Page 1 Anesthesia for Thoracic Surgery: Challenging Cases • Lung Isolation: Practical aspects, pitfalls, DLTs vs BB • Lung Isolation for the Difficult Airway • Hypoxemia and Increased Airway Pressure During OLV • Preoperative Pulmonary Evaluation for Lung Resection • Anterior Mediastinal Mass • Postoperative Complications • Airway Management for Tracheal/carinal resection Hypoxemia and Increased Airway Pressure During One Lung Ventilation 76 y.o. 68 kg man w/ adenoCA for mediastinoscopy & R upper lobectomy • PMH: • Previous blunt chest trauma > multiple rib fx, splenectomy,tracheostomy and R chest tube • Cigarette smoking (30 pack years) •Pulmonary Function Testing • FEV 1 86% of predicted • DL CO 81% of predicted Malik: Anesth Analg 95:570, 2002 • Anesthesia Management - Radial artery catheter and T5 epidural inserted - Gen Anes induced - trachea intubated with 8.0 SLT - Following staging mediastinoscopy, a 35 Fr left- sided double-lumen tube was inserted. Correct positioning confirmed by fiberoptic visualization through tracheal and bronchial lumens. - Patient positioned for surgery and tube position reconfirmed via fiberscope Hypoxemia and Increased Airway Pressure During One Lung Ventilation • Anesthesia Management (cont) - During two-lung ventilation: VT E 600 ml, PIP 16 cm H 2 O, f 10 and SpO 2 99% - One-lung ventilation initiated at thoracotomy VT E 550 ml, PIP 28 cm H 2 O, and SpO 2 98% - Within 10 minutes of one-lung ventilation: VT E 150 ml, PIP 60 cm H 2 O, SpO 2 87% Systolic BP decreased from 120 to 85 mm Hg - Two-lung ventilation resumed VT E 360 ml, PIP 36 cm H 2 O, SpO 2 96% BP supported with phenylephrine – WHAT NOW? Hypoxemia and Increased Airway Pressure During One Lung Ventilation Anesthesia Management (cont) • Differential diagnosis & Next steps • DLT position checked - Fiberoptic visualization via tracheal lumen > no change. - Fiberoptic visualization via bronchial lumen > no secretions but…. - DLT malposition, light anesthesia, secretions, bronchospasm, anaphylaxis, pneumothorax Hypoxemia and Increased Airway Pressure During One Lung Ventilation Left Upper Lobe Left Lower Lobe

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Page 1
Anesthesia for Thoracic Surgery: Challenging Cases
• Lung Isolation: Practical aspects, pitfalls, DLTs vs BB
• Lung Isolation for the Difficult Airway
• Hypoxemia and Increased Airway Pressure During OLV
• Preoperative Pulmonary Evaluation for Lung Resection
• Anterior Mediastinal Mass
• Postoperative Complications
• Airway Management for Tracheal/carinal resection
Hypoxemia and Increased Airway Pressure During One Lung Ventilation
76 y.o. 68 kg man w/ adenoCA for mediastinoscopy & R upper lobectomy
• PMH:
• Previous blunt chest trauma > multiple rib fx, splenectomy,tracheostomy and R chest tube
• Cigarette smoking (30 pack years)
• Pulmonary Function Testing
• FEV1 86% of predicted
• DLCO 81% of predicted Malik: Anesth Analg 95:570, 2002
• Anesthesia Management
- Radial artery catheter and T5 epidural inserted - Gen Anes induced - trachea intubated with 8.0 SLT - Following staging mediastinoscopy, a 35 Fr left- sided double-lumen tube was inserted. Correct
positioning confirmed by fiberoptic visualization through tracheal and bronchial lumens.
- Patient positioned for surgery and tube position reconfirmed via fiberscope
Hypoxemia and Increased Airway Pressure During One Lung Ventilation
• Anesthesia Management (cont) - During two-lung ventilation:
VTE 600 ml, PIP 16 cm H2O, f 10 and SpO2 99% - One-lung ventilation initiated at thoracotomy
VTE 550 ml, PIP 28 cm H2O, and SpO2 98% - Within 10 minutes of one-lung ventilation: VTE 150 ml, PIP 60 cm H2O, SpO2 87%
Systolic BP decreased from 120 to 85 mm Hg
- Two-lung ventilation resumed VTE 360 ml, PIP 36 cm H2O, SpO2 96%
BP supported with phenylephrine – WHAT NOW?
Hypoxemia and Increased Airway Pressure During One Lung Ventilation
Anesthesia Management (cont) • Differential diagnosis & Next steps
• DLT position checked - Fiberoptic visualization via tracheal lumen
> no change. - Fiberoptic visualization via bronchial lumen
> no secretions but….
- DLT malposition, light anesthesia, secretions, bronchospasm, anaphylaxis, pneumothorax
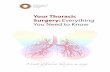
Hypoxemia and Increased Airway Pressure During One Lung Ventilation
Left Upper Lobe
Left Lower Lobe

Page 2
Heart DLT
Management (cont) • Left chest tube inserted
- Respiratory mechanics, oxygen exchange and blood pressure improved during OLV
(VTE 550 ml, PIP 30 cm H2O, and SpO2 98%) • Fiberoptic visualization via bronchial lumen now showed ….
Hypoxemia and Increased Airway Pressure During One Lung Ventilation
Left Upper Lobe
Left Lower Lobe
Contralateral Tension Pneumothorax During One-lung Ventilation
• Dependent-lung tension pneumothorax is a feared but RARE complication during OLV • Etiology in this patient is uncertain • Potential mechanisms include
- Barotrauma - Could the undersized 35 Fr DLT have permitted initial placement in lobar bronchus such that the entire tidal volume was directed to one lobe?
- Air trapping exacerbated by the 35 Fr DLT - Tracheobronchial injury during DLT placement - Lung injury from epidural, CVP, or mediastinoscopy
Benumof, Anesthesia for Thoracic Surgery 2nd ed, 1995
Distribution of Pulmonary Blood Flow
Benumof, Anesthesia for Thoracic Surgery 2nd ed, 1995
Determinants of Blood Flow Distribution During OLV

Page 3
Arterial PaO2 During Lateral Thoracotomy
Katz, Anesthesiology 56:164, 1981
Preoperative Pulmonary Blood flow to the Operative Lung and PaO2 During One-lung Ventilation
Hurford: Anesthesiology 67:841, 1987
- Facilitate lung collapse: • FI O2 ~ 1.0 prior to OLV, then titrate - Lung protective ventilation: • VT 5 - 6 ml/kg, PEEP 5 cm H2O • Adjust respiratory frequency but avoid PEEPi • Recruitment maneuvers PRN • PCV appealing but has not been shown
to provide important benefit. - Mild hypercapnia acceptable – check ABG
Management of One-lung Ventilation Treatment Strategies for Hypoxemia During OLV
Increase FIO2 to 1.0 Precipitous O2 Desaturation
• Stop Surgery • Two-lung ventilation • F.O.B.
Treat Cause Ventilated lung
Adjust DLT position Aspirate secretions / blood
Recruitment maneuvers Nonventilated lung
Increase PO2 in Alveolus Decrease perfusion
Improve Cardiac Output Consider RV dysfunction
Decrease Anesthetic Optimize blood volume Does pt. have PFO?
Think about RAP vs LAP
Gradual O2 Desaturation
• Continue OLV • Verify saturation • F.O.B. • Optimize V/Q
SpO2 < 90%
Ventilator
Dependent Lung Recruitment - Temporary Hyperinflation - PEEP titration
é Perfusion - Limit PEEPi - Inhaled NO
ê Perfusion - Clamp PA - IV Almitrine (increases HPV)
Options to Improve Oxygenation During OLV
Rozé. Anesthesiology 114:167, 2011
- CPAP w/ O2 - Intermittent Inflation w/ O2
Composite data Slinger, ANESTHESIA 7th ed, 2010
For pts w/ COPD CPAP more effective than PEEP

Page 4
Related Documents






![Clinical Research in Pulmonology€¦ · embolism, high-risk surgery (e.g., thoracic or major abdominal surgery), and an anesthesia duration of more than 3 hours [1,2]. Risk factors](https://static.cupdf.com/doc/110x72/60615dbe89868e648942a333/clinical-research-in-pulmonology-embolism-high-risk-surgery-eg-thoracic-or.jpg)