Review article Analysis of the validation of existing behavioral pain and distress scales for use in the procedural setting DIANNE CRELLIN RN BN MN NP RN BN MN NP *‡, THOMAS P. SULLIVAN B. B.Med ed S c i ci †, FRANZ E. BABL MD MPH FRACP FAAP MD MPH FRACP FAAP *†‡, RONAN O’SULLIVAN MD FRCSI FCER MD FRCSI FCER * AND ADRIAN HUTCHINSON RN BN RN BN * *Department of Emergency, Royal Children’s Hospital, †Melbourne University and ‡Murdoch Children’s Research Institute, Melbourne, Victoria, Australia Summary Background: Assessing procedural pain and distress in young children is difficult. A number of behavior-based pain and distress scales exist which can be used in preverbal and early-verbal children, and these are validated in particular settings and to variable degrees. Methods: We identified validated preverbal and early-verbal behavioral pain and distress scales and critically analysed the validation and reliability testing of these scales as well as their use in procedural pain and distress research. We analysed in detail six behavioral pain and distress scales: Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS), Faces Legs Activity Cry Consolability Pain Scale (FLACC), Toddler Preschooler Postoperative Pain Scale (TPPPS), Preverbal Early Verbal Pediatric Pain Scale (PEPPS), the observer Visual Analog Scale (VASobs) and the Observation Scale of Behavioral Distress (OSBD). Results: Despite their use in procedural pain studies none of the behavioral pain scales reviewed had been adequately validated in the procedural setting and validation of the single distress scale was limited. Conclusions: There is a need to validate behavioral pain and distress scales for procedural use in preverbal or early-verbal children. Keywords: pain; validation studies; pain measurement; procedure; child Introduction Children presenting to emergency departments (ED) frequently undergo diagnostic and therapeutic pro- cedures during their admission. Tools to accurately assess the level of pain and distress experienced are essential to improve the management of children undergoing painful procedures in clinical practice and through research. It is widely accepted that assessing pain and distress in preverbal and early- verbal children in particular is inherently difficult. They are developmentally unable to self-report pain Correspondence to: Franz E Babl, Clinical Associate Professor, The University of Melbourne Consultant Emergency Paediatrician, ED, Royal Children’s Hospital, Parkville, Victoria 3052, Australia (email: [email protected]). Pediatric Anesthesia 2007 17: 720–733 doi:10.1111/j.1460-9592.2007.02218.x Ó 2007 The Authors 720 Journal compilation Ó 2007 Blackwell Publishing Ltd

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Review article
Analysis of the validation of existing behavioralpain and distress scales for use in the proceduralsetting
DIANNE CRELLIN R N B N M N N PR N B N M N N P*‡, THOMAS P. SULLIVAN
B .B . MMeded SS c ic i†, FRANZ E. BABL M D M P H F R A C P F A A PM D M P H F R A C P F A A P*†‡,
RONAN O’SULLIVAN M D F R C S I F C E RM D F R C S I F C E R* AND ADRIAN
HUTCHINSON R N B NR N B N*
*Department of Emergency, Royal Children’s Hospital, †Melbourne University and ‡MurdochChildren’s Research Institute, Melbourne, Victoria, Australia
SummaryBackground: Assessing procedural pain and distress in young children
is difficult. A number of behavior-based pain and distress scales exist
which can be used in preverbal and early-verbal children, and these
are validated in particular settings and to variable degrees.
Methods: We identified validated preverbal and early-verbal behavioral
pain and distress scales and critically analysed the validation and
reliability testing of these scales as well as their use in procedural pain
and distress research. We analysed in detail six behavioral pain and
distress scales: Children’s Hospital of Eastern Ontario Pain Scale
(CHEOPS), Faces Legs Activity Cry Consolability Pain Scale (FLACC),
Toddler Preschooler Postoperative Pain Scale (TPPPS), Preverbal Early
Verbal Pediatric Pain Scale (PEPPS), the observer Visual Analog Scale
(VASobs) and the Observation Scale of Behavioral Distress (OSBD).
Results: Despite their use in procedural pain studies none of the
behavioral pain scales reviewed had been adequately validated in the
procedural setting and validation of the single distress scale was limited.
Conclusions: There is a need to validate behavioral pain and distress
scales for procedural use in preverbal or early-verbal children.
Keywords: pain; validation studies; pain measurement; procedure;
child
Introduction
Children presenting to emergency departments (ED)
frequently undergo diagnostic and therapeutic pro-
cedures during their admission. Tools to accurately
assess the level of pain and distress experienced are
essential to improve the management of children
undergoing painful procedures in clinical practice
and through research. It is widely accepted that
assessing pain and distress in preverbal and early-
verbal children in particular is inherently difficult.
They are developmentally unable to self-report pain
Correspondence to: Franz E Babl, Clinical Associate Professor, TheUniversity of Melbourne Consultant Emergency Paediatrician,ED, Royal Children’s Hospital, Parkville, Victoria 3052, Australia(email: [email protected]).
Pediatric Anesthesia 2007 17: 720–733 doi:10.1111/j.1460-9592.2007.02218.x
� 2007 The Authors720 Journal compilation � 2007 Blackwell Publishing Ltd

and distress and assessment is primarily based on
observation of behavior. A number of pain and
distress scales exist which have been used in
preverbal and early-verbal children and these are
validated in particular settings and to variable
degrees.
Recommendations and clinical practice guidelines
detailing the importance of minimizing pain and
distress associated with diagnostic and therapeutic
procedures abound in the emergency literature
(1–4). In line with this focus on procedural pain,
increasing numbers of clinical studies are conducted
in EDs aimed at evaluating the value of interven-
tions designed to minimize the level of pain and
distress experienced during painful procedures
(5–24).
Despite the attention procedural pain has received
in the pain and emergency literature, pain assess-
ment in pre- and early-verbal children is largely
dependent on observational tools developed for use
in nonprocedural settings (e.g., postoperative pain).
The aim of a recent systematic review of observa-
tional behavior measures of pain for children and
adolescents aged 3–18 years by von Baeyer and
Spagrud (25) was to identify scales that could be
recommended for use in clinical trials for a variety of
clinical settings. For ‘medical procedures and brief
painful events’ they recommend Faces Legs Activity
Cry Consolability Pain Scale (FLACC) and Chil-
dren’s Hospital of Eastern Ontario Pain Scale (CHE-
OPS) for pain assessment in children aged 3–
18 years. We set out to determine whether scales
frequently used in clinical trials and those recom-
mended in the literature (e.g., the scales recommen-
ded by von Baeyer and Spagrud) have indeed been
validated for the assessment of procedural pain in
pre- and early-verbal children. Our aim was to make
recommendations about which scales may be used
to measure procedural pain in pre- and early-verbal
children for clinical research in the ED.
A review of the existing literature was conducted
to identify validated preverbal and early-verbal
behavioral pain and distress scales. We selected
scales that had been either validated in the proce-
dural setting as pain or distress tools, or had been
validated in the nonprocedural setting and either
used in published research or could be potentially
used to assess procedural pain and distress in the
preverbal and early-verbal population. A critical
analysis of the validity and reliability testing of these
scales as well as their use in procedural pain and
distress research was then conducted.
Elements of validity and reliability
The clinical and research utility of a pain and
distress scale depends primarily on the adequacy
of its validity and reliability testing (26). An exam-
ination of the validity and reliability of an instru-
ment requires an understanding of the various
components of each and the methods by which they
may be tested.
An instrument is valid if it measures the construct
it intends to measure (27,28). The various aspects of
validity commonly assessed include content, criter-
ion, and construct validity.
Content validity reflects the extent to which the
instrument is representative or inclusive of all
features of the construct. Reviewing the literature
and canvassing experts informs the development of
the instrument, which is usually assessed by expert
opinion to establish content validity (26,28,29). Con-
tent validity is important for the development of an
instrument, but does not provide acceptable evi-
dence of validity beyond the development phase of
the instrument (27).
Criterion validity indicates the extent that a
subject’s performance on the instrument is related
to actual behavior (28). Concurrent validity is a
component of criterion validity (28) and describes
the level of correlation between two instruments
considered to measure the same construct when
applied at the same time. High correlation indicates
a high level of agreement between the two measures
and therefore increased likelihood that they are a
valid measure of the construct (28). In pain mea-
surement, this standard is usually a self-report.
Observer ratings, on a Visual Analog Scale (VAS),
have often been used as a proxy for self-report in
preverbal and early-verbal children (30).
Construct validity provides the strongest evi-
dence for validity (29) and is determined by the
extent to which the measurement reflects the
actual construct (28). Construct validity will exam-
ine whether the tool detects theoretically predict-
able changes in the construct, e.g., whether pain
scores change with administration of analgesia
(26,28). This assessment of validity may also be
BEHAVIORAL PAIN AND DISTRESS SCALES 721
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733

established by comparison with a previously vali-
dated instrument (28,29). Finally, establishing
construct validity requires demonstration of the
capacity of the instrument to discriminate between
the construct and other similar concepts, i.e., a
pain scale should have the capacity to discriminate
between pain and fear. Establishing construct
validity may require several studies using a
number of different approaches.
Reliability is a measure of the consistency of a
tool. There are three major components of reli-
ability – intrarater reliability, interrater reliability
and internal consistency. Intrarater reliability
examines the stability of the instrument across time
(27,28). Interrater reliability is a measure of equiv-
alence and assesses the agreement among users of
the tool (27,28). Internal consistency assesses the
extent that the components of the tool are measuring
the same construct (27,28). Beyer and Wells (26)
suggest that interrater reliability is important when
observation is the method of data collection, and
internal consistency is important when several items
are summed to provide a global score.
The difficulty in establishing the validity and
reliability of a scale means that a single study is
insufficient to establish either validity or reliability
(26). Rather, multiple studies by researchers other
than the original authors of a scale are necessary
before a scale is deemed adequate for either research
or clinical use (26). Further, the assessment of
validity and reliability of a scale should be conduc-
ted prior to using the scale in either of these settings
(26).
Methods
Search strategy and scale selection
A search of the literature was undertaken to identify
published work relevant to the aims of this review,
which were to identify valid behavioral scales for
assessment of procedural pain in pre- and early-
verbal children. An online search using MEDLINE
(1966–December 2006) was conducted for seminal
works detailing scale development and validation
studies using the search terms ‘pain assessment’,
‘infant’ and ‘child’ and ‘pediatrics’.
A second online search was conducted using
MEDLINE (January 1996–December 2006) to identify
the clinical studies evaluating pain management
strategies for painful procedures conducted in the
ED and current clinical practice guidelines devel-
oped for ED pain management. The terms ‘emer-
gency services,’ ‘pain assessment,’ ‘infant,’ ‘child’
and ‘pediatrics’ were used for this search. Finally, a
MEDLINE (January 1966–December 2006) search
was conducted using the name of the selected scales
as the search term.
Searches were supplemented by reviewing the
reference lists of relevant papers identified in the
MEDLINE searches. Websites for relevant profes-
sional bodies, in particular, Initiative on Methods,
Measurements and Pain Assessment in Clinical
Trials (IMMPACT http://www.impact.org) and
the International Association for the Study of Pain
(IASP http://www.iasp-pain.org) were also
reviewed for material that may have contributed to
this review.
Studies were considered relevant if they
addressed validation of a pain and distress scale
for use in pre- or early-verbal children (6 months–
4 years) or use of a pain and distress scale in
procedural pain in children of any age.
Review of the published material sourced identi-
fied a number of scales which had been validated in
previous studies and ⁄ or were used as outcome
measures in clinical trials.
Scales recommended in the emergency literature,
which had not been validated for pre- and early-
verbal children or for procedural use were excluded
unless they had also been used extensively in clinical
trials in the procedural setting. Additionally, scales
that had been designed and validated for neo-
nates and sedated patients were excluded from
consideration.
A number of scales identified in the literature
deemed similar to other scales were excluded. The
Procedure Behavioral Rating Scale (PBRS) (31) has
given rise to several derivatives, i.e., the Procedural
Behavior Checklist (PBC) (32) and the Observation
Scale for Behavioral Distress (OSBD) (33). The
OSBD has been used and validated most exten-
sively in the literature. Therefore, the similar PBRS
and PBC were excluded from the review. The
Modified Behavioral Pain Scale (34) a derivative of
CHEOPS was also rejected as the original scale
appears more frequently in validation studies and
clinical trials.
722 D. CRELLIN ET AL.
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733

Three scales arising from studies attempting to
validate scales for use in the ED were initially
considered but closer scrutiny resulted in their
exclusion. Bulloch and Tenenbein (35) conducted a
study to validate two pain scales for use in the ED.
However, the scales used in this study ‘Colour
Analog Scale’ and a ‘7-point Faces Pain Scale’ are
both self report scales for children aged 5–16 years
of age and focused on acute pain assessment
associated with the presenting complaint, therefore
adding little to the search for a tool to assess
procedural pain in pre- and early-verbal children.
Another recent study conducted in the ED attemp-
ted to validate the Alder Hey Triage Pain Scale in
similar circumstances for children too young to self-
report (36). However, once again this scale was not
validated for procedural use and has not been used
for clinical studies in procedural pain.
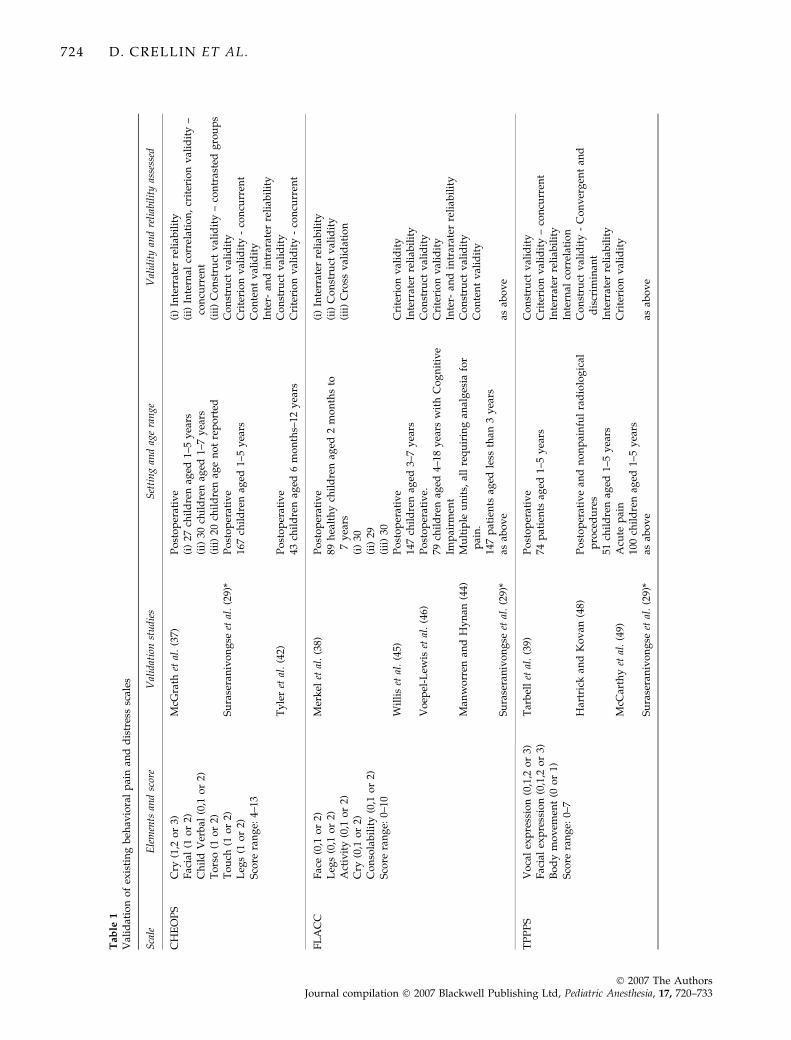
The scales critically analysed (Table 1) were the
Children’s Hospital of Eastern Ontario Pain Scale
(CHEOPS) (37), Faces Legs Activity Cry Consolabi-
lity (FLACC) (38), Toddler Preschooler Postopera-
tive Pain Scale (TPPPS) (39), Preverbal, Early Verbal
Pediatric Pain Scale (PEPPS), Observer Visual Ana-
log Scales (VASobs) (40,41), and the Observation
Scale of Behavioral Distress (OSBD) (33).
Results
Analysis of selected behavioral pain anddistress scales
Children’s Hospital of Eastern Ontario Pain Scale. The
Children’s Hospital of Eastern Ontario Pain Scale
(CHEOPS) is an observational pain scale consisting
of six behavioral components that provide a global
score ranging from four to thirteen (Table 1) (37).
The scale was developed following consultation
with experienced postanesthesia care unit (PACU)
nurses and underwent piloting before further refine-
ment. CHEOPS is scored in time periods, each
consisting of 5 s to observe the child’s behavior
followed by 25 s to record the score.
The initial validation study was conducted by
McGrath et al. (1985) (37) postoperatively and con-
sisted of four components. CHEOPS was shown to
be a reliable scale, with average item correlation
between two nurses ranging from 0.9 to 0.99.
CHEOPS showed good internal correlation, with
good item-to-total-score correlations and moderate
to good item-to-item correlation.
Concurrent validity was demonstrated by com-
paring simultaneous CHEOPS scores, rated by a
researcher, with observer VAS pain scores, rated
independently by two PACU nurses. However, the
scale was a culmination of the behavioral markers
used by PACU nurses to indicate pain, which are
likely to be similar to those used to inform a global
assessment of pain (VASobs) resulting in predictably
high correlation between the two scores. The authors
attempted to demonstrate construct validity by
showing a significant drop in CHEOPS scores
following analgesia administration. However, the
nurse applying CHEOPS was the treating nurse and
so not blinded to the analgesia, which weakens
support for the establishment of construct validity.
McGrath and colleagues also undertook ‘social
validation,’ a method of validity testing the authors
acknowledge as unproven in pain assessment.
Eighty-eight teachers viewed 14 five-second seg-
ments of footage of children in PACU, and then
independently rated the child’s pain using a VAS.
The teacher scores correlated well with CHEOPS.
However, this method is unproven and cannot be
considered a determinant of validity.
The postoperative setting was used in a second
study aimed at validating CHEOPS for pain assess-
ment (42). CHEOPS and the Objective Pain Scale
(OPS) were applied to the youngest age group
(6 months to 3 years) and compared with establish
concurrent validity. The Faces Scale was added for
older children (3–6.5 years) and CHEOPS, the Faces
Scale and self report VAS were used for comparison
in the oldest age group (6.5–12 years). Pearson’s
correlation demonstrated high levels of correlation
between the various scales (r = 0.743–0.921).
Construct validity was established by analysing
the trend in pain scores collected prior to surgery,
before and after analgesia postoperatively and
scores collected once oral analgesia was commenced.
Significant trends existed for all scales.
The authors’ of this methodologically sound study
conclude that all scales can be considered valid for
postoperative pain assessment in children aged
6 months to 12 years.
In a more recent effort, Suraseranivongse et al. (29)
conducted a cross validation study to evaluate
CHEOPS, FLACC, TPPS, and OPS in 167 children
BEHAVIORAL PAIN AND DISTRESS SCALES 723
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733
Tab
le1
Val
idat
ion
of
exis
tin
gb
ehav
iora
lp
ain
and
dis
tres
ssc
ales
Sca
leE
lem
ents
and
scor
eV
alid
atio
nst
udi
esS
etti
ng
and
age
ran
geV
alid
ity
and
reli
abil
ity
asse
ssed
CH
EO
PS
Cry
(1,2
or
3)F
acia
l(1
or
2)C
hil
dV
erb
al(0
,1o
r2)
To
rso
(1o
r2)
To
uch
(1o
r2)
Leg
s(1
or
2)S
core
ran
ge:
4–13
McG
rath
etal
.(3
7)P
ost
op
erat
ive
(i)
27ch
ild
ren
aged
1–5
yea
rs(i
i)30
chil
dre
nag
ed1–
7y
ears
(iii
)20
chil
dre
nag
en
ot
rep
ort
ed
(i)
Inte
rrat
erre
liab
ilit
y(i
i)In
tern
alco
rrel
atio
n,
crit
erio
nv
alid
ity
–co
ncu
rren
t(i
ii)
Co
nst
ruct
val
idit
y–
con
tras
ted
gro
up
sS
ura
sera
niv
on
gse
etal
.(2
9)*
Po
sto
per
ativ
e16
7ch
ild
ren
aged
1–5
yea
rsC
on
stru
ctv
alid
ity
Cri
teri
on
val
idit
y-
con
curr
ent
Co
nte
nt
val
idit
yIn
ter-
and
intr
arat
erre
liab
ilit
yT
yle
ret
al.
(42)
Po
sto
per
ativ
e43
chil
dre
nag
ed6
mo
nth
s–12
yea
rsC
on
stru
ctv
alid
ity
Cri
teri
on
val
idit
y-
con
curr
ent
FL
AC
CF
ace
(0,1
or
2)L
egs
(0,1
or
2)A
ctiv
ity
(0,1
or
2)C
ry(0
,1o
r2)
Co
nso
lab
ilit
y(0
,1o
r2)
Sco
rera
ng
e:0–
10
Mer
kel
etal
.(3
8)P
ost
op
erat
ive
89h
ealt
hy
chil
dre
nag
ed2
mo
nth
sto
7y
ears
(i)
30(i
i)29
(iii
)30
(i)
Inte
rrat
erre
liab
ilit
y(i
i)C
on
stru
ctv
alid
ity
(iii
)C
ross
val
idat
ion
Wil
lis
etal
.(4
5)P
ost
op
erat
ive
147
chil
dre
nag
ed3–
7y
ears
Cri
teri
on
val
idit
yIn
terr
ater
reli
abil
ity
Vo
epel
-Lew
iset
al.
(46)
Po
sto
per
ativ
e.79
chil
dre
nag
ed4–
18y
ears
wit
hC
og
nit
ive
Imp
airm
ent
Co
nst
ruct
val
idit
yC
rite
rio
nv
alid
ity
Inte
r-an
din
trar
ater
reli
abil
ity
Man
wo
rren
and
Hy
nan
(44)
Mu
ltip
leu
nit
s,al
lre
qu
irin
gan
alg
esia
for
pai
n.
147
pat
ien
tsag
edle
ssth
an3
yea
rs
Co
nst
ruct
val
idit
yC
on
ten
tv
alid
ity
Su
rase
ran
ivo
ng
seet
al.
(29)
*as
abo
ve
asab
ov
e
TP
PP
SV
oca
lex
pre
ssio
n(0
,1,2
or
3)F
acia
lex
pre
ssio
n(0
,1,2
or
3)B
od
ym
ov
emen
t(0
or
1)S
core
ran
ge:
0–7
Tar
bel
let
al.
(39)
Po
sto
per
ativ
e74
pat
ien
tsag
ed1–
5y
ears
Co
nst
ruct
val
idit
yC
rite
rio
nv
alid
ity
–co
ncu
rren
tIn
terr
ater
reli
abil
ity
Inte
rnal
corr
elat
ion
Har
tric
kan
dK
ov
an(4
8)P
ost
op
erat
ive
and
no
np
ain
ful
rad
iolo
gic
alp
roce
du
res
51ch
ild
ren
aged
1–5
yea
rs
Co
nst
ruct
val
idit
y-
Co
nv
erg
ent
and
dis
crim
inan
tIn
terr
ater
reli
abil
ity
McC
arth
yet
al.
(49)
Acu
tep
ain
100
chil
dre
nag
ed1–
5y
ears
Cri
teri
on
val
idit
y
Su
rase
ran
ivo
ng
seet
al.
(29)
*as
abo
ve
asab
ov
e
724 D. CRELLIN ET AL.
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733
Ta
ble
1(C
onti
nu
ed)
Sca
leE
lem
ents
and
scor
eV
alid
atio
nst
udi
esS
etti
ng
and
age
ran
geV
alid
ity
and
reli
abil
ity
asse
ssed
PE
PP
SH
eart
Rat
e(0
,1,2
,3
or
4)F
acia
l(0
,1,2
,3
or
4)C
ry(0
,1,2
,3
or
4)C
on
sola
bil
ity
(0,1
,2,
3o
r4)
Bo
dy
po
stu
re(0
,1,2
,3
or
4)S
oci
abil
ity
(0,1
,2,
3o
r4)
Su
ckin
g⁄f
eed
ing
(0,1
,2,
3o
r4)
Sco
rera
ng
e:0–
28
Sch
ult
zet
al.
(15)
Po
sto
per
ativ
e40
chil
dre
n,
aged
12–2
4m
on
ths.
Co
nst
ruct
val
idit
yIn
terr
ater
reli
abil
ity
Intr
arat
erre
liab
ilit
yIn
tern
alco
nsi
sten
cy
VA
S(o
bs)
100
mm
ho
rizo
nta
lli
ne
–m
ark
edat
each
end
wit
h‘n
op
ain
’an
d‘m
ost
pai
n’.
Ob
serv
erm
ark
so
nth
eli
ne
the
lev
elo
fp
erce
ived
pai
nex
per
ien
ced
by
the
chil
d
Sin
ger
etal
.(5
9)P
roce
du
ral
pai
n1,
171
adu
ltp
roce
du
res
Sin
ger
etal
.(4
1)A
cute
pai
nan
dp
roce
du
ral
pai
n63
chil
dre
nag
ed4–
7y
ears
Co
nst
ruct
val
idit
y–
Co
nv
erg
ent
Cri
teri
on
val
idit
yK
elly
etal
.(4
0)A
cute
pai
n78
chil
dre
nag
ed8–
15y
ears
OS
BD
Sco
red
for
pre
sen
ce(0
for
abse
nce
).B
rack
etin
dic
ates
wei
gh
tin
gIn
form
atio
nse
ekin
g(1
.5)
Cry
(1.5
)S
crea
m(4
.0)
Ph
ysi
cal
rest
rain
t(4
.0)
Ver
bal
resi
stan
ce(2
.5)
See
ks
emo
tio
nal
sup
po
rt(2
.0)
Ver
bal
pai
n(2
.5)
Fla
il(4
.0)
Ver
bal
fear
(2.5
)**
Mu
scu
lar
rig
idit
y(2
.5)*
*N
erv
ou
sb
ehav
ior
(1.0
)**
Sco
rera
ng
e:0–
28
Jay
etal
.(3
3)P
roce
du
ral
(BM
A)
42ca
nce
rp
atie
nts
aged
2–20
yea
rsC
rite
rio
nv
alid
ity
Inte
rrat
erre
liab
ilit
y
Ell
iott
etal
.(6
5)P
roce
du
ral
(BM
A)
55ch
ild
ren
aged
3–13
yea
rsC
on
ver
gen
tv
alid
ity
Inte
rrat
erre
liab
ilit
y
CH
EO
PS
,C
hil
dre
n’s
Ho
spit
alo
fE
aste
rnO
nta
rio
Pai
nS
cale
;F
LA
CC
,F
aces
Leg
sA
ctiv
ity
Cry
Co
nso
lab
ilit
yP
ain
Sca
le;
TP
PP
S,
To
dd
ler
Pre
sch
oo
ler
Po
sto
per
ativ
eP
ain
Sca
le;
PE
PP
S,
Pre
ver
bal
,E
arly
Ver
bal
Ped
iatr
icP
ain
Sca
le;
VA
So
bs,
Vis
ual
An
alo
gS
cale
(ob
serv
er);
OS
BD
,O
bse
rvat
ion
Sca
leo
fB
ehav
iora
lD
istr
ess;
BM
A,
Bo
ne
mar
row
asp
irat
e.*N
ote
:A
cro
ssv
alid
atio
nst
ud
yex
amin
ing
CH
EO
PS
,F
LA
CC
,T
PP
PS
and
Ob
ject
ive
Pai
nsc
ale
(OP
S).
BEHAVIORAL PAIN AND DISTRESS SCALES 725
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733

aged 1–5 years. Children were video taped prior to
surgery and following surgery before analgesia was
given. Four observers viewed the video segments
and pain scores were recorded using each of the four
scales.
Comparison of presurgery scores with those
obtained afterwards, when children may reason-
ably expect to be experiencing pain, demonstrated
that all scales had the capacity to discriminate
(P = 0.001) between varying levels of pain. Con-
current validity was established by comparing the
scores achieved with the scales with each other
and moderate to good correlation was found
(r = 0.62–0.77). The highest level of agreement
between scales and the clinical decision to treat
pain was achieved with CHEOPS. Inter- and
intrarater reliability was also tested and found to
be high for all scales.
The authors recommend CHEOPS for pain assess-
ment in the immediate postoperative phase for
children aged 1–5 years. This decision appeared to
be based on the high level of agreement with the
clinical decision to treat as little else discriminated
the validity of the scales from one another.
In a clinical trial (20) evaluating the analgesic
effectiveness of topical local anaesthetic and nitrous
oxide (N2O) or use of the combination for venous
cannulation, the results showed that CHEOPS scores
may be moderated by the use of N2O. CHEOPS
scores measured before and during cannulation were
significantly increased during cannulation for those
treated with N2O but to a significantly lesser extent
than those treated with topical local anesthetic.
However, the self-reported pain scores for both
treatment groups were not significantly different.
These results introduce doubt about the ability of
CHEOPS to adequately reflect the pain experience.
Furthermore, Beyer et al. (43) found that CHEOPS
scores were generally low after discharge from
PACU and at that over time correlated increasingly
poorly with self-reports of pain. Thus, CHEOPS may
be valid only for the immediate postsurgery period.
Willis et al. (45) suggest CHEOPS as the gold
standard preverbal pain tool for comparative pur-
poses. However, as a consequence of the tight
observational and recording intervals and many
types of behavior to evaluate it is burdensome to
apply. Tarbell et al. (39) also note that the strong
correlation between CHEOPS and observer VAS
measures of pain may mean it is more practical to
use a VAS.
A number of studies have provided varying levels
of support for the validity of CHEOPS for the
assessment of pain in postoperative children. How-
ever, CHEOPS has not been validated in the acute
procedural setting, although a number of clinical
trials, including many conducted in the ED have
used CHEOPS to assess procedural pain (20–24).
Von Baeyer and Spagrud (25) report ‘excellent’
evidence of validity and recommend this scale’s
use in medical procedures. However, it is unclear
how validity for the use of CHEOPS to assess pain
during medical procedures was established.
Face Legs Activity Cry Consolability Pain Scale. The
Faces Legs Activity Cry Consolability (FLACC) Pain
Scale is an observational pain scale consisting of five
behavioral components that provide a global pain
score ranging from 0 to 10 (Table 1) (38,44–46).
FLACC was designed for use after a period of up to
5 min of observation. The authors suggest observing
the child with their legs uncovered, testing tone and
tenseness, and initiating consoling of the child when
applying FLACC (47).
The initial validation study of FLACC by Merkel
and colleagues (38), included 89 children aged
2 months to 7 years, was conducted postoperatively
and consisted of three parts.
Interrater reliability was reported as good, and
was assessed by correlating FLACC scores of two
nurses, who simultaneously and independently
applied FLACC to 30 children.
Construct validity was assessed by applying
FLACC to 29 children before and after analgesia
administration, and showed a significant decrease in
FLACC score following analgesia. However, the
treating nurse also applied FLACC and so was not
blinded to analgesia administered.
In part three, 30 children were simultaneously
rated by two independent nurses, one using a pain
scale identified by the authors as previously valid-
ated and the other using FLACC. The two scales
demonstrated good correlation and thus concurrent
validity.
The study supported the preliminary validity and
reliability of FLACC, although the sample size was
small and all children were English speaking with-
out cognitive impairment.
726 D. CRELLIN ET AL.
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733

Willis et al. (45) conducted a further validation
study on 30 children aged 3–7 years, at least 18 and a
mean of 20 h after surgery. The same nurse scored
all 30 children after a period of observation. These
scores were compared with the child’s report of pain
using a Faces pain scale. To establish reliability, a
second nurse independently applied FLACC to 6 of
the 30 children.
Overall, FLACC and the Faces self-report scale
showed good agreement – supporting concurrent
validity – and interrater reliability was 100%. How-
ever, there was no agreement between the self-report
and FLACC scores of children younger than 5 years
of age, which suggests that either the younger
children failed to comprehend the Faces Scale or
that FLACC is not valid in this population.
The study was undertaken on a small sample size,
limited to English speaking children without cogni-
tive impairment, and did not assess any other form
of validity.
Voepel-Lewis et al. (46) examined the validity and
reliability of FLACC for postoperative use in chil-
dren with cognitive impairment. They enrolled 79
children, aged 4–18 years, undergoing general or
orthopedic surgery. Postsurgery but prior to anal-
gesia administration, each child was filmed for later
review. The treating nurse and a parent simulta-
neously rated the child’s pain using FLACC and a
VAS respectively. Those children who received
analgesia in PACU were filmed and scored a second
time. Two nurses, blinded to analgesia, independ-
ently viewed the videos in random order and
applied FLACC. Fifty were viewed for a second
time 2 months later to establish intrarater reliability.
The study found by deos FLACC had good inter-
and intrarater reliability, demonstrated construct
validity with a decrease in FLACC following anal-
gesia and at concurrent validity was supported by a
strong correlation between FLACC and parent VAS
scores.
All children were tested for the ability to self-
report, and although 16 children were deemed
capable of providing a self-report of pain, only eight
did. Thus, FLACC scores were unable to be reliably
compared with self-report.
Manworren and Hynan (44) tested FLACC in a
variety of settings, including PACU; the pediatric
intensive care unit; surgery ⁄ trauma unit; hemato-
logy ⁄ oncology unit; and the infant unit. One hundred
and forty-seven children aged less than 3 years who
had analgesia ordered on an ‘as required’ basis were
included in the study. A pilot study was conducted,
and 25 volunteer nurses assessed ten video segments
to establish interrater reliability. Nineteen nurses
showed sufficient reliability; fourteen collected data.
Children deemed to be in pain by their treating
nurse were then rated, at the bedside, by one of the
research nurses before and after analgesic adminis-
tration. Construct validity was demonstrated by a
fall in FLACC score after analgesic administration.
The nurses were not blinded to the analgesia. This
study lends preliminary support to the use of
FLACC in a variety of nonprocedural settings.
FLACC has not been validated in the acute
procedural setting, however like CHEOPS, FLACC
appears in the literature as the outcome measure in
clinical trials examining interventions to minimise
procedural pain in young children (18,19). Further-
more, it is also recommended by von Baeyer and
Spagrud (25) for use in pain associated with ‘proce-
dures and other brief painful events.’ Once again the
basis on which they established the validity of this
scale in this setting is unclear.
Toddler Preschooler Postoperative Pain Scale. The
Toddler Preschooler Postoperative Pain Scale
(TPPPS) is an observational pain scale consisting of
three categories that provide a global score ranging
from zero to seven (Table 1) (39). The scale compo-
nents were derived from preliminary studies and
observed pain behavior in other studies (39).
The initial validation of TPPPS was conducted by
Tarbell et al. (39) on 74 children, aged 1–5 years,
emerging from anesthesia following surgical repair
of a hernia or a hydrocoele. Children were
observed for six 5 min intervals following arousal
from anesthesia and the treating nurse rated the
child’s pain using TPPPS. A second independent
nurse observed 28 of the children to assess reliab-
ility and interrater reliability was reported as good
across both the scale as a whole and its individual
items.
The authors assessed internal consistency by
comparing the six interval scores for each patient,
and by aggregating the six scores and comparing the
total between patients. High item-to-total-score cor-
relations were observed in both the individual and
aggregated TPPPS scores, however, the correlation
BEHAVIORAL PAIN AND DISTRESS SCALES 727
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733
between the individual items varied from poor to
good. This may reflect the different degrees of ‘pain’
that the various items are measuring.
Construct validity was demonstrated by a signi-
ficant fall in TPPPS scores following postoperative
analgesia, observed in the 25 children who received
further analgesia.
The study demonstrates preliminary validity and
reliability of TPPPS, but has a number of weaknes-
ses. The population consisted of predominately
Caucasian boys and the nurses were not blinded to
analgesic administration.
The authors note that although TPPPS was found
to be sensitive to analgesic regimens, they are
uncertain whether this sensitivity was because of
decreased pain experienced by the child or as a
consequence of the sedative action of some analge-
sics.
Hartrick and Kovan (48) conducted a further
validation study on 51 children aged 1–5 years.
The study was conducted in three parts and two
nurses observed each patient simultaneously and
independently at 5 min intervals.
In part one, twenty patients were observed in
PACU following ear, nose and throat (ENT) surgery
until discharge to the ward. Part one demonstrated
good interrater reliability and construct validity,
with a significant fall in TPPPS score following
analgesia administration.
Part two compared the scores obtained in part one
with the scores from two other groups: eight
children who had undergone urological surgery
and were treated for pain with caudal anesthesia;
and 11 patients emerging from anesthesia following
nonpainful radiological procedures. No statistical
difference in pain scores between the radiological
and urological groups was observed. However,
patients undergoing ENT surgery had significantly
higher TPPPS scores than the radiological group,
demonstrating discriminate validity.
Part three was a cross-validation study of TPPPS,
FLACC and a third pain scale, undertaken on 12
children emerging from anesthesia. Both of the
observing nurses applied all three scales at each
observation interval. All three scales showed a
response to analgesia, although the authors con-
clude that TPPPS may be better than FLACC for
discriminating between painful and nonpainful
situations.
The study provides further support for the valid-
ity of TPPPS, however, a small sample size and lack
of blinding limit the ability to generalize the study’s
findings. The authors also query whether TPPPS is a
measure of pain or generalized distress.
McCarthy et al. (49) conducted an exploratory
study using a modified version of TPPPS to assess
the pain of 100 children, aged 1–5 years, presenting
to the ED. This study was not an attempt to examine
its use for procedural pain. The child’s pain was
assessed by a researcher using the modified TPPPS
and by parents and nursing staff using a VAS.
TPPPS scores correlated significantly with both the
nurse and parent VAS scores, and the authors
conclude that TPPPS may be appropriate to assess
pain in the ED, but that more research is required.
This is one of only two attempts to validate a pain
assessment tool for use in the ED.
Despite one attempt to validate TPPPS in the ED,
there have been no further attempts to validate the
scale in this setting and no attempts to validate it for
the acute procedural setting. However, TPPPS has
been used in clinical research as an outcome meas-
ure in nonprocedural settings in several trials
(16,17).
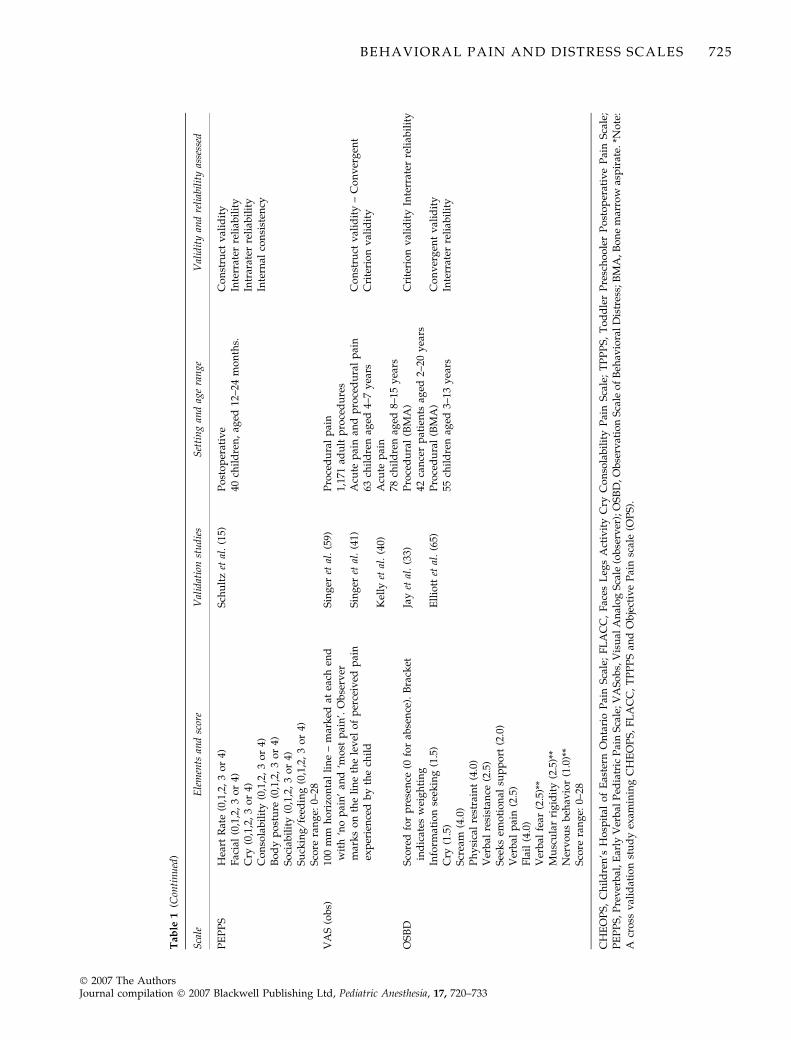
Preverbal, Early Verbal Pediatric Pain Scale. The Pre-
verbal, Early Verbal Pediatric Pain Scale (PEPPS) is
an observational pain scale consisting of seven
behavioral categories that provide a global score
ranging from 0 to 26 (Table 1) (15). PEPPS was
developed in consultation with experienced pediat-
ric nurses following a review of the literature and
observation of children’s pain behavior (15).
The preliminary validity of PEPPS was assessed
by Schultz et al. (15). Forty children, aged 12 months
to 24 months, were filmed postoperatively following
abdominal or urological surgery. The footage was
then split into 3 min segments and two to four
segments of footage from each child were collated,
totalling 120 segments. These segments of footage
were randomly ordered and then presented inde-
pendently to four pediatric research nurses, all
blinded to analgesia administration, who applied
PEPPS.
Interrater and intrarater reliability were reported
as very good, while item-to-item correlations varied
from poor to good, and item-to-total score correla-
tions from moderate to good. However, the authors
728 D. CRELLIN ET AL.
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733

suggest that eliminating those items with poorer
item-to-total score correlations would only slightly
improve internal consistency. Construct validity was
demonstrated by significant differences in pre- and
postanalgesia PEPPS scores.
The main limitations of the study are the small
sample size, male dominated population (35 patients
were boys) and limited age-range.
The Preverbal, Early Verbal Pediatric Pain Scale
has not been validated in the acute procedural
setting. However, PEPPS has been used as an
outcome measure in procedural pain research con-
ducted in the ED (15).
Observer Visual Analog Scale. Visual Analog Scales
(VAS) have been validated and repeatedly used to
quantify self reports of pain intensity in adults and
children as young as five years (50–52). Younger
children (4 years) have been shown to be capable of
reliably self-reporting pain using modified self
report scales, which often use a series of faces or
other visual representations of pain intensity (33,53–
58). However, for pre- and early-verbal children,
unable to self report, observer VAS (VASobs)
appears in the literature as a proxy for self-report
(5,11–14).
Several attempts to validate the use of VASobs for
pain assessment have been made. Singer et al. (59)
conducted a study comparing patient self report
using a 100 mm VAS with independent reports
provided by clinicians using the same tool for adults
undergoing painful procedures in the ED. Patient
and clinician scores for 1171 procedures performed
during the study period were evaluated. The mean
VAS for patients was 20.8 mm (95% CI: 19.4–
22.2 mm) and for clinicians 23.5 mm (95% CI:
22.3–24.6 mm). However, the trend for higher scores
for clinicians was not consistent across different
types of procedures and the correlation (Pearson’s
correlation coefficient) between patient and clinician
VASobs varied from r = 0.26–0.68.
Singer et al. in a more recent study focused on
children aged 4–7 years presenting to the ED with
acute pain or when undergoing a painful procedure
and compared self- report of pain with the ratings
provided by clinicians and their parent (41). The
children in this study used the Smiley Analog Scale,
which was validated for use in a study by Pothman
(60). The self-report scores of 57 children were
compared with the scores recorded independently
by their parent and a clinician using a 100 mm VAS.
The correlation between the child’s and their par-
ent’s scores was 0.47 (P < 0.001) and the correlation
between the child’s and the clinician’s scores was
0.08 (P = 0.54).
In a similar Study these results were reproduced
for children presenting to the ED when the child’s
self-report is compared with the parents rating of the
child’s pain (40). Children aged 5–16 years requiring
treatment for painful conditions and their parents
independently rated their pain using the 100 mm
VAS on 4 occasions during their admission to the
ED. A total of 78 children and their parents were
enrolled in the study and provided 289 score sets.
Correlation between the child and parent scores was
0.63 (95% CI: 0.56–0.70).
A study exploring the pain associated with naso-
gastric tube insertion enrolled a total of 36 children
aged 2–18 years (61). Self-report pain scores, parent
and nurse VASobs were provided for 29 participants
and show similar trends to previous studies reveal-
ing that parents and clinicians regularly under-
report the pain experience of children. However,
formal validity testing was not undertaken in this
study.
A range of studies demonstrate similar discord-
ance between self-report and observer reports of
pain in other clinical settings, such as in postoper-
ative pain (62–64). These studies indicate that con-
current validity cannot be established for VASobs as
clinicians are poor judges of a child’s pain and their
parents are only slightly better. However, the scale is
frequently used in studies attempting to validate a
newly developed pain assessment tool (30,34,37,39).
Researchers would argue where strong correlation
exists between scores that this indirectly supports
the concurrent validity of the VASobs. However,
with poor correlation between self-report (gold
standard) and observer reports of pain the validity
of this approach is weak. Furthermore, VASobs is
used repeatedly in clinical trials evaluating the
efficacy of interventions aimed at reducing pain
associated with medical procedures, including stud-
ies conducted in the ED (5,11–14).
Observation Scale of Behavioral Distress. The Observa-
tion Scale of Behavioral Distress (OSBD) is a revised
version of the Procedural Behavior Rating Scale (31)
BEHAVIORAL PAIN AND DISTRESS SCALES 729
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733
and consists of 11 types of behavior indicative of
anxiety or distress in children (Table 1) (33). The
OSBD is scored in 15s intervals, with five seconds to
observe the child followed by 10 s to record the
OSBD score. The total score for a period of time is
then averaged. In addition, each indicator is weigh-
ted from one to four according to its intensity,
providing a global score from 0 to 28 (33).
The initial validation of OSBD was conducted by
Jay et al. (33) on 42 cancer patients aged 2–20 years
undergoing bone marrow aspiration (BMA).
Prior to each procedure the parents of all
children and children aged 8 years and older were
asked to complete a number of questionnaires and
measurements, identified by the authors as valid,
to assess child and parent anxiety levels and
coping skills. Included in these questionnaires and
measurements was a ‘Pain thermometer,’ used by
the child prior to the procedure to rate their
anticipated pain, and after the procedure to rate
their experienced pain.
Each procedure was observed by one of the two
researchers who applied the OSBD every 15 s. For
the purpose of analysis, the procedure was divided
into four separate phases.
Seven of the procedures were reviewed by both
researchers to assess interrater reliability. Inter- and
intrarater reliability were reported as good across all
time points and in total.
Validity was assessed by correlating the various
questionnaires and pain thermometer ratings with
OSBD scores. The total OSBD scores correlated
significantly with child’s Trait Anxiety scores and
anticipated and experienced pain ratings. Good
correlation was also seen between the parent’s
ratings of their child’s anxiety, obtained prior to
the procedure, and procedural distress measured
using OSBD.
A number of other measures used showed no
correlation with OSBD. Further, children were asked
to rate their pain but not ‘distress’ or ‘anxiety.’
However, the conceptual difficulty in defining ‘dis-
tress’ or ‘anxiety’ to younger children may make use
of this scale burdensome.
In light of the different developmental levels of the
participants, with a small sample spread over a wide
age range, interpretation of the results may be difficult.
The authors report that children younger than 7 years
of age experience five times the level of distress that
children older than 7 years do. However, it is possible
that older children fail to show the behavioral cues
present in the OSBD, and so record lower distress
levels.
The same group of authors that developed OSBD
conducted a subsequent validation study in 55
children, aged 3–13 years, undergoing BMA (65).
Each procedure was observed by one of the two
researchers trained in the use of the OSBD. To
establish interrater reliability and assess agreement
between the raters, both of which were reported as
good, both researchers observed 11 of the procedures.
The authors assessed two versions of the OSBD.
The ‘original OSBD’ is the OSBD scored in 15 s
intervals with weighted indicators, as explained
above. The ‘recalculated OSBD’ is the OSBD scored
once in each phase, without item weighting, such
that the scale provides a global score ranging from
zero to 11.
Validity was assessed by correlating a range of
variables with both OSBD scores. The variables
measured included heart rate and blood pressure,
taken immediately before and after the procedure;
self-reports of anticipated and experienced pain,
using a Pain Thermometer; and nurse ratings of
child distress on a 5-point Likert Scale.
The authors cite nine of the twelve variables
measured as showing ‘significant correlations’ with
OSBD, thus providing evidence of validity. All
these variables have low P values, which indicate
that the statistics obtained are likely to be a true
reflection of the population studied. However, only
two of these nine variables (nurse ratings of distress
and child heart rate during the procedure) show
moderate to strong correlation with OSBD. Only
these two measures, which show statistically signi-
ficant results and good correlation with OSBD,
provide evidence for the validity of OSBD. The
remaining variables show poor or no correlation
with OSBD.
The authors also found that the original and
recalculated OSBD scales are ‘valid’ and have
similar reliability. They conducted further analysis
on the scale, eliminating three items, reducing the
scale to revised eight item distress scale. This revised
scale, the OSBD-R, appears widely in clinical trials
focusing on interventions aimed at reducing proce-
dural pain in children (6–10), despite the limitations
of the validity testing.
730 D. CRELLIN ET AL.
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733

Discussion
We analysed six major behavioral pain and dis-
tress scales with a particular focus on their
validation and reliability. The intent was to iden-
tify a scale addressing procedural pain which is
suitable for use in clinical practice and research in
the ED. Observer VAS is used frequently in
clinical research evaluating the efficacy of inter-
ventions aimed at alleviating pain even though it
has repeatedly been shown to be an inadequate
measure of pain. It is a practical tool to use,
however, its continued use in clinical research
should be discouraged as it does not correlate well
with self-reported pain. Although TPPPS and
PEPPS demonstrate greater levels of validity than
observer VAS in nonprocedural settings, these
scales have not been validated for use in proce-
dural pain. Despite their use in clinical trials, we
cannot recommend their use for this purpose in
pre- and early-verbal children undergoing painful
procedures.
The OSBD has been subject to limited validation
in procedural pain and distress using children aged
3–18 years suffering with cancer. These children are
older than those for which we are seeking a valid
scale and may be expected to have experienced
multiple procedures. This further limits the capacity
for assuming validity in otherwise well pre- and
early-verbal children experiencing acute procedural
pain. Additional testing is warranted if we are to
recommend this scale for use in clinical trials in
procedural pain. Furthermore, as noted by von
Baeyer and Spagrud (25) this scale attempts to
assess distress and anxiety associated with medical
procedures. Scales focusing more specifically on
pain behavior may be more appropriate tools for
clinical trials evaluating the efficacy of pain man-
agement. Finally, this scale relies heavily on verbal
markers, which will be absent in preverbal children.
Two of the scales reviewed (CHEOPS and
FLACC) have been validated for use in settings
such as postoperative pain. Additionally, they have
been used extensively in clinical trials examining
procedural pain and von Baeyer and Spagrud (25) in
their recent systematic review recommend both as
valid measures of pain in the procedural setting.
While showing potential for this purpose, CHEOPS
and FLACC have not been validated for use in
pre- and early-verbal children undergoing painful
procedures. However, until additional validation
studies are conducted we suggest their continued
use in clinical trials. A more important recommen-
dation to arise from this review is the need for
validation studies for behavioral pain and distress
tools for pre- and early-verbal children undergoing
painful procedures.
Acknowledgment
We acknowledge grant support from the Victor
Smorgon Charitable Fund, Melbourne, Australia.
References1 American Academy of Pediatrics Committee on Psychosocial
Aspects of Child Family Health and American Pain SocietyTask Force on Pain in Infants Children Adolescents. Theassessment and management of acute pain in infants, children,and adolescents. Pediatrics 2001; 108: 793–797.
2 Kelly AM. A process approach to improving pain manage-ment in the emergency department: development andevaluation. [see comment]. J Accident Emerg Med 2000; 17:185–187.
3 Royal Australasian College of Physicians, Paediatric and ChildHealth Division. Guideline Statement: Management of Procedure-related Pain in Children and Adolescents. Sydney: Royal Austra-lasian College of Physicians, 2005.
4 Zempsky WT, Cravero JP. Relief of pain and anxiety in pedi-atric patients in emergency medical systems. Pediatrics 2004;114: 1348–1356.
5 Green DA, Linares MYR, Garcia Pena BM et al. Randomizedcomparison of pain perception during radial head subluxationreduction using supination-flexion or forced pronation. PediatrEmerg Care 2006; 22: 235–238.
6 Kleiber C, Craft-Rosenberg M, Harper DC. Parents as dis-traction coaches during I.V. insertion: a randomized study. JPain Symptom Manage 2001; 22: 851–861.
7 Kanagasundaram SA, Lane LJ, Cavalletto BP et al. Efficacy andsafety of nitrous oxide in alleviating pain and anxiety duringpainful procedures. Arch Dis Childhood 2001; 84: 492–495.
8 Luhmann JD, Kennedy RM, Porter FL et al. A randomizedclinical trial of continuous-flow nitrous oxide and midazolamfor sedation of young children during laceration repair. AnnEmerg Med 2001; 37: 20–27.
9 Stevenson MD, Bivins CM, O’Brien K et al. Child lifeintervention during angiocatheter insertion in the PediatricEmergency Department. Pediatr Emerg Care 2005; 21: 712–718.
10 Tobias JD. Weak analgesics and nonsteroidal anti-inflamma-tory agents in the management of children with acute pain.Pediatr Clinics North America 2000; 47: 527–543.
11 Lewindon PJ, Harkness L, Lewindon N. Randomised con-trolled trial of sucrose by mouth for the relief of infant cryingafter immunisation. Arch Dis Childhood 1998; 78: 453–456.
12 Lindh V, Wiklund U, Blomquist HK et al. EMLA cream andoral glucose for immunization pain in 3-month-old infants.Pain 2003; 104: 381–388.
BEHAVIORAL PAIN AND DISTRESS SCALES 731
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733
13 Schultz AA, Strout TD, Jordan P et al. Safety, tolerability, andefficacy of iontophoresis with lidocaine for dermal anesthesiain ED pediatric patients. J Emerg Nurs 2002; 28: 289–296.
14 McErlean M, Bartfield JM, Karunakar TA et al. Midazolamsyrup as a premedication to reduce the discomfort associatedwith pediatric intravenous catheter insertion. J Pediatr 2003;142: 429–430.
15 Schultz AA, Murphy E, Morton J et al. Preverbal, Early VerbalPediatric Pain Scale (PEPPS): development and early psycho-metric testing. J Pediatr Nurs 1999; 14: 19–27.
16 Memi D, Turan A, Karamanliolu B et al. Caudal neostigminefor postoperative analgesia in paediatric surgery. PaediatrAnaesth 2003; 13: 324–328.
17 Prosser DP, Davis A, Booker PD et al. Caudal tramadol forpostoperative analgesia in pediatric hypospadias surgery. Br JAnaesth 1997; 79: 293–296.
18 Bar-Meir E, Zaslansky R, Regev E et al. Nitrous oxide admin-istered by the plastic surgeon for repair of facial lacerations inchildren in the emergency room. Plast Reconstr Surg 2006; 117:
1571–1575.19 Vaughan M, Paton EA, Bush A et al. Does lidocaine gel alle-
viate the pain of bladder catheterization in young children? Arandomized, controlled trial. Pediatrics 2005; 116: 917–920.
20 Hee HI, Goy RW, Ng AS. Effective reduction of anxiety andpain during venous cannulation in children: a comparison ofanalgesic efficacy conferred by nitrous oxide, EMLA andcombination. Paediatr Anaesth 2003; 13: 210–216.
21 Burton JH, Auble TE, Fuchs SM. Effectiveness of 50% nitrousoxide ⁄ 50% oxygen during laceration repair in children. AcadEmerg Med 1998; 5: 112–117.
22 Klein EJ, Diekema DS, Paris CA et al. A randomized, clinicaltrial of oral midazolam plus placebo versus oral midazolamplus oral transmucosal fentanyl for sedation during lacerationrepair. Pediatrics 2002; 109: 894–897.
23 Pierce MC, Fuchs S. Evaluation of ketorolac in children withforearm fractures. Acad Emerg Med 1997; 4: 22–26.
24 Schutzman SA, Liebelt E, Wisk M et al. Comparison of oraltransmucosal fentanyl citrate and intramuscular meperidine,promethazine, and chlorpromazine for conscious sedation ofchildren undergoing laceration repair. Ann Emerg Med 1996;28: 385–390.
25 von Baeyer CL, Spagrud LJ. Systematic review of observational(behavioral) measures of pain for children and adolescentsaged 3 to 18 years. Pain 2007; 127: 140–150.
26 Beyer JE, Wells N. The Assessment of Pain in Children. PediatrClin North America 1989; 36: 837–854.
27 Burns N, Grove SK. The Concepts of Measurement. In: BurnsN, Grove SK, eds. The Practice of Nursing Research, 3rd edn.Philadelphia: W.B. Saunders Company, 1997: 319–341.
28 LoBiondo-Wood G, Haber J. Reliability and Validity. In:LoBiondo-Wood G, Haber J, eds. Nursing Research: Methods,Clinical Appraisal and Utilization, 4th edn. St. Louis: Mosby,1998: 327–350.
29 Suraseranivongse S, Santawat U, Kraiprasit K et al.Cross-validation of a composite pain scale for preschoolchildren within 24 hours of surgery. Br J Anaesth 2001; 87: 400–405.
30 Lawrence J, Alcock D, McGrath P et al. The developmentof a tool to assess neonatal pain. Neonatal Network 1993; 12: 59–66.
31 Katz ER, Kellerman J, Siegel SE. Behavioral distress in childrenwith cancer undergoing medical procedures: developmentalconsiderations. J Consult Clin Psychol 1980; 48: 356–365.
32 LeBaron S, Zeltzer L. Assessment of acute pain and anxiety inchildren and adolescents by self-reports, observer reports, anda behavior checklist. J Consult Clin Psychol 1984; 52: 729–738.
33 Jay SM, Ozolins M, Elliot CH et al. Assessment of Children’sDistress During Medical Procedures. Health Psychol 1983; 2:
133–147.34 Taddio A, Nulman I, Koren BS et al. A revised measure of
acute pain in infants. J Pain Symptom Manage 1995; 10: 456–463.35 Bulloch B, Tenenbein M. Validation of 2 pain scales for use in
the pediatric emergency department. Pediatrics 2002; 110:
e33–e38.36 Stewart B, Lancaster G, Lawson J et al. Validation of the Alder
Hey Triage Pain Score. Arch Dis Child 2004; 89: 625–630.37 McGrath PJ, Johnson G, Goodman JT et al. CHEOPS: A
Behavioral Scale for Rating Postoperative Pain in Children. In:Fields HL, Dubner R, Cervero F, eds. Advances in Pain Researchand Therapy. New York: Raven Press, 1985: 395–402.
38 Merkel SI, Voepel-Lewis T, Shayevitz JR et al. The FLACC: abehavioral scale for scoring postoperative pain in young chil-dren. Pediatr Nurs 1997; 23: 293–297.
39 Tarbell SE, Cohen IT, Marsh JL. The Toddler-PreschoolerPostoperative Pain Scale: an observational scale for measuringpostoperative pain in children aged 1–5. Preliminary report.Pain 1992; 50: 273–280.
40 Kelly AM, Powell C, Williams A. Parent visual analogue scaleratings of children’s pain do not reliably reflect pain reportedby child. Pediat Emerg Care 2002; 18: 159–162.
41 Singer AJ, Gulla J, Thode HC Jr. Parents and practitioners arepoor judges of young children’s pain severity. Acad Emerg Med2002; 9: 609–612.
42 Tyler DC, Tu A, Douthit J et al. Toward validation of painmeasurement tools for children: a pilot study. Pain 1993; 52:301–309.
43 Beyer JE, McGrath PJ, Berde CB. Discordance between self-report and behavioral pain measures in children aged 3–7 years after surgery. J Pain Symptom Manag 1990; 5: 350–356.
44 Manworren RC, Hynan LS. Clinical validation of FLACC:preverbal patient pain scale. Pediatr Nurs 2003; 29: 140–146.
45 Willis MHW, Merkel SI, Voepel-Lewis T et al. FLACC beha-vioral pain assessment scale: A comparison with a child’sself-report. Pediatr Nurs 2003; 29: 195–198.
46 Voepel-Lewis T, Merkel S, Tait AR et al. The reliability andvalidity of the Face, Legs, Activity, Cry, Consolability obser-vational tool as a measure of pain in children with cognitiveimpairment. Anesth Analg 2002; 95: 1224–1229.
47 Merkel S, Voepel-Lewis T, Malviya S. Pain assessment ininfants and young children: the FLACC scale. Am J Nurs 2002;102: 55–58.
48 Hartrick CT, Kovan JP. Pain assessment following generalanesthesia using the Toddler Preschooler Postoperative PainScale: a comparative study. J Clin Anesth 2002; 14: 411–415.
49 McCarthy C, Hewitt S, Choonara I. Pain in young childrenattending an accident and emergency department. J AccidentEmerg Med 2000; 17: 265–267.
50 Abu-Saad H. Assessing children’s responses to pain. Pain 1984;19: 163–171.
51 Goodenough B, Champion GD, Laubreaux L et al. Needle painseverity in children: Does the relationship between self-reportand observed behavior vary as a function of age? Austral JPsychol 1998; 50: 1–9.
52 Goodenough B, Addicoat L, Champion GD et al. Pain in 4- to6-year-old children receiving intramuscular injections: a
732 D. CRELLIN ET AL.
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733

comparison of the Faces Pain Scale with other self-report andbehavioral measures. Clin J Pain 1997; 13: 60–73.
53 Bieri D, Reeve RA, Champion GD et al. The Faces Pain Scalefor the self-assessment of the severity of pain experienced bychildren: development, initial validation, and preliminaryinvestigation for ratio scale properties. Pain 1990; 41: 139–150.
54 Hicks CL, von Baeyer CL, Spafford PA et al. The Faces PainScale-Revised: toward a common metric in pediatric painmeasurement. Pain 2001; 93: 173–183.
55 Keck JF, Gerkensmeyer JE, Joyce BA et al. Reliability andvalidity of the Faces and Word Descriptor Scales to measureprocedural pain. J Pediatr Nurs 1996; 11: 368–374.
56 Whaley LF, Wong DL. Nursing Care of Infants and Children.St Louis, 5th edn: Mosby Year Book, 1991.
57 Beyer JE, Aradine CR. Content validity of an instrument tomeasure young children’s perceptions of the intensity of theirpain. J Pediatr Nurs 1986; 1: 386–395.
58 Benini F, Griffith P, Lago P et al. Evaluating pain in children:experience with a ‘‘do-it-yourself’’ visual analogue scale. ActaPaediatr 1996; 85: 762.
59 Singer AJ, Richman PB, Kowalska A et al. Comparison of pa-tient and practitioner assessments of pain from commonlyperformed emergency department procedures. Ann Emerg Med1999; 33: 652–658.
60 Pothman R. Comparison of the visual analogue scale (VAS)and the smiley analogue scale (SAS) for the evaluation of painin children. Adv Pain Res Ther 2000; 15: 95–99.
61 Crellin L, Johnston L. A preliminary exploration of pain asso-ciated with nasogastric tube insertion in a paediatric popula-tion. Neonatal, Paediatric Child Health Nurs 2005; 8: 19–23.
62 Hendrickson M, Myre L, Johnson DG et al. Postoperativeanalgesia in children: a prospective study in intermittentintramuscular injection versus continuous intravenous infu-sion of morphine. J Pediatr Surg 1990; 25: 185–190.
63 LaMontagne LL, Johnson BD, Hepworth JT. Children’s ratingsof postoperative pain compared to ratings by nurses andphysicians. Issues in Comprehensive Pediatr Nurs 1991; 14: 241–247.
64 Miller D. Comparisons of pain ratings from postoperativechildren, their mothers, and their nurses. Pediatr Nurs 1996; 22:
145–149.65 Elliott CH, Jay SM, Woody P. An observation scale for mea-
suring children’s distress during medical procedures. J PediatrPsychol 1987; 12: 543–551.
Accepted 30 January 2007
BEHAVIORAL PAIN AND DISTRESS SCALES 733
� 2007 The AuthorsJournal compilation � 2007 Blackwell Publishing Ltd, Pediatric Anesthesia, 17, 720–733
Related Documents