精神衛生護理雜誌 7卷1期.中華民國101年10月 廣泛性焦慮症照護反思 1 An Overview of Generalized Anxiety Disorder and Reflections on the Effective Nursing Care of Patients with This Disorder Chueh-Fen Lu 1 • Miau-Chuan Chen 2 • Shih-Chieh Shu 3 AbsTRACT: In Taiwan, students of psychiatric nursing are taught about anxiety disorders as a whole. Consequently, they have vague knowledge of nursing care of specific anxiety disorders. Generalized anxiety disorder (GAD) has the highest prevalence rate compared to other diseases. Thus, a better understanding of GAD is vital to providing efficient care to most anxiety patients. This article aims to advance the understanding of GAD, including epidemiology, cost, historical background, aetiology, characteristics, help seeking behaviours, treatments, and prognosis. Moreover, the latest revision of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM V) provides a clearer view of GAD. Based on this knowledge, nurses can reflect on how more appropriate nursing interventions may be designed. Despite improved medications and claims of efficacy of cognitive behaviour therapies, GAD remains a chronic disease with co-morbidities. Therefore, nurses need to be alert to mood changes, especially in patients with depression. Led by traditional pathological viewpoint. nurses tend to treat anxiety as a negative emotional state and this needs to be reconsidered. If the nursing profession views the patient as a holistic being, it should seek a different view of anxiety, for example, place it in the context of Chinese culture. In this way, patient empowerment can facilitate management of GAD. Key Words: generalized anxiety disorder, nursing, reflection. Introduction The epidemiological data show that, among men- tal disorders, anxiety disorders have one of the highest prevalence rates and, among anxiety disorders, general- ized anxiety disorder (GAD) has the highest prevalence rate (Csémy, 2011). However, GAD is often overlooked as it is covered in only a small section of the chapter on anxiety disorders of the textbook used in the course on psychiatric nursing. Therefore, having a better under- standing of GAD is important because it can improve de- livery of appropriate nursing care to patients with GAD. 1 PhD, Associate Professor, School of Nursing, Chang Gung University of Science and Technology. 2 Instructor, School of Nursing, Chang Gung University of Science and Technology. 3 MD, Chang Gung Hospital. Received: August 19, 2011 Accepted: June 28, 2012 Address Correspondence to: Chueh Fen Lu, No. 261, Wen-hwa 1st Rd., Kwei-shan, Taoyuan, Taiwan 33303 Tel: 886(3)2118999 ext. 3441; E-mail: cfl[email protected] In line with the revisions to the Diagnostic and Statistical Manual of Mental Disorders (DSM) made in DSM V (Goldberg, Regier, Kendler & Sirovatka, 2010), this ar- ticle aims to review the knowledge on GAD that applies to current nursing practice so that nursing interventions can be improved. Generalized anxiety disorder According to the DSM IV-TR, generalized anxiety disorder is a subcategory of anxiety disorders

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
精神衛生護理雜誌 7卷1期.中華民國101年10月
廣泛性焦慮症照護反思 1
An Overview of Generalized Anxiety Disorder and Reflections on the Effective Nursing Care of Patients
with This Disorder
Chueh-Fen Lu1 • Miau-Chuan Chen2 • Shih-Chieh Shu3
AbsTRACT: In Taiwan, students of psychiatric nursing are taught about anxiety disorders as a whole. Consequently, they have vague knowledge of nursing care of specific anxiety disorders.Generalized anxiety disorder (GAD) has the highest prevalence rate compared to other diseases. Thus, a better understanding of GAD is vital to providing efficient care to most anxiety patients. This article aims to advance the understanding of GAD, including epidemiology, cost, historical background, aetiology, characteristics, help seeking behaviours, treatments, and prognosis. Moreover, the latest revision of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM V) provides a clearer view of GAD. Based on this knowledge, nurses can reflect on how more appropriate nursing interventions may be designed. Despite improved medications and claims of efficacy of cognitive behaviour therapies, GAD remains a chronic disease with co-morbidities. Therefore, nurses need to be alert to mood changes, especially in patients with depression. Led by traditional pathological viewpoint. nurses tend to treat anxiety as a negative emotional state and this needs to be reconsidered. If the nursing profession views the patient as a holistic being, it should seek a different view of anxiety, for example, place it in the context of Chinese culture. In this way, patient empowerment can facilitate management of GAD.
Key Words: generalizedanxietydisorder,nursing,reflection.
Introduction
The epidemiological data show that, among men-tal disorders, anxiety disorders have one of the highest prevalence rates and, among anxiety disorders, general-ized anxiety disorder (GAD) has the highest prevalence rate (Csémy, 2011). However, GAD is often overlooked as it is covered in only a small section of the chapter on anxiety disorders of the textbook used in the course on psychiatric nursing. Therefore, having a better under-standing of GAD is important because it can improve de-livery of appropriate nursing care to patients with GAD.
1PhD, Associate Professor, School of Nursing, Chang Gung University of Science and Technology. 2Instructor, School of Nursing, Chang Gung University of Science and Technology. 3MD, Chang Gung Hospital.Received: August 19, 2011 Accepted: June 28, 2012Address Correspondence to: Chueh Fen Lu, No. 261, Wen-hwa 1st Rd., Kwei-shan, Taoyuan, Taiwan 33303Tel: 886(3)2118999 ext. 3441; E-mail: [email protected]
In line with the revisions to the Diagnostic and Statistical Manual of Mental Disorders (DSM) made in DSM V (Goldberg, Regier, Kendler & Sirovatka, 2010), this ar-ticle aims to review the knowledge on GAD that applies to current nursing practice so that nursing interventions can be improved.
Generalized anxiety disorder
Accord ing to the DSM IV-TR, genera l ized anxiety disorder is a subcategory of anxiety disorders

精神衛生護理雜誌 7卷1期.中華民國101年10月
2 Nursing Reflections of Generalized Anxiety Disorder
(American Psychiatric Association, 2000, p. 472). The International Classification of Diseases (ICD) also includes GAD as a diagnosis (Alonso, et al. 2004). The aspects related to nursing care of patients with GAD are discussed, including epidemiology, budget consumption, characteristics, help seeking behaviours, treatments, and prognosis.
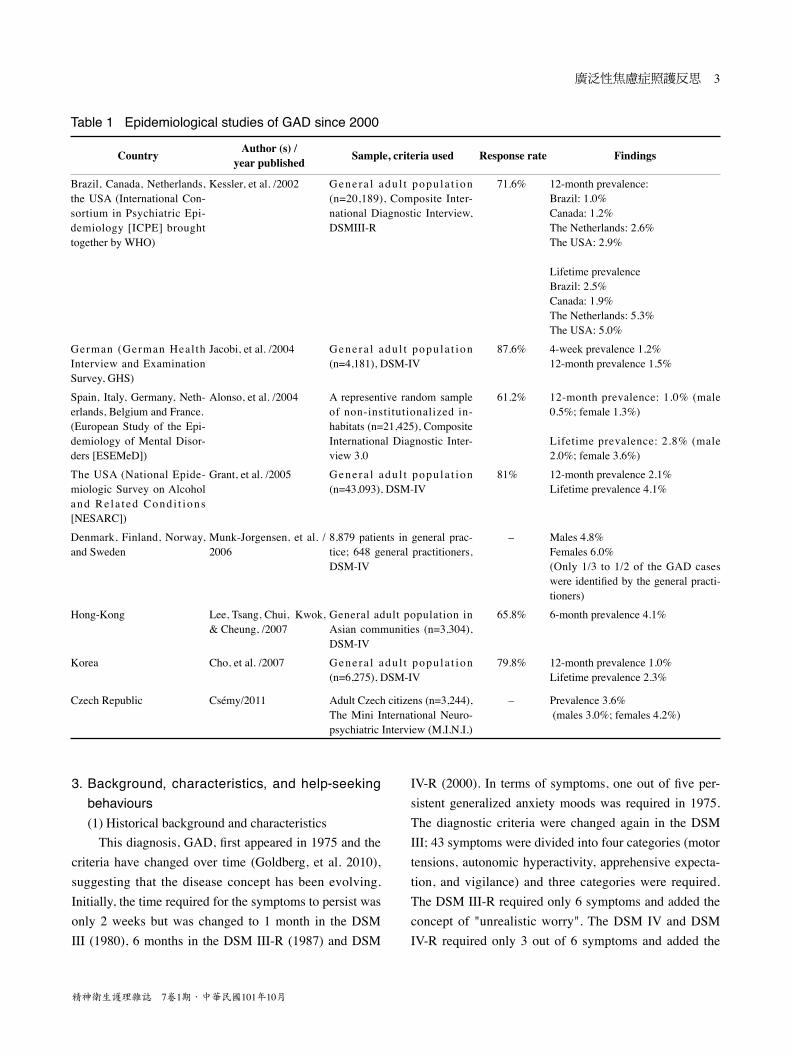
1. EpidemiologyThe most recent prevalence rates of GAD in adults
in the general population of different countries are summarized in Table 1. Twelve-month prevalence rates range from 1.0% (Brazil and Korea) to 3.6% (The Czech Republic) and lifetime prevalence rates range from 1.9% (Canada) to 5.3% (Netherlands). Prevalence rates appear to be similar in these countries. These figures indicate that GAD is a highly prevalent mental illness and the most frequent mental disorder in communities (Kessler, 2007; Csémy, 2011).
It is believed that prevalence rates of GAD are underestimated as a result of social stigma and atypi-cal symptoms (Bandelow, 2003; Chien, Chou, Lin, Bih, Chou, 2004; Munk-Jorgensen, et al. 2006). Unlike panic disorder or obsessive compulsive disorder, GAD has features and atypical clinical symptoms that may escape investigators’ notice (Bandelow, 2003; 湯&葉, 2003). Wittchen (2002) indicated that it may take 5–10 years before GAD is diagnosed. Furthermore, Munk-Jorgensen, et al. (2006) pointed out that not all GAD cases are rec-ognized by general practitioners; only 33% of cases in Denmark and 53% in Norway were recognized.
According to the Taiwan Psychiatric Epidemiology Project (TPEP) (Hwu, Yeh & Chang, 1989), the 12-month prevalence of GAD varies in different areas of Taiwan: 3.7% (city, Taipei), 9.3% (suburb, Shu-Lin), and 6.9% (rural, Tsao-Tun). The lifetime prevalence rates are 4.8% (Taipei), 13.1% (Shu-Lin), and 9.3% (Tsao-Tun). The overall lifetime prevalence rate is 7.8%, which is higher than rates in other countries. In the latest investigation, using Taiwan National Health Insurance database, Chien, et al. (2004) reported that, compared to other psychiatric disorders, anxiety disorders have the highest 12-month
prevalence rate (1.48%). This is twice the second highest rate (0.76% for neurotic depression) and three times the third highest rate (0.46% for schizophrenic disorders). However, the data sources used by these two studies were different. The TPEP used randomized community-based samples to determine the actual prevalence rate, while Chien et al. (2004) used the Taiwan National Health Insurance database which includes only people who use medical resources. This accounts for the 2.5–6-fold differences between various areas. The prevalence rate determined by the TPEP is more accurate since the general population was sampled.
2. The cost of GADCompared with those who have other psychiatric
disorders, people with anxiety disorders utilize more resources and more frequently present to general practitioners than to psychiatric professionals, placing a strain upon the healthcare system (Lepine, 2002; Kessler, 2007). The economic costs of anxiety disorders include treatment costs (for psychiatric non-psychiatric care) and the costs of decreased productivity and absenteeism from work (Antai-Otang, 2003). In the USA, the economic and personal cost attributable to anxiety disorders was almost one third of the total mental health budget (Wittchen, 2002). Based on a national survey, Grant, et al. (2005) concluded that disability and impairment stemming from pure GAD were equivalent to that from pure mood disorders and significantly greater than that from pure substance use and other anxiety and personality disorders.
Similarly, doctor-shopping behaviour among GAD patients is common in Taiwan and affects health service consumption greatly (湯&葉, 2003). Taiwanese patients can seek help from specialist physicians directly without a referral. As a result, patients with GAD in Taiwan visit a wide range of specialists including cardiologists, general internal medicine physicians, and neurologists before pro-ceeding to psychiatric clinics (湯&葉, 2003). Apart from western medical treatment, folk therapies are sought and expenditures for this are hard to estimate (湯&葉, 2003;葉&林, 2006).
精神衛生護理雜誌 7卷1期.中華民國101年10月
廣泛性焦慮症照護反思 3
Table 1 Epidemiological studies of GAD since 2000
Country Author (s) / year published sample, criteria used Response rate Findings
Brazil, Canada, Netherlands, the USA (International Con-sortium in Psychiatric Epi-demiology [ICPE] brought together by WHO)
Kessler, et al. /2002 Genera l adu l t popu la t ion (n=20,189), Composite Inter-national Diagnostic Interview, DSMIII-R
71.6% 12-month prevalence: Brazil: 1.0% Canada: 1.2% The Netherlands: 2.6%The USA: 2.9%
Lifetime prevalence Brazil: 2.5%Canada: 1.9% The Netherlands: 5.3%The USA: 5.0%
German (German Heal th Interview and Examination Survey, GHS)
Jacobi, et al. /2004 Genera l adu l t popu la t ion (n=4,181), DSM-IV
87.6% 4-week prevalence 1.2%12-month prevalence 1.5%
Spain, Italy, Germany, Neth-erlands, Belgium and France. (European Study of the Epi-demiology of Mental Disor-ders [ESEMeD])
Alonso, et al. /2004 A representive random sample of non-institutionalized in-habitats (n=21,425), Composite International Diagnostic Inter-view 3.0
61.2% 12-month prevalence: 1.0% (male 0.5%; female 1.3%)
Lifetime prevalence: 2.8% (male 2.0%; female 3.6%)
The USA (National Epide-miologic Survey on Alcohol and Re la t ed Cond i t ions [NESARC])
Grant, et al. /2005 Genera l adu l t popu la t ion (n=43,093), DSM-IV
81% 12-month prevalence 2.1% Lifetime prevalence 4.1%
Denmark, Finland, Norway, and Sweden
Munk-Jorgensen, et al. / 2006
8,879 patients in general prac-tice; 648 general practitioners, DSM-IV
– Males 4.8%Females 6.0%(Only 1/3 to 1/2 of the GAD caseswere identified by the general practi-tioners)
Hong-Kong Lee, Tsang, Chui, Kwok, & Cheung, /2007
General adult population in Asian communities (n=3,304), DSM-IV
65.8% 6-month prevalence 4.1%
Korea Cho, et al. /2007 Genera l adu l t popu la t ion (n=6,275), DSM-IV
79.8% 12-month prevalence 1.0%Lifetime prevalence 2.3%
Czech Republic Csémy/2011 Adult Czech citizens (n=3,244),The Mini International Neuro-psychiatric Interview (M.I.N.I.)
– Prevalence 3.6%(males 3.0%; females 4.2%)
3. Background, characteristics, and help-seekingbehaviours(1) Historical background and characteristics
This diagnosis, GAD, first appeared in 1975 and the criteria have changed over time (Goldberg, et al. 2010), suggesting that the disease concept has been evolving. Initially, the time required for the symptoms to persist was only 2 weeks but was changed to 1 month in the DSM III (1980), 6 months in the DSM III-R (1987) and DSM
IV-R (2000). In terms of symptoms, one out of five per-sistent generalized anxiety moods was required in 1975. The diagnostic criteria were changed again in the DSM III; 43 symptoms were divided into four categories (motor tensions, autonomic hyperactivity, apprehensive expecta-tion, and vigilance) and three categories were required. The DSM III-R required only 6 symptoms and added the concept of "unrealistic worry". The DSM IV and DSM IV-R required only 3 out of 6 symptoms and added the

精神衛生護理雜誌 7卷1期.中華民國101年10月
4 Nursing Reflections of Generalized Anxiety Disorder
concept of “the person finds it difficult to control the worry”. Clinical features included emotional (anxiety), cognitive (uncontrollable worry, poor concentration), somatic (muscle tension, autonomic symptoms, somatic preoccupations), and behavioural symptoms (irritability, restlessness) (Grant, et al. 2005). Responding to the revi-sions in the DSM V, Goldberg, et al. (2010) stated that making nosological decisions is like setting social policy in many ways. The possibility of taking GAD out from under the umbrella of "anxiety disorder" is considered in order, for example, to combine GAD with major depres-sion and form a category "Distress disorder". However, consideration of more than the scientific facts is needed, as the consequences of creating a new diagnosis or mak-ing a change in DSM nosology are huge (Beesdo-Baum, et al., 2011).
Other features of GAD are early onset (usually in adolescence) (Sadock & Sadock, 2007) and gender dif-ference (female to male ratio, 2 to 1) (湯&葉, 2003). Co-morbidity is an important issue of GAD. Analysis of rates and odds ratios (ORs) of GAD comorbidities in Taiwan identified phobia (14%), major depression (6.8%), minor depression (5.5%), and panic disorder (3.8%) as the most frequent co-morbid diseases (湯&葉, 2003). Finally, cul-tural factors play a vital role, i.e., they influence somatic symptoms or cognitive symptoms or whether worries about certain situations are excessive (DSM IV-R 2000, p. 473).
(2) Help-seeking behavioursOver 80–90% of GAD patients in Taiwan, like GAD
patients in western countries, fail to seek help (Wittchen, 2002; Bandelow, 2003). Moreover, when Taiwanese patients do seek help, most of them seek western medi-cal treatment (the rate of utilization of western medical resources being several times higher than that for other resources). For patients with depression, rates of help-seeking behaviour are similar regardless of residence in cities, suburbs, or rural areas (葉&林, 2006).
湯&葉(2003) reported that the rate of psychotherapy use is low (only 3.4% in Taipei, 1.48% in Shu-Lin and 0% in Tsao-Tun). On the other hand, the rate of folk therapy use was equal to or much higher than that of psy-chotherapy use (3.4% in Taipei, 7.1% in Shu-Lin and 3.0%
in Tsao-Tun). Poor accessibility to psychotherapy and lack of familiarity with psychological approaches rooted in western culture may account for this disparity (葉 & 林, 2006).
4. TreatmentDue to the accessibility and the rapid development of
psychiatric pharmacology, pharmacotherapy has become commonplace (Feltner, Wittchen, Kavoussi, Brock, et al., 2008). Mitte, Noack, Steil, & Hautzinger (2005) conducted a meta-analysis (n>12,000) that examined the efficacy of the pharmacological treatment of GAD with over 26 drugs and concluded that pharmacotherapy was superior to placebo in all symptom categories. However, the disadvantage of pharmacotherapy was its side effects, including anticholinergic effects, gastrointestinal distress, and sexual side effects for selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) (Mitte, Noack, Steil, & Hautzinger, 2005). Moreover, patients who respond to pharmacologic treatment can still exhibit subsyndromal symptoms that predispose them to relapse. GAD is a chronic condition that may be lifelong (Sadock & Sadock, 2007). Therefore, it is vital for nurses to meet the health care needs of patients with GAD.
Cognitive-behavioural treatment (CBT) is the most common anxiety disorder treatment (Norton & Price, 2007). The overall goal of CBT is to teach coping skills that encourage an active, problem-solving approach to stressful events and a greater tolerance to (or acceptance of) anxiety symptoms (Durham, 2004). Meta-analyses of studies that examined the efficacy of CBT on GAD have reported effect sizes between 0.21 and 1.80 and three of them reported effect sizes of around 0.70, indicating fairly good efficacy of CBT for anxiety disorders (Hunot, Churchill, Teixeira & Silva de Lima, 2007; Wells & King, 2006; Roemer & Orsillo, 2007; Hofmann & Smits, 2008). To conclude, CBT can benefit most patients with anxiety disorders.
In addition to the most common western treatments mentioned above, alternative therapies may benefit GAD patients as they fit into the socio-cultural context of the Far East (DSM IV-R, 2000, p. 474) and have no side

精神衛生護理雜誌 7卷1期.中華民國101年10月
廣泛性焦慮症照護反思 5
effects (Lakhan & Vieira, 2010). These therapies include nutritional, herbal supplements, therapeutic massage, and various types of meditation, i.e., Zen and mindfulness meditation (Lakhan & Vieira, 2010; Krisanaprakornkit, Krisanaprakornkit, Piyavhatkul, & Laopaiboon, 2008; Kavan, Elsasser & Barone, 2009; Sherman, Ludman, Cook, Hawkes, et al., 2010). The selection of the most appropriate therapies should take into consideration patient preference, prior success with using alternative therapies, and factors that could affect adherence and subsequent effectiveness (Kavan, et al., 2009).
5. PrognosisGAD is a chronic, fluctuating illness that often
worsens during times of stress (DSM-IV, 2000, p. 474). It is associated with significant morbidity and long-term treatment (Katzman, 2009). Studies pointed out several factors that are associated with poor long-term outcome: co-morbid anxiety and depressive disorders combined with personality disorders, high symptom severity, poor social adjustment, low socioeconomic status, and unemployment (Durham,2004; Cairney, Corna, Veldhuizen, Kurdyak & Streiner, 2008). The remission rates are only 40% (Rickels & Rynn, 2002) or, in young adults, around 50% over a 20-year follow-up period (Angst, Gamma, Baldwin, Ajdacic-Gross & Rössler, 2009).
Nursing care for patients with GAD
With the current knowledge of GAD in mind, the discussion of nursing interventions starts with traditional
concepts of nursing care, then the necessity of assessing depressive mood, considering the positive beliefs about worry held by patients, and how they learn to live with GAD.
1. The traditional concepts of nursing care forpatients with GAD
Nursing interventions for patients with GAD are not obviously different from that for other anxiety disorders. This is likely because anxiety is the basis of both GAD and other anxiety disorders, and this idea is supported by a genetic study (Goldberg, et al., 2010). Tradition-ally, nursing interventions aim to comfort or relieve the distress of anxious patients. The principles and practices are summarized in Table 2. Nursing strategies to eliminate anxiety have been developed systematically (Stuart & Laraia, 2008).
2. The necessity of assessment of depressive moodAlthough anxiety and responses to fear are regarded
as core problems in patients, it is important to be aware of depressive mood. This is because co-morbidity is a key feature of GAD and major depression is one of the most common GAD-associated mental disorders (Kessler, et al., 2002; Bandelow, 2003; Grant, et al., 2005; Katzman, 2009). The familial aggregation and genetics study of Goldberg, et al. (2010) indicates that major depression and GAD share some genetic risk factors. This evidence was used to create a new category "Distress disorder" for the combination of GAD with major depression in the latest version of the DSM in the USA (i.e., DSM V; Gold-berg, et al., 2010).
Table 2 Nursing interventions for patients with GADPrinciples Examples of practices Recognition of anxiety lAssess anxiety symptoms and behaviours.
lHelp patients to describe and to identify fear-related symptoms or behaviours.
Insight into anxiety lBy linking the threats to situations or underlying causes, learn which values are being threat-ened.
Coping with the worry lEncourage patients to use the previous coping strategies that have been constructive.lHelp patients problem solve by applying cognitive and behavioural concepts, i.e., monitoring
thoughts and feelings.
Promotion of relaxation responses using various methods
lExplore with patients individual ways to produce a relaxation response so that the feeling of control can be regained.
lIn addition to conventional muscle relaxation methods, apply alternative therapies, such as massage, herbal supplementation, and meditation.

精神衛生護理雜誌 7卷1期.中華民國101年10月
6 Nursing Reflections of Generalized Anxiety Disorder
Therefore, it is clear that depression and GAD co-exist in many individuals, and failure to recognize them as closely related entities may delay provision of the appropriate intervention. That is, concepts of depression should be integrated into the nursing care of GAD. Thus, symptoms such as loss of pleasure, depressive mood, and low self-esteem and, most important, self-harm and sui-cidal behaviours should be carefully assessed.
3. Consideration of the positive beliefs about worryheld by patients
Worry as the cardinal symptom of GAD (Covin, Quimet, Seeds & Dozois, 2008) first appeared in the DSM III-R. A cognitive model can be used to interpret the rationales for worries held by GAD patients (Du-gas & Robichaud, 2007). They reported positive beliefs regarding worry. Thus, worry can be a means to prevent or minimize negative outcomes (negative reinforcement) and a positive action for finding a solution to a problem (positive reinforcement). Dugas & Robichaud (2007) sug-gested that these beliefs play a role in the development and maintenance of GAD.
Interestingly, these findings can be easily understood and widely accepted by Taiwanese people inasmuch as the idea of “being prepared for unexpected situations” is a virtue. In the Analects of Confucius, the adage "The person has no foresight, having the immediate worries necessarily", is recognized by our society and is the basis of our compulsory education system (Ames, 1999).
These findings apply to nursing care in two respects. Firstly, nurses need to clarify the extent to which patients with GAD believe “worry is foresight” and how this af-fects their behaviour. Secondly, nurses need to examine the advantages and disadvantages of these beliefs and their relationship to the symptoms of GAD. In other words, nurses can help patients develop insight into assumptions that reinforce worrying.
4. Learning to live with GADBecause GAD tends to be chronic, the inevitable les-
son for patients with GAD is to learn to live with anxiety. First, as nurses we need to be aware that pathology is
the basis of medicine and psychology. For example, the purpose of all types of anxiety scales is to measure anxi-ety severity and impairment. Decrease in anxiety score is an indicator of symptomatic improvement (Covin, et al., 2008; Arbabzadeh-Bouchez & Lepine, 2003). Con-sequently, without that awareness, we are led to treat anxiety with negative notions only.
However, nurses need to challenge the notion that anxiety or worry is a negative concept. Influenced by Tai-wanese culture, our perspective may differ from the per-spective of pathology. That is, the negative idea of worry should be re-considered.
On the other hand, the positive qualities of patients with GAD such as thoughtfulness and the pursuit of excellence should be recognized as these contribute to their work and benefit their families in some ways (May, 1977). By recognition of these qualities as virtues, nurses can provide positive feedback to patients with GAD. Thus, patients can be empowered to live with GAD in a healthier, more productive manner especially when they no longer expect to be cured.
Summary
GAD is the most common mental disorder, yet ex-posure to GAD in the nursing curriculum is inadequate in Taiwan. Although treatments of GAD have improved considerably over the last decade, patients with GAD still suffer chronically and are subject to recurrent episodes (Bandelow, Wedekind & Leon, 2007; Goldberg et al., 2010). Therefore, understanding GAD from a nursing perspective is crucial, particularly when GAD does not seem to be curable. Nurses are concerned with not only cure, but also how to apply the current knowledge to the “life” of patients with GAD. This article discusses anxiety management in relation to traditional notions of anxiety, medical treatment, and cognitive behaviour therapy. Moreover, assessment of depressive mood and identifica-tion of the positive characteristics of GAD based on Tai-wanese culture are addressed.
精神衛生護理雜誌 7卷1期.中華民國101年10月
廣泛性焦慮症照護反思 7
References
Alonso, J., Angermeyer, M. C., Bernert, S., Bruffaerts, R., Brugha, T. S., Bryson, H., Vollebergh, P. (2004). Preva-lence of mental disorders in Europe: results from the Euro-pean Study of the Epidemiology of Mental Disorders (ES-EMeD) project. Acta Psychiatrica Scandinavica, 109(420), 21-27. doi:10.1111/j.1600-0047.2004.00327.x
Ames, R. T. (1999). Analects of Confucius. Taipei, Taiwan: Bal-lantine Books.
American Psychiatric Association (2000). Diagnostic and
Statistical Manual of Mental Disorders, 4th ed. Text
Revision (DSM-IV-TR®). Washington, DC: American Psychiatric Association.
Angst, J., Gamma, A., Baldwin, D. S., Ajdacic-Gross, V. & Rössler, W. (2009). The generalized anxiety spectrum: prevalence, onset, course and outcome. European Archives
of Psychiatry and Clinical Neuroscience, 259(1), 37-45. doi: 10.1007/s00406-008-0832-9
Antai-Otang, D. (2003). Anxiety disorders: treatment considerations. Nursing Clinics of North America, 38(1), 35-44.
Arbabzadeh-Bouchez, S. & Lepine J. P. (2003). Measurements of depression and anxiety disorders. In Kasper S., Den Boer J. A. & Sitsen, J. M. (eds.) Handbook of Depression
and Anxiety-Revised and Expanded 2nd ed. (pp. 127-150). New York, NY: Marcel Dekker.
Bandelow, B. (2003). Epidemiology of depression and anxiety. In S. Kasper & J.A.Den Boer & J.M.Sitsen (eds.) Hand-
book of Depression and Anxiety 2nd ed. Revised and Ex-
panded (pp. 49-68). New York, NY: Marcel Dekker.Bandelow, B., Wedekind, D. & Leon, T. (2007). Pregabalin
for the treatment of generalized anxiety disorder: a novel pharmacologic intervention. Expert Review of
Neurotherapeutics, 7(7), 769-781. doi:10.1586/14737175.7.7.769
Beesdo-Baum, K., Winkel, S., Pine, D. S., Hoyer, J., Höfler, M., Lieb, R., & Wittchen, H. (2011). The diagnostic threshold of generalized anxiety disorder in the community: A developmental perspective. Journal of Psychiatric
Research, 45(7), 962-972. doi: S0022-3956(10)00348-1Cairney, J., Corna, L.M., Veldhuizen, S., Kurdyak, P., &
Streiner, D. L. (2008). The social epidemiology of affective
and anxiety disorders in later life in Canada. The Canadian
Journal of Psychiatry, 53(2), 104-111.
Chien, I. C., Chou, Y. J., Lin, C. H., Bih, S. H., Chou, P. (2004). Prevalence of psychiatric disorders among National Health Insurance enrollees in Taiwan. Psychiatric Services, 55(6), 691-697. doi:10.1176/appi.ps.55.6.691
Cho, M. J., Kim J. K., Jeon, H. J., Suh, T., Chung, I. W., Hong, J. P., Bae, J. N. (2007). Lifetime and 12-month prevalence of DSM-IV psychiatric disorders among Korean adults. Journal of Nervous & Mental Disease, 195(3), 203-210. doi:10.1097/01.nmd.0000243826.40732.45
Covin, R., Ouimet, A. J., & Seeds, P. M. & Dozois, D. J. A. (2008). A meta-analysis of CBT for pathological worry among clients with GAD. Journal of Anxiety Disorders,
22,108-116. doi:10.1016/j.janxdis,2007.01.002Csémy, L. L. (2011). Epidemiology of generalized anxiety
disorder (GAD) and other anxiety disorders in the Czech Republic. European Psychiatry, 26(1), 524. doi:10.1016/S0924-9338(11)72231-3
Dugas, M. & Robichaud, M. (2007). Cognitive-behavioural
Treatment for Generalized Anxiety Disorder: From Science
to Practice. New York, NY: Routledge.Durham, R. (2004). Treatment of generalized anxiety
disorder. Psychiatry, 6(5), 183-187 . doi:10.1016/j.mppsy.2007.03.003
Feltner, D., Wittchen, H.U., Kavoussi, R., Brock, J., Baldinetti, F. & Pande, A.C. (2008). Long-term efficacy of pregabalin in generalized anxiety disorder. International Clinical
Psychopharmacology, 23(1), 18-28. doi:10.1097/YIC.0b013e3282f0f0d7
Goldberg, D., Regier, D.A., Kendler, K. S. & Sirovatka, P. J. (2010). Diagnostic Issues in Depression and Generalized
Anxiety Disorder: Refining the Research Agenda for
DSM-V. Arlington, VA: American Psychiatric Association.Grant, B. F., Hasin, D. S., Stinson, F. S., Dawson, D. A., June,
R. W., Goldstein, R. B… Smith, S. M. (2005). Prevalence, correlates, co-morbidity, and comparative disability of DSM-IV generalized anxiety disorder in the USA: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Psychological Medicine, 35(12), 1747-1759. doi:10.1017/S0033291705006069
Hofmann, S. G. & Smits J. A. J. (2008). Cognitive-behavioral therapy for adult anxiety disorders: A meta-analysis of
精神衛生護理雜誌 7卷1期.中華民國101年10月
8 Nursing Reflections of Generalized Anxiety Disorder
randomized placebo-controlled trials. Journal of Clinical
Psychiatry, 69(4), 621-632.Hunot, V., Churchill, R., Teixeira, V. & Silva de Lima M. (2007).
Psychotherapies for generalized anxiety disorder. Co-
chrane Database of Systemic Reviews. Issue 1: 1-24.Hwu, H. G., Yeh, E. K., & Chang, L. Y. (1989). Prevalence of
psychiatric disorders in Taiwan defined by the Chinese Diagnostic Interview Schedule. Acta Psychiatric
Scandanavia, 79, 136-147. Doi:10.1111/j.1600-0447.1989.tb08581.x
Jacobi, F., Wittchen, H., Holting, C., Sommer, S., Lieb, R., Hofler, M., & Pfister, H. (2004). Prevalence, co-morbidity and correlates of mental disorders in the general population, results from the German Health Interview and Examination Survey (GHS). Psychological Medicine 34,
597-611. doi:10.1017/S0033291703001399Kavan, M., Elsasser, G., & Barone, E. (2009). Generalized
anxiety disorder: practical assessment and management. American Family Physician, 79(9), 785-791.
Katzman, M. (2009). Current considerations in the treatment of generalized anxiety disorder. CNS Drugs, 23(2), 103-120. doi:10.2165/00023210-200923020-00002
Kessler, R. C., (2007). The global burden of anxiety and mood disorders, Putting the European Study of the Epidemiology of Mental Disorders (ESEMeD) findings into perspective. Journal of Clinical Psychiatry 68 (Supplement 2), 10-19.
Kessler, R. C., Andrade L. H., Bijl R. V., Offord D. R., Demler, O. V., & Stein D. J., (2002). The effects of co-morbidity on the onset and persistence of generalized anxiety disorder in the ICPE surveys. Psychological Medicine, 32(7), 1213-1225.
Krisanaprakornkit, T., Krisanaprakornkit, W., Piyavhatkul, N. & Laopaiboon, M. (2008). Meditation therapy for anxiety disorders. Cochrane Database of Systematic Reviews no. 1. doi: 10.1002/14651858.CD004998.pub2
Lakhan, S., & Vieira, K. (2010). Nutritional and herbal supplements for anxiety and anxiety-related disorders: systematic review. Nutrition Journal, 9: 42. doi:10.1186/1475-2891-9-42
Lee, S., Tsang, A., Chui, H., Kwok, K., & Cheung, E. (2007). A community epidemiological survey of generalized anxiety disorder in Hong Kong. Community Mental Health
Journal, 43(4), 305-19. doi:10.1007/s10597-006-9077-0
Lepine, J. P. (2002). The epidemiology of anxiety disorders, Prevalence and societal costs. Journal of Clinical
Psychiatry, 63(Supplement 14), 4-8. May, R. (1977). The Meaning of Anxiety (rev. ed.). New York,
NY: Norton. pp, 218-236.Mitte, K., Noack, P., Steil, R., & Hautzinger. M. (2005). A
meta-analytic review of the efficacy of drug treatment in generalized anxiety disorder. Journal of Clinical
Psychopharmacology, 25(2), 141-150. doi:10.1097/01.jcp.0000155821.74832.f9
Munk-Jorgensen, P., Allgulander, C., Dahl, A. A., Foldager, L., Holm, M., Rasmussen, I, Virta, (2006). Prevalence of generalized anxiety disorder in general practice in Denmark, Finland, Norway, and Sweden. Psychiatric
Serv ices , 57 (12) , 1738-1744. doi :10 .1176/appi .ps.57.12.1738
Norton, P. J., & Price, E. C. (2007). A meta-Analytic Review of Adult Cognitive- Behavioral Treatment Outcome across the Anxiety Disorders. The Journal of Nervous
and Mental Disease, 195, 521-531. doi:10.1097/01.nmd.0000253843.70149.9a
Rickels, K. & Rynn, M. (2002) Pharmacotherapy of generalized anxiety disorder. Journal of Cl inical Psychiatry
63(Suppliment14), 9-16.Roemer, L. & Orsillo S. M. (2007). An open trial of an
acceptance-based behavior therapy for generalized anxiety disorder. Behavior Therapy 38(1), 72-85. doi:10.1016/j.beth.2006.04.004
Sadock, B. J. & Sadock, V. A. (2007). Synopsis of Psychiatry:
Behavioural Sciences/Clinical Psychiatry (10th ed.) (pp, 634). Philadelphia, PA: Lippincott William & Wilkins.
Sherman, K., Ludman, E., Cook, A., Hawkes, R., Roy-Byrne, P., Bentley, S., ... Cherkin, D. (2010). Effectiveness of therapeutic massage for generalized anxiety disorder: a randomized controlled trial. Depression and Anxiety, 27(5), 441-450.
Stuart, G. W., & Laraia, M. T. (2008). Principles and Practice of
Psychiatric Nursing (9th ed.). St. Louis, Missouri: Mosby. doi:10.1002/da.20671
Wells, A. & King, P. (2006). Metacognitive therapy for generalized anxiety disorder: An open trial. Journal of
Behavior Therapy and Experimental Psychiatry 37(3), 206-212. doi:10.1016/j.jbtep.2005.07.002
精神衛生護理雜誌 7卷1期.中華民國101年10月
廣泛性焦慮症照護反思 9
Wittchen, H. U. (2002). General anxiety disorder, prevalence, burden, and cost to society. Depression and Anxiety, 16(4),
162-171. doi:10.1002/da.10065湯華盛、葉英堃(2003).泛焦慮症之社區流行病學.當
代醫學,30(2),119-126。
葉雅馨、林家興(2006).臺灣民眾憂鬱程度與求助
行為的調查研究.中華心理衛生學刊 ,1 9(2),
125-148。
精神衛生護理雜誌 7卷1期.中華民國101年10月
10 Nursing Reflections of Generalized Anxiety Disorder
廣泛性焦慮症新知與有效性護理照護反思
呂雀芬1 陳妙絹2 許世杰3
摘 要: 護理教育中對焦慮疾患的認識,一直是以一個綜合的概念被介紹或以一個涵括式的視框來理解,其中個別疾患的認識是相對模糊的。焦慮疾患中盛行率最高者是廣泛性焦慮症(GAD),因此值得對其有更清楚的認識,以便
提供護理給這佔大多數個案的精神衛生需求。本文以廣泛性焦慮症為範疇,介紹其盛行率、花費、歷史背景、病
因、症狀表現、求醫行為、治療及預後,也包含將於2012年出版的DSM-V對GAD疾病分類之觀點。本文旨在藉對
新知的理解與討論,來思考如何可以是一個適切的護理措施。亦即,儘管藥物治療有長足進步,或是認知行為治
療指出其效能具顯著差異,然而並非所有的人都能受益,GAD仍具有慢性化特性。且因其共病性的特質,護理師
對焦慮症患者情緒表現,特別是憂鬱狀態,應具備敏感的覺察。然,更重要的是,護理本身對「焦慮」之價值觀
為何或立場必須有所思辨。如當我們從病理的角度來看待焦慮,則引發了以減低或消除焦慮的類醫療價值觀之護
理態度。以全人關懷為範疇的護理專業並不等同於醫學哲學。在醫學框架之外,精神衛生護理應尋找多元的角度
來理解或論述焦慮,也是護理之獨特性,例如從文化,而使患者的賦能以及與病和諧共存有所可能。
關鍵詞: 廣泛性焦慮症、護理處置、反思。
1長庚科技大學副教授 2長庚科技大學講師 3長庚醫院主治醫師
受文日期:100年8月19日 接受刊載:101年6月28日
通訊作者地址:呂雀芬 33303桃園縣龜山鄉文化一路261號
電 話:(03)2118999—3441
Related Documents