Anatomy of Anterior Cruciate Anatomy of Anterior Cruciate Ligament Ligament By- Dr. Armaan Singh By- Dr. Armaan Singh

Anatomy of anterior_cruciate_ligament_by- dr. armaan singh
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Anatomy of Anterior Cruciate Anatomy of Anterior Cruciate LigamentLigament
By- Dr. Armaan SinghBy- Dr. Armaan Singh
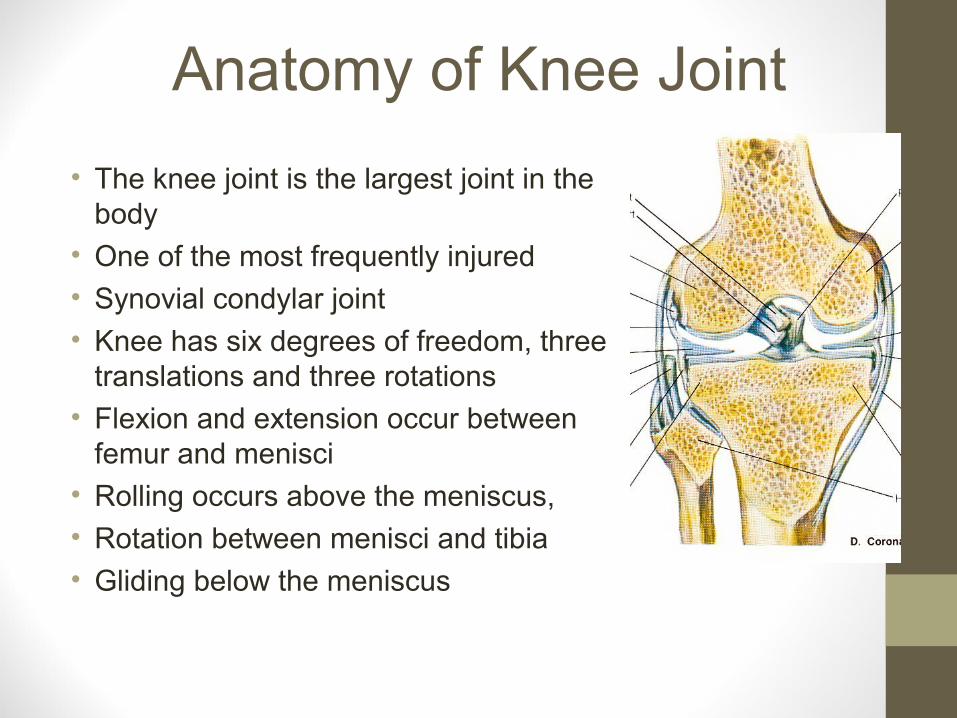
Anatomy of Knee Joint
• The knee joint is the largest joint in the body
• One of the most frequently injured
• Synovial condylar joint
• Knee has six degrees of freedom, three translations and three rotations
• Flexion and extension occur between femur and menisci
• Rolling occurs above the meniscus,
• Rotation between menisci and tibia
• Gliding below the meniscus
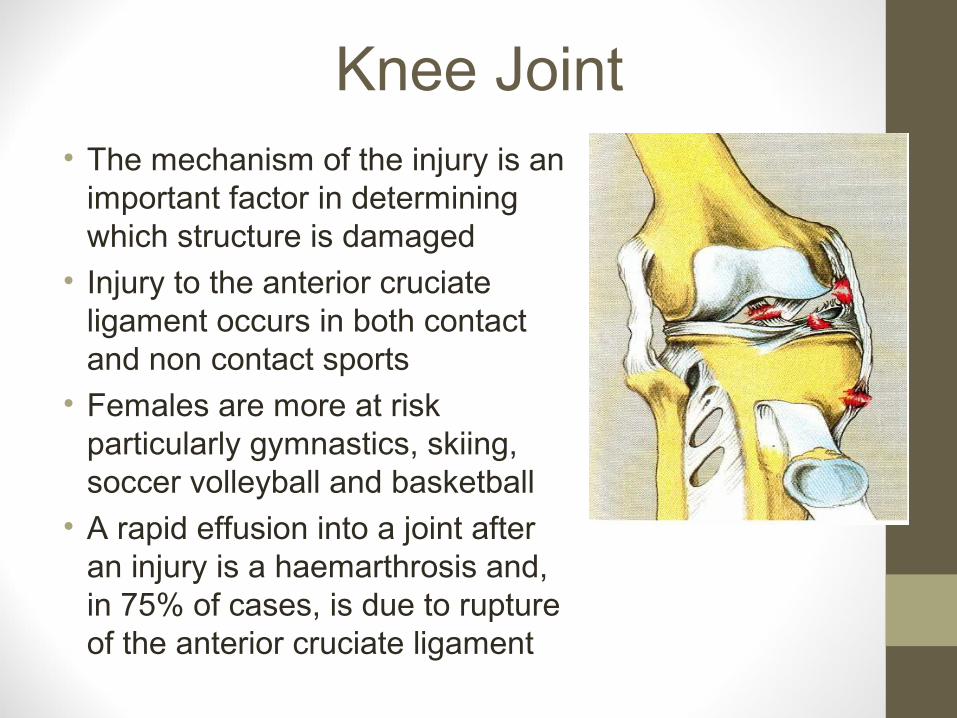
Knee Joint• The mechanism of the injury is an
important factor in determining which structure is damaged
• Injury to the anterior cruciate ligament occurs in both contact and non contact sports
• Females are more at risk particularly gymnastics, skiing, soccer volleyball and basketball
• A rapid effusion into a joint after an injury is a haemarthrosis and, in 75% of cases, is due to rupture of the anterior cruciate ligament
Close-Packed• Stable position
• Surfaces fit together
• Ligaments taut
• Spiral twist
• Screw home articular surface
Least-Packed
• Joint more likely to be injured least-packed
• Capsule slackest
• Joint held in this
• Position when injured
• Knee in 20°flexion

Articular Surfaces• The femoral articular
surfaces are the medial and lateral femoral condyles
• The medial condyle has a longer articular surface
• The superior aspect of the medial and lateral tibial condyles
• The posterior aspect of the patella
ACL

Articular Surfaces• Two condyles are separated behind
by the intercondylar notch
• Joined in front by the trochlear surface for the patella
• Femoral condyles are eccentrically curved
• Medial is of more constant width. It is narrow, longer and more curved
• Lateral condyle is broad and straight and diverges slightly distally and posteriorly, wider in front than at the back
Last, 1984
medial

Femoral Condyles
• The radius of the condyles' curvature isin the saggital plane,
• Becomes smaller toward the back
• This diminishing radius produces a series of involute midpoints (i.e. located on a spiral)
• The resulting series of transverse axes, permit the sliding and rolling motion in the flexing knee
• While ensuring the collateral ligaments are sufficiently lax to permit the rotation associated with the curvature of the medial condyle about a vertical axis
Platzer, 2004
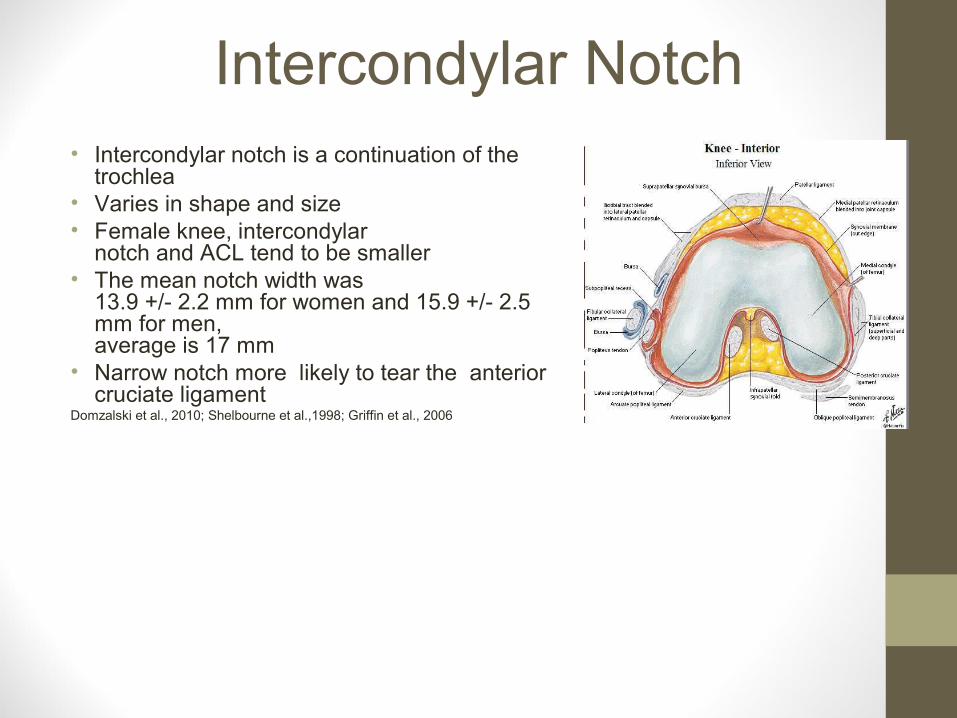
Intercondylar Notch• Intercondylar notch is a continuation of the
trochlea • Varies in shape and size• Female knee, intercondylar
notch and ACL tend to be smaller• The mean notch width was
13.9 +/- 2.2 mm for women and 15.9 +/- 2.5 mm for men, average is 17 mm
• Narrow notch more likely to tear the anterior cruciate ligament
Domzalski et al., 2010; Shelbourne et al.,1998; Griffin et al., 2006
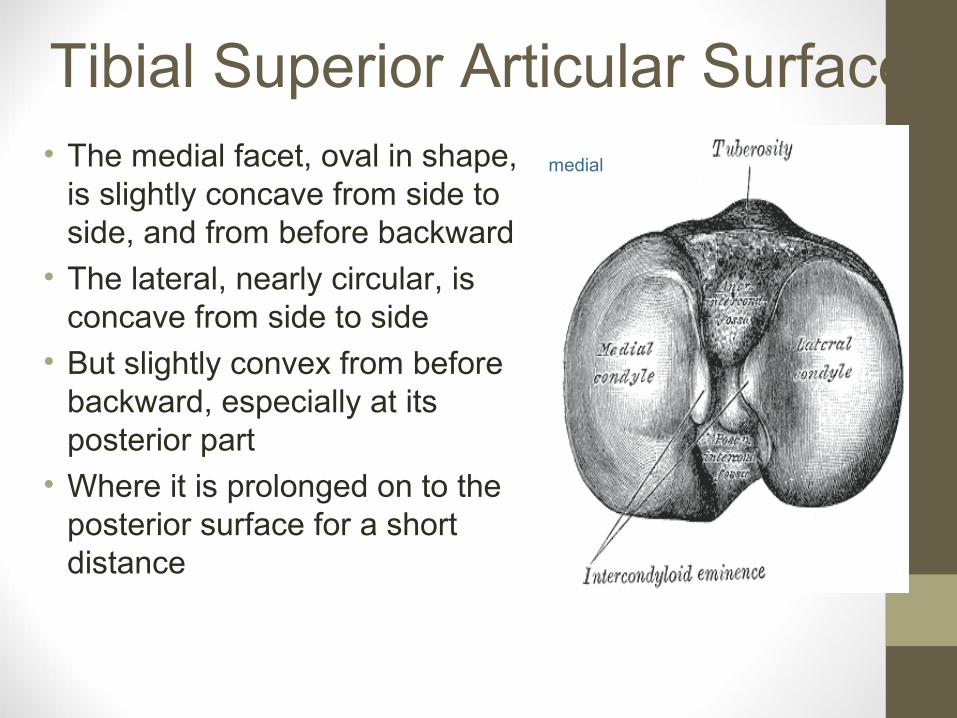
Tibial Superior Articular Surface• The medial facet, oval in shape,
is slightly concave from side to side, and from before backward
• The lateral, nearly circular, is concave from side to side
• But slightly convex from before backward, especially at its posterior part
• Where it is prolonged on to the posterior surface for a short distance
medial

• The central portions of these facets articulate with the condyles of the femur
• Their peripheral portions support the menisci of the knee-joint
• The intercondylar eminence is between the articular facets
• Nearer the posterior than the anterior aspect of the bone
Tibial Superior Articular Surface

Tibial Superior Articular Surface• In front and behind the
intercondylar eminence are rough depressions for the attachment of the anterior and posterior cruciate ligaments and the menisci
• The shape of the cruciate attachments vary
anterior
ACL
lateral meniscus
PCL
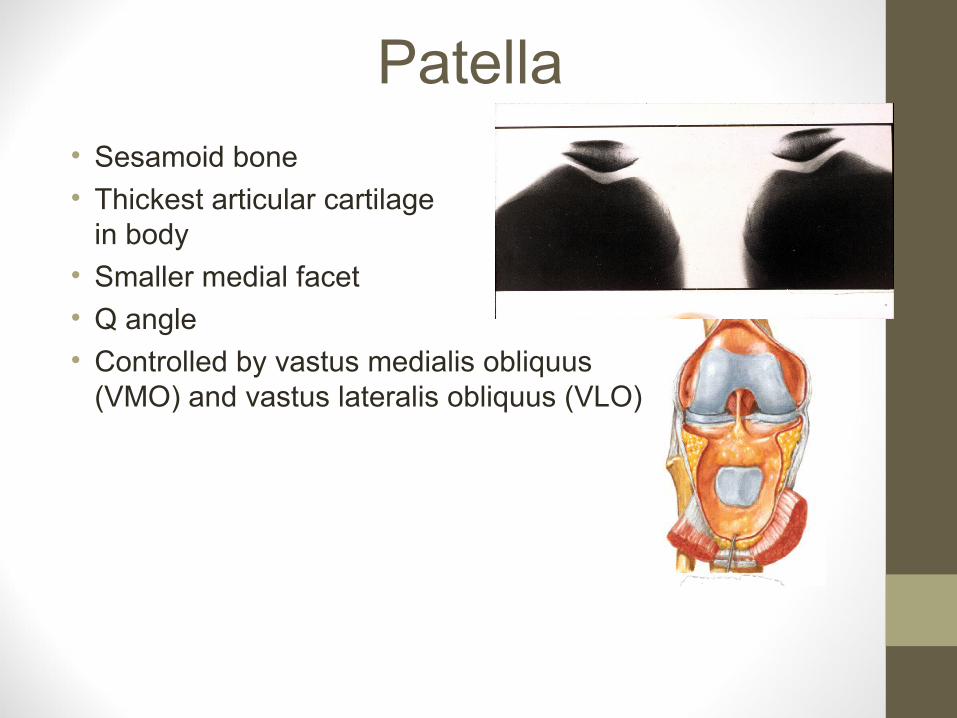
Patella • Sesamoid bone
• Thickest articular cartilage in body
• Smaller medial facet
• Q angle
• Controlled by vastus medialis obliquus (VMO) and vastus lateralis obliquus (VLO)
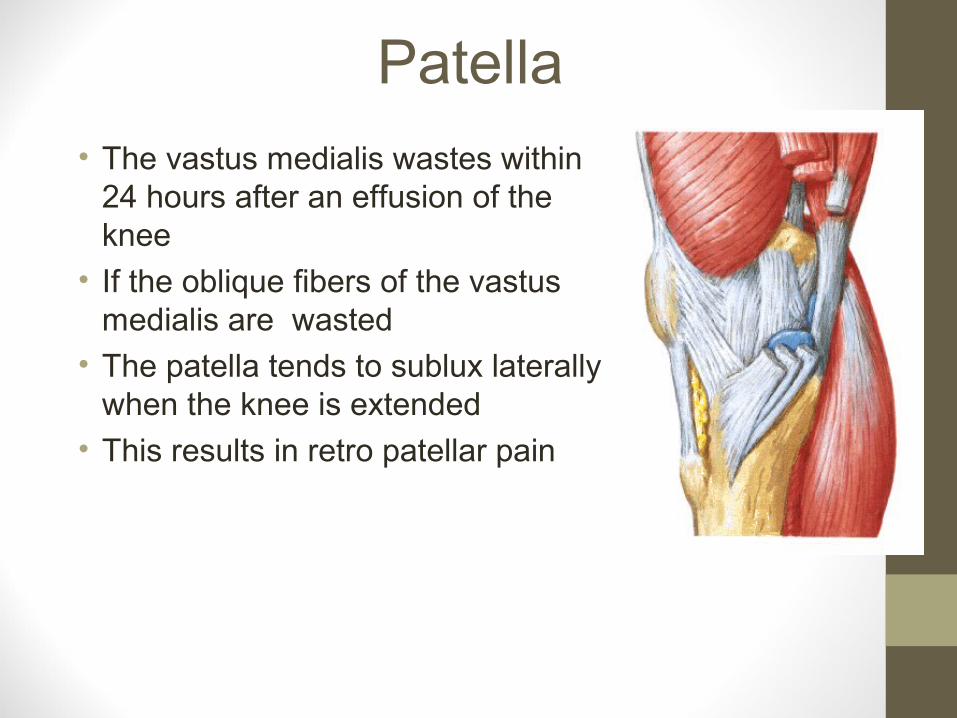
Patella • The vastus medialis wastes within
24 hours after an effusion of the knee
• If the oblique fibers of the vastus medialis are wasted
• The patella tends to sublux laterally when the knee is extended
• This results in retro patellar pain

Capsular Ligaments• Quadriceps
• Retinacular fibres
• Patellar tendon
• Coronary ligaments
• Medial and lateral ligaments
• Posterior oblique ligament

Infrapatellar Fat Pad (IFP)• Posteriorly • Covered by synovial membrane• Forms alar folds • Blood supply of fat is by the inferior genicular
arteries
• Also supply the lower part of the ACL from network of synovial membrane of fat pad
• Centre of fat pad has a limited blood supply
• Lateral arthroscopic approach to avoid injuryWilliams & Warick, 1980; Eriksson et al., 1980; Kohn et al., 1995
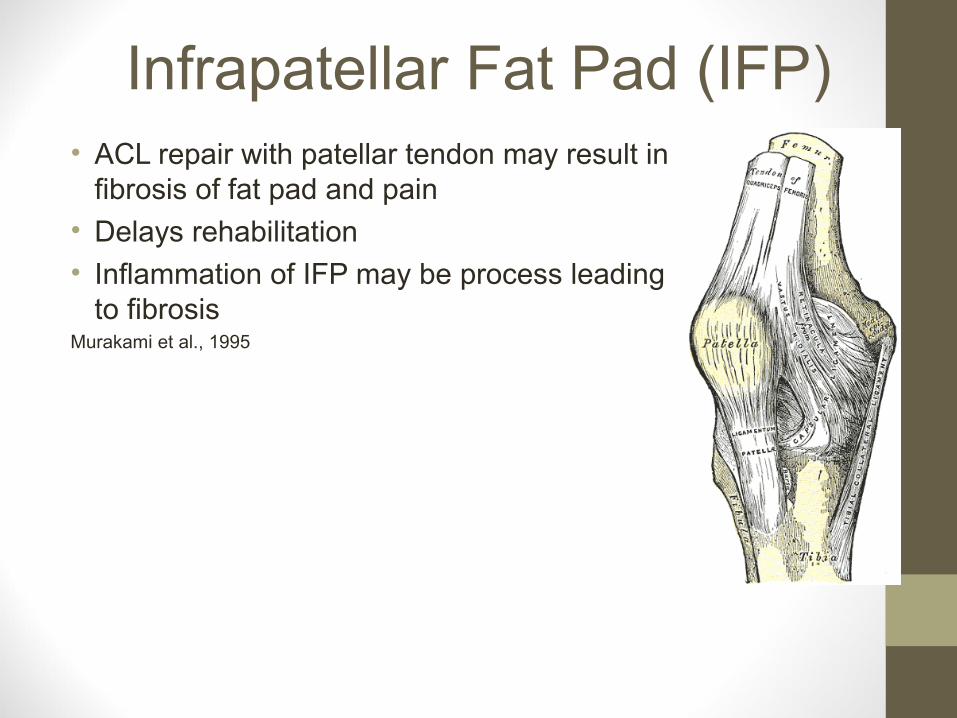
Infrapatellar Fat Pad (IFP)• ACL repair with patellar tendon may result in
fibrosis of fat pad and pain
• Delays rehabilitation
• Inflammation of IFP may be process leading to fibrosis
Murakami et al., 1995

Anterior and Posterior Cruciates• Anatomically named by their
tibial attachments
• Clinically, femoral attachments are called the origin
• Cruciates are intracapsular but extrasynovial
• Cross in the sagittal plane
• Covered by synovial membrane on anterior and on both sides which is reflected from capsule, i.e. oblique popliteal ligament
• Bursa between them on lateral aspect
anterior
lateral
oblique popliteal ligaments
ACL
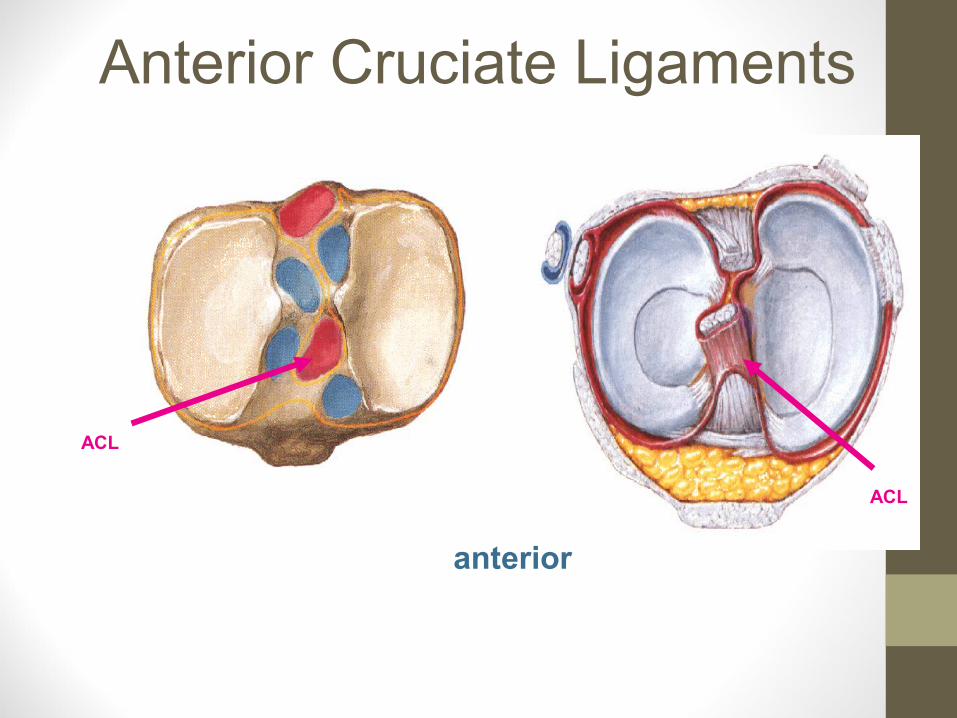
Anterior Cruciate Ligaments
anterior
ACL
ACL
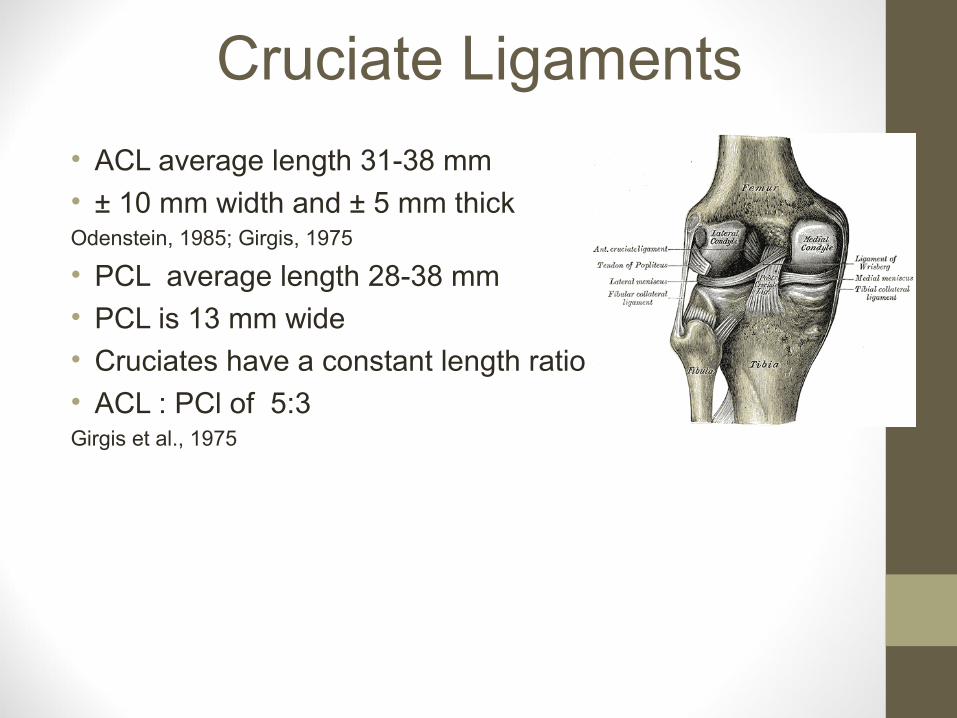
Cruciate Ligaments
• ACL average length 31-38 mm
• ± 10 mm width and ± 5 mm thickOdenstein, 1985; Girgis, 1975
• PCL average length 28-38 mm
• PCL is 13 mm wide
• Cruciates have a constant length ratio
• ACL : PCl of 5:3Girgis et al., 1975
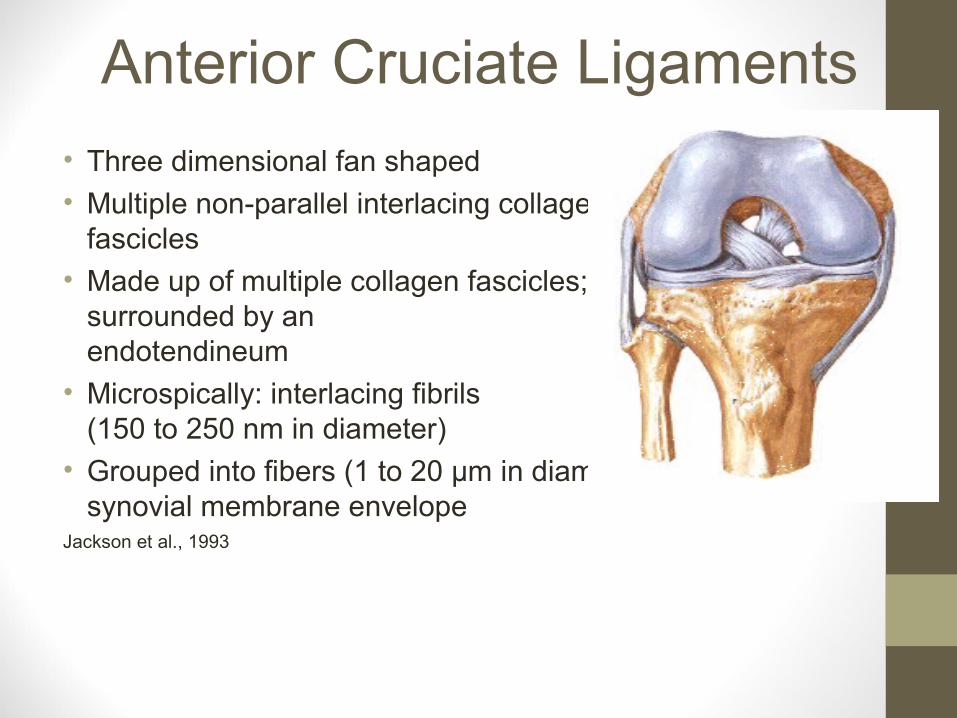
Anterior Cruciate Ligaments
• Three dimensional fan shaped
• Multiple non-parallel interlacing collagenous fascicles
• Made up of multiple collagen fascicles; surrounded by an endotendineum
• Microspically: interlacing fibrils (150 to 250 nm in diameter)
• Grouped into fibers (1 to 20 µm in diameter) synovial membrane envelope
Jackson et al., 1993

Anterior Cruciate Ligaments• Anterior cruciate is attached to
anterior aspect of the superior surface of the tibia
• Behind the anterior horn of medial meniscus and in front of the anterior horn of the lateral meniscus
• Passes upwards and laterally to the posterior aspect of medial surface of lateral femoral condyle
ACL
lateral
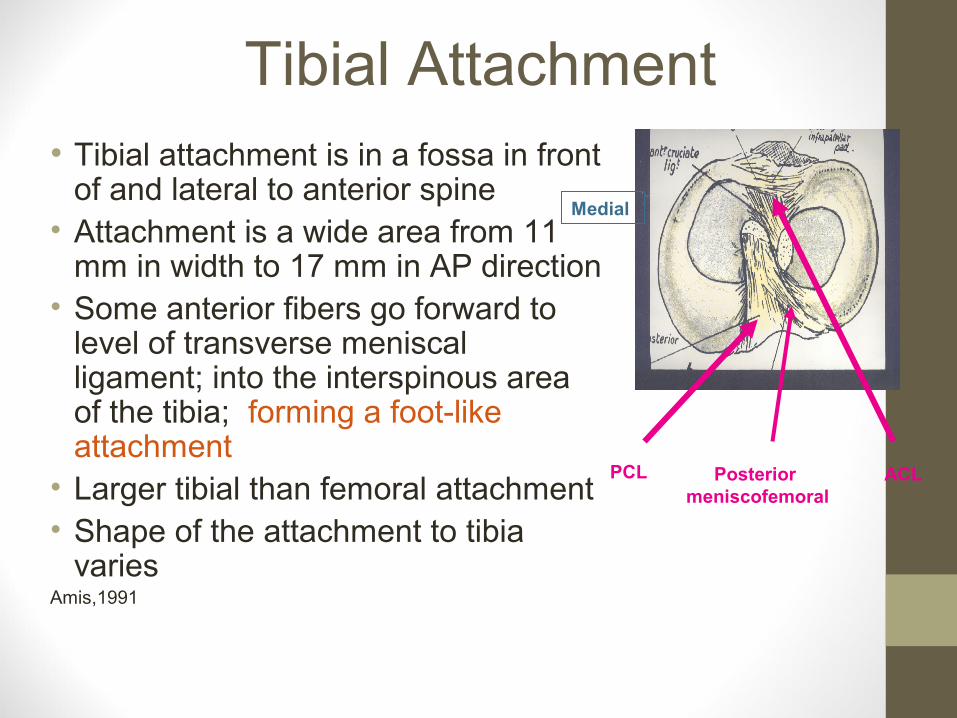
Tibial Attachment• Tibial attachment is in a fossa in front
of and lateral to anterior spine• Attachment is a wide area from 11
mm in width to 17 mm in AP direction• Some anterior fibers go forward to
level of transverse meniscal ligament; into the interspinous area of the tibia; forming a foot-like attachment
• Larger tibial than femoral attachment• Shape of the attachment to tibia
variesAmis,1991
ACL
Medial
PCL Posterior meniscofemoral

Femoral Attachment• ACL attached to a fossa on the
posteromedial corner of medial aspect of lateral femoral condyle in the intercondylar notch
• Femoral attachment of ACL is well posterior to longitudinal axis of the femoral shaft.
• Femoral attachment is in the form of a segmented circle
• Anterior border is straight, posterior border convex
Arnoczky et al 1983

Femoral Attachment
• Attachment is actually an interdigitation of collagen fibers and rigid bone, through a transitional zone of fibrocartilage and mineralized fibrocartilage
• Attachment lies on a line which forms a 40°angle with the long axis of the femur
Muller, 1982; Frazer, 1975
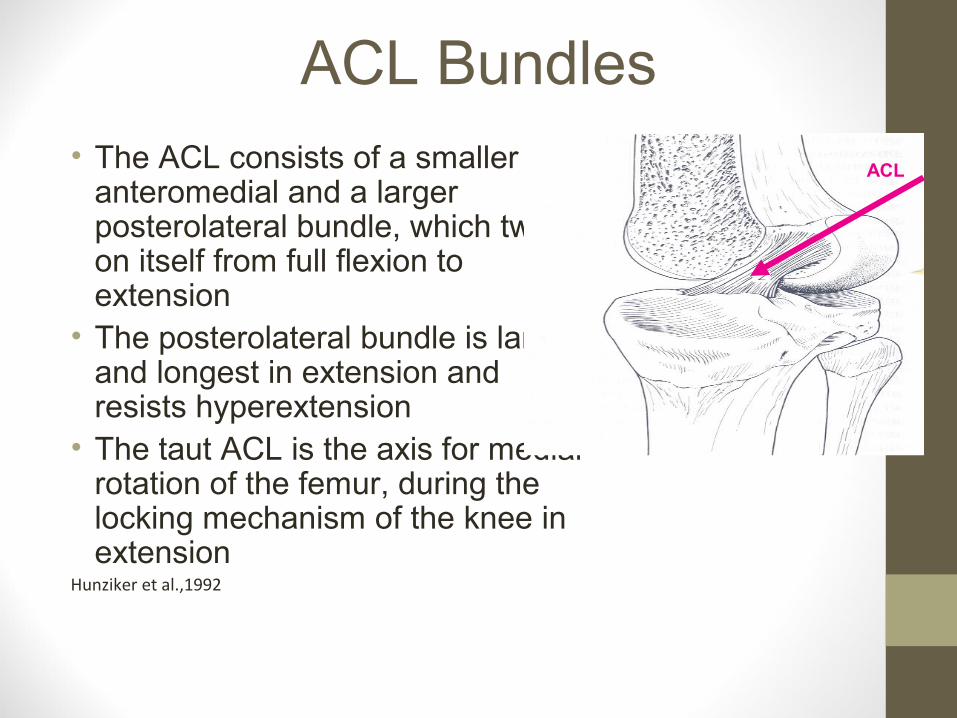
ACL Bundles• The ACL consists of a smaller
anteromedial and a larger posterolateral bundle, which twists on itself from full flexion to extension
• The posterolateral bundle is larger and longest in extension and resists hyperextension
• The taut ACL is the axis for medial rotation of the femur, during the locking mechanism of the knee in extension
Hunziker et al.,1992
ACL
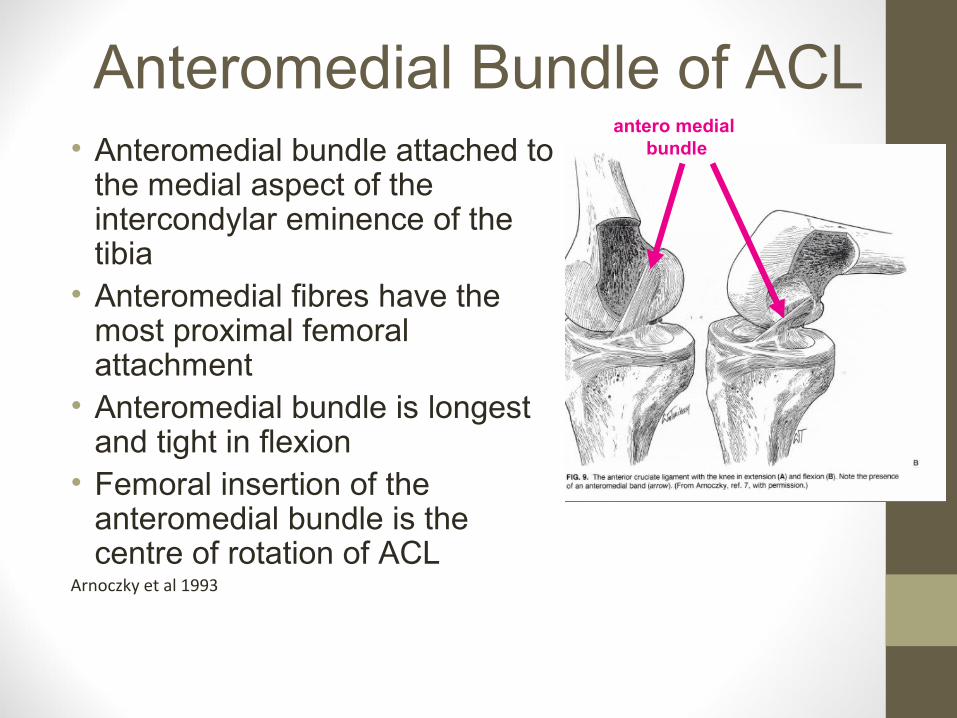
Anteromedial Bundle of ACL• Anteromedial bundle attached to
the medial aspect of the intercondylar eminence of the tibia
• Anteromedial fibres have the most proximal femoral attachment
• Anteromedial bundle is longest and tight in flexion
• Femoral insertion of the anteromedial bundle is the centre of rotation of ACL
Arnoczky et al 1993
antero medial bundle
Anteromedial Bundle• Anteromedial bundle has an isometric
behaviour
• Tightens in flexion, while the postero lateral bundle relaxes in flexion
• Is more prone to injury with the knee in flexion
• Anteromedial band is primary check against anterior translation of tibia on femur
• When anterior drawer test is performed in usual manner with knee flexed
• Contributes to anteromedial stabilityO’Brien, 1992

Posterolateral Bundle
• Posterolateral is attached just lateral to midline of the intercondylar eminence
• Fibres are most inferior on femur, most posterior on tibia
• The bulkier posterolateral bundle is not isometric
• ACL bundles are vertical and parallel in extension
• Posterolateral bundle is tight in extension
• Both bundles of ACL are horizontal at 90°flexion Arnoczky, 1983
posterolateral
anteromedial
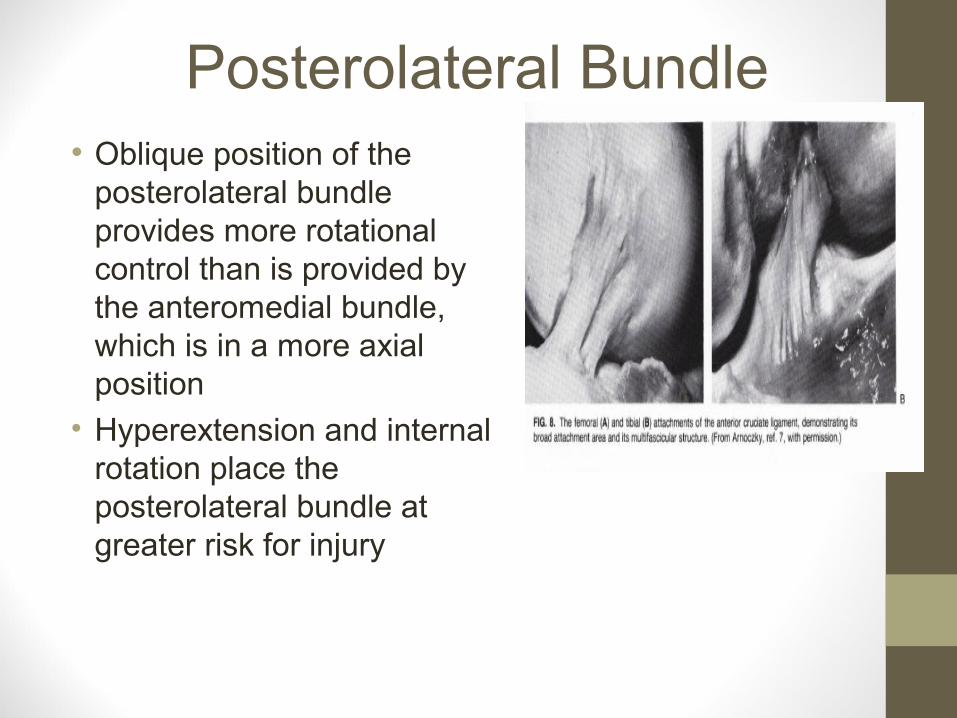
Posterolateral Bundle• Oblique position of the
posterolateral bundle provides more rotational control than is provided by the anteromedial bundle, which is in a more axial position
• Hyperextension and internal rotation place the posterolateral bundle at greater risk for injury

Posterolateral Bundle• It limits anterior translation,
hyperextension, and rotation during flexion • Femoral insertion site of the
postero lateral bundle moves anteriorly
• Both bundles are crossed • Posterolateral bundle loosens
in flexion
Anterior Cruciate Ligaments
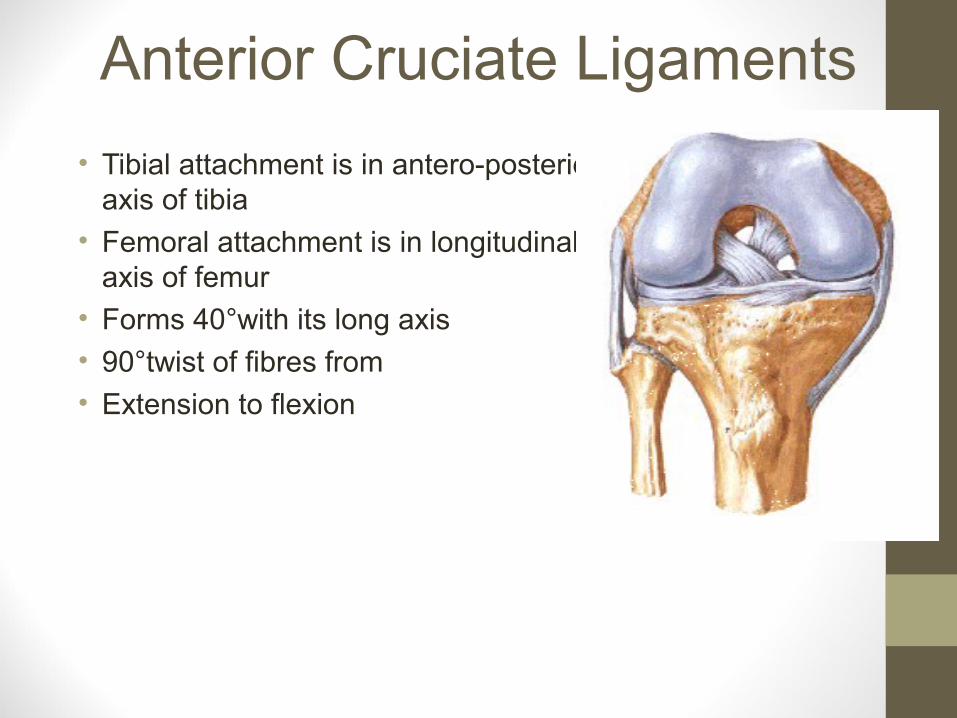
• Tibial attachment is in antero-posterior axis of tibia
• Femoral attachment is in longitudinal axis of femur
• Forms 40°with its long axis
• 90°twist of fibres from
• Extension to flexion
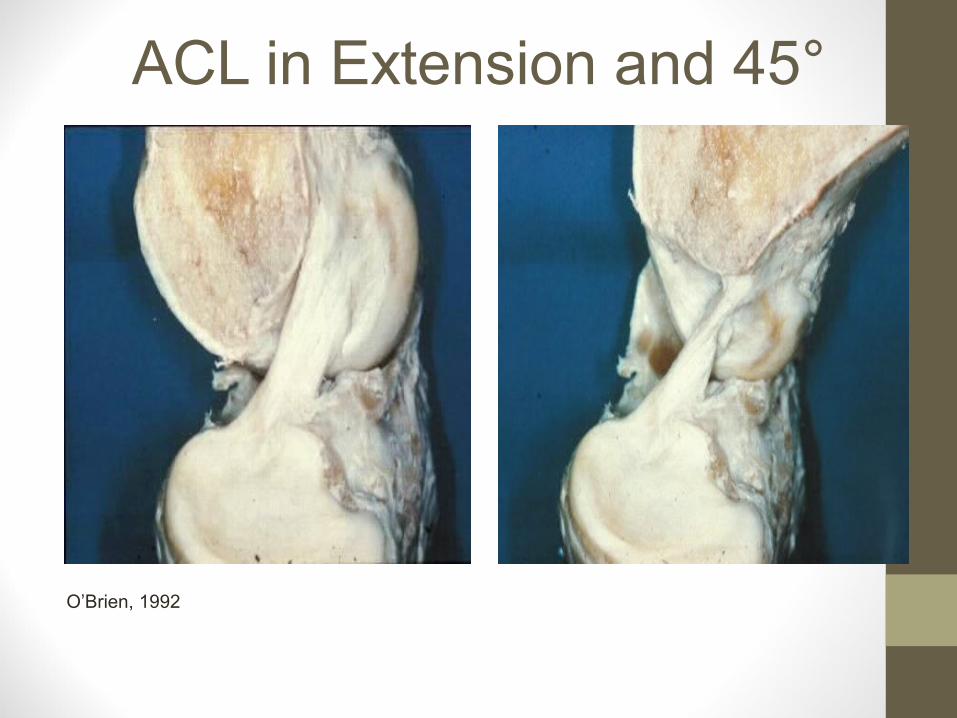
ACL in Extension and 45°
O’Brien, 1992
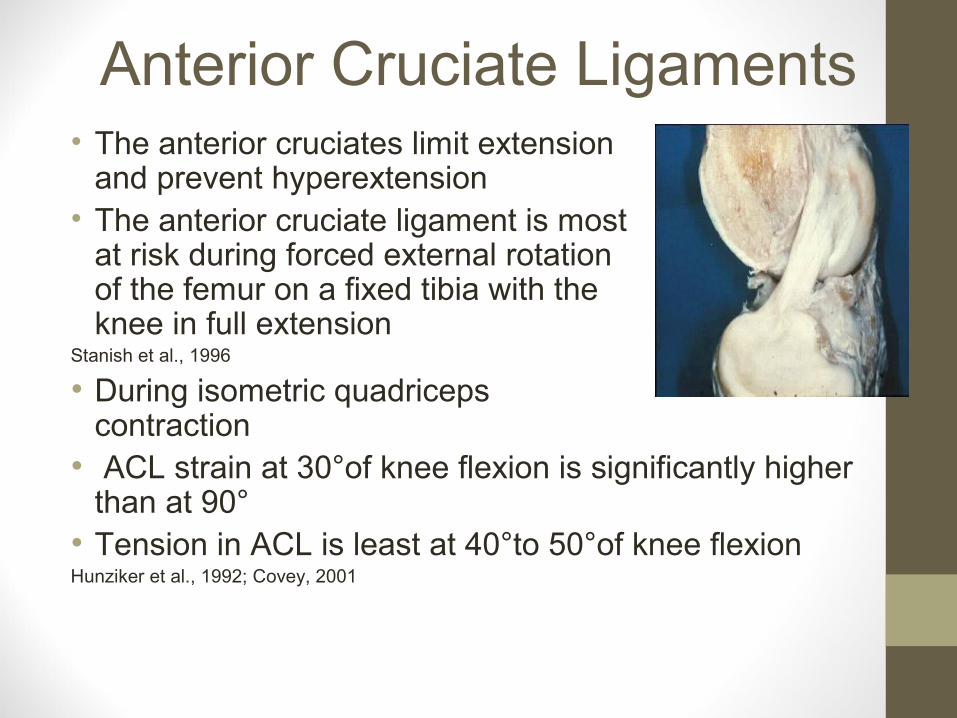
Anterior Cruciate Ligaments• The anterior cruciates limit extension
and prevent hyperextension• The anterior cruciate ligament is most
at risk during forced external rotation of the femur on a fixed tibia with the knee in full extension
Stanish et al., 1996
• During isometric quadriceps contraction
• ACL strain at 30°of knee flexion is significantly higher than at 90°
• Tension in ACL is least at 40°to 50°of knee flexion Hunziker et al., 1992; Covey, 2001

Anterior and Posterior Cruciate• ACL
• Provides 86% of restraint to anterior displacement
• PCL
• Provides 94% of restraint to posterior displacement
• Hyperextension of the knee develops much higher forces in ACL than in the PCL

Posterior Cruciate• PCL is the strongest ligament of
knee• It tends to be shorter • More vertical• Less oblique • Twice as strong as ACL • Closely applied to the centre of
rotation of knee• It is the principle stabiliserHunziker et al., 1992

Attachment of the PCL• The tibial attachment of the
PCL was on the sloping posterior portion of the tibial intercondylar area
• Extended 11.5-17.3 mm distal to the tibial plateau
• Anterior to tibial articular margin
• Blends with periosteum and capsule
Javadpour & O’ Brien, 1992
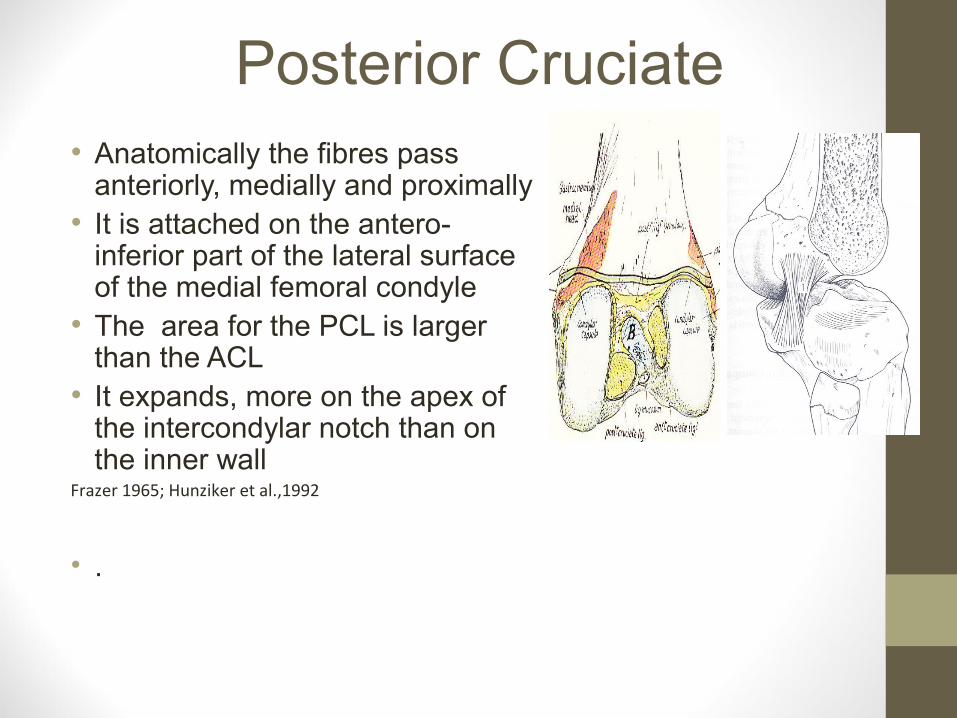
Posterior Cruciate• Anatomically the fibres pass
anteriorly, medially and proximally• It is attached on the antero-
inferior part of the lateral surface of the medial femoral condyle
• The area for the PCL is larger than the ACL
• It expands, more on the apex of the intercondylar notch than on the inner wall
Frazer 1965; Hunziker et al.,1992
• .
Cruciates Microscopic• Collagen fibrils 150-200 µm in diameter
• Fibres 1-20 µm in diameter
• A subfascicular unit from100-250 µm
• 3 to 20 subfascicular units form collagen fasciculus, 250 µm to several millimetres
Hunziker et al.,1992

Blood Supply ofAnterior Cruciate Ligaments
• Middle genicular enters upper third and is the major blood supply via synovium
• Inferior medial genicular and Inferior lateral genicular arteries supply via infrapatellar fat pad
• Bony attachments do not provide a significant source of blood to distal or proximal ligaments
Arnoczky 1987

Blood Supply of Cruciates
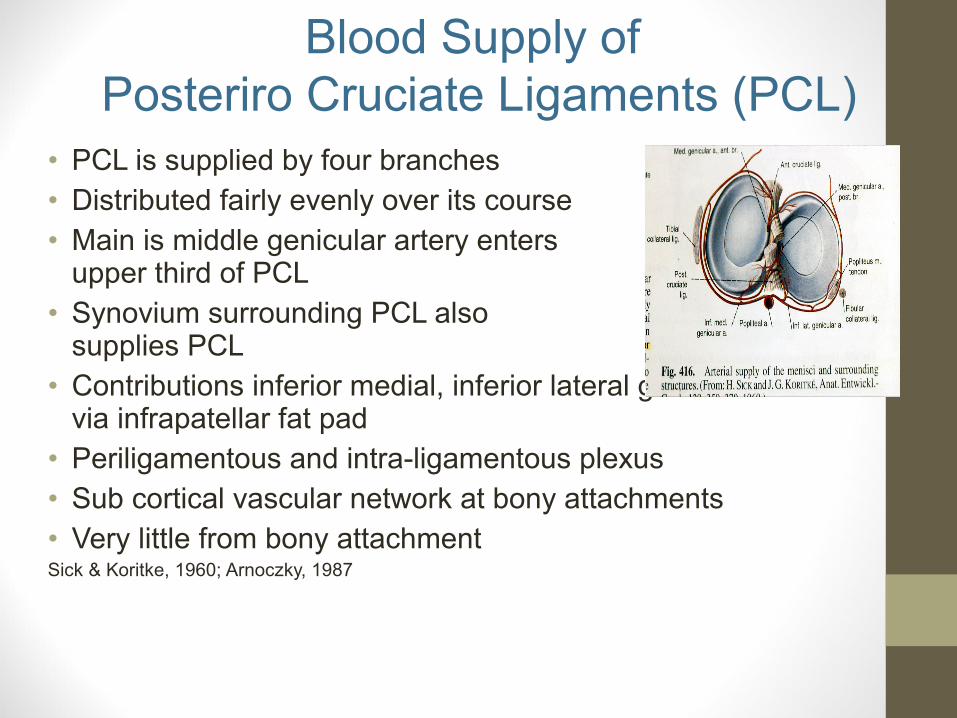
• PCL is supplied by four branches• Distributed fairly evenly over its course • Main is middle genicular artery enters
upper third of PCL• Synovium surrounding PCL also
supplies PCL• Contributions inferior medial, inferior lateral genicular arteries
via infrapatellar fat pad• Periligamentous and intra-ligamentous plexus• Sub cortical vascular network at bony attachments • Very little from bony attachment Sick & Koritke, 1960; Arnoczky, 1987
Blood Supply of Posteriro Cruciate Ligaments (PCL)
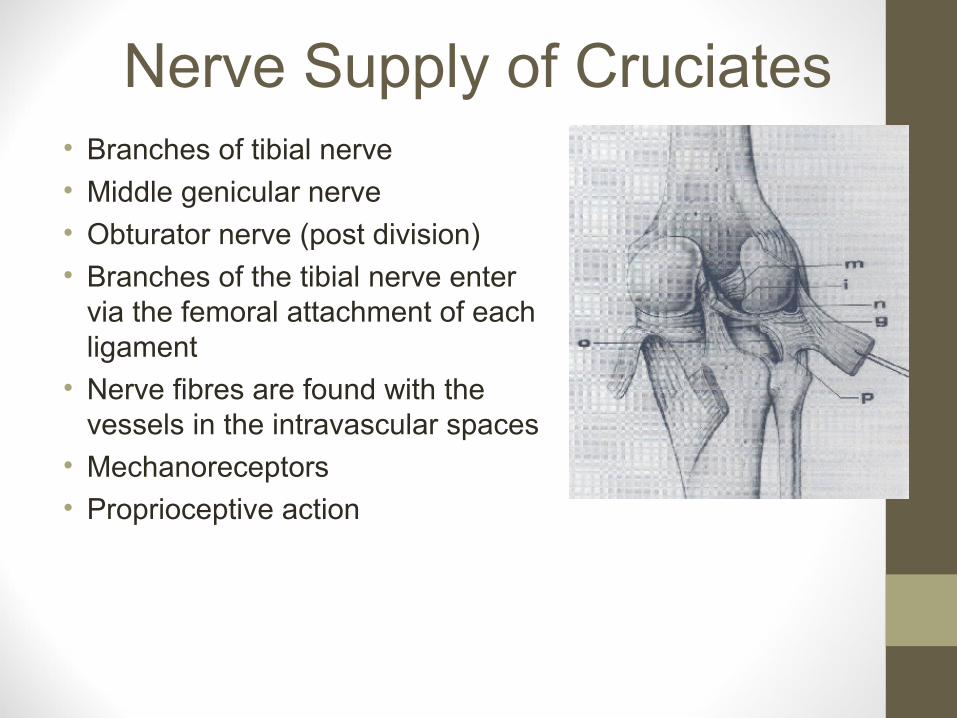
Nerve Supply of Cruciates• Branches of tibial nerve
• Middle genicular nerve
• Obturator nerve (post division)
• Branches of the tibial nerve enter via the femoral attachment of each ligament
• Nerve fibres are found with the vessels in the intravascular spaces
• Mechanoreceptors
• Proprioceptive action
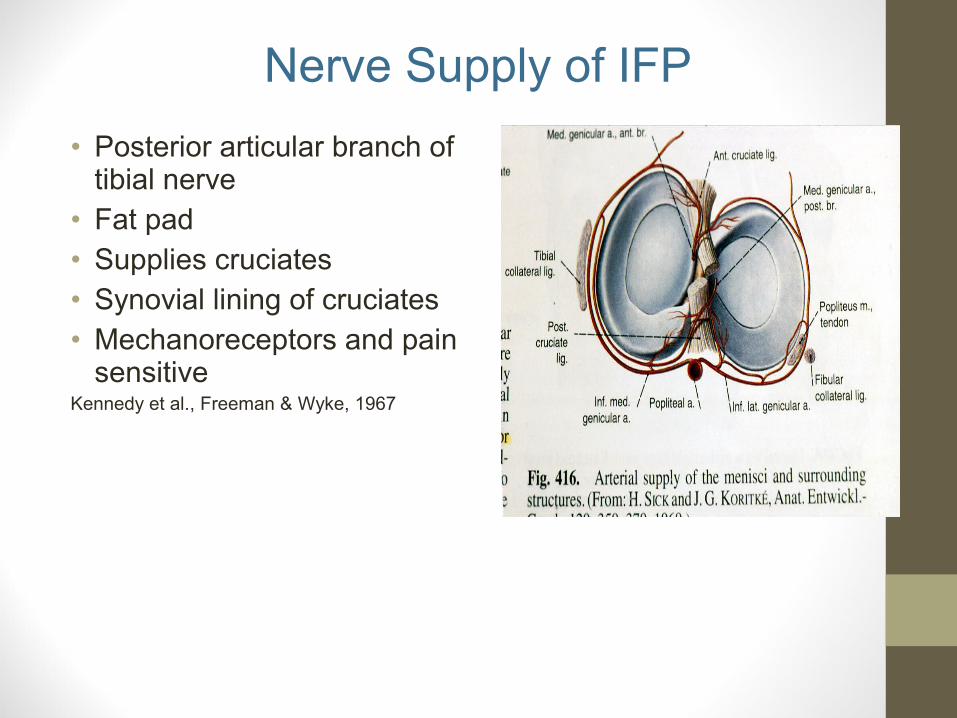
• Posterior articular branch of tibial nerve
• Fat pad• Supplies cruciates • Synovial lining of cruciates • Mechanoreceptors and pain
sensitiveKennedy et al., Freeman & Wyke, 1967
Nerve Supply of IFP
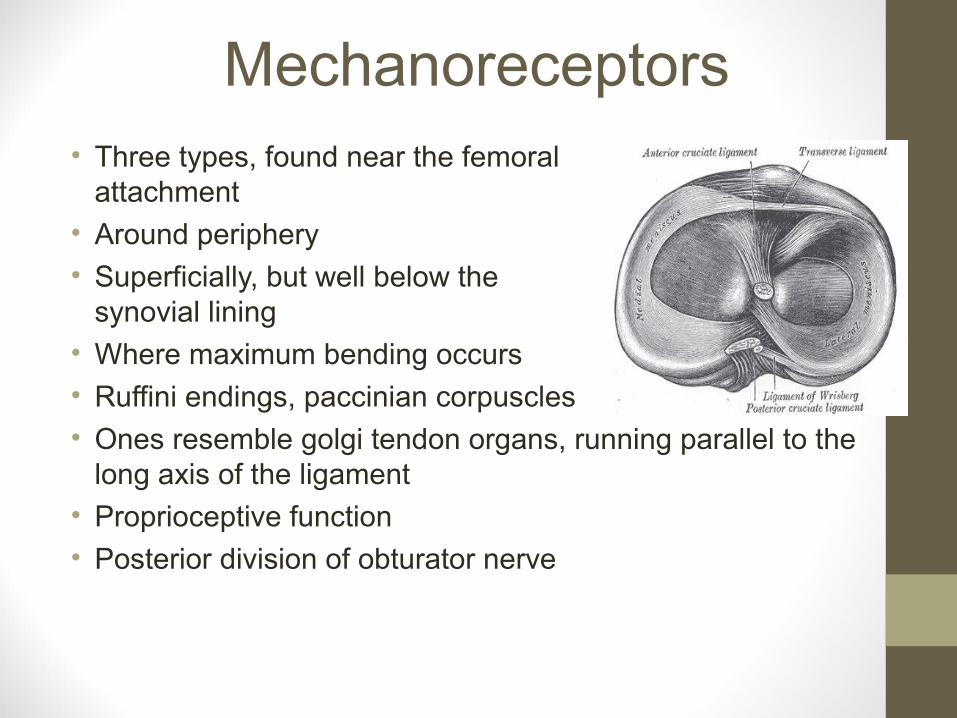
Mechanoreceptors• Three types, found near the femoral
attachment
• Around periphery
• Superficially, but well below the synovial lining
• Where maximum bending occurs
• Ruffini endings, paccinian corpuscles
• Ones resemble golgi tendon organs, running parallel to the long axis of the ligament
• Proprioceptive function
• Posterior division of obturator nerve
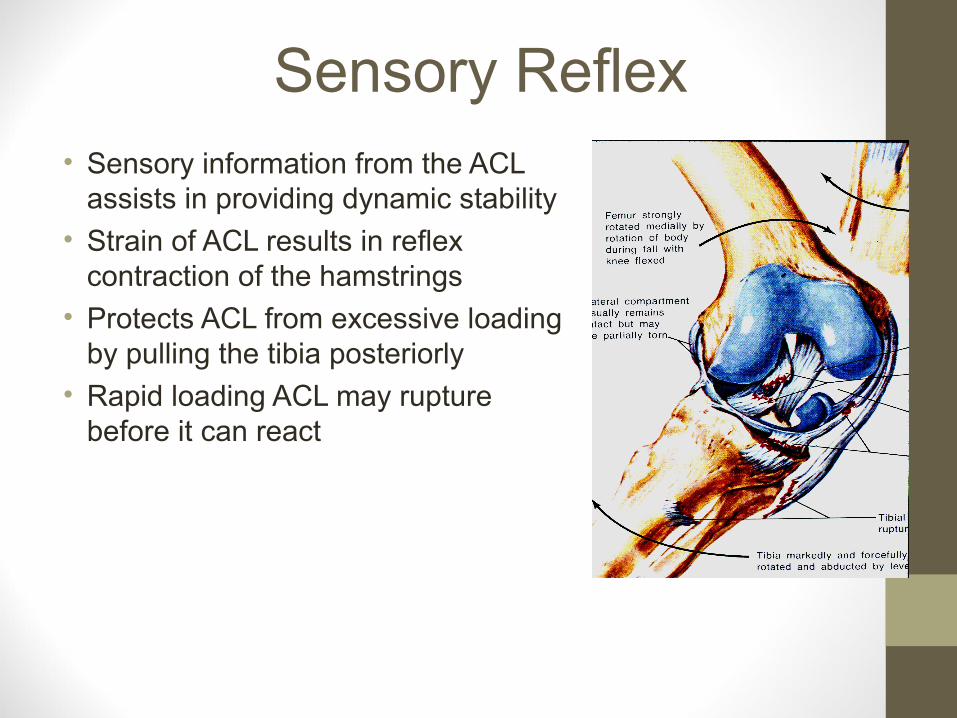
Sensory Reflex• Sensory information from the ACL
assists in providing dynamic stability
• Strain of ACL results in reflex contraction of the hamstrings
• Protects ACL from excessive loading by pulling the tibia posteriorly
• Rapid loading ACL may rupture before it can react
Extension Screw Home • Contraction of the quadriceps results in
extension
• The anterior cruciate becomes taut
• And medial rotation of the femur occurs around the taut anterior cruciate to accommodate the longer surface of the medial condyle
• During extension the ACL lies in a smaller anterolateral notch in the main intercondylar notch
• It can be kinked or torn here during hyperextension, particularly if there is violent hyperextension and internal rotation

Extension
• The anterior horns of the menisci block further movement of the femoral condyles
• The posterior portion of the capsule and the collateral ligaments are also tight: this is the close-packed position of the joint

• Popliteus laterally rotates the femur to unlock the knee
• So flexion can occur
• Then the hamstrings flex the knee
• The axis around which the motion takes place is not a fixed one, but shifts forward during extension and backward during flexion
popliteus
Flexion
Screw-Home in Extension• The effect of the screw-home
is to transform the leg into a rigid unit, sufficiently stable for the quadriceps to relax
• Little muscular effort is then needed to maintain the standing posture
• The screw-home action is due to the inability of the central ligaments to increase in length
Screw-Home in Extension• The screw-home does not
occur in the absence of the controlling ligaments
• If the anterior cruciate and postero-lateral complex are missing, the lateral condyle is not drawn forwards, resulting in a positive pivot shift test
• Which is the abnormal displacement of the lateral tibial condyle on the femur

Anatomy of the Menisci
• Menisci are made of fibro cartilage
• Wedge shaped on cross section
• Medial is comma shaped with the wide portion posteriorly
• Lateral is smaller, two horns closer together round
• They are intracapsular and intra synovial
anterior
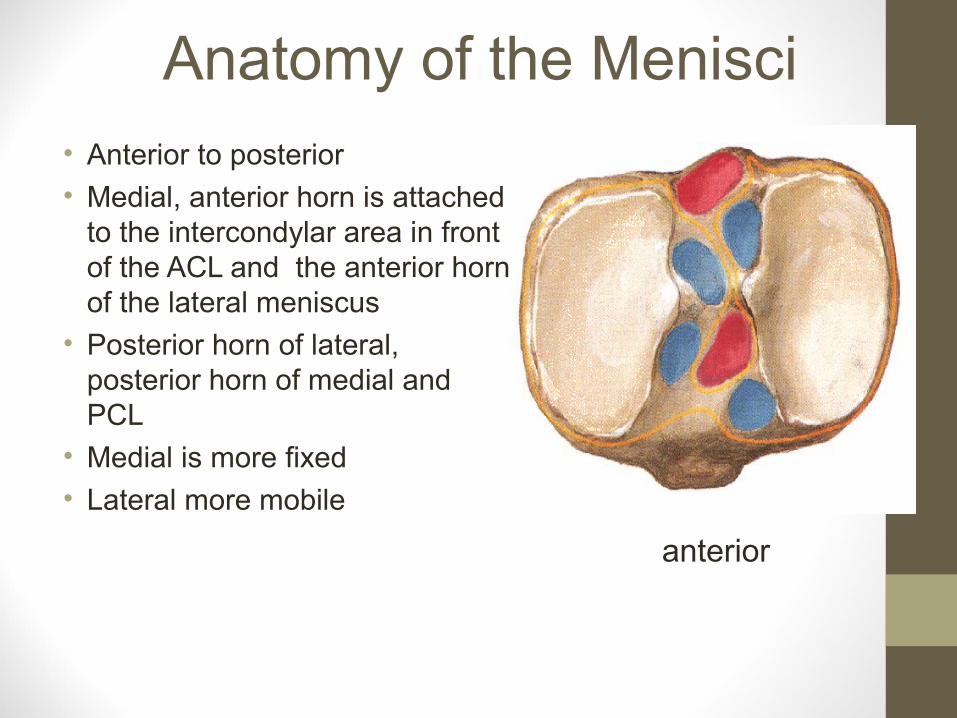
Anatomy of the Menisci• Anterior to posterior
• Medial, anterior horn is attached to the intercondylar area in front of the ACL and the anterior horn of the lateral meniscus
• Posterior horn of lateral, posterior horn of medial and PCL
• Medial is more fixed
• Lateral more mobile
anterior
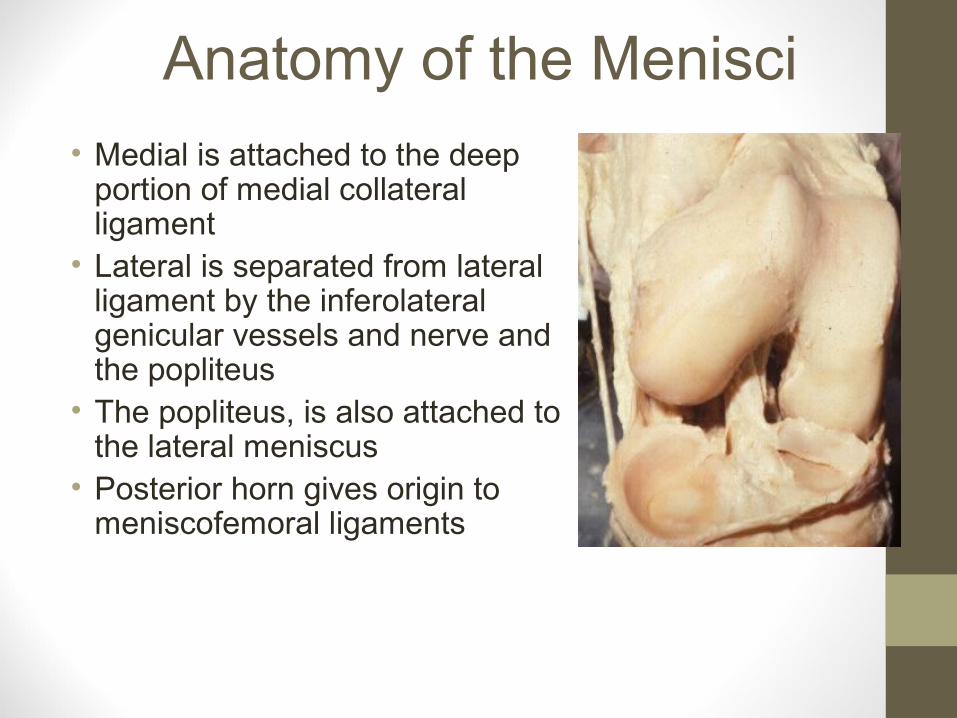
Anatomy of the Menisci• Medial is attached to the deep
portion of medial collateral ligament
• Lateral is separated from lateral ligament by the inferolateral genicular vessels and nerve and the popliteus
• The popliteus, is also attached to the lateral meniscus
• Posterior horn gives origin to meniscofemoral ligaments

Menisco-femoral Ligaments
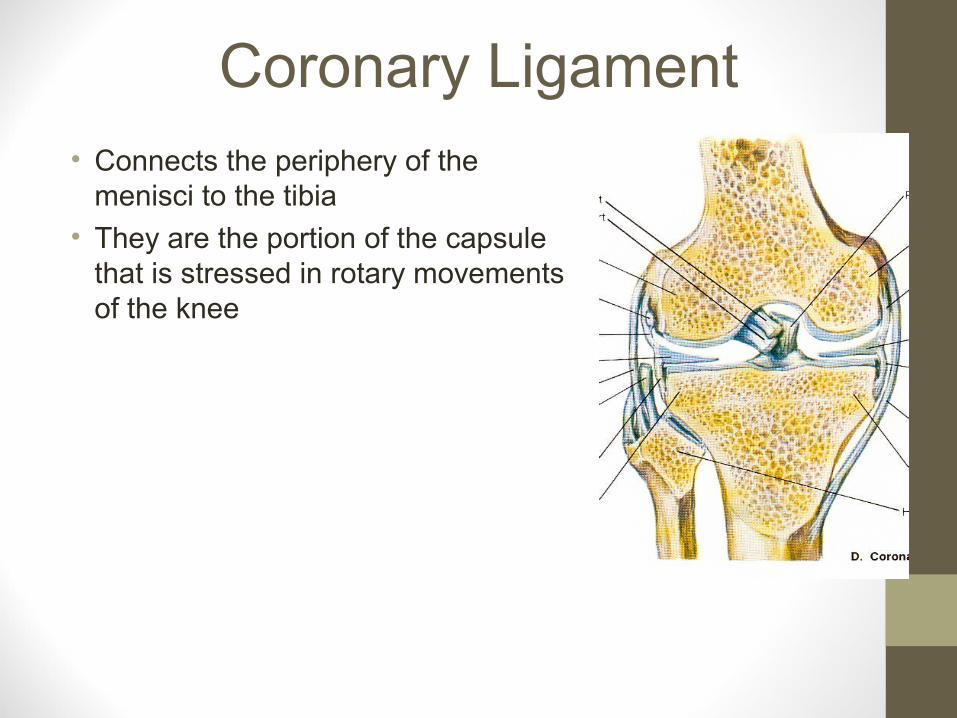
Coronary Ligament• Connects the periphery of the
menisci to the tibia
• They are the portion of the capsule that is stressed in rotary movements of the knee
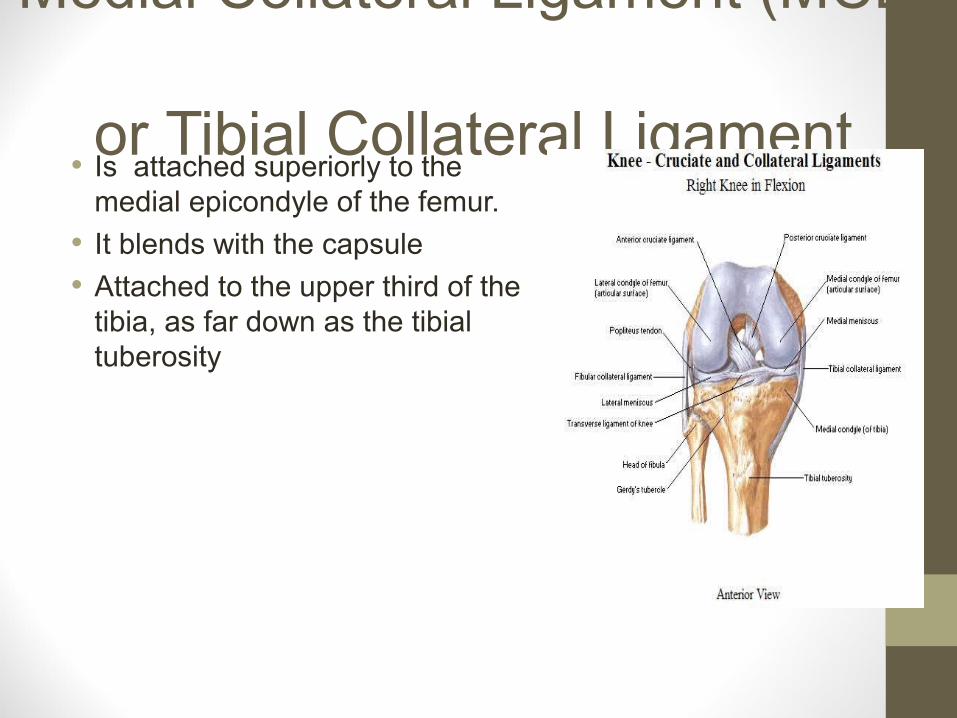
Medial Collateral Ligament (MCL)
or Tibial Collateral Ligament• Is attached superiorly to the
medial epicondyle of the femur.
• It blends with the capsule
• Attached to the upper third of the tibia, as far down as the tibial tuberosity
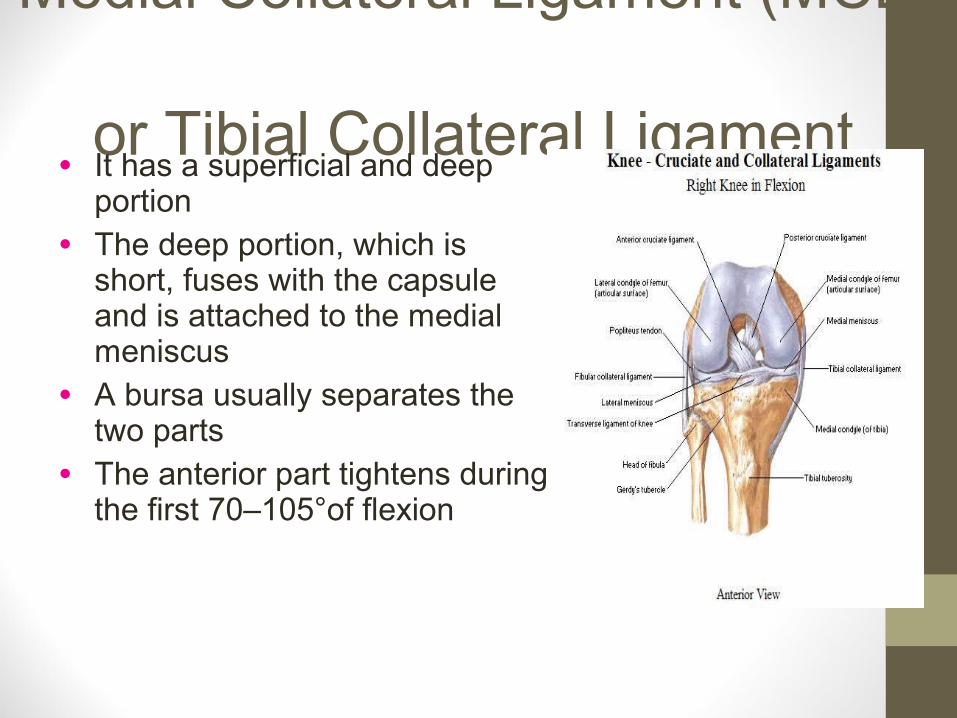
Medial Collateral Ligament (MCL)
or Tibial Collateral Ligament• It has a superficial and deep
portion
• The deep portion, which is short, fuses with the capsule and is attached to the medial meniscus
• A bursa usually separates the two parts
• The anterior part tightens during the first 70–105°of flexion

Medial Collateral Ligament (MCL)
• Medial ligament, tightens in extension
• And at the extremes of medial and lateral rotation
• A valgus stress will put a strain on the ligament
• If gapping occurs when the knee is extended, this is due to a tear of posterior medial part of capsule
• If gapping only occurs at 15º flexion, this is due to tear of medial ligament
Related Documents











