Selected Technique Funnel Technique for EVAR: ‘‘A Way Out’’ for Abdominal Aortic Aneurisms With Ectatic Proximal Necks Salvatore Ronsivalle, 1 Francesca Faresin, 1 Francesca Franz, 1 Carlo Rettore, 2 Mario Zanchetta, 3 and Loretta Zonta, 2 Cittadella, Padua, Italy Background: To describe an endovascular technique for proximal stent-graft fixation in patients with an abdominal aortic aneurysm and an ectatic aortic neck. Methods: We describe a method in which using currently available devices in a hybrid assembly offers another option for circumventing the limitations of problematic proximal fixation. Conclusions: Through four examples, we illustrate the feasibility of placing a straight endograft as proximal extension of a bifurcated or aorto-uni-iliac graft in patients with a dilated proximal aortic neck. It appears secure and effective, with no type I endoleak or migration over a midterm follow-up. INTRODUCTION Endovascular aneurysm repair (EVAR) is used increasingly to treat abdominal aortic aneurysm (AAA) in patients with suitable anatomy. 1,2 However, as many as 20-50% of AAA patients have anatomy that is not suitable for endovascular repair. 3-5 Therefore, the adverse features of an individual’s vascular anatomy, such as the mor- phologic characteristics of the proximal and distal fixation sites, must be studied carefully to make decisions regarding the suitability and feasibility of endografting. Moreover, secure fixation and adequate sealing at the proximal and distal AAA necks are the most important factors in predicting a successful outcome of EVAR. Whereas the management of ectatic common iliac arteries by using iliac flared extension (bell- bottom) 6 has become an option used worldwide, it is not so easy to use when treating ectatic proximal aortic necks. In fact, there are no devices currently available for this purpose. Patients with ectatic necks often require complex surgical open repair, which is associated with high perioperative mortality and morbidity. In most patients, given the high anesthetic risk (ASA 3- ASA 4) due to comorbidity conditions, modifying the technique of EVAR may be required to success- fully exclude aneurysm. 5 One such modification is the ‘‘funnel technique.’’ As reported in an our previous case report, 7 we describe a method for stent-graft fixation in ectatic aortic necks in patients with AAA, in which using currently available devices in a hybrid assembly offers another option for circumventing the limita- tions of problematic proximal fixation (Fig. 1A). We use four clinical cases to illustrate the feasibility of placing a straight thoracic endograft as a proximal extension of a bifurcated aortic or aorto-uni-iliac endograft in patients with an abdominal aortic aneu- rysm and a dilated proximal aortic neck. 1 Department of Cardiovascular Disease, Vascular and Endovascular Surgery and Angiology, Cittadella Hospital, Cittadella, Padua, Italy. 2 Department of Radiology, Cittadella Hospital, Cittadella, Padua, Italy. 3 Division of Cardiology, Cittadella Hospital, Cittadella, Padua, Italy. Correspondence to: Salvatore Ronsivalle, MD, Department of Cardio- vascular Disease, Vascular and Endovascular Surgery, Via Riva dell’Ospedale, 35013 Cittadella, Padua, Italy, E-mail: vascolare_cit@ ulss15.pd.it Ann Vasc Surg 2012; 26: 141-148 DOI: 10.1016/j.avsg.2011.03.019 Ó Annals of Vascular Surgery Inc. Published online: November 2, 2011 141

Ann Vasc Surg 2012 Funnel Technique
Aug 09, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Selected Technique
Funnel Technique for EVAR: ‘‘A Way Out’’for Abdominal Aortic Aneurisms With EctaticProximal Necks
Salvatore Ronsivalle,1 Francesca Faresin,1 Francesca Franz,1 Carlo Rettore,2 Mario Zanchetta,3
and Loretta Zonta,2 Cittadella, Padua, Italy
Background: To describe an endovascular technique for proximal stent-graft fixation inpatients with an abdominal aortic aneurysm and an ectatic aortic neck.Methods: We describe a method in which using currently available devices in a hybridassembly offers another option for circumventing the limitations of problematic proximal fixation.Conclusions: Through four examples, we illustrate the feasibility of placing a straight endograftas proximal extension of a bifurcated or aorto-uni-iliac graft in patients with a dilated proximalaortic neck. It appears secure and effective, with no type I endoleak or migration over a midtermfollow-up.
INTRODUCTION
Endovascular aneurysm repair (EVAR) is usedincreasingly to treat abdominal aortic aneurysm(AAA) in patients with suitable anatomy.1,2
However, as many as 20-50% of AAA patientshave anatomy that is not suitable for endovascularrepair.3-5 Therefore, the adverse features of anindividual’s vascular anatomy, such as the mor-phologic characteristics of the proximal and distalfixation sites, must be studied carefully to makedecisions regarding the suitability and feasibilityof endografting.
Moreover, secure fixation and adequate sealingat the proximal and distal AAA necks are the most
important factors in predicting a successful outcomeof EVAR.
Whereas the management of ectatic commoniliac arteries by using iliac flared extension (bell-bottom)6 has become an option used worldwide, itis not so easy to use when treating ectatic proximalaortic necks.
In fact, there are no devices currently availablefor this purpose.
Patients with ectatic necks often require complexsurgical open repair, which is associated with highperioperative mortality and morbidity. In mostpatients, given the high anesthetic risk (ASA 3-ASA 4) due to comorbidity conditions, modifyingthe technique of EVAR may be required to success-fully exclude aneurysm.5
One suchmodification is the ‘‘funnel technique.’’As reported in an our previous case report,7 we
describe a method for stent-graft fixation in ectaticaortic necks in patients with AAA, in which usingcurrently available devices in a hybrid assemblyoffers another option for circumventing the limita-tions of problematic proximal fixation (Fig. 1A).
Weuse four clinical cases to illustrate the feasibilityof placing a straight thoracic endograft as a proximalextension of a bifurcated aortic or aorto-uni-iliacendograft in patients with an abdominal aortic aneu-rysm and a dilated proximal aortic neck.
1Department of Cardiovascular Disease, Vascular and EndovascularSurgery and Angiology, Cittadella Hospital, Cittadella, Padua, Italy.
2Department of Radiology, Cittadella Hospital, Cittadella, Padua,Italy.
3Division of Cardiology, Cittadella Hospital, Cittadella, Padua, Italy.
Correspondence to: Salvatore Ronsivalle, MD, Department of Cardio-vascular Disease, Vascular and Endovascular Surgery, Via Rivadell’Ospedale, 35013 Cittadella, Padua, Italy, E-mail: [email protected]
Ann Vasc Surg 2012; 26: 141-148DOI: 10.1016/j.avsg.2011.03.019! Annals of Vascular Surgery Inc.Published online: November 2, 2011
141

To guarantee a correct choice and positioning of theendograft it is mandatory to measure the ectatic neckdiameter and length, the AAA length and the distancebetween the lower renal artery and aortic carrefour.
Currently, aortic straight thoracic standard en-dografts (100 mm), straight thoracic custom-madeendografts, and both abdominal aortic bifurcatedand aorto-uni-iliac endografts are all available.
After careful examination of all the measure-ments, it is possible to plan the hybrid assembly toguarantee a correct proximal and distal sealing andan adequate component overlap.
TECHNIQUE, MATERIAL ANDMETHODS, AND RESULTS
Preoperative assessment included standard contrastarteriography with a marker catheter and computedtomography (CT) with intravenous contrast andimaging acquisition at 0.6-mm intervals.
Given the high anesthetic risk (ASA 3-ASA 4) dueto patients’ comorbidity conditions (chronic obstruc-tive pulmonary disease, hypertension, peripheraland carotid arterial disease, coronary artery diseasewith severely impaired left ventricular function), webelieved they could be candidates for EVAR.
The endovascular procedures were carried out inan operating room under fluoroscopic and angio-graphic guidance by a team of vascular surgeonsand interventional cardiologists.
A portable C-arm fluoroscopy device (ZIEHMIMAGING-Vision RFD mobile C-arm; ZIEHMIMAGING GmbH, Nuremberg, Germany) anda radiolucent operating table (MAQUET 115016B0Rastatt, Germany) were used.
Surgery was performed under general anesthesiaor regional anesthesia and local anesthesia in the arm.
Through an oblique incision of 3-4 cm below theinguinal ligament, the common femoral artery wasisolated in the groin bilaterally, and the deviceswere introduced over a stiff guidewire in a brachialartery femoral loop.
For endoleak prevention, all patients underwentEVAR with sac thrombization and stabilizationthrough intrasac biomaterial insertion.8
During follow-up, all patients underwent a colorduplex ultrasonography (CDU) at discharge, at 3, 6,and 12months, and once every 6months thereafter.For each patient, two abdominal radiographs weretaken, the first at discharge and the second a yearlater, and a spiral CT scan at 6 months.
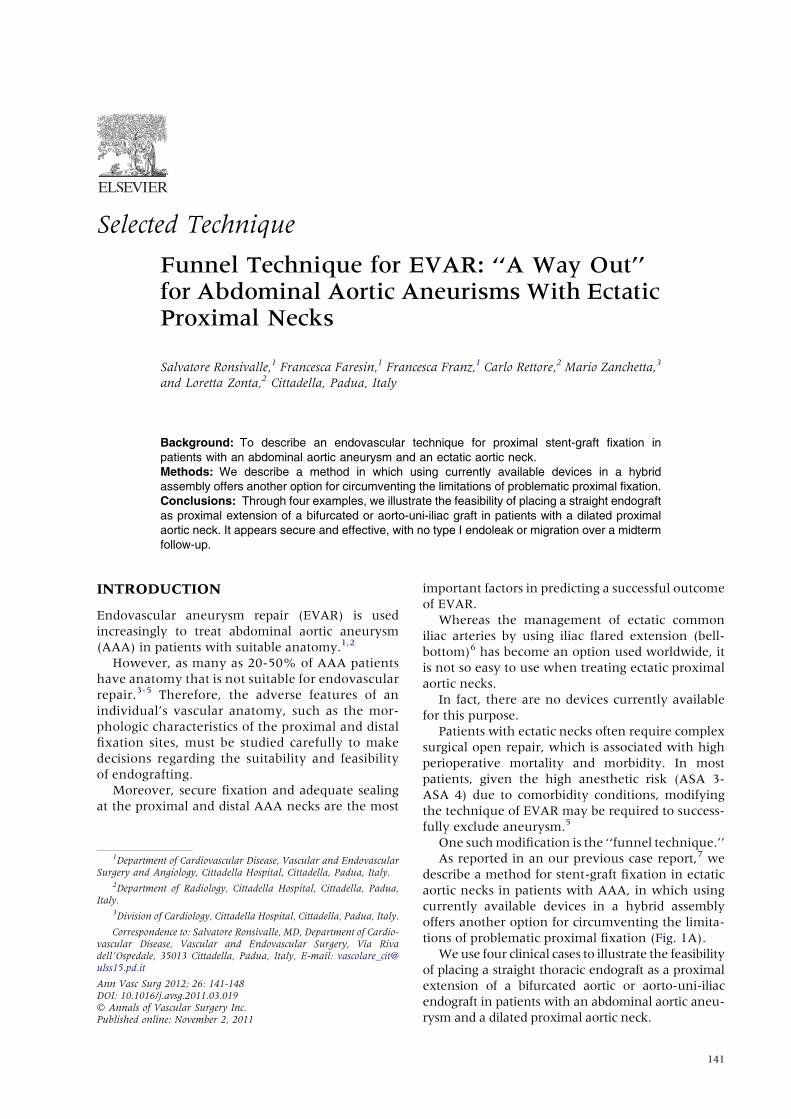
First case: R.O., an 84-year-old man diagnosedwith a 70-mm asymptomatic infrarenal AAA and
Fig. 1. (A) Currently available grafts; (B) Currently available grafts in a hybrid assembly.
142 Ronsivalle et al. Annals of Vascular Surgery
having an ectatic neck with a diameter of 38 mmand length of 32 mm.
A 34! 16! 170-mmTalent bifurcated stent-graftwas placed in the lower part of the aneurysm afterexamining the measurements and characteristicsof aneurysm and neck.
A 44-mm-diameter, 90-mm-long thoracic tubeendograft (Talent) with a 16-mm free-flow proximal
stent was selected on the basis of the adventitia-to-adventitia CT measurement of the aortic neck diam-eter, allowing 6 mm of oversizing (Fig. 2A). The tubegraft was delivered to the proximal neck through thebifurcated device via the ipsilateral femoral access; itwas deployed with at least 30 mm of overlap, leavingmore than40mmextending beyond themainbodyofthe bifurcated device to ensure expansion to its
Fig. 2. (A) First case’s graft in a hybrid assembly (thoracic graft 44-44-90 and aorto-bifurcated graft 34-16-170). (B) a:abdominal X-rays follow-up; b, c: postsurgery angio-CT scan follow-up.
Vol. 26, No. 1, January 2012 Funnel technique for EVAR 143
nominal diameter aswell as an adequate seal. An iliacextension was deployed into the left external iliacartery to obtain adequate distal vessel wall appositionand hemostatic seal. Finally, the sac was excluded byinserting twosequential iliac extensions fromthe inte-gral limb of the bifurcated stent-graft to the right CIAin a bell-bottom configuration.
The resultant ‘‘funnel configuration’’ at theinfrarenal aortic neck is evident on the control CTscan, which shows the intact structure of thecomposite three-component stent-graft, with noendoleak or migration (Fig. 2B).
The patient was regularly followed up; he died4 years later of prostatic cancer.
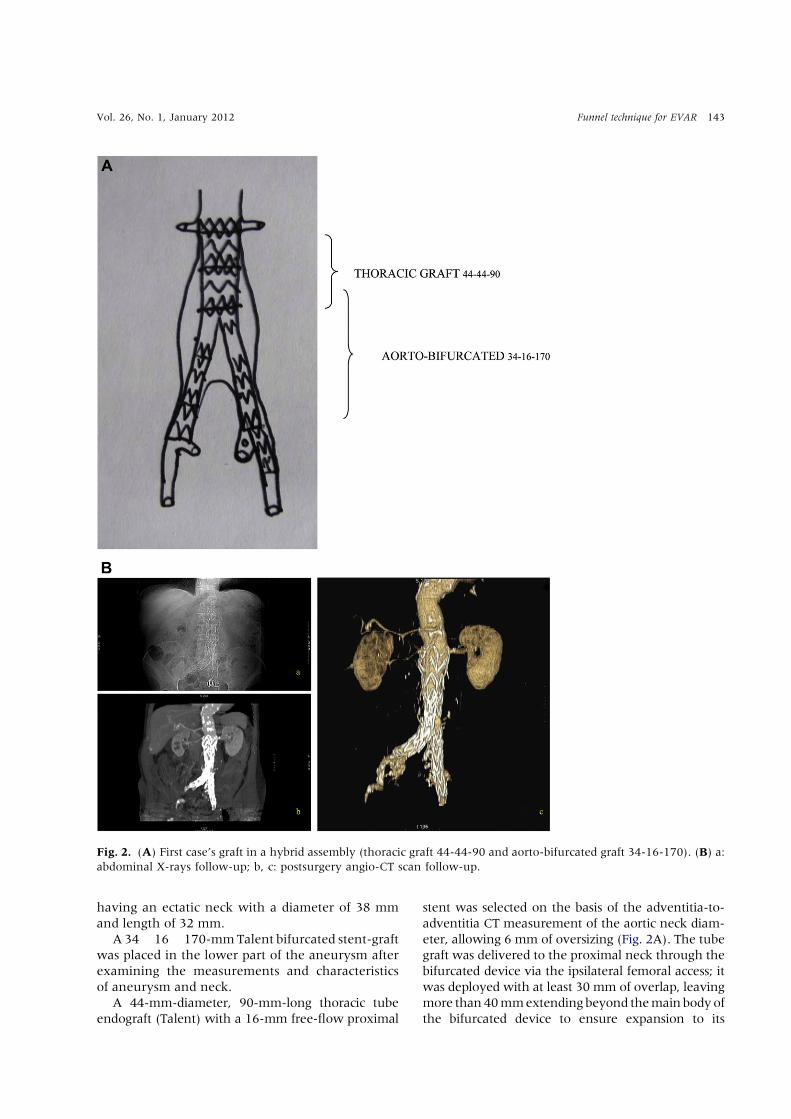
Fig. 3. (A) Second case’s graft in a hybrid assembly (thoracic graft 44-44-80 and aorto-bisiliac graft 34-18-170). (B)Presurgery (a) and postsurgery (b) angio-CT scan follow-up.
144 Ronsivalle et al. Annals of Vascular Surgery

During the follow-up, the aneurysmatic sacdiameter remained stable (69 mm at 3 months,68.6 mm at 6 months, 68.2 mm at 1 year, 68 mmat 2 years, 68 mm at 3 years).
Second case: T.A., a 77-year-old man hospitalizedwith a 74.7-mm asymptomatic infrarenal AAA, witha 35.3-mm-wide and 49.2-mm-long ectatic neck.
Given the measurements and characteristics ofaneurysm and neck, a bifurcated stent-graft (E-Vita 34 ! 18 ! 170 mm) and its contralateral rightleg 16 ! 18 ! 90 mm were chosen and placed inthe lower part of the aneurysm.
Thereafter, a thoracic stent-graft (E-Vita, custom-made 70SO4440508-00) was delivered to the prox-imal neck through the bifurcated device via the rightfemoral access (Fig. 3A).
It was deployed with at least 45 mm of overlap,leaving more than 35 mm extending beyond themain body of the bifurcated device to ensure expans-ion to its nominal diameter aswell as an adequate seal.
The postoperative CT scan demonstrates the fun-nel configuration at the infrarenal aortic neck andevidence of the intact structure of componentstent-graft, with no endoleak or migration (Fig. 3B).
The patient is stable after 2 years of follow-up.During the follow-up the aneurysmatic sac
diameter remained stable (74 mm at 3 months,73.8 mm at 6 months, 73.7 mm at 1 year. 73 mmafter 2 years).
Third case: R.M.A., a 74-year-old man was diag-nosed with a 60-mm asymptomatic infrarenalAAA, with a 36-mm-wide and 38.6-mm long ectaticneck (Fig. 4A).
We discovered that opening the contralateralgate limb to deliver a bifurcated stent-graft was notpossible due to the length and diameter of the ectaticneck, the length of AAA, and the distance betweenthe lower renal artery and aortic carrefour.
Therefore, an aorto-uni-iliac stent-graft (Talent36 ! 16 ! 124 mm) was placed in the lower partof the aneurysm.
Then, a thoracic extension (Valiant 40 ! 40 !100 mm) was delivered to the proximal neckthrough the device via the right femoral access.
Finally, an occluder (OCL22, Medtronic Cardio-Vascular, Santa Rosa, CA) was inserted in leftcommon iliac artery, and a righteleft femoro-femoral crossover bypass was sewn (Fig. 4B).
Fig. 4. (A) Presurgery angio-CT scan (a), diameter of theaneurysm neck (b), and diameter of the aneurysm (c).(B) Third case’s graft in a hybrid assembly (thoracic graft
40-40-100, aorto-uni-iliac graft 36-16-124, and occluderOCL22). (C) Postsurgery angio-CT scan follow-up.
Vol. 26, No. 1, January 2012 Funnel technique for EVAR 145
The resultant funnel configuration at the infrare-nal aortic neck is evident on the control CT scan,which shows the intact structure of componentstent-graft, with no endoleak or migration (Fig. 4C).
The patient is stable after 1 year of follow-up.During the follow-up, the aneurysmatic sac
diameter remained stable (59 mm at 3 months,58.8 mm at 6 months, 58.4 mm at 1 year).
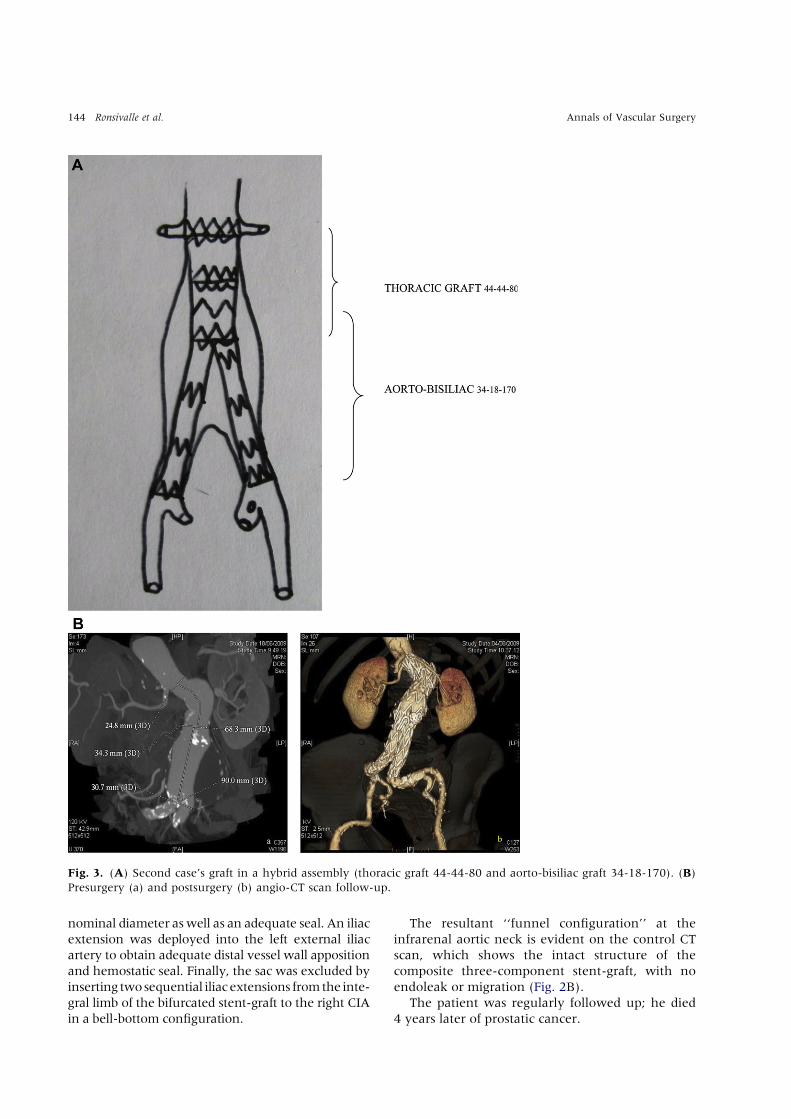
Fourth case: L.A., a 66-year-old man diagnosedwith a 69-mm asymptomatic abdominal aneurysmwith an ectatic neck with a diameter of 43 mmand a length of 43.3 mm; he had also an aneurysmof the thoracic aorta.
Given the particular characteristics of the aneu-rysm and neck, a bifurcated stent-graft (TalentLY3216C155) using the bilateral bell-bottom
Fig. 5. (A) Fourth case’s graft in a hybrid assembly (thoracic graft 44-44-80, aorto-bisiliac graft 32-15-155). (B) Post-surgery angio-CT scan follow-up.
146 Ronsivalle et al. Annals of Vascular Surgery

technique (Talent IXW, Q8 16x 22x 80 mm) wasplaced in the lower part of the aneurysm, anda custom made thoracic stentgraft E-Vita70SO4440508-00was accessed via ipsilateral femoralartery through the bifurcated device into the prox-imal neck (Fig. 5A).
It was deployed with at least 40 mm of overlap,leaving more than 40 mm extending beyond themain body of the bifurcated device to ensure expan-sion to its nominal diameter as well as an adequateseal.
In the same procedure, three thoracic stent-grafts,namely, E-vita 70SO4440S17-00, 70SO4444S17-00,and 70ST4040F15-00 were placed from the aorticisthmus under the left subclavian artery up to 1 cmfrom the celiac trunk in order to correct the thoracicaneurysm.
Again, the resulting funnel configuration at theinfrarenal aortic neck is evident on the controlCT scan showing the intact structure of componentstent-graft, with no endoleak or migration(Fig. 5B).
The patient is stable after 2 years of follow-up.During the follow-up, the aneurysmatic sac diam-
eter remained stable (68 mm at 3 months, 67.7 mmat 6 months, 67.6 mm at 1 year, 67 at 2 years).
DISCUSSION
Large or wide infrarenal necks in patients with AAAremain a challenge for endovascular interventionists.
Hybrid assembly with latest-generation devicesoffers another option for circumventing the limita-tions of problematic proximal fixation.
The funnel technique in which a straight thoracicstent-graft is placed through the main body ofa bifurcated or aorto-uni-iliac endograft may repre-sent an appealing alternative.
In all cases, the thoracic tube endograft wasdeployed with at least 30-40 mm of overlap toensure expansion to its nominal diameter as wellas an adequate seal.
A greater oversizing of 10% and central posi-tioning of the thoracic graft so that one-half ofits length extends into the native infrarenal aortaand the other into the bifurcated aortic or aorto-uni-iliac endograft are mandatory to ensureexpansion of the straight thoracic graft to itsnominal diameter to guarantee a correct proximalfixation and prevent type I endoleak or migrationdue to the loss of device fixation over a midtermfollow-up.
All the procedures were performed with Med-tronic or Jotec devices because these are theones that we are most familiar with and that
have shown to be best suitable to the characteris-tics of the grafts.
It is also possible to use other brands as longas they fit the patient’s anatomic measures andcharacteristics.
In all cases, the aneurysmatic sac diameterremained stable during the follow-up, but the obser-vational time was short.
The first patient died 4 years later of prostaticcancer, whereas the other patients are still beingregularly followed.
To prevent endoleaks, all patients undergo EVARwith sac thrombization and stabilization throughintrasac biomaterials insertion in our hospital.8
Our experience indicates a lower risk of type IIendoleak in patients who were treated with intrasac‘‘thrombization’’ during EVAR using biomaterialscompared to patients having undergone standardEVAR alone.8 They form a structure that acceleratesand consolidates the clot formation process forminga ‘‘concrete’’ compound, resulting in manifestinga durable, long-lasting, sturdy stabilization of thewhole complex fixed en bloc.8
Patients are also treated with brachial arteryfemoral loop. This technique allows for the deviceto advance more easily, overcoming kinking orstenosis, and therefore consenting to a more precisereleasing of the endograft in the presence of angled,flared, or short necks. This, in turn, enables thedevice to reach the iliac axis with less difficulty forthe positioning of the prosthetic contralateral leg.
CONCLUSIONS
These four cases illustrate the feasibility of placinga straight endograft as proximal extension of a bifur-cated or aorto-uni-iliac graft in patients withabdominal aortic aneurysm and a dilated proximalaortic neck.
These endograft configurations are found to besecure and effective, with no type I endoleak ormigration over a midterm follow-up.
REFERENCES
1. Malkawi AH, Hinchliffe RJ, Holt PJ, Loftus IM,Thompson MM. Percutaneous access for endovascular aneu-
rysm repair: a systematic review. Eur J Vasc Endovasc Surg
2010;39:676-682.
2. Dang W, Kilian M, Peterson MD, Cin!a C. Relationshipbetween access side used to deliver tha main body of bifur-
cated prosthesis for endovascular aneurysm repair and speed
of cannulation of the contralateral limb. J Vasc Surg 2010;51:
33-37.3. Elkouri S, Martelli E, Gloviczki P, et al. Most patients with
abdominal aortic aneurysm are not suitable for endovascular
Vol. 26, No. 1, January 2012 Funnel technique for EVAR 147

repair using currently approved bifurcated stent-grafts. Vasc
Endovasc Surg 2004;38:401-412.4. Sanchez LA; Talent eLps IDE Trial Investigators. Five-year
outcomes of the Medtronic Talent AAA StentdGraft
Pivotal IDE trial. Abstract presented at 2009 Society forvascular Surgery Annual Meeting, June 12, 2009, Den-
ver, CO.
5. Allaqaband S, Jan MF, Bajwa T. The chimney graft"- a simple
technique for endovascular repair of complex juxtarenalabdominal aortic aneurysm in no option patients. Catheter
Cardiovasc Interv 2010;75:1111-1115.
6. Kritpracha B, Pigott JP, Russel TE, et al. Bellebottom aortoil-
iac endografts: an alternative that preserves pelvic blood flow.J Vasc Surg 2002;35:874-881.
7. Zanchetta M, Faresin F, Pedon L, et al. Funnel technique for
first-line endovascular treatment of an abdominal aorticaneurysm with an ectatic proximal neck. J Endovasc Ther
2006;13:775-778.
8. Ronsivalle S, Faresin F, Franz F, Rettore C, Zanchetta M.
Aneurysm sac "thrombization" and stabilization in EVAR:a technique to reduce the risk of type II endoleak. J Endovasc
Ther 2010;17:517-524.
148 Ronsivalle et al. Annals of Vascular Surgery
Related Documents











