ANEMIA FREE PREGNANCY

Anemia Free Pregnancy
Dec 15, 2015
Anemia In Pregnancy
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ANEMIA FREE PREGNANCY
DEFINITION OF ANEMIA
Deficiency in the oxygen-carrying capacity of the blood due to a diminished erythrocyte mass.
May be due to:Erythrocyte loss (bleeding)Decreased Erythrocyte production
low erythropoietinDecreased marrow response to erythropoietin
Increased Erythrocyte destruction (hemolysis)

MEASUREMENTS OF ANEMIA
• Hemoglobin = grams of hemoglobin per 100 mL of whole blood (g/dL)
• Hematocrit = percent of a sample of whole blood occupied by intact red blood cells
• RBC = millions of red blood cells per microL of whole blood
• MCV = Mean corpuscular volume• If > 100 → Macrocytic anemia• If 80 – 100 → Normocytic anemia• If < 80 → Microcytic anemia
• RDW = Red blood cell distribution width• = (Standard deviation of red cell volume ÷ mean cell volume) ×
100 • Normal value is 11-15%• If elevated, suggests large variability in sizes of RBCs
LABORATORY DEFINITION OF ANEMIA
• Hb:• Women: <12.0• Men: < 13.5
• Hct:• Women: < 36• Men: <41

SYMPTOMS OF ANEMIA
• Decreased oxygenation• Exertional dyspnea• Dyspnea at rest• Fatigue• Bounding pulses• Lethargy, confusion
• Decreased volume• Fatigue• Muscle cramps• Postural dizziness• syncope
SPECIAL CONSIDERATIONS IN DETERMINING ANEMIA
• Acute Bleed• Drop in Hgb or Hct may not be shown until 36 to 48
hours after acute bleed (even though patient may be hypotensive)
• Pregnancy• In third trimester, RBC and plasma volume are
expanded by 25 and 50%, respectively.• Labs will show reductions in Hgb, Hct, and RBC
count, often to anemic levels, but according to RBC mass, they are actually polycythemic
• Volume Depletion• Patient’s who are severely volume depleted may not
show anemia until after rehydrated

IRON DEFICIENCY ANEMIA

IRON DEFICIENCY ANEMIA - KOILONYCHIA
IRON DEFICIENCY ANEMIA – LAB FINDINGS
• Serum Iron• LOW (< 60 micrograms/dL)
• Total Iron Binding Capacity (TIBC)• HIGH ( > 360 micrograms/dL)
• Serum Ferritin• LOW (< 20 nanograms/mL)• Can be “falsely”normal in inflammatory states

Prevalence of anaemia Source: WHO
Global Developed Developing India Urban Rural
Children<5 yrs 43 12 51 60 70Children > 5yrs 37 7 46 50 60Men 18 3 26 35 45Women 35 11 47 50 60Pregnant 59 14 51 65 75Women
About one third of the global population ( over 2 billion persons ) are anaemic .
Anaemia is the most common nutritional deficiency disorder in the world
Prevalence of anaemia is higher in developing countries Prevalence of anaemia in India is very high in all groups of
the population
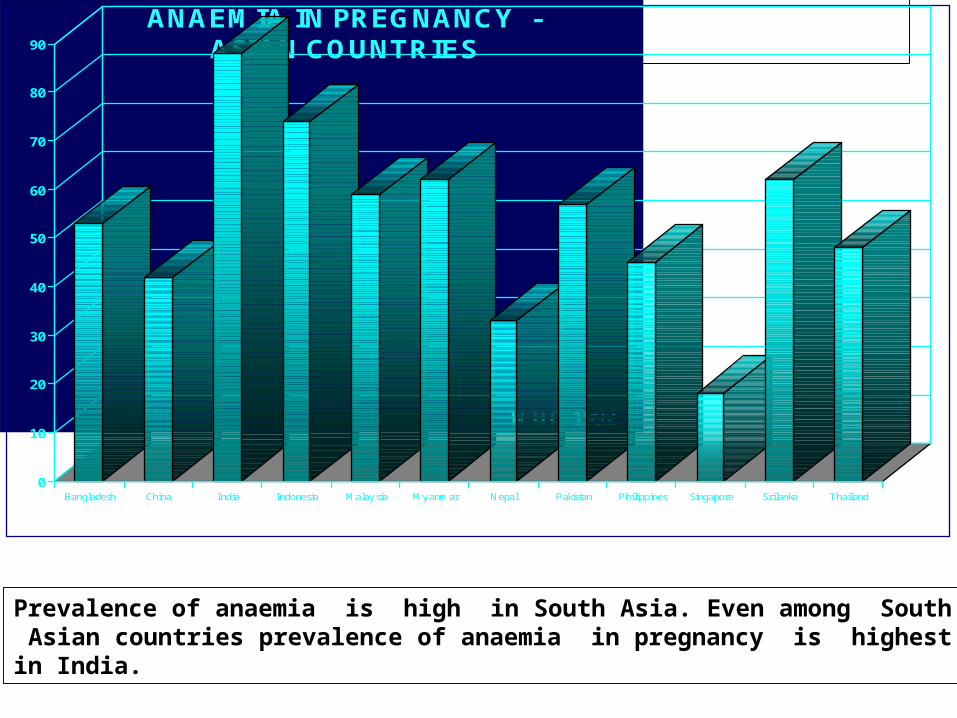
AN AEM IA IN PR EG NA NC Y -
ASIA N CO U NTR IES
W H O 1992
0
10
20
30
40
50
60
70
80
90
Bangladesh China India Indonesia Malaysia Myanmar Nepal Pakistan Philippines Singapore Srilanka Thailand
Prevalence of anaemia is high in South Asia. Even among South Asian countries prevalence of anaemia in pregnancy is highest in India.

YEAR AUTHOR PLACE PREVALENCE %
1975 Sood et al Delhi 80
1982 Prema Hyderabad 75
1987 Agarwal et al Bihar & UP 87
1989 Christian et al Chandrapur, Panchmahal 87,88
1988-92 Agarwal et al Rural Varanasi 94
1989 ICMR 11 states 87
1994 Sheshadri Baroda 74
2000 NFHS 2 All India 52.0?
99- 2000 ICMR 11 states 84.6
2002-04 DLHS –2 All districts 90.4
2006 NNMB 8 states 70.3
2007 MFHS 3 All India 57.9?
Trends in prevalence of anaemia in pregnant women in India
Over 70 % of pregnant women in India are anaemic. There has been no decline
in anaemia in the last three decades

Prevalence of Anaemia (%){DLHS 2003}
0%
20%
40%
60%
80%
100%
preschoolchildren
adolescent girls pregnant w omen
Group
Perc
enta
ge
severe moderate mild no anaemia
Anaemia begins in childhood, worsens during adolescence in girls and gets aggravated during pregnancy

Source: NNMB 2003
Among the southern states, prevalence of anaemia in pregnancy is lower in Kerala and Tamil Nadu -?due to better access to health care

Anaemia pregnant women, India (Age between 15 - 44 years)
50.9
52.9
51.4
36
36
36
3
2
3
RURAL
URBAN
TOTAL
Mild Moderate Severe
Source : DLHS2
DLHS –2 showed that over 90% of pregnant women are anaemic both in urban and in rural areas

Prevalence of anaemia in children, adolescent girls and pregnant women from 3 surveys
0
20
40
60
80
100
NNMB ICMR DLHS NNMB ICMR DLHS NNMB DLHS
Pregnant w omen Adolescent girls Children
Normal Mild Moderate Severe
Source NNBM
Majority of children, adolescents, adult men& women are anaemic.Anaemia antedates pregnancy& gets aggravated during pregnancy. Maternal
anaemia results in poor iron stores in foetus
Prevalence anaemia in children is high because of poor iron stores, low iron content of breast milk and complementary foods.
There is thus an intergenerational self perpetuating vicious cycle of anaemia in all age groups

Prevalence of anaemia in adolescent girls & pregnant women by education & standard of living index
0
20
40
60
80Ill
itera
te
0-9
yrs
>10yr
s
Low
Mediu
m
Hig
h
Illite
rate
0-9
yrs
>10yr
s
Low
Mediu
m
Hig
h
Education Standard of livingindex
Education Standard of livingindex
Adolescent girls Pregnant women Severe ModerateSource: Ref 7.11.1.6
Prevalence of anaemia is high even in high income groups and among well educated pregnant women

Why is anemia so common
Major causes of anemia
Inadequate iron, folate intake due to low vegetable consumption and perhaps low B12 intake Poor bioavailability of dietary iron from the fibre, phytate rich Indian diets Chronic blood loss
Increased requirement of iron during pregnancy
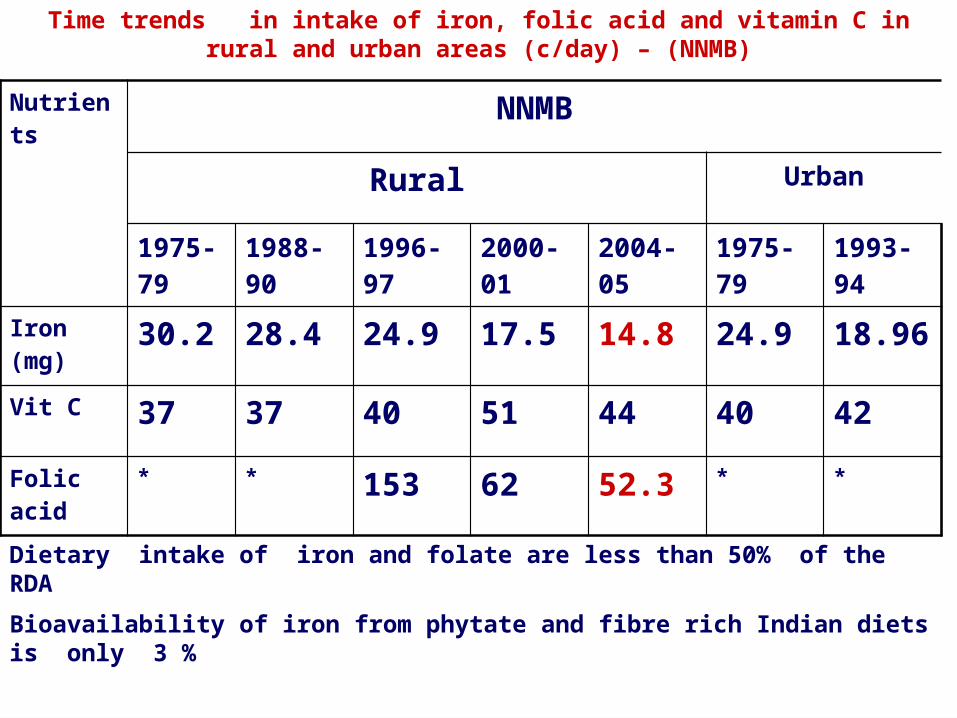
Nutrients NNMB
Rural Urban
1975-79
1988-90 1996-97 2000-01 2004-05 1975-79 1993-94
Iron (mg) 30.2 28.4 24.9 17.5 14.8 24.9 18.96
Vit C 37 37 40 51 44 40 42
Folic acid
* * 153 62 52.3 * *
Time trends in intake of iron, folic acid and vitamin C in rural and urban areas (c/day) – (NNMB)
Dietary intake of iron and folate are less than 50% of the RDA
Bioavailability of iron from phytate and fibre rich Indian diets is only 3 %

Time trends in intake of iron (mg / day) in different groups
Age group 1975-79 1996-97 2000-01 2004-05
10-12B 19 20 12.2 12G 18 19 12.1 11.5
13-15B 21 21 15.4 13.3G 20 21 12.9 13
16-17B 25 26 16.7 16.4G 22 22 15.3 13.4
Adult males 26 27 17.5 19.6Adult females(NPNL) 21 22 17.1 13.8
Pregnant women 20 23 14 14Lactating women 23 23 14.6 14.7
Iron intake is low in all age groups and does not increase in pregnancy; there has been no increase in iron intake over 3 decades
Why is anaemia in pregnancy a cause of grave concern

INDIA
India’s share in global maternal deaths
It is estimated that globally there are over 5 lakh maternal deaths every year.
There are about 1 to 1.2 lakh maternal deaths in India every year
India with 16% global population accounts for 20-25 % % of all maternal deaths in the world
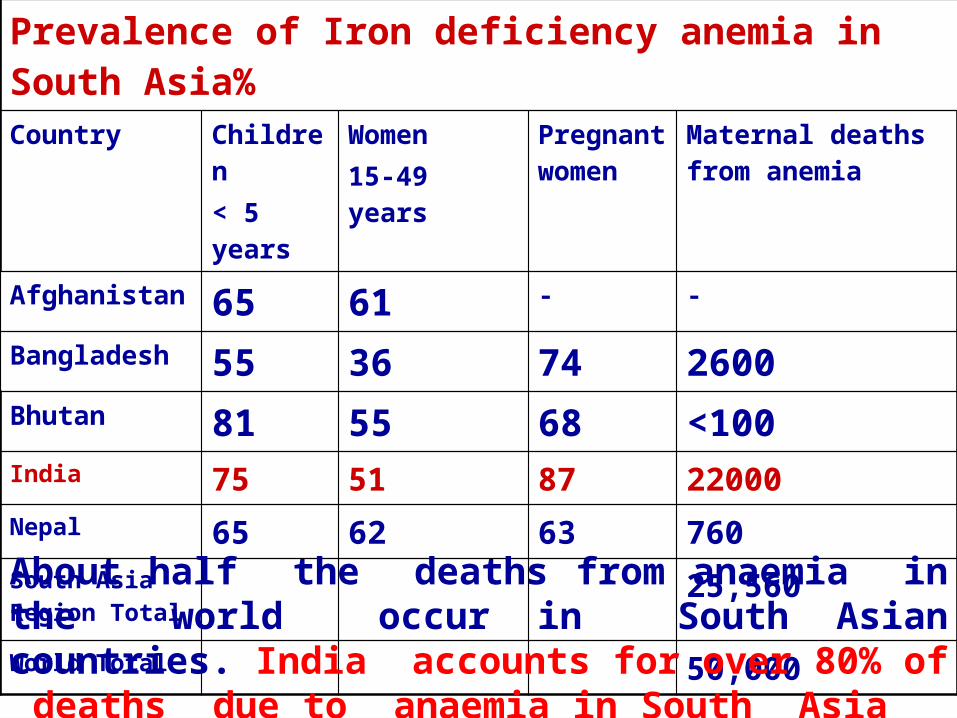
Prevalence of Iron deficiency anemia in South Asia% Country Children
< 5 yearsWomen15-49 years
Pregnant women
Maternal deaths from anemia
Afghanistan 65 61 - -
Bangladesh 55 36 74 2600Bhutan 81 55 68 <100India 75 51 87 22000Nepal 65 62 63 760South Asia Region Total
25,560
World Total 50,000About half the deaths from anaemia in the world occur in South Asian countries. India accounts for over 80% of deaths due to anaemia in South Asia

Hemorrhage30%
Anemia19%
Sepsis16%
Abortion9%
Obst. Lab10%
Toxemia8%
Others8%
CAUSES OF MATERNAL MORTALITY SRS-1998
Anaemia directly causes 20% of maternal deaths and indirectly accounts for another 20% of maternal deaths.These figures have remained unchanged in the last five decades

CONSEQUENCES OF ANAEMIA IN PREGNANCY
• 8-11 g/dL: easy fatigability, poor work capacity • 5-7.9 g/dL: impaired immune function, increased
morbidity due to infections • <5 g/dL: compensated stage: increased morbidity and
maternal mortality due to inability to withstand even small amount of bleeding during pregnancy /delivery and increased risk of infections
• <5 g/dL: decompensated stage about 1/3rd develop severe congestive cardiac failure and many with congestive failure succumb either during pregnancy or during labour
• There is 8 to 10 fold increase in MMR when the Hb is <5 g%
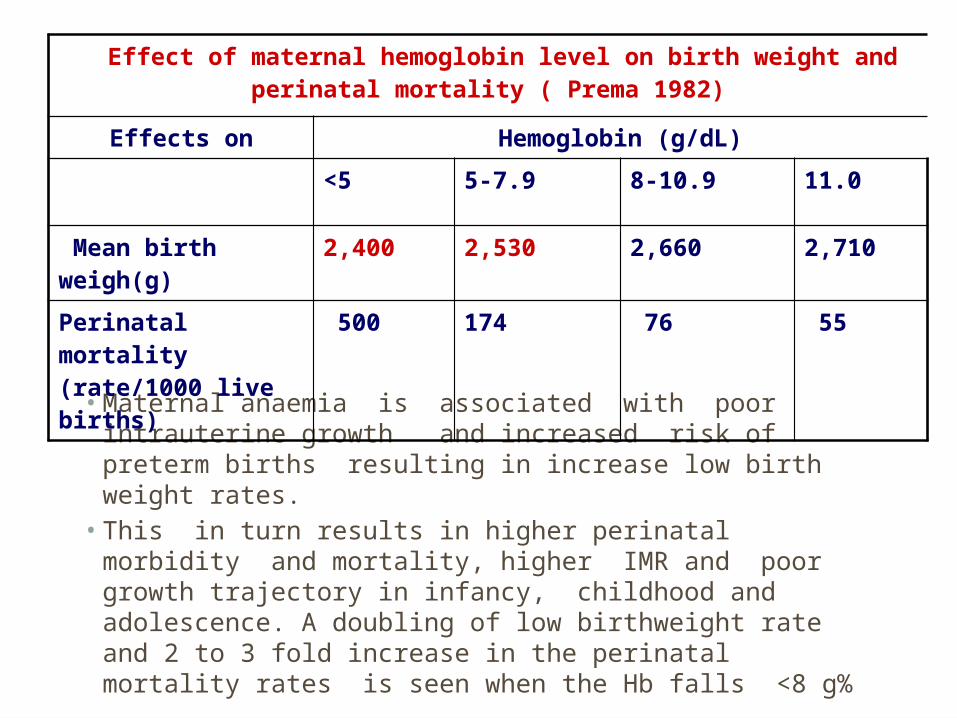
• Maternal anaemia is associated with poor intrauterine growth and increased risk of preterm births resulting in increase low birth weight rates.
• This in turn results in higher perinatal morbidity and mortality, higher IMR and poor growth trajectory in infancy, childhood and adolescence. A doubling of low birthweight rate and 2 to 3 fold increase in the perinatal mortality rates is seen when the Hb falls <8 g%
Effect of maternal hemoglobin level on birth weight and perinatal mortality ( Prema 1982)
Effects on Hemoglobin (g/dL)
<5 5-7.9 8-10.9 11.0
Mean birth weigh(g) 2,400 2,530 2,660 2,710
Perinatal mortality (rate/1000 live births)
500 174 76 55
IMMUNE STATUS OF ANAEMIC PREGNANT WOMEN
• There is a fall in T and B cell count when maternal Hb is below < 11 g/dL
• The fall in T and B cell counts are significant when Hb is <8g/dL
• There is no alterations in lymphocyte transformation or in cell mediated immunity
• Prevalence of morbidity due to infections including asymptomatic bacteriuria is higher in anaemic pregnant women
• Higher morbidity rates might contribute to the higher low birth-weight rates in anaemic pregnant women

TREATMENT

MANAGEMENT OF IDA
Blood transfusion if heart failure is eminentIV or IM iron in pregnant womenOral iron 3-5 mg Fe/kg/dayTreat underlying causeDietary education
UNTOWARD EFFECTS OF ORAL IRON PREPARATIONS
• Gastrointestinal side-effects such as epigastric discomfort, nausea, vomiting, constipation, and diarrhoea
• The frequency of these side-effects is directly related to the dose of iron or % of elemental iron in tablet
• Iron consumed with a meal is better tolerated than when it is taken on an empty stomach
• Although the amount of iron absorbed is reduced• Liquid preparations may cause blackening of teeth
and makes faeces black due to formation of iron sulfide and metallic taste
LIMITATIONS OF CURRENT ORAL IRON THERAPY

• .Large number of iron salts is available in market
• In clinical practice oral iron supplementation commonly used are Fe sulfate, Fe fumarate
• These conventional iron preparations are cheap
• But have more gastrointestinal intolerance
DRAWBACKS OF CONVENTIONAL DOSAGE FORM
• Poor patient compliance, increased chances of missing the dose of a drug with short half-life for which frequent administration is necessary
• The unavoidable fluctuations in drug concentration may lead to under medication or over medication
• A typical peak-valley plasma concentration time profile is obtained which makes attainment of steady-state condition difficult
• The fluctuations in drug levels may lead to precipitation of adverse effects especially of a drug with small therapeutic index whenever over medication occur
Dusane Abhijeet Ratilal et al/ IJRAP 2011, 2(6) 1701-1708

The major reason for the failure of iron therapy is non-compliance due to
the side-effects caused by an excessively high initial dose of iron.

THE SOLUTION
Use of Slow-release preparations instead of conventional iron

BENEFITS OF MODIFIED DRUG DELIVERY SYSTEM
• Decrease in dosing frequency• Reduced peak to trough ratio of drug in systemic
circulation• Reduced rate of rise of drug concentration in
blood• Sustained and consistent blood level within the
therapeutic window• Enhanced bioavailability• Customized delivery profile• Reduced side effects• Improved patient compliance
Dusane Abhijeet Ratilal et al/ IJRAP 2011, 2(6) 1701-1708

Related Documents











