ANTEPARTUM HAEMORRHAGE

ANTEPARTUM HAEMORRHAGE. Obstetric Haemorrhage Ranks as the First cause of maternal mortality accounting for 25 – 50 % of maternal deaths.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ANTEPARTUM HAEMORRHAGE
Obstetric Haemorrhage
Ranks as the First cause of maternal mortality accounting for 25 – 50 % of maternal deaths

APH: Epediology & Causes Magnitude: 4% of women may develop APH.
Causes: placenta previa (1/200) placental abruption (1/100) uterine rupture (<1% in scarred uterus) vasa previa (1/2000-3000) Local causes Unknown origin
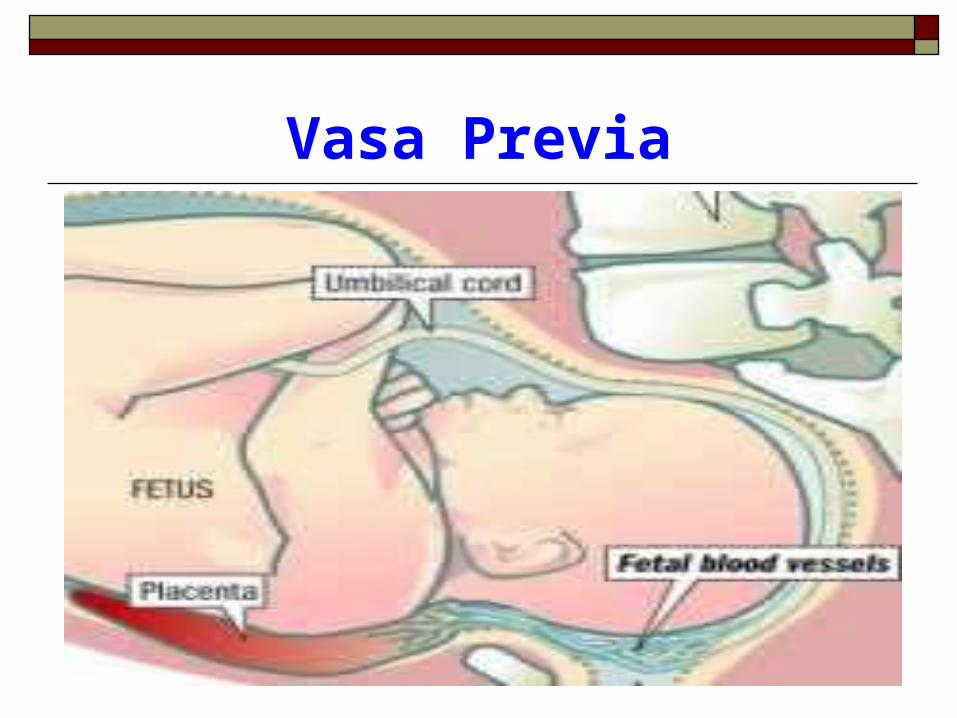
Vasa Previa
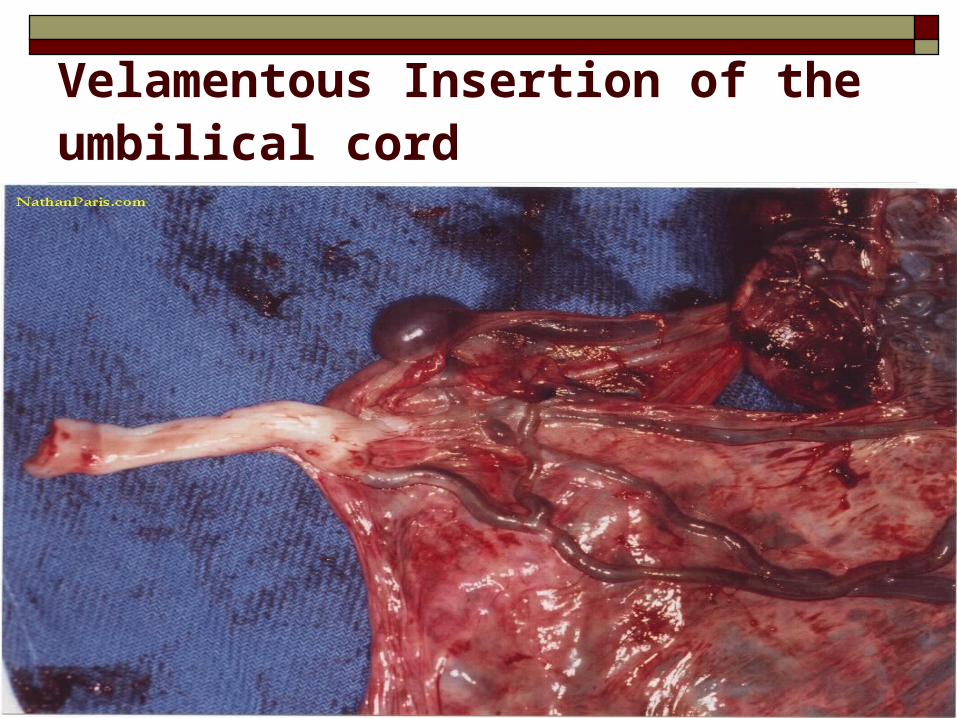
Velamentous Insertion of the umbilical cord

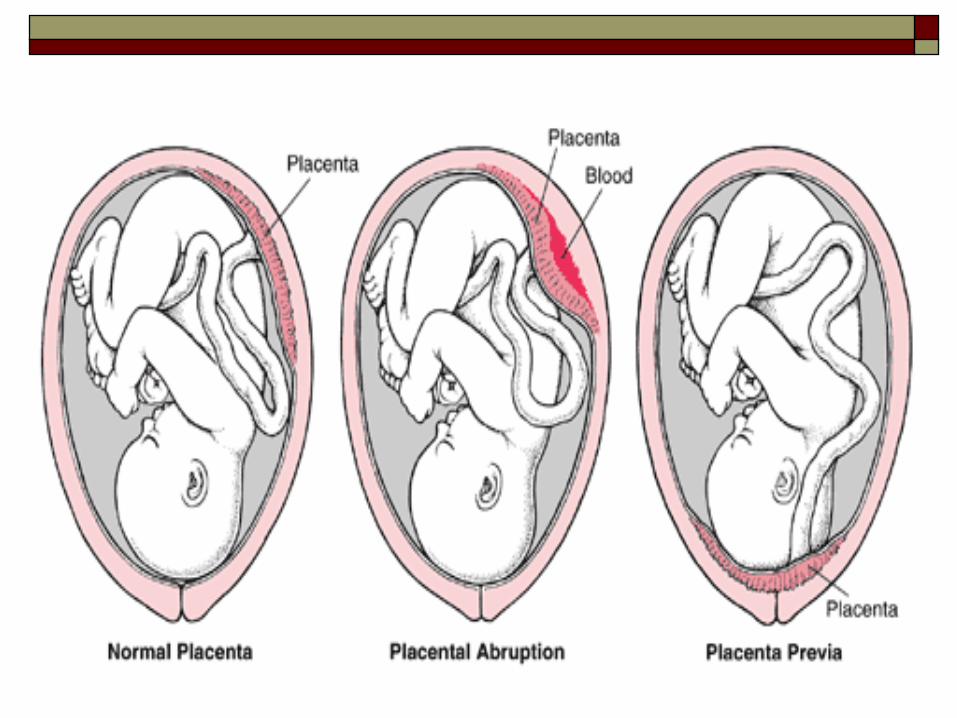
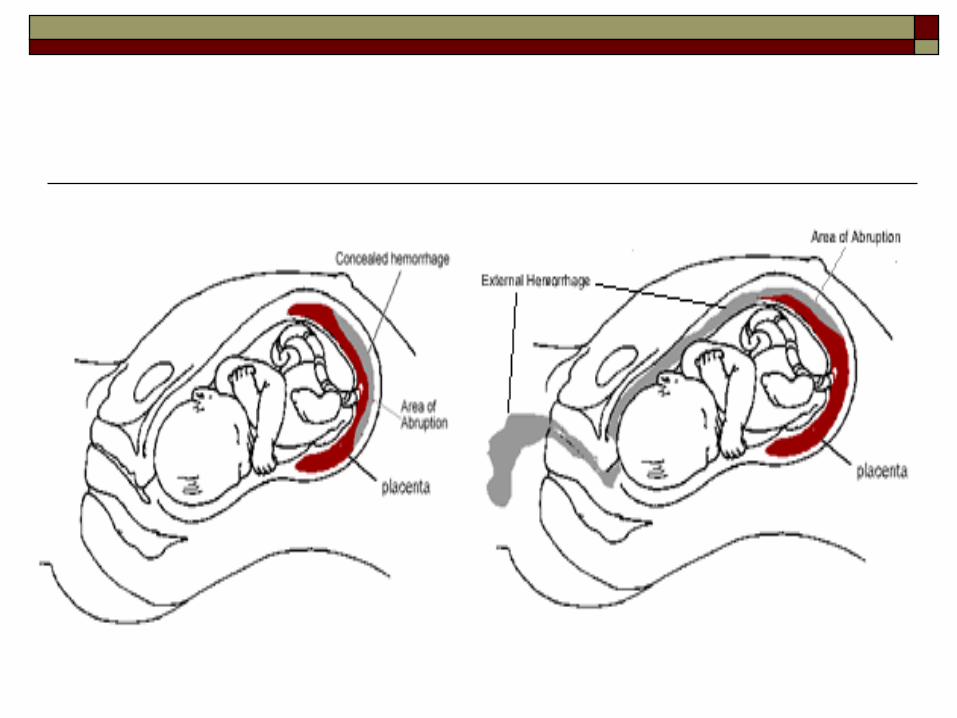
I. ABRUPTIO PLACENTA
Definition: Early separation of the normally implanted
placenta after 28/40 and before the end of
second stage of labour
Recurrence: The risk of recurrent abruption in a
subsequent pregnancy is high.
Abruptio placenta: Classifications
Are based on
1. Extent of separation: Partial vs complete
2. Location of separation: Marginal Vs central
3. Clinical presentation: Revealed, concealed and
mixed
4. Clinical Severity: Mild, Moderate and Severe
Class 1 Mildest form: approx 48% of all cases.
• No vaginal bleeding to mild vaginal bleeding
• Slightly tender uterus• Normal maternal BP and
heart rate• No coagulopathy
(clotting problems)• No fetal distress
Clinical Severity
Class 2: moderate -approx 27% of all cases.
• No vaginal bleeding to moderate vaginal bleeding
• Moderate-to-severe uterine tenderness with possible tetanic contractions
• Maternal tachycardia with orthostatic changes in BP and heart rate
• Fetal distress• Low fibrinogen levels present
(causing clotting problems)
Class 3: Severe form: Approx 24% of all cases.
• No vaginal bleeding to heavy vaginal bleeding
• Very painful tetanic uterus
• Maternal shock
• Coagulopathy
• Fetal death
Clinical Severity
I. Abruptio placenta: Risk factors
Hypertensive Disease
Multiple pregnancy
Trauma
PPROM
I. Abruptio placenta: Risk factors
Anaemia
Polyhydramnios – sudden
↓intrauterine pressure
Short cord
Uterine leiomyoma: esp if located
behind the placental implantation
site, predispose to abruption

Abruptio Placenta: Abruptio Placenta: FeaturesFeatures
Pain and tenderness Initially localized then becomes
generalized due to endometrial injury – extravasations of blood
Vaginal bleeding Maternal distress Often I.U.F.D
Placental Abruption: Complications
Shock Acute renal failure
Cause: ?seriously impaired renal perfusion 2° to ↓CO and intrarenal vasospasm as in preeclampsia
DIC Consumptive coagulopathy 2° to
hypofibrinogenemia along with elevated levels of fibrinogen–fibrin degradation products
Placental Abruption: Complications
Fetal distress/demise
PPH
Couvelaire Uterus: Widespread extravasation of blood into the uterine
musculature and beneath the uterine serosa.
Sheehan syndrome
Puerperal sepsis
Placental Abruption: Management
Management depends on: fetal maturity, degree of severity, viability of the fetus/fetal distress
Treatment modalities Expectant management of pregnancy Induction/augmentation of labor Caesarean section

Placental Abruption: General Management
1. Delivery
Resuscitation
FFP, whole blood, IV fluids
Monitor BP
Catherization - monitor urine output
Placental Abruption: General Management
ARM
Induce/Augment labour
Oxytocin infusion or prostaglandin if
necessary to induce contractions
Bed site clotting time
Done regularly
Placental Abruption: General Management
2. Caesarean Section Indications for Caesarean Section
salvageable baby, Severe vaginal bleeding, Poor progress, Transverse lie, inadequate pelvis
Post delivery -watch out for PPH Why?
Myometrial myofibrin loose contractility Failure to clot

PLACENTA PRAEVIA PLACENTA PRAEVIA - DEGREES- DEGREES
1. Total placenta praevia
The internal cervical os is covered
completely by placenta.
2. Partial placenta praevia
The internal os is partially covered
by placenta.
PLACENTA PRAEVIA PLACENTA PRAEVIA - DEGREES- DEGREES
3. Marginal placenta praevia
The edge of the placenta is at the margin of the internal os.
4. Low-lying placenta
The placenta is implanted in the lower uterine segment such that the placental edge actually does not reach the internal os but is in close proximity to it.
PLACENTA PRAEVIA: PLACENTA PRAEVIA: Predisposing factors
Multiparity
Advanced maternal age
Prior C/S or other uterine surgery
Prior placenta previa

Placenta Previa: Diagnosis
Painless vaginal bleeding in 2nd/3rd trimester
Confirmed by ultrasound
Up to 10% may have simultaneous abruption
Maternal shock is uncommon with 1st
presentation of bleeding

Placenta Previa: Obstetric Management
Vaginal exams are avoided
If possible, delay delivery until fetus is mature.
34 weeks - buy time for steroids
Prevent contractions with tocolytics -indocid
Mobilize blood donors
Placenta Previa: Obstetric Management Resuscitate - IV fluid and blood, Monitor BP and amount of bleeding Deliveryi. Mild non persistent bleeding
GA 34 weeks Buy time for steroids and hospitalization. Prevent contractions with tocolytics - Mobilize blood donors Oral haematenics
GA 37 weeks = consider Elective CSii. Persistent bleeding requires immediate delivery
whatever the gestation
Placenta Previa: Management
Indications for delivery: Persistent bleeding requires delivery whatever the
gestation Active labor Documented fetal lung maturity 37 weeks gestational age. Excessive bleeding Development of another obstetric complication
mandating delivery

Placenta PraeviaPlacenta Praevia
Elective caesarean if 37 weeks
? Never cut through the placenta
PLACENTA PRAEVIA
Lower segment may need to be packed
Placenta previa may be assoc. with placenta accreta, increta or percreta → PPH
PPH - 2° to poorly contractile nature of the LS of uterus.
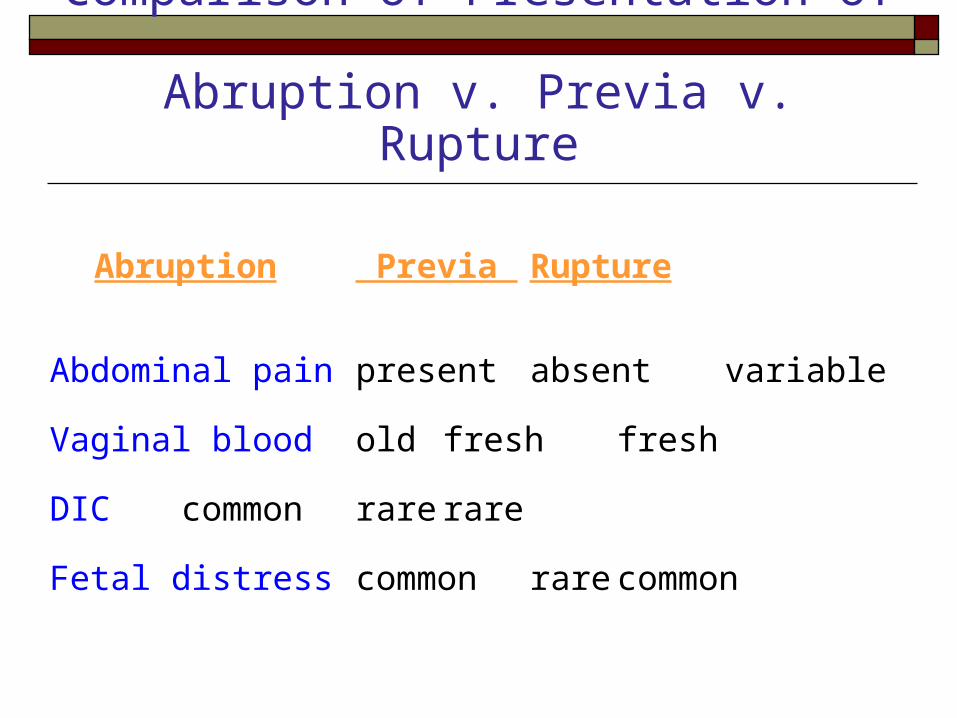
Comparison of Presentation of Abruption v. Previa v. Rupture
Abruption Previa Rupture
Abdominal pain present absent variable
Vaginal blood old fresh fresh
DIC common rare rare
Fetal distress common rare common
Vasa Previa “Umbilical vessels separate in the membranes
at a distance from the placental margin and some of the vessels (fetal) cross the internal os and occupy a position ahead of the presenting part of the fetus.”
ROM may cause fetal exsanguination.
High fetal mortality (50-75%)
Risk factor: multiple gestation (esp., triplets).
Vasa Praevia Diagnosis
Moderate vag bleeding + fetal distress Vessels may be palpable thru dilated cervix Vessels may be visible on ultrasound
Difficult to distinguish clinically from abruption.
Treatment C/S, Resuscitation of infant (volume)

Local & Unknown CausesLocal & Unknown Causes of APH of APH
Rupture of uterus
Carcinoma of cervix
Trauma
Cervical polyp
Bilharzia of cervix Cervicitis
Related Documents











