An in vitro investigation of meticillin resistant Staphylococcus aureus (MRSA) decolonisation treatment failure Dr Sue Lang

An in vitro investigation of meticillin resistant Staphylococcus aureus (MRSA) decolonisation treatment failure Dr Sue Lang.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

An in vitro investigation of meticillin resistant Staphylococcus aureus (MRSA) decolonisation
treatment failure
Dr Sue Lang

Staphylococcus aureus infections in Scotland
• Large reductions in MRSA bacteraemia since 2006, MSSA rates have remained largely unchanged
Healthcare Associated Infection Annual Report 2013

A need to decolonise?• Decolonisation; treatment to eradicate S. aureus colonisation• An infection prevention measure:
– Nasal colonisation with MRSA is the single most important determinant of subsequent MRSA infections (Nguyen et al., 1999)
– The risk of infection in nasal carriers of MRSA is estimated to be 15 times higher than in those who are not colonised (HPS Pathfinder 2009)
– Reduce cross transmission
• Pre-surgical decolonization has lead to reduction in infection of:– Surgical patients eg cardiothoracic: 58% decrease– Haemodialysis and peritoneal dialysis patients: decrease up to
80%

Decolonisation strategy
• Intra nasal application of mupirocin alone or in combination with use of antiseptic soaps or systemic antimicrobial agents– 2% mupirocin for nasal carriage and
chlorhexidine wash for skin carriage for 5 days
– If skin lesions present add in systemic antibiotic for 7 days
• Elimination from nares (VN) results in disappearance from other sites

S. aureus colonisation• 30% of healthy adults are
colonised with S. aureus– 20% persistently colonised– 30% intermittently
colonised– 50% non-carriers
• High carriage in:– Hospitalised patients– IVDA– Insulin-dependant diabetics– HIV positives– Haemodialysis patients

Decolonisation strategy• Short term decolonisation may be sufficient
– Prior to surgery• Post-operative S. aureus infection rate of 3.4%
(decolonised of S. aureus) vs 7.7% in control group (Bode et al., 2010)
• Mupirocin ointment has been shown to be 97% effective in temporarily decolonising S. aureus nasal carriers (Wertheim, 2005)
• Long term desirable– Patients frequently attending healthcare facilities,
eg undergoing dialysis
Mupirocin• Mupirocin available as a nasal ointment, Bactroban • Mixture of pseudomonic acids produced by
Pseudomonas fluorescens• Consists of 90% pseudomonic acid A and structurally
different to any other clinically relevant antibiotic
• Prevents bacterial protein synthesis by inhibiting the bacterial isoleucyl-tRNA synthetase (IleRS)

Resistance to mupirocin
• Low level resistance (LLR); MIC of 8-256mg/L– Conferred by mutations in native
isoleucine synthetase– Implicated in relapse after
treatment (Lee et al., 2011)
• High level resistance (HLR); MIC >512mg/L– Conferred by mupA; encodes an
additional isoleucine synthetase (IRS) enzyme
– mupA carriage has been associated with multi-drug resistance and decolonisation failure
LLR HLR
EUCAST database 07.11.14

Resistance to mupirocin
• 2009 – 2012; mupirocin use has slightly decreased• Resistance rates have not yet been seen to increase
Healthcare Associated Infection Annual Report 2013

Shortcomings of mupirocin decolonisation
• The current decolonisation regime may not be fit for purpose– The median length of stay is 3-4 days for all MRSA
colonised patient admissions (HPS, 2011)
– Only 3.1% of patients completed decolonisation treatment (HPS, 2011)
– 10 days median time for successful decolonisation (Ammerlan et al., 2011)

Shortcomings of mupirocin decolonisation
• MRSA decolonisation isn’t always successful:– Successful for 62% of patients with mupirocin sensitive
strains (mupS), 29% of cases with LLR, 24% of cases with HLR
• One eradication attempt may not be sufficient– Eradication achieved in 60% of patients with only one
decolonisation attempt– Increased to 80% with multiple attempts (Ammerlan et al.,
2011)
• Success rate is over estimated– Relapse is thought to occur at high rate– 38% re-colonisation after 6 months (Coates et al., 2009)

Shortcomings of mupirocin decolonisation
• Driver for the development of resistance– Patients previously exposed to mupirocin have a
substantially increased risk of mupirocin resistant MRSA
• Resistance to mupirocin complicates decolonisation– After initial success, only 25% of patients with LLR
remained culture-negative at 4 weeks (Coates et al., 2009)
– When patients do present with resistant strains often the correct treatment is not administered (Howard and Morris, 2012)
– LLR and qacA/B has been associated with decolonisation failure at 12 months

Aim of the study
To investigate mupirocin decolonisation treatment failure
1. Biofilm-related tolerance2. Low level resistance (LLR) to
mupirocin (Mup)3. Antibiotic induced stress
(Stringent Response)

1. Efficacy of Mup on biofilm-associated cells
LIVE/DEAD® staining of MupS 177 biofilms. A) without Mup treatment, B) 30 min exposure to 200mg/l Mup
Control
1 x
MIC
4 x
MIC
10 x
MIC
100
x M
IC
200m
g/l0
50
100
150
n=12error bars SEMMup concentration
Cel
l sur
viva
l (%
of
untr
eate
d co
ntro
l)
A B
• Despite exposure to concentrations of Mup greatly in excess of the MIC, a substantial proportion of cells remained metabolically active

189
190
194
195
196
0
25
50
75
1004 x MIC10 x MIC
200 mg/l
MSSA
Ce
ll S
urv
ival
(%
of
con
tro
l)
1. Efficacy of Mup on biofilm-associated cells
• Tolerance of biofilm-associated S. aureus cells was consistent between strains
Error bars SEM
1. Efficacy of Mup on biofilm-associated cells
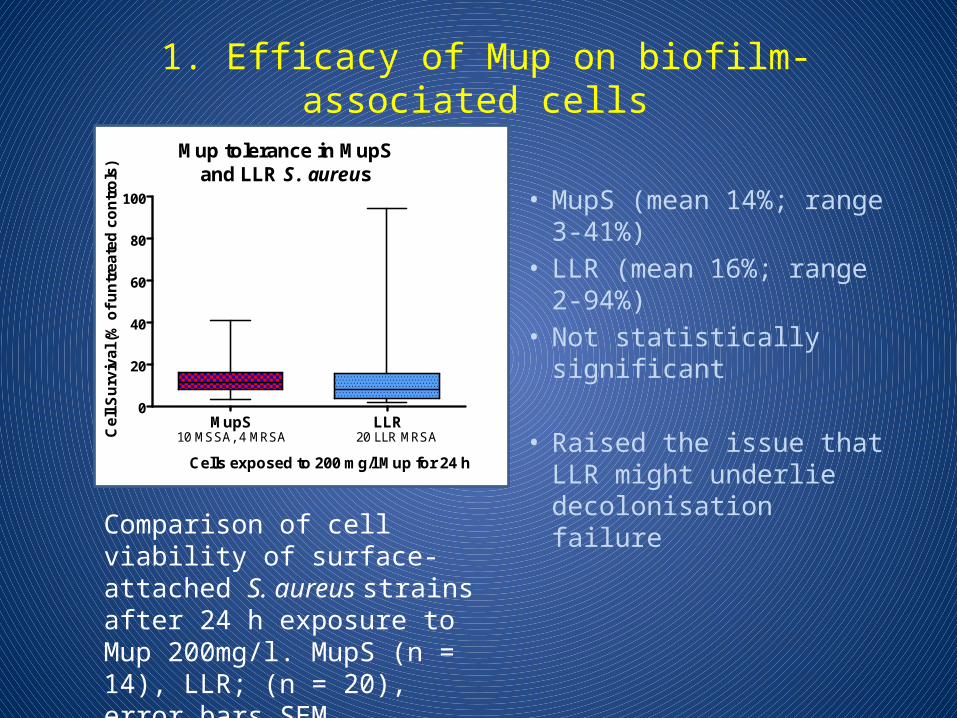
• MupS (mean 14%; range 3-41%)
• LLR (mean 16%; range 2-94%)
• Not statistically significant
• Raised the issue that LLR might underlie decolonisation failure
Comparison of cell viability of surface-attached S. aureus strains after 24 h exposure to Mup 200mg/l. MupS (n = 14), LLR; (n = 20), error bars SEM
MupS LLR0
20
40
60
80
100
Mup tolerance in MupSand LLR S. aureus
Cells exposed to 200 mg/l Mup for 24 h
10 MSSA, 4 MRSA 20 LLR MRSACe
ll S
urv
iva
l (%
of
un
tre
ate
d c
on
tro
ls)

2. Efficacy of Mup on LLR strains• 35 clinical isolates of S. aureus
– 14 MupS (4 MRSA, 10 MSSA) and 21 LLR (20 MRSA, 1 MSSA)• S. aureus attached to wells coated with 0.25% mucin to mimic
colonisation– 1 x 105 cfu/mucin coated well incubated for 4 h at 37C on a rocking
platform to allow attachment• Exposure to Mup 200mg/l
– (at least 6-fold above the MIC for all strains) for 1, 4, 6, 12 and 24 h• Cell viability determined by incubation with the metabolic dye
resazurin– Fluorogenic product recorded as an indirect measure of cell viability
• Antibiotic induced inhibition and cell recovery evaluated over a time period of 24 h– Viability of untreated and treated surface-attached cells compared in
triplicate

MRSA 5
0
MRSA 1
44
MRSA 1
77
MSSA 1
87
MSSA 1
88
MSSA 1
890
20
40
60
Ce
ll s
urv
iva
l (%
of
un
tre
ate
d c
on
tro
ls)
1 h4 h6 h12 h24 h
2. Exposure of MupS strains to Mup
• All the MupS strains showed a loss in cell viability proportionate to exposure time
MupS cell viability as a percentage of untreated controls after exposure of surface-attached cells to Mup 200 mg/l for 1, 4, 6, 12, or 24 h, error bars represent SEM - 6 representative strains shown

0
20
40
60
12 h
1 h4 h6 h
24 h
Ce
ll v
iab
ilit
y (
% o
f u
ntr
ea
ted
co
ntr
ol)
2. Exposure of LLR strains to MupOf the 21 LLR strains;• 9/21 showed a decrease in
viability comparable to the MupS isolates (not shown)
• 6/21 LLR showed a significant recovery in cell number after 12 h exposure following an initial reduction (p <0.05) (LLR mean 36% cell survival; range 28 – 44% vs. MupS mean 24% cell survival, range 12 – 22%)
LLR cell viability as a percentage of untreated controls after exposure of surface-attached cells to Mup 200 mg/l for 1, 4, 6, 12, or 24 h, error bars represent SEM

2. Exposure of LLR strains to MupOf the 21 LLR strains;• 6/21 LLR strains, there
was a statistically significant cell recovery observed after 24 h exposure to Mup; LLR mean 105%; 20 – 286% vs. MupS mean 14%, 3 – 41% (p<0.05)
• The observed tolerance to Mup was genotype independent (data not shown)
LLR 100
LLR 205
LLR 206
LLR 4
LLR 13
LLR 15
0
20
40
60
100150200250300
1 h
4 h
6 h
12 h
24 h
Cel
l Su
rviv
al (
% o
f u
ntr
eate
d c
on
tro
l)
LLR cell viability as a percentage of untreated controls after exposure of surface-attached cells to Mup 200 mg/l for 1, 4, 6, 12, or 24 h, error bars represent SEM

2. Repeated exposure mimicking treatment
• Three surface adherent strains challenged with 200 mg/L Mup for 1 h twice a day for 5 days mimicking treatment
• After treatment cells were allowed to recover in antibiotic free broth for 11 h prior to the next treatment
• Cell viability was recorded and the extent of recovery between treatments determined
T = sampling point after 1 h Mup exposure, every 12 h for 5 days

T0T1 T2 T3 T4 T5 T6 T7 T8 T9
T101.0105
1.0106
1.0107
1.0108
1.0109
Mupirocin (Exposure time points)
Nu
mb
er o
f ce
lls (
cfu
/ml)
T0T1 T2 T3 T4 T5 T6 T7 T8 T9
T101.0105
1.0106
1.0107
1.0108
1.0109
Mupirocin (Exposure time points)
2. Repeated exposure mimicking treatment
S. aureus cell numbers as a percentage of untreated controls after repeated exposure of surface-attached cells to Mup 200 mg/l, black untreated, blue treated, error bars SEM
• After 5 days the viable cell number of the MS strain was reduced to 15% of the control, whereas for the two LLR strains 20% and 39% of cells remained compared to untreated cultures, though this did not reach statistical significance
MupS 177 LLR 17 LLR 206
T0T1 T2 T3 T4 T5 T6 T7 T8 T9
T101.0105
1.0106
1.0107
1.0108
1.0109
Mupirocin (Exposure time points)

3. Antibiotic induced stress - Stringent Response
• Antibiotic tolerant bacteria can resist cell killing but are not resistant
• Environmental stresses can provoke a stress phenomenon in bacterial cells termed the Stringent Response
• Hallmark of response – small molecule alarmones, pppGpp and ppGpp
• Bifunctional RelA synthetase (S)/hydrolase (H) enzyme

3. Antibiotic induced stress - Stringent Response
Global cellular reprogramming
↓ rRNA synthesis ↓ anabolic processes
↑ amino acid biosynthesis
↑ stress survival genes
U A C
Bacteriostatic
Pi Pi
GTPATP
RelA synthetase
ppGpp
GDP
pppGpp
RelA hydrolase PPi
GTP poolsDe-represses CodY
(transcriptional repressor)
Ribosome
E P A
3’
5’
SH
SH
RelA
Summary• Binding of S. aureus to a mucin-coated surface confers
tolerance to mupirocin
• LLR conveys an increased level of tolerance after single dose and repeated exposures to mupirocin
• The in vitro tolerance to mupirocin observed in LLR strains might underlie the higher rate of relapse following decolonisation therapy
• The impact of a mupirocin-induced Stringent Response on decolonisation therapy remains to be fully determined

Acknowledgements
Andrew AnyakwoDr Lesley PriceDr Kirsty Skinner
Dr Liz Dickson, Scottish MRSA Reference Laboratory, GRI
Related Documents











