What are the salient features of the case?
GROUP 4
1. Nallathambi, Aiswarya 2. Nagarajan, Venkateshwari3. Narayanaswamy, Nithya4. Nallagatla, Susmitha5. Narra, Vindhya Rani Anaphylaxis 1. What are the salient features of the case?Age 42 y.o Stung on the forearm while working in the garden. Localised swelling. Within minutes, she experienced flushing, sweating followed by shortness of breath and dyspnea. Followed by confusion and respiratory distress.
The physical presentation of respiratory distress is generally referred to as labored breathing, while the sensation of respiratory distress is called shortness of breath or dyspnea.E.R T = 37.2 P = 120 beats per min(tachykardia)RR = 39 breaths per min(tachypnea)BP = 69/45 (Severe hypotension)
Vital signsParameterNormal Range Pulse 60 100 beats per min Blood pressure (systolic) 90 140mmHgBlood pressure (diastolic)60 90mmHgRespiratory rate 12 20breaths per min Normal Vital Signs Generalised urticaria - Urticaria refers to a group of disorders affecting adults and children, in which red patches and weals occur in the skin. A weal is a swelling of the surface skin. The name urticaria is derived from the common European stinging nettle 'Urtica dioica'.UrticariaThe skin swelling seen in urticaria is due to the release of chemicals such as histamine from mast cells and basophils in the skin, which causes small blood vessels to leak. The weals can be a few millimetres or several centimetres in diameter, coloured white or red, often surrounded by a red flare, and frequently itchy. Each weal may last a few minutes or several hours, and may change shape. Weals may be round, or form rings, a map-like pattern or giant patches.The surface weals may be accompanied by deeper swelling of eyelids, lips, hands and elsewhere.
Urticaria and Angioedema
The patient was noted to have wheezing. And she had encountered insect stings in the past without reaction on several occasions.Other symptoms
2. What are your differentials?Tachycardia Damage to heart tissues from heart diseaseAbnormal electrical pathways in the heart present at birth (congenital)Disease or congenital abnormality of the heartAnemiaExerciseSudden stress, such as frightHigh blood pressureAnaphylactic shockDifferential for the vital signs In anaphylaxis, the patient experiences tachykardia as the heart pumps faster to compensate for the drop in BPSevere hypotension mainly caused by Blood lossSevere infection (septicemia)Severe allergic reaction (anaphylaxis)Lack of nutrients in diet In this case, the insect bite will trigger the release of histamine in the body cells which causes widespread dilatation of the blood vessels which accounts for the drop in BP.
Differential diagnosis of AnaphylaxisV
Vasodepressor (vasovagal) reaction (probably the most common masquerader)Globus hystericus(a lump in ones throat)Hereditary angioedemaOther forms of shock (ie, hypovolemic, cardiogenic, septic)Flushing syndrome, including red man syndrome (vancomycin), pancreatic polypeptide tumors, postmenopausal patient, ethanol-induced, autonomic epilepsyMonosodium glutamate poisoningCapillary leak syndromePulmonary embolismMyocardial dysfunctionForeign body aspiration (young children, especially)Poisoning, acuteNeurologic (stroke, seizure)
3. What is your final diagnosis? Support your diagnosis. The final diagnosis is that the patient is suffering from Anaphylaxis. The clinical diagnosis of anaphylaxis is based on probability and pattern recognition. Anaphylaxis is considered likely to be present if any 1 of the 3 following clinical criteria is satisfied within minutes to hours:
1. Acute symptoms involving skin, mucosal surface, or both, as well as at least one of the following: respiratory compromise, hypotension, or end-organ dysfunction.
2. Two or more of the following occur rapidly after exposure to a likely allergen: hypotension, respiratory compromise, persistent gastrointestinal symptoms, or involvement of skin or mucosal surface.
3. Hypotension develops after exposure to an allergen known to cause symptoms for that patient: age-specific low blood pressure or decline of systolic blood pressure of more than 30% compared to baseline.
However, anaphylaxis occurs as part of a clinical continuum that can begin with relatively mild features and rapidly progress to life-endangering respiratory or cardiovascular manifestations. Delaying the diagnosis until multiorgan manifestations of anaphylaxis are present is risky because the severity of a reaction is difficult or impossible to predict at the time of symptom onset.4. What lab tests can be requested?Plasma histamine levels rise within 10 minutes of onset but fall again within 30 minutes. Urinary histamine levels are generally not dependable, as this test can be affected by diet and by bacteria in the urine.Plasma histamine levels Tryptase is a trypsinlike proteinase that is most abundant in human mast cells and basophils.Serum mature tryptase (previously called beta-tryptase) levels peak 60-90 minutes after the start of an episode and may persist for as long as 5 hours. Serum levels are normally less than 11.5 ng/mL. Elevated levels of serum tryptase occur in both anaphylactic and anaphylactoid reactions.Serum tryptase levelIf the patients history suggests an insect sting, allergen-specific skin testing to Hymenoptera venoms should be performed.If those tests remain negative after 6 weeks in a patient with a serious reaction, then further testing can include in vitro IgE tests.Skin Testing and Invitro IgE testingSkin testing and in vitro IgE testing should be performed 4-6 weeks following the episode of anaphylaxis to improve the sensitivity of the diagnostic test. Skin testing for imported fire ant hypersensitivity should be performed using whole-body extracts. Skin testing and in vitro Ig-e testingPatients ability to identify the type of flying insect is unreliable (eg, many confuse yellow jackets and bees), generally mandating testing for all flying Hymenoptera. However, exceptions to this mandate can be made for patients whose stings were accompanied by sterile pustule formation within 24 hours (pathognomonic for fire ant sting) or for whom an impaled stinger and abdominal remnant were found at the sting site (the honeybee eviscerates itself as it stings)
Explain the pathophysiology of the immunological process What is anaphylaxis?Ana (without), phylaxis (protection).Acute multi-systemic allergic reaction involving the skin, airway, vascular system, and GI.The result of a re-exposure to an antigen that elicits an IgE mediated responseUsually caused by a common environmental protein that is not intrinsically harmfulOften caused by medications, foods, and insect stingsIt is a Type I hypersensitivity
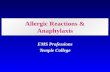
32Hypersensitivity ReactionInjurious, or pathologic, immune reactions are called hypersensitivity reactions. Hypersensitivity reactions may occur in two situations. First, responses to foreign antigens may be dysregulated or uncontrolled, resulting in tissue injury. Second, the immune responses may be directed against self antigens, as a result of the failure of self-tolerance (autoimmunity).Types of hyper sensitivity reactionsEtiologyWhat is happening?Occurs after reexposure to an antigen to which that person has produced a specific IgE antibody.Initial exposure sensitizes mast cells.Antigen specific IgE molecules attach to high affinity Fc receptors on the mast cell surface.On re-exposure Cross linking of IgE molecules on surface causes intracellular signaling pathwayInflammatory mediators are released upon degranulationPathophysiologyFirst exposureActivation of TH2 cell Stimulate IgE switchingAllergenTH2 CellB CellPathophysiologyFirst exposureIgE productionIgE secreting B cellIgEPathophysiologyFirst exposureIgE bind to mast cellMast cellFcRIIgEPathophysiologySecond exposureRecognitionAllergenMast cellFcRIIgEPathophysiologySecond exposureActivation of mast cell to release histamine and other mediatorsAllergenMediatorsMast cellFcRIIgEPathophysiologySigns and symptoms primarily due toSudden release of histamine and other potent mediatorsSmooth muscle contractionIncreased vascular permeabilityVasodilation
May include life-threatening reactions involving the airways, blood vessels, and heart
Symptoms generally have onset within minutes but can rarely occur as late as several hours after exposure to the offending antigen
42Pathologic features of anaphylaxisLaryngeal edemaPulmonary hyperinflationMyocardial edemaVisceral congestion or hemorrhageEosinophilic infiltration Elevated tryptase levelsDeath from cardiovascular collapse or respiratory obstruction
Mediators InvolvedInclude histamine, proteases, chemotactic factors, leukotrienes, prostaglandin D, and cytokinesPrimary: released before degranulationInterleukin 4 used by T cells induces B cell maturationIL-3 and IL-5 released by T and mast cells are chemo attractants for eosinophilsSecondary: come from granules
PathophysiologyHistamineSynthesized and stored in granulesThe primary mediator in the granulesMany of the signs and symptoms of anaphylaxis are attributable to binding of histamine to its receptors3 receptorsH1H2H3 Binding to H1 receptors mediates pruritis, rhinorrhea, tachycardia, and bronchospasm. On the other hand, both H1 and H2 receptors participate in producing headache, flushing, and hypotension.
Tissue Effects of HistamineCardiovascularDecreased blood pressureIncreased heart rateEdema (separation of endothelial cells & increased permeability)Respiratorybroncho constrictionGastrointestinalSmooth muscle contraction and diarrheaSkinUrticaria
Effects of histamine on airways Histamine
Bronchoconstriction by stimulation of H1 receptors on smooth muscles. Mucosal edema from increased microvascular permeability (H1) leading to transudation of fluid and macromolecules through wide intercellular gaps (> 12 nm).Direct stimulation of vagal (cholinergic) nerves can induce airway smoothmuscle contractionStimulation of H1 receptors increases mucus secretions, and stimulation of H2 receptors increases mucus viscosity.
Effects of histamine on the heartH1 receptors mediate coronary artery vasoconstriction and increased vascular permeability.
H2 receptors mediate atrial and ventricular contractile forces, atrial rate, and coronary artery vasodilation. Decreased diastolic pressure and increased pulse pressure
HistamineH1 receptor on endothelial cellL-arginineNitric oxide
Decreases venous returnOther MediatorsMetabolites of arachadonic acid, including prostaglandins, principally prostaglandin D2 (PGD2) and leukotrienes, principally leukotriene C4 (LTC4). PGD2 mediates bronchospasm and vascular dilatation, principle manifestations of anaphylaxis. LTC4 is converted into LTD4 and LTE4, mediators of hypotension, bronchospasm, and mucous secretion during anaphylaxis in addition to acting as chemotactic signals for eosinophils and neutrophils.Other pathways active during anaphylaxis are the complement system, the kallikrein-kinin system, the clotting cascade, and the fibrinolytic systemAnaphylactic Reaction (Summary) Phil Lieberman: Anaphylaxis,a cliicians manualMast CellMast cell granulesAllergenIgE antibodyImmediate reactionWheezeUrticariaHypotensionAbdominal cramping
Late-phase reaction54Anaphylactic reactions begin when an allergen interacts with cell-bound IgE antibodies following a breach of the hosts immunological barriers (e.g. skin, mucous membranes, etc). The antigen then encounters highly reactive, sensitized cells in tissue (mast cells) or blood (basophils).The release of cellular mediators leads to end-organ responses in the skin, respiratory tract, cardiovascular system, and/or gastrointestinal system. The strength of the reaction is dependent upon the trigger. Reactions may be immediate and uniphasic but may also include delayed onset, protracted, or biphasic.
Lieberman P. Ananphylaxis, a clinicians manual. In press.6. Differentiate anaphylactic from anaphylactoid reactionSpecifically, the condition anaphylaxis requires the patient to be sensitized, and their reaction mediated through immunoglobin E (IgE) antibodies.
An anaphylactoid reaction doesnt need the presence of IgE antibodies for a hypersensitivity reaction to occur.
Substances initiating the anaphylactoid reaction, such as radiopaque contrast media, nonsteroidal anti-inflammatory drugs (NSAIDs) and aspirin cause a direct breakdown of the mast cell and basophil membranes.An anaphylactic reaction occurs only after the patient has been previously exposed at least once to the antigen and is sensitized.
An anaphylactoid reaction can occur following a single, first-time exposure to certain agents in nonsensitized patients.
Because anaphylactic and anaphylactoid reactions produce the same clinical manifestations and are treated exactly the same way, we use the term anaphylaxis to refer to both conditions. 7. Structure and function of immunoglobulin involved
structural features of IGEIt is a monomer and its structure is very similar to IG M except the fact that it contains an extra constant domain that replaces the hinge.There are two cysteine residues per CE2 domain.They are located within the carboxyl terminal close to one another which are linked by disulfide bond to the other heavy chain.Tailpiece is absent.
Function of IgEThe major function of Ig E is its ability to bind Fc receptors specific for Fc region in IgE. It is of two types. 1. Tight binding receptors -mast cells and basophils
2. Weaker binding receptor -lymphocytes -monocytes -macrophages -eosinophils and platelets
This binding stimulates degranulation of cells releasing chemicals. So this Ig is found to be involved in hypersensitivity allergic reactions.Stimulates eosinophils to secrete enzymes and protects against worm infections.Main host defense against helminthic infections.
8. Enumerate the most common triggers of the immunological processBacteriaVirusesParasitesFungiNon-pathogens:Food: Many foods can trigger Anaphylaxis:This may occur upon the first Known ingestion.Common triggering foods vary around the world.In westren cultures,ingestion of exposure to peanuts,wheat,nuts,certain types of seafood like shellfish,milk and eggs are the most prevalent causes.
Blood typing mismatchedBlood type postreactionsChemicalsPollensDrugs:- the most common are lactam antibiotics (such as penicillin) followed by aspirin and NSAIDS. Other antibiotics are implicated less frequently and the reactions to NSAIDS are agent specific meaning that if one is allergic to one NSAIDS they can typically tolerate a different one.Other relatively common causes include:ChemotherapyVaccinesProtamineHerbal preparations.Some medications (vancomycin,morphine ,x-ray contrast among others) cause anaphylaxis by triggering mast cell degranulation.StingsBee Venom
9. Explain the clinical presentation of the patientClinical presentations 1. Localized swelling 2. Flushing 3. Sweating 4. Shortness of breath and dyspnea 5. Urticaria and wheezing. T 37.2:- Normal P 120:- Tachycardia R 39:-Tachypnea BP 69/45:- Hypotension.
HistamineHistamine is an organic nitrogen compound involved in local immune responses as well as regulating physiological function in the gut and acting as a neurotransmitter.
Histamine triggers the inflammatory response.PATHOPHYSIOLOGY OF ANAPHYLAXISAllergen crosses an epithelial and/or endothelial barrierAccess to the reactive, sensitized cells mast cells, basophilsRelease of cellular mediators leads to end-organ response in the skin, respiratory tract , cardiovascular system , gastrointestinal tract, nervous system.
HistamineH1 receptorPruritusRhinorrheaTachycardiaBronchospasmH1,H2 receptorsHeadacheFlushingHypotensionH3 receptorLeft ventricular function
Effects of histamine on airways Histamine
Bronchoconstriction by stimulation of H1 receptors on smooth muscles. Mucosal edema from increased microvascular permeability (H1) leading to transudation of fluid and macromolecules through wide intercellular gaps (> 12 nm).Direct stimulation of vagal (cholinergic) nerves can induce airway smooth muscle contractionStimulation of H1 receptors increases mucus secretions, and stimulation of H2 receptors increases mucus viscosity. Effects of histamine on the heartH1 receptors mediate coronary artery vasoconstriction and increased vascular permeability.
H2 receptors mediate atrial and ventricular contractile forces, atrial rate, and coronary artery vasodilation. Decreased diastolic pressure and increased pulse pressure
HistamineH1 receptor on endothelial cellL-arginineNitric oxide
Decreases venous return
10. Discuss the initial treatment algorithm of this medical emergencyAnaphylactic emergencyAnaphylaxisTreatment& Management.
If you are at risk of anaphylaxis, carry auto-injectable epinephrine (adrenaline). This is a single dose of medication that is injected into the thigh during an anaphylactic emergency.
MILD TO MODERATE ALLERGIC REACTION
In some cases, anaphylaxis is preceded by signs of a mild to moderate allergic reaction:
Swelling of face, lips and eyesHives or welts on the skinTingling mouthStomach pain, vomiting (these are signs of a mild to moderate allergic reaction to most allergens, however, in insect allergy these are signs of anaphylaxis).ACTION
For insect allergy, flick out the sting if it can be seen (but do not remove ticks)Stay with person and call for help.Give medications if prescribed(whilst antihistamines may be used to treat mild to moderate allergic reactions, if these progress to anaphylaxis then adrenaline is the only suitable medication)Locateadrenaline autoinjectorif available.Contact parent/guardian or other emergency contact.
ANAPHYLAXIS (SEVERE ALLERGIC REACTION)
Continue to watch for any one of the following signs of anaphylaxis (severe allergic reaction):
Difficult/noisy breathingSwelling of tongueSwelling/tightness in throatDifficulty talking and/or hoarse voiceWheeze or persistent coughPersistent dizziness or collapsePale and floppy (in young children)
ACTIONLay person flat - if breathing is difficult, allow to sit - do not allow them to stand or walk
Give the adrenaline autoinjectorif available (instructions are included in the ASCIA Action Plan for Anaphylaxis, stored with the adrenaline autoinjector)
Further adrenaline doses may be given (when an additional adrenaline autoinjector is available), if there is no response after 5 minutes.If in doubt, give the adrenaline autoinjector.
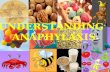
If uncertain whether it is asthma or anaphylaxis, give adrenaline autoinjector FIRST, then asthma reliever.Adrenaline is life saving and must be used promptly. Withholding or delaying the giving of adrenaline can result in deterioration and death. This is why giving the adrenaline autoinjector is the first instruction on the Action Plan for Anaphylaxis. If cardiopulmonary resuscitation (CPR) is given before this step there is a risk that adrenaline is delayed or not given.In the ambulanceoxygen will usually be administered to the patient by paramedics.Medical observationof the patient in hospital for at least 4 hours is recommended after anaphylaxis.An epinephrine autoinjector is a medical device used to deliver a measured dose (or doses) of epinephrine (also known as adrenaline) using autoinjector technology, most frequently for the treatment of anaphylaxis.
Trade names for this device include EpiPen, Emerade, Twinject, Adrenaclick, Anapen, Jext, Allerject, and Auvi-Q. Adrenaline autoinjector
In our case:Mild symptoms such as pruritus and urticaria can be controlled by administration of 0.3 to 0.5 mL of 1:1000 (1 mg/mL) epinephrine SC or IM, with repeated doses as required at 5- to 20-min intervals for a severe reaction.
If the antigenic material was injected into an extremity, the rate of absorption may be reduced by prompt application of a tourniquet proximal to the reaction site administration of 0.2 mL of 1:1000 epinephrine into the site, and removal without compression of an insect stinger, if present.
An IV infusion should be initiated to provide a route for administration of 2.5 mL epinephrine, diluted1:10,000, at 5- to 10-min intervals,11. What adjunct medications can you give to treat?11.Adjunct treatmentEpinephrineis the most effective immediate treatment for anaphylaxis.
It rapidly reverses the uncomfortable flushing anditchingas well as the more serious problems with breathing and dangerous drop in blood pressure that accompanies most anaphylactic reactions.
More importantly, if given in time, epinephrine can reverse the life-threatening symptoms of anaphylactic shock..
If you are allergic to insect stingsor any of the foods that cause anaphylaxis, or if you ever have had an anaphylactic reaction, you should contact your physician about providing an epinephrine injection kit. (Epi-Pen is one common brand name.)
Volume expanders such as normal saline, and vasopressor agents such as dopamine can be given for hypotension.
Replacement of intravascular volume due to postcapillary venular leakage may require several liters of saline.
Epinephrine provides both - and -adrenergic effects, resulting in vasoconstriction, bronchial smooth-muscle relaxation, and attenuation of enhanced venular permeability.
When epinephrine fails to control the anaphylactic reaction, hypoxia due to airway obstruction or related to a cardiac arrhythmia, or both, must be considered.
Oxygen therapy for respiratory distressOxygen alone via a nasal catheter or with nebulized albuterol may be helpful, but either endotracheal intubation or a tracheostomy is mandatory for oxygen delivery if progressive hypoxia develops. Victim of anaphylaxis stops breathing, perform cardiopulmonary resuscitation (CPR) immediately. Continue CPR until the person begins breathing again or emergency medical personnel take over.
If wheezing is caused by asthma,your doctor may recommend some or all of the following to reduce inflammation and open the airways:
A fast-acting bronchodilator inhaler -- albuterol (Proventil HFA, Ventolin HFA), levalbuterol (Xopenex ) -- to dilate constricted airways when you have respiratory symptoms
An inhaled corticosteroid -- mometasone (Asmanex), ciclesonide (Alvesco), beclomethasone (Qvar), flunisolide (Aerospan), fluticasone (Flovent), budesonide (Pulmicort)
A long-acting bronchodilator/corticosteroid combination -- fluticasone/salmeterol (Advair), budesonide/formoterol (Symbicort)
An asthma controller pill to reduce airway inflammation -- zafirlukast (Accolate), montelukast (Singulair)
A non-sedating antihistamine pill -- loratadine (Claritin, Alavert), fexofenadine (Allegra), cetirizine (Zyrtec) or a prescription nasal spray -- fluticasone propionate (Flonase), triamcinolone acetonide (Nasacort AQ), mometasone furoate (Nasonex) -- if you have nasal allergies
Anti- histamineAncillary agents such as the antihistamine diphenhydramine, 50100 mg IM or IV, and aminophylline, 0.250.5 g IV, are appropriate for urticaria-angioedema and bronchospasm, respectively.
SteroidsIntravenous glucocorticoids, 0.51 mg/kg of medrol, are not effective for the acute event but may alleviate later recurrence of bronchospasm, hypotension, or urticaria. Due to their delayed effect, corticosteroids are not first-line treatments.Steroiddrugs(such asprednisoneor methylprednisolone)H2-blocking antihistamines theoretically are attractive agents for dermal and gastrointestinal (GI) manifestations, but evidence supporting their clinical effectiveness is less than that for H1-blocking agents. Some evidence suggests that combining H1and H2blockers may be more effective than H1blockers alone. Glucagon may be useful in treating refractory cardiovascular effects in patients taking beta-blockers.
12. Advice for long term care Advice for long term care:Certain medicines, such as beta-blockers (often given for high blood pressure) and angiotensin-converting enzyme (ACE) inhibitors (often given forheart disease), may hinder the successful treatment of an anaphylactic reaction.So they both should be avoided.Do NOTDo NOT assume that any allergy shots the person has already received will provide complete protection.Do NOT place a pillow under the person's head if he or she is having trouble breathing. This can block the airways.Do NOT give the person anything by mouth if the person is having trouble breathing.
A different form of protection involves the development of blocking antibody of the IgG class, which protects against Hymenoptera venominduced anaphylaxis by interacting with antigen so that less reaches the sensitized tissue mast cells.
Specific interventions to reduce or prevent anaphylaxis recurrences from some triggers (examples include venom immunotherapy for those with anaphylaxis from stinging insects such as bees, yellow jackets, wasps, and hornets, and desensitization for those with anaphylaxis from some medications)