Anaemia in pregnancy Dr varsha deshmukh Asso prof & unit incharge Govt medical college aurangabad

Anaemia in pregnancy vld
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Anaemia in pregnancy
Dr varsha deshmukh
Asso prof & unit incharge
Govt medical college
aurangabad

Magnitude of problem
• Globally, is about 30 %• In developing countries & India,
incidence is around 40 – 90%.• Responsible for 40% of maternal deaths
in third world countries.• Important cause of direct and
indirect maternal deaths - Vitere FE Adv Exp Med Biol 1994;352:127
Indian scenario
• 87% indian pregnant women are anaemic
• 46%-urban area
• 10%-severely anaemic
• (ICMR 2000)
• Direct death caused-20%(MMR)
• ASSO CAUSE-17-47%(ICMR 2000)

DEFINITION• Anemia - insufficient Hb to carry out O2
requirement by tissues.
• WHO definition : Hb conc. < 11 gm %
• CDC definition : Hb conc. < 11gm % in 1st and 3rd trimesters and < 10.5 gm% in 2nd trimeste WHO technical report Series no. 405, Geneva
1968For developing countries : cut off level suggested is 10 gm %
Centre for disease control, MMWR 1989;38:400-4

Degree Hb% Haematocrit (%)
Moderate 7-10.9 24-37%
Severe 4-6.9 13-23%
Very Severe <4 <13%
Degree Hb% Haematocrit (%)
Moderate 7-10.9 24-37%
Severe 4-6.9 13-23%
Very Severe <4 <13%
Irritability
Fatigue
Weakness
Lack of Concentration
Infection
Palpitation
Symptoms

Pallor of skin And m/m
Edema
PlatynychiaKoilonychia PlatynychiaKoilonychia
Glossitis
Stomatitis
Tachycardi
a
Soft ejectionsystolic murmur
Signs


Causes of anaemia
Physiological
Pathological
• Nutritional
• Haemorrhagic
• Haemolytic
Causes of anaemia
• Low socioeconomic status and poor hygiene
• Chronic malnutrition
• Poor availability of iron due to predominantly veg diet, diet low in calories but rich in phytates. Food and religious taboos
• GI infections and infestations (e.g. Kala azar, worm infestations)


Fetal Iron Stores
Infancy (92%)
Pre school (70%)
Adolescent (55 - 95%)
Adult women (60%)
Pregnancy (80%)
+ Menstruation


Causes of anaemia• Poor pre-pregnancy iron balance due to –
untreated systemic diseases & menstrual disorders
• Improper supplementation of iron in pregnancy ( late registration and poor follow up)
• Repeated childbearing• Lack of awareness and illliteracy
Effect of anaemia in preg
IUGR
IUD IUH
CCF
INFECTION
PRETERM LABOUR
PIH
Medical Disorder

Iron loss @ absorptionIron Absorption Iron Absorption ∝∝ 1
Amount of iron in the body
Iron Loss
Skin
Urine
Feces
Menstruation
1-2mg/d
20-30mg/c

Iron absorption
-ve
Iron absorption
↓ Bioavailabil i ty of Iron
-ve-ve
Phosphate phytate
Worm infestation
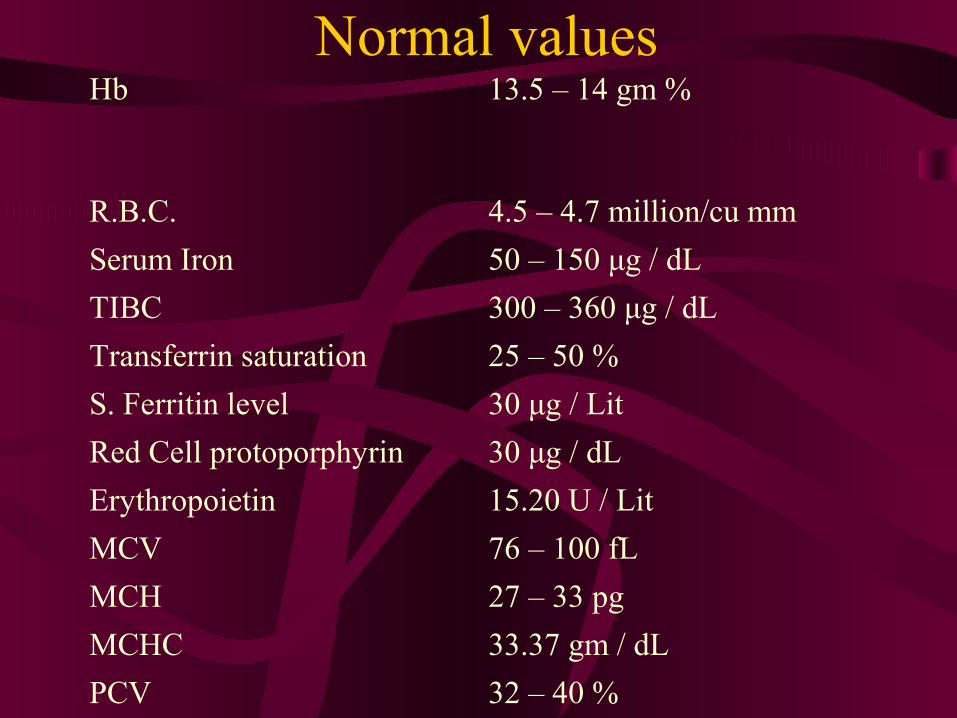
Normal valuesHb 13.5 – 14 gm %
R.B.C. 4.5 – 4.7 million/cu mm
Serum Iron 50 – 150 μg / dL
TIBC 300 – 360 μg / dL
Transferrin saturation 25 – 50 %
S. Ferritin level 30 μg / Lit
Red Cell protoporphyrin 30 μg / dL
Erythropoietin 15.20 U / Lit
MCV 76 – 100 fL
MCH 27 – 33 pg
MCHC 33.37 gm / dL
PCV 32 – 40 %
diagnosis
EASY TO DIAGNOSE
SIMPLE TO TREAT

Hookworm infestations
♦ Common cause of anaemia in developing countries
♦ Most common – hookworm infestation, Round worm, whip worm, etc.
♦ Oral iron therapy becomes ineffective
♦ Treatment by antihelminthics is a must
Treatment
♦ Mebendazole : 100mg twice daily for three days
♦ Pyrantel pamoate : 10mg / kg in single dose.
♦ Albendazole : 400mg once a day for three days


Treatment of iron def anaemia
FS + FA
Pregnancy
Lactating mothers
Family planning acceptors
Children – 1 to 11 years

prevention
Pre – pregnancy :
• Treat the cause before conception
• Pre-pregnancy balanced diet, education
and health support.
• Build up iron stores during adolescent
phase


Iron supplementation• Ideal dose – 100mg per day (prophylactic)
• Ferrous gluconate, ferrous fumarate, ferrous succinate, ferrous sulphate, ferrous ascorbate citrate
• Rise in Hb – 0.8 gm / dl / week
• Side effects -G I upset most common
• Pt. compliance not guaranteed
• Ineffective in pts with worm infestations
• Inconclusive evidence on benefit of controlled release Iron preparation



Types of iron preparations
Oral IronBlood
transfusionParenteral
Parenteral iron therapy
100 mg elemental Iron
Anaphylactic Anaphylactic reactionreaction
Anaphylactic Anaphylactic reactionreaction
I.M. I.V.

Indications of parenteral therpy
• Intolerance to oral iron
• Poor compliance to oral iron
• Gastrointestinal disorders
• Malabsorption syndromes
• Rapid blood loss

Indications of parenteral therapy
• Inability to maintain iron balance (haemodialysis)
• Patient donating large amount of blood
for auto-transfusion programme
• ? Pregnant women with severe IDA, presenting late in pregnancy

Folic acid deficiency
Special considerations in diagnosis
• FDA is suspected when the expected response
to adequate iron therapy is not achieved
• Macrocytosis can occur in pregnancy in absence
of FDA
• If FDA + IDA present, it will be masked by IDA
• Definitive diagnosis – Bone marrow aspirate
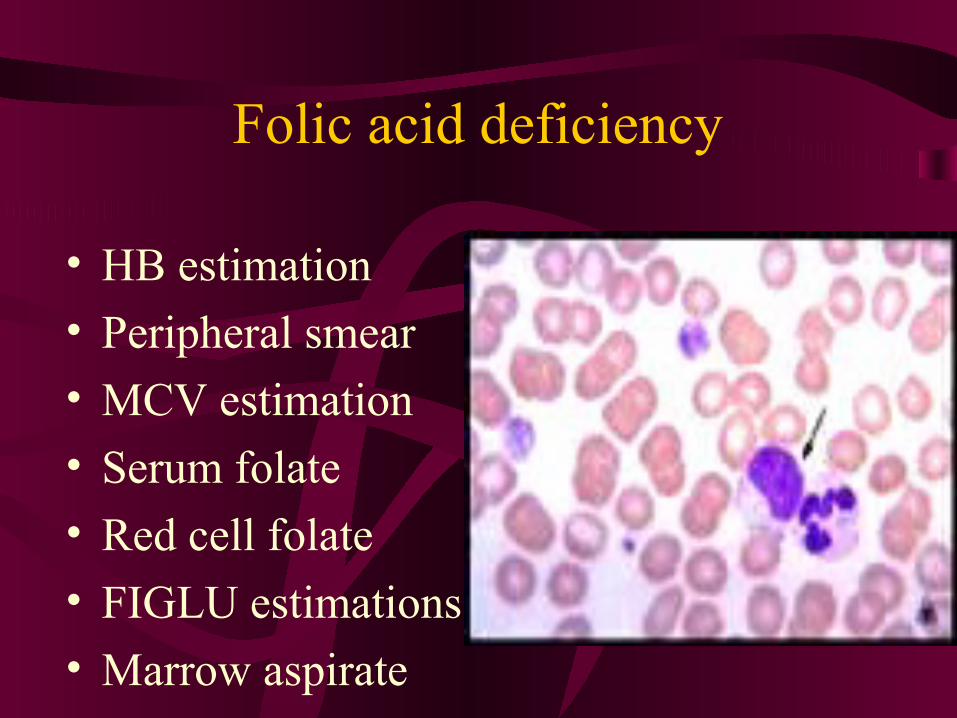
• HB estimation
• Peripheral smear
• MCV estimation
• Serum folate
• Red cell folate
• FIGLU estimations
• Marrow aspirate
Folic acid deficiency
Folic acid deficiency
♦ Strong case for routine prophylaxis
♦ Prophylaxis with anti convulsants
♦ Continue routine oral therapy for
hemolytic anaemia
♦ Parenteral therapy for severe deficiency

Blood transfusion
‘‘ transfusion should be transfusion should be prescribed prescribed ONLYONLY for for
condit ions for which there is condit ions for which there is NONO OTHER TREATMENT’ OTHER TREATMENT’

♦ Anaemia although preventable is a global
problem
♦ Anaemia still is the commonest cause of maternal
mortality and morbidity in spite of easy diagnosis
and treatment
♦ Anaemia can be due to a number of causes,
including certain diseases or a shortage of iron,
folic
acid or Vitamin B12.
♦ The most common cause of anemia in pregnancy
is
iron deficiency.
♦ Iron therapy is best given orally
Take Home Message

• The youth need to be educated about diet, sanitation and personal hygiene
• Hookworm infestation should be treated
• Pregnant women should be given Iron and folate supplements
Take Home Message

Related Documents