1 Annual Report 2016/17

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Annual Report 2016/17

2
Contents PERFORMANCE REPORT ....................................................................................... 3 1. Performance Overview ........................................................................................ 4 2. Performance Analysis ........................................................................................ 10 ACCOUNTABILITY REPORT ................................................................................. 28 1. Corporate Governance Report........................................................................... 29
1.1. Members Report ....................................................................................... 29 1.2. Statement of Accountable Officer’s Responsibilities ................................. 32 1.3. Governance Statement ............................................................................. 34
2. Remuneration and Staff Report ......................................................................... 55 2.1. Remuneration Report ................................................................................ 55 2.2. Staff Report ............................................................................................... 64
3. Parliamentary Accountability and Audit Report .................................................. 70 ANNUAL ACCOUNTS ............................................................................................. 71

3
PERFORMANCE REPORT
Mrs Jackie Pederson Accountable Officer 25 May 2017
4
1. Performance Overview The purpose of this overview is to give our stakeholders a short summary with sufficient information to understand our organisation, our purpose, the key risks to the achievement of our objectives, and how we have performed during the year. 1.1. Statement from the Chief Officer We have seen some exciting commissioning developments in the last year including a new intermediate care Rapid Response Falls Service launched at the end of January 2017, which brings together a multi-skilled team of staff from local NHS organisations and Doncaster Council to help keep vulnerable people out of hospital by caring for them at home, instead of on a ward, after they have had a fall. We also commissioned, in partnership, a new Doncaster Admiral Service which includes dedicated dementia specialists called Admiral Nurses and Dementia Advisors who have made a big impact on local families who have been touched by dementia. We have committed investment into a collaborative mental health crisis response and care pathway, alongside investment for community support and accommodation. We have been commissioning for improvements in urgent care including enhancing our Front Door Assessment & Signposting Service in A&E, and in cancer we have been recognised by the All-Party Parliamentary Group for being one of the most improved areas in the country for patients living with cancer for at least one year after diagnosis. We have also reduced waiting lists for children’s autism assessments and published a Care Home Strategy jointly with Doncaster Council. We added Planned Care as a Delivery Plan area in November 2016 in recognition of work already underway on a number of planned care pathways of care, and also in response to the national RightCare programme of work. We have developed a Commissioning for Value Decision Making Framework which supports us in transparent and coherent prioritisation for the commissioning of health and wellbeing services. We took on delegated responsibility from NHS England for commissioning primary medical care services from 1 April 2016, and we have been busy working through our newly-established Primary Care Commissioning Committee to drive forward quality improvements for patient. We have enacted our Primary Care Strategic Framework into developing more responsive primary care services to the needs of the most vulnerable patients in general practices. Despite increasing financial constraints and demands placed upon the local healthcare system, we have achieved our statutory financial duties as an NHS commissioning organisation, ending the year with our required financial surplus. 2016/17 has seen an increasing focus on collaborative commissioning with our local partners across the Health and Social Care system. We have led the development of, and in October 2016 published, a local Doncaster Place Plan across statutory organisations in Doncaster. This is the first time in Doncaster that we have articulated a shared vision across health and social care. We have also become a

5
partner in the Sustainability & Transformation Plan (STP) across South Yorkshire & Bassetlaw; published in November 2016 this plan builds on strong partnerships already in place across South Yorkshire and Bassetlaw to review services better commissioned “at scale”. We have also become a member of a new Working Together Joint Committee of CCGs which has initiated public consultation on Hyper Acute Stroke Services and Children’s Surgery & Anaesthesia. We are a key member of Team Doncaster, the Local Strategic Partnership, and during the year our Chair has been nominated as the Vice Chair of the Doncaster Health & Wellbeing Board. As a Membership organisation composed of our 43 Member Practices, clinical insights and experience have driven forward our system transformation programmes to improve healthcare services for the Doncaster population. We have continued to work towards the ambitions in our five year commissioning strategy Moving Forward, Getting Better, and our Governing Body has refreshed and reaffirmed this strategic direction with our focus remaining on care out of hospital, care of the elderly, and coordinated care delivered through 12 transformational outcome-based delivery plans, which also align to the Doncaster Place Plan and the Sustainability & Transformation Plan. We have seen changes in our leadership team in the last year, starting the year in April 2016 with a new Chair in Dr David Crichton, and with myself as a new Chief Officer. During the year we also had changes in leadership in both our Chief Nurse and Chief of Strategy & Delivery posts. The refreshed Governing Body is driving forward the commissioning agenda together, working ever closer with commissioners in Doncaster Council. 2017/18 and the years that follow will be increasingly challenging financially for the entire NHS, and Doncaster is no exception. Our goal is to strive for continuous quality improvements whilst seeking to operate within a very challenging financial environment with increasing demands placed upon healthcare services. We believe that working in partnership across health and social care is fundamental to meeting these challenges and to ensuring integration of care for patients. We all look forward to meeting these challenges together.
Jackie Pederson Chief Officer
6
1.2. Purpose and activities of the organisation Our role: As a clinically-led statutory NHS body, we are responsible for planning and commissioning health care services for our local area to achieve the best possible health outcomes for our local population, and in doing so acting effectively, efficiently and economically. We do this by assessing local needs, agreeing priorities and strategies, and then commissioning services on behalf of our population from a range of providers whilst constantly responding to changing local needs. Vision and values: Our vision is to work with others to invest in quality healthcare for Doncaster patients, and our values are:
• The needs of patients are paramount
• Drive forward continuous improvement
• Relationships based on integrity and trust Our strategy: Our 5 year commissioning strategy Moving Forward, Getting Better is refreshed annually, enacted into Commissioning & Contracting Intentions for our providers, and sets out our clear and credible plans for delivering our vision for health care services in partnership to meet the needs of the Doncaster population. It recognises the challenge in ensuring healthcare services are affordable and sustainable in an environment of low financial growth, but in the context of continuing demand for services and a reduction in funding for public services. We know that we must commission for transformational change in order to achieve greater efficiency and effectiveness of spend on health services whilst continuously improving quality. We therefore have significant continuity in priorities from our previous annual reports:
Three strategic ambitions
• Care out of Hospital
• Care of the elderly services
• Coordinated Care
Twelve delivery plans
• Urgent Care: embedding the new service model and supporting the wider health and social care system.
• Intermediate Care: design, implementation and testing of an integrated care model across health and social care.
• Cancer: focused on survival outcomes.
• Mental Health and Learning Disabilities: crisis and specialist mental health, primary mental healthcare and inpatient mental healthcare.
• Primary Care: implementing our strategy through enhancing the offer to patients across four “pillars” of primary care – Keeping People Well, Responsive Care, Proactive/Coordinated Care and Extended Primary Care, as well as supporting Practices to work more closely together.
• Community Services: embedding holistic community nursing care across Doncaster, and moving on to focus on more specialist services.
• End of Life Care: delivering and maintaining the new community model.
• Children’s and Maternity: focused on improved services.
• Dementia: focused on improving diagnosis rates and effective post diagnostic support.

7
• Care Homes: focused on quality improvements, education and market development.
• Medicines Management: improving prescribing quality.
• Planned Care: reducing elective care demand on acute providers, and linking to the national RightCare programme and service / pathway redesign.
Our Constitution: Through our Constitution, our 43 Member Practices delegate responsibility for running the organisation to our Governing Body, which in turn is supported by a range of strategic Committees and forums. Our Governing Body’s role is to set the strategic direction of the organisation, seek assurance that the strategy is being delivered, and to set the culture of the organisation. Our culture: The culture of our organisation is one of distributed leadership across clinicians, managers and support staff. We aim to align our strategy, our people and our processes to drive forward our vision and effectively enact our strategic plan Moving Forward, Getting Better. In the last year we have refreshed our Organisational Development Strategy, with facilitated external support, and in close liaison with all our local stakeholders; this has ensured alignment to our collaborative commissioning commitments across the Doncaster Place Plan and Sustainability & Transformation Plan. The refreshed Strategy was approved by our Governing Body in December 2016. The Strategy focusses on three different audiences: a) Governing Body, b) CCG Staff Team, c) Wider Partners. The associated action plan covers three elements of leadership: leading as individuals, leading the organisation, and, importantly as we work ever more collaboratively with our commissioning partners, leading the system. There is a Governing Body “Sponsor” for each element of the Action Plan, and close liaison with our Colleague Engagement Group (representatives of our staffing body) and our Joint Negotiation and Consultative Forum with our Staff Side colleagues. Our partnerships: We are committed to partnership working and to the benefits which collaborative commissioning arrangements can bring. We therefore actively participate in and contribute to the Team Doncaster Local Strategic Partnership with particular emphasis on the Doncaster Health & Wellbeing Board. We are also a member of a healthcare commissioner programme of work called Working Together to review and redesign services across a wider geography. We have led the development of and published a partnership Local Digital Roadmap for Doncaster. Our 360 Survey results show that the majority of respondents rate their overall working relationship with us as very good or fairly good, and there is a general upwards trend of improvement across all questions when compared to previous years. This is a positive outcome and reflects the open, transparent and engaging CCG leadership culture which we are trying to foster. We also host a shared service on behalf of 12 local CCGs (including our own) providing Previously Un-assessed Periods of Care assessments for Continuing Healthcare.
1.3. Key issues and risks Our annual Governance Statement later in this report contains a full schedule of risks managed throughout the year. In summary:
8
Efficiency programme: We have managed a risk on our Governing Body Assurance Framework throughout the year relating to achievement of our ambitious 2016/17 efficiency programme. Progress has been reported through the Finance Report to each monthly Governing Body meeting. At the Governing Body meeting in January 2017 positive assurances for 2016/17 were noted. We have achieved all our year-end financial duties within the business rules under which we are required to operate, including achievement of our required surplus. Towards year-end the risk was therefore amended to reflect the challenges in the 2017/18 forecast position. Progress on developing efficiency plans in response to the 2017/18 financial position is positive with initiatives identified to close the efficiency gap, however many of the initiatives are ambitious and will be challenging to achieve. Collaborative commissioning: We have closely reviewed risks associated with the different commissioning footprints and collaborations which emerged at a rapid pace throughout the year. Urgent and emergency care: As with many areas across the country, we continue to focus on the four-hour waiting standard in Accident and Emergency (A&E). Recognising that this isn’t just about what happens in A&E but also in the rest of the hospital and the wider health and care system, we have focused on this with all partners and within our newly instituted A&E Delivery Board. Our focus as a CCG has been two-fold: driving forward the opportunities for patients to be seen in the most appropriate setting as close to home as possible, and avoiding unnecessary attendance at A&E through services like our Same Day Health Centre and our Urgent Care Centre, with a streaming service at the front door of A&E to direct patients to the most appropriate service for their need. Going concern: We remain a going concern as a statutory NHS Body. 1.4. Performance summary
CCG Improvement &
Assessment Framework
The 2016/17 year-end CCG Improvement & Assessment Framework
rating for our CCG will be available on MYNHS from July 2017 www.nhs.uk/service-search/Performance/Search.
Our Delivery Plans
We have monitored progress against our Delivery Plans throughout the year. We have had particular successes with:
• Our Urgent Care system: We have increased use of our Same Day Health Centre and our Urgent Care Centre, and increasing numbers of patients are being streamed into more appropriate settings by the Front Door Assessment & Signposting Service in A&E. Waiting times for A&E at Doncaster & Bassetlaw Teaching Hospitals were better than the England average in 2016/17.
• Intermediate Care: We have developed a robust case for change, agreed joint commissioning principles with Doncaster Council for the future commissioning of an integrated intermediate care service, and we are piloting this approach with an integrated Rapid Response Falls Service. The new Falls service has quickly made its mark - in its first six weeks it helped 44 people, with over 90 per cent of them being able to remain at home after assessment, with specialist support to aid their recovery.
9
• Cancer: The All-Party Parliamentary Group on Cancer gave recognition to Doncaster for being one of the most improved areas in the country when it comes to patients living with cancer for at least one year after diagnosis. Our Chair is now the Senior Responsible Officer for the Cancer Alliance Group for Prevention, Early Identification and Diagnosis of Cancer. NHS Doncaster CCG, Doncaster & Bassetlaw Teaching Hospitals and the Cancer Alliance are undertaking extensive work to improve waiting times with a particular focus on inter-provider transfers.
• Children’s and Maternity: We have reduced waiting lists for children’s autism assessments, which is important as we have a higher number of referrals compared to similar areas to ours in other parts of the country. A successful charity-based sleep service which we have funded in Doncaster for local parents is supporting care closer to home, saving hospital appointments, and reducing medication requirements. It was featured positively on the BBC’s Panorama programme towards the end of the year.
• Dementia: A partnership between the CCG, Doncaster Council, the statutory and Voluntary Sector has resulted in the formation of The Doncaster Admiral Service. This includes dedicated dementia specialists called Admiral Nurses and Dementia Advisors who have made a big impact on local families who have been touched by dementia. 1,700 people and their families affected by dementia now living at home in Doncaster have access to timely and effective post diagnostic care and support.
• Care Homes: We have developed and published a Care Home Strategy. The commissioned Care Home Liaison Service continues to delivery effective support to Care Homes enabling residents to receive quality care and prevent unnecessary hospital admission.
Financial Performance
NHS Doncaster CCG’s revenue resources were allocated to our contracts with providers and to the investment programmes within Delivery Plans. We remained in a positive financial position throughout the year. The Annual Accounts have demonstrated the achievement of all financial targets, in particular a Surplus of £12,508,000 against a resource allocation of £498,520,000.
The Annual Accounts have been prepared under International Financial Reporting Standards and in accordance with the Annual Reporting Guidance issued by NHS England and the Department of Health Manual for Accounts. The Integrated Single Financial Environment ledger system facilitates the national consolidation of all sets of Accounts within the NHS England resource boundary, is open to view by NHS England colleagues, and thus has facilitated in-year performance management by the NHS England Area Team.
Provider Performance
Our Governing Body receives a monthly report on all provider performance measures. These reports are available on our website www.doncasterccg.nhs.uk. Challenges in-year have included the Cancer 62 day referral to treatment target in respect of Inter-Trust transfers, and, in common with other areas of the country the A&E 4-hour wait, Ambulance handover times, and Referral to Treatment Times (RTT). Areas which are identified as being significantly off track are subject to remedial action plans with providers.
10
Statutory duties
We have achieved all required statutory duties.
2. Performance Analysis 2.1. How we measure performance The table below details our approach to measuring performance.
NHS England’s CCG Assurance
Framework
We monitor our performance against the domains within the NHS England CCG Improvement & Assessment Framework on an ongoing basis. NHS England produce a dashboard each quarter showing CCG performance against the indicators underpinning the domains. This is reported to Governing Body along with an update on actions being undertaken to address areas of poor performance. Our Executive Team meets with NHS England on a quarterly basis in a “Checkpoint” meeting to formally take stock of our performance against the domains. The outcomes from this assessment are reported to our Governing Body via our monthly Chair & Chief Officer Report.
Our Delivery Plans
Each of our delivery areas is subject to a Delivery Plan. Each plan is designed to a) illustrate the specific outcome for the key local challenge, b) understand the effect that actions have on service quality, c) identify the success indicators or milestones to provide assurance that we are on track to achieve the overall outcomes, and d) identify the actions which will support us to deliver the success indicators and the high level outcomes.
We monitor progress against our Delivery Plans on a monthly basis. The performance and outcomes identified within the local Delivery Plans are included into the Key Performance Indicators and reporting requirements during annual contract negotiations with our local providers. Progress against indicators for all Delivery Plans is updated and reported monthly. These reports are used to stimulate discussion on the progress made and the actions taken with regards to whether the actions are having the anticipated impact on outcomes. Each action is rated where appropriate to stimulate discussion. Exceptions to our Delivery Plans are reported to the Governing Body either through specific reports such as on Intermediate Care or via our Chair & Chief Officer Reports.
Financial performance
Our Finance & Contracting Team monitor our financial performance on an ongoing basis, and our financial performance, including progress on meeting our efficiency savings target, is reported to our Governing Body on a monthly basis in our Finance Report.
Provider performance
including NHS Constitution standards
We measure the performance of our providers using contractually agreed schedules of key performance indicators and quality indicators. The indicators include both those mandated in the NHS Standard Contract and locally agreed measures based on our Delivery Plans and other identified key areas for improvement. Data is provided on a regular basis by our providers in line with the contracted schedules which

11
demonstrates their performance against the required standards.
The quality and completeness of the data received is continually assessed by the CCG’s Performance and Intelligence Team. Where performance is below the required standard for a single, or for multiple measures, the Provider is asked for an explanation including actions and timeframes to bring the performance or quality of care back up to the required standard. This is undertaken between Performance and Quality colleagues in each organisation throughout the year, and formally at monthly Finance, Performance and Information Group (FPIG) meetings. Relevant items discussed at FPIG are escalated through the governance structure to the Strategic Contracting Meeting for the provider where the issue is discussed with senior management representatives from both organisations.
Outstanding issues are also reported monthly to the CCG’s Governing Body via the Quality & Performance Report, and to our Senior Management Team. Where an issue is not resolved by the Provider in a satisfactory way, we may choose to issue a contractual Performance Notice to the provider, outlining the problem and the expectations for resolution. A full report on performance against NHS Constitution standards and performance by each of our main providers is reported to the Governing Body via our monthly Quality & Performance Report; exceptions are highlighted in the coversheet to the report.
Better Care Fund
The Better Care Fund (BCF) is intended to transform local health and social care services so that they work together to provide improved and joined up care and support. It is a government initiative, bringing existing resources from the NHS and local authorities into a single pooled budget. Performance against the pooled budget is reported to our Governing Body on a monthly basis within our Finance Report.
2.2. Development and performance in-year 2.2.1. CCG Assurance Framework We have monitored our progress against the domains within the CCG Improvement & Assessment Framework throughout the year. The framework recognises that assurance is a continuous process which considers the breadth of a CCG’s responsibilities. The 2016/17 year-end CCG Improvement & Assessment Framework rating for our CCG will be available on MYNHS from July 2017 www.nhs.uk/service-search/Performance/Search. Following a year-end baseline assessment in 2015/16 of “Good”, positive quarterly interim reviews with NHS England culminated in a positive Annual Review for our CCG in April 2017. 2.2.2. CCG Performance on Delivery Plans
Urgent Care
• Urgent Care systems across the country have been under pressure throughout the past year, and the same is true for Doncaster. Whilst the 4 hour wait target in A&E has not been met in every month of the year, Doncaster & Bassetlaw Teaching Hospital NHS Foundation Trust performance has generally remained above the national average. Recognising that pressures in A&E are not just about what
12
happens in A&E but also in the rest of the hospital and the wider health and care system, we have developed strong partnership working arrangements through the local Doncaster System Resilience Group which we chair, and through our new partnership A&E Delivery Board with NHS Bassetlaw CCG.
• From October 2015 we commissioned a new Urgent Care system comprising services such as our Same Day Health Centre, our Urgent Care Centre, Emergency Care Practitioners, a GP Out of Hours service, and a streaming service at the front door of A&E to direct patients to the most appropriate service for their need. This has supported us in trying to avoid unnecessary attendance at A&E. We have refined the model throughout the past year, and we have also been keen to understand patient experience of the new streaming service; we have worked in partnership with Co:Create to evaluate patient experience, which has proved to be positive.
• The Paramedic Pathfinder project, which is aimed at reducing the number of people taken to A&E through linking in to alternative care provision in the community, is under implementation in Doncaster
• We have worked with colleagues across South Yorkshire and Bassetlaw on the developing Urgent and Emergency Care Network.
Intermediate Care
• “Intermediate Care” comprises a range of integrated services to promote faster recovery from illness, prevent unnecessary acute hospital admission and premature admission to long-term residential care, support timely discharge from hospital and maximise independent living.
• Our review of intermediate health and social care needs was launched as one of the Better Care Fund schemes of work. The evidence collected in the review has been used to produce a “case for change”. Via co-production with our partners and our patients, we have designed a future model and we are testing this through a pilot Rapid Response Falls Service.
• In 2017/18 we aim to roll out a single point of access and assessment to four types of integrated service responses with shared records, a flexible workforce and a more person centred approach to planning and delivering care. The four types of service are: a rapid/urgent response, an intensive/short term community response, a medium term community response, and a smaller bed based response supported by a number of longer term interventions.
Cancer
• In the past year the All-Party Parliamentary Group on Cancer gave recognition to Doncaster for being one of the most improved areas in the country when it comes to patients living with cancer for at least one year after diagnosis.
• Our Chair is now the Senior Responsible Officer of the Cancer Alliance Group for Prevention, Early Identification and Diagnosis of Cancer.
• We have been achieving the majority of the national Cancer targets, with the exception of the 62 day referral to treatment target, where we are working to support improved Inter-Trust transfers of care where our patients need care outside of Doncaster.
• A review of a new Chemotherapy model has been undertaken and assessments around the needs of South Yorkshire, Bassetlaw and North East Derbyshire patients have contributed to inform and
13
implement the model. Recommendations will be submitted to the Cancer Alliance Board.
Mental Health and Learning Disabilities
• Our Wellness for Life Event, held at the end of the last financial year, was a great opportunity for local services and people to come together to share ideas and experiences to help shape mental health in Doncaster. The outcomes from this have shaped our mental health commissioning work in 2016/17. Our Mental Health Strategic Alliance, a partnership made up of the CCG, wider NHS, Doncaster Council and charities, has focused on improving services for local people and supporting community mental health interests such as the People Focused Group (PFG) in Doncaster.
• We have aligned our Mental Health Delivery Plan with the national guidance Implementing the Five Year Forward View for Mental Health published by NHS England in July 2016, and we are working with our partners to develop services – having invested in the development and expansion of mental health services over the last few years.
• We have committed investment into a collaborative crisis response and care pathway, including into the Crisis Hub which was evaluated in-year and extended into 2017/18, and investment for community support and accommodation. We have also invested non-recurrent funding to expand crisis prevention services by supporting capital developments within the Third Sector for safe places.
• Work has been undertaken to consolidate and enhance Acute Psychiatric Liaison services.
• In Doncaster, we have more than 1400 people who are registered with learning disabilities. We want to do more to improve their mental and physical health and make services easier for them to access and we have been co-producing improvements to care pathways with partners and patients. We have been working with Choice for All Doncaster (ChAD), a Committee of adults with learning disabilities who speak up for themselves and their peers about issues which affect their lives. ChAD has representatives at our Learning Disability Partnership Board meetings. ChAD members helped us to develop a new poster campaign which aims to increase awareness of the symptoms of bowel cancer amongst people with learning disabilities.
• We chair the South Yorkshire and North Lincolnshire Transforming Care Partnership (TCP) which is made up of Rotherham, Doncaster, Sheffield and North Lincolnshire CCGs. The partnership aims to transform care for people with a learning disability and autism, and has developed a plan showing how we will lower the number of people with learning disabilities in inpatient hospital beds; early work on this is already showing a reduction in numbers in Doncaster.
Primary Care
• We have developed a Primary Care Strategic Framework which takes learning from the 5 Year Forward View and the Prime Ministers Challenge Fund Vanguard Sites to inform and support Primary Care transformation in Doncaster. This Framework sets out our ambitions and those of our Member Practices to position Primary Care at the heart of system transformation. The strategic approach is comprised of four pillars of care which represent the enhanced patient offer in the areas of self-management and prevention, responsive and accessible care, proactive co-ordinated care, and

14
extended services in primary care. Each of these pillars will be commissioned via a dedicated service specification, with the required additional investment in primary care. The proactive specification was the first to be developed.
• We have an extensive engagement approach with General Practice in Doncaster, which is multi-faceted including:
• Monthly slots at TARGET (our education event) for engagement on current commissioning topics;
• A monthly meeting of our Primary Care Provider Engagement Group, which is open to all practices;
• Regular meetings of the 5 CCG commissioning localities, attended by all Member Practices, alongside 2 to 3 Doncaster-wide events per annum hosted by the CCG to allow continuous awareness, participation and influence in strategic direction;
• Bi-monthly meetings of the CCG Clinical Reference Group;
• Regular meetings between CCG representatives and the Local Medical Committee and Local Pharmaceutical Committee to maintain positive relationships.
• We have also supported the emergence of Federations of General Practices as providers in Doncaster.
Community Services
• We have continued to evaluate the 24/7 community nursing services, and taken opportunities to transfer further care into the community and partnership. We have also reviewed the interface between core and specialist nursing teams to reform specialist nurse functions in order to create a focus on specialist advice and support to primary / community care with a reduced emphasis on caseload and delivery of routine activity within specialist functions. We have worked to better integrate the Domiciliary Care service with community nursing to provide holistic end of life care.
• We have undertaken a stocktake of the therapy services offered in Doncaster including activity, costs, staffing, referral routes, gaps in provision and cohorts of patients. We have worked together with Providers to develop quality standards and patient focussed outcomes with the aim of working to enhance and improve services including Speech & Language Therapy and Dietetics.
• We have reviewed services available for patients with Parkinson Disease across acute and community services and developed a refreshed pathway to deliver improved patient outcomes.
15
End of Life Care
• In 2015/16 we commissioned a new community model for end of life care for people who are in the last few days of their life. Acting on referrals from healthcare professionals, the Woodfield 24 Care Services staff are called in, often at very short notice, to provide care and support to those who want to die at home rather than at hospital or in a hospice. We have continued to embed the model throughout the past year, and on evaluation it has proved very successful and has achieved good integration with the Community Nursing service.
• We held our inaugural End of Life Care conference in April 2016, bringing together experts and practitioners from across the local patch to share learning on areas such as advance care planning, end of life for people with dementia, and legal Issues surrounding end of life.
• September 2016 saw the launch of the Doncaster Community Specialist Palliative Care Service, which strives to make care even better for terminally ill Doncaster people and help support their families. The new service model has been tested and evaluated during late 2016/17.
• We have further increased the number of primary care practices completing Gold Standards Framework training and we have also supported the training into wards at Doncaster & Bassetlaw Hospitals, and rolled out local packages of training across community services.
Children’s and Maternity
• We have worked to reduce waiting lists for children’s autism assessments as we have a higher number of referrals compared to similar areas to ours in other parts of the country.
• A successful charity-based sleep service which we have funded in Doncaster for local parents was featured positively on Panorama towards the end of the year.
• In partnership with partner CCGs in the Working Together collaborative, we have asked Doncaster people for their views on proposals to change children’s surgery and anaesthesia services across South Yorkshire, Wakefield, Bassetlaw and Chesterfield. Decisions will be made in 2017/18.
• In partnership with Doncaster Council, we have been working with an organisation called Young Minds to develop a way to include the voice and opinions of children and young people in commissioning.
• Doncaster’s Local Transformation Plan for promoting, protecting and improving our children and young people’s emotional wellbeing and mental health was refreshed during the year and reflects the progress made in year one and the plans to continue to make improvements across the system.
• In partnership with the Local Maternity System Board we have worked to develop a new Local Maternity System offer.
• We have seen a reduction in emergency admissions for long term conditions (epilepsy, asthma and diabetes).
Dementia
• We have continued to raise awareness and reduce stigma of dementia with pre diagnosis information and support, including a successful Dementia Friends campaign. Doncaster now has over 16,000 Dementia Friends and over 100 Dementia Champions.
• Doncaster’s diagnosis rate is now over 75%, well above the Prime

16
Ministers challenge of 67% and well above national and regional averages.
• Having such a good diagnostic rate has enabled us to develop effective post diagnostic services. The Doncaster Admiral Service now provides effective and timely care and support for 1,700 people and their families affected by dementia living at home.
• We have embedded the needs of dementia patients within the Care
Home Strategy. There are 900 people with dementia in Doncaster Care Homes. The commissioned Care Home Liaison Service continues to delivery effective support to Care Homes enabling residents to receive quality care and prevent unnecessary hospital admission.
• We have continued to foster co-production of services with people affected by dementia, their carers and families. An ex carer chairs the Doncaster Dementia Forum and a lady with Young Onset Dementia co-chairs the Doncaster Dementia Strategic Partnership. The voice of people with dementia feeds right through our governance structure to Team Doncaster.
Care Homes
• Care Homes are an essential part of the Health and Social Care landscape, providing care to some of the most vulnerable people in society. It is essential that the provision of care within Care Homes is high quality and meets the needs of the people who live there. In partnership with Doncaster Council we have developed a Care Home Strategy which sets out our joint 5 year approach to this sector of care, providing a clear direction of travel for existing care providers and a clear indication to new providers wishing to become part of the Doncaster Care Home market.
• The strategy’s key aim is to look at how a model of care provision can be developed that leads to individuals being able to remain in their own home for longer, because this is what our population have told us that they want.
• Work has been ongoing throughout the year to enact the action plans contained within the Strategy. This has included extensive work focusing on the workforce and their education and development needs, reviewing the current “organisation” of care being delivered.
• NHS England has also recently released a document recently looking at ‘Enhancing Care in Care Homes’, and this is also being used to reinforce and influence the local Care Homes Strategy.
Medicines Management
• As part of the national RightCare programme analysis, we identified prescribing as an area of further focus for us as an organisation. As a result we developed a delivery plan for Medicines Management. As one of the actions from this we introduced a Gain Share Local Enhanced Service with our Member Practices to focus on areas of prescribing where we were identified as an outlier compared to other CCGs.
• We also introduced a piece of new software (OptimizeRx®) to all our Member Practices. This system delivers messages within the GP clinical systems at the point of prescribing or review. The intention of this is to assist practitioners to align with the Doncaster Formulary, Traffic Light List and local and national guidelines, thus addressing both quality and cost issues.
17
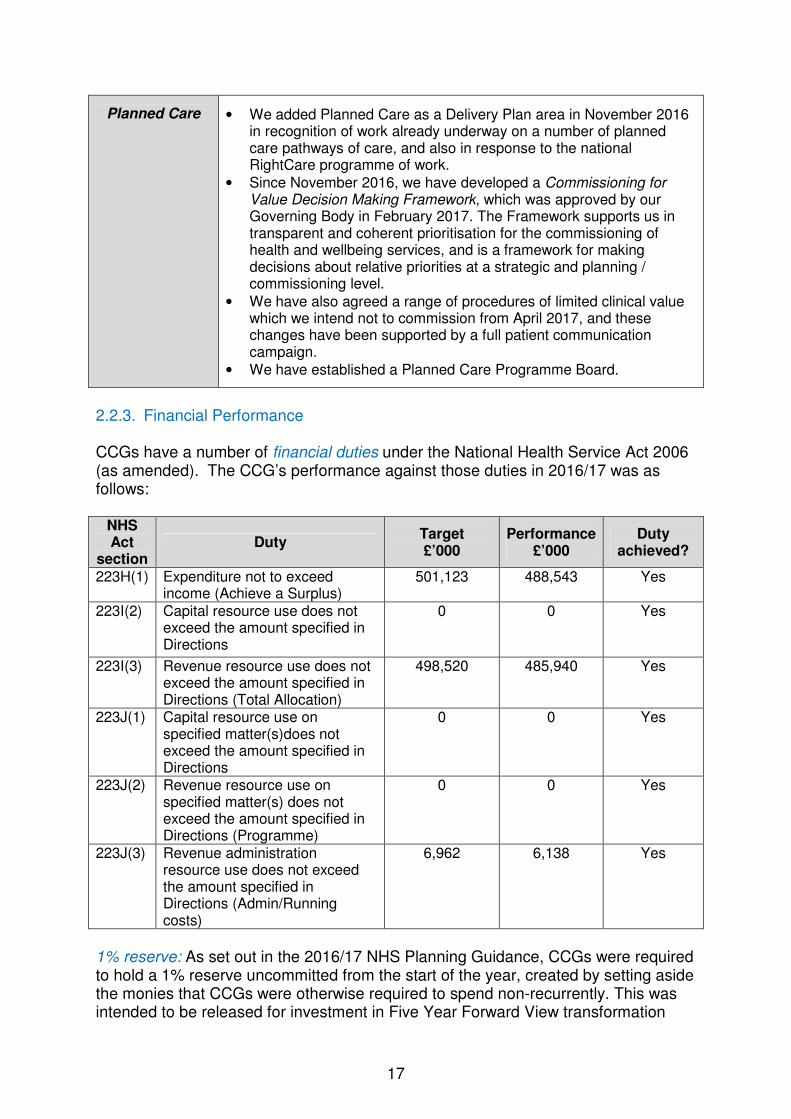
Planned Care
• We added Planned Care as a Delivery Plan area in November 2016 in recognition of work already underway on a number of planned care pathways of care, and also in response to the national RightCare programme of work.
• Since November 2016, we have developed a Commissioning for Value Decision Making Framework, which was approved by our Governing Body in February 2017. The Framework supports us in transparent and coherent prioritisation for the commissioning of health and wellbeing services, and is a framework for making decisions about relative priorities at a strategic and planning / commissioning level.
• We have also agreed a range of procedures of limited clinical value which we intend not to commission from April 2017, and these changes have been supported by a full patient communication campaign.
• We have established a Planned Care Programme Board.
2.2.3. Financial Performance CCGs have a number of financial duties under the National Health Service Act 2006 (as amended). The CCG’s performance against those duties in 2016/17 was as follows:
NHS Act
section Duty
Target £’000
Performance £’000
Duty achieved?
223H(1) Expenditure not to exceed income (Achieve a Surplus)
501,123 488,543 Yes
223I(2) Capital resource use does not exceed the amount specified in Directions
0 0 Yes
223I(3) Revenue resource use does not exceed the amount specified in Directions (Total Allocation)
498,520 485,940 Yes
223J(1) Capital resource use on specified matter(s)does not exceed the amount specified in Directions
0 0 Yes
223J(2) Revenue resource use on specified matter(s) does not exceed the amount specified in Directions (Programme)
0 0 Yes
223J(3) Revenue administration resource use does not exceed the amount specified in Directions (Admin/Running costs)
6,962 6,138 Yes
1% reserve: As set out in the 2016/17 NHS Planning Guidance, CCGs were required to hold a 1% reserve uncommitted from the start of the year, created by setting aside the monies that CCGs were otherwise required to spend non-recurrently. This was intended to be released for investment in Five Year Forward View transformation
18
priorities to the extent that evidence emerged of risks not arising or being effectively mitigated through other means. In the event, the national position across the provider sector has been such that NHS England has been unable to allow CCGs’ 1% non-recurrent monies to be spent. Therefore, to comply with this requirement, NHS Doncaster CCG has released its 1% reserve to the bottom line, resulting in an additional surplus for the year of £4.8m. This additional surplus will be carried forward for drawdown in future years. Financial risks have been managed in-year including:
• Doncaster & Bassetlaw Hospitals NHS Foundation Trust (DBHFT) contract over-performance in-year due to increased activity. This position has been well managed during the year.
• Prescribing and High Cost Drugs – work to address variations in both outcomes and costs has been and will continue to be taken forward as part of the Primary Care Strategic Framework, specifically the medicine optimisation work within the Medicines Management Delivery Plan. A prior approval process was initiated with the Acute Trust from 1 April 2016 to address any non-compliance with NICE guidance and correct charging through the Payment by Results (PbR) tariff mechanism. This has had a positive impact on costs.
• Over performance on smaller contracts. This has been managed in-year.
• The CCG assumed devolved responsibility for Primary Medical Care commissioning with effect from April 2016. The total allocation devolved from NHS England was £41m and expenditure has been contained within this budget. The financial position is discussed regularly at the Primary Care Commissioning Committee, including developments for 2017/18 and implementation of the GP Five Year Forward View.
• Increased Individual Placements activity (including Continuing Healthcare, Specialist Placements and Section 117 packages) including cases being stepped down from NHS England, however some of this has been offset by a reduction in Continuing Healthcare costs. This position has been closely monitored and managed throughout the year.
• An additional risk arose in-year in relation to the nationally agreed rates for Funded Nursing Care (FNC) which caused an additional cost pressure of approximately £600,000. Following a national review, the rate increased by 39% from £112 per week to £156.25 per week; the CCG has had no choice but to implement this rate. The further national review on the agency element of the FNC has not impacted on the rates for 2016/17, but will impact on 2017/18.
• The CCG’s running costs have been maintained within the prescribed funding envelope.
To help manage and offset these risks a small contingency fund of £2.2m was established, and delivery of the year-end position was effectively managed. Our financial plans for 2017/18 are very challenging, with the CCG facing unprecedented pressures and an £11.6m efficiency target. In support of these financial pressures, we also aim to:
• Strengthen our underlying financial position by committing funding non-recurrently where possible to pump prime new services that will lead to overall reduced costs, accelerated efficiencies or increased productivity.

19
• Link any investment back to one of our delivery plans or achievement of Doncaster Place Plan or Sustainability & Transformation Plan commitments.
• Closely monitor our running costs to ensure that we do not exceed our statutory running cost allowance.
• Deliver an £11.6m ambitious efficiency programme. This is key to providing the finances required to drive investment forward, and failure to deliver the programme is one of the major risks we face which would result in the need to curtail the investment programme.
We are aware of the potential future risks and drivers that could affect the financial performance and have assessed the potential impacts and have a strategy in place to deal with them should the need arise. The following issues could influence the delivery of this plan:
• If growth in the acute sector cannot be contained.
• If levels of required disinvestments cannot be delivered.
• If growth in high cost case numbers (e.g. Continuing Healthcare) is above that projected.
• An unanticipated growth in registered population.
• If in-year cost pressures exceed planning assumptions and cannot be managed down to affordable levels.
• The impact of unpredictable costs, such as the impact of new technologies cannot be afforded within current assumptions.
Where there is downside risk this will be mitigated by utilisation of the contingency reserve, a reprioritisation and re-profiling of investments, identifying and delivering additional efficiency opportunities and the planned surplus. Upside risk will allow us to bring forward schemes planned for future years or invest in further initiatives which benefit the health of the population of Doncaster. 2.2.4. Provider Performance Our monthly Quality & Performance Reports received by our Governing Body meeting held in public provide detailed information on Provider performance. The section below highlights some key areas on which the Governing Body has focussed particular attention throughout the year.
A&E
• Performance against the 4 hour target in Quarter 4 was 88.86% (Quarter 3 90.07%), which is below the NHS Constitution standard (95%) and the trajectory set by NHS England (also 95%). Full year performance is 91.41%. Whilst these fall below the national target, our local Acute Trust has performed comparatively better than the national average against a picture of significant pressures mirrored nationally.
Cancer Waiting Times
• Cancer waiting times from referral to treatment within 62 days have been below the required standard at various points throughout the year but this is consistent with national average performance.
• Robust action is being taken to improve performance including weekly reporting of the position, electronic system flags at early points in the pathway, discussion of individual breach reports to ensure learning is in place, e-referral pathways and the development of electronic transfer

20
protocols, and improved access to diagnostics.
• We review demand for key tumour sites via the Cancer Capacity and Demand group, and one of the aims of our Cancer Delivery Plan is achievement and maintenance of all cancer waiting times standards.
• Joint work across South Yorkshire & Bassetlaw is taking place on inter provider transfer (IPT) under the Cancer Alliance.
Referral to Treatment
(RTT)
• We have not achieved the standard of 92% of active waiters waiting under 18 weeks since September 2016, however performance was better than the national average for the whole of 2016/17.
• 8 specialties are struggling to achieve the 92% standard: General Surgery, Urology, General Medicine, Dermatology, Ophthalmology, Rheumatology, Trauma & Orthopaedics, and ENT.
• Robust actions are being undertaken to improve the position including securing additional capacity both internally and through outsourcing, holding turnaround sessions with Care Groups, collaborative working on referral management and support in reduce demand, an increase in Pre-Assessment capacity, dedicated Pathway Coordinators in Care Groups to manage specialty level pathways to improve planning and performance, and a validation process between Care Group and the Data Quality Team alongside improved Business Intelligence.
• The Recovery Plan, alongside our Planned Care Delivery Plan, is being overseen by our recently-formed Planned Care Programme Board.
Ambulance Response
Times
• The Ambulance Response Programme clinical coding pilot began in April. Yorkshire Ambulance Service has failed to achieve the 75% standard for calls being responded to within 8 minutes in 2016/17.
• Ambulance Handover times have improved from 2015/16.
• We had a change to the lead commissioner arrangement commenced from April 2016, ahead of developing a Joint Committee in 2017/18.
• Yorkshire Ambulance Service’s latest Care Quality Commission rating is “Good”.
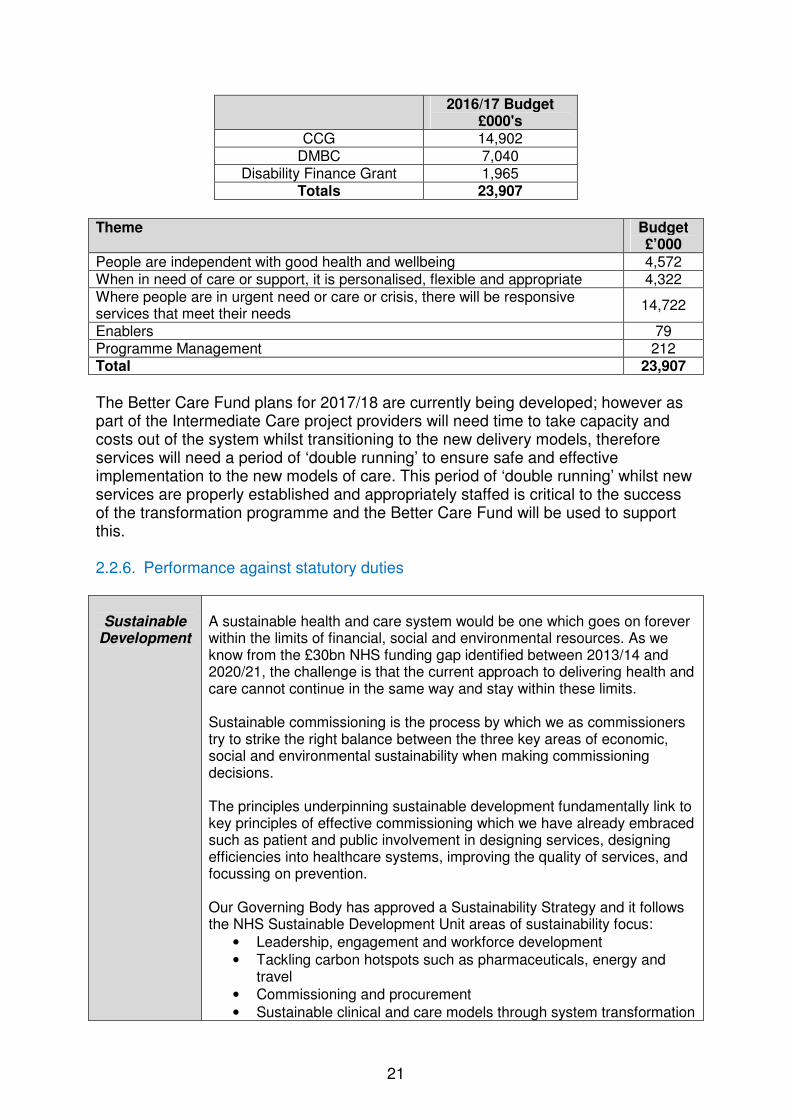
2.2.5. Better Care Fund Performance The Better Care Fund (BCF) is a single pooled budget that was set in 2015/16 and aims to facilitate a transformation in integrated health and social care. There is a structured partnership framework in place to coordinate, communicate, manage and control the activities of the Better Care Fund. We have a Section 75 agreement with Doncaster Council for the Better Care Fund and the fund is overseen by a Strategic Health and Social Care Partnership Board reporting to the Health and Wellbeing Board. The total pooled budget is £23,907,000 and is summarised overleaf. The CCG’s £14.9m is utilised for historical CCG contracts which are linked to common priorities with the local authority. The £7m Doncaster Council element is used jointly for shared priorities such as Intermediate Care.
21
2016/17 Budget
£000's CCG 14,902
DMBC 7,040 Disability Finance Grant 1,965
Totals 23,907
Theme Budget
£’000
People are independent with good health and wellbeing 4,572 When in need of care or support, it is personalised, flexible and appropriate 4,322 Where people are in urgent need or care or crisis, there will be responsive services that meet their needs
14,722
Enablers 79 Programme Management 212 Total 23,907
The Better Care Fund plans for 2017/18 are currently being developed; however as part of the Intermediate Care project providers will need time to take capacity and costs out of the system whilst transitioning to the new delivery models, therefore services will need a period of ‘double running’ to ensure safe and effective implementation to the new models of care. This period of ‘double running’ whilst new services are properly established and appropriately staffed is critical to the success of the transformation programme and the Better Care Fund will be used to support this. 2.2.6. Performance against statutory duties
Sustainable
Development
A sustainable health and care system would be one which goes on forever within the limits of financial, social and environmental resources. As we know from the £30bn NHS funding gap identified between 2013/14 and 2020/21, the challenge is that the current approach to delivering health and care cannot continue in the same way and stay within these limits. Sustainable commissioning is the process by which we as commissioners try to strike the right balance between the three key areas of economic, social and environmental sustainability when making commissioning decisions. The principles underpinning sustainable development fundamentally link to key principles of effective commissioning which we have already embraced such as patient and public involvement in designing services, designing efficiencies into healthcare systems, improving the quality of services, and focussing on prevention. Our Governing Body has approved a Sustainability Strategy and it follows the NHS Sustainable Development Unit areas of sustainability focus:
• Leadership, engagement and workforce development
• Tackling carbon hotspots such as pharmaceuticals, energy and travel
• Commissioning and procurement
• Sustainable clinical and care models through system transformation

22
• Supporting the growth of healthy, sustainable and resilient communities
• Developing proportionate sustainabilility metrics
• Innovation, Technology and Research & Development
• Creating social value from commissioning e.g. care closer to home Our Strategy summarises our refreshed sustainability commitments, many of which have already been embedded into complimentary areas of our commissioning activities such as our Communication, Engagement & Experience Strategy and our Information Technology Strategy. Headquarters sustainability data is detailed below. Electricity 2016/17
Use kWh 151,259.2 Cost £ 16,307.04
Gas 2016/17
Use kWh 68,853.77 Cost £ 1,852.58
Water 2016/17
Use m3 1,119.75
Cost £ 3,685.71
Waste 2016/17
Clinical Use t - Cost £ -
Domestic Use t 2.12 Cost £ 802.00
Hazardous Use t - Cost £ -
Recycling Use t - Cost £ -
Confidential Use t - Cost £ -
These figures show an increase since 2015/16 because we took on responsibility for additional staff during late 2015/16 who are accommodated on a single floor in an additional building.
Improving
quality
• The NHS Constitution places a requirement on all providers of healthcare to strive to deliver high quality and safe care to patients. Commissioners of healthcare have an important role in driving quality improvement and gaining assurance around the quality of care delivered by the provider organisations that they commission.
• A Quality & Performance Report is presented monthly to our Governing Body by our Chief Nurse and our Chief of Strategy & Delivery. The report covers all NHS Constitution commitments and CCG Improvement & Assessment Framework standards, the performance of our main contracts, quality indicators, and a summary of performance against our own Delivery Plan areas. Our Quality & Performance Reports are supplemented with “Spotlight reports” on relevant areas such as safeguarding. For example, our March Governing Body meeting received a Spotlight Report on our role as a Corporate Parent to Looked After Children, noted an improvement in the quality of Initial

23
Health Assessments for Looked After Children, and agreed recommendations to improve our performance as a Corporate Parent.
• We have a Quality & Patient Safety Committee which is chaired by our Governing Body Secondary Care Doctor Member. The Committee’s remit is to monitor the quality and safety of all healthcare services commissioned by the CCG. Quality and clinical risks are reviewed and actions agreed and monitored through the Committee, and where required issues are escalated to the Governing Body through the monthly Quality & Performance Report.
• We have a nominated clinical Locality Lead for clinical quality who sits on the Quality & Patient Safety Committee and champions clinical quality, alongside the Chief Nurse, at Governing Body.
• Our Chief Nurse participates in the South Yorkshire & Bassetlaw Quality Surveillance Group, taking issues as required, and supporting effective partnership resolution.
• We have a robust Quality Assurance approach which has been set by the Quality & Patient Safety Committee and has also been considered and supported by our Audit Committee:
o Stage 1: Routine quality assurance monitoring. Each contract contains a quality schedule and reporting framework. Reports against this schedule are received through the Clinical Quality Review Group meetings held with our main providers.
o Stage 2: Routine quality assurance meetings. A range of meetings take place with providers as part of contractual arrangements where confirm and challenge to reports takes place and areas for improvement are identified.
o Stage 3: Enhanced quality assurance meetings. We have a programme of site visits and patient safety ward visits in place with our main providers. Members of the Quality & Safety Team also follow patients through various pathways, e.g. our Designated Nurse sits in Case Conferences and Team-around-the-Child Meetings.
o Stage 4: Targeted quality assurance visits. If there is insufficient assurance, risks are identified and a full risk profile developed on a specific provider. As a result of this profile, and working closely with the provider, a decision will be made on whether to undertake a targeted quality assurance visit using an appreciative enquiry approach.
• We have developed a strong relationship with the Care Quality Commission, liaising on relevant issues such as primary medical care performance and care home quality.
• We have a Primary Care Dashboard which has been recognised as good practice and shared with other CCGs, and we have developed a Primary Care Matrix & Analyst Service which General Practices can use to benchmark themselves.
• We have commissioned a range of Internal Audits, which in 2016/17 has included a review of the effectiveness of the Quality & Patient Safety Committee; all recommendations from this audit have been implemented.
• Sections 2.2.2 and 2.2.4 of this report comment on any areas of quality or performance success or risk.
Patient &
• Having high quality patient and public engagement is the key to
24
Public Involvement
unlocking many benefits for good patient experience, better value for healthcare resources and trusted relationships in the community. We recognise that good commissioning happens when patients and the public are at the heart of the decisions being made. This means that, for health services to be improved, understanding and acting on what matters to people is of the highest importance – involving them as partners to help design and commission services. It is our ambition to make sure that patients and the public can contribute to improve the quality of healthcare services and the experience of patients in Doncaster.
• We are working to achieve the following outcomes: o Better Information – Turning information and feedback into easy
to understand “Talking Points” to communicate to our public, stakeholders and communities and so trigger engagement opportunities.
o Engaged Communities – Engaging proactively with our public, stakeholders and communities (including more seldom heard communities) through a range of engagement methodologies directly influencing CCG commissioning. We aim to employ different engagement methodologies best suited to each area within our commissioning cycle: a) consultation on our strategic plans and priorities, b) engagement on how we specify outcomes, redesign pathways or services and procure services, and c) validation of the quality and performance of the services we commission.
o Experience of appropriate and responsive services – Receiving as near to real-time as possible patient experience from those accessing our commissioned services to help us check the quality of the services we commission. Emerging themes from patient experience are also embedded within our commissioning activities and transformational programmes and used as the cornerstone of engagement work moving forward.
• Patient experience is collated through our Engagement & Experience Committee, which is a Committee of the Governing Body and meets monthly. The Committee’s remit is to ensure the engagement of the public, patients and carers, the coordination of patient experience data, compliance with the public sector duties under the Equality Act and with the duties contained within the NHS Constitution. The Committee is led by our Lay Member for Patient & Public Engagement, and is supported by 2 clinical leads.
• Key highlights of our engagement work in the past year have included: o A pilot “Health Ambassador” scheme to hear the diverse voices
of some of our most vulnerable population groups. o Supporting Patient Participation Groups (PPGs) in our Member
Practices and coordinating a PPG Network to bring PPG members from across Doncaster together to share learning and input their voice to CCG commissioning.
o Working with Club Doncaster – the community arm of our local football club Doncaster Rovers – to raise awareness of cancers that we all need to get better at spotting earlier.
o Proactively disseminating information on our commissioning activities through press releases, a weekly column from our Chair in the Doncaster Free Press, a monthly InTouch Newsletter, video information and patient stories, our public
25
website, and using social media. o Evolving our patient experience dashboard which identifies
themes and trends to feed into commissioning. o We engaged formally in partnership with the other CCGs in the
Working Together collaborative partnership on the proposed changes to Hyper Acute Stroke Services and Children’s Surgery & Anaesthesia. An analysis report has been produced and will influence the final decision making.
o In the Transforming Care Partnership for Learning Disabilities in which we are an Exemplar, we have developed “Experts by Experience” – recruiting staff, co-producing the vision and plans, and sitting on the Board.
• Engagement and the use of patient experience is embedded within coversheets for Governing Body and its Committees, and within our Business Case Template.
• We use an evidence base to identify patient need including: o the Joint Strategic Needs Assessment o Specially commissioned Needs Assessment (e.g. a recent BME
Needs Assessment received by the Health & Wellbeing Board) o Patient experience collated through our Engagement &
Experience Committee – we have a patient experience tracker, meaning that we consider existing patient experience data prior to any engagement activity.
o Patient Stories and Patient Questions at the beginning of every Governing Body meeting
• We commissioned a Diagnostic of our Engagement & Communication systems during 2016, and as a result refreshed our engagement principles and prioritised engagement to improve health outcomes.
Reducing
health inequality
• There are three main routes through which we believe we can have the greatest impact on health inequalities:
o Direct commissioning of services. We commission universal healthcare services that meet the needs of all who need to use the service, as well as targeted services that meet the particular needs of specific vulnerable groups such as asylum seekers and refugees, proportionate to their health needs (this is referred to as proportionate universalism).
o Commissioning of primary medical care services. Through our Primary Care Strategic Framework we are commissioning to improve the quality of primary care by supporting a reduction in unwarranted variation in access and treatment between practices.
o System leadership in respect of the Doncaster Place Plan and the South Yorkshire & Bassetlaw Sustainability & Transformation Plan. We have embedded the need to identify and address inequalities in both these plans, and we hope to have the greatest impact by coordinating action by all local organisations.
• We contribute to the work of the Doncaster Health and Wellbeing Board including the Health and Wellbeing Strategy, and a key purpose of the Strategy is to reduce inequalities.
• We use the Joint Strategic Needs Assessment (JSNA) to inform our commissioning activities. To aid prioritisation, the Joint Strategic Needs

26
Assessment covers four areas: o How is Doncaster currently performing against the national
average? o Is Doncaster improving from past performance? o Is Doncaster narrowing the gap with the national average? o Are inequalities improving between communities in Doncaster?
The inequalities section is specifically used to track commissioning impact.
• We commission specific Health Needs Assessments where we lack data – this year we have supported the development of a refreshed Black & Minority Ethnic Needs Assessment led by Doncaster Council.
• We have developed two vision statements in our Equality & Diversity Strategy, which has been refreshed in-year: a) Hear a diverse range of Doncaster voices and use equality data to help us to commission effective services that meet identified health needs and reduce health inequalities, and b) Ensure that we pay due regard to our Public Sector Equality Duties and equal opportunities within employment.
• Our Equality & Diversity Strategy now includes our approach to identifying and tackling wider health inequalities – we are working in partnership with statutory organisations across Doncaster as part of a Health Inequalities Working Group within the Team Doncaster structure.
• We use health inequality information to complete equality analysis of our commissioning activities.
• Every year we publish our annual summary of our approach to inequalities.
• Well North is a collaborative programme which is developing, testing and piloting a set of linked interventions to improve the health of the poorest, fastest, in some of the most deprived areas of the North of England. Doncaster is one of the pilot sites for Well North (locally – Well Doncaster), and Denaby is the pilot area. We are a key member of Well Doncaster and our Chief of Partnership Commissioning and Primary Care has been closely working with the development team since its inception.
• We developing and performance managing Delivery Plans in our key outcome areas that aim to reduce health inequalities.
• We are a member of the Inclusion & Fairness Forum which has been set up by Team Doncaster as an independent advisory group to explore and identify ways in which we can make Doncaster a fairer place to live and work.
Health & Wellbeing Strategy
• Doncaster’s Health & Wellbeing Board aims to improve health and wellbeing for the residents of Doncaster and reduce inequalities in health outcomes. The Board commissions and approves the Joint Strategic Needs Assessment (JSNA), commissions and approves the Joint Health and Wellbeing Strategy, approves and oversees the Better Care Fund, sets the health and social care commissioning framework, is the focal point for health and wellbeing decision making, and drives collaboration, integration and joint commissioning. We are represented on the Board by both our Chair and our Chief Officer. In the past year
our Chair has been nominated as the Vice Chair of the Health & Wellbeing Board.
• The Health & Wellbeing Strategy identified 4 key themes for
27
development to improve health and wellbeing outcomes in Doncaster. The CCG’s priorities align well to the above areas, and we are working closely with partner organisations to deliver improvements. areas:
o Wellbeing: whether this is social and emotional wellbeing, economic wellbeing, environmental wellbeing, educational wellbeing or physical health. We have invested in a Social Prescribing scheme to support the wider social issues affecting health, and we have embedded a wellbeing approach into our mental health commissioning plans.
o Health and Social Care Transformation: embedding person centred integrated care to support independence, to ensure personalised and flexible care when people are in need of support to stay healthy and independent, and to ensure efficient and effective services are available when people are in urgent need or crisis. The community nursing services which we have commissioned take a holistic approach to care.
o Five Areas of Focus: Substance Misuse (Drugs and Alcohol), Obesity, Families, Dementia, Mental Health.
o Reducing Health Inequalities: working together to improve wellbeing and quality of life for everyone, whether inequalities are socio-economic, related to lifestyle and health behaviours, in access to services, or in health outcomes.
• We have worked closely with the Health & Wellbeing Board throughout the year, and so our annual report is a true reflection of the activity we have already reported to the Board. We have additionally provided the Chair of the Health & Wellbeing Board with a copy of our draft annual report for comment and no issues were raised.

28
ACCOUNTABILITY REPORT
Mrs Jackie Pederson Accountable Officer 25 May 2017

29
1. Corporate Governance Report
1.1. Members Report 1.1.1. Member profiles Throughout the financial year and up to the signing of the Annual Report and Accounts, our Chair was Dr David Crichton and our Chief Officer was Mrs Jackie Pederson. Our Senior Manager Team comprises five Chiefs of Service – Chief of Strategy & Delivery, Chief Nurse, Chief of Partnership Commissioning & Primary Care, and Chief of Corporate Services. 1.1.2. Member Practices The following 43 General Practices comprise our CCG Member Practices: North West Locality (11)
• Scawsby Health Centre
• The Ransome Practice
• Bentley Surgery
• Dr. Sheikh’s Surgery
• Petersgate Medical Centre
• The Nelson Practice
• The Lakeside Practice
• Princess Medical Centre
• The Askern Medical Practice
• Conisbrough Medical Practice
• Carcroft Doctors Group
South West Locality (10)
• The Conisbrough Group Practice
• Park View Surgery
• Barnburgh Surgery
• The New Surgery
• Mexborough Health Centre
• Church View Surgery
• The Scott Practice
• St. John’s Group Practice
• Dr. Zaidi & Partners
• The Nayar Practice
Central Locality (8)
• The Mount Group Practice
• Regent Square Group Practice
• The Burns Medical Practice
• Kingthorne Group Practice
• St. Vincent Medical Centre
• The Flying Scotsman Health Centre
• The Sandringham Practice
• The Oakwood Surgery
North East Locality (5)
• Field Road Surgery
• Northfield Surgery
• Hatfield Health Centre
• Dunsville Medical Centre
• Thorne Moor Practice
South East Locality (9)
• The Mayflower Medical Practice
• The Rossington Practice
• Tickhill & Colliery Medical Practice
• The Phoenix Medical Practice
• West End Clinic
• The Medical Centre
• Auckley Surgery
• Whitehouse Farm Medical Centre
• The Village Practice

30
1.1.3. Composition of Governing Body Our Governing Body comprised 18 formal members throughout the financial year 2016/17. Other named attendees who are formally in attendance at the meeting but without voting rights are also listed below. Members Name Chair Dr. David Crichton 2 x North East Locality elected GPs Dr. Andrew Oakford (to 06/04/17)
Dr. Jeremy Bradley 2 x North West Locality elected GPs Dr. Niki Seddon
Dr. Marco Pieri 2 x Central Locality elected GPs Dr. Sam Feeney } (To 31/08/16)
Dr Nick Tupper } (From 01/09/16)
Vacancy 2 x South East Locality elected GPs Dr. Pat Barbour
Dr Khaimraj Singh 2 x South West Locality elected GPs Dr. Lindsey Britten
Dr. Karen Wagstaff Lay Member – Audit & Governance Miss Anthea Morris Lay Member – Public & Patient Engagement Mrs Sarah Whittle (From 01/09/16) Lay Member – Primary Care Commissioning Mrs Linda Tully Chief Officer Mrs Jackie Pederson Chief Finance Officer Mrs Hayley Tingle Registered Nurse Mrs Mary Shepherd (To 31/08/16)
Mr Andrew Russell (From 01/09/16) Secondary Care Doctor Dr Emyr Wyn Jones Attendees Name Chief of Strategy & Delivery Mr Anthony Fitzgerald (From 01/08/16) Chief of Corporate Services Mrs Sarah Atkins Whatley Chief of Partnership Commissioning & Primary Care
Mrs Laura Sherburn
Local Authority representative Ms Kim Curry Public Health representative Dr Rupert Suckling Healthwatch Doncaster representative Mr Steven Shore 1.1.4. Committee(s), including Audit Committee NHS Doncaster CCG’s Audit Committee comprises the following Members
• Lay Member – Audit & Governance (Chair)
• Lay Member – Public & Patient Engagement
• Locality Leads x2
• Governing Body Secondary Care Doctor The Audit Committee includes the following attendees:
• Chief Finance Officer
• External Audit representative
• Internal Audit representative

31
• NHS Protect (Counter Fraud) representative
• Chief of Corporate Services / Group Secretary Please refer to our Remuneration Report for details of the membership of the Remuneration Committee, and to the Governance Statement for details of and membership of all other Governing Body and Membership Body Committees. 1.1.5. Register of Interests Our Declarations of Interest Register is available on our website: http://www.doncasterccg.nhs.uk/about-us/public-information/publications-scheme/lists-and-registers/ We achieved full compliance in our Conflicts of Interest Internal Audit.
1.1.6. Personal data related incidents We had no Serious Untoward Incidents relating to data security breaches, and none that were reported to the Information Commissioner. 1.1.7. Statement of Disclosure to Auditors Each individual who is a member of the CCG at the time the Members’ Report is approved confirms:
• so far as the member is aware, there is no relevant audit information of which the CCG’s auditor is unaware that would be relevant for the purposes of their audit report
• the member has taken all the steps that they ought to have taken in order to make him or herself aware of any relevant audit information and to establish that the CCG’s auditor is aware of it.
1.1.8. Modern Slavery Act NHS Doncaster CCG fully supports the Government’s objectives to eradicate modern slavery and human trafficking but does not meet the requirements for producing an annual Slavery and Human Trafficking Statement as set out in the Modern Slavery Act 2015.
32
1.2. Statement of Accountable Officer’s Responsibilities The National Health Service Act 2006 (as amended) states that each Clinical Commissioning Group shall have an Accountable Officer and that Officer shall be appointed by the NHS Commissioning Board (NHS England). NHS England has appointed the Chief Officer to be the Accountable Officer of NHS Doncaster CCG. The responsibilities of an Accountable Officer are set out under the National Health Service Act 2006 (as amended), Managing Public Money and in the Clinical Commissioning Group Accountable Officer Appointment Letter. They include responsibilities for:
• The propriety and regularity of the public finances for which the Accountable Officer is answerable,
• For keeping proper accounting records (which disclose with reasonable accuracy at any time the financial position of the Clinical Commissioning Group and enable them to ensure that the accounts comply with the requirements of the Accounts Direction),
• For safeguarding the Clinical Commissioning Group’s assets (and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities).
• The relevant responsibilities of accounting officers under Managing Public Money,
• Ensuring the CCG exercises its functions effectively, efficiently and economically (in accordance with Section 14Q of the National Health Service Act 2006 (as amended)) and with a view to securing continuous improvement in the quality of services (in accordance with Section14R of the National Health Service Act 2006 (as amended)),
• Ensuring that the CCG complies with its financial duties under Sections 223H to 223J of the National Health Service Act 2006 (as amended).
Under the National Health Service Act 2006 (as amended), NHS England has directed each Clinical Commissioning Group to prepare for each financial year financial statements in the form and on the basis set out in the Accounts Direction. The financial statements are prepared on an accruals basis and must give a true and fair view of the state of affairs of the Clinical Commissioning Group and of its net expenditure, changes in taxpayers’ equity and cash flows for the financial year. In preparing the financial statements, the Accountable Officer is required to comply with the requirements of the Group Accounting Manual issued by the Department of Health and in particular to:
• Observe the Accounts Direction issued by NHS England, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis;
• Make judgements and estimates on a reasonable basis;
• State whether applicable accounting standards as set out in the Group Accounting Manual issued by the Department of Health have been followed, and disclose and explain any material departures in the financial statements; and,
• Prepare the financial statements on a going concern basis.
33
To the best of my knowledge and belief, I have properly discharged the responsibilities set out under the National Health Service Act 2006 (as amended), Managing Public Money and in my Clinical Commissioning Group Accountable Officer Appointment Letter. I also confirm that:
• as far as I am aware, there is no relevant audit information of which the CCG’s auditors are unaware, and that as Accountable Officer, I have taken all the steps that I ought to have taken to make myself aware of any relevant audit information and to establish that the CCG’s auditors are aware of that information.
• that the annual report and accounts as a whole is fair, balanced and understandable and that I take personal responsibility for the annual report and accounts and the judgments required for determining that it is fair, balanced and understandable

34
1.3. Governance Statement Introduction and context NHS Doncaster CCG is a body corporate established by NHS England on 1 April 2013 under the National Health Service Act 2006 (as amended). The clinical commissioning group’s statutory functions are set out under the National Health Service Act 2006 (as amended). The CCG’s general function is arranging the provision of services for persons for the purposes of the health service in England. The CCG is, in particular, required to arrange for the provision of certain health services to such extent as it considers necessary to meet the reasonable requirements of its local population. As at 1 April 2016, the clinical commissioning group is not subject to any directions from NHS England issued under Section 14Z21 of the National Health Service Act 2006. Scope of responsibility As Accountable Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of the clinical commissioning group’s policies, aims and objectives, whilst safeguarding the public funds and assets for which I am personally responsible, in accordance with the responsibilities assigned to me in Managing Public Money. I also acknowledge my responsibilities as set out under the National Health Service Act 2006 (as amended) and in my Clinical Commissioning Group Accountable Officer Appointment Letter. I am responsible for ensuring that the clinical commissioning group is administered prudently and economically and that resources are applied efficiently and effectively, safeguarding financial propriety and regularity. I also have responsibility for reviewing the effectiveness of the system of internal control within the clinical commissioning group as set out in this governance statement. Governance arrangements and effectiveness The main function of the Governing Body is to ensure that the group has made appropriate arrangements for ensuring that it exercises its functions effectively, efficiently and economically and complies with such generally accepted principles of good governance as are relevant to it. Our governance meeting structure is headed by our Governing Body which has responsibility to undertake the roles and responsibilities as delegated through the Constitution signed by the 43 Member Practices which constitute the clinical commissioning group. The Governing Body is supported in fulfilling its functions by Committees of the Governing Body as detailed overleaf. The table which follows this diagram details the function of each of these Committees, performance / highlights, composition and attendance (including nominated deputies).

35

36
Our Member Practices are grouped into 5 Localities and regular Locality Meetings, led by Locality Leads and attended by nominated Practice Representatives from each Member Practice, are held in each Locality to ensure engagement of Member Practices in the work of their Governing Body and to hold the Governing Body to account. Our Membership have reserved to themselves a number of matters including Constitutional amendments, appointing Locality Leads as clinical leaders who represent their views on the Governing Body, and agreeing the vision, values and overall strategic direction of the Group. Any concerns are raised via Locality Leads, and if unresolved via a Constitutional dispute process.
Governing Body Function:
The Governing Body has the following functions conferred on it by sections 14L(2) and (3) of the 2006 NHS Act, inserted by section 25 the 2012 Health & Social Care Act, together with any other functions connected with its main functions as may be specified in regulations or in our Constitution. The Governing Body has responsibility for:
• ensuring that the Group has appropriate arrangements in place to exercise its functions effectively, efficiently and economically and in accordance with the Groups principles of good governance (its main function);
• determining the remuneration, fees and other allowances payable to employees or other persons providing services to the Group and the allowances payable under any pension scheme it may establish under paragraph 11(4) of Schedule 1A of the 2006 Act, inserted by Schedule 2 of the 2012 Act;
• approving any functions of the Group that are specified in regulations;
• approving commissioning plans;
• monitoring performance against plans and taking action to address performance issues through appropriate routes including contractual routes for areas of commissioning responsibility as required;
• providing assurance of strategic risk through the Assurance Framework and putting into place action plans to mitigate risk above the agreed risk tolerance threshold as required;
• establishing further Committees and Sub Committees to support the delivery of delegated functions.
Assurance:
The Governing Body has met twelve times during the year, and was quorate at each meeting. An Extraordinary meeting was held on 26 May 2016 to agree the Annual Accounts. The Governing Body approves our organisational strategy and key strategic documents, and receives regular assurance reports including a monthly Quality & Performance Report with “spotlight” reports on key areas, a monthly finance report, and quarterly it receives the Assurance Framework and a Corporate Assurance Report. Corporate governance and risk management activity through the Governing Body and its strategic Committees is captured in the quarterly Corporate Assurance Reports received by both the Audit Committee and the Governing Body. The Governing Body commissioned external support during late 2016 to support a review of effectiveness.
Membership and attendance: Role Name Attendance Chair Dr David Crichton 91.7%
Locality Lead – North East Locality Dr Andrew Oakford 91.7%
Locality Lead – North East Locality Dr Jeremy Bradley 91.7%
Locality Lead – North West Locality Dr Niki Seddon 75.0%
Locality Lead – North West Locality Dr Marco Pieri 83.3%
Locality Lead – Central Locality Dr Sam Feeney (To 31/08/16) 80.0% Dr Nick Tupper (From 01/09/16) 85.7%
Locality Lead – Central Locality Vacancy N/A
Locality Lead – South East Locality Dr Pat Barbour 91.7%
Locality Lead – South East Locality Dr Khaimraj Singh 83.3%
Locality Lead – South West Locality Dr Lindsey Britten 75.0%
Locality Lead – South West Locality Dr Karen Wagstaff 91.7% Lay Member – Audit & Governance Miss Anthea Morris 91.7%
Lay Member – Patient & Public Engagement Mrs Linda Tully (To 31/08/16 – dual role) 100%

37
Mrs Sarah Whittle (From 01/09/16) 85.7%
Lay Member – Primary Care Commissioning Mrs Linda Tully (as above: dual role to 31/08/16) 91.7%
Registered Nurse Mrs Mary Shepherd (To 31/08/16) 50.0% Mr Andrew Russell (From 01/09/16) 85.7%
Secondary Care Specialist Doctor Dr Emyr Wyn Jones 91.7%
Accountable Officer Mrs Jackie Pederson 91.7%
Chief Finance Officer Mrs Hayley Tingle 91.7%
Audit Committee Function:
Chaired by the Lay Member for Audit & Governance, the Audit Committee has delegated responsibility from the Governing Body for oversight of integrated governance, risk management and internal control, internal audit, external audit, reviewing the findings of other significant assurance functions, counter fraud and financial reporting.
Performance / highlights:
The Committee is required to meet formally at least five times a year. The Committee met six times in 2016/17. Attendance records demonstrate that the Committee was quorate at each meeting (minimum of 2 members).
Performance / highlights:
• Review of Annual Accounts.
• Programme of Internal Audits from our Internal Audit Service, 360 Assurance, alongside a Counter Fraud work programme and Counter Fraud Self Review Tool (SRT) assessment.
• Review of Standing Orders, Scheme of Delegation and Standing Financial Instructions.
• Review of the quarterly Corporate Assurance Report, Assurance Framework and associated “deep dive” report, the Probity Register, and Financial Governance report.
• Annual review of the Risk Register.
• A Corporate Governance Management Group to support the Committee in operational aspects of corporate assurance.
• Approved a refreshed Business Continuity Management Policy & Plan, refreshed Fraud Corruption & Bribery Policy, refreshed Whistleblowing Policy, refreshed Freedom of Information Policy and refreshed Information Governance Strategy & Policy.
• Committee effectiveness self-assessment.
Membership and attendance: Role Name Attendance
Lay Member – Audit & Governance (Chair) Miss Anthea Morris 100%
Lay Member – Patient & Public Engagement Mrs Linda Tully (To 31/08/16) 33.3%
Mrs Sarah Whittle (From 01/09/16) 66.6%
Locality Lead Dr Karen Wagstaff 83.0%
Locality Lead Dr Andrew Oakford 100% Secondary Care Specialist Doctor Dr Emyr Wyn Jones 66.6%
Remuneration Committee Function:
Chaired by the Lay Member for Audit & Governance, the Remuneration Committee has delegated responsibility from the Governing Body for advising the Governing Body on all aspects of salary not covered by Agenda for Change, arrangements for termination of employment, remuneration, allowances and terms of service of senior managers covered by the Very Senior Managers pay framework, and for approving strategic human resources policies and procedures.
Performance / highlights:
The Committee is required to meet formally at least once a year. The Committee met twice in 2016/17. Attendance records demonstrate that the Committee was quorate at each meeting (minimum of 2 members).
Performance / highlights:
• Consideration of Chief Officer remuneration in line with a new appointment in April 2017, and Chief Finance Officer remuneration as the identified Deputy Chief Officer.
• Application of nationally agreed cost of living rises.
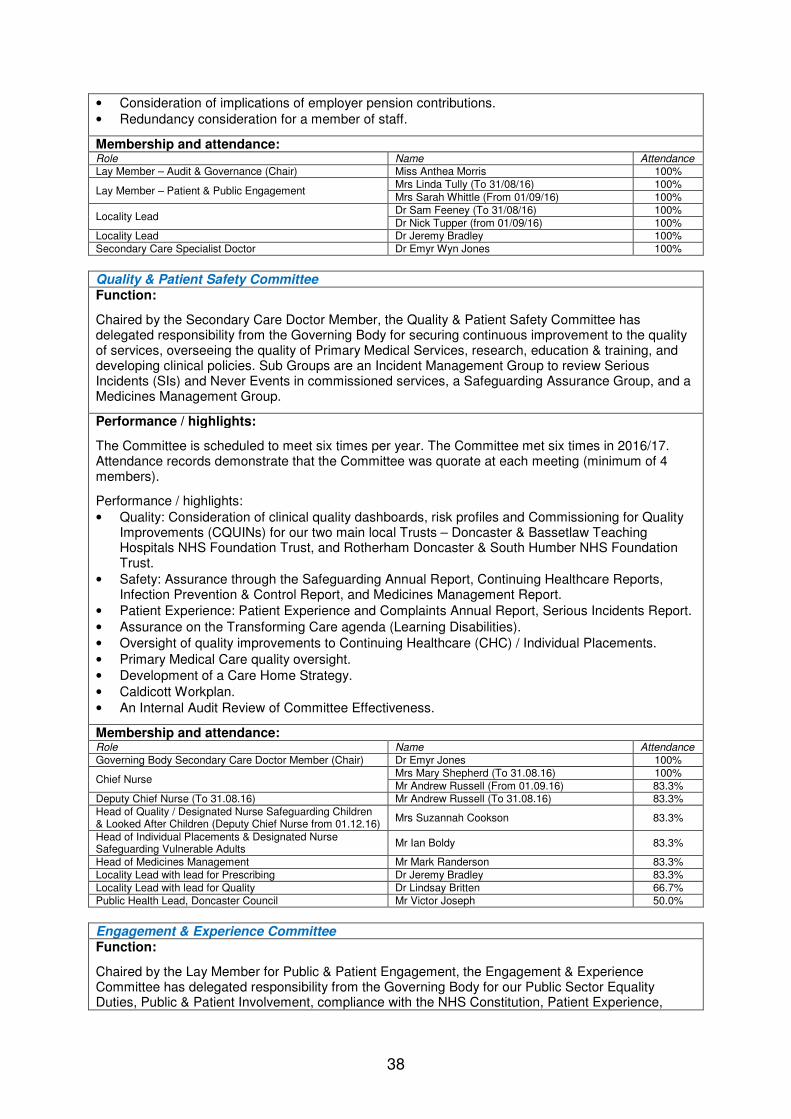
38
• Consideration of implications of employer pension contributions.
• Redundancy consideration for a member of staff.
Membership and attendance: Role Name Attendance Lay Member – Audit & Governance (Chair) Miss Anthea Morris 100%
Lay Member – Patient & Public Engagement Mrs Linda Tully (To 31/08/16) 100%
Mrs Sarah Whittle (From 01/09/16) 100%
Locality Lead Dr Sam Feeney (To 31/08/16) 100%
Dr Nick Tupper (from 01/09/16) 100% Locality Lead Dr Jeremy Bradley 100%
Secondary Care Specialist Doctor Dr Emyr Wyn Jones 100%
Quality & Patient Safety Committee Function:
Chaired by the Secondary Care Doctor Member, the Quality & Patient Safety Committee has delegated responsibility from the Governing Body for securing continuous improvement to the quality of services, overseeing the quality of Primary Medical Services, research, education & training, and developing clinical policies. Sub Groups are an Incident Management Group to review Serious Incidents (SIs) and Never Events in commissioned services, a Safeguarding Assurance Group, and a Medicines Management Group.
Performance / highlights:
The Committee is scheduled to meet six times per year. The Committee met six times in 2016/17. Attendance records demonstrate that the Committee was quorate at each meeting (minimum of 4 members).
Performance / highlights:
• Quality: Consideration of clinical quality dashboards, risk profiles and Commissioning for Quality Improvements (CQUINs) for our two main local Trusts – Doncaster & Bassetlaw Teaching Hospitals NHS Foundation Trust, and Rotherham Doncaster & South Humber NHS Foundation Trust.
• Safety: Assurance through the Safeguarding Annual Report, Continuing Healthcare Reports, Infection Prevention & Control Report, and Medicines Management Report.
• Patient Experience: Patient Experience and Complaints Annual Report, Serious Incidents Report.
• Assurance on the Transforming Care agenda (Learning Disabilities).
• Oversight of quality improvements to Continuing Healthcare (CHC) / Individual Placements.
• Primary Medical Care quality oversight.
• Development of a Care Home Strategy.
• Caldicott Workplan.
• An Internal Audit Review of Committee Effectiveness.
Membership and attendance: Role Name Attendance
Governing Body Secondary Care Doctor Member (Chair) Dr Emyr Jones 100%
Chief Nurse Mrs Mary Shepherd (To 31.08.16) 100%
Mr Andrew Russell (From 01.09.16) 83.3% Deputy Chief Nurse (To 31.08.16) Mr Andrew Russell (To 31.08.16) 83.3%
Head of Quality / Designated Nurse Safeguarding Children & Looked After Children (Deputy Chief Nurse from 01.12.16)
Mrs Suzannah Cookson 83.3%
Head of Individual Placements & Designated Nurse Safeguarding Vulnerable Adults
Mr Ian Boldy 83.3%
Head of Medicines Management Mr Mark Randerson 83.3%
Locality Lead with lead for Prescribing Dr Jeremy Bradley 83.3%
Locality Lead with lead for Quality Dr Lindsay Britten 66.7%
Public Health Lead, Doncaster Council Mr Victor Joseph 50.0%
Engagement & Experience Committee Function:
Chaired by the Lay Member for Public & Patient Engagement, the Engagement & Experience Committee has delegated responsibility from the Governing Body for our Public Sector Equality Duties, Public & Patient Involvement, compliance with the NHS Constitution, Patient Experience,
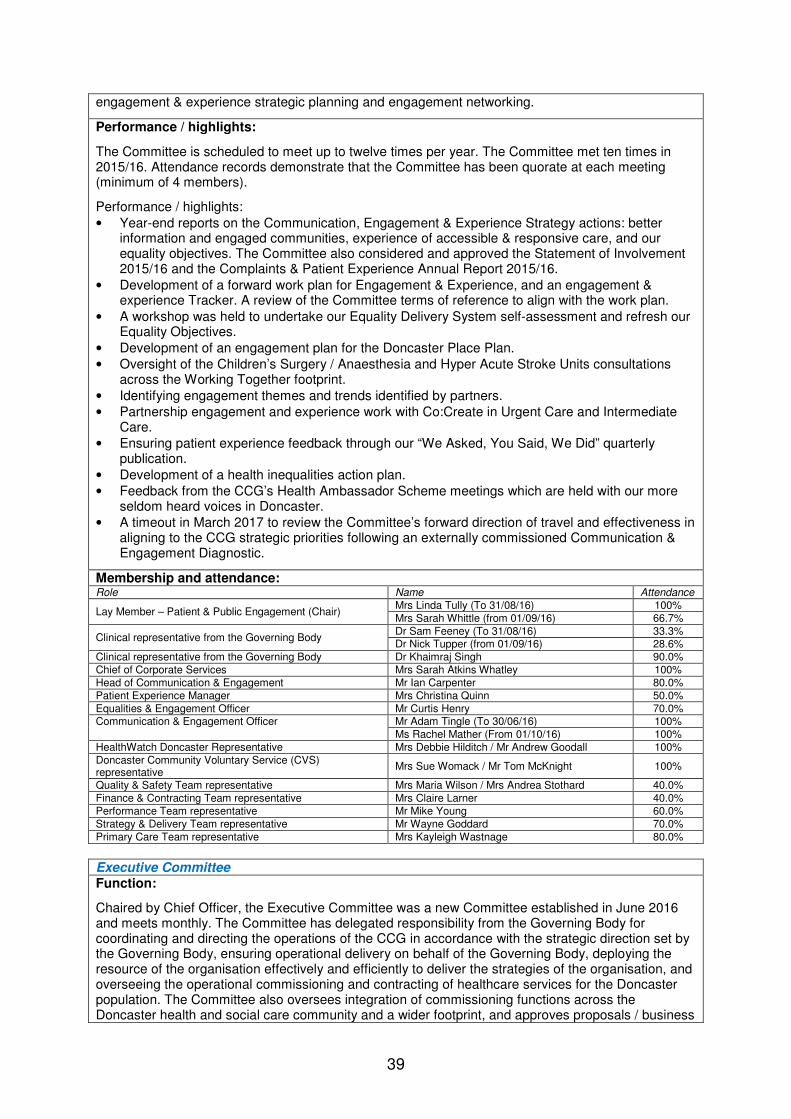
39
engagement & experience strategic planning and engagement networking.
Performance / highlights:
The Committee is scheduled to meet up to twelve times per year. The Committee met ten times in 2015/16. Attendance records demonstrate that the Committee has been quorate at each meeting (minimum of 4 members).
Performance / highlights:
• Year-end reports on the Communication, Engagement & Experience Strategy actions: better information and engaged communities, experience of accessible & responsive care, and our equality objectives. The Committee also considered and approved the Statement of Involvement 2015/16 and the Complaints & Patient Experience Annual Report 2015/16.
• Development of a forward work plan for Engagement & Experience, and an engagement & experience Tracker. A review of the Committee terms of reference to align with the work plan.
• A workshop was held to undertake our Equality Delivery System self-assessment and refresh our Equality Objectives.
• Development of an engagement plan for the Doncaster Place Plan.
• Oversight of the Children’s Surgery / Anaesthesia and Hyper Acute Stroke Units consultations across the Working Together footprint.
• Identifying engagement themes and trends identified by partners.
• Partnership engagement and experience work with Co:Create in Urgent Care and Intermediate Care.
• Ensuring patient experience feedback through our “We Asked, You Said, We Did” quarterly publication.
• Development of a health inequalities action plan.
• Feedback from the CCG’s Health Ambassador Scheme meetings which are held with our more seldom heard voices in Doncaster.
• A timeout in March 2017 to review the Committee’s forward direction of travel and effectiveness in aligning to the CCG strategic priorities following an externally commissioned Communication & Engagement Diagnostic.
Membership and attendance: Role Name Attendance
Lay Member – Patient & Public Engagement (Chair) Mrs Linda Tully (To 31/08/16) 100%
Mrs Sarah Whittle (from 01/09/16) 66.7%
Clinical representative from the Governing Body Dr Sam Feeney (To 31/08/16) 33.3% Dr Nick Tupper (from 01/09/16) 28.6%
Clinical representative from the Governing Body Dr Khaimraj Singh 90.0%
Chief of Corporate Services Mrs Sarah Atkins Whatley 100%
Head of Communication & Engagement Mr Ian Carpenter 80.0%
Patient Experience Manager Mrs Christina Quinn 50.0%
Equalities & Engagement Officer Mr Curtis Henry 70.0% Communication & Engagement Officer Mr Adam Tingle (To 30/06/16) 100%
Ms Rachel Mather (From 01/10/16) 100%
HealthWatch Doncaster Representative Mrs Debbie Hilditch / Mr Andrew Goodall 100%
Doncaster Community Voluntary Service (CVS) representative
Mrs Sue Womack / Mr Tom McKnight 100%
Quality & Safety Team representative Mrs Maria Wilson / Mrs Andrea Stothard 40.0%
Finance & Contracting Team representative Mrs Claire Larner 40.0%
Performance Team representative Mr Mike Young 60.0%
Strategy & Delivery Team representative Mr Wayne Goddard 70.0%
Primary Care Team representative Mrs Kayleigh Wastnage 80.0%
Executive Committee Function:
Chaired by Chief Officer, the Executive Committee was a new Committee established in June 2016 and meets monthly. The Committee has delegated responsibility from the Governing Body for coordinating and directing the operations of the CCG in accordance with the strategic direction set by the Governing Body, ensuring operational delivery on behalf of the Governing Body, deploying the resource of the organisation effectively and efficiently to deliver the strategies of the organisation, and overseeing the operational commissioning and contracting of healthcare services for the Doncaster population. The Committee also oversees integration of commissioning functions across the Doncaster health and social care community and a wider footprint, and approves proposals / business
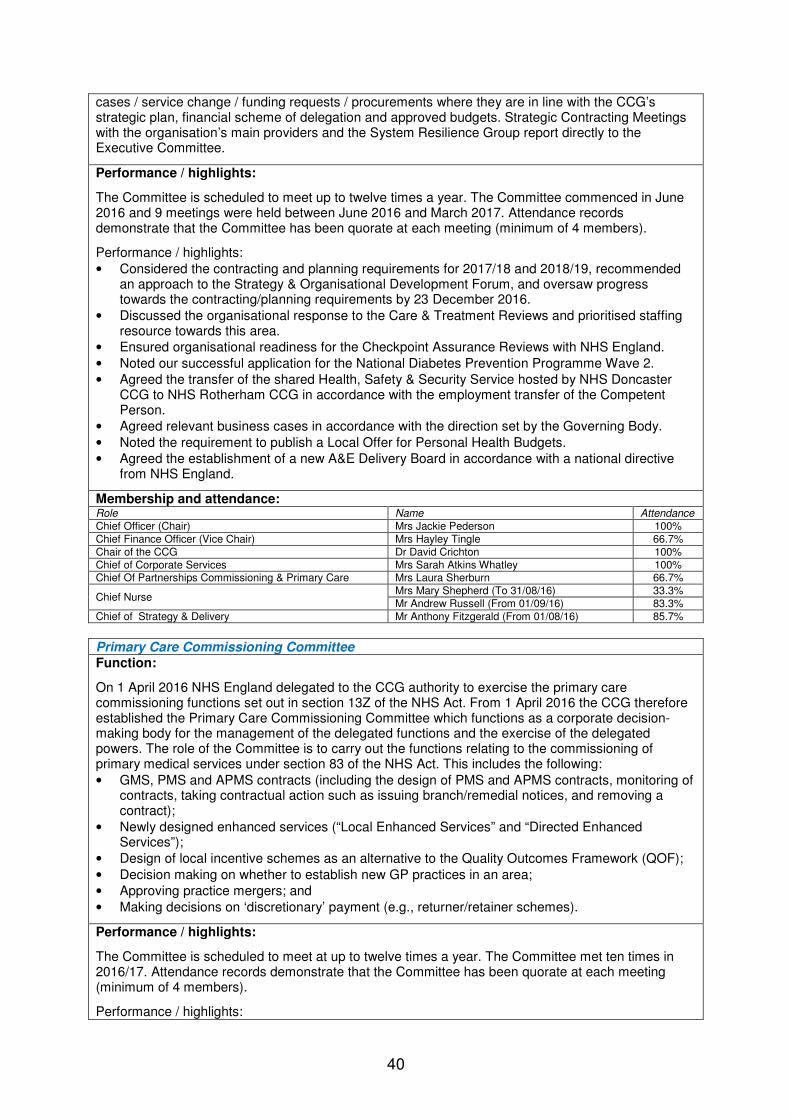
40
cases / service change / funding requests / procurements where they are in line with the CCG’s strategic plan, financial scheme of delegation and approved budgets. Strategic Contracting Meetings with the organisation’s main providers and the System Resilience Group report directly to the Executive Committee.
Performance / highlights:
The Committee is scheduled to meet up to twelve times a year. The Committee commenced in June 2016 and 9 meetings were held between June 2016 and March 2017. Attendance records demonstrate that the Committee has been quorate at each meeting (minimum of 4 members).
Performance / highlights:
• Considered the contracting and planning requirements for 2017/18 and 2018/19, recommended an approach to the Strategy & Organisational Development Forum, and oversaw progress towards the contracting/planning requirements by 23 December 2016.
• Discussed the organisational response to the Care & Treatment Reviews and prioritised staffing resource towards this area.
• Ensured organisational readiness for the Checkpoint Assurance Reviews with NHS England.
• Noted our successful application for the National Diabetes Prevention Programme Wave 2.
• Agreed the transfer of the shared Health, Safety & Security Service hosted by NHS Doncaster CCG to NHS Rotherham CCG in accordance with the employment transfer of the Competent Person.
• Agreed relevant business cases in accordance with the direction set by the Governing Body.
• Noted the requirement to publish a Local Offer for Personal Health Budgets.
• Agreed the establishment of a new A&E Delivery Board in accordance with a national directive from NHS England.
Membership and attendance: Role Name Attendance
Chief Officer (Chair) Mrs Jackie Pederson 100%
Chief Finance Officer (Vice Chair) Mrs Hayley Tingle 66.7%
Chair of the CCG Dr David Crichton 100%
Chief of Corporate Services Mrs Sarah Atkins Whatley 100% Chief Of Partnerships Commissioning & Primary Care Mrs Laura Sherburn 66.7%
Chief Nurse Mrs Mary Shepherd (To 31/08/16) 33.3%
Mr Andrew Russell (From 01/09/16) 83.3%
Chief of Strategy & Delivery Mr Anthony Fitzgerald (From 01/08/16) 85.7%
Primary Care Commissioning Committee Function:
On 1 April 2016 NHS England delegated to the CCG authority to exercise the primary care commissioning functions set out in section 13Z of the NHS Act. From 1 April 2016 the CCG therefore established the Primary Care Commissioning Committee which functions as a corporate decision-making body for the management of the delegated functions and the exercise of the delegated powers. The role of the Committee is to carry out the functions relating to the commissioning of primary medical services under section 83 of the NHS Act. This includes the following:
• GMS, PMS and APMS contracts (including the design of PMS and APMS contracts, monitoring of contracts, taking contractual action such as issuing branch/remedial notices, and removing a contract);
• Newly designed enhanced services (“Local Enhanced Services” and “Directed Enhanced Services”);
• Design of local incentive schemes as an alternative to the Quality Outcomes Framework (QOF);
• Decision making on whether to establish new GP practices in an area;
• Approving practice mergers; and
• Making decisions on ‘discretionary’ payment (e.g., returner/retainer schemes).
Performance / highlights:
The Committee is scheduled to meet at up to twelve times a year. The Committee met ten times in 2016/17. Attendance records demonstrate that the Committee has been quorate at each meeting (minimum of 4 members).
Performance / highlights:

41
• Noted the terms of reference delegated by NHS England and populated the list of members with named individuals.
• Received updates on the Primary Care Strategic Model and shaped the development of a specification for the first “pillar” of the strategy – proactive coordinated primary care. Oversaw mobilisation plans for the Extended Primary Care Pillar, and the Keeping Well Pillar.
• Approved a Primary Care Quality Assurance Strategy.
• Considered a primary care stakeholder engagement plan.
• Considered and approved investment proposals for allocating transforming primary care funding and for allocating capital/IT investment.
• Considered approaches to transforming prescribing, and subsequently approved a primary care gain share prescribing scheme launched during summer 2016.
• Approved a proposal for a phased reduction and re-allocation of PMS premiums, and an approach to PMS uplifts.
• Agreed the Draft Contingency Planning document for contract termination in General Practice and developed a programme of support to Practices which could potentially be classed as vulnerable.
• Considered and advised on a proposed practice merger business case in terms of IT, estates requirements and patient consultation.
• Considered the GP Forward View Implementation Plan, and agreed recommendations and the process for developing the transactional detail.
• Received minutes from the Primary Care Management Group and the Primary Care Provider Engagement Group.
• Received an Internal Audit report on Primary Care Commissioning Committee governance. Any recommendations made by Internal Audit have been addressed and as a result the Committee is now fully compliant with the recommendations.
Membership and attendance: Role Name Attendance
Chair – Lay Member Primary Care Commissioning Mrs Linda Tully 90.0% Vice Chair – Lay Member Audit & Governance Miss Anthea Morris (To 31/08/16) 80%
Vice Chair – Lay Member Patient & Public Engagement Mrs Sarah Whittle (From 01/09/16 100%
Chief Finance Officer Mrs Hayley Tingle 90.0%
Chief Officer Mrs Jackie Pederson 70.0%
Chief of Partnerships Commissioning & Primary Care Mrs Laura Sherburn 100%
Locality Lead Dr Niki Seddon 80.0% Locality Lead Dr Pat Barbour 80.0%
Primary Care Contract Manager, NHS England Mrs Carolyn Ogle 90.0%
Other Forums Function:
In addition to these formal meetings, we have included in our meeting structure two non-decision-making forums:
• Strategy & Organisational Development Forum
• Clinical Reference Group
Chaired by the Chair of the Governing Body, the Strategy & Organisational Development Forum is a monthly non-decision-making forum which serves as a debate and strategic intelligence sharing forum for Governing Body members on key organisational issues such as intelligence gathering and planning timeout sessions for the development of our strategic commissioning intentions, reviewing Organisational Development (OD) priorities, and considering partnership networking opportunities. Performance / highlights have included confirm and challenge on performance against Delivery Plans, consideration of proposed commissioning models, engagement in the annual planning rounds, and debates on key development areas such as Continuing Healthcare, Unplanned Care, Integrated Commissioning, and Intermediate Care.
Chaired by the Secondary Care Doctor Member from the Governing Body, the Clinical Reference Group is a bi-monthly clinical non-decision-making forum which aims to provide strong clinical leadership to commissioning debate and discussion. The group facilitates clinical dialogue and leadership across primary/community/secondary care, developing productive working relationships with wider clinical colleagues to ensure multidisciplinary input, advice and guidance on commissioning developments from the very beginning of clinical strategy development and service/care pathway redesigns and procurements. The Group stimulates, challenges and proposes innovative solutions to

42
transformation and service/care pathway improvements in order to improve outcomes for patients.
In terms of joint commissioning arrangements, we have joined with other local Clinical Commissioning Groups for the CCG collaborative arrangements known as Working Together and we have a Memorandum of Understanding to support this arrangement; the Joint Committee will be formally established and meeting in public from April 2017. In the future, we also aim to develop a Joint Committee for joint commissioning of 999 and 111 services. We are committed to working with local partners and ensure the establishment of robust governance arrangements that place emphasis on integrated working and mutual accountability through:
• Membership of the Health and Wellbeing Board;
• Joint Commissioning arrangements with the Local Authority;
• Joint commissioning and partnership work with other local Clinical Commissioning Groups;
• Our relationship with Clinical Networks.
UK Corporate Governance Code NHS Bodies are not required to comply with the UK Code of Corporate Governance. However, we reflect on our Corporate Governance arrangements by drawing upon best practice available, including those aspects of the UK Corporate Governance Code we consider to be relevant to the CCG and best practice.
Leadership
Our organisation is headed by an effective unitary Governing Body comprising Clinical, Lay and Executive Members plus other attendees. The Governing Body has a clear delegation of responsibilities to its strategic Committees and its Officers, a clear process for decision-making, and a Chair responsible for leadership of the Governing Body. Members of the Governing Body constructively challenge assurance and support the development of proposals on strategy. The Governing Body has approved a refreshed Organisational Development Strategy during 2016/17 and has invested in organisational development programmes.
Effectiveness
Our organisation is comprised of a range of individuals with a range of skills, experience and knowledge. There is a formal process for appointments as described in our Constitution, and by election for those roles subject to elections (Locality Leads and Clinical Chair). The time commitment of members is reviewed by their line manager, and flexed to take account of any changing organisational needs. Induction and training is provided based on individual needs of Governing Body members, who are also subject to mandatory/statutory training requirements. The Governing Body is provided with a range of strategic information covering quality, finance, performance, strategy, policy and risk at the monthly meetings. Governing Body performance is subject to annual evaluation via the Annual Governance Statement and additionally as part of our organisational development programme, which in 2016/17 included externally facilitated timeout sessions.
Accountability
Through the Risk Management Framework and the supporting Assurance Framework and Risk Register, the Governing Body has set the risk appetite for the organisation. This determines the nature and extent of the significant risks it is willing to take in achieving its strategic objectives. We ensure effective management of conflicts of interest and a robust process for risk management and internal control which is monitored through quarterly Corporate Assurance Reports. A positive relationship has been developed with both Internal Audit (360 Assurance) and External Audit

43
(KPMG).
Remuneration
Levels of remuneration are recommended by the Remuneration Committee for Governing Body members, and it takes into account a range of factors in its recommendations including that levels of remuneration are sufficient to attract, retain and motivate staff. The national Agenda for Change process links progression through the pay spines to performance. Conflicts of interest are well managed so that no individual is involved in considering their own remuneration.
Relations with Stakeholders
There are effective partnership arrangements in place through the Team Doncaster local strategic partnership which includes the local Health & Wellbeing Board. There are a range of other partnerships relevant to stakeholder groups including Patient Participation Groups, the local Safeguarding Boards, Working Together for CCG collaborative commissioning arrangements, and meetings with NHS England both to provide assurance and as a co-commissioner. Arrangements are in place to effectively share information between partners. We achieve a dialogue with our stakeholders based on a mutual understanding of our objectives by engaging our stakeholders in our strategic planning rounds and in specific clinical leadership engagements. We schedule an Annual General Meeting for wider stakeholder communication, and at least 3 meetings per year of the Practice Representatives convened by the Clinical Chair of the Governing Body. Our Governing Body meetings are held in public and there is a section at the beginning of each meeting for patient stories and public questions in order to increase the Governing Body’s direct engagement with members of the public for whom we commission services.
Discharge of Statutory Functions In light of recommendations of the 1983 Harris Review, the clinical commissioning group has reviewed all of the statutory duties and powers conferred on it by the National Health Service Act 2006 (as amended) and other associated legislative and regulations. As a result, I can confirm that the clinical commissioning group is clear about the legislative requirements associated with each of the statutory functions for which it is responsible, including any restrictions on delegation of those functions. Responsibility for each duty and power has been clearly allocated to a lead Director. Directorates have confirmed that their structures provide the necessary capability and capacity to undertake all of the clinical commissioning group’s statutory duties. Risk management arrangements and effectiveness Our Integrated Risk Management Framework - Strategy, Policy & Procedure was reviewed and re-approved by our Governing Body in February 2016. Our strategic aim is to control risks to patients, to staff and to the organisation as far as is reasonably practicable and in accordance with current guidance, legislation and best practice. We recognise and accept our duty and legal responsibility to provide a safe and healthy working environment for all our employees, patients, visitors and all others who may be affected by the working activities of the organisation.
44
We have a proactive approach aiming to identify, assess, evaluate, record and review risks, so as to reduce the likelihood of them causing harm to patients or staff or loss to the clinical commissioning group and to reduce the impact of such harm or losses should they occur. The Integrated Risk Management Framework - Strategy, Policy & Procedure covers risk identification, evaluation, control, review and assurance and:
• Has been endorsed by the Governing Body.
• Sets out the organisational attitude to and appetite for risk which was established by the Governing Body and who agreed that any risk scored as High or above should be treated; a risk may therefore be tolerated where the score is 11 or below.
• Clearly defines the structures for the management and ownership of risk.
• Clearly identifies how to manage situations in which a potential risk develops into an actual risk.
• Specifies the way in which risk issues are considered at each level of business planning - ranging from the capture of strategic risks on the Assurance Framework to the capture of operational team risks on team Risk Registers and the capture of project risks on project risk logs.
• Specifies how new and existing activities are assessed for risk, and, dependent on the level of risk, are then incorporated into either the Assurance Framework, the Risk Register, or into a project risk log.
• Identifies controls and measures which are in place to control the risk and reduce its likelihood of occurring.
• Uses common terminology and scoring in relation to risk issues which is replicated across the Assurance Framework and Risk Register.
• Defines the structures for gaining assurance about the management of risk – including quarterly reporting via the Corporate Assurance Report to Governing Body and receipt of the Assurance Framework.
• Defines the criteria which inform assessment of risk and the definition of specific risks as “key” i.e. those risks which threaten the achievement of our principal objectives are captured on the Assurance Framework. The more operational team-level risks are captured on the Risk Register.
• Defines the way in which the Risk Register and risk evaluation criteria will be regularly reviewed.
• Is set out in a single document and is easily available to all staff on the organisation’s website.
Risk management is embedded in the activity of the organisation through the above measures and also through assessments of specific risks (e.g. information governance, business continuity) and through our Governing Body and Committee coversheets which map items to the Assurance Framework and assess equality impact. We have a clear process for reporting, managing, investigating and learning from incidents captured in our Incident Management Policy. Some risks impact across our partnerships; we have shared risks and mitigation plans for joint commissioning such as the Better Care Fund and we also have helpful oversight from the Health & Wellbeing Board in overseeing system-wide risks. We develop risk share processes with our Providers which are contractualised.

45
Capacity to Handle Risk The principal risks to our organisation are those captured on the Assurance Framework, which captures both new and emerging risks. The Assurance Framework is mapped to our strategic objectives which are detailed in our Constitution. Each Assurance Framework risk is assigned to a lead Chief of Service or Head of Service. On at least a quarterly basis, the Chief of Corporate Services as the custodian of the Governing Body Assurance Framework meets with the assigned lead to monitor progress on any actions, challenge controls and assurances, and support identification of new or emerging risk areas within that lead’s area of responsibility. The Governing Body receives the full Assurance Framework on a quarterly basis, reviews it to ensure that it accurately reflects the current risk profile of the organisation and identifies any new/emerging risks or gaps in control/assurance for inclusion on the Framework. The Governing Body is able to identify these risks/gaps in terms of provider assurance through the monthly Quality and Performance Report and the minutes of the Quality & Patient Safety Committee, the Engagement & Experience Committee, the Executive Committee and the Primary Care Commissioning Committee. The Governing Body is able to identify risks or gaps in control/assurance in terms of corporate performance as a statutory body through the monthly Finance Report, the quarterly Corporate Assurance Report, and the minutes of the Audit Committee. The Audit Committee receives the full Assurance Framework periodically and its role is to undertake a deeper dive on a range of the risks, controls and assurances. As well as testing during the Audit Committee meetings, the Audit Committee periodically requests a “deep dive” exercise into random Assurance Framework risks to ensure that assurances can be produced under test conditions. The Audit Committee also receives the full Risk Register on an annual basis, and a summary of the Risk Register is reported quarterly to the Audit Committee and the Governing Body through the Corporate Assurance Report. This process ensures effective management of risks between the Assurance Framework and Risk Register. All staff are offered risk management training commensurate with their duties and responsibilities. All staff are expected to undertake 3 yearly Risk Awareness training which is incorporated into Health, Safety & Security e-learning and will receive any Risk Awareness required as part of their induction. Governing Body members and Senior Managers require risk management training every 2 years in accordance with national guidance. There is a specially designed induction session for Governing Body Members and Senior Managers. We learn as an organisation from good risk management practice by working with our Internal Auditors, 360 Assurance, by participating in benchmarking exercises run by 360 Assurance, and by attending relevant best practice workshops.

46
Risk Assessment Risk identification, assessment and monitoring is a continuous structured process in ensuring that we work within the legal and regulatory framework, identifying and assessing possible risks facing the organisation, and planning to prevent and respond to these. The process of risk management covers the following 5 steps to risk assessment:
• Step 1 – Identify the Risk
• Step 2 – Assess the Risk
• Step 3 – Evaluate the Risk
• Step 4 – Record the Risk
• Step 5 – Review the Risk A standard 5x5 risk matrix as depicted below has been adopted and is used across our activities, the Risk Register and the Assurance Framework. Our risk tolerance/appetite under which risks can be tolerated is a score of 11 or below where the assessment has been undertaken following the implementation of controls and assurances. This risk appetite was agreed by our Governing Body during its approval of the Integrated Risk Management Framework - Strategy, Policy & Procedure.
Risk Matrix
Likelihood
1 2 3 4 5
Rare Unlikely Possible Likely Almost certain
Co
nseq
uen
ce
(1) Negligible 1 2 3 4 5
(2) Minor 2 4 6 8 10
(3) Moderate 3 6 9 12 15
(4) Major 4 8 12 16 20
(5) Extreme 5 10 15 20 25
1-5 Low
6-10 Medium
12-15 High
16-20 Very High
25 Extreme
The Governing Body Assurance Framework Risk Profile at year-end was.
Risks
2016/17 Q1 Q2 Q3 Q4
Total risks on the Assurance Framework
20 21 21 20
Risks in excess of the toleration threshold
2 3 3 3
Risks in excess of toleration threshold being treated
2 3 3 3
Risks below the toleration threshold being treated
1 3 1 0
New risks added to the Assurance Framework
0 1 0 0
Risks removed from the Assurance Framework
0 0 0 1
Score Rating Number
of risks 1-5 Low 0 6-11 Medium 17
12-15 High 2 16-20 Very High 1
25 Extreme 0
Risk treatment Number of risks
Treat 3 Tolerate 17
Terminate 0 Transfer 0

47
There have been no major risks to governance, risk management and internal control during the reporting period, including no risks to compliance with our licence. One new risk was added during Quarter 2 of the reporting period (Risk 4.4) relating to different commissioning footprints and collaborations emerging at a rapid pace (score of 12), and this risk continues to be treated. Risk 1.4 relating to our efficiency programme for 2016/17 has been running at a score of 12 throughout the year. At the Governing Body meeting in January 2017, the positive assurance for 2016/17 was noted and it was agreed that the risk should be amended to reflect the challenges in the 2017/18 forecast position. This left the new risk description at a residual risk at a score of 16. The financial position is reported monthly to Governing Body, alongside any developments. Progress on developing Quality, Innovation, Productivity & Prevention initiatives in response to the 2017/18 financial position is progressing well, with initiatives being identified to close the gap. However many of the initiatives are ambitious and will be challenging to achieve. Other sources of assurance Internal Control Framework A system of internal control is the set of processes and procedures in place in the clinical commissioning group to ensure it delivers its policies, aims and objectives. It is designed to identify and prioritise the risks, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically. The system of internal control allows risk to be managed to a reasonable level rather than eliminating all risk; it can therefore only provide reasonable and not absolute assurance of effectiveness. We employ a range of controls ranging from preventative controls (stopping the risk occurring e.g. access controls, financial authorisation levels), to detective controls (if the risk is threatening to occur, how would we know e.g. performance monitoring, quality reporting), and directive controls (instructions or guidance in place to reduce the chance of the risk occurring e.g. policies, training). When scoring risks, the “uncontrolled risk score” is the score if there were no controls in place and this helps us to prioritise risks. The “actual risk score” is the current score with the current controls in place which may serve to reduce the likelihood of the risk occurring. Annual audit of conflicts of interest management The revised statutory guidance on managing conflicts of interest for CCGs (published June 2016) requires CCGs to undertake an annual internal audit of conflicts of interest management. To support CCGs to undertake this task, NHS England has published a template audit framework. Our Internal Auditors have carried out our annual internal audit of conflicts of interest and the findings of the audit were:

48
Scope area Compliance level
Governance arrangements Compliant Declarations of interest and gifts and hospitality Compliant Registers of interest, gifts and hospitality and procurement decisions
Compliant
Decision making processes and contract monitoring Compliant Identifying and managing non-compliance Compliant
Data Quality Quality data is essential for commissioning effective, relevant and timely care, efficient administrative processes, management and strategic planning, establishing acceptable service agreements/contracts for healthcare provision, identification of local priorities and health needs assessments, ensuring that the organisation’s expenditure is accurately calculated, providing reliable intelligence regarding local providers, and delivery of local and national priorities. Data therefore needs to be accurate, credible, reliable and secure. We regard data as being of high quality if it is: valid (checked for correctness and meaningfulness), complete, consistent, accurate, relevant, available when needed, stored securely and confidentially, and timely (up to date). These are the criteria against which the Governing Body assesses the quality of data which it receives, and has concluded that the data is receives is of sufficient quality to meet its purposes. Information Governance The NHS Information Governance Framework sets the processes and procedures by which the NHS handles information about patients and employees, in particular personal identifiable information. The NHS Information Governance Framework is supported by an information governance toolkit and the annual submission process provides assurances to the clinical commissioning group, other organisations and to individuals that personal information is dealt with legally, securely, efficiently and effectively. The level of compliance demonstrated by completion of the 2016/17 Information Governance (IG) Toolkit is 77% with all standards at a score of at least 2, which is deemed by NHS Digital to be satisfactory. Our IG Toolkit was also reviewed by our Internal Auditors, and this audit resulted in an outcome of significant assurance. We have in place a Senior Information Risk Owner to support our arrangements for managing and controlling risks relating to information / data security. We develop an annual Information Security Management Statement and Assurance Plan, the outputs from which are reported through the Corporate Assurance Report. There have been no data security related incidents reported to the Information Commissioner during the reporting period. Our information governance risks have been mitigated to a tolerated level through robust use of the Information Governance Toolkit. Information Governance activity and assurance is presented quarterly to our Governing Body in the Corporate Assurance Report. Our Corporate Governance Management Group has maintained a specific focus on Information Governance.

49
We place high importance on ensuring that we have robust information governance systems and processes in place to help protect patient and corporate information. We have established an information governance management framework and have developed information governance processes and procedures in line with the information governance toolkit. We have ensured all staff undertake annual information governance training to maintain staff awareness of their information governance roles and responsibilities. There are processes in place for incident reporting and investigation of serious incidents. We have in place information risk assessment and management procedures and a programme which continues to fully embed an information risk culture throughout the organisation. Business Critical Models An appropriate framework and environment is in place via our Business Continuity Policy and our Business Continuity Plan to provide quality assurance of business critical models - inputs, methodology and outputs. We have no business critical models which meet the threshold criteria within the Macpherson Report 2013. Our Business Continuity Plan is overseen by the Corporate Governance Team, and a quarterly update is provided to the Corporate Governance Management Group, which reports to the Audit Committee. Our Business Continuity Policy and Plan are approved by the Audit Committee. Third party assurances We receive third party assurances from:
• NHS Shared Business Services via assurances received by our Chief Finance Officer relating to the provision of Financial and Accounting Services
• McKesson on the operation of the Electronic Staff record (ESR) Payroll infrastructure and service.
• North East Commissioning Services (NECS) relating to Data Management and Integration. Assurance is received through the contract which we hold with NECS and through the oversight of the flow of data by an Information Sharing Contract which we hold with NHS Digital and an Information Sharing Agreement.
• eMBED Health Consortium. Assurance is received through the contract which we hold with eMBED in relation to minor services such as our Registration Authority.
• Local CCGs in South Yorkshire & Bassetlaw with which we are in partnership arrangements for hosted services. All partnership arrangements were overseen by NHS England at establishment, and are supported by Memorandums of Understanding. Each hosted service has established formal arrangements through their Memorandum of Understanding for review and assurance of the service. For example, the Continuing Healthcare hosted service has a formal partnership meeting attended by all parties to the service through which assurances are received, and the Health & Safety hosted services is assured through the mechanism of the South Yorkshire & Bassetlaw Governance Leads meeting.
• The Working Together collaborative partnership of 8 CCGs and NHS England, which focusses on developing and enacting shared commissioning principles for
50
Hyper Acute Stroke Unit Services and Children’s Surgery & Anaesthesia. Assurance is provided via a Manual Agreement and Terms of Reference and receipt of minutes and recommendations by the Governing Body. The Working Together collaborative partnership will become a formal Joint Committee of CCGs meeting in public from April 2017.
• The collaborative commissioning arrangements for 999 and 111 services across CCGs in the Yorkshire & Humber region. Assurance is provided via a Memorandum of Understanding and local representation at the Joint Strategic Commissioning Board. This will become a Joint Committee of CCGs in due course.
• Sustainability & Transformation Plan (STP) Collaborative Partnership Board, a collaborative non-decision-making forum where commissioner and provider partners across South Yorkshire & Bassetlaw meet to discuss STP progress. Assurance is provided via Chief Officer representation at the Collaborative Partnership Board and receipt of minutes and recommendations by the Governing Body.
The Chief Finance Officer reviews all Service Auditor Reports received, considers the implications of any deficiencies in control which they highlight, and advises the Audit Committee accordingly. Control Issues During the year, we did not identify any governance, risk management or control issues which were significant to the organisation. One of our Internal Audit reports resulted in an opinion of limited assurance. Patients detained in hospital under a relevant section of the Mental Health Act 1983 for whom NHS Doncaster CCG was identified as one of the Responsible Commissioners are generally having their aftercare services arranged and provided for them in line with the statutory responsibilities placed on the CCG. However, the lack of an agreed discharge process and formalised Quality Assurance Framework, along with weaknesses identified with management information and governance / reporting resulted in a Limited Assurance that the CCG was able to meet its objectives. The Internal Audit report acknowledged that the CCG was already aware of the control issues, and was addressing this through an action plan. This action plan has now been formalised and is being monitored by the Quality & Patient Safety Committee. The limited assurance opinion has not affected our Head of Internal Audit Opinion and has not prejudiced the achievement of priorities or undermined the integrity or reputation of the CCG. Review of economy, efficiency & effectiveness of the use of resources The Governing Body has overarching responsibility for ensuring that the clinical commissioning group has appropriate arrangements in place to exercise its functions effectively, efficiently and economically and in accordance with the Groups principles of good governance (its main function). Our Constitution delegates responsibility to ensure appropriate arrangements are in place for us to fulfil this duty to the Audit Committee and requires that this Committee undertakes functions as set out in its

51
Terms of Reference as agreed by the Governing Body. The Audit Committee receives regular reports on financial governance and reviews the annual accounts. In terms of our rating for the Quality of Leadership indicator within the CCG Improvement and Assessment Framework 2016/17, we have been advised that the year-end position for this indicator will now not be published until after the publication of CCG annual reports. Our latest available results are available on MyNHS (Quarter 2 2016/17), and the year end results for the Quality of leadership Indicator will be available from July 2017 at www.nhs.uk/service-search/scorecard/results/1175. The Chief Finance Officer is a member of the Governing Body and is responsible for providing financial advice to the Group and for supervising financial control and accounting systems. The Chief Finance Officer presents the Financial Strategy to the Governing Body for agreement at the beginning of each financial year, and then presents Finance Reports to each Governing Body meeting, where open challenge on the progress of the finances against the strategy takes place. The monthly Finance Report also includes commentary on our running costs, our efficiency programmes, and associated controls. The annual accounts process ensures that our accounts are effectively closed down and accounts produced. Annual Accounts scrutiny has been via the Audit Committee, with the final accounts being approved at an extraordinary Governing Body meeting. Systems of financial control have been reviewed by our Internal Auditor, 360 Assurance, which resulted in an outcome of significant assurance. During the reporting period our External Auditors have been KPMG, and during the year the Chief Finance Officer and the Audit Committee have worked constructively with the Audit Manager and their team. The progress of the External Audit work programme is monitored by the Audit Committee through regular written progress reports, which have also included useful technical updates of developments elsewhere in public services both nationally and internationally. During the reporting period our Internal Auditors have been 360 Assurance, and during the year the Chief Finance Officer, team members and the Audit Committee have worked constructively with the Internal Audit team. The Audit Committee agreed the Internal Audit programme at the beginning of the year and has regularly reviewed and considered the progress and findings of Internal Audit. Delegation of functions The Working Together collaborative partnership of 8 CCGs and NHS England focusses on developing and enacting shared commissioning principles for Hyper Acute Stroke Unit Services and Children’s Surgery & Anaesthesia. Assurance is provided via a Manual Agreement and Terms of Reference and receipt of minutes and recommendations by the Governing Body. The Working Together collaborative partnership will become a formal Joint Committee of CCGs meeting in public from April 2017 with delegated decision making functions as described in the terms of reference.
52
We have collaborative commissioning arrangements for 999 and 111 services across CCGs in the Yorkshire & Humber region. Assurance is provided via a Memorandum of Understanding and local representation at the Joint Strategic Commissioning Board. This Commissioning Board will become a Joint Committee of CCGs in due course. Limited delegation is in place to the Commissioning Board through a Memorandum of Understanding. Counter fraud arrangements An Accredited Counter Fraud Specialist is contracted from 360 Assurance (our Internal Auditors) to undertake counter fraud work proportionate to identified risks. Our Chief Finance Officer is the Senior Responsible Officer for fraud, bribery and corruption. Our Audit Committee receives a report against the Standards for Commissioners using the national Self Reporting Tool (SRT) on an annual basis, with exception reports throughout the year. The Counter Fraud Specialist recommends appropriate action regarding any NHS Protect quality assurance recommendations, and action is assured by the Chief Finance Officer. A proportionate proactive counter fraud work plan is developed at the beginning of each year to address identified risks. Head of Internal Audit Opinion Following completion of the planned audit work for the financial year for the clinical commissioning group, the Head of Internal Audit issued an independent and objective opinion on the adequacy and effectiveness of the clinical commissioning group’s system of risk management, governance and internal control. The Head of Internal Audit concluded that:
In providing an opinion for the financial year, it is important to reflect on the environment in which the organisation has been required to function and the impact of an on-going need to meet quality challenges whilst reducing costs, along with responding to the sustainability and transformation agenda. This will undoubtedly impact on the operation of control, however, the system of internal control is designed to manage risk to a reasonable level rather than eliminate all risk of failure. From my review of your systems of internal control, primarily through the operation of your Governing Body’s Assurance Framework in the year to date, and the outcome of individual assignments also completed in the year, I am providing a Significant Assurance that there is a generally sound system of internal control, designed to meet the organisation’s objectives, and that controls are generally being applied consistently. It should be recognised that the CCG’s current systems of control and arrangements for governance and the management of risk will need to continue to develop in the coming year, particularly reflecting on increasing cross-organisation and sector partnerships, as these arrangements will bring additional challenges in terms of the management of risk and ensuring that all partners understand the inter-relationships.
53
During the year, Internal Audit issued the following audit reports: Area of Audit Level of Assurance Given
Budgetary Control & Key Financial Systems
Significant
Information Governance Toolkit Significant
Monitoring the Quality of Care in Care Homes
Split: Significant Assurance for progress made since the last review, and Limited Assurance for overall arrangements for achieving stated aims for this area.
Review of Section 117 (Mental Health Aftercare) Arrangements
Limited
Governing Body Assurance Framework Review / Head of Internal Audit Opinion
Significant
Primary Care Co-Commissioning
Significant
Conflicts of Interest All Areas Compliant
Review of the effectiveness of governance, risk management and internal control My review of the effectiveness of the system of internal control is informed by the work of the internal auditors, executive managers and clinical leads within the clinical commissioning group who have responsibility for the development and maintenance of the internal control framework. I have drawn on performance information available to me. My review is also informed by comments made by the external auditors in their annual audit letter and other reports. Our assurance framework provides me with evidence that the effectiveness of controls that manage risks to the clinical commissioning group achieving its principles objectives have been reviewed. I have been advised on the implications of the result of this review by:
• Governing Body: Responsible for providing clear commitment and direction for Risk Management within the organisation. The Governing Body delegates responsibility for oversight of risk and non-clinical risk management to the Audit Committee and delegates responsibility for clinical risk management to the Quality & Patient Safety Committee. Following receipt of a range of reports covering finance, quality, commissioning and corporate areas, the Governing Body has concluded positively upon the system of internal control.
• Audit Committee: Responsible for providing an independent overview of the arrangements for risk management within the organisation, with specific responsibilities for financial risk management. It undertakes an annual self-assessment of its effectiveness and reviews Internal and External Audits, the Assurance Framework and financial governance reports and the Probity Register. The Audit Committee has been assured by the reports provided to it, and has been given the opportunity to raise any areas of note to the Governing Body on a monthly basis.
• Quality & Patient Safety Committee: As the Committee with overarching responsibility for clinical risk management, it provides assurance to the

54
Governing Body that appropriate clinical risk management arrangements are in place across the organisation. The Quality & Patient Safety Committee is underpinned by various Sub Groups covering areas including safeguarding, incidents and medicines management.
• Senior Management Team: The Chief Finance Officer has concluded positively upon the system of financial control, the Chief of Corporate Services has concluded positively upon the system of corporate control, and the Chief Nurse has concluded positively upon the system of quality and safety control.
• Internal Audit: Internal Audit reviews of systems of internal control and progress reports to the Audit Committee have supported my review.
• NHS England Area Team: We have quarterly Assurance Reviews with the local Area Team of NHS England. Reviews during the reporting period have been positive.
Conclusion My review confirms that there are no significant control issues for the clinical commissioning group.
Mrs Jackie Pederson Accountable Officer 25 May 2017
55
2. Remuneration and Staff Report 2.1. Remuneration Report 2.1.1. Remuneration Committee Chaired by the Lay Member for Audit & Governance, our Remuneration Committee has delegated responsibility from the Governing Body for advising the Governing Body on all aspects of salary not covered by Agenda for Change, arrangements for termination of employment, remuneration, allowances and terms of service of senior managers covered by the Very Senior Managers pay framework, and approving human resources policies and procedures. Our Remuneration Committee comprises the following Members
• Lay Member – Audit & Governance (Chair)
• Lay Member – Public & Patient Engagement
• Locality Leads x2
• Governing Body Secondary Care Doctor 2.1.2. Policy on the remuneration of senior managers The Remuneration Committee is required to recommend remuneration to the Governing Body within the constraints of national guidance, taking into account the prevailing economic climate, local market conditions and the requirement to obtain best possible value for money. The costs of posts are met from the notified CCG running cost allowance. The onus is on the CCG to ensure it has an affordable staffing and remuneration structure within this running cost allowance. The guidance used to determine the staffing body pay is the national Agenda for Change guidance from NHS Employers. The policy for all staff subject to Agenda for Change contracts aligns to the national agenda for change guidance on duration, notice periods and termination payments. Further information on termination payments is detailed in the CCG Management of Change Policy. Senior Manager performance is subject to evaluation in the same way as the main staffing body – through our Managing Performance Policy. Performance measures are aligned to the strategic direction of the organisation and set by the line manager of each employee. No performance related premia policy is in place for Senior Managers or Governing Body members. 2.1.3. Remuneration of Very Senior Managers Where one or more senior managers of a CCG are paid more than £142,500 per annum, the remuneration report must explain the steps the CCG has taken to satisfy itself that this remuneration is reasonable. No senior managers of the CCG are paid more than £142,500 per annum. Remuneration report tables are shown overleaf.

56
Senior manager remuneration (including salary and pension entitlements)
Name and Title
2016/17
(a) Salary
(bands of £5,000)
(b) Expense payments (taxable)
to nearest £100*
(c) Performance
pay and bonuses (bands of £5,000)
(d) Long term
performance pay and bonuses (bands of £5,000)
(e) All pension-
related benefits
(bands of £2,500)
(f) TOTAL (a to e)
(bands of £5,000)
£000 £ £000 £000 £000 £000
Executive Members:
Dr David Crichton Chair
95-100 600 0 0 35-37.5 130-135
Mrs Jackie Pederson Chief Officer
125-130 1100 0 0 260-262.5 385-390
Mrs Hayley Tingle Chief Finance Officer
100-105 500 0 0 92.5-95 195-200
Mrs Mary Shepherd Chief Nurse (To 31/08/16)
40-45 600 0 0 15-17.5 55-60
Mr Andrew Russell Chief Nurse (From 01/09/16)
45-50 1000 0 0 167.5-170 215-220
Mr Anthony Fitzgerald Chief of Strategy & Delivery (From 01/08/16)
60-65 500 0 0 42.5-45 105-110
Mrs Sarah Atkins Whatley Chief of Corporate Services
75-80 100 0 0 52.5-55 130-135
Mrs Laura Sherburn Chief of Partnership Commissioning & Primary Care
80-85 0 0 0 37.5-40 120-125
Locality Leads:
Dr Andrew Oakford Locality Lead, North East Locality
55-60 0
0 0 22.5-25 75-80
Dr Jeremy Bradley Locality Lead, North East Locality
40-45 0 0 0 12.5-15 55-60
Dr Niki Seddon Locality Lead, North West Locality
40-45 0 0 0 12.5-15 55-60
Dr Marco Pieri Locality Lead, North West Locality
40-45 0 0 0 12.5-15 55-60
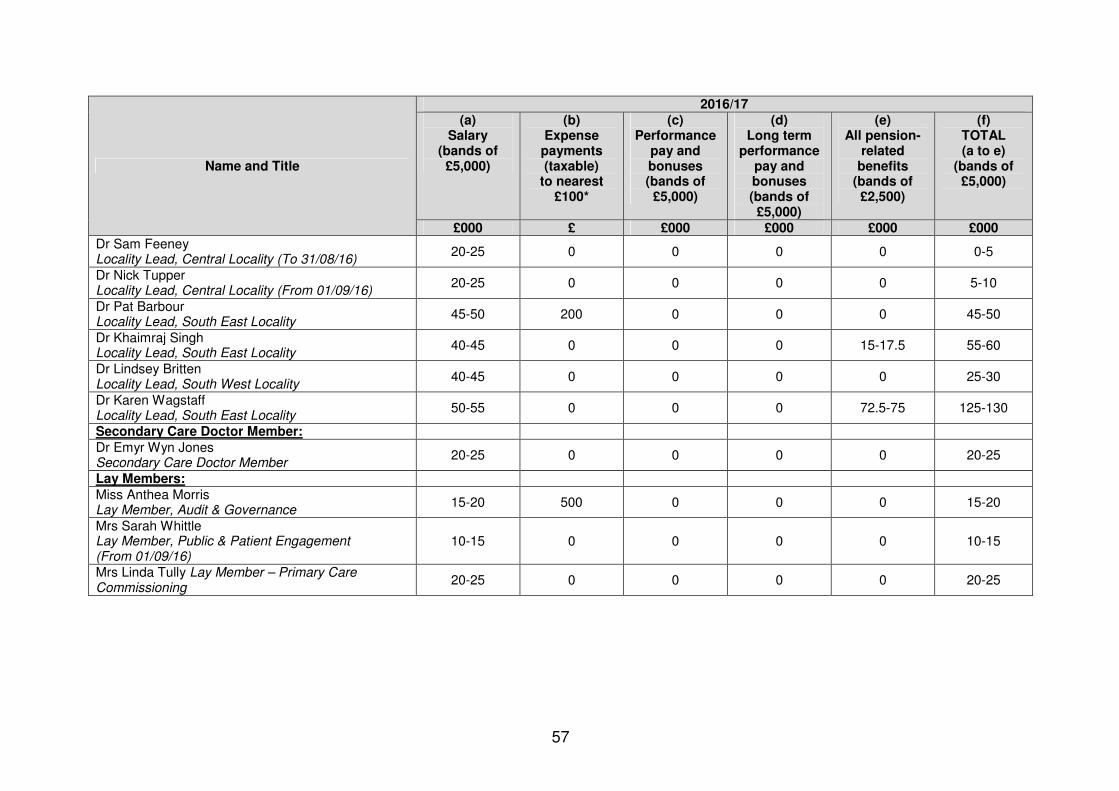
57
Name and Title
2016/17
(a) Salary
(bands of £5,000)
(b) Expense payments (taxable)
to nearest £100*
(c) Performance
pay and bonuses (bands of £5,000)
(d) Long term
performance pay and bonuses (bands of £5,000)
(e) All pension-
related benefits
(bands of £2,500)
(f) TOTAL (a to e)
(bands of £5,000)
£000 £ £000 £000 £000 £000
Dr Sam Feeney Locality Lead, Central Locality (To 31/08/16)
20-25 0 0 0 0 0-5
Dr Nick Tupper Locality Lead, Central Locality (From 01/09/16)
20-25 0 0 0 0 5-10
Dr Pat Barbour Locality Lead, South East Locality
45-50 200 0 0 0 45-50
Dr Khaimraj Singh Locality Lead, South East Locality
40-45 0 0 0 15-17.5 55-60
Dr Lindsey Britten Locality Lead, South West Locality
40-45 0 0 0 0 25-30
Dr Karen Wagstaff Locality Lead, South East Locality
50-55 0 0 0 72.5-75 125-130
Secondary Care Doctor Member:
Dr Emyr Wyn Jones Secondary Care Doctor Member
20-25 0 0 0 0 20-25
Lay Members:
Miss Anthea Morris Lay Member, Audit & Governance
15-20 500 0 0 0 15-20
Mrs Sarah Whittle Lay Member, Public & Patient Engagement (From 01/09/16)
10-15 0 0 0 0 10-15
Mrs Linda Tully Lay Member – Primary Care Commissioning
20-25 0 0 0 0 20-25

58
Name and Title
2015/16
(a) Salary
(bands of £5,000)
(b) Expense payments (taxable)
to nearest £100*
(c) Performance
pay and bonuses (bands of £5,000)
(d) Long term
performance pay and bonuses (bands of £5,000)
(e) All pension-
related benefits
(bands of £2,500)
(f) TOTAL (a to e)
(bands of £5,000)
£000 £ £000 £000 £000 £000
Executive Members:
Dr Nick Tupper Chair
90-95 0 0 0 65-67.5 160-165
Mr Chris Stainforth Chief Officer
120-125 0 0 0 25-27.5 145-150
Mrs Hayley Tingle Chief Finance Officer
90-95 500 0 0 27.5-30 115-120
Mrs Mary Shepherd Chief Nurse
90-95 800 0 0 17.5-20 105-110
Mrs Jackie Pederson Chief of Strategy & Delivery
95-100 300 0 0 25-27.5 125-130
Mrs Sarah Atkins Whatley Chief of Corporate Services
70-75 200 0 0 47.5-50 120-125
Mrs Laura Sherburn Chief of Partnerships Commissioning
80-85 0 0 0 260-262.5 340-345
Mrs Martha Coulman Chief of Primary Care (To 31/12/15)
45-50 400 0 0 462.5-465 510-515
Locality Leads:
Dr Andrew Oakford Locality Lead, North East Locality
55-60 0 0 0 20-22.5 75-80
Dr Jeremy Bradley Locality Lead, North East Locality
40-45 0 0 0 10-12.5 50-55
Dr Niki Seddon Locality Lead, North West Locality
40-45 0 0 0 10-12.5 50-55
Dr Marco Pieri Locality Lead, North West Locality
40-45 0 0 0 10-12.5 50-55
Dr Sam Feeney Locality Lead, Central Locality
45-50 0 0 0 47.5-50 95-100
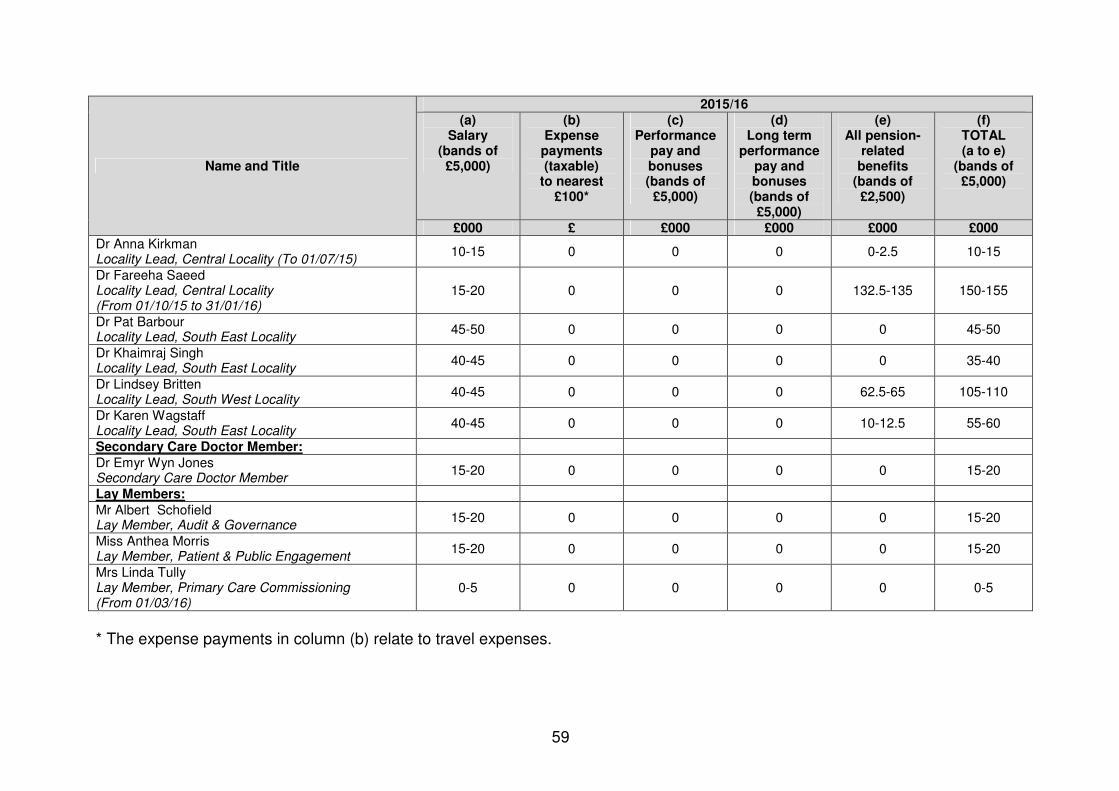
59
Name and Title
2015/16
(a) Salary
(bands of £5,000)
(b) Expense payments (taxable)
to nearest £100*
(c) Performance
pay and bonuses (bands of £5,000)
(d) Long term
performance pay and bonuses (bands of £5,000)
(e) All pension-
related benefits
(bands of £2,500)
(f) TOTAL (a to e)
(bands of £5,000)
£000 £ £000 £000 £000 £000
Dr Anna Kirkman Locality Lead, Central Locality (To 01/07/15)
10-15 0 0 0 0-2.5 10-15
Dr Fareeha Saeed Locality Lead, Central Locality (From 01/10/15 to 31/01/16)
15-20 0 0 0 132.5-135 150-155
Dr Pat Barbour Locality Lead, South East Locality
45-50 0 0 0 0 45-50
Dr Khaimraj Singh Locality Lead, South East Locality
40-45 0 0 0 0 35-40
Dr Lindsey Britten Locality Lead, South West Locality
40-45 0 0 0 62.5-65 105-110
Dr Karen Wagstaff Locality Lead, South East Locality
40-45 0 0 0 10-12.5 55-60
Secondary Care Doctor Member:
Dr Emyr Wyn Jones Secondary Care Doctor Member
15-20 0 0 0 0 15-20
Lay Members:
Mr Albert Schofield Lay Member, Audit & Governance
15-20 0 0 0 0 15-20
Miss Anthea Morris Lay Member, Patient & Public Engagement
15-20 0 0 0 0 15-20
Mrs Linda Tully Lay Member, Primary Care Commissioning (From 01/03/16)
0-5 0 0 0 0 0-5
* The expense payments in column (b) relate to travel expenses.
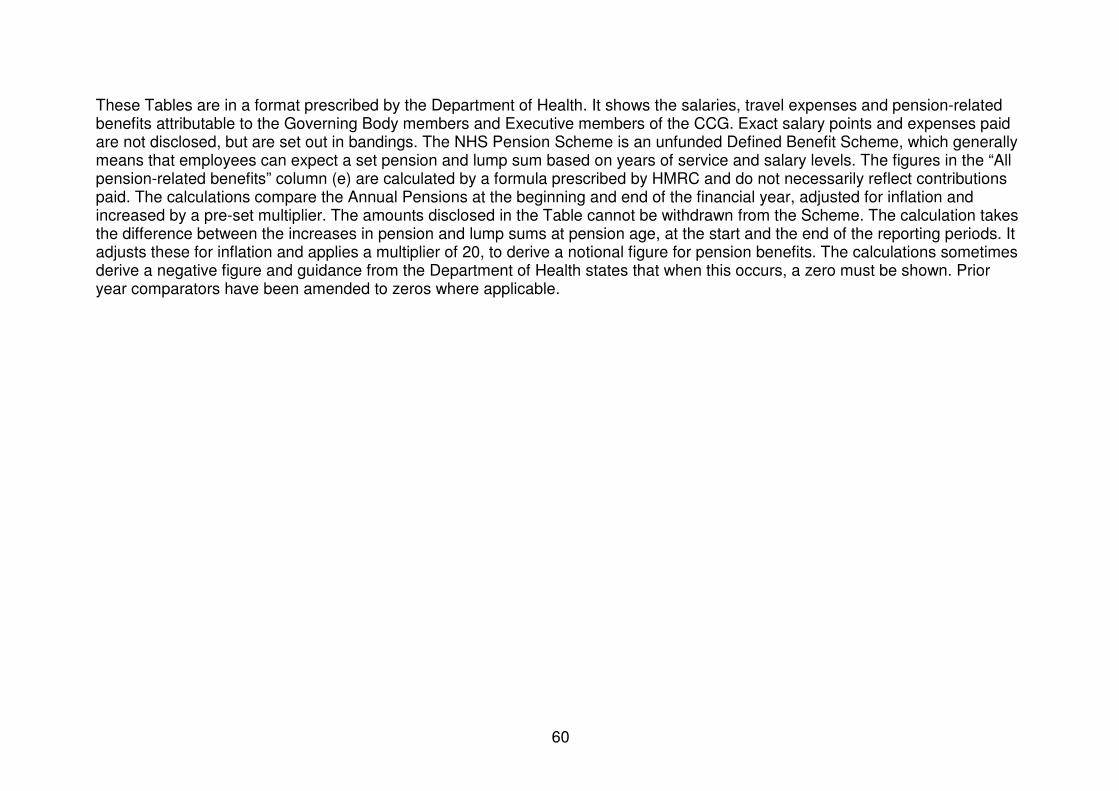
60
These Tables are in a format prescribed by the Department of Health. It shows the salaries, travel expenses and pension-related benefits attributable to the Governing Body members and Executive members of the CCG. Exact salary points and expenses paid are not disclosed, but are set out in bandings. The NHS Pension Scheme is an unfunded Defined Benefit Scheme, which generally means that employees can expect a set pension and lump sum based on years of service and salary levels. The figures in the “All pension-related benefits” column (e) are calculated by a formula prescribed by HMRC and do not necessarily reflect contributions paid. The calculations compare the Annual Pensions at the beginning and end of the financial year, adjusted for inflation and increased by a pre-set multiplier. The amounts disclosed in the Table cannot be withdrawn from the Scheme. The calculation takes the difference between the increases in pension and lump sums at pension age, at the start and the end of the reporting periods. It adjusts these for inflation and applies a multiplier of 20, to derive a notional figure for pension benefits. The calculations sometimes derive a negative figure and guidance from the Department of Health states that when this occurs, a zero must be shown. Prior year comparators have been amended to zeros where applicable.
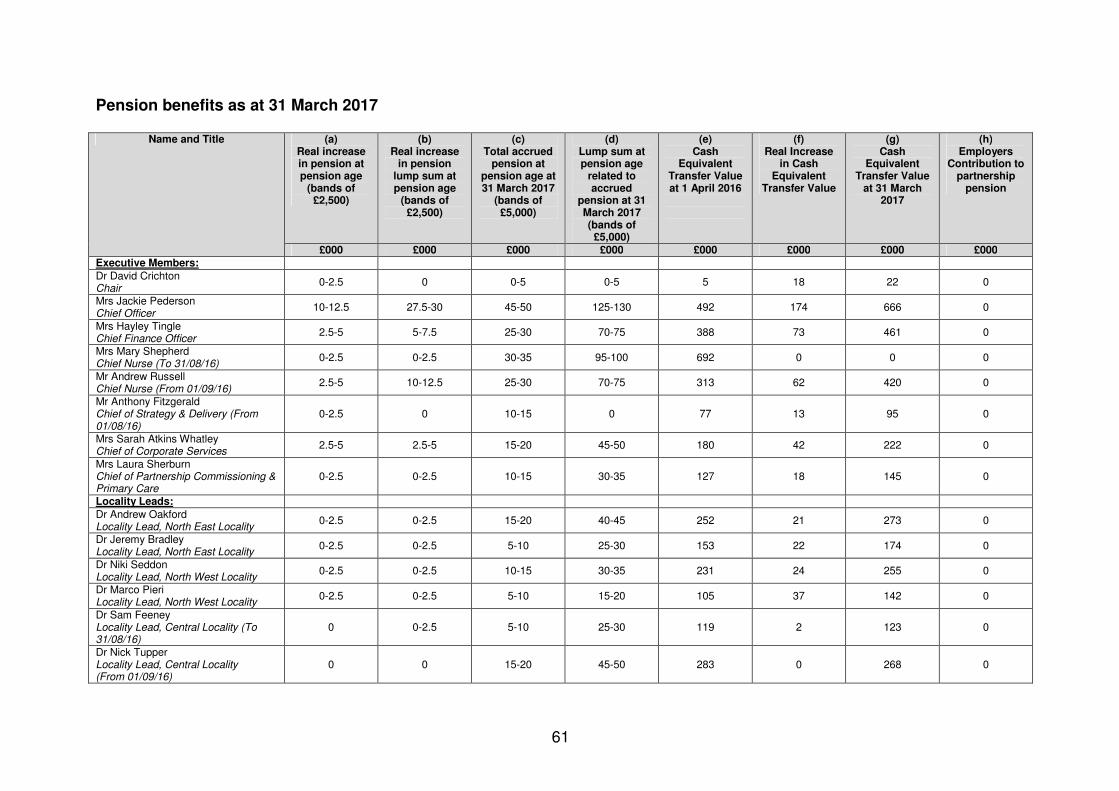
61
Pension benefits as at 31 March 2017
Name and Title (a) Real increase in pension at pension age
(bands of £2,500)
(b) Real increase
in pension lump sum at pension age
(bands of £2,500)
(c) Total accrued
pension at pension age at 31 March 2017
(bands of £5,000)
(d) Lump sum at pension age
related to accrued
pension at 31 March 2017 (bands of £5,000)
(e) Cash
Equivalent Transfer Value at 1 April 2016
(f) Real Increase
in Cash Equivalent
Transfer Value
(g) Cash
Equivalent Transfer Value
at 31 March 2017
(h) Employers
Contribution to partnership
pension
£000 £000 £000 £000 £000 £000 £000 £000
Executive Members:
Dr David Crichton Chair
0-2.5 0 0-5 0-5 5 18 22 0
Mrs Jackie Pederson Chief Officer
10-12.5 27.5-30 45-50 125-130 492 174 666 0
Mrs Hayley Tingle Chief Finance Officer
2.5-5 5-7.5 25-30 70-75 388 73 461 0
Mrs Mary Shepherd Chief Nurse (To 31/08/16)
0-2.5 0-2.5 30-35 95-100 692 0 0 0
Mr Andrew Russell Chief Nurse (From 01/09/16)
2.5-5 10-12.5 25-30 70-75 313 62 420 0
Mr Anthony Fitzgerald Chief of Strategy & Delivery (From 01/08/16)
0-2.5 0 10-15 0 77 13 95 0
Mrs Sarah Atkins Whatley Chief of Corporate Services
2.5-5 2.5-5 15-20 45-50 180 42 222 0
Mrs Laura Sherburn Chief of Partnership Commissioning & Primary Care
0-2.5 0-2.5 10-15 30-35 127 18 145 0
Locality Leads:
Dr Andrew Oakford Locality Lead, North East Locality
0-2.5 0-2.5 15-20 40-45 252 21 273 0
Dr Jeremy Bradley Locality Lead, North East Locality
0-2.5 0-2.5 5-10 25-30 153 22 174 0
Dr Niki Seddon Locality Lead, North West Locality
0-2.5 0-2.5 10-15 30-35 231 24 255 0
Dr Marco Pieri Locality Lead, North West Locality
0-2.5 0-2.5 5-10 15-20 105 37 142 0
Dr Sam Feeney Locality Lead, Central Locality (To 31/08/16)
0 0-2.5 5-10 25-30 119 2 123 0
Dr Nick Tupper Locality Lead, Central Locality (From 01/09/16)
0 0 15-20 45-50 283 0 268 0

62
Dr Pat Barbour Locality Lead, South East Locality
0 0 0 0 0 0 0 0
Dr Khaimraj Singh Locality Lead, South East Locality
0-2.5 0-2.5 5-10 15-20 78 14 92 0
Dr Lindsey Britten Locality Lead, South West Locality
0 0-2.5 10-15 25-30 170 5 175 0
Dr Karen Wagstaff Locality Lead, South East Locality
2.5-5 7.5-10 25-30 80-85 457 92 549 0
Secondary Care Doctor Member:
Dr Emyr Wyn Jones Secondary Care Doctor Member
0 0 0 0 0 0 0 0
Lay Members:
Miss Anthea Morris Lay Member, Audit & Governance
0 0 0 0 0 0 0 0
Mrs Sarah Whittle Lay Member, Public & Patient Engagement (From 01/09/16)
0 0 0 0 0 0 0 0
Mrs Linda Tully Lay Member – Primary Care Commissioning
0 0 0 0 0 0 0 0
This Table presents the figures supplied by the NHS Pensions Agency and gives the detail behind the figures used for the calculation of “All pension-related benefits”. The Pension Benefits Disclosures for Non Locality Leads include all contributions, including those from non-CCG employments. The Pension Benefits Disclosures for Locality Leads only relate to Non-Practitioner contributions and do not include Pension Benefits relating to earnings from GMS or PMS Contracts. Certain Members do not receive pensionable remuneration from the CCG therefore there will be no entries in respect of pensions for certain Members. Cash equivalent transfer values A cash equivalent transfer value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time. The benefits valued are the member’s accrued benefits and any contingent spouse’s (or other allowable beneficiary’s) pension payable from the scheme. A CETV is a payment made by a pension scheme or arrangement to secure pension benefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme. The pension
63
figures shown relate to the benefits that the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which disclosure applies. The CETV figures and the other pension details include the value of any pension benefits in another scheme or arrangement which the individual has transferred to the NHS pension scheme. They also include any additional pension benefit accrued to the member as a result of their purchasing additional years of pension service in the scheme at their own cost. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries. Real increase in CETV This reflects the increase in CETV effectively funded by the employer. It takes account of the increase in accrued pension due to inflation, contributions paid by the employee (including the value of any benefits transferred from another scheme or arrangement) and uses common market valuation factors for the start and end of the period.
64
2.1.4. Compensation on early retirement of for loss of office No payments have been made in compensation for early retirement or for loss of office. 2.1.5. Payments to past members No payments have been made to past members. 2.1.6. Pay multiples Reporting bodies are required to disclose the relationship between the remuneration of the highest-paid director/Member in their organisation and the median remuneration of the organisation’s workforce. The banded remuneration of the highest paid director/Member in NHS Doncaster CCG in the financial year 2016-17 was £155,000-£160,000 (2015-16, £155,000-£160,000)*. This was 4.91 times (2015-16, 3.84)* the median remuneration of the workforce, which was £32,407 (2015-16, £40,964). * Note the 2015/16 comparator has been updated.
In 2016-17, one (2015-16, nil) employee received remuneration in excess of the highest-paid director/member. Remuneration ranged from £175,000 to £180,000 (2015-16, n/a). Total remuneration includes salary, non-consolidated performance-related pay, benefits-in-kind, but not severance payments. It does not include employer pension contributions and the cash equivalent transfer value of pensions. The increase in the ratio is due to the following:
• The median salary has decreased by £8,557 due to NHS Doncaster CCG now hosting the Continuing Healthcare (CHC) Previously Un-assessed Periods of Care (PUPOC) service. This has doubled the workforce numbers and the majority of these staff are administrative and therefore on lower salaries than the average.
2.2. Staff Report 2.2.1. Number of senior managers The number of senior managers (classified as those in our Senior Management Team and disclosed in the Remuneration Report) by band are:
• 2 x Very Senior Manager posts
• 1 x Band 9 post (senior management)
• 1 x Band 9 post (senior nursing)
• 2 x Band 8d posts (senior management) 2.2.2. Staff numbers and costs The table below details the average staff numbers and actual costs (including Governing Body Members but excluding Lay Members) for 2016/17.

65
Category Permanently employed staff
Other staff (short term contracts, agency, inward
secondees) Average WTE Cost £000 Average WTE Cost £000
Governing Body Clinical Members
6.10 646 0 0
Administration and estates staff
101.77 4,163 1.36 316
Nursing, midwifery and health visiting staff
44.93 1,848 0 0
0 0
Scientific, Therapeutic and Technical
10.04 571 0 0
Medical & Dental 1.45 186 0 0 Totals 164.29 7,414 1.36 316
The average number of people employed (whole time equivalents) for 2016/17 was 164.28 – see note 4.2 in the Annual Accounts. 2.2.3. Staff composition We are required to analyse and report our workforce by gender. The numbers of the workforce in post (actual headcount) by gender as at 31st March 2017 was: Category Male Female
Members of the Governing Body 8 9 All other senior managers, including all managers at grade VSM, not included above
1 2
All other employees not included in either of the previous two categories
36 123
2.2.4. Sickness absence data Details of the total days lost, total staff years and the average number of working days lost due to Staff Sickness Absence are included in Note 4.3 of the Annual Accounts. 2.2.5. Staff policies Consultation and engagement with employees is a fundamental principle of good employment practice. We hold regular Staff Briefs open to all staff, and Chiefs of Service hold team meetings with their teams. Staff are engaged through their team meetings and open Staff Briefs on the strategic direction and delivery of the organisation, and in its performance. We welcome suggestions and ideas from all staff on how we can improve our performance as an organisation. We participated in the national NHS Staff Survey. We have an active Colleague Engagement Group to seek feedback and ideas from team members and to support us in developing an action plan from the Staff Survey results. We engage with Staff Side representatives through a Joint Negotiation and Consultative Forum.

66
NHS Doncaster CCG is committed to supporting employees in the workplace. We have an Equal Opportunities Policy, Sickness Absence Policy and a Flexible Working Policy which support us to make reasonable adaptations to support our disabled employees and manage any periods of disability related sickness absence appropriately. We have asked all staff for their disability status so that we may target support and development opportunities appropriately. An Equality Report is produced every January which further refers to our equality practices and is available on our website www.doncasterccg.nhs.uk. Our recruitment and selection procedures ensure that all prospective candidates can participate fully in the application process and we offer adjustments where required. 2.2.6. Expenditure on consultancy NHS Doncaster CCG spent £104,795 on Administrative Consultancy. 2.2.7. Off-payroll engagements Table 1: Off-payroll engagements longer than 6 months For all off-payroll engagements as at 31 March 2017, for more than £220 per day and that last longer than six months: Number Number of existing engagements as of 31 March 2017 0 Of which, the number that have existed:
for less than one year at the time of reporting 0 for between one and two years at the time of reporting 0 for between 2 and 3 years at the time of reporting 0 for between 3 and 4 years at the time of reporting 0 for 4 or more years at the time of reporting 0
Table 2: New off-payroll engagements
For all new off-payroll engagements between 01 April 2016 and 31 March 2017, for more than £220 per day and that last longer than six months: Number
Number of new engagements, or those that reached six months in duration, between 1 April 2016 and 31 March 2017
0
Number of new engagements which include contractual clauses giving NHS Doncaster CCG the right to request assurance in relation to income tax and National Insurance obligations
0
Number for whom assurance has been requested 0 Of which:
assurance has been received 0 assurance has not been received 0 engagements terminated as a result of assurance not being received. 0

67
Table 3: Off-payroll engagements / senior official engagements For any off-payroll engagements of Board members and / or senior officials with significant financial responsibility, between 01 April 2016 and 31 March 2017.
Number of off-payroll engagements of board members, and/or senior officers with significant financial responsibility, during the financial year
0
Total no. of individuals on payroll and off-payroll that have been deemed “board members, and/or, senior officials with significant financial responsibility”, during the financial year. This figure should include both on payroll and off-payroll engagements.
0
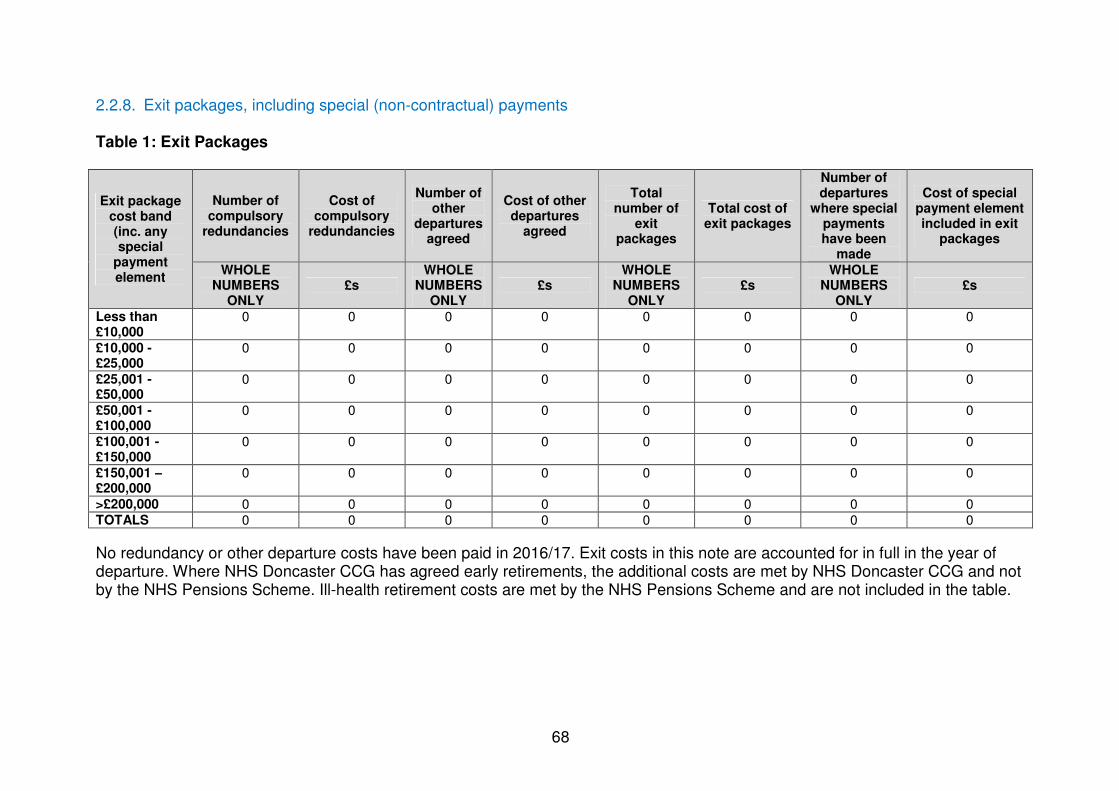
68
2.2.8. Exit packages, including special (non-contractual) payments Table 1: Exit Packages
Exit package cost band (inc. any special
payment element
Number of compulsory
redundancies
Cost of compulsory
redundancies
Number of other
departures agreed
Cost of other departures
agreed
Total number of
exit packages
Total cost of exit packages
Number of departures
where special payments have been
made
Cost of special payment element included in exit
packages
WHOLE NUMBERS
ONLY £s
WHOLE NUMBERS
ONLY £s
WHOLE NUMBERS
ONLY £s
WHOLE NUMBERS
ONLY £s
Less than £10,000
0 0 0 0 0 0 0 0
£10,000 - £25,000
0 0 0 0 0 0 0 0
£25,001 - £50,000
0 0 0 0 0 0 0 0
£50,001 - £100,000
0 0 0 0 0 0 0 0
£100,001 - £150,000
0 0 0 0 0 0 0 0
£150,001 –£200,000
0 0 0 0 0 0 0 0
>£200,000 0 0 0 0 0 0 0 0 TOTALS 0 0 0 0 0 0 0 0
No redundancy or other departure costs have been paid in 2016/17. Exit costs in this note are accounted for in full in the year of departure. Where NHS Doncaster CCG has agreed early retirements, the additional costs are met by NHS Doncaster CCG and not by the NHS Pensions Scheme. Ill-health retirement costs are met by the NHS Pensions Scheme and are not included in the table.

69
Table 2: Analysis of Other Departures Agreements Total Value of agreements Number £000s Voluntary redundancies including early retirement contractual costs
0 0
Mutually agreed resignations (MARS) contractual costs
0 0
Early retirements in the efficiency of the service contractual costs
0 0
Contractual payments in lieu of notice*
0 0
Exit payments following Employment Tribunals or court orders
0 0
Non-contractual payments requiring HMT approval**
0 0
TOTAL 0 0
As a single exit package can be made up of several components each of which will be counted separately in this Note, the total number above will not necessarily match the total numbers in Note 4.4 which will be the number of individuals. *any non-contractual payments in lieu of notice are disclosed under “non-contracted payments requiring HMT approval” below. **includes any non-contractual severance payment made following judicial mediation, and X (list amounts) relating to non-contractual payments in lieu of notice. No non-contractual payments were made to individuals where the payment value was more than 12 months’ of their annual salary. The Remuneration Report includes disclosure of exit packages payable to individuals named in that Report.
Mrs Jackie Pederson Accountable Officer 25 May 2017

70
3. Parliamentary Accountability and Audit Report NHS Doncaster CCG is not required to produce a Parliamentary Accountability and Audit Report. Disclosures on remote contingent liabilities, losses and special payments, gifts, and fees and charges are included as notes in the Financial Statements of this report at Page 80 onwards. An audit certificate and report is also included in this Annual Report at Page 72.
71
ANNUAL ACCOUNTS
Mrs Jackie Pederson Accountable Officer 25 May 2017

saraha
Rectangle

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Page Number
The Primary Statements:
Statement of Comprehensive Net Expenditure for the year ended 31st March 2017 76
Statement of Financial Position as at 31st March 2017 77
Statement of Changes in Taxpayers' Equity for the year ended 31st March 2017 78
Statement of Cash Flows for the year ended 31st March 2017 79
Notes to the Accounts
Accounting policies 80
Other operating revenue 86
Revenue 86
Employee benefits and staff numbers 87
Operating expenses 91
Better payment practice code 92
Income generation activities 92
Investment revenue 92
Other gains and losses 92
Finance costs 92
Net gain/(loss) on transfer by absorption 93
Operating leases 93
Property, plant and equipment 94
Intangible non-current assets 96
Investment property 96
Inventories 96
Trade and other receivables 97
Other financial assets 97
Other current assets 97
Cash and cash equivalents 98
Non-current assets held for sale 98
Analysis of impairments and reversals 98
Trade and other payables 99
Other financial liabilities 99
Borrowings 99
Private finance initiative, LIFT and other service concession arrangements 99
Finance lease obligations 99
Finance lease receivables 99
Provisions 100
Contingencies 100
Commitments 100
Financial instruments 100
Operating segments 102
Pooled budgets 102
NHS Lift investments 102
Intra-government and other balances 103
Related party transactions 104
Events after the end of the reporting period 105
Losses and special payments 105
Third party assets 105
Financial performance targets 105
Impact of IFRS 105
Analysis of charitable reserves 105
CONTENTS
75
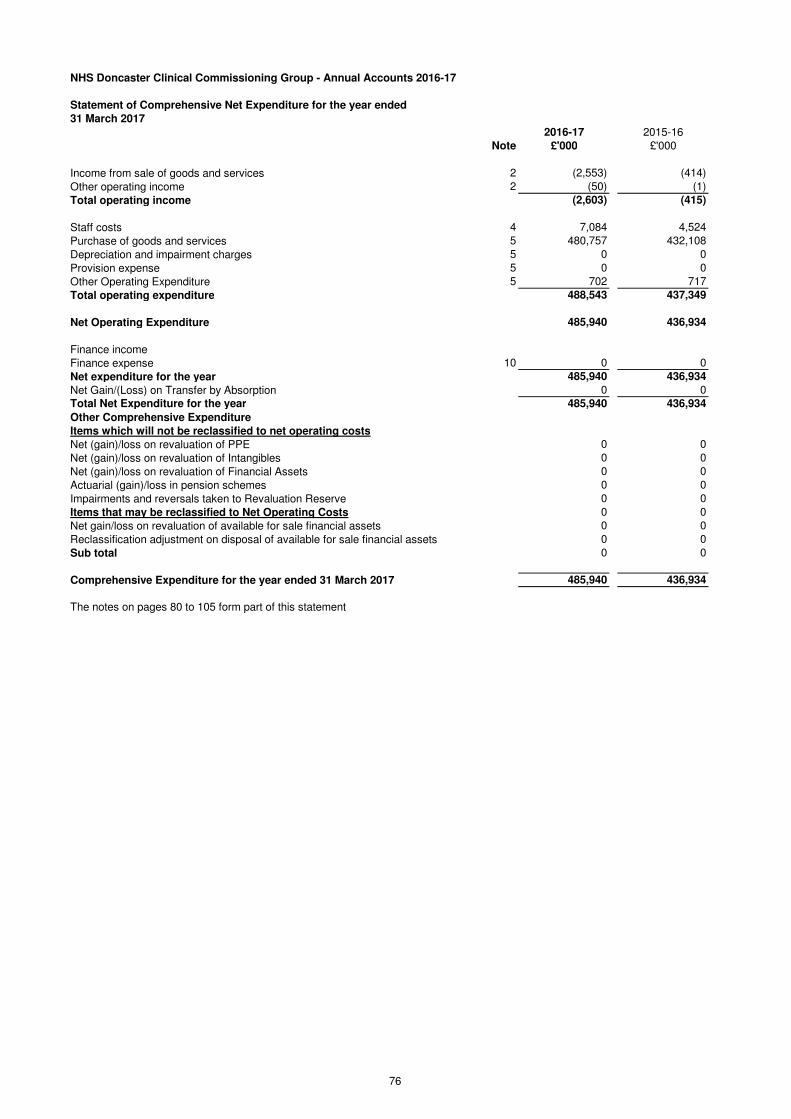
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Statement of Comprehensive Net Expenditure for the year ended
31 March 2017
2016-17 2015-16
Note £'000 £'000
Income from sale of goods and services 2 (2,553) (414)
Other operating income 2 (50) (1)
Total operating income (2,603) (415)
Staff costs 4 7,084 4,524
Purchase of goods and services 5 480,757 432,108
Depreciation and impairment charges 5 0 0
Provision expense 5 0 0
Other Operating Expenditure 5 702 717
Total operating expenditure 488,543 437,349
Net Operating Expenditure 485,940 436,934
Finance income
Finance expense 10 0 0
Net expenditure for the year 485,940 436,934
Net Gain/(Loss) on Transfer by Absorption 0 0
Total Net Expenditure for the year 485,940 436,934
Other Comprehensive Expenditure
Items which will not be reclassified to net operating costs
Net (gain)/loss on revaluation of PPE 0 0
Net (gain)/loss on revaluation of Intangibles 0 0
Net (gain)/loss on revaluation of Financial Assets 0 0
Actuarial (gain)/loss in pension schemes 0 0
Impairments and reversals taken to Revaluation Reserve 0 0
Items that may be reclassified to Net Operating Costs 0 0
Net gain/loss on revaluation of available for sale financial assets 0 0
Reclassification adjustment on disposal of available for sale financial assets 0 0
Sub total 0 0
Comprehensive Expenditure for the year ended 31 March 2017 485,940 436,934
The notes on pages 80 to 105 form part of this statement
76

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Statement of Financial Position as at
31 March 2017
2016-17 2015-16
Note £'000 £'000
Non-current assets:
Property, plant and equipment 13 0 0
Intangible assets 14 0 0
Investment property 15 0 0
Trade and other receivables 17 0 0
Other financial assets 18 0 0
Total non-current assets 0 0
Current assets:
Inventories 16 0 0
Trade and other receivables 17 3,696 3,330
Other financial assets 18 0 0
Other current assets 19 0 0
Cash and cash equivalents 20 36 3
Total current assets 3,732 3,333
Non-current assets held for sale 21 0 0
Total current assets 3,732 3,333
Total assets 3,732 3,333
Current liabilities
Trade and other payables 23 (33,949) (28,654)
Other financial liabilities 24 0 0
Other liabilities 25 0 0
Borrowings 26 0 0
Provisions 30 0 0
Total current liabilities (33,949) (28,654)
Non-Current Assets plus/less Net Current Assets/Liabilities (30,217) (25,321)
Non-current liabilities
Trade and other payables 23 0 0
Other financial liabilities 24 0 0
Other liabilities 25 0 0
Borrowings 26 0 0
Provisions 30 0 0
Total non-current liabilities 0 0
Assets less Liabilities (30,217) (25,321)
Financed by Taxpayers’ Equity
General fund (30,217) (25,321)
Revaluation reserve 0 0
Other reserves 0 0
Charitable Reserves 0 0
Total taxpayers' equity: (30,217) (25,321)
The notes on pages 80 to 105 form part of this statement
The financial statements on pages 76 to 105 were approved by the Governing Body on 25 May 2017 and signed on its behalf by:
Chief Accountable Officer
Jackie Pederson
77
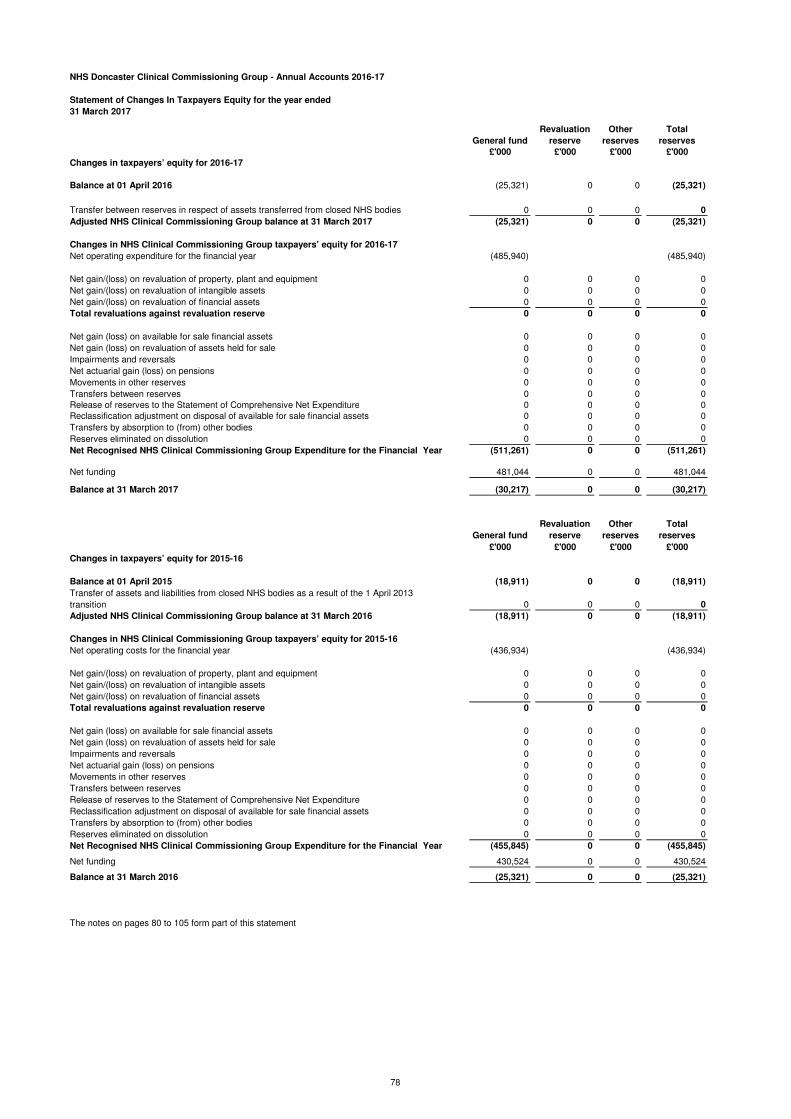
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Statement of Changes In Taxpayers Equity for the year ended
31 March 2017
General fund
Revaluation
reserve
Other
reserves
Total
reserves
£'000 £'000 £'000 £'000
Changes in taxpayers’ equity for 2016-17
Balance at 01 April 2016 (25,321) 0 0 (25,321)
Transfer between reserves in respect of assets transferred from closed NHS bodies 0 0 0 0
Adjusted NHS Clinical Commissioning Group balance at 31 March 2017 (25,321) 0 0 (25,321)
Changes in NHS Clinical Commissioning Group taxpayers’ equity for 2016-17
Net operating expenditure for the financial year (485,940) (485,940)
Net gain/(loss) on revaluation of property, plant and equipment 0 0 0 0
Net gain/(loss) on revaluation of intangible assets 0 0 0 0
Net gain/(loss) on revaluation of financial assets 0 0 0 0
Total revaluations against revaluation reserve 0 0 0 0
Net gain (loss) on available for sale financial assets 0 0 0 0
Net gain (loss) on revaluation of assets held for sale 0 0 0 0
Impairments and reversals 0 0 0 0
Net actuarial gain (loss) on pensions 0 0 0 0
Movements in other reserves 0 0 0 0
Transfers between reserves 0 0 0 0
Release of reserves to the Statement of Comprehensive Net Expenditure 0 0 0 0
Reclassification adjustment on disposal of available for sale financial assets 0 0 0 0
Transfers by absorption to (from) other bodies 0 0 0 0
Reserves eliminated on dissolution 0 0 0 0
Net Recognised NHS Clinical Commissioning Group Expenditure for the Financial Year (511,261) 0 0 (511,261)
Net funding 481,044 0 0 481,044
Balance at 31 March 2017 (30,217) 0 0 (30,217)
General fund
Revaluation
reserve
Other
reserves
Total
reserves
£'000 £'000 £'000 £'000
Changes in taxpayers’ equity for 2015-16
Balance at 01 April 2015 (18,911) 0 0 (18,911)
Transfer of assets and liabilities from closed NHS bodies as a result of the 1 April 2013
transition 0 0 0 0
Adjusted NHS Clinical Commissioning Group balance at 31 March 2016 (18,911) 0 0 (18,911)
Changes in NHS Clinical Commissioning Group taxpayers’ equity for 2015-16
Net operating costs for the financial year (436,934) (436,934)
Net gain/(loss) on revaluation of property, plant and equipment 0 0 0 0
Net gain/(loss) on revaluation of intangible assets 0 0 0 0
Net gain/(loss) on revaluation of financial assets 0 0 0 0
Total revaluations against revaluation reserve 0 0 0 0
Net gain (loss) on available for sale financial assets 0 0 0 0
Net gain (loss) on revaluation of assets held for sale 0 0 0 0
Impairments and reversals 0 0 0 0
Net actuarial gain (loss) on pensions 0 0 0 0
Movements in other reserves 0 0 0 0
Transfers between reserves 0 0 0 0
Release of reserves to the Statement of Comprehensive Net Expenditure 0 0 0 0
Reclassification adjustment on disposal of available for sale financial assets 0 0 0 0
Transfers by absorption to (from) other bodies 0 0 0 0
Reserves eliminated on dissolution 0 0 0 0
Net Recognised NHS Clinical Commissioning Group Expenditure for the Financial Year (455,845) 0 0 (455,845)
Net funding 430,524 0 0 430,524
Balance at 31 March 2016 (25,321) 0 0 (25,321)
The notes on pages 80 to 105 form part of this statement
78

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Statement of Cash Flows for the year ended
31 March 2017
2016-17 2015-16
Note £'000 £'000
Cash Flows from Operating Activities
Net operating expenditure for the financial year 5 (485,940) (436,934)
Depreciation and amortisation 0 0
Impairments and reversals 0 0
Movement due to transfer by Modified Absorption 0 0
Other gains (losses) on foreign exchange 0 0
Donated assets received credited to revenue but non-cash 0 0
Government granted assets received credited to revenue but non-cash 0 0
Interest paid 0 0
Release of PFI deferred credit 0 0
Other Gains & Losses 0 0
Finance Costs 0 0
Unwinding of Discounts 0 0
(Increase)/decrease in inventories 0 0
(Increase)/decrease in trade & other receivables 17 (366) 1,244
(Increase)/decrease in other current assets 0 0
Increase/(decrease) in trade & other payables 23 5,295 5,460
Increase/(decrease) in other current liabilities 0 0
Provisions utilised 0 0
Increase/(decrease) in provisions 0 0
Net Cash Inflow (Outflow) from Operating Activities (481,011) (430,230)
Cash Flows from Investing Activities
Interest received 0 0
(Payments) for property, plant and equipment 0 0
(Payments) for intangible assets 0 0
(Payments) for investments with the Department of Health 0 0
(Payments) for other financial assets 0 0
(Payments) for financial assets (LIFT) 0 0
Proceeds from disposal of assets held for sale: property, plant and equipment 0 0
Proceeds from disposal of assets held for sale: intangible assets 0 0
Proceeds from disposal of investments with the Department of Health 0 0
Proceeds from disposal of other financial assets 0 0
Proceeds from disposal of financial assets (LIFT) 0 0
Loans made in respect of LIFT 0 0
Loans repaid in respect of LIFT 0 0
Rental revenue 0 0
Net Cash Inflow (Outflow) from Investing Activities 0 0
Net Cash Inflow (Outflow) before Financing (481,011) (430,230)
Cash Flows from Financing Activities
Grant in Aid Funding Received 481,044 430,524
Other loans received 0 0
Other loans repaid 0 0
Capital element of payments in respect of finance leases and on Statement of Financial Position PFI and LIFT 0 0
Capital grants and other capital receipts 0 0
Capital receipts surrendered 0 0
Net Cash Inflow (Outflow) from Financing Activities 481,044 430,524
Net Increase (Decrease) in Cash & Cash Equivalents 20 33 294
Cash & Cash Equivalents at the Beginning of the Financial Year 3 (291)
Effect of exchange rate changes on the balance of cash and cash equivalents held in foreign currencies 0 0
Cash & Cash Equivalents (including bank overdrafts) at the End of the Financial Year 36 3
The notes on pages 80 to 105 form part of this statement
79
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Notes to the financial statements
1 Accounting Policies
NHS England has directed that the financial statements of clinical commissioning groups shall meet the accounting requirements of the Group
Accounting Manual issued by the Department of Health. Consequently, the following financial statements have been prepared in accordance with
the Group Accounting Manual 2016-17 issued by the Department of Health. The accounting policies contained in the Group Accounting Manual
follow International Financial Reporting Standards to the extent that they are meaningful and appropriate to clinical commissioning groups, as
determined by HM Treasury, which is advised by the Financial Reporting Advisory Board. Where the Group Accounting Manual permits a choice
of accounting policy, the accounting policy which is judged to be most appropriate to the particular circumstances of the clinical commissioning
group for the purpose of giving a true and fair view has been selected. The particular policies adopted by the clinical commissioning group are
described below. They have been applied consistently in dealing with items considered material in relation to the accounts.
1.1 Going Concern
These accounts have been prepared on the going concern basis (despite the issue of a report to the Secretary of State for Health under Section
30 of the Local Audit and Accountability Act 2014).
Public sector bodies are assumed to be going concerns where the continuation of the provision of a service in the future is anticipated, as
evidenced by inclusion of financial provision for that service in published documents.
Where a clinical commissioning group ceases to exist, it considers whether or not its services will continue to be provided (using the same assets,
by another public sector entity) in determining whether to use the concept of going concern for the final set of Financial Statements. If services will
continue to be provided the financial statements are prepared on the going concern basis.
1.2 Accounting Convention
These accounts have been prepared under the historical cost convention modified to account for the revaluation of property, plant and equipment,
intangible assets, inventories and certain financial assets and financial liabilities.
1.3 Acquisitions & Discontinued OperationsActivities are considered to be ‘acquired’ only if they are taken on from outside the public sector. Activities are considered to be ‘discontinued’ only
if they cease entirely. They are not considered to be ‘discontinued’ if they transfer from one public sector body to another.
1.4 Movement of Assets within the Department of Health Group
Transfers as part of reorganisation fall to be accounted for by use of absorption accounting in line with the Government Financial Reporting
Manual, issued by HM Treasury. The Government Financial Reporting Manual does not require retrospective adoption, so prior year transactions
(which have been accounted for under merger accounting) have not been restated. Absorption accounting requires that entities account for their
transactions in the period in which they took place, with no restatement of performance required when functions transfer within the public sector.
Where assets and liabilities transfer, the gain or loss resulting is recognised in the Statement of Comprehensive Net Expenditure, and is disclosed
separately from operating costs.
Other transfers of assets and liabilities within the Department of Health Group are accounted for in line with IAS 20 and similarly give rise to
income and expenditure entries.
1.5 Charitable Funds
NHS Doncaster CCG did not hold any Charitable Funds during 2016-17.
1.6 Pooled Budgets
Where the clinical commissioning group has entered into a pooled budget arrangement under Section 75 of the National Health Service Act 2006
the clinical commissioning group accounts for its share of the assets, liabilities, income and expenditure arising from the activities of the pooled
budget, identified in accordance with the pooled budget agreement.
If the clinical commissioning group is in a “jointly controlled operation”, the clinical commissioning group recognises:
· The assets the clinical commissioning group controls;
· The liabilities the clinical commissioning group incurs;
· The expenses the clinical commissioning group incurs; and,
· The clinical commissioning group’s share of the income from the pooled budget activities.
If the clinical commissioning group is involved in a “jointly controlled assets” arrangement, in addition to the above, the clinical commissioning
group recognises:
· The clinical commissioning group’s share of the jointly controlled assets (classified according to the nature of the assets);
· The clinical commissioning group’s share of any liabilities incurred jointly; and,
· The clinical commissioning group’s share of the expenses jointly incurred.
1.7 Critical Accounting Judgements & Key Sources of Estimation Uncertainty
In the application of the clinical commissioning group’s accounting policies, management is required to make judgements, estimates and
assumptions about the carrying amounts of assets and liabilities that are not readily apparent from other sources. The estimates and associated
assumptions are based on historical experience and other factors that are considered to be relevant. Actual results may differ from those
estimates and the estimates and underlying assumptions are continually reviewed. Revisions to accounting estimates are recognised in the period
in which the estimate is revised if the revision affects only that period or in the period of the revision and future periods if the revision affects both
current and future periods.
1.7.1 Critical Judgements in Applying Accounting Policies
The following are the critical judgements, apart from those involving estimations (see below) that management has made in the process of
applying the clinical commissioning group’s accounting policies that have the most significant effect on the amounts recognised in the financial
statements:
Operating lease commitments - NHS Doncaster CCG has in substance, several property lease arrangements with NHS Property Services Ltd. It
has been determined that as NHS Doncaster CCG has not obtained substantially all the risks and rewards of ownership of these properties, the
leases have been classified as operating leases and accounted for accordingly.
1.7.2 Key Sources of Estimation Uncertainty
The following are the key estimations that management has made in the process of applying the clinical commissioning group’s accounting
policies that have the most significant effect on the amounts recognised in the financial statements:
Basis of estimation of key accruals - the CCG has included certain accruals within the financial statements which are estimates. The key areas
requiring estimation are Healthcare contracts with main providers (these are based on the estimated activity and performance data outstanding as
at 31st March 2017 and agreed through the Agreement of Balances Process), Continuing Healthcare (based on patient activity information held on
the CCG's database, not yet invoiced) and Prescribing (based on the profile of estimated prescriptions dispensed, not yet charged by the BSA
which approximately equates to two month's worth of activity).
1.8 Revenue
Revenue in respect of services provided is recognised when, and to the extent that, performance occurs, and is measured at the fair value of the
consideration receivable.
Where income is received for a specific activity that is to be delivered in the following year, that income is deferred.
80

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Notes to the financial statements
1.9 Employee Benefits
1.9.1 Short-term Employee Benefits
Salaries, wages and employment-related payments are recognised in the period in which the service is received from employees, including
bonuses earned but not yet taken.
The cost of leave earned but not taken by employees at the end of the period is recognised in the financial statements to the extent that
employees are permitted to carry forward leave into the following period.
1.9.2 Retirement Benefit Costs
Past and present employees are covered by the provisions of the NHS Pensions Scheme. The scheme is an unfunded, defined benefit scheme
that covers NHS employers, General Practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The
scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities.
Therefore, the scheme is accounted for as if it were a defined contribution scheme: the cost to the clinical commissioning group of participating in
the scheme is taken as equal to the contributions payable to the scheme for the accounting period.For early retirements other than those due to ill health the additional pension liabilities are not funded by the scheme. The full amount of the liability
for the additional costs is charged to expenditure at the time the clinical commissioning group commits itself to the retirement, regardless of the
method of payment.
1.10 Other Expenses
Other operating expenses are recognised when, and to the extent that, the goods or services have been received. They are measured at the fair
value of the consideration payable.
Expenses and liabilities in respect of grants are recognised when the clinical commissioning group has a present legal or constructive obligation,
which occurs when all of the conditions attached to the payment have been met.
1.11 Property, Plant & Equipment
1.11.1 Recognition
Property, plant and equipment is capitalised if:
· It is held for use in delivering services or for administrative purposes;
· It is probable that future economic benefits will flow to, or service potential will be supplied to the clinical commissioning group;
· It is expected to be used for more than one financial year;
· The cost of the item can be measured reliably; and,
· The item has a cost of at least £5,000; or,
· Collectively, a number of items have a cost of at least £5,000 and individually have a cost of more than £250, where the assets are
functionally interdependent, they had broadly simultaneous purchase dates, are anticipated to have simultaneous disposal dates and are under
single managerial control; or,
· Items form part of the initial equipping and setting-up cost of a new building, ward or unit, irrespective of their individual or collective
cost.
Where a large asset, for example a building, includes a number of components with significantly different asset lives, the components are treated
as separate assets and depreciated over their own useful economic lives.
1.11.2 Valuation
All property, plant and equipment are measured initially at cost, representing the cost directly attributable to acquiring or constructing the asset and
bringing it to the location and condition necessary for it to be capable of operating in the manner intended by management. All assets are
measured subsequently at valuation.
Land and buildings used for the clinical commissioning group’s services or for administrative purposes are stated in the statement of financial
position at their re-valued amounts, being the fair value at the date of revaluation less any impairment.
Revaluations are performed with sufficient regularity to ensure that carrying amounts are not materially different from those that would be
determined at the end of the reporting period. Fair values are determined as follows:
· Land and non-specialised buildings – market value for existing use; and,
· Specialised buildings – depreciated replacement cost.
HM Treasury has adopted a standard approach to depreciated replacement cost valuations based on modern equivalent assets and, where it
would meet the location requirements of the service being provided, an alternative site can be valued.
Properties in the course of construction for service or administration purposes are carried at cost, less any impairment loss. Cost includes
professional fees but not borrowing costs, which are recognised as expenses immediately, as allowed by IAS 23 for assets held at fair value.
Assets are re-valued and depreciation commences when they are brought into use.
Fixtures and equipment are carried at depreciated historic cost as this is not considered to be materially different from current value in existing
use.
An increase arising on revaluation is taken to the revaluation reserve except when it reverses an impairment for the same asset previously
recognised in expenditure, in which case it is credited to expenditure to the extent of the decrease previously charged there. A revaluation
decrease that does not result from a loss of economic value or service potential is recognised as an impairment charged to the revaluation
reserve to the extent that there is a balance on the reserve for the asset and, thereafter, to expenditure. Impairment losses that arise from a clear
consumption of economic benefit are taken to expenditure. Gains and losses recognised in the revaluation reserve are reported as other
comprehensive income in the Statement of Comprehensive Net Expenditure.
1.11.3 Subsequent Expenditure
Where subsequent expenditure enhances an asset beyond its original specification, the directly attributable cost is capitalised. Where subsequent
expenditure restores the asset to its original specification, the expenditure is capitalised and any existing carrying value of the item replaced is
written-out and charged to operating expenses.
81

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Notes to the financial statements
1.12 Intangible Assets
1.12.1 Recognition
Intangible assets are non-monetary assets without physical substance, which are capable of sale separately from the rest of the clinical
commissioning group’s business or which arise from contractual or other legal rights. They are recognised only:
· When it is probable that future economic benefits will flow to, or service potential be provided to, the clinical commissioning group;
· Where the cost of the asset can be measured reliably; and,
· Where the cost is at least £5,000.
Intangible assets acquired separately are initially recognised at fair value. Software that is integral to the operating of hardware, for example an
operating system, is capitalised as part of the relevant item of property, plant and equipment. Software that is not integral to the operation of
hardware, for example application software, is capitalised as an intangible asset. Expenditure on research is not capitalised but is recognised as
an operating expense in the period in which it is incurred. Internally-generated assets are recognised if, and only if, all of the following have been
demonstrated:
· The technical feasibility of completing the intangible asset so that it will be available for use;
· The intention to complete the intangible asset and use it;
· The ability to sell or use the intangible asset;
· How the intangible asset will generate probable future economic benefits or service potential;
· The availability of adequate technical, financial and other resources to complete the intangible asset and sell or use it; and,
· The ability to measure reliably the expenditure attributable to the intangible asset during its development.
1.12.2 Measurement
The amount initially recognised for internally-generated intangible assets is the sum of the expenditure incurred from the date when the criteria
above are initially met. Where no internally-generated intangible asset can be recognised, the expenditure is recognised in the period in which it is
incurred.Following initial recognition, intangible assets are carried at current value in existing use by reference to an active market, or, where no active
market exists, at the lower of depreciated replacement cost or the value in use where the asset is income generating . Internally-developed
software is held at historic cost to reflect the opposing effects of increases in development costs and technological advances.
1.13 Depreciation, Amortisation & Impairments
Freehold land, properties under construction, and assets held for sale are not depreciated.
Otherwise, depreciation and amortisation are charged to write off the costs or valuation of property, plant and equipment and intangible non-
current assets, less any residual value, over their estimated useful lives, in a manner that reflects the consumption of economic benefits or service
potential of the assets. The estimated useful life of an asset is the period over which the clinical commissioning group expects to obtain economic
benefits or service potential from the asset. This is specific to the clinical commissioning group and may be shorter than the physical life of the
asset itself. Estimated useful lives and residual values are reviewed each year end, with the effect of any changes recognised on a prospective
basis. Assets held under finance leases are depreciated over their estimated useful lives.
At each reporting period end, the clinical commissioning group checks whether there is any indication that any of its tangible or intangible non-
current assets have suffered an impairment loss. If there is indication of an impairment loss, the recoverable amount of the asset is estimated to
determine whether there has been a loss and, if so, its amount. Intangible assets not yet available for use are tested for impairment annually.
A revaluation decrease that does not result from a loss of economic value or service potential is recognised as an impairment charged to the
revaluation reserve to the extent that there is a balance on the reserve for the asset and, thereafter, to expenditure. Impairment losses that arise
from a clear consumption of economic benefit are taken to expenditure. Where an impairment loss subsequently reverses, the carrying amount of
the asset is increased to the revised estimate of the recoverable amount but capped at the amount that would have been determined had there
been no initial impairment loss. The reversal of the impairment loss is credited to expenditure to the extent of the decrease previously charged
there and thereafter to the revaluation reserve.
1.14 Donated AssetsDonated non-current assets are capitalised at their fair value on receipt, with a matching credit to Income. They are valued, depreciated and
impaired as described above for purchased assets. Gains and losses on revaluations, impairments and sales are as described above for
purchased assets. Deferred income is recognised only where conditions attached to the donation preclude immediate recognition of the gain.
1.15 Government Grants
The value of assets received by means of a government grant are credited directly to income. Deferred income is recognised only where
conditions attached to the grant preclude immediate recognition of the gain.
1.16 Non-current Assets Held For Sale
Non-current assets are classified as held for sale if their carrying amount will be recovered principally through a sale transaction rather than
through continuing use. This condition is regarded as met when:
· The sale is highly probable;
· The asset is available for immediate sale in its present condition; and,
· Management is committed to the sale, which is expected to qualify for recognition as a completed sale within one year from the date of
classification.
Non-current assets held for sale are measured at the lower of their previous carrying amount and fair value less costs to sell. Fair value is open
market value including alternative uses.
The profit or loss arising on disposal of an asset is the difference between the sale proceeds and the carrying amount and is recognised in the
Statement of Comprehensive Net Expenditure. On disposal, the balance for the asset on the revaluation reserve is transferred to the general
reserve.
Property, plant and equipment that is to be scrapped or demolished does not qualify for recognition as held for sale. Instead, it is retained as an
operational asset and its economic life is adjusted. The asset is de-recognised when it is scrapped or demolished.
1.17 Leases
Leases are classified as finance leases when substantially all the risks and rewards of ownership are transferred to the lessee. All other leases
are classified as operating leases.
1.17.1 The Clinical Commissioning Group as Lessee
Property, plant and equipment held under finance leases are initially recognised, at the inception of the lease, at fair value or, if lower, at the
present value of the minimum lease payments, with a matching liability for the lease obligation to the lessor. Lease payments are apportioned
between finance charges and reduction of the lease obligation so as to achieve a constant rate on interest on the remaining balance of the liability.
Finance charges are recognised in calculating the clinical commissioning group’s surplus/deficit.
Operating lease payments are recognised as an expense on a straight-line basis over the lease term. Lease incentives are recognised initially as
a liability and subsequently as a reduction of rentals on a straight-line basis over the lease term.
Contingent rentals are recognised as an expense in the period in which they are incurred.
Where a lease is for land and buildings, the land and building components are separated and individually assessed as to whether they are
operating or finance leases.
82

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Notes to the financial statements
1.17.2 The Clinical Commissioning Group as Lessor
Amounts due from lessees under finance leases are recorded as receivables at the amount of the clinical commissioning group’s net investment
in the leases. Finance lease income is allocated to accounting periods so as to reflect a constant periodic rate of return on the clinical
commissioning group’s net investment outstanding in respect of the leases.
Rental income from operating leases is recognised on a straight-line basis over the term of the lease. Initial direct costs incurred in negotiating and
arranging an operating lease are added to the carrying amount of the leased asset and recognised on a straight-line basis over the lease term.
1.18 Private Finance Initiative Transactions
NHS Doncaster CCG did not have any PFI transactions during 2016-17
1.19 Inventories
NHS Doncaster did not have any inventories during 2016-17
1.20 Cash & Cash Equivalents
Cash is cash in hand and deposits with any financial institution repayable without penalty on notice of not more than 24 hours. Cash equivalents
are investments that mature in 3 months or less from the date of acquisition and that are readily convertible to known amounts of cash with
insignificant risk of change in value.
In the Statement of Cash Flows, cash and cash equivalents are shown net of bank overdrafts that are repayable on demand and that form an
integral part of the clinical commissioning group’s cash management.
1.21 Provisions
Provisions are recognised when the clinical commissioning group has a present legal or constructive obligation as a result of a past event, it is
probable that the clinical commissioning group will be required to settle the obligation, and a reliable estimate can be made of the amount of the
obligation. The amount recognised as a provision is the best estimate of the expenditure required to settle the obligation at the end of the reporting
period, taking into account the risks and uncertainties. Where a provision is measured using the cash flows estimated to settle the obligation, its
carrying amount is the present value of those cash flows using HM Treasury’s discount rate as follows:
· Timing of cash flows (0 to 5 years inclusive): Minus 2.70% (previously: minus 1.55%)
· Timing of cash flows (6 to 10 years inclusive): Minus 1.95% (previously: minus 1.%)
· Timing of cash flows (over 10 years): Minus 0.80% (previously: minus 0.80%)
When some or all of the economic benefits required to settle a provision are expected to be recovered from a third party, the receivable is
recognised as an asset if it is virtually certain that reimbursements will be received and the amount of the receivable can be measured reliably.
A restructuring provision is recognised when the clinical commissioning group has developed a detailed formal plan for the restructuring and has
raised a valid expectation in those affected that it will carry out the restructuring by starting to implement the plan or announcing its main features
to those affected by it. The measurement of a restructuring provision includes only the direct expenditures arising from the restructuring, which are
those amounts that are both necessarily entailed by the restructuring and not associated with on-going activities of the entity.
1.22 Clinical Negligence Costs
The NHS Litigation Authority operates a risk pooling scheme under which the clinical commissioning group pays an annual contribution to the NHS
Litigation Authority which in return settles all clinical negligence claims. The contribution is charged to expenditure. Although the NHS Litigation
Authority is administratively responsible for all clinical negligence cases the legal liability remains with the clinical commissioning group.
1.23 Non-clinical Risk Pooling
The clinical commissioning group participates in the Property Expenses Scheme and the Liabilities to Third Parties Scheme. Both are risk pooling
schemes under which the clinical commissioning group pays an annual contribution to the NHS Litigation Authority and, in return, receives
assistance with the costs of claims arising. The annual membership contributions, and any excesses payable in respect of particular claims are
charged to operating expenses as and when they become due.
1.24 Continuing Healthcare Risk PoolingIn 2014-15 a risk pool scheme was introduced by NHS England for continuing healthcare claims, for claim periods prior to 31 March 2013. Under
the scheme clinical commissioning group contribute annually to a pooled fund, which is used to settle the claims.
1.25 Carbon Reduction Commitment SchemeCarbon Reduction Commitment and similar allowances are accounted for as government grant funded intangible assets if they are not expected to
be realised within twelve months, and otherwise as other current assets. They are valued at open market value. As the clinical commissioning
group makes emissions, a provision is recognised with an offsetting transfer from deferred income. The provision is settled on surrender of the
allowances. The asset, provision and deferred income amounts are valued at fair value at the end of the reporting period.
1.26 Contingencies
A contingent liability is a possible obligation that arises from past events and whose existence will be confirmed only by the occurrence or non-
occurrence of one or more uncertain future events not wholly within the control of the clinical commissioning group, or a present obligation that is
not recognised because it is not probable that a payment will be required to settle the obligation or the amount of the obligation cannot be
measured sufficiently reliably. A contingent liability is disclosed unless the possibility of a payment is remote.
A contingent asset is a possible asset that arises from past events and whose existence will be confirmed by the occurrence or non-occurrence of
one or more uncertain future events not wholly within the control of the clinical commissioning group. A contingent asset is disclosed where an
inflow of economic benefits is probable.
Where the time value of money is material, contingencies are disclosed at their present value.
1.27 Financial Assets
Financial assets are recognised when the clinical commissioning group becomes party to the financial instrument contract or, in the case of trade
receivables, when the goods or services have been delivered. Financial assets are derecognised when the contractual rights have expired or the
asset has been transferred.
Financial assets are classified into the following categories:
· Financial assets at fair value through profit and loss;
· Held to maturity investments;
· Available for sale financial assets; and,
· Loans and receivables.
The classification depends on the nature and purpose of the financial assets and is determined at the time of initial recognition.
1.27.1 Financial Assets at Fair Value Through Profit and Loss
Embedded derivatives that have different risks and characteristics to their host contracts, and contracts with embedded derivatives whose
separate value cannot be ascertained, are treated as financial assets at fair value through profit and loss. They are held at fair value, with any
resultant gain or loss recognised in calculating the clinical commissioning group’s surplus or deficit for the year. The net gain or loss incorporates
any interest earned on the financial asset.
NHS Doncaster CCG did not hold any embedded derivatives during 2016-17.
83
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Notes to the financial statements
1.27.2 Held to Maturity Assets
Held to maturity investments are non-derivative financial assets with fixed or determinable payments and fixed maturity, and there is a positive
intention and ability to hold to maturity. After initial recognition, they are held at amortised cost using the effective interest method, less any
impairment. Interest is recognised using the effective interest method.
1.27.3 Available For Sale Financial Assets
Available for sale financial assets are non-derivative financial assets that are designated as available for sale or that do not fall within any of the
other three financial asset classifications. They are measured at fair value with changes in value taken to the revaluation reserve, with the
exception of impairment losses. Accumulated gains or losses are recycled to surplus/deficit on de-recognition.
NHS Doncaster does not hold any Available For Sale Financial Assets during 2016-17.
1.27.4 Loans & Receivables
Loans and receivables are non-derivative financial assets with fixed or determinable payments which are not quoted in an active market. After
initial recognition, they are measured at amortised cost using the effective interest method, less any impairment. Interest is recognised using the
effective interest method.
Fair value is determined by reference to quoted market prices where possible, otherwise by valuation techniques.
[Disclose valuation techniques as appropriate.]
The effective interest rate is the rate that exactly discounts estimated future cash receipts through the expected life of the financial asset, to the
initial fair value of the financial asset.
At the end of the reporting period, the clinical commissioning group assesses whether any financial assets, other than those held at ‘fair value
through profit and loss’ are impaired. Financial assets are impaired and impairment losses recognised if there is objective evidence of impairment
as a result of one or more events which occurred after the initial recognition of the asset and which has an impact on the estimated future cash
flows of the asset.
For financial assets carried at amortised cost, the amount of the impairment loss is measured as the difference between the asset’s carrying
amount and the present value of the revised future cash flows discounted at the asset’s original effective interest rate. The loss is recognised in
expenditure and the carrying amount of the asset is reduced through a provision for impairment of receivables.
If, in a subsequent period, the amount of the impairment loss decreases and the decrease can be related objectively to an event occurring after
the impairment was recognised, the previously recognised impairment loss is reversed through expenditure to the extent that the carrying amount
of the receivable at the date of the impairment is reversed does not exceed what the amortised cost would have been had the impairment not
been recognised.
1.28 Financial Liabilities
Financial liabilities are recognised on the statement of financial position when the clinical commissioning group becomes party to the contractual
provisions of the financial instrument or, in the case of trade payables, when the goods or services have been received. Financial liabilities are de-
recognised when the liability has been discharged, that is, the liability has been paid or has expired.
1.28.1 Financial Guarantee Contract Liabilities
Financial guarantee contract liabilities are subsequently measured at the higher of:
· The premium received (or imputed) for entering into the guarantee less cumulative amortisation; and,
· The amount of the obligation under the contract, as determined in accordance with IAS 37: Provisions, Contingent Liabilities and
Contingent Assets.
1.28.2 Financial Liabilities at Fair Value Through Profit and Loss
Embedded derivatives that have different risks and characteristics to their host contracts, and contracts with embedded derivatives whose
separate value cannot be ascertained, are treated as financial liabilities at fair value through profit and loss. They are held at fair value, with any
resultant gain or loss recognised in the clinical commissioning group’s surplus/deficit. The net gain or loss incorporates any interest payable on the
financial liability.
NHS Doncaster CCG did not hold any embedded derivatives during 2016-17.
1.28.3 Other Financial Liabilities
After initial recognition, all other financial liabilities are measured at amortised cost using the effective interest method, except for loans from
Department of Health, which are carried at historic cost. The effective interest rate is the rate that exactly discounts estimated future cash
payments through the life of the asset, to the net carrying amount of the financial liability. Interest is recognised using the effective interest method.
1.29 Value Added Tax
Most of the activities of the clinical commissioning group are outside the scope of VAT and, in general, output tax does not apply and input tax on
purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of
fixed assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT.
1.3 Foreign Currencies
The clinical commissioning group’s functional currency and presentational currency is sterling. Transactions denominated in a foreign currency are
translated into sterling at the exchange rate ruling on the dates of the transactions. At the end of the reporting period, monetary items denominated
in foreign currencies are retranslated at the spot exchange rate on 31 March. Resulting exchange gains and losses for either of these are
recognised in the clinical commissioning group’s surplus/deficit in the period in which they arise.
1.31 Third Party Assets
NHS Doncaster CCG did not hold any third party assets during 2016-17.
1.32 Losses & Special PaymentsLosses and special payments are items that Parliament would not have contemplated when it agreed funds for the health service or passed
legislation. By their nature they are items that ideally should not arise. They are therefore subject to special control procedures compared with the
generality of payments. They are divided into different categories, which govern the way that individual cases are handled.
Losses and special payments are charged to the relevant functional headings in expenditure on an accruals basis, including losses which would
have been made good through insurance cover had the clinical commissioning group not been bearing its own risks (with insurance premiums
then being included as normal revenue expenditure).
1.33 Subsidiaries
NHS Doncaster CCG did not have any subsidiaries during 2016-17.
1.34 Associates
NHS Doncaster CCG did not have any associates during 2016-17.
1.35 Joint Ventures
NHS Doncaster CCG did not have any joint ventures during 2016-17.
1.36 Joint Operations
Joint operations are activities undertaken by the clinical commissioning group in conjunction with one or more other parties but which are not
performed through a separate entity. The clinical commissioning group records its share of the income and expenditure; gains and losses; assets
and liabilities; and cash flows.
1.37 Research & Development
NHS Doncaster CCG did not undertake any research or development during 2016-17.
84

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Notes to the financial statements
1.38 Accounting Standards That Have Been Issued But Have Not Yet Been Adopted
The Government Financial Reporting Manual does not require the following Standards and Interpretations to be applied in 2016-17, all of which
are subject to consultation:
· IFRS 9: Financial Instruments ( application from 1 January 2018)
· IFRS 14: Regulatory Deferral Accounts ( not applicable to DH groups bodies)
· IFRS 15: Revenue for Contract with Customers (application from 1 January 2018)
· IFRS 16: Leases (application from 1 January 2019)
The application of the Standards as revised would not have a material impact on the accounts for 2016-17, were they applied in that year.
85
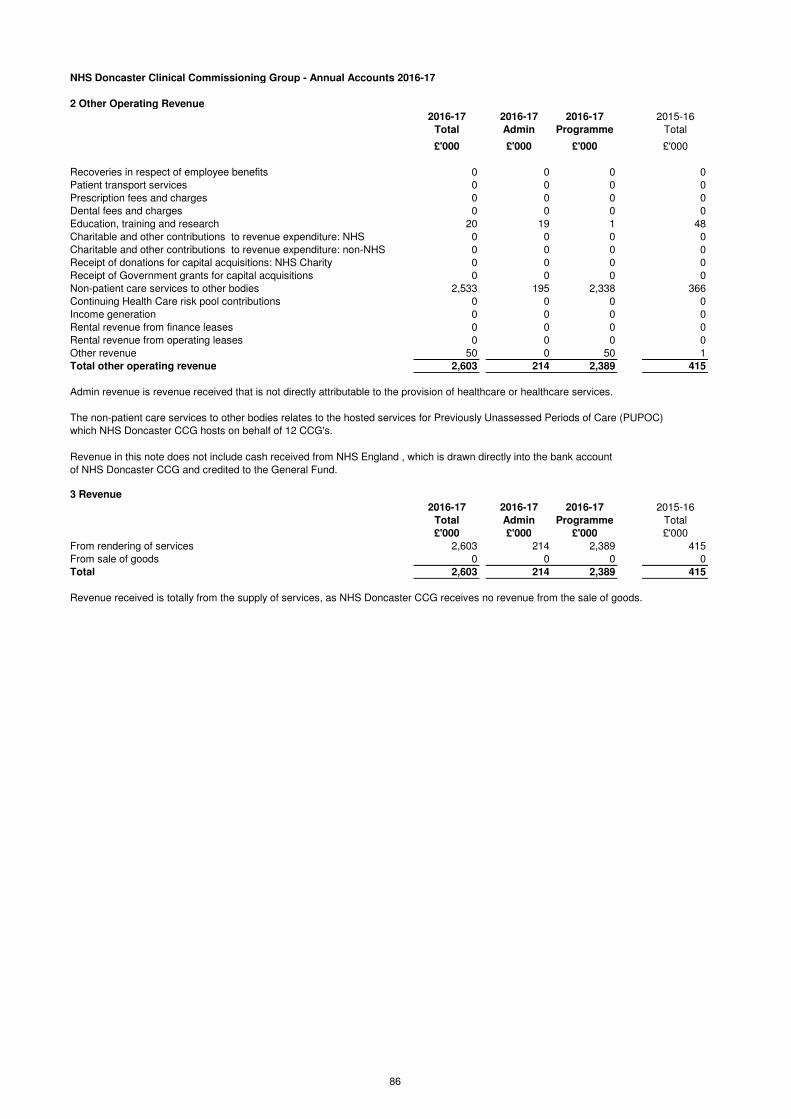
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
2 Other Operating Revenue
2016-17 2016-17 2016-17 2015-16
Total Admin Programme Total
£'000 £'000 £'000 £'000
Recoveries in respect of employee benefits 0 0 0 0
Patient transport services 0 0 0 0
Prescription fees and charges 0 0 0 0
Dental fees and charges 0 0 0 0
Education, training and research 20 19 1 48
Charitable and other contributions to revenue expenditure: NHS 0 0 0 0
Charitable and other contributions to revenue expenditure: non-NHS 0 0 0 0
Receipt of donations for capital acquisitions: NHS Charity 0 0 0 0
Receipt of Government grants for capital acquisitions 0 0 0 0
Non-patient care services to other bodies 2,533 195 2,338 366
Continuing Health Care risk pool contributions 0 0 0 0
Income generation 0 0 0 0
Rental revenue from finance leases 0 0 0 0
Rental revenue from operating leases 0 0 0 0
Other revenue 50 0 50 1
Total other operating revenue 2,603 214 2,389 415
Admin revenue is revenue received that is not directly attributable to the provision of healthcare or healthcare services.
The non-patient care services to other bodies relates to the hosted services for Previously Unassessed Periods of Care (PUPOC)
which NHS Doncaster CCG hosts on behalf of 12 CCG's.
3 Revenue
2016-17 2016-17 2016-17 2015-16
Total Admin Programme Total
£'000 £'000 £'000 £'000
From rendering of services 2,603 214 2,389 415
From sale of goods 0 0 0 0
Total 2,603 214 2,389 415
Revenue received is totally from the supply of services, as NHS Doncaster CCG receives no revenue from the sale of goods.
Revenue in this note does not include cash received from NHS England , which is drawn directly into the bank account
of NHS Doncaster CCG and credited to the General Fund.
86

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
4. Employee benefits and staff numbers
4.1.1 Employee benefits 2016-17
Total
Permanent
Employees Other
£'000 £'000 £'000
Employee Benefits
Salaries and wages 5,820 5,504 316
Social security costs 570 570 0
Employer Contributions to NHS Pension scheme 694 694 0
Other pension costs 0 0 0
Other post-employment benefits 0 0 0
Other employment benefits 0 0 0
Termination benefits 0 0 0
Gross employee benefits expenditure 7,084 6,768 316
Less recoveries in respect of employee benefits (note 4.1.2) 0 0 0
Total - Net admin employee benefits including capitalised costs 7,084 6,768 316
Less: Employee costs capitalised 0 0 0
Net employee benefits excluding capitalised costs 7,084 6,768 316
4.1.1 Employee benefits 2015-16
Total
Permanent
Employees Other
£'000 £'000 £'000
Employee Benefits
Salaries and wages 3,726 3,384 342
Social security costs 306 306 0
Employer Contributions to NHS Pension scheme 462 462 0
Other pension costs 0 0 0
Other post-employment benefits 0 0 0
Other employment benefits 0 0 0
Termination benefits 30 30 0
Gross employee benefits expenditure 4,524 4,182 342
Less recoveries in respect of employee benefits (note 4.1.2) 0 0 0
Total - Net admin employee benefits including capitalised costs 4,524 4,182 342
Less: Employee costs capitalised 0 0 0
Net employee benefits excluding capitalised costs 4,524 4,182 342
The increase in costs between 2015-16 and 2016-17 is due to NHS Doncaster CCG now hosting a PUPOC service (Previously Unassessed
Periods of Care) on behalf of 12 CCG's across the region.
4.1.2 Recoveries in respect of employee benefits 2016-17 2015-16
Total
Permanent
Employees Other Total
£'000 £'000 £'000 £'000
Employee Benefits - Revenue
Salaries and wages 0 0 0 0
Social security costs 0 0 0 0
Employer contributions to the NHS Pension Scheme 0 0 0 0
Other pension costs 0 0 0 0
Other post-employment benefits 0 0 0 0
Other employment benefits 0 0 0 0
Termination benefits 0 0 0 0
Total recoveries in respect of employee benefits 0 0 0 0
Total
Total
87

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
4.2 Average number of people employed
2015-16
Total
Permanently
employed Other Total
Number Number Number Number
Total 166 164 1 93
Of the above:Number of whole time equivalent people engaged
on capital projects 0 0 0 0
The significant increase in the number of people employed in 2016-17 is due to NHS Doncaster CCG hosting the PUPOC service (Previously
Unassessed Periods of Care) on behalf of 12 other CCG's across the region.
4.3 Staff sickness absence and ill health retirements
2016-17 2015-16
Number Number
Total Days Lost 1,091 554
Total Staff Years 166 95
Average working Days Lost 6.57 5.83
2016-17 2015-16
Number Number
Number of persons retired early on ill health grounds 0 0
£'000 £'000
Total additional Pensions liabilities accrued in the year 0 0
Ill health retirement costs are met by the NHS Pension Scheme
4.4 Exit packages agreed in the financial year
Number £ Number £ Number £
Less than £10,000 0 0 0 0 0 0
£10,001 to £25,000 0 0 0 0 0 0
£25,001 to £50,000 0 0 0 0 0 0
£50,001 to £100,000 0 0 0 0 0 0
£100,001 to £150,000 0 0 0 0 0 0
£150,001 to £200,000 0 0 0 0 0 0
Over £200,001 0 0 0 0 0 0Total 0 0 0 0 0 0
Number £ Number £ Number £
Less than £10,000 0 0 0 0 0 0
£10,001 to £25,000 0 0 0 0 0 0
£25,001 to £50,000 0 0 1 29,704 1 29,704
£50,001 to £100,000 0 0 0 0 0 0
£100,001 to £150,000 0 0 0 0 0 0
£150,001 to £200,000 0 0 0 0 0 0
Over £200,001 0 0 0 0 0 0
Total 0 0 1 29,704 1 29,704
Number £ Number £
Less than £10,000 0 0 0 0
£10,001 to £25,000 0 0 0 0
£25,001 to £50,000 0 0 0 0
£50,001 to £100,000 0 0 0 0
£100,001 to £150,000 0 0 0 0
£150,001 to £200,000 0 0 0 0
Over £200,001 0 0 0 0Total 0 0 0 0
2016-17
Compulsory redundancies Other agreed departures Total
Departures where special
payments have been made
2015-16 2015-16
Departures where special
payments have been made
2015-162016-17
Total
The Staff Sickness Absence rate is calculated by the Health and Social Information Centre. The Sickness Absence rate is
calculated by dividing the sum total sickness absence days (including non-working days) by the sum total days available per
month for each member of staff. The data is based on January to December 2016.
2016-17 2016-17 2016-17
Other agreed departuresCompulsory redundancies
2015-16
88

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Analysis of Other Agreed Departures
Number £ Number £
Voluntary redundancies including early retirement contractual costs 0 0 0 0
Mutually agreed resignations (MARS) contractual costs 0 0 0 0
Early retirements in the efficiency of the service contractual costs 0 0 0 0
Contractual payments in lieu of notice 0 0 1 29,704
Exit payments following Employment Tribunals or court orders 0 0 0 0
Non-contractual payments requiring HMT approval* 0 0 0 0
Total 0 0 1 29,704
2016-17 2015-16
Where the CCG has agreed early retirements, the additional costs are met by NHS the CCG and not by the NHS Pension Scheme, and are included in the
tables. Ill-health retirement costs are met by the NHS Pension Scheme and are not included in the tables.
The Remuneration Report includes the disclosure of exit payments payable to individuals named in that Report.
Other agreed departures Other agreed departures
* As a single exit package can be made up of several components each of which will be counted separately in this table, the total number will not necessarily
match the total number in the table above, which will be the number of individuals.
These tables report the number and value of exit packages agreed in the financial year. The expense associated with these departures may have been
recognised in part or in full in a previous period.
Redundancy and other departure costs have been paid in accordance with the provisions of the Agenda For Change Scheme
Exit costs are accounted for in accordance with relevant accounting standards and at the latest in full in the year of departure.
89

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
4.5 Pension costs
Past and present employees are covered by the provisions of the NHS Pension Scheme. Details of the benefits payable under these
provisions can be found on the NHS Pensions website at www.nhsbsa.nhs.uk/Pensions.
The Scheme is an unfunded, defined benefit scheme that covers NHS employers, GP practices and other bodies, allowed under the
direction of the Secretary of State, in England and Wales. The Scheme is not designed to be run in a way that would enable NHS
bodies to identify their share of the underlying scheme assets and liabilities.
Therefore, the Scheme is accounted for as if it were a defined contribution scheme: the cost to the clinical commissioning group of
participating in the Scheme is taken as equal to the contributions payable to the Scheme for the accounting period.
The Scheme is subject to a full actuarial valuation every four years (until 2004, every five years) and an accounting valuation every
year. An outline of these follows:
4.5.1 Full actuarial (funding) valuation
The purpose of this valuation is to assess the level of liability in respect of the benefits due under the Scheme (taking into account its
recent demographic experience), and to recommend the contribution rates to be paid by employers and scheme members. The last
such valuation, which determined current contribution rates was undertaken as at 31 March 2012 and covered the period from 1 April
2008 to that date. Details can be found on the pension scheme website at www.nhsbsa.nhs.uk/pensions.
For 2016-17, employers’ contributions of £694,000 were payable to the NHS Pensions Scheme (2015-16: £462,000) at the rate of
14.3% of pensionable pay. The scheme’s actuary reviews employer contributions, usually every four years and now based on HMT
Valuation Directions, following a full scheme valuation. The latest review used data from 31 March 2012 and was published on the
Government website on 9 June 2014. These costs are included in the NHS pension line of note 4.1.
90
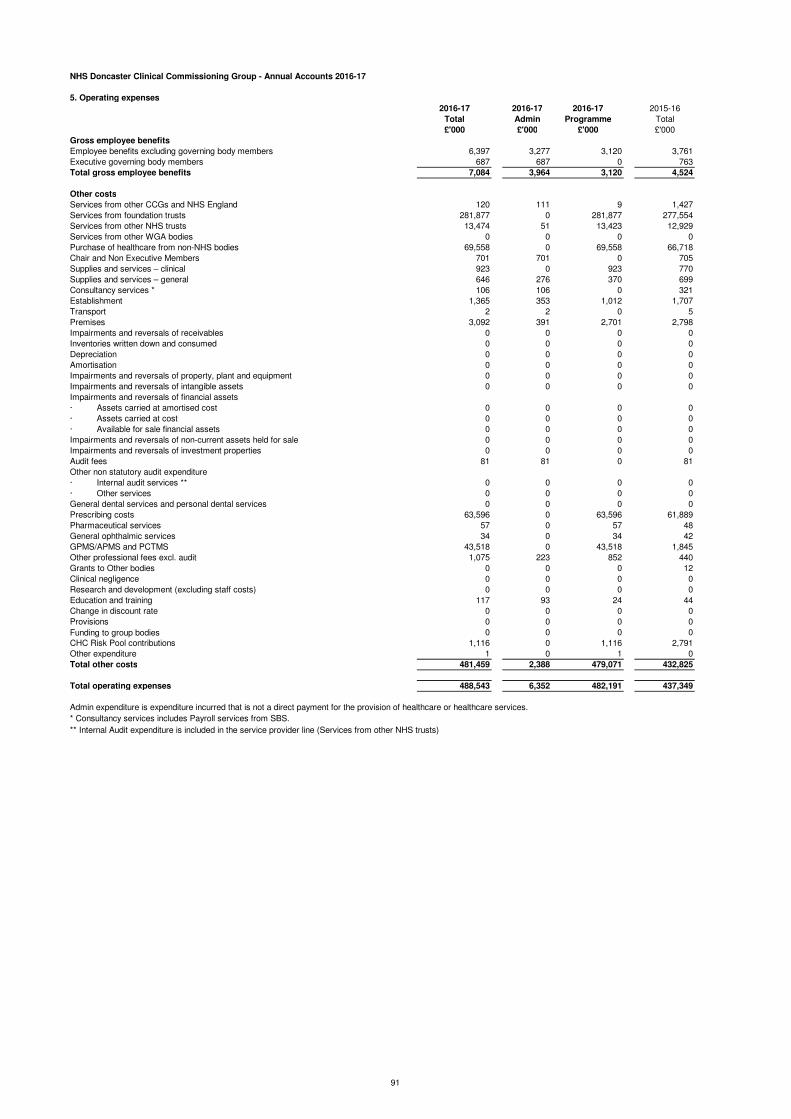
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
5. Operating expenses
2016-17 2016-17 2016-17 2015-16
Total Admin Programme Total
£'000 £'000 £'000 £'000
Gross employee benefits
Employee benefits excluding governing body members 6,397 3,277 3,120 3,761
Executive governing body members 687 687 0 763
Total gross employee benefits 7,084 3,964 3,120 4,524
Other costs
Services from other CCGs and NHS England 120 111 9 1,427
Services from foundation trusts 281,877 0 281,877 277,554
Services from other NHS trusts 13,474 51 13,423 12,929
Services from other WGA bodies 0 0 0 0
Purchase of healthcare from non-NHS bodies 69,558 0 69,558 66,718
Chair and Non Executive Members 701 701 0 705
Supplies and services – clinical 923 0 923 770
Supplies and services – general 646 276 370 699
Consultancy services * 106 106 0 321
Establishment 1,365 353 1,012 1,707
Transport 2 2 0 5
Premises 3,092 391 2,701 2,798
Impairments and reversals of receivables 0 0 0 0
Inventories written down and consumed 0 0 0 0
Depreciation 0 0 0 0
Amortisation 0 0 0 0
Impairments and reversals of property, plant and equipment 0 0 0 0
Impairments and reversals of intangible assets 0 0 0 0
Impairments and reversals of financial assets
· Assets carried at amortised cost 0 0 0 0
· Assets carried at cost 0 0 0 0
· Available for sale financial assets 0 0 0 0
Impairments and reversals of non-current assets held for sale 0 0 0 0
Impairments and reversals of investment properties 0 0 0 0
Audit fees 81 81 0 81
Other non statutory audit expenditure
· Internal audit services ** 0 0 0 0
· Other services 0 0 0 0
General dental services and personal dental services 0 0 0 0
Prescribing costs 63,596 0 63,596 61,889
Pharmaceutical services 57 0 57 48
General ophthalmic services 34 0 34 42
GPMS/APMS and PCTMS 43,518 0 43,518 1,845
Other professional fees excl. audit 1,075 223 852 440
Grants to Other bodies 0 0 0 12
Clinical negligence 0 0 0 0
Research and development (excluding staff costs) 0 0 0 0
Education and training 117 93 24 44
Change in discount rate 0 0 0 0
Provisions 0 0 0 0
Funding to group bodies 0 0 0 0
CHC Risk Pool contributions 1,116 0 1,116 2,791
Other expenditure 1 0 1 0
Total other costs 481,459 2,388 479,071 432,825
Total operating expenses 488,543 6,352 482,191 437,349
* Consultancy services includes Payroll services from SBS.
** Internal Audit expenditure is included in the service provider line (Services from other NHS trusts)
Admin expenditure is expenditure incurred that is not a direct payment for the provision of healthcare or healthcare services.
91

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
6.1 Better Payment Practice Code
Measure of compliance 2016-17 2016-17 2015-16 2015-16
Number £'000 Number £'000
Non-NHS Payables
Total Non-NHS Trade invoices paid in the Year 16,565 118,229 16,893 72,422
Total Non-NHS Trade Invoices paid within target 16,337 116,523 16,742 72,213Percentage of Non-NHS Trade invoices paid within target 98.62% 98.56% 99.11% 99.71%
NHS Payables
Total NHS Trade Invoices Paid in the Year 3,042 301,930 2,998 293,243
Total NHS Trade Invoices Paid within target 2,962 301,674 2,949 292,634Percentage of NHS Trade Invoices paid within target 97.37% 99.92% 98.37% 99.79%
6.2 The Late Payment of Commercial Debts (Interest) Act 1998 2016-17 2015-16
£'000 £'000
Amounts included in finance costs from claims made under this legislation 0 0
Compensation paid to cover debt recovery costs under this legislation 0 0Total 0 0
7 Income Generation Activities
NHS Doncaster CCG had no income generation activities during 2016-17.
8. Investment revenue
NHS Doncaster CCG did not have any investment income in 2016-17.
9. Other gains and losses
NHS Doncaster CCG did not have any gains and losses in 2016-17.
10. Finance costs
NHS Doncaster CCG did not have any finance costs in 2016-17.
92
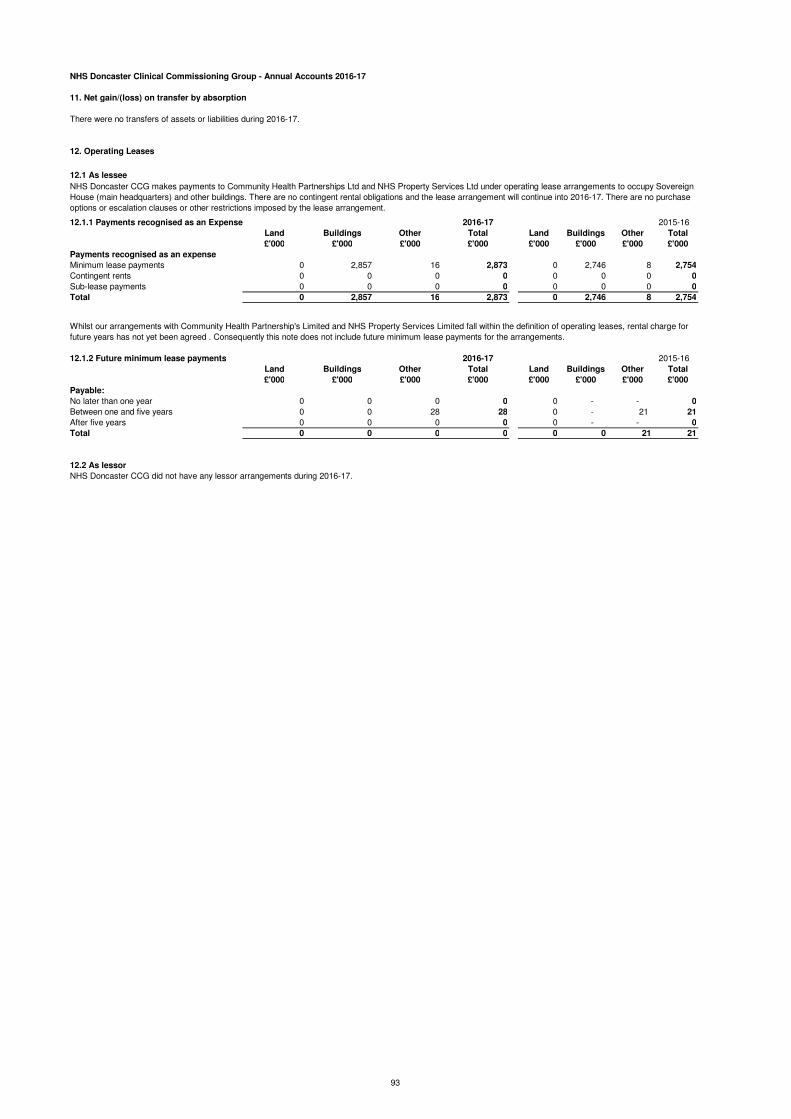
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
11. Net gain/(loss) on transfer by absorption
There were no transfers of assets or liabilities during 2016-17.
12. Operating Leases
12.1 As lessee
12.1.1 Payments recognised as an Expense 2016-17 2015-16
Land Buildings Other Total Land Buildings Other Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Payments recognised as an expense
Minimum lease payments 0 2,857 16 2,873 0 2,746 8 2,754
Contingent rents 0 0 0 0 0 0 0 0
Sub-lease payments 0 0 0 0 0 0 0 0
Total 0 2,857 16 2,873 0 2,746 8 2,754
12.1.2 Future minimum lease payments 2016-17 2015-16
Land Buildings Other Total Land Buildings Other Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Payable:
No later than one year 0 0 0 0 0 - - 0
Between one and five years 0 0 28 28 0 - 21 21
After five years 0 0 0 0 0 - - 0
Total 0 0 0 0 0 0 21 21
12.2 As lessor
NHS Doncaster CCG did not have any lessor arrangements during 2016-17.
NHS Doncaster CCG makes payments to Community Health Partnerships Ltd and NHS Property Services Ltd under operating lease arrangements to occupy Sovereign
House (main headquarters) and other buildings. There are no contingent rental obligations and the lease arrangement will continue into 2016-17. There are no purchase
options or escalation clauses or other restrictions imposed by the lease arrangement.
Whilst our arrangements with Community Health Partnership's Limited and NHS Property Services Limited fall within the definition of operating leases, rental charge for
future years has not yet been agreed . Consequently this note does not include future minimum lease payments for the arrangements.
93

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
13 Property, plant and equipment
2016-17 Land
Buildings
excluding
dwellings Dwellings
Assets under
construction and
payments on
account
Plant &
machinery
Transport
equipment
Information
technology
Furniture &
fittings Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Cost or valuation at 01 April 2016 0 0 0 0 6 0 32 0 38
Addition of assets under construction and payments on account 0 0
Additions purchased 0 0 0 0 0 0 0 0 0
Additions donated 0 0 0 0 0 0 0 0 0
Additions government granted 0 0 0 0 0 0 0 0 0
Additions leased 0 0 0 0 0 0 0 0 0
Reclassifications 0 0 0 0 0 0 0 0 0
Reclassified as held for sale and reversals 0 0 0 0 0 0 0 0 0
Disposals other than by sale 0 0 0 0 0 0 0 0 0
Upward revaluation gains 0 0 0 0 0 0 0 0 0
Impairments charged 0 0 0 0 0 0 0 0 0
Reversal of impairments 0 0 0 0 0 0 0 0 0
Transfer (to)/from other public sector body 0 0 0 0 0 0 0 0 0
Cumulative depreciation adjustment following revaluation 0 0 0 0 0 0 0 0 0
Cost/Valuation at 31 March 2017 0 0 0 0 6 0 32 0 38
Depreciation 01 April 2016 0 0 0 0 6 0 32 0 38
Reclassifications 0 0 0 0 0 0 0 0 0
Reclassified as held for sale and reversals 0 0 0 0 0 0 0 0 0
Disposals other than by sale 0 0 0 0 0 0 0 0 0
Upward revaluation gains 0 0 0 0 0 0 0 0 0
Impairments charged 0 0 0 0 0 0 0 0 0
Reversal of impairments 0 0 0 0 0 0 0 0 0
Charged during the year 0 0 0 0 0 0 0 0 0
Transfer (to)/from other public sector body 0 0 0 0 0 0 0 0 0
Cumulative depreciation adjustment following revaluation 0 0 0 0 0 0 0 0 0
Depreciation at 31 March 2017 0 0 0 0 6 0 32 0 38
Net Book Value at 31 March 2017 0 0 0 0 0 0 0 0 0
Purchased 0 0 0 0 0 0 0 0 0
Donated 0 0 0 0 0 0 0 0 0
Government Granted 0 0 0 0 0 0 0 0 0
Total at 31 March 2017 0 0 0 0 0 0 0 0 0
Asset financing:
Owned 0 0 0 0 0 0 0 0 0
Held on finance lease 0 0 0 0 0 0 0 0 0
On-SOFP Lift contracts 0 0 0 0 0 0 0 0 0
PFI residual: interests 0 0 0 0 0 0 0 0 0
Total at 31 March 2017 0 0 0 0 0 0 0 0 0
Revaluation Reserve Balance for Property, Plant & Equipment
Land Buildings Dwellings
Assets under
construction &
payments on
account
Plant &
machinery
Transport
equipment
Information
technology
Furniture &
fittings Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Balance at 01 April 2016 0 0 0 0 0 0 0 0 0
Revaluation gains 0 0 0 0 0 0 0 0 0
Impairments 0 0 0 0 0 0 0 0 0
Release to general fund 0 0 0 0 0 0 0 0 0
Other movements 0 0 0 0 0 0 0 0 0
Balance at 31 March 2017 0 0 0 0 0 0 0 0 0
94

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
13 Property, plant and equipment cont'd
13.1 Additions to assets under construction
NHS Doncaster CCG did not have any assets under construction in 2016-17.
13.2 Donated assets
NHS Doncaster CCG did not have any donated assets in 2016-17.
13.3 Government granted assets
NHS Doncaster CCG did not have any government granted assets in 2016-17.
13.4 Property revaluation
NHS Doncaster CCG did not have any property, plant or equipment in 2016-17.
13.5 Compensation from third parties
NHS Doncaster CCG did not receive any compensation from third parties in 2016-17.
13.6 Write downs to recoverable amount
NHS Doncaster CCG did not have any assets written down to recoverable amounts in 2016-17.
13.7 Temporarily idle assets
NHS Doncaster CCG did not have any temporary idle assets in 2016-17.
13.8 Cost or valuation of fully depreciated assets
NHS Doncaster CCG did not have any fully depreciated assets in 2016-17.
13.9 Economic lives
NHS Doncaster CCG did not have any assets in 2016-17.
95

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
14 Intangible non-current assets
NHS Doncaster CCG did not have any intangible assets in 2016-17.
14.1 Donated assets
NHS Doncaster CCG did not have any donated intangible assets in 2016-17.
14.2 Government granted assets
NHS Doncaster CCG did not have any government granted intangible assets in 2016-17.
14.3 Revaluation
NHS Doncaster CCG did not have any intangible assets in 2016-17.
14.4 Compensation from third parties
14.5 Write downs to recoverable amount
NHS Doncaster CCG did have any intangible assets written down to recoverable amounts in 2016-17.
14.6 Non-capitalised assets
NHS Doncaster CCG did not have any non-capitalised intangible assets in 2016-17.
14.7 Temporarily idle assets
NHS Doncaster CCG did not have any temporary idle intangible assets in 2016-17.
14.8 Cost or valuation of fully amortised assets
NHS Doncaster CCG did not have any fully amortised intangible assets in 2016-17.
14.9 Economic lives
NHS Doncaster CCG did not have any intangible assets in 2016-17.
15 Investment property
NHS Doncaster CCG did not have any investment property in 2016-17.
15.1 Investment property transactions
NHS Doncaster CCG did not have any investment property transactions in 2016-17.
16 Inventories
NHS Doncaster CCG did not have any inventories in 2016-17.
NHS Doncaster CCG did not receive any compensation from third parties for intangible assets impaired, lost
or given up in 2016-17.
96
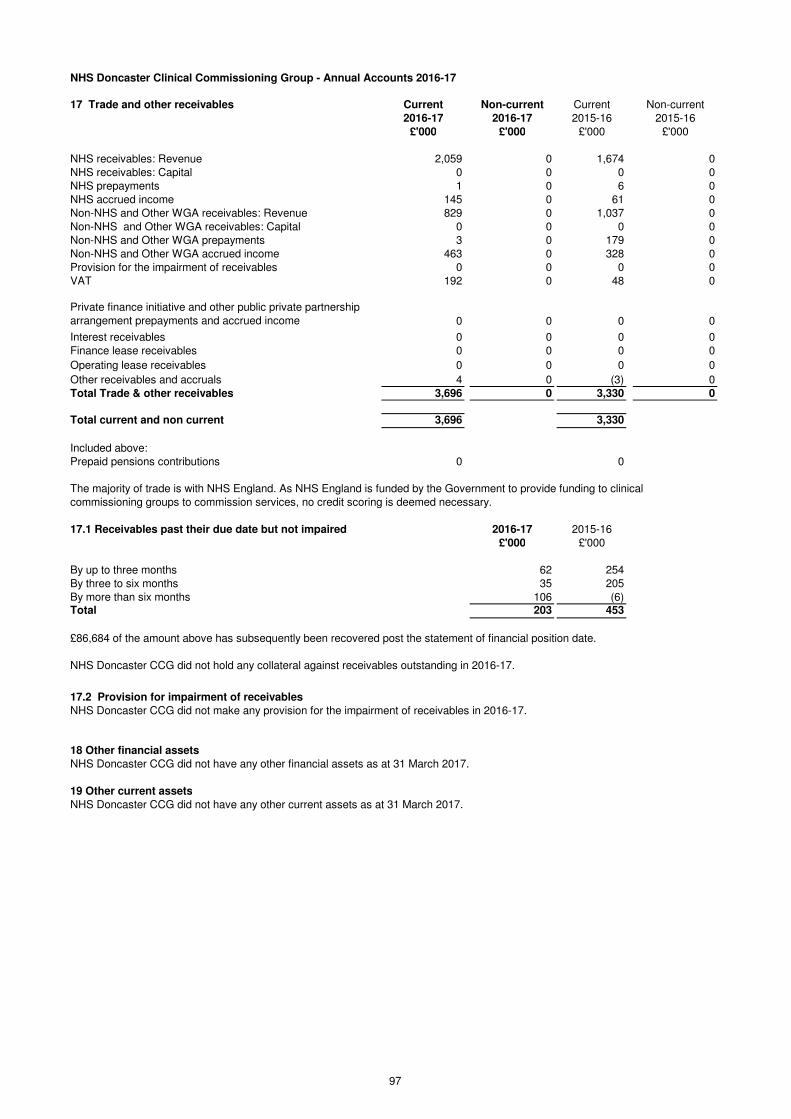
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
17 Trade and other receivables Current Non-current Current Non-current
2016-17 2016-17 2015-16 2015-16
£'000 £'000 £'000 £'000
NHS receivables: Revenue 2,059 0 1,674 0
NHS receivables: Capital 0 0 0 0
NHS prepayments 1 0 6 0
NHS accrued income 145 0 61 0
Non-NHS and Other WGA receivables: Revenue 829 0 1,037 0
Non-NHS and Other WGA receivables: Capital 0 0 0 0
Non-NHS and Other WGA prepayments 3 0 179 0
Non-NHS and Other WGA accrued income 463 0 328 0
Provision for the impairment of receivables 0 0 0 0
VAT 192 0 48 0
Private finance initiative and other public private partnership
arrangement prepayments and accrued income 0 0 0 0
Interest receivables 0 0 0 0
Finance lease receivables 0 0 0 0
Operating lease receivables 0 0 0 0
Other receivables and accruals 4 0 (3) 0
Total Trade & other receivables 3,696 0 3,330 0
Total current and non current 3,696 3,330
Included above:
Prepaid pensions contributions 0 0
17.1 Receivables past their due date but not impaired 2016-17 2015-16
£'000 £'000
By up to three months 62 254
By three to six months 35 205
By more than six months 106 (6)Total 203 453
£86,684 of the amount above has subsequently been recovered post the statement of financial position date.
NHS Doncaster CCG did not hold any collateral against receivables outstanding in 2016-17.
17.2 Provision for impairment of receivables
NHS Doncaster CCG did not make any provision for the impairment of receivables in 2016-17.
18 Other financial assets
NHS Doncaster CCG did not have any other financial assets as at 31 March 2017.
19 Other current assets
NHS Doncaster CCG did not have any other current assets as at 31 March 2017.
The majority of trade is with NHS England. As NHS England is funded by the Government to provide funding to clinical
commissioning groups to commission services, no credit scoring is deemed necessary.
97
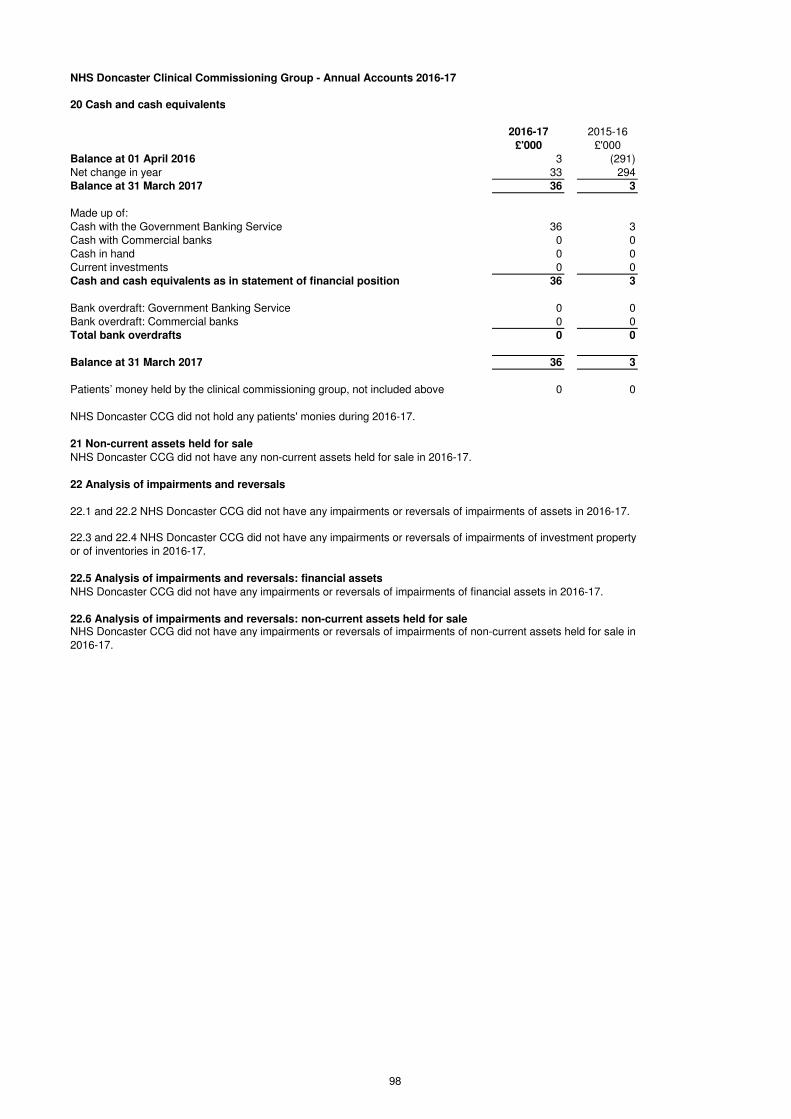
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
20 Cash and cash equivalents
2016-17 2015-16
£'000 £'000
Balance at 01 April 2016 3 (291)
Net change in year 33 294
Balance at 31 March 2017 36 3
Made up of:
Cash with the Government Banking Service 36 3
Cash with Commercial banks 0 0
Cash in hand 0 0
Current investments 0 0
Cash and cash equivalents as in statement of financial position 36 3
Bank overdraft: Government Banking Service 0 0
Bank overdraft: Commercial banks 0 0
Total bank overdrafts 0 0
Balance at 31 March 2017 36 3
Patients’ money held by the clinical commissioning group, not included above 0 0
NHS Doncaster CCG did not hold any patients' monies during 2016-17.
21 Non-current assets held for sale
NHS Doncaster CCG did not have any non-current assets held for sale in 2016-17.
22 Analysis of impairments and reversals
22.5 Analysis of impairments and reversals: financial assets
NHS Doncaster CCG did not have any impairments or reversals of impairments of financial assets in 2016-17.
22.6 Analysis of impairments and reversals: non-current assets held for saleNHS Doncaster CCG did not have any impairments or reversals of impairments of non-current assets held for sale in
2016-17.
22.3 and 22.4 NHS Doncaster CCG did not have any impairments or reversals of impairments of investment property
or of inventories in 2016-17.
22.1 and 22.2 NHS Doncaster CCG did not have any impairments or reversals of impairments of assets in 2016-17.
98

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
Current Non-current Current Non-current
2016-17 2016-17 2015-16 2015-16
£'000 £'000 £'000 £'000
Interest payable 0 0 0 0
NHS payables: revenue 2,896 0 679 0
NHS payables: capital 0 0 0 0
NHS accruals 1,386 0 3,348 0
NHS deferred income 0 0 0 0
Non-NHS and Other WGA payables: Revenue 867 0 1,234 0
Non-NHS and Other WGA payables: Capital 0 0 0 0
Non-NHS and Other WGA accruals 27,845 0 22,726 0
Non-NHS and Other WGA deferred income 0 0 0 0
Social security costs 90 0 79 0
VAT 0 0 0 0
Tax 73 0 74 0
Payments received on account 0 0 0 0
Other payables and accruals 792 0 514 0
Total Trade & Other Payables 33,949 0 28,654 0
Total current and non-current 33,949 28,654
Other payables include £393,886 outstanding pension contributions (including GP pensions) at 31 March 2017
24 Other financial liabilities
NHS Doncaster CCG did not have any other financial liabilities as at 31 March 2017.
25 Other liabilities
NHS Doncaster CCG did not have any other liabilities as at 31 March 2017.
26 Borrowings
NHS Doncaster CCG did not have any borrowings as at 31 March 2017.
27 Private finance initiative, LIFT and other service concession arrangements
NHS Doncaster CCG did not have any private finance initiative, LIFT or other service concession arrangements during 2016-17.
28 Finance lease obligations
NHS Doncaster CCG had no finance lease obligations during 2016-17.
29 Finance lease receivables
NHS Doncaster CCG had no finance lease receivables during 2016-17.
23 Trade and other payables
99
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
30 Provisions
NHS Doncaster CCG had no new provisions arising during 2016-17 and none carried forward from prior years.
31 Contingencies
32 Commitments
NHS Doncaster CCG had no contracted capital commitments or non-cancellable contracts as at 31 March 2017.
33 Financial instruments
33.1 Financial risk management
33.1.1 Currency risk
33.1.2 Interest rate risk
33.1.3 Credit risk
33.1.4 Liquidity risk
NHS Doncaster Clinical Commissioning Group is principally a domestic organisation with the great majority of transactions, assets and
liabilities being in the UK and sterling based. The NHS Clinical Commissioning Group has no overseas operations. The NHS Clinical
Commissioning Group and therefore has low exposure to currency rate fluctuations.
NHS Doncaster CCG borrows from government for capital expenditure, subject to affordability as confirmed by NHS England. The
borrowings are for 1 to 25 years, in line with the life of the associated assets, and interest is charged at the National Loans Fund rate,
fixed for the life of the loan. The CCG therefore has low exposure to interest rate fluctuations.
As the majority of the NHS Doncaster CCG'S revenue comes from parliamentary funding, the CCG has low exposure to credit risk. The
maximum exposures as at the end of the financial year are in receivables from customers, as disclosed in the trade and other
receivables note.
NHS Doncaster CCG is required to operate within revenue and capital resource limits, which are financed from resources voted
annually by Parliament. The CCG draws down cash to cover expenditure, as the need arises. The CCG is not, therefore, exposed to
significant liquidity risks.
Under the Accounts Direction issued by NHS England on 12 February 2014, NHS England is responsible for accounting for liabilities
relating to NHS Continuing Healthcare claims relating to periods of care before the establishment of the CCG. However, the legal
liability remains with the CCG. All claims have now reached an eligibility decision, however as a number of these have been appealed
a contingency has been provided for by NHS England on behalf of the CCG. The value of this is £1,386,000 as at 31 March 2017.
Financial reporting standard IFRS 7 requires disclosure of the role that financial instruments have had during the period in creating or
changing the risks a body faces in undertaking its activities.
As NHS Doncaster CCG is financed through parliamentary funding, it is not exposed to the degree of financial risk faced by business
entities. Also, financial instruments play a much more limited role in creating or changing risk than would be typical of listed companies,
to which the financial reporting standards mainly apply. The CCG has limited powers to borrow or invest surplus funds and financial
assets and liabilities are generated by day-to-day operational activities rather than being held to change the risks facing the clinical
commissioning group in undertaking its activities.
Treasury management operations are carried out by the finance department, within parameters defined formally within the CCG's
Standing Financial Instructions and policies agreed by the Governing Body. Treasury activity is subject to review by the CCG and its
internal auditors.
100
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
33 Financial instruments cont'd
33.2 Financial assets
At ‘fair value
through profit and
loss’
Loans and
Receivables
Available for
Sale Total
2016-17 2016-17 2016-17 2016-17
£'000 £'000 £'000 £'000
Embedded derivatives 0 0 0 0
Receivables:
· NHS 0 2,204 0 2,204
· Non-NHS 0 1,292 0 1,292
Cash at bank and in hand 0 36 0 36
Other financial assets 0 4 0 4
Total at 31 March 2017 0 3,536 0 3,536
At ‘fair value
through profit and
loss’
Loans and
Receivables
Available for
Sale Total
2015-16 2015-16 2015-16 2015-16
£'000 £'000 £'000 £'000
Embedded derivatives 0 0 0 0
Receivables:
· NHS 0 1,734 0 1,734
· Non-NHS 0 1,365 0 1,365
Cash at bank and in hand 0 3 0 3
Other financial assets 0 (2) 0 (2)
Total at 31 March 2016 0 3,100 0 3,100
33.3 Financial liabilities
At ‘fair value
through profit and
loss’ Other Total
2016-17 2016-17 2016-17
£'000 £'000 £'000
Embedded derivatives 0 0 0
Payables:
· NHS 0 4,282 4,282
· Non-NHS 0 29,503 29,503
Private finance initiative, LIFT and finance lease obligations 0 0 0
Other borrowings 0 0 0
Other financial liabilities 0 0 0
Total at 31 March 2017 0 33,785 33,785
The financial liabilities existing as at 31 March 2017 all mature in less than one year.
At ‘fair value
through profit and
loss’ Other Total
2015-16 2015-16 2015-16
£'000 £'000 £'000
Embedded derivatives 0 0 0
Payables:
· NHS 0 4,027 4,027
· Non-NHS 0 24,474 24,474
Private finance initiative, LIFT and finance lease obligations 0 0 0
Other borrowings 0 0 0
Other financial liabilities 0 0 0
Total at 31 March 2016 0 28,501 28,501
101
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
34 Operating segments
NHS Doncaster CCG considers that it has only one operating segment: commissioning of healthcare services.
35 Pooled budgets
2016-17 2015-16£'000 £'000
Income 23,907 22,079
Expenditure (23,907) (22,079)
0 0
The CCG had a section 75 in place during 2016-17 with the Local Authority (Doncaster Metropolitan Borough Council) in relation to
the Better Care Fund. The Better Care Fund totalled £24 million and was made up as follows -
2016-17 2015-16
£'000 £'000
CCG Contribution - in CCG allocation 14,902 15,159
DMBC Contribution - in CCG allocation 7,040 6,920
Disabled Facilities Grant - direct allocation to DMBC 1,124 1,244
Social Care Capital grant - direct allocation to DMBC 841 841
Total Allocation 23,907 24,164
The allocation has been utilised as per the table below -
Area of Spend £'000
People are independent with good health and wellbeing 4,572
When in need of care / or support it is personalised flexible & appropriate 4,322
Where people are in urgent need of care or crisis, there will be responsive
services that meet their needs14,722
Enablers 79
Programme Management 212
Total Spend 23,907
£22m was included in the CCG's allocation and £2m was given directly to the Local Authority. The
CCG passed £7.0m to the Local Authority for them to pay providers directly in relation to the contracts
held by them. The CCG retained £15m which it utilised on its own contracts. There were no jointly
commissioned contracts which both parties contributed to.
The Local Authority accounts for its spend in its own financial systems and the CCG accounts for
its own spend within its financial systems. A joint monitoring arrangement exists for the
whole Better Care Fund which both parties feed into.
36 NHS Lift investments
NHS Doncaster CCG had no NHS LIFT investments during 2016-17.
The NHS Clinical Commissioning Group shares of the income and expenditure handled by the pooled budget in the financial year were:
102
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
37 Intra-government and other balances Current
Receivables
Non-current
Receivables
Current
Payables
Non-current
Payables
2016-17 2016-17 2016-17 2016-17
£000 £000 £000 £000
Balances with:
· Other Central Government bodies 50 0 77 0
· Local Authorities 827 0 2,040 0
Balances with NHS bodies:
· NHS bodies outside the Departmental Group 0 0 0 0
· NHS bodies within the NHS England Group 404 0 91 0
· NHS Trusts and Foundation Trusts 1,801 0 4,191 0
Total of balances with NHS bodies: 2,205 0 4,282 0
· Public corporations and trading funds 0 0 0 0
· Bodies external to Government 614 0 27,550 0
Total balances at 31-March-2017 3,696 0 33,949 0
Current
Receivables
Non-current
Receivables
Current
Payables
Non-current
Payables
2015-16 2015-16 2015-16 2015-16
£000 £000 £000 £000
Balances with:
· Other Central Government bodies 0 0 383 0
· Local Authorities 855 0 100 0
· NHS bodies outside the Departmental Group 125 0 0 0
· NHS bodies within the NHS England Group 633 0 383 0
· NHS Trusts and Foundation Trusts 983 0 3,644 0
· Public corporations and trading funds 0 0 0 0
· Bodies external to Government 734 0 24,144 0
Total balances at 31 March 2016 3,330 0 28,654 0
103

NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
38 Related party transactions
Payments to
Related Party
Receipts
from
Related
Party
Amounts
owed to
Related
Party
Amounts
due from
Related
Party
£'000 £'000 £'000 £'000
Dr D Crichton(Bentley Surgery) 887 0 44 0
Dr Nick Tupper (kingthorne Group Practice)From 5.9.16 696 0 72 0
Dr Nick Tupper (Employed FCMS in Out of Hours)From 5.9.16 3,101 0 23 0
Dr Andrew Oakford(Dr Brown & Partners) 1,342 0 67 0
Dr Andrew Oakford (Employed FCMS in Out of Hours) 5,441 0 23 0
Dr Andrew Oakford (Onehealth) 284 0 0 0
Dr Jeremy Bradley(Dr Simmonite & Partners) 1,474 0 69 0
Dr Pat Barbour(Francis St Medical Centre) 1,223 0 42 0
Dr Pat Barbour (Capsticks) 7 0 103 0
Dr Sam Feeney(Mount Group Practice )To 25.9.16 728 0 82 0
Dr Niki Seddon(Carcroft Drs Group ) 1,101 0 84 0
Dr Marco Pieri(Petersgate Medical Centre) 1,052 0 52 0
Dr Lindsey Britten(Scott Practice) 1,676 0 82 0
Dr Lindsey Britten(Church View Surgery) From 1.2.17 132 0 0 0
Dr Karen Wagstaff(Barnburgh Surgery) 342 0 20 0
Dr Karen Wagstaff(Church View Surgery) From 1.12.16 273 0 0 0
Dr Kaimraj Singh(The Rossington Practice) 1,019 0 59 0
L Tully (Club Doncaster) 60 0 0 0
NHS England 451 -116 0 -313
NHS Sheffield CCG 676 -256 67 -5
Leeds Teaching Hospitals NHS Trust 833 0 41 0
Mid Yorkshire Hospitals NHS Trust 519 0 0 -56
Yorkshire Ambulance Servies NHS Trust 11,088 0 108 0
Barnsley Hospitals NHS Foundastion Trust 458 0 3 0
Doncaster & Bassetlaw NHS Foundation Trust 189,031 0 1,291 -1,450
Northern Lincolnshire & Goole Hospitals NHS Foundation Trust 760 0 0 -45
Rotherham Doncaster & South Humber NHS Foundation Trust 70,483 0 1,065 -54
Sheffield Childrens NHS Foundation Trust 1,777 0 90 0
Sheffield Teaching Hospitals NHS Foundation Trust 14,580 0 745 -30
The Rotherham NHS Foundation Trust 4,583 0 17 -113
NHS Property Services Ltd 394 0 11 0
* Jackie Pederson is a Partner Governor of Doncaster & Bassetlaw Hospitals NHS Foundation Trust
** Dr Niki Seddon (Carcroft Doctors Group) is a Partner Governor of Rotherham Doncaster and South Humber NHS Foundation Trust
Details of related party transactions with individuals are as follows:
104
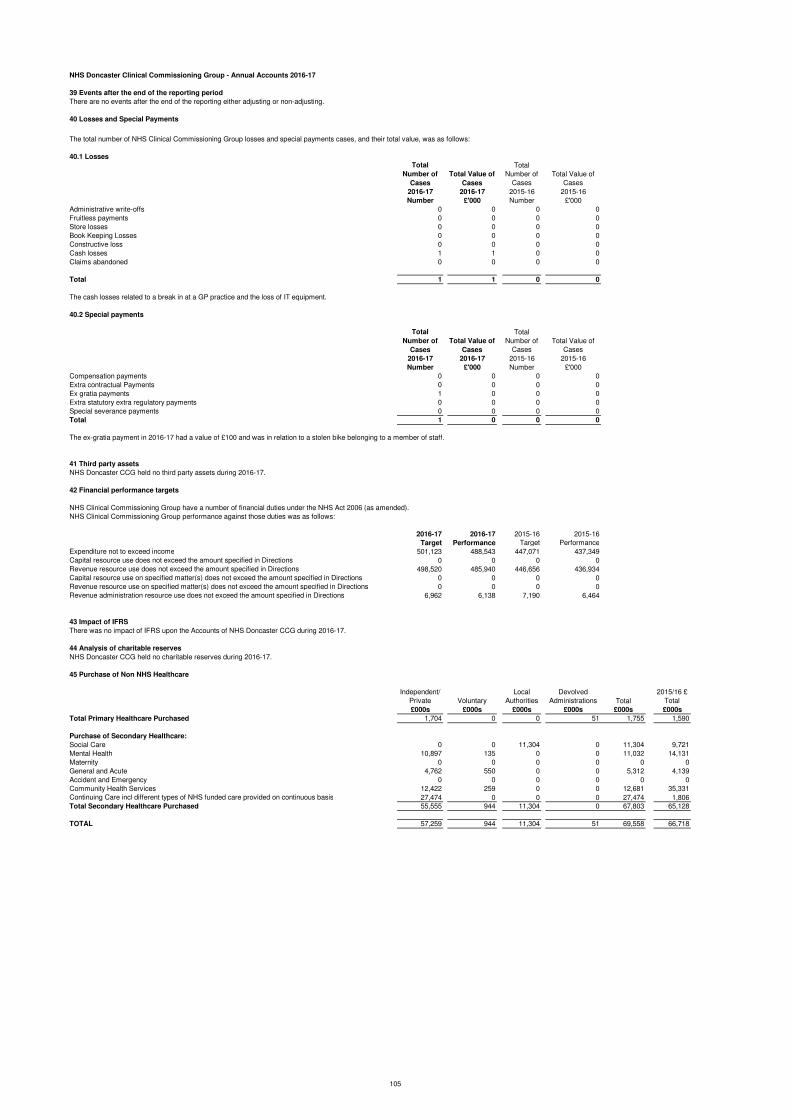
NHS Doncaster Clinical Commissioning Group - Annual Accounts 2016-17
39 Events after the end of the reporting period
There are no events after the end of the reporting either adjusting or non-adjusting.
40 Losses and Special Payments
40.1 Losses
Total
Number of
Cases
Total Value of
Cases
Total
Number of
Cases
Total Value of
Cases
2016-17 2016-17 2015-16 2015-16
Number £'000 Number £'000
Administrative write-offs 0 0 0 0
Fruitless payments 0 0 0 0
Store losses 0 0 0 0
Book Keeping Losses 0 0 0 0
Constructive loss 0 0 0 0
Cash losses 1 1 0 0
Claims abandoned 0 0 0 0
Total 1 1 0 0
The cash losses related to a break in at a GP practice and the loss of IT equipment.
40.2 Special payments
Total
Number of
Cases
Total Value of
Cases
Total
Number of
Cases
Total Value of
Cases
2016-17 2016-17 2015-16 2015-16
Number £'000 Number £'000
Compensation payments 0 0 0 0
Extra contractual Payments 0 0 0 0
Ex gratia payments 1 0 0 0
Extra statutory extra regulatory payments 0 0 0 0
Special severance payments 0 0 0 0
Total 1 0 0 0
The ex-gratia payment in 2016-17 had a value of £100 and was in relation to a stolen bike belonging to a member of staff.
41 Third party assets
NHS Doncaster CCG held no third party assets during 2016-17.
42 Financial performance targets
NHS Clinical Commissioning Group have a number of financial duties under the NHS Act 2006 (as amended).
NHS Clinical Commissioning Group performance against those duties was as follows:
2016-17 2016-17 2015-16 2015-16
Target Performance Target Performance
Expenditure not to exceed income 501,123 488,543 447,071 437,349
Capital resource use does not exceed the amount specified in Directions 0 0 0 0
Revenue resource use does not exceed the amount specified in Directions 498,520 485,940 446,656 436,934
Capital resource use on specified matter(s) does not exceed the amount specified in Directions 0 0 0 0
Revenue resource use on specified matter(s) does not exceed the amount specified in Directions 0 0 0 0
Revenue administration resource use does not exceed the amount specified in Directions 6,962 6,138 7,190 6,464
43 Impact of IFRS
44 Analysis of charitable reserves
45 Purchase of Non NHS Healthcare
Independent/
Private Voluntary
Local
Authorities
Devolved
Administrations Total
2015/16 £
Total
£000s £000s £000s £000s £000s £000s
Total Primary Healthcare Purchased 1,704 0 0 51 1,755 1,590
Purchase of Secondary Healthcare:
Social Care 0 0 11,304 0 11,304 9,721
Mental Health 10,897 135 0 0 11,032 14,131
Maternity 0 0 0 0 0 0
General and Acute 4,762 550 0 0 5,312 4,139
Accident and Emergency 0 0 0 0 0 0
Community Health Services 12,422 259 0 0 12,681 35,331
Continuing Care incl different types of NHS funded care provided on continuous basis 27,474 0 0 0 27,474 1,806
Total Secondary Healthcare Purchased 55,555 944 11,304 0 67,803 65,128
TOTAL 57,259 944 11,304 51 69,558 66,718
NHS Doncaster CCG held no charitable reserves during 2016-17.
The total number of NHS Clinical Commissioning Group losses and special payments cases, and their total value, was as follows:
There was no impact of IFRS upon the Accounts of NHS Doncaster CCG during 2016-17.
105
Related Documents











