doi:10.1016/j.ultrasmedbio.2006.08.004 ● Original Contribution ANATOMICAL FLOW PHANTOMS OF THE NONPLANAR CAROTID BIFURCATION, PART II: EXPERIMENTAL VALIDATION WITH DOPPLER ULTRASOUND S. MEAGHER,* T. L. POEPPING,* a K. V. RAMNARINE,* b R. A. BLACK, † and P. R. HOSKINS* *Department of Medical Physics, University of Edinburgh, Edinburgh; and † Division of Clinical Engineering, School of Clinical Sciences, University of Liverpool, Liverpool, UK (Received 8 November 2005; revised 28 July 2006; in final form 10 August 2006) Abstract—A nonplanar wall-less anatomical flow phantom of a healthy human carotid artery is described, the construction of which is based on a lost-core technique described in the companion paper (Part I) by Watts et al. (2006). The core was made by rapid prototyping of an idealized three-dimensional computer model of the carotid artery. Flow phantoms were built using these idealized non planar carotid artery bifurcations. Physio- logically realistic flow waveforms were produced with resistance index values of 0.75, 0.72 and 0.63 in the common, external and internal carotid artery branches, respectively. Distension of the common carotid using M-mode imaging was found to be at 10% of diameter. Although differences in vessel diameter between the phantom and that of the original computer model were statistically significant (p < 0.05), there was no difference (p > 0.05) in measurements made on the lost-cores and those obtained by B-mode ultrasound on the resulting flow phantoms. In conclusion, it was possible to reliably reproduce geometrically similar anatomical flow phantoms that are capable of producing realistic physiological flow patterns and distensions. (E-mail: [email protected]) © 2007 World Federation for Ultrasound in Medicine & Biology. Key Words: Anatomical flow phantom, Carotid arteries, Doppler ultrasound. INTRODUCTION It is possible to measure several velocity-related quanti- ties using modern ultrasound imaging systems. In clini- cal practice, it is common to measure peak systolic velocity for the assessment of degree of stenosis (Grant et al. 2003). Other quantities that can be measured in- clude mean velocity, usually expressed in terms of volu- metric flow, and, in recent years, several groups have attempted to measure wall shear rate (Brands et al. 1995; Forsberg et al. 2000) despite there being several sources of uncertainty in the measurement of velocity (Hoskins 1999). Clinical ultrasound systems overestimate maxi- mum velocity when measured from the spectral wave- form, as a result of geometric spectral broadening (Daigle et al. 1990; Hoskins et al. 1991; Hoskins 1996). There are other known sources of error, such as velocity- gradient broadening and lack of knowledge of the true direction of motion due to the single-component nature of commercial Doppler systems. In general, arterial flows are complex and there is a need to assess the accuracy of such measurements in a phantom for which the velocity distribution is accurately known. Many different types of flow phantoms have been used to validate and investigate the accuracy of velocity measurements obtained by ultrasound systems. Straight tube phantoms are easy to construct and have been used in studies on the accuracy of ultrasound measurement of volumetric flow (Deane et al.1997; Embree et al. 1990), wall shear rate (Hughes et al. 1993) and to investigate the relationship between estimated maximum velocity and the degree of stenosis (Allard et al. 1995; Hoskins 1997; Vattyam et al. 1991). These simplistic phantoms do not take into account important anatomical features such as arterial branching and bending, which can affect ultra- sound measurements. It is possible to produce realistic flow phantoms with curves and bifurcations using post- mortem arteries (Bale-Glickman et al. 2003; Keber et al. 1992; Motomiya et al. 1984); however, explanted arter- Address correspondence to: Siobhan Meagher, Medical Physics, The University of Edinburgh, The Chancellors Building, 49 Little France Crescent, Edinburgh EH16 4SB, UK. E-mail: smeagher@ staffmail.ed.ac.uk a Now at Department of Physics and Astronomy, University of Western Ontario, London, Canada. b Now at Medical Physics, University Hospitals of Leicester NHS Trust, UK. Ultrasound in Med. & Biol., Vol. 33, No. 2, pp. 303–310, 2007 Copyright © 2007 World Federation for Ultrasound in Medicine & Biology Printed in the USA. All rights reserved 0301-5629/07/$–see front matter 303

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Ultrasound in Med. & Biol., Vol. 33, No. 2, pp. 303–310, 2007Copyright © 2007 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/07/$–see front matter
doi:10.1016/j.ultrasmedbio.2006.08.004
● Original Contribution
ANATOMICAL FLOW PHANTOMS OF THE NONPLANAR CAROTIDBIFURCATION, PART II: EXPERIMENTAL VALIDATION WITH
DOPPLER ULTRASOUND
S. MEAGHER,* T. L. POEPPING,*a K. V. RAMNARINE,*b R. A. BLACK,† and P. R. HOSKINS**Department of Medical Physics, University of Edinburgh, Edinburgh; and †Division of Clinical Engineering,
School of Clinical Sciences, University of Liverpool, Liverpool, UK
(Received 8 November 2005; revised 28 July 2006; in final form 10 August 2006)
Abstract—A nonplanar wall-less anatomical flow phantom of a healthy human carotid artery is described, theconstruction of which is based on a lost-core technique described in the companion paper (Part I) by Watts etal. (2006). The core was made by rapid prototyping of an idealized three-dimensional computer model of thecarotid artery. Flow phantoms were built using these idealized non planar carotid artery bifurcations. Physio-logically realistic flow waveforms were produced with resistance index values of 0.75, 0.72 and 0.63 in thecommon, external and internal carotid artery branches, respectively. Distension of the common carotid usingM-mode imaging was found to be at 10% of diameter. Although differences in vessel diameter between thephantom and that of the original computer model were statistically significant (p < 0.05), there was no difference(p > 0.05) in measurements made on the lost-cores and those obtained by B-mode ultrasound on the resultingflow phantoms. In conclusion, it was possible to reliably reproduce geometrically similar anatomical flowphantoms that are capable of producing realistic physiological flow patterns and distensions. (E-mail:[email protected]) © 2007 World Federation for Ultrasound in Medicine & Biology.
Key Words: Anatomical flow phantom, Carotid arteries, Doppler ultrasound.
INTRODUCTION
It is possible to measure several velocity-related quanti-ties using modern ultrasound imaging systems. In clini-cal practice, it is common to measure peak systolicvelocity for the assessment of degree of stenosis (Grantet al. 2003). Other quantities that can be measured in-clude mean velocity, usually expressed in terms of volu-metric flow, and, in recent years, several groups haveattempted to measure wall shear rate (Brands et al. 1995;Forsberg et al. 2000) despite there being several sourcesof uncertainty in the measurement of velocity (Hoskins1999). Clinical ultrasound systems overestimate maxi-mum velocity when measured from the spectral wave-form, as a result of geometric spectral broadening(Daigle et al. 1990; Hoskins et al. 1991; Hoskins 1996).
Address correspondence to: Siobhan Meagher, Medical Physics,The University of Edinburgh, The Chancellors Building, 49 LittleFrance Crescent, Edinburgh EH16 4SB, UK. E-mail: [email protected]
a Now at Department of Physics and Astronomy, University ofWestern Ontario, London, Canada.
b
Now at Medical Physics, University Hospitals of LeicesterNHS Trust, UK.303
There are other known sources of error, such as velocity-gradient broadening and lack of knowledge of the truedirection of motion due to the single-component natureof commercial Doppler systems. In general, arterialflows are complex and there is a need to assess theaccuracy of such measurements in a phantom for whichthe velocity distribution is accurately known.
Many different types of flow phantoms have beenused to validate and investigate the accuracy of velocitymeasurements obtained by ultrasound systems. Straighttube phantoms are easy to construct and have been usedin studies on the accuracy of ultrasound measurement ofvolumetric flow (Deane et al.1997; Embree et al. 1990),wall shear rate (Hughes et al. 1993) and to investigate therelationship between estimated maximum velocity andthe degree of stenosis (Allard et al. 1995; Hoskins 1997;Vattyam et al. 1991). These simplistic phantoms do nottake into account important anatomical features such asarterial branching and bending, which can affect ultra-sound measurements. It is possible to produce realisticflow phantoms with curves and bifurcations using post-mortem arteries (Bale-Glickman et al. 2003; Keber et al.
1992; Motomiya et al. 1984); however, explanted arter-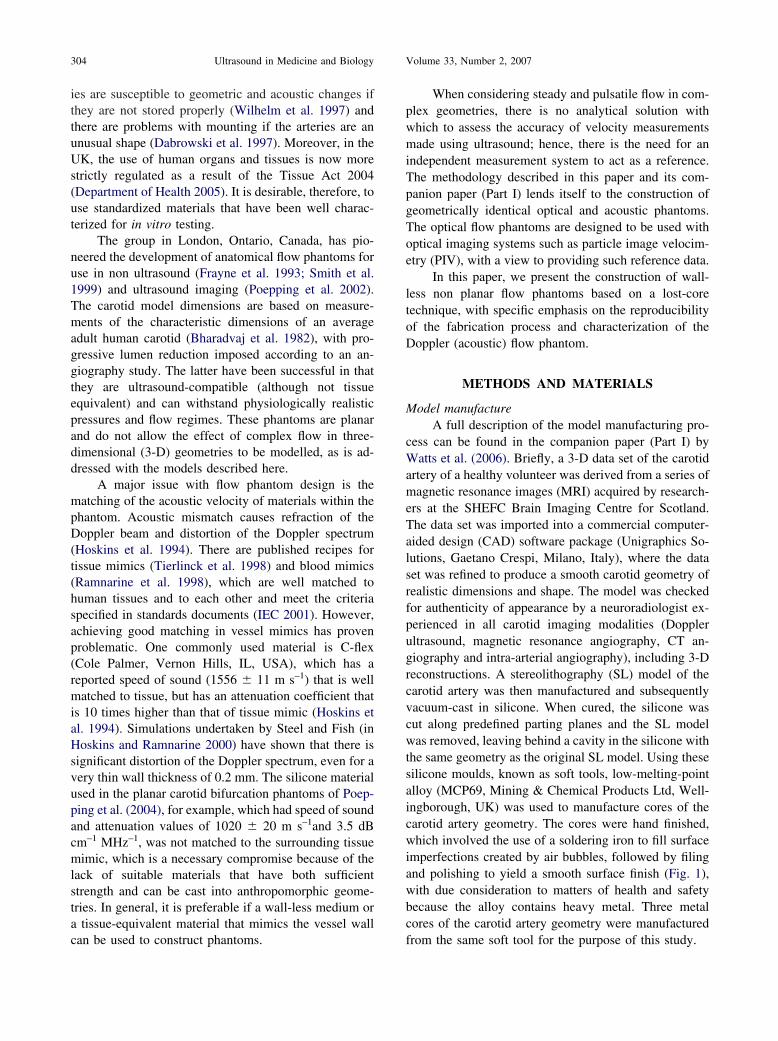
304 Ultrasound in Medicine and Biology Volume 33, Number 2, 2007
ies are susceptible to geometric and acoustic changes ifthey are not stored properly (Wilhelm et al. 1997) andthere are problems with mounting if the arteries are anunusual shape (Dabrowski et al. 1997). Moreover, in theUK, the use of human organs and tissues is now morestrictly regulated as a result of the Tissue Act 2004(Department of Health 2005). It is desirable, therefore, touse standardized materials that have been well charac-terized for in vitro testing.
The group in London, Ontario, Canada, has pio-neered the development of anatomical flow phantoms foruse in non ultrasound (Frayne et al. 1993; Smith et al.1999) and ultrasound imaging (Poepping et al. 2002).The carotid model dimensions are based on measure-ments of the characteristic dimensions of an averageadult human carotid (Bharadvaj et al. 1982), with pro-gressive lumen reduction imposed according to an an-giography study. The latter have been successful in thatthey are ultrasound-compatible (although not tissueequivalent) and can withstand physiologically realisticpressures and flow regimes. These phantoms are planarand do not allow the effect of complex flow in three-dimensional (3-D) geometries to be modelled, as is ad-dressed with the models described here.
A major issue with flow phantom design is thematching of the acoustic velocity of materials within thephantom. Acoustic mismatch causes refraction of theDoppler beam and distortion of the Doppler spectrum(Hoskins et al. 1994). There are published recipes fortissue mimics (Tierlinck et al. 1998) and blood mimics(Ramnarine et al. 1998), which are well matched tohuman tissues and to each other and meet the criteriaspecified in standards documents (IEC 2001). However,achieving good matching in vessel mimics has provenproblematic. One commonly used material is C-flex(Cole Palmer, Vernon Hills, IL, USA), which has areported speed of sound (1556 � 11 m s–1) that is wellmatched to tissue, but has an attenuation coefficient thatis 10 times higher than that of tissue mimic (Hoskins etal. 1994). Simulations undertaken by Steel and Fish (inHoskins and Ramnarine 2000) have shown that there issignificant distortion of the Doppler spectrum, even for avery thin wall thickness of 0.2 mm. The silicone materialused in the planar carotid bifurcation phantoms of Poep-ping et al. (2004), for example, which had speed of soundand attenuation values of 1020 � 20 m s–1and 3.5 dBcm–1 MHz–1, was not matched to the surrounding tissuemimic, which is a necessary compromise because of thelack of suitable materials that have both sufficientstrength and can be cast into anthropomorphic geome-tries. In general, it is preferable if a wall-less medium ora tissue-equivalent material that mimics the vessel wall
can be used to construct phantoms.When considering steady and pulsatile flow in com-plex geometries, there is no analytical solution withwhich to assess the accuracy of velocity measurementsmade using ultrasound; hence, there is the need for anindependent measurement system to act as a reference.The methodology described in this paper and its com-panion paper (Part I) lends itself to the construction ofgeometrically identical optical and acoustic phantoms.The optical flow phantoms are designed to be used withoptical imaging systems such as particle image velocim-etry (PIV), with a view to providing such reference data.
In this paper, we present the construction of wall-less non planar flow phantoms based on a lost-coretechnique, with specific emphasis on the reproducibilityof the fabrication process and characterization of theDoppler (acoustic) flow phantom.
METHODS AND MATERIALS
Model manufactureA full description of the model manufacturing pro-
cess can be found in the companion paper (Part I) byWatts et al. (2006). Briefly, a 3-D data set of the carotidartery of a healthy volunteer was derived from a series ofmagnetic resonance images (MRI) acquired by research-ers at the SHEFC Brain Imaging Centre for Scotland.The data set was imported into a commercial computer-aided design (CAD) software package (Unigraphics So-lutions, Gaetano Crespi, Milano, Italy), where the dataset was refined to produce a smooth carotid geometry ofrealistic dimensions and shape. The model was checkedfor authenticity of appearance by a neuroradiologist ex-perienced in all carotid imaging modalities (Dopplerultrasound, magnetic resonance angiography, CT an-giography and intra-arterial angiography), including 3-Dreconstructions. A stereolithography (SL) model of thecarotid artery was then manufactured and subsequentlyvacuum-cast in silicone. When cured, the silicone wascut along predefined parting planes and the SL modelwas removed, leaving behind a cavity in the silicone withthe same geometry as the original SL model. Using thesesilicone moulds, known as soft tools, low-melting-pointalloy (MCP69, Mining & Chemical Products Ltd, Well-ingborough, UK) was used to manufacture cores of thecarotid artery geometry. The cores were hand finished,which involved the use of a soldering iron to fill surfaceimperfections created by air bubbles, followed by filingand polishing to yield a smooth surface finish (Fig. 1),with due consideration to matters of health and safetybecause the alloy contains heavy metal. Three metalcores of the carotid artery geometry were manufactured
from the same soft tool for the purpose of this study.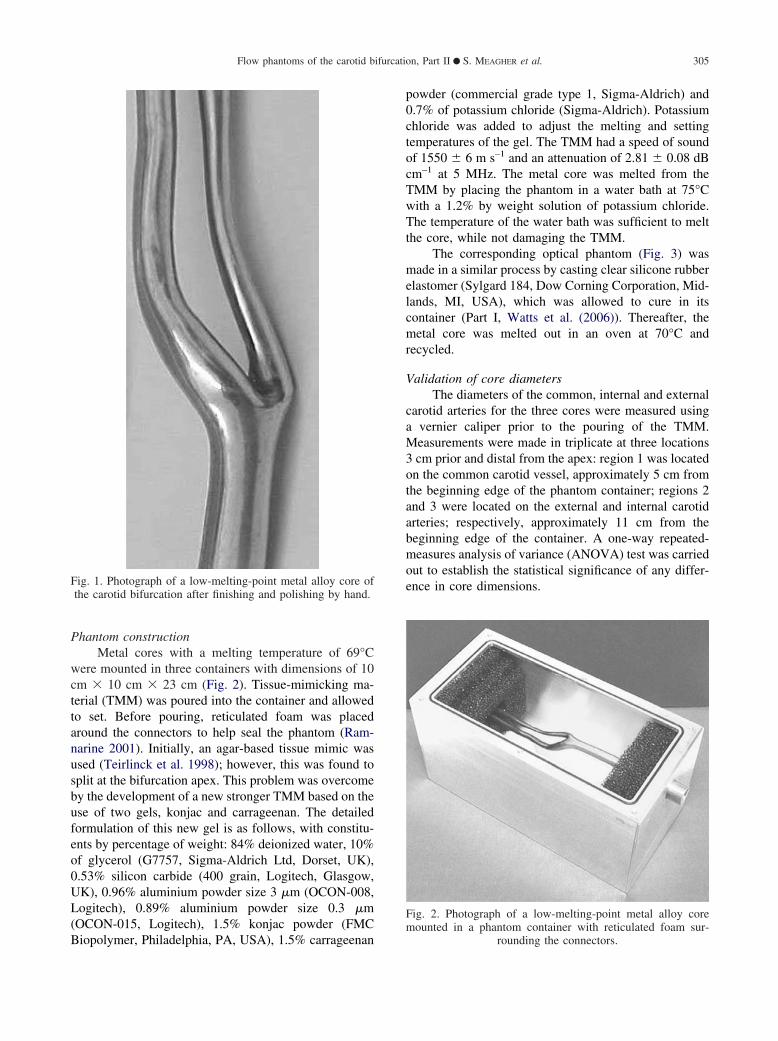
Flow phantoms of the carotid bifurcation, Part II ● S. MEAGHER et al. 305
Phantom constructionMetal cores with a melting temperature of 69°C
were mounted in three containers with dimensions of 10cm � 10 cm � 23 cm (Fig. 2). Tissue-mimicking ma-terial (TMM) was poured into the container and allowedto set. Before pouring, reticulated foam was placedaround the connectors to help seal the phantom (Ram-narine 2001). Initially, an agar-based tissue mimic wasused (Teirlinck et al. 1998); however, this was found tosplit at the bifurcation apex. This problem was overcomeby the development of a new stronger TMM based on theuse of two gels, konjac and carrageenan. The detailedformulation of this new gel is as follows, with constitu-ents by percentage of weight: 84% deionized water, 10%of glycerol (G7757, Sigma-Aldrich Ltd, Dorset, UK),0.53% silicon carbide (400 grain, Logitech, Glasgow,UK), 0.96% aluminium powder size 3 �m (OCON-008,Logitech), 0.89% aluminium powder size 0.3 �m(OCON-015, Logitech), 1.5% konjac powder (FMC
Fig. 1. Photograph of a low-melting-point metal alloy core ofthe carotid bifurcation after finishing and polishing by hand.
Biopolymer, Philadelphia, PA, USA), 1.5% carrageenan
powder (commercial grade type 1, Sigma-Aldrich) and0.7% of potassium chloride (Sigma-Aldrich). Potassiumchloride was added to adjust the melting and settingtemperatures of the gel. The TMM had a speed of soundof 1550 � 6 m s–1 and an attenuation of 2.81 � 0.08 dBcm–1 at 5 MHz. The metal core was melted from theTMM by placing the phantom in a water bath at 75°Cwith a 1.2% by weight solution of potassium chloride.The temperature of the water bath was sufficient to meltthe core, while not damaging the TMM.
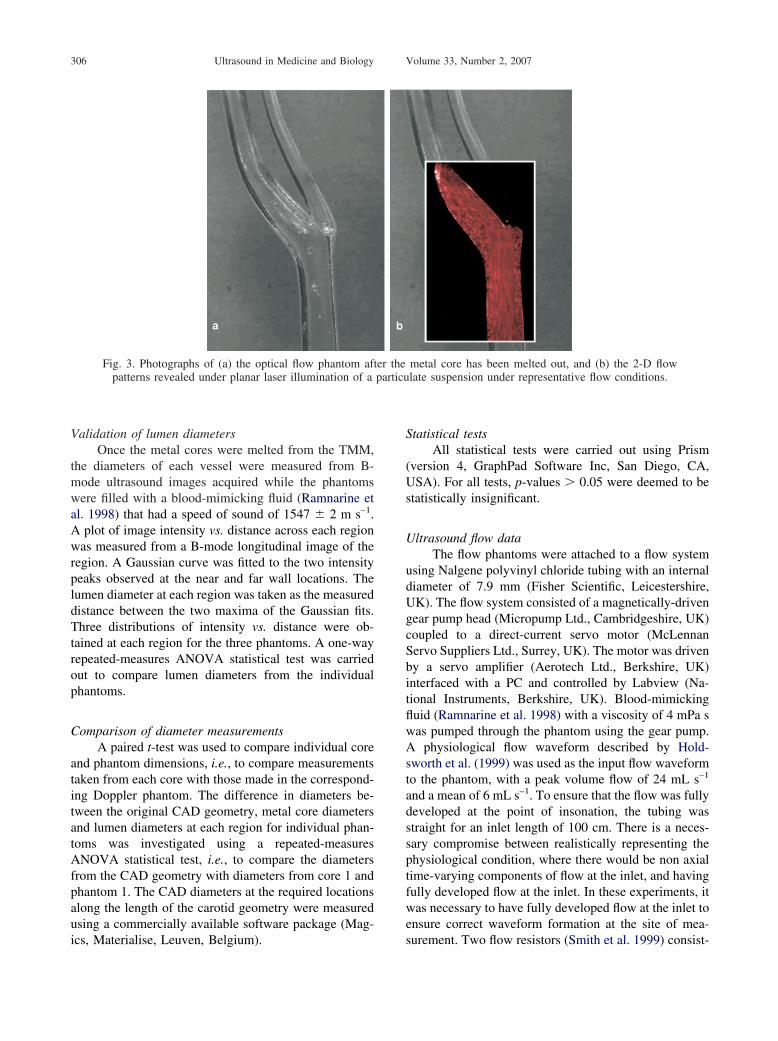
The corresponding optical phantom (Fig. 3) wasmade in a similar process by casting clear silicone rubberelastomer (Sylgard 184, Dow Corning Corporation, Mid-lands, MI, USA), which was allowed to cure in itscontainer (Part I, Watts et al. (2006)). Thereafter, themetal core was melted out in an oven at 70°C andrecycled.
Validation of core diametersThe diameters of the common, internal and external
carotid arteries for the three cores were measured usinga vernier caliper prior to the pouring of the TMM.Measurements were made in triplicate at three locations3 cm prior and distal from the apex: region 1 was locatedon the common carotid vessel, approximately 5 cm fromthe beginning edge of the phantom container; regions 2and 3 were located on the external and internal carotidarteries; respectively, approximately 11 cm from thebeginning edge of the container. A one-way repeated-measures analysis of variance (ANOVA) test was carriedout to establish the statistical significance of any differ-ence in core dimensions.
Fig. 2. Photograph of a low-melting-point metal alloy coremounted in a phantom container with reticulated foam sur-
rounding the connectors.
particu
306 Ultrasound in Medicine and Biology Volume 33, Number 2, 2007
Validation of lumen diametersOnce the metal cores were melted from the TMM,
the diameters of each vessel were measured from B-mode ultrasound images acquired while the phantomswere filled with a blood-mimicking fluid (Ramnarine etal. 1998) that had a speed of sound of 1547 � 2 m s–1.A plot of image intensity vs. distance across each regionwas measured from a B-mode longitudinal image of theregion. A Gaussian curve was fitted to the two intensitypeaks observed at the near and far wall locations. Thelumen diameter at each region was taken as the measureddistance between the two maxima of the Gaussian fits.Three distributions of intensity vs. distance were ob-tained at each region for the three phantoms. A one-wayrepeated-measures ANOVA statistical test was carriedout to compare lumen diameters from the individualphantoms.
Comparison of diameter measurementsA paired t-test was used to compare individual core
and phantom dimensions, i.e., to compare measurementstaken from each core with those made in the correspond-ing Doppler phantom. The difference in diameters be-tween the original CAD geometry, metal core diametersand lumen diameters at each region for individual phan-toms was investigated using a repeated-measuresANOVA statistical test, i.e., to compare the diametersfrom the CAD geometry with diameters from core 1 andphantom 1. The CAD diameters at the required locationsalong the length of the carotid geometry were measuredusing a commercially available software package (Mag-
Fig. 3. Photographs of (a) the optical flow phantom afpatterns revealed under planar laser illumination of a
ics, Materialise, Leuven, Belgium).
Statistical testsAll statistical tests were carried out using Prism
(version 4, GraphPad Software Inc, San Diego, CA,USA). For all tests, p-values � 0.05 were deemed to bestatistically insignificant.
Ultrasound flow dataThe flow phantoms were attached to a flow system
using Nalgene polyvinyl chloride tubing with an internaldiameter of 7.9 mm (Fisher Scientific, Leicestershire,UK). The flow system consisted of a magnetically-drivengear pump head (Micropump Ltd., Cambridgeshire, UK)coupled to a direct-current servo motor (McLennanServo Suppliers Ltd., Surrey, UK). The motor was drivenby a servo amplifier (Aerotech Ltd., Berkshire, UK)interfaced with a PC and controlled by Labview (Na-tional Instruments, Berkshire, UK). Blood-mimickingfluid (Ramnarine et al. 1998) with a viscosity of 4 mPa swas pumped through the phantom using the gear pump.A physiological flow waveform described by Hold-sworth et al. (1999) was used as the input flow waveformto the phantom, with a peak volume flow of 24 mL s–1
and a mean of 6 mL s–1. To ensure that the flow was fullydeveloped at the point of insonation, the tubing wasstraight for an inlet length of 100 cm. There is a neces-sary compromise between realistically representing thephysiological condition, where there would be non axialtime-varying components of flow at the inlet, and havingfully developed flow at the inlet. In these experiments, itwas necessary to have fully developed flow at the inlet toensure correct waveform formation at the site of mea-
metal core has been melted out, and (b) the 2-D flowlate suspension under representative flow conditions.
ter the
surement. Two flow resistors (Smith et al. 1999) consist-
n diam
Flow phantoms of the carotid bifurcation, Part II ● S. MEAGHER et al. 307
ing of 3.2 mm inner-diameter C-flex tubing of length 2 mand 1 m, were connected to the external and internalcarotid artery outlets, respectively. These flow resistorsrepresented the resistance of the distal vascular bed andhelped to damp out any reflections from tubing connec-tions. Using these types of flow resistors, a volume flowratio between the internal and the external carotid arter-ies, similar to that found in vivo, can be achieved (65:35),thus ensuring physiologically realistic flow waveforms inthe phantoms.
An HDI 5000 (Philips Medical Systems, Bothell,WA, USA) ultrasound system was used to collect spec-tral data at sites within the common carotid and justdownstream of the bifurcation in both the external andinternal carotid arteries. An L12-5 ultrasound probe wasused to collect longitudinal images of each region, witha 1-mm Doppler sample volume in the center of eachregion from which spectral data were collected. In eachregion, angle correction was made by aligning the anglecursor to the vessel wall. The spectral gain was adjusteduntil a clear spectrum could be seen on the screen.Resistance indices (Pourcelot 1974; Dudley et al. 1990)were measured for each of the waveforms. Resistance
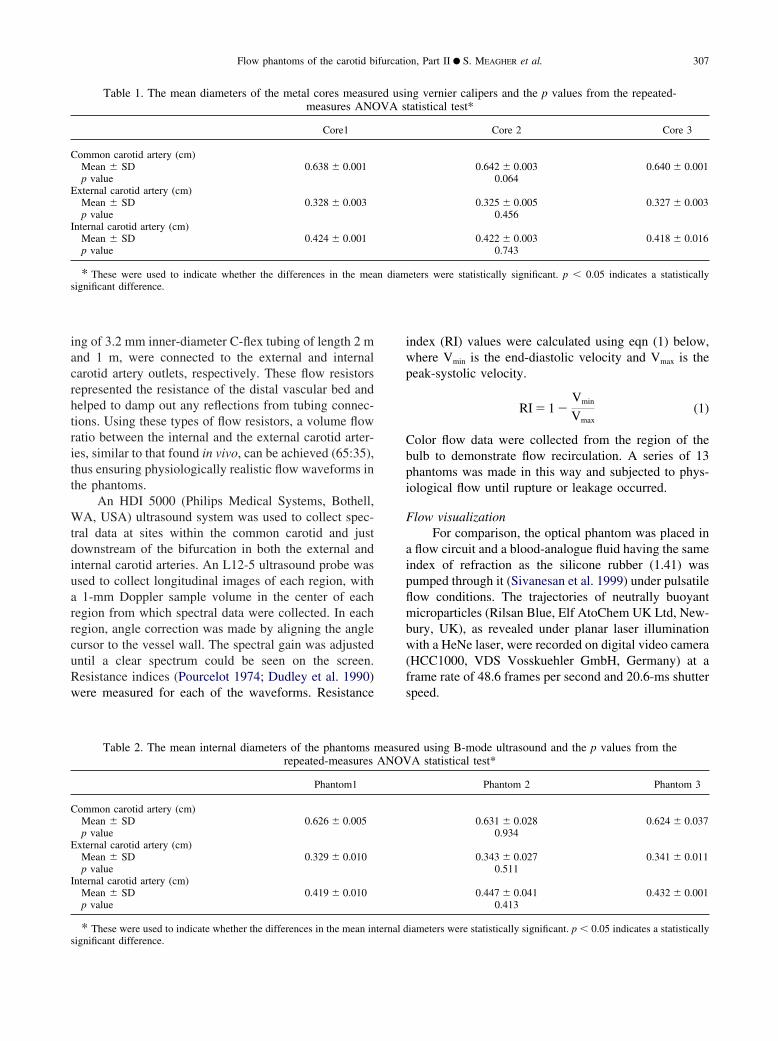
Table 1. The mean diameters of the metal cores measurmeasures ANO
Core1
Common carotid artery (cm)Mean � SD 0.638 � 0.001p value
External carotid artery (cm)Mean � SD 0.328 � 0.003p value
Internal carotid artery (cm)Mean � SD 0.424 � 0.001p value
* These were used to indicate whether the differences in the measignificant difference.
Table 2. The mean internal diameters of the phantomsrepeated-measures
Phantom1
Common carotid artery (cm)Mean � SD 0.626 � 0.005p value
External carotid artery (cm)Mean � SD 0.329 � 0.010p value
Internal carotid artery (cm)Mean � SD 0.419 � 0.010p value
* These were used to indicate whether the differences in the mean internal dsignificant difference.
index (RI) values were calculated using eqn (1) below,where Vmin is the end-diastolic velocity and Vmax is thepeak-systolic velocity.
RI � 1 �Vmin
Vmax(1)
Color flow data were collected from the region of thebulb to demonstrate flow recirculation. A series of 13phantoms was made in this way and subjected to phys-iological flow until rupture or leakage occurred.
Flow visualizationFor comparison, the optical phantom was placed in
a flow circuit and a blood-analogue fluid having the sameindex of refraction as the silicone rubber (1.41) waspumped through it (Sivanesan et al. 1999) under pulsatileflow conditions. The trajectories of neutrally buoyantmicroparticles (Rilsan Blue, Elf AtoChem UK Ltd, New-bury, UK), as revealed under planar laser illuminationwith a HeNe laser, were recorded on digital video camera(HCC1000, VDS Vosskuehler GmbH, Germany) at aframe rate of 48.6 frames per second and 20.6-ms shutterspeed.
ng vernier calipers and the p values from the repeated-tatistical test*
Core 2 Core 3
0.642 � 0.003 0.640 � 0.0010.064
0.325 � 0.005 0.327 � 0.0030.456
0.422 � 0.003 0.418 � 0.0160.743
eters were statistically significant. p � 0.05 indicates a statistically
ed using B-mode ultrasound and the p values from theA statistical test*
Phantom 2 Phantom 3
0.631 � 0.028 0.624 � 0.0370.934
0.343 � 0.027 0.341 � 0.0110.511
0.447 � 0.041 0.432 � 0.0010.413
ed usiVA s
measurANOV
iameters were statistically significant. p � 0.05 indicates a statistically
308 Ultrasound in Medicine and Biology Volume 33, Number 2, 2007
Percent distensionWall distension in the Doppler phantom was mea-
sured using M-mode ultrasound. The built-in software onthe HDI 5000 ultrasound system was used to mark op-posite points on the anterior and posterior walls of thecommon carotid artery. Distension was calculated ac-cording to eqn (2), where Dsys is the diameter measuredat peak systole and Ddias is the diameter measured at enddiastole.
Distension � �Dsys � Ddias
Ddias �� 100 (2)
RESULTS
Validation of metal alloy core diametersTable 1 shows the mean of the three repeated di-
ameter measurements made on each of the metal alloycores at each region. The standard deviation (SD) of thethree measurements can be used as a measure of the errorin measurement. The repeated-measures ANOVA statis-tical test showed that the variation in the measurement ofdiameter at each region between the cores was not sig-nificant (p � 0.05).
Validation of lumen diametersTable 2 shows the mean of the three diameter mea-
surements made on the phantoms at each region. The
Table 3. The p values calculated from paired t-tests*
Core 1Phantom 1
Core 2Phantom 2
Core 3Phantom 3
Common carotid arteryp value 0.057 0.537 0.526
External carotid arteryp value 0.968 0.441 0.102
Internal carotid arteryp value 0.494 0.331 0.278
* Used to compare differences in core diameters and the internaldiameters of the phantoms. p values � 0.05 indicate a statisticallysignificant difference.
Table 4. Diameters of the metal cores, the inCAD geo
CAD Core 1 Phantom 1
Common carotid arteryDiameters (cm) 0.794 0.638 0.626p value 0.0001
External carotid arteryDiameters (cm) 0.414 0.328 0.329p value 0.0001
Internal carotid arteryDiameters (cm) 0.534 0.424 0.419p value 0.0001
The p values indicate the result of a repeated-measures ANOVA test, whichCAD geometry, the metal cores and the internal diameter of the phantoms. p
repeated-measures ANOVA statistical test showed thatthe variation in the measurement of diameter at eachregion between the phantoms was not significant (p �0.05).
Comparison of diameter measurementsThe results from the paired t-test (Table 3) showed
that there were statistically insignificant differences indiameters between the cores, and the phantoms that theywere used to construct (p � 0.05). Table 4 show thatthere were significant differences (p � 0.05) in diametersbetween the metal cores, internal diameters of the phan-toms and the original CAD geometry.
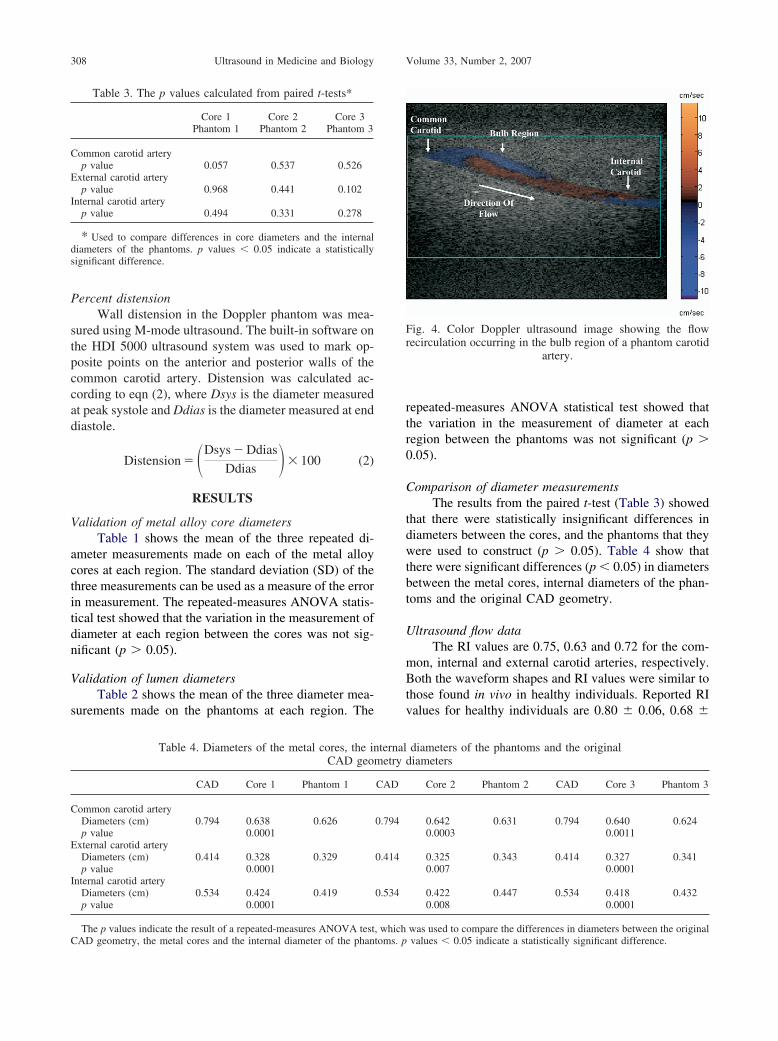
Ultrasound flow dataThe RI values are 0.75, 0.63 and 0.72 for the com-
mon, internal and external carotid arteries, respectively.Both the waveform shapes and RI values were similar tothose found in vivo in healthy individuals. Reported RIvalues for healthy individuals are 0.80 � 0.06, 0.68 �
Fig. 4. Color Doppler ultrasound image showing the flowrecirculation occurring in the bulb region of a phantom carotid
artery.
diameters of the phantoms and the originaldiameters
Core 2 Phantom 2 CAD Core 3 Phantom 3
0.642 0.631 0.794 0.640 0.6240.0003 0.0011
0.325 0.343 0.414 0.327 0.3410.007 0.0001
0.422 0.447 0.534 0.418 0.4320.008 0.0001
ternalmetry
CAD
0.794
0.414
0.534
was used to compare the differences in diameters between the originalvalues � 0.05 indicate a statistically significant difference.

Flow phantoms of the carotid bifurcation, Part II ● S. MEAGHER et al. 309
0.07 and 0.82 � 0.08 for the common, internal andexternal carotid arteries, respectively (Naessen et al.2001).
Technical success rateNone of the 13 phantoms ruptured within the lumen.
Eleven of the 13 phantoms leaked within 1 h of startingflow, all at the interface between the common carotidinlet and the tissue mimic. One phantom leaked between1 and 2 h, and one phantom was not leaking at 4 h.
Flow visualizationWhen viewed under planar laser illumination, the
flow patterns in the optical phantoms’ internal carotidbulb region were revealed (Fig. 3). The correspondingDoppler color flow image obtained in the acoustic phan-tom is shown in Fig. 4.
DistensionWall distension in the Doppler phantom (10 � 1%)
was similar to that measured in the common carotidarteries of an average 45-y-old male (8.3 � 0.8 %)(Hansen et al. 1995).
DISCUSSION
The method described for creation of anatomicalmodels, using a rapid prototyping approach, can in prin-ciple be adopted for more complex geometries, althoughthe core manufacture and phantom manufacture processwould be more challenging.
This paper and its companion paper describe thecreation of dual phantoms with identical geometries; onefor particle image velocimetry (PIV) and one for ultra-sound imaging. PIV is a quantitative velocity measure-ment technique in which particles seeded within a fluidflowing through a transparent model are illuminated bylaser light and consecutive images are taken of the par-ticles. The velocity distribution is then estimated usingcross-correlation techniques, in much the same way thatspeckle tracking is used in ultrasound (Bohs et al. 2000).By making use of this approach, involving pairs ofphantoms developed according to this and the compan-ion paper (Part I, Watts et al. (2006)), we believe that amethod for calibration of ultrasound-based measure-ments of velocity may be found. However, before wecould implement this approach, the problem of leakagehad to be solved.
To ensure dynamic similarity between the two flowsystems, the flow rate of the PIV fluid needs be scaled bythe ratio of the two system fluids’ kinematic viscosities,and the time period of the PIV fluid flow rate needs to bescaled by the reciprocal of the viscosities. By ensuring
that we have dynamic similarity between the flow sys-tems and that the flow conditions for both the optical andultrasound flow phantoms are the same, the flow dynam-ics in both systems will be identical, allowing us tocalibrate ultrasound flow measurements against thosemade by the PIV system. The restrictions to calibrationwill be in distension properties of both phantoms. Sincethe corresponding PIV flow waveform must be dynam-ically scaled, it may still be possible for the distensionwaveforms of both phantoms to be substantially thesame. Further work in measuring distension properties inthe two flow systems is needed, however. Wall shearmeasurements may also be affected due to differences inwall positions between the phantoms. The difference inelasticity between the phantoms is an inherent limitationof this ultrasound calibration method.
The key aspect of the phantom that we were inter-ested in mimicking was the distension of the wall, which,at 10%, is similar to that recorded in the carotid artery invivo (8.3%, Hansen et al.1995). More complex consid-erations of tissue movement away from the wall arelikely to reveal differences between the phantom and thein vivo case because, in reality, a vessel is surrounded byother tissue, whereas in the phantom, there is a singlebody of tissue mimic.
The significant differences evident in Table 4 are aresult of the hand-finishing techniques applied to themetal cores to produce a smooth surface finish, whichinevitably resulted in a reduction in diameter. Neverthe-less, the statistically insignificant differences in corediameters (Table 1), lumen diameters (Table 2) andbetween core and lumen diameters (Table 3) show thereliability of our production methods in creating geomet-rically similar phantoms with near identical dimensions.
The overall shapes of the spectral waveforms col-lected along the carotid phantom agreed well with pub-lished literature, without rupturing of the tissue mimicmaterial. The leakage at the interface between commoncarotid artery inlet and the tissue mimic is a more minortechnical problem that has yet to be overcome consis-tently. The flow recirculation observed in Fig. 3b, thebulb region of the optical flow phantom and in the colorflow image of the bulb region of the Doppler phantom(Fig. 4) show the same complex flow as has been ob-served in vivo (Zierler et al. 1987).
CONCLUSION
The above study has shown that it is possible toproduce anatomical flow phantoms with non planar ge-ometries. Although there are differences in diametersbetween the original CAD carotid artery geometry andthe low-melting-point metal alloy carotid artery cores,the differences between individual cores and the phan-
toms that they are used to construct is insignificant. In
310 Ultrasound in Medicine and Biology Volume 33, Number 2, 2007
conclusion, we have shown how rapid manufacturingtechnology and investment casting may be used to re-produce geometrically similar anatomical flow phantomsthat exhibit realistic physiological flow patterns and dis-tensions.
Acknowledgements—In this paper, author order consists of the re-searchers in descending order of contribution followed by projectsupervisors in ascending order of contribution. The authors gratefullyacknowledge the financial support of the UK Engineering and PhysicalSciences Research Council (EPSRC grants GR/N16747/01, GR/N16778/01 and GR/R19793/01).
REFERENCES
Allard L, Cloutier G, Durand LG. Doppler velocity ratio measurementsevaluated in a phantom model of multiple arterial disease. Ultra-sound Med Biol 1995;21:471–480.
Bale-Glickman J, Selby K, Saloner D, Savas O. Experimental flowstudies in exact-replica phantoms of atherosclerotic carotid bifur-cations under steady input conditions. J Biomech Eng 2003;125:38–48.
Bharadvaj BK, Mabon RF, Giddens DP. Steady flow in a model of thehuman carotid bifurcation. Part I–flow visualization. J Biomech1982;15:349–362.
Bohs LN, Geiman BJ, Anderson ME, Gebhart SC, Trahey GE. Speckletracking for multi-dimensional flow estimation. Ultrasonics 2000;38:369–375.
Brands PJ, Hoeks APG, Hofstra L, Reneman RS. A noninvasivemethod to estimate wall shear rate using ultrasound. UltrasoundMed Biol 1995;21:171–185.
Dabrowski W, Dunmore-Buyze J, Rankin RN, Holdsworth DW, Fen-ster A. A real vessel phantom for imaging experimentation. MedPhys 1997;24:687–693.
Daigle RJ, Stravros AT, Lees RM. Overestimation of velocity andfrequency values by multi-element linear array Dopplers. J VascTechnol 1990;14:206–213.
Deane CR, Markus HS. Colour velocity flow measurement: In vitrovalidation and application to human carotid arteries. UltrasoundMed Biol 1997;23:447–452.
Department of Health. The Human Tissue Act 2004: New legislationon human organs and tissue. Available at: https://www.tsoshop.co.uk/. Accessed 9/11/2006.
Dudley NJ, Green IR, Griffiths PA. Monitoring of recovery followingexercise in the Doppler ultrasound evaluation of lower limb arterialdisease. Clin Phys Physiol Meas 1990;11:193–199.
Embree PM, O’Brien WD. Volumetric blood flow via time-domaincorrelation: Experimental Verification. IEEE Transact UltrasonFerroelectr Freq Control 1990;37:332–336.
Frayne R, Gowman LM, Rickey DW, et al. A geometrically accuratevascular phantom for comparative studies of x-ray, ultrasound, andmagnetic resonance vascular imaging: Construction and geometri-cal verification. Med Phys 1993;20:415–425.
Forsberg F, Morvay Z, Rawool NM, Deane CR, Needleman L. Shearrate estimation using a clinical ultrasound scanner. J UltrasoundMed 2000;19:323–327.
Grant EG, Benson CB, Moneta GL, et al. Carotid artery stenosis:Gray-scale and Doppler US diagnosis—Society of Radiologists inUltrasound consensus conference. Radiology 2003;229:340–346.
Hansen F, Mangell P, Sonesson B, Lanne T. Diameter and compliancein the human common carotid artery—Variations with age and sex.
Ultrasound Med Biol 1995;21:1–9.Holdsworth DW, Norley CJ, Frayne R, Steinman DA, Rutt BK. Char-acterization of common carotid artery blood-flow waveforms innormal human subjects. Physiol Meas 1999;20:219–240.
Hoskins PR, Li SF, McDicken WN. Velocity estimation using duplexscanners. Ultrasound Med Biol 1991;17:195–199.
Hoskins PR, Sherriff SB, Evans JA. Testing of Doppler ultrasoundequipment. York: IPSM; 1994:12–27.
Hoskins PR. Accuracy of maximum velocity estimates made usingDoppler ultrasound systems. Br J Radiol 1996;69:172–177.
Hoskins PR, Ramnarine KV. Doppler test devices. In Evans DH,McDicken WN (eds): Doppler Ultrasound, ed 2. Chichester: Wiley;2000:382–404.
Hoskins PR. A review of the measurement of blood velocity and relatedquantities using Doppler ultrasound. Proc Inst Mech Engrs 1999;213(H):391–400.
Hughes PE, How TV. Quantitative measurement of wall shear rate bypulsed Doppler ultrasound. J Med Eng Technol 1993;17:58–64.
IEC 61685. Ultrasonics—Flow measurement systems, flow test object,2001. International Electrotechnical Commission, Geneva, Switzer-land.
Kerber CW, Heilman CB. Flow dynamics in the human carotid artery:Preliminary observations using a transparent elastic model. Am JNeuroradiol 1992;13:173–180.
Motomiya M, Karino T. Flow patterns in the human carotid arterybifurcation. Stroke 1984;15:50–56.
Naessen T, Bakos O. Carotid vascular resistance in long-term estrogenusers. Obstet Gynecol 2001;97:327–332.
Pourcelot L. Applications cliniques de l’examen Doppler transcutaneVilocime’trie UIrrasonore Doppler. Seminuire INSERM Paris1974:213–240.
Poepping TL, Nikolov HN, Rankin RN, Lee M, Holdsworth DW. Anin vitro system for Doppler ultrasound flow studies in the stenosedcarotid artery bifurcation. Ultrasound Med Biol 2002;28:495–506.
Poepping TL, Nikolov HN, Thorne ML, Holdsworth DW. A thin-walled carotid vessel phantom for Doppler ultrasound flow studies.Ultrasound Med Biol 2004;30:1067–1078.
Ramnarine KV, Nassiri DK, Hoskins PR, Lubbers J. Validation of anew blood mimicking fluid for use in Doppler flow test objects.Ultrasound Med. Biol 1998;24:451–459.
Ramnarine KV, Anderson T, Hoskins PR. Construction and geometricstability of physiological flow rate wall-less stenosis phantoms.Ultrasound Med Biol 2001;27:245–250.
Sivanesan S, How TV, Black RA, Bakran A. Flow patterns in theradiocephalic arteriovenous fistula: An in vitro study. J Biomech1999;32:915–925.
Smith RF, Rutt BK, Holdsworth DW. Anthropomorphic carotid bifur-cation phantom for MRI applications. J Magn Reson Imaging1999;10:533–544.
Teirlinck CJ, Bezemer RA, Kollmann C, et al. Development of anexample test object and comparison of five of these test objects,constructed in various laboratories. Ultrasonics 1998;36:653–660.
Vattyam HM, Shu MC, Rittgers SE. Quantification of Doppler colorflow images from a stenosed carotid artery model. Ultrasound MedBiol 1992;18:195–203.
Watts DM, Sutcliffe CJ, Morgan RH, et al. Anatomical flow phantomsof the nonplanar carotid bifurcation. Part I: computer-aided designand fabrication. Ultrasound Med Biol 2007;33:296–302
Wilhjelm JE, Vogt K, Jespersen SK, Sillesen H. Influence of tissuepreservation methods on arterial geometry and echogenicity. Ultra-sound Med Biol 1997;23:1071–1082.
Zierler RE, Phillips DJ, Beach KW, Primozich JF, Strandness DE Jr.Noninvasive assessment of normal carotid bifurcation hemodynam-ics with color-flow ultrasound imaging. Ultrasound Med Biol 1987;
13:471–476.
Related Documents











