50) but doesnot appear in the other WHO documents. It isendorsed by US Congress Office of TechnologyAssessment (6), which identifies a potentialproblem with Medicaid and Medicare reim-bursement policies. This issue deserves widerconsideration in a global context. In addition toconsidering reimbursement for prescribing, theextent to which privatization of laboratoriesthreatens the surveillance of antibiotic resistanceor infection control should be investigated.
• Consider recommendations (51) about trade restrictionsagainst countries that systematically neglect recognizedprinciples and practices for antimicrobial use
In the context of environmental protection, traderestrictions seeking to change a production proc-ess in another country, rather than to protectagainst health dangers from a particular prod-uct, have been ruled incompatible with interna-tional trade law. As part of a general strategy tocombat antimicrobial misuse, legitimate traderestrictions against countries that systematicallyneglect recognized principles and practices forantimicrobial use might be considered; such amove would elevate the status of Codex’s Codeof Practice for Control of the Use of VeterinaryDrugs and Guidelines for the Establishment ofa Regulatory Program for Control of VeterinaryDrug Residues in Foods (52), in the same wayas the Sanitary Phytosanitary (SPS) Agreement haselevated the importance of Codex’s MaximumResidue Levels for Veterinary Drugs in Foods.
• Identify opportunities to link financial incentives to im-plementation of policies at the national or regional level
In the United States the most powerful strategywould be to make implementation of state poli-cies to curb the misuse of antimicrobial drugsmandatory before states receive federal fundsearmarked for public health. Similar opportu-nities should be explored in other countries.
• Investigate methods for mandating technical or finan-cial support from developed countries to developingcountries
Fulfilment of legal duties often hinges on suffi-cient resources. In many developing countries,public health systems may be inadequate. Thus,financial and technical leadership is needed fromnational governments towards local authorities,and from international organizations towards de-veloping countries. A precedent can be foundin the proposed Convention on the Provisionof Telecommunication Resources for DisasterMitigation and Relief Operations, which obli-gates the parties, where possible, to lower orremove regulatory barriers for using telecommu-nication resources during disasters.
• Investigate international law on personal control anddata protection issues relating to antimicrobial resist-ance
At a time when antimicrobial resistance may havecreated a greater need for personal control meas-ures for public health (e.g., with multidrug-resistant tuberculosis), the status of internationallaw on the scope and nature of a government’spower to undertake such measures should bereviewed. Lessons from international environ-mental efforts suggest that international lawmust play a major role in setting internationalstandards for implementation at the nationallevel, and creating the political, technical, andfinancial conditions necessary to integrate in-ternational and national law.
• Build on experience in EU countries of legislation againstuse of antibiotics in growth promotion
The EU has passed legislation to eliminate anti-biotics that are used in humans from being usedas growth promoters in animal feeds. However,Denmark and Sweden have banned growth pro-moters entirely. If other governments are to fol-low that lead, they will need to be reassured thatthere are no adverse economic consequences.Therefore, data about the impact of legislationin Denmark and Sweden should be collected andpublicized (see also Chapter V).
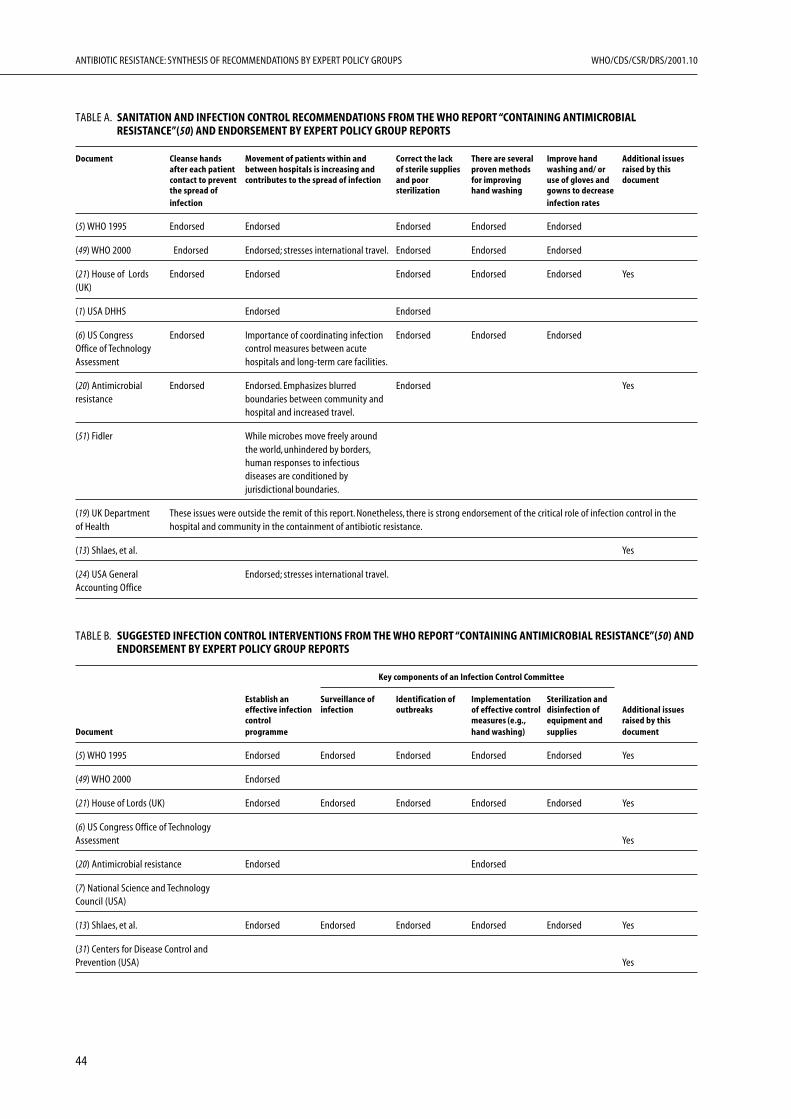
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
44
TABLE A. SANITATION AND INFECTION CONTROL RECOMMENDATIONS FROM THE WHO REPORT “CONTAINING ANTIMICROBIALRESISTANCE”(50) AND ENDORSEMENT BY EXPERT POLICY GROUP REPORTS
Document Cleanse hands Movement of patients within and Correct the lack There are several Improve hand Additional issuesafter each patient between hospitals is increasing and of sterile supplies proven methods washing and/ or raised by thiscontact to prevent contributes to the spread of infection and poor for improving use of gloves and documentthe spread of sterilization hand washing gowns to decreaseinfection infection rates
(5) WHO 1995 Endorsed Endorsed Endorsed Endorsed Endorsed
(49) WHO 2000 Endorsed Endorsed; stresses international travel. Endorsed Endorsed Endorsed
(21) House of Lords Endorsed Endorsed Endorsed Endorsed Endorsed Yes(UK)
(1) USA DHHS Endorsed Endorsed
(6) US Congress Endorsed Importance of coordinating infection Endorsed Endorsed EndorsedOffice of Technology control measures between acuteAssessment hospitals and long-term care facilities.
(20) Antimicrobial Endorsed Endorsed. Emphasizes blurred Endorsed Yesresistance boundaries between community and
hospital and increased travel.
(51) Fidler While microbes move freely aroundthe world, unhindered by borders,human responses to infectiousdiseases are conditioned byjurisdictional boundaries.
(19) UK Department These issues were outside the remit of this report. Nonetheless, there is strong endorsement of the critical role of infection control in theof Health hospital and community in the containment of antibiotic resistance.
(13) Shlaes, et al. Yes
(24) USA General Endorsed; stresses international travel.Accounting Office
TABLE B. SUGGESTED INFECTION CONTROL INTERVENTIONS FROM THE WHO REPORT “CONTAINING ANTIMICROBIAL RESISTANCE”(50) ANDENDORSEMENT BY EXPERT POLICY GROUP REPORTS
Key components of an Infection Control Committee
Establish an Surveillance of Identification of Implementation Sterilization andeffective infection infection outbreaks of effective control disinfection of Additional issuescontrol measures (e.g., equipment and raised by this
Document programme hand washing) supplies document
(5) WHO 1995 Endorsed Endorsed Endorsed Endorsed Endorsed Yes
(49) WHO 2000 Endorsed
(21) House of Lords (UK) Endorsed Endorsed Endorsed Endorsed Endorsed Yes
(6) US Congress Office of TechnologyAssessment Yes
(20) Antimicrobial resistance Endorsed Endorsed
(7) National Science and TechnologyCouncil (USA)
(13) Shlaes, et al. Endorsed Endorsed Endorsed Endorsed Endorsed Yes
(31) Centers for Disease Control andPrevention (USA) Yes
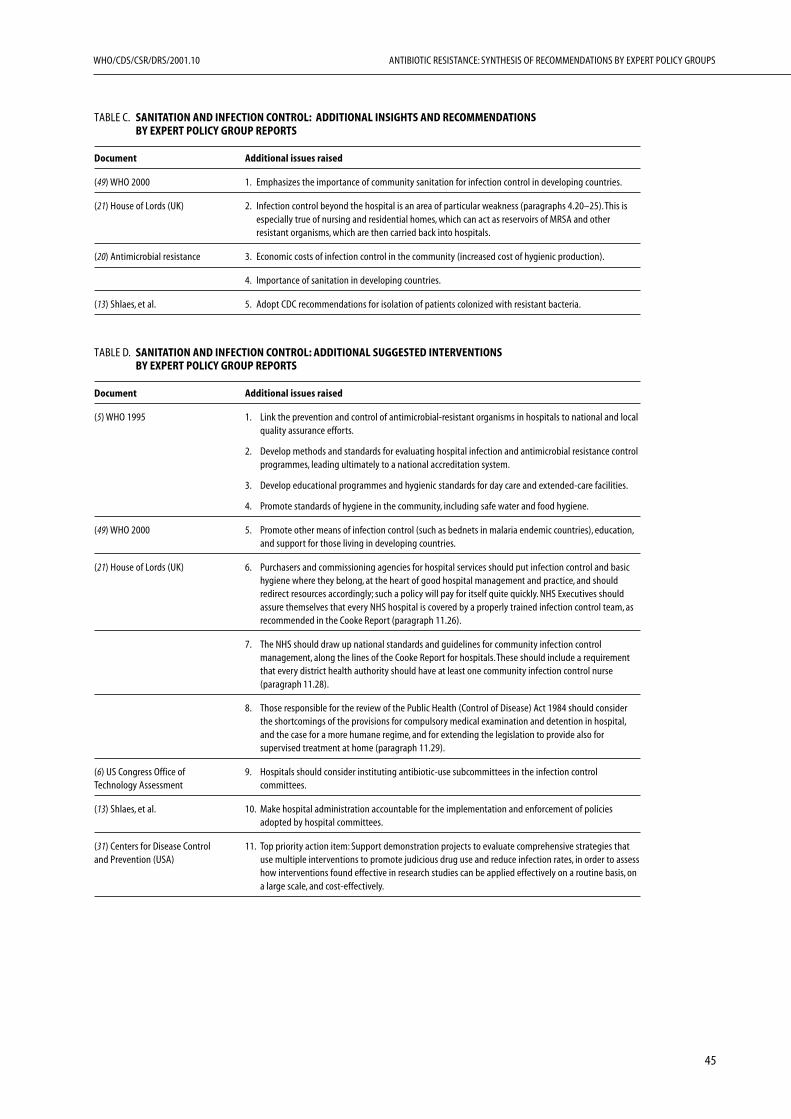
45
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
TABLE C. SANITATION AND INFECTION CONTROL: ADDITIONAL INSIGHTS AND RECOMMENDATIONSBY EXPERT POLICY GROUP REPORTS
Document Additional issues raised
(49) WHO 2000 1. Emphasizes the importance of community sanitation for infection control in developing countries.
(21) House of Lords (UK) 2. Infection control beyond the hospital is an area of particular weakness (paragraphs 4.20–25). This isespecially true of nursing and residential homes, which can act as reservoirs of MRSA and otherresistant organisms, which are then carried back into hospitals.
(20) Antimicrobial resistance 3. Economic costs of infection control in the community (increased cost of hygienic production).
4. Importance of sanitation in developing countries.
(13) Shlaes, et al. 5. Adopt CDC recommendations for isolation of patients colonized with resistant bacteria.
TABLE D. SANITATION AND INFECTION CONTROL: ADDITIONAL SUGGESTED INTERVENTIONSBY EXPERT POLICY GROUP REPORTS
Document Additional issues raised
(5) WHO 1995 1. Link the prevention and control of antimicrobial-resistant organisms in hospitals to national and localquality assurance efforts.
2. Develop methods and standards for evaluating hospital infection and antimicrobial resistance controlprogrammes, leading ultimately to a national accreditation system.
3. Develop educational programmes and hygienic standards for day care and extended-care facilities.
4. Promote standards of hygiene in the community, including safe water and food hygiene.
(49) WHO 2000 5. Promote other means of infection control (such as bednets in malaria endemic countries), education,and support for those living in developing countries.
(21) House of Lords (UK) 6. Purchasers and commissioning agencies for hospital services should put infection control and basichygiene where they belong, at the heart of good hospital management and practice, and shouldredirect resources accordingly; such a policy will pay for itself quite quickly. NHS Executives shouldassure themselves that every NHS hospital is covered by a properly trained infection control team, asrecommended in the Cooke Report (paragraph 11.26).
7. The NHS should draw up national standards and guidelines for community infection controlmanagement, along the lines of the Cooke Report for hospitals. These should include a requirementthat every district health authority should have at least one community infection control nurse(paragraph 11.28).
8. Those responsible for the review of the Public Health (Control of Disease) Act 1984 should considerthe shortcomings of the provisions for compulsory medical examination and detention in hospital,and the case for a more humane regime, and for extending the legislation to provide also forsupervised treatment at home (paragraph 11.29).
(6) US Congress Office of 9. Hospitals should consider instituting antibiotic-use subcommittees in the infection controlTechnology Assessment committees.
(13) Shlaes, et al. 10. Make hospital administration accountable for the implementation and enforcement of policiesadopted by hospital committees.
(31) Centers for Disease Control 11. Top priority action item: Support demonstration projects to evaluate comprehensive strategies thatand Prevention (USA) use multiple interventions to promote judicious drug use and reduce infection rates, in order to assess
how interventions found effective in research studies can be applied effectively on a routine basis, ona large scale, and cost-effectively.
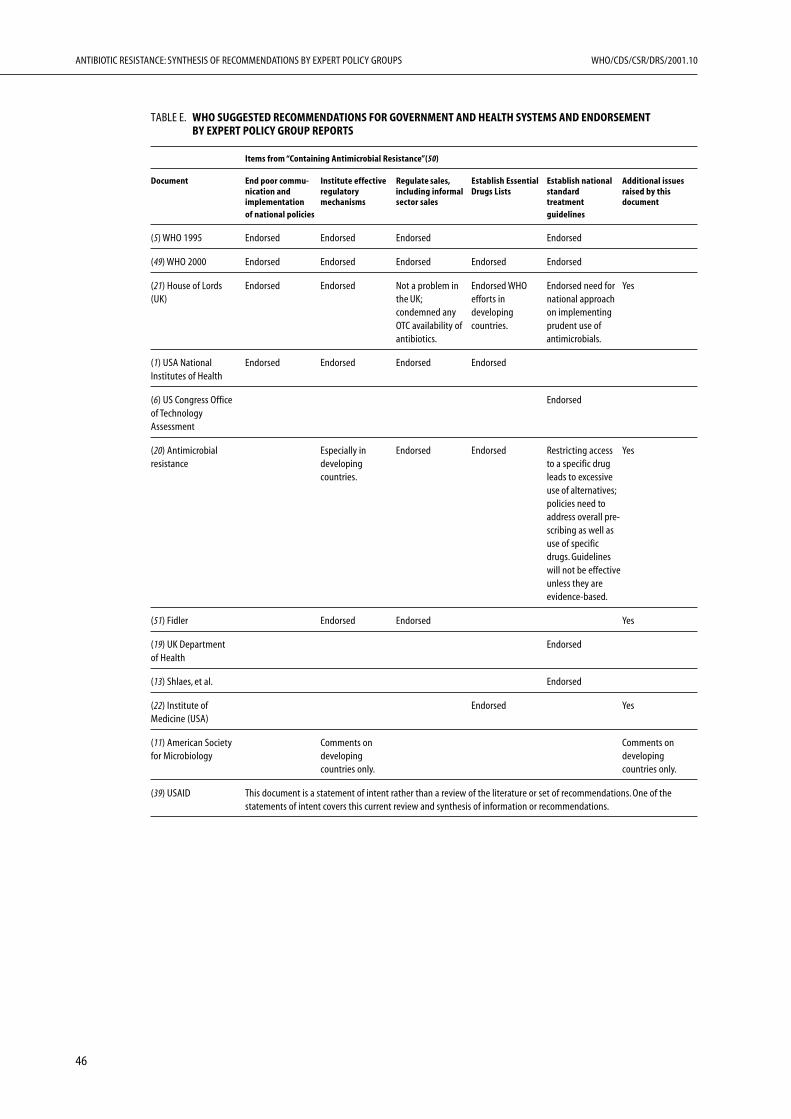
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
46
TABLE E. WHO SUGGESTED RECOMMENDATIONS FOR GOVERNMENT AND HEALTH SYSTEMS AND ENDORSEMENTBY EXPERT POLICY GROUP REPORTS
Items from “Containing Antimicrobial Resistance”(50)
Document End poor commu- Institute effective Regulate sales, Establish Essential Establish national Additional issuesnication and regulatory including informal Drugs Lists standard raised by thisimplementation mechanisms sector sales treatment documentof national policies guidelines
(5) WHO 1995 Endorsed Endorsed Endorsed Endorsed
(49) WHO 2000 Endorsed Endorsed Endorsed Endorsed Endorsed
(21) House of Lords Endorsed Endorsed Not a problem in Endorsed WHO Endorsed need for Yes(UK) the UK; efforts in national approach
condemned any developing on implementingOTC availability of countries. prudent use ofantibiotics. antimicrobials.
(1) USA National Endorsed Endorsed Endorsed EndorsedInstitutes of Health
(6) US Congress Office Endorsedof TechnologyAssessment
(20) Antimicrobial Especially in Endorsed Endorsed Restricting access Yesresistance developing to a specific drug
countries. leads to excessiveuse of alternatives;policies need toaddress overall pre-scribing as well asuse of specificdrugs. Guidelineswill not be effectiveunless they areevidence-based.
(51) Fidler Endorsed Endorsed Yes
(19) UK Department Endorsedof Health
(13) Shlaes, et al. Endorsed
(22) Institute of Endorsed YesMedicine (USA)
(11) American Society Comments on Comments onfor Microbiology developing developing
countries only. countries only.
(39) USAID This document is a statement of intent rather than a review of the literature or set of recommendations. One of thestatements of intent covers this current review and synthesis of information or recommendations.
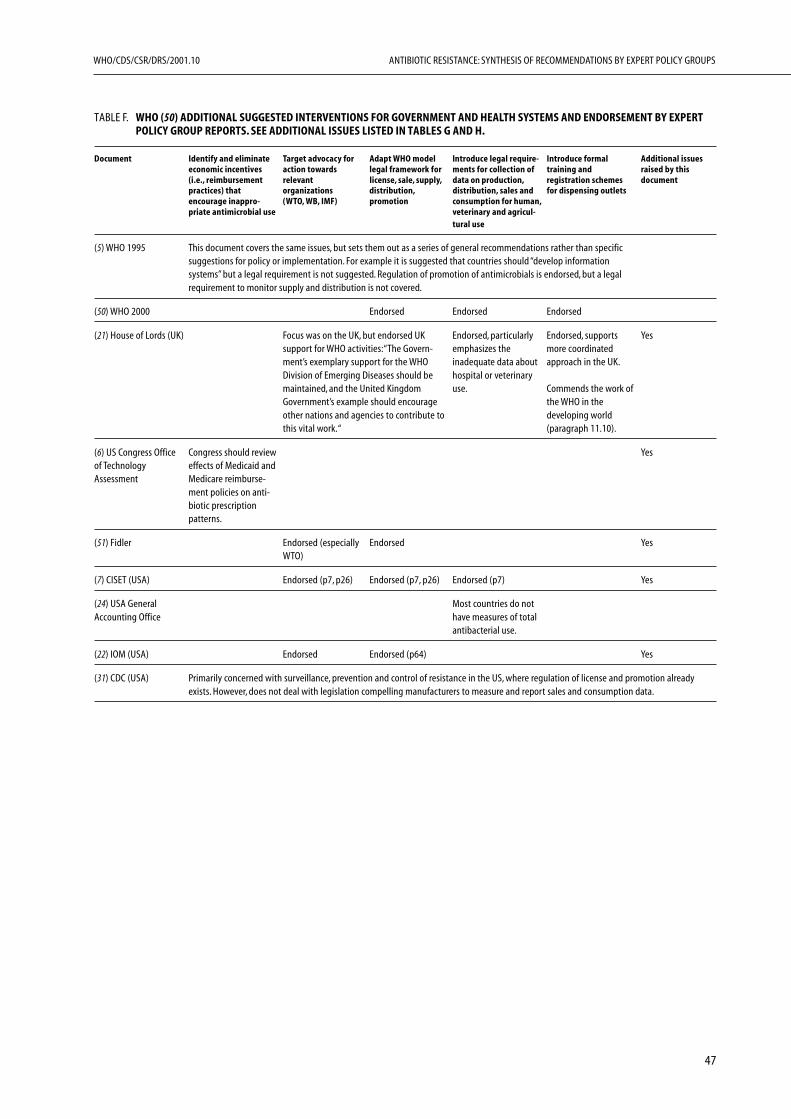
47
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
TABLE F. WHO (50) ADDITIONAL SUGGESTED INTERVENTIONS FOR GOVERNMENT AND HEALTH SYSTEMS AND ENDORSEMENT BY EXPERTPOLICY GROUP REPORTS. SEE ADDITIONAL ISSUES LISTED IN TABLES G AND H.
Document Identify and eliminate Target advocacy for Adapt WHO model Introduce legal require- Introduce formal Additional issueseconomic incentives action towards legal framework for ments for collection of training and raised by this(i.e., reimbursement relevant license, sale, supply, data on production, registration schemes documentpractices) that organizations distribution, distribution, sales and for dispensing outletsencourage inappro- (WTO, WB, IMF) promotion consumption for human,priate antimicrobial use veterinary and agricul-
tural use
(5) WHO 1995 This document covers the same issues, but sets them out as a series of general recommendations rather than specificsuggestions for policy or implementation. For example it is suggested that countries should “develop informationsystems” but a legal requirement is not suggested. Regulation of promotion of antimicrobials is endorsed, but a legalrequirement to monitor supply and distribution is not covered.
(50) WHO 2000 Endorsed Endorsed Endorsed
(21) House of Lords (UK) Focus was on the UK, but endorsed UK Endorsed, particularly Endorsed, supports Yessupport for WHO activities: “The Govern- emphasizes the more coordinatedment’s exemplary support for the WHO inadequate data about approach in the UK.Division of Emerging Diseases should be hospital or veterinarymaintained, and the United Kingdom use. Commends the work ofGovernment’s example should encourage the WHO in theother nations and agencies to contribute to developing worldthis vital work. “ (paragraph 11.10).
(6) US Congress Office Congress should review Yesof Technology effects of Medicaid andAssessment Medicare reimburse-
ment policies on anti-biotic prescriptionpatterns.
(51) Fidler Endorsed (especially Endorsed YesWTO)
(7) CISET (USA) Endorsed (p7, p26) Endorsed (p7, p26) Endorsed (p7) Yes
(24) USA General Most countries do notAccounting Office have measures of total
antibacterial use.
(22) IOM (USA) Endorsed Endorsed (p64) Yes
(31) CDC (USA) Primarily concerned with surveillance, prevention and control of resistance in the US, where regulation of license and promotion alreadyexists. However, does not deal with legislation compelling manufacturers to measure and report sales and consumption data.
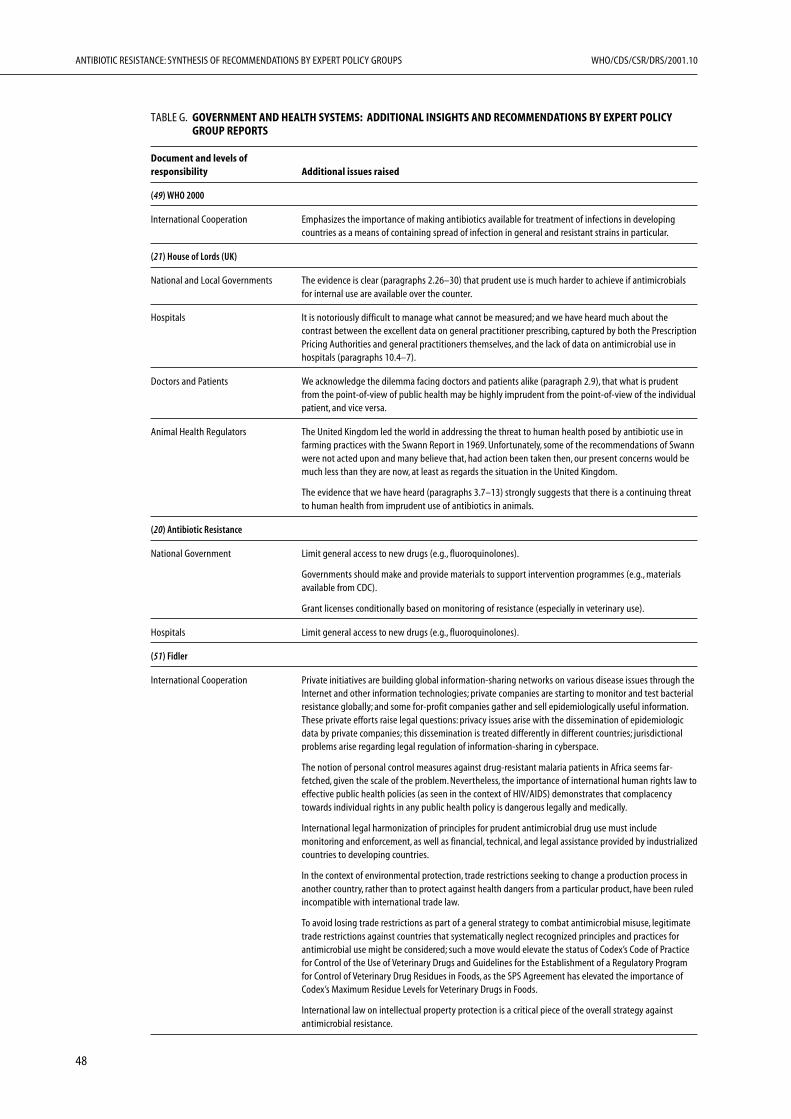
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
48
TABLE G. GOVERNMENT AND HEALTH SYSTEMS: ADDITIONAL INSIGHTS AND RECOMMENDATIONS BY EXPERT POLICYGROUP REPORTS
Document and levels ofresponsibility Additional issues raised
(49) WHO 2000
International Cooperation Emphasizes the importance of making antibiotics available for treatment of infections in developingcountries as a means of containing spread of infection in general and resistant strains in particular.
(21) House of Lords (UK)
National and Local Governments The evidence is clear (paragraphs 2.26–30) that prudent use is much harder to achieve if antimicrobialsfor internal use are available over the counter.
Hospitals It is notoriously difficult to manage what cannot be measured; and we have heard much about thecontrast between the excellent data on general practitioner prescribing, captured by both the PrescriptionPricing Authorities and general practitioners themselves, and the lack of data on antimicrobial use inhospitals (paragraphs 10.4–7).
Doctors and Patients We acknowledge the dilemma facing doctors and patients alike (paragraph 2.9), that what is prudentfrom the point-of-view of public health may be highly imprudent from the point-of-view of the individualpatient, and vice versa.
Animal Health Regulators The United Kingdom led the world in addressing the threat to human health posed by antibiotic use infarming practices with the Swann Report in 1969. Unfortunately, some of the recommendations of Swannwere not acted upon and many believe that, had action been taken then, our present concerns would bemuch less than they are now, at least as regards the situation in the United Kingdom.
The evidence that we have heard (paragraphs 3.7–13) strongly suggests that there is a continuing threatto human health from imprudent use of antibiotics in animals.
(20) Antibiotic Resistance
National Government Limit general access to new drugs (e.g., fluoroquinolones).
Governments should make and provide materials to support intervention programmes (e.g., materialsavailable from CDC).
Grant licenses conditionally based on monitoring of resistance (especially in veterinary use).
Hospitals Limit general access to new drugs (e.g., fluoroquinolones).
(51) Fidler
International Cooperation Private initiatives are building global information-sharing networks on various disease issues through theInternet and other information technologies; private companies are starting to monitor and test bacterialresistance globally; and some for-profit companies gather and sell epidemiologically useful information.These private efforts raise legal questions: privacy issues arise with the dissemination of epidemiologicdata by private companies; this dissemination is treated differently in different countries; jurisdictionalproblems arise regarding legal regulation of information-sharing in cyberspace.
The notion of personal control measures against drug-resistant malaria patients in Africa seems far-fetched, given the scale of the problem. Nevertheless, the importance of international human rights law toeffective public health policies (as seen in the context of HIV/AIDS) demonstrates that complacencytowards individual rights in any public health policy is dangerous legally and medically.
International legal harmonization of principles for prudent antimicrobial drug use must includemonitoring and enforcement, as well as financial, technical, and legal assistance provided by industrializedcountries to developing countries.
In the context of environmental protection, trade restrictions seeking to change a production process inanother country, rather than to protect against health dangers from a particular product, have been ruledincompatible with international trade law.
To avoid losing trade restrictions as part of a general strategy to combat antimicrobial misuse, legitimatetrade restrictions against countries that systematically neglect recognized principles and practices forantimicrobial use might be considered; such a move would elevate the status of Codex’s Code of Practicefor Control of the Use of Veterinary Drugs and Guidelines for the Establishment of a Regulatory Programfor Control of Veterinary Drug Residues in Foods, as the SPS Agreement has elevated the importance ofCodex’s Maximum Residue Levels for Veterinary Drugs in Foods.
International law on intellectual property protection is a critical piece of the overall strategy againstantimicrobial resistance.
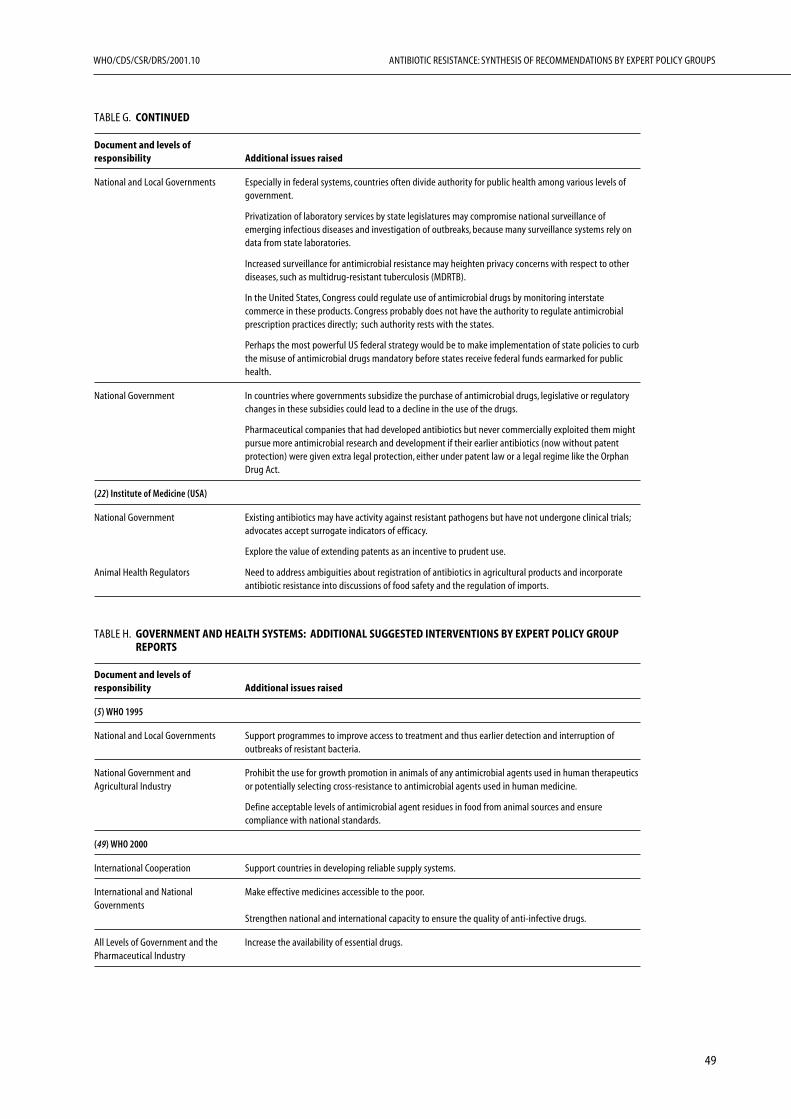
49
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
TABLE G. CONTINUED
Document and levels ofresponsibility Additional issues raised
National and Local Governments Especially in federal systems, countries often divide authority for public health among various levels ofgovernment.
Privatization of laboratory services by state legislatures may compromise national surveillance ofemerging infectious diseases and investigation of outbreaks, because many surveillance systems rely ondata from state laboratories.
Increased surveillance for antimicrobial resistance may heighten privacy concerns with respect to otherdiseases, such as multidrug-resistant tuberculosis (MDRTB).
In the United States, Congress could regulate use of antimicrobial drugs by monitoring interstatecommerce in these products. Congress probably does not have the authority to regulate antimicrobialprescription practices directly; such authority rests with the states.
Perhaps the most powerful US federal strategy would be to make implementation of state policies to curbthe misuse of antimicrobial drugs mandatory before states receive federal funds earmarked for publichealth.
National Government In countries where governments subsidize the purchase of antimicrobial drugs, legislative or regulatorychanges in these subsidies could lead to a decline in the use of the drugs.
Pharmaceutical companies that had developed antibiotics but never commercially exploited them mightpursue more antimicrobial research and development if their earlier antibiotics (now without patentprotection) were given extra legal protection, either under patent law or a legal regime like the OrphanDrug Act.
(22) Institute of Medicine (USA)
National Government Existing antibiotics may have activity against resistant pathogens but have not undergone clinical trials;advocates accept surrogate indicators of efficacy.
Explore the value of extending patents as an incentive to prudent use.
Animal Health Regulators Need to address ambiguities about registration of antibiotics in agricultural products and incorporateantibiotic resistance into discussions of food safety and the regulation of imports.
TABLE H. GOVERNMENT AND HEALTH SYSTEMS: ADDITIONAL SUGGESTED INTERVENTIONS BY EXPERT POLICY GROUPREPORTS
Document and levels ofresponsibility Additional issues raised
(5) WHO 1995
National and Local Governments Support programmes to improve access to treatment and thus earlier detection and interruption ofoutbreaks of resistant bacteria.
National Government and Prohibit the use for growth promotion in animals of any antimicrobial agents used in human therapeuticsAgricultural Industry or potentially selecting cross-resistance to antimicrobial agents used in human medicine.
Define acceptable levels of antimicrobial agent residues in food from animal sources and ensurecompliance with national standards.
(49) WHO 2000
International Cooperation Support countries in developing reliable supply systems.
International and National Make effective medicines accessible to the poor.Governments
Strengthen national and international capacity to ensure the quality of anti-infective drugs.
All Levels of Government and the Increase the availability of essential drugs.Pharmaceutical Industry

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
50
TABLE H. CONTINUED
Document and levels ofresponsibility Additional issues raised
(21) House of Lords (UK)
International Cooperation We commend the Government and the ABPI for their firm stand against over-the-counter antibiotics, andurge them not to give way. Since this is an area of EU responsibility, and the position in several otherMember States appears to be different, we recommend that the Government should engage in activediplomacy to ensure that, should the issue be raised in the Council of Ministers, their position isunderstood and their allies are in place; and, in the long term, to induce those Member States which arecurrently more relaxed about over-the-counter antibiotics to introduce more controls.
National Government The Government and the health authorities must do more to educate the public about the proper use ofantimicrobials. In particular, we recommend a campaign targeted at mothers of young children.
The Education Committee of the General Medical Council and the medical Royal Colleges should reviewthe evidence that undergraduate curricula give insufficient emphasis to infectious diseases andantimicrobial therapy, and the Royal Colleges should increase the attention paid to antimicrobial therapyin their programmes of postgraduate education and vocational training (paragraph 11.6).
The Medicines Control Agency should consider whether the drug licensing system could be used moreeffectively to encourage prudent use in the interest of public health (paragraph 11.9).
The Government should respond positively to the EU proposal for an “orphan drug” regime, and shouldseek to ensure that the scheme gives the pharmaceutical industry a real incentive to work on noveltreatments for problem diseases, particularly diseases of the world’s poor, such as malaria (paragraph11.40).
Local Government The NHS Executive must work towards the goal of compatible and interconnected information technologyfor every general practitioner, every hospital ward and infection control team, and every clinicalmicrobiology laboratory. They must accept the considerable cost involved; and they must give a stronglead from the centre to ensure compatibility (paragraph 11.51).
Hospitals All hospitals should install computer systems for patient-specific prescribing information at ward level.
Doctors We do not recommend that general practitioners should be required to establish antimicrobialsusceptibility before prescribing (paragraph 2.22). This, we believe, would at present be impracticable, andwould overload diagnostic services which are already stretched. But improved access to microbiologicaltesting clearly reduces uncertainty in prescribing.
Veterinarians The veterinary profession must address the use of potent agents important to human medicine (e.g.,fluoroquinolones), by introducing rapidly a Code of Practice on when such compounds should beprescribed (e.g., when other agents have failed) and how (e.g., for no longer than necessary); werecommend self-regulation in preference to legislation.
(1) USA National Institutes of Health
National Government In countries with more restrictive legislation and more effective enforcement of antibiotics prescriptions,studies should be carried out on the effects of such legislation on requirements for training of health-carepersonnel and on economic and other consequences for patients and national health-care deliverysystems.
Legal restrictions on the use of antibacterial drugs may exert positive or negative effects on mortality andmorbidity, especially among children.
National Government and Hospitals Longitudinal studies must determine whether regulations and effective enforcement have any effect onthe emergence of resistance.
National Government and The public health consequences of restrictions on antibacterial use in food production and animalAgricultural Industry husbandry should be investigated.
(6) US Congress Office of Technology Assessment
National Government Congress can provide FDA with authority to negotiate extended market exclusivity to manufacturers thatagree to restrictions on marketing of antibiotics.
Congress could authorize FDA to extend market exclusivity for “off-patent” antibiotics that are effectiveagainst drug resistant bacteria.
Congress could provide research support for a federal programme to conduct clinical trials of antibiotics todetermine if they have uses against antibiotic resistant bacteria.
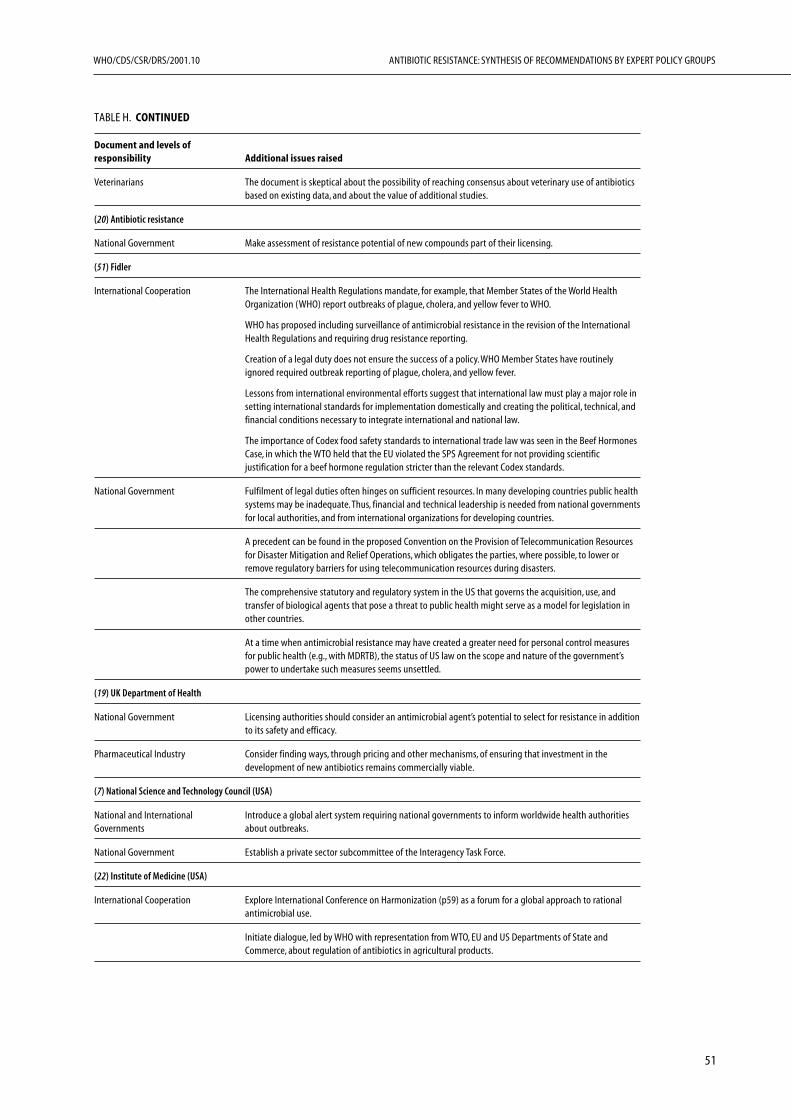
51
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
TABLE H. CONTINUED
Document and levels ofresponsibility Additional issues raised
Veterinarians The document is skeptical about the possibility of reaching consensus about veterinary use of antibioticsbased on existing data, and about the value of additional studies.
(20) Antibiotic resistance
National Government Make assessment of resistance potential of new compounds part of their licensing.
(51) Fidler
International Cooperation The International Health Regulations mandate, for example, that Member States of the World HealthOrganization (WHO) report outbreaks of plague, cholera, and yellow fever to WHO.
WHO has proposed including surveillance of antimicrobial resistance in the revision of the InternationalHealth Regulations and requiring drug resistance reporting.
Creation of a legal duty does not ensure the success of a policy. WHO Member States have routinelyignored required outbreak reporting of plague, cholera, and yellow fever.
Lessons from international environmental efforts suggest that international law must play a major role insetting international standards for implementation domestically and creating the political, technical, andfinancial conditions necessary to integrate international and national law.
The importance of Codex food safety standards to international trade law was seen in the Beef HormonesCase, in which the WTO held that the EU violated the SPS Agreement for not providing scientificjustification for a beef hormone regulation stricter than the relevant Codex standards.
National Government Fulfilment of legal duties often hinges on sufficient resources. In many developing countries public healthsystems may be inadequate. Thus, financial and technical leadership is needed from national governmentsfor local authorities, and from international organizations for developing countries.
A precedent can be found in the proposed Convention on the Provision of Telecommunication Resourcesfor Disaster Mitigation and Relief Operations, which obligates the parties, where possible, to lower orremove regulatory barriers for using telecommunication resources during disasters.
The comprehensive statutory and regulatory system in the US that governs the acquisition, use, andtransfer of biological agents that pose a threat to public health might serve as a model for legislation inother countries.
At a time when antimicrobial resistance may have created a greater need for personal control measuresfor public health (e.g., with MDRTB), the status of US law on the scope and nature of the government’spower to undertake such measures seems unsettled.
(19) UK Department of Health
National Government Licensing authorities should consider an antimicrobial agent’s potential to select for resistance in additionto its safety and efficacy.
Pharmaceutical Industry Consider finding ways, through pricing and other mechanisms, of ensuring that investment in thedevelopment of new antibiotics remains commercially viable.
(7) National Science and Technology Council (USA)
National and International Introduce a global alert system requiring national governments to inform worldwide health authoritiesGovernments about outbreaks.
National Government Establish a private sector subcommittee of the Interagency Task Force.
(22) Institute of Medicine (USA)
International Cooperation Explore International Conference on Harmonization (p59) as a forum for a global approach to rationalantimicrobial use.
Initiate dialogue, led by WHO with representation from WTO, EU and US Departments of State andCommerce, about regulation of antibiotics in agricultural products.


CHAPTER IV
Encourage research and product developmentJohn F. Barrett
and deterioration of public welfare as infectiousdisease concerns continue to increase worldwide(1,5,6,7,8,11,19,20,21,22,39,49,50,53). In addi-tion, many reports address antibiotic resistance inspecific circumstances and microorganisms, and allidentify antibiotic resistance as a growing problem(54–69).
The 1992 Institute for Medicine’s (IOM) reporton “Emerging Infections: Microbial Threats toHealth” (71) indicates that “changes in technologyand industry” are among those risk factors that havecontributed to the inability to prevent or controlmicrobial diseases. This IOM report (70) lists sixgeneral factors leading to the emergence of infec-tious diseases and antimicrobial resistance:
• environmental change and land use;
• breakdown of public interest health measures;
• international travel (transporting infectiousdiseases globally);
• changes in social behaviour;
• changes in technology and industry; and
• microbial adaptation and change (includingresistance development).
The world is no longer simply a matter of geo-graphical division of diseases, as the spread ofinfectious diseases continues to be demonstratedwith the emergence of “developing nation diseases”in specific geographical centres in the industrial-ized world (e.g., tuberculosis, dysentery, etc.).
A practical way to look at emerging diseases isthat a disease in one geographical area could easilybe transmitted to the unaffected area, by simpledelivery of the infectious disease by human carrier.Thus it is naive to believe that antimicrobial resist-ance in any part of the world is an “isolated prob-lem”.
The industrialized countries, by virtue ofadvanced technology and improved basic livingstandards, are privileged to not be subject to themassive outbreaks of infectious diseases that we seein the developing world. Basic sanitation, basic edu-
Abstract
The areas of research and development offertremendous possibilities to have an impact on theantimicrobial resistance crisis worldwide. A histori-cal review of support for antimicrobial resistanceresearch and development, as a subset of infectiousdisease research including tuberculosis research, hasdetermined a gross under-funding of this area, inacademic, governmental and industrial laboratoriesover the past 10–15 years. There is a need toencourage federal, university, and private sector col-laboration in basic and applied research.
Consensus points by governing bodies review-ing antimicrobial resistance over the past five years,consistent with current key-opinion-leader senti-ment, show that the major needs include: basicresearch is needed to delineate the genetic and meta-bolic pathways, microbial physiology, and the causesof antimicrobial resistance; an increase in researchfor the identification and development of new drugsto fight antimicrobial resistance; and an increase inbasic and applied research for new vaccines andother preventive measures.
In broader terms, research and developmentneeds to cover a more global effort to provide com-pelling evidence for the prudent use of antibiotics,including the use in humans, animals and plants;provide incentives for the discovery and develop-ment of agents to combat antimicrobial resistance;facilitate innovative approaches to fight against re-sistance; and build worldwide alliances and part-nerships to increase sensible access to antimicrobials(1,5,6,7,8,11,19,20,21,22,39,49,50,53).
Introduction
There is significant consensus among research pro-fessionals that the US Surgeon General, WilliamStewart, was wrong in 1969 when he was quotedas saying that we (the US population) could“…close the book on infectious diseases…” in ad-dressing public concerns (from a health standpoint).All position-piece documents reviewed for thischapter make observations about the seriousness
53
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
54
cation on maintaining good health, and widespreadimmunization against disease, provides a tremen-dous advantage to the occupants of the industrial-ized world. Short- and long-term gains are a matterof basic education and building a foundation sothe next generation of developing countries’ chil-dren have the same advantages as industrializedcountries’ children in sanitation and health care.However, research and development in the devel-oping countries is virtually non-existent, and theshort-term possibilities for changing this are remote.
This chapter reviews the expert reports (1,5,6,7,8,11,19,20,21,22,39,49,50,53,54) and other rel-evant literature from the viewpoint of research(basic and applied) and product development andattempts to summarize their recommendations.
Basic and applied research
Identification of research needs
All the expert reports reviewed made at least somemention of research and many had extensive sec-tions devoted to research needs both to improvethe understanding and management of antimicro-bial resistance and to develop new drugs, vaccinesand diagnostic tools. Recommendations from Wiseand colleagues in the British Medical Journal’sspecial (1998) issue on antimicrobial resistanceinclude the need for increased understanding of an-timicrobial resistance processes; and for encourage-ment to the pharmaceutical industry to increase itscommitment to antimicrobial research (71,72).Huovinen and Cars (73) emphasize research [bothbasic and applied] as “…a cornerstone in the fightagainst bacterial resistance.” From a better under-standing of the microbiology and genetics of ourendogenous flora, we may better understand thecollateral damage of normal antibiotic usage in fa-cilitating the evolution of resistance and the mecha-nism of transmissibility of resistant bacteria. Moreprudent use of antibiotics will be attained by thedevelopment of diagnostic technologies to enablerapid identification of bacterial versus viral patho-gens.
A synthesis of the key research needs identifiedin the expert reports reviewed (1,5,6,7,8,11,19,20,21,22,39,49,50,53,54) follows:
Infrastructure and training
• Improvement in basic and applied research in-frastructure (academic and industrial);
• Improvement in basic research training inacademia to ensure a critical mass of researchersin the antimicrobial resistance field of research.
Infectious disease and microbial pathogenicity
• Improvement in understanding of how to pre-vent the infectious disease state and to treat newinfectious diseases; basic research related to newand re-emerging pathogens/infections andbetter understanding of the infectious diseaselink to chronic diseases
• Basic research in molecular pathogenesis, includ-ing:— the evolution of pathogenicity;— the epidemiology and spread of pathogens
and infectious disease transmission;
• Resources to enable the sequencing of the entiregenome of additional microbial pathogens(including problem pathogens in developingcountries).
Antimicrobial resistance
• Research into the source of antibiotic resistancegenes; the mechanisms/frequency of ‘reassort-ment’ of these genes, the emergence and trans-fer of resistance genes among pathogens in vivo(in the host), and the distribution and dissemi-nation of specific antimicrobial resistance genesover time, and factors affecting the loss ofresistance determinants;
• Research on the correlations between resistancedeterminants in normal flora and the prevalenceof resistant pathogens;
• A better understanding of the ability of geneticmaterial to transfer in the bacterial ecosystem;
• Studies on the ability of bacteria to amplify genesand exchange genes leading to multiple drugresistance in bacteria;
• Mechanisms of antimicrobial resistance emer-gence, acquisition, spread, persistence, and de-cline of multidrug-resistant microorganisms;
• Research on factors that accelerate the develop-ment of drug resistance and methods to delayor reverse drug resistance;
• The need for more research examining ways todecrease resistance frequency.
55
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
New technologies
• Provide technologies to researchers to allow forthe identification of quality, novel targets;
• Develop tools such as microbial genomesequence data, comparative genomics, DNAchip technology, and bioinformatics;
• Research in molecular genetics to identify noveltargets.
New antimicrobials, vaccines, disease prevention anddiagnostics
• Provide opportunities to translate basic researchfindings into applied, medically useful products/devices/technologies (i.e., drugs, diagnostics,vaccines, and other tools to inhibit antimicro-bial resistance);
• Research the role of host factors and immuno-modulation in clinical resistance and the humanimmune response to infectious diseases;
• Basic research towards the development ofeffective vaccines;
• Research of development of vector controlinterventions;
• Basic research on other disease preventativemeasures;
• Support of research and development and stand-ardization of diagnostic tests;
• Research to discover/design/develop more reli-able, rapid diagnostic techniques for identifica-tion of infections causing specific disease states;
• Increased research into methods to detect resist-ance to antimicrobial agents;
• Tools for the clinical/epidemiological researcherthat can be used to more accurately and effi-ciently identify optimal therapeutic options fortreatment of antibiotic resistant strains.
Research on antimicrobial use
• Links between prescribing and resistance at boththe individual and population levels;
• Concepts concerning antibiotic use and theirinfluence on delivery and compliance;
• Factors leading to inappropriate prescribing;
• An understanding of variation in antimicrobialuse patterns that affect emergence and spread ofresistance;
• Effect of preventative, therapeutic and growth-promoting agents used in the animal use fieldon the community microbiota.
Surveillance and information management
• Research to improve of surveillance tools, includ-ing computer programmes for data managementand reporting;
• Research in methods for monitoring drug resist-ance;
• Development and assessment of computerizeddecision-support systems in hospitals;
• Encourage sharing of antimicrobial resistancedata between industry, universities, and govern-mental authorities.
Additional research areas to consider
Understanding the costs of resistance
a) to the bacterium
One of the major research areas only minimallytouched on in the reports reviewed was that of thecost of resistance to the bacterium (1,74). Theunderstanding of the cost to the bacterium thatreceives or adapts to the resistant state is betterunderstood in terms of the change in pathogenic-ity as the ‘expense’ of increased resistance. Wherepreviously, resistance acquisition was viewed as acrippling event, it is now understood that it mayactually confer a selective advantage to the patho-gen (74).
b) costs to the health care system
A new field of marketing research and businessmanagement has arisen over the past years dealingwith the pharmacoeconomics of health care (75),in which factors indirectly related to outcomes maybe drawn into the value of one action over the other.For example, the ‘cost’ of antimicrobial resistancein the patient population may take into accountloss of work time, allowing a quantitative assess-ment of the ‘cost’ of infection beyond the drug costsalone. If a treatment regimen gets the patient outof the hospital on oral medication, rather than con-tinuation of therapy by intravenous administration,then the ‘cost’ of therapy overall, in terms of meas-uring the ‘cost’ of antimicrobial resistance, mayfactor in the absence of 2–5 additional hospital days(that may range from $1500–$2500 per day). Eventhe selection of the ‘right’ first-line antibiotic the

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
56
first time by the practicing physician, versus requir-ing a follow-up visit because the ‘older’ or genericantibiotic (with cost saving) did not work, has a‘cost’ associated with the patient’s return to thephysician, as well as the cost to the physician. Oneof the criticisms of the for-profit-managed healthcare delivery systems may be that by providing anallotment of dollars per patient per year to the phy-sician by contact regardless of the true cost, pushesthe physician to cost-cutting methods (includingthe choice of an inappropriate antibiotic).
Areas where there is lack of consensus
There is no consensus as to the cause, effect, orsolution to the worldwide antimicrobial resistanceproblem, nor as to the origin of antimicrobial re-sistance genes. However, it is clear that antimicro-bial resistance stems from the use of antibiotics.While there is no high-level disagreement aboutthe unmet medical need posed by antimicrobialresistance, there are differences in opinion vis-a-visthe scientific priorities.
Not surprisingly, there is no consensus as to thespecific ‘cause-and-effect’ and assignment of ‘blame’on the increase in antimicrobial resistance (1,5,6,7,8,11,19,20,21,22,39,49,50,53,54,60–69); morebasic and applied research is needed to answer thiscomplex question definitively. However, it is clearto virtually all opinion leaders that antimicrobialresistance begins with the routine use of antibiot-ics for human health care, animal health, and agri-cultural purposes. There is most probably a link tothe resistance emergence to the most frequentlyprescribed antibiotics and the alarming increase inresistant bacteria (11). For example, greater than90% of Staphylococcus aureus were resistant to peni-cillin and other β-lactams as of 1994, and there isan notable increase in vancomycin resistance inenterococci. Likewise, but of unknown clinical rel-evance, there is an increase in the resistance topenicillins by Streptococcus pneumoniae.
Concerning resistance and selective pressure,there is not consensus among scientists as towhether removal of an antibiotic from the treat-ment regimen will: reduce the risk and/or expan-sion of resistance in the pathogen population;reverse the resistance frequency or prevalence in thebacterial population; or have no effect on the re-sistance frequency. In the House of Lords report(21) Reeves is quoted as stating “There is plenty ofevidence, that if you remove the selection pressure,the organisms will slowly revert [to susceptible]….”,
whereas Davey provided evidence directly linkingresistance to overall usage. In contrast to Reeves,Levin was quoted (21) that resistance is a one-waystreet, that if antibiotic use is cut back sharply, theproportion of resistant strains wanes slowly (if atall).
Effective efforts
The review of the expert reports seems to indicatethe effectiveness of basic research in increasing ourunderstanding of antibiotic resistance and the de-velopment of new drugs. Extensive research effortsin academia continue, albeit dwarfed by supportto AIDS research, and have yielded excellent re-sults from a better understanding of the molecularmechanisms responsible for antibacterial resistance,(72, and references cited therein) to new medicinalchemistry approaches to combat resistance in bac-teria (76, and references cited therein). Historically,basic research has provided numerous advance-ments in understanding of microbes which has beenapplied to the engineering of drugs by pharmaceu-tical companies.
Ineffective efforts
Many of the US reports indicate funding (that isUS-based) is woefully lacking for basic and appliedresearch concerning antimicrobial resistance. Aspathogens can vary greatly in industrialized versusdeveloping countries (77), the priorities of ‘medi-cal need’ are often misaligned. Priorities for fund-ing have shifted away from bacteria-associatedresearch to AIDS research over the past fifteen years.The lone exception appears to be the increase inTB research support (although this is still dispro-portionately small considering the worldwide mor-bidity and mortality due to TB).
Research and development efforts to providecompelling support for the ‘prudent’ use of antibi-otics have failed to translate into prudent use;Reducing inappropriate use of antibiotics with sup-portive basic and applied research (1,50,39,78,79)has proved ineffective.
A critical role for new technologies
There is consensus (1,5,6,7,8,11,19,20,21,22,39,49,50,53,54) that the molecular detection ofgenes that are associated with antimicrobial resist-ance is expected to be ascertained by the analysesof microbial genomes (22). The principles and

57
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
implications of mapping the prokaryotic genome(s)are to acquire the full sequence of microbial genesand to manage great volumes of sequence datathrough bioinformatics. It is hoped that once this‘raw’ data is collected in analysable form (hence the‘informatics’ in bioinformatics), this ‘knowledge’(as opposed to raw data) will provide a foundationfor the discovery and development of new antimi-crobial agents, new vaccines, and new diagnostictools for infectious diseases.
Consensus throughout the documents (1,5,6,7,8,11,19,20,21,22,39,49,50,53,54) holds that com-parative genomics (i.e., the ability to compare fulllength sequences of different bacterial, or eveneukaryotic, genomes) may present the opportunityfor the informatic-assignment of ‘putative’ essen-tial function in microbes based on consistency ofsequence similarity, but wet-biology proof is neededto confirm this informatics assignment. The bestexample of successful gene sequencing/bio-informatics may be The Institute for GenomicResearch (TIGR), with the intention to sequence50–100 microbial genomes within just a few years.But beyond the cataloging of raw sequences, TIGRand other groups are developing gene array tech-nology that will allow for the simultaneous assess-ment of expression of all genes in a microbe underdifferent environmental conditions (growth con-dition changes, stress, antibiotic insult, etc.).Among the data expected to be ascertained are: 1)the identification of genes involved in susceptibil-ity or resistance to antimicrobial agents; 2) specificknowledge of gene function, including regulatoryfunctions of different genes; 3) the identificationof polymorphism shifts signaling the evolution ofinfectivity (virulence) and/or susceptibility/resist-ance to antimicrobials; and 4) the identification ofpotential antigens/proteins against which vaccinesmay be devised (22).
The genetic basis of resistance in bacteria maysupersede the phenotypic (macro-) detection ofresistances, frequently based on microbiologicalsusceptibilities (minimal inhibitory concentrations,etc.). Undertaking the identification of the geno-typic cause for changes in susceptibility mayprovide insight into the development of novelapproaches to combat resistance. A shortcomingof genotypic characterization of resistance factorsis that it provides but a ‘snapshot’ of genotypic char-acter; it gives a single time point of ‘data’, but notnecessarily a proven link to the resistance pattern,or an understanding of antimicrobial resistance. Amatch of both genotypic and phenotypic data is
most probably the best approach and will mostlikely provide the greatest opportunities for ad-vancements in the short-term. The expanded andcoordinated use of resistance surveillance systemssuch as SENTRY or the Alexander Project (80,81)would provide ‘live’ tracking of antimicrobial re-sistance, allowing action to be taken as appropriateto contain antimicrobial resistance, as well as pre-dict emerging deleterious trends or appearance ofemerging pathogen susceptibility problems.
There is agreement (1,5 ,6,7,8,11,19,20,21,22,39,49,50,53,54) that practical applications arisingfrom genomic analyses and bioinformatic tallying/annotation of sequence function of microbialgenomes may be limited only by the imaginationof the researcher. From these analyses a selection ofhigh quality novel targets is expected to emerge,allowing the applied research groups to select anyof the following subsets of data: 1) essential genes;2) virulence/pathogenicity genes (non-essentialgenes); 3) broad spectrum genes (gram-positive andgram-negative); 4) narrow spectrum genes (gram-positive or gram-negative); and 5) targeted spec-trum genes (i.e., Mycobacterium tuberculosis,Chlamydia pneumoniae). In addition, selectivityand specificity may be ascertained by comparativegenomic analyses, such as comparison to eukaryoticsequences, to determine minimal sequence overlapas a surrogate “in silico” indication of selectivityfor the microbial target (i.e. decrease in toxicity)(22).
Additionally, molecular technologies can andhave been employed downstream to identify “insilico” essentiality of genes, and subsequently provenby so-called “knock-out” approaches in which theselective inhibition of expression of individual genesand monitoring of survival and/or growth of theknock-outs, is a surrogate of ‘essential function’ invitro (albeit negative selection data-based). Alter-natively, genomic footprinting methodologies andtemperature-sensitive mutants also provide surro-gate assays for ‘essentiality’ determination in bac-teria.
Consensus throughout the documents (1,5,6,7,8,11,19,20,21,22,39,49,50,53,54,55) holds thattaking genomic sequence information to practicalapplication of screen design has provided a varietyof high-throughput screening assay formats includ-ing cell-free biochemical or genetic assays, assaysbased on phenotypic changes, binding assays,enzymatic assays, etc. Genetic technologies mayultimately allow multiplexing of prokaryotic tar-gets, which in turn may increase the chances of

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
58
success and decrease overall research and develop-ment costs (22). Thus these new technologies areseen to play a critical role in future discoveryefforts for new antimicrobials.
Funding for research
The estimate for infectious disease deaths through-out the world in 1998 was over 13 million (54) oralmost a quarter of all deaths worldwide. Of thesedeaths, 3.5 million were due to pneumonia, 2.2million to diarrhoeal disease, 1.5 million to M.tuberculosis, 2.3 million to AIDS, 1.1 million tomalaria, and 1 million to measles (54). The firstthree of these diseases, totaling 7.2 million deaths,were the top infectious disease killers as well as theoverall top three causes of deaths worldwide in 1900(54), indicating little impact of research and devel-opment on reducing this infectious diseaseburden.The current estimate is that less than 2%of the total health research expenditures through-out the world is devoted to antimicrobial usage,delivery, and resistance (49). To quote from theWHO report (49): “Incentives are needed to en-courage pharmaceutical companies to discover anddevelop new compounds, as well as intensify re-search into dosage regimens calculated to minimizethe likelihood of selecting for resistance.”
US funding of infectious disease, AIDS, andtuberculosis research
The priorities for research in the United States canbe clearly identified in a review of funding amountsfrom 1993 through 2001 (estimated), in which overan 8-year period the total research budget doubledfrom $9.765 billion (1993) to $18,812 billion(2001, estimated). The AIDS research portion ofthis budget increased by 1.97-fold increase in fund-ing support. Infectious disease research (other thanAIDS and TB) received a 1.97-fold increase andTB research increased from $35 million (1993) to$86.8 million (2001, estimated), or a 2.48-foldincrease in the research funding. Although the TBresearch budget represents a disproportionate in-crease in funding, it is in turn disproportionatelyless than that for AIDS research (82,83). From the1995 CISET report (7), funding of work relatedto infectious diseases other than AIDS or TB wasc.5% of total research funding; the Centers forDisease Control and Prevention (CDC) dedicatedc.95% of its budget for prevention and control ofinfectious diseases to AIDS, TB, sexually transmit-
ted diseases and vaccine-preventable diseases (7).
Product development—antibiotics,vaccines and diagnostics
Antibiotics
The UK Standing Medical Advisory Committeewas commissioned to examine the issue of antimi-crobial resistance in relation to clinical prescribingpractices (19). Their mission was to examine allfactors that may contribute to antimicrobial resist-ance, including the role of research. From this re-port, one very relevant observation is made: “Thethrust of this report is focused on the conservationof present antimicrobial agents. However, it mustbe recognized that the way in which past resistanceproblems have been overcome (if only temporar-ily) has been by the development of new agents.”
The “Report of the ASM Task Force on Antibi-otic Resistance” (8), based on the workshop on“Antibiotic Resistance: Current Status and Futuredirections” held in 1994, drew consensus from agroup of almost three dozen scientists fromacademia, government and industry. It states: “Therelative utility of antibiotics is eroding, tipping thebalance in favor of multidrug-resistant pathogens,and there appears to be few new drugs in the pipe-lines of the USA pharmaceutical companies. Thesedevelopments amount to an incipient public healthemergency, albeit one that is poorly appreciated orrecognized” (8).
Also from the Task Force report (8), “…it shouldbe realized that the research-intensive pharmaceu-tical industry is the source for most new drugs andthat industries need to profit from their investmentsin order to pay for the research.” As marketing pro-jections are primarily based on historical usage, theymay be misleading. Marketing and businessspecialists in industry should be involved in dis-cussions on the problems of emerging antibioticresistance (8). In addition, as cost can drive pre-scription use, the national and regional health careproviders/payers should be involved in the consid-eration of use of antibiotics, balancing the use ofantibiotics and risk of emergence of resistanceagainst cost in the selection of appropriate type anduse of antibiotics. In exchange for the rational mar-ket-support approach for selling products, indus-try should help support national efforts for theprudent use of antibiotics (8). In addition, the po-tential association of infectious diseases (includingbacterial infection) with chronic diseases needs tobe better understood (82), and this will require an

59
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
immense, long-term, research investment. Overall,research has been found to be ‘cost effective’ (11).
This section contains a synthesis of the manysuggestions and recommendations for product de-velopment that came from the reports cited in thereferences. A summary is given at the end of thesection.
Industry engagement
Industrial infectious disease research remains a puz-zle. Clearly in the 1970s and 1980s major compa-nies decreased support for their infectious diseaseefforts (84,85), especially antibacterials, with theunderstanding that the antibacterial needs werediminished, but the reality is that pharmaceuticalcompanies have continued to support to some de-gree infectious disease, moving towards antiviral andin some cases antifungal research efforts, but notto the same extent as the increases in non-infec-tious disease research areas such as cardiovascular,CNS, lipid disorders, oncology, dermatology, etc.The success rate for antibacterial discovery anddevelopment, much diminished since the ‘hey days’of the 1960s–1970s, continues to pose a “value risk”for industry (21). There is, however, no shortageof good ideas (84,86,87).
The UK Standing Medical Advisory Commit-tee (SMAC) report (19) notes that: “It is also rec-ognized that over recent years the pharmaceuticalindustry has developed vastly more efficient sys-tems for seeking new antimicrobial agents. Thesestrategies will, hopefully, yield new generations ofantimicrobial agents by the end of the next dec-ade.” According to the report (19), developmentof a new antimicrobial agent costs about $500 mil-lion (£350 million), over an estimated 7–10 yearperiod (within a 17–20 year window of patent life,depending on country of filing). The costs, togetherwith an understanding that these agents will be usedfor a relatively short period of time in a therapeuticarea subject to the development of resistance andhigh competition, it is easy to see why pharmaceu-tical companies may elect to invest in research inother therapeutic areas (84,85).
A survey of the public domain reports (seeTable 1), databases and literature by this authorindicates major efforts by large pharmaceutical com-panies, start-up biotechnology-based pharmaceu-tical companies, and many smaller start-upinitiatives, directed towards antibacterial resistanceproblems. But with success being harder to comeby and with very few new antimicrobial agents
reaching the market, the perception of lack-of-effort is apparent.
TABLE 1
Company Research area(s)
Abbott Labs Antibacterials/genomics
Astra-Zeneca Antibacterials/antifungals/genomics
Bristol-Myers Squibb Antibacterials/antifungals/genomics
Cubist Pharmaceuticals Antibacterials/genomics
Eli Lilly Antibacterials/antifungals
Glaxo-Wellcome1 Antibacterials/antifungals/genomics
Johnson & Johnson Antibacterials/antifungals
Merck Antibacterials/antifungals
Microcide Pharmaceuticals Antibacterials/antifungals/genomics
Pfizer Pharmaceuticals2 Antibacterials/antifungals/genomics
Schering-Plough Antibacterials/antifungals/genomics
SmithKline-Beecham Antibacterials/genomics
1 Now one research unit.2 Through strategic external aliances
The decrease in industrial support may be re-vealed by the number of commercial InvestigationalNew Drug (IND) submissions in infectious dis-eases from 1991 to 1999, dropping from 327(1991) to 265 (1995) to 52 (1999) (82,83). At theequivalent interval of 9 years (but shifted backwardsin real time due to unavailability of more currentdata), overall funding for research (all therapeuticareas) by industry increased at a rate more than 50%higher than that of government funding for re-search, with industry support rising from $6.19billion (1986) to $18.65 billion (1995) (82,83).However, this increase does not reflect a commit-ment to infectious disease, but rather an increasein funding in the chronic disease areas, with anemphasis on non-infectious disease research.
As most INDs submitted for infectious diseasesare not for individual, novel chemical entities, anexamination of the serious downtrend in industrialsupport for infectious diseases can be seen in thecomparison of New Molecular Entity (NME) sub-missions in the FDA Division of Anti-InfectiveDrug Products, indicating a decreasing trend in thedeliverability of novel agents (82,83). The NMEapprovals in the years from 1991 to 1999 are sum-marized in Table 2. NMEs dropped from 4–6 peryear in the early 1990s to just 1 per year in the late
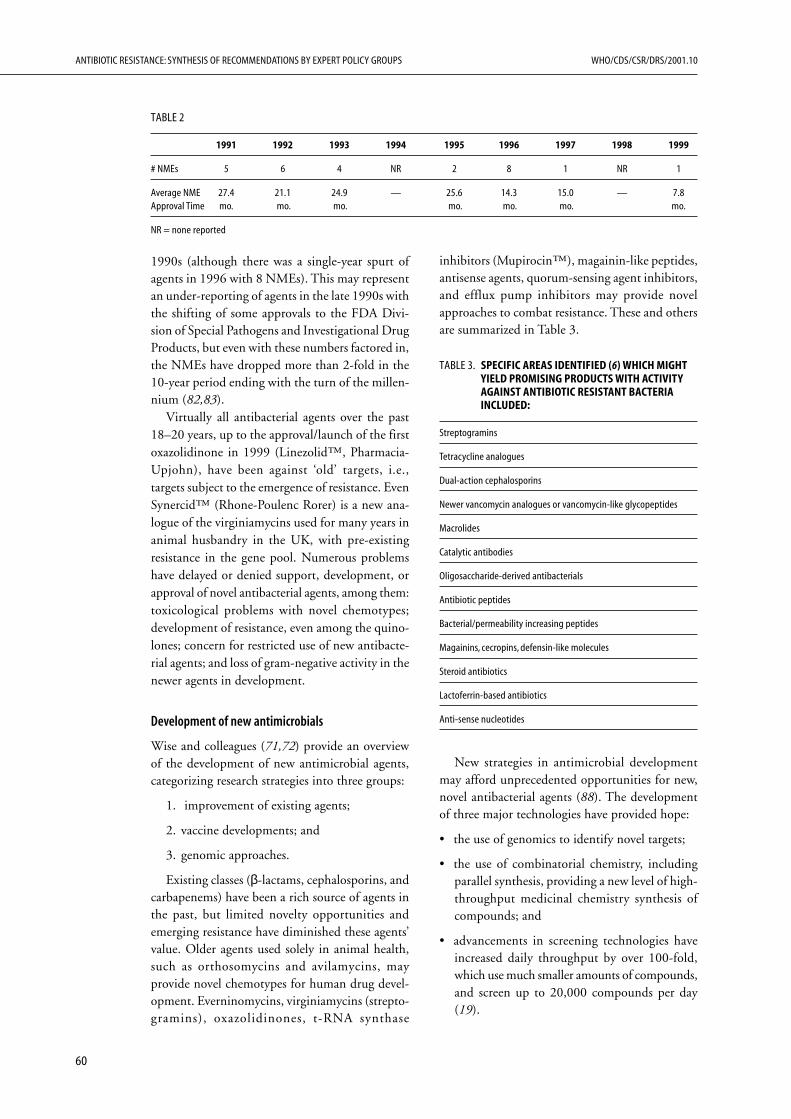
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
60
1990s (although there was a single-year spurt ofagents in 1996 with 8 NMEs). This may representan under-reporting of agents in the late 1990s withthe shifting of some approvals to the FDA Divi-sion of Special Pathogens and Investigational DrugProducts, but even with these numbers factored in,the NMEs have dropped more than 2-fold in the10-year period ending with the turn of the millen-nium (82,83).
Virtually all antibacterial agents over the past18–20 years, up to the approval/launch of the firstoxazolidinone in 1999 (Linezolid™, Pharmacia-Upjohn), have been against ‘old’ targets, i.e.,targets subject to the emergence of resistance. EvenSynercid™ (Rhone-Poulenc Rorer) is a new ana-logue of the virginiamycins used for many years inanimal husbandry in the UK, with pre-existingresistance in the gene pool. Numerous problemshave delayed or denied support, development, orapproval of novel antibacterial agents, among them:toxicological problems with novel chemotypes;development of resistance, even among the quino-lones; concern for restricted use of new antibacte-rial agents; and loss of gram-negative activity in thenewer agents in development.
Development of new antimicrobials
Wise and colleagues (71,72) provide an overviewof the development of new antimicrobial agents,categorizing research strategies into three groups:
1. improvement of existing agents;
2. vaccine developments; and
3. genomic approaches.
Existing classes (β-lactams, cephalosporins, andcarbapenems) have been a rich source of agents inthe past, but limited novelty opportunities andemerging resistance have diminished these agents’value. Older agents used solely in animal health,such as orthosomycins and avilamycins, mayprovide novel chemotypes for human drug devel-opment. Everninomycins, virginiamycins (strepto-gramins), oxazolidinones, t-RNA synthase
inhibitors (Mupirocin™), magainin-like peptides,antisense agents, quorum-sensing agent inhibitors,and efflux pump inhibitors may provide novelapproaches to combat resistance. These and othersare summarized in Table 3.
TABLE 3. SPECIFIC AREAS IDENTIFIED (6) WHICH MIGHTYIELD PROMISING PRODUCTS WITH ACTIVITYAGAINST ANTIBIOTIC RESISTANT BACTERIAINCLUDED:
Streptogramins
Tetracycline analogues
Dual-action cephalosporins
Newer vancomycin analogues or vancomycin-like glycopeptides
Macrolides
Catalytic antibodies
Oligosaccharide-derived antibacterials
Antibiotic peptides
Bacterial/permeability increasing peptides
Magainins, cecropins, defensin-like molecules
Steroid antibiotics
Lactoferrin-based antibiotics
Anti-sense nucleotides
New strategies in antimicrobial developmentmay afford unprecedented opportunities for new,novel antibacterial agents (88). The developmentof three major technologies have provided hope:
• the use of genomics to identify novel targets;
• the use of combinatorial chemistry, includingparallel synthesis, providing a new level of high-throughput medicinal chemistry synthesis ofcompounds; and
• advancements in screening technologies haveincreased daily throughput by over 100-fold,which use much smaller amounts of compounds,and screen up to 20,000 compounds per day(19).
TABLE 2
1991 1992 1993 1994 1995 1996 1997 1998 1999
# NMEs 5 6 4 NR 2 8 1 NR 1
Average NME 27.4 21.1 24.9 — 25.6 14.3 15.0 — 7.8Approval Time mo. mo. mo. mo. mo. mo. mo.
NR = none reported

61
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Partnerships and incentives for development of newantimicrobials
The Office of Technology Assessment (OTA) re-port (6), concerning research and development andits impact on antimicrobial resistance, suggestedseveral options for encouraging the developmentof new antibiotics; among them was a common-theme found in many of the other reports i.e., theneed for cooperative research among the govern-ment regulatory bodies, academia, and industry (6).
In the SMAC report (19), the following incen-tive recommendation is made to increase the phar-maceutical company support in a competitive andprofit-limited ‘competitive’ market: “One possibleway forward, balancing the need for continued in-novation with that of drug conservation, lies in thetrade-off between extended patent life and increasedrestriction.”
Vaccines
“Vaccination is one of the safest and most cost-effective ways of preventing disease” (19).
Vaccines may represent the best chance for tar-geted coverage of a pathogen, although “resistance”to a vaccine may also be unavoidable if variants ofthe pathogen emerge which are not covered by thevaccine. McKeller et al. (89) suggest that the use ofvaccines rather than prophylactic use of antibioticsshould be the norm in infection management inanimal health.
Vaccines may pose the most straightforwardoption for long-term solutions to the resistanceproblem e.g., for meningitis (pneumococcal,Haemophilus influenzae or Neisseria) (6,21,90).However, scientific feasibility, production capacity,delivery infrastructure, social compliance, politicalpressures, and cost constraints are not always easilymanaged in industrial countries, let alone develop-ing countries (6,21,90).There are a number ofimportant issues to deal with in developing a vac-cine i.e.:
• Selection of disease states, microorganisms totarget (geographical, patient population differ-ences such as age, gender, culture);
• Risk versus benefit;
• Efficacy (different efficacies and length of pro-tection);
• Antigenic variation of pathogens (that reduce theefficacy of the vaccine);
• Use of therapeutic vaccines;
• Choice in industrialized versus developing worldvaccine targets;
• Delivery of a vaccination programme to devel-oping world needs.
Also vaccination against a pathogen that is alsoa member of the normal commensal flora (e.g.,Escherichia coli, enterococci, etc.) may be problem-atic or deleterious for the host.
Worldwide medical needs for bacterial vaccinesare summarised in Table 4 (6,21).
TABLE 4
Bacteria Infection
Neisseria meningitidis Meningococcal infection(serotype B)
Mycobacterium tuberculosis Tuberculosis
Streptoccoccus pneumoniae Pneumonia for children under12 years of age
MRSA Systemic infections; endocarditis
Vancomycin-resistant Systemic infections; endocarditisenterococci
Neisseria gonorrhoeae STDs
Staphylococcus species Skin and soft tissue infections; Upperrespiratory, including sinusitus
Helicobacter pylori GI diseases (ulcer)
Group A streptococci Pharyngitis
Clostridium difficile Colitis
Shigella flexneri Gastrointestinal dysentery
Pseudomonas aeruginosa Respiratory (cystis fibrosis);burn wounds
Chlamydia STDs; coronary artery disease
The National Institute for Biological Standardsand Controls cited in (21) suggested that muchmore needs to be done about vaccine research anddevelopment, especially aspects of research in im-munology, microbial genetics, epidemiology, andpathogenesis. In addition, issues surrounding theformulation and delivery of vaccines are in need ofmajor initiatives worldwide.
Diagnostics
The delay in the diagnosis of a specific pathogen inan infectious state may be the major reason for so-called “empirical use” of antibiotics and increasesthe risk of inappropriate use. As the typical anti-

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
62
microbial susceptibility testing takes ≥48 hours, theoverall process from first contact with medical careto delivery of a specific diagnostic report (21) maybe longer.
Among the new technology detection systemsfor rapid diagnosis of bacterial pathogens and re-sistance are (6):
• DNA probe assays.
• Target amplification methods.
• Enzymatic tests for specifically detecting resist-ance (i.e., β-lactamases).
• Tests based on indicator dyes or light-produc-ing enzymes.
• DNA-based methods for testing antibiotic re-sistance.
Whereas rapid and reproducible bacterial iden-tification in the clinic may become reality in thefuture, the estimates are minimally 5–10 years out,and most probably much longer when one consid-ers the standardization issues, technology limita-tions, scale-up issues, cost constraints, politics, andlegal issues (risk of putative action for making thewrong call). Genotypic testing, in which polymerasechain reaction (PCR) technology is used to amplifyas little as a single bacterium’s DNA (in vitro), may betechnically feasible but the scale-up and applicationin the clinic will be a major undertaking. Most im-portantly, the identification of a microorganism bythis technique in the patient may not always signala causal relationship to the infection.
Novel interventions
Levy (91) encourages the prudent use of antibiot-ics and for us to stop trying “…to sterilize our en-vironment.” Levy argues that we need to reviewhow antibiotics are used and where resistant strainsreside, since resistance is mobile from country tocountry. We need to examine the “ecology” of theresistance, as this may tell us where the future re-sistance may occur from selective pressures. Lastly,the indiscriminate use of disinfectants designed to“…indiscriminately destroy bacteria…” rather thanreserving the arsenal for a defensive approach,diminishes our capacity and capability to act whenhuman health is threatened by multidrug-resistantpathogens (91).
A new approach to combating antimicrobialresistance has emerged in which relevant humanhost factors are identified and stimulated, especially
at the first site of pathogen attack, the epithelialsurface. Study of the intrinsic resistance of oral-nasal-pulmonary sites, gastrointestinal sites, andgenitourinary sites may provide opportunities forhost-facilitated resistance to microbial invaders. Thelink of pathogenesis and immunological responseto microbial insult is a new field of study (beyondthe many years of vaccine development), and mayprovide an “immunoprotective” approach to com-bating antimicrobial resistance (22).
Summary of recommendations forresearch and development
The generalized strategies from the USAID Report(39) with five key recommendations, the Epiloguefrom the Task Force on “Antimicrobial Use andResistance Worldwide” (1) with eleven recommen-dations, and the 1999 WHO report (50) witheleven key recommendations, and the recommen-dations of other expert groups can be summarizedand focused towards industrialized and developingcountries as follows:
Industrialized countries
• Fund basic and applied research in academia,government and industry to better understandall relevant aspects of antimicrobial resistance(genetic, epidemiological, mechanisms, transferof genetic material, etc.) and to ascertain short-term gains to combat the ongoing threat of anti-microbial resistance. Support surveillance ofantimicrobial resistance as a research tool, andlink the data from surveillance to action inresponse to the data (i.e., update old productlabelling for pathogen/indication coverage forolder antimicrobial agents that may be contrib-uting to antimicrobial resistance by inappropri-ate use).
• Provide incentives to industry to address unmetmedical needs and provide new antibacterials tocombat antimicrobial resistance worldwide inthe short term, while encouraging partnershipsbetween industry, academia and government tobetter exploit existing and new technologies tocombat antimicrobial resistance (drugs, vaccines,diagnostics). Remove ‘anti-trust’ risk of havingindustry collaborate on antimicrobial resistance.Provide intellectual property protection rightsand enforcement to encourage industry to in-vest in antibiotic research and development indeveloping countries.

63
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
• Where industrial concerns elect to “pass” on in-fectious disease opportunities, provide a mecha-nism for a government or not-for-profitleadership/risk in development of an essentialinfectious disease therapy product (such asvaccine or drug or diagnostic test); in a reversestrategy of industry licensing-in from academia,rather establish the option for the reverse proc-ess (license from the industrial concerns) tooccur.
• Ramp-up applied research, pairing pre-clinicaland clinical research to better assess the correla-tion between in vitro antimicrobial resistance andclinical efficacy of drugs, and the links betweenthe bacterial infectious state and chronic diseases.
• Provide sound experimental support for therational and prudent use of antibiotics, in par-ticular:
— Engage in clinical data-proven epidemiologi-cal outcomes research to determine meth-odology to decrease antimicrobial resistanceby improvement in best practices for antibi-otic use.
— Demonstrate proof of concept of using themost active (and safe) appropriate anti-bacterial regardless of cost, rather than thehistorical or least expensive agent;
— Explore clinical usage of ‘resistance suppres-sive’ agents (agents with decreased resistancedevelopment) such as the new quinoloneantibacterial agents with the C8-methoxysubstituent, and other chemotype anti-bacterials or anti-resistance agents if clinicaldata supports in-vitro data;
— Explore the use of adjunct therapy with“non-antibiotics”, similar to β-lactamase in-hibitors, to control or reverse antimicrobialresistance (e.g., efflux inhibitors);
— Stop using ‘old’ antibacterials with pooractivity and efficacy and adopt more appro-priate therapeutic agents (regardless of cost).This can be accomplished by the use of sur-veillance of antimicrobial resistance to guideappropriate therapeutic decisions;
— Examine pharmacokinetics, pharmacody-namics, and dosage regimens of antibioticsin relationship to resistance emergence prob-ability;
— Recognize that the “prudent use of antibiot-ics” is not synonymous with “restriction ofantibiotic use” in man.
— Address the use of antibiotics in agriculturaland animal husbandry/feed (growth promot-ers) and act appropriately on the basis ofdefinitive data/conclusions.
• Ramp-up basic research to provide for the ex-ploitation of new technologies to capitalize onthe genomic revolution. Exploit genomic infor-mation in its basic form to turn ‘data’ into‘knowledge’ and extract information for newtargets, new opportunities for vaccines, newopportunities for diagnostics, new insights intomolecular mechanisms of antimicrobial resist-ance, and to identify up-and-coming antimicro-bial resistance problems
Developing countries
• Identify and implement plans to identify solu-tions to major impact diseases in developingcountries providing new therapeutic interven-tion options.
• Fund basic and applied research in academia,government and industry to better understandall relevant aspects of antimicrobial resistance inthe developing world and provide research anddevelopment support for successful delivery oftreatment regimens to developing countries thatdo not have the infrastructure to do so them-selves by innovative approaches to treatmentoptions.
• Invest in improving the quality of life and healthoverall, thus decreasing the risk of spreading in-fectious disease. Invest in local research and de-velopment to specifically address antimicrobialresistance problems and solutions.
• Invest in education about the appropriate treat-ment regimen (preventative measures, drugtherapy, vaccines); provide support to invest indeveloping world diseases (even developmentswithout industrial country ‘value’); assist in im-plementation of preventive strategies throughimproving social infrastructure, sanitation, andwater supply systems. Provide education aboutthe relevance of surveillance that may be em-ployed to implement appropriate antibiotictreatment regimens. Invest in education to pro-vide a framework for future research and devel-opment in developing countries themselves.
• Help provide developing countries the sameopportunity to build a quality infrastructure toaddress health needs in the long term, includ-

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
64
ing self-investment in research and development,through sharing of resources with developingcountries.
• Invest in a vaccine strategy to combat antimi-crobial resistance by preventing infectious dis-eases in man from vaccine-preventable diseasesworldwide. Consider combining genetically-en-gineered vaccines and food stuffs as a deliverysystem for both food and vaccines (i.e., engi-neer specific antigens into the potato or riceplant).
• Remove governmental control/blockage fromefforts to address antimicrobial resistance world-wide.
Conclusion
The need for basic and applied research and fornew product development is recognized through-out the literature reviewed. The introduction of newtechnologies in drug discovery provide hope for thefuture but the lack of research support for non-AIDS infectious disease research, especially TB re-search and other unmet medical needs in thedeveloping world, remains a serious limitation toglobal solutions of antimicrobial research. The re-fusal to recognize antimicrobial resistance in theclinic as a serious, relevant, real problem compro-mises world health.

65
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
CHAPTER V
Improve antibiotic use in animalsScott A. McEwen
Introduction
The human health impact of non-human uses ofantimicrobials is an exceedingly controversial partof the overall resistance problem, and a part that isnot very well understood. Antimicrobials have foryears been used in food animals, pets, and farmedfish for treatment of disease and in some cases forgrowth promotion and disease prophylaxis; theyhave even been used to prevent bacterial infectionsin fruit. Humans do not live in a bubble; we sharethe environment with animals and plants. Bacteriathat are around us and within us can move rela-tively freely throughout the ecosystem in food,water, air, and the soil. Most of the attention onnon-human use has focused on animal agriculturebecause of the large volumes used there: as muchas 50% of total antimicrobial production by weight.
Important findings from theliterature review
Most of the documents reviewed made at least somereference to the public health problems of antimi-crobial resistance from antimicrobial use in animals,plants, and aquaculture. A few documents(9,18,24,25,92–95) were wholly devoted to thesubject. Some mentioned concerns about using re-sistance genes as markers in genetically-engineeredplants. While there is uncertainty about the envi-ronmental impact of resistance marker genes, it isbelieved that the probability of their transfer tomicroorganisms leading to health problems is ex-tremely low (95).
Antimicrobials are used therapeutically to treatfood animals (cattle, sheep, poultry, fish, etc.) andpets for bacterial infections (9,20,25,93). Someanimals are treated individually, although food ani-mals may be treated in groups through medicatedfeed or water if individual animal administration isnot feasible (e.g., poultry, fish) or is less efficient.Therapeutic doses are administered for varyingperiods of time, ranging from one to several days,depending upon the drug and approved applica-tion as indicated on product labels. In some cases,
Abstract
Expert scientific panels from all over the world havereviewed the evidence for resistance selection infood animals and resultant human disease. Reportsof several of the most recent expert deliberationsare reviewed here, some of them devoted wholly tothe subject of non-human antimicrobial use. Whilemany uncertainties remain, recent studies haveshown that agricultural uses of antimicrobials dohave an impact. There is consensus among thedocuments reviewed that antimicrobial use in ani-mals selects for resistance in zoonotic pathogens andcommensal bacteria, and these resistant bacteria canbe transmitted to humans through contact withanimals or food, and that they can infect humansand cause disease which can be more severe orlonger lasting than non-resistant infections. Fur-thermore, there is increasing concern about the res-ervoir of resistance that is building in entericcommensals of animals (e.g., Escherichia coli, Ente-rococcus faecium) which may be transferred torelated, or even completely unrelated humancommensals and pathogens through exchange ofgenetic material.
A number of strategies have been recommendedto reduce human health impacts from non-humanuses of antimicrobials, the most important beingto increase surveillance of resistance and antimi-crobial use, to implement good regulation to con-trol antimicrobial use in animals in light ofresistance concerns, and to take steps to ensure theprudent use of antimicrobials in animals, especiallyby reducing exposure of animals to low doses ofantimicrobials for long periods of time (i.e., growthpromoters and prophylactics) if such uses select forresistance to drugs used in human medicine. Otherstrategies include educational programmes forveterinarians, food animal producers, and dispens-ers of antimicrobials for non-human uses, reduc-ing the need for antimicrobials through alternativetreatments and infection control, and research.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
66
veterinarians prescribe antimicrobials in an extra-label manner (e.g., increased dose or duration oftreatment), either because labeled drugs are un-available for the condition, or they are consideredno longer effective.
Food animals, especially those raised intensively,may also be administered antimicrobials (usually,but not always under veterinary prescription) forprophylactic purposes during especially high-riskperiods for infectious disease (e.g., after weaningor transport) or when one or more animals in thegroup are observed with clinical disease and morecases can be expected. Fruit may also be treatedwith antimicrobials (e.g., tetracycline and strepto-mycin) in some countries to prevent certain bacte-rial infections, for example, Erwinia amylovora(19,21).
Most controversially, food animals may also beadministered antimicrobials for growth promotionor performance enhancement purposes (e.g., feedefficiency). In some cases, the distinction betweenprophylaxis and growth promotion is unclear be-cause certain drugs may be approved for both pur-poses, and growth promoters may have diseaseprophylaxis benefits. Growth promoters are usu-ally administered in relatively low concentrations,ranging from 2.5–5 mg/kg (ppm) depending onthe drug and to some extent the species treated (93).Despite the fact that these drugs have been usedextensively in agriculture for over three decades(21), scientists are not sure exactly how they im-prove growth efficiencies. It is believed, however,that in addition to dampening the effects of sub-clinical disease on growth, the drugs may suppresscertain susceptible bacteria that compete for nutri-ents with the host animal. It has been pointed outthat the benefits are greater under poor hygieneconditions, and their current efficacy is questionedbecause other means of controlling disease (e.g.,biosecurity, vaccination) have been introduced morewidely into intensive animal husbandry. It is be-lieved that efficiencies of 1–11% can be realized(21,93). Another purported benefit of growth pro-moters is a reduction of total nitrogen and fecaloutput per animal marketed, which has environ-mental impact implications. One expert panel (25)went so far as to state that antimicrobials, in par-ticular at sub-therapeutic doses (as in growth pro-motion and disease prophylaxis), had an importantpositive role in facilitating the intensification offood animal agriculture that is characteristic ofmany industrialized and some developing countries,thereby enabling the production of abundant quan-
tities of food. Other reports contend that this in-tensification of food animal production is at leastpartially responsible for antimicrobial resistanceproblems in agriculture, by increasing the need forantimicrobial use. Aside from growth promoter use,which is more common under intensive animal rear-ing conditions than in extensive, or pasture-basedhusbandry, intensive rearing can increase the needfor treatment by fostering the spread and clinicalexpression of infectious diseases of animals, and byenhancing the spread of resistant foodborne patho-gens and other bacteria among animals.
Antimicrobial use data are sparse and most docu-ments cite the difficulty in obtaining accurate, up-to-date consumption figures by species andintended use. It has, however, been estimated thatas much as 50% of total antibiotic production (byweight) is used in animals and plants, with 50–80%used in some countries for growth promotion ordisease prophylaxis and the rest used for therapeu-tic purposes (9,20,21). Usage patterns vary tremen-dously, but in some countries, a majority of foodanimals receive antibiotics at some point in theirlives, and many for extended periods of time atsubtherapeutic doses.
Many antimicrobials are administered to animalsunder veterinary prescription, but in some coun-tries, they may also be available for veterinary usewithout a prescription. These drugs are frequentlyavailable over the counter in feed stores and petshops and may be included in purchased feeds with-out veterinary prescription. Financial incentivesexist for the production and distribution of veteri-nary drugs, just as they do for human anti-microbials. Pharmaceutical companies, importers,pharmacies and other retailers may all profit fromthe sale of antimicrobials to animal owners.Veterinarians may also profit from the sale ofantimicrobials to food animal producers, and it hasbeen reported that as much as 40% of their incomecan come from this source (50).
Most of the classes of drugs used in human medi-cine are also used in veterinary medicine, althoughthere is considerable variability within and betweencountries in the range of drugs approved for use invarious animal species. Some examples of anti-microbials approved (as of 1999) in the UnitedStates are presented in the Table.
Very little attention was given to antimicrobialuse in pets in the documents reviewed, althoughthis area will probably receive more attention inthe future. Pets are frequently in close contact withtheir owners and when ill they are often treated

67
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
with the same drugs used in human medicine.Regulatory approval for use of antimicrobials in
animals and plants, when it is accompanied byhuman health risk assessment by competentnational regulatory authorities, may not includeconsiderations of microbial safety (especially resist-ance). In fact, until recently only a small numberof countries considered resistance at all in the vet-erinary drug approval process (93). Traditionally,human health safety determinations of veterinaryantimicrobials focused on the effects of antimicro-bial residues in foods of animal origin. The UnitedStates (18) required pharmaceutical companies tocompile and report microbial safety data in theirpre-approval submissions to regulatory authoritiesfor drugs intended for long-term prophylactic orgrowth promotion use in feeds. Even in recent yearswhen antimicrobial resistance issues have been inthe forefront, some countries approved importantdrugs (e.g., fluoroquinolones) in light of epidemio-logical evidence from other countries of resistanceemergence in foodborne pathogens (19). This sug-gests that antimicrobial resistance concerns were notaddressed in the approvals, or any human healthrisks that were identified were insufficient to over-ride other considerations.
There is consensus among the documents re-viewed that treatment of animals and plants withantimicrobials leads to resistance in bacteria. Theselection pressure of antimicrobial usage is thoughtto be greatest during low-dose, long-term exposure,which is characteristic of growth promoters andsome disease prophylaxis. However, therapeutic
TABLE. EXAMPLES OF ANTIMICROBIALS APPROVED FOR USE IN THE UNITED STATES (ADAPTED FROM 25)
Antibiotics approved in the United States for various species
Purpose Cattle Swine Poultry Fish
Treatment of various Amoxicillin Amoxicillin Erythromycin Ormetopriminfections Cephapirin Ampicillin Fluoroquinolone Sulfadimethoxine
Erythromycin Chlortetracycline Gentamycin OxytetracyclineGentamycin Erythromycin NeomycinNovobiocin Gentamycin PenicillinPenicillin Lincomycin SpectinomycinSulfonamides Sulfamethazine TetracyclinesTilmicosin Tiamulin TylosinTylosin Tylosin Virginiamycin
Growth and feed efficiency Ampicillin Arsenilic acid BambermycinBacitracin Bacitracin BacitracinChlortetracylcine Bambermycin ChlortetracyclineLasalocid Chlortetracycline PenicillinMonensin Penicillin TylosinOxytetracylcine Tiamulin Virginiamycin
TylosinVirginiamycin
treatments, administered at higher doses for shorterperiods of time to individuals or groups of animals,can also select for resistance. Enteric bacteria of foodanimals are especially exposed to selection pressurebecause many drugs are administered in food orwater but bacteria in other anatomic locations mayalso be exposed because many drugs are absorbedfrom the gut and others are administered parenter-ally. In addition, many drugs are excreted in activeform in urine or faeces and peresist in the environ-ment for prolonged periods of time, where theymay exert selection pressure on environmental bac-teria. In fish farming, for example, it has been esti-mated that as much as 70–80% of antimicrobialsadministered may end up in the sediment of thebody of water (96). In general, the implications ofthis environmental exposure are poorly understood.
Antimicrobial resistance occurs in the targetspecies of organisms (animal pathogens in the caseof veterinary drugs) and in a variety of non-targetspecies in the gut or in other sites. Resistance inthe animal pathogens of most importance to ani-mal health is often of little direct human healthsignificance. While there are many bacterial infec-tions of animals that can cause disease in humans(zoonoses), few of these (Salmonella is a notableexception) are important causes of clinical diseasein food animals or pets. There are a variety of ways,however, that antimicrobial resistance arising in ag-riculture can have a negative impact on publichealth. The first two were most frequently men-tioned in the reviewed documents:

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
68
1. Treatment of animals with antimicrobials im-portant in human medicine, or drugs of the samefamily or class, can select for resistance to thesedrugs in zoonotic pathogens (e.g., Salmonella,Campylobacter). Resistant zoonotic pathogenscan be transmitted from animals to humansthrough direct contact or indirectly through foodor water, and cause illness which does not re-spond to treatment. Exposure of animals todrugs not used in humans (or no longer used inhumans) can also select for resistance to drugsimportant in human medicine if the resistancedeterminants are genetically linked. For this rea-son, the linkage of two or more resistance geneson transmissible elements such as plasmids is ofincreasing concern. This phenomenon alsomakes the separation of antibiotics into “animal”and “human” use categories less tenable from aresistance point of view.
2. Genetic determinants of resistance in commen-sals of animals (e.g., Escherichia coli, enterococci)may be shared by exchanging plasmids, trans-posons or other transferable elements withrelated or even unrelated human pathogens dur-ing transient colonization of the gut of humansafter ingestion of contaminated food or water.
Some of the documents drew attention to otherpotential human health impacts:
3. Extending the principle in (2) above, resistantbacteria from animals or plants are part of a largerantimicrobial resistance ecosystem, and theirresistance genes could find their way through avariety of poorly understood, indirect pathwaysto human pathogens. These pathways couldinvolve transfer of resistance genes through in-termediary environmental organisms. Concernin some quarters has been expressed aboutinclusion of resistance markers in genetically-modified plants, however the documents re-viewed do not consider this as an important issue(93,21).
4. As a consequence of taking an antimicrobial forsome other reason (e.g., ear infection or pneu-monia), people become more susceptible to dis-ease when exposed through food or other sourceto a pathogen from animals that happens to beresistant to that drug (e.g., multi-resistantSalmonella spp.).
5. Resistance may be linked with other geneticdeterminants which render pathogens morecapable of causing disease, and thereby increase
their virulence. In this instance, resistant patho-gens may cause more severe or longer-lastingdisease in people than comparable susceptiblepathogens.
6. Antimicrobial use in food animals may, in somecases, lead to an increase in the shedding ofzoonotic pathogens (e.g., Salmonella) in animalfaeces and thereby available for human exposure,whether or not the pathogen is resistant. This isa phenomenon called “pathogen load”, and itcould occur through a number of complex andpoorly understood mechanisms whereby anti-microbial use in animals results, for example, inan increase in the duration of faecal shedding offoodborne pathogens, or an increase in the con-centration of pathogens in faeces which may thencontaminate food or water.
7. There is some concern that antibiotic residueseliminated in animal faeces and urine may exertresistance selective pressure on bacteria in soiland water. Treated animals and humans may ex-crete considerable quantities of active drug ormetabolite and many of these residues are slowto degrade in the environment.
Most of the documents acknowledge that thepublic health impacts of antimicrobial use in ani-mals and plants are complex and poorly understood.These issues have been the subject of considerablecontroversy and scientific debate for decades. Thereis consensus, however, that resistance does occur inzoonotic pathogens and commensals when animalsare treated, that humans are occasionally exposedto these bacteria through contaminated food andwater, and that illness, and sometimes treatmentfailure, does occur due to these resistant zoonoticinfections. There is also consensus, however, thatmuch uncertainty remains about the frequency withwhich these events occur, and the overall magni-tude (numbers of people affected, severity of out-come, economic impact, etc.) of the public healthimpact of resistance arising in agriculture.
Some of the uncertainties were reconciled inrecent years through a number of well-conductedepidemiological studies, carried out principally inEurope and the United States. The results of thesestudies are summarized later in the chapter. How-ever, the reviewed documents were virtually unani-mous in recommending more research andenhanced surveillance to better understand resist-ance in both medical and veterinary medicine. Sur-veillance of antimicrobial resistance among zoonoticpathogens and commensals in food animals, food

69
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
products, and foodborne infections of humans, aswell as monitoring non-human uses of antimi-crobials is thought to be the best way to identifyand quantify the effects of non-human antimicro-bial use on resistance throughout the food chain.“Only quantitative data, obtained through appli-cation of standardized laboratory methods, willallow for meaningful epidemiological analysis andevaluation” (9).
Antimicrobial resistance from agriculture is inmany ways a food and water safety issue (8). Overthe past couple of decades, food and waterbornediseases appear to have increased in incidence in anumber of countries. A number of factors are prob-ably responsible for this, including a greater bur-den of pathogens (resistant and susceptible) that istransmitted through the food chain from animalpopulations and plant products to humans. Nodoubt myriad factors are responsible for the emer-gence and dissemination of the wide range of thesefood and waterborne infections that are major pub-lic health problems for both industrialized anddeveloping countries. These same factors may beimportant in promoting the spread of resistantzoonotic pathogens and commensals, as well asenvironmental bacteria, to humans. By the sametoken, steps that are being taken throughout thefood chain to reduce the impact of food andwaterborne infections in which resistance is not yetrecognized to be a problem (e.g., E. coli O157:H7,Salmonella enteritidis) may also reduce the publichealth burden of resistance. Some of these stepsinclude Hazard Analysis, Critical Control Point(HACCP) programmes, quality assurance pro-grammes, irradiation and pasteurization (19,92).
The most important strategies that were recom-mended specifically to reduce the public healthimpact of antimicrobial use in agriculture fell intothe following major categories (9,25,50,53,92–95):government regulation; education and prudent orjudicious antimicrobial use guidelines; monitoringof antimicrobial use; surveillance of resistance; re-ducing the need for antimicrobials through alter-native treatments and infection control; andresearch.
Effective and non-effective strategies
The human health impact of antimicrobial use inagriculture has been the subject of debate, discus-sion, analysis, expert panel deliberation, and quali-tative risk assessment for decades. National andinternational expert panels and committees have
produced a large number of documents; many ofthose are reviewed here. One of the most cited ofthese was the UK Swann Report of 1969 (97). Thisreport is remembered as one of the first recom-mending that antimicrobial growth promoters andother drugs used without prescription in animalfeeds should be restricted to antimicrobials that havelittle or no application as therapeutic agents in hu-mans or animals, and will not impair the efficacyof a prescribed therapeutic drug through develop-ment of resistance. Secondly, the Swann Reportrecommended that therapeutic antimicrobials foranimals should only be available under a veterinaryprescription. These principles have been endorsedby most subsequent expert panels and task forcesand lay a foundation for modern recommendations.The British government later implemented theSwann recommendations, and some credit wasgiven to a reduction in antimicrobial-resistantSalmonella infections. Some have claimed, however,that the measures recommended by Swann werenot effective because total antimicrobial consump-tion in UK agriculture did not decline, and furtheroutbreaks of antimicrobial resistant salmonellosiseventually occurred. In reality, it is difficult to de-termine the effects on resistance and total use be-cause there was no comprehensive surveillancesystem in place at the time. The US Food and DrugAdministration (FDA) proposed in the 1970s tostop the sub-therapeutic (growth promotion andprophylactic) use of penicillin and tetracycline inanimal feeds but was criticized because there wasinadequate evidence of adverse human healtheffects and the proposal was unsuccessful (6,24).
In 1986, Sweden banned the use of growth pro-moters in animal production (21). Unfortunately,at the time the Swedish government did not have aresistance surveillance system in place with whichto measure the effects of the ban on resistance inanimals, foods, and humans. However, the quanti-ties of antimicrobials sold for use in animals weremonitored. Animal health statistics show that inthe early stages after the rather abruptly introducedban, increases in morbidity and mortality wereobserved (e.g., post-weaning diarrhoea in pigletsand necrotic enteritis in chickens). To counteractthis, antimicrobials used earlier for growth promo-tion were prescribed for prophylaxis during high-risk periods. Efforts were made to improvemanagement, feed, and hygiene in order to adaptto non-routine use of antimicrobials. In the early1990s, zinc oxide replaced antibiotics as prophy-laxis for piglets. Since 1998, zinc oxide is only avail-

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
70
able in Sweden on prescription and use has declinedto less than 10% of its maximum. Total sales of allantimicrobials for animals decreased fairly substan-tially (by approximately 60%) (98).
In the 1990s, public health surveillance in theUK and elsewhere in Europe identified some newresistance issues that once again heightened con-cerns about agricultural use of antimicrobials.Among these issues were the increase in Salmonellatyphimurium DT104 infection in humans and ani-mals, the appearance of fluoroquinolone-resistantCampylobacter jejuni infections in humans andpoultry, and the occurrence of vancomycin-resist-ant enterococci (VRE) in pigs and poultry.
Salmonella typhimurium DT 104 was first iden-tified in the UK but has since been found in manycountries throughout the world where it is an im-portant cause of disease in humans, cattle, pigs,poultry, and other animals. Salmonella strainsappear to come and go in “waves” every few years(epidemics of DT29, DT204, DT193 and DT104strains were observed in the UK (21) but DT104was particularly concerning to public and animalhealth officials because of its pathogenicity and thefact that most isolates were resistant to at least fiveantimicrobials (pentaresistance). While the role ofagricultural antimicrobial use in the genesis andspread of Salmonella typhimurium DT104 is un-known, there is good evidence that antimicrobialuse in animals was associated with development ofreduced susceptibility to fluoroquinolones amongsome isolates of this organism. This evidence restsmainly on the temporal relationship between ap-proval of fluoroquinolones for use in food animalsand identification of resistant (reduced susceptibil-ity) strains. Shortly after fluoroquinolones werelicensed as therapeutic agents for food animals inthe UK, public health laboratories began to iden-tify isolates with decreased susceptibility toquinolone drugs. This was particularly alarmingbecause fluoroquinolones are very valuable drugsfor treating humans for a variety of infections, in-cluding invasive salmonellosis.
Similarly, investigators in other European coun-tries, (e.g., the Netherlands, Spain) wherefluoroquinolones were approved for therapeutictreatment of poultry, identified substantial increasesin the prevalence of fluoroquinolone resistanceamong poultry and human isolates of Campylo-bacter jejuni. This type of resistance was remark-able in the rapidity with which it appeared andincreased in prevalence (21,92). Other countrieshave reported similar findings.
Avoparcin is a glycopeptide antimicrobial in thesame family as vancomycin. It was approved foruse in many European countries as a growth pro-moter. At the time since vancomycin was not widelyused, there was little reason to be concerned aboutresistance problems in humans. Things changed,however, when vancomycin became critical inhuman medicine for treatment of methicillin-resistant Staphylococcus aureus (MRSA) and otherserious infections. Resistance to vancomycin, espe-cially among enterococci (VRE) became an impor-tant public health problem in many countries.Researchers identified VRE in food animals exposedto avoparcin, where they were not found in ani-mals in countries where avoparcin was not used asa growth promoter. Furthermore, the prevalenceof VRE among non-hospitalized people in the com-munity was much higher in countries that usedavoparcin. There is evidence that VRE in foodanimals may have been a reservoir for resistance inhumans, perhaps through exchange of geneticmaterial between animal and human strains, orthrough transient colonization of the human gutby animal strains.
It is worth reiterating that prior to identifica-tion of the link between avoparcin use and VRE infood animals, the drug was thought to be anappropriate choice for a growth promoter. This is agood example of a major problem confronting theanimal and pharmaceutical industries and thosecharged with drug regulation. Growth promoterdrugs that are seemingly safe today because theyare not used in people and do not select for resist-ance in people may not be in the same positiontomorrow, if the same or related drugs becomeimportant in human medicine. Some older fami-lies of pharmaceuticals, previously not considerednecessary or desirable for human medicine, are “re-trieved” in order to combat new resistance prob-lems (e.g., vancomycin for MRSA). More recently,the same sort of thing has happened withvirginiamycin, which is a streptogramin antimicro-bial that has been used for many years in agricul-ture, principally as a growth promoter in poultryand pigs but also in some cases for disease prophy-laxis. There is now evidence that virginiamycin useselected for streptogramin resistance in enterococciand there is considerable concern that this couldcompromise the usefulness of related streptogramindrugs (e.g., pristinamycin and quinupristin-dalfopristin), which have been recently introducedfor treatment of vancomycin-resistant enterococciand other bacterial infections in humans.

71
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Growth promoters do not necessarily cause re-sistance problems in humans. For example,ionophores are a group of antimicrobials usedwidely in veterinary medicine for growth promo-tion in a variety of species, and for treatment andprevention of coccidiosis in poultry. Resistance hasso far not been identified as a problem in animalsand there are no indications that the family of drugswill become useful in humans, perhaps because oftoxicity concerns.
It is important to point out that these examplesof recent resistance concerns involve both growthpromoters (avoparcin, virginiamycin) and therapeu-tic drugs (fluoroquinolones). Strategies to addressthese concerns are likely to be somewhat different;with the former, regulatory measures (i.e., decisionto permit their use or not) are most important; withthe latter, assurance of prudent use is very impor-tant in minimizing concerns.
Collectively, public health concerns arising fromSalmonella typhimurium DT104, quinolone resist-ance in Campylobacter jejuni and Salmonella, andglycopeptide and streptogramin resistance in ente-rococci substantially raised the profile of antimi-crobial resistance as a public health issue in theveterinary, agricultural and food industries. Somestrategies have been implemented to reduce thepublic health impact, or to improve understand-ing of the type and magnitude of the impacts andthese are discussed below.
Government regulation
Mention has already been made about the meas-ures taken in UK after the Swann Report of 1969(97) to restrict the use of growth promoters to drugsnot used in human medicine, and about the sug-gestions in the literature that these measures werenot effective in reducing total antimicrobial use inanimals. There may, however, have been benefitsin reducing incidence of resistant Salmonella.Although not discussed in the reports reviewed, ithas been pointed out in the literature that any re-duction in usage achieved through restrictions ongrowth promoters was compensated by increasesin prescription drug use. This underscores the needin any overall strategy to carefully monitor all usesof antimicrobials and take appropriate controlaction if excesses are detected, and to reduce theneed for antimicrobials by making improvementsin animal management, hygiene, and health.
Many countries, most notably in Europe, havebanned the use of avoparcin in animal feeds, and
in some countries (e.g., Australia) the drug has beenwithdrawn voluntarily. Fortunately, some countrieshave monitored VRE prevalence in animals, foodand humans and there are reports that the preva-lence in food animals (initially in poultry) hasdecreased in Denmark and Germany since the with-drawal (4). Although immediate decreases were notseen in pigs in Denmark, recent data suggest thatthe prevalence of VRE in pigs is decreasing, andthat levels may have been maintained, at least inpart, by cross-resistance with macrolides (e.g.,tylosin). Reduction in tylosin use has been accom-panied by a decrease in VRE prevalence (99).
In 1999, four drugs (tylosin, virginiamycin,spiramicin, and bacitracin) were banned as growthpromoters on the basis of the precautionary prin-ciple that they or related drugs are used in humanmedicine, or select for resistance to drugs used inhuman medicine. This action was also consistentwith recommendations from the Swann Report andWHO. While this action was mentioned in thereviewed documents, the ban is so recent that therewere no data available on its effects in terms ofresistance trends among zoonotic or commensalbacteria, trends in antimicrobial usage in animals,or in terms of effects on the health of animals orindices of production (e.g., feed conversion, daysto market, etc.). It is too early to tell what theseeffects will be; nevertheless, there are some recentlypublished data from Denmark where reductionsbegan a little sooner than in the rest of Europe (99).Danish farmers had actually decided voluntarily in1998 to stop feeding growth promoters to foodanimals and phase out their use by 2000. TheDANMAP 99 report (Danish Integrated Antimi-crobial Resistance and Research Program) describesdrug use patterns in the country in 1998, after thereductions were in place (99). The early stages ofreduction in growth promoters were not accompa-nied by an increase in consumption of therapeuticdrugs, but between 1998 and 1999 there was anincrease in tetracycline use for treatment of entericdisease in swine.Time will tell whether additionalpositive or negative effects on therapeutic drug usewill be seen in Denmark.
The effects of the European ban of 4 growthpromoters on resistance in zoonotic bacteria andcommensals are also largely unknown because theban is so recent. DANMAP reported that sampling-related problems made the Danish Salmonellaresults from 1998 difficult to interpret, becausemany isolates from both animals and humans werelinked epidemiologically. Resistance in Campylo-

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
72
bacter coli to erythromycin dropped by almost 50%in 1998, and this was attributed to withdrawal oftylosin (another macrolide) as a growth promoter.Among enterococci of pigs and poultry, reductionin resistance to vancomycin, virginiamycin, anderythromycin were observed after the ban. AmongE. coli, the proportion of isolates resistant to oneor more antimicrobials decreased over the same pe-riod, but changes in prevalence of resistance to spe-cific banned growth promoters were not observed(99).
Another important regulatory development thathas taken place in some, but not all countries, isthe inclusion of antimicrobial resistance considera-tions in the drug approval process. In the UnitedStates, a great deal of attention has been given tothe so-called “Framework Document” (ProposedFramework For Evaluating And Assuring TheHuman Safety Of The Microbial Effects Of Anti-microbial New Animal Drugs Intended For Use InFood-Producing Animals), developed within theFood and Drug Administration and published in1998 (24). The Framework is “intended to pro-vide a mechanism for evaluating and ensuring thehuman safety of antibiotics and other antimicrobialsused in food animals, including those used forgrowth promotion” (24). The Framework is a con-ceptual risk-based process with the stated goal ofpreserving the effectiveness of drugs which are im-portant in human medicine while enabling the safeuse of antimicrobials in food animals. It providesfor categorization of antimicrobials on the basis ofan assessment of their importance to human medi-cine. Category I drugs (or members of a class ofdrugs) are essential for treatment of life-threaten-ing diseases of humans, or are important for treat-ment of foodborne diseases of humans, or aremembers of a unique class of drugs used inhumans. Examples include quinolones, vancomy-cin, and quinupristin-dalfopristin. Category IIdrugs are important for treatment of potentiallyserious human diseases, but for which suitable al-ternatives exist (e.g., ampicillin, erythromycin).Category III drugs have little or no use in humanmedicine or are not the drug of first choice forhuman infections.
Importantly, the Framework strategy would alsocategorize, into high, medium and low, the likeli-hood of human exposure of resistant human patho-gens arising from the use of drugs in food animals.This is an attempt to use in the characterization ofrisk information on the ability of the drug to selectfor resistance in bacteria, the likelihood that resist-
ant bacteria will be transmitted to humans throughfoods or other sources, and the likelihood that thistransfer will result in the loss of treatment options.Categorization would include consideration of drugattributes (e.g., mechanism and rate of resistanceor cross-resistance induction), the expected prod-uct use patterns (e.g., duration of treatment, spe-cies, number, and type of animals treated), andpotential human contact (e.g., bacteria of concern,environmental and food contamination, foodprocessing effects). Examples that were given in-clude: a growth promoter used in multiple speciesand inducing resistance to an antimicrobial usedin human medicine would be placed in the highpotential human exposure category; a drug usedfor entire herd therapy during outbreaks of diseasewhich occur in a small fraction of herds would beplaced in the medium category; and a drug usedfor individual animal treatment of only occasionalanimals in herds, for a short duration, would beplaced in the low category.
Another very important feature of the Frame-work in a regulatory sense is the notion of estab-lishing safe resistance threshold levels forantimicrobials. Conceptually, the threshold levelcould be set at the level of resistance that carrieswith it insignificant likelihood of transfer tohumans, if it were possible to accurately determinesuch a level. There is also provision for establishinglevels for Category I drugs to be used in post-approval monitoring of resistance and which couldserve as an early warning system indicating thatresistance was reaching a level of concern. The docu-ment acknowledges that the usefulness of suchthresholds depends upon the ability to demonstratethat they are sufficiently protective of public health,and that there is a capability of detecting when suchlevels are reached.
The Framework document also makes provisionfor requiring pharmaceutical companies to conductpre-approval studies of drugs in order to character-ize the type and rate of resistance development.Post-approval monitoring studies may also berequired of certain drugs in order to identify emer-gence of resistance of sufficient concern to publichealth to trigger intervention and mitigation strat-egies. Finally, there is provision for requiring sub-mission by pharmaceutical companies of detaileddrug sales information by species, state, dosageform, year, and estimate of active units sold.
Another important initiative undertaken byFDA in 1999 was preparation and public presen-tation of a “Draft Risk Assessment on the Human

73
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Health Impact of Fluoroquinolone ResistantCampylobacter Associated with the Consumptionof Chicken”. This effort could be a milestone inevidence-based regulatory decision-making in thearea of antimicrobial resistance in agriculture. Therisk assessment is a highly focused, structured as-sembly of scientific and public health informationfrom a variety of relevant sources, including thescientific literature, public health surveillancedatabases, and expert opinion. The assessment isan attempt to estimate in quantitative terms thepublic health risk in one year from resistant food-borne pathogens due to the use of antimicrobialsin food producing animals. Within the assessment,a mathematical model was developed which relatedthe prevalence of fluoroquinolone-resistantCampylobacter infections in humans to the preva-lence of fluoroquinolone-resistant Campylobacter inchickens (a major source of Campylobacter jejuniinfection in the United States). Fluoroquinoloneresistance in Campylobacter was selected becausecampylobacteriosis is the most commonly reportedbacterial foodborne disease in the United States,fluoroquinolones are important drugs in humanmedicine which are sometimes used to treat peoplesick with this disease, and fluoroquinolones areapproved for use as therapeutic agents in poultry.As previously mentioned, fluoroquinolone resist-ance has been identified as a problem in Campylo-bacter jejuni in a variety of other countries wherethese drugs are used to treat poultry.
Using data from epidemiological studies and theFOODNET surveillance system in the UnitedStates, the model estimated the most likely and es-timated range of cases of fluoroquinolone-resistantCampylobacter jejuni infections that occur in oneyear in the United States, and which are treatedwith fluoroquinolones by physicians. The risk as-sessment clearly describes the assumptions that aremade in construction of the model and identifiesthe various uncertainties that arise from lack ofknowledge or variability in data inputs. As anexample of one outcome from this model, the esti-mated mean number of people with fluoro-quinolone-resistant Campylobacter infection fromchicken who received fluoroquinolone in 1998 was5065 (with a 90% confidence interval of 2585,8595).
This risk assessment is important for a numberof reasons. Many stakeholders in the veterinary,animal production, and pharmaceutical sectors havefor years been asking for a risk-based regulatorydecision-making process on antimicrobials. Quan-
titative risk assessment is used in a number of fieldsto assist risk management decision-making whenthe magnitude of health impacts is clouded by com-plexity and uncertainty. This is certainly the casewith estimating the human health impacts of anti-microbial use in agriculture. The FDA assessmentis also a good example of the use of available sur-veillance data to estimate quantitatively the humanhealth impact. Quantitative risk assessment is be-ing used increasingly in other microbial food safetyissues, and experience and confidence in the proc-ess are growing. An important next step for regula-tors is to identify the public health risks fromresistance that are “acceptable” to society. A gener-ally acceptable level of cancer risk from environ-mental chemicals is one per million in thepopulation over a lifetime of exposure. It remainsto be seen whether acceptable levels for microbialrisks can be agreed upon internationally. If suchlevels (or “risk standards”) can be agreed upon,quantitative risk assessment could be used to iden-tify resistance thresholds, beyond which publichealth impacts become unacceptable. This will nodoubt prove to be a difficult, but important task.
Education and prudent use of antimicrobials
None of the documents reviewed educational orprudent antimicrobial use strategies which havebeen shown to be effective in reducing resistancerisks, nor was evidence presented that any haveactually been implemented. There are anecdotalreports in the scientific literature that a number ofnational and international organizations (e.g., pro-fessional veterinary associations) have begun todevelop prudent or judicious use guidelines forantimicrobials in animals, and in some cases, codesof antimicrobial prescription in veterinary practice.There are also some reports of attempts to drawattention to the issue in the minds of veterinariansand food animal producers, many of whom stillbelieve that the only public health concerns thatarise from antimicrobial use in food animals areresidues of drugs in edible tissues.
Although not mentioned in the documents,Denmark has recently put significant limits on theability of veterinarians to profit from the sale ofantimicrobials in food animal production. Theeffects of this measure on antimicrobial sales andconsumption are not yet known.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
74
Monitoring of antimicrobial use
Some of the documents mentioned that some coun-tries (notably in Scandinavia) have been assemblingnational antimicrobial consumption data, or haverecently instituted the assembly of these data.Sweden was able to document the effects of theirgrowth promoter ban on consumption ofantimicrobials for prophylactic and therapeuticpurposes because they had an antimicrobial usemonitoring system in place. As described above,the United States has declared plans to require thesubmission of antimicrobial sales data to the FDA,which can be used to monitor trends in consump-tion, and in epidemiological and risk assessmentstudies addressing the associations between anti-microbial use and resistance in animals and humans.Although not specifically mentioned in the docu-ments reviewed, Denmark has instituted an anti-microbial use monitoring system (DANMAP) toaccompany its resistance monitoring.
Surveillance of resistance
Calls for resistance surveillance systems figureprominently in nearly all reviewed documents. Itis generally hoped that these systems will providedescriptive data on resistance, which will enable theidentification of temporal trends, emerging issues,and the extent of resistance in human and animalpopulations and food products.
Many countries have for some time had elementsof national resistance surveillance in place. It wassurveillance of resistance data assembled by thePublic Health Laboratory Service in the UK whichidentified the emergence of decreased susceptibil-ity to fluoroquinolones among Salmonellatyphimurium DT104 isolates (21). Public healthscientists in other countries have made similar con-tributions to our understanding of resistance issues.
Two comparatively new antimicrobial resistancesurveillance programmes are the previously men-tioned DANMAP in Denmark, and NARMS inthe United States. DANMAP is run by the DanishVeterinary Laboratory (22,99). DANMAP reportsare issued annually and describe antimicrobial con-sumption data in animals and humans, resistancein zoonotic bacteria (e.g., Salmonella, Campylo-bacter), resistance in indicator bacteria (e.g., E. coli,enterococci), and resistance in bacteria from diag-nostic submissions from humans and animals. Sum-maries are included which include interpretationof observed trends, relationships between antimi-crobial use patterns and resistance, and sources of
potential bias. This programme is able to documentthe effectiveness of some of the strategies that havebeen used in Denmark to curtail resistance fromfood animals, most notably the ban on growth pro-moters.
In the United States, NARMS (National Anti-microbial Resistance Monitoring System) EntericBacteria Program tests antimicrobial resistance re-lated to agriculture (22,24). It began in 1996 as ajoint effort by the Centers for Disease Control andPrevention (CDC), FDA and US Department ofAgriculture. Isolates (initially Salmonella, with ad-dition of Campylobacter in 1997) are obtained fromhuman clinical specimens, animal clinical speci-mens, normal animals, and carcasses at slaughterfrom across the United States. Data from NARMSwere used in the FDA’s quantitative risk assessmentof fluoroquinolone-resistant Campylobacter fromchicken (described above) and have been presentedin a variety of scientific venues.
Alternative treatments and infection control
As mentioned above, Sweden reported that farm-ers eventually adapted to the ban on growth pro-moters by a number of means, including theimplementing improved husbandry practices andincreased use of zinc oxide (which has been criti-cized on environmental grounds (21), but nowappears to be under control (98). While this is evi-dence that antimicrobial needs were reduced, therewas no resistance monitoring in place that couldmeasure the effect of management changes onresistance.
Barriers to action
There are many disincentives and barriers to thefurther implementation of resistance risk reductionstrategies. These include a general lack of accept-ance among veterinarians and food animal produc-ers that a resistance problem exists in agriculture; alack of scientific information on the extent andmagnitude of public health risks; conflicting eco-nomic interests; the costs of implementing alter-natives; lack of regulatory will and capability; lackof efficacious and economical alternatives toantimicrobials; and lack of resources to develop andimplement strategies.
A major barrier is the lack of acceptance thatagriculture and veterinary medicine are significantcontributors to the human health impacts of re-sistance. Large numbers of veterinarians, other sci-

75
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
entists involved in agriculture, and food animalproducers simply do not believe that antimicrobialuse in food animals has substantial negative healtheffect on humans. This is not simply a lack of aware-ness due to inadequate or insufficient education ortraining, but has to do with the relative lack (untilrecently) of concrete examples clearly document-ing the impacts. Unlike physicians, who see patientswith disease caused by resistant bacteria, and whocan see that resistance in hospital and community-derived pathogens is related to use of antimicrobialsin those settings, veterinarians and producers donot see these cases. Until recently, few well-documented examples of human illness fromresistant pathogens originating on the farm havebeen described, (e.g., the recently-described caseof ceftriaxone resistant salmonellosis in a childapparently infected on a farm) (100). The tremen-dous complexity of the food production, process-ing, distribution and food service system inindustrialized countries makes it extremely diffi-cult to trace infections and resistance genes. Ifpeople do not believe that their practices and be-haviours create public health risks, it is more diffi-cult to get them to change these behaviours.
The lack of scientific information presents afurther barrier to obtaining general agreement, evenamong people without a financial stake in theissue, when intervention strategies are warranted.Almost intuitively, many stakeholders in foodanimal industry and veterinary medicine call for a“science-based” or “risk-based” regulatory decision-making process on resistance issues. Many govern-ment agencies themselves call for more evidencebefore implementing interventions (24). There is aconflict between those who believe that enoughevidence exists to warrant risk-reduction actions,and those who believe there is a need for more evi-dence of the nature and extent of the problem be-fore attempting to fix it.
Balancing the risks of resistance against the ben-efits of antimicrobial use in agriculture is also abarrier to action. One of the reasons for this is thatthe risks and benefits are borne by different groups.The food animal producer might save the life of ananimal (and therefore his investment) by treatingit; he realizes directly the benefit of treatment. Anyresistance risks arising from that treatment wouldmost likely be realized by someone exposed to theresistant bacteria, far down the food chain. Con-versely, if the producer reduces antibiotic use onhis farm, he may not realize any direct benefit.
Just as there are some financial incentives for
antibiotic use in humans, strong financial reasonsexist for continued use of antibiotics in food-producing animals for food animal producers,veterinarians, and pharmaceutical companies.
If society as a whole is not prepared to acceptsome risk from the non-human use of anti-microbials then all uses would be banned fromagriculture. Few people subscribe to this extremeview. This implies that some level of risk, howeversmall, is acceptable in exchange for the perceivedbenefits of treating sick animals (alleviation of ani-mal suffering) or reducing losses due to disease inanimals. The difficulty comes in identifying the lineof demarcation between acceptable and unaccept-able risk. The general feeling among the veterinaryand animal production communities is that thebenefits of antimicrobial use in treating and pre-venting infectious disease in animals far outweighthe risks associated with their use in animals. Aslong as this feeling prevails, it will be a majorbarrier to implementing the strategies intended toreduce any risks that are indeed present.
There is a strong perception in some quartersthat more drugs are needed in veterinary medicineso that food animal production can continue to beefficient and sick animals can be treated. The ma-jority of bacterial infections of animals are notzoonotic and most veterinarians and producers feelthat resistance among these pathogens is purely ananimal health concern. Historically, the responseto problems of resistance in veterinary medicinehas been to reach into the cabinet for another newdrug. Notably, an antimicrobial resistance crisis hasnot been perceived in veterinary medicine, as is thecase in human medicine. Hence, some groups callfor more regulatory approvals of new drug applica-tions without acknowledging in any substantial waythe need for stewardship of available antimicrobialsin agriculture (25). There does not appear to be anappreciation of the animal health costs of antimi-crobial resistance and that there are good animalhealth reasons to preserve the currently availabledrugs. Perhaps in the past, new drugs were so read-ily available that this was unnecessary, or pharma-ceutical companies were sufficiently successful inmarketing their new products that veterinarians andproducers looked to new drugs rather than preserv-ing the existing ones. In many ways, the effective-ness of drugs that have been available for therapyin veterinary medicine (e.g., penicillin, tetracycline)has in some countries been squandered by theirexcessive use as prophylactic agents or growth pro-moters.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
76
Another barrier is the financial interest of vari-ous participants in food animal and plant produc-tion. These are not simply the interest inminimizing losses due to bacterial disease, or thefinancial interests of the pharmaceutical industries,which are essentially the same as those encounteredin human medicine. Unlike physicians in most in-dustrialized countries, antimicrobial sales are oftenan important source of income for veterinarians.Many include charges for other services (healthmanagement advice, for example) within the mark-up for drugs, and this source of income helps sus-tain rural veterinary practice, which can be difficultin many areas. Most professional organizations andindividual veterinarians would recoil at the sugges-tion that profit was a motive for prescribingantimicrobials, and few if any data are available tosupport the contention. It would nevertheless bedesirable to remove such financial incentives.
Many food animal producers operate on verynarrow profit margins, and to stay in business theyneed to be as efficient and economical as possible.The costs of implementing animal husbandry orother management changes that could decreaseresistance risks are a barrier. Many food animal in-dustries have made major investments in controlof infectious diseases for the simple reason that itwas in their interest (and in their animals’ inter-ests) to eliminate or substantially reduce the im-pact of infectious diseases on their operations.Measures that reduce clinical disease in animals willdecrease the need for antimicrobial treatment,which could reduce human health resistance risk.Some, perhaps many, of these changes (e.g.,biosecurity measures) may also reduce transfer anddissemination of resistant zoonotic agents andcommensals. However, few of the commonly usedbiosecurity measures or vaccination programmes areaimed specifically at foodborne zoonotic pathogensor commensals (with the exception of Salmonellaprogrammes in some species), because they arenormally not important causes of clinical diseasein animals.
The lack of suitable, economically attractive,alternatives to antimicrobials is also a barrier tochange. The experience of major changes institutedin some countries (e.g., Sweden, Denmark) is hav-ing an impact in other countries, but it would helpgreatly to have local examples of alternatives in placeon typical farms in many or most countries, rel-evant to the agricultural systems of those countries.
From a regulatory standpoint (which is argu-ably more important to resistance containment for
non-human than human uses of drugs) there are anumber of barriers to implementation. There maybe a lack of regulatory will in some countries be-cause the subject is so controversial and rife withuncertainty, and effective political lobbying maybe conducted by those in opposition to resistancecontrol measures. Many countries lack the resourcesto conduct risk assessments to support regulatorychange, and resources to implement surveillanceprogrammes. There may also be reluctance orinability to regulate prescribing practices ofveterinarians at the national level.
Recommended strategies
A recent WHO document (94) relevant to use ofantimicrobials in animals has been produced whichcontains specific recommendations on a numberof these strategies. This document is the most com-plete and recent set of recommendations pertain-ing to animal use and the interested reader shouldrefer to the original in its entirety.
The document entitled “A Public Health ActionPlan To Combat Antimicrobial Resistance” con-tains many action items for the implementation ofstrategies to address antimicrobial resistance withinthe United States (53). These are presented at a levelof detail not found in most of the other documentsmaking mention of non-human uses of anti-microbials and the interested reader should also tothe original document for details.
Many of the documents reviewed mentionedthat antimicrobial resistance is a global issue andsteps are needed to control the international spreadof resistance through movement of humans, ani-mals and food products (7). One major documentrelating to the animal area was much more con-servative than the others in its recommendationspertaining to resistance from agriculture (25). Thisdocument was prepared by a committee that wasmuch more heavily representative of veterinary andpharmaceutical company interests than was the casewith the other reviewed documents. It did not in-clude in any of its major recommendations a callfor the abolition or withdrawal of growth promot-ers of a similar class to drugs used in human medi-cine, or which select for resistance to these drugs.Nor did it recommend greater efforts to ensure theprudent use of antimicrobials. The other documentscalled for these actions.
The general strategies are presented below inabbreviated form from the original documents(7,9,25,50, 53,92–95), and in descending order of

77
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
priority. The main headings are given in order ofpriority (e.g., “surveillance of resistance” first), thenspecific strategies under each heading are prioritizedby this author. In general, the most important strat-egies are to increase surveillance of resistance andantimicrobial use, to implement good regulationto control antimicrobial use in animals in light ofresistance concerns, and to take steps to ensure theprudent use of antimicrobials in animals, especiallyby reducing exposure of animals to low doses ofantimicrobials for long periods of time (i.e., growthpromoters and prophylactics) if such uses select forresistance to drugs used in human medicine.
The top priority strategy is to improve surveil-lance of resistance arising in agriculture. Increasedsurveillance of resistance in foodborne pathogens,commensals of animals and humans, and moni-toring of drug use is essential for the assembly ofdata that can be used to identify the importanthuman (and animal) health impacts of resistance,and how these impacts relate to actual drug use inanimals. This information is vital to good policy-making, and to convince people where the prob-lems exist. To date, only a few countries have beenable to construct reasonably comprehensive surveil-lance systems and none has a perfect programmein place. Other industrialized countries should beable to implement surveillance systems within 2–3years. Developing countries in particular will havedifficulties with this strategy, given the financial,human and other resource demands required forimplementation. International cooperation isneeded to disseminate the results of surveillanceamong all countries, so that even those without theinfrastructure can use the results to conduct riskassessment, make policy, and manage risk.
Secondly, good regulation at the national levelis urgently needed in all countries to control anti-microbial use. Since many countries have not evenconsidered resistance issues when developingcurrent policies, these need to be revised appropri-ately. Most countries will not have the resources toundertake elaborate risk assessments of all drugsused, however, examples of regulation and policy withsupporting data should be made available throughWHO to countries that can make use of it.
Third, encouraging prudent use of anti-microbials in all aspects of animal and plantproduction is essential. Veterinarians and animalowners in particular must be made aware of thefacts of the impact of resistance on humans, and ofthe costs of resistance to themselves, their familiesand animals, and to the public. People need to have
good reasons to modify their behaviour and theseshould be provided to them.
Surveillance of resistance
• Identify the components of a national post-approval resistance surveillance plan includingorganisms (zoonotic pathogens, entericcommensals from animals, food, humans),standards and methodologies, and core capacity(laboratory, etc);
• Undertake regular monitoring for resistant bac-terial pathogens and commensals in food-producing animal populations and animal-basedfood products;
• Resistance monitoring in food animals shouldallow for correlation with similar data fromhumans;
• Data generated from surveillance of resistanceand antimicrobial use should play a key role inthe development of national policies;
• Closely monitor the use of antimicrobials inanimal surveillance programmes. Post-approvalsurveillance is essential and should be able todetect resistance in time to take corrective meas-ures;
• The threshold levels of resistance that are ofpublic health concern must be defined; theselevels should be low enough that any interven-tions they may trigger can still be efficacious;
• If resistance increases above levels of concern,then incremental interventions up to withdrawalof the drug from the market should be consid-ered;
• Evaluate the usefulness of monitoring sentinelhuman populations (e.g., farm and abattoirworkers) and people in the community for in-fection with resistant bacteria;
• Incorporate antimicrobial resistance explicitly infood safety monitoring of imported foods.
Monitoring of antimicrobial use
• Monitor closely the use of antimicrobials inanimal surveillance programmes;
• Post-approval surveillance is essential and shouldbe able to detect resistance in time to takecorrective measures.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
78
Government regulation
• Enforcement policies should be designed toensure compliance with laws and regulationspertaining to the authorization, distribution,sale, and the use of antimicrobials in food-producing animals;
• Licensing of veterinary antimicrobial productsshould include consideration of safety issues re-lated to the human health impact of resistancedeveloping in food animals;
• Abolish the use of antimicrobials that are of asimilar class to those used for treating humansas growth promoters in animals;
• A single, multidisciplinary government commit-tee should oversee the regulation of antimi-crobials in both human and non-human fields;
• Threshold levels of resistance for post-approvalsurveillance should be defined and provisionshould be made to modify or suspend the mar-keting of antimicrobials if thresholds aresurpassed;
• Governments should assess the risks and ben-efits of antimicrobial use in agriculture; a risk-based evaluation of human health effects of allantimicrobials should be conducted, includingcurrently registered products;
• Registration decisions should include considera-tion of the potential rate of resistance in thepre-approval evaluation.
Prudent or judicious use
• Encourage the prudent use of antimicrobials inanimals, in accordance with similar strategies forhumans; recommended dosages should be opti-mal for therapy and minimize the developmentof resistance;
• Develop and implement standards of practiceto ensure that antimicrobials are not used as sub-stitute for good farm hygiene;
• Ensure that animal producers employ produc-tion systems that promote animal health/welfare such that the use of antimicrobial agentsis part of, not a replacement for, an integratedanimal health programme;
• Prophylactic use of antimicrobials can only bejustified when it can be shown that a particulardisease is present or likely to occur, and such
use should be regularly assessed for effectivenessand need;
• Establish codes of practice for veterinarians thatreflect antimicrobial resistance concerns;
• Locally derived treatment guidelines should in-clude a list of antimicrobials for conditions com-monly presented in various species and offer arational treatment choice based on scientificdata;
• Treatment records should be kept and veteri-narians should continuously evaluate theirprescribing practices;
• Evaluate the impact of making all systemicveterinary antimicrobials available by prescrip-tion only;
• Support demonstration projects to evaluate pro-grammes which use multiple interventions topromote judicious drug use and reduce infec-tion rates;
• If sufficient evidence exists that profit from salesnegatively impacts on prescribing, appropriatecountermeasures should be taken;
• Advertising and promotion of animal healthproducts should comply with national guidelinesand codes of practice.
Education
• Conduct education programmes for veteri-narians and farmers on the prudent use ofantimicrobials (including the potential risks tohuman health of emerging resistance);
• Veterinary undergraduate, postgraduate and con-tinuing education should be evaluated to ensurethat prudent antimicrobial use and resistance aregiven high priority;
• Convey information to involved parties (e.g.,veterinarians, farmers and dispensers) thatfacilitates understanding of the human healthimpacts of resistance;
• Expand the understanding of the ecology ofantimicrobial resistance among involved parties;
• Support public health education campaigns onfood safety and the merits of irradiation forreducing foodborne infections.

79
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Research
• Evaluate the nature and magnitude of impactsof antimicrobial growth promoters and use theinformation to assist in risk-benefit assessmentsof each use;
• Seek alternatives (including vaccines) to anti-microbials for food animals;
• Conduct research to define the effects of anti-microbials in veterinary use and used in plantson the emergence of resistant bacteria;
• Evaluate the effect of current food processingand distribution methods on the emergence andspread of resistant organisms;
• Conduct research to better understand themolecular epidemiology and mechanisms ofgene transfer, and the population biology andepidemiology of resistance;
• Assess the impact on household contacts ofantimicrobial use in pets;
• Conduct pilot studies to assess the extent ofenvironmental contamination by antimicrobialresidues and resistant organisms that enter thesoil or water from human and animal waste;
• Gather information on the relationship betweenantimicrobial pesticides and emergence of resist-ance.
Alternatives to antimicrobials
• Streamline the regulatory process for drugs andproducts that are not likely to cause antimicro-bial resistance;
• Seek alternatives to antimicrobial growth pro-moters (vaccines, nutrition, etc).


ConclusionStuart B. Levy
mark’s success. By eliciting support from researchscientists, health care providers, educators, andpolicy-makers, the resistance problem can be con-trolled in each country.
Because infectious disease seriously threatens thehealth and economy of each country, preservingthe power of antibiotics should become a nationalpriority. The WHO global strategy (26) providesan excellent framework for action by all country.Industrialized countries can take the lead in com-mitting resources for more basic, clinical andapplied research, and related interventions to curbantibiotic resistance. In all countries, government,non-governmental organizations, professional so-cieties and clinical leaders at appropriate levels ofjurisdiction must develop feasible approaches thatare tailored to local conditions and available re-sources. In some instances, a simple hand washingor “antibiotic use improvement programme” willmake an enormous difference (20). It is the com-bined efforts of these individual interventions thatwill become the global solution.
The year 2000 was a banner year for the recogni-tion of antibiotic resistance as a priority publichealth problem around the world. The WorldHealth Organization provided leadership in devel-oping a global strategy for addressing antibioticresistance (26). United States governmental organi-zations developed a detailed interagency plan withspecific agency assignments (53). In addition, theUnited Kingdom, Sweden, Canada, and othersbegan strong public awareness campaigns to im-prove antibiotic use. Even more remarkable is thecommitment of countries with limited resourceswhich have instituted national regulations to pro-tect the potency of existing antimicrobial agents intheir region. Of note, Chile, Panama and CostaRica have recently established national regulationsfor the sale and prescription of antibiotics. To buildon this momentum, a commitment from eachcountry and institution is needed to roll back anti-biotic resistance on a global basis.
Optimism for the future
Nations and local institutions must work togetherto preserve the power of antibiotics. Each countryneeds to act as a steward of antibiotics to pass themon to the next generation. Individual countriesshould maximize accessibility to ap-propriate antibiotics and minimizetheir misuse in order to extend theirlife in the country. The literature nowdocuments that national and institu-tional initiatives can dramatically re-duce the prevalence of antibioticresistance (14,20). The strict enforce-ment of antibiotic use policies in hos-pitals has helped Denmark achieve adrastic reduction in the incidence ofmethicillin-resistant Staphylococcusaureus (see graph, 101). Compliancewith infection control proceduresand the inclusion of clinicalmicrobiologists in the prescribingprocess have also contributed to Den- Source: V.T. Rosdahl, and A.M. Knudson (101). Reprinted with permission from SLACK, Inc.
20
15
10
5
0
1960 1965 1970 1975 1980 1985
Perc
ent r
esist
ant s
trai
ns
FREQUENCY OF METHICILLIN-RESISTANT STAPHYLOCOCCUS AUREUS (MRSA) IN DENMARK
81
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS

References
immediate threat to the nation’s health. The role ofresearch. 1997.
12. Royal Society of Medicine. Resistant Organisms:Global impact on continuum of care. Proceedingsof a conference sponsored by 3M Health Care andRegent Medical, London, September 27, 1996.
13. Shlaes DM, Gerding DN, John JF, Craig WA,Bornstein DL, Duncan RA, et al. Society forHealthcare Epidemiology of America and InfectiousDiseases Society of America Joint Committee on theprevention of microbial resistance: guidelines for theprevention of antimicrobial resistance in hospitals.Infect Control Hosp Epidemiol 1997;18:275–291.
14. Chadwick D, Goode J, editors. Antibiotic resistance:origins, evolution, selection and spread. Proceedingsfrom a Ciba Foundation Syposium, London July 16–18, 1996.John Wiley & Sons, Inc. 1997.
15. World Health Organization. The current status ofantimicrobial resistance surveillance in Europe. Re-port of a World Health Organization workshop incollaboration with the Italian Associazone CulturaleMicrobiologia Medica; 1997 Dec 12; Verona, Italy.Geneva, World Health Organization, Geneva 1998.WHO/EMC/BAC/98.1.
16. Proceedings of the international conference onemerging infectious diseases, Atlanta, March 1998.Emerging Infectious Diseases, special issue.
17. Centers for Disease Control and Prevention. Pre-venting emerging infectious diseases: a strategy forthe 21st century, 1998.
18. Food and Drug Administration. Antibacterial drugsin animal feeds. Human health safety criteria guide-line 18, 1998.
19. Department of Health, UK. The path of least resist-ance. Main report of the Standing Medical Advi-sory Committee, Sub-Group on AntimicrobialResistance. London, UK: Department of Health;1998.
20. Antimicrobial resistance. Br Med J 1998 Sep;317:609–690.
21. House of Lords, UK. Resistance to antibiotics andother antimicrobial agents. Seventh Report of theHouse of Lords’ Select Committee on Science andTechnology; 1997–98. London, UK: The Station-ary Office; 1998.
1. Levy SB, Burke JP, Wallace CK, editors. Antibioticuse and antibiotic resistance worldwide: report of astudy sponsored by the Fogarty International Centerof the National Institutes of Health, 1983–1986.Rev Infect Dis 1987; 9(suppl3):231–316.
2. Public Health Service USA. Healthy People 2000:National Health Promotion and Disease Prevention.Full report with Commentary, 1990.
3. Lederberg J, Shope RE, Oats SC, editors. Emerginginfections: microbial threats to health in the UnitedStates. Report from the Institute of Medicine Com-mittee on Emerging Microbial Threats to Health.Washington, DC: National Academy Press; 1992.
4. Centers for Disease Control and Prevention.Addressing emerging infectious disease threats: aprevention strategy for the United States. 1994.
5. World Health Organization. Proceedings of theWHO Scientific Working Group on Monitoring andManagement of Bacterial Resistance to Antimicro-bial Agents; 1994 Nov 29–Dec 2; Geneva, Switzer-land. Geneva Switzerland: World HealthOrganization; 1995.
6. Office of Technology Assessment, US Congress.Impacts of antibiotic-resistant bacteria. Washington,DC: US Government Printing Office; 1995.
7. National Science and Technology Council, US. In-fectious disease—a global health threat. Report ofthe National Science and Technology Council Com-mittee on International Science, Engineering, andTechnology Working Group on Emerging and Re-emerging Infectious Diseases. Washington DC: USGovernment Printing Office; 1995.
8. American Society for Microbiology. Report of theASM taskforce on antibiotic resistance. Proceedingsof the American Society for Microbiology; 1994 Jul6; Washington, DC. Washington DC: Office ofPublic Affairs, American Society for Microbiology;1995.
9. World Health Organization. The medical impact ofthe use of antimicrobials in food animals. Reportand proceedings of a WHO meeting, Berlin, Ger-many, 13–17 October 1997. WHO/EMC/ZOO/97.4.
10. Institute of Medicine. America’s vital interest inglobal health, report of a workshop, November 1995.
11. American Society for Microbiology. New andreemerging infectious doseases: a global crisis and
83
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
84
22. Harrison PF, Lederberg J, editors. Antimicrobial re-sistance: issues and options, workshop report. Pro-ceedings of the Forum on Emerging Infections ofthe Division of Health Sciences Policy, Institute ofMedicine; 1997 Jul. Washington DC: NationalAcademy Press; 1998.
23. Centers for Science in the Public Interest. Protect-ing the crown jewels of medicine: a strategic plan topreserve the effectiveness of antibiotics. 1998.
24. General Accounting Office. The agricultural use ofantibiotics and its implications for human health.1999.
25. National Research Council. The use of drugs in foodanimals: benefits and risks.1999.
26. WHO Global Strategy for the Containment of Anti-microbial Resistance. World Health Organization2001. WHO/CDS/CSR/DRS/2001.2.
27. World Health Organization. WHO internationalcollaborative study of antibiotic sensitivity testing,1968–1970. In: ACTA et Microbiologia Scandina-via. Suppl 217; Sec B; 1971.
28. World Health Organization. WHO scientific work-ing group on microbial resistance. Proceeds from aworking group; 1981 Nov 23–27; Geneva, Switzer-land. Geneva, Switzerland: World Health Organi-zation; 1982.
29. World Health Organization. WHO consultationgroup for surveillance of antimicrobial resistance.Proceedings from a conference of the World HealthOrganization; 1982 Nov 22–26; Geneva, Switzer-land. Geneva, Switzerland: World Health Organi-zation; 1982.
30. American Academy of Microbiology. Report fromthe American Academy of Microbiology: antimicro-bial resistance, an ecological perspective. Washing-ton DC: American Society of Microbiology; 1999.
31. US Interagency Task Force on Antimicrobial Resist-ance. Draft public health action plan to combat an-timicrobial resistance. Proceeds from a task forceco-chaired by the Centers for Disease Control andPrevention, the Food and Drug Administration, andthe National Institutes of Health; 1999. Draft forcomment; 2000.
32. Avorn JL, Solomon DH. Cultural and economicfactors that (mis)shape antibiotic use: the non-pharmacologic basis of therapeutics. Ann Intern Med2000;133:128–135.
33. Metlay JP, Stafford RS, Singer DE. National trendsin the use of antibiotics by primary care physiciansfor adult patients with cough. Arch Intern Med1998;158:1813–1818.
34. Gonzales R, Steiner JF, Sande MA. Antibiotic pre-scribing for adults with colds, upper respiratory tractinfections, and bronchitis by ambulatory care phy-sicians. JAMA 1997;278:901–904.
35. Avorn, J, et al. Information and education as deter-minants of antibiotic use: report of task force 5. RevInfect Dis 1987;9:S286–S296.
36. Wilson AA, Crane LA, Barrett PH, Gonzales R.Public beliefs and use of antibiotics for acute respi-ratory illness. J Gen Intern Med 1999;14:658–662.
37. Watson RL et al. Antimicrobial use for pediatricupper respiratory infections: reported practice,actual practice, and parent beliefs. Pediatrics 1999;104:1251–1257.
38. Bell RA, Kravitz RL, Wilkes MS. Direct-to-consumer prescription drug advertising and the pub-lic. J Gen Intern Med 1999;14:651–657.
39. US Agency for International Development. Reduc-ing the threat of infectious diseases of major publichealth importance: USAID’s initiative to prevent andcontrol infectious diseases. Manuscript; 1998.
40. Davis DA, Thomson MA, Oxman AD, Haynes RB.Changing physician performance. A systematic re-view of the effects of continuing medical educationstrategies. JAMA 1995;274:700–705.
41. Soumerai SB, Avorn J. Economic and policy analy-sis of university-based drug “detailing.” Med Care1986;24:313–331.
42. Green LW and Kreuter MW. Health PromotionPlanning: an Educational and EnvironmentalApproach. Mountain View, Calif.: Mayfield Publish-ing Co., 1991.
43. Prochaska JO, DiClemente CC, Norcross JC. Insearch of how people change. American Psychologist1992;47:1102–1114.
44. Ross-Degnan D, Laing R, Santoso B, Ofori-AdjeiD, Diwan V, Lamoureux C, Hogerzeil H. Improv-ing pharmaceutical use in primary care in develop-ing countries: a critical review of experience and lackof experience. Prepared for the International Con-ference on Improving Use of Medications; 1997;Chaing Mai, Thailand.
45. Pestonik SL, Classen DC, Evans RS, Burke JP.Implementing antibiotic practice guidelines throughcomputer-assisted decision support: clinical andfinancial outcomes. Ann Intern Med 1996;124:884–890.
46. Pestonik SL et al. Therapeutic antibiotic monitor-ing: surveillance using a computerized expertsystem. Am J Med 1990;88:43–48.
47. Shojania KG et al. Reducing vancomycin use utiliz-ing a computer guideline: results of a randomizedcontrolled trial. J Amer Med Inform Assoc 1998;5:554–562.
48. Gonzales R et al. Decreasing antibiotic use inambulatory practice: impact of a multidimensionalintervention on the treatment of uncomplicatedacute bronchitis in adults. JAMA 1999;281:1512–1519.
85
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
49. Overcoming antimicrobial resistance. World HealthOrganization, Geneva, Switzerland 2000.
50. World Health Organization. Containing antimicro-bial resistance: review of the literature and report ofa WHO workshop on the development of a globalstrategy for the containment of antimicrobial resist-ance. Proceedings of a WHO workshop; 1999 Feb4–5; Geneva, Switzerland. Geneva, Switzerland:World Health Organization; 1999. WHO/CDS/CSR/DRS/99.2.
51. Fidler DP. Legal issues associated with antimicro-bial drug resistance. Emerg Infect Dis 1998;4:169–177.
52. Codex Alimentarius. FAD/WHO Standards. CodexCommittee on residues of veterinary drugs in foods.Discussion paper on antimicrobial resistance. Draft-ing group meeting, May 15–16, 2001.
53. Centers for Disease Control and Prevention. Publichealth action plan to combat antimicrobial resist-ance. Atlanta, GA: Centers for Disease Control andPrevention; draft manuscript; 2000.
54. Cohen ML. Changing patterns of infectious diseases.Nature 2000;406:762–767.
55. Dougherty TJ et al. Antimicrobial resistance-why dowe have it and what can we do about it? Exp OpinInvest Drugs 2000;9:1707–9.
56. Bjorkman J, Anderson DJ. The cost of antibioticresistance from a bacterial perspective. Drug Resist-ance Update 2000;3:327–345.
57. Mazel D, Davies J. Antibiotic resistance: the big pic-ture. Adv Exp Med Biol 1998;456:1–6.
58. Liu HH. Antibiotic resistance in bacteria: a currentand future problem. Adv Exp Med Biol. 1999;455:387–396.
59. Guillemot D. Antibiotic use in humans and bacte-rial resistance. Curr Opin Microbiol 1999;2:494–498.
60. Barker KF. Antibiotic resistance: a current perspec-tive. Br J Clin Pharmacol 1999;48:109–124.
61. Phillips I. The subtleties of antibiotic resistance.J Antimicrob Chemother 1998;42:5–12.
62. Levy SB. Antimicrobial resistance: bacteria on thedefense. Resistance stems from misguided efforts tosterilize our environment. BMJ 1998;217:612–613.
63. Rao GG. Risk factors for the spread of antibiotic-resistant bacteria. Drugs 1998;55:323–330.
64. Bergogne-Berezin E. Who or what is the source ofantibiotic resistance? J Med Microbiol 1997;46:461–464.
65. Kumar A. Microbial resistance to drugs—a univer-sal problem in urgent need of a comprehensiveapproach. Natl Med J India 1997;10:221–224.
66. Baquero F, Nergi MC. Strategies to minimize thedevelopment of antibiotic resistance. J Chemother1997;9(suppl3):29–37.
67. Levy SB. Antibiotic resistance: an ecological imbal-ance. Ciba Found Symp 1997;207:1–9.
68. Postier RG. Antibiotic-resistant organism infection.Am Surg 2000;66:112–116.
69. Lipsitch M, Bergstrom CT, Levin BR. The epide-miology of antibiotic resistance in hospitals: para-doxes and prescriptions. PNAS 2000;97:1938–1943.
70. Institute of Medicine. Emerging infections: micro-bial threats to health in the United States. Washing-ton, DC: National Academy Press; 1992.
71. Wise R et al. Antimicrobial resistance is a majorthreat to public health. BMJ 1998;317:609–610.
72. Wise R. The development of new antimicrobialagents. BMJ 1998;317:643–644.
73. Huovinen P, Cars O. Control of antimicrobial re-sistance: time for action. The essentials of controlare already known. BMJ 1998;317:613–614.
74. Eandi M, Zara GP. Economic impact of resistancein the community. J Clin Pract 1998;95(JunSuppl):27–38.
75. Nathwani D, Malek M. Cost considerations in theevaluation of new therapies for Gram-positivebacteria. Int J Antimicrob Agents 1999;13:71–78.
76. Wright GD. Resisting resistance: new chemical strat-egies for battling superbugs. Chem Biol 2000;7:R127–132.
77. Urassa W, Lyamuya E, Mhalu F. Recent trends onbacterial resistance to antibiotics. East Afr Med J1997;74:129–133.
78. Fauci AS. New and reemerging diseases: the impor-tance of biomedical research. Emerg Infect Dis1998;4:374–378.
79. Relman DA. Detection and identification of previ-ously unrecognized microbial pathogens. EmergInfect Dis 1998;4:382–389.
80. Sentry: http://www.ewi.med.uu.nl/enare/sentry_antimicrobial_surveillance.html
81. Alexander project : http://www.nearchus.com
82. NIH funding data; public domain through websearching.
83. Parexels Pharmaceutical R&D Statistical Source-book. 2000.
84. Bax R. Antibiotic resistance: a view from the phar-maceutical industry. Clin Inf Dis 1997;24:S151–S153.
85. Culotta E. Funding crunch hobbles antibioticresistance research. Science 1994;264:362–363.
86. Walsh C. Molecular mechanisms that confer anti-bacterial drug resistance. Nature 2000;406:775–781.
87. Kessler RE. Perspective on chemotherapeuticapproaches to antibiotic-resistant bacteria. Clin InfDis 1997;24(Suppl 1):S146–S147.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
86
88. Kotra LP, Vakuleno S, Mobashery S. From genes tosequences to antibiotics: prospects for future devel-opment of microbial genomics. Microbes Infect2000;2:651–658.
89. McKeller QA. Antimicrobial resistance: a veterinaryperspective. Antimicrobials are important for ani-mal welfare but need to be used prudently. BMJ1998;317:610–611.
90. Mawle AC. Vaccine-preventable diseases. EmergInfect Dis 1998;4:404.
91. Levy SB. The challenge of antibiotic resistance. SciAmer 1998;278(3):46–53.
92. Advisory Committee on the Microbiological Safetyof Food, UK. Report on Microbial AntibioticResistance in Relation to Food Safety. London, UK:The Stationery Office; 1999.
93. Joint Expert Advisory Committee on AntibioticResistance (JETACAR). The use of antibiotics infood-producing animals: antibiotic resistant bacte-ria in animals and humans. Australia: Common-wealth Department of Health and Aged Care,Commonwealth Department of Agriculture, Fish-eries and Forestry; 1999.
94. World Health Organization. WHO global princi-ples for the containment of antimicrobial resistancein animals intended for food. report of a WHO con-sultation 5–9 June 2000.Geneva, Switzerland.WHO/CDS/CSR/APH/2000.4.
95. European Commission, Scientific Steering Commit-tee. Opinion of the Scientific Steering Committeeon antimicrobial resistance. Brussels: EuropeanCommission, Directorate-General DGXXIV; 1999.
96. Health, Education, and Human Services Division,USA General Accounting Office. Antimicrobialresistance: data to assess public health threat fromresistant bacteria are limited. Washington, DC:USA General Accounting Office; 1999.
97. Report of the Jt. Committee on the use of Antibi-otics in Animal Husbandry and Veterinary Medi-cine. Chairman Professor M. Swann, Cmnd 4190.The Stationary Office, London UK, 1969.
98. Greko C. Sweden and the European Union: whatis happening in relation to antibiotics in feed. In:Annual conference proceedings of Australianveterinarians in industry and Australian veteri-natrians in public health. Proceedings of Austral-ian Veterinarian Association Annual Conference;2000 June 26–30; Perth, Australia. 2000. p. 18–22.
99. Bager F, editor. DANMAP99. Danish ZoonosisCentre, Danish Veterinary Laboratory, bulowsvej27 DK-1790 Copenhagen V, Denmark. (http://www.svs.dk).
100. Fey PD et al. Ceftriaxone-resistant Salmonella in-fection acquired by a child from cattle. N Engl JMed 2000; Apr 27;342:1242–1249.
101. Rosdahl VT, Knudson AM. The decline of methi-cillin resistance among Danish Staphylococcusaureus strains. Infect Control Hosp Epidemiol 1991;12:83–88.
102. Thomas M, editor. Guidelines to antibiotic policy.Proceedings from a workshop of the World HealthOrganization in collaboration with the ChristianMedical College; 1998 Jan 22–23; Vellore, India.Emppee Graphics;1998.
87
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Some useful web sites
■ Alliance for the Prudent Use of Antibioticswww.apua.org
■ BUBL Catalog of Internet Resources—Infectious Diseaseshttp://bubl.ac.uk/link/i/infectiousdiseases.htm
■ Canadian Committee on Antibiotic Resistancehttp://www.ccar-ccra.org
■ Center for Adaptation Genetics and Drug Resistancehttp://www.healthsci.tufts.edu/labs/Sblevy/home.html
■ Center for Complex Infectious Diseaseshttp://www.ccid.org/
■ Centers for Disease Control and Preventionwww.cdc.gov
■ Eurosurveillancehttp://www.eurosurv.org/
■ Global Polio Eradication Initiativehttp://www.polioeradication.org
■ National Institute of Allergy and Infectious Diseaseswww.niaid.nih.gov/factsheets/antimicro.htm
■ Infectious Disease Newshttp://www.slackinc.com/general/idn/idnhome.htm
■ Infectious Diseases Society of Americawww.journals.uchicago.edu/IDSA/guide/SE39_584.pdf
■ International Society for Infectious Diseaseshttp://www.isid.org
■ Johns Hopkins University—Infectious Diseaseshttp://www.hopkins-id.edu/index_id_links. html
■ Karolinska Institut, Swedenhttp://micf.mic.ki.se/Diseases/
■ National Foundation for Infectious Diseases, USAhttp://www.nfid.org/
■ Project Icare: Intensive Care Antimicrobial Resistance Epidemiologyhttp://www.sph.emory.edu/ICARE/
■ Roll Back Malariahttp://www.rbm.who.int/
■ TDR (Special Programme for Tropical Disease and Research)http://www.who.int/tdr
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
88
■ The Copenhagen Recommendations. http://www.sum.dk/publika/micro98These recommendations are a report from a conference on “The Microbial Threat,” which promotescollection of data concerning the supply and sales of antimicrobials from individual nations to be sharedinternationally.
■ The Epic Project: Developing National Evidence-Based Guidelines for Preventing Health-care-Associ-ated Infection.http://www.epic.tvu.ac.uk/
■ The Hot Zone: Emerging Infectious Diseases Reports and Web Siteshttp://www.qis.net/~edwardmc/eid.htm
■ The HELICS project: (Hospitals in Europe Link for Infection Control Through Surveillance).http://helics.univ-lyon1.fr
■ The MIKSTRA Programmehttp://www.stakes.fi/mikstra/e/
■ The Scottish Intercollegiate Guideline Network (SIGN) Guideline on Antibiotic Prophylaxis in Surgery.http://www.show.scot.nhs.uk/sign/home.htm.
This has national guidelines on antibiotic prophylaxis in surgery which addresses the benefits and risksinvolved in using antibiotics to prevent surgical site infections.
■ The Swedish Strategic Program for the Rational Use of Antimicrobial Agents and Surveillance of Resist-ancehttp://www.strama.org
■ UK Public Health Laboratoryhttp://www.phls.co.uk/
■ UK Public Health Laboratory Service’s Management of Infection Guidance for Primary Care.http://www.phls.co.uk/advice/antibiotic/old/phls%20antibiotic%20guides%20refs% 2009.01.01.rtf
The guidance template found on the website is designed so that the antibiotics and advice given may bechanged to suit local circumstances, for example to reflect laboratory resistance data and cost.
■ USA National Center for Infectious Diseaseshttp://www.cdc.gov/ncidod
■ Washington University Infectious Disease Divisionhttp://www.id.wustl.edu/
■ World Health Organizationhttp://www.who.int/
■ WHO Antimicrobial Resistance InfoBankhttp://oms2.b3e.jussieu.fr/arinfobank/
■ WHO Communicable Diseases home pagehttp://www.who.int/health-topics/idindex.htm
89
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
APPENDIX A
Summaries of reports by expert policy groups(1987–2000)
• Support for and expansion of WHO’s surveil-lance program for the global prevalence of anti-bacterial resistance.
• Studies on the mechanics of antibiotic resistanceon the level of genetic elements, in order todevise plans on how to contain and reduce re-sistance.
• Research studies on antibacterial regulation thatinclude the following:— Long-term, multicountry studies to deter-
mine whether or not regulation of antibi-otic use and the enforcement of such ruleshave any effect on the development of anti-biotic resistance.
— Studies of the consequences of implement-ing restrictive regulations and enforcement,including the need to train health care per-sonnel and possible economic impacts.
— Studies that specifically examine the effectsthat regulations and enforcement have onchildren.
— Investigation of the potential consequencesto human health that would arise fromrestrictions on antibacterial use in foodproduction and animal husbandry.
— Studies that examine how national, regional,and institutional antibiotic use policies in-fluence the training and education of physi-cians and other health care workers.
• Improved communications between the regula-tory agencies that govern antibacterial use, andthe people responsible for prescribing and usingsuch agents.
• Research studies on antibacterial use in devel-oping countries that include the following:— Studies that determine the efficacy of
national formulary schemes, including drugcosts, availability, as well as research and de-velopment of new agents.
— Studies on the effects that having access tomicrobiology laboratory tests has on antibi-otic prescription and use.
• Redesign of the curricula of medical schools indeveloping countries to provide more thorough
(1) *Task Force Reports on Antibiotic Useand Resistance Worldwide (FogartyReport)
Organization: National Institutes of Health, FogartyCenter
Year published: 1987
Selected key findings• Antibiotic use varies greatly from country to
country; surveillance data on antibiotic use,emergence of resistant strains, and availabilityto consumers were difficult or impossible toobtain.
• Practitioner knowledge, drug availability, anddrug price are the three key factors that influ-ence a prescriber’s choice of antibiotics. Whereantibiotics are available without a prescription,the same factors influence the choice of theconsumer.
• The task force did not find enough evidence toprove that the implementation of firmerregulations regarding antibiotic use, or stricterenforcement of or better compliance with suchregulations, slows the development or spread ofresistance.
• Medical students in developing countries oftenreceive inadequate training in basic bacteriology,infectious diseases diagnosis, and antimicrobialuse. Theories of antimicrobial therapy are notalways integrated with practical experience.
• There are almost no regulated requirements forhealth care providers to continue their educa-tion in pharmacological developments beyondtheir formal training. This lack is evident in bothdeveloping and industrialized countries.
Key recommendations• Uniform data-collection systems at the national
level.
* The number in parenthesis refers to the citation listed inReferences.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
90
education on diagnosing and managing infec-tious diseases.
• Creation of systems which will disseminateinformation on patterns of antibiotic use anddevelopment of antibiotic resistance to hospitalstaff.
• Research studies on the effects of education andinformation on determining antibiotic use,including: cultural and social reasons behindpatient demand; the quality of physician educa-tion on the use of antibiotics, both during thecourse of study and after graduation; and theeffects of pharmaceutical marketing campaignson physicians’ prescriptions of antibiotics.
• Evaluation of current policies on the use ofantibiotics to determine what effects they haveon the pharmaceutical industry’s incentives toresearch, develop, and market new antibiotics.
Implementation suggestions• To achieve standardized data on antibiotic use,
institute “a standard index for measuring druguse in each country by using the same system ofdrug classification, the same unit of measure-ment (e.g., DDDs/1,000 population per day orgrams/1,000 population per day), and the samepoint in the distribution channel in each coun-try [and] by obtaining access to data of this typethat are currently collected by private compa-nies (i.e., International Medical Statistics) butare not made publicly available.”
• WHO, USA Public Health Service, and minis-tries of health in other countries “should sup-port research studies proposed by the task force,assist countries in establishing or improving theirsystems of drug regulation, facilitate collabora-tive research among investigators in differentcountries, and improve cooperation among regu-latory agencies, physicians and other healthworkers, and drug companies.”
• Regional and international centers for the studyof antibiotic resistance should be established inAsia, Africa and Latin America by WHO, NIH,and CDC/USA Public Health Service/USADepartment of Health and Human Services, incollaboration with ministries of health and otherrelevant agencies.
• “Establishment of field surveillance teamslocated in representative regions in developingnations. Such teams would gather informationon actual antibiotic use, develop affordable strat-egies for preventing or curing infectious diseases,and determine the social, behavioral, and eco-
nomic determinants of antibiotic usage forparticular geographic areas and demographicgroups.”
Conclusions“The importance of social and behavioral charac-teristics of individuals receiving antimicrobialtherapy (as well as the supply and variety of antibi-otics available) was noted in plenary discussions asinfluencing courses of antibiotic therapy. Studiesof such variables are needed in order to answerquestions related to under- or overutilization ofantibiotics.”
“There was the consensus that there is consider-able suboptimal antibiotic use in the developingcountries, where there is a tendency...for higher lev-els of microbial resistance... The developing nationshave environmental conditions, infectious diseaseburdens, and associated needs and factors affectingantibiotic use and resistance patterns that differfrom those in the developed nations. The partici-pants in this project stressed the importance of rec-ognizing and addressing these distinctions.”
“Better data on utilization of antimicrobialagents in the developing world are needed. Thiswould include information from studies on themagnitude of inadequate doses resulting in thefailure to achieve bactericidal concentrations, onimproper duration of therapy...and on the use of asingle capsule or a limited number of capsules...forcultural, financial, or idiosyncratic reasons (associ-ated with a transient sense of well-being).”
“Projects focusing on improving our understand-ing of the observed correlation between antibioticuse and subsequent resistance should be carriedout... Multiple parameters should be assessed:microbiologic susceptibility patterns of the organ-isms principally involved; the kinds of diagnostictests being performed; demographic patterns andassociated social and behavioral characteristics;policies affecting antibiotic utilization; and thequantity and cost of antibiotics used. Such dataassembled in one system have heretofore not beenavailable.”
“What is lacking, and of fundamental impor-tance, is detailed information on the distributionover time of specific antimicrobial resistance genesand plasmids in the global bacterial ecosystem.Geographic information on individual compo-nents... is needed to trace and understand betterthe emerging patterns of such resistance.”
“Some unified way to follow the incidence andprevalence of microbial resistance on a global scale

91
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
is required; however, it is not yet clear how best toproceed... It is, therefore, recommended that aworkshop be convened to help elucidate the direc-tion in which future surveillance studies shouldproceed, as well as to work out the details of a uni-form methodology for collection and comparisonof data.”
“Fundamental studies at the cellular level con-cerning the cell’s impressive capacity over time todefend itself against foreign agents should be sup-ported and extended, particularly studies involv-ing genetics and mechanisms for gene amplificationand gene exchange leading to multidrug resistance.”
“New diagnostic tools, simplified, appropriate,and more accurate and sensitive than tests currentlyavailable, are coming into use. The utilization ofthese newer techniques at the central surveillancelevel needs to be encouraged. These central surveil-lance systems, particularly those focusing onselected and important infectious disease in thedeveloping nations...and on specific etiology agents...should be expanded.”
“Vaccine development and newer, more rapiddiagnostic tests should provide additional meansto combat the problem. Economic conditions anda climate favorable for the continued progress andexpansion of medical therapeutics, as well as thewidespread utilization of new antimicrobial agents,remain important factors in considering antibioticuse and antibiotic resistance worldwide.”
Authors: Task Force participants: Stuart B. Levy (Gen-eral Chairperson and Guest Editor), Jacques F. Acar,Gianni Acocella, Jerry Avorn, Ingebjorg Baksaas,Fernando Baquero, Gilles Bardelay, F. Ralph Batchelor,Karen Bell, Ulf Bergman, Enriquetta Bond, KennethBridbord, James J. Burchall, John P. Burke (GuestEditor), Felipe C. Cabello, Charles C.J. Carpenter III,Georges Y. Causse, Leighton E. Cluff, Mitchell Cohen,Nananda F. Col, John V. Copeland, George Curlin,Joseph T. Curti, I. Damansjah, F. Daschner, Irving P.Delappe, M.N.G. Dukes, John M. Eisenberg, TamaraErickson, Enrique Feffer, Susan E. Feinman, Peter I.Folb, Ernst Freese, Ryochi Fujii, Aleksander Goic, JulioGonzales-Molina, Joseph E. Grady, Richard L.Guerrant, Richard Gustafson, Ken Harvey, AndrewHerxheimer, Scott D. Holmberg, M. Imdadul Huq,Hu Zhen, N. Islam, John E. Jefferis, Amir Jivani, BengtJönsson, William S. Jordan, Jr., Edward H. Kass,Dianne Kennedy, Thomas Kereselidze, H.H.Kleeberg, Dieter Koch-Weser, Goran Kronvall, CalvinM. Kunin, Yankel M. Kupersztoch, Louis Lasagna,Norman W. Lavy, Donald Le Blanc, David Lee, Philip
R. Lee, Alan H. Linton, Helen Levens Lipton, RobertH. Liss, Hubert Loncin, Per Knut Lunde, Edgar J.Martin, R. Russel Martin, Ramiro Martines-Silva,Charles Medawar, Dianna Melrose, Arnold S. Monto,Stuart L. Nightingale, Richard Norton, Thomas F.O’Brien, Ronald W. O’Connor, Makoto Ohashi, JorgeOlarte, Nancy Olins, Peng Wen Wei, Maria EugeniaPinto, Philip A. Pizzo, Richard J. Plumridge, WayneRay, J.P Revill, Ahmed Rhazaoui, Frederick C.Robbins, O.P.W. Robinson, Heonir Rocha, VidalRodriguez-Lemoine, Bernard Rowe, T. DonaldRucker, Theodore Sacks, Jay P. Sanford, WilliamSchaffner, William E. Scheckler, Roy Shaffer, K.B.Sharma, Richard P. Silver, Harold J. Simon, Ewe HuiSng, Stephen B. Soumerai, Visanu Thamlikitkul, JohnF. Timoney, A. Tognoni, Luiz R. Trabulsi, ThemlmaTupasi, John R. Virts, V. Vymola, Craig K. Wallace(Guest Editor), Wang Fu, Bernd Wiedemann, SidneyWolfe
Type of publication: Supplement to Reviews of Infec-tious Diseases; Volume 9, Supplement 3, May–June1987
Pages: 89
Intended audience: International; policy-makers, gov-ernment, health care providers
Study timeframe: The Task Forces met between fallof 1983 and spring of 1986.
Study process: Six task forces were assembled, com-prised of representatives from different disciplinesand countries. Each Task Force focused on a dif-ferent aspect of antibiotic resistance; they developedtheir sections of the report over a year and a half ofmeetings and revisions.
Type of organization: Professional society
Languages (published in): English
Key contactOrdering information: International StudiesBranch, Fogarty International Center, Bethesda,MD 20892Content: Stuart Levy, General Chairperson for theTask Force

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
92
(2) Healthy People 2000: National HealthPromotion and Disease Prevention. Fullreport, with commentary
Organization: Public Health Service; USA Depart-ment of Health and Human Services
Year published: 1990
Selected key findings• Patients in hospital Intensive Care Units account
for about 15% of hospital admissions, but atleast 50% of nosocomial infections (data from1990).
• Approximately 40,000 people die each year fromcomplications arising from pneumococcaldisease.
Key recommendationsBy the year 2000:• “Reduce by at least 10 % the incidence of surgi-
cal wound infections and nosocomial infectionsin intensive care patients;
• Reduce acute middle ear infections among chil-dren aged 4 and younger, as measured by daysof restricted activity or school absenteeism, tono more than 105 days per 100 children;
• Increase to at least 90 % the proportion of pub-lic health departments that provide adultimmunization for influenza, pneumococcaldisease, hepatitis B, tetanus, and diphtheria;
• Develop a set of health status indicators appro-priate for Federal, State, and local health agenciesand establish use of the set in at least 40 states.”
Implementation suggestionsReduction of nosocomial infections to be achievedthrough collaboration of hospital epidemiologists,infection control practitioners, the Association ofPractitioners in Infection Control, Society of Hos-pital Epidemiologists of America, Surgical Infec-tion Society, American Hospital Association, JointCommission on the Accreditation of Health CareOrganizations, and the Health Care FinancingAdministration.
Conclusions/Executive Summary“In addition to application of specific measures,such as immunization and regulation of food,water, and sewage disposal, there is a need for con-tinued public education about basic hygienicpractices, in home, school, and occupational set-tings; for continued education of health carestudents and workers about the epidemiology and
prevention of these diseases; and for research toimprove immunizations, diagnostic methods, andtherapeutic modalities.”
Authors: Principal staff/editors: James A. Herrell, LynnM. Artz, Ashley Files, David Baker. Project Coordinationand Development: Barbara Anderson, John Bailar, Am-ber Barnato, Sandra Buesking, Mary Jo Deering,Christopher DeGraw, Olga Emgushov, Martha G.Grazier, Toni M. Goodwin, Linda M. Harris, Doug-las B. Kamero, Thomas Kim, Loretta M. Logan,Patricia Lynch, Caroline McNeil, Linda D. Meyers,Diane Rittenhouse, Marilyn K. Schulenberg, Sara L.White, Jennifer Woods, Christina Wypijewski,Michael Yao, Daniel Yarano
Type of publication: Report
Pages: 692
Intended audience: United States; citizens, policy-makers
Study timeframe: N/A
Study process: The report is the result of a collabora-tion of 22 expert working groups, a consortiumincluding almost 300 national organizations andall state health departments, and the Institute ofMedicine of the National Academy of Sciences. TheIOM and the USA Public Health Service heldregional and national hearings and gathered testi-mony from over 750 individuals and organizations.More than 10,000 people participated in the pub-lic review, after which the objectives were revisedand refined.
Type of organization: United States Federal Govern-ment
Languages (published in): English
Key contactOrdering Information: Superintendent of Docu-ments, Government Printing Office, Washington,DC 20402-9325; tel.: (202) 783-3238; fax:(202)275-0019.
(3) Emerging Infections: Microbial Threatsto Health in the United States
Organization: Institute of Medicine
Year published: 1992
Selected key findingsThe Committee focused on factors that contributeto the emergence and re-emergence of infectiousdiseases, including:

93
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
• Human demographics and behavior. Contribut-ing factors are movement of the ever-growingglobal population into urban areas, with corre-sponding crowded conditions, poor hygiene andsanitation, and lack of clean water supplies; in-creasing numbers of people with suppressedimmune systems, including the elderly andpeople infected with HIV; and the transmissionof disease through sexual activity and substanceabuse.
• Technology and industry. Hospitals are increas-ingly implicated as sources of infection; manynosocomial infections have developed resistanceto antibiotics thanks to the combination of apopulation very susceptible to infection, and thewidespread therapeutic and prophylactic use ofantibiotics.
• Microbial adaptation and change. The evolution-ary mechanisms of microbial pathogens allowthem to adapt to new host cells or host species,produce “new” toxins, bypass or suppress inflam-matory and immune responses, and developresistance to drugs and antibodies.
• Breakdown of public health measures. Inadequatesanitation, complacency on the part of medicalofficials, physicians, researchers and other pub-lic health workers, war, economic hardship, andnatural disasters may all undermine any progressmade by advances in science and technology.
Key recommendations• “The committee recommends the development
and implementation of strategies that wouldstrengthen state and federal efforts in USA sur-veillance. Strategy development could be a func-tion of the Centers for Disease Control (CDC).Alternatively, the strategy development and co-ordination functions could be assigned to a fed-eral coordinating body (e.g., a subcommittee ofthe Federal Coordinating Council for Science,Engineering, and Technology’s Committee onLife Sciences and Health), specifically consti-tuted to address this issue.”
• “The committee recommends that additionalresources be allocated to the to the Centers forDisease Control to enhance the National Noso-comial Infections Surveillance System in thefollowing ways:— Include data on antiviral drug resistance.— Include information on morbidity and mor-
tality from nosocomial infections.— Increase the number of NNISS member
hospitals.
— Strive to make NNISS member hospitalsmore representative of all USA hospitals.
— Evaluate the sensitivity and specificity ofnosocomial infection surveillance activitiesperformed in NNISS member hospitals.
— Determine the reliability of antimicrobialsusceptibility testing performed in NNISSmember hospitals.”
• “The committee recommends that the USAPublic Health Service develop a comprehensive,computerized infectious disease database.”
• “The committee recommends that internationalinfectious disease surveillance activities of USAgovernment agencies be coordinated by theCenters for Disease Control (CDC). Alterna-tively, a federal coordinating body could beassigned the coordinating function. Implemen-tation of surveillance activities, however, shouldremain with the appropriate federal agencies(e.g., the CDC, Department of Defense,National Institutions of Health, USA Depart-ment of Agriculture).”
• “The committee recommends that the UnitedStates take the lead in promoting the develop-ment and implementation of a comprehensiveglobal infectious disease surveillance system.Such an effort could be undertaken through theUSA representatives to the World HealthAssembly.”
• “The committee recommends the expansion andcoordination of National Institutes of Health-supported research on the agent, host, vector,and environmental factors that lead to emer-gence of infectious diseases. Such research shouldinclude studies on the agents and their biology,pathogenesis, and evolution; vectors and theircontrol; vaccines; and antimicrobial drugs. Oneapproach might be to issue a request for pro-posals (RFP) to address specific factors relatedto infectious disease emergence.”
• “The committee recommends increased researchon surveillance methods and applied controlstrategies; on the costs and benefits of preven-tion, control, and treatment of infectious dis-ease; and on the development and evaluation ofdiagnostic tests for infectious diseases. Reinstat-ing and expanding (both in size and scope) theextramural grant program at the Centers forDisease Control, which ceased in 1973, wouldbe one important step in this direction. Simi-larly, the Food and Drug Administration’s (FDA)extramural grant program should be expandedto place greater emphasis on the development

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
94
of improved laboratory tests for detecting emerg-ing pathogens in food.”
• “The committee recommends the domestic andglobal expansion of the CDC’s Epidemic Intel-ligence Service program and continued supportfor Centers for Disease Control’s (CDC) role inthe Field Epidemiology Training Program.”
• “The committee recommends continuedsupport, at a minimum at their current level offunding, of Department of Defense overseas in-fectious disease laboratories.”
• “The committee recommends that Congressconsider legislation to fund a program, modeledon the National Health Service Corps, for train-ing in public health and related disciplines, suchas epidemiology, infectious diseases, and medi-cal entomology.”
• “The committee recommends that clinicians, theresearch and development community, and theUSA government introduce measures to ensurethe availability and usefulness of antimicrobialsand to prevent the emergence of resistance. Thesemeasures should include the education of healthcare personnel, veterinarians, and users in theagricultural sector regarding the importance ofrational use of antimicrobials (to preclude theirunwarranted use), a peer review process to moni-tor the use of antimicrobials, and surveillanceof newly resistant organisms. Where required,there should be a commitment to publiclyfinanced rapid development and expeditedapproval of new antimicrobials.”
• “The committee recommends that the NationalInstitutes of Health give increased priority toresearch on personal and community healthpractices relevant to disease transmission. Atten-tion should also be focused on developing moreeffective ways to use education to enhance thehealth-promoting behavior of diverse targetgroups.”
Implementation suggestionsResponsibilities delegated to various governmentagencies and departments of the United States,primarily CDC and NIH.
Conclusions/Executive Summary“The key to recognizing new or emerging infec-tious diseases, and to tracking the prevalence ofmore established ones, is surveillance. A well-designed, well-implemented surveillance programcan detect unusual clusters of disease, documentthe geographic and demographic spread of an out-
break, and estimate the magnitude of the problem.It can also help to describe the natural history of adisease, identify factors responsible for emergence,facilitate laboratory and epidemiological research,and assess the success of specific intervention ef-forts. The importance of surveillance to the detec-tion and control of emerging microbial threatscannot be overemphasized. Effective interventionagainst [emerging] diseases necessitates coordinatedefforts by a variety of individuals, government agen-cies, and private organizations. The committeebelieves that the current USA capability for re-sponding to microbial threats to health lacksorganization and resources. Vaccines and antimi-crobial drugs have led to significant improvementsin public health in the United States and in manyother nations during the latter half of this century.Despite this encouraging history, the committee isconcerned that many of the vaccines and drugsavailable today are the same ones that have beenused for decades. It believes that there is a need toreview the present vaccine and drug armamentariawith a view toward improving availability andcapacity, as well as safety and efficacy.”
Authors: Edited by: Joshua Lederberg, Robert E. Shope,and Barry R. Bloom. Task Force Members: Robert L.Buchanan, John R. David, Ciro A. De Quadros,Patricia N. Fultz, John J. Holland, Dean T. Jamison,Edwin D. Kilbourne, Adel A.F. Mahmoud, GeraldL. Mandell, Stephen S. Morse, June E. Osborn,William C. Reeves, Philip K. Russell, Alexis Shelokov,P. Frederick Sparling, Andrew Spielman. Project Staff:Ruth Ellen Bulger, Polly F. Harrison, Stanley C. Oaks,Jr., Elizabeth E. Meyer, Nancy Diener, Greg W.Pearson.
Type of publication: Report
Pages: 294
Intended audience: Primarily the United States; policy-makers, lay public, government, scientists, physi-cians
Study timeframe: February 1991 to July 1992
Study process: 19-member multidisciplinary commit-tee convened to identify significant emerging in-fectious diseases, develop plans on how to deal withthem, and make recommendations on how toapproach similar threats in the future. The full com-mittee met four times during the 18-month study.Four task forces and subcommittees also formedaccording to specialties, and met to address morespecific topics.

95
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Type of organization: Non-profit public health andadvisory organization; advisor to Federal Govern-ment on issues of public health
Languages (published in): English
Key contactOrdering information: National Academy Press,www.nap.eduContent: Joshua Lederberg and Robert E. Shope,Committee Co-chairs
(4) Addressing Emerging InfectiousDisease Threats.A Prevention Strategyfor the United States
Organization: Centers for Disease Control and Pre-vention; National Center for Infectious Diseases
Year published: 1994
Selected key findingsSurveillance is the key to tracking the developmentand spread of infectious diseases, reservoirs of dis-ease, and antimicrobial drug resistance.
One weakness in the United States’ strategy tocontrol infectious diseases is the lack of multi-disciplinary approaches. The USA needs strongerconnections between laboratory science and pub-lic health practices, as well as economic analyses ofthe impacts of both infectious diseases and the in-terventions proposed to stop them.
Most federal government funds dedicated tosurveillance of infectious diseases at the state levelgo towards only four categories of disease: tuber-culosis, HIV/AIDS, sexually transmitted diseases,and certain vaccine-preventable diseases. This leavesa large number of other emerging infectious dis-eases under-funded and under-observed.
The current approach to public health in theUnited States (i.e., the focus on treatment ratherthan prevention; reactive rather than proactive poli-cies; and general complacency) leads to the emer-gence and spread of infectious diseases that oughtto be preventable.
Key recommendations• “Expand and coordinate surveillance systems for
the early detection, tracking, and evaluation ofemerging infections in the United States;
• Develop more effective international surveillancenetworks for the anticipation, recognition,control, and prevention of emerging infectiousdiseases;
• Improve surveillance and rapid laboratory iden-
tification to ensure early detection of antimicro-bial resistance;
• Strengthen and integrate programs to monitorand prevent emerging infections associated withfood/water, new technology, and environmen-tal forces;
• Strengthen and integrate programs to monitor,control, and prevent emerging vector-borne andzoonotic diseases;
• Expand epidemiologic and prevention effective-ness research;
• Improve laboratory and epidemiologic tech-niques for the rapid identification of new patho-gens and syndromes;
• Ensure timely development, appropriate use, andavailability of diagnostic tests and reagents;
• Use diverse communication methods for widerand more effective delivery of critical publichealth messages;
• Establish the mechanisms and partnerships neededto ensure the rapid and effective development andimplementation of prevention measures;
• Ensure the ready availability of the professionalexpertise and support personnel needed to bet-ter understand, monitor, and control emerginginfections;
• Make available state-of-the-art physical resources(laboratory space, training facilities, equipment)needed to safely and effectively support thepreceding goals and objectives.”
Implementation suggestions“Between 1994 and 1996, CDC intended to im-plement its recommendations by establishingpriority goals in the four areas of Surveillance,Applied Research, Prevention and Control, andInfrastructure. They include the following:• Strengthen notifiable disease surveillance at the
state and local levels;• Establish two physician-based Sentinel Surveil-
lance Networks to detect and monitor emerg-ing diseases;
• Establish four population-based Emerging In-fections Epidemiology and Prevention Centersto conduct focused epidemiology/preventionprojects emphasizing foodborne and waterborneinfectious diseases and potentially vaccine pre-ventable diseases;
• Strengthen and link four existing sites for aglobal consortium to promote the detection,monitoring, and investigation of infectionsemerging internationally that could affect thehealth of Americans;

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
96
• Reestablish an extramural program to supportemerging infectious disease prevention andcontrol activities, such as evaluating the role ofprescribing practices in the development ofantimicrobial drug-resistant pathogens;
• Initiate prevention effectiveness studies to assessthe impact of food preparation guidelines on theincidence of foodborne infections such as E. coliO157:H7 and Salmonella enteritidis;
• Develop additional means to deliver laboratoryand public health information informing healthprofessionals about emerging infections andantimicrobial drug resistance;
• Develop and implement guidelines for theprevention of opportunistic infections inimmunosuppressed persons;
• Provide state-of-the-art training in diagnosticevaluation and testing for medical laboratorypersonnel to ensure the diagnosis and surveil-lance of emerging infection;
• Establish a public health laboratory fellowshipin infectious diseases that will train medicalmicrobiologists in public health approaches todiagnosis and molecular epidemiology.”
Conclusions“As the United States moves towards comprehen-sive health care reform, it is crucial that emerginginfectious disease threats be addressed and that thebasic tenets of prevention-oriented public healthpolicy form an internal component of plans forhealth care reform.
Strengthened efforts in the prevention and con-trol of emerging infectious diseases will comple-ment and improve the effectiveness of currentefforts in HIV/AIDS, TB, STDs, and immuniza-tions as well as other important infectious diseases.To provide the vigilance and rapid response requiredto effectively address emerging infectious diseases,significant improvements in public health policy,program design, and infrastructure are needed. Afar-reaching and comprehensive strategy, carefullyintegrated with broader plans for health care re-form is required.
Effective public health policy results from in-teraction, cooperation, and coordination among awide range of public and private organizations andindividuals. Particularly critical to this process areCDC’s partnerships with state and territorial healthdepartments; other federal agencies; professionalorganizations; academic institutions; private healthcare providers; health maintenance organizationsand health alliances; local community organiza-
tions; private industry; and international partners,including WHO and international service organi-zations and foundations. Each of these partners willplay an integral role in the cooperative efforts re-quired to safeguard the public’s health from emerg-ing infectious disease threats.”
Authors: Emerging Infections Working Group:Ralph T. Bryan, M.D., Robert W. Pinner, M.D.,Robert P. Gaynes, M.D., C.J. Peters, M.D.,Meredith A. Hickson, M.P.H., Judith R. Aguilar
Type of publication: Report
Pages: 46
Study timeframe: The Advisory Committee consid-ered scientific literature from 1976 to 1993.
Study process: The plan was developed by the CDCin partnership with representatives from state andlocal public health organizations, other federal agen-cies, health care professionals, members of medicaland public health professional associations, infec-tious disease experts, and public service organiza-tions. Committee members met several times todiscuss the plan and gather additional inputbetween December 1992 and June 1993.
Type of organization: Federal Government
Intended audience: United States; physicians and otherhealth care providers, policy-makers
Languages (published in): English
Key contactOrdering Information: Centers for Disease Con-trol and Prevention, National Center for InfectiousDiseases, Office of Program Resources EP, MailstopC-14, 1600 Clifton Road, Atlanta, GA 30333
(5) WHO Scientific Working Group onMonitoring and Management ofBacterial Resistance to AntimicrobialAgents
Organization: World Health Organization, Divisionof Bacterial, Viral Diseases and Immunology.
Year published: 1994
Selected key findings• There is a lack of data on the economic conse-
quences of antibiotic resistance and of commu-nity-acquired infections.
• It may be useful to reconsider older alternativesto antibiotics, including bacterial interference,serum therapy, and bacteriophages.

97
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
• The approach of the pharmaceutical industry tothe development and spread of antimicrobialresistance includes: continued chemical modifi-cation of existing agent classes; interference withresistance mechanisms to increase target access;and searching for agents with novel mechanismsof action.
Key recommendationsRecommendations for WHO:• “Communicate the importance of the problem
of antimicrobial resistance to developed anddeveloping countries and other internationalhealth agencies;
• Improve systems for surveillance of antimicro-bial resistance;
• Develop recommendations to improve clinicaluse of antimicrobial agents and decrease selec-tion of resistant bacteria;
• Develop strategies to decrease the selection andtransmission of resistant microorganisms inmedical centers;
• Develop strategies to decrease transmission ofresistant microorganisms in the community andplans for responding to outbreaks of bacterialpathogens;
• Develop strategies to decrease the emergence anddissemination of resistant organisms in veteri-nary medicine and the environment;
• Support the development and evaluation of newpreventive and curative modalities.”
Implementation suggestions• Communication would be improved through
distribution of newsletters and bulletins (i.e.,Weekly Epidemiological Record, WHO DrugInformation Bulletin); facilitation of interactionamong government agencies, academic institu-tions and the pharmaceutical industry; and datasharing and surveillance system linkage.
• Improvement of surveillance systems would beachieved by helping national laboratories todetermine their current status and needs to suc-cessfully identify bacterial pathogens and testthem for susceptibility; distribute and help toinstall WHONET software in laboratories; helplaboratories to develop quality control andassurance programs.
• Reduction of antibacterial resistance in medicalcenters would be achieved by developing edu-cational programs and hygienic standards indaycare centers and long-term care facilities; in-fection control training programs for hospital
personnel; and linkage between hospital infec-tion control programs to quality assuranceefforts at the national and local levels.
• Transmission of resistant organisms in the com-munity would be decreased through promotionof community hygiene standards for safe waterand food and support of programs for improvedaccess to treatment.
• The emergence and spread of resistant organ-isms in veterinary medicine and the environmentwould be decreased by ensuring that only quali-fied veterinary personnel be permitted to pre-scribe antimicrobial agents for the treatment ofinfections in animals; prohibiting the use ofantimicrobial agents for growth promotion thatare also used in human medicine; and by dis-couraging “the unnecessary use of therapeuticantimicrobials for prophylaxis in food animals.”
Conclusions/Executive Summary“Antimicrobial resistance represents a crisis at thepresent time. It stems from a wide range of prob-lems, but there are a number of key factors. Aprimary one is the heavy usage of antimicrobialagents. The intense selective pressure resulting fromantimicrobial overuse has been an importantfactor in the rapid emergence of resistance. The dis-semination of resistant strains in hospitals and otherinstitutional settings is largely attributable toperson-to-person transmission, due to the incon-sistent application of basic infection control tech-niques and treatment of patients not guided bysusceptibility testing. Meanwhile, environmentalcontamination with antimicrobial-resistant patho-gens adds another dimension to the problem ofprevention and control. In addition, in some coun-tries, availability of antimicrobial agents withoutprescription is a major factor in their misuse. Else-where, the use of antimicrobial agents in animalhusbandry, particularly for growth promotion andprophylaxis of infection, provides an additionalselective pressure which encourages the emergenceof drug-resistant organisms. Addressing the manychallenges posed by emerging antimicrobial resist-ance requires a strategy at institutional, commu-nity, regional, national, and international levels.Partners in the development and implementationof such a strategy should include representativesfrom clinical and veterinary medicine, publichealth, microbiology, animal husbandry, the phar-maceutical, agriculture and aquaculture industries,as well as the behavioral sciences.”

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
98
Authors: Participants: Dr. Y.Z. Abou, Dr. J.F. Acar, Dr.G.A.J. Ayliffe, Dr. N. Citri, Dr. B. Cookson, Dr. WangFu, Dr. D.A. Goldmann, Dr. D. Grossklaus, Dr. M.Guzman, Dr. R.E.W. Hancock, Dr. R. Helmuth, Dr.P. Huovinen, Dr. J.M. Hughes, Dr. W. Johnson, Dr.E.L. Kaplan, Dr. T.S. Kereselidze, Dr. P. Kriz, Dr. G.Kronvall, Dr. A. Kucers, Dr. M.K. Lalitha, Dr. R.Leclercq, Dr. B. Levin, Dr. I. Lind, Dr. A. Marton,Dr. A. Medeiros, Dr. G.H. Miller, Dr. T.F. O’Brien,Dr. G. Orefici, Dr. K. Rahal, Dr. B. Tasmussen, Dr.B. Rowe, Dr. R. Bradley Sack, Dr. J. Schindler, Dr.N.A. Semina, Dr. J. Stelling, Dr. F. Tenover, Dr. A.Tomasz. Observers: Dr. R. Bax, Dr. D.H. Bouanchaud,Dr. E. Bozkurg, Dr. I. Carugo, Dr. R. Charnas, Ms.M. Cone, Dr. H. Dekoning-Gans, Dr. R. Kessler, Dr.C. Krasemann, Dr. H. Locher, Dr. J.S. Mantell, Dr.O. Morin, Dr. G. Mosely, Dr. D. Pontani, Dr. A.Roos, Dr. C.D. Rothermel. WHO Secretariat: Dr. M.Couper, Dr. D. Cohn, Dr. Svein-Erik Ekeid, Dr.M.M. El-Nageh, Mrs. K. Esteves, Dr. E. Griffiths,Dr. C.-C. Heuck, Dr. J.W. LeDuc, Dr. L.J. Martinex,Dr. N. Pearce, Dr. A. Pio, Dr. J. Perriens, Dr. M.Raviglione, Dr. K.B. Sharma, Dr. Hulian Sima, Dr.A. Sow, Dr. K. Tankari, Dr. E. Tikhomirov, Dr. G.Torrigiani, Dr. P.I. Trigg
Type of publication: Meeting report
Pages: 33
Intended audience: Global; policy-makers, pharma-ceutical industry, health care providers
Study timeframe: The working group met fromNovember 29 to December 2, 1994.
Study process: The working group, comprised ofprofessionals from the fields of clinical medicine,research and public health, met to review the cur-rent status of the nature and consequences of anti-microbial resistance, and to make recommendationson alleviating the problem.
Type of organization: International, non-governmen-tal, public health agency
Languages (published in): English
Key contactOrdering Information: Communicable DiseaseSurveillance and Response Documents, WorldHealth Organization, CH-1211 Geneva 27, Swit-zerland; fax: +41 22 791 4198, attention CSRDocuments; email: [email protected], attention Docu-ments.
(6) Impacts of Antibiotic-ResistantBacteria
Organization: Office of Technology Assessment; Con-gress of the United States
Year published: 1995
Selected key findings• Inappropriate antibiotic use contributes to the
increase of selection pressure for the selectionand spread of antibiotic resistance. It is possiblethat as much as 50% of antibiotic use is inap-propriate.
• Although only one-third to one-half of the 24.5million otitis media cases that occur each yearbenefit from antibiotics, physicians often pre-scribe them. Parental pressure and time con-straints that keep physicians from testing for viralsources of the disease are common reasons forresorting to potentially ineffective antibioticprescriptions.
• At any given time, 25% to 35% of all hospital-ized patients are receiving antibiotic treatment,whether therapeutic or prophylactic. The resultof such heavy use among a very vulnerable popu-lation often leads to the emergence and spreadof antibiotic-resistant bacteria.
Key recommendations(The Advisory Board presents options, rather thandirect recommendations)
Surveillance• “Congress could support the establishment of a
national surveillance system, including provid-ing funding. The features of current, limitedsystems can be incorporated and combined toproduce a system of desired size, complexity, andcost. Any system must have a strong advisorygroup that includes diagnostic laboratory andcomputer experts, clinicians, hospital adminis-trators, pharmaceutical company researchers,academic scientists, and federal and state regu-latory and health officials.”
Infection control• “Congress could encourage all states to adopt
guidelines for the coordination of infection con-trol measures between acute care and long-termcare facilities and to extend guidelines to includeall antibiotic-resistant bacteria.”
Research funding• “Congress can make money available for studies
of the development, transfer, and persistence of

99
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
antibiotic resistance [and] for research into thebasic biology of bacteria;
• Congress can make resources available for thestudy of appropriate use of devices that presentinfection risks to hospitalized patients.”
Controlling antibiotic use• “Review Medicare and Medicaid reimbursement
policies for their unanticipated effects on anti-biotic prescription patterns.”
Antibiotics in animal husbandry• “Collect information about associations between
animal husbandry uses of antibiotics and anti-biotic-resistant bacteria in humans;
• Design a study to determine the sources of anti-biotic-resistant bacteria in the human diet;
• Study the benefits of antibiotic use in animalhusbandry. An analysis of written informationcould probably determine the costs of the anti-biotics in feeds.”
Negotiated marketing agreements for antibiotics:• “Congress can provide FDA with authority to
negotiate extended market exclusivity to manu-facturers that agree to restrictions on marketingof antibiotics.”
Development of off-patent compounds as antibiotics• “Congress could authorize FDA to extend
market exclusivity for off-patent antibiotics thatare shown to be effective against antibiotic-resistant bacteria;
• Congress could establish a federal program to con-duct clinical trials of antibiotics to determine if theyhave uses against antibiotic-resistant bacteria.”
Implementation suggestionsThe Advisory Panel suggested delegation of respon-sibilities to various government agencies and de-partments of the United States. Increased fundingfor the creation of surveillance systems and infec-tion control guidelines, and for research and devel-opment would come from Congress. FDA wouldbe responsible for facilitating the development ofnew antibiotics, and for helping to determine thefuture uses of antibiotics in food animals and plants.Internal hospital surveillance systems should con-tinue, and should be linked to other hospitals withina geographical area, with the eventual goal of a na-tion-wide system overseen by CDC.
Conclusions/Executive Summary“The problems caused by antibiotic-resistant bac-teria can be ameliorated through two major routes:
1) prolonging the effectiveness of currently avail-able antibiotics through infection control and op-timal use of existing antibiotics and 2) developingnew antibiotics to treat resistant bacteria.”
“Although all persons are susceptible to illnessesrelated to antibiotic-resistant bacteria, some are morethan others. The poor, people without adequatehealth care, the incarcerated, the homeless, mili-tary personnel, children in daycare facilities, theelderly, and the immuno-suppressed are more sus-ceptible to these illnesses than the general popula-tion. However, because most of the general publiccomes in contact with members of these vulner-able populations daily, the general public is at riskbecause the diseases or illnesses can spread fromperson to person... Therefore, it is crucial that thescientific and medical communities, the pharma-ceutical industry, and the general public cooperateto find solutions that will slow the pace of antibi-otic resistance and lessen the impact of illness onpublic health.”
Authors: Advisory Panel: Gail Cassell, PhD; AnneBolmstrom; Robert J. Bywater, PhD; Barry Eisenstein,MD; Prabhavathi B. Fernandes, PhD; WinstonFrederick, MD; Joshua Lederberg, PhD; StephenLerner, MD; Stuart Levy, MD; Robert C. Moellering,Jr., MD; Barbara Murray, MD; Tom O’Brien, MD;Lone Simonsen, PhD; Harry Taber, PhD; AlexanderTomasz, PhD; Richard Wenzel, MD, MSc; CraigTownsend, PhD; Michael Zasloff, MD, PhD
Type of publication: Report
Pages: 183
Intended audience: United States; policy-makers,health care providers
Study timeframe: The Advisory Panel reviewed thescientific literature from 1961 to 1995, with a fewreferences from the late 1930s and 1940s.
Study process: The Advisory panel reviewed scien-tific literature, explored biological mechanismsbehind antibiotic resistance, and researched newantibiotics.
Type of organization: Federal Government
Languages (published in): English
Key contactOrdering information: USA Government PrintingOffice, Superintendent of Documents, Mail Stop:SSOP, Washington, DC 20402-9328

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
100
(7) Infectious Disease: A Global HealthThreat
Organization: National Science and TechnologyCouncil; Committee on International Science,Engineering, and Technology Policy (CISET)
Year published: 1995
Selected key findings• The re-emergence of infectious diseases may be
linked to human behavior (increased travel andtrade across borders, shifts in populationdemographics, the poor quality of public healthinfrastructures) and ecological changes (climateand weather changes, evolution of microorgan-isms, disruption of ecosystems due to humanuse patterns).
• The cost of treating antibiotic-resistant bacte-rial infections in the United States was $4 bil-lion in 1994, and projected to increase.
• The USA response to reports of outbreaks ofinfectious disease is often informal, loosely co-ordinated among government agencies, andhampered by a lack of funding to conduct a com-plete investigation.
Key recommendationsWork in partnership with other countries, withWHO, and with other international organizationsto improve worldwide disease surveillance, report-ing, and response by:• Establishing regional disease surveillance and
response networks linking national health min-istries, WHO regional offices, USA Governmentlaboratories and field stations abroad, foreignlaboratories and medical centers, and WHO col-laborating centers;
• Ensuring that reliable lines of communicationexist between local and national medical centersand between national and regional or interna-tional reference facilities, especially in parts ofthe world where modern communications arelacking;
• Developing a global alert system whereby na-tional governments can inform appropriateworldwide health authorities of outbreaks of in-fectious disease in a timely manner.
Strengthen the USA capacity to combat emerg-ing infectious diseases by:• Enhancing collaborations among USA agencies
to ensure maximum use of existing resources fordomestic and international surveillance and re-sponse activities;
• Rebuilding the USA infectious disease surveil-lance public health infrastructure at the local,state, and federal levels;
• Working with the private and public sectors toimprove USA capacity for the emergency pro-duction of diagnostic tests, drugs, and vaccines;
• Strengthening technical training programs indisciplines related to infectious disease surveil-lance and response;
• Establishing an Interagency Task Force to coor-dinate the implementation of these recommen-dations;
• Establishing a private sector subcommittee of theInteragency Task Force that includes representa-tives of the USA pharmaceutical industry, medi-cal practitioners and educators, and biomedicalscientists.
Implementation suggestionsThe committee recommends giving greater author-ity to certain government agencies and departmentsto monitor and respond to disease outbreaks. Tothis end, it recommends the convening of anInteragency Task Force, consisting of Centers forDisease Control and Prevention, Food and DrugAdministration, National Institutes of Health, theDepartment of State, Department of Defense, andUSA Agency for International Development, andothers as necessary.
ConclusionsThe elements of a global network for disease sur-veillance already exist but need to be strengthened,linked, and coordinated. For instance, many USAGovernment department and agencies maintain orsupport field stations and laboratories in Africa,Asia, and the Americas that may be electronicallylinked to provide an initial framework for a net-work for global infectious disease reporting. In part-nership with other countries and with WHO, thisskeletal surveillance network could be expandedover time to include many international resources,including national health ministries, WHOCollaborating Centers, hospitals, and laboratoriesoperated by other nations, and American and for-eign private voluntary organizations.
Authors: Report generated by members of CISETand its working group comprised of members from28 government agencies and departments
Type of publication: Report
Pages: 56
101
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Intended audience: United States; policy-makers
Study timeframe: Working group convened Decem-ber 14, 1994
Study process: Various government agencies anddepartments contributed input on the role of theUnited States in detecting, reporting, and respond-ing to outbreaks of new and re-emerging infectiousdiseases.
Type of organization: Government
Languages (published in): English
Key contactCenters for Disease Control and Prevention,Office of the Director, National Center for Infec-tious Diseases: (404) 639-2603
(8) Report of the ASM Task Force onAntibiotic Resistance
Organization: American Society for Microbiology
Year published: 1995
Selected key findings• Broad spectrum antibiotic use for otitis media
is selecting for resistance against other moredangerous pathogens.
• Physicians contribute to the resistance problemby inadequately diagnosing ailments before pre-scribing antibiotics, prescribing antibiotics totreat viral illnesses, inappropriately prescribingbroad spectrum antibiotics, and acquiescing topatient demand for antibiotic prescriptions whentheir use would be ineffective.
• Nearly one half of antibiotics used in the USAare used in farm animals (according to 1988report by the National Academy of Sciences).
• The estimated yearly cost of treating infectionsin humans that are related to antibiotic-resist-ant organisms in the United States is over $4billion.
Key recommendations• Establish a national surveillance system to do the
following:— “Focus on the most prevalent bacterial and
fungal pathogens (not viral) that concernhuman health. This will assess isolates fromclinical disease cases and routine isolates sothat no bias from one center testing only the“problem” isolate or more resistant isolatescompromises the results. Attention will begiven to the trend in upward “creep” of MICs
[Minimal Inhibitory Concentration]. Thereis also a need to monitor food sources suchas animal products at the supermarket levelas well as imported fruits, vegetables, andother products that may carry colonizing,drug-resistant bacteria and colonizing fecalflora in some patient populations. Salmonellaand Shigella both should be monitored.Salmonella gives the best window into theimpact of uses of antibiotics in the animalworld, and the fraction of Shigella that isimported gives us an excellent view of theimpact of antibiotic uses in the developingworld. Monitoring of soil waste in farmsshould also be considered;
— Establish a baseline of antimicrobial in vitroefficacy to which the following can be com-pared: earlier data from similar surveillancestudies found in medical literature reviews,especially if these studies utilized compara-ble methodologies and surveillance techniques;subsequent surveillance data resulting fromthe establishment of a national surveillancesystem analyzed in a longitudinal manner;non-USA data to assess the internationalrisks of resistance;
— Accumulate concurrent demographic profileinformation to assess the relationshipsbetween organisms emerging in hospitals ofvarious sizes or disease therapy focuses andpathogens prevalent among ambulatory pa-tients in the community and animals housedin various environments. The role of druguse in these environments shall be addressed;
— Establish a mechanism whereby organismspossessing certain phenotypic and genotypicresistance patterns will be referred to ad-equately funded laboratories for detailed study.Various molecular typing and investigativeprocedures can lead to earlier understand-ing of developing resistance mechanisms andspread of epidemic clones;
— Allow for the future assessment of theencountered resistant pathogens’ effect onpatient outcomes, general communityhealth, and the costs of health care delivery.Surveillance will target areas for specific in-tensive interventions for prevention (likevaccine campaigns and antimicrobial use re-duction programs). Surveillance will alsoidentify areas where epidemiologic investi-gations are needed to improve understand-ing of spread of drug-resistant strains and to

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
102
identify ways to interfere with spread;— Maximize the possibility that data will lead
to significant forms of professional healthcare intervention to reduce the probabilitythat resistance to the drug will be spreadwidely and have an adverse impact on thenational quality of health care outcomes.Interventions ideally should be focused at thelocal level but regional and national inter-ventions could also provide great benefits;
— Provide expert federal agencies and societiesthe information to modify recommendationsregarding therapy or prophylaxis of diseaseor regarding testing procedures. These canbe implemented at various levels related topatient or institutional demographics or bygeography (local, regional, national);
— Provide a compatible system in which sub-sets of participants could be grouped forcommon benefits. Examples include federalhospitals (Veterans Administration [VA],military, etc.), animal care facilities (univer-sity-based, USA Department of Agriculture[USDA], etc.), recognized HMO-like pro-grams, and academic institutions such asuniversity teaching hospitals;
— Provide the accumulated data to pharmaceu-tical manufacturers, thus providing thevalidations of contemporary drug spectrums.This will be valuable in establishing mean-ingful organism coverage indications inantimicrobial agent package inserts;
— Provide a system that can be modified toaddress any discovered area of concern relatedto the effective therapy of infectious organ-isms. This could allow expansion to coverfungi, viruses, cell-associated organisms, andsome parasites.”
— Monitor bacterial pathogens consideredimportant in human and animal infections.Testing schedules of various strains and spe-cies will vary according to the recommenda-tions of the surveillance oversight panel. Asignificant number of organisms should betested, with medical statisticians contribut-ing input to the final list.
— Conduct a broad sampling of geographicallydispersed laboratory isolates, with a focus onhuman pathogens. Criteria for selection oflaboratories will be based on state popula-tion density and diversity of demographicpopulations.
— Monitor demographic profiles of participat-ing hospitals and laboratories with yearlyupdates.
— Establish testing methods that are of refer-ence quality and closely follow the docu-ments published by the NCCLS. Wherepossible, conduct initial screening using thedisk diffusion method (MCCLS M2-A5) forthose pathogen-antimicrobial combinationsthat can be accurately tested.”
• Strengthen professional and public education inthe area of infectious diseases and antibiotics toreduce inappropriate usage of antibiotics.— “An urgent need exists for more appropriate
selection and use of antimicrobial drugs. Thecurriculum of health professional (medical,dental, nursing, and veterinary) schools andpostgraduate educational programs shouldbe strengthened in the areas of sterilization,disinfection, hazards of inappropriate anti-microbial drug use, appropriate diagnosisand treatment of infectious diseases, andantibiotic resistance. These efforts shouldresult in reduction of spread of infectiousagents and more prudent use of antibiotics;
— Better guidelines should be established andenforced to reduce the spread of infectiousagents and antibiotic resistance in the hos-pital environment, nursing homes, daycarefacilities, and food production industries;
— Educational materials should be developedand widely distributed to patients and foodproducers. The need for partnerships in im-proving antimicrobial use of cost-effectivetreatment of infections and to preserve theeffectiveness of antimicrobial drugs for thefuture should be emphasized.”
• “There is an urgent need for more basic researchdirected toward development of new antimicro-bial compounds, effective vaccines, and otherprevention measures.— In FY 1994 allocations to the National In-
stitute of Allergy and Infectious Diseases ofthe NIH for funding of non-AIDS infectiousdisease research were reduced by $20 mil-lion. Increased appropriations are urgentlyneeded to fund areas of research directly re-lated to new and re-emerging infections andantibiotic resistance;
— More basic research is needed to delineate thegenetic and metabolic pathways, includingessential regulatory factors, that determinevirulence as well as antibiotic susceptibility

103
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
or resistance in pathogens of human andveterinary importance...;
— More resources should be devoted to thesequencing of the entire genome of micro-bial pathogens, particularly in closed popu-lations (i.e., hospitals, child care facilities,and food production facilities);
— More basic research is needed to better un-derstand the genetics of microorganisms andthe development of antibiotic resistance,particularly in fungi and newly describedpathogens;
— Research is needed for development of rapid,reliable diagnostic techniques for identify-ing specific infectious causes of illness…;
— More basic research is needed to facilitatedevelopment of effective vaccines and otherprevention measures.”
Implementation suggestionsImplementation of the task force’s recommenda-tions would be conducted by the National Centerfor Infectious Diseases of the CDC. Establishmentof priorities and implementation of policies wouldbe carried out by the National Institute of Allergyand Infectious Diseases of the National Institutesof Health (NIH), the USA Department of Agri-culture, the Environmental Protection Agency, andthe Food and Drug Administration.
Conclusions/Executive Summary“There is an urgent need for effective domestic andglobal surveillance of antibiotic resistance in ani-mals and humans. There is also an urgent need formore prudent use of antibiotics in both human andveterinary medicine, particularly as it relates to foodproduction. Of equal urgency is the need for bet-ter hospital infection control and implementationof guidelines to reduce spread of infection and an-tibiotic-resistant pathogens in the hospital environ-ment. There is a great need for strengthening thecurriculum of human and veterinary health careprofessionals in the areas of sterilization and disin-fection, mechanisms of antibiotic resistance, andfactors contributing to its spread, including inap-propriate antibiotic usage. There is also a need forpatient education regarding appropriate uses of anti-biotics. More basic research is needed to more clearlydelineate mechanisms of antibiotic resistance andto identify new antimicrobial targets. Lastly, greateremphasis must be placed upon research related torapid, reliable diagnostic tests and vaccines for pre-vention and control of infectious diseases.”
Authors: Task force: Gail H. Cassell, Ph.D., Gordon L.Archer, M.D., Thomas R. Bear, M.D., Mary J.Gilchrist, Ph.D., Donald Goldmann, M.D., DavidC. Hooper, M.D., Ronald N. Jones, M.D., StanleyH. Kleven, D.V.M., Ph.D., Joshua Lederberg, Ph.D.,Stuart B. Levy, M.D., Donald H. Lein, D.V.M.,Ph.D., Robert C. Moellering, M.D., Thomas F.O’Brien, M.D., Bennie Osburn, D.V.M., Ph.D.,Michael Osterholm, Ph.D., David M. Shlaes, M.D.,Ph.D., Martin Terry, D.V.M., Sue A. Tolin, Ph.D.,Alexander Tomasz, Ph.D. Government Liasions: RobertF. Breiman, M.D., Jean Cooper, Ph.D., James M.Hughes, M.D., John La Motagne, Ph.D., EdwardMcSweegan, Ph.D., Albert T. Sheldon, Ph.D., FredTenover, Ph.D. Industrial Liasions: Jerry Boscia, M.D.,Carl J. Craft, M.D., Susan Froshauer, Ph.D., MichaelMcCabe, D.V.M., Catherine Reese, Ph.D., Ray Testa,Ph.D. Office of Technology Assessment: Sean Tunis,M.D., Justin Latus, M.P.P.
Type of publication: Report
Pages: 23
Intended audience: United States; microbiologists
Study timeframe: N/A
Study process: Task Force members participated in aworkshop conducted July 6, 1994, and reviewedrelevant scientific literature.
Type of organization: Non-profit, life science society
Languages (published in): English
Key contactASM Headquarters, 202-737-3600.Available on the web at: http://www.asmusa.org/pasrc/pdfs/antibiot.pdf
(9) The Medical Impact of the Use ofAntimicrobials in Food Animals. Reportof a WHO Meeting.
Organization: World Health Organization, Divisionof Emerging and Other Communicable DiseasesSurveillance and Control.
Year published: 1997
Selected key findings• At the time of the report, Salmonella serotypes
showing reduced susceptibility to fluoro-quinolones in humans had been observed inFrance, Germany, Ireland, the Netherlands, Rus-sia, Spain and the United Kingdom.
• There is a lack of quantifiable data on the preva-

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
104
lence and spread of resistance in zoonotic bacte-ria or indicator agents, including Escherichia coli,Entereococcus faecium and Enterococcus faecalis.
• Prior to the use of fluoroquinolones in poultryproduction, there has been a dramatic rise inthe incidence of fluoroquinolone-resistantCampylobacter jejuni in live poultry, poultry meatand from infected humans.
Key recommendations• Adherence to the recommendation made by the
WHO advisory group of 1994, specifically: “Theuse of any antimicrobial agent for growth pro-motion in animals should be terminated if it is:used in human therapeutics; or known to selectfor cross-resistance to antimicrobials used inhuman medicine.”
• “National authorities should define thresholdlevels of resistance in bacteria and circumstanceswhere mitigation procedures should be insti-gated and, if such procedures are unsuccessful,when approval should be withdrawn;
• No antimicrobial should be administered to afood animal unless it has been evaluated andauthorized by competent national authorities.This evaluation should include a thorough riskassessment which includes the development ofresistance that may impact public health; andpost-market monitoring program to detect emer-gence of resistance of public health significance.If such emergence is detected, appropriateaction should be taken, which may include thewithdrawal of the antimicrobial in question;
• Increased concerns regarding risks to publichealth resulting from the use of antimicrobialgrowth promoters indicated that it is essentialto have a systematic approach towards replacinggrowth-promoting antimicrobials with safernon-antimicrobial alternatives;
• Request the Codex Alimentarius Commissionto include issues of antimicrobial resistanceamong the terms of reference of the Codex com-mittee on Residues of Veterinary Drugs in Foods;
• National authorities should maintain records ofexport/import figures of bulk chemicals withpotential antimicrobial use, as such informationis vital for quantitative assessments of the medi-cal risks related to the use of antimicrobials inlivestock production;
• WHO should continue to support ongoingefforts to harmonize residue standards interna-tionally;
• Countries should ascertain and monitor the
prevalence of resistant bacteria in food-produc-ing animal populations and animal-based foodproducts;
• Classes or organisms to be included in nationalmonitoring programs should be the importantzoonotic foodborne bacteria (with Salmonella asthe primary group of organisms) and key indi-cator bacteria… If feasible, programs shouldinclude E. coli and Campylobacter. In addition,other potential veterinary and human pathogens(e.g., Enterococcus) should be considered, basedon an individual country’s requirements;
• National practices of antimicrobial use in ani-mals would be reviewed, and antimicrobial usepolicies be developed to reduce the risks ofselection and dissemination of antimicrobialresistance.”
Implementation suggestions• WHO’s Program on Antimicrobial Resistance
Monitoring would be responsible for coordinat-ing international efforts to conduct surveillanceof resistant bacteria in food animals and foodfrom animal sources, and for training personnelin the medical and veterinary sectors on antimi-crobial resistance testing and national policyframework development activities.
• An expanded version of the WHONET softwarewould be used to monitor data on bacteria col-lected from food animals and food of animalorigin.
• Collaborations among the medical, veterinaryand agricultural sectors would be responsible forcoordinating surveillance efforts at the local,regional, or national level.
• WHO and the Food and Agricultural Associa-tion of the United Nations would conveneexperts to develop international guidelines forprudent use of antimicrobials in food animalproduction.
Conclusions/Executive Summary“Microbiological and clinical evidence is mount-ing that resistant bacteria or resistance determinantsmight be passed from animals to humans, result-ing in infections that are more difficult to treat.With an increase in the prevalence and distribu-tion of antimicrobial-resistant infections in hospi-tals and the community, the question has beenraised as to how this escalation of resistance couldhave been influenced by the use of antimicrobialsin livestock production. Timely public healthaction is needed to control or mitigate any medical

105
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
problem that might be related to the widespreadapplication of antimicrobials outside the medicalsphere. The most desirable action is the limitation,or more prudent use, of antimicrobials, particu-larly where alternatives are available. In situationswhere there is evidence of a link to medical prob-lems, appropriate control action is needed. In lightof shrinking public resources and the increasingneed to conduct scientifically-substantiated riskassessments for prioritizing public health action,national policies on the use of antimicrobials inanimals must balance the possible benefits to live-stock production against the medical risk and publichealth consequences deriving from their use.”
Authors: Participants: Professor J. Acar, Dr. F. Angulo,Dr. D. Bell, Professor T. Blaha, Dr. J. Boisseau, Dr. J.Borvendég, Dr. Anne Brisabois, Dr. R. Buchanan, Dr.Celia Carlos, Dr. Paula Fedorka-Cray, Professor A.Franklin, Professor C. Friis, Professor H. Goossens,Professor J. Gropp, Dr. R. Helmuth, Dr.A. Hoszowski,Professor S. Jin, Dr. I.A. Kroetz, Dr. Hilde Kruse, Dr.J.-P. Lafont, Professor R. LeClerq, Dr. S. Levy, Dr. J.MacKinnon, Dr. J.L. Martel, Dr. G. Martin, Dr. S.McEwen, Dr. S. McOrist, Dr. M.N. Mohd Nordin,Professor A. Panin, Dr. Laura Piddock, Professor M.Pugh, Dr. A. Rattan, Professor L. Songkram, Dr. S.Sundlof, Dr. W. Thiel, Dr. Linda Tollefson, Dr. H.Trolldenier, Dr. J. Turnidge, Dr. P. Wall, Dr. U. C.Warsa, Dr. H. Wegener, Professor B. Wiedemann,Professor M. Wierup, Professor W. Witte, Dr. C. Wray,Dr. M. Zervos, Dr. Dorothée André, Dr. J. Blancou,Dr. J. Paakkanen, Dr. J. Perez-Lanzac, Professor P.Peters, Dr. Barbara Röstel, Dr. M. Rutter Observers:Dr. P.P. Bosman, Dr. S. Brown, Dr. R. Bywater,Dr. R. Carnevale, Dr. R. Froyman, Dr. T. Gomez,Dr. S. Lens, Dr. M. Lütoz, Dr. Margaret Miller, Dr.K. Morita, Dr. S. Pitlik, Dr. Andrea Sanwidi, Dr. T.Shyrock, Dr. P. Sundberg, Dr. T. Tselentis, Dr. C.Verschueren, Dr. L. Vogel WHO Secretariat: Dr. R.Crom, Mr. G. Hartl, Dr. Sudarshan Kumari, Dr. N.Moran, Dr. A. Reilly, Dr. K. Stöhr, Dr. RosamundWilliams.
Type of publication: Meeting Report
Pages: 24
Intended audience: Global; policy-makers, agriculturalindustry
Study timeframe: The meeting was held from the13th to the 17th of October, 1997.
Study process: During the four weeks prior to themeeting, 522 experts received 39 presentations
prepared by those who would be participating inor observing the meeting. The experts discussed andcommented on the material. Presentations weregiven and discussed during the first three days ofthe meeting. On the last two days, working groupsdrafted reports on medical impacts of antimicro-bial use in livestock production, surveillance andrisk management. The reports were discussed andadopted during the meeting’s final session.
Type of organization: International, non-governmen-tal, public health agency
Languages (published in): English
Key contactOrdering Information: Communicable DiseaseSurveillance and Response Documents, WorldHealth Organization, CH-1211 Geneva 27, Swit-zerland; fax: +41 22 791 4198, attention CSRDocuments; email: [email protected], attention Docu-ments.
Available on the web at: http://www.who.int/emc-documents/zoonoses/whoemczoo974c.html
(10) America’s Vital Interest in GlobalHealth: Protecting Our People,Enhancing Our Economy, andAdvancing Our InternationalInterests
Organization: Institute of Medicine
Year published: 1997
Selected key findings• The United States lacks a coordinated, national
plan for conducting basic health research anddevelopment and applying it towards the im-provement of global health.
• Prevention is the most cost-effective approachto infectious disease, with millions of dollarssaved globally each year once a major disease iseradicated.
Key recommendations“The USA government should:• act to facilitate the development of an effective
global network for surveillance of infectiousdiseases, using the full potential of the informa-tion and communications revolution andfostering the capacity of developing countriesin both biomedical surveillance and communi-cations;
• further develop and extend the network to pro-

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
106
vide an early warning system for possible bio-logical or chemical attacks;
• take an active role in global efforts to share in-formation between countries on the most effec-tive means of financing and delivering healthcare in order to maximize efficiency and equity;
• increase its investment in research and develop-ment in biomedical science related to majorglobal health problems through expanded part-nerships and cost-sharing with other govern-ments and international donors;
• continue federal support for the education andtraining of health researchers and practitionersfrom other countries as an international publicgood toward health leadership that benefits bothour own nation and others;
• form an Interagency Task Force on GlobalHealth within the government to anticipate andaddress global health needs and to take advan-tage of opportunities in a coordinated and stra-tegic fashion.”
Implementation suggestionsThe Task Force designates the USA Department ofHealth and Human Services as the organizationmost capable of carrying out the recommendationsin the report, including setting of priorities andcoordinating the efforts of other health agenciesaround the world.
Greater financial support of the United Nationsby the United States would help to implement moreeffective strategies for achieving better global health,and give the USA more leverage to enact the kindsof global policies that it considers to be necessary.
Conclusions/Executive Summary“For the United States to engage successfully in glo-bal health, coordination among the multiple USAagencies with statutory responsibilities in the areawill be needed, as well as the formation of partner-ships with the USA industrial and academic sec-tors and nongovernmental organizations, othernations, and international organizations. Withoutactive USA engagement and coordination, in con-cert with the complementary efforts of othernations, the struggle to ensure health around theglobe threatens to fragment or falter, with the likelyoutcome that our own national health, economicviability, and security will suffer. This report out-lines the compelling case for America’s activeengagement in global health and offers recommen-dations on how this may best be achieved.”
Authors: Barry R. Bloom, Harvey V. Fineberg,Jacquelyn Campbell, Richard G. A. Feachem, JulioFrenk, Dean Jamison, Eileen T. Kennedy, ArthurKleinman, William E. Paul, Allan Rosenfield,Patricia L. Rosenfield, Thomas J. Ryan, Susan C.M. Scrimshaw, June E. Osborn, John H. Bryant,William H. Foege, David P. Rall
Type of publication: Report
Pages: 62
Intended audience: United States; policy-makers
Study timeframe: The report considers informationfrom 1985 to 1997.
Study process: Committee members conducted aworkshop in November of 1995, and solicited in-put from national and international public healthand government organizations.
Type of organization: Non-profit public health andadvisory organization; advisor to Federal Govern-ment on issues of public health
Languages (published in): English
Key contactOrdering information: National Academy Press,www.nap.eduContent: Barry R. Bloom and Harvey V. Fineberg,Co-Chairs of the IOM Board on InternationalHealth
(11) New and Re-emerging InfectiousDiseases: A Global Crisis andImmediate Threat to the Nation’sHealth; the Role of Research
Organization: American Society for Microbiology
Year published: 1997
Selected key findings• Antibiotic-resistant bacterial infections in the
United States cost approximately $4 billion inmedical costs annually.
• Infectious diseases were the third leading causeof death in the United States in 1996.
• From 1980 to 1996, the death rate from infec-tious diseases in the United States has increasedmore than 50 percent.
Key recommendations• Encourage investment in research in the fields
of microbiology, immunology and infectiousdiseases.

107
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
• Focus research on molecular genetics and thebiochemistry of bacteria, viruses, and fungi.
Implementation suggestionsImplementation of recommendations can beachieved by increasing funding to USA governmentagencies, including the National Institute of Allergyand Infectious Diseases and the National Institutesof Health.
Conclusions/Executive Summary“Increased research funding is critical to address thecurrent threats from new and re-emerging infec-tious diseases through the development of betterdiagnostic tests, new drugs, and vaccines. In addi-tion, increased funding would provide new oppor-tunities for making major advances to define thepotential role of infectious agents in chronicdiseases, such as cancer, that currently have noknown causes.”
Authors: Not specified
Type of publication: Booklet
Pages: 13
Intended audience: United States; scientists, policy-makers
Study timeframe: Report considers scientific litera-ture from 1992 to 1996
Study process: Analysis of documents on emerginginfectious diseases
Type of organization: Non-profit, Life Sciences Soci-ety
Languages (published in): English
Key contactAmerican Society for Microbiology, Public AffairsOffice, 202-942-9209
Available on the web at: http://www.asmusa.org/pasrc/pdfs/newandre.pdf
(12) Resistant Organisms: Global Impact onContinuum of Care
Organization: Royal Society of Medicine
Year published: 1997
Selected key findings• Attitudes of patients and physicians are key
factors that contribute to the inappropriate pre-scribing and use of antibiotics (Levy; Plotnick).
• Resistance is a local problem, dependent onpatterns of use within a hospital and on eachhospital’s infection control programs (Levy).
• Resistance is an ecological problem; overuse ofantibiotics has removed susceptible organismsand seen their replacement with resistant ones.It is possible to reverse the problem through thereduction of antibiotic use (Levy).
• Factors such as sterility and type of instruments,wound preparation, wound closure, etc. contrib-ute to the likelihood of infection during surgi-cal procedures (Henderson).
Key recommendations• More accurate diagnosis before prescribing any
medication (Levy; Plotnick).• Resuscitate efforts to identify and monitor the
emergence and spread of infectious diseases(Plotnick).
• Evaluate different methods of antibiotic use,including shorter or cyclical courses.
• Improve staff to patient ratios in hospitals, toallow for better diagnosis and prescribing (Lee).
• Modify prescribing practices to eliminate exces-sive antibiotic prophylaxis before surgery(Henderson).
Implementation suggestionsRear Admiral Plotnick and Laura Lee both recom-mended strategies developed by the CDC (in co-operation with a variety of regional, national, andinternational public and private organizations)which act on issues of surveillance, research, pre-vention, control, and institutional management.
Conclusions/Executive SummaryThe abatement of the problem of antibiotic resist-ance can only be achieved through cooperation ofprescribers, patients, government, pharmaceuticaland agricultural industries. Surveillance, infectioncontrol, and improved prescribing practices are allimportant components of any collaborative effort.
Authors: Jean Davis, Professor S. Michael Emmerson,David K. Henderson, MD (co-editor), Laura Lee,Stuart B. Levy, MD (co-editor), Rear Admiral JuliaR. Plotnick
Type of publication: Conference proceedings
Pages: 70
Intended audience: United States, United Kingdom;health care providers
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
108
Study timeframe: Conference held September 27,1996
Study process: Varies with each presentation
Type of organization: Independent professional organi-zation
Languages (published in): English
Key contactOrdering information: Royal Society of MedicinePress, Lmt., +44 (0) 20 7290 3945; email: [email protected]
(13) Guidelines for the Prevention ofAntimicrobial Resistance in Hospitals(SHEA Position Paper)
Organization: Society for Healthcare Epidemiologyof America; Infectious Diseases Society of America
Year published: 1997
Selected key findings• The authors contend that, contrary to many
studies, antibiotic-resistant bacteria are not nec-essarily less virulent than their susceptibleparents, and that even in cases where the secondgeneration bacteria are less virulent, they are noless dangerous to vulnerable hospitalpopulations.
• Making a definite connection between antimi-crobial use and antimicrobial resistance in hos-pitals is often confounded by lack of consistencyfrom hospital to hospital in defining resistance,methodologies used in susceptibility testing, andother variables.
Key recommendationsRecommendations for hospitals• “Establish a system for monitoring bacterial
resistance and antibiotic usage;• Establish practice guidelines and other institu-
tional policies to control the use of antibiotics,and respond to data from the monitoringsystem;
• Adopt the recommendations of the Centers forDisease Control and Prevention’s (CDC) Guide-lines for Isolation Precautions in Hospitals, asconcerns the isolation of patients colonized orinfected with resistant microorganisms.”
Recommendations for prevention & reduction ofantimicrobial resistance in hospitals• “It is recommended that hospitals have a system
for monitoring antimicrobial resistance of bothcommunity and nosocomial isolate on a monthlybasis or at a frequency appropriate to the vol-ume of isolates.
• It is recommended that hospitals monitor therelationship between antimicrobial use andresistance, and assign responsibility throughpractice guidelines or other institutional poli-cies.
• It is recommended that hospitals apply ContactPrecautions to specified patients known orsuspected to be colonized or infected withepidemiologically important microorganismsthat can be transmitted by direct or indirect con-tact.”
Recommendations for future studies• “It is recommended that research to define the
mechanism of transfer of bacteria and theirresistance determinants among patient popu-lations and to determine methods to preventemergence and transfer of resistance, includingcontrol of antibiotic usage, be supported withincreases in targeted research funding.
• The development and testing of protocols formeasuring the effect of a variety of antimicro-bial usage controls is recommended for use inmultiple hospitals to determine the most effec-tive ways to prevent and reduce antimicrobialresistance in specific species to specific antimi-crobials.
• It is recommended that educational methods,including those that are interactive and compu-ter-based, be developed to improve the appro-priateness of antimicrobial prescribing.
• The efficacy of various levels of infectioncontrol precautions should be documented bycontrolled trials.
• Controlled studies of behavior modification,including novel approaches, to permit the effi-cient application of recommended guidelineswithin hospitals are recommended.
• The efficacy of quality improvement approachesto control of resistance should be studied.”
Implementation suggestionsGuidelines developed by the CDC and the NationalCommittee for Clinical Laboratory Standards aresuggested as ways for microbiologists and physi-cians to monitor antibiotic prescribing and use.
Conclusions/Executive Summary“There is convincing evidence that we share a

109
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
single ecosystem globally in terms of resistance. Theselection of resistance in one organism in one partof the world, even within an animal population,may have long-term, important implications forhuman health globally. Therefore, management ofthe problem of antimicrobial resistance within hos-pitals is a community responsibility, both withinand outside of the hospital…Good stewardship ofantibiotic usage combined with strong infectioncontrol will be required. To achieve this, all levelsof personnel within the hospital must be involved,from top administration down to individuals per-forming services and providing patient care.”
Authors: David M. Shlaes, MD, PhD; Dale N.Gerding, MD; Joseph F. John, Jr., MD; William A.Craig, MD; Donald L. Bornstein, MD; Robert A.Duncan, MD; Mark R. Eckman, MD; William E.Farrer, MD; William H. Greene, MD; Victor Lorian,MD; Stuart Levy, MD; John E. McGowan, Jr., MD;Sindy M. Paul, MD; Joel Ruskin, MD; Fred C.Tenover, MD; Chatrchai Watanakunakorn, MD
Type of publication: Position paper
Pages: 17
Intended audience: United States; scientific commu-nity
Study timeframe: The authors reviewed scientificliterature dating from 1977 to 1996.
Study process: The authors analyzed existing scien-tific literature on antibiotic resistance mechanismsand spread.
Type of organization: Non-profit public health organi-zation
Languages (published in): English
Key contactReprint requests: David M. Shlaes, MD, Wyeth-Ayerst Research, 401 N. Middletown Rd., PearlRiver, NY 10965
(14) Symposium on Antibiotic Resistance:Origins, Evolution, Selection andSpread
Organization: Ciba Foundation
Year published: 1997
Selected key findings• Antibiotic resistance is an ecological problem,
in that the balance between susceptible and re-sistant bacteria has been disrupted.
• In order to determine the extent of antibioticresistance in hospitals, it is necessary to take intoaccount each hospital’s pattern of antibiotic use.
• A report on the monitoring of antibiotic use ina hospital in Greece proved the efficacy of a rig-orous program of prescription control. The com-bination of prescription monitoring, improvedhygiene, educational programs and the limita-tion of certain antibiotics resulted in (for exam-ple) ceftazidime-resistant P. aeruginosa levelsdecreasing from 45% to 8% after three years.(Giamerellou & Antoniadou)
Key recommendations• Increase development of novel antibiotic agents.• Increase emphasis on infection control and hy-
gienic practices.• Enact multidisciplinary approaches to reducing
hospital resistance rates, including cooperationbetween pharmacies and diagnostic laboratories,and between infectious disease physicians andclinicians.
Implementation suggestionsNot given
Conclusions/Executive Summary“This meeting has put these issues [antibiotic useand mechanisms of resistance] aside in order tofocus on a larger view of the problem, and todefine the potential for return to a healthier statevis-à-vis susceptible flora. There is a need for newguidelines on more rational utilization of futurenovel antimicrobials within the context of ecology.There is also a cost to discover and develop these.Thus, we shall want to keep them from succumb-ing to a similar fate, i.e., encountering resistance.In this effort, consumers can join physicians andthe pharmaceutical industry in maintaining thisefficacy. Whether antibiotics are available over-the-counter in developing countries or demanded andstockpiled in the developed countries, they are toooften in the hands of consumers who use them in-correctly.”
Authors: S.B. Levy, J.E. Davies, P. Huovinen, H.Sepplälä, J. Kataja, T. Klaukka, R. Gaynes, D. Monnet,W. Witte, H. Giamarellou, A. Antoniadou, F. Baquero,M.C. Negri, M.I. Morosini, J. Blazquez, M. Lipsitch,B.R. Levin, R.E. Lenski, K. Bush, R.A. Skurray, N.Firth, R.M. Hall, M.C. Roberts, M.L. Cohen
Type of publication: Report
Pages: 250

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
110
Intended audience: Global; scientists
Study timeframe: 3-day symposium in July of 1996.
Study process: Participating scientists discussed a va-riety of pre-submitted articles on antibiotic resist-ance.
Type of organization: International scientific and edu-cational non-profit
Languages (published in): English
Key contactOrdering: John Wiley & Sons, Ltd., [email protected]; telephone: +44 1243 779777Content: Stuart B. Levy, MD, Symposium Chair-man 1996
(15) The Current Status of AntimicrobialResistance Surveillance in Europe:Report of a WHO Workshop held inCollaboration with the ItalianAssociazione Culturale MicrobiologiaMedica
Organization: World Health Organization, Divisionof Emerging and Other Communicable DiseasesSurveillance and Control
Year published: 1998
Selected key findings• There is not enough communication between
antimicrobial resistance surveillance networksand the decision makers at the regional and na-tional levels in Europe.
• Quality assurance standards that evaluate thevalidity of surveillance data vary throughoutEurope, making it difficult to make accuratecomparisons.
• A coordinated effort by the various Europeansurveillance systems is necessary to effectivelyaddress the emergence and spread of antimicro-bial resistance.
Key recommendations• “The communication chain between antimicro-
bial resistance surveillance networks and nationaland regional decision makers must be strength-ened and used.”
• “There is a need to harmonize quality assurancestandards throughout Europe.”
• “Adequate support for microbiology and epide-miology training programs, for laboratoryinfrastructure, and for data analysis and com-munication, is required.”
• “Further discussions are necessary, to developcollaboration between existing antimicrobialresistance surveillance programmes.”
Implementation suggestionsAccording to participants’ responses to a question-naire circulated before the workshop, implementa-tion of any recommendations or improvementsdepends on adequate funding, standardized meth-odologies of susceptibility testing, improved gov-ernment support, a greater number of trainedprofessionals to carry out surveillance efforts, andincreased awareness of the resistance problem byhealth care providers.
Conclusions/Executive Summary“The emergence and spread of antimicrobial resist-ance is a significant problem to all people in allcountries, both developed and developing. It im-pacts both patients with infections and cliniciansfacing growing limitations on their efficacious useof antimicrobials. It influences a health care sys-tem’s ability to implement rational drug use poli-cies and efficiently allocate resources. Because theemergence of antimicrobial resistance is a globalproblem that affects us all, national and interna-tional efforts are needed to address the problem.Information and experience, must be shared so thatall can learn and benefit.”
“At present, many groups are attempting to har-monize local, national and international antimicro-bial resistance surveillance methodologies. Theseattempts are not necessarily coordinated with oneanother, however, and there is a growing percep-tion, reinforced by discussions held during thisworkshop, that a positive role could be played by apan-European coordinating group. Such a groupcould reflect the various national and European-wide interests in antimicrobial resistance surveil-lance. It could be initiated as a study group of theEuropean Society of Clinical Microbiology andInfectious Diseases and focus on actively promot-ing the performance of good-quality local studieswhich generate internationally comparable data.Such data could, in turn, be used to facilitate theaccurate interpretation of results between studiesand generate information on the extent of antimi-crobial resistance in Europe. An essential compo-nent of any group’s success, of course, will beadequate funding.” (I. Phillips)
Authors: Participants: Professor Jacques F. Acar, Profes-sor Fernando Baquero, Dr. Andre Bryskier, Dr. Otto

111
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Cars, Dr. Giuseppe Cornaglia, Dr. Patrice Courvalin,Dr. Roberta Fontana, Dr. Herman Goossens, Dr.Marija Gubina, Dr. Waleria Hryniewicz, Dr. PenttiHuovinen, Dr. Vincent Jarlier, Dr. Mark E. Jones,Professor Smilja Kalenic, Professor Conor T. Keane,Dr. Marianne Konkoly, Dr. Karl G. Kristinsson, Pro-fessor Herminia de Lencastre, Dr. David Livermore,Professor Enrico Magliano, Dr. Boyka Markova, Dr.Anna Marton, Dr. Jolanta Miciuleviciene, Dr. HelmutMittermayer, Dr. Kathrin Muelemann, Professor CarlErik Nord, Professor Alvaro Pascual, Professor IanPhillips, Professor Arne C. Rodloff, Professor JiríSchindler, Dr. Ivonna Selga, Dr. Anatoly Shapiro, Dr.Thomas Lund Sørensen, Dr. Marc Sprenger, Dr. Mar-tin Steinbakk, Professor Leonid Stratchounsky, Pro-fessor Marc Struelens, Dr. Alkiviadis C. Vatapoulos,Professor Jan Verhoef, Professor Richard Wise. WHOSecretariat: Dr. Ana Estrela, Dr. Colette Roure, Dr.John Stelling, Dr. Rosamund Williams, Dr. ClaraWitt.
Type of publication: Meeting report
Pages: 80
Intended audience: Europe; policy-makers, micro-biologists, those who are responsible for surveillancenetworks
Study timeframe: The workshop was held on De-cember 12, 1997.
Study process: The participants met to present anddiscuss the variety of antimicrobial resistance sys-tems in operation throughout Europe, to highlightthe features of successful programs, and to discusshow those features may be incorporated into othersystems.
Type of organization: International, non-governmen-tal, public health agency
Languages (published in): English
Key contactOrdering Information: Communicable DiseaseSurveillance and Response Documents, WorldHealth Organization, CH-1211 Geneva 27, Swit-zerland; fax: +41 22 791 4198, attention CSRDocuments; email: [email protected], attention Docu-ments.
Available on the web at: http://www.who.int/emc-documents/antimicrobial_resistance/whoemcbac981c.html
(16) Papers presented at the InternationalConference on Emerging InfectiousDiseases in Atlanta, GA, March 1998.Compiled in Emerging InfectiousDiseases 4(3): 353–515
Organization: Centers for Disease Control and Pre-vention, National Center for Infectious Diseases
Year published: 1998
Selected key findings• The National Institute of Allergy and Infectious
Disease (NIAID) dedicates about 21% of itsnon-AIDS infectious disease budget to emerg-ing infectious diseases. NIAID’s total emergingdiseases budget increased from $39.3 million in1993 to a projected $85 million in 1999. (Fauci)
• Nosocomial infections were estimated to be re-sponsible for 88,000 deaths and $4.5 billion intreatment costs in 1995. Approximately one-third of such diseases are preventable.(Weinstein)
Key recommendationsSurveillanceOne author recommends “...dramatically strength-ened local surveillance, including both laboratoryand epidemiologic capacity; commitment on thepart of local governments; and a strong collabora-tive international research and response system.”(Broome)
ResearchThe NIH recommends expanding research on theecologic and environmental aspects of disease emer-gence and transmission; expanding research on themicrobial mechanics of disease emergence; support-ing the development of vaccines and other preven-tive therapies, especially for diseases that arethreatening to emerge or reemerge; and “strength-ening the current USA research and training infra-structure for detection and responding to outbreaksof infectious diseases.” (Fauci)
Nosocomial infectionsImprove national surveillance of nosocomial infec-tions that occur in the hospital and in home health-care settings; improve the design of devices that areassociated with nosocomial infections; instituteaggressive antibiotic control programs, perhapsmaking them mandatory for hospitals that receivefederal reimbursements; and develop new andmicrobiologic methods for detecting and investi-gating outbreaks of multidrug-resistant pathogens.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
112
Implementation suggestions• Continuation and strengthening of Field Epi-
demiology Training Programs that respond toreports of emerging infections. Use of the Inter-net and other communication technologies togather and share surveillance information.(Broome)
• Continued collaboration between the public andprivate sectors. (Fauci)
• Hospital personnel would be responsible forimplementing infection control policies,especially those concerning basic hygiene.(Weinstein)
Conclusions• “We are better able in 1998 to address the threats
of emerging infections, but we are by no meansfully prepared. We must have the capacity toidentify new or reemerging threats and to re-spond successfully. We need to be creative andefficient in identifying necessary resources…Eradication activities also contribute to healthcapacity development, and the laboratory andsurveillance capacities created for polio eradica-tion should also be useful in detection of andresponse to emerging infectious diseases. Manyother creative approaches and collaborations areneeded for an effective global response to what-ever our microbial adversaries may produce.”(Broome)
• “The importance of basic research to the con-trol of emerging and reemerging diseases can-not be overemphasized. Emerging diseasesresearch encompasses many disciplines, and re-search advances that fall under the rubric ofemerging diseases will be relevant not only tospecific diseases being studied but to a broadrange of disciplines such as vaccinology, immu-nology, and drug development.” (Fauci)
• “Several enduring truths characterize the fieldof infection control. Hospitals will become morelike ICUs, and more routine care will be deliv-ered on an outpatient basis. Given the choice ofimproving technology or improving humanbehavior, technology is the better choice. Themajor advances in overall control of infectiousdiseases have resulted from immunization andimproved hygiene, particularly hand washing.We must work with hospital personnel on bet-ter implementation of existing infection controltechnologies so that we will not need to relysolely on technologic advances.” (Weinstein)
Authors: Stephen A. Morse, Donna E. Shalala, ClaireBroome, James Hughes, David Heymann, GuenaelRodier, Joshua Lederberg, D. Peter Drotman,Anthony Fauci, Karen Hein, David Relman, Sir JohnPattison, Bradley Perkins, Thomas Nchinda, AlisonMawle, Martin Cetron, Jay Keystone, David Shilm,Robert Steffen, Kenneth Castro, Mary E. Chamber-land, Jay Epstein, Roger Y.Dodd, David Persing,Robert G.Will, Alfred DeMaria, Jr., Jean C.Emmanuel, Beatrice Pierce, Rima Khabbaz, WilliamFoege, Donald Hopkins, Robert Weinstein, JonathanKaplan, Gary Roselle, Kent Sepkowitz, JanetMcNicholl, Susan Cookson, Ronald Waldman, BrianGushulak, Douglas MacPherson, Frederick Burkle,Jr., Christophe Paquet, Erich Kliewer, Patricia Walker,Frederick Murphy, Robert G. Webster, Duane Gubler,R Colwell, P. Epstein, M. Hall, P. Reiter, J. Shukla,W. Sprigg, E. Takafuji, J. Trtanj, James Childs, RobertE. Shope, Durland Fish, Francois X. Meslin, ClarenceJ. Peters, Karl Johnson, Emilio Debess, David Dennis,Suzanne Jenkins, Robert Tauxe, Samantha Yang,Deborah Deppe, James LeDuc, Robert Pinner, Brad-ford Kay, Ralph J. Timperi, Stephen S. Morse, DavidForslund, Julie J. McGowan, Tom OíBrien, LelaFolkers, Maria Teresa Cerqueira, Robert E. Quick,James Kanu, Gauden Galea, EliasAbrutyn, Ann MarieKimball, Carrie Horwitch, Patrick OíCarroll,Sumarjati Arjoso, Chaiyos Kunanusont, Ya-Shin Lin,Clifford Meyer, Laura Schubert, Phillip Dunham,David Bell, Gail Cassell, D. A. Henderson, JosephMcDade, David Franz, Stanley Falkow, GeorgeAlleyne, May C. Chu, Alexandra Levitt, Karl West-ern
Type of publication: Peer-reviewed journal
Pages: 164
Intended audience: United States; policy-makers,government agencies, hospital personnel
Study timeframe: Varies
Study process: Varies
Type of organization: Federal Government
Languages (published in): English
Key contactOrdering information: EID Editor, CDC/NCID/MS C12, 1600 Clifton Road, NE, Atlanta, GA30333
Available on the web at: http://www.cdc.gov/ncidod/eid/vol4no3/contents.htm
113
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
(17) Preventing Emerging InfectiousDiseases: A Strategy for the 21stCentury
Organization: Centers for Disease Control and Pre-vention, National Center for Infectious Diseases
Year published: 1998
Selected key findings• New developments since 1994 that necessitated
an update of Preventing Emerging Infectious Dis-eases include: new emerging threats; advancedscientific findings; new methods of discovering,tracking, and communicating outbreaks;changes in health care delivery; and increasedpublic awareness and government response.
• Implementation of CDC guidelines on group Bstreptococcal disease helped to reduce its inci-dence by over 40% between 1993 and 1995 inthe communities that followed the guidelines.
• A combination of improved practices in the foodindustry, surveillance, and public education de-creased the incidence of invasive listeriosis by44% between 1989 and 1993; the reduction wasmaintained through 1996, the last date cited inthe report.
Key recommendationsSurveillance• “Strengthen infectious disease surveillance and
response;• Improve methods for gathering and evaluating
surveillance data;• Ensure the use of surveillance data to improve
public health practice and medical treatment;• Strengthen global capacity to monitor and re-
spond to emerging infectious diseases.”
Applied research• “Develop, evaluate, and disseminate tools for
identifying and understanding emerging infec-tious diseases;
• Identify the behaviors, environments, and hostfactors that put people at increased risk for in-fectious diseases and their sequelae.
• Enhance epidemiologic and laboratory capacity;• Improve CDC’s ability to communicate elec-
tronically with state and local health depart-ments, USA quarantine stations, health careprofessionals, and others;
• Enhance the nation’s capacity to respond to com-plex infectious disease threats in the UnitedStates and internationally, including outbreaksthat may result from bioterrorism;
• Provide training opportunities in infectious dis-ease epidemiology and diagnosis in the UnitedStates and throughout the world.”
Prevention and control• “Implement, support, and evaluate programs for
the prevention and control of emerging infec-tious diseases;
• Develop, evaluate, and promote strategies to helphealth care providers and other individualschange behaviors that facilitate disease transmis-sion;
• Support and promote disease control and pre-vention internationally.”
Implementation suggestionsSurveillance• “Extend the ELC [Epidemiology and Labora-
tory Capacity] program to all state, territorial,and large local health departments;
• Strengthen the EIP [Emerging Infections Pro-gram] network by increasing its demographicand geographic representativeness and enhanc-ing its laboratory and epidemiologic capacity;
• Use the existing provider-based sentinel networksto monitor syndromes and diseases, and estab-lish at least one additional network;
• Integrate public health information and surveil-lance systems;
• Use surveillance data to analyze questions ofpublic health importance;
• Facilitate access to surveillance data that can beused in clinical practice;
• Assist global surveillance and response effortsthrough increased support of CDC-based WHOCollaborating Centers;
• Help monitor conditions that favor the emer-gence or spread of infectious diseases.”
Applied research• “Develop, evaluate, and disseminate testing
methods for infectious agents;• Identify factors that influence the risk of devel-
oping infectious diseases;• Assess the role of infectious agents in causing or
exacerbating chronic diseases and syndromes forwhich the causative agents are unknown;
• In collaboration with other organizations, sup-port research to develop and evaluate new anti-microbial drugs and prophylactic agents, as wellas methods to control disease vectors and reser-voirs;
• Support research to develop new methods ofdisinfection;

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
114
• Support social science and behavioral researchto develop better prevention programs.”
Infrastructure and training• “Define core public health functions and capaci-
ties needed for monitoring the spread ofmicrobes and responding to infectious diseaseoutbreaks, and provide personnel in state andlarge local health departments with essentialequipment and training;
• Strengthen CDC’s capacity to serve as the na-tional and international reference laboratory fordiagnosis of infectious diseases and for drug-resistance testing;
• Promote the development and production ofdiagnostic and reference reagents for use by pub-lic health laboratories;
• Work with state health departments to stand-ardize new diagnostic techniques and facilitatetheir use throughout the United States;
• Assist other USA agencies, international organi-zations, and other nations in building globalcapacity for disease surveillance and response;
• Enhance national surge capacity for respondingto outbreaks of unusual size, duration, andseverity;
• Ensure the continued training of epidemiolo-gists in problems related to emerging infectiousdiseases;
• Increase the number of laboratory scientiststrained in infectious diseases through the Emerg-ing Infectious Diseases (EID) LaboratoryFellowship Program and add a track for inter-national students;
• Expand CDC’s efforts to train counterparts indeveloping countries in the use of epidemiologicand laboratory methods for combating emerg-ing infectious diseases.”
Prevention and control• “Expand existing community-based programs;• Develop and support new community-based
demonstration programs in the target areas.• Evaluate the impact and cost-effectiveness of
alternative approaches to reducing infectiousdiseases;
• Increase the use of vaccines to prevent and con-trol emerging infectious diseases;
• Work with health care providers, hospitals, man-aged care organizations, and others to improvepatient outcomes related to infectious diseases;
• Work with private industry, government agen-cies, and others to develop systems that promoteprompt identification of infectious disease prob-
lems and rapid implementation of control meas-ures;
• Develop, implement, and evaluate disease pre-vention guidelines that can be used by the pub-lic, health care providers, and health care systems;
• Work with foreign governments, WHO, theUSA-European Union Task Force on Commu-nicable Disease, other international partners, andthe CISET Emerging Infectious Disease TaskForce to promote global programs for the pre-vention and control of infectious diseases;
• Provide technical assistance and transfer cost-effective technologies to other countries, usinggovernmental and nongovernmental channels;
• Participate in bilateral and multilateral initiativesto improve global infectious disease preventionand control;
• Work with WHO and other partners to com-plete the revision of International Health Regu-lations;
• Work with developing countries to sustain healthcare improvements and surveillance efforts afteroutbreaks.”
Conclusions/Executive Summary“Achievement of the objectives described in thisplan will improve our ability to understand, de-tect, control, and prevent infectious diseases. Theoutcome will be a stronger, more flexible USA pub-lic health infrastructure well-prepared to respondto well-known disease problems and to address theunexpected, whether it is an influenza pandemic, adisease caused by an unknown organism, or abioterrorist attack.”
Authors: Sue Binder, M.D., Alexandra M. Levitt,Ph.D., Judith R. Aguilar, David M. Bell, M.D., Mar-tin S. Cetron, M.D., Mary E. Chamberland, M.D.,Mark L. Eberhard, Ph.D., Duane J. Gubler, Sc.D.,Meredith A. Hickson, M.P.H., Jonathan E. Kaplan,M.D., Rima F. Khabbaz, M.D., James W. LeDuc,M.D., Susan A. Maloney, M.D., William J. Martin,Ph.D., Alison C. Mawle, Ph.D., Patrick McConnon,M.P.H., Martin I. Meltzer, Ph.D., Siobhan O’Connor,M.D., Alan J. Parkinson, Ph.D., Anne Schuchat,M.D., Steven L. Solomon, M.D., Robert V. Tauxe,M.D., Fred C. Tenover, Ph.D., Theodore F. Tsai,M.D., Robert B. Wainwright, M.D., Helene D. Gayle,M.D., Walter A. Orenstein, M.D., Barbara R.Holloway, M.P.H., James S. Marks, M.D., M.P.H.,Edward J. Sondik, Ph.D., Linda Rosenstock, M.D.,M.P.H., Walter W. Williams, M.D., M.P.H., StephenB. Blount, M.D., M.P.H., Karen K. Steinberg, Ph.D.,Edward L. Baker, M.D., M.P.H.

115
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Type of publication: Report
Pages: 75
Intended audience: United States; physicians andother health care providers; policy-makers
Study timeframe: The Steering Committee reviewedscientific literature from 1982 to 1998, with thebulk of material from the mid- to late-1990s.
Study process: The Committee evaluated and up-dated CDC’s plan from 1994, Preventing EmergingInfectious Diseases.
Type of organization: Federal Government
Languages (published in): English
Key contactOrdering information: Office of Health Commu-nication, National Center for Infectious Diseases,Centers for Disease Control and Prevention,Mailstop C-14, 1600 Clifton Road, Atlanta, GA30333. Available online at http://www.cdc.gov/ncidod/emergplan
(18) Human Health Safety Criteria.Guideline 18.
Organization: Food and Drug Administration, Centerfor Veterinary Medicine; USA Department ofHealth and Human Services
Year published: Updated on July 28, 2000.
Selected key findingsNo findings are presented.
Key recommendationsAntibacterial drugs that are used in the treatmentof animals and have not been found to transferresistance to antibacterial drugs that are used inhuman clinical medicine must undertake the fol-lowing studies:• Controlled studies to determine whether or not
the antibacterial drug, given at subtherapeuticlevels, causes “an increase in the relative quan-tity or prevalence of Salmonella in animals orthe duration of shedding of these Salmonella ascompared to controls; and/or an increase in theproportion of resistant Salmonella, the degree ofresistance, and the resistance spectrum;”
• Controlled studies to determine whether or notantibacterial drugs administered to animals in-crease the number of coliforms that are resistantto antibacterial drugs that are used in humanclinical medicine and may transfer that resist-ance to human intestinal tracts;
• Controlled studies “to determine whether theconsumption of food produced by animalsreceiving antibacterial drugs will result in: a. Anincrease in the intestinal flora of the prevalenceof pathogenic bacteria; b. An increase in thedegree and spectrum of resistance of the intesti-nal flora to drugs used in human clinical medi-cine.”
The guideline also recommends the conductingof a literature survey, “to determine the incidenceof reports of hypersensitivity resulting from anti-bacterial drugs in food.”
Implementation suggestionsThe criteria are guidelines for implementing thepolicies and complying with the regulations man-dated by Congress and FDA.
Conclusions/Executive Summary“The...criteria must be satisfied in order to estab-lish that the use of low and/or intermediate levelsof an antibacterial drug in animal feeds is a safepractice from the aspect of human health. In gen-eral terms, such drug use should not result in: (1) asignificant adverse effect in the relative quantity,prevalence and shedding of Salmonella organismsin animals, (2) a significant increase of Salmonellaorganisms resistant to drugs used in human clini-cal medicine in the animal, (3) a significant increasein the resistance of coliforms to antibacterial drugsused in human clinical medicine provided this re-sistance is transferable to bacteria in man, (4) en-hancement of pathogenicity of bacteria, or (5)adverse effect to humans due to ingestion of residuesof the antibacterial drug, metabolites, or degrada-tion products.”
Authors: Not identified
Type of publication: One of 98 guidance documentscreated by the Center for Veterinary Medicine toclarify the laws made by Congress or the Food andDrug Administration that affect regulated indus-tries. They include guidance on testing procedures,manufacturing processes and scientific protocols.
Pages: 3
Intended audience: United States; regulated animalhealth/food production industries, FDA employ-ees responsible for enforcement
Study timeframe: N/A
Study process: N/A
Type of organization: Federal Government

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
116
Languages (published in): English
Key contactOrdering information: Food and Drug Adminis-tration, Center for Veterinary Medicine, Commu-nications Staff, 7500 Standish Place, HFV-12,Rockville, Maryland 20855; Telephone: (301) 594-1755
Available on the web at: http://www.fda.gov/cvm/fda/TOCs/guideline18.htmlComments and questions to: Policy and Regula-tions, Team (HFV-6), Center for Veterinary Medi-cine, Food and Drug Administration, 7500Standish Place, Rockville, MD, 20855
(19) The Path of Least Resistance
Organization: United Kingdom Department ofHealth, Standing Medical Advisory Committee,Sub-Group on Antimicrobial Resistance
Year published: 1998
Selected key findings• Although only 20% of prescriptions of anti-
microbials for human use in the UK are forhospital use, they are the site of the greatest re-sistance problems.
• Of the 50 million antibiotic prescriptionswritten each year in the UK, about 50% are forrespiratory tract infections; about 15% are forurinary tract infections.
• Incidence of methicillin-resistant Staphylococcusaureus (MRSA) increased dramatically between1989 and 1997: 1.5% of the organisms wereresistant in 1989, compared to 31.7% in 1997.
• There is every reason to anticipate the furtherspread of resistance to currently susceptibleorganisms. The most likely of these would bevancomycin-intermediate MRSA, quinoloneresistant E. coli, and the resistance of gram-negative bacteria to carbapenems. The emer-gence of penicillin resistant Neisseria meningitidisand Streptococcus pyogenes are also possible.
• The pressures of time and volume of patients inhospital emergency wards often increases thelikelihood of inappropriate antibiotic prescrip-tions.
• A lack of clinical trials on antibiotic use in long-term care facilities, combined with the vulner-able nature of the population and inadequatediagnostic capabilities, have hampered efforts tocontrol antibiotic resistance in such facilities inthe UK and the USA.
Key recommendationsThe Sub-Group recommends:• The implementation of a two-tiered national
campaign to improve community prescribing ofantibiotics: a Campaign on Antibiotic Treatmentfor general practitioners, and a National Adviceto the Public campaign for patients and con-sumers;
• “That further support for appropriate prescrib-ing in primary care be provided by developingand promulgating evidence-based nationalguidelines for the management of certain infec-tions, under the aegis of the National Institutefor Clinical Excellence [and] that such nationalguidelines are adapted for local use during thedevelopment of Health Improvement Plans;
• That [guidelines] should be integrated withincomputerized decision-support systems as soonas possible. These guidelines should also bepromulgated widely through the medical litera-ture;
• That studies be undertaken in selected hospitalsto develop and test one or more prototype deci-sion-supported systems. To be fully effective,these computer-based advisory systems shouldinclude information from local antimicrobialsensitivity profiles. These in turn should feed intoregional and national surveillance databases;
• That local prescribing information should,whenever possible, be harmonized with that inthe British National Formulary (BNF) and otherformularies. Guidelines and formularies shouldalso take account of the proposed national evi-dence-based guidelines to be produced under theaegis of the National Institute of Clinical Excel-lence all such local guidelines should include,as a minimum, certain standard items of infor-mation on the drug, dosage and duration oftherapy;”
• That greater emphasis be placed on the teach-ing of guidelines for antimicrobial prescribingto medical, dental, pharmaceutical, nursing andveterinary students;
• “That a strategic system for resistance surveil-lance of antimicrobial resistance should be de-veloped as swiftly as possible, and that thisshould cover the whole of the UK;
• That research into antimicrobial resistanceshould become a high priority for all fundingbodies concerned with health care and biomedi-cal research;”
• That existing guidelines for hospital infectioncontrol be more closely adhered to, and that

117
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
guidelines for infection control in the commu-nity be developed;
• “That the use of antibiotics in animals shouldbe guided by the same principles as those forprescribing in humans—namely, they should beused only for those clinical conditions wheretheir use is likely to provide a genuine healthbenefit;
• That alternative means of animal husbandry bedeveloped so that the use of antibiotics as growthpromoters can be discontinued;
• That consideration be given by the appropriatebodies to finding ways through pricing and othermechanisms of ensuring that investment in thedevelopment of new antibiotics remains com-mercially viable for the industry;
• That industry should be encouraged to under-take studies of optimum prescribing regimensfor new antimicrobial agents, for each indica-tion and in adults and children as appropriate;
• That every effort is made by the Government toraise the profile of antimicrobial resistance as amajor public halt issue meriting priority actionfrom all Member States of the EuropeanUnion.”
Implementation suggestionsThe committee recommends the establishment ofa National Steering Group to institute the first phaseof the national strategy to counter the developmentof antibiotic resistance. The NSG’s mandate is toform sub-groups consisting of experts who can fo-cus on particular aspects of the problem, and thento report to the Chief Medical Officer within a year.The CMO in turn may request that the StandingMedical Advisory Committee reconvene the Anti-microbial Resistance Sub-Group in order to developthe strategy’s next phase.
Conclusions/Executive Summary“The recommendations in this Report are directedtowards ensuring that best practice in antimicro-bial prescribing becomes routine practice. This willrequire a willingness, on the part of health careprofessionals and the public alike, to treat antimi-crobial agents as a valuable and non-renewableresource, to be treasured and protected in their own,and everyone else’s interest.”
Authors: Sub-Group Members: Dr. Diana Walford, A.Close, Dr. A. Dearmun, Professor T. Duckworth, A.Ewing, Dr. J. Gilley, Dr. R. Horne, Professor A.Johnson, Professor C. Peckham, Dr. S. Willatts, Dr.G. Youngs, Dr. A.M. Johnston, Professor P. Littlejohns,
C. Murphy, Dr. G. Patou, Dr. M. Powell, Dr. P. Wilkie,Professor R. Wise, Dr. P. Clappison, I. Cooper, Pro-fessor B.I. Duerden, R. Fenner, Dr. J. Leese, Dr. K.Ridge, Dr. W. Smith, M. Hart, Dr. D.M. Livermore,Dr. J.R. Weinberg
Type of publication: Report
Pages: 152
Intended audience: Primarily United Kingdom, butalso implications for global audience; policy-makers, prescribers, consumers and patients
Study timeframe: The Sub-Group reviewed literaturedating from 1969 to 1997, with a few referencesfrom the 1930s and 40s.
Study process: Review of case-studies, review of thebasis and impact of resistance, commission of anindependent review of evidence
Type of organization: Government
Languages (published in): English
Key contact: Available on the web at http://www.doh.gov.uk/smac1.htm
and from: Publications Unit, PHLS, HeadquartersOffice, 61 Colindale Avenue, London NW9 5DF;tel: 0181 200 1295
(20) Antimicrobial Resistance: A specialedition of the British Medical Journal
Organization: British Medical Journal
Year published: 1998
Selected key findings• Butler, et al., assessed the attitudes of physicians
and patients in South Wales when prescribingor withholding antibiotics for sore throats.Patient expectations for antibiotics were foundto be a compelling factor for prescription, eventhough the drugs are largely ineffective for thecondition.
• Ferranti, et al., demonstrated that amoxycillinand folate inhibitors are just as effective as newer,more expensive broad-spectrum antibiotics inthe treatment of uncomplicated acute sinusitis.
Key recommendations• Increase patient and prescriber education, sur-
veillance, and research.• For developing countries: improve prescription
regulation, access to diagnostic tools, surveil-lance, and education of the public, doctors andveterinarians.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
118
• For international organizations: achieve interna-tional consensus standards for resistance surveil-lance, and create a global repository ofinformation on resistance in key pathogens.
• For hospitals: encourage multidisciplinarycooperation in policy implementation, timelydetection and reporting of antibiotic resistantstrains, and aggressive control of the transmis-sion of epidemic resistant bacteria.
Implementation suggestionsDeveloping countries: Not specified.
International organizations: Adoption of resolutionon antimicrobial resistance that was presented at1998 World Health Assembly.
Hospitals: Needs and resources vary from hospitalto hospital; programs for infection control or thedevelopment of policies should be tailored withthose differences in mind.
Conclusions/Executive Summary“The increasing resistance problems of recent yearsare probably related to the use of increasingly broadspectrum agents (cephalosporins and fluoro-quinolones) and crowding of the most vulnerablemembers of society in daycare centers and nursinghomes. These problems are compounded by theworldwide phenomena of pressure on health caresystems for greater efficiency, with higher bedoccupancies and stretched nursing and medical care.Added to this are pressures to allow over-the-counter use of antibiotics in western countries soas to reduce health care costs. To effect change muchwill be required by the medical profession, politi-cians, the pharmaceutical industry, and not leastpatients.”
Authors: Richard Wise, Tony Hart, Otto Cars, ReinenHelmuth, Pentti Huovinen, Q. A. McKellar, DavidM. Livermore, Alasdair P. Macgowan, Martin C. J.Wale, Stef L. A. M. Bronzwaer, Richard Coker, Bjorn-Erik Kristiansen, Yngvar Tveten, Andrew Jenkins,David Wilkinson, S. B. Squire, Paul Garner, Alan P.Johnson, Marina Warner, Neil Woodford, David C.E. Speller, Valerie Schwoebel, Benedicte Decludt,Anne-Claire de Benoist, Sylvie Haeghebaert, GabrielaTorrea, Veronique Vincent, Jacques Grosset, Sarah D.de Ferranti, John P. A. Ioannidis, Joseph Lau, WilliamV. Anninger, Michael Barza, Christopher C. Butler,Stephen Rollnick, Roisin Pill, Frances Maggs-Rapport,Nigel Stott, John Turnidge, C. A. Hart, S. Kariuki, R.J. Williams, M. J. Ryan, Marc J. Struelens, HermanGoossens, Marc J. W. Sprenger, Peter M. Hawkey,
Deenan Pillay, Maria Zambon, Claude Carbon, Ri-chard P. Bax, A. M. Johnston, Christopher C. Butler,Edward A. Belongia, Benjamin Schwartz, Paul Farmer,Jim Yong Kim
Type of publication: Peer-reviewed journal
Pages: 90
Intended audience: Global; physicians, other healthcare providers
Study timeframe: varies
Study process: varies
Type of organization: Private company
Languages (published in): English, and local editionsin Belgium, Brazil, China, Greece, Hungary, LatinAmerica, Middle East, Netherlands, Pakistan,Poland, Portugal, Romania, Scandinavia, SouthAfrica, South East Asia, Turkey and West Africa
Key contactEditor, Richard Smith: [email protected];Telephone: +44 (0) 171 387 4499
(21) Select Committee on Science andTechnology: Resistance to Antibioticsand Other Antimicrobial Agents
Organization: House of Lords
Year published: 1998
Selected key findings• Drug formularies and policies vary widely
throughout the United Kingdom’s hospital sys-tem; they are often created without input fromjunior staff, and new staff are not well informedof existing policies.
• Increased hospital infections may be linked to adecline in hygiene, staffing shortages, and aNational Health Service policy of maximumoccupancy for beds.
• Reporting of resistance to the Public HealthLaboratory Service is voluntary and informal.The PHLS favors mandatory reporting of cer-tain resistances and of any unusual or unexpectedresistance markers in any microorganisms.
Key recommendations• “The Royal Colleges should increase the atten-
tion paid to antimicrobial therapy in their pro-grams of postgraduate education and vocationaltraining.
• Health authorities should step up their effortsin the areas of prescribing audits, feedback and

119
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
educational outreach (including communicationskills).
• The pharmaceutical industry and grant-givingbodies should give priority to work on rapidaffordable systems for diagnosis and susceptibil-ity testing.
• The Medicines Control Agency should considerwhether the drug licensing system could be usedmore effectively to encourage prudent use in theinterest of public health.
• Antibiotic growth promoters, such as virginia-mycin, which belong to classes of antimicrobialagent used (or proposed to be used) in man andare therefore most likely to contribute to resist-ance in human medicine, should be phased out,preferably by voluntary agreement between theprofessions and industries concerned, but bylegislation if necessary.
• The UK National Health Service should set it-self targets for controlling MRSA in hospitals,and publish its achievements. The NHS shouldalso draw up national standards and guidelinesfor community infection control management.”
Implementation suggestionsResponsibilities were delegated to various govern-ment agencies and departments of the United King-dom.
Conclusions/Executive Summary“This enquiry has been an alarming experience,which leaves us convinced that resistance to antibi-otics and other anti-infective agents constitutes amajor threat to public health and ought to be rec-ognized as such more widely than it is at present.We commend the current trend towards local anti-biotic formularies and evidence-based clinicalguidelines, giving professionals agreed definitionsof prudent practice in particular situations. But theissuing of documents is not enough to turn policyinto practice; it must be followed through in pro-fessional education, and continuing professionaldevelopment. We do not recommend that GPsshould be required to establish antimicrobialsusceptibility before prescribing. This, we believe,would at present be impracticable, and would over-load diagnostic series which are already stretched.But improved access to microbiological testingclearly reduces uncertainty in prescribing. Potentagents important to human medicine, such as thefluoroquinolones, deserve extreme economy of usein veterinary practice. There is still much that needsto be done to increase understanding of the mecha-
nisms of resistance and the action of antimicrobialsand, in the clinical sphere, methods of using agentsto best advantage.”
Authors: Sub-Committee members: Lord Dixon-Smith,Lord Gregson, Lord Jenkin of Roding, BaronessMcFarlane of Llandaff, Baroness Masham of Ilton,Lord Perry of Walton, Baroness Platt of Writtle,Lord Porter of Luddenham, Lord Rea, Lord Soulsbyof Swaffham Prior, Lord Walton of Detchant, LordWinston; with Specialist Advisors Professor HaroldLambert and Professor Richard Wise
Type of publication: Report
Pages: 108
Intended audience: United Kingdom; policy-makers,general public
Study timeframe: July 1997 to March 1998
Study process: Sub-Committee members conductedinterviews at the Headquarters of the Public HealthLaboratory Service, King’s College Hospital, andwith individual experts in the United States andUnited Kingdom. Members also gathered evidencefrom the agricultural and pharmaceutical industries,international and regional health organizations, andprofessional medical and scientific societies.
Type of organization: Government
Languages (published in): English
Key contactThe Publications Centre: PO Box 276, LondonSW8 5Dt; Tel. +44 0345 58 54 63; fax +44 0170873 8200; Web site: http://www.hmso.gov.uk/
(22) Antimicrobial Resistance: Issues andOptions. Workshop Report from theForum on Emerging Infections
Organization: Institute of Medicine
Year published: 1998
Selected key findings• The global effort to control antibiotic resistance
lacks adequate surveillance mechanisms andcomprehensive databases.
• There is a lack of research on the greater im-pacts of antibiotic use in animals, including thetransfer of resistance.
• There has been insufficient analysis of the reser-voir of antimicrobial drug-resistant genes.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
120
Key recommendationsSurveillance:• “Funding, implementation, assumption, or
assignment of leadership, and formation of part-nerships for implementing the 1995 AmericanSociety of Microbiology’s detailed recommen-dations for a comprehensive resistance surveil-lance program;
• Improving data gathering and analysis, perhapsthrough national systems that would continu-ously monitor antimicrobial usage in hospitals,community and farm environments;
• Including information about the effects ofresistance on the outcome of infections in datacollection systems;
• Selecting and strengthening the laboratories ina set of sentinel hospitals as bases for globalassessment of the prevalence and transmissionof the most critical antibiotic-resistant genes,including training laboratory personnel in sen-tinel hospitals in standardized methodologies;
• Designing categories and pathways for reducingdata sets into comprehensive packages for useby clinicians and researchers;
• Expanding distribution of NCCLS Guidelinesand perhaps increasing the frequency with whichthey are updated.”
The use of antibiotics in food production• “Collaborative access to data from veterinary
reference laboratories;• Systematic, collaborative development, by the
United States Department of Agriculture, theAmerican Veterinary Medical Association, theFood and Drug Administration and producerorganizations, of strategies and educationalmaterials toward expanding ecological under-standing;
• Developing cost-benefit and cost-effectivenessmodels of different on-farm antibiotic usages toenhance the public health community’s under-standing of farmer perspectives.”
Prolonging antibiotic effectiveness• “Implementing a joint project involving all per-
tinent professional societies in developing uni-tary guidelines (including checklists for providersto use in clinical settings) for antimicrobial use,implementing their extensive dissemination,and, very importantly, updating them periodi-cally based on annual data from longitudinalstudies;
• Quantifying the risks of injudicious antimicro-bial use and developing descriptive and predic-
tive models of the differences that judicious usewould make, to help in policy development,advocacy, and action;
• Designing and implementing research on clini-cal outcomes from shorter courses of therapy anddifferent dosing regimens, as the basis for up-dating practice guidelines and revising labeling.”
Developing new products• “Conduct studies of gene flow in order to
understand the diversity and prevalence of re-sistant gene families and to discern the originsof resistant genes and how they spread from oneorganism to another.”
Legal and regulatory approaches• “Exploring whether increased resistance and
rapid diminution of effectiveness of existing an-tibiotics might justify awarding greater author-ity to the CDC to monitor and enforce legalduties regarding resistance, and consideration ofthe means by which this might be accomplished;
• Developing alternative ways to define efficacy-for example, surrogate markers, in vitro tech-nologies, and animal models-to address the lackof well-defined populations for clinical trials.”
Implementation suggestionsExisting projects of various government agenciesand departments of the United States are cited asfoundations for implementing the above recom-mendations, including: a surveillance projectbeing conducted by CDC, USDA and FDA; theUSDA’s reports on food safety and antibiotic re-sistance; and the EPA’s considerations of the use ofantibiotic pesticides. The food-production indus-try is also cited as a potential source of funding,research, and the development of guidelines forprudent antibiotic use in food-producing animals.
Conclusions/Executive Summary“The evidence and opinions presented at this work-shop suggest…that the transition from a histori-cally generous armamentarium to one at leasttemporarily much less lavish could be mitigated bywiser policies, both to conserve what remains andto plan for what is to come; policies for the mostcost-effective use of antibiotics; evidence-basedregulation, with transparent balancing of risks andbenefits; and as already exemplified in genomeprojects, social investment in the underlying sci-ence needed to develop new antimicrobial agents.Also, because antimicrobial drug resistance is in-creasingly known to be a global problem, it can be

121
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
addressed only with international cooperation, ata minimum in the acquisition and sharing of in-formation. Whatever frictions might ensue fromshaping and implementing such policies would bemore than offset by the savings in medical and hos-pital costs and, most importantly, by the deaths anddisability avoided.”
Authors: Editors: Polly F. Harrison and JoshuaLederberg. Forum Participants: Joshua Lederberg, Vin-cent I. Ahonkhai, Steven J. Brickner, Gail H.Cassell, Gordon H. Defriese, Nancy Carter Foster,Renu Gupta, Margaret A. Hamburg, DieterHinzen, James M. Hughes, J. Stanley Hull, SamuelL. Katz, Kenneth W. Kizer, William Kohlbrenner,John R. LaMontagne, Carlos Lopez, Stephen S.Morse, Solomon Mowshowitz, Stuart L. Nightin-gale, Michael T. Osterholm, David M. Shlaes, JohnD. Siegfried, P. Frederick Sparling. Forum Liaisons:Barry R. Bloom, Enriqueta C. Bond, GaryChristopherson, Michael Hughes, Stephanie James,C. Michelle Limoli, Stephen M. Ostroff, GaryRoselle, Fred Tenover. Study Staff: Jonathan R. Davis,Polly F. Harrison, Gretchen G. Kidder, ChristinaThacker
Type of publication: Workshop Report
Pages: 115
Intended audience: United States; policy-makers, gov-ernment
Study timeframe: Workshop conducted in July of1997
Study process: Workshop discussion, with partici-pants from government, industry and academia
Type of organization: Non-profit public health andadvisory organization; advisor to Federal Govern-ment on issues of public health
Languages (published in): English
Key contactOrdering information: National Academy Press,http://www.nap.eduContent: Joshua Lederberg, Chair, Forum onEmerging Infections
(23) Protecting the Crown Jewels ofMedicine: A Strategic Plan to Preservethe Effectiveness of Antibiotics
Organization: Center for Science in the Public Inter-est
Year published: 1998
Selected key findingsNo original key findings; report cites findings fromoriginal sources of research.
Key recommendations• Congress should allocate funding for an antibi-
otic use initiative (including public and profes-sional education, national surveillance, researchand development, etc.).
• The Department of Health and Human Servicesshould include goals for decreasing inappropri-ate use of antibiotics and antibiotic resistance inits Healthy People 2010 initiative.
• The FDA should change its policies on antibi-otic advertising to curtail inappropriate antibi-otic use.
• The FDA should ban all subtherapeutic uses ofantimicrobial agents that are used in humanmedicine or might select for cross resistance toantimicrobials used in human medicine.
Implementation suggestions• Increased funding from Congress to implement
national education programs and surveillance.• Government health care facilities should serve
as models for the prudent use of antibiotics.
Conclusions/Executive Summary“Despite antibiotics’ extraordinary value, the over-use of those miracle drugs in medicine and agricul-ture endangers their continued effectiveness. Themore antibiotics are used, the more likely it is thatbacteria will develop mechanisms to evade them.The development of new antibiotics has not keptup with the development of antibiotic resistance.The time has come when public and private insti-tutions, as well as the general public, must changetheir policies and practices to prevent further in-creases in antibiotic resistance. Rather than believ-ing that new drugs continually can be developedto treat antibiotic-resistant infections, public-healthprevention measures should be adopted.”
Authors: Patricia B. Lieberman, Ph.D., Margo G.Wootan, D.Sc.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
122
Type of publication: Booklet
Pages: 27
Intended audience: United States; general public
Study timeframe: Works cited incorporate researchfindings from 1972 to 1998.
Study process: Compilation of statistics and infor-mation from other sources (USDHHS, CDC,American Society for Microbiology, scientific jour-nal articles, etc.).
Type of organization: Non-profit, public health organi-zation
Languages (published in): English
Key contactCenter for Science in the Public Interest, 202-332-9110
(24) The Agricultural Use of Antibioticsand Its Implications for HumanHealth
Organization: United States General Accounting Of-fice
Year published: 1999
Selected key findingsExperts from the Department of Health andHuman Services, CDC and FDA “believe that re-sistant strains of three specific organisms that causeillness or disease in humans—Salmonella, Campylo-bacter, and E. coli—are linked to the use of antibi-otics in animals.”
There is only one federal program that specifi-cally tests for antimicrobial resistance related toagriculture: the National Antimicrobial ResistanceMonitoring System’s Enteric Bacteria program. Theprogram tests samples of Campylobacter andSalmonella from humans and animals for suscepti-bility to 17 antibiotics.
“About 95 percent of Salmonella DT-104 strainsare resistant to five antimicrobials—ampicillin,chloramphenicol, streptomycin, sulfonamides, andtetracycline.”
Between two and four million people each yearcontract Campylobacter infections; out of every1,000 reported cases, one will develop into Guillain-Barré Syndrome, which may result in paralysis.
Key recommendationDevelopment and implementation of a plan by theSecretaries of Agriculture and of Health and
Human Services that creates a framework for evalu-ating the risks and benefits of the current andfuture uses of antibiotics in agriculture.
Implementation suggestionsThe Departments of Agriculture and Health andHuman Services would create the plan, devisingthe goals and timeframes, and identifying the re-sources necessary to determine the safest uses ofantibiotics in agriculture. The Departments will alsosee to the filling of the existing gaps in data andresearch.
Conclusions/Executive Summary“Although research has linked the use of antibiot-ics in agriculture to antibiotic-resistant strains ofspecific foodborne pathogens that affect humans,agricultural use is only one factor in the emergenceof antibiotic resistance in non-foodborne patho-gens. Debate exists over whether the role ofagricultural use in the overall burden of antibiotic-resistant infections of humans warrants furtherregulation or restriction. CDC believes the poten-tial human health risks call for action to restrictantibiotics for growth promotion in animals. Wefirst raised concerns in 1977 about the potentialhuman health risks of this practice. Today, morethan two decades later, federal agencies have notreached agreement on the safe use of antibiotics inagriculture. In developing a federal response, bothhuman health concerns and the impact on the ag-riculture industry are factors to consider.”
Authors: Major Contributors: Robert E. Robertson, ErinLansburgh, Stuart Ryba, Natalie Herzog, JerrySeigler, Shannon Bondi.
Type of publication: Report to Senator Tom Harkin,Ranking Minority Member, Committee on Agri-culture, Nutrition, and Forestry.
Pages: 33
Intended audience: United States
Study timeframe: The review was conducted betweenMay 1998 and April 1999. It covered material from1969 through 1999.
Study process: The authors conducted interviews withrepresentatives from USA government agencies, theagricultural industry, and agricultural associations.They also reviewed existing research on the subjectand consulted with experts and officials from CDC,FDA, USDA, and others to get their opinions onthe material.

123
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Type of organization: Federal Government
Languages (published in): English
Key contactOrdering information: USA General AccountingOffice, P.O. Box 30750, Washington, D.C., 20013;tel.: (202) 512-6000; fax: (202) 512-6061
Available on the web at: http://www.gao.gov/
(25) The Use of Drugs in Food Animals:Benefits and Risks. Report by theCommittee on Drug Use in FoodAnimals and the Panel on AnimalHealth, Food Safety, and PublicHealth
Organization: National Research Council
Year published: 1999
Selected key findings• “Use of antibiotics increases the risk of emer-
gence of microorganisms that are resistant tospecific, and perhaps other, antibiotics. Devel-opment of this kind of resistance is not restrictedto antibiotic use in food animals; it is far moreprevalent because of misuses in human medi-cine;
• A link can be demonstrated between the use ofantibiotics in food animals, the development ofresistant microorganisms in those animals, andthe zoonotic spread of pathogens to humans. Theincidence of the spread of human disease in thatway is historically very low, but data are seriouslyinadequate to ascertain whether the incidenceis changing;
• A major impediment to determining the effectof antibiotic use in food animals on humanhealth risk is the complexity of food animal drugtreatment and subsequent food-processing andhandling interactions. Post-farm good process-ing, storage and improper handling and cook-ing are major contributors to the chain of eventsthat allows the pathogen to contaminate theproduct, proliferate on or in the food, and at-tain the large numbers that cause disease;
• Substantial information gaps contribute to thedifficulty of assessing the effect of antibiotic usein food animals on human health.”
Key recommendations• “The Center for Veterinary Medicine should
continue procedural reform to expedite the drugapproval review process and broaden its perspec-
tive on efficacy and risk assessment to encom-pass review of data on products already approvedand used elsewhere in the world;
• To improve drug availability, worldwide harmo-nization of requirements for drug developmentand review should be considered and furtherenhanced among the federal agencies that areresponsible for ensuring the safety of the foodsupply;
• The Center for Veterinary Medicine should basedrug use guidelines on maximal safe dosage regi-mens for specific food animals, consider greateremphasis on the pharmacokinetics of drug elimi-nation from tissues that are consumed in largequantity, and set drug withdrawal times accord-ingly;
• Increased funding for basic research that exploresand discovers new or novel antibiotics andmechanisms of their action, including the de-velopment of more rapid and wide-screen diag-nostics to improve the tracking of emergingantibiotic resistance and zoonotic disease;
• Establishment of integrated national databasesto support a rational, visible, science-driven de-cision-making process and policy developmentfor regulatory approval and use of antibiotics infood animals, which would ensure the effective-ness of these drugs and the safety of foods ofanimal origin;
• The committee recommends that further devel-opment and use of antibiotics in both humanmedicine and food animal practices have over-sight by an interdisciplinary panel of expertscomposed of representatives of the veterinaryand animal health industry, the human medi-cine community, consumer advocacy, the ani-mal production industry, research, epidemiology,and the regulatory agencies;
• Increased public- and private-sector research onthe effect of nutrition and management prac-tices on immune function and disease resistancein all species of food animals;
• Increased public- and private-sector research onstrategies for the development of new vaccina-tion techniques, on a better understanding ofthe biochemical basis of antibody production,and on genetic selection and molecular geneticengineering for disease resistance.”
Implementation suggestionsIssues concerning antibiotic use in food animals andhumans should be coordinated with regard to usepatterns, resistance trends, surveillance data, and

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
124
recommendations for use in a partnership of regu-latory agencies, pharmaceutical companies, the foodanimal industry, and animal and human health careprofessionals.
Conclusions/Executive Summary“The committee concludes that the use of drugs inthe food animal production industry is not with-out some problems and concerns, but it does notappear to constitute an immediate public healthconcern; additional data might alter this conclu-sion. The greatest concern is associated with theuse of antibiotics in food animals in such a waythat there is a potential for antibiotic resistance todevelop in or be transferred to pathogens that cancause disease in humans. This report acknowledgesthat there is a link between the use of antibiotics infood animals, the development of bacterial resist-ance to these drugs, and human disease—althoughthe incidence of such disease is very low. A sub-stantial change in the human health risk posed byantibiotic use would affect not only how animaldrugs are reviewed, approved, and used, but alsohow food animals are produced. It should be notedthat antibiotics are still effective for their intendedpurposes at the recommended dosages. New anti-biotic drugs are needed to combat emerginganimal diseases that do not respond to traditionaldrugs and so threaten public confidence in animalagriculture and human medicine. Professionals inhuman health care should be concerned that theydo not have enough specialty antibiotics to treatresistant and emerging infections in humans, asshould veterinarians. The question is, should newlydiscovered medications be held in reserve forhuman or animal use only? Antibiotics should beavailable to treat specific human and animal dis-ease with proper accountability and oversight ofthe drugs used.”
Authors: Committee on Drug Use in Food Animals: JamesR. Coffman, George W. Beran, Harvey R. Colten,Connie Greig, Jean Halloran, Dermont Hayes, JohnB. Kaneene, Kristin McNutt, David Meeker, StephenC. Nickerson, Thomas Seay, R. Gregory Stewart. Panelon Animal Health, Food Safety, and Public Health: John
A. Shadduck, Kenneth Berns, Michael P. Doyle, HollisN. Erb, John Ferry, Jere E. Goyan, Werner Heuschele,Helen H. Jensen, Franklin M. Loew, Joy A. Mench,Harley Moon, Wilson G. Pond, R. Gregory Stewart.Board on Agriculture: Dale E. Bauman, John M. Antle,Sandra S. Batie, May R. Berenbaum, Leonard S. Bull,William B. Delauder, Anthony S. Earl, Essex E.Finney, Jr., Cornelia Flora, George R. Hallberg, Ri-chard R. Harwood, t. Kent Kirk, Harley W. Moon,William L. Ogren, George E. Seidel, John W. Suttie,James J. Zuiches. Food and Nutrition Board: CuthbertoGarza, John W. Erdman, Lindsay H. Allen, BenjaminCaballero, Fergus M. Clydesdale, Robert J. cousins,Michael P. Doyle, Johanna T. Dwyer, Scott M.Grundy, Charles H. Hennekens, Janet C. King,Sanford A. Miller, Ross L. Prentice, A. Catharine Ross,Robert E. Smith, Virginia A. Stallings, Vernon R.Young.
Type of publication: Report
Pages: 253
Intended audience: United States; food-productionindustry, policy-makers, veterinarians
Study timeframe: The report considers informationfrom 1968 to 1998.
Study process: The Committee reviewed the majorclasses of drugs used in food animals; reviewed sci-entific literature; heard testimony on animal-drug-related issues; reviewed federal regulations thatprovide guidelines and list mandatory practices fordrug use, monitoring capabilities for drugs andresidues in foods, veterinary oversight in prescrip-tion drug use, rates of violations, and instances ofdocumented health problems.
Type of organization: Non-profit organization, theworking arm of the National Academy of Sciencesand the National Academy of Engineering
Languages (published in): English
Key contactOrdering information: National Academy Press,http://www.nap.eduContent: James R. Coffman, Chair, committee onDrug Use in Food Animals

125
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
APPENDIX B
Local action around the world
Activities of the APUA Latin American Initiative
The Latin America Initiative increases the impactand reach of chapter work by providing a mecha-nism to link countries and share resources, infor-mation, and expertise. Activities supported throughthe initiative include country-specific projects aswell as efforts to develop regional communicationsand region-wide research and educational activi-ties. These activities are coordinated to build onPAHO activities at the country and regional levels.This section includes a list of activities in the re-gion supported by APUA or conducted in collabo-ration with WHO, PAHO, ministries of health,and other institutions and organizations.
Chapter development activities
The Latin America Initiative has grown from theinitial group of five country chapters to include thefollowing countries: Argentina, Chile, Colombia,Cuba, Dominican Republic, Ecuador, Guatemala,Mexico, Venezuela and Uruguay. Efforts are cur-rently underway to establish APUA chapters in thefollowing countries:Bolivia, Brazil, Costa Rica, ElSalvador, Honduras, Nicaragua, Paraguay and Peru.
Research activities
• A study conducted by our Uruguay chapter in1999 compared the rate at which antibiotics wereprescribed for children with pharyngitis to theactual need for antibiotics, based on the percent-age who tested positive for Streptococcus pyogenes.The study showed that while 75% of the 212children who presented with pharnygitis at anoutpatient clinic were prescribed antibiotics,only 15% tested positive for Group A Strepto-coccus pyogenes (GAS). By demonstrating theoveruse of antibiotics for children with pharyn-gitis, the study aims to persuade pediatriciansto modify their prescribing habits. The study wasfunded by the Ministry of Health, PAHO, andAPUA.
■ APUA Latin American Initiative
Report prepared by APUA
The mission of APUA is to promote the prudentuse of antibiotics in order to preserve their powerfor future generations. The establishment of for-eign-affiliated chapters to conduct research andeducation activities tailored to local needs is animportant vehicle for achieving this goal. APUA’sLatin America Initiative was developed tostrengthen and expand existing APUA country ac-tivities to curb the development of antibiotic re-sistance and to coordinate these activities withrelated activities in the region. Through the Initia-tive, APUA’s regional network of chapters has grownfrom five to ten, with eight additional countries inthe process of developing chapters. This regionalinitiative has been funded largely by the UnitedStates Agency for International Development(USAID) and the Pan American Health Organiza-tion (PAHO) and is being implemented in collabo-ration with PAHO’s IMCI (IntegratedManagement of Childhood Illness) Unit.
A key feature of the Initiative is the network ofAPUA country chapters. With a strong foundationin microbiology and infectious disease, chaptermembers work at the grassroots level to tailor in-terventions to local situations and to provide a linkbetween data and action within their countries.Through the Initiative, APUA is collaborating withPAHO and its Member States to develop interven-tions to curb antibiotic resistance. PAHO, withAPUA and other partners, has been involved indeveloping a strategic plan for the surveillance ofantibiotic resistance as well as laboratory trainingactivities to support a regional surveillance network.APUA has also been working with the IMCI Unitof PAHO to develop and implement projects tocurb antibiotic resistance within the context ofIMCI. APUA will continue to expand its networkof chapters in Latin America and support existingchapters as they work more aggressively towardsdocumenting, understanding, and containing an-tibiotic resistance.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
126
• In 2000, APUA funded a study by its Guatema-lan chapter titled “Study of the Risk Factors forAntibiotic Resistance of S. pneumoniae amongGuatemalan Children from Different Socio-Economic Strata and Health Care Delivery Sys-tems”, to be completed in 2001.
• APUA, in collaboration with PAHO, is conduct-ing a regional survey of physician’s knowledge,attitudes, and practices (KAP) regarding antibi-otic resistance and use. The survey, developedby APUA and pilot-tested in Argentina, willinitially be conducted in 9 countries, and willinform the development of appropriate treat-ment guidelines and provider educationalmaterials.
• APUA provides technical assistance to chaptersin the region, including help with meeting andconference planning, providing speakers, sup-porting the south-to-south exchange of exper-tise, and proposal development for grants fromAPUA and other funding sources.
• Five chapters were awarded grants from the 2000Joint Initiative to conduct research on antibi-otic use. APUA provided technical supportduring proposal development.
• APUA chapters contributed to the IMCI Newsbulletin produced by PAHO.
• The new APUA chapter in Colombia has plansto develop a surveillance and reporting networkfor antibiotic resistance in tertiary hospitalsthroughout the country using WHONET soft-ware. The plan includes the dissemination ofregular reports on resistance to hospitals andnational health authorities, including a formalannual report from the network.
Training and educational activities
• APUA conducted a Continuing Medical Edu-cation session on “Improving Antibiotic Use inthe Management of Childhood Illnesses” heldin June 2000 at the Global Health Council an-nual meeting in Washington, DC. This session,attended by clinicians, public health profession-als and policy makers, featured background in-formation on the antimicrobial resistanceproblem, specifically as it relates to children’shealth in Latin America. It also described theAPUA-PAHO/ IMCI partnership as a model forcollaborative work to contain resistance andother related projects sponsored by the two
organizations, such as surveillance, capacity-building, and provider trainings.
• APUA provided assistance in the design of acomprehensive one-week training course in test-ing organisms for susceptibility to antibiotics andresistance surveillance, which was conducted bythe Ministry of Health in Argentina, in collabo-ration with PAHO and the APUA-Argentinachapter. APUA plans to adapt the course for usein other countries in the region, in collabora-tion with PAHO.
• In collaboration with PAHO, APUA produceda Spanish version of the APUA patient educa-tion brochure and health care provider wallposter for distribution via PAHO and APUAchapters throughout Latin America.
• APUA supported the development or transla-tion of articles in Spanish on otitis media andthe prevention and treatment of pneumococcalinfections, that were published on the APUAWeb site and in the monthly bulletin of PAHO’sIMCI programme.
• A week-long Latin America regional trainingcourse on laboratory surveillance methods fordetecting antimicrobial resistance, was held inApril 2000 in Buenos Aires, Argentina. Thecourse was organized and designed by theArgentine Ministry of Health and foundingmembers of APUA-Argentina, with assistancefrom PAHO and APUA. One hundred micro-biologists from Argentina, as well as 20 partici-pants from other Latin American countries,attended this hands-on training to improve andupdate their skills and knowledge in suscepti-bility testing techniques, specific organisms,interpreting test results, quality control, and themanagement of susceptibility data. Participantswill take these newly-acquired skills and knowl-edge back to their colleagues. APUA and PAHOplan to sponsor similar trainings in other LatinAmerican countries, after adapting the courseto address challenges faced by less developedcountries in the area. The refined curriculumwill also serve as a model for other countries withlimited resources outside of the region.
Conference and networking activities
• APUA, in collaboration with PAHO and the PanAmerican Association for Infectious Diseases,organized a symposium on “Prudent Use ofAntibiotics in the Developing World” during the

127
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
International Congress on Infectious Diseases(ICID) in Buenos Aires in April 2000. The sym-posium covered partnerships to address antibi-otic resistance, the application of communityresearch results to clinical practice, effective strat-egies for provider education, and the process ofdesigning clinical guidelines for antibiotic use.
• APUA has established a Spanish-languagelistserve for the Latin America region. Thelistserve, moderated by APUA’s Latin AmericaProject Director, allows Latin American healthprofessionals to regularly exchange informationon research related to antibiotic resistance anduse, offer or seek technical assistance from otherparticipants, and post announcements of up-coming meetings and funding opportunities.
■ Moldova: Nongovernmentalorganizations and antibioticprogrammes
Report prepared by Natalia Cebotarenco, Ph.D., Directorof the Association Drugs, President APUA Moldova,“natalie”@drugs.mldnet.com [email protected]
Antibiotics have revolutionized the treatment ofcommon bacterial infections and have a vital rolein reducing child mortality. Since antibiotics werefirst introduced, their consumption has increaseddramatically in most parts of the world. Resistantbacterial strains have emerged and spread through-out the world because of the remarkable geneticplasticity of the microorganisms, heavy selectivepressures of antibiotic use, and the mobility of theworld’s population.
The problem of resistance to antimicrobial drugsis particularly troublesome in a country like theRepublic of Moldova that also has economic andsocietal problems. After the collapse of the Sovietsystem, Moldova instituted an economic reformthat tried to establish a market economy. The eco-nomic changes led to increasing numbers ofprivate pharmacies. Moldova has 4.35 million citi-zens and 1500 registered pharmacies. More than85% of the pharmacies are private. This situationbrought a flood of medicines on the market inMoldova and created a situation of uncontrolleddispensing of medicines.
Increasing the availability of antibiotics and en-hancing their appropriate use are two interrelatedaims. With the increasing quantity and variety ofpharmaceuticals available today in Moldova, the
potential inappropriate use of antibiotics is a grow-ing concern. The sale of medicines by prescription,including antibiotics, has almost ceased in Moldova.Officially, antibiotics are prescription-only drugsin Moldova. In practice, they are widely availablein many pharmacies and even on the streets. Thedoctors’ recommendations are often ignored as pa-tients are lured by drug store offers. On the otherhand, doctors are extremely underpaid in Moldovaand can gain some money by selling or prescribingantibiotics. Thus it is often hard to discuss the con-cept of a rational choice of an antibiotic with healthcare providers and the general public.
The situation in Moldova shows several prob-lems associated with the use of antibiotics includ-ing widespread inappropriate antibiotic use, youngchildren frequently medicated with antibiotics fortoo short a course, and a vast majority of self-medi-cated treatment regimes. Only one-sixth or one-seventh of the antibiotics are recommended by adoctor and resistant respiratory pathogens are wide-spread among the children.
A non-governmental medical organization is formed toprovide drug information
With new political possibilities in 1995, a medicalnon-government organization, AssociationDRUGS, was established in Moldova. The Asso-ciation DRUGS provides unbiased, up-to-dateinformation on the safety and efficacy of drugs tointerested health professionals, consumers andgovernment institutions such as the Ministry ofHealth, the National Institute of Pharmacy, theMoldavian Medical and Pharmacy University“N.Testemitanu”.
The first project by the Association DRUGS in1995 was the establishment of the InformationCentre with the goal of promoting rational druguse and the Essential Drugs concept in Moldova.
Since its beginning, the Association DRUGS hasprovided 47 seminars and training sessions on vari-ous aspects of rational drug use at the hospitals inChisinau (capital of Moldova) and in regions ofMoldova, as well as the Postgraduate Faculty of theMedical and Pharmacy University of the Republic.More than 2,700 physicians and pharmacists tookpart in its educational programmes. Since January1996, 34 issues of the independent Drug Bulletinwere published with 1,500 samples distributed free-of charge for physicians and pharmacists. Throughthe activity of Association DRUGS, a network wascreated for rational drug use in Moldova, which

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
128
included authorities from the Ministry of Health,the National Institute of Pharmacy, Medical andPharmaceutical University of Moldova, pharma-cists, physicians, journalists and non-governmen-tal organizations.
From the beginning of the activity in 1995, theAssociation DRUGS analysed 1500 records fromthe children’s hospital “V. Ignatenco” in Chisinau(the capital of Moldova), focusing on physicians’antibiotic prescriptions. The most commonpediatricians’ problems were inappropriate antibi-otics prescriptions that included polytherapy andthe overprescribing of antibiotics:
• Acute respiratory infections were treated with1–2 antimicrobials
• Acute pneumonia was treated with 2–3 anti-microbials, occasionally 4 antimicrobials
• Predominance of antibiotic injections
• Duration of treatment too short (fewer than 3days) or too long (more than 15 days)
• Overuse and too high a dose of antimicrobials
• Inappropriate choice of antibiotic group
• Predominance of gentamicin and cefalosporinsof the second or third generation
• Non-consideration of microbiology controlbefore or during treatment course by antibiotic
• Non-consideration of the problem of antibioticresistance in daily work.
The survey showed that there was no professionalawareness of the problem of antibiotic resistance.Antibiotic resistance problems have not been andare not identified as national priorities of the healthcare system.
Was education of pediatricians carried out continually?Were guidelines for treatment developed?
Given the chronic state of deficient funding thatcovers only 5–7% of the hospitals’ needs, the anti-biotic resistance problem must be approached bychanging the educational system for physicians.However, the education programmes in the medi-cal school and University of Moldova do not in-clude the themes “Formulary system in thehospital”, “Analyzing the cost-effectiveness of treat-ment”, “Essential Drugs Lists development”,“Rational drug use” and other items in the update.
In Moldova, the guidelines for the treatment ofthe most common infectious diseases were devel-oped and distributed without general discussion orfollow-up; a few scientific seminars were formal-
ized but were not necessarily interactive. Practicallyspeaking, the treatment guidelines are not availableto many physicians. Many Moldavian pediatricians’English knowledge is not good enough to allowthem to get information or enable them to followinternational recommendations and guidelines. Forthese reasons the guidelines do not work in Moldovayet.
Considering that the incorrect prescribing ofantibiotics by physicians is one of the factors thatstimulates the development of antimicrobial resist-ance, it is necessary to create an appropriate educa-tional strategy.
How can the behaviour of pediatricians be changed?
As poor prescription practices were originallyattributed to a lack of appropriate prescribing in-formation, the main strategy focused on providingup-to-date information regarding appropriate pre-scriptions of antibiotics and the antimicrobialresistance problem. Education on the proper useof antibiotics has a limited effect if the existing drugdistribution patterns and information sources arenot rationalized. Health workers who try to changepatterns of antibiotic use realize more and morethat what is rational depends very much on whatpeople think is rational, what their living condi-tions are and what drugs and diagnostic tools areavailable in the health care context.
In order to improve the situation with inappro-priate antibiotic prescriptions, a training pro-gramme has been developed with the support ofthe APUA and United States Pharmacopoeia incollaboration with the Association DRUGS inMoldova. The health training programme wascreated in 1998-1999 to help middle and lower levelhealth workers, especially pediatricians, learn to useantibiotics more wisely and to help prevent antibi-otic resistance.
A pilot training programme was conducted atthe Moldavian Medical and Pharmacy Universityto explore the practicalities, acceptance and educa-tional value of the postgraduate department’spediatricians. During a needs assessment period,meetings were held with authorities from the Min-istry of Health, pediatricians from the different lev-els of the health system, and pharmacists to helpidentify barriers to rational antibiotic use. In addi-tion, teachers from academic institutions becameinvolved. These groups see the need to change themedical curriculum to include the antibiotic resist-ance problem and to monitor prescribing practices

129
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
in different health care facilities. Concerns expressedincluded the high number of prescriptions, inad-equate information about antibiotic use, and prob-lems with the poor quality of donated antibiotics.
The educational programme had five compo-nents:
1. Questionnaire assessment of Knowledge,Attitude and Practice Survey (KAPS) of middleand lower level pediatricians.
2. “Improving Antibiotics Use” Training.
3. Distribution of the manual, “AntibacterialTherapy”, in Russian to the participants of thetraining issued by the United States Pharmaco-poeia.
4. Distribution of the APUA Newsletter amongpediatricians and publishing the result of theKAPS-survey in the informational bulletin of theAssociation DRUGS.
5. Using mass media to attract the public’s atten-tion to the topics of antibiotic rational use andantibiotic resistance.
The session of the training “Improving Antibi-otics Use”consisted of:
• How to choose the most cost-effective anti-biotics for essential drug list and formulary
• Control the rise of antibiotic resistance
• Limit antibiotic over-prescribing
• Limit over-prescribing due to patient pres-sure
• Guidelines for drug donations
• Risks of using antibiotics for the treatmentof acute respiratory infections.
The effectiveness of the training in increasingthe students’ knowledge of rational antibiotic useand antibiotic resistance problems was measuredby a pre-test and post-test multiple choice exami-nation. Evaluations showed that the course in-creased the knowledge and understanding ofpediatricians, helped them develop more positiveattitudes, and demonstrated the importance ofmultiprofessional teamwork and communicationamong the physicians’ different specialities. Partici-pating pediatricians believed that postgraduatecourses should include early and regular opportu-nities for shared learning.
The key principle underpinning this frameworkis that a range of educational transactions may needto occur for learning to be effective.
The development of training programmes in
hospitals is still largely at a rudimentary level inMoldova. Appropriate training experiences in man-aged care organizations may be a valuable strategyto address the current disconnect between thetraditional hospital-based education of pediatriciansand the expanded competencies necessary to prac-tice in intensively managed, integrated and account-able health systems. A main assumption is that anew learning strategy will either fit into existingpatterns or trigger changes in the way that teach-ers/trainers and learners talk together.
References
1. Kunin CM. Ann Intern Med 1993 Apr 1;118(7):557–61.
2. Ansari MZ. JPMA J Pak Med Assoc 1995 Jan;45(1):18–23.
3. Ireland LM; Powell C. Br J Nurs 1997 JUN 26–Jul9;6(12):686–90.
4. Parsell G; Spalding R; Bligh J Med Educ 1998 May;32(3):304–11.
5. Okeke IN; Lamikanra A; Edelman R. Emerg InfectDis 1999 Jan-Feb;5(1):18–27.
6. Quick JD et al., eds. Managing Drug Supply, 2nded. USA Kumarian Press 1997
■ Nepal: Developing a nationalantibiotic policy
Report prepared by Mr. Shyam P. Lohani, M. Pharm.,Programme Coordinator, United Hands to Nepal,Chapter Coordinator, APUA Nepal. Contact:[email protected]
Background
The Drug Act was promulgated in Nepal in 1978to 1) control the production, distribution, sale,export and import of drugs and 2) to ensure theavailability of safe, quality and efficacious drugs tothe general public. Its first amendment was addedin 1988. To prevent misuse and abuse of drugs, allof the available drugs are classified into three cat-egories according to their composition, efficacy anduse as per the provision of the Drug Act. The threecategories are:
1. Group ‘Ka’—Narcotic, psychotropic drugs andpotent active therapeutic agents.
2. Group ‘Kha’—Antibiotics, hormones and gen-eral therapeutic agents.
3. Group ‘Ga’—Other common drugs which aresafer.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
130
Drugs in groups ‘Ka’ and ‘Kha’ are prescriptivedrugs while those in group ‘Ga’ are over the coun-ter drugs. According to the Drug Act, drugs placedin the ‘Ka’ and ‘Kha’ categories are to be prescribedby practitioners registered with the Nepal MedicalCouncil.
His Majesty’s Government (HMG) of Nepalpublished a National Essential Drug List in 1986,which was revised in 1992 and again in 1997. Topromote appropriate use of anti-infective drugs, theNational Essential Drug List categorized the drugsaccording to the different levels of health care.
• Sub-health posts (the most peripheral health carefacilities, which are a part of each Village Devel-opment Committee): amoxicillin, cotrimoxazoleand tetracycline.
• Health posts (775 health care facilities): amoxi-cillin, procaine benzyl penicillin, chlorampheni-col, cotrimoxazole, and tetracycline.
• District level (75 public health offices and 50 dis-trict hospitals): amoxicillin, benzathin penicil-lin, benzyl penicillin, cloxacillin, procaine benzylpenicillin, chloramphenicol, ciprofloxacin,erythromycin, gentamicin, metronidazole, tet-racycline, rifampicin, streptomycin, ethambu-tol, sulfaacetamide, doxycycline andnitrofurantoin.
• National List: The national list includes all thedrugs from the district level plus Cefotaxime.
In addition to the antibiotics in the national list,other antibiotics available in the private sector re-tail shops need to be registered with the Depart-ment of Drug Administration (DDA), Nepal. Anew molecule, including an antibiotic, is not regis-tered in Nepal until it is included in the recognizedpharmacopoeia as per the convention adopted bythe Drug Advisory Committee.
Antibiotic use pattern in Nepal
Several research studies examined the prevalenceof antibiotic prescriptions:
• In 1994, in collaboration with the WHO, theDDA studied the prescribing habits of privatepractitioners; this study showed that antibioticswere prescribed in 49.85% of all cases.
• In 1997, in collaboration with PHCP/GTZ,another DDA study (the Rapid Assessment ofPharmaceutical Management and Utilization)showed that antibiotics were prescribed in 59%of all encounters in health facilities.
• In 1998, PHON conducted a study on Priorityand Misused Drugs in health facilities and pri-vate sector practitioners which showed thatantibacterials were prescribed in 50.7% of allencounters.
Research on dispensing practices showed recom-mendations of antibiotics for diarrhoeal diseases,fevers and viral infections.
Large amounts of antibiotics are used in animalsnot only as curative agents, but also as prophylac-tic agents and as growth promoters. The totalamount of antibiotics used in food animals and infeed in Nepal is not known. However, restrictingattention to the human use of antibiotics is notenough to curb bacterial resistance.
The participants of a regional drug informationworkshop at Nepalgunj and Pokhara on January9–14, 1999, advocated for the need for a separatepolicy for antibiotics. It was felt that a policy shouldbe developed for prescribing of antibiotics and rais-ing the general public’s awareness of bacterial re-sistance to antibiotics.
In response to this, the APUA-Nepal chapter,on the request of the Department of Drug Admin-istration and the Ministry of Health, prepared adraft of a National Antibiotic Policy developed bya committee of experts from the health, veterinary,agriculture and other fields. The initial draft of theNational Antibiotic Policy was presented in a work-shop on May 18–20, 2000, at Dhulikhel, Nepal.The participants presented their comments andsuggestions on the draft. These comments were usedto prepare a final draft which is pending at theMinistry of Health for approval.
Details of the proposed national antibiotic policy(2000)
The draft policy has nine sections: the preamble,definition, main policy, objectives, strategic guide-lines, national antibiotic control committee,research and development, technical cooperationand monitoring and supervision. The draft recom-mends:• Classifying antibiotics into three categories:
reserved, restricted, and semi-restricted.
• Dispensing antibiotics only with a prescriptionor within a nationally approved protocol.
• Establishing interagency cooperation amonggovernmental, non-governmental and privateinstitutions to promote the prudent use of anti-biotics by health care professionals and the gen-
131
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
eral public, with the assistance of His Majesty’sGovernment (HMG) of Nepal.
• Creating a National Antibiotic Control Com-mittee comprised of concerned experts fromhuman and animal health, agriculture, profes-sional organizations, and organizations involvedin consumer rights and awareness under theauspices of HMG.
• Establishing a national antibiotic surveillancesystem.
• Developing curricula for training and educationon the prudent use of antibiotics, and incorpo-rating them at all levels of prescribers’ and dis-pensers’ education.
• Promoting prudent use of antibiotics by imple-menting periodic training of health care work-ers who are eligible to prescribe drugs.
• Creating and regulating a National AntibioticTherapeutic Advisory Committee (NATAC)comprised of concerned experts from relevantsectors, under the auspices of HMG.
• Facilitating research on prescribing, dispensing,and use of antibiotics as well as antibiotic resist-ance.
• Encouraging the involvement of national andinternational agencies in technical training, edu-cation, and research related to the prudent useof antibiotics.
• Creating subcommittees of the National Anti-biotic Control Committee to be responsible foreffective implementation of the antibiotic policyas well as for monitoring and supervising its im-plementation.
• Requiring that antibiotics used for therapeuticpurpose in humans and animals not be used asgrowth promoters or prophylactic agents in ani-mal feed.
• Developing national antibiotic guidelines, whichwill assist individual health and veterinary insti-tutions to formulate local antibiotic guidelines.
• Developing facilities for antimicrobial resistancetesting and detection of antibiotic residue in live-stock products in health and veterinary institu-tions, with the help of HMG.
■ Viet Nam: Hospital case study andnational antibiotic policy
Report prepared by Dr. Hoang Thuy Long, Director ofNational Institute for Hygiene and Epidemiology,Vietnam. Chapter Head, APUA Vietnam.Contact: [email protected]
Policy of the Ministry of Health on the rational, safe,and effective use of drugs
In 1997–1998, the Vietnamese Ministry of Healthenacted a set of regulations to ensure the rational,safe, effective and economic use of drugs. Theseregulations:
• Established a Drug and Therapeutic Commit-tee (DTC) in each hospital whose function wasto oversee correct drug provision, management,and use.
• Strengthened the policy of rational, safe and eco-nomic use of drugs in the clinic and polyclinicinstitutions.
The Drug and Therapeutic Committee’s tasks are:
• To implement the national policy of using drugsin hospitals.
• To set up basic regulations concerning the sup-ply, management, and use of drugs in hospitalsand then submit the regulations to the hospi-tal’s director for approval.
• To set up the lists of drugs used in hospitals andsubmit the lists to the hospital’s director forapproval.
• To set up the drugs’ distribution procedure, sub-mit the procedure to the hospital’s director forapproval and help the director to implement theprocedure.
• To help the hospital’s director carry out the fol-lowing activities:
— Supervise rational prescription of drugs:— Set a rational prescription standard.— Check the contents of case histories that
refer to the drug use process.— Supervise adverse drug reactions in the hos-
pital.— Organize drug information.— Organize scientific research and training on
current knowledge of drugs.— Set up a cooperative relationship between the
pharmacist and the physicians and nurses fordrug use in patients.
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
132
Prior enactment, these Instructions were testedfor a year in four city or provincial hospitals inNorth Vietnam. In 1999, the Ministry of Healthorganized a conference to evaluate the impact ofthe Drug and Therapeutic Committees after twoyears of operation.
The results of this evaluation showed:
• Active participation by the Drug and Therapeu-tic Committee in the drug regulation in thehospitals.
• Enhanced supervision of adverse drug reactions.
• The Pharmacy Departments supplied a sufficientquantity of drugs of good quality.
• In some hospitals:
— The Pharmacy Department was able toadvise and provide drug information.
— A good working relationship was establishedbetween physicians, pharmacists and nursesto consult about drug use in patients.
• In many hospitals the Drug and TherapeuticCommittee had just been established and is notyet a fully functioning entity.
Lessons learned from this experience
• Instruction and management by the Ministry ofHealth of the activities of the Drug and Thera-peutic Committee
• Instructional activities of the Drug and Thera-peutic Committees and of the provincial healthservice
■ Utilization and management ofantibiotic use in Hospital Gynecology-Obstetric Hanoi (1995–1999)
Bui Suong, MD, Hospital Gynecology-Obstetric Hanoiand Nguyen Thi Vinh PhD, Medical College Hanoi,Viet Nam
This article is from the report of the workshop“Rational, safety use of antibiotics” held on Febru-ary 28–29, 2000 in Hanoi.
Bacterial infection remains one of several fac-tors leading to high mortality rates. Antimicrobialagents play a decisive role in reducing the mortal-ity and the incidence of bacterial infections. Todayantibiotics are widely and inappropriately used.
Anybody can buy antibiotics without a prescrip-tion. Hundreds of different brands of antibioticproducts are on the market and lack of informa-tion favours their misuse, such as unnecessary use,incorrect choice, incorrect dose, incorrect admin-istration, or poor drug quality. This misuse is thereason for increasing bacterial resistance, leadingto prolonged treatments in hospitals and increasedexpenses for drugs and services.
In March 1996, as one of the four pilot projects,the Ministry of Health established the Drug andTherapeutic Committee (DTC) at the HospitalGynecology-Obstetric Hanoi (HGOH). TheHGOH is a top-ranked hospital in Gynecology andObstetrics in Hanoi City. The HGOH treatsgynecological diseases and pathologic pregnancies,provides sterility treatment, family planning andobstetric services. The registered capacity of thehospital is 200 beds, but it is always working atovercapacity with both out- and in-patients. Thehospital is a reliable institution for women in Ha-noi and surroundings.
After being established, the HGOH Drug andTherapeutic Committee organized regular meetingsto encourage appropriate prescribing models anddrug choice for each patient. As time went on,models were reviewed and improved as needed. Theappropriate choice of antibiotic:
• Was specific for the pathogen germ.
• Was quickly and well absorbed at the infectionsite.
• Was appropriate to the treatment goal:gynecological, obstetric, post- obstetric, new-born, inpatient, or outpatient.
• Was appropriate to the treatment subject, i.e,pregnant, newborn.
• Minimized adverse drug reactions.
• Was of reasonable cost and acceptable to patients.
The HGOH’s Drug and Therapeutic Commit-tee has observed changes in antibiotic use since theCommittee was implemented.
1. The proportion of patients using antibioticsin the hospital
About 90% of patients used antibiotics. The re-maining 10% included pregnant patients planningto nurse their newborns and some doubtful casesof ex-uterine pregnancies; antibiotics were not usedin these cases.
133
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
TABLE 3. PROPORTION OF PATIENTS USING ANTIBIOTIC COMBINATION THERAPY
1995 1996 1997 1998 1999
Percent of patients using antibiotics 91.7% 91% 90.8% 90.5% 80.5%
Percent of patients using one antibiotic 50.8% 57.4% 71.4% 74.6% 68.6%
Percent of patients using two antibiotics 30.3% 25% 15.3% 12.3% 10.5%
Percent of patients using ≥ 3 antibiotics 10.6% 80.6% 4.1% 3.6% 1.4%
• Generally, only one antibiotic was used forprophylaxis after abortion or delivery with epi-siotomy.
• When necessary, antibiotic combination therapywas used as follows:
— β-lactam (ampicillin) + aminoglycoside (gen-tamicin) were the main combination used
— β-lactam (cephalosporine) + metronidazole— β-lactam + aminoglycoside + metronidazole— Quinolone + aminoglycoside (few/gyneco-
TABLE 1. OUT- AND IN-PATIENTS AT HOSPITAL GYNECOLOGY-OBSTETRIC HANOI
1995 1996 1997 1998 1999
1. Total number of patients examined 46,030 52,147 60,868 74,974 75,068
Total number of examinations 68,902 78,061 90,746 105,886 105,021
Total number of abortions 4,931 5,417 6,150 7,099 7,619
2. Total number of inpatients 10,487 12,007 12,342 13,061 14,600
Total number of deliveries 5,778 6,139 6,924 7,204 7,682
* Difficult 2,419 2,893 2,992 3,207 3,057
* Normal 3,359 3,246 3,932 3,997 4,625
Total number of operations 1,943 2,393 2,540 2,979 3,100
* Gynecological 593 784 976 1,193 1,142
* Obstetric 1,353 1,609 1,549 1,777 1,958
3. Average duration of therapy (days) 6.7 6.3 6.0 6.4 5.8
TABLE 2. ANTIBIOTIC USE BY PATIENTS
1995 1996 1997 1998 1999
Number of patients using antibiotics 9,616 10,926 11,207 11,820 11,753
Total number of patients 10,487 12,007 12,342 13,061 14,600
% 91.7% 91% 90.8% 90.5% 80.5%
logic)— Antibiotic + antifungi
• Antibiotic combination therapy was reduced in1999 because antibiotic prophylaxis was intro-duced in surgery in 1996 and was implementedhospital-wide in 1998.
• Antibiotic use was greatly reduced in 1999(19.5%) because antibiotic use was removed forall cases of normal delivery with tidy amnioticfluid, entire placenta, no episiotomy.
TABLE 4. PROPORTION OF EXPENDITURE FOR ANTIBIOTICS
1995 1996 1997 1998 1999
Expenditure for antibiotics (thousands Vndong) 322,127 646,867 905,159 1,010,433 1,043,799
% of total drugs expenditure 45.8% 45.6% 44.3% 43.8% 43.5%

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
134
• The expenditure for antibiotics is appropriatefor a top-ranked hospital for Gynecology andObstetric Surgery in Hanoi City.
• The proportion of antibiotic expenses was gradu-ally reduced from 1995 to 1999.
Today about twenty antibiotics are being used,with ten in common use. The Drug and Therapeu-tic Committee considers every sort of antibiotic.To be chosen, the antibiotic must be therapeuti-cally effective, have few adverse drug reactions, andbe manufactured by a reliable firm. Only one brandproduct of every antibiotic is used, making super-vision and management easier. While the kinds ofantibiotics may be increased or decreased, the quan-tity of expensive antibiotics was reduced from 1995to 1999.
2. Antimicrobial prophylaxis
From 1996 the hospital has used cefuroxime 0.75gx 03 (or 04) ports/case to test for prophylaxis insurgery (gynecological and obstetric) due to theshort duration. Hygienic measures, sterilization anddisinfection methods reduced the post-operativeinfection rate considerably (from 19.8% to 11.7%in the period studied). Because of its success, thisis now the standard order for antimicrobial prophy-laxis in the hospital. The post-operative infectionrate is 5% (fever 38.5–39 °C, inflammation at in-cision site) with no cases of serious post-operativeinfection.
Today, antimicrobial prophylaxis achieves goodresults, reducing pain for patients, shortening an-tibiotic duration, avoiding drug complications, re-ducing the effect on the mother’s milk (childbirthoperation). In addition, good economic results wereachieved, reducing medical service and reducingtotal expense for treatment in comparison to long-term therapy with antibiotics. The antimicrobialprophylaxis regimen could help to reduce the riseand spread of antibiotics resistant pathogens also.
3. Managing measures for rational, safe use ofantibiotics by the Drug and TherapeuticCommittee
In 1998, the HGOH’s Drug and Therapeutic Com-mittee became a full-fledged, independent entityin the hospital. The Committee has eight mem-bers, with the director as the chairman and the headof Pharmacy Department as the permanent secre-tary. Since its establishment, the Committee has
been advising the director on the rational, safe andeffective use of drugs, including antibiotics. All lead-ers of the hospital understand the necessity of therational, safe and effective use of drugs for therapy,as promoted by the Ministry of Health.
The Drug and Therapeutic Committee guide-lines for the Pharmacy Department and thePlanning Department are:
Drug providing
• The Pharmacy Department provides sufficientdrugs on time and at high quality. Drugs aregenerally obtained from state pharmaceuticalfirms.
• Only one of several products under the samegeneric name is used; this product must be ofgood quality and meet the therapeutic demandto facilitate the management and supervision ofantibiotic use in the hospital.
Prescribing
• On a yearly basis, experts are invited to give lec-tures on special topics in clinical pharmacy, suchas antibiotics, vitamins, drug interactions,adverse drug reactions. The audience is madeup of physicians, pharmacists and nurses fromthe whole hospital.
• One pharmacist and two physicians (special firstlevel) revise, advise and help the physicians toprescribe rational, safe, effective antibiotics.
• A clinic pharmacist helps physicians chooseappropriate drugs for treatment of patients.
• At the weekly general meeting of the hospital,the Pharmacy Department reports the casehistories of inappropriate drug use in order tocorrect future problems.
• Monthly, if a sudden change in the quantity ofdrug use is recognized, the Pharmacy Depart-ment reviews the case histories to find a reasonfor the change. It reports to the Drug and Thera-peutic Committee and makes suggestions forsolving the problem to gradually improve thequality of treatment.
Drug use
• The Pharmacy Department regularly makesguidelines and supervises the nurses and mid-wives in using drugs according to prescription.The Pharmacy Department cooperates with the
135
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
clinical departments to watch the effectivenessof drug use and report any decrease in effective-ness to the Drug and Therapeutic Committee.The Pharmacy Department monitors anyadverse drug reactions in time to recover. In fouryears, fifty cases of adverse drug reaction werefound, in which 38 cases were caused by antibi-otics. All cases were treated in time with no com-plication.
• The physicians prescribe according to the guide-lines and the list of drugs, which are rewrittenby the Drug and Therapeutic Committee eachyear, so that the use of antibiotics in the hospi-tal is becoming more rational, safe and effec-tive. The post-operative infection rate is beingreduced. Therefore, although the number ofinpatients is increasing, the average duration oftreatment is decreasing (from 6.7 days in 1995to 5.8 days in 1999).
Conclusion
Enacting the policies of the Ministry of Health withthe determination of the director of the board andunder the leadership of the Drug and TherapeuticCommittee, all physicians adhere strictly to theprescribing regulations and therapeutic guideline.Antimicrobial prophylaxis and the rational, safe useof antibiotics showed a high degree of effectiveness.
To improve results, we will promote the effec-tiveness of the Drug and Therapeutic Committeeactivity by:
• Strengthening science research activities in thehospital.
• Encouraging and providing conditions forpersonnel to improve their professional knowl-edge.
• Re-educating physicians on prescribing regula-tions, principles of drug use in general and ofantibiotic use in particular.
• Regularly providing to physicians, pharmacistsand nurses sufficient and up-to-date informa-tion about drugs in the drug list and theiradministration.
• Reinforcing surveillance on therapeutical effec-tiveness of drugs being used in the hospital, find-ing out about drugs with bad activity and/oradverse drug reactions in order to eliminate thatdrug from the drug list.
• Strengthening supervision on rational, safe use
of drugs in the whole hospital (including in- andout-patients) from the examination phasethrough prescribing and realization of medicalorders to the final result. There could be pun-ishment for infringed cases.
■ Greece: Hospital case study of anantibiotic policy
Report prepared by Helen Giamarellou, MD, PhD,Professor of Internal Medicine, Athens University Schoolof Medicine, Sismanoglio General Hospital, Athens,Greece; President, APUA Greece; Anastasia Antoniadou,MD, Nearchos Galanakis, MD, George Petrikkos, MD,Erasmia Sarmi, Pharmacist. Contact Dr. HelenGiamarellou at: [email protected]
This is a report on the encouraging results of ourimplementation of an antibiotic resistance policyin Laiko General Hospital during the period 1992–1998.
In Greece, as in other settings, high antibioticresistance rates run in parallel with huge antibioticconsumption in hospitals and in the community.We implemented a antibiotic restriction policy ina 500 bed University teaching hospital. In this hos-pital, antibiotic consumption before 1990 rangedbetween 62–78% with the highest rates in the Gen-eral Surgery and Urology Departments (75–100%).The main overuse involved long-term surgicalprophylaxis, while one-third to one-half of antibi-otic consumption involved the unjustified use ofthird generation cephalosporins, carbapenems,newer quinolones and vancomycin. Resistance ratesamong Gram-negative isolates were already high(Table 1) and the threat of losing all new activecompounds because of their unjustified overuse wasa reality.
Since 1991, an antibiotic restriction programmeproposed by Professor Giamarellou and her teamwas implemented by the Infection Control Com-mittee of the Laiko General Hospital. Accordingto the programme, all new antimicrobials (third andforth generation cephalosporins, aztreonam,imipenem and later meropenem, vancomycin andlater teicoplanin and all newer quinolones) wereordered to the hospital pharmacy only after physi-cians had completed a restricted antibiotic form,which had to be inspected and signed by the hos-pital infectious diseases clinicians (Laiko Hospitalhad 3 of them) or by physicians with a proven in-terest in infectious diseases. The programme wasalso supplemented by enforcement of the rules of
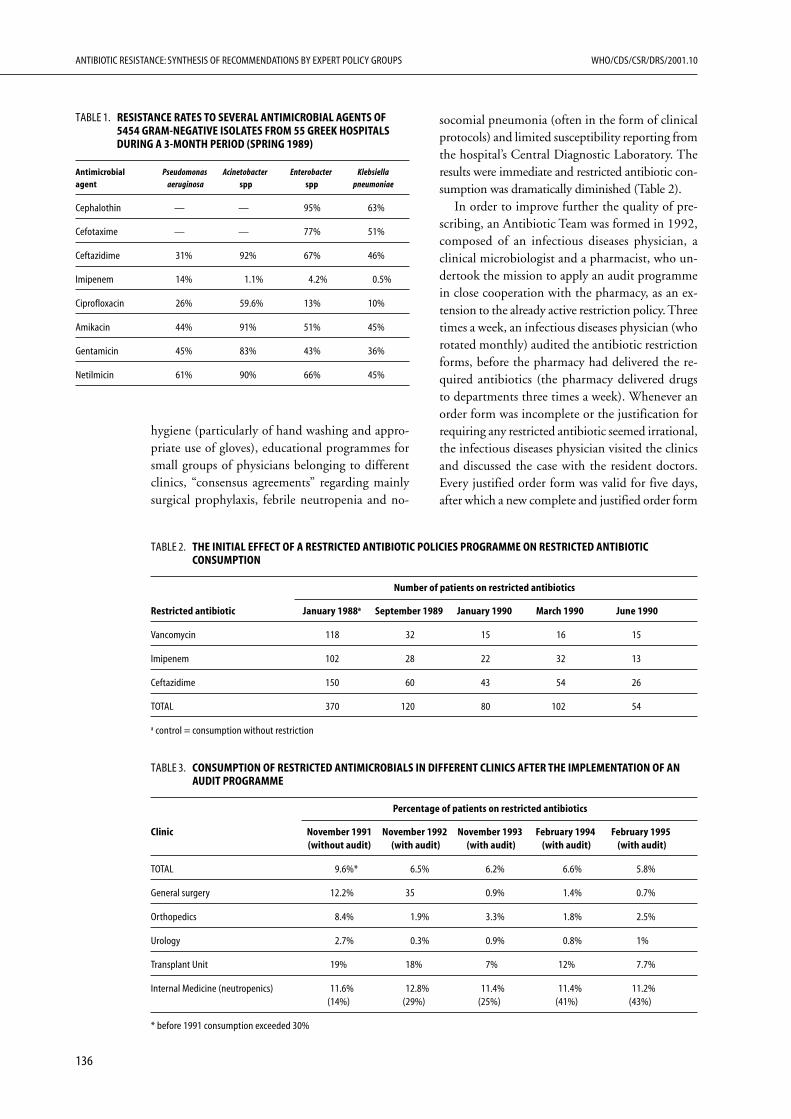
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
136
hygiene (particularly of hand washing and appro-priate use of gloves), educational programmes forsmall groups of physicians belonging to differentclinics, “consensus agreements” regarding mainlysurgical prophylaxis, febrile neutropenia and no-
socomial pneumonia (often in the form of clinicalprotocols) and limited susceptibility reporting fromthe hospital’s Central Diagnostic Laboratory. Theresults were immediate and restricted antibiotic con-sumption was dramatically diminished (Table 2).
In order to improve further the quality of pre-scribing, an Antibiotic Team was formed in 1992,composed of an infectious diseases physician, aclinical microbiologist and a pharmacist, who un-dertook the mission to apply an audit programmein close cooperation with the pharmacy, as an ex-tension to the already active restriction policy. Threetimes a week, an infectious diseases physician (whorotated monthly) audited the antibiotic restrictionforms, before the pharmacy had delivered the re-quired antibiotics (the pharmacy delivered drugsto departments three times a week). Whenever anorder form was incomplete or the justification forrequiring any restricted antibiotic seemed irrational,the infectious diseases physician visited the clinicsand discussed the case with the resident doctors.Every justified order form was valid for five days,after which a new complete and justified order form
TABLE 1. RESISTANCE RATES TO SEVERAL ANTIMICROBIAL AGENTS OF5454 GRAM-NEGATIVE ISOLATES FROM 55 GREEK HOSPITALSDURING A 3-MONTH PERIOD (SPRING 1989)
Antimicrobial Pseudomonas Acinetobacter Enterobacter Klebsiellaagent aeruginosa spp spp pneumoniae
Cephalothin — — 95% 63%
Cefotaxime — — 77% 51%
Ceftazidime 31% 92% 67% 46%
Imipenem 14% 1.1% 4.2% 0.5%
Ciprofloxacin 26% 59.6% 13% 10%
Amikacin 44% 91% 51% 45%
Gentamicin 45% 83% 43% 36%
Netilmicin 61% 90% 66% 45%
TABLE 2. THE INITIAL EFFECT OF A RESTRICTED ANTIBIOTIC POLICIES PROGRAMME ON RESTRICTED ANTIBIOTICCONSUMPTION
Number of patients on restricted antibiotics
Restricted antibiotic January 1988a September 1989 January 1990 March 1990 June 1990
Vancomycin 118 32 15 16 15
Imipenem 102 28 22 32 13
Ceftazidime 150 60 43 54 26
TOTAL 370 120 80 102 54
a control = consumption without restriction
TABLE 3. CONSUMPTION OF RESTRICTED ANTIMICROBIALS IN DIFFERENT CLINICS AFTER THE IMPLEMENTATION OF ANAUDIT PROGRAMME
Percentage of patients on restricted antibiotics
Clinic November 1991 November 1992 November 1993 February 1994 February 1995(without audit) (with audit) (with audit) (with audit) (with audit)
TOTAL 9.6%* 6.5% 6.2% 6.6% 5.8%
General surgery 12.2% 35 0.9% 1.4% 0.7%
Orthopedics 8.4% 1.9% 3.3% 1.8% 2.5%
Urology 2.7% 0.3% 0.9% 0.8% 1%
Transplant Unit 19% 18% 7% 12% 7.7%
Internal Medicine (neutropenics) 11.6% 12.8% 11.4% 11.4% 11.2%(14%) (29%) (25%) (41%) (43%)
* before 1991 consumption exceeded 30%
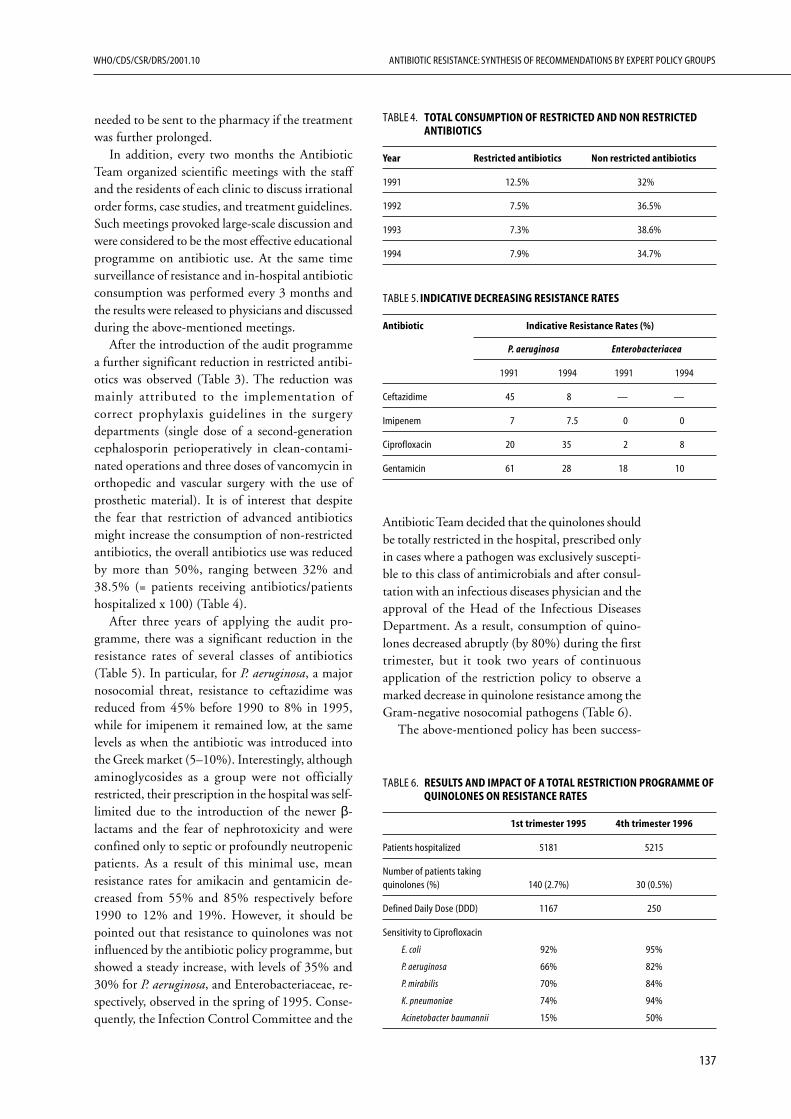
137
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
needed to be sent to the pharmacy if the treatmentwas further prolonged.
In addition, every two months the AntibioticTeam organized scientific meetings with the staffand the residents of each clinic to discuss irrationalorder forms, case studies, and treatment guidelines.Such meetings provoked large-scale discussion andwere considered to be the most effective educationalprogramme on antibiotic use. At the same timesurveillance of resistance and in-hospital antibioticconsumption was performed every 3 months andthe results were released to physicians and discussedduring the above-mentioned meetings.
After the introduction of the audit programmea further significant reduction in restricted antibi-otics was observed (Table 3). The reduction wasmainly attributed to the implementation ofcorrect prophylaxis guidelines in the surgerydepartments (single dose of a second-generationcephalosporin perioperatively in clean-contami-nated operations and three doses of vancomycin inorthopedic and vascular surgery with the use ofprosthetic material). It is of interest that despitethe fear that restriction of advanced antibioticsmight increase the consumption of non-restrictedantibiotics, the overall antibiotics use was reducedby more than 50%, ranging between 32% and38.5% (= patients receiving antibiotics/patientshospitalized x 100) (Table 4).
After three years of applying the audit pro-gramme, there was a significant reduction in theresistance rates of several classes of antibiotics(Table 5). In particular, for P. aeruginosa, a majornosocomial threat, resistance to ceftazidime wasreduced from 45% before 1990 to 8% in 1995,while for imipenem it remained low, at the samelevels as when the antibiotic was introduced intothe Greek market (5–10%). Interestingly, althoughaminoglycosides as a group were not officiallyrestricted, their prescription in the hospital was self-limited due to the introduction of the newer β-lactams and the fear of nephrotoxicity and wereconfined only to septic or profoundly neutropenicpatients. As a result of this minimal use, meanresistance rates for amikacin and gentamicin de-creased from 55% and 85% respectively before1990 to 12% and 19%. However, it should bepointed out that resistance to quinolones was notinfluenced by the antibiotic policy programme, butshowed a steady increase, with levels of 35% and30% for P. aeruginosa, and Enterobacteriaceae, re-spectively, observed in the spring of 1995. Conse-quently, the Infection Control Committee and the
TABLE 4. TOTAL CONSUMPTION OF RESTRICTED AND NON RESTRICTEDANTIBIOTICS
Year Restricted antibiotics Non restricted antibiotics
1991 12.5% 32%
1992 7.5% 36.5%
1993 7.3% 38.6%
1994 7.9% 34.7%
TABLE 5. INDICATIVE DECREASING RESISTANCE RATES
Antibiotic Indicative Resistance Rates (%)
P. aeruginosa Enterobacteriacea
1991 1994 1991 1994
Ceftazidime 45 8 — —
Imipenem 7 7.5 0 0
Ciprofloxacin 20 35 2 8
Gentamicin 61 28 18 10
Antibiotic Team decided that the quinolones shouldbe totally restricted in the hospital, prescribed onlyin cases where a pathogen was exclusively suscepti-ble to this class of antimicrobials and after consul-tation with an infectious diseases physician and theapproval of the Head of the Infectious DiseasesDepartment. As a result, consumption of quino-lones decreased abruptly (by 80%) during the firsttrimester, but it took two years of continuousapplication of the restriction policy to observe amarked decrease in quinolone resistance among theGram-negative nosocomial pathogens (Table 6).
The above-mentioned policy has been success-
TABLE 6. RESULTS AND IMPACT OF A TOTAL RESTRICTION PROGRAMME OFQUINOLONES ON RESISTANCE RATES
1st trimester 1995 4th trimester 1996
Patients hospitalized 5181 5215
Number of patients takingquinolones (%) 140 (2.7%) 30 (0.5%)
Defined Daily Dose (DDD) 1167 250
Sensitivity to Ciprofloxacin
E. coli 92% 95%
P. aeruginosa 66% 82%
P. mirabilis 70% 84%
K. pneumoniae 74% 94%
Acinetobacter baumannii 15% 50%

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
138
ful in decreasing resistance rates in the closed sys-tem within a university hospital, because:
• Although restriction and audit were the mainparameters of the policy, as an entity it was amultidisciplinary programme including surveil-lance, education, treatment guidelines, limitedreporting sensitivity testing, consultation, andimplementation of hygiene measures;
• The audit was effective because infectious dis-eases physicians had the cooperation of themicrobiology laboratory and the pharmacy;
• The team that tried to apply it consisted mainlyof infectious diseases physicians who workedwith enthusiasm and belief, despite initial diffi-culties with their fellow doctors’ attitude;
• Respected opinion leaders in the field of infec-tious diseases guided the programme, a fact thatmade the work of the Antibiotic Team easier.
The lessons we learned from this experience,especially the fact that controlling and limitingantibiotic use can reverse increased microbial re-sistance, can be applied to hospitals and the com-munity. We are trying now to implement such apolicy in hospitals on a national scale. Of course aprerequisite is the presence of an infectious diseasesphysician in every hospital who will be responsiblefor the implementation of the policy.
■ Russia: Hospital Case Studies ofAntibiotic Policies
Report prepared by Leonid S. Stratchounski, MD, PhD,Director, Institute of Antimicrobial Chemotherapy (IAC),Russian Federation, Smolensk; President, APUA Russia;Roman S. Kozlov, MD, MSc, PhD, Deputy Director ofScience, Institute of Antimicrobial Chemotherapy (IAC),Russian Federation, Smolensk; Coordinator, APUA Russia;Alla S. Andreeva, MD, Clinical Pharmacologist, SmolenskRegional Hospital, Russian Federation, Smolensk; andOleg L. Rozenson, MD, PhD, Assistant Professor,Department of Clinical Pharmacology & AntimicrobialChemotherapy, Smolensk State Medical Academy,Russian Federation, Smolensk.Contact Dr. Roman Kozlov:[email protected]
Antibiotic Policy: Introduction of an antibiotic policyinto a large regional hospital
This is a report of the implementation of an anti-biotic policy in the Smolensk Regional Hospital(SRH): 1,320 beds, 30 wards.
Background
The introduction of an antibiotic policy into hos-pitals has previously been shown to be an effectivetool in the curbing of antimicrobial resistance. Suchpolicies have not been used extensively in Russiapreviously for a variety of reasons, including:
• Isolation of practicing doctors from moderninternational trends in antimicrobial chemo-therapy.
• The results of microbiological investigations(including susceptibility testing) have little in-fluence on clinical practice.
• Presence of a ‘gap’ between microbiologists andclinicians.
Description of the antibiotic policy
• Clinicians were taught about rational antimicro-bial chemotherapy on a regular basis via semi-nars, case discussions, distribution of literature,participation in symposia and postgraduatecourses.
• Clinical pharmacologists were appointed to theSRH and provided regular consultation withphysicians on the choice of antimicrobials.
• A Formulary Committee was established withthe introduction of a formulary and its regularupdate.
• Microbiological services were improved bymeans of:
— Continuous education of personnel in themicrobiological laboratory (including theprinciples of selective reporting of suscepti-bility testing results);
— After-hours coverage;— Implementation of internationally recog-
nized guidelines (National Committee forClinical and Laboratory Standards(NCCLS)) for susceptibility testing withinthe microbiological laboratory;
— Establishment of resistance monitoring pro-grammes and data management (usingWHONET and other software).
The main areas addressed in the antibiotic policy
• The analysis of antimicrobials use within theSRH and by different wards (using the recom-mended WHO ATC/DDD methodology).
139
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
• Education of both microbiologists and clinicianson clinical pharmacology of antimicrobials andcurrent issues on antimicrobial resistance.
• Development and implementation of antimicro-bial drug formularies.
• Policy to restrict the prescription of III-IVgeneration of cephalosporins, carbapenems,amikacin, vancomycin, and so on.
• Improvements in the microbiological serviceprovided.
Level of policy enacted
This was a regional level policy that could be usedas an example for other hospitals wishing to imple-ment a similar strategy.
Interim results of the antibiotic policy
In 1999, a total of 33 antimicrobials were used inthe SRH and 4 antibiotics were not given in com-parison with 1997.
Over the same time period, hospital expenseson antimicrobials decreased by 40%.
Interim analysis of intensive care unit (ICU) datafrom 1997 was compared with data from 1997 (be-fore and after implementing the above policy).
In general, the consumption of antimicrobialsdecreased 1.3-fold in 1999 compared with 1997(from 214.43 DDDs to 162.95 per 100 beds/days,respectively). This was mainly due to a 1.2-folddecrease in the use of penicillins (from 118.6 to98.23 DDDs per 100 beds/days in 1997 and 1999,respectively), a 1.8 times decrease in the use of allcephalosporins (from 20.4 to 11.4 DDDs per 100beds/days in 1997 and 1999, respectively) and a1.4-fold decrease in the use of aminoglycosides,especially gentamicin (from 48.9 to 34.0 DDDsper 100 beds/days). There was also a decrease inthe consumption of imipenem and ciprofloxacin.
There was a decrease in resistance amongst no-socomial gram-negative bacteria: the resistance ofP. aeruginosa to gentamicin decreased from 75.0%to 31.2% in 1997 and 1999, respectively and toamikacin from 7.0% to 1.8%.
At the same time, no changes were noted in re-sistance profiles of E. coli, Klebsiella spp., Entero-bacter spp. and Acinetobacter spp.
In conclusion, the interim analysis showed thatthe establishment of an antibiotic policy in the SRH(by means of education of health care providers,antimicrobial resistance surveillance, and a formu-
lary system) had financial advantages (a total 2.2-fold decrease in hospital spending onantimicrobials) and led to improvement in the re-sistance profiles of the most prevalent pathogen inthe ICU (P. aeruginosa). An analysis of the influ-ence of the antibiotic policy on the developmentof antimicrobial resistance in other hospital wardsis currently under investigation.
Lessons learned from the above policy applicable toother countries
Education of health care providers, implementa-tion of antimicrobial formulary and establishmentof close connections between microbiologists andclinicians have proved to be the most crucialissues. Such approaches could be successfully usedin both industrialized and developing countries.
Antibiotic Prophylaxis Policy: Optimization ofantibiotic prophylaxis in surgical wards ofSmolensk Regional Hospital (SRH)
Background
Antibiotic prophylaxis in surgery is an area wherethe consumption of antimicrobials remains veryhigh. The analysis of indications, regimens andduration of antibiotic prophylaxis in the hospitalindicated that optimization in this area is required,due to:
• Non-evidence-based administration of antibioticprophylaxis.
• Irrational selection of antimicrobials for prophy-laxis.
• Long duration of antibiotic prophylaxis.
All the above have led to the establishment ofthe main objective of the study: to evaluate the prac-tice of antibiotic prophylaxis, conduct economicanalysis of antibiotic prophylaxis in abdominal sur-gery in the SRH, and to evaluate the impact ofeducational and administrative activities on anti-biotic prophylaxis.
Description of the antibiotic prophylaxis policy
• Targeted teaching of surgeons about the mod-ern concept of antibiotic prophylaxis. Specialattention was given to heads of departments.
• In collaboration with SRH authorities, the de-velopment and distribution of official recom-mendations on antibiotic prophylaxis within thesurgical wards of SRH.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
140
The main areas addressed in the antibioticprophylaxis policy
• The education of surgeons on rational antibi-otic prophylaxis and the principles of evidence-based medicine.
• The development and implementation of prac-tical recommendations on antibiotic prophylaxiswithin the surgical wards of the SRH.
• Involvement of the authorities of the SRH inthe implementation of antibiotic prophylaxis.
Level of policy enacted
This was a regional level policy, which could beused as an example for other hospitals wishing toimplement a similar strategy.
Results of the antibiotic prophylaxis policy impact
Analysis was based on patient data, gathered retro-spectively in 1993 and 1998. Three hundred andtwenty-seven patients who underwent open chole-cystectomy (OCE), appendectomy (AE) andhernia repair (HR) were included in the analysis.Antibiotic prophylaxis frequency and quality(selection of antimicrobials, dosage regimens, routeof administration, post-operative duration) wereassessed. In 1993, none of the patients receivedpreoperative antibiotic prophylaxis, however, manypatients received antimicrobial treatment after theiroperation for 5 to 8 days. In 1998, the followingpreoperative antibiotic prophylaxis frequency wasregistered: OCE–78%, AE–0%, HR–46%. In1993, antibacterial administration without evidenceof postoperative infection was registered for OCEin 82% cases compared to 31% cases in 1998.
Lessons learned from the antibiotic prophylaxis policyapplicable to other countries
• Educational and administrative activities have apositive impact on antibiotic prophylaxis prac-tice in surgery.
• The monitoring of antibiotic prophylaxis prac-tice and feedback to surgeons needs to beimplemented in hospitals for the optimizationof antibiotic prophylaxis.
In our opinion, this policy can also be used indeveloping countries.
■ Bulgaria: Hospital Case Studies andNational Antibiotic Policy
Emma E. Keuleyan, PhD, Assistant Professor,Department of Microbiology, Head AntimicrobialResistance Laboratory, Medical University, Sofia,Bulgaria; Coordinator APUA Bulgaria Chapter.Contact: [email protected]
In Bulgaria, as in other countries, the emergenceand dissemination of antimicrobial resistance hasbeen recognized as a major obstacle in antimicro-bial chemotherapy, as well as an event with widebiologic significance. Several years after R - plasmidshave been discovered by Okhiai and Akiba inJapan, the scientists started investigations on thegenetic mechanisms of resistance and its epidemi-ology.
Some publications from the 1960s are citedbelow:• Tyagunenko Y and Z Kyolean. 1967. Transmis-
sion of Multiple Antimicrobial Resistance inStrains of Fam. Enterobacteriaceae. EpidemiolMicrobiol Infect Dis (Sofia). 4, 1, 26–31
• Tyagunenko Y and Z Kiolean. 1968. Studies onsome characteristics in the transmission andmanifestations of an episome with 5 R–mark-ers. Proceedings of the Postgraduate MedicalInstitute ISUL. 15, 1, 35–41 (English).
With time, new aspects, new methods, and newapproaches got more people interested in the anti-biotic problem. The Department of Microbiologyat Medical University,Sofia and the NationalCentre of Infectious and Parasitic Diseases haveplayed the leading role in this evolution of knowl-edge, research, and activities.
As shown by experience, antibiotic resistancecontinues to increase and spread globally. Bulgariahas had some success in decreasing the antibioticresistance problem, illustrated by the followingexamples.
A. Institutional level
Some hospitals, primarily at universities, have ini-tiated programmes for resistance surveillance andcontrol of infections, and established therapeuticcommittees to optimize antibiotic use.
1. Alexander’s Hospital—Medical University, Sofia(1, 2)
While third generation cephalosporins, tetracyclinesand aminopenicillins were widely used in 1993–
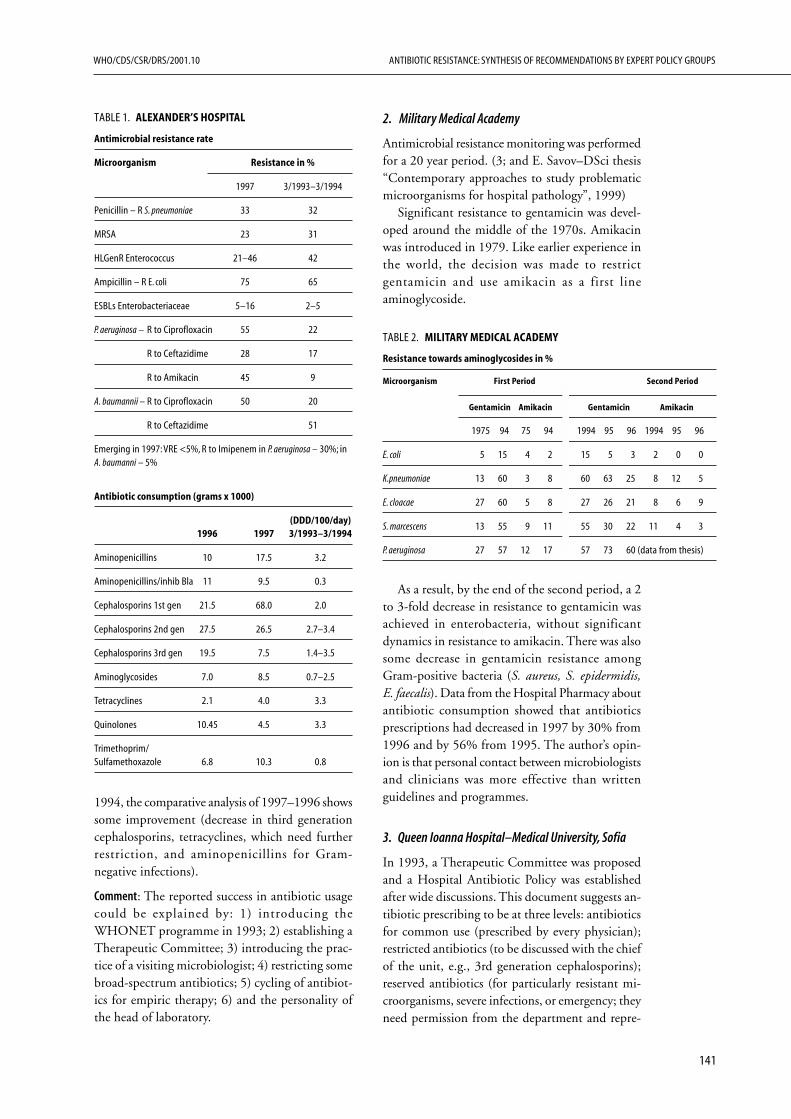
141
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
1994, the comparative analysis of 1997–1996 showssome improvement (decrease in third generationcephalosporins, tetracyclines, which need furtherrestriction, and aminopenicillins for Gram-negative infections).
Comment: The reported success in antibiotic usagecould be explained by: 1) introducing theWHONET programme in 1993; 2) establishing aTherapeutic Committee; 3) introducing the prac-tice of a visiting microbiologist; 4) restricting somebroad-spectrum antibiotics; 5) cycling of antibiot-ics for empiric therapy; 6) and the personality ofthe head of laboratory.
TABLE 1. ALEXANDER’S HOSPITAL
Antimicrobial resistance rate
Microorganism Resistance in %
1997 3/1993–3/1994
Penicillin – R S. pneumoniae 33 32
MRSA 23 31
HLGenR Enterococcus 21–46 42
Ampicillin – R E. coli 75 65
ESBLs Enterobacteriaceae 5–16 2–5
P. aeruginosa – R to Ciprofloxacin 55 22
R to Ceftazidime 28 17
R to Amikacin 45 9
A. baumannii – R to Ciprofloxacin 50 20
R to Ceftazidime 51
Emerging in 1997: VRE <5%, R to Imipenem in P. aeruginosa – 30%; inA. baumanni – 5%
Antibiotic consumption (grams x 1000)
(DDD/100/day)1996 1997 3/1993–3/1994
Aminopenicillins 10 17.5 3.2
Aminopenicillins/inhib Bla 11 9.5 0.3
Cephalosporins 1st gen 21.5 68.0 2.0
Cephalosporins 2nd gen 27.5 26.5 2.7–3.4
Cephalosporins 3rd gen 19.5 7.5 1.4–3.5
Aminoglycosides 7.0 8.5 0.7–2.5
Tetracyclines 2.1 4.0 3.3
Quinolones 10.45 4.5 3.3
Trimethoprim/Sulfamethoxazole 6.8 10.3 0.8
2. Military Medical Academy
Antimicrobial resistance monitoring was performedfor a 20 year period. (3; and E. Savov–DSci thesis“Contemporary approaches to study problematicmicroorganisms for hospital pathology”, 1999)
Significant resistance to gentamicin was devel-oped around the middle of the 1970s. Amikacinwas introduced in 1979. Like earlier experience inthe world, the decision was made to restrictgentamicin and use amikacin as a first lineaminoglycoside.
As a result, by the end of the second period, a 2to 3-fold decrease in resistance to gentamicin wasachieved in enterobacteria, without significantdynamics in resistance to amikacin. There was alsosome decrease in gentamicin resistance amongGram-positive bacteria (S. aureus, S. epidermidis,E. faecalis). Data from the Hospital Pharmacy aboutantibiotic consumption showed that antibioticsprescriptions had decreased in 1997 by 30% from1996 and by 56% from 1995. The author’s opin-ion is that personal contact between microbiologistsand clinicians was more effective than writtenguidelines and programmes.
3. Queen Ioanna Hospital–Medical University, Sofia
In 1993, a Therapeutic Committee was proposedand a Hospital Antibiotic Policy was establishedafter wide discussions. This document suggests an-tibiotic prescribing to be at three levels: antibioticsfor common use (prescribed by every physician);restricted antibiotics (to be discussed with the chiefof the unit, e.g., 3rd generation cephalosporins);reserved antibiotics (for particularly resistant mi-croorganisms, severe infections, or emergency; theyneed permission from the department and repre-
TABLE 2. MILITARY MEDICAL ACADEMY
Resistance towards aminoglycosides in %
Microorganism First Period Second Period
Gentamicin Amikacin Gentamicin Amikacin
1975 94 75 94 1994 95 96 1994 95 96
E. coli 5 15 4 2 15 5 3 2 0 0
K.pneumoniae 13 60 3 8 60 63 25 8 12 5
E. cloacae 27 60 5 8 27 26 21 8 6 9
S. marcescens 13 55 9 11 55 30 22 11 4 3
P. aeruginosa 27 57 12 17 57 73 60 (data from thesis)
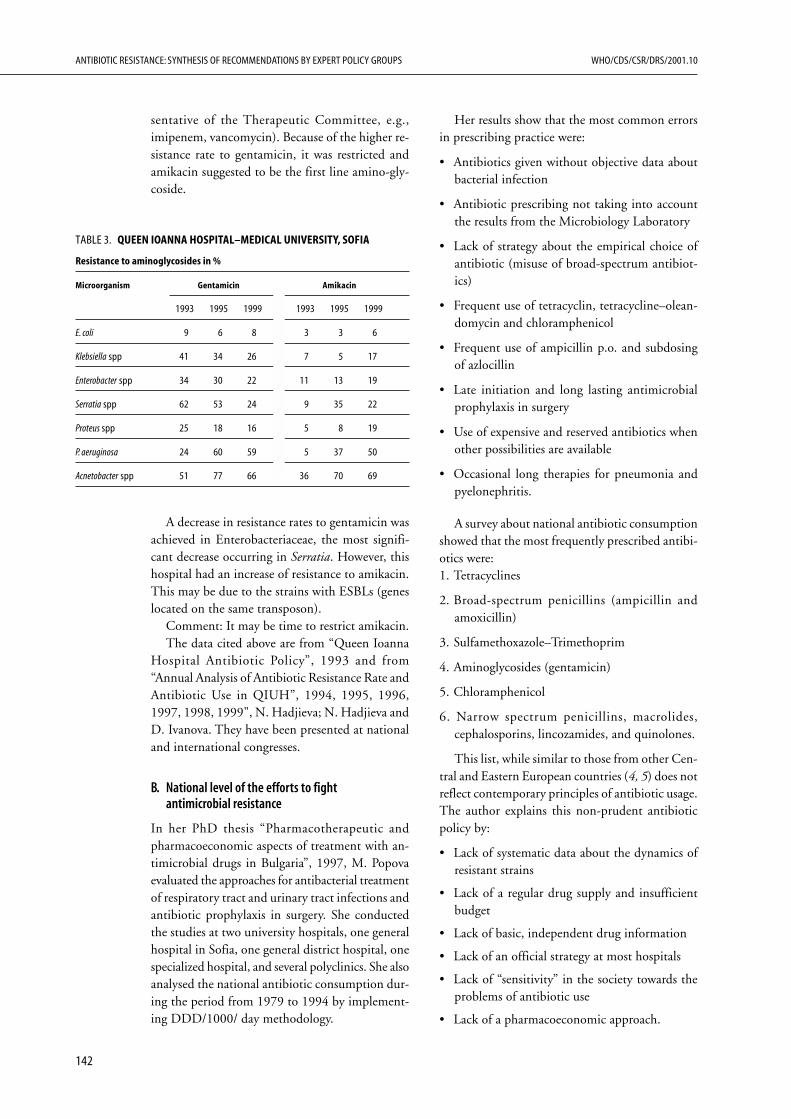
ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
142
sentative of the Therapeutic Committee, e.g.,imipenem, vancomycin). Because of the higher re-sistance rate to gentamicin, it was restricted andamikacin suggested to be the first line amino-gly-coside.
Her results show that the most common errorsin prescribing practice were:
• Antibiotics given without objective data aboutbacterial infection
• Antibiotic prescribing not taking into accountthe results from the Microbiology Laboratory
• Lack of strategy about the empirical choice ofantibiotic (misuse of broad-spectrum antibiot-ics)
• Frequent use of tetracyclin, tetracycline–olean-domycin and chloramphenicol
• Frequent use of ampicillin p.o. and subdosingof azlocillin
• Late initiation and long lasting antimicrobialprophylaxis in surgery
• Use of expensive and reserved antibiotics whenother possibilities are available
• Occasional long therapies for pneumonia andpyelonephritis.
A survey about national antibiotic consumptionshowed that the most frequently prescribed antibi-otics were:1. Tetracyclines
2. Broad-spectrum penicillins (ampicillin andamoxicillin)
3. Sulfamethoxazole–Trimethoprim
4. Aminoglycosides (gentamicin)
5. Chloramphenicol
6. Narrow spectrum penicillins, macrolides,cephalosporins, lincozamides, and quinolones.
This list, while similar to those from other Cen-tral and Eastern European countries (4, 5) does notreflect contemporary principles of antibiotic usage.The author explains this non-prudent antibioticpolicy by:
• Lack of systematic data about the dynamics ofresistant strains
• Lack of a regular drug supply and insufficientbudget
• Lack of basic, independent drug information
• Lack of an official strategy at most hospitals
• Lack of “sensitivity” in the society towards theproblems of antibiotic use
• Lack of a pharmacoeconomic approach.
TABLE 3. QUEEN IOANNA HOSPITAL–MEDICAL UNIVERSITY, SOFIA
Resistance to aminoglycosides in %
Microorganism Gentamicin Amikacin
1993 1995 1999 1993 1995 1999
E. coli 9 6 8 3 3 6
Klebsiella spp 41 34 26 7 5 17
Enterobacter spp 34 30 22 11 13 19
Serratia spp 62 53 24 9 35 22
Proteus spp 25 18 16 5 8 19
P. aeruginosa 24 60 59 5 37 50
Acnetobacter spp 51 77 66 36 70 69
A decrease in resistance rates to gentamicin wasachieved in Enterobacteriaceae, the most signifi-cant decrease occurring in Serratia. However, thishospital had an increase of resistance to amikacin.This may be due to the strains with ESBLs (geneslocated on the same transposon).
Comment: It may be time to restrict amikacin.The data cited above are from “Queen Ioanna
Hospital Antibiotic Policy”, 1993 and from“Annual Analysis of Antibiotic Resistance Rate andAntibiotic Use in QIUH”, 1994, 1995, 1996,1997, 1998, 1999", N. Hadjieva; N. Hadjieva andD. Ivanova. They have been presented at nationaland international congresses.
B. National level of the efforts to fightantimicrobial resistance
In her PhD thesis “Pharmacotherapeutic andpharmacoeconomic aspects of treatment with an-timicrobial drugs in Bulgaria”, 1997, M. Popovaevaluated the approaches for antibacterial treatmentof respiratory tract and urinary tract infections andantibiotic prophylaxis in surgery. She conductedthe studies at two university hospitals, one generalhospital in Sofia, one general district hospital, onespecialized hospital, and several polyclinics. She alsoanalysed the national antibiotic consumption dur-ing the period from 1979 to 1994 by implement-ing DDD/1000/ day methodology.
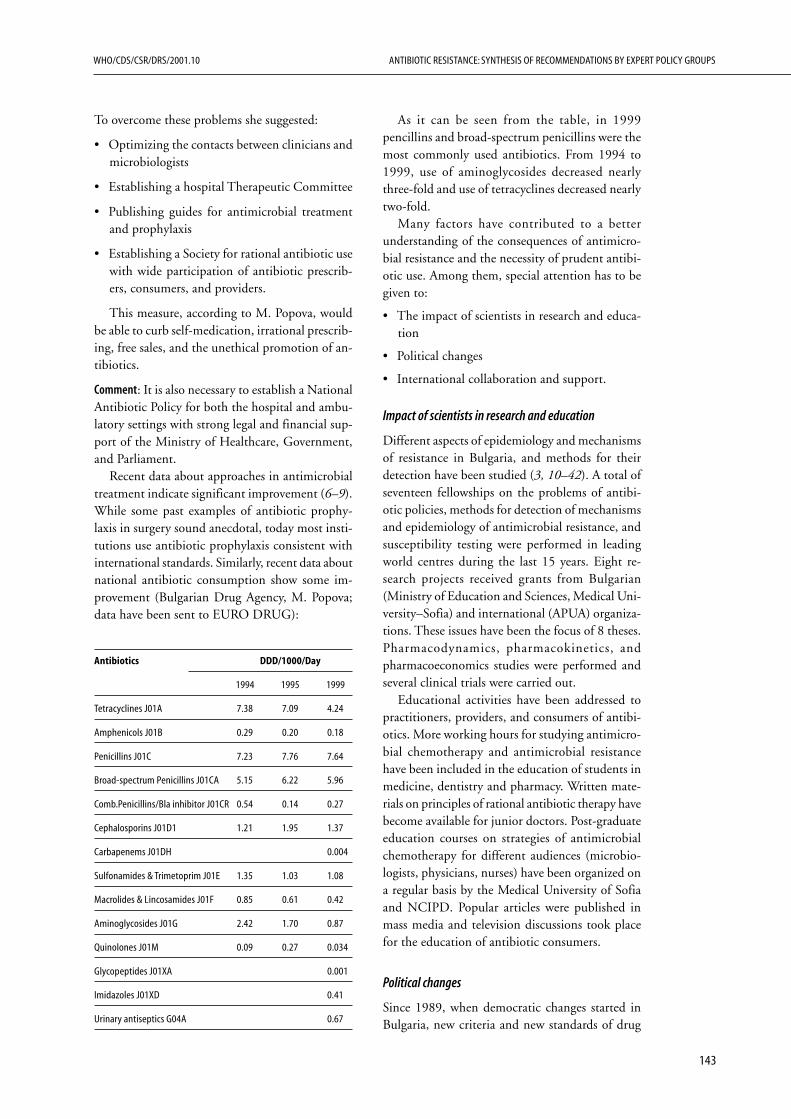
143
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
To overcome these problems she suggested:
• Optimizing the contacts between clinicians andmicrobiologists
• Establishing a hospital Therapeutic Committee
• Publishing guides for antimicrobial treatmentand prophylaxis
• Establishing a Society for rational antibiotic usewith wide participation of antibiotic prescrib-ers, consumers, and providers.
This measure, according to M. Popova, wouldbe able to curb self-medication, irrational prescrib-ing, free sales, and the unethical promotion of an-tibiotics.
Comment: It is also necessary to establish a NationalAntibiotic Policy for both the hospital and ambu-latory settings with strong legal and financial sup-port of the Ministry of Healthcare, Government,and Parliament.
Recent data about approaches in antimicrobialtreatment indicate significant improvement (6–9).While some past examples of antibiotic prophy-laxis in surgery sound anecdotal, today most insti-tutions use antibiotic prophylaxis consistent withinternational standards. Similarly, recent data aboutnational antibiotic consumption show some im-provement (Bulgarian Drug Agency, M. Popova;data have been sent to EURO DRUG):
Antibiotics DDD/1000/Day
1994 1995 1999
Tetracyclines J01A 7.38 7.09 4.24
Amphenicols J01B 0.29 0.20 0.18
Penicillins J01C 7.23 7.76 7.64
Broad-spectrum Penicillins J01CA 5.15 6.22 5.96
Comb.Penicillins/Bla inhibitor J01CR 0.54 0.14 0.27
Cephalosporins J01D1 1.21 1.95 1.37
Carbapenems J01DH 0.004
Sulfonamides & Trimetoprim J01E 1.35 1.03 1.08
Macrolides & Lincosamides J01F 0.85 0.61 0.42
Aminoglycosides J01G 2.42 1.70 0.87
Quinolones J01M 0.09 0.27 0.034
Glycopeptides J01XA 0.001
Imidazoles J01XD 0.41
Urinary antiseptics G04A 0.67
As it can be seen from the table, in 1999pencillins and broad-spectrum penicillins were themost commonly used antibiotics. From 1994 to1999, use of aminoglycosides decreased nearlythree-fold and use of tetracyclines decreased nearlytwo-fold.
Many factors have contributed to a betterunderstanding of the consequences of antimicro-bial resistance and the necessity of prudent antibi-otic use. Among them, special attention has to begiven to:
• The impact of scientists in research and educa-tion
• Political changes
• International collaboration and support.
Impact of scientists in research and education
Different aspects of epidemiology and mechanismsof resistance in Bulgaria, and methods for theirdetection have been studied (3, 10–42). A total ofseventeen fellowships on the problems of antibi-otic policies, methods for detection of mechanismsand epidemiology of antimicrobial resistance, andsusceptibility testing were performed in leadingworld centres during the last 15 years. Eight re-search projects received grants from Bulgarian(Ministry of Education and Sciences, Medical Uni-versity–Sofia) and international (APUA) organiza-tions. These issues have been the focus of 8 theses.Pharmacodynamics, pharmacokinetics, andpharmacoeconomics studies were performed andseveral clinical trials were carried out.
Educational activities have been addressed topractitioners, providers, and consumers of antibi-otics. More working hours for studying antimicro-bial chemotherapy and antimicrobial resistancehave been included in the education of students inmedicine, dentistry and pharmacy. Written mate-rials on principles of rational antibiotic therapy havebecome available for junior doctors. Post-graduateeducation courses on strategies of antimicrobialchemotherapy for different audiences (microbio-logists, physicians, nurses) have been organized ona regular basis by the Medical University of Sofiaand NCIPD. Popular articles were published inmass media and television discussions took placefor the education of antibiotic consumers.
Political changes
Since 1989, when democratic changes started inBulgaria, new criteria and new standards of drug

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
144
use were developed. State laws about drugs andpharmacies in human medicine were published andupdated. Significant changes were made in drugregulation. As new antibiotics are licensed, each isgiven a complete description of dosage regimen andindications for all forms. The Ministry of Health-care, National Drug Institute and Medical Univer-sity’s Pharmacy Faculty elaborated “Indicators toFollow up the National Drug Policy in Bulgaria”(1994–1996)—P. Uzunov, T Benisheva, G Petrova,Y Uzumov. A health care reform started on July 1,2000, whose aim is to change the previously cen-tralized state health care system to an insurance-based practice.
International cooperation and support
The progress during the last few years would nothave been possible without the support of differ-ent international organizations. The World HealthOrganization (WHO) supported many differentprojects and activities. Professor Thomas O’Briencame personally to Bulgaria to speak on antimicro-bial resistance and to introduce his WHONETprogramme for resistance surveillance. This pro-gramme now performs most resistance monitoringin Bulgaria. APUA supported the establishment ofthe APUA Bulgaria Chapter in 1998. The APUAhas funded the current research project: “Survey ofAntimicrobial Resistance in Bulgaria—first step inunderstanding the necessity of rational antibioticpolicy” (E. Keuleyan and E. Savov) and recentlysupported another project: “Attempt to improveantibiotic use in Bulgarian hospitals” (E. Keuleyanand T. Sokolov). The European Community hasseveral programmes to support education (Tempus),research, and other activities (PHARE). Due to aPHARE project, many international journals be-came available to Bulgarian scientists. PHARE sup-ported the edition, “Bulgarian Therapeutic School”,in 1995.
The Open Society Foundation has supportedactivities for Bulgarian scientists, including train-ing courses, fellowships, participation at congresses,and organizing of symposia. During 1998 it sup-ported a conference in Sofia on anaerobic infec-tions with participation of the American Societyfor Microbiology. Bulgarian scientists participatein different international programmes, projects andorganizations: WHO (Essential Drugs, EURODRUG, Emergency Diseases); APUA; NationalCommittee for Clinical and Laboratory Standards(NCCLS); WHO/CDC External Quality Assur-
ance Programme; European Study Group on Anti-biotic Policy; European Study Group for Antimi-crobial Resistance Surveillance; European StudyGroup of Nosocomial Infections; European Soci-ety for Clinical Microbiology and InfectiousDiseases (ESCMID); European Antimicrobial Re-sistance Surveillance System (EARSS); etc. All theseforms of international collaboration are playing asubstantial role in developing different activities toovercome the antimicrobial resistance problem.
Numerous additional organizations are takingpart in the improvement of antibiotic use in Bul-garia; they can not all be cited and acknowledgedin this brief review. It is also difficult to assess theparticular impact of all factors, events, activities,and works that are dealing with developments inthis area. The author’s opinion is that fellowshipsin the prestigious world centres play a very impor-tant role for the development of future leaders inscience, clinical work, and education. Among theactivities that have not been mentioned, some thatdeserve to be noted are:
• In 1994 a National Society of Chemotherapywas created, which became a member of the In-ternational Society of Chemotherapy (ISC), theEuropean Society of Chemotherapy (FESCI)and the Mediterranean Society of Chemo-therapy. The First National Conference onChemotherapy took place in Sofia in 1995.
• In 1998, the First National Conference onPharmacoeconomics was organized in Sofia.
• Materials about antibiotic resistance are beingdiscussed at the meetings of the National Socie-ties of Clinical Microbiology and MedicalMicrobiology,.
• Efforts have begun for standardization and qual-ity assessment in Clinical Microbiology (43). Aspecialized laboratory for these purposes was es-tablished at the National Center of Infectiousand Parasitic Diseases. In April 2000, a Confer-ence on Standardization and Quality Controlwas organized by Becton Dickinson—Bulgariaand NCIPD in Borovetz.
• An Expert Committee on Antibiotic Policyworking with the Ministry of Healthcare wascreated in August 2000, to work on developingand establishing a national programme for arational antibiotic strategy.
In conclusion, these are some examples of whathas been done in recent years in Bulgaria to curb

145
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
antimicrobial resistance. This experience is on asmall scale. Many more people need to be engagedto accomplish the goal. Many more people need tobe educated and convinced of the problem. Theperfection of antimicrobial chemotherapy will notcome with the efforts of a small group of people orwith fleeting interest. World experience shows thatthis is a difficult and long process. Curbing anti-microbial resistance will take more knowledge,work, education and funds.
References
1. Markova B. Analysis of resistance of bacterial patho-gens in order to optimize antibacterial therapy. In-formative bulletins of Department of Microbiology,Medical University, Sofia and Clinical Microbiol-ogy Laboratory, Alexander’s University Hospital.1993–1998;1–8.
2. Markova B, Bobtcheva S, Topalova S, Kolevsky A.Approaches for the optimization of diagnosis andantimicrobial therapy of infections at theAlexandrovska State University Hospital. Proceed-ings of the Ninth Congress of the Bulgarianmicrobiologists with foreign participation. 1998 V.1. Clinical Microbiology, Sofia. 1998;1:324–329.
3. Savov E. Analysis of the structure of bacterial infec-tions and antimicrobial resistance in order tooptimize antimicrobial chemotherapy. Departmentof Military Epidemiology, Hygiene and Microbiol-ogy, Military Medical Academy, Sofia. 1996, 1997,1998.
4. Kiivet RA, Biba V, Enache D, Fottau V, GuilbinovicJ, Oltvanyi N, Orazem A, Popova M, Stika L.Changes in the use of antibacterial drugs in the coun-tries of Central and Eastern Europe. Eur J ClinPharmacol 1995;48:299–304.
5. Popova M, Popova P, Guencheva G. Consumptionof anti-infective drugs in Bulgaria for the period from1979 to 1994. Pharm World 1997;19(2):93–100.
6. Hadjiisky O. Antibacterial therapy in burns-phar-macokinetics, particularities and indications. J EmergMed 1999;7(2):5–12.
7. Pentcheva P. Strategy of antimicrobial chemotherapyin emergency medicine. J Emerg Med 1993;1(2):6–13.
8. Terziisky G. Programme for Antibiotic Policy ofMedical Institute of Transport. Sofia, 1993.
9. Vachkov P. Contemporary treatment of deepmycoses. Infectious Diseases. Medical Review2000;31(2):3–22.
10. Detcheva A, Chankova D, Kotcheva B, Savov E,Dragijeva E, Genova V, Zamfirova E, Protich N,Tomova I. Monitoring of the Antibiotic Suscepti-bility in Group A Streptococci 1994–1997. Proceed-ings of the Ninth Congress of the Bulgarian
microbiologists with foreign participation; 1998 V.1. Clinical Microbiology, Sofia. 1998;1:380–382.
11. Grigorova V, Sredkova M, Popova V. Susceptibilityof S. pneumoniae strains towards different antibiot-ics. Ibidem. p.392–396.
12. Keuleyan E. Aminoglycoside-Aminocyclitols.Mechanisms of action and antimicrobial resistance.Medico-biologic information 1990;3:3–11 (English/Russian).
13. Keuleyan E and R Avramova. Gentamicin-resistantEnterobacteriaceae and the problem of theirpolyresistance. Probl Infect Parasit Dis NCIPD,Sofia 1994;21:19–20.
14. Keuleyan E, Avramova R, Barzashka S, Boyanova L,Gergova R, Mitov I. Analysis of antibiotic suscepti-bility in orthopedics and trauma hospital. ProblInfect Parasit Dis 1998;26(1):24–27.
15. Keuleyan E, Gergova R, Haralambieva I, MarkovskaR, Sredkova M, Savov E, Dragijeva E, Genova V,Gergova G, Toshkova K. Problematic MRSA/MRSE-comparative susceptibility to antimicrobialagents. Proceedings of the Ninth Congress of theBulgarian microbiologists with foreign participation.1998 V. 1. Clinical Microbiology, Sofia. 1998;1:363–367.
16. Keuleyan E, Markovska R, Savov E, Toshkova K,Dragijeva E, Genova V, Borissova V, Sredkova M.Susceptibility of clinically significant S. aureustowards Macrolides, Lincosamides and Strepto-gramins. Ibidem. 358–362.
17. Keuleyan E, Savov E, Sabtcheva S, Balabanova M,Gergova R, Haralambieva I, Guirgitzova B. Prob-lematic Enterococcus: HLAR and Van-resistant:Comparative study of strains from different hospi-tals. Ibidem. 401–405.
18. Nashev D and K Toshkova. Information on dissemi-nation of methicillin-resistant Staphylococci during1996. Informative Journal of National Center ofInfectious and Parasitic Diseases 1998;2:4–7.
19. Ribarova N and Y Mitova. Etiological characteris-tics of the nosocomial infection in different types ofhigh risk hospital departments. Infectology 2000;37(1):27–32.
20. Sabtcheva S, Borissova V, Kantardjiev T. Occurrenceand fetection of β-lactamases in clinical isolates ofthe family Enterobacteriaceae. Proceedings of theNinth Congress of the Bulgarian microbiologistswith foreign participation. 1998 V. 1. Clinical Micro-biology, Sofia. 1998;1:333–342.
21. Savov E. Plasmids as epidemiological markers ofmicroorganisms in hospital infections. V Med Delo1993;2:41–44.
22. Savov E. Clonal conception in epidemiology andclinical microbiology. Military Medicine and Phar-macy 1997;1:41–43.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
146
23. Savov E, Toshkova K, van Belkum A, van LeenwenW. Use of AP-RAPD polymerase chain reaction fortyping of Staphylococcus aureus strains. Infectology1997;1:15–18.
24. Sotirova P, Tyagunenko Y. Plasmid Profile Analysisof Clinical Isolates of A. baumannii. Proceedings ofthe Ninth Congress of the Bulgarian microbiologistswith foreign participation. 1998 V. 1. Clinical Micro-biology, Sofia. 1998;1:427–433.
25. Sredkova M. 1998. Resistance to penicillins,aminoglycosides and vancomycin of clinical strainsof enterococci. Ibidem. 397–400.
26. Sredkova MP and SI Patchkova. Informative Bulle-tins: Resistance towards antimicrobial agents in clini-cal isolates. Department of Microbiology, HigherMedical Institute–Pleven (1996, 1997; 1, 2).
27. Toshkova K. Methicillin-resistant Staphylococcus.Sofia; 1995.
28. Vatcheva R, Savov E. Detection of clinical isolatesof Family Enterobacteriaceae producing broad spec-trum β-lactamases. Proceedings of the Ninth Con-gress of the Bulgarian microbiologists with foreignparticipation. 1998 V. 1. Clinical Microbiology,Sofia. 1998;1:330–332.
29. Avramova R, Keuleyan E, Ekimova E. Resistance tothird generation cephalospoins in clinical strains ofEnterobacteriaceae. J Chemother 1993;Suppl 3:262–264.
30. Boyanova L, Spassova Z, Kraslev Z, Petrov S,Stancheva I, Docheva J, Mitov I, Koumanova R.Characteristics and trends in macrolide resistanceamong Helicobacter pylori strains isolated in Bulgariaover four years. Diagn Microbiol Infect Dis 1999;34(4):309–313.
31. Boyanova L, Stancheva I, Spassova Z, Katzarov N,Mitov I, Koumanova R. Primary and combined re-sistance to four antimicrobial agents in Helicobacterpylori in Sofia, Bulgaria. J Med Microbiol 2000;49(5):415–418.
32. Keuleyan E. Biochemical determinants of amino-glycoside resistance in Gram-negative microorgan-isms, isolated from urocultures. J Hyg EpidemiolMicrobiol Immunol 1989;33(3):289–97(Czechoslo-vakia).
33. Keuleyan E. Aminoglycoside resistance among Gramnegative bacilli in Sofia, Bulgaria. APUA Newsletter1992;10(4):1–2, 7.
34. Keuleyan E. Presence of acetyltransferases and adeny-lyltransferases in gentamicin-resistant trans-conjugants. Pathol Biol 1992;40(5):556–60 (France).
35. Keuleyan EE, Haralambieva YH, Gergova RT,Markovska RD, Mitov IG. Antibiotic resistance intwo University Hospitals in Sofia, Bulgaria. APUANewsletter 1997;15(3):1, 4–5.
36. Keuleyan EE In: Schouten MA, Voss A, Hookamp-Korstanje JAA and the European VRE Study Group.
Antimicrobial susceptibility patterns of Enterococcicausing infections in Europe. Antimicrob AgentsChemother 1999;43(10):2542–2546.
37. Keuleyan E In: Jones RN, Hare RS, Sabatelli FJ andthe Ziracin Susceptibility Testing Group. In VitroGram-positive antimicrobial activity of Evernimicin(SCH 27899, Ziracin®), a new oligosaccharide com-pared with other antimicrobials: a multicenter in-ternational trial. J Antimicrob Chemother, in press.
38. Setchanova L, Tomasz A. Molecular characterizationof penicilln-resistant Streptococcus pneumoniaeisolated from Bulgaria. J Clin Microbiol 1999;37(3):638–648.
39. Setchanova L In: Jacobs MR, Dagan R, AppelbaumPC, Burch DJ. Prevalence of antimicrobial-resistantpathogens in middle ear fluid: multinational studyof 917 children with acute otitis media. AntimicrobAgents Chemother 1998;42(3):389–395.
40. Toshkova K, Savov E, Soedarmanto I, Lammler CU,Chankova D, van Belkum A, Verbrugh HA, vanLeenwen W. Typing of Staphylococcus aureus isolatedfrom nasal carriers. Zbl Bact 1997;286:547–555.
41. Toshkova K In: Marples RR, Rosdohl VT and Mem-bers of the IUMS Subcommittee. International qual-ity control of phage typing of Staphylococcus aureus.J Med Microbiol 1997;46:511–516.
42. Von R Prager, Savov E, Tschape H. NosokomialeVerbreitung von Resistenzplasmiden durch die Praxisder Kombinationstheraie mit Aminoglycosid- undβ-Lactam–Antibiotika. Bundesgesunbl 1994;1:24–30(Germany).
43. Kantardjiev T, Batchvarova A, Velinov T, KouzmanovA. Development of external quality assessment formicrobiology in Bulgaria. Infectology 2000;37(1)27–32.
■ Sweden: National Antibiotic Use andSurveillance Projects
Major change in the use of antibiotics following anational programme: Swedish Strategic Program for theRational Use of Antimicrobial Agents and Surveillanceof Resistance (STRAMA). Sigvard Molstad, Otto Cars.Scand J Infect Dis 31:191–5, 1999. Report prepared byOtto Cars, Swedish Institute of Infectious DiseaseControl, Solna, Sweden; Chairman, STRAMA, Leader,APUA Sweden, [email protected]
STRAMA
The increase in bacterial resistance in Europe, theincreasing sales of antibiotics in Sweden and thespread of penicillin-resistant S. pneumoniae (PRSP)in southern Sweden have alarmed both the medi-cal profession and national health authorities.Therefore a national project named STRAMA,

147
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
Swedish Strategic Program for the Rational Use ofAntimicrobial Agents and Surveillance of Resist-ance, was initiated in 1994.
National STRAMA-group
A national STRAMA group (www.strama.org) wasappointed which was composed of specialists ininfectious diseases, microbiology, general practice,ear, nose and throat (ENT), and pediatrics, fromthe Swedish Reference Group for Antibiotics. Inaddition, the national STRAMA-group includedmembers from the Swedish Institute for InfectiousDisease Control, the Swedish Medical ProductsAgency, the National Board on Health and Wel-fare, the National Corporation of Pharmacies, theSwedish Veterinary Agency, the Society of CountyMedical Officers for Communicable Diseases, andthe Swedish Network for Pharmacoepidemiology(NEPI). The primary goal of the NationalSTRAMA-group was to stimulate the formationof STRAMA-groups in each county. Together withthese regional groups, the national STRAMA-groupmission was to increase knowledge and understand-ing of the relationship between antibiotic consump-tion and bacterial resistance by both the medicalprofession and the public at large. The main objec-tives were to minimize the development and spreadof resistance, both in outpatients and in hospitals,by a reduction of inappropriate antibiotic use,especially of broad-spectrum antibiotics, and tofurther develop and support resistance surveillanceprogrammes.
Regional STRAMA-groups
In each county at least one STRAMA-group hasbeen formed. The County Medical Officers forCommunicable Diseases are chairing these regionalgroups, which include specialists from differentmedical fields, e.g., infectious diseases, ENT,pediatrics, microbiology, general practice and phar-macy. Some of the groups also include primary carenurses. The groups’ main objective is to evaluatethe use of antibiotics in the area and the pattern ofresistance. After identifying problems in the area,the group uses its knowledge to influence healthcare workers to improve diagnostic procedures andthe prescribing pattern of antibiotics. In some coun-ties with tertiary care hospitals, special groups areformed to influence the use of antibiotics in hospi-tals. Since the immediate threat was the increasingincidence of PRSP, in most counties the initial work
concentrated on the treatment of respiratory tractinfections and antibiotic usage in pre-schoolchildren.
Antibiotic sales statistics
Apoteket AB (Corporation of Swedish pharmacies)keeps records of sales of medicinal products fromthe wholesalers to the pharmacies. From thesedatabases, raw data on sales of antibiotics are ex-tracted. The Anatomical Therapeutic Chemicalclassification system (ATC) is used for classifica-tion of drugs. The unit of measurement is defineddaily doses (DDD) for human medicine and forveterinary medicine mostly in Kg of active sub-stance. Dispensing of antinbiotics is monitored byall pharmacies. This implies that data are brokendown according to hospital or community use. Pre-scriptions statistics are available for outpatients asDDD as well as number of prescribed items/ 1000inhabitants/ day. From 1980 to 1995 this has beenbased on a sample of 1 out of 25 prescriptions,after 1996 all prescriptions served have been regis-tered. The statistics are produced at national, countyand since 1998 also at community level. It can bebroken down to individual drugs, sex and agegroups.
The Swedish Reference Group for Antibiotics(SRGA) and the Swedish Institute for InfectiousDisease Control have developed a national recom-mendation for standardized antimicrobial suscep-tibility testing (www.srga.org). All 30 Swedishmicrobiological laboratories use the SRGA stand-ardized disc diffusion method. The species relatedMIC and zone-diameter breakpoints from SRGAhave been uniformly adopted as well as SRGA rec-ommendations for external and internal qualityassessment programmes. SRGA and the SwedishInstitute for Infectious Disease Control performyearly surveys of approximately 3000 strains (100per laboratory) of each of S. pyogenes, H. influenzae,S. pneumoniae and every second year of E. coli,Klebsiella spp., Enterobacter spp, against a specifiednumber of commonly used antibiotics. Special sur-veys have been directed towards antibiotic resist-ance in Gram-negative hospital isolates, UTIpathogens from primary care isolates and patho-gens isolated from patients at Intensive Care Units.Findings of methicillin-resistant pneumococci(MIC>0.5 mg/l) and vancomycin-resistant entero-cocci (VRE) has been made notifiable.
In 2001, an Antibiotic Resistance SteeringGroup was formed at the Swedish Institute for

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
148
Infectious Disease Control. The aim of this groupis to coordinate an extended national surveillanceof resistance built on existing networks of clinicallaboratories.
Activities and results
Between 1993 and 1997 the total antibiotic usewas reduced by 22%; the reduction was especiallyevident for macrolides and broad-spectrum antibi-otics. The reduction of antibiotic consumption hasbeen more prominent in Sweden than in the otherNordic countries. Recommendations have beenproduced for the use of macrolides, vancomycin,fluoroquinolones and on the treatment of urinarytract infections, chronic bronchitis and skin andwound infections. A folder with information onrespiratory tract infections, antibiotics and resist-ance has been distributed to all Swedish medicalhealth care centres. Three symposia have beenarranged for the regional groups. Media interest forthe project has further increased the knowledge andunderstanding of the problem in the general popu-lation. During the last year Sweden has been en-gaged in several European Union (EU) projectsconcerning antibiotic resistance. The nationalSTRAMA-group will continue to regularly followthe use of antibiotics and the incidence of resist-ance, coordinate necessary surveillance programmesand other activities in the counties and, if needed,make recommendations on identified problem areas.
The South Swedish PneumococcalIntervention Project
Role of communicable disease control measures inaffecting the spread of resistant pneumococci: theSwedish model. Karl Ekdahl, Otto Cars. Clin MicrobiolInfect 1999; 5: 4S48-4S54.
During the last 20 years, the spread of penicillinresistant and multiresistant Streptococcus pneumo-niae has become an increasing international prob-lem. In the early years of the 1990s, the incidencefigures in Malmöhus County in southern Swedenincreased to 8–15%, while the corresponding fig-ures for the rest of Sweden have remained at lowerlevels. Recommendations from a national expertcommittee were issued in 1995, outlining possibleintervention measures against the spread of peni-cillin-resistant pneumococci (PRP) with minimalinhibitory concentration (MIC) for penicillin G(PcG) ≥0.5 mg/L among small children. The firstlarge-scale attempt to implement these recommen-
dations was started in Malmöhus County, in March1995. The project is still running and has been fol-lowed by similar initiatives in most other Swedishcounties.
Since March 1995, all PRP with MIC for PcG≥0.5 mg/L have been directly reported from thethree microbiology laboratories in the county tothe Regional Center of Communicable DiseaseControl (RCCDC) in Malmö. Comprehensive ret-rospective data are available from January 1995.
Whenever an individual with an infection dueto PRP is identified (“index case”), the RCCDCcontacts the local health care centre of that patient.The local physician is then responsible for secur-ing nasopharyngeal specimens from family mem-bers and other close contacts (e.g., day care group)of the index case, in order to identify carriers in thesurrounding area (“contact cases”). All carriers(index cases as well as contact cases) are followedwith weekly nasopharyngeal cultures, until two con-secutive negative specimens have been obtained(“PRP negative”). All control cultures, and otherhealth care contacts due to the project, are free ofcharge for the individual patient. If an identifiedcarrier is a child participating in any form of childday care, nasopharyngeal specimens are also ob-tained from the staff and other children in that daycare group. If more carriers are found, the screen-ing procedures can be extended to the whole daycare centre. Repeated cultures are then obtainedevery 1–2 weeks from the children and staff, untilno more carriers are identified. Pre-school childrenwho are identified as carriers stay away from groupday care until they are PRP negative. The parentsof these children are able to stay at home with fullreimbursement from the social security system, ifthe day care cannot be arranged in any other way.
During the period from January 1, 1995 to June30, 1998, 1545 PRP carriers (1492 individuals)were identified in Malmöhus County. Of the 1545episodes, 642 (41%) were in index cases and 903(59%) in contact cases. The pattern of carriage hasshown a pronounced seasonal pattern, with mostcases occurring during the winter months. Alto-gether 170 of approximately 600 day care centresin the county have been screened for PRP duringthe period. The number of PRP carriers in eachday care centre has varied within great intervals(median 2, interval 1–23), and in half of the daycare centres no further PRP carrier was identified.Screening cultures were, on average, obtained twicein each day care centre, before the day care centrecould be declared “PRP-free”.

149
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
The “Swedish intervention model” has appliedtraditional communicable disease actions (contacttracing and isolation) to a new phenomenon (anti-biotic resistance). The measures are under continu-ing evaluation and the final conclusions have notyet been drawn.
Audit project
Medical audit changes physicians’ prescribing ofantibiotics for respiratory tract infections. Eva Melanderet al. Scand J Prim Health Care 1999; 17:180–84.
In Sweden a prescription is needed to receive anantibiotic, and 60% of all antibiotics are prescribedfor respiratory tract infections (RTIs). Several guide-lines have been issued on a national level, givingrather strict criteria for antibiotic prescribing forRTIs. However, the actual sales of antibiotics donot show compliance with given recommendationsin guidelines. Different methods have been triedto change the prescribing of antibiotics for RTIs,but the habits of physicians seem difficult to change.A group studied the diagnostic procedure and pre-scribing of antibiotics in clinical practice by apply-ing the special Audit Project Odense model (APO)for quality development. The APO model has beenapplied in Denmark and Sweden for some years,and the method is based on a registration of con-sultations in a diagnostic area (e.g., hypertension,diabetes), where each participating physician dur-ing a limited period of time should be able to reg-ister a considerable amount of consultations.Participating physicians choose the registrationparameters before the registration. Statistics are col-lected from the registered parameters. Each par-ticipating physician receives his own personal result,making a comparison between his own prescribingand the general group possible. The aggregated dataof all consultations reflects clinical practice, whichin turn can be compared with guidelines, nationalrecommendations or other studies in the same field.The same registration shall be performed after ap-proximately one year. Most importantly, betweenthe two registrations a discussion should take placeand an educational programme based on the resultof the first registration be formulated.
The APO method was asked for in Orup, amedical district in Malmöhus County, to see if achange in the antibiotic prescribing habits of par-ticipating physicians could be obtained. Consulta-tions for RTIs during the same periods among 25doctors from a neighboring area who had not takenpart in any intervention or follow-up discussion
served as a control. The first registration took placeduring 4 weeks in January–February and thesecond during 4 weeks in November–December.The physicians registered diagnosis, diagnosticmethods, C-reactive protein, bacterial culture,X-ray, ultrasound, antibiotic prescribing (penicil-lin V, ampicillins, macrolides, tetracyclines,cephalosporins, “other antibiotics” and “no antibi-otic”).
In Orup, 33 physicians participated in the firstregistration, 25 in the second. Twenty GPs whoparticipated in both registrations were included inthe study and registered 1124 consultations forRTIs during the first period and 926 during thesecond. In the control group the 25 GPs registered1313 consultations for RTIs during the first pe-riod and 1309 during the second.
The proportion of patients not prescribed anyantibiotic increased in both groups—in the inter-vention group from 45 to 55% and in the controlgroup from 36 to 40%.
The APO model is a method for internal revi-sion of medical practice. The method is based onknowledge of recorded aspects of work and, throughdiscussion, the participants agree on what is betterand what is worse general practice and change theircare accordingly. The registrations are anonymousand the individual physician’s result is known onlyto himself. The APO model has been used on sev-eral occasions in Sweden but has not previouslybeen evaluated.
■ United Kingdom: Tackling antibioticresistance in the UK and Europe
A Personal Perspective by Ian M. Gould, ConsultantMicrobiologist, Department of Medical Microbiology,Aberdeen Royal Infirmary, Aberdeen Royal Hospital,Aberdeen, Scotland. Contact: [email protected]
In 1988, the British Society for AntimicrobialChemotherapy (BSAC) formed a working party(WP), having been stimulated into action by theInfectious Diseases Society of America (IDSA) TaskForce Reports. Up until then, there had been nonational initiatives concerning antibiotic prescrib-ing, which historically was probably at a lower levelthan in the United States.
In addition, because of the National Health Serv-ice, with free care for all, there was less of an issuein the costs of antibiotics which, at least in hospi-tals, amounted to less than 20% of hospital druguse.

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
150
With a nationwide survey the BSAC WP estab-lished which control measures were then opera-tional in UK hospitals, amounts of consumptionin general practice, and educational practices formedical students. Serious deficiencies were notedin antibiotic policies and other control measures.Recommendations were made for minimumcontrol measures to be implemented in hospitals.Educational activities were established as sub-opti-mal and levels of consumption in general practicewere noted to be rising at 2–3% per year (past num-bers). However, as measured by DDDs, consump-tion levels seemed moderate by comparison to manyother European countries (20 DDD/ 1000 patientdays).
These working party reports were published in1993–4. In subsequent years little seems to havehappened except for local initiatives complicatedby reforms of the National Health Service and in-troduction of the purchase-provider split which mayhave been counter-productive by reducing the useof laboratory services by general practitioners whothen had to pay for these services. The same cost-conscious reforms in hospitals led to a markedreduction in bed numbers with consequent over-crowding, bed shortages, and boarding possiblyleading to an upsurge in nosocomial spread ofmultidrug-resistant bacterial clones. There was alsopressure to increase the emphasis on broad-spec-trum empiric therapy and reduce the use of timelylaboratory investigations to discharge patients early.
At this time an increase in hospital cases ofC. difficile colitis was attributed to over-zealous in-terpretation of the British Thoracic Society guide-lines for hospital treatment of community-acquiredpneumonia which recommended third generationcephalosporin therapy for severe pneumonia butwhich were commonly re-interpreted as recom-mending this treatment for any case of pneumoniarequiring hospital admission.
At the time of the House of Lords enquiry intothe problem (1997), which may have been initi-ated by the personal experiences of one or two oftheir Lordships after they or their relatives acquireda methicillin resistant Staphylococcus aureus (MRSA)infection in a hospital, there had already been someactivity at a European level with the Commissionstarting to give grants for Pan-European surveil-lance of resistance. Learned societies like the Euro-pean Society for Biomodulation and Chemotherapy(ESBIC) and The European Society for ClinicalMicrobiology and Infectious Diseases (ESCMID)formed study groups to study resistance surveil-
lance, nosocomial infection, and antibiotic policiessuch as ESGAP (www.escmid.org). Communityaction groups such as SWAB (Holland) andSTRAMA (Sweden) were formed to educate boththe public and prescribers; the European MedicinesEvaluation Agency (EMEA) and the Office Inter-national des Epizooties (OIE) formed workinggroups to address resistance and surveillance issues;and the Copenhagen meeting brought all theEuropean Union (EU) countries together to addressthe issues in 1998.
The most notable result of this meeting was theban on the use of antibiotic growth promoters in1999, which is currently implemented but is beingdebated in the courts by two pharmaceutical manu-facturers. Nevertheless, it seems to have had amajor impact on the animal consumption of anti-biotics in all European Union countries, if officialfigures are to be believed. No doubt there is a largeblack market which we know little about.
In light of the House of Lords Report (1998),the UK government was stimulated into action withits own expert Standing Medical Advisory Com-mittee Report and its separate response to the Houseof Lords Report (1999). The first result of this wasa public education campaign advising patients notto pressure their doctors to give them antibiotics forcolds and flu and recommending 3 days treatmentfor simple UTIs. There is some evidence now, fromthis and similar local campaigns, of reduced expecta-tions by patients, but no sudden downturn in com-munity prescribing of antibiotics-there has been aslow (3%) annual downturn since the mid 1990s.
Meanwhile, the Public Health Laboratory Serv-ice in England and Wales (PHLS), WMA (WelshMicrobiological Association), SMA (ScottishMicrobiology Association) and a local NorthernIreland initiative have been using computerizedlaboratory facilities to organize national surveillancesystems both for nosocomial infection and antibi-otic resistance, although all are still in their pilotphases. The Scottish Government produced twodocuments underlining the importance of infec-tion control and nosocomial infection surveillanceand the PHLS published results of a large surveyon nosocomial infection. Combined with a reportfrom the National Audit Office (NAO) andothers, criticizing the levels of nosocomial infec-tion and poor standards of hospital cleanliness, theUK government (1999) (and latterly the ScottishGovernment) have formed multi-disciplinaryexpert advisory groups on antibiotic resistancesurveillance and nosocomial infection.

151
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
It is also the intention to monitor antibiotic con-sumption and quality of prescribing and there is acommitment to computerized prescribing in hos-pitals by 2005 and computer links between labora-tories and general practitioners by 2001. All generalpractitioners should have had computerized pre-scribing facilities and links to the Internet by theend of 2000. At the moment, all prescriptions ingeneral practice are monitored but there is little dataavailable on the indications for prescribing.Approximately 80% of antibiotic consumptiontakes place in the community. At the moment thereis no formal measurement of prescribing in hospi-tals but the little data in the public domain sug-gests a continued annual increase in cost and DDD,although, as a percentage of hospital drug budgets,it probably remains stable at 20%.
The little available comparative data suggests theUK hospital antibiotic consumption comparesquite well with most European countries (40DDDper 100 Patient Days). This area is also a priorityfor the EU.
It is hoped that the latest round of reforms ofthe National Health Service, with its drive to im-prove quality and ensure better education of andperformance by doctors, will improve antibioticprescribing. This includes the introduction of Clini-cal Governance which intends to make doctorsresponsible for the quality of their antibiotic pre-scribing and empower their employers to ensurethat this quality is achieved. At the moment,accreditation of doctors (and hospitals) is in its in-fancy but developing rapidly, and it is hoped thatCPD will have a large part devoted to antibioticresistance although legislatively. The matter of howmuch can be done legislatively to force the issuesof Antibiotic Resistance and Nosocomial Infectionwith hospitals is another matter.
The newly formed Clinical Standards Board(Scotland) and Commission for Health Improve-ment (England, Wales & Northern Ireland) shouldhave the teeth to deal with this and considerationis being given to benchmarking hospitals of simi-lar types for infection and antibiotic resistance rates.There are encouraging signs from the governmentthat they intend hospitals to carry the issue of anti-biotic resistance forward as a Strategic Goal.
The drive towards evidence-based guidelines andpolicies is slowly progressing with separate govern-ment, PHLS, BSAC, Royal College of Physicians,and other institutions’ initiatives, and the PHLShave published evidence-based guidance for pri-mary care doctors on the Internet (www.phls.co.uk)
The BSAC has also reformed its Education Work-ing Party and the National Prescribing Centre inLiverpool has developed a computer self educationand assessment programme for changing doctors’practices, which looks specifically at antibioticprescribing.
With the merger of many pharmaceutical com-panies, consequent movement out of the UK, andthe development of European Registration of newantibiotics, there is a great concern in the UK atthe loss of a research base from which to developnew antibiotics, so new initiatives in this field arelikely. While there are always counter rumors, theredoes seem to be a genuine, continued desire bothat a UK and a European level to continue with theseinitiatives, not withstanding the politics!
It is too early yet to evaluate the success of anyof this activity. With devolution and the establish-ment of the Scottish Parliament and the Welsh andNorthern Ireland General Assemblies there is evenmore danger of duplication of activities than therewould have been otherwise, so one of the mainconcerns will be to ensure coordination. To this endthere are a relatively small number of core opin-ion-leaders who seem to serve on most of the UKcentral and devolved advisory committees andworking parties and it is hoped that they will en-sure as little duplication as possible.
At a European level the commission in Luxem-bourg has an interest in many aspects of the issuesand has recently issued a draft resolution callingfor a publicity campaign with an annual Antibi-otic Free Day. They are also interested in as muchharmonization of antibiotic use and control meas-ures between member states as is possible and thereis some possibility of legislative control on meas-urement of antibiotic consumption, both inanimals and humans. On the issue of antibiotic re-sistance surveillance, Pan-European initiatives areproving expensive and there is a move to improv-ing the quality of routinely generated data fromdiagnostic laboratories so that it can be used forEuropean surveillance purposes.
Unfortunately there are several systems of sus-ceptibility testing in common use in Europe inaddition to National Committee for Clinical andLaboratory Standards (NCCLS). These includeSwedish, French (CA-SFM), German (DIN) andUK (British Society for Antimicrobial Chemo-therapy, BSAC) methods, all with different inter-pretative criteria. There have been calls for aEuropean system, perhaps adopting NCCLS in allcountries, but we are nowhere near reaching agree-

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
152
ment. Many people consider the diversity of sus-ceptibility testing methods a strength, especiallywhen discovering new resistance mechanisms, andthey suggest that establishing comparabilitybetween different systems will be a satisfactory com-promise. They have, though, been saying this for30 years and we don’t seem to be any further for-ward. Scotland, which does not have a PHLS, hasdecided to adopt NCCLS and also the NISS sys-tem for nosocomial infection surveillance and Walesand Northern Ireland may well do the same. Eng-land (through the PHLS) looks as though it willadopt the BSAC methodology for susceptibilitytesting and the NINS (Nosocomial InfectionNational Surveillance) system for nosocomialinfection surveillance. This latter system uses a dif-ferent set of risk factors than NISS (NosocomialInfection Surveillance System)
■ Scotland: Antimicrobial ResistanceStrategy and Action Plan 2001
Ian M.Gould, Consultant Microbiologist, Department ofMedical Microbiology, Royal Infirmary, Aberdeen RoyalHospital, Aberdeen, Scotland.Contact: [email protected]
The main causes of antibiotic resistance bacteria indiseases of humans in the UK at present are:
1. Excess antibiotic use in primary care
2. Excess use in hospitals exacerbated by epidem-ics of antibiotic resistant bacteria in our hospi-tals.
The underlying reasons are prescriber ignoranceand lack of ownership of the problem.
Audits repeatedly show poor quality, often com-pletely unnecessary antibiotic prescribing, poorcleaning standards in hospitals, and poor compli-ance with infection control procedures. The actionplan concentrates on recommendations to addressthese areas with detail on implementation.
In hospitals, audits repeatedly show unnecessaryantibiotic use in the absence of positive microbiol-ogy and in patients with no sepsis parameters.Often unnecessary, expensive, broad spectrum,toxic agents are administered by the IV route fortoo long, in often inappropriate doses. There is bothinappropriate and under-utilization of laboratories.There is a lack of understanding of how the labo-ratories can help in therapeutic decision-making,such as deciding the need for empiric therapy, thechoice of antibiotic, or how to streamline or stopthe therapy. Finally, there is poor compliance withantibiotic policies.
Poor compliance with policies for hospital clean-ing, hand washing, standard precautions, barriernursing, and isolation of colonized or infectedpatients also occurs due to ignorance, bad practice,overcrowding, or lack of facilities.
The solutions are:
1. Via education, persuade all doctors, health ad-ministration and managers to accept ownershipof the problem.
2. Use incentives, penalties, or extensive, aggres-sive education to get doctors to change their waysof practice (known to be very difficult). Imple-mentation and audit should become prioritiesfor health boards, hospital trusts, etc.
3. Increase resources to allow better patient isola-tion, improved laboratory facilities, (includingaccess to them and communication by them),improved hospital cleanliness, increased staff-patient ratios and reduced overcrowding/board-ing of patients.
Animals and horticulture, surveillance and re-search are all important (but side) issues. We knowthere is a major problem, albeit much greater inmost other countries than in the UK, and weunderstand enough about the causes to addressthem now.

153
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
APPENDIX C
About the authors
August of 1998 was President of the InternationalSociety of Pharmaco-Epidemiology. Dr. Avorn isthe author of over 150 papers in the medical litera-ture on medication use and its outcomes.
John F. Barrett, Ph.D.
Executive Director, Microbiology DepartmentBristol-Myers Squibb CompanyPharmaceutical Research Institute5 Research ParkwayWallingford, CT 06492-7660Phone: 203-677-6499Fax: 203-677-6771E-mail: [email protected]
Currently Executive Director of Anti-InfectivesResearch at Bristol-Myers Squibb, Wallingford, CT.With 16 years experience in the pharmaceuticalindustry, he has experience in a wide breadth ofantibacterial and antifungal discovery and devel-opment efforts at Pfizer and Johnson & Johnson’sRW Johnson Pharmaceutical Research Institute. Dr.Barrett received his B.S. in Biochemistry from Tem-ple University in Philadelphia, PA, and his doctor-ate in Microbiology and Microbial Physiology fromTemple University School of Medicine, with thelate Gerry Shockman, Ph.D. He completed apostdoctoral fellowship in genetic engineering withRoy Curtiss III, Ph.D. (UAB and WashingtonUniversity), and joined Pfizer in 1985, RWJPRI in1989, and BMS in 1997. His research efforts haveincluded β-lactams, penams, penems, β-lactamaseinhibitors, quinolones, novel gyrase inhibitors, HIVgp120/CD4 antagonists, cephems, signal transduc-tion inhibitors, virulence factors, and mammaliantopoisomerase II inhibitors. Dr. Barrett is a mem-ber of numerous editorial boards and author of over160 publications, as well as the 1999–2000Division A Chair of the American Society of Micro-biology. He became a Fellow in the AmericanAcademy of Microbiology in 2000. He leads agroup of research scientists seeking the identifica-tion and development of novel antimicrobials and
Alliance for the Prudent Use of Antibiotics(APUA)
75 Kneeland StreetBoston, MA 02111-1901Phone: 617-636-0966Fax: 617-636-3999E-mail: [email protected]
Jerry L. Avorn, M.D.
Director, Program for the Analysis of ClinicalStrategiesBrigham and Women’s HospitalSuite 341221 Longwood AvenueBoston, MA 02115-5822Phone: 617-278-0930E-mail: [email protected]
Associate Professor of Medicine at Harvard Medi-cal School and Chief of the Division of Pharmaco-Epidemiology and Pharmacoeconomics at Brighamand Women’s Hospital. An internist, geriatrician,and pharmaco-epidemiologist, his research centreson medication use, with particular reference to eld-erly patients and chronic disease. Topics of particu-lar interest include: scientific, policy, and socialdeterminants of physician prescribing practices;efficacy and effectiveness of specific medications;compliance by patients with prescribed regimens;methods to improve the appropriateness of drugprescribing and drug taking; quantification of risksand benefits of drugs; and pharmaceutical cost-effectiveness analysis. Dr. Avorn is also director ofthe Program for the Analysis of Clinical Strategies,a research unit with faculty and staff representingthe disciplines of epidemiology, internal medicine,health services research, psychiatry, and biostatis-tics. He attended Columbia College and HarvardMedical School, and completed a residency ininternal medicine at the Beth Israel Hospital in Bos-ton. Dr. Avorn serves on several national andinternational panels as an expert on the determi-nants and outcomes of medication use, and until

ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS WHO/CDS/CSR/DRS/2001.10
154
antifungals through a combination of classical dis-covery strategies and techniques and a proprietarygenomics effort. Dr. Barrett has been involved withthe development of several antibacterials currentlyon the market including ofloxacin, levofloxacin, andgatifloxacin, and is currently working on the de-velopment of a novel MRSA-cephem (BMS-247243) and the des-quinolone (BMS-284756/T-3811) at Bristol-Myers Squibb.
Peter G. Davey, M.D.
Professor of Clinical PharmacologyUniversity of DundeeNethergate, Dundee DD1 4HNScotland, UKPhone: +44 (0)1382 660111E-mail: [email protected]
Has expertise in clinical pharmacology, infectiousdiseases, and health economics. He has served as aProfessor of Pharmacoeconomics, Clinical Pharma-cology and Infectious Diseases at the University ofDundee, Scotland. Among his many teaching ac-tivities, he has developed new curricula focusingon antimicrobials for a number of courses for medi-cal and dental students. He has extensive researchexperience, including clinical trials and evaluationsof antimicrobials, assessments of antimicrobial ac-tion in vitro and in experimental animals; clinicalpharmacokinetic studies of antimicrobials, andstudies of gentamicin treatment. Since 1996, Dr.Davey has served as Head of Pharmacoeconomicsfor the Medicines Monitoring Unit (MEMO),where he focuses on economic evaluation and out-comes research of drug treatment, and on antibi-otic policies and their influence on the developmentof drug resistance in hospitals and the community.He has helped develop treatment guidelines andnational policies on antibiotic use in Scotland,served as an advisor to the House of Lords Com-mission on Antimicrobial Resistance, and hasspoken extensively on antimicrobial use at interna-tional symposia, conferences, and meetings.
Stuart B. Levy, M.D.
President, Alliance for the Prudent Use of Anti-bioticsRoom 704, South CoveTufts University School of Medicine136 Harrison AvenueBoston, MA 02111-1817
Phone: 617-636-6765Fax: 617-636-0458E-mail: [email protected]
President and founder of the Alliance for the Pru-dent Use of Antibiotics, and immediate past presi-dent of the American Society for Microbiology. Amicrobiologist and physician, Dr. Levy discoveredthe mechanism for tetracycline resistance (efflux)and was among the first to document the transferof drug resistance among animals and humans. Dr.Levy is the author of one of the most importantbooks on the subject, The Antibiotic Paradox: HowMiracle Drugs are Destroying the Miracle, which hasbeen widely cited in both the lay and scientificmedia. He has also written more than 200 scien-tific and medical papers and special journal edi-tions on the topic. A world-renowned leader in thefield of antibiotic use and resistance, he has chairedand served on numerous national and internationaladvisory boards and committees, including: theNIH Fogarty Center’s study on The Use of Antibi-otics Worldwide (as Chairman); the advisory panelfor the USA Office of Technology Assessment re-port on the Impacts of Antibiotic Resistant Bacte-ria; the EPA Subcommittees on Health andAntibiotic Resistance; and the WHO ScientificAdvisory Group on Antimicrobial Resistance. Dr.Levy has also served as a consultant for the WorldHealth Organization, the USA FDA, the NationalInstitutes of Health, and other national and inter-national organizations. He is currently Professor ofMedicine and of Molecular Biology/Microbiology,the Director of the Center for Adaptation Genet-ics and Drug Resistance at Tufts University Schoolof Medicine, and a Staff Physician at the New Eng-land Medical Center.
Scott A. McEwen, D.V.M.
Professor, Department of Population MedicineUniversity of GuelphGuelph, Ontario N1G 2W1CanadaPhone: 519-824-4120, ext. 4751E-mail: [email protected]
Professor in the Department of Population Medi-cine, Ontario Veterinary College, University ofGuelph. He is a veterinarian whose research focuseson the epidemiology of food-borne infections infood animal populations, particularly Salmonella,E. coli and antibiotic resistant organisms. He has

155
WHO/CDS/CSR/DRS/2001.10 ANTIBIOTIC RESISTANCE: SYNTHESIS OF RECOMMENDATIONS BY EXPERT POLICY GROUPS
conducted extensive research on human healthimpacts of antimicrobial use in animals, includingstudies of antibiotic and chemical residues in milkand meat, and the association between resistanceand antibiotic use on farms, and has published morethan 80 papers in peer review journals. Dr. McEwenhas served as a consultant for WHO on the humanhealth impact of antimicrobials in food animals,and as panel member for the U.S. FDA on antimi-crobial resistance risk assessment. He also chairedthe Health Canada Advisory Committee on Ani-mal Uses of Antimicrobials and their Impact onResistance and Human Health. Dr. McEwenteaches food safety to veterinary students and gradu-ate students at the University of Guelph.
Thomas F. O’Brien, M.D.
Medical Director, Microbiology LabBrigham and Women’s Hospital75 Francis StreetBoston, MA 02115-6110Phone: 617-732-6803E-mail: [email protected]
Vice President of APUA, is a leading authority onantibiotic resistance and AMR surveillance. An in-fectious disease specialist and microbiologist, Dr.O’Brien helped develop the WHONET surveil-
lance program. He also set up the WHO Collabo-rating Center for Surveillance of Resistance toAntimicrobial Agents at Brigham and Women’sHospital in Boston in 1985, which has establishedan international network of microbiology labora-tories dealing with antimicrobial resistance surveil-lance. Dr. O’Brien has served as an advisor onnumerous national and international committeesdealing with antimicrobial resistance, including theNIH Task Force on Antibiotic Resistance, whichhe chaired from 1984 to 1986; the WHO Scien-tific Working Group on AMR (1981); the FDA’sVeterinary Medicine Advisory Committee (since1994); the Office of Technology AssessmentAdvisory Panel on Impacts of Antibiotic-ResistantBacteria; the Inter-Agency (FDA, CDC, USDA)Working Group on Antimicrobial Resistance; andthe CDC Working Group on Drug Resistant Strep-tococcus pneumoniae. He has also served as a con-sultant on antimicrobial resistance to WHO (inGeneva and Manila), PAHO, the British House ofLords, and the National Health Research Instituteof Taiwan, among others. Medical Director of theMicrobiology Laboratory at Brigham and Wom-en’s Hospital for the past 20 years, Dr. O’Brien is apioneering researcher in the area of antimicrobialresistance, having conducted microbiological stud-ies on resistance since the mid-1960s.

Related Documents











