An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine at Dartmouth Hanover, NH, USA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

An Overview of Genital Stromal Tumors
By Konstantinos Linos MD, FCAP, FASDP
Bone, Soft Tissue and Dermatopathology
Assistant Professor of Pathology
Dartmouth-Hitchcock Medical Center
Geisel School of Medicine at Dartmouth
Hanover, NH, USA

• Book Royalties
Financial disclosures

• Broad variety of soft tissue tumors exclusively in vulvovaginal and inguinoscrotal sites
• Probably originate from a distinct zone of subepithelial stromal cells or subepithelialmesenchyme extending from the endocervix
• Striking morphologic, immunophenotypic and genetic overlap
General

• Fibroepithelial Polyp• Superficial Myofibroblastoma• Cellular angiofibroma• Mammary-type myofibroblastoma• Angiomyofibroblastoma• Deep/”Aggressive” angiomyxoma• Superficial Angiomyxoma• Prepubertal Vulvar Fibroma• Lipoblastoma-Like tumor of the vulva• Smooth Muscle Tumors of the external
genitalia

• Synonyms• Mesodermal stromal polyp• Cellular Pseudosarcomatous fibroepithelial
stromal polyp• Pseudosarcoma botryoides
• Benign polypoid growth of the vagina, vulva or cervix
• Strongly tied to hormonal stimulation
Fibroepithelial Stromal Polyp

• Most often during pregnancy • also in reproductive age women• Postmenopausal women undergoing hormonal
replacement
• Regression in the postpartum period is typical
• Typical clinical presentation is one or more polyps that may be symptomatic
• Usually 1-5cm






Immunohistochemistry
• Consistently reactive for• Desmin• Estrogen Receptor (ER)• Progesetrone Receptor (PR)• Sometimes Smooth Muscle Actin



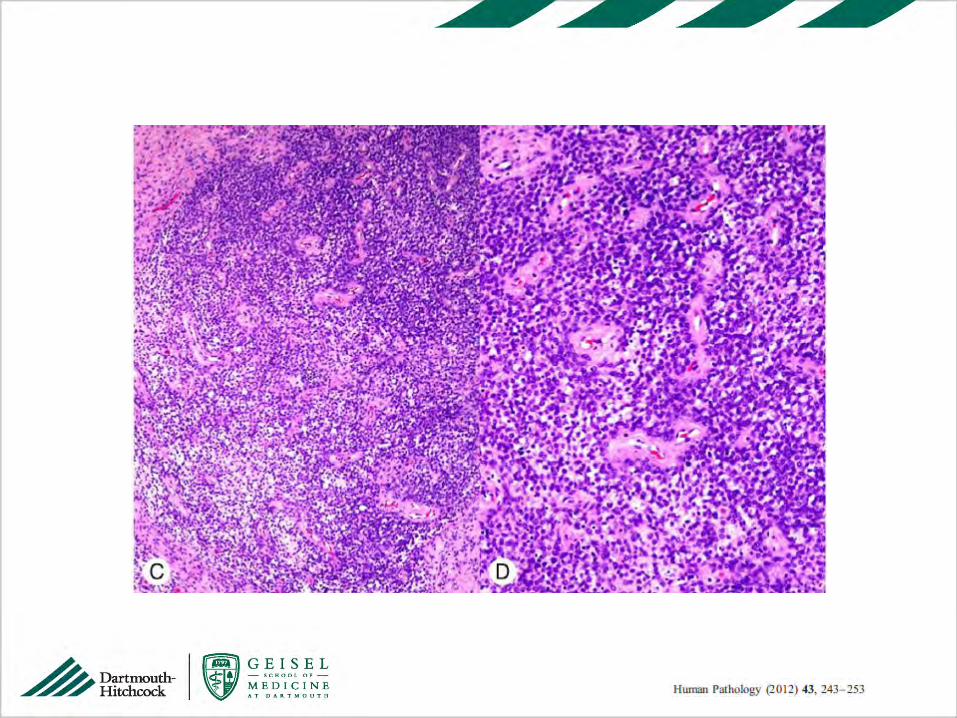
Enbryonal
Rhabdo-
myosarcoma
Rhabdomyoma

Superficial (cervicovaginal) myofibroblastoma
• Benign tumor that may arise in the vulva, vagina or cervix
• Nodular or polypoid painless mass in adults most commonly in their 50s
• Grossly well-circumscribed, firm and dense mass from 1 to 6.5cm



Immunohistochemistry• Desmin in 75-100% of cases
• ER/PR in 80-100%
• CD34 in 50-85%
• SMA in 0-45%

Cellular Angiofibroma• Synonym
• Angiomyofibroblastoma-like tumor of the male genital tract
• Benign neoplasm in vulvovaginal and inguinoscrotal areas
• Middle-aged patients with a female predominance
• Classically subcutaneous painless nodule usually not exceeding 7cm








Immunohistochemistry
• Inconsistent expression
• Variable expression of CD34, desmin, SMA
• P16 positivity in sarcomatous areas
p16

Mammary-type Myofibroblastoma
• Initially described in breast • Can arise anywhere in soft tissue • Predilection for inguinal and pelvic region
• Most cases occur in men
• Median age 53
• Range 1-22cm (median size of 6cm)





Immunohistochemistry
• Frequently positive for CD34 and Desmin (~90%)
• Rare cases negative for both (~3%)
CD34 Desmin

• Benign tumor
• Local excision curative
• No evidence of significant recurrence risk even in the presence of positive resection margins
Prognosis

RB1 and Genital Stromal Tumors

Mammary-type
myofibroblastoma
Cellular
Angiofibroma
RB1
RB1

• Benign mesenchymal neoplasm of the vulva and vagina
• Uncommonly may present as a penduculatedlesion
• Most grossly well-circumscribed and smaller than 5cm
Angiomyofibroblastoma




Immunohistochemistry • Positive for
Desmin, ER & PR
• Less commonly CD34 and SMA positivity
Desmin


• Synonym: “Aggressive” angiomyxoma• Low Grade, locally infiltrative myxomatous
neoplasm specific to the deep vulvovaginal, perineal and pelvic tissues
• Strong female predisposition • In men in the analogous inguinoscrotal and
perineal regions • Usually 4th decade of life with painless cystic
mass often exceeding 10cm
Deep Angiomyxoma

• Less aggressive course than initially described if completely excised with negative margins
• Potential for local destructive recurrence some times years (often decades) after initial excision• Even tumors as small as 3cm have recurred
multiple times• Grossly soft gelatinous tumor with ill-defined
margins • In recurrent cases may have more fibrous
appearance



Immunohistochemistry• Typically positive for:
• Desmin• SMA• ER/PR• Variable CD34 positivity
• Structural rearrangements of the region 12q15• ~30% of tumors, intragenic/extragenic
• HMGA2 and CDK4 IHCs positive• When positive, useful in confirming the diagnosis
and assessing margins status in a subset of cases

Reactive changes Smooth Muscle Tumor
WDL Superficial Angiomyxoma

Superficial Angiomyxoma• Can also occur in the genital region of women • Include this entity in the differential of
myxoid lesions of the distal female genital tract
• Association with Carney complex less clear with lesions in the genital area
• Typically polypoid and usually less than 5cm• Potential for local nondestructive recurrence in
~30-40% of cases



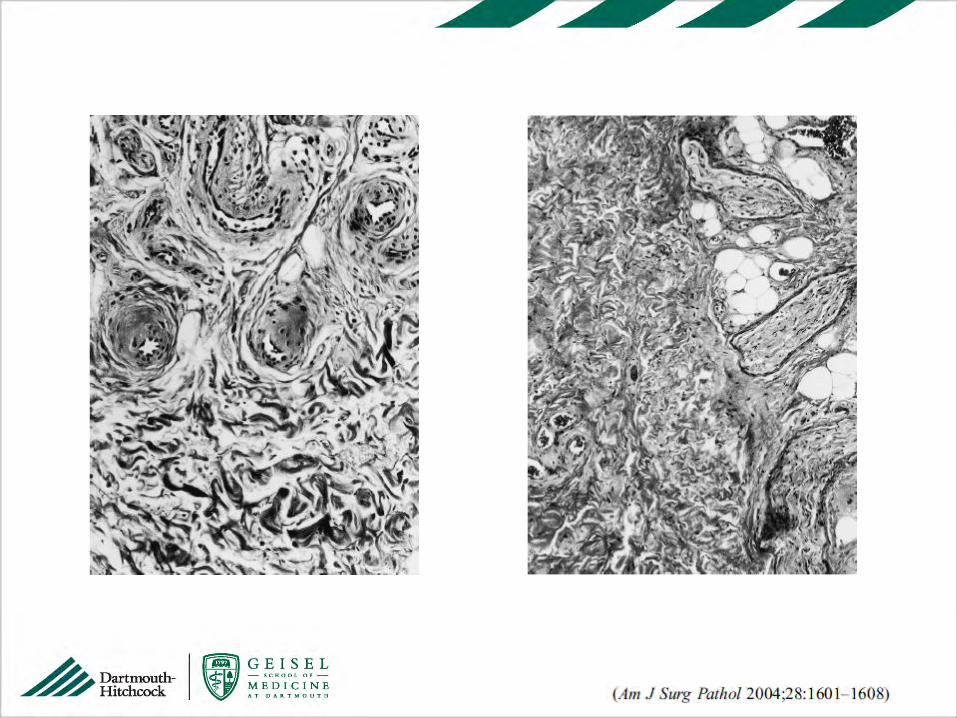
Prepubertal Vulval Fibroma


Myxoid Collagenous





Loss of RB1 by IHC
• Lack of PLAG1 and HMGA2
expression suggests it is
distinct from “true”
lipoblastomas
• Loss of Rb1 suggests possible
role of 13q chromosomal
alterations
• Possible relationship with the
Spindle cell lipoma family

Practical approach
• Correct Identification of Aggressive Angiomyxoma is critical
• If above has been excluded and definitive classification is not possible you can use label• “Benign Genital Stromal Tumor”

Smooth Muscle Tumors of the External Genitalia
• Smooth muscle tumors of vulva, vagina, and scrotum have similar gross and pathologic features to soft tissue and uterine counterparts
• Criteria for malignancy depend on the specific site
• Soft tissue• Superficial (including nipple)• Genital • Deep seated

Epithelioid morphology
Myxoid changes
LEIOMYOMA

LEIOMYOSARCOMA
Some combination of
• cytologic atypia,
• increased mitotic
activity
• Increased size
• infiltrative growth

Smooth Muscle Tumors of the Vulva
• Leiomyomas of the vulva is one of the more common vulvar mesenchymal neoplasms • Present in 4th to 5th decade as a small (<3cm)
mass• Mutliple leiomyomas may be manifestation of
Alport Syndrome• Hereditary disorder
• Glomerulonephritis, ocular abnormalities & hearing loss
• Mutation in COL4A3, COL4A4, COL4A5




Smooth Muscle Tumors of the Scrotum
• Uncommon and most are leiomyosarcomas• Cytologic atypia, mitotic activity and necrosis
• Rare in this location tumors with absence of atypia or mitotic activity• Extensive sample is necessary before apply the
diagnosis of leiomyoma • Note long-term clinical follow-up
• Any mitotic activity warrants classification as malignant

• Neurofibroma• S100-protein/SOX 10 +
• Solitary Fibrous Tumor• STAT6 positive
• Inflammatory Myofibroblastic Tumor• ALK + in 50-60% of cases
• Sarcomatoid Carcinoma• Diffuse cytokeratin expression• Examine for High Grade Squamous Intraepithelial
lesion or dVIN
Differential Diagnosis

Related Documents











