© European Delirium Association 2012 www.europeandeliriumassociation.com Annals of Delirium July 2012 Editorial A Delirium Tipping Point Why does delirium continue to be persistently under recognised and mismanaged across the health care spectrum? What reasons do we have to explain the fact that despite sound ethical, empirical and economical arguments this highly preventable condition continues to be ignored by healthcare planners? Perhaps most perplexing, how can such a devastating disease remain invisible to the general public for so long? Conspicuous by their absence are patient and carer delirium support groups. These are the questions we, as an emerging group of passionate clinicians, researchers and educators within the European Delirium Association, wrestle with on a daily basis. The answers are undoubtedly complex and to use a favourite word amongst delirium cognoscenti, "multifactorial". Arguably a toxic mix of the complexity of the illness together with an, as yet, comparatively less well understood pathophysiology may account for the lack of ownership encountered at so many different levels. In trying to piece together the pieces of this jigsaw puzzle and answer the big questions I am reminded of the efforts of the committed group of clinicians and researchers led by Blessed and Roth studying dementia in the late 60s and early 70s. The challenge was great however by a series of small but significant steps, all of which increased our understanding of dementia, a tipping point was reached. Tackling the issue of complexity, in this edition of Annals, Dr Emma Vardy offers a personal insight into the problems associated with applying the Confusion Assessment Method in the acute setting. The challenges in unravelling the pathophysiology of delirium are well known and in a cutting edge article Dr Colm Cunningham considers the value of animal models in basic sciences. Importantly, he is not afraid to honestly answer the key questions as we try to link bench to clinical findings. So as we increase our understanding of delirium, how near are we to reaching a delirium tipping point? The challenges remain in terms of recognition and raising awareness however two recent events that I have encountered provide hope that we may not be far away. Firstly, whilst visiting a Dignity award winning Trust in Birmingham, I was introduced to a simple yet effective initiative called, ”Another cup of tea and a slice of cake". This very English innovation involves trying to reduce dehydration and malnutrition as well as increase stimulation on wards. With military precision volunteers, managed by an activities coordinator, facilitate a posh tea party within each ward bay complete with china plates, fine tea and cake. When asked what the driver for this was staff were quite clear it was about preventing delirium through good hydration and nutrition. The collective response made me wonder whether finally staff recognise the importance of delirium prevention and crucially link delirium to dignity.

Annals of Delirium July 2012
Oct 26, 2014
The Annals of Delirium is published by the European Delirium Association
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

© European Delirium Association 2012 www.europeandeliriumassociation.com
Annals of Delirium July 2012 Editorial
A Delirium Tipping Point
Why does delirium continue to be persistently under recognised and mismanaged across the health care spectrum? What reasons do we have to explain the fact that despite sound ethical, empirical and economical arguments this highly preventable condition continues to be ignored by healthcare planners? Perhaps most perplexing, how can such a devastating disease remain invisible to the general public for so long? Conspicuous by their absence are patient and carer delirium support groups.
These are the questions we, as an emerging group of passionate clinicians, researchers and educators within the European Delirium Association, wrestle with on a daily basis. The answers are undoubtedly complex and to use a favourite word amongst delirium cognoscenti, "multifactorial". Arguably a toxic mix of the complexity of the illness together with an, as yet, comparatively less well understood pathophysiology may account for the lack of ownership encountered at so many different levels.
In trying to piece together the pieces of this jigsaw puzzle and answer the big questions I am reminded of the efforts of the committed group of clinicians and researchers led by Blessed and Roth studying dementia in the late 60s and early 70s. The challenge was great however by a series of small but significant steps, all of which increased our understanding of dementia, a tipping point was reached.
Tackling the issue of complexity, in this edition of Annals, Dr Emma Vardy offers a personal insight into the problems associated with applying the Confusion Assessment Method in the acute setting. The challenges in unravelling the pathophysiology of delirium are well known and in a cutting edge article Dr Colm Cunningham considers the value of animal models in basic sciences. Importantly, he is not afraid to honestly answer the key questions as we try to link bench to clinical findings.
So as we increase our understanding of delirium, how near are we to reaching a delirium tipping point? The challenges remain in terms of recognition and raising awareness however two recent events that I have encountered provide hope that we may not be far away.
Firstly, whilst visiting a Dignity award winning Trust in Birmingham, I was introduced to a simple yet effective initiative called, ”Another cup of tea and a slice of cake". This very English innovation involves trying to reduce dehydration and malnutrition as well as increase stimulation on wards. With military precision volunteers, managed by an activities coordinator, facilitate a posh tea party within each ward bay complete with china plates, fine tea and cake. When asked what the driver for this was staff were quite clear it was about preventing delirium through good hydration and nutrition. The collective response made me wonder whether finally staff recognise the importance of delirium prevention and crucially link delirium to dignity.

© European Delirium Association 2012 www.europeandeliriumassociation.com
The second delirium story of hope occurred recently when assessing an OSCE examination station for medical students. The task for the students was to explain a diagnosis of delirium to a distressed relative. As expected they struggled with describing delirium indicators confidently. However, since assessment drives learning, the fact that delirium was a core part of the exam process represents significant progress for tomorrows doctors. Even more encouraging was a chance remark from the seasoned role player playing the part of the relative of a delirious patient. Reflecting back on the session she specifically mentioned how real and important the scenario was. Finally it appears the reality that delirium is more than an epiphenomenon is being recognised.
Of course these are but two stories of hope but we should take heart from them. If we continue on our quest for greater understanding and couple it with raising delirium on the public agenda we can remain confident that a larger number of such positive encounters will emerge. Different challenges will present themselves however under recognition may no longer be chief amongst them.
Dr Andrew Teodorczuk
A new animal model with potential to reconcile and dissect cholinergic and neuroinflammatory hypotheses of delirium
Colm Cunningham, Delirium Basic Research Group, Trinity College Dublin
It has been recognized for some time that existing memory impairment is one of the biggest risk factors for the subsequent occurrence of delirium. However, it is not clear how this prior impairment interacts with the typical acute precipitants of delirium, to induce the deficits observed in patients. This is just one among many
questions in delirium pathophysiology that remain unanswered.
The lack of animal models relevant to delirium pathophysiology has been one of the significant gaps in the delirium research field and recent studies by our laboratory have tried to address this problem, using new mouse models to replicate aspects of prior degenerative pathology and superimposed systemic inflammation (Field et al, 2012; Murray et al., 2012). Significantly, we showed in the first of these studies, that mild/moderate systemic inflammation in a normal animal is insufficient to induce working memory deficits but when the same inflammatory challenge is made in animals with prior pathology, these animals now show acute and transient working memory deficits (Murray et al., 2012). This ‘prior pathology’ consists of robust synaptic loss in the hippocampus and thalamus, induced by the ME7 model of prion disease, and microglia that are primed by the primary pathology to produce exaggerated responses to subsequent inflammatory insult (Cunningham et al., 2005). Many researchers might argue that this prion disease model is not directly relevant to more common predisposing factors for delirium, such as Alzheimer’s disease and age-‐associated cognitive impairment. While this is an understandable view, what these data show, unequivocally, is that where there is existing pathology or ‘vulnerability’ in particular regions of the brain, systemic inflammation can selectively disrupt function in those regions more easily than it can in normal animals. As such, it provides a plausible recapitulation of the observation that systemic infection can produce profound CNS effects in some patients while leaving others unaffected. Understanding this dichotomy is central to elucidating delirium pathophysiology. Useful mechanistic information will emerge from this model.
Making a better model
Nonetheless, there are good reasons to try to take this observation out of the prion disease setting and replicate it in a neuropathological

© European Delirium Association 2012 www.europeandeliriumassociation.com
setting not involving prions and in a neuroanatomical/neurochemical setting that is relevant to delirium as it is observed in the geriatric population. Prominent hypotheses of delirium pathophysiology include both hypocholinergic and neuroinflammatory hypotheses and whether these are parallel and/or interacting is largely unknown.
Last month in The Journal of Neuroscience we published new findings (Field et al., 2012) showing that systemic inflammation induced by gram-‐negative bacterial endotoxin (LPS) induces working memory deficits, but only in animals with prior pathology in the basal forebrain cholinergic nuclei (BFCN). The BFCN, which comprises the medial septum, the diagonal bands and the nucleus basalis (see Figure 1), is the source of most acetylcholine in the forebrain and this area degenerates markedly during Alzheimer’s disease. To specifically lesion this region we used the ribosomal toxin saporin, covalently linked to an antibody directed against the p75 neurotrophin receptor that is highly expressed on basal forebrain cholinergic neurons. We showed that intracerebroventricular injection of this toxin (p75NTR-‐saporin) at low doses could induce approximately 20% destruction of the cholinergic cells of the medial septum without obvious effect on working memory function. However, if these animals were allowed to recover for 40 days post-‐surgery, and then challenged with systemic LPS, only those animals with prior lesions showed acute working memory deficits. Many of our previous predictions about the interaction of prior pathology and systemic inflammation were based on the original demonstration of microglial priming and subsequent exaggerated inflammatory responses to systemic inflammatory insult (Cunningham et al., 2005). However, 40 days after p75NTR-‐saporin lesions, microglia did not show exaggerated inflammatory cytokine induction after systemic inflammation. Thus the acute working memory deficits appear to occur in the absence of microglial priming.
This independence of microglial priming does not imply a lack of CNS inflammatory response to systemic LPS, it simply means that
microglia appear to respond equally to systemic inflammation in the lesioned and normal animals. This implies that the ‘vulnerability’ in these animals represents a neuronal susceptibility to disruption of function. We showed, using the acetylcholine muscarinic receptor antagonist scopolamine, that the T-‐maze working memory task used in these studies was indeed dependent on cholinergic function and further showed that treatment with the acetylcholinesterase inhibitor donepezil, 1 hour after LPS, protected against the working memory deficit observed. Collectively these data show that the loss of 20% of cholinergic neurons of the basal forebrain cholinergic system does not robustly affect cognitive function under normal conditions, but leaves these animals vulnerable to significant cognitive disruption upon an acute systemic inflammatory insult. The data also show that preserving acetylcholine levels using an acetylcholinesterase inhibitor is protective in this setting, which may have relevance for the recent trial of rivastigmine for ICU delirium (discussed below).
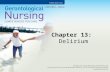
Figure 1

© European Delirium Association 2012 www.europeandeliriumassociation.com
We believe that these findings have significant implications for delirium, particularly in the setting of existing cognitive
impairment/dementia and that this limited cholinergic lesion model will be an extremely useful tool in delineating molecular pathways to dysfunction that are relevant to delirium. However, it is clear that many delirium researchers are hesitant about the application, to clinical delirium, of data arising from these animal models and a number of pertinent questions do arise.
Q Can we really say that these mice are delirious?
Q Is this a hippocampal phenomenon?
Q What, therefore, is the role of the prefrontal cortex?
The occurrence of working memory deficits using a task that has been shown to be hippocampal-‐dependent has made it easy to ignore or dismiss these data as not relevant to delirium. We do not imply that delirium is a hippocampal phenomenon. Firstly, we cannot yet say what other regions of the brain are also recruited by this task. Secondly, the induction of these cognitive deficits by recapitulation of key etiological factors for delirium must be emphasized: there are simply no other studies that have even attempted to address the multi-‐factorial nature of dysfunction during delirium and as such, the data from our studies on the interaction of systemic inflammation and prior CNS pathology have a utility for delirium research irrespective of whether the cognitive impairments observed constitute delirium per se. Thirdly, it is important to stress that mice and men are different and while we cannot say that these mice are definitely delirious nor can we assert that they are not. However, we can say that they have an acute onset and transient attentional/working memory deficit, induced by a systemic inflammatory challenge, which occurs only in mice with prior cholinergic pathology. Asking the most relevant questions of mice during acute episodes of sickness, in which appetitive and exploratory drives are profoundly suppressed is challenging. The water-‐motivated, working memory, T-‐maze
Figure 1
Prior pathology and superimposed systemic inflammation interact to produce acute and transient working memory deficits: towards reconciling cholinergic and inflammatory hypotheses of delirium. This scheme shows the basal forebrain cholinergic nuclei (BFCN), illustrating the septohippocampal pathway, the ventral diagonal band projections to the amygdala and piriform and insular cortices and the nucleus basalis projection to the frontal, parietal and temporal cortices (after Wolff 1991). Intracerebroventricular injection (left panel) of the ribosomal toxin saporin, linked to an antibody against the p75 neurotrophin receptor, which is enriched on BFCN cells, induces selective neuronal death in these regions. This approach facilitates targeted, selective and limitable lesioning of this area and consequently decreased cholinergic tone (shown in grey, right panel) in these projection fields. In lesioned animals, LPS induces acute and transient working memory deficits, resembling delirium. Neither lesion nor LPS alone were sufficient to induce such deficits. LPS-‐induced CNS inflammatory responses were equivalent in lesioned and non-‐lesioned animals and the acetylcholinesterase inhibitor donepezil could block these deficits (Field et al., 2012). Thus systemic inflammation in ‘vulnerable’ animals may be used to interrogate aspects of delirium pathophysiology

© European Delirium Association 2012 www.europeandeliriumassociation.com
represents a task that is tailored to assess correct and incorrect responses in a task reliant on both attention and working memory, in a manner that is not confounded by sickness-‐induced performance deficits such as suppressed activity, slower response time, suppressed appetite etc. In order to successfully solve the T-‐maze task, animals must attend to the maze exit on first entry, be attentive to the body-‐turn they made to escape the maze and recall this choice just 30 seconds later, in order to make the opposite turn to find the new location of the exit on re-‐exposure to the maze. Whether the deficit is attentional or purely working memory is difficult to dissect, but it is undeniably distinct from longer term, or reference, memory. We have clearly shown that mice are not impaired on that type of hippocampal-‐memory after LPS treatment (Cunningham et al., 2009). This is consistent with data showing that patients with delirium were able to access previously learned information but showed impairments on tasks involving online processing of novel, trial specific, information (Brown et al., 2011). Thus there are important parallels between the type of cogntive impairments seen in delirium and those in animals with cholinergic “vulnerability”: we are not simply describing a generalised hippocampal deficit.
As for the relative contribution of the basal forebrain, the hippocampus and the prefrontal cortex, it appears that the dose and route of p75NTR-‐saporin used in the current study appeared to target the septal neurons that project to the hippocampus more than they affected the nucleus basalis neurons that project to the prefrontal cortex. This latter path and the prefrontal cortex in general, are less developed in mice than in humans and this is a limitation of mouse research for many fields of neuroscience, including delirium. This does not invalidate the use of mice to investigate the mechanisms by which systemic inflammation and prior CNS pathology interact. It is worth noting that most neuropsychological and even neurodegenerative conditions, including depression, schizophrenia, Alzheimer’s disease and Parkinson’s disease, are studied using models that do not
recapitulate several key features of these conditions. This is the reality in developing and using animal models and the important thing is to focus on the questions that these models can answer.
Q Despite the long-standing cholinergic hypothesis of delirium, there are now data showing that acetylcholinesterase inhibition is not helpful in ICU delirium. Can these findings be reconciled with the current data?
The clinical study of van Eijk and colleagues (2010) found no protective effect of rivastigmine against delirium in the ICU. However, our data are most relevant to patients where there is existing cholinergic vulnerability, as is frequently the case in Alzheimer’s disease and in some other age-‐related CNS pathologies. If the individual has neurodegeneration in the cholinergic system and then suffers a moderate systemic inflammatory insult such as infection or surgery, it is plausible that boosting cholinergic function would protect against the deleterious effects of this inflammation, as we have shown to be the case in our mouse study. However, in ICU patients who have suffered severe trauma or severe sepsis, we believe that it is highly unlikely that bolstering a single neurotransmitter system will be able to correct the marked divergence from homeostasis in multiple systems, including severe inflammation, impaired tissue perfusion and hypoxia, blood brain barrier breakdown and multi organ dysfunction. Obviously the multiple, often quite divergent, routes to delirium will influence correct treatment strategies. We do not propose that cholinergic dysfunction is the ‘final common pathway’ in delirium pathhophysiology but we believe that our data demonstrate that systemic inflammation and cholinergic vulnerability interact to induce acute attentional and/or working memory deficits and in that scenario, bolstering cholinergic function was found to be beneficial. This clearly has relevance for delirium, at least in the geriatric population. The fact that donepezil offered only partial protection even in animals that had a known cholinergic deficit

© European Delirium Association 2012 www.europeandeliriumassociation.com
already actually predicts that cholinergic enhancement would be unlikely to be beneficial in settings such as ICU delirium. Therefore this study and the results of the rivastigmine trial are by no means incompatible and this animal model allows us to ask simple questions in this domain and to provide empirical evidence that can contribute to supporting or rejecting clinical hypotheses. We now know that moderate systemic inflammation can produce dysfunction in an already compromised cholinergic system but cannot do so in intact animals. Severe trauma and sepsis is likely to lead to CNS dysfunction by multiple routes, against which cholinesterase inhibition is apparently powerless. Just as it is too simplistic to assume that hypocholinergic function is the final common pathway to delirium simply because robust cholinergic inhibition can produce a delirious state, so is it unwise to reject the importance of cholinergic function just because cholinesterase inhibition did not protect against delirium in one profoundly sick population.
Q Since the deficits observed here are independent of microglial priming, does this rule out a role for this phenomenon in delirium?
What these data show is that loss of cholinergic input is, of itself, sufficient to make neurons proximal to the terminal fields of cholinergic neurons susceptible to dysfunction upon exposure to inflammatory mediators. This means that priming is not essential for the acute dysfunction. However, priming leads to higher levels of inflammatory mediators being produced in the areas of prior pathology and thus their presence would be predicted to further exacerbate the effects. Therefore, there are both inflammatory and neuronal vulnerabilities to consider. There are two main factors that might have influenced microglial priming in this model: the time post-‐surgical injection of p75NTR-‐saporin and the degree of loss of cholinergic input.
1) Time post-‐surgery: CNS pathology primes microglia and we have previously shown that this can last up to 28 days post axonal degeneration (Palin et al, 2008). It is clearly no longer present at 40 days post-‐insult in the current study and we must investigate whether priming actually occurs and how long it lasts in the current model. 2) Loss of cholinergic tone: acetylcholine can directly suppress macrophage/microglial activation (Tracey et al. 2007). We show that a limited cholinergic lesion (<20%) does not prime the microglia. However, one might predict that larger lesions will be required to remove sufficient acetylcholine to lift this suppression of microglia activity. This is also under investigation. The prediction is that if cholinergic dysfunction is sufficient for acute deficits, in the absence of microglial priming, then the additional factor of microglial priming will only add to the severity and duration of these deficits.
Concluding remarks
In considering the value of this and other animal models, purportedly relevant to delirium, clinical researchers must be measured in their expectations. It may be difficult to recapitulate delirium in a mouse and even if one can achieve this it will be extremely difficult to verify that mice are indeed delirious. What we must focus on is recreating key etiologies that lead to delirium in the clinic, demonstrating that these factors interact in ways that are consistent with clinical observations and then using these models to delineate mechanisms and to make predictions for ongoing clinical studies.
In other words, we must focus on what these models do provide rather than on what they do not provide. Our recent studies show unequivocally that systemic inflammation induces acute and transient attentional/working memory deficits, which are relevant to delirium, in animals with prior pathology in the basal forebrain cholinergic

© European Delirium Association 2012 www.europeandeliriumassociation.com
system. Whether or not these animals fit all the criteria for delirium, in as much as anyone can definitively say what these criteria should be in a mouse, they offer a unique tool to investigate the interaction between cholinergic and neuroinflammatory routes to acute
neuropsychological dysfunction and this already represents a significant advance on previous knowledge in this field. In particular, this model allows us to interrogate whether it is microglial priming, hypocholinergia or some other aspect of neuronal susceptibility, or indeed all three that create the susceptibility to systemic infection-‐induced dysfunction in vulnerable individuals. The data arising from such models should obviously form part of the discussion on delirium pathophysiology.
Full reference for citation
Prior Pathology in the Basal Forebrain Cholinergic System Predisposes to Inflammation-‐Induced Working Memory Deficits: Reconciling Inflammatory and Cholinergic Hypotheses of Delirium. The Journal of Neuroscience, May 2, 2012 • 32(18):6288 – 6294
Robert H. Field, Anna Gossen, and Colm Cunningham This article is freely available (open access) through The Journal of Neuroscience References Fiel Murray, C., Sanderson, D.J., Barkus, C., Deacon, R.M., Rawlins, J.N., Bannerman, D.M. & Cunningham, C. (2012) Systemic inflammation induces acute working memory deficits in the primed brain: relevance for delirium. Neurobiol Aging, 33, 603-‐616 e 603.
Field, R.H., Gossen, A. & Cunningham, C. (2012) Prior pathology in the basal forebrain cholinergic system predisposes to inflammation induced working memory deficits: reconciling inflammatory and
cholinergic hypotheses of delirium. Journal of Neuroscience, 32 6288-‐6294.
Cunningham, C., Wilcockson, D.C., Campion, S., Lunnon, K. & Perry, V.H. (2005) Central and systemic endotoxin challenges exacerbate the local inflammatory response and increase neuronal death during chronic neurodegeneration. J Neurosci, 25, 9275-‐9284.
Cunningham, C., Campion, S., Lunnon, K., Murray, C.L., Woods, J.F., Deacon, R.M., Rawlins, J.N. & Perry, V.H. (2009) Systemic inflammation induces acute behavioral and cognitive changes and accelerates neurodegenerative disease. Biol Psychiatry, 65, 304-‐312.
Brown, L.J., Ferner, H.S., Robertson, J., Mills, N.L., Pessotto, R., Deary, I.J. & MacLullich, A.M. (2011) Differential effects of delirium on fluid and crystallized cognitive abilities. Arch Gerontol Geriatr, 52, 153-‐158.
van Eijk, M.M., Roes, K.C., Honing, M.L., Kuiper, M.A., Karakus, A., van der Jagt, M., Spronk, P.E., van Gool, W.A., van der Mast, R.C., Kesecioglu, J. & Slooter, A.J. (2010) Effect of rivastigmine as an adjunct to usual care with haloperidol on duration of delirium and mortality in critically ill patients: a multicentre, double-‐blind, placebo-‐controlled randomised trial. Lancet, 376, 1829-‐1837.
Palin, K., Cunningham, C., Forse, P., Perry, V.H. & Platt, N. (2008) Systemic inflammation switches the inflammatory cytokine profile in CNS Wallerian degeneration. Neurobiol Dis, 30, 19-‐29.
Tracey, K.J. (2007) Physiology and immunology of the cholinergic antiinflammatory pathway. J Clin Invest, 117, 289-‐296

© European Delirium Association 2012 www.europeandeliriumassociation.com
Personal experience of the complexity of diagnosing delirium
Dr Emma Vardy
I am a Consultant Geriatrician and Associate Clinical lecturer. My clinical role involves elderly medical inpatient work as well as providing an older peoples liaison service on the general medical and medical assessment wards. Until recently my research interest has focussed on dementia, mainly Alzheimer’s disease. More recently I have become more interested in delirium at both a clinical and a research level. This opinion piece describes my journey into delirium:
The continuing development of any healthcare professional involves being open to the fact that there is always something to learn, even on subjects about which you thought you knew a lot! I shall describe here my recent re-‐evaluation of my skills in the diagnosis of delirium.
Through preparing a protocol for a piece of clinical research I started to explore the ‘gold standard’ method for diagnosis of delirium. Perhaps to be expected was the fact that there were of course tests that I had not any experience of, such as the Delirium Rating Scale (DRS). I rapidly became aware that with research into delirium comes a variety of methods for delirium assessment. First there are a number of different tests and combinations of tests. They differ in terms of goal, that is some are diagnostic, others measure severity. Secondly methodologies differ in both the frequency and timing of application of these tests. Added to this is the fact that currently available methods come in different formats , for example the confusion assessment method (CAM) and the CAM-‐ICU, in recognition of the fact that most definitely one size does not fit all. As my knowledge of methods of diagnosis of delirium broadened I started to question what I had previously seen as the ‘basics’ in diagnosing delirium, not something I had originally expected.
Many of us will be using tools such as the confusion assessment method (CAM), and this comes recommended both in the NICE guidelines (guidance.nice.org.uk) and those of the British Geriatrics Society (www.bgs.org.uk). This is certainly the test with which I am most familiar. The CAM consists of 4 simple questions, but are they really so simple? The CAM is easily accessible, not always so readily available are details of how to assess each of the criterion. Inattention and disorganised thinking are signs that take careful and detailed assessment, this question requires a yes or no in terms of diagnosis, but actually eliciting this feature is more complex. The waters have become a little clearer for me on my recent discovery of the CAM training manual (http://hospitalelderlifeprogram.org).
My own personal professional development in the diagnosis of delirium has led me to evaluate my own practice but also my expectations of the junior doctors I work with. I often ask them to apply the CAM in the medical inpatient setting. But through re-‐evaluating my own skills I have started to consider just how much I have perhaps presumed of some of my juniors in the past. I have considered whether the junior doctors that I work with have ever had any comprehensive training on applying the CAM? Have I ever even asked? In retrospect I have probably presumed skills that the junior members, and dare I say some more senior members of the team, just don’t have. What about the time element? Eliciting these signs properly takes time but is not something that can often be pondered over by our junior doctors, for example, whilst on call. In fact in recognition of this the NIHR Health technology assessment programme has just put out a call for triage tools for delirium (http://www.hta.ac.uk/funding/standardcalls/11_143cb.pdf). This recognition of a need for a simple and easy to apply diagnostic tool is particularly timely, as the detection of delirium becomes increasingly important, with progress in terms of the dementia strategy in acute hospitals.

© European Delirium Association 2012 www.europeandeliriumassociation.com
The rewards of a good diagnosis of delirium abound, leading to identification and treatment of underlying cause, reduced morbidity and mortality and increased understanding and support for carers and relatives. But it is important that the assessment for delirium is done well and that delirium is correctly diagnosed. There are various examples in the literature of poor detection of delirium. Perhaps less evident are the consequences of incorrectly diagnosing delirium. Over the course of my career two examples come to mind. One was a patient who had more than one admission with ‘delirium’. Brain imaging after the second or third repeat admission revealed underlying brain metastases. The second case relates to a lady with an ‘acute confusion state’. Brain imaging was performed, after a delay, revealing an extradural haematoma which was operated upon. The safe-‐guard to ensuring such cases are not missed are present in the NICE guidelines, which state at the end of the treatment algorithm that there should be re-‐evaluation for underlying causes. However these examples are a sobering reminder of the importance of ensuring accuracy of diagnosis and following a procedure of re-‐evaluation of diagnosis.
In summary my research into methods of diagnosis of delirium led me to re-‐evaluate my own clinical practice but also reflect on my own presumptions of others knowledge. There may be new and improved methods for diagnosing delirium on the horizon, perhaps more readily deliverable. But in the interim perhaps those of us at the coal face need to reflect on what our colleagues, particularly junior doctors, may find hard about making a diagnosis of delirium and seek to raise clinical standards overall.
Dr Emma Vardy
Newcastle upon Tyne hospitals NHS foundation trust and Newcastle University
Report on 2nd Annual ADS Meeting, June 3-5, Indianapolis, Indiana
The second annual American Delirium Society meeting was well attended; we were very pleased that this year we had 123 participants; a 33% increase over last year’s meeting. Delegates came from China, Canada, US (20 states), Norway, Portugal, Ireland, England, Australia and Denmark. Speakers from several continents were included and the program was full enough that parallel sessions were held. A very broad range of speakers and topics were presented, demonstrating delirium’s ascendance as a highly valued and increasingly well studied aspect of geriatric care. ADS’ new president Malaz Boustani, MD,MPH provided an address during opening night reception which explored ways that drugs targeted to symptomatic relief or disease modification of delirium could be assessed and regulated on a global scale. The president elect, Karin Neufeld, MD,MPH and new treasurer, Ann Gruber-‐Baldini, PhD, were introduced, as were new ADS Board members. A number of new collaborations were developed in the course of this meeting, an achievement that all of us in ADS heartily applaud and endorse!
On June 4th, a session on pathophysiology and biomarkers was initiated by Edward Marcantonio, MD, who reviewed technical aspects of biomarker research. Other speakers included Alasdair MacLullich, MB/ChB, PhD,Stacie Denier, MD, James Root, PhD, and Malaz Boustani, MD, MPH, and included studies relating to CSF, MRI/structural ICU, and surgical aspects of delirium. The parallel session was devoted to delirium measurement, and was introduced by Paula Trzepacz, MD, who presented updates on her collaborative work on the phenomenology of delirium. This has provided a replicable pattern of symptomatology that may inform studies of delirium pathophysiology. Other work on screening, measurement, and operationalization of delirium measurement was presented by Laura Hoofring, MSN, ARNP-‐PMH, Jean-‐David Gaudreau, MD, Edward Marcantonio, MD, and Ann

© European Delirium Association 2012 www.europeandeliriumassociation.com
Gruber-‐Baldini, PhD. The final session of the day explored postoperative delirium; this was initiated by Gregory Crosby, MD, who discussed aspects of vulnerability in the aging CNS, and was followed by work on baseline cognitive function and its impact on post-‐operative outcomes, the assessment of delirium/emergent delirium in the PACU, brain dysfunction in critical care, the impact of analgesic agents in the postoperative setting, and the method of “ABCDE bundle” in addressing and maximizing postoperative care complicated by delirium. Speakers included Thomas Robinson, MD, Karin Neufeld, MD, MPH, Yoanna Skrobik, MD, and Michele Balas PhD,RN, CRNP, CCRN.
The second and final day included morning sessions on long term outcomes of delirium and clinically specific aspects of the care of delirium. The outcomes session included a study by Daniel Davis, MD, which involved a large retrospective chart review with implications that the pathophysiology of Alzheimer’s Dementia may be distinct from that of delirium. Other speakers included Dimitry Davydow, MD, Alasdair MacLullich, MD, ChB, PhD. Talks on the psychological sequelae of delirium as well as the impact of pre-‐operative cognitive dysfunction on delirium outcomes were presented by O. Bienvenu MD, PhD and Frederick Sieber MD. A comprehensive literature review of pharmacological prevention strategies in delirium by Jose Maldonado, MD completed the session. The symposium on clinically specific aspects of delirium care included a session by James Rudolph, MD,MS on a comprehensive approach to delirium identification and management in acute settings (the “Delirium Toolbox”), a highly practical and effective session on ways to de-‐escalate agitated and irrational patients (the T-‐A-‐DA method, representing “tolerate-‐anticipate-‐don’t agitate”) which involved acting the parts of patient and nurse by the speakers, Joseph Flaherty, MD and Sharon Gordon, PhD, and sessions on medications presenting risk to patients with delirium by Noll Campbell, PharmD, the role of sleep in the presentation and management of delirium in the ICU by Wes Ely,
MD,MPH, and techniques of early mobilization for patients with critical illness, by Amy Pawlik, PT,DPT, CCS and Cheryl Estbrook OT. The final session presented clinical trial updates provided by Wes Ely (“MIND-‐USA”), a new delirium assessment tool for emergency room use (Jin Han, MD), and other work by Simon Mears, MD, Laura Sands, PhD, MA, Babar Khan, MD, MS, Don-‐Zin Wang MD, PhD, Jeff Silverstein, MD, and Gideon Caplan, MB, MS, and included studies of new agents and pharmacological approaches to minimizing delirium in different settings; Dr Caplan’s study reported new findings on CN S blood flow abnormalities in patients with delirium.
Keynote speakers included Sharon Inouye, MD, MPH, who spoke on the future of research in delirium, including an emphasis on the need to codify and simplify diagnostic categories of delirium in the ICD. The Delirium Champion Award 2012 was presented to Dr Inouye in recognition of her outstanding contribution to the field. Ann Kolanowski, PhD, RN spoke about the vital role nurses play in delirium assessment and intervention, and provided updates on the methodology of dissemination of delirium teaching for nurses. There were 16 posters accepted for presentation.
Next year’s conference will be in Indianapolis, Indiana, in June -‐ actual date to be confirmed shortly. Preparations are being made for a conference in Baltimore, MD area for the following year (2014). We sincerely hope that this year’s meeting was helpful and gratifying for attendees, and that next year’s will be even better!
Barbara Kamholz, MD
Board Member, EDA and ADS

© European Delirium Association 2012 www.europeandeliriumassociation.com
Raising delirium consciousness using the media
Dr Valerie Page, Consultant Anaesthesia and Critical Care, Watford General Hospital,
Dr Daniel Davis, Research Fellow, Institute of Public Health, University of Cambridge
Tony Jameson-‐Allen, Accredited Knowledge Management Consultant and Director, Evolution Networking Ltd, UK. www.evolution-‐networking.com
Introduction “The greatest trick the devil ever played was convincing the world that he did not exist.” Charles Baudelaire
Delirium occurs in one in five general hospital patients. It remains underappreciated and under researched. The European Delirium Association remit includes campaigning at local, national and international levels in order to influence policy. The area of advocacy has remained under addressed.
There needs to be an increased awareness of delirium clinically, politically and publicly. This project assessed the effectiveness of using traditional advertising, websites and social media to achieve this. The aim was to discover how best to use traditional and modern forms of media to lobby on behalf of patients with delirium.
Methods Stage 1: Selected websites and social media resources relating to delirium were identified (see table 1). The effectiveness was judged by the number of times a webpage was viewed.
Stage 2: A banner advert was purchased for the UK national newspaper Guardian website directing readers to the UK ICU delirium website; the number of clicks resulting from this advert was collected. (Figure 1).
Results
The web pages had large variations in number of times they were viewed. The most successful was the Wikipedia delirium page with an average of nearly 44,000 per month. Encouragingly the UK Youtube clip was activated 43 400 times in less than 4 years. (Figure 2) Conversely the Guardian banner advert generated an astoundingly low total of 12 responses from over 25,000 appearances
Resource Date started Outcome/’Hits’
Wikipedia Delirium Page Dec 2002 527 317 last 12 months
Youtube ICU delirium clip
Aug 2008 43 500 views since launch
ICU delirium website Aug 2008 Average 1000 visits per month
Delirium videocasts* April 2009 3468 views since launch
EDA** website July 2009 73 556 page views
EDA** facebook group June 2011 49 members
Guardian web banner advert
July 2011 21 clicks from 18 000 appearances

© European Delirium Association 2012 www.europeandeliriumassociation.com
Discussion
Heightened media attention to an issue has been shown to pressurise policy makers to generate immediate, short-‐term solutions to the problem which then shift to long-‐term solutions. Delirium needs a simple but powerful device as a means of disseminating knowledge on the impact on patient outcomes – death and dementia.
After the massacre of schoolchildren in Dunblane, Scotland, Parliament was introducing a law to ban certain firearms, but not .22 handguns. The team, with no money and no time, decide to act. They discovered that Robert Kennedy had been assassinated with a .22 gun. Using a stock photograph of Kennedy, they had a poster printed to go on a lorry parked outside Parliament on the day of the debate. "If a .22 handgun is less deadly," it asked, "why isn't he less dead?" An amendment was added to include the banning of .22 guns.
Regarding promotional campaigns Ed Jones of Saatchi & Saatchi said "Your message has to be really powerful and life-‐transforming, otherwise you are wasting your money." There is no doubt that the facts of delirium are as powerful as cancer or HIV yet still the subject does not feature in the public or to a lesser extent the clinical consciousness. On the BBC health website cancer is covered in great depth with a number of helpful links; delirium does not even feature.
There is growing interest in use of Facebook for disseminating information and establishing informal networks. It has been demonstrated that spending money on a single advert was nowhere near as effective as entries on high profile social media based websites such as Wikipedia and Youtube. Currently the Internet can be freely utilized to educate and influence politically, clinically and publicly. There is growing interest in use of Facebook for disseminating information and establishing informal networks.
This project was a means in discovering how best to use different forms of media to lobby on behalf of patients with delirium. The findings suggest that currently the use of responsive, informal, and contemporary means will gain greater exposure to delirium than a traditional advertising campaign. It would be reasonable to assume that will generate a higher awareness amongst clinicians and the public. Further work is needed to discover how to promote delirium publicly, build on the momentum that has been established, to manage the response and to capitalize on any media opportunities as they arise.
Figure 1 Banner advertisement for ICU delirium website

© European Delirium Association 2012 www.europeandeliriumassociation.com
Figure 2 CAM-‐ICU demonstration on Youtube
*“Haloperidol prophylaxis decreases delirium incidence in elderly patients after noncardiac surgery: A randomized controlled trial”
W Wang, HL Li, DX Wang , et al, Crit Care Med 2012: 40 (3); 731-‐739
Earlier this year, a Chinese group published the results of a study examining the potential role of haloperidol for prophylaxis in surgical patients admitted to critical care*. The study was carefully designed, using a prospective, randomised, double blind placebo controlled method conducted across two sites. Subjects were older patients (>65 years old), post non-‐cardiac surgery and admitted to ICU post operatively. Exclusion criteria were rigorous, the entire study was safety conscious and this meant that the doses of haloperidol used in the active arm were very conservative. A 0.5mg bolus of haloperidol was followed by a 12 hour infusion running at 0.1mg of haloperidol an hour. The total prophylactic dose of haloperidol given was thus 1.7mg versus the control arm, where patients received a matching volume of saline. Usual sedation (propofol or midazolam) was used and titrated to RASS -‐2 to +1, with daily sedation breaks for intubated patients. Postoperative pain was managed with patient controlled analgesia administered intravenously or epidurally, with supplemental analgesia being given as fentanyl boluses +/-‐ a fentanyl infusion. Multicomponent interventions to reduce modifiable delirium risk factors were used in all patients. Delirium assessments were carried out once a day in the early evening using CAM-‐ICU. The primary end point was delirium incidence in the first 7 days post-‐operatively, with multiple secondary endpoints.
The final analysis was made on 229 patients in the haloperidol group compared with 228 patients in the placebo group. Overall the groups were well matched on baseline characteristics. There were some statistically significant differences noted in perioperative variables, the duration of anaesthesia was longer in the haloperidol group (5.51

© European Delirium Association 2012 www.europeandeliriumassociation.com
vs 4.81 hours, p=0.003), the duration of surgery was longer in the haloperidol group (4.51 vs 3.79 hours, p=0.001) and the total intraoperative infusion volume was greater in the haloperidol group (2700ml vs 2550ml, p=0.048). All other variables were not statistically different, including the total doses of opioid analgesics and sedatives administered.
The primary outcome results showed an incidence of delirium in the 7 days post surgery of 15.3% in the haloperidol group compared with 23.2% in the placebo group which translates into an NNT of 13 to prevent one case of delirium. Much of the benefit appears to be confined to patients who received intra-‐abdominal surgery, representing about three quarters of the cohort. The difference in delirium incidence in the rest of the cohort (intra-‐thoracic surgery, spinal and extremital surgery and superficial surgery) was not apparently numerically large, nor statistically significant. This gives rise to the obvious question (‘why?’), however the authors do not speculate.
Overall, the reported ICU length of stay was short, with a median of 21.3 hours in the haloperidol group and 23.0 hours in the placebo group (p=0.024). When looking at just patients who developed delirium, the intervention resulted in a reduced ICU length of stay (19.6 hours haloperidol group, 41.4 hours placebo group, p=0.006).
The reported time to onset of delirium was quite long, on average 6.2 days in the haloperidol group and 5.7 days in the placebo group (p=0.021), however, this analysis included all the patients who did not suffer delirium, which when expressed as a mean, would make the onset of delirium time very long. As a bonus, because of the reduced incidence of delirium in one group, it also makes the difference statistically significant. When more realistically analysing only
patients who suffered delirium, the mean time to onset of delirium was found to be 1.7 days (haloperidol group) vs 1.5 days (placebo group) and was not statistically significant. The mean number of delirium free days was 5.7 (haloperidol group) vs 5.6 (placebo group) and was also not statistically significant. So the intervention reduces the numbers of patients experiencing delirium, but not the time to the onset of delirium for those who suffer from it.
There was no difference in hospital length of stay overall (11.0 days for both groups, p=0.255), or between the groups in patients who went on to develop delirium (14 days haloperidol group vs 12 days placebo group, p=0.512).
In terms of overall safety, there were no differences between the groups with respect to arrhythmia’s, extended QTc interval, extrapyramidal symptoms, RASS or mortality. The intervention is clearly safe.
Overall, this study shows that a small prophylactic dose of haloperidol reduces the incidence of delirium in the first 7 days for older patients admitted to ICU after non-‐cardiac surgery (NNT=13) and that the effect is largely confined to patients receiving abdominal surgery. The intervention reduces median ICU length of stay in delirious patients by 21.8 hours which is both clinically meaningful and statistically significant. There was no effect on the time to onset of delirium in delirious patients or any effect on hospital length of stay, either overall or for the delirious subgroup. The haloperidol dose used resulted in no adverse effects and is therefore safe. The authors conclude that further investigation is warranted.

© European Delirium Association 2012 www.europeandeliriumassociation.com
Editor’s Choice
The relationship between delirium duration, white matter integrity, and cognitive impairment in intensive care unit survivors as determined by diffusion tensor imaging: The VISIONS prospective cohort magnetic resonance imaging study* Morandi A, Rogers BP, Gunther MLet al for the VISIONS Investigation (VISualizing Icu SurvivOrs Neuroradiological Sequelae). Crit Care Med. 2012 Jul;40(7):2182-‐2189.
The association between brain volumes, delirium duration, and cognitive outcomes in intensive care unit survivors: The VISIONS cohort magnetic resonance imaging study* Gunther ML, Morandi A, Krauskopf E et al for VISIONS Investigation (VISualizing Icu SurvivOrs Neuroradiological Sequelae). Crit Care Med. 2012 Jul;40(7):2022-‐2032.
Neuroimaging offers a means to help unravel the pathogenesis of delirium. The Vanderbilt group in Nashville published 2 papers in the July edition of Critical Care Medicine which describe MRI findings on 47 patients who survived critical illness. These papers are worth looking up firstly because they add to the ever increasing body of evidence that suggest delirium results in actual brain damage; secondly they have excellent descriptions how MRI scanning can be used to determine pathological changes in the brain.
The first study demonstrated an association between delirium duration and white matter disruption using MRI with diffusion tensor imaging (DTI). White matter consists mostly of myelinated axons, white matter integrity is required to control consciousness and attention. The use of MRI with DTI provides investigators with quantitative assessment of the integrity of white matter and white matter tracts – fractional anisotropy. This study provided
preliminary data to inform the hypothesis connecting white matter integrity with delirium duration and long-‐term cognitive impairment.
The second paper showed that longer duration of delirium is associated with smaller brain volumes up to 3 months after discharge, and that smaller brain volumes are associated with long-‐term cognitive impairment up to 12 months. They did point out that they could not rule out that patients had smaller brain volumes before admission. The ventricle-‐to-‐brain ratio as determined by MRI is an excellent indicator of generalised brain atrophy. The authors illustrate their findings by comparing scans of 2 previously fit, cognitively intact women in their mid-‐forties only one of which suffered ICU delirium (figure 2).
Acute confusional States in the elderly-‐diagnosis and treatment. Lorenzl S, Füsgen I, Noachtar S. Dtsch Arztebl Int. 2012 May;109(21):391-‐400. Epub 2012 May 25.
This is a useful overview of delirium in the elderly from Deutsches Ärzteblatt International (even if it does not have delirium in the title!) It is free to download.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3371633/?tool=pubmed
Mental Illness – Comprehensive Evaluation or Checklist? P McHugh and P Slavney The New England Journal of Medicine 2012; 366: 1853-‐55
This excellent opinion piece discusses some of the issues relating to the Diagnostic and Statistical Manual of Mental Disorders -‐ DSM. The following quote hits the nail on the head regarding delirium.

© European Delirium Association 2012 www.europeandeliriumassociation.com
“Identifying a disorder by its symptoms does not translate into understanding it. Clinicians need some heuristic concept of its nature, grasped in terms of cause or mechanism, to render it intelligible and to justify their actions in practice and research”.
Free to read http://www.nejm.org/doi/full/10.1056/NEJMp1202555
Valerie Page
News
October Delirium Congress The European Delirium Association annual congress is in Bielefeld, Germany from October 18th to 19th. It is always a quality meeting so if you only go to one meeting a year -‐ make it this one!
Further details: www.eda2012bielefeld.org
European Survey – you can help The EDA has decided to conduct a survey to help understand the range of opinions among mailing list members on various aspect of delirium care. We greatly appreciate your expertise and we believe that this survey will provide a significant advancement in our understanding of current practice. The findings will be presented at EDA Bielefeld 2012, and submitted for publication in a peer-‐reviewed journal.
You can find the survey here: http://tiny.cc/gm2nbw
EDA membership benefits
• Access to the member’s only section of the EDA website • Reduction in the annual EDA conference registration fee • Eligibility to become EDA Board Member • Opportunities to contact and exchange ideas with delirium experts.
The annual fee is 30 Euros. This fee will be used to support development of the website, the costs of online Board meetings (around 200 Euros, twice per year), to underwrite our annual meeting, and for other costs. All accounts will be published annually
Payment may be by a standing order or by a cheque sent to John Young, Treasurer The bank account details: Royal Bank of Scotland, East Parade, Leeds, LS1 5PS, UK. Account no: 10147495 Sort Code: 16-‐23-‐17 IBAN& SWFT No: BG64RBOS16231710147495 John Young, Treasurer EDA, Professor of Elderly Care Medicine Academic Unit of Elderly Care and Rehabilitation Bradford Institute for Health Research Temple Bank House Bradford Royal Infirmary Duckworth Lane Bradford, UK, BD9 6RJ
Related Documents