ANA ASLAN ANA ASLAN INTERNATIONAL INTERNATIONAL ACADEMY OF ACADEMY OF AGING AGING ANA ASLAN ANA ASLAN INTERNATIONA INTERNATIONA L FOUNDATION FOUNDATION 1 PAIN QUANTIFICATION IN SEVERE ALZHEIMER’S DISEASE: ADVANTAGES AND DISADVANTAGES OF PAIN ASSESSMENT SCALES Ioana Ioancio, MD, PhD Ana Aslan International Academy of Aging, “Elias” University Emergency Hospital, Bucharest, Romania Ileana Turcu , , PhD Ana Aslan International Academy of Aging, Bucharest, Romania Luiza Spiru, MD, PhD Head of the Day Hospital of Memory Diseases, President of Ana Aslan International Foundation Vice-President of Ana Aslan International Academy of Aging, Professor of Geriatric Dept. ”Carol Davila” University of Medicine and Pharmacy, “Elias” University Emergency Hospital, Bucharest, Romania 26 th International Conference of Alzheimer Disease International ADI 2011 26-29 March 2011 Toronto, Canada Toronto, Canada

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ANA ASLANANA ASLANINTERNATIONALINTERNATIONAL
ACADEMY OF ACADEMY OF AGINGAGING
ANA ASLANANA ASLANINTERNATIONINTERNATIONALALFOUNDATIONFOUNDATION
1
PAIN QUANTIFICATION IN SEVERE ALZHEIMER’S DISEASE: ADVANTAGES AND DISADVANTAGES
OF PAIN ASSESSMENT SCALES
Ioana Ioancio, MD, PhD Ana Aslan International Academy of Aging,
“Elias” University Emergency Hospital, Bucharest, Romania
Ileana Turcu, , PhDAna Aslan International Academy of Aging,
Bucharest, Romania
Luiza Spiru, MD, PhDHead of the Day Hospital of Memory Diseases,
President of Ana Aslan International FoundationVice-President of Ana Aslan International
Academy of Aging, Professor of Geriatric Dept. ”Carol Davila” University of Medicine and Pharmacy,
“Elias” University Emergency Hospital, Bucharest, Romania
26th International Conference of Alzheimer Disease International ADI 2011
26-29 March 2011Toronto, CanadaToronto, Canada
26th International Conference of Alzheimer Disease International ADI 2011
26-29 March 2011Toronto, CanadaToronto, Canada
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
2
Content
Background ‘Alzheimer’s Crisis’Personality changes in dementias
Our studyAimsSubjectsMethodsResultsDiscussionsConclusions
To do in the management of behavioral symptoms
2
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
Background
3
50-85% of the geriatric patients have pain
32-53% of the patients with dementia have pain daily
Dementia is associated with SNC changes that alter pain tolerance, but not pain thresholds.
Horgas AL et al., 2009. Pain assessment in Persons with Dementia: Relationship
Between Self Report and Behavioral Observation. J Am Geriatr Soc 57:126-132
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
4
Horgas AL et al., 2009. Pain assessment in Persons with Dementia: Relationship
Between Self Report and Behavioral Observation. J Am Geriatr Soc 57:126-132
PAIN SELF REPORT a standard criterion of pain assessment , but INSUFFICIENT ! often underestimates patient’s pain.
Pain Self-Report contains: pain presence disclosed by Structured Pain Interview pain intensity pain duration pain location
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
5
Catananti C, Gambassi G, 2010. Pain
assessment in the elderly. Surgical
Oncology, 9:140-148.
Pain reporting depends of :
Biology Age older people experience less pain the perception that pain is an inevitable part of
aging
Culture pain is something to be endured pain means weakness Religion Ethnicity Cognitive impairment
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
6
Linda Mc Auliffe et al., 2008. Pain assessment in older people with dementia:
Literature review. Journal of Advanced Nursing.
Barriers in pain recognition:
’no - pain’ subset of people with dementia,
stoical attitudes.
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
7
Quantitative Assessment of Pain :
1. Visual Analogue Scale (VAS)2. The faces pain scale3. The verbal rating scale4. The numerical rating scale.
1.Catananti C, Gambassi G, 2010. Pain assessment in the elderly.
Surgical Oncology, 9:140-148.
Pain measurementthe most adequate assessment.
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
8
Quantitative Assessment of Pain :
Involves:
Localisation and referral pattern of pain + complete functional physical examination
Characteristics of pain McGill Pain Questionnaire (emotional, sensory and evaluative dimensions of pain)
Quantification of response to analgesic therapies. Patient’s current level of functioning (ADL,IADL, Barthel
Score) Consideration of:
Affective disorders (anxiety, anger) the Geriatric Depression Scale
Cognitive impairment , delirium and behaviour disturbances
Sleep disorders
Frequent re-evaluation is an essential part of effective management 1.Catananti C, Gambassi G, 2010. Pain assessment in
the elderly.Surgical Oncology, 9:140-148.
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
9
Dementia a major impediment in the evaluation and management of pain.
Cross-sectional studies less analgesics were administrated in Alzheimer’s patients than in non-cognitively impaired old people.
Cognitive impairment may be aggravated by uncontrolled pain.
In clinical practice the ability to remember, interpret and respond to pain can be altered in patients with dementia.
1.Catananti C, Gambassi G, 2010. Pain assessment in the elderly.
Surgical Oncology, 9:140-148.
Pain assessment in Dementia
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
10
The Pain Assessment in Advanced Dementia (PAINAD) includes:
assesses breathing, negative vocalisation, facial expression, body language .
The Pain Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC) -60 items organized in 4 groups:
facial expression, activity/body movement, social/personality/mood indicators physiological needs
Cf. Catananti C, Gambassi G, 2010. Pain assessment in the
elderly. Surgical Oncology, 9:140-148.
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
11
Dolophus 2: 5 somatic items: somatic complaints, protective body posture adopted at rest, protection of sore areas, facial expression and gaze, sleep pattern),
2 psychomotor items:based on observation of washing and/or dressing and mobility3 psychosocial items: communication, social interaction, behaviour)
The Elderly Pain Caring Assessment -2(EPCA-2)8 item behavioural scale to rate the intensity of pain in non-verbally communicating older patients.Cf. Catananti C, Gambassi G, 2010. Pain
assessment in theelderly. Surgical Oncology, 9:140-148.
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
12
Our study
The aim:
Quantitative estimation of pain intensity using various pain scales,
Detection of different scales power
on patients referred to our Ana Aslan Memory Clinic from Bucharest, Romania.
12
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
13
Methods
Patients:
510 patients diagnosed with severe Alzheimer dementia 398 females 112 males mean age 73.5 years
Assessment tools:
Visual Analog Scale, Graphic Scale, Verbal Scale, Word Descriptor ScaleScales for Evaluation of Functional Performance (ADL, IADL).
13
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
14
For an accurate assessment of pain we had to identify the type of pain, the characteristics and severity of pain .
The pain was quantified : at the first visit periodically afterwards.
Only 10% (n=51) of all patients could be assessed using all 5 scales.
14
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
1515
Results
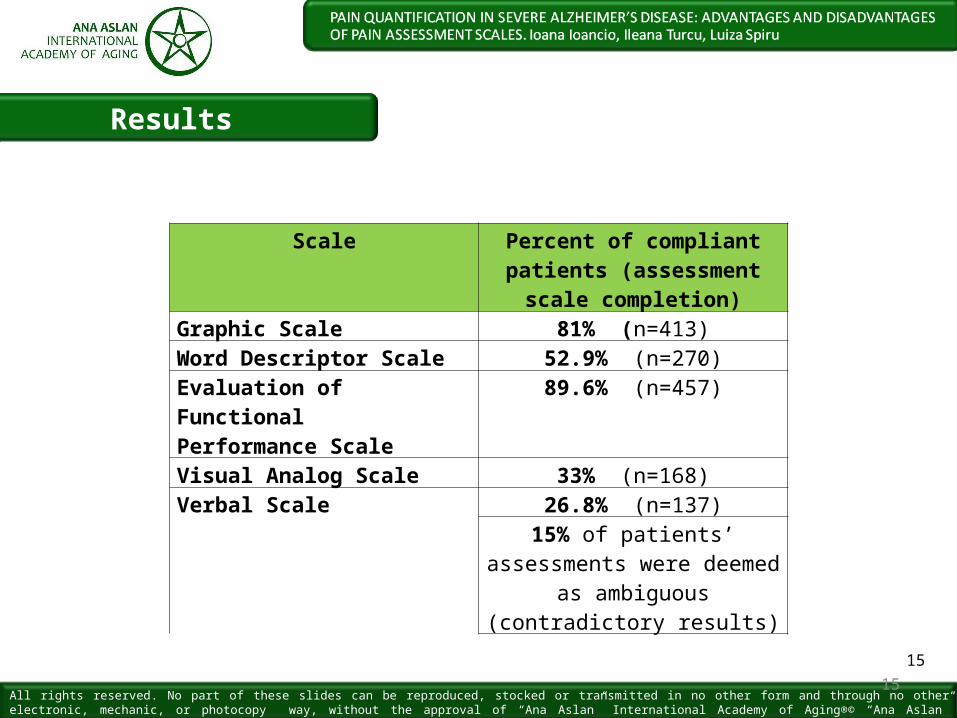
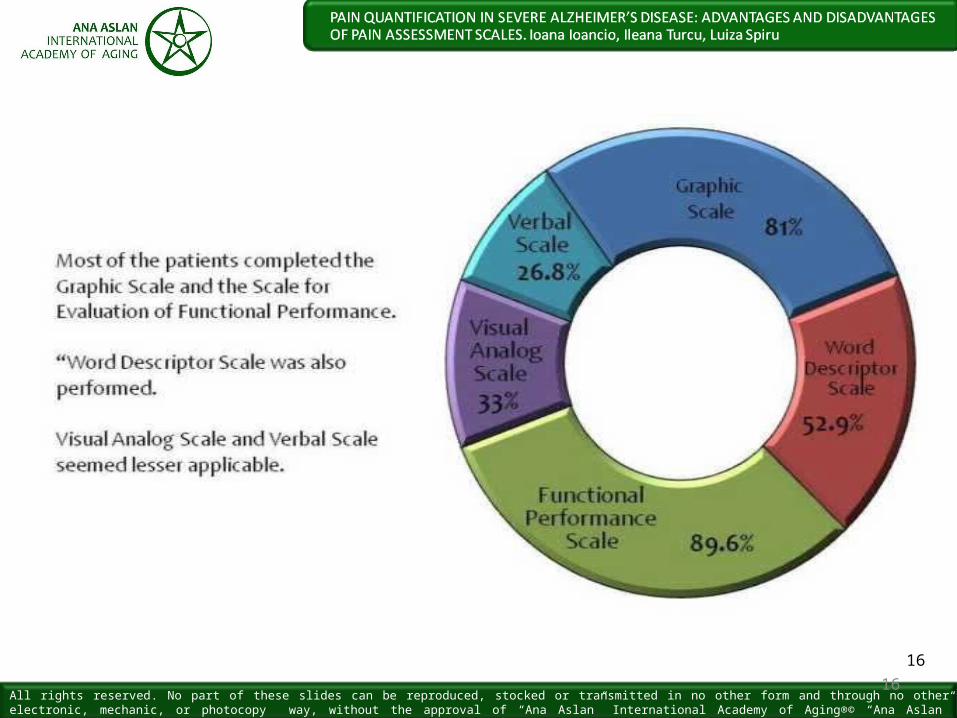
Scale Percent of compliant patients (assessment
scale completion)Graphic Scale 81% (n=413)Word Descriptor Scale 52.9% (n=270)Evaluation of Functional Performance Scale
89.6% (n=457)
Visual Analog Scale 33% (n=168)Verbal Scale 26.8% (n=137)
15% of patients’ assessments were deemed
as ambiguous (contradictory results)
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
1616
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
1717
Conclusions
Because our patients have: severe memory impairment difficulty integrating pain experiences over time,
A single pain quantification scale: is far to reflect the involvement of pain in the patient’s
situation to offer sufficient information for his/her management
As much as possible scales must be applied They must be correlated with:
the severity of cognitive impairments (psychometric scales scores)
the outcomes of analgesic medication Information provided by the caregiver.
All rights reserved. No part of these slides can be reproduced, stocked or transmitted in no other form and through no other electronic, mechanic, or photocopy way, without the approval of “Ana Aslan” International Academy of Aging®© “Ana Aslan” International Foundation ®© Brain Aging International Journal ®©.
1818
Only then we can adjust: timing dosage
of different drugs administration (either for the
disease per se or analgesics),
or we can react by suggesting nondrugtherapies for more physical,
psychological,social and spiritual comfort.
ANA ASLANINTERNATIONAL
ACADEMY OF AGING
ANA ASLANINTERNATIONALFOUNDATION
Thank you for
attention
and feedback
HealthyBrain Aging
Healthy Aging
Ioana Ioancio, MD, [email protected]
Ileana Turcu, [email protected]
Luiza Spiru, MD, [email protected]
Related Documents











